Drugs, Health Technologies, Health Systems
Health Technology Review
Teleoptometry for Eye Exams
Key Messages
What Is the Issue?
Teleoptometry can offer vision and eye health services to people living in areas where there is a shortage of optometrists and ophthalmologists. However, there is a need to evaluate the potential benefits and potential harms of teleoptometry to ensure that all people receive high-quality eye care, regardless of their place of residence.
The relative accuracy and utility of teleoptometry compared to in-person eye exams is unclear. The need for this review was identified by a policy decision-maker, and this review is a response to that request.
What Did We Do?
To inform decisions on the use of teleoptometry for comprehensive eye exams and for screening, diagnosing, and monitoring eye disease, we conducted a Rapid Review to summarize evidence that compared the clinical effectiveness, diagnostic test accuracy, and clinical utility of teleoptometry to in-person eye exams. We also sought to identify evidence-based guidelines regarding the use of teleoptometry.
We searched key resources, including journal citation databases, and conducted a focused internet search for relevant evidence published since 2020.
The purpose of this report is to summarize and critically appraise the available evidence on the topic, but it does not provide formal recommendations about teleoptometry. The report was externally reviewed by a clinical expert.
What Did We Find?
We identified several limitations with relevant studies that impact the interpretation of their findings and the generalizability of the evidence. Teleoptometry exams varied greatly in how they were delivered (e.g., asynchronous, synchronous), the types and number of eye tests included, and who performed the in-person components. Some studies included only a small number of eye tests for the teleoptometry and the in-person exam, which may not reflect current clinical practice. In general, the study participants were relatively young, and most studies did not account for disease severity, limiting conclusions for older adults and different stages of disease.
For adults with no known vision or eye conditions, teleoptometry may be similar to in-person eye exams in detecting and managing reduced vision due to uncorrected refractive error. However, teleoptometry may miss some ocular health abnormalities. Eye care providers may feel less confident, and patients less satisfied, with teleoptometry. These findings are based on the results from 1 cross-sectional study.
When used for screening eye diseases and conditions, teleoptometry showed high specificity in most studies (9 test accuracy studies). This means it is generally good at correctly classifying people who do not have certain eye diseases or conditions.
The sensitivity of teleoptometry to detect eye diseases and conditions varied within and across the 9 included studies. Teleoptometry showed good to high sensitivity for some conditions (i.e., cataracts; clinically significant macular edema; nystagmus; and abnormalities of the cornea, anterior chamber, iris, or lens), correctly identifying about 85% to 93% of people with these indications. However, sensitivity was very low to moderate for other conditions (e.g., diabetic retinopathy, glaucoma, age-related macular degeneration), meaning these conditions may be missed in teleoptometry exams.
Teleoptometry may offer a similar ability to inform patient management plans as an in-person exam in pediatric patients with some ocular features or pathologies. These findings are based on the results from 1 cross-sectional study. We did not find any evidence about the clinical utility of teleoptometry for the screening, diagnosing, or monitoring of eye diseases in adults.
For people with diabetic retinopathy, 1 guideline recommends that teleoptometry programs may use retinal imaging (stereoscopic or non-stereoscopic), reimage or refer individuals with poor-quality images, and use relevant clinical history to support image interpretation and reporting.
For people with primary open-angle glaucoma, 1 guideline recommends that teleoptometry can improve access to care but that teleoptometry should not be used alone or for the assessment or management of moderate or advanced disease.
We did not find any studies that compared teleoptometry to in-person comprehensive eye exams in children, and we did not find any guidelines about the use of teleoptometry for routine comprehensive eye exams in adults or children.
What Does This Mean?
Teleoptometry may be a suitable alternative to an in-person eye exam in some adults for assessing reduced vision due to uncorrected refractive error and identifying some ocular conditions. However, the evidence was limited to 1 study with a small number of participants, and it is unclear whether teleoptometry would be a suitable replacement for a comprehensive eye exam.
The accuracy of teleoptometry for screening and diagnosing eye diseases varies by condition and may depend on the diagnostic tests performed and the training of the individual collecting the data. Teleoptometry is generally good at identifying people without eye diseases but may miss some conditions in people who do have them. Several study limitations lower our confidence in these results, suggesting that teleoptometry may not fully replace in-person eye care in all clinical situations.
To inform their decisions about the use of teleoptometry, decision-makers can consider the limitations of the technology, whether it is appropriate for the clinical scenario, the type and design of the teleoptometry exam, and the individual needs and preferences of the individuals being examined.
Decision-makers may also wish to consider whether the provision of teleoptometry would impact access to eye care, particularly in areas or populations that may otherwise be underserved by eye care professionals. In such areas, teleoptometry may serve to increase access to eye care or augment in-person eye care.
Abbreviations
AMD
age-related macular degeneration
AOA
American Optometric Association
ATA
American Telemedicine Association
CAO
Canadian Association of Optometrists
CI
confidence interval
KAC
Krippendorf alpha coefficient
SR
systematic review
Research Questions
What is the clinical effectiveness of teleoptometry versus an in-person eye examination for a comprehensive eye exam?
What is the diagnostic test accuracy of teleoptometry versus an in-person eye examination for screening and diagnosing eye diseases and conditions?
What is the clinical utility of teleoptometry versus an in-person eye examination for screening, diagnosing, and monitoring eye diseases and conditions?
What are the recommendations regarding the use of teleoptometry for comprehensive eye exams?
What are the recommendations regarding the use of teleoptometry for screening, diagnosing, and monitoring eye diseases?
Context and Policy Issues
Eye Exams and Eye Health
Vision quality and eye health are important parts of overall health and well-being. Vision loss can have negative impacts on quality of life because it can impact employment opportunities, activities of daily living, and social interaction and can increase the risk of falls and fractures.1 The results from the 2021 Canadian longitudinal study on aging suggest that factors associated with the 3-year incidence of visual impairment include older age, race self-reported as Black, lower household income, status as a current smoker, and province of residence.2 Sex, education level, and living in a rural and/or remote location were not associated with the 3-year incidence of visual impairment.2
A comprehensive eye exam, also known as a general eye exam, includes an optometrist’s assessment of vision quality, visual function (e.g., eye movement, eye coordination, the ability of the eyes to focus), and the internal and external health of the eyes.3 The components of a comprehensive eye exam include case history, measurement of visual acuity with and without corrective lenses, assessment of refractive error, evaluation of binocular vision status, and examination of eye health (i.e., intraocular pressure, slit lamp assessment, dilated fundus exam) to check for eye conditions and diseases.4,5 In addition to determining vision issues, comprehensive eye exams are an important part of preventive health care, as they can detect eye conditions and diseases such as dry eye, diabetic retinopathy, glaucoma, and age-related macular degeneration (AMD).4 Many eye diseases do not have symptoms in the early stages and may initially go unnoticed, but regular eye exams can help identify these diseases early to help prevent vision loss.6 The Canadian Association of Optometrists (CAO) recommends that adults aged 20 to 64 years should have a comprehensive eye exam at least every 2 years.3 The CAO also recommends a comprehensive eye exam at least once a year for adults living with diabetes and adults aged 65 and older and a comprehensive eye exam every 12 months in school-aged children. The presence of other systemic or ocular health conditions may require more frequent partial or comprehensive eye exams, but their frequency is determined by clinicians based on the ocular health condition and the individual’s personal medical history and family history.
Coverage for comprehensive eye exams is at the discretion of each province and territory, is unequal across Canada, and is dependent on the geographical location and age of the person being examined.7 For individuals who do not fall within the groups covered by provincial health insurance programs, comprehensive eye exams may be covered through insurance plans (private or job based) or through government-funded benefits programs,8,9 or they may need to be paid for out of pocket. In November 2024, an act was tabled to establish a national strategy for eye care to ensure better health outcomes for people living in Canada.10 Signalling the importance of supporting the prevention and treatment of eye diseases and vision rehabilitation, the national strategy may include measures to identify the training and guidance needs for health care professionals, promote research and improve data collection, promote information sharing between different levels of government, and ensure that the Minister of Health is able to rapidly examine (as appropriate) drug and device applications intended for use for eye diseases.10
In a 2025 report, the CAO described regional variation in the number of optometrists in Canada, ranging from 22.2 optometrists per 100,000 people in Alberta to 11.2 optometrists per 100,000 people in Newfoundland and Labrador (based on 2021 census data).11 The CAO identified a “notable shortage” of optometrists in areas outside of urban centres in every province, including rural and remote areas. This suggests that access to an eye care provider depends, in part, on where people live. The CAO also noted that some underserved populations, such as First Nations communities and certain populations within urban centres (not further described), may experience difficulty accessing optometric care.11 For people living in areas with a shortage of optometry and ophthalmology services or for populations that may otherwise experience difficulty accessing traditional in-person eye care services, teleoptometry may be a suitable alternative to provide vision and eye health services.
What Is Teleoptometry?
Teleoptometry is the provision of vision and eye health services using electronic health information and medical and communication technologies without physical contact between the health care provider and the person being examined.12,13 It can be used to provide comprehensive eye exams, including screening for specific ocular diseases such as diabetic retinopathy, glaucoma, and AMD.14,15 However, some components of a comprehensive eye exam are currently challenging or unable to be performed remotely (e.g., slit lamp examination of the anterior segment, assessment of pupillary reflexes, dilated fundus exam, gonioscopy).14,16
Teleoptometry can be delivered synchronously, asynchronously, or through a combination of both modalities.12,16
Synchronous teleoptometry: The eye exam is conducted in real time, with the person being examined and the optometric assistant in the clinic and the optometrist in another location.12,16
Certain tests require the support of an assistant (e.g., cover test, eye movements) and can be video-streamed live for synchronous evaluation; other tests can be controlled remotely by the optometrist (e.g., subjective refraction, certain binocular vision tests).16
The workflow is similar to the experience and expectations of an in-person exam.12
Asynchronous teleoptometry: This modality relies on an optometric assistant to gather clinical data (e.g., automated tests, questionnaires) without the presence of an optometrist. The data are collected and sent for review by the optometrist at a later time (e.g., a video of a test is recorded for asynchronous review). This model is also known as “store and forward.”12,16 This model of teleoptometry has strengths and limitations, including:
It offers flexibility for the clinician (e.g., clinical data can be reviewed at any time and from any location).12
Retesting or improving the quality of the data are not possible once the person being examined has left the clinic.12
Not all components of the exam can be performed by an optometric assistant, and an asynchronous model alone is incompatible with a comprehensive eye exam.
Uses for asynchronous teleoptometry could include remote patient monitoring and disease-specific screening.14
Current Status of Teleoptometry in Canada
Although interest in virtual care, including teleoptometry, has been increasing for decades, the COVID-19 pandemic expanded and accelerated its use and acceptance in Canada.12,16 In a 2021 position statement, the CAO supported the ongoing use of teleoptometry to augment in-person care and its use as an essential mechanism for the provision of eye care when there are barriers to care.17 The CAO also “supports fair and equitable reimbursement and coverage for teleoptometry services.”17
According to the CAO, for the provision of teleoptometry, providers must be familiar with the health care system in their geographical region and that of the person being examined, and optometrists must adhere to their provincial regulator’s guidelines on teleoptometry or, should provincial guidelines not exist, to the Federation of Optometric Regulatory Authorities of Canada policy on teleoptometry.16
Several considerations may impact the adoption of teleoptometry in Canada. As with any form of virtual care, there are concerns about data ownership, privacy, and cybersecurity due to the collection, storage, transmission, and use of personal health data.12,16 Teleoptometry requires a stable and high-speed internet connection for the remote operation of equipment (e.g., digital phoropter) for synchronous teleoptometry and for the forwarding of data for asynchronous teleoptometry, which may be an issue in some remote areas.12,14,16 Providers may also experience technical challenges when learning to work with new technology (e.g., new software and equipment) and adapting to providing care from behind a computer.16 Another potential barrier is that the initial setup and equipment for teleoptometry can be expensive, and the cost may vary depending on whether it is integrated into a pre-existing optometry clinic or located elsewhere (e.g., within primary care or a community centre).14 Teleoptometry also requires an onsite optometric assistant to conduct delegated tasks and operate equipment. There is currently no designated professional or specific training associated with the assistant role for teleoptometry in Canada.14 Optometric assistants are trained by their supervising optometrist, and the level of training they receive will influence the quality of the data collected during the exam.14 There is also a concern that the acceptance of teleoptometry may be limited in some First Nations, Métis, and Inuit communities, as remote care may not be perceived as culturally appropriate without corresponding culturally informed in-person care.14 To ensure the provision of culturally appropriate teleoptometry care for First Nations, Métis, and Inuit communities, the delivery of these services should be planned jointly with these communities.14
Why Is It Important to Do This Review?
Routine comprehensive eye exams are important for vision quality and eye health; however, access to an in-person optometrist or ophthalmologist varies across the country. Given the shortage of optometrists in rural and remote areas in Canada,11 teleoptometry has the potential to improve access to comprehensive eye exams and eye disease–specific screening in underserved areas, particularly for those living in rural, remote, Northern and First Nations, Inuit, and Métis communities who may otherwise need to travel long distances to receive eye care.12,16 However, not all aspects of eye care are possible to conduct remotely, and there is a need to evaluate the potential benefits and potential harms of teleoptometry to help ensure that all people living in Canada receive high-quality eye care.
Objectives
To support decision-making about the use of teleoptometry, we prepared this Rapid Review to summarize and critically appraise the available evidence on the clinical effectiveness of teleoptometry compared to an in-person eye exam for people of all ages, as well as the evidence on the clinical utility and diagnostic test accuracy of teleoptometry compared to an in-person eye exam for people at risk of or with suspected or confirmed eye diseases. This review also summarizes the related guideline recommendations available for these populations.
The need for this review was identified by a policy decision-maker, and this review is a response to that request. Given the needs of the customer and the scope of the request, we focused this Rapid Review on the general use of teleoptometry for the provision of vision and eye health services (i.e., using tools that would be available in primary health care facilities or teleoptometry clinics), and we excluded specialized ophthalmic investigations (e.g., optical coherence tomography).
Methods
An information specialist conducted a customized literature search, balancing comprehensiveness with relevancy, of multiple sources and grey literature on August 5, 2025.
Two reviewers screened citations and selected studies based on the inclusion criteria presented in Table 1, and critically appraised the included publications using A MeaSurement Tool to Assess systematic Reviews 2 (AMSTAR 2)18 for systematic reviews (SRs), the Downs and Black checklist19 for randomized and nonrandomized studies, the Quality Assessment of Diagnostic Accuracy Studies 2 (QUADAS-2) checklist20 for diagnostic test accuracy studies, and the Appraisal of Guidelines for Research and Evaluation (AGREE) II instrument21 for guidelines.
Appendix 1 presents a detailed description of the methods and selection criteria for the included studies.
Criteria | Description |
|---|---|
Population | Q1 and Q4: People of all ages requiring eye care Q2: People at risk for eye diseases or conditions or with suspected eye diseases or conditions Q3 and Q5: People at risk for eye diseases or conditions, with suspected eye diseases or conditions, or with confirmed eye diseases or conditions |
Intervention | Q1 and Q4: Teleoptometry administered by a health care provider for a comprehensive eye exam Q2, Q3, and Q5: Teleoptometry administered by a health care provider for eye disease–specific or condition-specific exams |
Comparator | Q1, Q2, and Q3: Standard in-person eye exam provided by an optometrist or ophthalmologist Q4 and Q5: Not applicable |
Outcomes | Q1: Clinical benefits (e.g., correct identification of prescription, visual acuity, and ocular health; time to referral; time to treatment; and patient satisfaction, quality of life, and visual comfort) and harms (e.g., misdiagnosed conditions such as dry eye or blepharitis) Q2: Diagnostic accuracy (e.g., sensitivity, specificity, positive predictive value, negative predictive value) Q3: Clinical utility (e.g., adherence to screening, patient satisfaction and quality of life, time to treatment, disease or condition detection) and harms Q4: Recommendations on best practices for the use of teleoptometry for comprehensive eye exams (e.g., which components of a comprehensive eye exam can or cannot be done with teleoptometry; which specialized tests can or cannot be done with teleoptometry) Q5: Recommendations on best practices for the use of teleoptometry for disease-specific eye exams (e.g., which teleoptometry tests can be used to screen, diagnose, or monitor different eye diseases) |
Study designs | Q1, Q2, and Q3: Health technology assessments, systematic reviews, randomized controlled trials, nonrandomized studies Q4 and Q5: Evidence-based guidelines |
Publication date | 2020 onward |
Summary of Evidence
Quantity of Research Available
This report includes 13 publications that met the inclusion criteria: 1 SR,22 10 cross-sectional studies,23-32 and 2 guidelines.33,34 One cross-sectional study32 addressed research question 1; 9 publications (1 SR22 and 8 cross-sectional studies23-30) addressed research question 2; 1 cross-sectional study31 addressed research question 3; and 2 guidelines33,34 addressed research question 5.
No publications were identified as meeting our inclusion criteria that addressed question 4; therefore, no summary can be provided on the recommendations for teleoptometry for comprehensive eye exams.
One SR by Chou et al.22 had broader inclusion criteria than this report (i.e., any diagnostic tests used to screen glaucoma), and we reported on the characteristics and results from the 2 relevant studies. However, 1 of the cross-sectional studies29 that was captured in the SR by Chou et al.,22 was also identified in our literature search, and the publication reported additional outcomes and clinical indications that were not reported in the SR by Chou et al. Thus, the data from the primary study have been extracted rather than using the information reported in the SR.
Appendix 2 presents the PRISMA35,36 flow chart of the study selection.
Summary of Study Characteristics
Summaries of study characteristics are organized by research question. Appendix 3 provides details of the characteristics of the included publications.
Studies Included for Research Question 1: Clinical Effectiveness of Teleoptometry for Comprehensive Eye Exams
We identified 1 cross-sectional study32 that compared the effectiveness of a teleoptometry exam versus an in-person examination for a comprehensive eye exam (i.e., vision and eye health assessments) (refer to Table 3). This study was conducted in Canada and used a repeated measures cross-sectional design in which all participants had 2 successive comprehensive eye exams — a hybrid teleoptometry exam and an in-person exam — in a random order. Both exams included an assessment of visual acuity, refractive measurements, visual function, and ocular health. Before the first exam, all participants were pretested with automated instruments by an optometric assistant. The hybrid teleoptometry exam was conducted by a remote optometrist (located in a different room at the same clinic) and included an asynchronous component (i.e., review of results for tests delegated to the optometric technician and review and optometrist interpretation of tests conducted and filmed by the optometric technician) and synchronous components (i.e., viewing of tests performed live by the technician and tests performed remotely by the optometrist). The in-person exam was conducted by a different optometrist using the same tests as the teleoptometry exam, with the addition of nondilated fundoscopy for the in-person exam, which can only be performed in person. Neither exam included a dilated fundus examination, which is a recommended element of a comprehensive eye exam in Canada.5
The study included 66 adults who had not previously received eye care (mean age = 29.7 years) and excluded people with acute ocular conditions or visual deficiency. The refractive error, as measured in person, ranged from –8.78 to +2.63 diopters. Aside from mean age, comprehensive participant characteristics, including PROGRESS-Plus37 criteria, were not reported in this study.32 For example, place of residence and gender or sex were not reported.
The relevant clinical outcomes included:
refractive measurements (sphere, cylinder, axis)
best corrected visual acuity
visual comfort with the prescription (i.e., quality of vision, presence of distortion, dizziness when walking, and acceptability of the prescription when worn daily)
visual function and ocular health assessment (i.e., entering distance visual acuity, colour vision, extraocular motility, pupillary reflexes, anterior segment, and posterior segment)
patient satisfaction
optometrist confidence level.
Studies Included for Research Question 2: Diagnostic Test Accuracy of Teleoptometry for Eye Diseases and Conditions
We identified 9 studies, including 1 SR22 (which included 2 relevant studies: 1 pilot study and 1 primary study,29 reported separately; refer to Table 2) and 8 cross-sectional studies23-30 (refer to Table 4).
These studies were conducted in Canada,27 the US,22,24,29 India,23 Israel,26 Hong Kong,25 Iran,28 and Kenya.30
Diagnostic Test Accuracy of Teleoptometry for Eye Diseases and Conditions in Children
Two studies were identified that examined the diagnostic test accuracy of teleoptometry in children. In 1 study,24 the target condition was anterior segment pathologies, and the authors compared synchronous and asynchronous teleoptometry to the reference standard of an anterior segment exam by an ophthalmologist. The anterior segment conditions identified were grouped into the following categories: eyelids or eyelashes (e.g., blepharitis), conjunctiva or sclera (e.g., papillae), cornea (e.g., cornea scar), anterior chamber (e.g., tube shunt), iris (e.g., irregular pupil), and lens (e.g., aphakia). The synchronous teleoptometry exam involved an ophthalmologist viewing the live stream of the in-person exam, with limited communication between the providers. The asynchronous teleoptometry exam involved the same ophthalmologist reviewing recordings of the in-person exam after 3 months. In the other study on children with suspected amblyopia, the target conditions were potentially related ocular features assessed as part of a pediatric eye exam.27 The authors compared an asynchronous teleoptometry exam (i.e., an ophthalmologist reviewed a recording of the in-person exam) to the reference standard of an in-person exam of ocular features by an ophthalmologist. One study reported the median age of its participants as 12 years,24 and the other study reported the mean age of its participants as 4.8 years.27 Both studies reported on the sex of the participants, with 1 study involving 55% male and 45% female participants24 and the other study involving 48% male and 52% female participants.27 No additional PROGRESS-Plus37 criteria were reported in either study. There was also no discussion on gender identities outside of male and female. The diagnostic test accuracy outcomes of interest were sensitivity and specificity in both studies.
Diagnostic Test Accuracy of Teleoptometry for Eye Diseases and Conditions in Adults
The other 7 studies were specific to adults, and examined the diagnostic test accuracy of teleoptometry for:
glaucoma (4 studies):22,23,25,29 of these, 2 studies grouped by glaucoma and glaucoma suspect,25,29 but only 1 reported the proportion of people within each group,25 and 2 studies diagnosed people with glaucoma without grouping by severity22,23
diabetic retinopathy (4 studies):23,28-30 of these, 1 study reported the proportion of people with any diabetic retinopathy and the proportion with diabetic retinopathy requiring referral,28 and 3 studies diagnosed people with any diabetic retinopathy23,29,30
AMD (3 studies):25,29,30 none of the studies diagnosed people with specific stages of AMD
cataracts (3 studies):23,25,29 of these, 2 studies grouped people by grade of cataracts23,25 (early, moderate, or late cataracts;25 immature or mature cataracts23), but only 1 study reported the proportion of people within each group,25 and 1 study diagnosed people with cataracts referred for surgery29
clinically significant macular edema (1 study)28
keratoconus (1 study)26
other eye conditions (1 study).23
The reference standard was a comprehensive in-person eye exam with an ophthalmologist in 5 studies,22,23,25,29,30 an eye exam with a retina specialist in 1 study,28 and an eye exam performed by an optometrist and a cornea surgeon in 1 study.26
In the studies on adults, comprehensive patient characteristics were reported in some of the studies on adults. Mean age was reported in 6 of the 7 studies and ranged from 29 years to 67 years.23,25,26,28-30 Six of these 7 studies reported the sex of the participants.23,25,26,28-30 Three studies reported the percentages of male and female participants, with the range for male participants being 39.4% to 57.6% and the range for female participants being 42.3% to 59.5%.23,25,30 Three studies reported the percentage for only 1 sex:26,28,29 1 reported that 66% of its participants were male;26 1 reported that 67.5% of its participants identified as female;28 and 1 reported that 86.7% of its participants identified as male.29 No studies reported on gender identities aside from male or female. Additional PROGRESS-Plus criteria or potential risk factors and comorbidities were described in 3 studies, which evaluated participants with a variety of eye diseases. One study included the race of the participants, with 0.4% identifying as Asian, 61.3% identifying as Black, and 38.3% identifying as white.29 One study reported diabetes and hypertension percentages, with 13.0% of participants having diabetes and 8.9% of participants having hypertension.23 Another study included the median years since diabetes diagnosis as 5 years.30 Some studies included or excluded participants based on their diabetes status: 1 excluded those who were living with diabetes,25 while 2 other studies only included participants living with diabetes.28,30 No additional PROGRESS-Plus37 criteria, such as education or occupation, were reported in the studies. One study did not report on any participant characteristics.22
For the studies in which glaucoma was a target condition, the index tests included hybrid teleoptometry (i.e., a combination of asynchronous data collection by technician and synchronous consultation with an ophthalmologist);23 asynchronous teleoptometry of clinical data;22 and asynchronous teleoptometry by an ophthalmologist (2 studies), where the clinical data and photos were collected by either an optometrist25 or an optometric assistant.29
For studies in which diabetic retinopathy was a target condition, the index tests included hybrid teleoptometry (i.e., a combination of asynchronous data collection by technician and synchronous consultation with an ophthalmologist);23 asynchronous teleoptometry by an ophthalmologist (2 studies), where the clinical data and photos were collected by either an optometric assistant29 or an ophthalmic assistant;30 and asynchronous teleoptometry by a retina specialist, where the photos were collected by a postgraduate student of medical informatics.28
For studies in which AMD was a target condition, the index tests were all asynchronous teleoptometry by an ophthalmologist, which varied based on whether the clinical data and photos were collected by an optometrist,25 an optometric assistant,29 or an ophthalmic assistant.30
For studies in which cataracts were a target condition, the index tests included hybrid teleoptometry (i.e., a combination of asynchronous data collection by a technician and synchronous consultation with an ophthalmologist)23 and asynchronous teleoptometry by an ophthalmologist (2 studies), where the clinical data and photos were collected by either an optometric assistant29 or an optometrist.25
In the study in which macular edema was a target condition, the index test was asynchronous teleoptometry by a retina specialist who reviewed a single digital image (dilated pupils, centred on the macula and showing the optic nerve and superior and inferior vascular arcades); the photos were collected by a postgraduate student of medical informatics.28
In the study in which keratoconus was the target condition, the index test was asynchronous teleoptometry in which an ophthalmologist reviewed the data obtained from the in-person exam (which was conducted by an optometrist and a cornea surgeon).26
For the study in which other eye conditions were a target condition, the index test was hybrid teleoptometry (i.e., a combination of asynchronous data collection by technician and synchronous consultation with an ophthalmologist)23 or asynchronous teleoptometry by an ophthalmologist, where the clinical data and photos were collected by an optometric assistant.29
There was considerable variation across the diagnostic tests performed in these studies, even among studies of the same target condition (refer to Table 4 in Appendix 3 for complete details).
The diagnostic test accuracy outcomes of interest included sensitivity and specificity in all 7 studies22,23,25,26,28-30 and positive predictive value and negative predictive value in 4 studies.23,25,26,30
Studies Included for Research Question 3: Clinical Utility of Teleoptometry for Eye Diseases and Conditions
CDA-AMC identified 1 cross-sectional study31 that met the inclusion criteria for addressing research question 3 (refer to Table 3). However, some of the outcomes were narrow in scope (e.g., focused only on participants with strabismus), rather than focusing on a broad range of ocular diseases or conditions. This study was conducted in the US and used a cross-sectional noninferiority study design. All participants underwent a synchronous teleoptometry exam, in which the eye exam was conducted by an in-person pediatric optometrist and live streamed by a pediatric ophthalmologist who interpreted the exam results. Later the same day, the same pediatric ophthalmologist conducted an in-person exam.
The study included 210 children (median age = 6 years) recruited from a vision centre, where they had been referred for further assessment or surgical consultation. There was some inclusion of participant characteristics, including PROGRESS-Plus37 criteria, in this study.31 The study consisted of 44% male participants and 56% female participants, but there was no discussion on gender, how gender or sex were defined, or gender identities outside of male and female. The race of participants was also determined, with 2% of participants (using the wording of the source study in quotations) identifying as “American Indian or Alaska Native,” 6% identifying as Asian, 10% identifying as Black or “African American,” 79% identifying as white, 3% identifying as “mixed or other,” and none identifying as “Native Hawaiian or other Pacific Islanders” [racial categories per original source.] The study also captured the ethnicity of participants but limited the outcomes to either Hispanic or Latino (78%) or not Hispanic or Latino (22%). The primary language of 45% of the participants was English; Spanish was the primary language of 50%, and 3% had another primary language. Further PROGRESS-Plus37 criteria, such as disability status, occupation, or education, were not discussed.
The relevant outcomes included agreement between the teleoptometry and in-person exams in diagnosis and management plans, as well as agreement in angle measurement and disease category for participants with strabismus (i.e., eye misalignment).
Studies Included for Research Question 5: Guidelines for Teleoptometry for Glaucoma and Diabetic Retinopathy
CDA-AMC identified 2 guidelines on the use of teleoptometry for screening, diagnosing, and monitoring eye diseases and conditions. Table 5 provides a detailed summary of the characteristics of the guidelines included for research question 5.
Two evidence-based guidelines, developed in the US and published in 202434 and 2020,33 are included in this review. One guideline, by the American Optometric Association (AOA), specifically focuses on people with primary open-angle glaucoma;34 the other guideline, developed by the American Telemedicine Association (ATA), focuses on people with diabetic retinopathy.33 The AOA guideline was developed for optometrists,34 and the ATA guideline was developed for practitioners, group and specialty practices, hospitals and health care systems, and other providers of health-related services for which telehealth interactions take place.33 The general outcomes of interest for the AOA guideline were the potential benefits and harms of interventions, such as the number of monitoring visits needed, side effects, reduced disease or delay in the onset of disease, and access to care.34 The general outcomes of interest for the ATA guideline were clinical, technical, and administrative issues.33
The ATA guideline reported that recommendations were informed by “evidence, professional consensus, and a rigorous review, including open public commentary period” but lacked a description of the assessment of the quality of individual studies and the quality of the body of evidence.33 The authors of this guideline provided a level of adherence for each recommendation “based on the quantity and quality of peer-reviewed evidence,” including “shall,” “shall not,” “should,” and “may.”33
The AOA guideline recommendations were based on evidence from an SR, a consensus process, and a public commentary period. The authors used predetermined grading criteria to assess the quality of the evidence and the strength of the recommendations.34 The quality of the evidence was graded as A, B, C, or D, and the grade was chosen based on the type of study design supporting the recommendation.34 The strength of the recommendation was classified as a strong recommendation, a recommendation, or discretional, depending on the type of study design of the supporting evidence.34
Summary of Critical Appraisal
Appendix 4 provides additional details about the strengths and limitations of the included publications.
Studies Included for Research Question 1: Clinical Effectiveness of Teleoptometry for Comprehensive Eye Exams
One repeated measures cross-sectional study32 that compared the clinical effectiveness of teleoptometry to in-person comprehensive eye exams for vision and eye health was included in this review (refer to Table 6 for study strengths and limitations). The aim of the study and the interventions were well described, and estimates of random variability were reported for most outcomes (i.e., refractive error, visual comfort, and patient and provider outcomes). For the comparative outcomes that reported P values (i.e., visual comfort with prescription, patient satisfaction, and optometrist confidence level), the actual P values were reported. However, for the ocular health outcomes, confidence intervals (CIs) were not reported alongside the level of agreement, which reduces confidence in these outcomes because the level of variability around the estimate is not known. All participants received both exams on the same day; thus, it is unlikely that the participants’ conditions changed between tests. The teleoptometry and in-person exams were conducted by different optometrists, reducing the chance that the results of either test were influenced by the results of the other test, although this was not explicitly reported. The study was conducted in Canada, and most of the tests and equipment were representative of those used in practice in Canada. However, the ocular health exam was limited because neither exam included a dilated fundus exam, which is not possible to perform remotely, though it is considered best practice in Canada for a comprehensive eye exam.5 The participants were recruited through social media and described with limited detail (i.e., only age was reported); thus, it is unclear whether the study population is representative of the population that is likely to need or to use teleoptometry in practice. The results of the study may also have been limited by the sample size (i.e., 66 participants) and by the exclusion of people with low vision (in whom it may be more difficult to assess refractive error and visual acuity). It is unclear whether these limitations could have biased the results in favour of improved results for teleoptometry. Both eye exams took place at the School of Optometry in Montreal, which is not representative of the setting of a teleoptometry exam in practice (e.g., in a rural setting with the optometrist in a different location) and would not have been subject to the same potential issues, such as unreliable internet connection or insufficient bandwidth. For the teleoptometry exam, the tests that would normally be delegated to or assisted by an optometric assistant were conducted by a third-year optometry student, and this may not be representative of teleoptometry in practice because optometry students may be more qualified than most optometric assistants in Canada; this may have biased the findings in favour of improved results for teleoptometry. Steps to ensure patient privacy and data security for the teleoptometry exam were not reported.
Studies Included for Research Question 2: Diagnostic Test Accuracy of Teleoptometry for Eye Diseases and Conditions
Systematic Reviews
The SR on glaucoma screening22 clearly stated the population, intervention, comparators, and outcomes of interest; however, it is unclear whether the methods were established before the conduct of the review, which increases the risk of reporting bias (refer to Table 7). The authors used a comprehensive search strategy, performed study selection and data extraction in duplicate, and provided a list of excluded studies (with the reasons for exclusion), reducing the likelihood that relevant studies were missed. The critical appraisal was conducted in duplicate, and the authors used predefined quality assessment criteria that addressed all the key critical appraisal domains for diagnostic accuracy studies. One limitation was that the studies were described with limited detail (e.g., missing some information on study design, interventions, population, or source of funding), which limits our understanding of the findings and our ability to assess whether the included studies are relevant to the current review. Steps to ensure patient privacy and data security for the teleoptometry exam were not reported.
Cross-Sectional Studies
Four studies recruited participants using a consecutive sample, and there is a low risk that the selection of participants would have introduced bias (refer to Table 8).23,25,26,30 However, in 3 studies the participant recruitment methods were unclear,24,27,28 and in 1 study29 participants self-volunteered to participate. It is unknown whether the methods in these studies could have introduced selection bias to the results. The participants matched the population of interest to this report in 7 studies (i.e., people at risk for or with suspected eye disease);23,25-30 however, in the other study,24 all the participants had previously been diagnosed with a type of anterior segment disease, which may have biased the results toward improved performance of the teleoptometry exam. In general, the studies reported limited information about the participants (i.e., most reported age and sex, but little to no other information, including PROGRESS-plus37 criteria, were reported), which limits our understanding about the generalizability of the findings to optometric practice in Canada.23-30 In some studies, there was a low prevalence of 1 or more of the target conditions in the study population,23,27,29,30 and in 1 study there was a higher than expected prevalence of target conditions in the study population,25 which may have contributed to imprecision in estimates of sensitivity or specificity (e.g., wide CIs around the estimates).
The choice of the index test directly matched the intervention of interest to this report (i.e., teleoptometry administered by a health care provider using approved equipment and delivered or reviewed remotely by an optometrist or ophthalmologist) in 4 studies.23,25,29,30 In the other 4 studies,24,26-28 the index test differed slightly from the intervention of interest to this report and may not reflect how teleoptometry is used in practice in Canada. In 3 studies, the teleoptometry exam only involved the synchronous or asynchronous review of a video of the in-person exam (which was conducted by an ophthalmologist)24,27 or the asynchronous review of the clinical data obtained from the in-person exam,26 rather than a separate teleoptometry exam conducted by a remote optometrist or ophthalmologist with support from an in-person optometric assistant. In practice, the in-person components of a teleoptometry exam would be conducted by or with assistance from an optometric assistant (rather than by an optometrist or ophthalmologist). Thus, using information obtained from the in-person exam may bias the study toward improved findings for the teleoptometry exam. In the fourth study, the teleoptometry exam only involved the asynchronous review of digital images taken by a postgraduate student of medical informatics, with no additional clinical data provided.28
The teleoptometry exams were interpreted without knowledge of the results of the in-person exam in 5 studies,23-25,29,30 which reduced the potential for bias due to prior knowledge when interpreting the exam results. In 1 of the other studies,27 it was unclear if the teleoptometry exam was interpreted without knowledge of the results of the in-person exam; in the other 2 studies,26,28 the same person who conducted the in-person exam also conducted some of the teleoptometry exams (after at least 4 weeks26 or 2 months28). It is unknown whether they would have remembered the results of the previous test, which may have biased the results toward improved findings for the teleoptometry exam.
In all 8 studies,23-30 the choice of the reference standard matched the reference standard targeted by this report (i.e., a standard in-person eye exam provided by an optometrist or ophthalmologist), all participants received the same reference standard, and the reference standard was interpreted without knowledge of the index test results. However, there was considerable variation in the diagnostic tests performed in these studies for both the index test and the reference standard, even across studies with the same target condition. This variation should be considered when reviewing the results from these studies as certain diseases require multiple tests to accurately diagnose and it is possible that a comprehensive evaluation for each disease was not always performed (i.e., the reference standard may not have reflected current diagnostic standards in Canada). For instance, in all 4 studies in which glaucoma was the target condition, intraocular pressure was assessed as part of the teleoptometry exam, and only some studies included additional disease-specific tests such as central corneal thickness22,29 or fundus photos.25,29 This distinction is important as the current standard of practice for a comprehensive glaucoma evaluation involves numerous diagnostic tests to ensure accurate diagnosis (e.g., patient history, slit lamp exam, intraocular pressure, blood pressure, pachymetry, gonioscopy, dilated exam, perimetry, ancillary objective imaging).38
In each study, the teleoptometry exam and the in-person exam were conducted on the same day (or using clinical information collected on the same day), which reduced the likelihood that misclassification might occur due to the timing of the tests.23-30 All participants were included in the analysis in 5 studies;23,24,26,27,29 however, in the other 3 studies,25,28,30 between 8 and 15 people (between 2% and 6% of the study samples) were excluded from the analysis due to poor-quality images from the teleoptometry exam, which may bias the results of the study toward improved findings for the teleoptometry exam.
The authors reported on the source of funding in all the studies, and no potential conflicts were identified.23-30
Of the 8 studies, 4 provided details about their efforts to maintain patient privacy and data security for the teleoptometry exam (e.g., video encryption, secure research databases, de-identification of participant photographs).24,27,29,30 In the other studies, efforts to ensure patient privacy and data security for the teleoptometry exam were not reported.
Studies Included for Research Question 3: Clinical Utility of Teleoptometry for Eye Diseases and Conditions
One cross-sectional study31 that compared the clinical utility of teleoptometry to that of an in-person eye exam for eye diseases and conditions was included in this review (refer to Table 9 for detailed study strengths and limitations). The aim of the study, the interventions, and the participants (including details on age, sex, race, ethnicity, and primary language) were well described. The teleoptometry exam and the in-person exam were both conducted on the same day; thus, it is unlikely that the condition of the eyes changed between tests. The teleoptometry exam was conducted before the in-person exam, and the results were interpreted without any knowledge of the results of the in-person exam. However, the same ophthalmologist conducted the teleoptometry and the in-person exam on the same day, which may have biased the results of the in-person exam because the ophthalmologist would have previous knowledge of the results of the teleoptometry exam.
The authors described this study in the methods as a noninferiority trial, and they set 2 margins for noninferiority (1 for each primary outcome); however, these margins were based on the feasibility of recruiting the necessary sample size, and it was unclear whether these margins were informed by other information (e.g., power calculation, findings from previous studies, clinical judgment). These margins for noninferiority were described in the methods and the discussion but were not included as part of the results of the study, limiting the interpretation of the findings. In general, the reporting of the results was unclear, with uncertainty regarding whether all participants had both exams, and the authors did not report simple outcome data for the main findings, nor did they provide estimates of random variability, limiting the interpretation of and reducing our confidence in the findings. The teleoptometry exam may not be representative of the setting or conditions in which teleoptometry would occur in practice. The teleoptometry exam took place at an urban vision centre rather than a rural or remote location; thus, it was not subject to the potential concerns that could exist in practice (e.g., unreliable internet connection or insufficient bandwidth). The in-person components of the teleoptometry exam were also conducted by an optometrist, rather than an optometric assistant, which is not representative of how teleoptometry is implemented in practice. The more skilled optometrist may have biased the results in favour of teleoptometry. Steps to ensure patient privacy and data security for the teleoptometry exam were not reported.
Studies Included for Research Question 5: Guidelines for Teleoptometry for Glaucoma and Diabetic Retinopathy
Both guidelines had clear objectives, described the population and target users of the guidelines, and included individuals from relevant professional groups (refer to Table 10). Neither guideline specifically described the health questions addressed in the guideline.
The AOA guideline development group34 sought the views and preferences of the target population to develop its guideline by including patient and public representatives in the guideline development group, but the guideline does not specify how the information from these representatives was used. The views and preferences of the target population were not included in the guideline by the ATA.33
The AOA guideline34 used systematic methods to search the literature for evidence to inform the recommendations and provided detailed inclusion and exclusion criteria for the selection of the evidence. The ATA guideline33 specified that it conducted a “rigorous review,” with no description of whether this review was systematic or of the criteria used to select the evidence. This increases the likelihood that relevant literature was missing. The methods used to formulate the recommendations were clearly described in the AOA guideline, and relevant supporting evidence and the benefits and risks associated with the recommendations were included. Furthermore, the recommendations in the AOA guideline were reviewed by experts before publication. The AOA guideline did not describe the risk of bias in individual studies, but the quality of the overall body of evidence was graded. While the ATA guideline includes a description stating that its recommendations were based on “evidence, professional consensus, and a rigorous review, including open public commentary period,” it lacks detail in describing each of these processes. Furthermore, the ATA guideline does not discuss the health benefits and risks associated with the recommendations, was not reviewed by experts before publication, and did not clearly provide supporting evidence for the recommendations or an assessment of evidence quality, and recommendations were sometimes vague. Therefore, our confidence in the ATA guideline is somewhat limited.
While both guidelines stated their funding source, there were no explicit statements that the funding bodies did not influence the content of the guidelines, making it unclear whether editorial independence was maintained between the guideline development groups and the funding organizations. Competing interests of the guideline development group members were recorded and addressed in the ATA guideline, but not in the AOA guideline. All participants provided full written disclosure of conflicts before their involvement with the AOA guideline development group, but the statements were not published alongside the guidelines.
Summary of Findings
Appendix 5 presents additional details on the main study findings.
Research Question 1: Clinical Effectiveness of Teleoptometry for Comprehensive Eye Exams
One cross-sectional study32 provided information on the clinical effectiveness of teleoptometry versus in-person comprehensive eye exams for assessing vision quality and ocular health. In general, there was good to excellent agreement or little to no difference between exam modalities regarding measures of refractive error and ocular health, although some participants and providers may prefer in-person care to teleoptometry.
Refractive Error
The teleoptometry exam had an excellent level of agreement with the in-person exam (interclass correlation coefficient > 0.90) for spherical and cylindrical refraction measurements and for best corrected visual acuity and a good level of agreement with the in-person exam (interclass correlation coefficient between 0.75 and 0.90) for axis refraction measurements (refer to Table 11).32 While teleoptometry resulted in a median hyperopic overcorrection of +0.07 diopters for spherical refraction measurements compared to the in-person exam, the authors reported that 98.49% of all spherical equivalent differences were within the clinical tolerance level of ±0.50 diopters.32
Visual Comfort With Prescription
When trial glasses were prepared and compared using the prescriptions obtained from the teleoptometry exam and from the in-person exam, the participants reported no statistically significant differences between the 2 modalities in terms of the quality of their vision, the presence of distortion, dizziness when walking, or the acceptability of wearing the new prescription daily (refer to Table 12).32
Visual Function and Ocular Health Assessment
For the visual function and ocular health assessments, the agreement for results that were “within normal limits” and “outside normal limits” was measured with the Krippendorf alpha coefficient (KAC).
The level of agreement between the teleoptometry exam and the in-person exam was:
“almost perfect” (i.e., KAC > 0.80) for entering distance visual acuity and colour vision
“substantial” (i.e., KAC, 0.60 to ≤ 0.80) for anterior and posterior segments
“fair” (i.e., KAC, 0.2 to ≤ 0.4) for extraocular motility.
No level of agreement was calculated for pupillary reflexes as there were no results “outside normal limits” for this test.
When participants were grouped based on their index of morbidity (i.e., severity of ocular health diagnoses), the level of agreement between the teleoptometry exam and the in-person exam was 86.4% for ocular conditions with little risk of harm, with 3 conditions not diagnosed in the teleoptometry exam (reported to be “mostly dry eye disease”) (refer to Table 13). The level of agreement between the teleoptometry exam and the in-person exam was 87.5% for conditions with higher morbidity, with 1 case of inactive corneal pannus not diagnosed in the teleoptometry exam and 1 case of suspected papilledema that could not be ruled out in the teleoptometry exam due to the quality of the fundus photo. However, neither exam included a dilated fundus exam, which is an important component of a comprehensive eye exam5 to ensure a thorough ocular health assessment.
Patient Satisfaction and Provider Confidence
The mean patient satisfaction level and the level of satisfaction for the 4 items on the scale (i.e., trust in the accuracy of the exam results, ease of communication, ease of establishing a relationship of trust with the optometrist, and general satisfaction) was statistically significantly higher for the in-person exam than for the teleoptometry exam (refer to Table 14).32 It was not reported whether this was a validated tool for assessing patient satisfaction with teleoptometry, limiting our interpretation of these findings.
The mean confidence level of the eye care providers and the level of confidence for each eye test was statistically significantly higher for the in-person exam than for the teleoptometry exam;32 however, the tool used to measure provider confidence level was not described, limiting our interpretation of these findings.
Research Question 2: Diagnostic Test Accuracy of Teleoptometry for Eye Diseases and Conditions
One SR (with 1 primary study)22 and 8 cross-sectional studies23-30 provided information on the diagnostic test accuracy of teleoptometry versus an in-person exam for eye diseases and conditions (i.e., diabetic retinopathy, cataracts, glaucoma, AMD, keratoconus progression, macular edema, and other conditions). Detailed study findings, including the severity of disease among study participants, when reported, are presented in Appendix 5 (Tables 15 to 21).
For Diabetic Retinopathy
A hybrid teleoptometry exam (i.e., a combination of asynchronous data collection by a technician and synchronous consultation with an ophthalmologist), when compared to an in-person exam (1 study),23 had:
very low sensitivity to detect any diabetic retinopathy (57.1%; 95% CI, 18.4% to 90.1%)
high specificity to detect participants who do not have diabetic retinopathy (98.2%; 95% CI, 96.9% to 99.1%)
very low positive predictive value (25.0%; 95% CI, 7.3% to 52.4%; prevalence of diabetic retinopathy = 1.0%)
high negative predictive value (99.5%; 95% CI, 98.7% to 99.9%; prevalence of diabetic retinopathy = 1.0%).
An asynchronous teleoptometry exam (which varied in terms of exam components and the health care providers involved across the 3 included studies), when compared to an in-person exam,28-30 had:
low to high sensitivity to detect any diabetic retinopathy (63% [95% CI, 25% to 92%] to 92% [95% CI not reported]; 3 studies)
high specificity to detect participants who do not have diabetic retinopathy (96% [95% CI not reported] to 99% [95% CI, 97% to 100%]; 3 studies)
moderate positive predictive value (75.0%; 95% CI, 61.2% to 85.1%; 1 study; prevalence of diabetic retinopathy = 15%)30
high negative predictive value (97.2%; 95% CI, 95.0% to 98.4%; 1 study; prevalence of diabetic retinopathy = 15%).30
Overall Accuracy Results for Diabetic Retinopathy Detection
Overall, teleoptometry had variable (very low to high) sensitivity to detect any diabetic retinopathy.23,28-30 This means that out of every 100 people with diabetic retinopathy, a teleoptometry exam could:
correctly detect between 57 and 92 people with diabetic retinopathy
miss between 8 and 43 people with diabetic retinopathy (i.e., false-negatives).
The 95% CIs for these studies23,28-30 suggest that the ability of teleoptometry to detect diabetic retinopathy could be as low as detecting 18 out of every 100 people with diabetic retinopathy (i.e., 82 false-negatives) and could be as high as detecting 92 out of every 100 people with diabetic retinopathy (i.e., 8 false-negatives).
Teleoptometry had high specificity to detect those who do not have diabetic retinopathy. This means that out of every 100 individuals who do not have diabetic retinopathy:
between 96 and 99 people could correctly test negative
around 4 people could be wrongly diagnosed as having diabetic retinopathy (i.e., false-positives).
The predictive value of a test depends on the prevalence of the disease in a population. In people with a negative test result by teleoptometry, the proportion who do not have diabetic retinopathy (i.e., true negatives) was high across both low-prevalence (1.0%)23 and high-prevalence (15%)30 study populations. However, the positive predictive value of teleoptometry varied depending on the prevalence in the study population; therefore, of those who test positive for diabetic retinopathy, the proportion that have diabetic retinopathy (i.e., true positives) could be very low to moderate.
Refer to Table 15 for more details on the diagnostic accuracy of teleoptometry for people living with diabetic retinopathy.
For Cataracts
A hybrid teleoptometry exam (i.e., a combination of asynchronous data collection by a technician and synchronous consultation with an ophthalmologist), when compared to an in-person exam (1 study, which grouped immature and mature cataracts),23 had:
high sensitivity to detect cataracts (91.7%; 95% CI, 80% to 97.7%)
high specificity to detect people who do not have cataracts (95.9%; 95% CI, 94.0% to 97.3%)
low positive predictive value (62.9%; 95% CI, 50.5% to 74.1%; prevalence of cataracts = 7.1%)
high negative predictive value (99.3%; 95% CI, 98.3% to 99.8%; prevalence of cataracts = 7.1%).
An asynchronous teleoptometry exam (which varied in terms of exam components and the health care providers involved), when compared to an in-person exam (1 study that grouped early, moderate, and late cataracts25 and 1 study that reported on cataracts referred for surgery29), had:
good sensitivity to detect cataracts (87.8% [95% CI not reported] for any cataract to 100% [95% CI, 69% to 100%] for cataracts referred for surgery; 2 studies)
high specificity to detect people who do not have cataracts (98% [95% CI, 95% to 99%] to 99.4% [95% CI not reported]; 2 studies)
high positive predictive value for cataracts referred for surgery (97.6%; 1 study; prevalence of cataracts = 75.3%)
high negative predictive value for cataracts referred for surgery (96.7%; 1 study; prevalence of cataracts = 75.3%).
Overall Accuracy Results for Cataracts Detection
Overall, based on the conditions in these studies, teleoptometry had variable (good to high) sensitivity to detect cataracts.23,25,29 This means that out of every 100 people with cataracts, a teleoptometry exam could:
correctly detect between 88 and 100 people with cataracts
miss around 12 people with cataracts (i.e., false-negatives).
The 95% CIs for these studies23,25,29 suggest that the ability of teleoptometry to detect cataracts could be as low as detecting 56 out of every 100 people with cataracts (i.e., 44 false-negatives) and could be as high as detecting 100 out of every 100 people with cataracts.
Teleoptometry had high specificity in these studies to detect those who do not have cataracts. This means that out of every 100 individuals who do not have cataracts:
between 95 and 99 people could correctly test negative
around 5 people could be wrongly diagnosed as having cataracts (i.e., false-positives).
The predictive value of a test depends on the prevalence of the disease in a population. In people with a negative test result by teleoptometry, the proportion of people who do not have cataracts (i.e., true negatives) was high across both low-prevalence (7.0%)23 and high-prevalence (75.3%)25 study populations. However, the positive predictive value of teleoptometry varied depending on the prevalence in the study population, which means that of those who test positive for cataracts, the proportion that have cataracts (i.e., true positives) could be low to high.
Refer to Table 16 for more details on the diagnostic accuracy of teleoptometry for people living with cataracts.
For Glaucoma
A hybrid teleoptometry exam (i.e., a combination of asynchronous data collection by a technician and synchronous consultation with an ophthalmologist), when compared to an in-person exam (1 study),23 had:
very low sensitivity to detect glaucoma (12.5%; 95% CI, 0.3% to 52.7%)
high specificity to detect people who do not have glaucoma (99.6%; 95% CI, 98.7% to 99.9%)
very low positive predictive value (25.0%; 95% CI, 1.0% to 80.6%; prevalence of glaucoma = 1.2%)
high negative predictive value (99.0%; 95% CI, 97.9% to 99.6%; prevalence of glaucoma = 1.2%).
An asynchronous teleoptometry exam (which varied in terms of exam components and the health care providers involved), when compared to an in-person exam (3 studies,22,25,29 of which 2 studies25,29 grouped glaucoma and glaucoma suspect), had:
very low to high sensitivity to detect glaucoma or glaucoma suspect (47% [95% CI, 35% to 60%] to 98.7% [95% CI not reported]; 3 studies)
moderate to high specificity to detect people who do not have glaucoma or glaucoma suspect (76.5% [95% CI not reported] to 97% [95% CI, 94% to 99%]; 3 studies)
high positive predictive value (90.5%; 1 study; prevalence of glaucoma or glaucoma suspect = 31.6%)
high positive predictive value (96.3%; 1 study; prevalence of glaucoma or glaucoma suspect = 31.6%).
Overall Accuracy Results for Glaucoma Detection
Overall, based on the conditions in these studies, teleoptometry had variable (very low to high) sensitivity to detect glaucoma or glaucoma suspect.22,23,25,29 This means that out of every 100 people with glaucoma or glaucoma suspect, a teleoptometry exam may:
correctly detect between 12 and 99 people with glaucoma or glaucoma suspect
miss between 1 and 88 people with glaucoma or glaucoma suspect (i.e., false-negatives).
The 95% CIs for these studies22,23,25,29 suggest that the ability of teleoptometry to detect glaucoma or glaucoma suspect could be as low as detecting 0 out of every 100 people with glaucoma or glaucoma suspect (i.e., 100 false-negatives) and could be as high as detecting 99 out of every 100 people with glaucoma or glaucoma suspect.
Teleoptometry had moderate to high specificity in these studies to detect those who do not have glaucoma or glaucoma suspect. This means that out of every 100 individuals who do not have glaucoma or glaucoma suspect:
between 76 and 99 people could correctly test negative
between 1 and 24 people could be wrongly diagnosed as having glaucoma or glaucoma suspect (i.e., false-positives).
The predictive value of a test depends on the prevalence of the disease in a population. In people with a negative test result by teleoptometry, the proportion who do not have glaucoma or glaucoma suspect (i.e., true negatives) was high across both low-prevalence (1.2%)23 and high-prevalence (31.6%)25 study populations. However, the positive predictive value of teleoptometry varied depending on the prevalence in the study population; therefore, of those who test positive for glaucoma or glaucoma suspect, the proportion that have glaucoma or glaucoma suspect (i.e., true positives) could be very low to high.
Refer to Table 17 for more details on the diagnostic accuracy of teleoptometry for people living with glaucoma or glaucoma suspect.
For AMD
Asynchronous teleoptometry (which varied in terms of exam components and the health care providers involved), when compared to an in-person exam (3 studies),25,29,30 had:
very low to high sensitivity to detect AMD (23.1% [95% CI, 5.0% to 53.8%] to 99.7% [95% CI not reported]; 3 studies)
high specificity to detect people who do not have AMD (95% [95% CI, 92% to 98%] to 99.5% [95% CI not reported]; 3 studies)
very low to high positive predictive value (27.3% [95% CI, 10.1% to 55.6%] to 99.3% [95% CI not reported]; 2 studies; prevalence of AMD = 2%29 or 12.4%24)
high negative predictive value (98.1% [95% CI, 97.5% to 98.6%] to 98.1% [95% CI not reported]; 2 studies; prevalence of AMD = 2%29 or 12.4%24).
Overall Accuracy Results for AMD Detection
Overall, based on the conditions in these studies, teleoptometry had variable (very low to high) sensitivity to detect AMD.25,29,30 This means that out of every 100 people with AMD, a teleoptometry exam could:
correctly detect between 23 and 99 people with AMD
miss between 1 and 77 people with AMD (i.e., false-negatives).
The 95% CIs for these studies25,29,30 suggest that the ability of teleoptometry to detect AMD could be as low as detecting 5 out of every 100 people with AMD (i.e., 95 false-negatives) and could be as high as detecting 99 out of every 100 people with AMD.
Teleoptometry had high specificity in these studies to detect those who do not have AMD. This means that out of every 100 individuals who do not have AMD:
between 95 and 99 people could correctly test negative
between 1 and 5 people could be wrongly diagnosed as having AMD (i.e., false-positives).
The predictive value of a test depends on the prevalence of the disease in a population. In people with a negative test result by teleoptometry, the proportion who do not have AMD (i.e., true negatives) was high across both low-prevalence (2%)30 and high- prevalence (12.4%)25 study populations. However, the positive predictive value of teleoptometry varied depending on the prevalence in the study population; therefore, of those who test positive for AMD, the proportion that have AMD (i.e., true positives) could be very low to high.
While AMD can be categorized into 4 stages based on disease severity,39 none of the included studies addressed this in their diagnostic test outcomes. Refer to Table 18 for more details on the diagnostic accuracy of teleoptometry for people living with AMD.
For Keratoconus Progression
An asynchronous teleoptometry exam (in which an ophthalmologist reviewed the data obtained from the in-person exam), when compared to an in-person exam (1 study),26 had:
low sensitivity to detect keratoconus progression (69.2%; 95% CI, 38.57% to 90.91%)
high specificity to detect people who do not have keratoconus progression (95.8%; 95% CI, 91.9% to 98.2%)
very low positive predictive value (52.9%; 95% CI, 34.3% to 70.8%; prevalence of keratoconus progression = 6%)
high negative predictive value (97.9%; 95% CI, 95.3% to 99%; prevalence of keratoconus progression = 6%).
Low sensitivity to detect keratoconus means that out of every 100 people with keratoconus progression, a teleoptometry exam could:
correctly detect around 69 people with keratoconus progression
miss around 31 people with keratoconus progression (i.e., false-negatives).
The 95% CI for this study26 suggests that the ability of teleoptometry to detect keratoconus progression could be as low as detecting 39 out of every 100 people with keratoconus progression (i.e., 61 false-negatives) and could be as high as detecting 91 out of every 100 people with keratoconus progression.
High specificity to detect those who do not have keratoconus progression means that out of every 100 individuals who do not have keratoconus progression:
around 95 people could correctly test negative
up to 5 people could be wrongly diagnosed as having keratoconus progression (i.e., false-positives).
In terms of the predictive value of teleoptometry in a population with 6% prevalence of keratoconus progression, the proportion of people who do not have keratoconus progression among those who received a negative test result by teleoptometry (i.e., true negatives) was high. However, the positive predictive value of teleoptometry in this same population was very low; therefore, of those who test positive for keratoconus progression, the proportion that have keratoconus progression (i.e., true positives) could be very low.
Refer to Table 19 for more details on the diagnostic accuracy of teleoptometry for people living with keratoconus.
For Macular Edema
An asynchronous teleoptometry exam (in which a retina specialist reviewed a single digital image taken by a postgraduate student of medical informatics),28 when compared to an in-person exam, had:
high sensitivity to detect clinically significant macular edema (93%; 95% CI not reported)
high specificity to detect people who do not have clinically significant macular edema (100%; 95% CI not reported).
Based on the conditions in this study, the findings mean that out of every 100 people with clinically significant macular edema, a teleoptometry exam could detect around 93 people with macular edema and miss around 7 people (i.e., false-negatives) and that out of every 100 individuals who do not have macular edema, up to 100 people could test negative.
Refer to Table 19 for more details on the diagnostic accuracy of teleoptometry for people living with clinically significant macular edema.
For Other Conditions in Adults
One study23 that compared a hybrid teleoptometry exam (i.e., a combination of asynchronous data collection by a technician and synchronous consultation with an ophthalmologist) to an in-person eye exam reported the diagnostic test accuracy for multiple eye conditions and found the following:
For nonserious eye injury:
Hybrid teleoptometry had very low sensitivity to detect nonserious eye injury (41.7%; 95% CI, 15.2% to 72.3%), meaning that out of every 100 people with a nonserious eye injury, a teleoptometry exam could detect around 42 people with a nonserious eye injury and miss around 58 people (i.e., false-negatives).
Hybrid teleoptometry had high specificity to detect people who do not have nonserious eye injury (99.8%; 95% CI, 99.2% to 100%), meaning that out of every 100 individuals who do not have a nonserious eye injury, around 99 people could correctly test negative.
Hybrid teleoptometry had good positive predictive value (83.3%; 95% CI, 35.9% to 99.6%; prevalence of nonserious eye injury = 1.8%), meaning that there is a good likelihood that those who test positive for nonserious eye injury in a population with 1.8% prevalence actually have a nonserious eye injury (i.e., true positives).
Hybrid teleoptometry had high negative predictive value (99.0%; 95% CI, 97.9% to 99.6%; prevalence of nonserious eye injury = 1.8%), meaning that there is a high likelihood that those who test negative for nonserious eye injury in a population with 1.8% prevalence do not have a nonserious eye injury.
For allergic conjunctivitis:
Hybrid teleoptometry had very low sensitivity to detect allergic conjunctivitis (43.0%; 95% CI, 32.4% to 54.2%), meaning that out of every 100 people with allergic conjunctivitis, a teleoptometry exam could detect around 43 people with allergic conjunctivitis and miss around 57 people (i.e., false-negatives).
Hybrid teleoptometry had high specificity to detect individuals who do not have allergic conjunctivitis (98.3%; 95% CI, 96.9% to 99.2%), meaning that out of every 100 people who do not have allergic conjunctivitis, around 98 people will correctly test negative.
Hybrid teleoptometry had moderate positive predictive value (78.7%; 95% CI, 64.3% to 89.3%; prevalence of allergic conjunctivitis = 12.7%), meaning that there is a moderate likelihood that those who test positive for allergic conjunctivitis in a population with 12.7% prevalence actually have allergic conjunctivitis (i.e., true positives).
Hybrid teleoptometry had high negative predictive value (92.2%; 95% CI, 89.9% to 94.2%; prevalence of allergic conjunctivitis = 12.7%), meaning that there is a high likelihood that those who test negative for allergic conjunctivitis in a population with 12.7% prevalence do not have allergic conjunctivitis.
For infective conjunctivitis:
Hybrid teleoptometry had moderate sensitivity to detect infective conjunctivitis (72.2%; 95% CI, 46.5% to 90.3%), meaning that out of every 100 people with infective conjunctivitis, a teleoptometry exam could detect around 72 people with infective conjunctivitis and miss around 28 people (i.e., false-negatives).
Hybrid teleoptometry had high specificity to detect people who do not have infective conjunctivitis (98.3%; 95% CI, 97.0% to 99.2%), meaning that out of every 100 people who do not have infective conjunctivitis, around 98 people will correctly test negative.
Hybrid teleoptometry had very low positive predictive value (54.2%; 95% CI, 32.8% to 74.4%; prevalence of infective conjunctivitis = 2.6%), meaning that there is a very low likelihood that those who test positive for infective conjunctivitis in a population with a 2.6% prevalence actually have infective conjunctivitis (i.e., true positives).
Hybrid teleoptometry had high negative predictive value (99.2%; 95% CI, 98.2% to 99.8%; prevalence of infective conjunctivitis = 2.6%), meaning that there is a high likelihood that those who test negative for infective conjunctivitis in a population with 2.6% prevalence do not have infective conjunctivitis.
For people who need surgery (not further defined):
Hybrid teleoptometry had very low sensitivity to detect people who need surgery (58.1%; 95% CI, 39.1% to 75.5%), meaning that out of 100 people who need surgery, a teleoptometry exam could detect around 58 people who need surgery and miss around 42 people (i.e., false-negatives).
Hybrid teleoptometry had high specificity to detect people who do not need surgery (99.0%; 95% CI, 97.2% to 99.8%), meaning that out of 100 people who do not need surgery, around 99 people will be identified as not needing surgery.
Hybrid teleoptometry had good positive predictive value (85.7%; 95% CI, 63.7% to 97.0%; prevalence of needing surgery = 9.1%), meaning that there is a good likelihood that those who test positive for needing surgery in a population with a 9.1% prevalence actually need surgery (i.e., true positives).
Hybrid teleoptometry had high negative predictive value (95.9%; 95% CI, 93.1% to 97.8%; prevalence of needing surgery = 9.1%), meaning that there is a high likelihood that those who test negative for needing surgery in a population with a 9.1% prevalence do not need surgery.
For people who need spectacles (not further defined):
Hybrid teleoptometry had moderate sensitivity to detect people who need spectacles (77.2%; 95% CI, 68.4% to 84.5%), meaning that out of 100 people who need spectacles, a teleoptometry exam could detect around 77 people who need spectacles and miss around 23 people (i.e., false-negatives).
Hybrid teleoptometry had high specificity to detect people who do not need spectacles (96.9%; 95% CI, 93.7% to 98.7%), meaning that out of 100 people who do not need spectacles, around 96 people will be identified as not needing spectacles.
Hybrid teleoptometry had high positive predictive value (92.6%; 95% CI, 85.4% to 97.0%; prevalence of needing spectacles = 33.6%), meaning that there is a high likelihood that those who test positive for needing spectacles in a population with a prevalence of 33.6% actually need spectacles (i.e., true positives).
Hybrid teleoptometry had good negative predictive value (89.3%; 95% CI, 84.8% to 92.9%; prevalence of needing spectacles = 33.6%), meaning that there is a good likelihood that those who test negative for needing spectacles in a population with a prevalence of 33.6% do not need spectacles.
For people who need medicine (not further defined):
Hybrid teleoptometry had moderate sensitivity to detect people who need medicine (75.6%; 95% CI, 68.5% to 81.7%), meaning that out of 100 people who need medicine, a teleoptometry exam could detect around 76 people who need medicine and miss around 24 people (i.e., false-negatives).
Hybrid teleoptometry had high specificity to detect people who do not need medicine (100%; 95% CI, 97.8% to 100%), meaning that out of 100 people who do not need medicine, around 100 people will be identified as not needing medicine.
Hybrid teleoptometry had high positive predictive value (100%; 95% CI, 97.3% to 100.0%; prevalence of needing medicine = 51.9%), meaning that there is a high likelihood that those who test positive for needing medicine in a population with a prevalence of 51.9% will actually need medicine (i.e., true positives).
Hybrid teleoptometry had moderate negative predictive value (79.1%; 95% CI, 72.9% to 84.5%; prevalence of needing medicine = 51.9%), meaning that there is a moderate likelihood that those who test negative for needing medicine in a population with a prevalence of 51.9% do not need medicine.
For people who need any referral (not further defined):
Hybrid teleoptometry had low sensitivity to detect people who need any referral (64.3%; 95% CI, 44.1% to 81.4%), meaning that out of 100 people who need any referral, a teleoptometry exam could detect around 64 people who need any referral and miss around 36 people (i.e., false-negatives).
Hybrid teleoptometry had high specificity to detect people who do not need any referral (93.9%; 95% CI, 90.6% to 96.3%), meaning that out of 100 people who do not need any referral, around 93 people will be identified as not needing a referral.
Hybrid teleoptometry had very low positive predictive value (48.6%; 95% CI, 31.9% to 65.6%; prevalence of needing any referral = 8.3%), meaning that there is a very low likelihood that those who test positive for needing a referral in a population with a prevalence of 8.3% actually need a referral (i.e., true positives).
Hybrid teleoptometry had high negative predictive value (96.7%; 95% CI, 94.0% to 98.4%; prevalence of needing any referral = 8.3%), meaning there is a high likelihood that those who test negative for needing a referral in a population with a prevalence of 8.3% will not need a referral.
One study29 compared an asynchronous teleoptometry exam (conducted by an ophthalmologist, where the clinical data and photos were collected by an optometric assistant) to an in-person eye exam and reported the diagnostic test accuracy from 2 different examiners for any diagnoses that resulted in referral (no further details on the reason for, urgency of, or severity of the referral were provided). This study found that asynchronous teleoptometry had:
moderate sensitivity to detect any diagnoses that resulted in referral (77% [95% CI, 68% to 84%] to 81% [95% CI, 73% to 88%])
very low to moderate specificity to detect people who do not have a diagnosis that resulted in referral (58% [95% CI, 50% to 66%] to 74% [95% CI, 66% to 81%]).
This means that out of every 100 people with any diagnoses that resulted in referral, a teleoptometry exam could detect between 77 and 81 people with any diagnoses that resulted in referral and miss around 19 to 23 people (i.e., false-negatives) and that out of every 100 individuals who do not have a diagnosis that resulted in referral, between 58 and 74 people could be identified as not needing a referral and up to 42 people could be wrongly diagnosed as needing a referral (i.e., false-positives).
Refer to Table 19 for more details on the diagnostic accuracy of teleoptometry for people living with other conditions.
For Ocular Features in Children With Suspected Amblyopia
In 1 study27 in children with suspected amblyopia, the authors compared asynchronous teleoptometry exam results from 2 different examiners (i.e., an ophthalmologist reviewed a recording of the in-person exam) to an in-person exam of ocular features by an ophthalmologist that consisted of 14 different test components. The diagnostic test accuracy of identifying cases with positive (or “abnormal”) findings from the 14 ocular exam components was reported.
For 9 of these ocular feature exams, between 0 and 2 positive cases were identified (i.e., ≤ 0.6% of eyes), in which the sensitivity either could not be calculated or had very wide CIs (e.g., 0% to 97%).
For the 5 other ocular feature exams, when an asynchronous teleoptometry exam was compared to an in-person eye exam, this study found the following:
For the presence of nystagmus:
Asynchronous teleoptometry had good sensitivity to detect the presence of nystagmus (85% [95% CI, 42% to 99%] to 86% [95% CI, 42% to 99%]).
Asynchronous teleoptometry had high specificity to detect children who do not have nystagmus (99% [95% CI, 96% to 100%]; both examiners).
This means that out of every 100 children with nystagmus, a teleoptometry exam could detect 85 to 86 children with nystagmus and miss 14 to 15 children (i.e., false-negatives) and that out of every 100 children who do not have nystagmus, around 99 children could test negative.
For the presence of torticollis:
Asynchronous teleoptometry had very low sensitivity to detect the presence of torticollis (10% [95% CI, 0% to 44%] to 33% [95% CI, 7% to 70%]).
Asynchronous teleoptometry had high specificity to detect children who do not have torticollis (99% [95% CI, 95% to 99%] to 100% [95% CI, 97% to 100%]).
This means that out of every 100 children with torticollis, a teleoptometry exam could detect 10 to 33 children with torticollis and miss up to 67 to 90 children (i.e., false-negatives) and that out of every 100 children who do not have torticollis, between 99 and 100 children could test negative.
For the presence of heterotropia:
Asynchronous teleoptometry had low to moderate sensitivity to detect the presence of heterotropia (64% [95% CI, 5% to 74%] to 72% [95% CI, 61% to 81%]).
Asynchronous teleoptometry had high specificity to detect children who do not have heterotropia (90% [95% CI, 81% to 95%] to 93% [95% CI, 84% to 97%]).
This means that out of every 100 children with heterotropia, a teleoptometry exam could detect 64 to 72 children with heterotropia and miss 28 to 36 children (i.e., false-negatives) and that out of every 100 children who do not have heterotropia, between 90 and 93 children could test negative.
For the presence of esotropia:
Asynchronous teleoptometry had low to moderate sensitivity to detect the presence of esotropia (60% [95% CI, 47% to 92%] to 74% [95% CI, 62% to 84%]).
Asynchronous teleoptometry had high specificity to detect children who do not have esotropia (97% [95% CI, 90% to 99]; both examiners).
This means that out of every 100 children with esotropia, a teleoptometry exam could detect 60 to 74 children with esotropia and miss 26 to 40 children (i.e., false-negatives) and that out of every 100 children who do not have esotropia, around 97 children could test negative.
For the presence of exotropia:
Asynchronous teleoptometry had very low to moderate sensitivity to detect the presence of exotropia (44% [95% CI, 13% to 79%] to 70% [95% CI, 34% to 93%]).
Asynchronous teleoptometry had high specificity to detect children who do not have exotropia (96% [95% CI, 91% to 98%] to 99% [95% CI, 95% to 99%]).
This means that out of every 100 children with exotropia, a teleoptometry exam could detect 44 to 70 children with exotropia and miss 30 to 56 children (i.e., false-negatives) and that out of every 100 children who do not have exotropia, between 96 and 99 children could test negative.
Refer to Table 20 for more details on the diagnostic accuracy of teleoptometry for children living with suspected amblyopia.
Anterior Segment Pathologies in Children
In 1 study,24 the authors compared synchronous teleoptometry (i.e., a live stream of the in-person exam) and asynchronous teleoptometry (i.e., reviewing recordings of the in-person exam) to an anterior segment exam by an ophthalmologist and reported the diagnostic test accuracy for identifying “abnormal” findings for 6 anterior segment pathologies in children. The evaluation of teleoptometry to detect anterior segment pathologies in this study was limited to those pathologies identified in the study population, which the authors grouped into categories for analysis. Of note, none of the children examined in this study had anterior uveitis, and the study authors noted that they “cannot comment on the ability to detect anterior chamber cell and flare by digital slit lamp.”24
For the anterior segment pathologies, when a teleoptometry exam was compared to an in-person eye exam, this study found the following:
For eyelid or eyelash pathologies (i.e., blepharitis, haemangioma, epiblepharon, and pigmentation):
Synchronous teleoptometry had:
very low sensitivity to detect children with eyelid or eyelash pathologies (54%; 95% CI, 37% to 70%)
high specificity to detect children who do not have eyelid or eyelash pathologies (92%; 95% CI, 81% to 98%).
Asynchronous teleoptometry had:
moderate sensitivity to detect children with eyelid or eyelash pathologies (72%; 95% CI, 55% to 85%)
high specificity to detect children who do not have eyelid or eyelash pathologies (94%; 95% CI, 84% to 99%).
This means that out of every 100 children with eyelid or eyelash pathologies, a teleoptometry exam could detect 54 to 72 children who have eyelid or eyelash pathologies and miss 28 to 46 children (i.e., false-negatives) and that out of every 100 children who do not have eyelid or eyelash pathologies, between 92 and 94 children could be identified as not having eyelid or eyelash pathologies.
For conjunctiva or sclera pathologies (i.e., papillae, injection, hemorrhage, or melanosis):
Synchronous teleoptometry had:
high sensitivity to detect children with conjunctiva or sclera pathologies (90%; 95% CI, 73% to 98%)
high specificity to detect children who do not have conjunctiva or sclera pathologies (97%; 95% CI, 89% to 100%).
Asynchronous teleoptometry had:
low sensitivity to detect children with conjunctiva or sclera pathologies (66%; 95% CI, 46% to 82%)
high specificity to detect children who do not have conjunctiva or sclera pathologies (98%; 95% CI, 91% to 100%).
This means that out of every 100 children with conjunctiva or sclera pathologies, a teleoptometry exam could detect 66 to 90 children who have conjunctiva or sclera pathologies and miss 10 to 34 children (i.e., false-negatives) and that out of every 100 children who do not have conjunctiva or sclera pathologies, between 97 and 98 children could be identified as not having conjunctiva or sclera pathologies.
For cornea pathologies (i.e., cornea scar, band keratopathy, graft, neovascularization, Haab striae, cornea clouding, keratic precipitates, pannus, contact lens, posterior embryotoxon, ulcer, or Vogt striae):
Synchronous teleoptometry had:
good sensitivity to detect children with cornea pathologies (88%; 95% CI, 76% to 96%)
high specificity to detect children who do not have cornea pathologies (90%; 95% CI, 76% to 97%).
Asynchronous teleoptometry had:
high sensitivity to detect children with cornea pathologies (92%; 95% CI, 81% to 98%)
good specificity to detect children who do not have cornea pathologies (87%; 95% CI, 73% to 96%).
This means that out of every 100 children with cornea pathologies, a teleoptometry exam could detect 88 to 92 children who have cornea pathologies and miss up 8 to 12 children (i.e., false-negatives) and that out of every 100 children who do not have cornea pathologies, between 87 and 90 children could be identified as not having cornea pathologies.
For anterior chamber pathologies (i.e., tube shunt, shallow, or iris cyst):
Synchronous teleoptometry had:
high sensitivity to detect children with anterior chamber pathologies (96%; 95% CI, 79% to 100%)
high specificity to detect children who do not have anterior chamber pathologies (100%; 95% CI, 95% to 100%).
Asynchronous teleoptometry had:
high sensitivity to detect children with anterior chamber pathologies (92%; 95% CI, 73% to 99%)
high specificity to detect children who do not have anterior chamber pathologies (100%; 95% CI, 95% to 100%).
This means that out of every 100 children with anterior chamber pathologies, a teleoptometry exam could detect 92 to 96 children who have anterior chamber pathologies and miss 4 to 8 children (i.e., false-negatives) and that out of every 100 children who do not have anterior chamber pathologies, around 100 children could be identified as not having anterior chamber pathologies.
For iris pathologies (i.e., irregular pupil, peripheral iridotomy, atrophy, aniridia, iridocorneal adhesion, posterior synechiae, or peripheral anterior synechiae):
Synchronous teleoptometry had:
good sensitivity to detect children with iris pathologies (89%; 95% CI, 70% to 98%)
high specificity to detect children who do not have iris pathologies (95%; 95% CI, 87% to 99%).
Asynchronous teleoptometry had:
high sensitivity to detect children with iris pathologies (96%; 95% CI, 80% to 100%)
good specificity to detect children who do not have iris pathologies (83%; 95% CI, 71% to 91%).
This means that out of every 100 children with iris pathologies, a teleoptometry exam could detect 89 to 96 children who have iris pathologies and miss 4 to 11 children (i.e., false-negatives) and that out of every 100 children who do not have iris pathologies, between 83 and 95 children could be identified as not having iris pathologies.
For lens conditions (i.e., aphakia, posterior chamber intraocular lens, posterior capsular cataract, nuclear sclerosis, or anterior pigment):
Synchronous teleoptometry had:
high sensitivity to detect children with lens pathologies (96%; 95% CI, 81% to 100%)
high specificity to detect children who do not have lens pathologies (95%; 95% CI, 87% to 99%).
Asynchronous teleoptometry had:
good sensitivity to detect children with lens pathologies (89%; 95% CI, 71% to 98%)
high specificity to detect children who do not have lens pathologies (95%; 95% CI, 87% to 99%).
This means that out of every 100 children with lens pathologies, a teleoptometry exam could detect 89 to 96 children who have lens pathologies and miss 4 to 11 children (i.e., false-negatives) and that out of every 100 children who do not have lens pathologies, around 95 children could be identified as not having lens pathologies.
Refer to Table 21 for more details on the diagnostic accuracy of teleoptometry for children living with anterior segment pathologies.
Research Question 3: Clinical Utility of Teleoptometry for Eye Diseases and Conditions
One cross-sectional study31 assessed the ability of synchronous teleoptometry to diagnose and manage pediatric eye conditions in children referred to a vision centre for further assessment or surgical consultation (refer to Table 22 for detailed findings).
This study included data related to more than 20 primary diagnoses and reported that “no primary diagnoses were changed” between the teleoptometry and the in-person exam (common primary diagnoses included strabismus, eyelid abnormalities, glaucoma suspect, and conjunctival disorders) but that 2 nonprimary diagnoses (i.e., “a tiny non-visually significant lens opacity and a small intermittent vertical deviation”) were observed in person but not during the teleoptometry exam; however, neither affected patient management plans (no further details were reported).31
This study also reported that “no management plans, including surgical plans” were different between the teleoptometry and the in-person exam (no further details were reported).31
In children with strabismus, the authors reported excellent agreement for primary gaze angle measurements (i.e., intraclass correlation coefficients, 0.98 to 1.00; P < 0.0001) and almost perfect agreement for motility disease categorization (i.e., kappa coefficients, 0.94 to 1.00; P < 0.0001) between teleoptometry and in-person exams.31
Research Question 5: Guidelines for Teleoptometry for Glaucoma and Diabetic Retinopathy
We identified 2 evidence-based guidelines33,34 that provide recommendations on the use of teleoptometry for eye diseases and conditions (refer to Table 23 for detailed findings). One guideline, by the AOA, addresses the use of teleoptometry for primary open-angle glaucoma;34 the other guideline, by the ATA, provides recommendations on the use of teleoptometry for diabetic retinopathy.33
Recommendations for Open-Angle Glaucoma
For people with primary open-angle glaucoma, the guideline by the AOA recommends that teleoptometry programs “can provide increased access to care but should not be used alone or for the assessment or management of moderate or advanced diseases” (strong recommendation based on grade B evidence).34 This guideline noted that there was considerable variation in the evidence on the sensitivity of teleoptometry screening programs for glaucoma, highlighting the need for more studies to determine its true efficacy.
Recommendations for Diabetic Retinopathy
The ATA provided several recommendations on the use of teleoptometry for people with diabetic retinopathy.33 The recommendations are organized in this report based on the level of adherence to the recommendation,. The guideline authors did not report on the quality of the evidence that informed the recommendations.
Required actions whenever feasible and/or practical:
Teleoptometry “shall conform to the same professional ethics that govern in-person care” (e.g., confidentiality, data integrity, adherence to regulations).33
Those taking images of the eye for teleoptometry “shall possess the knowledge and skills for imaging independently or with assistance and consultation by telephone.”33
Recommended action:
Due to the possibility that individuals with ungradable images have diabetic retinopathy, images that are not possible to obtain or grade “should be considered a positive finding”; these individuals “should be promptly reimaged or referred for a more advanced evaluation.”33
Actions that may be considered:
For the identification of the presence or severity of diabetic macular edema, images “may be acquired and reviewed stereoscopically,” or images “may” be acquired non-stereoscopically to determine the severity of diabetic macular edema, based on the teleoptometry programs’ operational preferences.33
Additional relevant information (e.g., medical and surgical history), “may” also be used when interpreting the images.33
Limitations
Methodology and Engagement Approach
As the nature and scope of the request was focused on reviewing published clinical data, we did not conduct direct engagement with patients, caregivers, or providers. We also did not search for or include literature on perspectives, experiences, or other evidence relevant to underserved groups. With this limited scope, we may have missed including the lived and living experience of individuals who are disproportionately affected by the shortage in optometrists (e.g., Indigenous Peoples in Canada, individuals living in areas of social isolation or remote areas). We acknowledge this as a limitation of our work, and that this Rapid Review may not highlight or identify perspectives and evidence of relevance to these underserved groups in Canada. Of note, as part of the CDA-AMC organizational commitment to reconciliation, we know it is important to consider and learn from Indigenous perspectives in our work. We also recognize that the research team consists of settler researchers, and we come to this work with our individual privileges and biases. Understanding the perspectives and priorities of Indigenous Peoples and other underserved groups as they relate to eye care and teleoptometry can support informed health care decision-making.
Evidence Gaps
We identified 1 cross-sectional study32 on the clinical effectiveness of teleoptometry versus an in-person comprehensive eye exam for assessments of refractive error and ocular health. This study included a limited number of adult participants (n = 66), with limited population characteristics provided (mean age = 29.7 years; no other information provided), which may limit the conclusions that can be drawn from this evidence. This study excluded children, people with low vision, and people with acute ocular conditions or diseases; thus, it is unknown if the findings are generalizable to these populations.
For the diagnostic test accuracy studies, we identified a limited quantity of evidence for some eye conditions or diseases, potentially limiting the reliability of the findings for these eye conditions or diseases, with findings contributed by 1 study each for clinically significant macular edema,28 keratoconus,26 ocular features in children with suspected amblyopia,27 pediatric anterior segment pathologies,24 nonserious eye injury,23 and conjunctivitis.23
In some of the diagnostic test accuracy studies there was also a small number of people with certain diseases or conditions (i.e., diabetic retinopathy [2 studies23,29 with ≤ 3% prevalence in the study population], glaucoma [1 study23 with 1.2% prevalence in the study population], AMD [2 studies29,30 with 2% prevalence in the study population], ocular features in children with suspected amblyopia [1 study,27 in which 12 of the 14 ocular exams had 0% to 2.8% of cases with positive findings]). This may have contributed to imprecision in calculating sensitivity or specificity (e.g., wide CIs around the estimates) or made it not possible to calculate sensitivity for these diseases or conditions.
We identified 1 cross-sectional study on the clinical utility of teleoptometry versus an in-person eye exam. This study was specific to children and included a limited number of relevant outcomes (i.e., agreement in diagnosis and management plans, and agreement in angle measurement and disease category in children with strabismus), some of which were narrower in scope than this report because they focused on children with strabismus. We did not identify any studies on the clinical utility of teleoptometry in adults nor any studies that reported other potentially relevant outcomes (e.g., time to treatment, patient satisfaction, harms), which limits the conclusions that can be drawn from these findings.
There were no evidence-based guidelines found regarding the use of teleoptometry for comprehensive eye exams; therefore, no conclusions can be formed on that research question.
Regarding the use of teleoptometry for screening, diagnosing, and monitoring eye diseases, we identified 1 guideline focused on people with primary open-angle glaucoma34 and 1 guideline focused on people with diabetic retinopathy33 but did not identify any other guidelines on the screening, diagnosing, or monitoring of other eye diseases; therefore, no conclusions can be formed regarding best practices for teleoptometry for those eye diseases.
The reporting of the participants’ characteristics was generally limited across the SR and the included primary studies. We used PROGRESS-Plus37 to guide data extraction, and while some primary studies provided basic demographic details, such as the mean age and the proportion of male or female participants, and 1 study31 reported race, ethnicity, and language, most of the PROGRESS-Plus37 criteria were not described (e.g., gender, race, ethnicity, culture, language, occupation, religion, education, socioeconomic status, social capital, discrimination [e.g., disability-based], or relationships).
For many eye diseases, such as cataracts, glaucoma, diabetic retinopathy, and AMD, the disease presents with varying degrees of severity. Clinical expert experience indicates that it is easier to diagnose more advanced cases than early ones, and the goal is to identify eye diseases in the earlier stages to improve prognosis. However, most of the diagnostic test accuracy studies in this report treated conditions as binary in the diagnostic test analysis (i.e., the participant has the disease or does not have the disease), rather than accounting for disease severity. For example, studies grouped different grades of cataracts together23,25,29 and combined cases of glaucoma suspect with cases of definite glaucoma.25,29 Grouping early-stage and late-stage disease limits our ability to assess how teleoptometry can identify disease at earlier stages.
Heterogeneity of the Evidence
There was substantial clinical heterogeneity in the interventions used in the studies that informed this review. The teleoptometry exams varied in terms of how they were delivered (i.e., asynchronously,22,24-30 synchronously,24,31 or a hybrid of both23,32), which tests or components of an eye exam were conducted (e.g., a comprehensive eye exam, select components, photos only), the type of eye care provider doing the remote assessment (e.g., optometrist, ophthalmologist, retina specialist), and the qualifications of the person performing the in-person tests (e.g., optometric assistant,29 ophthalmic assistant,30 optometrist,25,31 vision technician,23 ophthalmologist,24,27 cornea surgeon,26 postgraduate student of medical informatics,28 or third-year optometry student32). In addition, in some studies with multiple remote examiners,27 the teleoptometry findings differed between examiners, which suggests there is the potential that the technology skills of the remote examiners may influence the diagnostic accuracy results.
There was also considerable heterogeneity in the clinical indications, with teleoptometry being used for components of comprehensive eye exams (e.g., assessments of refractive error or ocular health)32 and to assess glaucoma,22,23,25,29 diabetic retinopathy,23,28-30 AMD,25,29,30 cataracts,23,25,29 macular edema,28 keratoconus,26 ocular features in children with suspected amblyopia,27 pediatric anterior segment pathologies,24 nonserious eye injury,23 and conjunctivitis.23
The differences in the teleoptometry exams and the clinical indications across the studies can make it difficult to draw conclusions about the overall clinical effectiveness, diagnostic test accuracy, or clinical utility of teleoptometry.
Generalizability
Two studies were conducted in Canada (1 clinical effectiveness study32 and 1 diagnostic test accuracy study27), and 1 study30 included authors from Canada but was conducted in Kenya. No other studies were conducted in Canada, and none of the guidelines were developed for use in Canada.
In Canada, it is likely that teleoptometry would primarily be considered for the provision of eye care when there are barriers to accessing in-person care, such as shortages of optometrists in areas outside urban centres (e.g., rural and remote locations), with an in-person optometric assistant performing some tasks and assisting the remote optometrist. We only identified 1 study23 where the teleoptometry exam took place at a rural vision centre with a remote ophthalmologist. In the other studies, the teleoptometry exam was conducted in an urban setting (e.g., hospital, university, clinic) with a remote optometrist located in a different room in the same building, or the setting was unclear. This setting is not representative of where most people would receive teleoptometry exams in Canada (i.e., in rural or remote locations) and would not be subject to the potential concerns that would exist in practice in these settings (e.g., reliability of internet connection or bandwidth for transmitting images or live stream consultations).
Some studies included limited assessments compared with what would typically be expected for those indications in standard optometric practice, and this may impact the generalizability of the findings. For the single study that examined the use of teleoptometry for comprehensive eye exams,32 neither the in-person nor the teleoptometry exam included a dilated fundus examination (which is not possible to perform remotely), which is an important component of a thorough ocular health exam. This omission may limit the conclusions that can be drawn about the ocular health assessments from this study and their relevance to clinical practice of comprehensive eye exams in Canada. For the single study that examined the diagnoses of clinically significant macular edema, the teleoptometry component consisted of the review of single digital images with no additional clinical data,28 and a clinical expert is uncertain that this would reliably diagnose macular edema, given that to accurately detect edema a dilated fundus exam, an optical coherence tomography scan, or at least a stereoscopic fundus photo, would be required.
In addition, in 6 studies,24,26-28,31,32 the conduct of the teleoptometry exam may not reflect how teleoptometry is applied in practice in Canada (i.e., a teleoptometry exam conducted by a remote optometrist or ophthalmologist with support from an in-person optometric assistant). Possible variation from clinical practice in Canada for these studies specifically related to the review of a recording of the in-person exam,24,27 the review of the clinical data obtained from the in-person exam,26 the review of digital images only with no additional clinical data,28 or in-person tests normally delegated to an optometric assistant that were conducted by a third-year optometry student32 or an optometrist.31 If the individual conducting the teleoptometry exam is more skilled than an optometric assistant (e.g., optometrist, ophthalmologist), then it may have biased the results in favour of better results for teleoptometry and may not reflect the success of teleoptometry in practice.
Collectively, these considerations may limit the generalizability of the findings from this Rapid Review to the health care context in Canada.
Conclusions and Implications for Decision- or Policy-Making
This Rapid Review evaluated the literature regarding the clinical effectiveness, diagnostic test accuracy, and clinical utility of teleoptometry compared to in-person eye exams for people requiring eye care and those at risk for or with confirmed or suspected eye diseases, as well as guidelines related to the use of teleoptometry for these populations. We identified 1 cross-sectional study32 for research question 1; 1 SR (with 1 relevant primary study)22 and 8 cross-sectional studies23-30 for research question 2; 1 cross-sectional study31 for research question 3; and 2 evidence-based guidelines for research question 5.33,34 We did not find any eligible guidelines for research question 4.
Evidence on Teleoptometry for Comprehensive Eye Exams
Limited evidence from adults who have not previously received eye care suggests that teleoptometry may offer a similar ability to identify and manage reduced vision related to refractive error when compared to an in-person exam (1 cross-sectional study); however, confidence in the evidence may be limited due to the small number of participants (n = 66).32 The refractive errors in the study population ranged from –8.78 to +2.63 diopters, which adequately covers myopic refractive errors but provides a narrow range of hyperopic refractive errors. This may limit understanding of the effectiveness of teleoptometry in identifying hyperopic refractive errors. Teleoptometry had good to excellent agreement with the in-person exam for refractive measurements (i.e., best corrected visual acuity, spherical, cylindrical, and axis refraction), and participants reported no differences in the quality of their vision, the presence of distortion, dizziness when walking, or the acceptability of wearing the new prescription daily when trial glasses using prescriptions obtained via teleoptometry versus in-person exams were compared.32
For the visual function and ocular health assessment (which excluded a dilated fundus exam), there was fair agreement for extraocular motility, substantial agreement for anterior and posterior segments, and almost perfect agreement for entering distance visual acuity and colour vision between the teleoptometry and the in-person exam. The small number of participants (n = 66), the relatively younger age of the participants (mean age = 29.7 years), and the low prevalence of ocular pathologies in this study may have limited the findings (e.g., there were no participants with pupil abnormalities; thus, no statistical analysis for such participants was possible). A larger sample with a wider age range and more ocular pathologies may be required to better evaluate the effectiveness of teleoptometry for assessing ocular health across different populations. The teleoptometry exam identified most ocular health abnormalities; 3 conditions with little risk of harm (mostly dry eye disease) and 1 case of inactive corneal pannus were not diagnosed, and 1 case of suspected papilledema could not be ruled out in the teleoptometry exam due to the quality of the fundus photo.32 Neither modality included a dilated fundus exam (which is not possible to perform remotely, though it is considered best practice in Canada for a comprehensive eye exam), which may limit the comprehensiveness of the ocular health assessment. Eye care providers were also less confident conducting the teleoptometry exam than the in-person exam.32
Participants were more satisfied with the in-person exam than the teleoptometry exam;32 however, as the relevant study was conducted in Montreal, where there is access to eye care, it is unclear whether the level of satisfaction with teleoptometry would differ in individuals who live in rural and remote areas or other underserved areas.
The findings of this study32 may have been influenced by the approach to the teleoptometry exam, in which a third-year optometry student conducted the tests that would normally be delegated to or assisted by an optometric assistant. This may not be representative of teleoptometry in practice and may have biased the findings in favour of improved results for teleoptometry.
We did not identify any evidence about the clinical effectiveness of teleoptometry for comprehensive eye exams in children, nor did we identify any evidence-based guidelines on teleoptometry for comprehensive eye exams that met the inclusion criteria for this report.
Evidence on Teleoptometry for Screening, Diagnosing, and Monitoring Eye Diseases
Adults
Diabetic Retinopathy
Teleoptometry had high specificity to detect those who do not have diabetic retinopathy, correctly classifying more than 96% of people who do not have diabetic retinopathy with a negative result across the included studies.23,28-30 This means that out of every 100 people who do not have diabetic retinopathy, 96 people could correctly test negative and up to 4 people could be wrongly diagnosed as having diabetic retinopathy. Teleoptometry also had a high negative predictive value across both low-prevalence and high-prevalence study populations (i.e., a high proportion of true negative test results).
However, teleoptometry had variable sensitivity for detecting diabetic retinopathy, correctly detecting between 57% and 92% of people with diabetic retinopathy.23,28-30 This means that out of every 100 people with diabetic retinopathy, a teleoptometry exam could correctly detect between 57 and 92 people with diabetic retinopathy but miss up to 43 people with diabetic retinopathy (i.e., possible false-negative test results), and a further in-person exam may be required to confirm the diagnosis. The positive predictive value of teleoptometry also varied from very low to moderate depending on the prevalence of diabetic retinopathy in the study sample, with some studies using teleoptometry to screen people with no known risk of diabetic retinopathy and others including people with diabetes and a higher prevalence of diabetic retinopathy in the study sample.
For the use of teleoptometry for people with diabetic retinopathy, in addition to recommendations regarding the types of imaging, the skills of the imagers, and the information to consider when making a diagnosis, the ATA recommends that individuals with unobtainable or ungradable images should be considered to have received a positive finding and that these people should be promptly reimaged or referred for further evaluation.33
None of the studies reported the findings by severity of diabetic retinopathy, with only 1 study28 reporting the proportion of participants with different stages of disease and reporting separate results for “any diabetic retinopathy” and “diabetic retinopathy requiring a referral”; thus, we cannot form conclusions about the accuracy of teleoptometry in diagnosing diabetic retinopathy across the different stages of the disease.
Cataracts
Under the conditions of the 3 included studies, teleoptometry had high specificity for cataracts, correctly classifying at least 95% of people who did not have cataracts with a negative test result.23,25,29 This means that out of every 100 people who do not have cataracts, around 95 people could correctly test negative and up to 5 people could be wrongly diagnosed as having cataracts. Teleoptometry also had a high negative predictive value for cataracts across both low-prevalence and high-prevalence study populations (i.e., a high proportion of true negative test results).
Teleoptometry also had variable (good to high) sensitivity for detecting cataracts, correctly detecting between 88% and 100% of people with cataracts.23,25,29 This means that out of every 100 people with cataracts, a teleoptometry exam could correctly detect between 88 and 100 people with cataracts but miss up to 12 people with cataracts (i.e., possible false-negative test results). The positive predictive value of teleoptometry varied from low to high depending on the prevalence of cataracts in the study sample.
Two studies23,25 grouped different grades of cataracts together, of which only 1 study25 reported the proportion of participants with each grade of cataract. The third study29 only reported cataracts that had been referred for surgery. These groupings limit our understanding of the accuracy of teleoptometry in diagnosing cataracts across the different stages of the disease.
Glaucoma
Under the conditions of the 4 included studies, teleoptometry had variable (very low to high) sensitivity for detecting glaucoma or glaucoma suspect, correctly detecting between 12% and 100% of people with glaucoma or glaucoma suspect.22,23,25,29 This means that out of every 100 people with glaucoma or glaucoma suspect, a teleoptometry exam could correctly detect between 12 and 100 people with glaucoma or glaucoma suspect but miss up to 88 people with glaucoma or glaucoma suspect (i.e., possible false-negative test results), and a further in-person exam may be required to confirm the diagnosis. The positive predictive value of teleoptometry varied from very low to high depending on the prevalence of glaucoma or glaucoma suspect in the study sample, with some studies23 using teleoptometry to screen people with no known risk of glaucoma and other studies25 including people at risk for glaucoma (e.g., blurry vision for > 3 months) in the study sample.
Teleoptometry also had variable (moderate to high) specificity for glaucoma or glaucoma suspect, correctly classifying more than 76% of people who did not have glaucoma or glaucoma suspect with a negative test result.22,23,25,29 This means that out of every 100 people who do not have glaucoma or glaucoma suspect, at least 76 people could correctly test negative and up to 24 people could be wrongly diagnosed as having glaucoma or glaucoma suspect. Teleoptometry also had a high negative predictive value for glaucoma or glaucoma suspect across both low-prevalence23 and high-prevalence25 study populations (i.e., a high proportion of true negative test results).
The variation in diagnostic tests performed across these studies should be considered when interpreting the accuracy of teleoptometry in diagnosing glaucoma or glaucoma suspect. While all 4 studies assessed intraocular pressure as part of the teleoptometry exam, only some studies included additional disease-specific tests such as central corneal thickness22,29 or fundus photos.25,29 These differences are important to consider as the current standard of practice for a comprehensive glaucoma evaluation involves numerous diagnostic tests to ensure accurate diagnosis.38
These findings on the diagnostic test accuracy of teleoptometry for glaucoma align with the recommendation from the AOA34 that teleoptometry can provide increased access to care in people with primary open-angle glaucoma but should not be used alone or for the assessment or management of moderate or advanced disease. In addition, the AOA found that teleoptometry had significant variation in estimations of sensitivity for glaucoma screening, emphasizing the need for more research to determine teleoptometry’s true accuracy.
Two studies25,29 grouped glaucoma and glaucoma suspect, of which only 1 study25 reported the proportion of participants by the grade of glaucoma. The other 2 studies22,23 reported the proportion of participants with glaucoma but did not report whether that included participants with glaucoma suspect. Thus, we CDA-AMC cannot draw conclusions about the accuracy of teleoptometry in diagnosing glaucoma across the different stages of the disease.
Age-Related Macular Degeneration
Under the conditions of the 3 included studies, teleoptometry had variable (very low to high) sensitivity for detecting AMD, correctly detecting between 23% and 99% of people with AMD.25,29,30 This means that out of every 100 people with AMD, a teleoptometry exam could correctly detect between 23 and 99 people with AMD but miss up to 77 people with AMD (i.e., possible false-negative test results), and a further in-person exam may be required to confirm the diagnosis. The positive predictive value of teleoptometry varied from very low to high depending on the prevalence of AMD in the study sample.
Teleoptometry also had high specificity for AMD, correctly classifying more than 95% of people who do not have AMD with a negative test result across the included studies.25,29,30 This means that out of every 100 individuals who do not have AMD, at least 95 people could correctly test negative and up to 5 people could be wrongly diagnosed as having AMD (i.e., possible false-positive test results). Teleoptometry also had a high negative predictive value for AMD across both low-prevalence30 and high-prevalence25 study populations (i.e., high proportion of true negative test results).
Of note, AMD can be categorized into 4 stages of severity;39 however, none of the included studies addressed this in their reporting of participant demographics or outcomes. Therefore, we cannot make any conclusions about the accuracy of teleoptometry in diagnosing AMD across the different stages of the disease.
Keratoconus Progression
A limited quantity of evidence from 1 study suggests that teleoptometry had low sensitivity to detect keratoconus progression, correctly identifying around 69% of people with keratoconus progression,26 which means that out of every 100 people with keratoconus progression, a teleoptometry exam could correctly detect 69 people with keratoconus progression but miss up to 31 people with keratoconus progression (i.e., possible false-negative test results). The positive predictive value of teleoptometry for keratoconus progression was very low in this study sample.
Teleoptometry has high specificity for keratoconus progression, correctly classifying around 95% of people who do not have keratoconus progression with a negative result,26 which means that out of every 100 individuals who do not have keratoconus progression, about 95 people could correctly test negative and up to 5 people could be wrongly diagnosed as having keratoconus progression (i.e., possible false-positive test results). Teleoptometry also had a high negative predictive value for keratoconus progression in this study sample (i.e., a high proportion of true negative test results).
The findings of this study26 may have been influenced by the conduct of the teleoptometry exam, which was conducted by an optometrist and a cornea surgeon. This may not be representative of teleoptometry in practice (i.e., normally the in-person tests would be delegated to or assisted by an optometric assistant) and may have biased the findings in favour of improved results for teleoptometry.
Macular Edema
A limited quantity of evidence from 1 study suggests that teleoptometry had high sensitivity to detect clinically significant macular edema, correctly identifying around 93% of people with clinically significant macular edema,28 which means that out of every 100 people with clinically significant macular edema, a teleoptometry exam could correctly detect 93 people with clinically significant macular edema and miss up to 7 people (i.e., possible false-negative test results). Teleoptometry also had high specificity for macular edema, correctly classifying 100% of people who do not have clinically significant macular edema with a negative result,28 which means that out of every 100 individuals who do not have clinically significant macular edema, up to 100 people could correctly test negative. This study did not report CIs or positive and negative predictive values, limiting our confidence in this finding. As this study only reported on the presence of clinically significant macular edema, we cannot make any conclusions about the accuracy of teleoptometry in diagnosing various stages of the disease. However, the teleoptometry component of this study only involved the review of a single digital image, and it is unclear whether this would be sufficient to accurately diagnose macular edema, thus reducing our confidence in the findings.
Other Eye Conditions
Teleoptometry had very low or low sensitivity for nonserious eye injury, allergic conjunctivitis, and need for surgery,23 correctly identifying around 41% of people with nonserious eye injury, 43% of people with allergic conjunctivitis, and 58% of people who need surgery. This means that out of every 100 people with these conditions, a teleoptometry exam could miss up to 59 people with nonserious eye injury, 57 people with allergic conjunctivitis, and 42 people who need surgery (i.e., possible false-negative test results). Teleoptometry had high specificity for nonserious eye injury, allergic conjunctivitis, and need for surgery,23 correctly classifying at least 98% of people who do not have these conditions with a negative result. The negative predictive value was high for all 3 conditions, and the positive predictive value was moderate to good.
Teleoptometry had moderate sensitivity for people with infective conjunctivitis, people who need spectacles, and people who need medicine,23 correctly identifying around 72% of people with infective conjunctivitis, 77% of people who need spectacles, and 75% of people who need medicine. This means that out of every 100 people with these conditions, a teleoptometry exam could miss up to 28 people with infective conjunctivitis, 23 people who need spectacles, and 25 people who need medicine (i.e., possible false-negative test results). Teleoptometry had high specificity for infective conjunctivitis, people who need spectacles, and people who need medicine,23 correctly classifying at least 96% of people who do not have these conditions. The positive and negative predictive values for these conditions differed by test.
Teleoptometry had variable (low to moderate) sensitivity to detect people with diagnoses that require a referral,23,29 correctly classifying between 64% and 77% of people who need a referral, which means that out of 100 people who need a referral, a teleoptometry exam could correctly detect between 64 and 77 people who need a referral but miss up to 36 people (i.e., possible false-negative test results). Teleoptometry has variable (very low to high) specificity to detect people with diagnoses that require a referral,23,29 correctly classifying between 58% and 93% of people who do not need a referral, which means that out of every 100 individuals who do not need a referral, at least 58 could correctly test negative and up to 42 could be wrongly diagnosed as needing a referral (i.e., possible false-positive test results). However, neither study that reported on this outcome further defined what they meant by the need for referral (e.g., referral for what or to whom), limiting the interpretation of these findings.
Clinical Utility
We did not identify any evidence about the clinical utility of teleoptometry for the screening, diagnosing, or monitoring of eye diseases in adults that met the inclusion criteria for this report.
Children
For the 5 ocular exams in children with suspected amblyopia in which more than 2 positive cases were identified (i.e., the presence of nystagmus, torticollis, heterotropia, esotropia, or exotropia), teleoptometry had high specificity, correctly classifying more than 90% of children who do not have these conditions with a negative result.27 This means that out of every 100 children who do not have these conditions, at least 90 people could correctly test negative and up to 10 people could be wrongly diagnosed as having 1 of these conditions.
Teleoptometry also had good sensitivity to detect the presence of nystagmus, correctly identifying around 85% of cases,27 which means that out of every 100 children with nystagmus, a teleoptometry exam could correctly detect 85 children with nystagmus but miss up to 15 children with nystagmus (i.e., possible false-negative test results). However, teleoptometry had very low to moderate sensitivity to detect the presence of torticollis, heterotropia, esotropia, or exotropia, correctly identifying between 10% and 74% of positive cases,27 which means that out of every 100 children with 1 of these conditions, a teleoptometry exam could correctly detect between 10 and 74 children with the condition but miss up to 90 children with the condition (depending on the condition), and a further in-person exam may be required to confirm the diagnosis.
In children, teleoptometry had variable (good to high) specificity to detect different anterior segment pathologies (i.e., pathologies of the eyelid, eyelash, conjunctiva, sclera, cornea, anterior chamber, iris, or lens), correctly classifying between 83% and 100% of children who do not have anterior segment pathologies with a negative result,24 which means that out of every 100 children who do not have these anterior segment pathologies, at least 83 children could correctly test negative and up to 17 children could be wrongly diagnosed as having these pathologies.
The sensitivity of teleoptometry to detect anterior segment pathologies in children varied by pathology, with very low to high sensitivity to detect pathologies of the eyelid, eyelash, conjunctiva, or sclera, detecting between 54% and 90% of these anterior segment pathologies,24 which means that out of every 100 children with 1 of these conditions, a teleoptometry exam could correctly detect between 54 and 90 children with the condition but miss up to 46 children with the condition, depending on the condition and the type of teleoptometry (i.e., asynchronous versus synchronous), and a further in-person exam may be required to confirm the diagnosis. However, teleoptometry had good to high sensitivity to detect pathologies of the cornea, anterior chamber, iris, or lens, correctly detecting between 87% and 96% of these anterior segment pathologies,24 which means that out of every 100 children with 1 of these conditions, a teleoptometry exam could correctly detect between 87 and 96 children with the condition but miss up to 13 children with the condition. These findings are limited to the specific anterior segment conditions identified in the study population, and the results should not be extrapolated to other pathologies of the anterior segment (e.g., uveitis) as there may be limitations in the ability of the teleoptometry exam to comprehensively assess for other conditions.
However, the teleoptometry exam in both these studies in children24,27 may not be representative of teleoptometry in practice, as it involved viewing a recording of the in-person exam, which was conducted by an ophthalmologist (rather than having the in-person tests conducted by an optometric assistant). This may have influenced the findings of the study in favour of teleoptometry.
Limited evidence suggests that teleoptometry may offer a similar ability to develop patient management plans as an in-person exam in children with certain eye conditions (1 cross-sectional study) and that in children with strabismus, teleoptometry had excellent to almost perfect agreement with the in-person exam for primary gaze measurements and motility disease categorization.31 However, the in-person components of the teleoptometry exam were conducted by a pediatric optometrist, rather than an optometric assistant,31 which is not representative of how teleoptometry is implemented in practice and may have influenced the results in favour of better results for teleoptometry. In addition, the participants in this study had been recruited from a vision centre, to which they had been referred for further assessment or surgical consultation due to abnormal findings. This referral-based recruitment may have influenced the study results in favour of improved diagnostic performance of the teleoptometry exams.
We did not identify any evidence-based guidelines on teleoptometry for screening, diagnosing, and monitoring eye diseases in children that met the inclusion criteria for this report.
Considerations for Future Research
To improve our understanding of the role of teleoptometry for comprehensive eye exams, additional studies are needed with larger sample sizes. Future studies on the use of teleoptometry for comprehensive eye exams should also consider including children, as well as people with low vision or other ocular conditions, to provide an understanding of the clinical effectiveness of teleoptometry in these populations in assessing vision quality and ocular health. The availability of additional primary studies would enable the development of evidence-based guidelines on the use of teleoptometry for comprehensive eye exams.
Additional studies on the diagnostic test accuracy or clinical utility of teleoptometry for screening, diagnosing, and monitoring eye diseases are also needed to improve our understanding of the role of teleoptometry in these clinical scenarios, particularly for those conditions or eye diseases for which we only identified 1 study that met the inclusion criteria for this report (i.e., for macular edema, keratoconus, children with suspected amblyopia, pediatric anterior segment pathologies, nonserious eye injury, and conjunctivitis). To improve the precision of the effect estimates, study authors should also ensure that the studies are adequately powered to detect the conditions or diseases of interest.
To help address the heterogeneity in the format of teleoptometry exam delivery, future research should consider a more standardized approach to teleoptometry (e.g., which tests are conducted and by whom). In Canada, for studies on comprehensive eye exams, authors may wish to consider the evidence-informed proposed clinical framework for providing comprehensive teleoptometry eye exams (developed by optometrists from Canada’s 2 schools of optometry), which outlines the exam workflow, the tasks delegated to the optometric assistant or the remote optometrist, and patient management.14
Study authors may also wish to consider the setting for the teleoptometry component of their study. Conducting the teleoptometry exam in a rural or remote location with a remote optometrist or ophthalmologist would help understanding of the effectiveness of teleoptometry in practice and may improve understanding of other important outcomes (e.g., patient satisfaction, time to treatment) or potential barriers to treatment (e.g., tests that cannot be conducted remotely, acceptance of teleoptometry, technical challenges such as unreliable internet connection or learning a new technology).
Additionally, study authors may consider reporting detailed participant characteristics across dimensions of diversity, such as age, religion, gender, ethnicity, mental and physical ability, and place of residence (or other PROGRESS-Plus criteria), to provide a better understanding of how the results of their study may apply to other populations.
Considerations for Decision- or Policy-Making
For adults requiring a comprehensive eye exam, limited evidence in this Rapid Review suggests that teleoptometry may be useful for identifying and managing reduced vision due to refractive error and for identifying whether certain tests of visual function are within normal limits (e.g., entering distance visual acuity, colour vision). However, decision-makers should be aware that there are limitations to the evidence included in this report, such as the limited ocular health assessments (which did not include a dilated fundus exam) and the small number of study participants, with a relatively young participant age and a narrow range of hyperopic refractive errors. These limitations hinder interpretation of the results and may limit the generalizability of the findings to other populations, to other ocular health outcomes, or to typical clinical practice in Canada. In addition, not all individuals and providers may be comfortable with teleoptometry. While we did not identify any evidence-based guidelines with specific recommendations for comprehensive eye exams, the CAO supports the use of teleoptometry to augment in-person care and as an essential mechanism for the provision of eye care when there are barriers to care.17
For screening and diagnosing eye diseases and conditions, the findings in this review suggest that, in general, teleoptometry has high specificity for the eye conditions and diseases of the included studies, which means that in most cases, teleoptometry exams may accurately classify people who do not have those diseases. This means that unnecessary additional assessments could be avoided in those who do not need them. The findings in this review also suggest that the sensitivity of teleoptometry to detect eye diseases and conditions varies by indication. Teleoptometry had good to high sensitivity for some eye diseases or conditions (i.e., cataracts; clinically significant macular edema; nystagmus; and pathologies of the cornea, anterior chamber, iris, or lens), which means that teleoptometry can correctly identify about 85% to 93% of people with these conditions. However, the very low to moderate sensitivity (e.g., 10% to 77%) of teleoptometry to detect the other eye diseases and conditions covered in this review (e.g., diabetic retinopathy; glaucoma; AMD; keratoconus progression; conjunctivitis; the presence of torticollis, heterotropia, esotropia, or exotropia; pathologies of the eyelid, eyelash, conjunctiva, or sclera) means that we cannot be sure that a person with those conditions will be diagnosed based on a teleoptometry exam result, and further in-person testing may be required. This may be an important consideration for the use of teleoptometry in populations at higher risk of these conditions (e.g., people living with diabetes).
A limitation of the evidence is that most studies did not distinguish between different stages or severity of the diseases, often grouping different stages of disease together (e.g., for cataracts, glaucoma, AMD, and diabetic retinopathy). By treating the conditions as binary (present or absent) in their analysis, the studies may have biased the findings for teleoptometry as it is easier to diagnose later stages of disease. However, in clinical practice the goal is to identify eye disease in earlier stages to improve prognosis, and not distinguishing diseases by stage or severity limits understanding of the ability of teleoptometry to diagnose diseases at different stages.
For teleoptometry exams that rely on images (e.g., fundus photographs) to diagnose certain conditions, decision-makers may wish to consider that the quality of the images may be a limitation, as images that are ungradable or unreadable (e.g., due to poor pupil dilation, media opacities, or poor image quality) may preclude diagnosis. It may be necessary to repeat the images if the quality is not acceptable, or the person being examined may need to be referred for an in-person visit, which is the approach suggested in the ATA guideline for diabetic retinopathy when images are unobtainable or ungradable.33 Repeating the images may be challenging if an asynchronous model is used and the individual is no longer available (e.g., when images are determined to be poor quality, the individual may no longer be in the clinic).
Decision-makers can use the information summarized in this review to inform their decisions about the use of teleoptometry for comprehensive eye exams and for screening and diagnosing eye diseases and conditions. The provision of eye care is complex and requires numerous tests and diagnostic tools, some of which are challenging to perform and interpret remotely (e.g., slit lamp of the anterior segment), and it is not possible to perform all tests remotely because they require in-person interpretation by an optometrist or ophthalmologist (e.g., dilated fundus exam).14,16 Some pathologies may only require a single test, such as digital imaging techniques like fundus photography, to diagnose; other eye diseases may require the integration of clinical data from multiple tests, patient history, and visual symptoms to reach an accurate diagnosis. There was considerable variation in the diagnostic tests performed across studies for the same condition, and it is possible that a comprehensive evaluation for each disease was not always performed, which could impact the accuracy results of these studies and our interpretation of the findings for teleoptometry. In addition to the clinical evidence, decision-makers may wish to consider whether teleoptometry impacts access to eye care, particularly in rural or remote or other underserved areas.
When making these decisions, careful consideration is needed for factors such as the type of teleoptometry (i.e., asynchronous, synchronous, or a hybrid of both), the diagnostic complexities inherent to eye care, which tests or images are included (i.e., an isolated ophthalmic test versus a comprehensive eye exam), the ability to maintain patient privacy and data security for teleoptometry exams, the clinical indication (i.e., comprehensive eye exam or disease-specific screening), the technical ability of the eye care providers (technicians, optometrists, and ophthalmologists) to perform the teleoptometry exam, the potential need for reimaging or referral for additional in-person assessment, and the individual needs and preferences of the person being examined.
The findings in this report suggest that teleoptometry may be useful in certain populations for identifying and managing certain eye diseases and conditions; however, the limitations of the technology and the identified evidence suggest that teleoptometry is not a replacement for all in-person eye care. Nonetheless, as supported by the CAO,17 teleoptometry may serve to increase access to eye care or to augment in-person eye care, particularly when there are barriers to accessing eye care.
Acknowledgements
The authors would like to thank the content expert who externally reviewed this document and who has granted permission to be cited.
Nadine M. Furtado, OD MSc FAAO
Associate Clinical Professor
University of Waterloo, School of Optometry and Vision Science
References
1.Canadian Association of Optometrists. Importance of Eye Health and Vision Care to Healthy Aging. 2019. Accessed September 9, 2025. https://opto.ca/sites/default/files/resources/documents/Importance%20of%20Eye%20Health%20and%20Vision%20Care%20to%20Healthy%20Aging%20EN.pdf
2.Kahiel Z, Aubin MJ, Buhrmann R, Kergoat MJ, Freeman EE. Incidence of visual impairment in Canada: the Canadian Longitudinal Study on Aging. Can J Ophthalmol. 2022;57(1):2-7. doi: 10.1016/j.jcjo.2021.01.020 PubMed
3.Canadian Association of Optometrists. The Eye Exam. 2023. Accessed August 19, 2025. https://opto.ca/eye-health-library/eye-exam
4.Canadian Association of Optometrists. Eye Exam vs Sight Test. 2023. Accessed August 19, 2025. https://opto.ca/eye-health-library/eye-exam-vs-sight-test
5.Canadian Ophthalmological Society evidence-based clinical practice guidelines for the periodic eye examination in adults in Canada. Can J Ophthalmol. 2007;42(1):39-45, 158-63. doi: 10.1139/i06-126e PubMed
6.Centers for Disease Control and Prevention. Why Eye Exams Are Important. 2024. Accessed September 9, 2025. https://www.cdc.gov/vision-health/about-eye-disorders/why-eye-exams-are-important.html
7.Huang KZY, Trope GE, Buys YM, Jin Y. Unequal access to routine eye exams in Canada: an analysis of government-funded eye exam coverage policy and associated vision health outcomes. Can J Ophthalmol. 2025;60(2):E297-E299. doi: 10.1016/j.jcjo.2024.11.008 PubMed
8.Government of Canada. Non-Insured Health Benefits program for First Nations and Inuit: Vision Care Benefits Guide. 2025. Accessed September 9, 2025. https://www.sac-isc.gc.ca/eng/1579545788749/1579545817396
9.Government of Canada. Eligibility for Health Care Programs - Canada Service Veteran. 2024. Accessed September 9, 2025. https://www.veterans.gc.ca/en/about-vac/reports-policies-and-legislation/policies/eligibility-health-care-programs-canada-service-veteran
10.Department of Justice Canada. National Strategy for Eye Care Act. 2025. Accessed August 19, 2025. https://lois.justice.gc.ca/eng/acts/n-16.77/page-1.html
11.Canadian Association of Optometrists. Optometry in Canada. 2025. Accessed August 19, 2025. https://opto.ca/sites/default/files/2025-01/CAO_Optometry_In_Canada_Report_2025..pdf
12.Woo S, Hanssens J-M, Warren A, Blais N. Canadian Optometry Schools Tele-Optometry Collaboration [letter to the editor]. Can J Optometry. 2023;85(3):7-8. Accessed June 17, 2025. https://openjournals.uwaterloo.ca/index.php/cjo/article/download/5415/5715/25072
13.Federation of Optometric Regulatory Authorities of Canada. FORAC-FAROC Policy on Teleoptometry. 2020. Accessed August 19, 2025. https://www.forac-faroc.ca/wp-content/uploads/2020/09/FORAC-FAROC-POLICY-ON-TELEOPTOMETRY-SEPT-2020.pdf
14.Blais N, Warren A, Woo S, Hanssens J-M. Comprehensive Teleoptometry Exams in Canada: A Proposed Clinical Framework. Can J Optometry. 2024;86(3):7-26. doi: 10.15353/cjo.v86i3.5576
15.Balas M, Micieli JA, Wong JCY. Integrating AI with tele-ophthalmology in Canada: a review. Can J Ophthalmol. 2025;60(3):e337-e343. doi: 10.1016/j.jcjo.2024.08.013 PubMed
16.Canadian Association of Optometrists. Teleoptometry and Artificial Intelligence: Opportunities and Challenges for the Profession. A Discussion Paper for OLF 2023. 2023. Accessed June 17, 2025. https://opto.ca/sites/default/files/resources/documents/OLF%202023%20Discussion%20Paper.pdf
17.Canadian Association of Optometrists. Position Statement: The use of Teleoptometry in post-COVID practice. 2021. Accessed June 17, 2025. https://opto.ca/document/use-teleoptometry-post-covid-practice
18.Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. doi: 10.1136/bmj.j4008 PubMed
19.Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377-384. doi: 10.1136/jech.52.6.377 PubMed
20.Whiting PF, Rutjes AW, Westwood ME, et al. QUADAS-2: a revised tool for the quality assessment of diagnostic accuracy studies. Ann Intern Med. 2011;155(8):529-536. doi: 10.7326/0003-4819-155-8-201110180-00009 PubMed
21.Agree Next Steps C. The AGREE II Instrument. AGREE Enterprise; 2017. Accessed January 1, 1800. https://www.agreetrust.org/wp-content/uploads/2017/12/AGREE-II-Users-Manual-and-23-item-Instrument-2009-Update-2017.pdf
22.Chou R SS, Blazina I, Bougatsos C, Jungbauer R, Fu R, Grusing S, Jonas D, Tehrani S. Screening for Glaucoma in Adults: A Systematic Review for the U.S. Preventive Services Task Force. Evidence Synthesis No. 214. Agency for Healthcare Research and Quality;; 2022. Accessed August 18, 2025. https://www.ncbi.nlm.nih.gov/books/NBK581087/
23.Joseph S, Rajendran VK, Khetwani D, et al. Evaluation of a telemedicine-enabled universal eye health delivery model in rural southern India. Eye. 2024;38(6):1202-1207. doi: 10.1038/s41433-023-02871-8 PubMed
24.Mulchandani D, Reiser BJ, Ho TC, et al. Evaluation of digital slit-lamp videos for paediatric anterior segment telemedicine consultations. J Telemed Telecare. 2023;29(6):467-473. doi: 10.1177/1357633x21990991 PubMed
25.Wong JK, Zhu MM, Lam JC, et al. Prospective Comparative Study Investigating Agreement between Tele-Ophthalmology and Face-to-face Consultations in Patients Presenting with Chronic Visual Loss. Ophthalmol Ther. 2022;11(3):1199-1213. doi: 10.1007/s40123-022-00506-x PubMed
26.Barequet D, Gutfreund S, Goldstein M, Loewenstein A, Gamzu R, Varssano D. Evaluation of a Telemedicine Model for Following Keratoconus Patients in the Era of COVID-19 Pandemic. Telemed J E Health. 2022;28(7):1023-1027. doi: 10.1089/tmj.2021.0178 PubMed
27.Sabri K, Moinul P, Tehrani N, Wiggins R, Fleming N, Farrokhyar F. Video interpretation and diagnosis of pediatric amblyopia and eye disease. J Telemed Telecare. 2021;27(2):116-122. doi: 10.1177/1357633x19864823 PubMed
28.Keshvardoost S, Bahaadinibeigy K, Shadman H, Tafreshi AG, Baneshi MR. Design, Development, and Evaluation of a Teleophthalmology System Using a Low-Cost Fundus Camera. Acta inform. 2020;28(1):12-17. doi: 10.5455/aim.2019.28.12-17 PubMed
29.Maa AY, Medert CM, Lu X, et al. Diagnostic Accuracy of Technology-based Eye Care Services: The Technology-based Eye Care Services Compare Trial Part I. Ophthalmology. 2020;127(1):38-44. doi: 10.1016/j.ophtha.2019.07.026 PubMed
30.Nanji K, Kherani IN, Damji KF, Nyenze M, Kiage D, Tennant MT. The Muranga Teleophthalmology Study: A Comparison of Virtual (Teleretina) Assessment with in-person Clinical Examination to Diagnose Diabetic Retinopathy and Age-related Macular Degeneration in Kenya. Middle East Afr J Ophthalmol. 2020;27(2):91-99. doi: 10.4103/meajo.MEAJO_144_19 PubMed
31.Stewart C, Coffey-Sandoval J, Reid MW, Ho TC, Lee TC, Nallasamy S. Reliability of telemedicine for real-time paediatric ophthalmology consultations. Br J Ophthalmol. 2022;106(8):1157-1163. doi: 10.1136/bjophthalmol-2020-318385 PubMed
32.Blais N, Tousignant B, Hanssens JM. Comprehensive Primary Eye Care: A Comparison Between an In-Person Eye Exam and a Tele-Eye Care Exam. Clin Optom (Auckl). 2024;16:17-30. doi: 10.2147/opto.S436659 PubMed
33.American Telemedicine Association. Practice Guidelines for Ocular Telehealth-Diabetic Retinopathy, Third Edition. Telemed J E Health. 2020;26(4):495-543. doi: 10.1089/tmj.2020.0006
34.American Optometric Association. Care of the Patient with Primary Open-Angle Glaucoma. 2024. Accessed August 8, 2025. https://www.aoa.org/AOA/Documents/Practice%20Management/Clinical%20Guidelines/EBO%20Guidelines/2024_FINAL%20EBO_Glaucoma_Guideline_digital_10_28_24.pdf
35.Page MJ, Moher D, Bossuyt PM, et al. PRISMA 2020 explanation and elaboration: updated guidance and exemplars for reporting systematic reviews. BMJ. 2021;372:n160. doi: 10.1136/bmj.n160 PubMed
36.Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. doi: 10.1136/bmj.n71 PubMed
37.O'Neill J, Tabish H, Welch V, et al. Applying an equity lens to interventions: using PROGRESS ensures consideration of socially stratifying factors to illuminate inequities in health. J Clin Epidemiol. 2014;67(1):56-64. doi: 10.1016/j.jclinepi.2013.08.005 PubMed
38.Canadian Association of Optometrists. Screening, Diagnosis, and Management of Open Angle Glaucoma:An Evidence-Based Guideline for Canadian Optometrists. 2017. Accessed December 8, 2025. https://openjournals.uwaterloo.ca/index.php/cjo/issue/view/227/CJO_v79_MacIverMacDonaldProkopich_Eng
39.A randomized, placebo-controlled, clinical trial of high-dose supplementation with vitamins C and E, beta carotene, and zinc for age-related macular degeneration and vision loss: AREDS report no. 8. Arch Ophthalmol. 2001;119(10):1417-36. doi: 10.1001/archopht.119.10.1417 PubMed
40.Canada's Drug Agency. Canada's Drug Agency style: A guide for Author's and Editor's. 2025. Accessed September 8, 2025. https://www.cda-amc.ca/sites/default/files/pdf/style_guide_2025_digital.pdf
Appendix 1: Detailed Methods and Selection of Included Studies
Please note that this appendix has not been copy-edited.
What Is a Rapid Review?
Rapid reviews are based on accelerated and abbreviated SR methods, balancing timeliness with rigour, to allow for timely decision-making. Due to these abbreviated methods, rapid reviews have some limitations. For example, we included studies published from 2020, excluding older studies. We attempted to mitigate this by searching for and including relevant SRs published in the past 5 years that included older studies. Focusing on more recently published articles may also be more reflective of current practices given the increased use and acceptance of virtual care since the onset of the COVID-19 pandemic. Of note, CDA-AMC Rapid Reviews summarize and critically appraise the available evidence on a topic, but do not provide formal recommendations.
Literature Search Methods
An information specialist conducted a literature search on key resources including MEDLINE, the Cochrane Database of Systematic Reviews, the International HTA Database, the websites of health technology assessment agencies in Canada and major international HTA agencies, as well as a focused internet search. The search approach was customized to retrieve a limited set of results, balancing comprehensiveness with relevance. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. Search concepts were developed based on the elements of the research questions and selection criteria. The main search concept was teleoptometry. The search was completed on August 5, 2025, and limited to English-language documents published since January 1, 2020. The search strategy is available on request.
Selection Criteria and Methods
Two reviewers were involved in screening citations and the selection of studies, and study screening and selection was divided between reviewers. In the first level of screening, titles and abstracts were reviewed by a single reviewer and potentially relevant articles were retrieved and assessed for inclusion. Full texts of titles and abstracts that were judged to be relevant by a single reviewer were included in the review. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, were duplicate publications, were published before 2020, or were guidelines with unclear methodology. We also excluded studies if the teleoptometry modality was not approved for use in health care settings and/or not administered by a health care provider (e.g., web or app-based tests; photos taken on a smartphone), or if it was administered exclusively via telephone or videocall (e.g., call to patient at their home). To meet the needs of the customer and the scope of their request (i.e., the general use of teleoptometry for the provision of vision and eye health services), teleoptometry that relied on the use of specialized ophthalmic investigations (such as optical coherence tomography) was also excluded.
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the following tools as a guide: A MeaSurement Tool to Assess systematic Reviews 2 (AMSTAR 2)18 for SRs, the Downs and Black checklist19 for randomized and nonrandomized studies, the Quality Assessment of Diagnostic Accuracy Studies 2 (QUADAS-2) checklist20 for diagnostic test accuracy studies, and the Appraisal of Guidelines for Research and Evaluation (AGREE) II instrument21 for guidelines. Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Data Extraction and Reporting
One reviewer extracted data directly into standardized tables created in Microsoft Word, which were modified as necessary. The extracted information included study characteristics, methodology (e.g., study design), population, intervention, comparator, and results regarding the outcomes of interest.
The PROGRESS-Plus37 framework guided equity considerations and includes place of residence, race (or ethnicity, culture), occupation, gender or sex, religion, education, SES, and social capital. These characteristics were extracted and are discussed across the evidence, where available.
When reporting on sex, gender, race, or ethnicity in this Rapid Review, we retained the language used by the original study authors, and, whenever possible, we referred to these groups based on guidance from the CDA-AMC Style Guide40 at the time this Rapid Review was conducted, with an understanding that language is constantly evolving.
For diagnostic test accuracy studies, when interpreting the results for sensitivity, specificity, positive predictive value and negative predictive we used the following cut-offs: 90% to 100% (high), 80% to 89% (good), 70% to 79% (moderate), 60% to 69% (low) and below 60% (very low).
External Review
The final report was externally reviewed by a content expert with expertise in optometry, including remote delivery of ocular health care.
Appendix 2: Selection of Included Studies
Please note that this appendix has not been copy-edited.
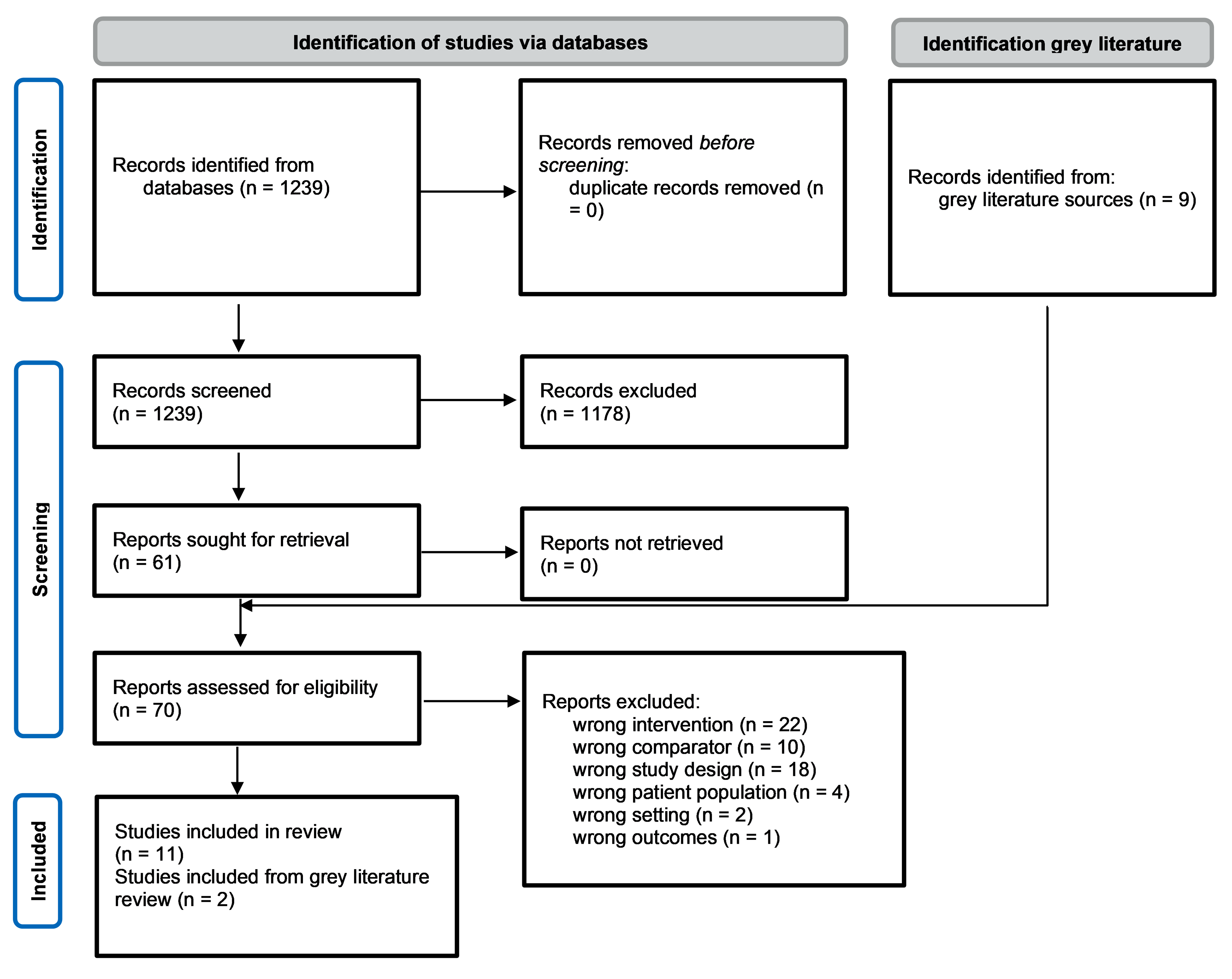
Appendix 3: Characteristics of Included Publications
Please note that this appendix has not been copy-edited.
Table 2: Characteristics of Included Systematic Review
Study citation, countries of eligible studies, funding source | Study designs and numbers of primary studies included | Population characteristics | Intervention and comparator(s) | Outcomes |
|---|---|---|---|---|
Chou et al. (2022)22 Countries of included studies eligible for the current review: US Funding source: not reported | Systematic review with 7 research questions on screening and treatment for glaucoma. Relevant to this review: population based cohort studies and cross-sectional diagnostic test accuracy studies Number of included studies relevant to this review: 1 pilot study (fair quality) and 1 cross-sectional study (good quality). The cross-sectional study29 was also identified in the search for this review, and includes additional outcomes, thus the data will be extracted from the primary study instead. | Eligibility: adults 40 years or older with open-angle glaucoma or glaucoma suspect Pilot study: N = 52 Age = NR Other PROGRESS-Plus criteria: NRa | Eligible Interventions: any diagnostic tests that are currently used to screen for glaucoma Relevant intervention: Asynchronous teleoptometry (IOP, central corneal thickness, visual acuity, patient history) Comparator: reference standard for open-angle glaucoma (as defined in the studies) Relevant comparator: in-person eye exam with ophthalmologist including IOP, autorefraction, visual acuity, pupil reactivity, chamber depth, afferent papillary defect, fundus photographs | Sensitivity and specificity for glaucoma |
IOP = intraocular pressure; NR = not reported.
aThe main PROGRESS-Plus criteria include place of residence, race, ethnicity, culture, language, occupation, gender, sex, religion, education, socioeconomic status, social capital, personal characteristics associated with discrimination (e.g., age, disability), features of relationships, and time-dependent relationships.37
Table 3: Characteristics of Included Primary Clinical Studies
Study citation, country, funding source | Study design | Population characteristics | Intervention and comparator(s) | Clinical outcomes |
|---|---|---|---|---|
Blais et al. (2024)32 Canada Funding source: Mitacs Accelerate Program | Cross-sectional (repeated measures) study Each patient had 2 successive comprehensive eye exams, in random order, at the School of Optometry at the University of Montreal. Best corrected visual acuity results from both exams were put into trial frames and visual comfort was compared between modalities in a random order, where neither the patient nor the assessor was aware of which prescription was put into the trial frames. | 66 eye care naive adults. People with acute ocular conditions or diseases and visual deficiency were excluded. Age (years), mean (SD): 29.7 (10.6) Range of refractive error (diopters): –8.78 to + 2.63 Other PROGRESS-Plus criteria: NRa | All patients had pretesting with automated instruments by an optometric assistant (i.e., lensometry, autorefraction, keratometry, noncontact tonometry, pachymetry, perimetry, fundus photography and optical coherence tomography of macula and optic nerve); results were sent to electronic medical record. Intervention: hybrid teleoptometry exam (includes both synchronous and asynchronous exams) performed by a remote optometrist (located in a different room at the same clinic) assisted by an in-clinic technician (a final year optometry student). Some tests were delegated to the technician (i.e., case history, visual acuity, colour vision, sensorial function, stereoscopic acuity, near point of convergence). Some tests were filmed by the technician and uploaded them to a digital platform for asynchronous interpretation by the optometrist (i.e., cover test, extraocular motility, pupillary reflexes). The slit lamp test was filmed live (synchronous) by the technician. Finally, the remote optometrist performed subjective refraction using the digital phoropter, and tested for heterophoria and fusional amplitudes. (synchronous exam). Comparator: In-person comprehensive eye exam performed by an optometrist, which included the same tests as the teleoptometry exam, and also included nondilated fundoscopy, which can only be performed in person. |
|
Stewart et al. (2022)31 US Funding source: Margie & Robert E. Petersen Foundation | Prospective, cross-sectional, noninferiority study. Patients recruited between February 2016 and April 2018 at a single vision centre where they had been referred for further assessment or surgical consultation. | Eligibility: Children younger than 18 years, who were able to participate in an age-appropriate manner. 210 patients Age (years), median (range): 6 (0 to 17) Sex: 44% male, 56% female Race, n (%) American Indian or Alaska Native: 4 (2) Asian: 13 (6) Black or African American: 20 (10) Native Hawaiian or other Pacific Islander: 0 (0) white: 166 (79) mixed or other: 7 (3) Ethnicity, n (%) Hispanic or Latino: 163 (78) Not Hispanic or Latino: 47 (22) Primary language, n (%) English: 94 (45) Spanish: 106 (50) Other: 7 (3) Other PROGRESS-Plus criteria: NRa | Intervention: Synchronous teleoptometry. A pediatric optometrist conducted an eye exam that was viewed (live stream via Pivothead glasses and a videoconferencing system) by a pediatric ophthalmologist. The exam included history, vision testing, stereoacuity, IOP, and the eye exam using a Topcon digital slit lamp with camera attachment and a digital indirect ophthalmoscope. The optometrist directed the ophthalmologist to areas of interest, while the latter viewed and guided the exam. Patients were not dilated unless clinically necessary. Comparator: In-person eye exam by the same pediatric ophthalmologist later on the same day (not further described). | Agreement in diagnosis and management plans for all patients. In patients with strabismus, agreement in angle measurement and disease category. |
NR = not reported.
aThe main PROGRESS-Plus criteria include place of residence, race, ethnicity, culture, language, occupation, gender, sex, religion, education, socioeconomic status, social capital, personal characteristics associated with discrimination (e.g., age, disability), features of relationships, and time-dependent relationships.37
Table 4: Characteristics of Included Diagnostic Test Accuracy Studies
Study citation, country, funding source | Study design, target condition(s) | Population characteristics | Index test(s) and reference standards | Outcomes |
|---|---|---|---|---|
Children | ||||
Mulchandani et al. (2023)24 US Funding source: Margie & Robert E. Peterson Foundation | Prospective, cross-sectional study September 2013 to August 2018 at a vision centre in a children’s hospital. 1 pediatric ophthalmologist conducted all in-person exams. A second pediatric ophthalmologist viewed the live stream videos, and then re-examined the videos at least 3 months later. Target conditions: anterior segment pathologies (pediatric) | Eligibility: Children aged 4 to 17 years, with previously diagnosed ocular anterior segment disease and able to participate in the slit lamp exam. 45 children (89 eyes) Age (years), median (range): 12 (5 to 17) Sex: 55% male and 45% female Other PROGRESS-Plus criteria: NRa | Index test: Teleoptometry review of the live video of the in-person exam either live streamed (synchronous) or recorded (asynchronous). During the live stream, there was limited communication between the remote and in-person examiner (e.g., prompting to record features again), but no history of symptoms relayed. Reference Standard: Anterior segment exam by ophthalmologist using a Topcon SL-D4 digital slit lap with DC-4 camera attachment. Exam recorded using Polycom RealPresence Group 500 videoconferencing system, which could be streamed live or recorded for asynchronous review. | Sensitivity and specificity for detecting anterior segment pathologies of the eyelids/eyelashes, conjunctiva/sclera, cornea, anterior chamber, iris, and lens. |
Sabri et al. (2021)27 Canada Funding source: a Physician Service Incorporated grant | Prospective cross-sectional Recruited children attending the pediatric eye clinic at the McMaster children’s hospital between February 2015 and March 2016. 1 person conducted the in-person exam, and 2 different people conducted a teleoptometry exam, and results are compared and reported separately by examiner Target condition: ocular features potentially related to amblyopia | Eligibility: Children with suspected amblyopia 160 kids (320 eyes) Age (years), mean (SD): 4.8 (2.5) Sex: 48% male and 52% female Other PROGRESS-Plus criteria: NRa | Index test: Asynchronous teleoptometry review by a pediatric ophthalmologist of the video recording of the in-person exam. Reference Standard: In-person exam by a pediatric ophthalmologist, with assessment of upper lid function, presence of ptosis, pupillary function (relative afferent pupillary defect and anisocoria), ocular motility, strabismus (using a cover test in the primary position), nystagmus in primary position, torticollis and presence of facial asymmetry | Sensitivity and specificity for detecting abnormal findings for each measured ocular feature. |
Adults | ||||
Joseph et al. (2024)23 India Funding source: Aravind Eye Care System, India | Prospective, cross-sectional study. Recruited consecutive patients at a single, community-based rural vision centre in January and February 2020. Patients completed the teleoptometry exam first, immediately followed by the in-person exam. The in-person ophthalmologist was masked to the diagnosis and treatment advice from the teleoptometry exam. Target conditions: eye conditions, diabetic retinopathy, cataracts, glaucoma | Eligibility: People aged 16 years and older, who were new to the clinic. 339 patients (678 eyes) Age (years), mean (SD): 43.5 (16.1) Sex: 46.9% female and 53.1% male Diabetes: 13.0% Hypertension: 8.9% Other PROGRESS-Plus criteria: NRa | Index test: Hybrid teleoptometry exam. Vision technician completed the initial workup (asynchronous): patient history and complaints, visual acuity, refraction, and slit lamp examination. Patients ≥ 40 years also had blood pressure, IOP (via applanation tonometry), and capillary blood glucose level. Followed by an eye exam (with or without dilation, as needed). A teleconsultation with a remote ophthalmologist via videoconference, the patient, and the vision technician, followed the initial workup (synchronous). Reference Standard: In-person exam performed by an ophthalmologist. They reviewed the standard information collected by the vision technician (i.e., patient history, visual acuity, refraction, IOP), then conducted in-person exam. | Sensitivity, specificity, positive predictive value, and negative predictive value for common ocular diagnoses (i.e., any diabetic retinopathy, cataracts (immature and mature), glaucoma, nonserious eye injury, conjunctivitis) and treatment advice (i.e., the need for surgery, referral, spectacles, or medicine). Specific stages of ocular disease were not considered in the analysis. |
Barequet et al. (2022)26 Israel Funding source: None received. | Retrospective, cross-sectional study Consecutive patients between November 2017 and September 2020. At an outpatient clinic. The same clinician performed the in-person exam and the teleoptometry assessment, but at least 4 weeks elapsed between office and remote assessments. Target condition: keratoconus progression | Eligibility: Patients with keratoconus who were treated and followed in the keratoconus outpatient clinic, with at least 1 clinic visit, and had completed refraction and corneal topographies. Patients were excluded if they were newly diagnosed with keratoconus. 102 patients (204 eyes) Age (years), mean (range): 29 (10 to 53) Sex: 66% male (no other information reported) Other PROGRESS-Plus criteria: NRa | Index test: Asynchronous teleoptometry. Ophthalmologist review of the data obtained from the in-person exam. First, only using patient demographics and the topography test results. Next, the manifest refraction and the clinical findings were revealed. Reference Standard: In-person clinical exam, including BCVA and manifest refraction performed by an optometrist, and a full ophthalmic exam by a cornea surgeon, including corneal topography. | Sensitivity, specificity, positive predictive value, and negative predictive value for keratoconus progression. |
Wong et al. (2022)25 Hong Kong Funding source: Health and Medical Research Fund, Food and Health Bureau, Hong Kong SAR Government | Prospective, cross-sectional Consecutive patients were recruited between August 1, 2019, and July 31, 2021. All study components were completed within 1 day at a specialist ophthalmology clinic. Target condition: cataracts, glaucoma, AMD | Eligibility: adults without diabetes aged 40 years or older, who were referred to the eye clinic for blurring vision for 3 months or more 430 people (860 eyes) included in the analysis. Age (years), mean (SD): 67 (11) Sex: 57.6% male and 42.3% female Other PROGRESS-Plus criteria: NRa | Index test: Store-and-forward (asynchronous) teleoptometry exam by ophthalmologist. They reviewed photos (taken by an optometrist) of the anterior segment of the eye taken with a digital camera attached to a slit lamp bio-microscope (diffuse and oblique illumination views) and photos of the retina (optic disc and macula centric views) taken with mydriatic fundus camera. They also reviewed the visual acuity and IOP (from the in-person exam) and the patient’s referral letter from the family physician. Reference Standard: In-person exam with an ophthalmologist, including visual acuity with pinhole, medical history, slit lamp bio-microscopy, IOP via applanation tonometry, and a mydriatic retinal exam with indirect ophthalmoscope. | Sensitivity, specificity, positive predictive value, and negative predictive value for the diagnosis of cataracts (graded as early, moderate, and late), AMD (stage not reported), and glaucoma or glaucoma suspect. Stages of ocular diseases were not considered separately in the analysis. |
Keshvardoost et al. (2020)28 Iran Funding source: Kerman University of Medical Sciences | Cross-sectional study Recruitment not described. 2 months after the in-person exam, 2 retina specialists (including the 1 who conducted the in-person exam [i.e., examiner 1]) analyzed the digital images. Images that were poor quality were considered ‘uninterpretable’ and excluded from analysis. Target condition: diabetic retinopathy, macular edema | Eligibility: patients with diabetes who had been referred to the ophthalmology centre. People were excluded if they had: AMD, severe cataracts, vitreous hemorrhage, previous vitreoretinal surgery. 125 patients recruited but 8 excluded due to poor image quality. Analysis of 117 patients. Age (years), mean (SD): 56.7 (9.3) Sex: 67.5% female (no other information reported) Other PROGRESS-Plus criteria: NRa | Index test: Asynchronous teleoptometry review by a retina specialist of a digital image (by a postgraduate student of medical informatics) of the dilated pupils using a nonmydriatic Horus scope camera (1,920 by 1,080 pixel resolution) taken after the in-person exam. A single-field image centred on the macula and showing the optic nerve and superior and inferior vascular arcades. Imaging was repeated if quality was not acceptable. Reference Standard: Visual acuity with a Snell chart, then a dilated pupil exam by a retina specialist using a Topcon slit lamp and a Volk 90 diopter lens. | Sensitivity and specificity for diabetic retinopathy, clinically significant macular edema. Diabetic retinopathy was graded as any diabetic retinopathy (non proliferative, high-risk, and advanced proliferative) and diabetic retinopathy requiring referral (for proliferative, high-risk proliferative, and advanced proliferative diabetic retinopathy). |
Maa et al. (2020)29 US Funding source: Atlanta Clinical and Translational Institute | Cross-sectional study Patients recruited between March 2015 and December 2017; eligible people were informed of the study by mail, and patients self-volunteered to participate. 1 ophthalmologist performed in the in-person exam, and 2 ophthalmologists individually conducted the teleoptometry exam. Target conditions: cataracts, glaucoma, AMD, diabetic retinopathy, referrals | Eligibility: Veterans with no known ocular disease who had not had an eye exam for 2 or more years 256 patients Age (years), mean (SD): 60.0 (11.6) Sex: 86.7% male (no other information reported) Race, n (%): Asian: 1 (0.4) Black: 157 (61.3) white: 98 (38.3) Other PROGRESS-Plus criteria: NRa | Before either exam, a technology-based eye care services screening protocol by an optometric technician was initiated that included: ocular history, main complaint, autorefraction, manifest refraction, BCVA, measures of the pupils, IOP, central corneal thickness, and anterior chamber depth, and colour fundus photos with dilated pupils. Index test: Asynchronous teleoptometry exam. Remote ophthalmologist review of patient history, clinical data, and ocular photos from the screening protocol from a secure research database. Reference Standard: in-person comprehensive eye exam by an ophthalmologist. | Sensitivity and specificity for cataracts referred for surgery, glaucoma suspect or glaucoma, AMD (stage not reported), any diabetic retinopathy, or any diagnosis resulting in referral. Stages of ocular diseases were not considered separately in the analysis. |
Nanji et al. (2020)30 Authors from Canada, Kenya and India, study location Kenya Funding source: Aga Khan University Research council, and Pfizer Canada. SDI software provided at no cost by the directors of the company. | Cross-sectional study. All patients who attended the hospital based diabetic clinic between August and October 2011 were included in the study. Blurry fundus photos were excluded from the study. Target conditions: diabetic retinopathy, AMD | Eligibility: Adults 30 or older with diabetes. Excluded people with ocular anatomy that inhibits adequate fundus photography, or with physical features that inhibited proper positioning for fundus photography. 314 patients (628 eyes). All patients completed in-person exam, and 8 did not complete the teleoptometry exam. 12% of fundus photos were unusable. Age (years), mean (SD): 62 (11.6) Gender, n (%): Male: 124 (39.4) Female: 187 (59.5) Missing information: 3 (0.95) Years since diabetes diagnosis, median: 5 Other PROGRESS-Plus criteria: NRa | Before either exam, an ophthalmic assistant conducted an ocular assessment that included ocular history, visual acuity, external ocular exam with a penlight, IOP with a Tonopen, visual field screening (with frequency doubling technology), and fundus photography (stereo images with dilated pupils). This information was uploaded into a secure patient data website by SDI at the University of Alberta. Index test: Asynchronous teleoptometry exam. Remote ophthalmologist reviews the history form, the examination form, the results of the visual field testing, and the colour fundus photographs. Reference Standard: In-person ophthalmologist reviews the history form, examination form, and the results of the visual field testing. Then they performed a dilated fundus (slit lamp) exam using a 90 diopter lens to examine the optic nerve and macula. | Sensitivity, specificity, positive predictive value, negative predictive value for diabetic retinopathy and AMD. Specific stages of ocular disease were not determined. |
AMD = age-related macular degeneration; BCVA = best corrected visual acuity; IOP = intraocular pressure.
aThe main PROGRESS-Plus criteria include place of residence, race, ethnicity, culture, language, occupation, gender, sex, religion, education, socioeconomic status, social capital, personal characteristics associated with discrimination (e.g., age, disability), features of relationships, and time-dependent relationships.37
Table 5: Characteristics of Included Guidelines for Teleoptometry for Eye Diseases
Intended users, target population | Intervention and practice considered | Major outcomes considered | Evidence collection, synthesis, and quality assessment | Recommendations development and evaluation | Guideline validation |
|---|---|---|---|---|---|
AOA Evidence-based Optometry Guideline Development Group (2024)34 | |||||
Intended users: Doctors of optometry Target population: Patients with primary open-angle glaucoma | Evidence-based clinical practice guidelines on the examination, treatment, and management of the target population. Screening and examination strategies, such as medical treatment, laser therapy, surgical treatment, self- or home-based monitoring, and telehealth. | Potential benefits and harms of relevant interventions (e.g., number of monitoring visits, side effects, reduce or delay onset of disease, access to care). | A systematic search was conducted in multiple electronic databases for English-only studies published between 2009 and 2023. The results of the relevant studies were summarized qualitatively. The quality of the evidence and clinical recommendations from each study were graded using predetermined grading criteria. | The Evidence-based Optometry Guideline Development Group developed recommendations informed by the systematic review. If scientific evidence to support a recommendation was lacking, a consensus process was completed to approve a recommendation. They graded the strength of the recommendation by assessing the quality of the research and benefits and risks of the procedure or therapy recommended. The strength of the recommendation was evaluated by predetermined grading criteria. The grades were A, B, C, and D based on the quality of the study and the type of study design. | The Evidence-based Optometry Guideline Development Group internally reviewed the first draft. Additional reviews were completed as necessary after revision by the writer and medical editor. The peer-reviewed draft was sent to the AOA Board of Trustees for approval to post for peer and public review on the AOA website. Final draft was reviewed by the AOA Board of Trustees and AOA Legal Counsel and was then guidelines were then posted to the AOA website for public use. |
ATA Diabetic Retinopathy Telehealth Practice Guidelines Working Group (2020)33 | |||||
Intended Users: Practitioners, group and specialty practices, hospitals and health care systems, and other providers of health-related services where telehealth interactions take place Target Population: Patients receiving ocular telehealth for diabetic retinopathy | Evidence-based clinical practice guidelines for designing, implementing, and operating an ocular telehealth diabetic retinopathy program. | Clinical, technical, and administrative issues. | “A rigorous review” was conducted (not further described). The quality of the evidence was reported to be assessed to inform the level of adherence given to each recommendation, but details on how it was assessed were not further described. | The Diabetic Retinopathy Telehealth Practice Guidelines Working Group developed recommendations informed by “evidence, professional consensus, and a rigorous review, including open public commentary period.” Based on the quality and quantity of peer-reviewed evidence, the guidelines were classified into 4 levels of adherence (shall, shall not, should, and may)a The assessment of the strength of the recommendation was not discussed. | The guideline validation process was not discussed. |
AOA = American Optometric Association; ATA = American Telemedicine Association; NR = not reported.
aThe guidelines by ATA Diabetic Retinopathy Telehealth Practice Guidelines Working Group provided a level of adherence for each recommendation “based on the quality and quantity of peer-reviewed evidence.” “Shall” indicates required action whenever feasible and/or practical. “Shall not” indicates a proscription or action that is strongly advised against. “Should” indicates a recommended action without excluding others. “May” indicates pertinent actions that may be considered to optimize the telemedicine encounter or operational process.
Appendix 4: Critical Appraisal of Included Publications
Please note that this appendix has not been copy-edited.
Table 6: Clinical Effectiveness of Teleoptometry for Genera Eye Exams: Strengths and Limitations of Clinical Study Using the Downs and Black Checklist19
Strengths | Limitations |
|---|---|
Blais et al. (2024)32 | |
The aim of the study and the interventions were well described. Simple outcome data are provided for most outcomes. Estimates of random variability (i.e., SD, CI) were reported for vision quality, visual comfort, and patient and provider outcomes. Actual P values were reported for comparative outcomes (i.e., visual comfort with prescription, patient satisfaction, and optometrist confidence level). Where possible given the study design, the patients and providers were masked to the intervention (i.e., the trial frames with the new prescription). All patients received the teleoptometry and the in-person eye exam. Study was conducted in Canada, and the tests and equipment are representative of what would be used in practice. The teleoptometry exam and the in-person exam were conducted and interpreted by different optometrists. Both eye exams were done on the same day, thus no chance of any changes in condition between tests. The authors declared that they had no conflicts of interest. The source of funding was reported and the authors declared that the funders had no influence on the conduct of the study. | Patients are described with limited detail (i.e., only age is provided, and no other details provided). Estimates of random variability (e.g., CI) were not provided for the level of agreement for the visual function and ocular health assessment (i.e., the variation around the point estimate is unclear), thus the level of confidence around the point estimate is unclear. Patients were recruited through social media, which may not be representative of the population that would be most likely to use teleoptometry. The study took place at the School of Optometry in Montreal, Canada, which is not representative of the setting where the majority of patients would receive teleoptometry exams (i.e., in rural or remote locations). As this wasn’t a remote location, there were not concerns about internet connection or bandwidth. Neither exam included a dilated fundus exam, which is considered best practice for comprehensive eye exams (but not possible to perform remotely). The reporting of some of the outcomes was unclear. For ocular health assessments, P values comparing the absolute outcomes were reported but the authors did not report the absolute outcomes for each group (only the level of agreement was reported). Unclear if study was limited by the sample size (i.e., 66 people). Excluded patients with low vision for whom it may be more difficult to assess their vision quality, and it is unclear whether this could have biased the results in favour of teleoptometry. The optometric assistant for the teleoptometry component was a third-year optometry student, which may not be representative of how teleoptometry is implemented in practice, as the optometry student may be more qualified than most optometric assistants. Patient privacy and data security for teleoptometry was not reported. |
CI = confidence interval; SD = standard deviation.
Table 7: Diagnostic Test Accuracy of Teleoptometry for Eye Diseases and Conditions: Strengths and Limitations of Systematic Reviews Using AMSTAR 218
Strengths | Limitations |
|---|---|
Chou et al. (2022)22 | |
The population, intervention, comparators, and outcomes of interest were clearly stated. The authors used a comprehensive search strategy. Study selection, data extraction, and quality assessments were performed in duplicate. A list of excluded studies and the reasons for exclusion were provided. The included studies are critically appraised using criteria that assesses the key domains for diagnostic accuracy studies. The authors declare that none of the investigators had any affiliations or financial involvement that conflicts with topic of the systematic review. | It was unclear if the methods were established before the conduct of the review. The included studies are described with limited detail (e.g., missing some information on the study design, interventions, population). The authors did not report the sources of funding for the included studies. Patient privacy and data security for teleoptometry was not reported. |
AMSTAR 2 = A MeaSurement Tool to Assess systematic Reviews 2.
Table 8: Diagnostic Test Accuracy of Teleoptometry for Eye Diseases and Conditions: Strengths and Limitations of Diagnostic Test Accuracy Studies Using the QUADAS-2 Checklist20
Strengths | Limitations |
|---|---|
Joseph et al. (2024)23 | |
Participants were recruited using a consecutive sample of all new patients at the clinic. Low risk that the selection of patients would have introduced bias. The study population, the index test, and the reference standard match those targeted by the review question. The index test and the reference standard were completed on the same day. The index test was interpreted without knowledge of the reference standard. Reference standard results were interpreted without knowledge of the index test. All patients received the same reference standard. All patients were included in the analysis. Estimates of random variability (i.e., CI) were reported alongside the findings. The authors reported the source of the funding. Teleoptometry exam took place at a rural vision centre with an in-person vision technician and video conferencing with the remote ophthalmologist, which is representative of the setting and setup for teleoptometry in Canada (e.g., at rural or remote locations) | Patient characteristics are described with limited detail. The authors reported on age and sex, but no other PROGRESS-plusa criteria were reported. There was a low prevalence of people with certain eye conditions in this sample (e.g., diabetic retinopathy, glaucoma), which may have contributed to imprecision for estimates of sensitivity (e.g., wide CIs around estimates). The vision technician who conducted the clinical data (e.g., patient history, visual acuity, refraction, intraocular pressure) for both the teleoptometry exam and the in-person exam received more training than is standard for optometric assistants in Canada, which may limit the generalizability of the findings to Canada. Patient privacy and data security for teleoptometry was not reported. |
Mulchandani et al. (2023)24 | |
The reference standard matches that targeted by the review question. The index test was interpreted without knowledge of the reference standard. Reference standard results were interpreted without knowledge of the index test. All patients received the same reference standard. All patients were included in the analysis. The index test and reference standard were completed using information collected on the same day. Estimates of random variability (i.e., CI) were reported alongside the findings. The source of funding was reported and the authors declared that the funders had no influence on the conduct of the study. Patient privacy and data security were taken into consideration as authors specified that video transmission was shared securely to a remote examiner by using an encrypted Polycom-to-Polycom video call. | Patient recruitment was unclear. All patients had previously been diagnosed with anterior segment disease (the target condition), which may have biased the results toward improved performance of the index test. Patients are described with limited detail. The authors reported on age and sex, but no other PROGRESS-plusa criteria were reported. The index test differs from that of the review question in that the teleoptometry component involved the synchronous or asynchronous review of a video of the in-person exam (conducted by an ophthalmologist), rather than an independent exam with support from an optometric assistant. This may not reflect how teleoptometry is used in practice in Canada. The teleoptometry component also took place at a children’s hospital, which is not representative of the setting where most patients would receive teleoptometry exams (i.e., in rural or remote locations), thus it wasn’t subject to the potential concerns that would exist in practice (e.g., internet connection or bandwidth). |
Barequet et al. (2022)26 | |
Patients were recruited using a consecutive sample. Low risk that the selection of patients would have introduced bias. The study population and reference standard match those targeted by the review question. The index test and reference standard were completed using information collected on the same day. Reference standard results were interpreted without knowledge of the index test. All patients received the same reference standard. All patients were included in the analysis. Estimates of random variability (i.e., CI) were reported alongside the findings. The authors reported that no funding was received for the work. | Patients are described with limited detail. The authors reported on age and male sex, but no other PROGRESS-plusa criteria were reported. It is unclear if the index test was interpreted without knowledge of the results of the reference standard, as the same ophthalmologist conducted both exams at least 4 weeks apart, and the teleoptometry consisted solely of the asynchronous review of the data obtained from the in-person exam. It is unknown if the ophthalmologist would have remembered the results of the previous test. The index test differs from that of the review question in that the teleoptometry component involved the same ophthalmologist reviewing the data obtained from the in-person exam, rather than an independent exam with support from an optometric assistant. This may not reflect how teleoptometry is used in practice in Canada. The setting for the teleoptometry component was unclear, but the asynchronous review of the clinical data suggests that it may not have been subject to the potential concerns that would exist in practice (e.g., internet connection or bandwidth in rural or remote settings). Patient privacy and data security for teleoptometry was not reported. |
Wong et al. (2022)25 | |
Patients were recruited using a consecutive sample. Low risk that the selection of patients would have introduced bias. The study population, the index test, and the reference standard match those targeted by the review question. The index test was interpreted without knowledge of the reference standard. Reference standard results were interpreted without knowledge of the index test. All patients received the same reference standard. The index test and reference standard were completed within 1 day. The source of funding was reported and the authors declared that the funders had no influence on the conduct of the study. | Not all patients were included in the analysis, as 15 people were excluded due to the poor quality of the retina photographs. While this was prespecified as part of the exclusion criteria, it may bias the study toward improved findings for teleoptometry, and may be less reflective of its use in practice. Patients are described with limited detail. The authors reported on age and sex, but no other PROGRESS-plusa criteria were reported. The study population had a higher than expected prevalence of cataracts, glaucoma, and age-related macular degeneration, but it is unclear whether this may have contributed to imprecision for estimates of sensitivity and specificity as the authors did not report CIs around the estimates. While a store-and-forward model was used for the teleoptometry exam (with images and clinical data transmitted over the internet), the ophthalmologist was located in a different room in the same clinic, thus it wasn’t subject to the potential concerns that would exist in practice (e.g., internet connection or bandwidth in a rural or remote setting). Patient privacy and data security for teleoptometry was not reported. |
Sabri et al. (2021)27 | |
The study population and the reference standard match those targeted by the review question. The index test and reference standard were completed using information collected on the same day. Reference standard results were interpreted without knowledge of the index test. All patients received the same reference standard. All patients were included in the analysis. Estimates of random variability (i.e., CI) were reported alongside the findings. The authors reported the source of the funding. Patient privacy and data security were considered by authors as video recordings were encrypted and uploaded securely onto a password protected server. | Patient recruitment was unclear. Patients are described with limited detail. The authors reported on age and sex, but no other PROGRESS-plusa criteria were reported. Unclear whether the results of the index test were interpreted without knowledge of the reference standard. The index test differs from that of the review question in that the teleoptometry component involved the asynchronous review of a video of the in-person exam (conducted by an ophthalmologist), rather than an independent exam with support from an optometric assistant. This may not reflect how teleoptometry is used in practice in Canada. The authors reported that the quality of the video recordings was affected by factors such as lighting, focus, and angle of the camera which may have affected the interpretation of the video by the remote examiners. The teleoptometry component also took place at a children’s hospital, which is not representative of the setting where most patients would receive teleoptometry exams (i.e., in rural or remote locations), thus it wasn’t subject to the potential concerns that would exist in practice (e.g., internet connection or bandwidth). There was a low prevalence of positive cases for most of the conditions, which may have contributed to imprecision for estimates of sensitivity (e.g., wide CIs around estimates). There were 2 different remote examiners, and the findings differed between examiners. The authors suggested that the technology skills of the remote examiners may have influenced the results. |
Keshvardoost et al. (2020)28 | |
The study population and the reference standard match those targeted by the review question. The index test and reference standard were completed using information collected on the same day. Reference standard results were interpreted without knowledge of the index test. All patients received the same reference standard. The authors reported the source of the funding. | Patient recruitment was unclear. Patients are described with limited detail. The authors reported on age and female sex, but no other PROGRESS-plusa criteria were reported. It was not reported whether the index test was interpreted without the knowledge of the results of the reference standard. This study reported the results of the index test from 2 retina specialists, 1 of whom had conducted the in-person exam 2 months prior, and it is unknown whether they would have remembered the results of the previous test. The index test differs from that of the review question in that the teleoptometry component involved only the asynchronous review of a digital image of the dilated pupils (taken by a postgraduate student of medical informatics), with no additional clinical data provided, rather than an independent exam with support from an optometric assistant. This may not reflect how teleoptometry is used in practice in Canada. Not all patients were included in the analysis, as 8 people were excluded due to the poor quality. While this was prespecified as part of the methods, it may bias the study toward improved findings for teleoptometry, and may be less reflective of its use in practice. Estimates of random variability (e.g., CI) were not reported for any of the findings, and specificity was not reported alongside sensitivity for all outcomes, which limits the interpretation of the findings. Patient privacy and data security for teleoptometry was not reported. |
Maa et al. (2020)29 | |
The study population, the index test, and the reference standard match those targeted by the review question. The authors conducted a power calculation and the study was powered to detect cases of glaucoma. The index test and the reference standard were completed on the same day. The index test was interpreted without knowledge of the reference standard. Reference standard results were interpreted without knowledge of the index test. All patients received the same reference standard. All patients were included in the analysis. Estimates of random variability (i.e., CI) were reported alongside the findings. The source of funding was reported and the authors declared that the funders had no influence on the conduct of the study. Patient privacy and data security were achieved by ensuring that each patient’s history, clinical data, and ocular photographs were de-identified and uploaded into a secure research database. | Patients self-volunteered to participate in the study, and it is unclear whether this approach to patient selection could have introduced selection bias to the results. Patients are described with limited detail. The authors reported on age, male sex, and race, but no other PROGRESS-plusa criteria were reported. The study population was US veterans, which may differ from the people living in Canada who would use teleoptometry, and may limit the generalizability to Canada. While the study was powered to detect cases of glaucoma, and the low prevalence of the other conditions in the patient population may have contributed to imprecision for estimates of sensitivity (e.g., wide CIs around estimates). |
Nanji et al. (2020)30 | |
Patients were recruited using a consecutive sample. Low risk that the selection of patients would have introduced bias. The study population, the index test, and the reference standard match those targeted by the review question. The index test and the reference standard were completed using information collected on the same day. The index test was interpreted without knowledge of the reference standard. Reference standard results were interpreted without knowledge of the index test. All patients received the same reference standard. Estimates of random variability (i.e., CI) were reported alongside the findings. The authors reported the source of the funding. Patient privacy and data security were achieved by placing the patient’s history form, examination form, colour photographs, and results of the visual field test into a secure patient data website that was operated by secure diagnostic imaging. | Not all patients were included in the analysis, as 8 people did not complete the teleoptometry exam and 12% of fundus photos were excluded due to the poor quality. This may bias the findings in favour of teleoptometry, and may be less reflective of its use in practice. Patients are described with limited detail. The authors reported on age, and gender, but no other PROGRESS-plusa criteria were reported. There was a low prevalence of age-related macular degeneration, which may have contributed to imprecision for estimates of sensitivity (e.g., wide CIs around estimates). |
QUADAS-2 = Quality Assessment of Diagnostic Accuracy Studies 2.
aThe main PROGRESS-Plus criteria include place of residence, race, ethnicity, culture, language, occupation, gender, sex, religion, education, socioeconomic status, social capital, personal characteristics associated with discrimination (e.g., age, disability), features of relationships, and time-dependent relationships.
Table 9: Clinical Utility of Teleoptometry for Eye Diseases and Conditions: Strengths and Limitations of Clinical Study Using the Downs and Black Checklist19
Strengths | Limitations |
|---|---|
Stewart et al. (2022)31 | |
The aim of the study and the interventions were well described. The patients were well described, including age, sex, race, ethnicity and primary language. The teleoptometry exam was conducted and interpreted without any knowledge of the results of the in-person exam. Both eye exams were done on the same day, thus no chance of any changes in condition between tests. The authors declared that they had no conflicts of interest. The source of funding was reported and the authors declared that the funders had no influence on the conduct of the study. | Reporting of the results was unclear, and it was not clear whether all patients had both the teleoptometry and the in-person exam. The reporting of the main outcomes is unclear, with the main findings only described in the text of the report and simple outcome data were not reported. Estimates of random variability (e.g., CI) were not reported for any of the findings, which limits our confidence in these our outcomes as the amount of variation around the point estimate is unknown. The authors described this study as a noninferiority trial and set 2 margins for noninferiority (one for each primary outcome). These margins were set based on the feasibility of the sample size and it was unclear whether these margins were informed by other information (e.g., power calculation, findings from previous studies). These margins were described in the methods and the discussion, but not reported as part of the results of the study. Patients were recruited by offering them the choice between a teleoptometry exam and an in-person exam, and only recruiting those who agreed to the teleoptometry exam (without explaining that all participants would receive both exams); and were not representative of the entire population for whom teleoptometry may be used. The teleoptometry exam took place at an urban vision centre, which is not representative of the setting where most patients would receive teleoptometry exams (i.e., in rural or remote locations), thus it wasn’t subject to the potential concerns that would exist in practice (e.g., internet connection or bandwidth). The teleoptometry exam was conducted by an optometrist and viewed by an ophthalmologist which is not representative of how teleoptometry is implemented in practice, where an optometric assistant would assist with the in-person components. The more skilled optometrist may bias the results in favour of better results for teleoptometry. The same ophthalmologist conducted the teleoptometry and the in-person exam on the same day, which may have biased the results of the in-person exam, as they would have previous knowledge of the results of the teleoptometry exam. Patient privacy and data security for teleoptometry was not reported. |
CI = confidence interval.
Table 10: Evidence-Based Guidelines for Teleoptometry: Strengths and Limitations of Guidelines Using AGREE II21
Item | AOA Evidence-based Optometry Guideline Development Group (2024)34 | ATA Diabetic Retinopathy Telehealth Practice Guidelines Working Group (2020)33 |
|---|---|---|
Domain 1: Scope and purpose | ||
1. The overall objective(s) of the guideline is (are) specifically described. | Yes | Yes |
2. The health question(s) covered by the guideline is (are) specifically described. | No | No |
3. The population (patients, public, etc.) to whom the guideline is meant to apply is specifically described. | Yes | Yes |
Domain 2: Stakeholder involvementa | ||
4. The guideline development group includes individuals from all relevant professional groups. | Yes | Yes |
5. The views and preferences of the target population (patients, public, etc.) have been sought. | Yes | No |
6. The target users of the guideline are clearly defined. | Yes | Yes |
Domain 3: Rigour of development | ||
7. Systematic methods were used to search for evidence. | Yes | Partial |
8. The criteria for selecting the evidence are clearly described. | Yes | No |
9. The strengths and limitations of the body of evidence are clearly described. | Partial | No |
10. The methods for formulating the recommendations are clearly described. | Yes | Partial |
11. The health benefits, side effects, and risks have been considered in formulating the recommendations. | Yes | No |
12. There is an explicit link between the recommendations and the supporting evidence. | Yes | No |
13. The guideline has been externally reviewed by experts before its publication. | Yes | No |
14. A procedure for updating the guideline is provided. | Yes | Partial |
Domain 4: Clarity of presentation | ||
15. The recommendations are specific and unambiguous. | Yes | Partial |
16. The different options for management of the condition or health issue are clearly presented. | Yes | No |
17. Key recommendations are easily identifiable. | Yes | No |
Domain 5: Applicability | ||
18. The guideline describes facilitators and barriers to its application. | No | Partial |
19. The guideline provides advice and/or tools on how the recommendations can be put into practice. | No | Partial |
20. The potential resource implications of applying the recommendations have been considered. | Yes | No |
21. The guideline presents monitoring and/or auditing criteria. | No | No |
Domain 6: Editorial independence | ||
22. The views of the funding body have not influenced the content of the guideline. | Partial | Partial |
23. Competing interests of guideline development group members have been recorded and addressed. | Partial | Yes |
AGREE II = Appraisal of Guidelines for Research and Evaluation II; AOA = American Optometric Association; ATA = American Telemedicine Association.
aWe retained the domain names that are included in the original AGREE II checklist, which includes the term stakeholder (i.e., in domain 2), to be clear that we assessed the strengths and limitations of guidelines using AGREE II. However, the CDA-AMC understands that language is constantly evolving and the word stakeholder has association with colonialism; whenever possible, CDA-AMC does not use this word in our reports.
Appendix 5: Main Study Findings
Please note that this appendix has not been copy-edited.
Table 11: Summary of Findings by Outcome — Refractive Error
Citation | Sample size | Outcome | Outcome result | Effect estimate (95% CI) | |
|---|---|---|---|---|---|
Teleoptometry | In-person exam | ||||
Blais et al. (2024)32 | 66 | Spherical refraction Seq (diopter), mean (SD) | –1.41 (2.48) | –1.48 (2.43) | ICCb = 0.997 (0.995 to 0.998) |
Cylinder refraction J0 (diopter), mean (SD) | 0.05 (0.40) | 0.04 (0.42) | ICCb = 0.978 (0.963 to 0.986) | ||
Axis refraction J45 (diopter), mean (SD) | –0.02 (0.16) | –0.04 (0.18) | ICCb = 0.867 (0.785 to 0.919) | ||
Best corrected visual acuitya (LogMar), mean (SD) | –0.08 (0.10) | –0.08 (0.11) | ICCb = 0.939 (0.901 to 0.963) | ||
CI = confidence interval; ICC = interclass correlation coefficient; SD = standard deviation.
aMonocular distance using LogMAR visual acuity was measured in trial frames, where neither the patient nor the in-clinic technician knew which frame contained the results from which exam.
bAs defined by study authors, an ICC above 0.90 is considered, an excellent level of agreement and an ICC between 0.75 and 0.90 is considered good level of agreement.
Table 12: Summary of Findings by Outcome — Visual Comfort With Prescription
Citation | Sample size | Outcome | Teleoptometry | In-person exam | P value |
|---|---|---|---|---|---|
Blais et al. (2024)32 | 66 | Quality of visiona, mean (SD) | 4.06 (0.84) | 4.03 (0.78) | 0.49 |
Presence of distortiona, mean (SD) | 4.27 (1.03) | 4.42 (0.92) | 0.15 | ||
Dizziness when walkinga, mean (SD) | 4.26 (1.09) | 4.45 (0.96) | 0.39 | ||
Acceptability to wear prescription dailya, mean (SD) | 3.65 (1.07) | 3.73 (1.03) | 0.75 |
SD = standard deviation.
aVisual comfort with the prescription from each modality was compared by having the patient walk and look at a distance of 6m, and rate each item using a 5-point Likert scale questionnaire (ranging from strongly agree to strongly disagree) that was adapted from previous studies measuring patient satisfaction with spectacle correction, but it was not reported whether this scale is a validated tool.
Table 13: Summary of Findings by Outcome — Visual Function and Ocular Health Assessment
Citation | Sample size | Outcome | Finding |
|---|---|---|---|
Blais et al. (2024)32 | 66 | Entering distance visual acuitya | KACc = 0.857 |
Colour visiona | KACc = 1.000 | ||
Extraocular motilitya | KACc = 0.267 | ||
Pupillary reflexesa | NA (due to there being no tests outside normal limits) | ||
Anterior segmenta | KACc = 0.660 | ||
Posterior segmenta | KACc = 0.624 | ||
Ocular health diagnoses, level 1 and 2 (i.e., conditions with little risk of harm)b | Did not diagnose 3 conditions (mostly mild dry eye). Agreement = 86.4% | ||
Ocular health diagnoses, level 3 and 4 (i.e., conditions with higher morbidity)b | Did not diagnose 1 condition (inactive corneal pannus) Could not rule out 1 case of suspected papilledema. Agreement = 87.5% |
CI = confidence interval; KAC = Krippendorff alpha coefficient.
aAs outcomes of these tests are qualitative and quantitative and have different units of measure, the authors assigned every test result that was “within normal limits” a value of 0, while test results that were “outside normal limits” were giving a value of 1. The level of agreement between tests that were “within normal limits” and “outside normal limits” was compared. Outcome measures not further described.
bThe authors developed an index of morbidity which was used to classify diagnoses according to the follow-up or referral timeline planned by the optometrist who made the diagnosis [ranging from ‘none’ to “referral STAT” (severe emergency)].
cAs defined by study authors, a KAC above 0.80 is considered an “almost perfect” level of agreement; a KAC greater between 0.60 and 0.80 is considered a “substantial” level of agreement; and a KAC between 0.2 and 0.4 is considered a “fair” level of agreement.
Table 14: Summary of Findings by Outcome — Patient Satisfaction and Provider Confidence
Citation | Sample size | Outcome | Teleoptometry | In-person exam | P value |
|---|---|---|---|---|---|
Blais et al. (2024)32 | 66 | Patient satisfaction, mean (SD)a | 4.52 (0.08) | 4.95 (0.03) | < 0.001b |
Optometrist overall confidence level, mean (SD)c | 4.30 (0.05) | 5.00 (0.01) | < 0.001 |
CI = confidence interval; SD = standard deviation; NR = not reported.
aIncluded level of trust in the accuracy of the exam results, ease to communicate, ease to establish a trust relationship with the optometrist, and general satisfaction, based on a 5-point Likert scale (scale options varied by question). It was not reported whether this was a validated tool.
bP value was < 0.001 for each question of the patient satisfaction questionnaire and the confidence level for each eye test (in favour of the in-person exam) and the overall score.
cOptometrist confidence level was assessed for the following tests: distance visual acuity, Ishihara (colour blindness test), extraocular mobility, pupillary reflexes, anterior segment, posterior segment, and best corrected visual acuity. The tool used to assess provider confidence level was not described.
Table 15: Summary of Findings by Outcome — DTA for Diabetic Retinopathy
Citation | Index test | Reference standard | Number of patients | Number with condition | Sensitivity, % (95% CI) | Specificity, % (95% CI) | PPV, % (95% CI) | NPV, % (95% CI) |
|---|---|---|---|---|---|---|---|---|
Joseph et al. (2024)23 | Hybrid comprehensive eye exam (technician completed workup, synchronous exam by ophthalmologist) | In-person comprehensive eye exam by ophthalmologist (with review of technician workup) | 339 patients (678 eyes) | Any DR, 7 (1.0%) | 57.1 (18.4 to 90.1) | 98.2 (96.9 to 99.1) | 25.0 (7.3 to 52.4) | 99.5 (98.7 to 99.9) |
Keshvardoost et al. (2020)28 | Asynchronous review of digital image of macula and optic nerve by retina specialist | Dilated pupil slit lamp exam by retina specialist | 117 patients | Any DR, 48 (41%)a | 92% (examiner 1) 88% (examiner 2) | 96% (examiner 1) 98% (examiner 2) | NR | NR |
DR requiring referralb, 32 (27%) | 92% (examiner 1) 85% (examiner 2) | NR | NR | NR | ||||
Maa et al. (2020)29 | Asynchronous review of TECSc screening by ophthalmologist (examiner 1) | In-person comprehensive eye exam by ophthalmologist | 256 patients | Any DR, 8 (3.1%) | 75 (35 to 97) | 99 (97 to 100) | NR | NR |
Asynchronous review of TECSc screening by ophthalmologist (examiner 2) | 63 (25 to 92) | 99 (97 to 100) | NR | NR | ||||
Nanji et al. (2020)30 | Asynchronous review of patient history, visual acuity, IOP, visual fields, and fundus photographs by ophthalmologist. | Review patient history, visual acuity, IOP, visual fields, and performed a dilated fundus (slit lamp) exam. | 314 patients (628 eyes) | 94 cases of DR (15% of eyes) | 76.6 (62.8 to 86.4) | 96.9 (94.7 to 98.2) | 75.0 (61.2 to 85.1) | 97.2 (95.0 to 98.4) |
CI = confidence interval; DR = diabetic retinopathy; IOP = intraocular pressure; NPV = negative predictive value; NR = not reported; PPV = positive predictive value; TECS = technology-based eye care services.
aOf those with any DR, 13.6% had non-proliferative DR, 22.2% had proliferative DR, 2.6% had high-risk DR and 2.6% had advanced proliferative DR.
bDR requiring referral to a specialist within 1 month includes proliferative DR, high-risk proliferative DR, and advanced proliferative DR.
cTECS screening protocol is conducted by an optometric assistant and includes ocular history, main complaint, autorefraction, manifest refraction, BCVA, measures of the pupils, IOP, central corneal thickness, and anterior chamber depth, and colour fundus photos with dilated pupils.
Table 16: Summary of Findings by Outcome — DTA for Cataracts
Citation | Index test | Reference standard | Number of patients | Number with cataracts | Sensitivity, % (95% CI) | Specificity, % (95% CI) | PPV, % (95% CI) | NPV, % (95% CI) |
|---|---|---|---|---|---|---|---|---|
Joseph et al. (2024)23 | Hybrid comprehensive eye exam (technician completed workup, synchronous exam by ophthalmologist) | In-person comprehensive eye exam by ophthalmologist (with review of technician workup) | 339 patients (678 eyes) | 48 (7.1%) (immature and mature) | 91.7 (80.0 to 97.7) | 95.9 (94.0 to 97.3) | 62.9 (50.5 to 74.1) | 99.3 (98.3 to 99.8) |
Wong et al. (2022)25 | Asynchronous review by ophthalmologist (photos, visual acuity, IOP) | In-person exam by ophthalmologist | 860 eyes | 75.3% of eyes (graded as: 64.4% early, 31.7% moderate, 3.6% late) | 87.8 | 99.4 | 97.6 | 96.7 |
Maa et al. (2020)29 | Asynchronous review of TECSa screening by ophthalmologist (examiner 1) | In-person comprehensive eye exam by ophthalmologist | 256 patients | Cataracts referred for surgery, 10 (3.9%) | 100 (69 to 100) | 98 (95 to 99) | NR | NR |
Asynchronous review of TECSa screening by ophthalmologist (examiner 2) | 90 (56 to 100) | 98 (95 to 99) | NR | NR |
CI = confidence interval; IOP = intraocular pressure: NPV = negative predictive value; NR = not reported; PPV = positive predictive value; TECS = technology-based eye care services.
aTECS screening protocol is conducted by an optometric assistant and includes ocular history, main complaint, autorefraction, manifest refraction, BCVA, measures of the pupils, IOP, central corneal thickness, and anterior chamber depth, and colour fundus photos with dilated pupils.
Table 17: Summary of Findings by Outcome — DTA for Glaucoma
Citation | Index test | Reference standard | Number of patients | Number with glaucoma | Sensitivity, % (95% CI) | Specificity, % (95% CI) | PPV, % (95% CI) | NPV, % (95% CI) |
|---|---|---|---|---|---|---|---|---|
Joseph et al. (2024)23 | Hybrid comprehensive eye exam (technician completed workup, synchronous exam by ophthalmologist) | In-person comprehensive eye exam by ophthalmologist (with review of technician workup) | 339 patients (678 eyes) | 8 (1.2%) with glaucoma | 12.5 (0.3 to 52.7) | 99.6 (98.7 to 99.9) | 25.0 (1.0 to 80.6) | 99.0 (97.9 to 99.6) |
Chou et al. (2022)22 Evidence from 1 pilot study | Asynchronous teleoptometry (IOP, central corneal thickness, visual acuity, patient history) | In-person exam including IOP, autorefraction, visual acuity, pupil reactivity, chamber depth, afferent papillary defect, fundus photographs | 52 | 26.9% with glaucoma | 64 (35 to 87) | 95 (82 to 99) | NR | NR |
Wong et al. (2022)25 | Asynchronous review by ophthalmologist (photos, visual acuity, IOP) | In-person exam by ophthalmologist | 860 eyes | 31.6% of eyes “possibly with glaucoma” (grading: 84.6% glaucoma suspect and 17.6% definite glaucoma) | 98.7 | 76.5 | 90.5 | 96.3 |
Maa et al. (2020)29 | Asynchronous review of TECSa screening by ophthalmologist (examiner 1) | In-person comprehensive eye exam by ophthalmologist | 256 patients | Glaucoma or glaucoma suspect, 68 (26.6%) (proportion by grading not reported) | 72 (60 to 82) | 91 (87 to 95) | NR | NR |
Asynchronous review of TECSa screening by ophthalmologist (examiner 2) | 47 (35 to 60) | 97 (94 to 99) | NR | NR |
CI = confidence interval; IOP = intraocular pressure; NPV = negative predictive value; NR = not reported; PPV = positive predictive value; TECS = technology-based eye care services.
aTECS screening protocol is conducted by an optometric assistant and includes ocular history, main complaint, autorefraction, manifest refraction, BCVA, measures of the pupils, IOP, central corneal thickness, and anterior chamber depth, and colour fundus photos with dilated pupils.
Table 18: Summary of Findings by Outcome — DTA for AMD
Citation | Index test | Reference standard | Number of patients | Number with AMD | Sensitivity, % (95% CI) | Specificity, % (95% CI) | PPV, % (95% CI) | NPV, % (95% CI) |
|---|---|---|---|---|---|---|---|---|
Wong et al. (2022)25 | Asynchronous review by ophthalmologist (photos, visual acuity, IOP) | In-person exam by ophthalmologist | 860 eyes | 12.4% of eyes | 99.7 | 99.5 | 99.3 | 98.1 |
Maa et al. (2020)29 | Asynchronous review of TECSa screening by ophthalmologist (examiner 1) | In-person comprehensive eye exam by ophthalmologist | 256 patients | 6 (2.3%) | 50 (12 to 88) | 99 (97 to 100) | NR | NR |
Asynchronous review of TECSa screening by ophthalmologist (examiner 2) | 67 (22 to 96) | 95 (92 to 98) | NR | NR | ||||
Nanji et al. (2020)30 | Asynchronous review of patient history, visual acuity, IOP, visual fields, and fundus photographs by ophthalmologist | Review patient history, visual acuity, IOP, visual fields, and performed a dilated fundus (slit lamp) exam | 314 patients (628 eyes) | 13 cases (2% of eyes) | 23.1 (5.0 to 53.8) | 98.5 (97.0 to 99.3) | 27.3 (10.1 to 55.6) | 98.1 (97.5 to 98.6) |
AMD = age-related macular degeneration; CI = confidence interval; IOP = intraocular pressure; NPV = negative predictive value; NR = not reported; PPV = positive predictive value; TECS = technology-based eye care services.
aTECS screening protocol is conducted by an optometric assistant and includes ocular history, main complaint, autorefraction, manifest refraction, BCVA, measures of the pupils, IOP, central corneal thickness, and anterior chamber depth, and colour fundus photos with dilated pupils.
Table 19: Summary of Findings by Outcome — DTA for Other Conditions
Citation | Index test | Reference standard | Number of patients | Condition or treatment advice, n (%) | Sensitivity, % (95% CI) | Specificity, % (95% CI) | PPV, % (95% CI) | NPV, % (95% CI) |
|---|---|---|---|---|---|---|---|---|
Joseph et al. (2024)23 | Hybrid comprehensive eye exam (technician completed workup, synchronous exam by ophthalmologist) | In-person comprehensive eye exam by ophthalmologist (with review of technician workup) | 339 patients (678 eyes) | Nonserious injury, 12 (1.8) | 41.7 (15.2 to 72.3) | 99.8 (99.2 to 100) | 83.3 (35.9 to 99.6) | 99.0 (97.9 to 99.6) |
Allergic conjunctivitis, 86 (12.7) | 43.0 (32.4 to 54.2) | 98.3 (96.9 to 99.2) | 78.7 (64.3 to 89.3) | 92.2 (89.9 to 94.2) | ||||
Infective conjunctivitis, 18 (2.6) | 72.2 (46.5 to 90.3) | 98.3 (97.0 to 99.2) | 54.2 (32.8 to 74.4) | 99.2 (98.2 to 99.8) | ||||
Needs surgerya, 31 (9.1) | 58.1 (39.1 to 75.5) | 99.0 (97.2 to 99.8) | 85.7 (63.7 to 97.0) | 95.9 (93.1 to 97.8) | ||||
Needs spectaclesa, 114 (33.6) | 77.2 (68.4 to 84.5) | 96.9 (93.7 to 98.7) | 92.6 (85.4 to 97.0) | 89.3 (84.8 to 92.9) | ||||
Needs medicinea, 176 (51.9) | 75.6 (68.5 to 81.7) | 100 (97.8 to 100.0) | 100 (97.3 to 100.0) | 79.1 (72.9 to 84.5) | ||||
Any referralsa, 28 (8.3) | 64.3 (44.1 to 81.4) | 93.9 (90.6 to 96.3) | 48.6 (31.9 to 65.6) | 96.7 (94.0 to 98.4) | ||||
Barequet et al. (2022)26 | Asynchronous review of data obtained from the in-person exam by ophthalmologist | In-person clinical exam with visual acuity and refraction by an optometrist and full ophthalmic exam by cornea surgeon | 102 patients (204 eyes) | Keratoconus progression, 13 eyes (6%) | 69.2 (38.57 to 90.91) | 95.8 (91.9 to 98.2) | 52.9 (34.3 to 70.8) | 97.9 (95.3 to 99) |
Keshvardoost et al. (2020)28 | Asynchronous review of a single digital image of macula and optic nerve by retina specialist | Dilated pupil slit lamp exam by retina specialist | 117 patients | Clinically significant macular edema, 15 (12.8%) | 93% (both examiners) | 100% (both examiners) | NR | NR |
Maa et al. (2020)29 | Asynchronous review of TECSb screening by ophthalmologist (examiner 1) | In-person comprehensive eye exam by ophthalmologist | 256 patients | Any diagnosis resulting in referral, 112 (43.8) | 77 (68 to 84) | 74 (66 to 81) | NR | NR |
Asynchronous review of TECSb screening by ophthalmologist (examiner 2) | 81 (73 to 88) | 58 (50 to 66) | NR | NR |
CI = confidence interval; NPV = negative predictive value; NR = not reported; PPV = positive predictive value; TECS = technology-based eye care services.
aIn this study, “Patients were given a diagnosis and treatment advice based on the evaluation of the in-person ophthalmologist.”23 Target condition not further described.
bTECS screening protocol is conducted by an optometric assistant and includes ocular history, main complaint, autorefraction, manifest refraction, BCVA, measures of the pupils, IOP, central corneal thickness, and anterior chamber depth, and colour fundus photos with dilated pupils.
Table 20: Summary of Findings by Outcome — DTA for Ocular Features in Pediatric Patients With Suspected Amblyopia in Sabri et al. (2021)27
Ocular exam | Number of cases with positive (abnormal) findings | Teleoptometry examiner | Sensitivity, % (95% CI) | Specificity, % (95% CI) |
|---|---|---|---|---|
Upper lid function | 0 | Examiner 2 | NA | 100 (98 to 100) |
Examiner 3 | NA | 100 (98 to 100) | ||
Presence of ptosis | 2 | Examiner 2 | 100 (16 to 100) | 100 (98 to 100) |
Examiner 3 | 50 (1 to 98) | 100 (98 to 100) | ||
Presence of RAPD | 1 | Examiner 2 | 100 (97 to 100) | 100 (97 to 100) |
Examiner 3 | 0 (0 to 97) | 100 (97 to 100) | ||
Presence of anisocoria | 2 | Examiner 2 | 50 (1 to 98) | 99 (96 to 98) |
Examiner 3 | 0 (0 to 84) | 99 (96 to 100) | ||
Assessment of abduction | 0 | Examiner 2 | 83 (43 to 97) | 97 (94 to 98) |
Examiner 3 | 12 (3 to 52) | 98 (95 to 99) | ||
Assessment of adduction | 0 | Examiner 2 | 100 (16 to 100) | 99 (96 to 99) |
Examiner 3 | 0 (0 to 84) | 99 (97 to 100) | ||
Assessment of elevation | 0 | Examiner 2 | NA | 100 (98 to 100) |
Examiner 3 | NA | 100 (99 to 100) | ||
Assessment of depression | 0 | Examiner 2 | NA | 99 (97 to 99) |
Examiner 3 | NA | 100 (99 to 100) | ||
Presence of nystagmus | 7 | Examiner 2 | 85 (42 to 99) | 99 (96 to 100) |
Examiner 3 | 86 (42 to 99) | 99 (96 to 100) | ||
Presence of torticollis | 9 | Examiner 2 | 33 (7 to 70) | 99 (95 to 99) |
Examiner 3 | 10 (0 to 44) | 100 (97 to 100) | ||
Presence of facial asymmetry | 0 | Examiner 2 | NA | 95 (90 to 98) |
Examiner 3 | NA | 99 (95 to 99) | ||
Presence of heterotropia (any) | 76 | Examiner 2 | 72 (61 to 81) | 93 (84 to 97) |
Examiner 3 | 64 (5 to 74) | 90 (81 to 95) | ||
Presence of esotropia | 67 | Examiner 2 | 74 (62 to 84) | 97 (90 to 99) |
Examiner 3 | 60 (47 to 92) | 97 (90 to 99) | ||
Presence of exotropia | 9 | Examiner 2 | 44 (13 to 79) | 99 (95 to 99) |
Examiner 3 | 70 (34 to 93) | 96 (91 to 98) |
CI = confidence interval; NA = not applicable; RAPD = relative afferent pupillary defect.
Note: Index test was asynchronous teleoptometry (i.e., review video recordings of the in-person exam) and the reference standard was a in-person exam. Both were conducted by pediatric ophthalmologists. Includes 320 eyes from 160 kids.
Table 21: Summary of Findings by Outcome — DTA for Anterior Segment Pathologies in Pediatric Patients in Mulchandani et al. (2023)24
Pathology | Number of cases with abnormal finding | Type of teleoptometry | Sensitivity, % (95% CI) | Specificity, % (95% CI) |
|---|---|---|---|---|
Eyelids or eyelashes | 43 | Live streamed | 54 (37 to 70) | 92 (81 to 98) |
Store and forward | 72 (55 to 85) | 94 (84 to 99) | ||
Conjunctiva or sclera | 29 | Live streamed | 90 (73 to 98) | 97 (89 to 100) |
Store and forward | 66 (46 to 82) | 98 (91 to 100) | ||
Cornea | 60 | Live streamed | 88 (76 to 96) | 90 (76 to 97) |
Store and forward | 92 (81 to 98) | 87 (73 to 96) | ||
Anterior chamber | 24 | Live streamed | 96 (79 to 100) | 100 (95 to 100) |
Store and forward | 92 (73 to 99) | 100 (95 to 100) | ||
Iris | 28 | Live streamed | 89 (70 to 98) | 95 (87 to 99) |
Store and forward | 96 (80 to 100) | 83 (71 to 91) | ||
Lens | 29 | Live streamed | 96 (81 to 100) | 95 (87 to 99) |
Store and forward | 89 (71 to 98) | 95 (87 to 99) |
CI = confidence interval.
Note: Two forms of teleoptometry were compared against the reference standard of an in-person exam. The in-person exam by the pediatric ophthalmologist of the anterior segment was live streamed for a synchronous teleoptometry review and recorded for an asynchronous (store-and-forward) teleoptometry exam. Includes 45 children (89 eyes).
Table 22: Summary of Findings by Outcome — Clinical Utility of Teleoptometry vs. In-Person Examination in Pediatric Patients With Strabismus in Stewart (2022)31
Outcome | Type of measurement | Number of patients | Effect estimatea |
|---|---|---|---|
Primary gaze angle measurements | |||
Distance without correction | Horizontal | 47 | 1.00 |
Vertical | 19 | 0.98 | |
Near without correction | Horizontal | 61 | 1.00 |
Vertical | 15 | 1.00 | |
Distance with correction | Horizontal | 26 | 1.00 |
Vertical | 13 | 0.98 | |
Near with correction | Horizontal | 34 | 1.00 |
Vertical | 12 | 0.98 | |
Motility disease categorization | |||
Distance without correction | Horizontal | 54 | 0.98 |
Vertical | 54 | 1.00 | |
Near without correction | Horizontal | 69 | 1.00 |
Vertical | 69 | 0.94 | |
Distance with correction | Horizontal | 31 | 0.96 |
Vertical | 31 | 1.00 | |
Near with correction | Horizontal | 36 | 0.97 |
Vertical | 36 | 1.00 | |
vs. = versus.
aThe effect estimates for primary gaze angle measurements are intraclass correlation coefficients, and the effect estimates for motility disease categorization are kappa coefficients.
Table 23: Summary of Recommendations in Included Guidelines
Recommendations and supporting evidence | Quality of evidence and strength of recommendations |
|---|---|
AOA Evidence-based Optometry Guideline Development Group (2024)34 | |
“Ocular telehealth programs can provide increased access to care but should not be used alone or for the assessment or management of moderate or advanced diseases in patients with primary open-angle glaucoma (POAG).” (p. 55) Supporting evidence: A systematic review found that there was variability in sensitivity of tele-glaucoma screening. They concluded that further studies are needed to establish the efficacy of tele-glaucoma screening. Sensitivity and specificity of glaucoma management needs to be improved before being used extensively. A prospective cohort study found that telehealth may be effective in screening for glaucoma, especially for remote and underserved communities. Finally, a cross-sectional study found that remote assessment alone may be inappropriate for the management of glaucoma because there is merely fair agreement between remote and in-person glaucoma assessments. | Quality of evidence: Grade Ba Strength of recommendation: Strong |
ATA Diabetic Retinopathy Telehealth Practice Guidelines Working Group (2020)33 | |
“Telemedicine practice shall conform to the same professional ethics that govern in-person care. This responsibility encompasses a broad range of issues including, but not limited to, confidentiality, image quality, data integrity, clinical accuracy, reliability, and adherence to all applicable national and local regulations such as Health Insurance Portability and Accountability Act (HIPAA).” (p. 498) Supporting evidence: NR. | Quality of evidence: NR Level of adherenceb: Shall |
“Because programs have reported referral-warranted ocular disease in many patients with ungradable images, inability to obtain or grade images should be considered a positive finding and patients with unobtainable or ungradable images should be promptly reimaged or referred for a more advanced evaluation.” (p. 499) Supporting evidence: NR. | Quality of evidence: NR Level of adherenceb: Should |
“Depending on the telehealth program operational preferences and validation category, images may be acquired and reviewed stereoscopically.” (p. 500) Supporting evidence: A review of the literature suggests that accurate identification of macular edema is not always possible using nonstereoscopic methods. If stereoscopic evaluation of retinal thickening was not directly assessed, the determination of diabetic macular edema would rely on hard exudates or microaneurysms in the macular field, which are not reliable markers. | Quality of evidence: NR Level of adherenceb: May |
“A program may use nonstereoscopic techniques to establish diabetic macular edema severity based upon its operational preferences and demonstrated validation category.” (p. 501) Supporting evidence: Two studies suggest that it is possible for a program without the ability to use stereoscopic methods to be validated to identify macular edema with nonstereoscopic methods. | Quality of evidence: NR Level of adherenceb: May |
“A licensed eye care professional may not be physically available at all times during a telehealth session, so imagers shall possess the knowledge and skills for imaging independently or with assistance and consultation by telephone, including:
Supporting evidence: NR. | Quality of evidence: NR Level of adherenceb: Shall |
“Additional relevant information such as medical and surgical history, and laboratory values may also be included as metadata of an image series or otherwise linked to the images for use during image interpretation and reporting.” (p. 503) Supporting evidence: NR. | Quality of evidence: NR Level of adherenceb: May |
AOA = American Optometric Association; ATA = American Telemedicine Association; HIPAA = Health Insurance Portability and Accountability Act; NR = not reported.; POAG = primary open-angle glaucoma.
aThe guidelines by AOA defined Grade B as evidence from randomized clinical trials, cohort studies, or diagnostic studies.
bThe guidelines by ATA Diabetic Retinopathy Telehealth Practice Guidelines Working Group provided a level of adherence for each recommendation “based on the quality and quantity of peer-reviewed evidence.” “Shall” indicates required action whenever feasible and/or practical. “Shall not” indicates a proscription or action that is strongly advised against. “Should” indicates a recommended action without excluding others. “May” indicates pertinent actions that may be considered to optimize the telemedicine encounter or operational process.
ISSN: 2563-6596
Canada’s Drug Agency (CDA-AMC) is a pan-Canadian health organization. Created and funded by Canada’s federal, provincial, and territorial governments, we’re responsible for driving better coordination, alignment, and public value within Canada’s drug and health technology landscape. We provide Canada’s health system leaders with independent evidence and advice so they can make informed drug, health technology, and health system decisions, and we collaborate with national and international partners to enhance our collective impact.
Disclaimer: CDA-AMC has taken care to ensure that the information in this document was accurate, complete, and up to date when it was published, but does not make any guarantee to that effect. Your use of this information is subject to this disclaimer and the Terms of Use at cda-amc.ca.
The information in this document is made available for informational and educational purposes only and should not be used as a substitute for professional medical advice, the application of clinical judgment in respect of the care of a particular patient, or other professional judgments in any decision-making process. You assume full responsibility for the use of the information and rely on it at your own risk.
CDA-AMC does not endorse any information, drugs, therapies, treatments, products, processes, or services. The views and opinions of third parties published in this document do not necessarily reflect those of CDA-AMC. The copyright and other intellectual property rights in this document are owned by the Canadian Agency for Drugs and Technologies in Health (operating as CDA-AMC) and its licensors.
Questions or requests for information about this report can be directed to Requests@CDA-AMC.ca.