CADTH Health Technology Review
Virtual Care Rapid Scoping: Main Report
Scoping Review
Acknowledgements
Authors
Chantelle C. Lachance, Nazia Darvesh, Sarah C. McGill, Robyn Butcher, Michelle Gates, Joanne Kim, Ransi Nayakarathna
Contributors
Bert Dolcine, Chris Kamel, David Kaunelis, Genevieve Chartrand, Krista Kaminski, Pierre Martinelli, Sara Khangura, Camille Santos, Robyn Haas, Nikolay Alabi, Claire Sharp
External Reviewer
This document was externally reviewed by a content expert, who has granted permission to be cited.
Onil Bhattacharyya, MD, PhD
Director, Women’s College Hospital Institute for Health Systems Solution and Virtual Care
Associate Professor, University of Toronto
Toronto ON
Abbreviations
CIHI
Canadian Institute for Health Information
MeSH
Medical Subject Headings
PRISMA
Preferred Reporting Items for Systematic reviews and Meta-Analyses
PRISMA-ScR
Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews
WIHV
Women’s College Hospital Institute for Health Systems Solutions and Virtual Care
Key Messages
We conducted rapid scoping of the literature, an adapted method of a scoping review, to quickly identify the available evidence and knowledge gaps for the clinical effectiveness, harms, implementation considerations, and guideline recommendations for virtual care.
We found 230 scoping reviews and 12 reports representing 11 evidence-based guidelines, all published between 2020 and 2022, about virtual health care involving remote communication between a health care provider and a person receiving care. Most scoping reviews focused on care for mental health, cardiovascular, and cancer-related conditions; and guidelines focused mostly on recommendations for cardiovascular, cancer, reproductive, and rheumatology-related conditions.
The scoping reviews mostly reported on how virtual care affects patient-focused outcomes and patients’ use of the health care system, and how patient and caregiver perspectives could be considered when using virtual care. There may be gaps in the existing evidence base for the effects of virtual care on changes in patients’ care plans and clinical harms for patients, and for the ethical aspects that could be considered when implementing virtual care. We found no scoping reviews that discussed environmental or climate considerations for virtual care use. Close to one-third of the scoping reviews referenced patients living in rural or remote settings, and 7% mentioned Indigenous Peoples.
All of the 11 guidelines provided clinical practice recommendations, and 8 of them provided other implementation recommendations. About half of the guidelines referenced patients living in rural or remote settings, and 1 guideline mentioned Indigenous Peoples. There may be gaps for guidelines that provide recommendations for primary health care and for those with certain conditions, such as mental health disorders and diabetes.
Abstract
Background
Given the increase in the use of virtual health care services during the COVID-19 pandemic, and their continued use expected going forward, the objective of this rapid scoping exercise was to identify the available evidence and knowledge gaps for the clinical effectiveness, harms, implementation considerations, and guideline recommendations for virtual care.
Methods
We conducted a rapid scoping exercise that included scoping reviews and evidence-based guidelines published between January 2020 and June 2022 from MEDLINE and Embase databases, focused internet searches, and grey literature sources. We included reports about populations of all ages using virtual care to interact or communicate with a health care provider for any health reason and in any context. Titles and abstracts were screened by 2 reviewers in duplicate following a liberal accelerated approach. A single reviewer then screened full-text records for inclusion and charted data, after attaining good agreement in a pilot round. Included references were charted and grouped by the following categories: age group and population type; evidence on clinical effectiveness, clinical harms, and implementation considerations (from scoping reviews) or clinical practice or other implementation recommendations (from guidelines); and virtual care format. Study design, language, country of focus, presence of caregiver, mention of Indigenous Peoples, and rural or remote setting were also charted to provide context and highlight literature that may provide insight on health equity considerations. We produced summary tables and visualizations of the data to showcase our findings.
Results
After screening 2,211 titles and abstracts and 785 full-text articles, 230 scoping reviews and 12 reports representing 11 evidence-based guidelines published between 2020 and 2022 met our eligibility criteria and were included in this report. Of these, there were 165 scoping reviews reporting on clinical effectiveness and harms, 208 scoping reviews reporting on implementation considerations, and 11 evidence-based guidelines providing recommendations for virtual care.
For the scoping reviews, 46.5% (n = 107) did not specify age group, 32.2% (n = 74) reported on adults, 26.5% (n = 61) specified children, and 19.6% (n = 45) described older adult populations. Most of the scoping reviews (89.1% [n = 205]) reported the population type; for example, 30.4% (n = 70) reported on populations with mental health disorders, 16.5% (n = 38) reported on people with cardiovascular conditions, and 15.7% (n = 36) reported on people with cancer. Seventeen scoping reviews (7.4%) reported on Indigenous Peoples, and 79 (34.3%) reported on people living in rural or remote areas. The top reported concepts within the clinical effectiveness and harms category were patient-focused outcomes and health care utilization. Changes in patients’ care plans (e.g., change in medical guidance, medication, or device use) and clinical harms (e.g., adverse events, clinical complications, or patient safety) were the least reported in this category. The top reported concepts within the implementation considerations category were patient or caregiver perspectives, competency, and experiences; and operational aspects of virtual care. Within implementation considerations, ethics related to virtual care were reported the least frequently, and no included studies reported outcomes related to environmental factors. Of the scoping reviews, 205 (89.1%) reported the virtual care format for at least 1 of the relevant studies included in their review: video was mentioned for 63.0% (n = 145), telephone calls for 62.2% (n = 143), text messages for 31.3% (n = 72), emails for 23.0% (n = 53), and other online methods for 44.8% (n = 103).
For the guidelines, 90.9% (n = 10) did not specify age group, while 18.2% (n = 2) specified adults, 9.1% (n = 1) specified children, and none specified older adult populations. In addition, each guideline provided recommendations for a specific health condition, and across all guidelines were 7 health conditions: 18.2% (n = 2) of the guidelines focused on populations with cancer, 18.2% (n = 2) on people with cardiovascular conditions,18.2% (n = 2) on populations seeking obstetrics/gynecology care, 18.2% (n = 2) on people seeking rheumatology care, and each of the remaining 3 guidelines focused on ear, nose, and throat conditions; pain management; or substance use disorders. One guideline (9.1%) reported on Indigenous Peoples, and 5 (45.5%) reported on people living in rural or remote areas. All guidelines provided clinical practice recommendations, and 8 guidelines (72.7%) provided other implementation recommendations. For virtual care format, 90.9% (n = 10) of the included guidelines referred to virtual care at least once without specifying the format, 54.5% (n = 6) referred to telephone calls, 45.5% (n = 5) referred to video, 9.1% (n = 1) referred to text messages, 18.2% (n = 2) referred to emails, and 27.3% (n = 3) referred to other online methods.
Conclusions
This rapid scoping exercise identified and characterized a growing body of evidence as well as existing clinical practice and other implementation recommendations that have been published on virtual care. Knowledge users from a variety of fields can use our findings to understand the current evidence landscape on virtual health care and to identify recommendations to consider when implementing virtual care. Potential gaps where there is limited to no evidence identified in our report, such as ethical and environmental considerations and the effects of virtual care on clinical harms for patients and changes in patients’ care plans, as well as recommendations for virtual care that appear to be lacking for mental health disorders and diabetes, can be used as a starting point for further research.
Introduction and Rationale
The COVID-19 pandemic, which was first publicly recognized by WHO in early 2020,1 spurred a change in how health care is provided in Canada. For example, provinces and territories began to implement more services using digital technologies to maintain health care for populations when physical distancing measures for COVID-19 reduced delivery of in-person care.2-5 The proportion of virtual care services changed when the pandemic started. For example, data from the Canadian Institute for Health Information (CIHI) show that in Ontario, the proportion of the population who received virtual care services was 1% in each month from April 2019 to February 2020 and then increased to 9% in March 2020.6 Between April 2020 and February 2021, the proportion ranged from 15% to 17%. The CIHI data also show increases in virtual care services for other provinces such as Manitoba, Saskatchewan, Alberta, and British Columbia. Overall, the use of virtual care has continued, and has not reduced to pre-pandemic proportions.6 Other data show that in April 2020, telemedicine accounted for 77% of ambulatory visits in Ontario, reflecting the large proportion of care visits being performed virtually.7
Several terms have been used to describe virtual health services. According to CIHI, the definition of digital health includes e-health and advanced computing science, and consists of virtual care, telehealth, and telemedicine.8 Virtual care is defined by the Women’s College Hospital Institute for Health Systems Solutions and Virtual Care (WIHV) as “any interaction between patients and/or members of their circle of care, occurring remotely, using any forms of communication or information technologies, with the aim of facilitating or maximizing the quality and effectiveness of patient care.”9 It can take place synchronously (communication in real time, using videoconferencing or telephone calls for example) or asynchronously (communication not in real time, for example via text messages).10 Virtual care may help to mitigate some of the challenges that affect the delivery of and access to in-person care, such as geographical distance, long wait times, pandemic-related measures such as cleaning and personal protective equipment use, and costs to people accessing care related to travelling or missing work.10-13
Virtual care has been used in Canada since the 1970s,14,15 and its use is expected to continue in the years to come.8 A national survey of 2,071 physicians conducted in 2021 by Canada Health Infoway and the Canadian Medical Association found that nearly all physicians who provided virtual care during the COVID-19 pandemic expected to continue after the pandemic.16 Of those physicians, 22% saw their use of virtual care increasing in the future, 42% expected it would remain the same, and 32% anticipated it would decrease.16 In addition, a Health Canada–commissioned analysis recommended that the newly expanded use of virtual care be maintained as “a core-part of our publicly-funded health delivery system.”17 Moreover, health charities, community service providers, and specialty clinical groups working in hospitals have found ways to continue to implement virtual care beyond the pandemic.11
The start of the COVID-19 pandemic led to a rapid increase in the use of virtual care across Canada, and there is a growing interest in evaluating its appropriateness to inform whether and where we continue or discontinue its use going forward. However, informal scoping indicates that the evidence base is large and rapidly evolving, and there is a need to better understand the nature of the available evidence before undertaking this assessment. We are aware of several existing scoping reviews in this area, and these tend to have a narrow scope — for example, a focus on implementation considerations for virtual care for underserved populations.18 CADTH has previously produced several reports on virtual care, most recently a reference list on virtual oncology visits published in July 202219 and a rapid review on virtual care use in primary care or specialist care settings published in August 2022,20 which also had narrow scopes. We undertook a rapid scoping exercise that will add to this previous work and quickly provide us with an understanding of the literature by broadening the scope to identify existing evidence and guidance on virtual health care for all types of health care services and in all populations. The findings of this exercise can support health care decision-making needs in Canada and identify areas for future research.
Objectives
We conducted a rapid scoping exercise to identify and organize available evidence and knowledge gaps in virtual health care, specifically related to clinical effectiveness, harms, and implementation considerations. We also aimed to identify relevant recommendations from evidence-based guidelines.
Research Questions
Q1. What evidence is available and what are the knowledge gaps regarding clinical effectiveness and harms for any patient-centred health care services that currently are or can be delivered virtually in any form (e.g., videoconference, telephone calls, text messages, email)?
Q2. What evidence is available and what are the knowledge gaps regarding implementation considerations for any patient-centred health care services that currently are or can be delivered virtually in any form (e.g., videoconference, telephone calls, text messages, email)?
Q3. What evidence-based guidelines for virtual care are currently available?
Methods
Protocol Development
To guide the conduct of this rapid scoping exercise, we produced a protocol for internal use and recorded all revisions with date stamps for transparency. Due to the time constraints of this rapid scoping exercise, we did not publish the protocol a priori; however, we engaged an internal methodologist throughout the process of protocol development.
To assess the feasibility of answering our research questions, research information specialists performed an informal literature search for existing scoping reviews on the topic, and we assessed this literature based on our draft inclusion and exclusion criteria. Over videoconference, we showcased our draft research questions and eligibility criteria to the requesting customer to ensure appropriate breadth and depth of the topic in addressing their needs, and incorporated any feedback to finalize our research questions and eligibility criteria before conducting the work.
Study Design
We took an iterative approach when considering eligible study designs for this report. The types of study designs included in this rapid scoping exercise were dependent on feasibility considerations (e.g., number of records to screen and chart, breadth of evidence found). We had initially planned a 3-phase approach, for which the first phase included scoping reviews and evidence-based guidelines. In the second and third phases, we planned to include evidence syntheses and primary studies, respectively, to address evidence gaps. The second and third phases were later considered not feasible within the time frame of the current scoping exercise, and we decided that the large volume of scoping reviews identified in the first phase would adequately address the research questions. Therefore, we conducted a rapid scoping exercise and included 2 types of studies in this report: existing scoping reviews and evidence-based guidelines. A scoping review is “a type of knowledge synthesis, following a systematic approach to map evidence on a topic and identify main concepts, theories, sources, and knowledge gaps.”21 Consistent with other rapid CADTH products, we defined an evidence-based guideline as a systematically developed statement or set of statements to assist practitioner and patient decisions about appropriate health care for specific clinical circumstances.
Our methodology was informed by the JBI methodological guidance for scoping reviews,22 and the scoping exercise has been reported according to Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews (PRISMA-ScR), with consideration for updates provided in PRISMA 2020.21,23 To complete the scoping exercise within a short time frame, we adapted our methodological approaches to make this review rapid: we produced an a priori protocol but did not register or obtain external peer-review feedback on the protocol; we limited the study design, time frame, and language of our eligibility criteria; and we used a single reviewer to conduct full-text screening and data charting following a pilot round.
For transparency, the PRISMA-ScR checklist was completed and is provided in the Supporting Information document (refer to Reporting Checklist). An external content expert and an internal methodologist reviewed the draft report and provided feedback, which was incorporated into the final report.
Literature Search Strategy
Research information specialists conducted a literature search of key resources including MEDLINE All (1946—) and Embase (1974—) via Ovid, and a focused internet search. The Supporting Information document (refer to Literature Search Methods) shows the complete search strategy. We ran Ovid searches simultaneously as a multi-file search. We removed duplicates using Ovid deduplication for multi-file searches, followed by manual deduplication in Endnote. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concept was virtual care. We applied CADTH-developed search filters to limit retrieval to guidelines or scoping reviews. We excluded conference abstracts, preprints, comments, newspaper articles, editorials, and letters. Where possible, we limited retrieval to the human population. The search was completed on June 27, 2022, and limited to English or French language documents published since January 1, 2020.
We identified grey literature (literature that is not commercially published) by searching sources listed in selected sections of the Grey Matters: A Practical Tool for Searching Health-Related Grey Literature checklist,24 which includes the websites of clinical guideline repositories. We used Google to search for additional internet-based materials. The Supporting Information document (refer to Literature Search Methods) includes more information on the grey literature search strategy.
For this rapid scoping exercise, we did not run article alerts as the report was completed within 3 months of the original search, which did not allow time to run, screen, and incorporate newer data.
Eligibility Criteria
Inclusion Criteria
Table 1 provides the eligibility criteria for our review.
Table 1: Eligibility Criteria for Research Questions
Category | Selection criteria |
|---|---|
Population | People of all ages accessing any health care service:
|
Concept | Any evidence of clinical effectiveness, harms, or implementation considerations for virtual health care interventions Q1: Clinical effectiveness and harms of virtual care interventions:
Q2: Implementation considerations for virtual care interventions in the following areas:
Q3: Recommendations from evidence-based guidelines from health or health care organizations. |
Context | All modes of virtual interaction between a health care provider and a person accessing care (e.g., videoconference, telephone calls, text messages, emails) |
Study design(s) | Scoping reviews and evidence-based guidelines Exclusions:
|
Time frame | January 1, 2020a to June 27, 2022 |
Language of publication | English and French |
aWe focused on scoping reviews and evidence-based guidelines published between 2020 and 2022 to capture evidence that may reflect virtual care learnings from the COVID-19 pandemic, when this health care delivery model was used more prominently in Canada.14 The scoping reviews published in this time frame would also likely capture evidence from post-2018 when the use of virtual care became more prominent in Canada.14
To be considered eligible, scoping reviews and evidence-based guidelines had to examine virtual care provided by health care professionals (e.g., physicians, nurses, psychologists) to people or patients using technology (e.g., telephone calls, emails, text messages, videoconferencing). Reports could be describing any type of clinical services for patients (e.g., primary care, specialist care), and people accessing care could be in any setting (e.g., rural, remote, urban).
We based our definition of virtual care on the 1 developed by WIHV in Toronto, Ontario: “any interaction between patients and/or members of their circle of care, occurring remotely, using any forms of communication or information technologies, with the aim of facilitating or maximizing the quality and effectiveness of patient care.”9 We focused on virtual care where there was an interaction between health care providers and patients or their circle of care and where delivery was synchronous (i.e., live and in real time) or asynchronous (e.g., communication over email with delays between responses). Other definitions of virtual care may be described as an umbrella term that encompasses all health care delivered using technology or as belonging to broader terms such as digital health, telehealth, telemedicine, e-health,25 or mobile health,26 which can include provider-to-provider communication, 1-way educational videos for patients, or passive 1-way monitoring or transmission of health data. Nevertheless, we considered the WIHV definition to be most relevant in the Canadian context and decided to include virtual care where the patient and provider were clearly and actively interacting.10
Scoping reviews were eligible if they included studies where virtual care was the sole intervention (e.g., video conferencing for appointments with a primary care physician) or where virtual care was a component of an intervention (e.g., telephone consultations for appointments with a primary care physician plus pre-recorded educational video modules). This was to ensure that we adequately captured the available evidence on health care services delivered virtually in any form, whether they were combined with another intervention component or not.
We considered a guideline to be evidence-based if the authors stated a systematic review or a systematic search of the literature was conducted to inform the recommendations. If recommendations were made that were not based on a systematic search of the literature but were from health or health care organizations or professional associations, we provided those in the Supporting Information document (refer to Included Reports and References of Potential Interest).
We limited eligible reports to those published in English or French between 2020 and 2022, based on feasibility and considering that it was likely that relevant literature published since virtual care became more prevalent (i.e., post-201814) would be captured by scoping reviews published after 2020. Additionally, this time frame limit would include virtual care learnings from the COVID-19 pandemic when this health care delivery model was used more prominently in Canada.
Exclusion Criteria
We excluded reports if they did not meet the selection criteria outlined in Table 1, if they were duplicate publications or scoping review protocols, or if they were published before 2020. Since our virtual care definition was based on provider and patient interaction, we excluded interventions that only contained digital aspects delivered by the technology itself and did not include communication or interaction with a designated health care professional (e.g., chatbots, 1-way pre-recorded educational videos, automated text messages such as reminders, self-management, or remote patient monitoring interventions without a described patient-provider component). We also excluded reports describing how to evaluate different virtual care technologies or those that described frameworks for evaluating virtual care or scoping reviews that summarized literature as lists, counts, or frequencies without addressing our research questions.
Selection Process
We used systematic review management software DistillerSR (Evidence Partners, Ottawa, Canada) to facilitate study selection. To ensure the eligibility criteria were applied consistently, 2 reviewers conducted a pilot screening exercise with 50 citations identified from the literature search. After high agreement was reached, the 2 reviewers independently screened titles and abstracts of all citations using a liberal accelerated approach;27,28 that is, titles and abstracts marked as “include” by 1 reviewer were included and passed onto the next stage of screening, while those marked as “exclude” by 1 reviewer were screened by the other reviewer to confirm or refute the exclusion.
In the next stage of screening, we assessed the full-text articles for each potentially relevant citation included after the first stage. Reviewers conducted a pilot screening exercise of 50 random full-text articles. After high agreement was reached, each full-text article was assessed for eligibility by 1 reviewer. We involved a second reviewer for instances in which the first reviewer was unclear on whether the record met the inclusion criteria, and we resolved disagreements by discussion. We did not intend to contact authors to clarify missing information that may have been needed to decide on inclusion or exclusion, as we did not expect that responses would be available in the time frame required for this project. We documented the reasons for exclusion at the full-text level and report this in our PRISMA flow chart in the Supporting Information document (refer to Selection of Included Reports). We have not presented an excluded studies list, as this was not feasible within the rapid timeline of the project.
Charting (Data Extraction)
We developed a charting form in Microsoft Excel (version 2205, Microsoft, Washington, US). Reviewers conducted a pilot exercise on a sample of 3 included reports; during the pilot, the reviewers reached a good level of agreement and the form seemed to adequately capture the information of interest. Following this, each report was charted by 1 reviewer to extract relevant data; the reliance on a single reviewer was to ensure that all data could be charted on a short timeline. As needed, reviewers met to discuss charting questions and made modifications to the charting form or data points using an iterative process.
The reviewers charted the following relevant information from the included scoping reviews and guidelines:
Report characteristics: study design (i.e., scoping review, evidence-based guideline), first author’s surname, year of publication (i.e., 2020, 2021, 2022), language (i.e., English, French), country/region of focus or to which the guidelines were intended to apply.
Population: age group (i.e., age not reported, children, adults, older adults) and population type, which included:
general population/population not reported
patients with or receiving care for:
cancer
cardiovascular conditions
chronic conditions
diabetes
ear, nose, and throat conditions
infectious diseases
kidney and urinary conditions
mental health disorders
musculoskeletal conditions
neurologic conditions
obstetrics, gynecology (non-cancer), prenatal care
pain care
palliation of symptoms (i.e., palliative care)
respirology conditions
rheumatology conditions
substance use disorders
recent or upcoming surgery
other
caregivers/circle of care when representing patients
Indigenous Peoples
patients from rural or remote settings.
Concept:
clinical effectiveness and harms from scoping reviews: patient-focused outcomes, health care utilization, health service delivery, change in a patient’s care plan, clinical harm.
implementation considerations from scoping reviews: economics; perspectives, competency, and experiences from any virtual care users (e.g., people accessing care, caregiver, provider, unspecified user); ethics; operational aspects; and environmental factors.
recommendations from evidence-based guidelines from health or health care organizations (e.g., clinical practice recommendations, implementation recommendations, other recommendations).
Context: virtual care format (i.e., format not reported, telephone calls, video, text message/short messaging service, email, other online methods).
We extracted the data as reported in the scoping reviews and characterized what had been identified and included within the scoping reviews, rather than eligibility criteria. As such, if there was an apparent knowledge gap, we did not know if it was because the included scoping reviews did not look for that information or looked and did not find the information. Because each individual study within a scoping review could be focused on multiple populations and outcomes, multiple fields could be selected for each included study within a single category of data to be extracted (except for study design, year of publication, and language); this means a single study could have been counted multiple times in our descriptive statistics and that proportions did not necessarily equal 100%. We did not check the original publications contained within the scoping reviews, nor did we extract data from them. If the research question for the scoping review being charted was on a topic broader than virtual care (e.g., a scoping review on all digital health technologies), we charted details only for the relevant studies if they reported on provider–patient interactions. If the research question for the guideline being charted was on a topic broader than virtual care, we charted all details about virtual care if they mentioned an interaction between a provider and a patient at least once. This difference in the approach taken was mainly taking account of the volume of the literature identified and included in this report (i.e., very high for scoping reviews and very low for guidelines). Due to the abbreviated timeline of the project, we were not able to check the overlap in studies between the included scoping reviews, and we did not contact authors to obtain or clarify relevant information within the scoping reviews or guidelines.
As the goal of the scoping review is not to comment on the quality of the evidence, we did not conduct any risk of bias assessments in our rapid scoping exercise.21,22
Descriptive Synthesis
We performed a descriptive synthesis of the charted data to map the characteristics of each included scoping review and evidence-based guideline, and we presented summary concepts that emerged from mapping in tables and figures (i.e., bar charts) and as narrative text.
For the characteristics of the included reports, we summarized the number of reports identified by study design (i.e., scoping reviews, evidence-based guidelines), year of publication, and country (i.e., country/region of focus for scoping reviews, country/region to which the evidence-based guidelines are meant to apply).
For population characteristics, we also summarized the proportions of scoping reviews and guidelines identified by age group of individuals accessing care and population type (e.g., those with diabetes, cancer, mental health disorders, or substance use disorders; presence of a caregiver; Indigenous Peoples; people from rural or remote settings). We focused on the descriptors of age, and not the numerical values, as reported in the scoping reviews and guidelines; we categorized age groups as children, adults, and older adults.
Scoping reviews that contained studies examining each of the main concepts, as well as their subcategories, were summarized in the tables and directly answered each research question about available evidence. Concepts or subcategories where no or few scoping reviews or guidelines were identified were considered to indicate a potential evidence gap, which is highlighted in the results section.
Results
Quantity of Research Available
We identified a total of 2,211 unique reports in the electronic literature search and removed 250 duplicate reports manually. Following screening of titles and abstracts, we excluded 1,233 reports and retrieved 728 potentially relevant reports for full-text review. We retrieved an additional 57 potentially relevant reports for full-text review from the grey literature search. Of these 785 potentially relevant reports, we excluded 543 and included 242 reports for this rapid scoping exercise. We outlined the selection process using a PRISMA flow chart in the Supporting Information document (refer to Selection of Included Reports). We present 2 reference lists that together identify all included reports (n = 242) and a reference list of guidelines and guidance documents from health or health care organizations or professional associations that did not meet our eligibility criteria (n = 158) in the Supporting Information document (refer to Included Reports and References of Potential Interest).
Of note, our results do not indicate the number of relevant studies included within each scoping review or informing each guideline.
Characteristics of Included Reports
Of the 242 included reports, 230 were scoping reviews (95.0%), and 12 reports represented 11 evidence-based guidelines (5.0%). There were 2 reports that represented 1 guideline out of the 11 guidelines in total; information from the 2 reports were counted once in our summary characteristics. We provide detailed summary tables of the included reports informed by our mapping of the evidence and recommendations identified in the Supporting Information document (refer to Summary Tables of Included Reports). The summary tables can be used to identify which populations, concepts, or context of interest were reported by each included scoping review or guideline. Further, the summary tables can also show where evidence or a recommendation has not been found for a particular population, concept, or context; these potential gaps can be used to inform future research in these areas. Using the summary tables and the reference lists provided in the Supporting Information document, readers of our report can identify the scoping review or guideline of interest and consult its content (e.g., the individual studies included in the scoping review or informing the guideline) to gain further details about its findings. Below, we provide narrative text and visualizations of our findings from the included reports by category.
All of the included reports were published between 2020 and 2022. Of the 230 scoping reviews, 47 scoping reviews were published in 2020 (20.4%; 34 scoping reviews addressed research question 1 [Q1] and 42 scoping reviews addressed research question 2 [Q2]); 100 scoping reviews were published in 2021 (43.4%; 71 scoping reviews addressed Q1 and 90 scoping reviews addressed Q2); and 83 scoping reviews were published in 2022 (36.1%; 60 scoping reviews addressed Q1 and 76 scoping reviews addressed Q2). Addressing research question 3 (Q3), out of the 11 evidence-based guidelines, 2 guidelines were published in 2020 (18.2%), 4 guidelines were published in 2021 (36.4%), and 5 guidelines were published in 2022 (45.5%). Refer to Figure 1 for a graph of the number of studies published over time by year of publication, separated by research question.
Figure 1: Number of Included Reports by Year of Publication
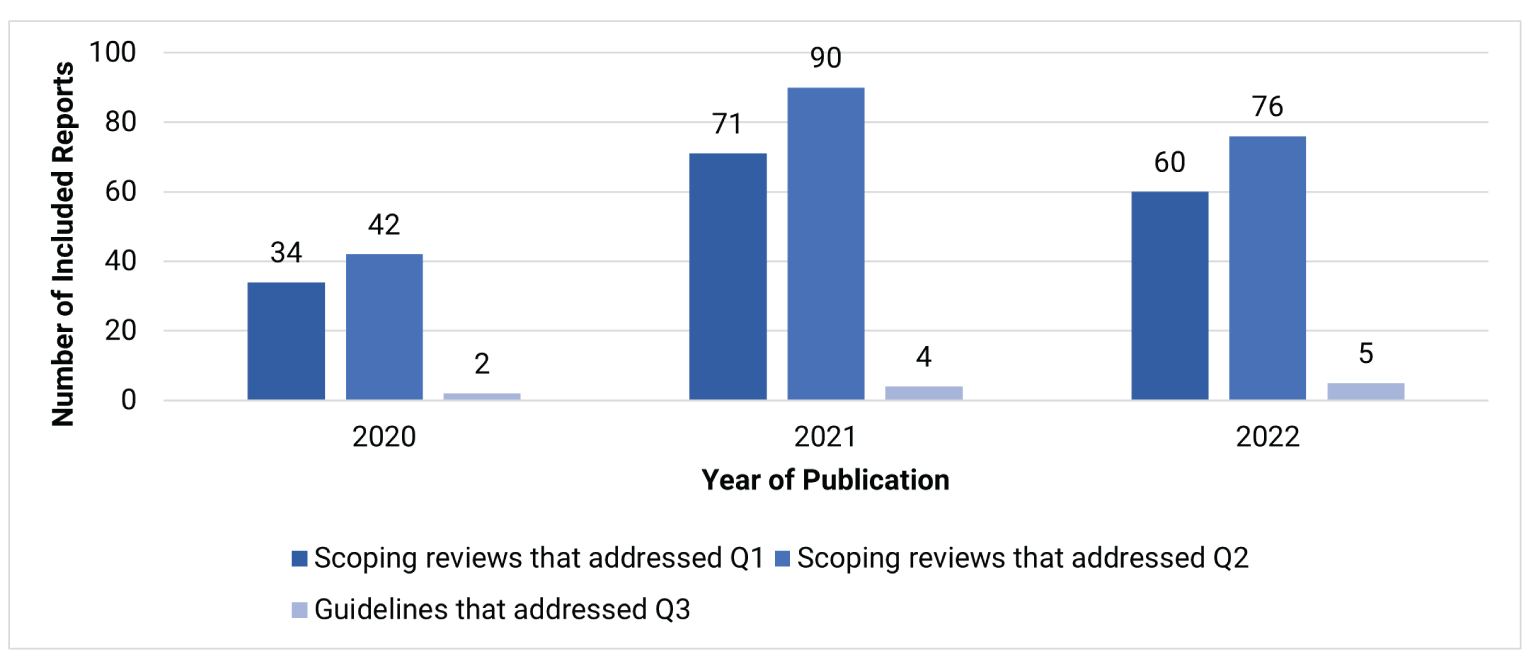
Q1 = research question 1; Q2 = research question 2; Q3 = research question 3.
There were 32 (13.9%) scoping reviews that focused on a particular country or region (20 scoping reviews addressed Q1; 29 scoping reviews addressed Q2). The remaining 198 scoping reviews (86.1%) were not focused on a particular country or region. Of note, descriptors of country or region of focus were transposed using the terms the authors of the included reports used, to prevent any potential misinterpretation of the reports’ findings. For example, if authors referred to a country as “higher income”, we used that descriptor in our report and acknowledge that it may not be the most appropriate way to categorize countries. Of the scoping reviews that were focused, the most prevalent countries or regions, as reported by the authors of the scoping reviews, were the US (n = 6 [addressed Q1], n = 6 [addressed Q2]), Australia (n = 4, n = 6), Canada (n = 4, n = 5), “low- and middle-income countries” (n = 4, n = 2), “high-income countries” (n = 1, n = 4), and other regions (n = 2, n = 5). The 11 evidence-based guidelines reported the countries or regions to which their guidelines are intended to apply. The most prevalent countries or regions, as reported by the authors of the guidelines, were the US (n = 4) and Canada (n = 2). Refer to Figure 2 for a graph of the number of studies by country or region of focus, separated by research question.
Despite our eligibility criteria being inclusive of studies published in English or French, all 242 included reports were published in English.
Figure 2: Number of Included Reports With a Country or Region of Focus
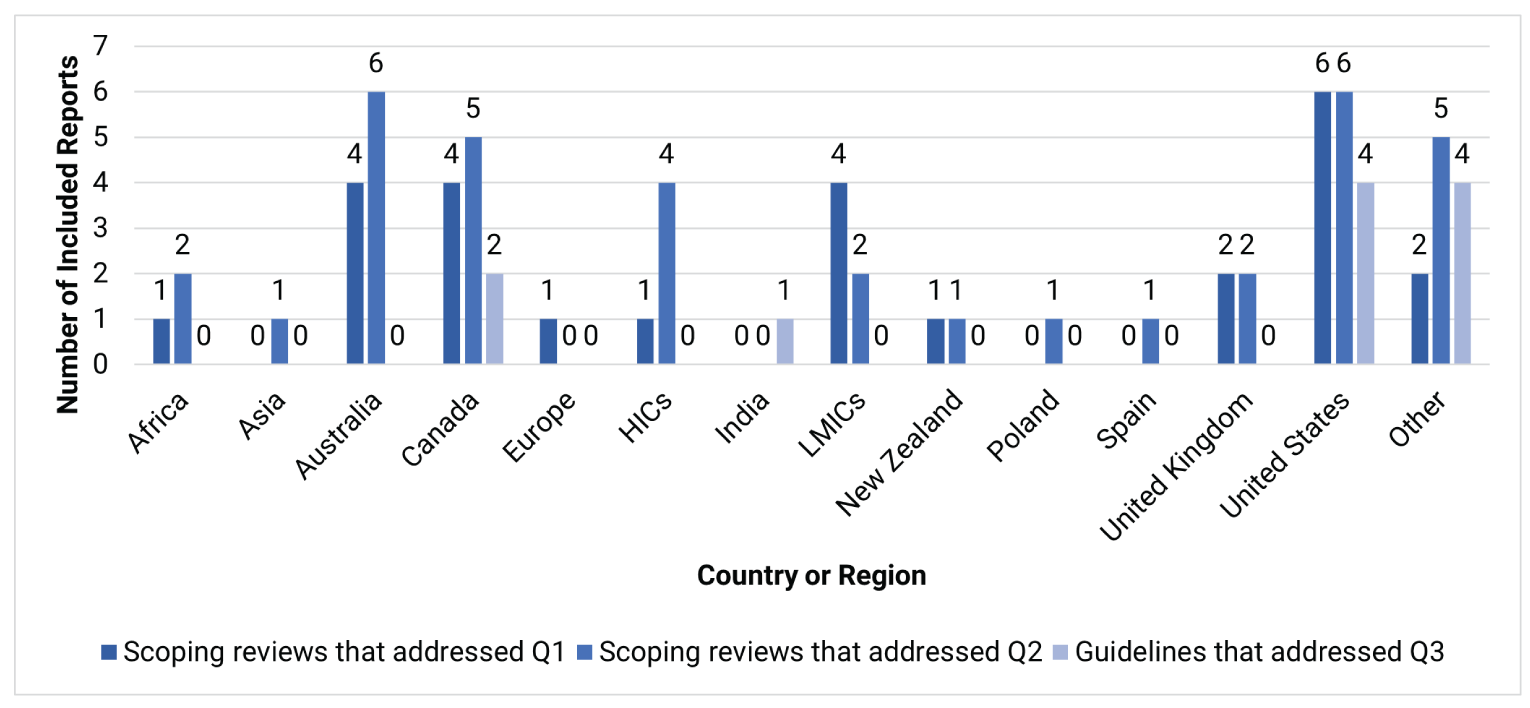
HICs = “high-income countries”; LMICs = “low- and middle-income countries”; Q1 = research question 1; Q2 = research question 2; Q3 = research question 3.
Notes: The “other” category for research question 1 represents geographically isolated locations (n = 1) and territories with high degrees of inequity within the scope of the Conexão Saúde Digital Project (n = 1). The “other” category for research question 2 represents circumpolar regions (n = 1), forested and mountainous areas (n = 1), geographically isolated locations (n = 1), Organization for Economic Co-operation and Development member countries (n = 1), and territories with high degrees of inequity within the scope of the Conexão Saúde Digital Project (n = 1). The “other” category for research question 3 represents an international panel of experts (US, Canada, UK, Netherlands, Portugal) on caring for individuals with pain during COVID-19 (n = 1); the “Arab region,” representing 16 Arab countries, as reported by the report authors (n = 1); the “Asia Pacific region” as reported by the report authors (n = 1); and German-speaking countries of Europe (n = 1).
Population Characteristics
Demographic Characteristics
Scoping Reviews (Q1 and Q2)
Of the 230 scoping reviews, 123 (53.5%) reported the age of the population for 1 or more of the relevant studies included in their review, and 107 (46.5%) did not. Of the included scoping reviews, 61 (26.5%) reported on studies that included children, 74 (32.2%) reported on adults, and 45 (19.6%) reported on older adults.
The scoping reviews reported on many different types of patients that could be classified under many different health care conditions. Of the 230 scoping reviews, 205 (89.1%) reported the population type for at least 1 of the relevant studies included in their review and 25 (10.9%) did not. Fifty (21.7%) scoping reviews included studies that involved a caregiver or someone in the patient’s circle of care. Seventy-nine (34.3%) scoping reviews reported on studies involving patients living in rural and/or remote areas. Seventeen (7.4%) scoping reviews reported on studies involving Indigenous Peoples. The population types also were categorized as patients with or receiving care for cancer (n = 36; 15.7%); cardiovascular conditions (e.g., hypertension, congestive heart failure, cardiovascular disease, stroke) (n = 38; 16.5%); chronic conditions (i.e., general or unspecified chronic conditions, chronic pain, chronic fatigue) (n = 25; 10.9%); diabetes (n = 35; 15.2%); infectious diseases (e.g., HIV, tuberculosis, COVID-19) (n = 25; 10.9%); kidney and urinary conditions (e.g., kidney disease) (n = 14; 6.1%); mental health disorders (e.g., post-traumatic stress disorder, experienced sexual violence, depression, eating disorders) (n = 70; 30.4%); musculoskeletal conditions including physical injuries (e.g., anterior cruciate ligament tears), arthritis, patients requiring physical rehabilitation, and non-surgical conditions (n = 18; 7.8%); neurological conditions (e.g., Parkinson disease, Huntington disease, epilepsy) (n = 13; 5.7%); obstetrics, gynecology (non-cancer), and prenatal care (n = 16; 7.0%); palliation of symptoms (i.e., palliative care) (n = 13 ; 5.7%); respirology conditions (e.g., asthma, chronic obstructive pulmonary disease) (n = 24; 10.4%); substance use disorders including smoking, alcohol, and drug use (n = 13; 5.7%); a recent or upcoming surgery (e.g., otolaryngology, orthopedic) (n = 21; 9.1%); and other health conditions (n = 47; 20.4%).
Refer to Figure 3 and Figure 4 for graphs of scoping reviews by age group and population type, respectively.
Guidelines (Q3)
Of the 11 guidelines, 1 guideline (9.1%) provided recommendations for children, 2 (18.2%) for adults, and none for older adults. Nine guidelines (81.8%) provided recommendations for a target population based on health condition rather than age. Each guideline focused on 1 health specialty, including: patients receiving care for cancer (n = 2; 18.2%); cardiovascular conditions including stroke (n = 2; 18.2%); ear, nose, and throat conditions (n = 1; 9.1%); obstetrics and gynecology needs (n = 2; 18.2%); pain during COVID-19 (n = 1; 9.1%); rheumatology needs (n = 2; 18.2%); and substance use disorders (n = 1; 9.1%).
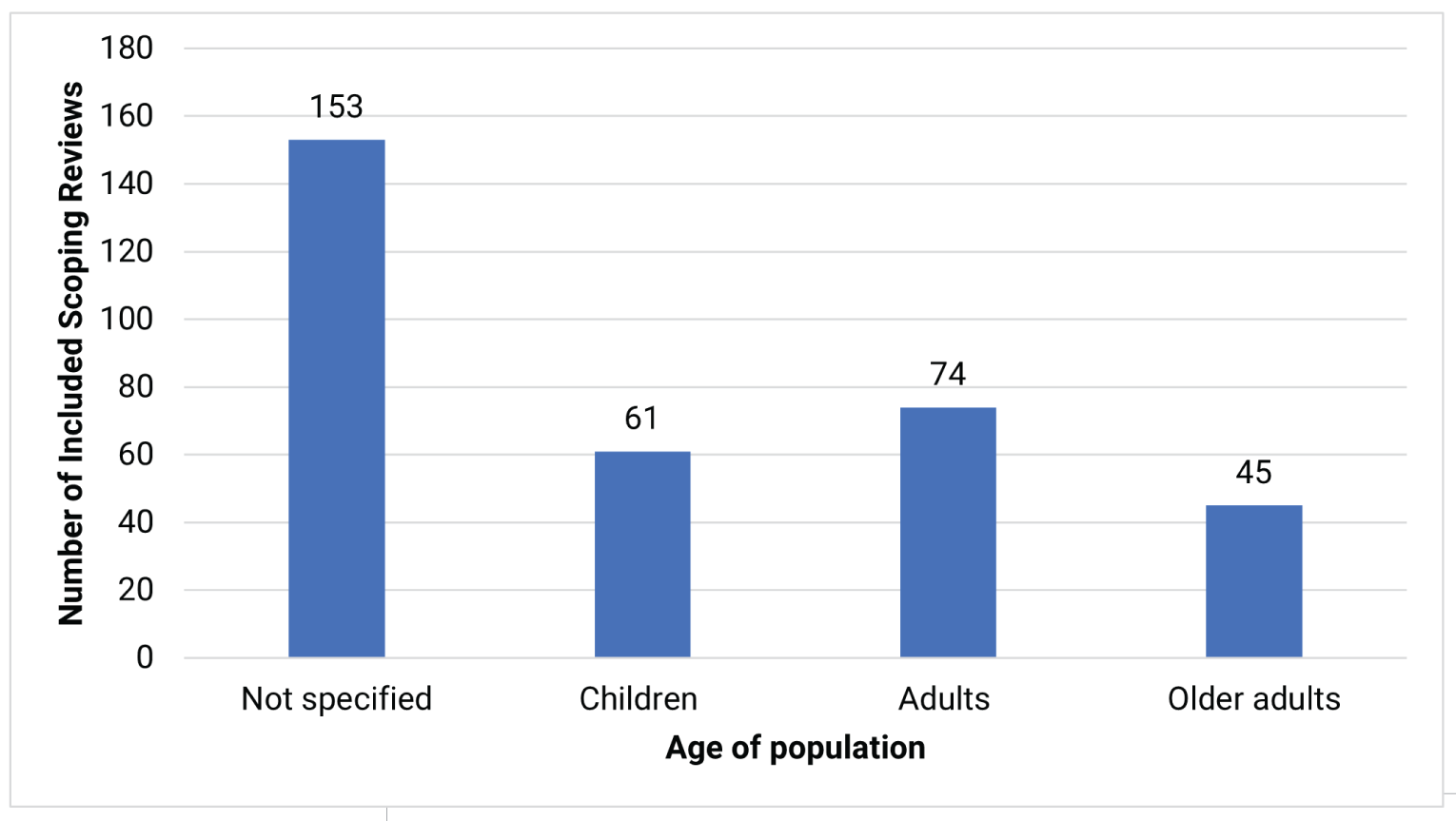
Figure 4: Number of Included Scoping Reviews Reporting About Population Type
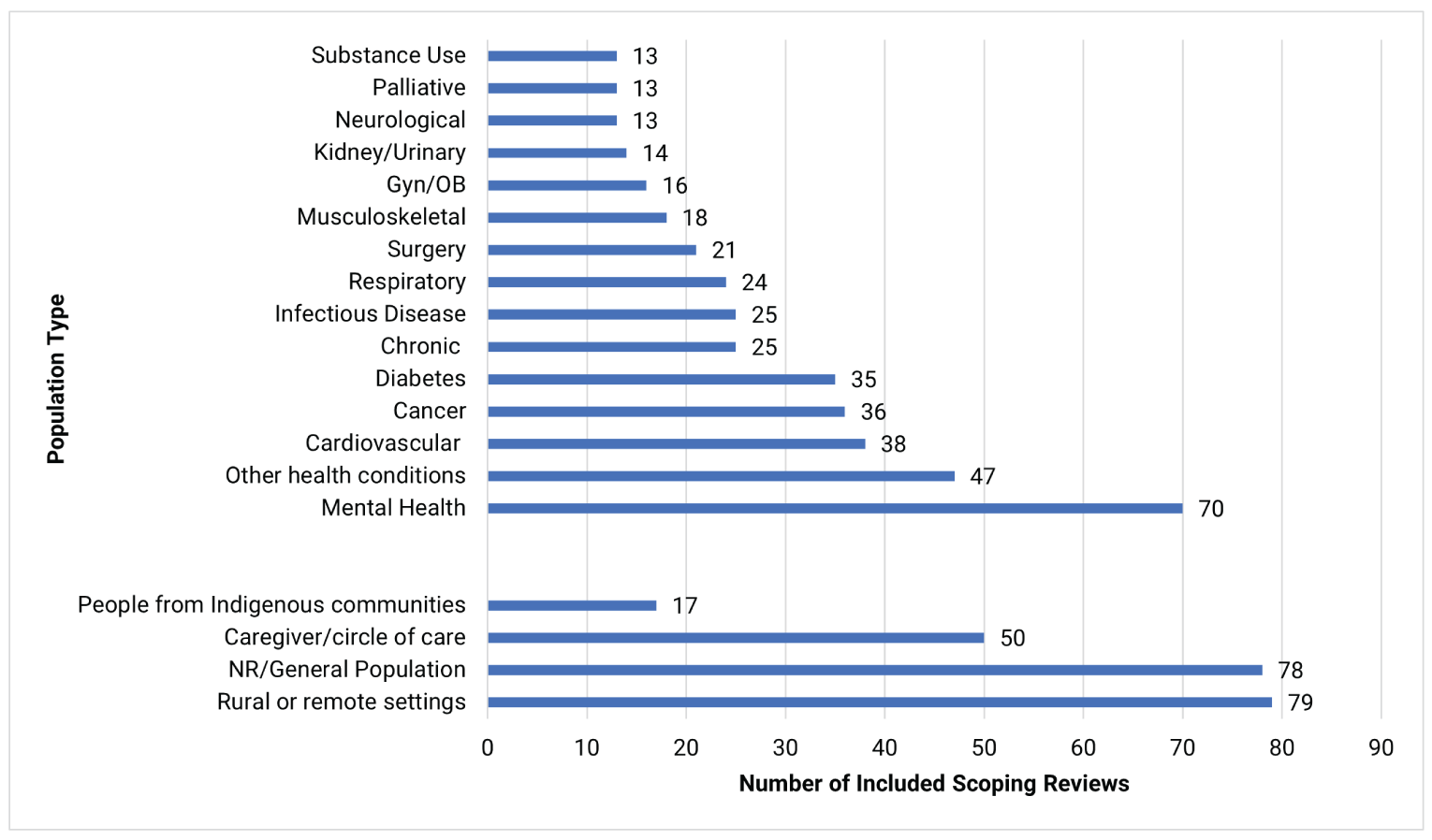
Gyn = gynecology; NR = not reported; OB = obstetrics.
Notes: The following conditions were included under the “other health conditions” category based on the number of included scoping reviews reporting the population type (i.e., < 10 studies): attention-deficit/hyperactivity disorder; autism spectrum disorder; brain injuries (i.e., acquired, traumatic); cognitive conditions (e.g., dementia, Alzheimer disease, cognitive impairment); ear, nose, and throat conditions; dental conditions; frailty; gastrointestinal conditions; hematological conditions (e.g., hemophilia, sickle cell anemia); intellectual or developmental disabilities (e.g., spina bifida, Down syndrome); malnourished populations; obesity; patients in the intensive care unit; skin conditions; sleep disorders; and speech-language conditions.
Two (18.2%) guidelines provided recommendations that involved caregivers, and 5 guidelines (45.5%) provided recommendations for patients living in rural and/or remote areas. One guideline (9.1%) mentioned recommendations for Indigenous Peoples.
Concepts
Main Concepts
We categorized the included scoping reviews as belonging to 1 or 2 concepts: clinical effectiveness and harms of virtual care interventions (Q1) or implementation considerations for virtual care interventions (Q2), with the latter being the more prevalent of the 2 concepts. The included scoping reviews by concept (i.e., research question) are presented in Figure 5 and Figure 6.
Figure 5: Number of Included Scoping Reviews Within Each Concept Under Research Question 1
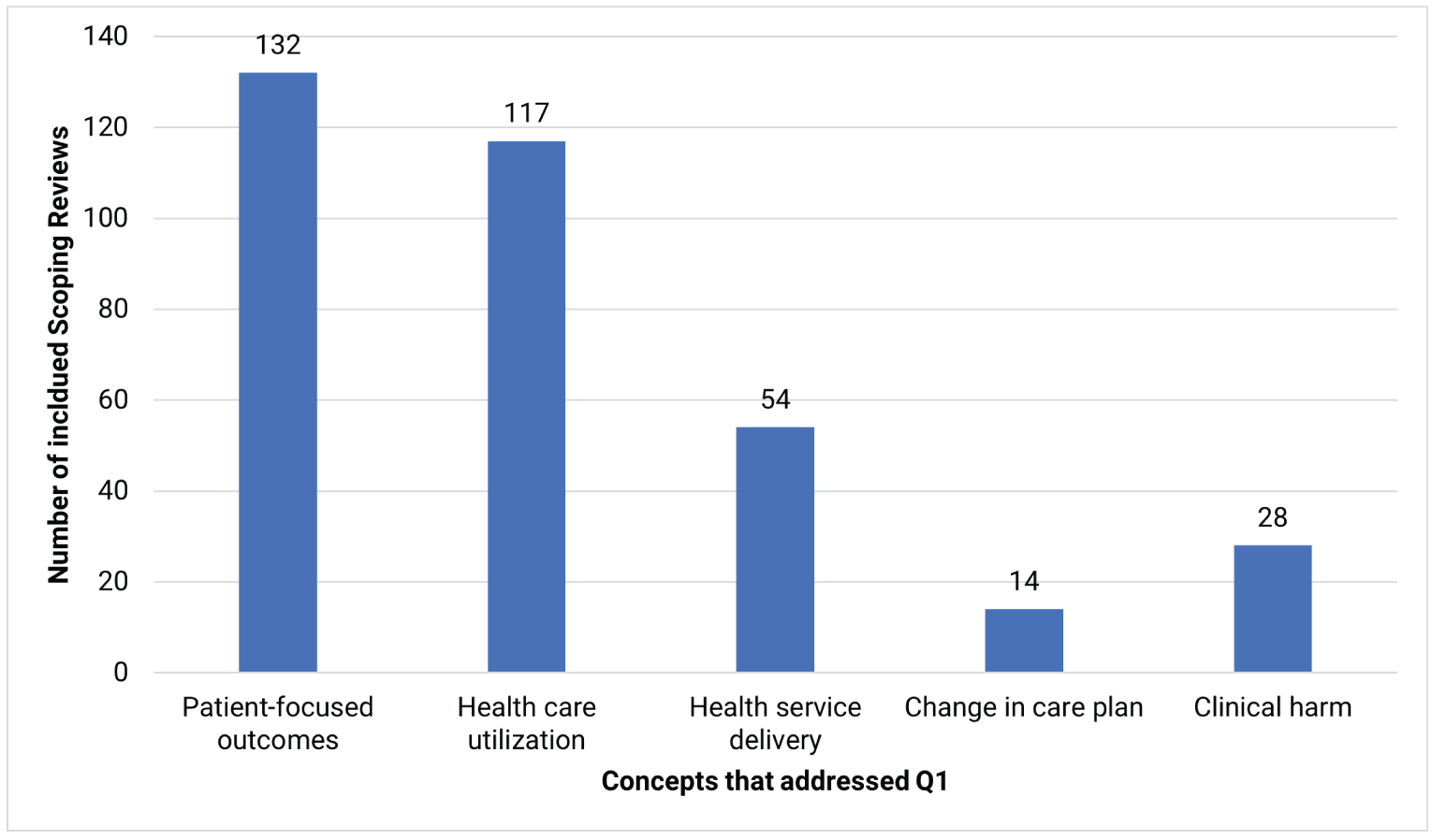
Q1 = research question 1.
Figure 6: Number of Included Scoping Reviews Within Each Concept Under Research Question 2
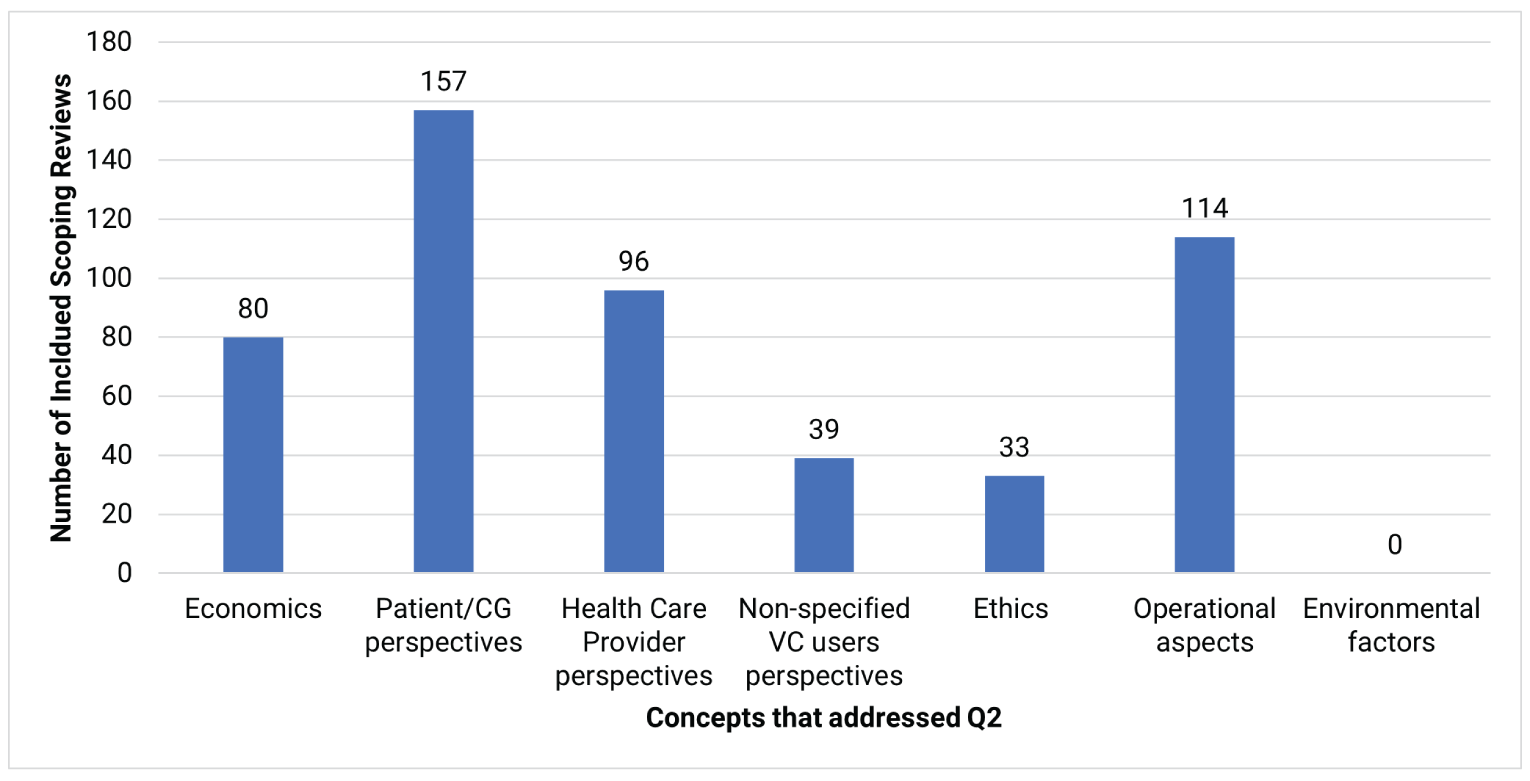
CG = caregiver; Q2 = research question 2; VC = virtual care.
Clinical Effectiveness and Harms (Q1)
Out of the 230 included scoping reviews, 165 (71.7%) reported on many clinical effectiveness and harms variables, each including at least 1 of the following:
patient-focused outcomes (examples of evidence we found include mortality, morbidity [e.g., depression], clinical surrogate measures [e.g., blood pressure], health-related quality of life, functioning, and symptoms [e.g., stress])
health care utilization (examples of evidence we found include general use of health care resources, emergency department visits, hospital admissions or stays, laboratory or imaging orders, specialist referrals, program adherence or uptake, and patient follow-up, adherence, attendance, compliance, or retention)
health service delivery, which focuses on the care being accessed (examples of evidence we found include time to receiving care, wait times, early or improved diagnosis or treatment, and care continuity)
change in a patient’s care plan (examples of evidence we found include change in medication or device use; using a new medical device; change in medical guidance; starting, stopping, or changing dose of medications)
clinical harm (examples of evidence we found include clinical complications, patient safety, and adverse events [any, minor serious], including self-reported events. For instance, outcomes described as harms included rates of hemorrhagic complications for patients receiving care for stroke, clinical complications for patients with spinal cord injuries, amputation and infection rates for patients receiving wound care, adverse chemotherapy side effects for patients receiving treatment for cancer, post-operative breast complications for patients with breast cancer, and withdrawal symptoms and nonfatal overdose for patients with substance use disorders. Outcomes described as safety included instances of contacting school or local authorities for patients receiving care for trauma-focused cognitive behavioural therapy).
Overall, the largest subcategories represented under clinical effectiveness and harms were patient-focused outcomes and health care utilization. In contrast, there were few studies identified by the scoping reviews related to changes in patients’ care plans. In Figure 5, we present a more detailed breakdown of the number of scoping reviews that included studies with evidence on these subcategories.
Implementation Considerations (Q2)
208 of the 230 included scoping reviews (90.4%) reported on many implementation considerations, each including at least 1 of the following:
economics (examples of evidence we found include provider compensation for virtual care visits, cost of virtual care interventions, cost outcomes that are not considered perspectives from patients, health care providers or non-specified virtual care users)
patient or caregiver perspectives, competency, and experiences (examples of evidence we found include preferences based on time, money, travel considerations, experience with digital tools, physical and digital privacy concerns, social support, competency [knowledge/skills/behaviours/confidence/self-management/self-efficacy/digital or technical literacy], and satisfaction)
health care provider perspectives, competency, and experiences (examples of evidence we found include patient–clinician trust, concerns about accuracy, education and training needs for health care providers, social support, competency [knowledge, skills, behaviours, confidence, self-management, self-efficacy, and digital or technical literacy], and satisfaction)
non-specified virtual care user perspectives and experiences for when the included report does not describe patient or health care provider (examples of evidence we found include social support, competency [knowledge, skills, behaviours, confidence, self-management, self-efficacy, and digital or technical literacy], and satisfaction)
ethics (examples of evidence we found include impact on health equity, and consideration of language or cultural needs of patients)
operational aspects (examples of evidence we found include barriers and facilitators to operationalize, how virtual care fits with the existing health care system, physical resources, technological considerations [e.g., equipment, access to technology], infrastructure, governance, government policy, laws, and feasibility).
Overall, the largest subcategories represented under implementation considerations were patients’, caregivers’, or providers’ perspectives, competency, and experiences; and operational aspects. Although we intended to include information from scoping reviews related to environmental factors (e.g., travel and related carbon emissions), we did not locate any scoping reviews that included studies related to these that were not already categorized as patients’ or providers’ perspectives about environmental factors. In Figure 6, we present a more detailed breakdown of the number of scoping reviews that included studies with evidence on these subcategories.
Guidelines (Q3)
A summary of the 11 included guidelines, organized by health specialty, is provided in Table 2.
The included guidelines provided recommendations from health or health care organizations in the following areas:
clinical practice recommendations (examples of recommendations we found include having follow-up appointments through virtual care)
other implementation recommendations (examples of recommendations we found include providing orientations on using technology, incorporating patient preferences)
other virtual care recommendations (examples of recommendations we found include standards for documenting care).
Refer to Figure 7 for a visual display of the number of guidelines that provided a recommendation related to each concept.
Table 2: Summary of Included Guidelines
Guideline name (professional organization, country, year) | Purpose and methods | Types of recommendations provided |
|---|---|---|
Oncology | ||
Delivery of Virtual Care in Oncology/Clinical Guidance for Person-Centred Virtual Cancer Care (Ontario Health [CCO], Canada, 2022)29,30 | Purpose: To provide guidance for health care professionals and administrators on providing virtual care to adult oncology outpatients Methods: Systematic review and Delphi consensus development process involving a multidisciplinary committee |
|
Telehealth in Oncology: ASCO Standards and Practice Recommendations (American Society of Clinical Oncology, US, 2021)31 | Purpose: To provide standards for health professionals and administrators on providing telehealth to oncology patients in general and specialty settings Methods: Systematic review and multidisciplinary expert panel consensus |
|
Obstetrics and gynecology | ||
Michigan Plan for Appropriate Tailored Healthcare in Pregnancy Prenatal Care Recommendations: A Practical Guide for Maternity Care Clinicians (American College of Obstetricians and Gynecologists/University of Michigan, US, 2021)32 | Purpose: To develop new prenatal care delivery recommendations for any maternity care provider in any setting treating average-risk patients Methods: Systematic review and Delphi consensus approach involving an expert panel, or expert opinion (if evidence was lacking) | • Considerations for integrating telemedicine into routine practice (patient preference, logistics, training) |
Guidance for Gynecologists Utilizing Telemedicine During COVID-19 Pandemic Based on Expert Consensus and Rapid Literature Reviews (Society of Gynecologic Surgeons, US, 2020)33 | Purpose: To provide guidance for gynecologists on how to manage common outpatient scenarios through telemedicine Methods: Systematic rapid review of the literature and expert consensus | • Considerations for counselling, assessment, and management of common conditions via telemedicine |
Rheumatology | ||
APLAR Recommendations on the Practice of Telemedicine in Rheumatology (APLAR, Asia Pacific region, 2022)34 | Purpose: To provide guidance on new approaches to rheumatology care via telemedicine Methods: Systematic review and Delphi consensus approach involving experts |
|
Telehealth in Rheumatology: The 2021 Arab League of Rheumatology Best Practice Guidelines (ArLAR, 2021)35 | Purpose: To develop a practical toolkit to assist in implementing telehealth into rheumatology clinics Methods: Literature review and Delphi consensus approach involving a multidisciplinary panel |
|
Cardiovascular conditions | ||
Cardiac Rehabilitation in German Speaking Countries of Europe - Evidence-based Guidelines from Germany, Austria and Switzerland LLKardReha-DACHa - Part 2 (LLKardReha-DACH,a Germany, Austria, and Switzerland, 2021)36 | Purpose: To provide guidance on the delivery of exercise-based cardiac rehabilitation, including via telemedicine Methods: Systematic review and development of the guideline using a consensus process facilitated by the GRADE Evidence-to-Decision Framework |
|
Canadian Stroke Best Practice Recommendations: Secondary Prevention of Stroke Update 2020 (Canadian Stroke Consortium, Canada, 2020)37 | Purpose: To provide guidance on the treatment of stroke for clinicians across a wide range of settings, including virtual care delivery of secondary stroke prevention Methods: Systematic review and consensus process involving an expert panel |
|
Other | ||
Ear, Nose, and Throat Practice Guidelines: An Update for COVID-19 (None, worldwide, 2021)38 | Purpose: To recommend strategies to health professionals that will reduce their exposure to COVID-19 during the pandemic while minimizing constraints to practice Methods: Systematic review |
|
The Management of Substance Use Disorders: Synopsis of the 2021 US Department of Veterans Affairs and US Department of Defense Clinical Practice Guideline (VA and DoD, US, 2021)39 | Purpose: To provide recommendations on the management of substance use disorder, including the use of technology to manage patients remotely Methods: Systematic review and development of the guideline using a consensus process using GRADE methodology |
|
Caring for Patients With Pain During the COVID-19 Pandemic: Consensus Recommendations From an International Expert Panel (International expert panel, global, 2020)40 | Purpose: To develop therapeutic considerations and recommendations to assist in health care providers in continuing to provide care to patients with chronic pain during the COVID-19 pandemic Methods: Systematic literature search and expert panel discussion |
|
APLAR = Asia Pacific League of Associations for Rheumatology; ArLAR = Arab League of Associations for Rheumatology; ASCO = American Society of Clinical Oncology; DoD = US Department of Defense; GRADE = Grading of Recommendations Assessment, Development, and Evaluation; VA = US Department of Veterans Affairs.
aIncludes the German Society for Cardiovascular Prevention and Rehabilitation, Austrian Society of Cardiology, and the Swiss Working Group for Cardiovascular Prevention, Rehabilitation, and Sports Cardiology.
Figure 7: Number of Included Guidelines Within Each Concept Under Research Question 3
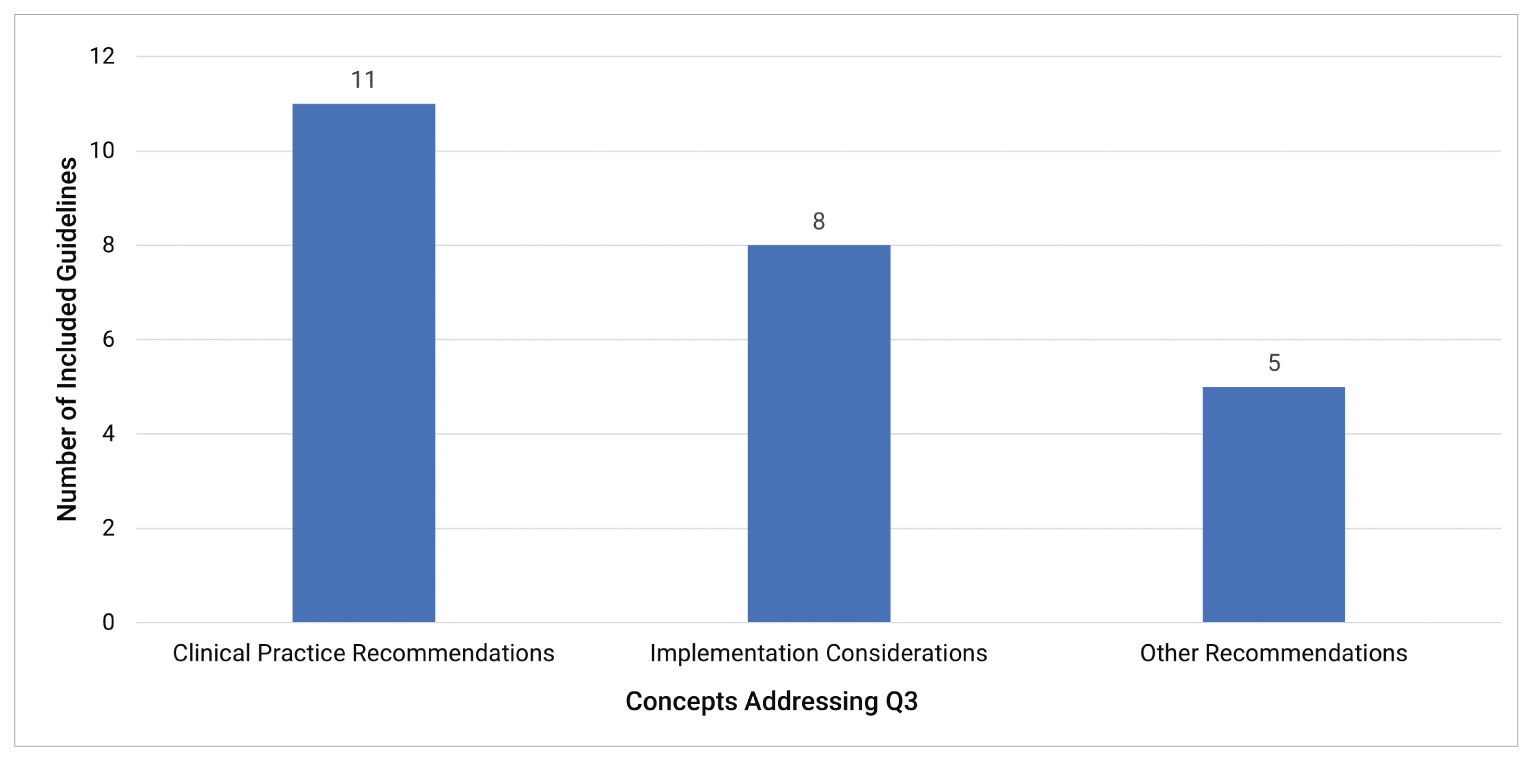
Q3 = research question 3.
Context
Scoping Reviews (Q1 and Q2)
We found that virtual care format was reported in a variety of ways across the included scoping reviews, and it was not always described clearly for each study within each scoping review. As shown in Figure 8, of the 230 included scoping reviews, 205 (89.1%) reported the virtual care format for at least 1 of the relevant studies included in their review, and 25 (11.0%) did not. The following virtual care formats were described: telephone calls (n = 143; 62.2%), video (n = 145; 63.0%), text messages or short messaging service (n = 72; 31.3%), emails (n = 53; 23.0%), or other online methods (n = 103; 44.8%). Examples of other online methods included mobile applications that allowed for the health care provider to connect with the patient and web-based patient portals with a chat feature.
Figure 8: Number of Included Scoping Reviews by Reported Virtual Care Format
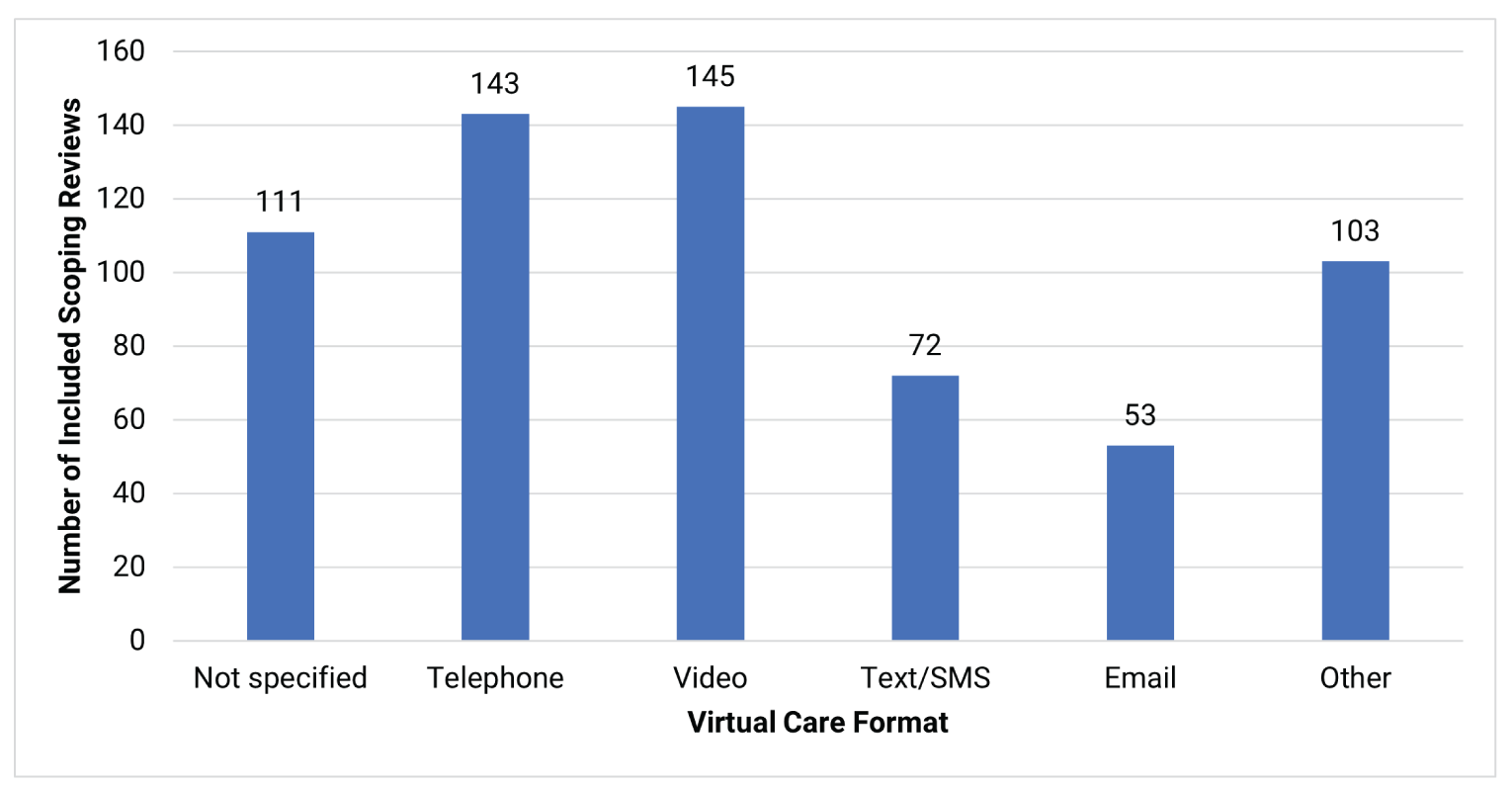
SMS = short message service.
Notes: The other category pertains to other online methods (e.g., mobile applications that allowed for the health care provider to connect with the patient, web-based patient portals with a chat feature).
Guidelines (Q3)
As shown in Figure 9, of the 11 included guidelines, 10 (90.9%) provided recommendations related to virtual care without specifying the format. Recommendations about the following virtual care formats were described: telephone calls (n = 6; 54.5%), video (n = 5; 45.5%), text messages (n = 1; 9.1%), emails (n = 2; 18.2%), or other online methods (n = 3; 27.3%).
We provide detailed summary tables of the included reports in the Supporting Information document (refer to Summary Tables of Included Reports), which can be used to understand which populations or outcomes are reported by each included report. Further, the summary tables can also show potential gaps where evidence or recommendations have not been found for a particular population or concept; these potential gaps can be used to inform future research in these areas. We have provided evidence maps of the charted data from all included reports in an Excel file (refer to CADTH’s Virtual Care Evidence Maps), which can be used to sort and identify references of interest. The reference lists in the Supporting Information document (refer to Included Reports and References of Potential Interest) can be further consulted to find the individual studies included in the scoping reviews or informing the guidelines to gain further details about populations, outcomes, and findings. The Supporting Information document (refer to Supplementary Report on Included Guidelines) provides a supplementary report on the 11 included evidence-based guidelines and their recommendations relevant to virtual care, which can be considered by health professionals to inform their practice.
Figure 9: Number of Included Guidelines by Reported Virtual Care Format
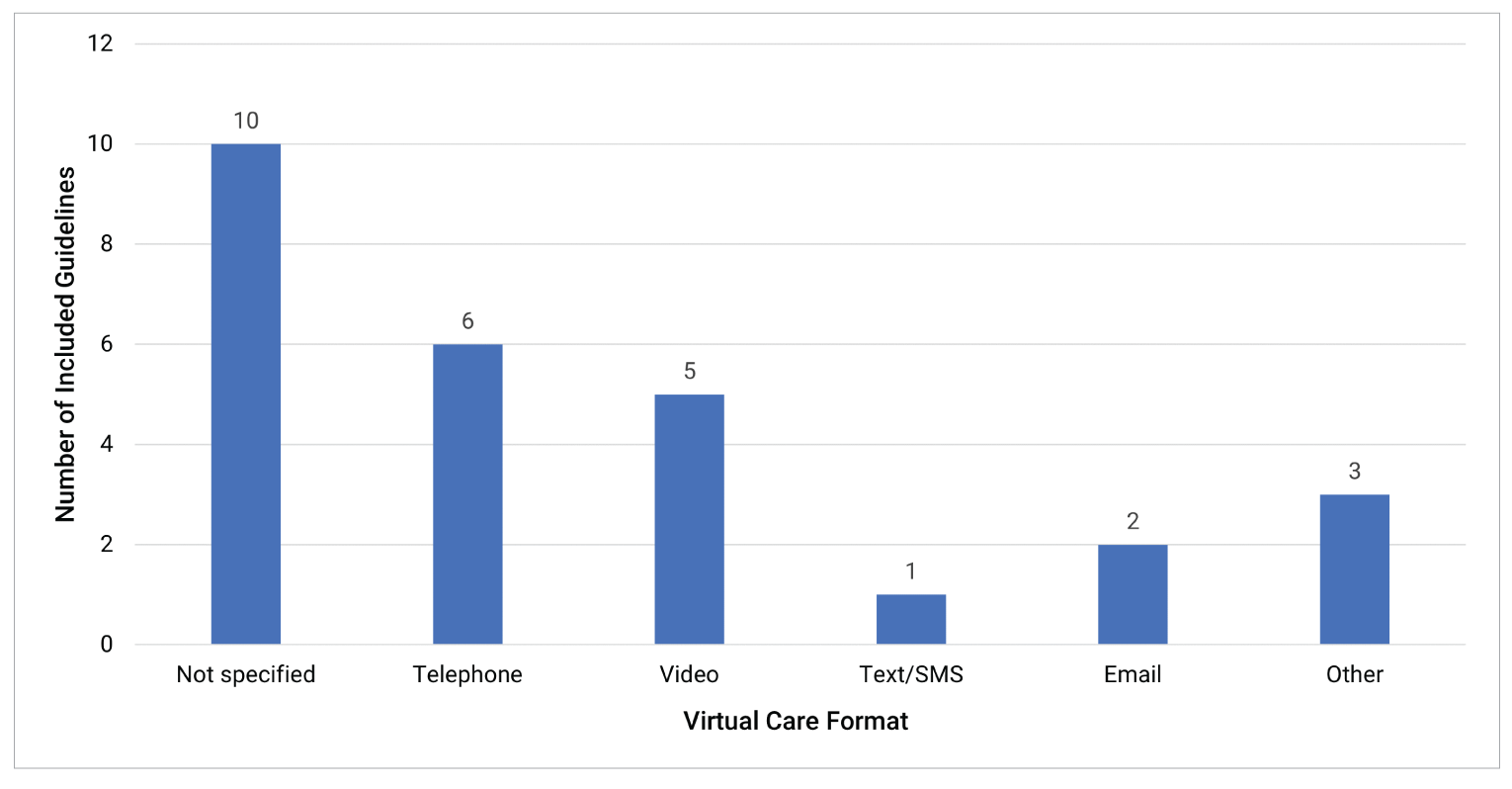
SMS = short message service.
Notes: The other category pertains to other online methods (e.g., mobile applications that allowed for the health care provider to connect with the patient, web-based patient portals with a chat feature).
Discussion
We conducted a rapid scoping exercise, an adapted method of a scoping review, to quickly identify evidence (via other scoping reviews) about the clinical effectiveness, harms, and implementation considerations for virtual health care interventions, as well as clinical practice recommendations and other implementation recommendations (via evidence-based guidelines) regarding virtual care, in people of all ages, across all geographic areas. Our work was most suited to scoping review methods since the aim was to identify the literature on this broad topic and display existing evidence and potential gaps through our summary tables. The potential gaps identified are areas where it may be feasible and informative to perform future work, which can contribute to health organizations’ larger digital health initiatives. We provide reference lists for the included reports so that readers can consult the original publications to gain further details. We also provide a supplementary report on the 11 included evidence-based guidelines and their recommendations relevant to virtual care, which can be considered by health professionals to inform their practice.
During this rapid scoping exercise, we identified 230 relevant scoping reviews from the literature search. These scoping reviews reported evidence in the form of clinical effectiveness outcomes (i.e., patient-focused outcomes, health care utilization, health service delivery, change in a patient’s care plan) and clinical harm outcomes (e.g., clinical complications, patient safety, adverse events). The scoping reviews also included studies that reported evidence of varying degrees for key implementation considerations including economics, ethics, operational aspects, and perspectives, competency, and experiences from any virtual care user. Moreover, we identified 11 relevant evidence-based guidelines, which provided recommendations for virtual health care: all guidelines provided clinical practice recommendations, and 8 provided implementation considerations.
Given the abbreviated timeline of the project, we took an iterative approach for this rapid scoping exercise, incorporating a phased approach to limit or expand the type of study designs to include based on the number of records to screen and the breadth of evidence found. We first included scoping reviews and evidence-based guidelines since these study designs would efficiently summarize and capture the breadth of literature in this emerging field. With the large volume of scoping reviews identified in the first phase, additional study designs, such as systematic reviews and primary studies, were not considered eligible, and our findings reflect the available evidence from the scoping reviews and evidence-based guidelines we have found.
The literature on virtual care is increasing over time, and this trend will likely continue, considering our search included literature from 2020 to 2022 and yielded a large quantity of scoping reviews. Most of the scoping reviews were not focused on a particular country or region, suggesting that these reviews aimed to capture evidence about virtual care globally. Since we did not restrict our eligibility criteria to specific patient populations, it is encouraging to see there is evidence relating to key clinical effectiveness and harms outcomes and implementation considerations across multiple facets of patient populations, including patient age, condition, and location of residence. Moreover, there was a similar distribution of studies that reported on each age group category, suggesting there is evidence and applicability of virtual care across the lifespan of an individual. Many patient conditions (e.g., cancer, diabetes, substance use disorders) were reported, with 30% of the included scoping reviews focusing on patients with or receiving care for mental health disorders, such as anxiety, depression, eating disorders, and post-traumatic stress disorder. Approximately one-third of the scoping reviews included studies on, and about half of guidelines referenced, patients residing in rural or remote settings, and 1 guideline and 7% of the scoping reviews included studies that reported about Indigenous Peoples. These data would be informative for knowledge users looking to service these communities; however, more work may be needed in these areas.
There were areas in our summary tables that indicated a large quantity of evidence as identified from the included scoping reviews and potential gaps. Much of the published literature on virtual care included in the scoping reviews has focused on perspectives, competency, and experiences of virtual care user groups. In contrast, fewer scoping reviews included studies that reported on changes in patients’ care plans, clinical harms for patients, environmental considerations, and ethical considerations. The 11 evidence-based guidelines covered 7 health specialties. There may be potential gaps for guidelines that have recommendations for primary health care and those with specific recommendations for certain conditions such as mental health disorders and diabetes.
This report extends on the previous CADTH work conducted about virtual care, most recently a reference list on virtual oncology visits published in July 202219 and a rapid review on virtual care use in primary care or specialist care settings published in August 2022.20 Potential gaps where there is limited to no evidence or recommendations identified in our report can be used as a starting point for further research. A proposed next step may be to focus on a subset of the topic (e.g., a specific population or type of virtual care format) to investigate further depth or context about the topic. This report may also be useful to inform future health technology assessments in virtual care.
Limitations
Our literature search was limited to studies published in English or French from 2020 or later, mainly based on feasibility of producing a rapid scoping report. Since the language restriction was applied at the level of the search, it is not clear how many studies may have been excluded for this reason, and findings could differ had other languages been included.
Due to the wide range of topics covered and time constraints, we limited our study design eligibility criteria to existing scoping reviews and evidence-based guidelines (i.e., first phase of the iterative rapid scoping approach), did not search reference lists of included studies, nor contact experts to supplement the search; as a result, there is a possibility that some relevant studies were missed, and it is uncertain whether this would have an impact on the overall high-level findings. The overlap between the scoping reviews was not investigated, and included studies are likely to have been captured by multiple scoping reviews. We used a virtual care definition that reflects how virtual care is defined in Canada,9 although there may have been differences in which studies were included and excluded if another definition was used. The variability of definitions for virtual care and classification across the spectrum of digital health is indicative of the rapidly evolving nature of this topic. We expect that the findings from this report will showcase virtual care from the lens that is most applicable to Canada, where CADTH and our customers reside.
For scoping reviews, we reported what the reviews found in the literature and not what they intended to include (i.e., their eligibility criteria). For the purposes of this rapid scoping, we believe this is the most productive approach to provide readers with a snapshot of what evidence exists thus far in the literature and what results can inform virtual care practice at this time. Another limitation is that our charting was based on several elements (e.g., age group, population condition, virtual care format) and several categories within each element, and if more than 1 category was selected within each element, then we would not be able to determine the specific combination of categories for which there is evidence. For example, if children, adults, diabetes, and cancer were all marked for a scoping review, it would not be clear whether there was 1 primary study within the scoping review with results for all of these groups, or if there were multiple primary studies within the scoping review that reported on various combinations of these categories. We also assumed that when evidence was not reported in the results of the included scoping reviews or in the recommendations from the included guidelines, it meant that there was a gap in the evidence. However, we relied on the authors of the scoping reviews and guidelines to comprehensively search the literature and report relevant findings; as such, gaps identified in our report are treated as potential gaps. To expand on our work, future studies could report what scoping reviews aimed to find and found no evidence for, as this would provide a more detailed picture of the gaps in the evidence base.
Another limitation is that we included scoping reviews and guidelines where there was clear reporting of an interaction between health care professionals and patients. In some cases, it was unclear whether certain studies included in the scoping reviews were about virtual care specifically or any digital health intervention, or whether recommendations in relevant guidelines applied only to virtual care or to all forms of digital health technologies. For scoping reviews, we only reported information from studies included in them if they were clearly about this interaction. For guidelines, we reported all recommendations where the guideline itself mentioned an interaction between a patient and a provider at least once; therefore, not all recommendations may be relevant for virtual care that involves this interaction.
Finally, knowledge user input on this rapid scoping exercise will be limited to peer review of the draft report by 1 clinical expert. People accessing any health care service through virtual care are an integral part of knowledge users, although they did not provide direct input for this rapid scoping exercise.
Conclusions
A large quantity of scoping reviews have been published since 2020 on virtual care. We provide visualizations of the existing evidence identified from the included scoping reviews, as well as potential gaps by age group, population type, clinical effectiveness and harms, and implementation considerations which can be used to identify relevant scoping reviews that report results in these areas. Many clinical practice recommendations and other implementation recommendations for virtual care were also identified from the included evidence-based guidelines that can be used to inform the appropriate practice of virtual care. Potential gaps where there is limited or no literature identified in our report are evidence on clinical harms, ethical considerations, environmental considerations, recommendations for virtual care for primary health care, and guidance for certain conditions such as mental health disorders and diabetes; these areas may be considered opportunities for future work.
References
1.World Health Organization. Archived: WHO Timeline - COVID-19. 2020; https://www.who.int/news/item/27-04-2020-who-timeline---covid-19. Accessed 2022 Aug 30.
2.Nunavut's Virtual Care Action Plan. Ottawa (ON): Health Canada; Nunavut Department of Health; 2022: https://www.canada.ca/en/health-canada/corporate/transparency/health-agreements/bilateral-agreement-pan-canadian-virtual-care-priorities-covid-19/nunavut-action-plan.html. Accessed 2022 Aug 31.
3.Virtual Care Task Force. Virtual care in Canada: progress and potential. Mississauga (ON): College of Family Physicians of Canada; 2022: https://www.royalcollege.ca/rcsite/documents/health-policy/report-virtual-care-task-force-2022-e.pdf. Accessed 2022 Sep 1.
4.Wang Y, Zeng L, Yao S, et al. Recommendations of protective measures for orthopedic surgeons during COVID-19 pandemic. Knee Surg Sports Traumatol Arthrosc. 2020;28(7):2027-2035. PubMed
5.Northwest Territories Health and Social Services Authority. Public notice - March 17th NTHSSA Operational Update. 2020; https://www.nthssa.ca/en/newsroom/public-notice-march-17th-nthssa-operational-update. Accessed 2022 Aug 31.
6.Canadian Institute for Health Information. Virtual care: A major shift for Canadians receiving physician services. Ottawa (ON): CIHI; 2022: https://www.cihi.ca/en/virtual-care-a-major-shift-for-canadians-receiving-physician-services. Accessed 2022 Aug 24.
7.Mehrotra A, Bhatia RS, Snoswell CL. Paying for telemedicine after the pandemic. JAMA. 2021;325(5):431-432. PubMed
8.Canadian Institute for Health Information. Virtual care in Canada: strengthening data and information. Ottawa (ON): CIHI; 2022: https://www.cihi.ca/sites/default/files/document/virtual-care-in-canada-strengthening-data-information-report-en.pdf. Accessed 2022 Sep 1.
9.Jamieson T, Wallace R, Armstrong K, et al. Virtual care: a framework for a patient-centric system. Toronto: Women’s College Hospital Institute for Health Systems Solutions and Virtual Care (WIHV); 2015: https://www.womenscollegehospital.ca/assets/pdf/wihv/WIHV_VirtualHealthSymposium.pdf. Accessed 2022 Aug 18.
10.CHIEF Executive Forum Virtual Care Working Group. Virtual care in Canada: lexicon. (CHIEF Executive Forum Resource). Toronto (ON): Digital Health Canada; 2022: https://digitalhealthcanada.com/wp-content/uploads/2022/06/Virtual-Care-National-Lexicon-v-JAN2521.pdf. Accessed 2022 Jul 28.
11.Bhatia RS, Jamieson T, Shaw J, Piovesan C, Kelley LT, Falk W. Canada’s virtual care revolution: a framework for success. (Commentary no. 586). Toronto: C.D. Howe Institute; 2020: https://www.cdhowe.org/sites/default/files/attachments/research_papers/mixed/Commentary_586.pdf. Accessed 2022 Sep 1.
12.Environmental and financial benefits of virtual care. Toronto: Canada Health Infoway; 2022: https://www.infoway-inforoute.ca/en/component/edocman/3885-environmental-and-financial-benefits-of-virtual-care-in-canada/view-document?Itemid=0. Accessed 2022 Aug 22.
13.Canada Health Infoway. Analysis of the current and potential benefits of virtual care in Canada. Toronto (ON): Canada Health Infoway; 2020: https://www.infoway-inforoute.ca/en/component/edocman/3819-analysis-of-the-current-and-potential-benefits-of-virtual-care-in-canada/view-document?Itemid=101. Accessed 2022 Jul 19.
14.CMA Health Summit. Virtual care in Canada: discussion paper. Ottawa (ON): Canadian Medical Association (CMA); 2019: https://www.cma.ca/sites/default/files/pdf/News/Virtual_Care_discussionpaper_v2EN.pdf. Accessed 2022 Aug 18.
15.House A, Roberts J. Telemedicine in Canada. Can Med Assoc J. 1977;117(4):386. PubMed
16.2021 national survey of Canadian physicians: quantitative market research report. Toronto: Canada Health Infoway; Canadian Medical Association (CMA); 2021: https://www.infoway-inforoute.ca/en/component/edocman/3935-2021-national-survey-of-canadian-physicians/view-document?Itemid=0. Accessed 2022 Aug 23.
17.Falk W. The state of virtual care in Canada as of wave three of the COVID-19 pandemic: an early diagnostique and policy recommendations. Ottawa (ON): Health Canada; 2021: https://www.canada.ca/content/dam/hc-sc/documents/corporate/transparency_229055456/health-agreements/bilateral-agreement-pan-canadian-virtual-care-priorities-covid-19/template-wf-report-eng.pdf. Accessed 2022 Jul 06.
18.Budhwani S, Fujioka J, Thomas-Jacques T, et al. Challenges and strategies for promoting health equity in virtual care: findings and policy directions from a scoping review of reviews. J Am Med Inform Assoc. 2022;29(5):990-999. PubMed
19.Khangura SD, Severn M. Virtual oncology visits. (CADTH reference list: summary of abstracts). Ottawa (ON): CADTH; 2022: https://www.cadth.ca/sites/default/files/pdf/htis/2022/RB1618Virtual-Oncology-Visits-Final.pdf. Accessed 2022 Jul 29.
20.Nayakarathna R, Neilson H, MacDougall D, Cowling T. Virtual care use in primary care or specialty care settings. (CADTH Health Technology Review). Can J Health Technol. 2022;2(8). https://canjhealthtechnol.ca/index.php/cjht/article/view/RC1444. Accessed 2022 Aug 30.
21.Tricco AC, Lillie E, Zarin W, et al. PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med. 2018;169(7):467-473. PubMed
22.Peters M, Godfrey C, McInerney P, Munn Z, Tricco A, Khalil H. Chapter 11: Scoping Reviews (2020 version). In: Aromataris E, Munn Z, eds. JBI Manual for Evidence Synthesis. Adelaide (Australia): JBI; 2020: https://synthesismanual.jbi.global. Accessed 2022 Apr 21.
23.Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Syst Rev. 2021;10(1):1-11. PubMed
24.CADTH. Grey matters: a practical tool for searching health-related grey literature. 2019; https://greymatters.cadth.ca/. Accessed 2022 Sep 1.
25.Health Canada. eHealth. 2010; https://www.canada.ca/en/health-canada/services/health-care-system/ehealth.html. Accessed 2022 Sep 12.
26.Jogova M, Shaw J, Jamieson T. The regulatory challenge of mobile health: lessons for Canada. Healthc Policy. 2019;14(3):19-28. PubMed
27.Khangura S, Konnyu K, Cushman R, Grimshaw J, Moher D. Evidence summaries: the evolution of a rapid review approach. Syst Rev. 2012;1(1):10. PubMed
28.O'Blenis P, Evidence Partners DistillerSR. One simple way to speed up your screening process. 2017; https://blog.evidencepartners.com/one-simple-way-to-speed-up-your-screening-process. Accessed 2022 Apr 21.
29.Ontario Health (Cancer Care Ontario). Person-centred virtual cancer care clinical guidance. Toronto: Ontario Health (Cancer Care Ontario); 2022: https://www.cancercareontario.ca/en/guidelines-advice/types-of-cancer/69581. Accessed 2022 Sep 1.
30.Cheung MC, Franco BB, Meti N, et al. Delivery of virtual care in oncology: province-wide interprofessional consensus statements using a modified Delphi process. Curr Oncol. 2021;28(6):5332-5345. PubMed
31.Zon RT, Kennedy EB, Adelson K, et al. Telehealth in oncology: ASCO standards and practice recommendations. JCO Oncol Pract. 2021;17(9):546-564. PubMed
32.Peahl AF, Turrentine M, Barfield W, Blackwell SC, Zahn CM. Michigan plan for appropriate tailored healthcare in pregnancy prenatal care recommendations: a practical guide for maternity care clinicians. J Womens Health. 2022;12:12. PubMed
33.Grimes CL, Balk EM, Dieter AA, et al. Guidance for gynecologists utilizing telemedicine during COVID-19 pandemic based on expert consensus and rapid literature reviews. Int J Gynaecol Obstet. 2020;150(3):288-298.PubMed
34.Ahmed S, Grainger R, Santosa A, et al. APLAR recommendations on the practice of telemedicine in rheumatology. Int J Rheum Dis. 2022;25(3):247-258. PubMed
35.Ziade N, Hmamouchi I, El Kibbi L, et al. Telehealth in rheumatology: the 2021 Arab League of Rheumatology best practice guidelines. Rheumatol Int. 2022;42(3):379-390. PubMed
36.Schwaab B, Bjarnason-Wehrens B, Meng K, et al. Cardiac rehabilitation in German speaking countries of Europe-evidence-based guidelines from Germany, Austria and Switzerland LLKardReha-DACH-Part 2. J Clin Med. 2021;10(14):12. PubMed
37.Gladstone DJ, Lindsay MP, Douketis J, et al. Canadian stroke best practice recommendations: secondary prevention of stroke update 2020. Can J Neurol Sci. 2022;49(3):315-337. PubMed
38.Kapoor S, Gupta A, Saidha PK. Ear, nose, and throat practice guidelines: an update for COVID-19. Int Arch Otorhinolaryngol. 2021;25(4):e621-e627. PubMed
39.Perry C, Liberto J, Milliken C, et al. The management of substance use disorders: synopsis of the 2021 U.S. Department of Veterans Affairs and U.S. Department of Defense clinical practice guideline. Ann Intern Med. 2022;175(5):720-731. PubMed
40.Shanthanna H, Strand NH, Provenzano DA, et al. Caring for patients with pain during the COVID-19 pandemic: consensus recommendations from an international expert panel. Anaesthesia. 2020;75(7):935-944. PubMed
ISSN: 2563-6596
Cite As: Virtual Care Rapid Scoping. Ottawa: CADTH; 2022 Nov (CADTH Health Technology Review).
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.