Drugs, Health Technologies, Health Systems
Health Technology Review
Antiviral Drugs for the Treatment of Suspected or Confirmed Influenza A or Influenza B
Authors: Shannon E. Kelly, Xiaoqin Wang, Annie Bai, Shuching Hsieh, Becky Skidmore, Melissa Brouwers, George A. Wells
This rapid review was conducted by the POst-market Drug Evaluation Team (PODET) through the Post-Market Drug Evaluation (PMDE) CoLab Network.
Key Messages
What Is the Issue?
Influenza is a serious viral respiratory infection that can lead to health complications and is among the top causes of death in Canada. Early treatment with antiviral drugs can reduce symptoms and complications.
Four antivirals are currently authorized by Health Canada for the treatment or prevention of influenza: oseltamivir, zanamivir, peramivir, and baloxavir marboxil. Oseltamivir (oral) and zanamivir (inhaled) are available by prescription and are stockpiled in Canada. Limited amounts of baloxavir marboxil (oral; marketed in March 2025) are available by prescription, and peramivir (IV; approved in January 2017 but not marketed) is available only through Health Canada’s Special Access Program.
The recommendations for Canada’s antiviral stockpiles were last updated in 2017, before baloxavir marboxil was authorized and without consideration of peramivir. Since then, the WHO has downgraded oseltamivir on its Essential Medicines List and recommends stockpiles include antivirals with different mechanisms of action.
There are important evidence gaps for the treatment of individuals with nonsevere influenza, and updated comparisons of antiviral efficacy, safety, and resistance are needed. The Public Health Agency of Canada is seeking the assistance of Canada’s Drug Agency to support multijurisdictional decisions on antiviral use for pandemic preparedness.
What Did We Do?
We identified a recently published systematic review (SR) and network meta-analysis (NMA), referred to as the landmark SR and NMA in our report, and critically appraised it.
We performed an updated literature search for studies published since the search period defined in the landmark SR and NMA and summarized the results from any new eligible randomized controlled trials.
What Did We Find?
Our critical appraisal of the landmark SR and NMA found that overall confidence in the results of the SR was high, and the NMA was methodologically strong and produced relevant and credible findings.
The landmark SR and NMA found that baloxavir marboxil, oseltamivir, peramivir, and zanamivir did not significantly reduce deaths or hospital admissions, and there was no increase in serious side effects compared to standard care or placebo. The antivirals did shorten the duration of influenza symptoms by up to 1 day.
There were no major differences between the antiviral drugs in comparisons of how well they worked for the same outcomes or for their side effects, even across different patient groups. However, baloxavir marboxil may increase the risk of developing drug-resistant virus strains.
A newer clinical trial comparing baloxavir marboxil and oseltamivir also found no difference in symptom relief or serious side effects. This study also detected some antiviral resistance following treatment with baloxavir marboxil using a different assessment approach, but not for oseltamivir.
Neither the landmark SR and NMA nor the updated search conducted on January 9, 2025, found any evidence reporting on study withdrawal due to side effects or on human-to-human transmission of the influenza virus. The lack of data on transmission is a noted limitation of the landmark SR and NMA.
What Does This Mean?
Decisions on stockpiling antivirals for influenza should consider the efficacy, safety, and potential benefits for populations at high risk for infection, as well as the impact of symptoms on health care resources and the risk of antiviral resistance. While baloxavir marboxil may provide some benefits, its potential for resistance requires careful management.
A diversified stockpile of antiviral medications, considering logistics and supply, may be warranted instead of reliance on drugs with a single mechanism of action.
Abbreviations
AE
adverse event
AMSTAR
A MeaSurement Tool to Assess systematic Reviews
CI
confidence interval
MID
minimal important difference
NACI
National Advisory Committee on Immunization
NAS
National Antiviral Stockpile
NESS
National Emergency Strategic Stockpile
NMA
network meta-analysis
PICO
population, intervention, comparator, and outcome
RCT
randomized controlled trial
RD
risk difference
RoB
risk of bias
SAE
serious adverse event
SR
systematic review
Introduction and Rationale
Background
Disease Background
Influenza, or the flu, is an acute viral respiratory infection that can cause substantial morbidity and mortality.1 There are 3 distinct types of influenza viruses that infect humans: influenza A, B, and C.1 Seasonal influenza A and B viruses circulate among humans worldwide.2 Influenza A infects multiple species including humans, swine, equines, and birds.1 It is more susceptible to antigenic mutations and hence is the major cause of pandemics.1 The surface of the virion envelope is covered with proteins hemagglutinin, neuraminidase, and matrix 2.1 Each influenza A subtype is characterized by the variation in the hemagglutinin and neuraminidase surface proteins present (e.g., H3N2, H5N1).1 Antigenic mutations are associated with changes in the hemagglutinin or neuraminidase surface proteins and are generally classified as antigenic drift or shift.1 Antigenic drift involves small, gradual amino acid substitutions of the hemagglutinin or neuraminidase proteins that can result in smaller outbreaks.1 Antigenic shift occurs when there are substantial changes in the hemagglutinin or neuraminidase proteins that create novel influenza subtypes with the potential to cause widespread pandemics.1
The infection is highly contagious, and the primary symptoms are abrupt onset of fever, cough, chills or sweats, muscle aches, and malaise.3 The onset is typically rapid and symptoms can persist for 2 to 8 days.3 Gastrointestinal symptoms, such as vomiting and diarrhea, can occur in children.1 Some patients, especially older adults, children, and those with comorbidities, can experience severe disease due to viral or secondary bacterial pneumonia with respiratory and multiorgan failure.1 There are many complications of influenza that can adversely affect cardiovascular, hematologic, musculoskeletal, neurologic, ocular, pulmonary, and renal systems.1 Patients can have an increased risk for complications from influenza due to the following reasons: having coexisting medical conditions, being aged 65 years or older, being aged 5 years or younger, being long-term care residents, or being pregnant or postpartum.1
Influenza is ranked among the top 10 leading causes of death in Canada.1 Influenza causes approximately 12,200 hospitalizations and 3,500 deaths each year in Canada.4,5 It is estimated that each influenza-related hospitalization can cost health care systems in Canada between $14,000 and $20,000, with a cumulative economic burden of $168 million to $240 million annually.6
In clinical practice, diagnosis of influenza is based on presenting signs and symptoms or influenza-associated complications, such as exacerbation of a chronic disease, concomitant pneumonia, or rhabdomyolysis (muscle breakdown).3 In outpatient and emergency department settings, testing for influenza is not necessary to start antiviral treatment in a patient with suspected influenza, especially during seasons in which influenza A or B viruses are circulating in the local community.3
Treatment of Influenza
Canada’s National Advisory Committee on Immunization (NACI) recommends treatment with antiviral drugs in persons with influenza symptoms who are considered to have a high-risk for severe influenza or who are severely ill.1,7,8 Early treatment with an antiviral drug has been shown to lead to shorter duration of symptoms and fewer complications.9 Two neuraminidase inhibitors, oral oseltamivir in capsule and powder form10 and inhaled zanamivir,11 are approved and marketed antiviral drugs for the treatment and prevention of influenza in Canada. Both are available by prescription and are stockpiled as part of the National Antiviral Stockpile (NAS) and National Emergency Strategic Stockpile (NESS). There is not a current recommendation for the NAS to stockpile IV zanamivir, which does not have market authorization, although it has provisional inclusion through NESS at this time.12 The cap-dependent endonuclease inhibitor, baloxavir marboxil in oral tablet is approved and marketed for treatment of influenza and available in limited quantities on prescription. IV peramivir,13 which is also a neuraminidase inhibitor approved for treatment of influenza, is not marketed and is only available through Health Canada’s Special Access Program.12
Policy Issue
As a shared responsibility between federal, provincial, and territorial jurisdictions in Canada, stockpiles of certain influenza antiviral drugs are maintained through the NAS and the NESS to ensure timely and equitable access to effective drugs during a pandemic or a potential global shortage. The most recent update to Canada’s antiviral stockpile recommendations occurred in 2017, before the market authorization of baloxavir marboxil (issued in January 2022) and without substantive consideration for peramivir, which received market authorization in January 2017. Since that time, the WHO has downgraded oseltamivir on its Essential Medicines List and now advises that national stockpiles include antivirals with diverse mechanisms of action.14 Notably, there remain critical evidence gaps regarding the clinical management of nonsevere influenza, particularly in populations at high risk for developing severe influenza and in equity-deserving populations. Therefore, there is a need for updated comparative evidence for the efficacy, safety, and resistance profiles of the antivirals to inform coordinated, multijurisdictional decision-making for pandemic preparedness. The Public Health Agency of Canada has engaged Canada’s Drug Agency to provide scientific and policy support related to the safe and appropriate use of antiviral drugs for influenza A and B for pandemic preparedness.
Policy Questions
The following policy questions are being addressed with this project:
Is there a need to stockpile antiviral drugs for prepandemic or pandemic preparedness for the treatment of influenza A or B?
Which influenza antivirals should be stockpiled for prepandemic or pandemic preparedness for treatment?
What does each influenza antiviral offer in the prepandemic or pandemic context, considering relevant outcomes for specific populations?
What are the priorities to treat groups at high risk for severe influenza or in high-risk settings with antivirals for influenza A or B?
Purpose
The aim of this project is to identify and assess evidence on the efficacy and safety of antiviral drugs approved in Canada for the treatment of individuals with suspected or confirmed type A or B influenza infection who are not hospitalized to inform assessments of the utility of pandemic stockpiling.
Research Questions
The project will address the following research questions. Details on the specific interventions and outcomes are included in Table 1.
What is the efficacy of antiviral drugs for the treatment of individuals with suspected or confirmed influenza A or B and not hospitalized?
What is the safety of antiviral drugs for the treatment of individuals with suspected or confirmed influenza A or B and not hospitalized?
Opportunities for Feedback
Interested parties from patient and medical advocacy groups and organizations were given the opportunity to provide feedback on the draft report.
Methods
Literature Search Methods
We identified a recent systematic review (SR) with network meta-analysis (NMA) through database notifications that included studies published up until September 20, 2023, which will be referred to as the landmark SR and NMA henceforth.15 Additionally, we performed an updated search on January 9, 2025, to identify eligible randomized controlled trials (RCTs) published since the previous search. The literature search was performed by an information specialist using a peer-reviewed search strategy according to the Peer Review of Electronic Search Strategies (PRESS) checklist.16 The search strategy is presented in Appendix 1.
Published literature was identified by searching the following bibliographic databases: MEDLINE, Embase, the Cochrane Library, and PubMed. The search strategy considered both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. Search filters were applied to limit retrieval to RCTs. Retrievals were not limited by language. Conference abstracts were excluded from the search results.
Grey literature (literature not published in peer-reviewed journals) was identified by searching the US National Institutes of Health clinicaltrials.gov website and the WHO’s International Clinical Trials Registry Platform (ICTRP) search portal. These searches were supplemented by reviewing the reference lists of included papers.
Selection Criteria and Methods
Two reviewers conducted a calibration exercise (N = 50 records) to ensure a consistent understanding of the screening criteria. The same 2 reviewers independently screened titles and abstracts for relevance to the research questions. Potentially relevant full-text articles were retrieved and independently assessed for eligibility in accordance with the predetermined selection criteria (Table 1). Any disagreements between reviewers were discussed for consensus, and a third reviewer was consulted when necessary. We used the web-based SR management platform DistillerSR to complete the screening process.17
Inclusion and Exclusion Criteria
We included RCTs that enrolled individuals with suspected or confirmed influenza A or B or nonspecified influenza strains (including influenza-like illness) who were not hospitalized. Studies with eligible participants, interventions, comparators, and study designs were eligible irrespective of whether they reported the outcomes of interest.
This Rapid Review focused on comparisons of baloxavir marboxil, oseltamivir, peramivir, and zanamivir or their combinations — either against each other (active control) or against placebo, no treatment, or standard of care.
Table 1: Selection Criteria for Primary Studies
Criteria | Description |
|---|---|
Populations | Individuals with suspected or confirmed influenza A or B or those presenting with influenza-like illness during the influenza season who were not hospitalized (i.e., those with nonsevere illness) Subgroups
|
Interventionsa |
|
Comparators |
|
Outcomes | Efficacy
Safety
|
Study design | Randomized controlled trials |
Settings |
|
Exclusions |
|
aIncluding comparing different doses, frequencies, or administrations of the same intervention.
bCombination treatment includes a neuraminidase inhibitor with another neuraminidase inhibitor or a neuraminidase inhibitor with baloxavir marboxil.
cPopulation that has not been vaccinated (i.e., before a vaccine is available).
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, were duplicate publications, or were published before 2023. Primary studies retrieved by the search were excluded if they were captured in the landmark SR and NMA.
Critical Appraisal
The included publications were critically appraised by 1 reviewer using A MeaSurement Tool to Assess systematic Reviews 2 (AMSTAR 2) for SRs,18 the “Questionnaire to assess the relevance and credibility of a network meta-analysis”19 for NMAs, and a modified Cochrane Collaboration Risk of Bias (RoB) tool (version 1.0)20 for RCTs. The modified RoB tool for RCTs was used to maintain consistency with the methods used in the landmark SR and NMA.15 Modifications were made to the response options in the RoB tool, which replaced the existing “unclear” response with 2 responses (“probably high” and “probably low”) to provide a more informative risk of bias assessment and avoid using the “unclear” rating. No summary scores were calculated based on each study assessment; rather, the strengths and limitations of each included publication were described narratively.
Summary of Evidence
Quantity of Research Available
We identified a landmark SR and NMA of 73 RCTs through database notifications. A total of 233 citations were identified in the updated literature search. Following the screening of titles and abstracts, 228 citations were excluded and 5 potentially relevant articles from the electronic search were retrieved for full-text review. A total of 42 potentially relevant reports were retrieved from the grey literature search for full-text review, but none met the inclusion criteria. Of the 5 potentially relevant articles, 4 publications were excluded for various reasons and 1 RCT21 publication met the inclusion criteria and was included in this report. Appendix 2 presents the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow chart of the study selection.
Landmark Systematic Review Characteristics
Landmark SR and NMA Study Overview
Gao and colleagues15 conducted an SR and NMA published 2025, with population, intervention, comparator, and outcome (PICO) questions that closely aligned with those of this report (Table 2). The methodological quality of the review was determined to be high based on AMSTAR 2 assessment.18 The review considered relevant RCTs published up to September 20, 2023, ensuring comprehensive coverage of the available evidence. Finally, the NMA was performed in a rigorous manner based on AMSTAR 2 and International Society for Pharmacoeconomics and Outcomes Research (ISPOR) evaluations.18,19 Details of the quality assessments can be found in Appendix 3 (Table 11, Table 12, and Table 13).
The landmark SR and NMA included intervention comparisons beyond those of interest to the present review. Specifically, the NMA included comparisons of antiviral drugs not approved in Canada, including umifenovir, amantadine, laninamivir, favipiravir, and rimantadine. Only relevant comparisons of interventions are described hereafter in this report.
Additional details regarding the characteristics of the landmark SR and NMA are provided in Appendix 4.
Table 2: Landmark Systematic Review Overview
Attribute | Description |
|---|---|
Citation15 | Gao Y, Zhao Y, Liu M, et al. Antiviral Medications for Treatment of Nonsevere Influenza: A Systematic Review and Network Meta-Analysis. JAMA Intern Med. 2025. doi:10.1001/jamainternmed.2024.7193 |
Study description | A systematic review with network meta-analysis models of randomized controlled trials for the effectiveness and safety of antiviral medications for treating nonsevere influenza. |
Study design | Frequentist network meta-analysis. A total of 73 randomized controlled trials were included in the network with 9 interventions compared to placebo or standard of care and to one another. The 14 available comparisons relevant to this report included:
|
Search period | From the database’s inception to September 20, 2023 |
Countries | China, Canada |
Funding source | The study was supported by the WHO. |
Scope of the SR and NMA | |
Population | Individuals with nonsevere suspected or confirmed influenza (A or B; any seasonal, pandemic, or zoonotic type) |
Intervention(s) or exposure(s) | Influenza antiviral drugs approved by the US FDA or other regulatory organizations worldwide, including:
|
Comparator(s) (if applicable) |
|
Subpopulations |
|
Outcomes | Efficacy:
Safety:
|
AE = adverse event; NMA = network meta-analysis; SR = systematic review; vs. = versus.
aInhaled and IV zanamivir are eligible.
bBeyond the scope of the current review.
Study Design
The landmark SR and NMA was published in 2025. The included RCTs were identified by searching bibliographic databases and grey literature from inception to September 20, 2023.
In this publication, authors performed frequentist random-effects NMAs. A total of 73 trials (34,332 participants) provided evidence on 9 interventions compared to placebo or standard of care. Of these, 58 RCTs considered interventions relevant to the current review (baloxavir marboxil, oseltamivir, zanamivir, peramivir, and oseltamivir combined with zanamivir) compared to placebo or standard of care.
Countries of Origin
Of the 58 relevant RCTs, 31 were multinational and 27 were each conducted in a single country, including Japan (n = 10 RCTs), the US (n = 7 RCTs), China (n = 3 RCTs), Germany, France, and Finland (n = 2 RCTs each), and Bangladesh (n = 1 RCT) (Appendix 4).
Patient Population
Patients with suspected or laboratory-confirmed nonsevere influenza (any type of influenza virus) were included. Authors used the WHO definitions for disease severity. Severe illness from influenza infection was defined as an illness that required hospitalization, and nonsevere influenza was defined as the absence of any criteria for severe influenza.15
Sample sizes of the 58 RCTs relevant to this report ranged from 14 participants to 3,266 participants, with a total of 28,462 participants. The median of RCT mean age was 35.0 years (range, 2.4 years to 73.4 years). The median proportion of female participants across the studies was 50.3% (range, 0.9% to 62.9%) and the median proportion of male participants was 49.7% (range, 37.1% to 99.1%). Most RCTs reported including participants with influenza A or influenza B (n = 52), while 6 did not report the type of influenza. The proportion of patients with confirmed influenza ranged from 24% to 100%. A total of 20 relevant RCTs reported inclusion of participants at high risk for severe clinical outcomes (median proportion = 14.0%; range, 3.9% to 100%). A total of 27 relevant RCTs reported inclusion of some participants with comorbidities such as chronic respiratory conditions, asthma, cardiovascular diseases, and diabetes (Appendix 4).
Several prespecified analyses of population subgroups were considered, including age and influenza subtype; however, there were insufficient data and no analyses were feasible. No results were reported separately for influenza A subtypes, and although the included trials considered a range of different age groups, study results were not summarized or stratified by age. Gao and colleagues categorized patients based on their perceived risk for severe outcomes of influenza as “low risk” and “high risk.” These categories consider individuals who are pregnant, older adults, and individuals who may have a chronic condition or immunosuppression. The review did not consider individual risk factors or the effect of multiple morbidities. There was no consideration for equity-denied populations or for participants’ influenza vaccination status.
Interventions and Comparators
The landmark SR and NMA focused on influenza antiviral drugs approved by the US FDA or other regulatory organizations worldwide, including baloxavir marboxil, oseltamivir, peramivir, zanamivir, laninamivir, umifenovir, favipiravir, amantadine, and rimantadine. As previously noted, laninamivir, umifenovir, favipiravir, amantadine, and rimantadine are not approved in Canada and are therefore beyond the scope of this review.
As noted in Table 2, combinations of drugs relevant to this review were also included in the landmark publication. The primary comparators were no intervention, placebo, standard of care, or treatment with another antiviral drug. Characteristics of each RCT relevant to this report are reported in Appendix 4.
In the trials included by Gao and colleagues, baloxavir marboxil was administered as a single oral dose, with dosing adjusted by body weight (40 mg for individuals who weigh 40 to < 80 kg and 80 mg for those who weigh ≥ 80 kg). Oseltamivir was administered orally at a dose of 75 mg twice daily for 5 days, which was consistent across studies. Peramivir was delivered intravenously, most commonly as a single 300 mg or 600 mg dose. Zanamivir was administered by inhalation using a dry powder inhaler, typically at a dose of 10 mg (2 inhalations of 5 mg) twice daily for 5 days. None of the included trials considered IV zanamivir.
Outcomes
The SR collected several patient-important outcomes, including mortality, admission to hospital, admission to intensive care unit, progression to mechanical ventilation, duration of mechanical ventilation, duration of hospitalization, time to alleviation of symptoms, hospital discharge destination, emergence of resistance, any adverse events (AEs), AEs related to treatments, and serious AEs (SAEs). Time to alleviation of symptoms was defined as the time from the start of treatment to the improvement of all influenza-associated symptoms.
Two outcomes of interest for this report were not reported in the SR (transmission of virus [human to human] and withdrawal due to AEs).
RCT Study Characteristics
Study Design
We identified 1 single-centre, randomized parallel-controlled trial published in 2024 by Qui and colleagues.21 The characteristics of this RCT are provided in Table 3.
Table 3: Characteristics of the Study and Patients From the Included RCT
Characteristic | Qiu et al. (2024)21 |
|---|---|
Publication status | Peer-reviewed publication |
Setting | China |
Patients | Individuals with laboratory-confirmed influenza A |
Randomized patients, N | 200 |
Age (years), mean (SD) | 42 (16.95) |
Age (years), range | 14 to 80 |
Sex
|
|
Pregnant, % | 0 |
Patients considered to be at high risk for severe influenza | 18 patients (12 with hypertension, 3 with diabetes, 1 with Hashimoto thyroiditis, 1 with rheumatoid arthritis, and 1 with osteoarthritis) |
Comorbidities, % | NR |
Type of influenza (%) | Type A (100) |
Confirmed influenza, % | 100 |
Time from onset of symptoms to treatment or randomization (hours), mean (SD) | 23.0 (6.95) |
Influenza vaccination, % | NR |
Treatment description | Group 1: Baloxavir marboxil (tablet, oral) single dose 40 mg followed by placebo tablets b.i.d. for 4 days Group 2: Oseltamivir (capsule, oral) 75 mg b.i.d. for 5 days |
Outcomes |
|
Funding source | No financial support declared |
B.i.d. = twice a day; NR = not reported; RCT = randomized controlled trial; SD = standard deviation.
aDefinition provided by study authors: “Total effective rate = (markedly effective cases + effective cases) / total cases × 100; markedly effective is defined as the patient’s body temperature dropping to normal level after 48 hours of medication and symptoms such as cough and sore throat alleviated significantly or completely; effective is defined as the patient’s body temperature returning to normal after 72 hours of medication with cough, sore throat, and other symptoms alleviated.”21
bDefinition provided by study authors: “Fever subsidence time, also disappearance time of fever or time to fever resolution, was defined as the time from the start of treatment until the body temperature was below 37°C for at least 24 hours.”21
cDefinition provided by study authors: “Cough improvement time, also disappearance time of cough.”21
dDefinition provided by study authors: “Sore throat improvement time, also disappearance time of sore throat.”21
Country of Origin
The study was conducted at the Wenzhou Central Hospital in China from January 2022 to March 2022.
Patient Population
Two hundred patients with laboratory-confirmed influenza A diagnosed in the hospital fever clinic were included in the study. Eligible individuals presented with flu-like symptoms (e.g., body temperature ≥ 37.3oC, headache, sore throat, cough, and fatigue), were aged 14 years to 80 years, and visited the clinic within 48 hours of symptom onset.
Individuals with severe or critical influenza, in combination with serious organic diseases, bacterial infection, or a positive test of influenza B or coronavirus; those who were pregnant or lactating; and those taking other antiviral drugs were excluded from the study. Of the 200 patients randomized, 9% had an underlying comorbid disease, including hypertension, diabetes, Hashimoto thyroiditis, rheumatoid arthritis, or osteoarthritis. Baseline characteristics were balanced between the 2 randomized treatment groups. Proportions of patients who had received influenza vaccination ranged from 0% to 57.9% in the included trials. A total of 16 RCTs did not report vaccination status.
Interventions and Comparators
Eligible patients were randomized to receive either oral baloxavir marboxil tablets (40 mg once followed by placebo pills twice a day for 4 days) or oral oseltamivir capsules (75 mg twice a day for 5 consecutive days). When a patient’s body temperature was noted to be higher than 38.5°C, oral antipyretics (ibuprofen suspension, 10 mL) were provided.
Outcomes
The primary outcome was the time to symptom alleviation, which was defined as the time from the start of treatment until all symptoms (e.g., fever, cough, and sore throat) were absent or very mild for at least 21.5 hours. No rationale or empirical data were presented to support the use of this time point (versus using 24 hours).
Total effective rate is calculated by dividing the sum of markedly effective cases and effective cases by the total number of cases, as given by the following formula: (markedly effective cases + effective cases)/total cases × 100%.
Markedly effective cases were defined as “those in which the patient’s body temperature dropped to a normal level after 48 hours of medication, and symptoms such as cough and sore throat disappeared essentially or completely.”21 Effective cases were defined as those in which the patient’s body temperature returned to normal after 72 hours of medication, with cough, sore throat, and other symptoms alleviated.
Also presented was the resolution time for individual clinical symptoms, including fever (defined as the time from the start of treatment until the body temperature was lower than 37°C for at least 24 hours) as well as disappearance or improvement of cough and sore throat symptoms. No additional details were provided about how these assessments were conducted in the RCT, including any description of concomitant medication use alongside the trial interventions.
Furthermore, the emergence of antimicrobial resistance and SAEs after 5 days of treatment was reported. After patients were treated with baloxavir marboxil, mutations were detected “using the virus’s polymerase acidic protein, which is an enzyme the virus uses to replicate.”21 No further information was presented describing this approach. Serious and adverse drug reactions were recorded based on the WHO’s definitions and classification.
Critical Appraisal of the Landmark SR and NMA
The landmark SR and NMA was not assessed to have any critical weaknesses based on AMSTAR 2. It was well conducted, with clear research questions and appropriate methods and processes for evidence synthesis, and any justification for heterogeneity or protocol deviations was reported. However, the SR was assessed to have several noncritical weaknesses including a lack of rationale for only including RCTs, the absence of a list of excluded studies, and the lack of consideration of the setting and funding source(s) for the included RCTs (Appendix 3, Table 11, Table 12, and Table 13).
The relevance of the NMA was assessed19 to be sufficient. All 4 items (1 through 4) related to the relevance subdomain, including the population, interventions, outcomes, and research context, were rated as strengths. The methods for the NMA were assessed to have met all the criteria and no fatal flaws were identified. The statistical methods preserved within-study randomization, and both direct and indirect comparisons are available for pairwise contrasts and in agreement. A valid rationale provided for the use of the fixed-effect models. Subgroup and sensitivity analyses and meta-regression were performed to assess the robustness of the treatment effects and the impact of heterogeneity. Gao and colleagues also conducted global and local statistical tests for inconsistency and reported no major violations. The review reports that the assumption of transitivity was supported, although as there are few head-to-head comparisons for many interventions of interest, some additional details would have been informative. We assessed this to be a reporting limitation. The analyses relied on aggregate (study-level) data for the outcomes of interest, and no participant level data were available.
One limitation within the context of relevance of outcomes is the lack of consideration for viral transmission (human to human) and withdrawals due to AEs. Viral transmission is less likely to be reported in the included RCTs, as they included patients with influenza (i.e., index cases) and not those without influenza (i.e., contact cases, such as household or health care contacts). While withdrawals due to AEs were not explicitly captured, the SR did consider treatment-related AEs.
The overall credibility of the NMA was assessed as sufficient. Strengths were identified across all subdomains of “Evidence base used for the indirect comparison or NMA,” “Analysis,” “Reporting quality and transparency,” “Interpretation,” and “Conflict of interest.” Under the subdomain of reporting quality, the NMA was assessed as having a weakness related to a lack of ranking of interventions based on the reported treatment effects and its uncertainty. This is not an item that assessors felt would affect the credibility of the reported findings. One methodological limitation in the analyses by Gao et al. is the lack of exploration into whether including or excluding trials with high or unclear risks of bias influenced treatment effect estimates. Given that a Grading of Recommendations Assessment, Development and Evaluation (GRADE) framework was used to consider risk of bias and other factors across the body of evidence, and the sensitivity analyses completed around the publication status (peer-reviewed) of the included studies, this was not an item that assessors felt would affect the credibility of the reported findings.
A detailed critical appraisal summary is presented in Appendix 3.
Critical Appraisal of the RCT
For randomization, the RCT used both a computer-generated random sequence and sealed envelopes to conceal the allocation, which reduced the risk of selection bias. Blinding of the assignment of patients to the intervention and applying identical-looking placebo tablets during the study made the risk of performance bias low. Blinding of the assignment of outcome assessors achieved a low risk of detection bias. The analysis included complete data from all randomized patients who completed the trial and did not have missing data. All prespecified outcomes were reported with no baseline imbalance or early trial discontinuation observed, resulting in a low risk of attrition, reporting bias, and other biases.
The study did not report whether patients’ treatment allocation was masked from health care providers, data collectors, and data analysts. This lack of blinding could introduce a potential risk of performance or detection bias, particularly for subjective outcomes related to patient symptoms. However, given that uncomplicated symptoms and symptom-related outcomes in this study are more likely to be reported by patients and verified by professional outcome observers, the risk of bias in this domain is likely low.
Overall, this RCT was assessed to have a low risk of bias. Nonetheless, several factors limit the generalizability of the findings: the exclusion of patients younger than 14 years, the single-centre study design, and the use of convenience sampling to recruit patients. Additionally, the relatively short study duration (3 months) and brief follow-up period (5 days) may fail to adequately capture seasonal variation in influenza A virus or longer-term patient response. The study may also have limited capacity to detect the emergence of baloxavir marboxil resistance. Due to the lack of a control group and the limited description of the outcome assessed, this finding may have a high risk of bias. Further research is warranted to evaluate the impact of resistance on treatment outcomes and to explore potential mitigation strategies.
A detailed summary of the assessment is reported in Appendix 3, Table 14.
Findings
In patients with nonsevere influenza who are at low risk for severe influenza, treatment with baloxavir marboxil, oseltamivir, peramivir, and zanamivir had little or no effect on mortality. Baloxavir marboxil, oseltamivir, and zanamivir also had little or no effect on hospital admissions. No data were available for peramivir related to hospitalization.
In patients with nonsevere influenza who are at high risk for severe influenza, treatment with baloxavir marboxil, oseltamivir, peramivir, and zanamivir had little or no effect on mortality. However, baloxavir marboxil may have reduced the risk of being admitted to hospital, although authors were not very confident in this finding. Oseltamivir and zanamivir had little or no effect on hospitalization and these results are more certain.
Baloxavir marboxil likely shortens the time to symptom relief by approximately 1 day compared to standard care and does not increase treatment-related side effects, but it may lead to antiviral resistance in about 10% of treated patients. Oseltamivir and zanamivir may also help with symptom duration. Combining 2 antivirals did not improve efficacy.
Overall, all antivirals have similar efficacy and safety profiles when compared to each other, though the certainty of results varies.
Findings of the Landmark SR and NMA
The analyses presented in the landmark SR and NMA include interventions that fall outside the scope of this review. As such, the numbers of RCTs and patients referred to in the results reflect all trials and participants included in the original analyses and are not limited to those related to the interventions of interest in the PICO. It was not possible to elucidate the exact number of RCTs and patients for the interventions in the PICO specifically. The findings for each outcome are restricted to interventions and comparisons of interest.
Mortality
Mortality outcomes were synthesized from 41 trials, including a total of 23,892 participants. The evidence network shows that a large proportion of the included trials compared oral oseltamivir or inhaled zanamivir to standard care or placebo. The NMA found that baloxavir marboxil, oseltamivir, peramivir, and zanamivir were each associated with little to no difference in mortality when compared with standard care or placebo. This was consistent for patients considered to be at low risk (absolute risk difference [RD] range, −0.12 to −0.02 per 1,000) or high risk (absolute RD range, −1.22 to −0.24 per 1,000) for severe influenza (Table 4). Comparisons between the individual antiviral drugs also showed no statistically significant differences in mortality. The certainty of evidence was rated as high across all NMA comparisons.
What This Means
The WHO used a minimal important difference (MID) of 3 per 1,000 patients to interpret the evidence in the 2024 guidelines for influenza. MID is defined as the smallest change in an outcome of interest that informed patients would perceive as important, whether beneficial or harmful. Based on this threshold, none of the interventions of interest meaningfully reduced mortality. Across all available antiviral treatments assessed, there is high-certainty evidence that these antiviral drugs do not meaningfully change the risk of death due to influenza, regardless of whether patients are at low or high risk for complications (Table 4). While small effect size differences were observed, none were large enough or consistent enough to suggest a real benefit or harm in terms of reducing mortality.
Table 4: Summary of Findings From the Landmark SR and NMA for Mortality
Comparison | NMA relative risk for mortality (95% CI) | NMA absolute risk difference for mortality (per 1,000 patients) (95% CI) | Certainty of evidence | |
|---|---|---|---|---|
Mortality in patients at low risk for severe influenza | Mortality in patients at high risk for severe influenza | |||
Peramivir vs. standard care or placebo | 0.39 (0.04 to 4.04) | −0.12 (−0.19 to 0.61) | −1.22 (−1.92 to 6.08) | High |
Baloxavir marboxil vs. standard care or placebo | 0.83 (0.14 to 4.82) | −0.03 (−0.17 to 0.76) | −0.34 (−1.72 to 7.64) | High |
Oseltamivir vs. standard care or placebo | 0.84 (0.34 to 2.07) | −0.03 (−0.13 to 0.21) | −0.32 (−1.32 to 2.14) | High |
Zanamivir vs. standard care or placebo | 0.88 (0.34 to 2.28) | −0.02 (−0.13 to 0.26) | −0.24 (−1.32 to 2.56) | High |
Baloxavir marboxil vs. oseltamivir | 0.98 (0.19 to 5.11) | 0.00 (−0.14 to 0.69) | −0.03 (−1.36 to 6.90) | High |
Baloxavir marboxil vs. peramivir | 2.11 (0.13 to 34.01) | 0.09 (−0.07 to 2.57) | 0.87 (−0.68 to 25.75) | High |
Baloxavir marboxil vs. zanamivir | 0.95 (0.13 to 7.02) | −0.01 (−0.15 to 1.06) | −0.09 (−1.53 to 10.60) | High |
Oseltamivir vs. peramivir | 2.15 (0.22 to 20.79) | 0.09 (−0.06 to 1.54) | 0.90 (−0.61 to 15.44) | High |
Oseltamivir vs. zanamivir | 0.96 (0.26 to 3.58) | −0.01 (−0.13 to 0.45) | −0.07 (−1.30 to 4.54) | High |
Peramivir vs. zanamivir | 0.45 (0.04 to 5.57) | −0.10 (−0.17 to 0.80) | −0.97 (−1.69 to 8.04) | High |
CI = confidence interval; NMA = network meta-analysis; SR = systematic review; vs. = versus.
Hospitalization
Hospitalization outcomes were evaluated across 28 trials and included data from 17,262 participants. The evidence network shows that a large proportion of the included trials compared treatment with oral oseltamivir to standard care or placebo. For patients considered to be at low risk for severe influenza, no individual antiviral was associated with a statistically significant reduction in hospital admissions compared with standard care or placebo. Absolute RDs were small (ranging from −2 to 1 per 1,000 patients) with high-certainty evidence. Among patients considered to be at high risk for severe influenza, the findings were more variable. Baloxavir marboxil showed a larger reduction in hospitalizations (RD = −16 per 1,000; 95% confidence interval [CI], −20 to 4), but the evidence was rated to be of low certainty, which limits confidence in this effect. Oseltamivir and zanamivir showed smaller and statistically nonsignificant effects (absolute RDs = −4 and 4 per 1,000, respectively) with certainty around the evidence rated as high (Table 5).
The direct comparisons between antivirals similarly did not show any significant differences in hospitalization, although point estimates for baloxavir marboxil suggested moderate reductions in admissions. This was mainly observed in patients considered to be at high risk and the certainty around this evidence was assessed as low to moderate.
What This Means
In 2024, the WHO used an MID of 15 hospitalizations per 1,000 patients to guide the interpretation of influenza evidence for antivirals.22,23 Across all comparisons, there is no consistent, high-certainty evidence that any of the antiviral drugs meaningfully reduce hospital admissions, particularly in patients considered to be at low risk for more severe complications. For patients considered to be at high risk for more severe complications, baloxavir marboxil may reduce the likelihood of hospitalization, but this finding is somewhat uncertain due to variability across studies. Comparisons between the individual antiviral drugs suggest no clear advantage of 1 drug over another in preventing hospitalization. Decisions about antiviral use, therefore, should consider other potential clinical or patient-important benefits alongside any potential prevention of hospital admission (Table 5).
Table 5: Summary of Findings From the Landmark SR and NMA for Hospitalization
Comparison | NMA relative risk for hospitalization (95% CI) | NMA absolute risk difference for hospitalization (per 1,000 patients) (95% CI) | Certainty of evidence | |
|---|---|---|---|---|
Hospitalization in patients at low risk for severe influenza | Hospitalization in patients at high risk for severe influenza | |||
Oseltamivir vs. standard care or placebo | 0.80 (0.54 to 1.18) | −1 (−1 to 1) | −4 (−10 to 4) | High |
Baloxavir marboxil vs. standard care or placebo | 0.24 (0.05 to 1.19) | −2 (−3 to 1) | −16 (−20 to 4) |
|
Zanamivir vs. standard care or placebo | 1.18 (0.81 to 1.72) | 1 (−1 to 2) | 4 (−4 to 15) | High |
Baloxavir marboxil vs. oseltamivir | 0.30 (0.06 to 1.47) | −2 (−2 to 1) | −12 (−16 to 8) |
|
Baloxavir marboxil vs. zanamivir | 0.21 (0.04 to 1.05) | −3 (−3 to 0) | −20 (−24 to 1) |
|
Oseltamivir vs. zanamivir | 0.68 (0.39 to 1.17) | −1 (−2 to 1) | −8 (−15 to 4) |
|
CI = confidence interval; NMA = network meta-analysis; SR = systematic review; vs. = versus.
Time to Alleviation of Influenza Symptoms
Time to alleviation of influenza symptoms was evaluated in 59 trials including 24,086 participants. The evidence network shows that a large proportion of the included trials compared oral oseltamivir or inhaled zanamivir to standard care or placebo. When compared to standard care or placebo, baloxavir marboxil was associated with the largest reduction in symptom duration, shortening the duration of symptoms measured by approximately 1 day (RD = −1.02 days; 95% CI, −1.41 days to −0.63 days; moderate certainty) (Table 6). Oseltamivir and zanamivir also reduced symptom duration to a lesser extent, by 0.75 days and 0.68 days respectively, with moderate certainty of evidence. Peramivir showed a comparable reduction (mean difference = −0.95 days), though the supporting evidence was of low certainty. In contrast, the combination of oseltamivir and zanamivir was shown to have increased the duration of symptoms, although this difference was not statistically significant and was based on low-certainty evidence. Direct comparisons between individual antivirals showed little to no meaningful differences in symptom duration.
What This Means
In 2024, the WHO used an MID of 1 day to guide the interpretation of influenza evidence for antivirals related to symptom duration.22,23 Evidence from the NMA demonstrated that most antivirals appear to shorten the symptomatic course of influenza by less than a day on average. Baloxavir marboxil may provide an important reduction in the time to alleviation of influenza symptoms. The combination of 2 antivirals did not improve efficacy and may even be less effective than antiviral monotherapy. Overall, the modest but consistent reduction in symptom duration may support the use of antivirals for patients seeking faster symptom resolution.
Table 6: Summary of Findings From the Landmark SR and NMA for Time to Alleviation of Influenza Symptoms
Comparison | NMA absolute risk difference, days (95% CI) | Certainty of evidence |
|---|---|---|
Baloxavir marboxil vs. standard care or placebo | −1.02 (−1.41 to −0.63) | Moderate |
Oseltamivir vs. standard care or placebo | −0.75 (−0.93 to −0.57) | Moderate |
Zanamivir vs. standard care or placebo | −0.68 (−0.93 to −0.43) | Moderate |
Peramivir vs. standard care or placebo | −0.95 (−1.28 to −0.62) | Low |
Oseltamivir combined with zanamivir vs. standard care or placebo | 1.36 (−0.07 to 2.78) | Low |
Baloxavir marboxil vs. oseltamivir | −0.27 (−0.68 to 0.14) | Moderate |
Baloxavir marboxil vs. zanamivir | −0.34 (−0.80 to 0.12) | Moderate |
Baloxavir marboxil vs. peramivir | −0.07 (−0.57 to 0.43) | Moderate |
Baloxavir marboxil vs. oseltamivir combined with zanamivir | −2.38 (−3.85 to −0.91) | Low |
Oseltamivir vs. zanamivir | −0.07 (−0.37 to 0.23) | Moderate |
Oseltamivir vs. peramivir | 0.20 (−0.12 to 0.52) | Moderate |
Oseltamivir vs oseltamivir combined with zanamivir | −2.67 (−4.12 to −1.22) | Moderate |
Peramivir vs. zanamivir | −0.27 (−0.67 to 0.13) | Moderate |
Oseltamivir combined with zanamivir vs. peramivir | 2.31 (0.86 to 3.76) | Low |
Oseltamivir combined with zanamivir vs. zanamivir | −0.16 (−2.01 to 1.69) | Very low |
CI = confidence interval; NMA = network meta-analysis; SR = systematic review; vs. = versus.
Emergence of Antiviral Resistance
As there were no relevant antiviral resistance outcomes reported in the standard care or placebo groups, the authors of the landmark SR with NMA pooled the prevalence rates of antiviral resistance rates for each intervention using meta-analyses of the proportion of actively treated patients in whom resistance occurred.
In 5 comparisons, resistance to antivirals was most observed in patients treated with baloxavir marboxil, with a pooled resistance prevalence of 9.97% (95% CI, 0.02% to 31.79%; low certainty). For peramivir, resistance was detected in 4.35% of treated individuals (95% CI, 0.07% to 12.66%; very low certainty). In contrast, oseltamivir was associated with a substantially lower pooled prevalence of resistance (0.42%; 95% CI, 0.00% to 3.06%; very low certainty). No resistance was observed in patients who received zanamivir (low certainty) or the combination of oseltamivir and zanamivir (low certainty), though sample sizes were small and associated CIs were wide. Due to the use of single-arm prevalence data and high heterogeneity across studies, these findings should be interpreted with caution (Table 7).
What This Means
Baloxavir marboxil may be associated with a higher likelihood of antiviral resistance emergence compared to other antivirals, but these findings are based on limited data and imprecise estimates. The true prevalence of antiviral resistance may be substantially higher or lower than documented in the landmark SR and NMA.
Table 7: Summary of Findings From the Landmark SR and NMA for Proportions of Patients With Antiviral Resistance
Antiviral | Studies reporting, N | Number of events | Number of individuals | Pooled prevalence (95% CI) | Certainty of evidence |
|---|---|---|---|---|---|
Baloxavir marboxil | 3 | 62 | 717 | 9.97 per 100 (0.02 to 31.79) | Low |
Oseltamivir | 7 | 14 | 579 | 0.42 per 100 (0.00 to 3.06) | Very low |
Peramivir | 1 | 2 | 46 | 4.35 per 100 (0.07 to 12.66) | Very low |
Zanamivir | 2 | 0 | 200 | 0 per 100 (0 to 11.66) | Low |
Oseltamivir combined with zanamivir | 1 | 0 | 12 | 0 per 100 (0 to 13.86) | Low |
CI = confidence interval; NMA = network meta-analysis; SR = systematic review.
Serious Adverse Events
SAEs were reported in 58 RCTs with 32,043 patients. None of the antivirals showed statistically significant increases in SAEs compared to placebo or to one another. Absolute RDs were mostly small (between −2 and 2 per 1,000 patients) (Table 8). The certainty of evidence ranged from moderate to very low depending on the comparison. Higher RDs for SAEs of 14 and 16 were observed when oseltamivir was combined with zanamivir, although these results were of low certainty and were not statistically significant.
In related additional analyses for AEs related to treatment (36 RCTs with 19,298 patients), baloxavir marboxil did not increase AEs related to treatment compared with standard care or placebo (high certainty). Oseltamivir likely increased AEs related to treatment (moderate certainty). In 49 trials with 22,868 patients, there was little to no difference in any AEs with baloxavir marboxil compared to placebo or standard care (high certainty). There was low certainty that inhaled zanamivir may not have resulted in an increase in total AEs compared with standard care or placebo, and data for oseltamivir were assessed to be of very low certainty (no difference).
What This Means
Across all antiviral drugs studied, there was no strong signal for increased risk of SAEs. Differences in SAE rates were generally small and none were statistically significant. This suggests that these medications do not increase SAEs and that monotherapy has broadly similar profiles when used for patients with influenza.
Table 8: Summary of Findings for Serious Adverse Events
Comparison | NMA absolute risk difference (per 1,000) (95% CI) | Certainty of evidence |
|---|---|---|
Baloxavir marboxil vs. standard care or placebo | 1 (−4 to 5) | Moderate |
Oseltamivir vs. standard care or placebo | 0 (−3 to 2) | Moderate |
Zanamivir vs. standard care or placebo | 2 (−1 to 6) | Low |
Peramivir vs. standard care or placebo | 0 (−7 to 6) | Low |
Oseltamivir combined with zanamivir vs. standard care or placebo | 16 (−4 to 36) | Low |
Baloxavir marboxil vs. oseltamivir | 1 (−4 to 5) | Moderate |
Baloxavir marboxil vs. oseltamivir combined with zanamivir | −15 (−36 to 5) | Very low |
Baloxavir marboxil vs. peramivir | 1 (−7 to 8) | Very low |
Baloxavir marboxil vs. zanamivir | −2 (−7 to 4) | Low |
Oseltamivir vs. oseltamivir combined with zanamivir | −16 (−36 to 4) | Low |
Oseltamivir vs. peramivir | 0 (−6 to 7) | Very low |
Oseltamivir vs. zanamivir | −2 (−6 to 2) | Low |
Oseltamivir combined with zanamivir vs. peramivir | 16 (−5 to 37) | Very low |
Oseltamivir combined with zanamivir vs. zanamivir | 14 (−7 to 34) | Very low |
Peramivir vs. zanamivir | −3 (−10 to 4) | Moderate |
CI = confidence interval; NMA = network meta-analysis; vs. = versus.
Subgroup Analyses
The landmark SR and NMA prespecified and explored several within-trial subgroup analyses. Specifically, the effects of zanamivir versus standard care or placebo were compared within subgroups defined by influenza virus type (seasonal or zoonotic) and by influenza diagnosis status (laboratory confirmed or suspected). Subgroup analyses were also conducted to examine age-related differences in treatment effects for baloxavir marboxil (for the outcome of hospitalization) and oseltamivir (for SAEs), comparing outcomes among infants, children, adolescents and adults, and older adults. A risk factor–based subgroup comparison was reported for zanamivir, with effect estimates stratified by baseline risk status. Mortality data for baloxavir marboxil were also presented by virus subtype and patient subgroup, although interpretation was limited by small sample sizes and low event rates.
Across all subgroup analyses, no statistically significant differences were detected. In addition, network meta-regression was used to explore whether variables such as mean age, proportion of influenza A cases, time from symptom onset to treatment, or influenza vaccination coverage modified the antiviral treatment effects. These variables only partially align with the subgroups of interest for the current PICO. Age was used as a continuous variable and populations considered to be at high risk for severe influenza were based on trial-level proportions. These analyses also yielded no evidence of significant subgroup effects.
Critically important subgroups, such as equity-denied populations and patients aged 85 years or older with comorbidities, were not considered, which may be due to a paucity of reported data within the included trials.
What This Means
The absence of significant subgroup effects suggests that there is no evidence at this time to conclude that the effectiveness or safety of antivirals meaningfully differs across the identified patient subgroups. This highlights the need for larger, well-powered trials to explore potential differential treatment effects, especially in underserved and understudied populations.
Findings of the RCT
Time to Alleviation of Influenza Symptoms
The RCT by Qui and colleagues reported 3 symptom-related outcomes including fever subsidence time, cough improvement time, and sore throat improvement time based on a follow-up time of 5 days.21 Results showed that both interventions improved symptoms in approximately 1 to 2 days, and there was no significant difference in time to alleviation of symptoms when baloxavir marboxil was compared with oseltamivir (Table 9). There was also no significant difference in the total effective rate between intervention groups (99% vs. 98%; P > 0.05).
What This Means
In this trial context, baloxavir marboxil and oseltamivir are similarly effective in alleviating influenza symptoms. These results are unlikely to change any of the findings from the landmark SR and NMA.
Table 9: Summary of Findings From the RCT for Time to Alleviation of Individual Influenza Symptoms
Outcome | Baloxavir marboxil | Oseltamivir | ||
|---|---|---|---|---|
Number of patients whose data were analyzed | Time to improvement in days, mean (SD) | Number of patients whose data were analyzed | Time to improvement in days, mean (SD) | |
Fever subsidence timea | 100 | 1.54 (0.66) | 100 | 1.67 (0.71) |
Cough improvement timeb | 100 | 2.26 (0.91) | 100 | 2.30 (0.90) |
Sore throat improvement timec | 100 | 2.06 (0.86) | 100 | 2.09 (0.83) |
RCT = randomized controlled trial; SD = Standard deviation.
aFever subsidence or disappearance time (time to fever resolution was defined as the time from the start of treatment until the body temperature was lower than 37°C for at least 24 hours).
bCough improvement or disappearance time.
cSore throat improvement or disappearance time.
Emergence of Antiviral Resistance
Qui and colleagues detected resistance mutations in polymerase acidic protein variants in 9.7% of 100 patients following baloxavir marboxil treatment. No data were reported for the oseltamivir group for this outcome and no rationale was provided.
What This Means
Findings for baloxavir marboxil in the trial by Qui and colleagues are consistent with the findings of the landmark SR and NMA.
Serious Adverse Events
No SAEs occurred in patients receiving baloxavir marboxil or oseltamivir after 5 days of follow-up.
What This Means
Findings suggest that both antivirals were well tolerated in the short term. The absence of SAEs in a single trial with limited duration and sample size does not rule out the possibility of rare or delayed harms. These results are unlikely to change any of the findings from the landmark SR and NMA.
Subgroup Analyses
No subgroups of interest were reported in the RCT.
What This Means
It is not possible to determine whether the effects of baloxavir marboxil or oseltamivir differ across important patient groups. Therefore, the findings should be interpreted as reflecting the average treatment effects in the overall study population.
Outcomes for Which No Evidence Was Identified
No relevant evidence regarding withdrawals due to AEs or regarding human-to-human transmission of the influenza virus was identified in the landmark SR and NMA or the additional RCT.
What This Means
It is not possible to draw conclusions about the tolerability of antivirals in patients with influenza based on treatment discontinuation or any documented impact on reducing transmission risk. These are important gaps in this evidence summary.
Limitations
While the landmark SR and NMA15 was conducted in a rigorous manner, there are some limitations in the literature that need to be considered. Current evidence is lacking on peramivir for hospitalization and only 1 RCT identified by the landmark SR and NMA has investigated the efficacy of the combination of eligible antiviral drugs.15 The combined drugs were both neuraminidase inhibitors, rather than different classes of drugs, which is a limitation of our findings. Furthermore, outcomes of interest including transmission of virus and withdrawal due to AEs were not reported in the SR and NMA or the newer RCT published in 2024. Due to limited RCT subgroup data in the landmark SR and NMA, the authors were only able to conduct subgroup analyses for select outcomes and interventions of interest. In addition, authors did not report results for subgroups such as those with neurologic disease, malignancy, or diabetes or equity-deserving populations (e.g., Indigenous populations), which were of interest for this report. These subgroup analyses were also lacking in the RCT found in the updated search. This gap restricts our ability to conclude whether the findings adequately reflect the unique health needs, cultural contexts, and structural barriers faced by First Nations, Inuit, and Métis communities and by other underserved and understudied communities. As part of the organizational commitment of Canada’s Drug Agency to reconciliation and to inclusion, diversity, equity, and accessibility, we know it is important to consider and learn from Indigenous Peoples and to include other diverse perspectives in our work. We also recognize that the research team consists of settler researchers, and we come to this work with our individual privileges and biases. Understanding the perspectives and priorities of Indigenous Peoples and other underserved groups as they relate to influenza can support informed health care decision-making.
For some patient-important outcomes (e.g., mortality, hospitalization), event rates were often very low. No additional data on the consistency of the methodology for the measurement of outcomes were reported. Authors of the landmark SR and NMA hypothesized that there would be a reduced treatment effect in patients with suspected influenza compared to those with confirmed influenza; however, sensitivity analyses including patients with confirmed influenza did not differ from the primary analyses. Many included studies may lack sufficient power to detect these outcomes, and even pooled analyses may not provide enough statistical power for a reliable assessment of antiviral treatments. Additionally, while the authors of the landmark SR and NMA assessed the emergence of antiviral resistance, it was a lower-priority outcome. While the emergence of antiviral resistance with baloxavir marboxil may be a concern, inferring antiviral resistance from the data presented remains challenging due to infrequent reporting, and the clinical relevance of the different resistant variants remains uncertain.
There was substantial heterogeneity among the included studies in the NMA, including variations in patient populations, timing of treatment initiation relative to symptom onset, drug dosages, and treatment durations. It is difficult to interpret the evidence presented for different contexts or settings based on the data presented, and this could affect how results are interpreted and applied in practice. Although the authors of the landmark SR and NMA endeavoured to consider the impact of heterogeneity on treatment effects, not all analyses were possible and this complicates the interpretation of the findings. Likewise, some trials were assessed to be at an unclear or high risk of bias due to limitations in blinding or outcome reporting, and it is unclear how this may influence findings. The evidence for some antiviral drugs (e.g., peramivir) was limited, and for some routes of administration (e.g., IV zanamivir) there was no evidence available. The WHO estimates for meaningful differences were noted to be lacking empirical evidence. As such, for outcomes such as symptom duration, different values may be placed on the importance of the differences noted. The range by which symptoms were shortened may be, based on clinical input, more clinically meaningful in populations at high risk for progression to severe influenza, for whom even a small improvement in symptom duration can prevent complications.
Evidence for some antivirals, and for specific patient subgroups, is still emerging or unclear. There are noted evidence gaps in the identified RCTs related to transmission outcomes and for population subgroups identified in the PICO who may be at most risk for progression to severe disease. Clinicians and patients should take these factors into account when considering the findings and their relevance to different clinical contexts.
Conclusions and Implications for Decision- or Policy-Making
Only antiviral treatments approved for use in Canada were considered in this report despite the SR and NMA’s inclusion of those not approved in Canada.
The landmark SR and NMA provides a robust synthesis of available RCT evidence for the benefits and harms of antiviral treatments for influenza currently approved for use in Canada. The findings show that baloxavir marboxil, oseltamivir, peramivir, and zanamivir are associated with modest reductions in symptom duration, which are generally less than 1 day, compared to standard care or placebo. Among the antiviral drugs, baloxavir marboxil may offer the greatest reduction in time to symptom resolution, though differences between drugs are small and of uncertain clinical importance.
For more severe outcomes, including mortality and hospitalization, none of the antivirals demonstrated a statistically significant benefit compared to placebo or to one another. However, comparisons of baloxavir marboxil in patients who may be considered at high risk for severe outcomes had confidence intervals that included potentially clinically meaningful effects, although the certainty of evidence was generally low. These findings suggest that while antiviral treatment is unlikely to prevent death or hospital admission in most patients, certain patients may still benefit. Unfortunately, the paucity of data for certain populations and treatments prevented comprehensive assessment. Baloxavir marboxil was associated with a higher observed prevalence of resistance mutations compared to other antivirals, though estimates were imprecise and based on a limited number of studies. The risk of SAEs was low across all agents, with no consistent signal for harm in comparisons to placebo or among the antivirals. No consistent subgroup effects were identified across age groups, influenza types, diagnostic certainty, or patient risk factors. Similarly, treatment effects did not vary significantly by time to treatment initiation, influenza A prevalence, or prior vaccination status. These findings suggest that the relative benefits and harms of antiviral therapies are broadly applicable across diverse patient populations and clinical settings, supporting a generalizable approach to decision-making rather than having to tailor decisions or policy based on these characteristics, although data were limited for some subgroups.
Overall, the SR and NMA supports the conclusion that antiviral treatments provide small to modest benefit in terms of symptom alleviation and are generally safe while underscoring the importance of ongoing resistance surveillance and the need for more targeted evidence for populations at high risk for severe influenza and for key patient subgroups that would help inform policy.
The findings of the additional RCT published in 2024 for the limited number of outcomes reported are consistent with the results of the landmark SR and NMA and are unlikely to influence the findings. In this short-term trial, baloxavir marboxil and oseltamivir showed comparable effectiveness in alleviating influenza symptoms, with no statistically significant differences in time to fever, cough, or sore throat resolution, nor in total clinical response rates. The absence of SAEs over the 5 days of patient follow-up suggests short-term tolerability, though rare or delayed harms cannot be excluded.
The antiviral stockpiles for NESS and NAS were last updated in 2017, before baloxavir marboxil was authorized for use in Canada in 2020. At that time, peramivir had recently received authorization by Health Canada and was not considered in the review of neuraminidase inhibitors conducted. Currently, the WHO has downgraded oseltamivir on its Essential Medicines List and now advises that national stockpiles include antivirals with diverse mechanisms of action.14 Decisions for stockpiling antivirals should take into account the clinical effectiveness and safety of available antiviral drugs for preventing severe influenza outcomes, especially in populations at high risk for severe influenza. Additionally, broader implications for public health and for health systems related to the duration and severity of symptoms and health care utilization must be considered. More importantly, the potential risk of developing antiviral resistance could also compromise future treatment effectiveness. The evidence in this Rapid Review revealed that baloxavir marboxil may offer modest benefits for patients considered to be at high risk for severe influenza; however, the potential for associated resistance warrants careful stewardship. A balanced and diversified stockpile of antiviral medications, which also considers supply and implementation logistics, may be warranted instead of reliance on any single drug.
Authors and Contributors
Authors
Shannon E. Kelly contributed to the conceptualization, scoping, and methodology of the review; provided research oversight; contributed to validation and formal analysis; reviewed the original report and provided substantial revisions; and drafted sections of the final report.
Xiaoqin Wang led the review and design; refined the scope; and coordinated and participated in the literature search, screening, and data extraction. Synthesized the data and wrote the original draft report.
Annie Bai was involved in clarifying the study scope and analytic approach; contributed to literature screening, critical appraisal, and data extraction or verification for all included studies; summarized and interpreted the updated primary study and drafted the corresponding section of the report; and reviewed the full report for accuracy, coherence, and consistency.
Shuching Hsieh conducted literature screening and study selection and provided methodological feedback.
Becky Skidmore designed and executed search strategies in consultation with the review team (data acquisition), provided search documentation, and wrote literature search methods.
Melissa Brouwers contributed to supervision, funding acquisition, editing, reviewing, and validation.
George A. Wells contributed to supervision, funding acquisition, editing, reviewing, validation, and methodology.
Contributors
Clinical Experts
These individuals kindly provided comments on this report:
Giorgia Sulis, MD, PhD
Assistant Professor and Canada Research Chair in Communicable Diseases Epidemiology
School of Epidemiology and Public Health, Faculty of Medicine, University of Ottawa
Darrell Tan, MD, FRCPC, PhD
Clinician-Scientist
St. Michael’s Hospital, Unity Health Toronto
Additional Acknowledgements
We thank Kaitryn Campbell, MSc, MLIS (Campbell Information Consulting, ON) for peer review of the MEDLINE search strategy.
We thank Nazmun Nahar for her assistance in retrieving full-text records during screening and selection.
Conflicts of Interest
George A. Wells disclosed the following:
Data Safety Monitoring Board Member
VBI Vaccines Inc. (2020-current) — CORONAVIRUS vaccine
Design and Analysis Advice for Preparation of FDA Submission
Thermedical (2021-current) — ablation system and catheter needle
VBI Vaccines Inc. (2020-current) — CORONAVIRUS vaccine
Darrell Tan disclosed the following:
Research Funding or Grants
Gilead — HIV PrEP and PEP
Glaxo Smith Kine – Antiretroviral Therapy for HIV
International Health Technology Assessment Agency Activities
CIHR Canadian HIV Trials Network — Canadian Guidelines on HIV pre- and post- exposure prophylaxis 2017 and current (2022–2024)
NACI — NACI guidance on Imvamune vaccine for mpox (2023–2024)
No other conflicts of interest were declared.
References
1.Health Canada. Flu (influenza): For health professionals. Government of Canada. 2024. Accessed 10 January 2025. https://www.canada.ca/en/public-health/services/diseases/flu-influenza/health-professionals.html
2.Halsey E, ed. CDC Yellow Book 2026: Health Information for International Travel. Oxford University Press; 2025.
3.Gaitonde DY, Moore FC, Morgan MK. Influenza: Diagnosis and Treatment. American Family Physician. 2019;100(12):751-758. PubMed
4.Culbert I. The Cost of Influenza is Nothing to Sneeze At. Canadian Public Health Association. 2019. Accessed 10 January 2025. https://cpha.ca/cost-influenza-nothing-sneeze
5.Schanzer DL, Sevenhuysen C, Winchester B, Mersereau T. Estimating influenza deaths in Canada, 1992–2009. PloS One. 2013;8(11):e80481. PubMed
6.Ng C, Ye L, Noorduyn SG, et al. Resource utilization and cost of influenza requiring hospitalization in Canadian adults: A study from the serious outcomes surveillance network of the Canadian Immunization Research Network. Influenza Other Respir Viruses. 2018;12(2):232-240. doi: 10.1111/irv.12521 PubMed
7.Public Health Agency of Canada. Guidance on human health issues related to avian influenza in Canada. Government of Canada. 2025. Accessed 10 January 2025. https://www.canada.ca/en/public-health/services/publications/diseases-conditions/guidance-human-health-issues-avian-influenza.html
8.Papenburg J, Mubareka S, Allen UD, et al. Guidance on the use of antiviral agents for the 2019-2020 influenza season. J Assoc Med Microbiol Infect Dis Can. 2020;5(2):57-60. doi: 10.3138/jammi.2020-01-13 PubMed
9.Harrison R, Mubareka S, Papenburg J, et al. AMMI Canada 2023 update on influenza: Management and emerging issues. J Assoc Med Microbiol Infect Dis Can. 2023;8(3):176-185. doi: 10.3138/jammi-2023-07-12 PubMed
10.Product Monograph: TAMIFLU (oseltamivir capsule/powder for oral suspension). Hoffmann-La Roche Limited. 2017. Accessed 10 January 2025. https://pdf.hres.ca/dpd_pm/00038482.PDF
11.Product Monograph: RELENZA (zanamivir dry powder for inhalation). GlaxoSmithKline Inc. 2018. Accessed 10 January 2025. https://health-products.canada.ca/dpd-bdpp/info?lang=eng&code=64454
12.Public Health Agency of C. Antiviral Annex: Canadian Pandemic Influenza Preparedness – Planning Guidance for the Health Sector. 2025. 2025. Accessed 22 May 2025. https://www.canada.ca/en/public-health/services/flu-influenza/canadian-pandemic-influenza-preparedness-planning-guidance-health-sector/the-use-of-antiviral-drugs-during-a-pandemic.html
13.Product Monograph: RAPIVAB (peramivir for injection). BioCryst Pharmaceuticals Inc. 2018. Accessed 10 January 2025. https://pdf.hres.ca/dpd_pm/00042945.PDF
14.Ebell MH. WHO downgrades status of oseltamivir. BMJ. 2017;358:j3266. doi: 10.1136/bmj.j3266 PubMed
15.Gao Y, Zhao Y, Liu M, et al. Antiviral Medications for Treatment of Nonsevere Influenza: A Systematic Review and Network Meta-Analysis. JAMA Internal Medicine. 2025;185(3):293-301. doi: 10.1001/jamainternmed.2024.7193 PubMed
16.McGowan J, Sampson M, Salzwedel DM, Cogo E, Foerster V, Lefebvre C. PRESS Peer Review of Electronic Search Strategies: 2015 Guideline Statement. J Clin Epidemiol. 2016;75:40-46. doi: 10.1016/j.jclinepi.2016.01.021 PubMed
17.DistillerSR: Systematic Review Software 10 January, 2025. Accessed 10 January 2025. https://www.distillersr.com/. Ottawa, Ontario, Canada.
18.Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. doi: 10.1136/bmj.j4008 PubMed
19.Jansen JP, Trikalinos T, Cappelleri JC, et al. Indirect treatment comparison/network meta-analysis study questionnaire to assess relevance and credibility to inform health care decision making: an ISPOR-AMCP-NPC Good Practice Task Force report. Value in Health. 2014;17(2):157-173. doi: 10.1016/j.jval.2014.01.004 PubMed
20.Guyatt G, Busse, J.W. Methods Commentary: Risk of Bias in Randomized Trials. Clarity Group via Evidence Partners. 2025. Accessed 10 January 2025. www.evidencepartners.com/resources/methodologicalresources/
21.Qiu C, Cheng F, Ye X, et al. Study on the clinical efficacy and safety of baloxavir marboxil tablets in the treatment of influenza A. Frontiers in Medicine (Lausanne). 2024;11:1339368. doi: 10.3389/fmed.2024.1339368 PubMed
22.World Health Organization. Clinical practice guidelines for influenza. 2024. Accessed 9 April 2025. https://www.ncbi.nlm.nih.gov/pubmed/39374347
23.Meixner J, Nussbaumer-Streit B, Sommer I. WHO clinical practice guidelines for influenza: an update. Gesundheitswesen (Bundesverband der Arzte des Offentlichen Gesundheitsdienstes (Germany)). 2025;87(7):484-486. doi: 10.1055/a-2571-3357
Appendix 1: Strategy of the Updating Search
Please note that this appendix has not been copy-edited.
Ovid Multifile
Database: Embase Classic+Embase <1947 to 2025 January 07>, Ovid MEDLINE(R) ALL <1946 to January 06, 2025>, EBM Reviews - Cochrane Central Register of Controlled Trials <December 2024>
Search Strategy:
--------------------------------------------------------------------------------
1 Influenza, Human/ (108304)
2 (influenza* or flu or flus or grippe).tw,kw,kf. (370572)
3 exp Influenza A virus/ (76576)
4 exp Alphainfluenzavirus/ (75679)
5 exp Betainfluenzavirus/ (7925)
6 (alphainfluenzavirus* or betainfluenzavirus* or FLUBV).tw,kw,kf. (79)
7 (H5N1 or HPAI or txid102793 or H5N6 or txid329376 or H7N9 or txid333278 or H1N1 or txid114727 or H2N2 or txid114729).tw,kw,kf. (69432)
8 or/1-7 [INFLUENZA A & B] (394847)
9 (baloxavir* or xofluza* or 4G86Y4JT3F or 505CXM6OHG or 505CXM6OHG or rg 6152 or rg6152 or "s 033188" or s033188 or s 33188 or s33188 or 1985605-59-1).tw,kw,kf,rn. (1328)
10 Oseltamivir/ (19193)
11 (oseltamivir* or ebilfumin* or en 241104 or en241104 or enzamir* or fluvir* or gs 4071 or gs4071 or gs 4104 or gs4104 or gs4104002 or "hgp 0919" or hgp0919 or hip 1403 or hip1403 or kewei* or "ro 64 0796" or ro 640796 or ro640796 or ro640796002 or segosana* or tamiflu* or tamivil* or 20O93L6F9H or 196618-13-0).tw,kw,kf,rn. (22901)
12 (peramivir* or bcx 1812 or bcx1812 or jnj 2 or jnj2 or peramiflu* or rapiacta* or rapivab* or rwj 270201 or rwj270201 or 330600-85-6).tw,kw,kf,rn. (2393)
13 Zanamivir/ (6601)
14 (zanamivir* or awp 09vdb s or awp09vdbs or dectova* or gg 167 or gg167 or gr 121167 or gr121167 or gr 121167x or gr121167x or relenza* or zanamivi* or L6O3XI777 or 139110-80-8).tw,kw,kf,rn. (7547)
15 ((neuraminidase or sialidase) adj (inhibit* or block*)).tw,kw,kf. (6933)
16 ((NAI or NAIs) and neuraminidase).tw,kw,kf. (987)
17 Antiviral Agents/ (200818)
18 (antiviral? or anti-viral? or antivirus$2 or anti-virus$2).tw,kw,kf. (346534)
19 ((viral or virus$2) adj (block* or inhibit* or repress*)).tw,kw,kf. (7262)
20 (vir#static* or virucid*).tw,kw,kf. (6222)
21 or/9-20 [ANTIVIRALS] (463995)
22 8 and 21 [INFLUENZA - ANTIVIRALS] (49391)
23 exp Animals/ not Humans/ (17981065)
24 22 not 23 [ANIMAL-ONLY REMOVED] (36715)
25 (comment or editorial or letter or news or newspaper article).pt. (4741489)
26 24 not 25 [OPINION PIECES REMOVED] (35168)
27 (Randomized Controlled Trial or Controlled Clinical Trial or Pragmatic Clinical Trial or Equivalence Trial or Clinical Trial, Phase III).pt. (725574)
28 exp Randomized Controlled Trials as Topic/ (521998)
29 exp Controlled Clinical Trials as Topic/ (537920)
30 Random Allocation/ (229784)
31 Double-Blind Method/ (561784)
32 Single-Blind Method/ (118244)
33 Placebos/ (439913)
34 Control Groups/ (126277)
35 (random* or sham or placebo*).ti,ab,hw,kf. (6309313)
36 ((singl* or doubl*) adj (blind* or dumm* or mask*)).ti,ab,hw,kf. (1113081)
37 ((tripl* or trebl*) adj (blind* or dumm* or mask*)).ti,ab,hw,kf. (8170)
38 (control* adj3 (study or studies or trial* or group*)).ti,ab,kf. (4038715)
39 (nonrandom* or non random* or non-random* or quasi-random* or quasirandom*).ti,ab,hw,kf. (150269)
40 allocated.ti,ab,hw,kf. (299347)
41 ((open label or open-label) adj5 (study or studies or trial*)).ti,ab,hw,kf. (210805)
42 ((equivalence or superiority or non-inferiority or noninferiority) adj3 (study or studies or trial*)).ti,ab,hw,kf. (54004)
43 (pragmatic study or pragmatic studies).ti,ab,hw,kf. (2213)
44 ((pragmatic or practical) adj3 trial*).ti,ab,hw,kf. (27554)
45 ((quasiexperimental or quasi-experimental) adj3 (study or studies or trial*)).ti,ab,hw,kf. (44725)
46 (phase adj3 (III or "3") adj3 (study or studies or trial*)).ti,hw,kf. (248531)
47 or/27-46 [RCT FILTER - CDA] (8514278)
48 26 and 47 [INFLUENZA - ANTIVIRALS - RCTS] (4087)
49 48 use medall [MEDLINE RECORDS] (1301)
50 influenza/ (152362)
51 (influenza* or flu or flus or grippe).tw,kw,kf. (370572)
52 exp influenza A/ (37447)
53 influenza B/ (5024)
54 exp influenzavirus A/ (76863)
55 exp influenzavirus B/ (8278)
56 (alphainfluenzavirus* or betainfluenzavirus* or FLUBV).tw,kw,kf. (79)
57 (H5N1 or HPAI or txid102793 or H5N6 or txid329376 or H7N9 or txid333278 or H1N1 or txid114727 or H2N2 or txid114729).tw,kw,kf. (69432)
58 or/50-57 [INFLUENZA A & B] (410629)
59 baloxavir marboxil/ (490)
60 (baloxavir* or xofluza* or 4G86Y4JT3F or 505CXM6OHG or 505CXM6OHG or rg 6152 or rg6152 or "s 033188" or s033188 or s 33188 or s33188 or 1985605-59-1).tw,kw,kf,rn. (1328)
61 oseltamivir/ (19193)
62 (oseltamivir* or ebilfumin* or en 241104 or en241104 or enzamir* or fluvir* or gs 4071 or gs4071 or gs 4104 or gs4104 or gs4104002 or "hgp 0919" or hgp0919 or hip 1403 or hip1403 or kewei* or "ro 64 0796" or ro 640796 or ro640796 or ro640796002 or segosana* or tamiflu* or tamivil* or 20O93L6F9H or 196618-13-0).tw,kw,kf,rn. (22901)
63 peramivir/ (1659)
64 (peramivir* or bcx 1812 or bcx1812 or jnj 2 or jnj2 or peramiflu* or rapiacta* or rapivab* or rwj 270201 or rwj270201 or 330600-85-6).tw,kw,kf,rn. (2393)
65 zanamivir/ (6601)
66 (zanamivir* or awp 09vdb s or awp09vdbs or dectova* or gg 167 or gg167 or gr 121167 or gr121167 or gr 121167x or gr121167x or relenza* or zanamivi* or L6O3XI777 or 139110-80-8).tw,kw,kf,rn. (7547)
67 sialidase inhibitor/ (3081)
68 ((neuraminidase or sialidase) adj (inhibit* or block*)).tw,kw,kf. (6933)
69 ((NAI or NAIs) and neuraminidase).tw,kw,kf. (987)
70 antivirus agent/ (107707)
71 (antiviral? or anti-viral? or antivirus$2 or anti-virus$2).tw,kw,kf. (346534)
72 ((viral or virus$2) adj (block* or inhibit* or repress*)).tw,kw,kf. (7262)
73 (vir#static* or virucid*).tw,kw,kf. (6222)
74 or/59-73 [ANTIVIRALS] (417245)
75 58 and 74 [INFLUENZA - ANTIVIRALS] (49652)
76 (exp animal/ or exp animal model/ or exp animal experiment/ or nonhuman/ or exp vertebrate/) not (exp human/ or exp human experiment/) (13719242)
77 75 not 76 [ANIMAL-ONLY REMOVED] (40240)
78 (editorial or letter).pt. (4205801)
79 77 not 78 [OPINION PIECES REMOVED] (38396)
80 conference abstract.pt. (5354305)
81 79 not 80 [CONFERENCE ABSTRACTS REMOVED] (35582)
82 exp randomized controlled trial/ (1499574)
83 exp "randomized controlled trial (topic)"/ (288428)
84 controlled clinical trial/ (571335)
85 "controlled clinical trial (topic)"/ (13708)
86 randomization/ (235019)
87 double blind procedure/ (230643)
88 single blind procedure/ (57755)
89 placebo/ (433568)
90 control group/ (126277)
91 (random* or sham or placebo*).ti,ab,hw,kf. (6309313)
92 ((singl* or doubl*) adj (blind* or dumm* or mask*)).ti,ab,hw,kf. (1113081)
93 ((tripl* or trebl*) adj (blind* or dumm* or mask*)).ti,ab,hw,kf. (8170)
94 (control* adj3 (study or studies or trial* or group*)).ti,ab,kf. (4038715)
95 (nonrandom* or non random* or non-random* or quasi-random* or quasirandom*).ti,ab,hw,kf. (150269)
96 allocated.ti,ab,hw,kf. (299347)
97 ((open label or open-label) adj5 (study or studies or trial*)).ti,ab,hw,kf. (210805)
98 ((equivalence or superiority or non-inferiority or noninferiority) adj3 (study or studies or trial*)).ti,ab,hw,kf. (54004)
99 (pragmatic study or pragmatic studies).ti,ab,hw,kf. (2213)
100 ((pragmatic or practical) adj3 trial*).ti,ab,hw,kf. (27554)
101 ((quasiexperimental or quasi-experimental) adj3 (study or studies or trial*)).ti,ab,hw,kf. (44725)
102 (phase adj3 (III or "3") adj3 (study or studies or trial*)).ti,hw,kf. (248531)
103 or/82-102 [RCT FILTER - CDA] (8639991)
104 81 and 103 [INFLUENZA - ANTIVIRALS - RCTS] (4521)
105 104 use emczd [EMBASE RECORDS] (2318)
106 Influenza, Human/ (108304)
107 (influenza* or flu or flus or grippe).ti,ab,kw. (369247)
108 exp Influenza A virus/ (76576)
109 exp Alphainfluenzavirus/ (75679)
110 exp Betainfluenzavirus/ (7925)
111 (alphainfluenzavirus* or betainfluenzavirus* or FLUBV).ti,ab,kw. (79)
112 (H5N1 or HPAI or txid102793 or H5N6 or txid329376 or H7N9 or txid333278 or H1N1 or txid114727 or H2N2 or txid114729).ti,ab,kw. (69114)
113 or/106-112 [INFLUENZA A & B] (393735)
114 (baloxavir* or xofluza* or 4G86Y4JT3F or 505CXM6OHG or 505CXM6OHG or rg 6152 or rg6152 or "s 033188" or s033188 or s 33188 or s33188 or 1985605-59-1).ti,ab,kw. (937)
115 Oseltamivir/ (19193)
116 (oseltamivir* or ebilfumin* or en 241104 or en241104 or enzamir* or fluvir* or gs 4071 or gs4071 or gs 4104 or gs4104 or gs4104002 or "hgp 0919" or hgp0919 or hip 1403 or hip1403 or kewei* or "ro 64 0796" or ro 640796 or ro640796 or ro640796002 or segosana* or tamiflu* or tamivil* or 20O93L6F9H or 196618-13-0).ti,ab,kw. (12502)
117 (peramivir* or bcx 1812 or bcx1812 or jnj 2 or jnj2 or peramiflu* or rapiacta* or rapivab* or rwj 270201 or rwj270201 or 330600-85-6).ti,ab,kw. (1275)
118 Zanamivir/ (6601)
119 (zanamivir* or awp 09vdb s or awp09vdbs or dectova* or gg 167 or gg167 or gr 121167 or gr121167 or gr 121167x or gr121167x or relenza* or zanamivi* or L6O3XI777 or 139110-80-8).ti,ab,kw. (3469)
120 ((neuraminidase or sialidase) adj (inhibit* or block*)).ti,ab,kw. (6573)
121 ((NAI or NAIs) and neuraminidase).ti,ab,kw. (982)
122 Antiviral Agents/ (200818)
123 (antiviral? or anti-viral? or antivirus$2 or anti-virus$2).ti,ab,kw. (339030)
124 ((viral or virus$2) adj (block* or inhibit* or repress*)).ti,ab,kw. (6964)
125 (vir#static* or virucid*).ti,ab,kw. (6220)
126 or/114-125 [ANTIVIRALS] (458076)
127 113 and 126 [INFLUENZA - ANTIVIRALS] (48658)
128 conference proceeding.pt. (250802)
129 127 not 128 [CONFERENCE ABSTRACTS REMOVED] (48567)
130 129 use cctr [CENTRAL RECORDS] (1218)
131 49 or 105 or 130 [ALL DATABASES] (4837)
132 remove duplicates from 131 (3211) [TOTAL UNIQUE RECORDS]
133 132 use medall [MEDLINE UNIQUE RECORDS] (1293)
134 132 use emczd [EMBASE UNIQUE RECORDS] (1294)
135 132 use cctr [CENTRAL UNIQUE RECORDS] (624)
***************************
PubMed
(MEDLINE records removed)
Table 10: PubMed Search Strategy
Set # | Query | Filters | Results |
|---|---|---|---|
33 | #31 NOT #32 | 245 | |
32 | #26 AND #30 | MEDLINE | 2,027 |
31 | #26 AND #30 | 2,272 | |
30 | #28 OR #29 | 4,755,469 | |
29 | "phase 3 study"[tiab:~3] OR "phase 3 studies"[tiab:~3] OR "phase 3 trial"[tiab:~3] OR "phase 3 trials"[tiab:~3] OR "phase III study"[tiab:~3] OR "phase III studies"[tiab:~3] OR "phase III trial"[tiab:~3] OR "phase III trials"[tiab:~3] | 58,593 | |
28 | "Randomized Controlled Trial"[pt] OR "Controlled Clinical Trial"[pt] OR "Pragmatic Clinical Trial"[pt] OR "Equivalence Trial"[pt] OR "Clinical Trial, Phase III"[pt] OR "Randomized Controlled Trials as Topic"[mh] OR "Controlled Clinical Trials as Topic"[mh] OR "Random Allocation"[mh] OR "Double-Blind Method"[mh] OR "Single-Blind Method"[mh] OR Placebos[Mesh:NoExp] OR "Control Groups"[mh] OR (random*[tiab] OR sham[tiab] OR placebo*[tiab]) OR ((singl*[tiab] OR doubl*[tiab]) AND (blind*[tiab] OR dumm*[tiab] OR mask*[tiab])) OR ((tripl*[tiab] OR trebl*[tiab]) AND (blind*[tiab] OR dumm*[tiab] OR mask*[tiab])) OR (control*[tiab] AND (study[tiab] OR studies[tiab] OR trial*[tiab] OR group*[tiab])) OR (Nonrandom*[tiab] OR "non random*"[tiab] OR "non-random*"[tiab] OR "quasi-random*"[tiab] OR quasirandom*[tiab]) OR allocated[tiab] OR (("open label"[tiab] OR "open-label"[tiab]) AND (study[tiab] OR studies[tiab] OR trial*[tiab])) OR ((equivalence[tiab] OR superiority[tiab] OR "non-inferiority"[tiab] OR noninferiority[tiab]) AND (study[tiab] OR studies[tiab] OR trial*[tiab])) OR ("pragmatic study"[tiab] OR "pragmatic studies"[tiab]) OR ((pragmatic[tiab] OR practical[tiab]) AND trial*[tiab]) OR ((quasiexperimental[tiab] OR "quasi-experimental"[tiab]) AND (study[tiab] OR studies[tiab] OR trial*[tiab])) | 4,735,856 | |
27 | Randomized Controlled Trial[Publication Type] OR Controlled Clinical Trial[Publication Type] OR Pragmatic Clinical Trial[Publication Type] OR Equivalence Trial[Publication Type] OR Clinical Trial, Phase III[Publication Type] | 724,991 | |
26 | #24 NOT #25 | 15,860 | |
25 | comment[Publication Type] OR editorial[Publication Type] OR letter[Publication Type] OR news[Publication Type] OR newspaper article[Publication Type] | 2,528,159 | |
24 | #22 NOT #23 | 16,762 | |
23 | Animals[mesh] NOT Humans[mesh] | 5,294,550 | |
22 | #8 AND #21 | 19,743 | |
21 | #9 OR #10 OR #11 OR #12 OR #13 OR #14 OR #15 OR #16 OR #17 OR #18 OR #19 OR #20 | 202,985 | |
20 | virostatic*[Title/Abstract] OR virucid*[Title/Abstract] OR virustatic*[Title/Abstract] | 2,751 | |
19 | viral block*[Title/Abstract] OR viral inhibitor*[Title/Abstract] OR viral repress*[Title/Abstract] OR virus block*[Title/Abstract] OR virus inhibitor*[Title/Abstract] OR virus repress*[Title/Abstract] | 1,280 | |
18 | antiviral[Title/Abstract] OR antivirals[Title/Abstract] OR "anti-viral"[Title/Abstract] OR "anti-virals"[Title/Abstract] OR antivirus*[Title/Abstract] OR anti-virus*[Title/Abstract] | 143,326 | |
17 | "Antiviral Agents"[mesh:noexp] | 105,662 | |
16 | (NAI[Title/Abstract] OR NAIs[Title/Abstract]) AND neuraminidase[Title/Abstract] | 439 | |
15 | neuraminidase inhibit*[Title/Abstract] OR neuraminidase block*[Title/Abstract] OR sialidase inhibit*[Title/Abstract] OR sialidase block*[Title/Abstract] | 3,864 | |
14 | zanamivir*[Title/Abstract] OR awp 09vdb s[Title/Abstract] OR awp09vdbs[Title/Abstract] OR dectova*[Title/Abstract] OR gg 167[Title/Abstract] OR gg167[Title/Abstract] OR gr 121167[Title/Abstract] OR gr121167[Title/Abstract] OR gr 121167x[Title/Abstract] OR gr121167x[Title/Abstract] OR relenza*[Title/Abstract] OR zanamivi*[Title/Abstract] OR L6O3XI777[Title/Abstract] OR 139110-80-8[Title/Abstract] | 1,512 | |
13 | Zanamivir[mesh] | 1,115 | |
12 | peramivir*[Title/Abstract] OR bcx 1812[Title/Abstract] OR bcx1812[Title/Abstract] OR jnj 2[Title/Abstract] OR jnj2[Title/Abstract] OR peramiflu*[Title/Abstract] OR rapiacta*[Title/Abstract] OR rapivab*[Title/Abstract] OR rwj 270201[Title/Abstract] OR rwj270201[Title/Abstract] OR 330600-85-6[Title/Abstract] | 2,811 | |
11 | oseltamivir*[Title/Abstract] OR ebilfumin*[Title/Abstract] OR en 241104[Title/Abstract] OR en241104[Title/Abstract] OR enzamir*[Title/Abstract] OR fluvir*[Title/Abstract] OR gs 4071[Title/Abstract] OR gs4071[Title/Abstract] OR gs 4104[Title/Abstract] OR gs4104[Title/Abstract] OR gs4104002[Title/Abstract] OR "hgp 0919"[Title/Abstract] OR hgp0919[Title/Abstract] OR hip 1403[Title/Abstract] OR hip1403[Title/Abstract] OR kewei*[Title/Abstract] OR "ro 64 0796"[Title/Abstract] OR ro 640796[Title/Abstract] OR ro640796[Title/Abstract] OR ro640796002[Title/Abstract] OR segosana*[Title/Abstract] OR tamiflu*[Title/Abstract] OR tamivil*[Title/Abstract] OR 20O93L6F9H[Title/Abstract] OR 196618-13-0[Title/Abstract] | 4,863 | |
10 | Oseltamivir[mesh] | 3,381 | |
9 | baloxavir*[Title/Abstract] OR xofluza*[Title/Abstract] OR 4G86Y4JT3F[Title/Abstract] OR 505CXM6OHG[Title/Abstract] OR 505CXM6OHG[Title/Abstract] OR rg 6152[Title/Abstract] OR rg6152[Title/Abstract] OR "s 033188"[Title/Abstract] OR s033188[Title/Abstract] OR s 33188[Title/Abstract] OR s33188[Title/Abstract] OR 1985605-59-1[Title/Abstract] | 405 | |
8 | #1 OR #2 OR #3 OR #4 OR #5 OR #6 OR #7 | 165,597 | |
7 | H5N1[Title/Abstract] OR HPAI[Title/Abstract] OR txid102793[Title/Abstract] OR H5N6[Title/Abstract] OR txid329376[Title/Abstract] OR H7N9[Title/Abstract] OR txid333278[Title/Abstract] OR H1N1[Title/Abstract] OR txid114727[Title/Abstract] OR H2N2[Title/Abstract] OR txid114729[Title/Abstract] | 30,645 | |
6 | alphainfluenzavirus*[Title/Abstract] OR betainfluenzavirus*[Title/Abstract] OR FLUBV[Title/Abstract] | 35 | |
5 | Betainfluenzavirus[mesh] | 4,977 | |
4 | Alphainfluenzavirus[mesh] | 51,648 | |
3 | "Influenza A virus"[mesh] | 51,403 | |
2 | influenza*[Title/Abstract] OR flu[Title/Abstract] OR flus[Title/Abstract] OR grippe[Title/Abstract] | 156,872 | |
1 | "Influenza, Human"[mesh] | 60,736 |
Appendix 2: Selection of Included Studies
Please note that this appendix has not been copy-edited.
Figure 1: PRISMA Flow Chart of Selected Reports
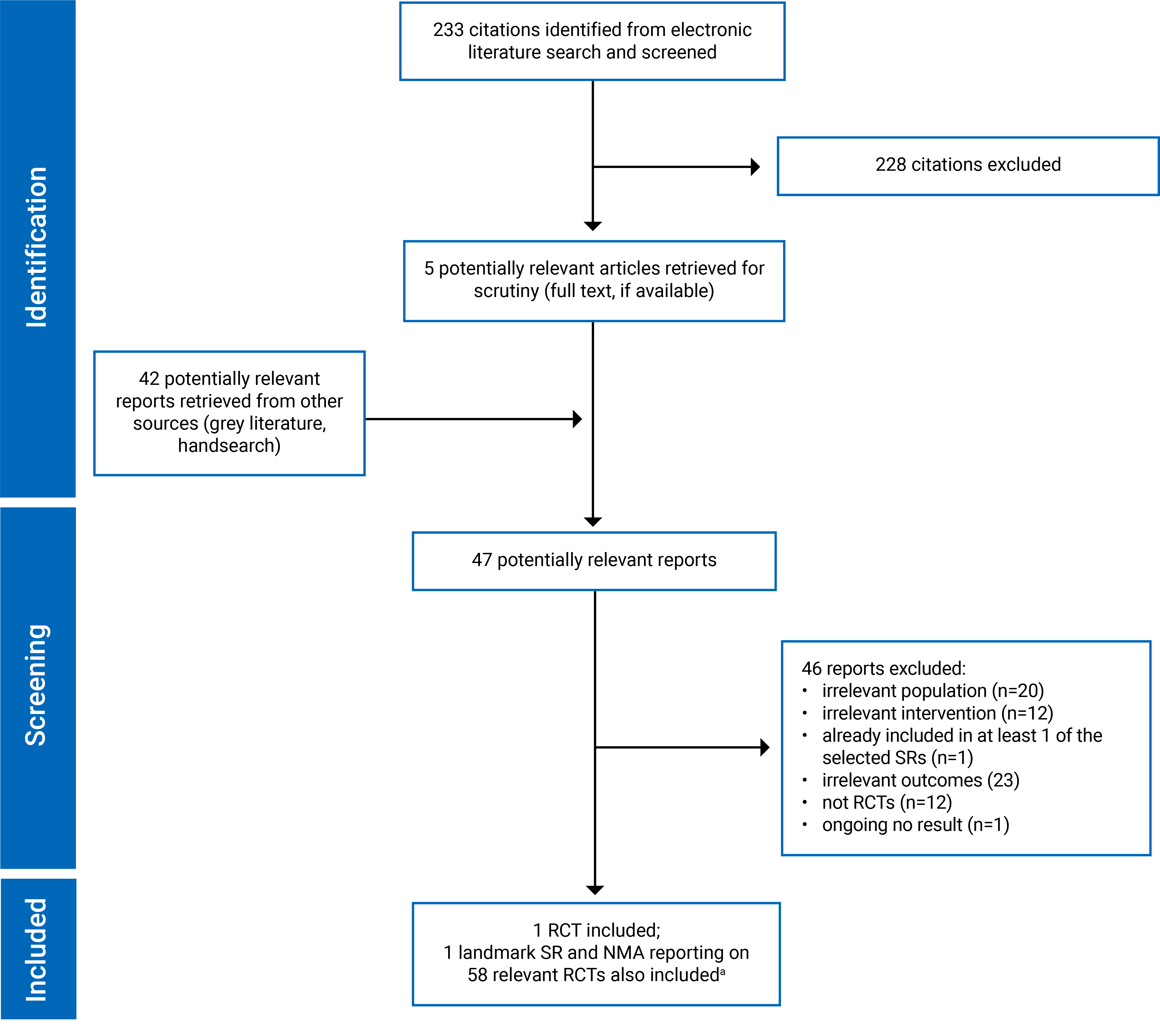
NMA = network meta-analysis; PRISMA = Preferred Reporting Items for Systematic Reviews and Meta-Analyses; RCT = randomized controlled trial; SR = systematic review.
aThe landmark SR and NMA was identified before the search and is not considered in the counts of records in the PRISMA diagram.
Appendix 3: Critical Appraisal
Please note that this appendix has not been copy-edited.
Table 11: Strengths and Limitations of the Landmark SR and NMA Using AMSTAR 2
Strengths | Limitations |
|---|---|
Gao (2025)15 assessment based on AMSTAR 2 | |
|
|
AMSTAR = A Measurement Tool to Assess Systematic Reviews; NMA = network meta-analysis; PICO = population, intervention, comparator, and outcome; RCT = randomized controlled trial; RoB = risk of bias; SR = systematic review.
Table 12: Assessment of the Landmark NMA Using ISPOR Criteria
Question number | Question | Strength | Weakness | Can’t answer |
|---|---|---|---|---|
Relevance: Rated as sufficient | ||||
1 | Is the population relevant? | Yes | No | — |
2 | Are any critical interventions missing? | No | Yes | — |
3 | Are any relevant outcomes missing? | No | Yes | — |
4 | Is the context (e.g., settings and circumstances) applicable to your population? | Yes | No | — |
Credibility: Rated as sufficient | ||||
Evidence base used for the indirect comparison or network meta-analysis | ||||
1 | Did the researchers attempt to identify and include all relevant randomized controlled trials? | Yes | No | — |
2 | Do the trials for the interventions of interest form one connected network of randomized controlled trials? | Yes | No | — |
3 | Is it apparent that poor quality studies were included thereby leading to bias? | No | Yes | — |
4 | Is it likely that bias was induced by selective reporting of outcomes in the studies? | No | Yes | — |
5 | Are there systematic differences in treatment effect modifiers (i.e., baseline patient or study characteristics that impact the treatment effects) across the different treatment comparisons in the network? | No | Yes | — |
6 | If yes (i.e., there are such systematic differences in treatment effect modifiers), were these imbalances in effect modifiers across the different treatment comparisons identified prior to comparing individual study results? | Yes | No | NA |
Analysis | ||||
7 | Were statistical methods used that preserve within-study randomization? (No naive comparisons) | Yes | No = Fatal flaw | — |
8 | If both direct and indirect comparisons are available for pairwise contrasts (i.e., closed loops), was agreement in treatment effects (i.e., consistency) evaluated or discussed? | Yes | No | NA |
9 | In the presence of consistency between direct and indirect comparisons, were both direct and indirect evidence included in the network meta-analysis? | Yes | No | NA |
10 | With inconsistency or an imbalance in the distribution of treatment effect modifiers across the different types of comparisons in the network of trials, did the researchers attempt to minimize this bias with the analysis? | Yes | No | — |
11 | Was a valid rationale provided for the use of random-effects or fixed-effect models? | Yes | No | — |
12 | If a random-effects model was used, were assumptions about heterogeneity explored or discussed? | Yes | No | NA |
13 | If there are indications of heterogeneity, were subgroup analyses or meta-regression analysis with prespecified covariates performed? | Yes | No | NA |
Reporting quality and transparency | ||||
14 | Is a graphical or tabular representation of the evidence network provided with information on the number of RCTs per direct comparison? | Yes | No | — |
15 | Are the individual study results reported? | Yes | No | — |
16 | Are results of direct comparisons reported separately from results of the indirect comparisons or network meta-analysis? | Yes | No | — |
17 | Are all pairwise contrasts between interventions as obtained with the network meta-analysis reported along with measures of uncertainty? | Yes | No | — |
18 | Is a ranking of interventions provided given the reported treatment effects and its uncertainty by outcome? | Yes | No | — |
19 | Is the impact of important patient characteristics on treatment effects reported? | Yes | No | — |
Interpretation | ||||
20 | Are the conclusions fair and balanced? | Yes | No | — |
Conflict of interest | ||||
21 | Were there any potential conflicts of interest? | No | Yes | — |
22 | If yes, were steps taken to address these? | Yes | No | — |
ISPOR = International Society for Pharmacoeconomics and Outcomes Research; NA = not applicable; NMA = network meta-analysis; RCT = randomized controlled trial.
Table 13: Assessment of the Landmark SR and NMA Using AMSTAR 2
AMSTAR 2 item | Assessment of the Gao et al. study (2025) |
|---|---|
1. Did the research questions and inclusion criteria for the review include the components of PICO? | Yes |
2. Did the report of the review contain an explicit statement that the review methods were established prior to the conduct of the review and did the report justify any significant deviations from the protocol? | Yes |
3. Did the review authors explain their selection of the study designs for inclusion in the review? | No |
4. Did the review authors use a comprehensive literature search strategy? | Partial yes |
5. Did the review authors perform study selection in duplicate? | Yes |
6. Did the review authors perform data extraction in duplicate? | Yes |
7. Did the review authors provide a list of excluded studies and justify the exclusions? | No |
8. Did the review authors describe the included studies in adequate detail? | Partial yes |
9. Did the review authors use a satisfactory technique for assessing the RoB in individual studies that were included in the review? | Yes |
10. Did the review authors report on the sources of funding for the studies included in the review? | No |
11. If meta-analysis was performed, did the review authors use appropriate methods for statistical combination of results? | Yes |
12. If meta-analysis was performed, did the review authors assess the potential impact of RoB in individual studies on the results of the meta-analysis or other evidence synthesis? | Yes |
13. Did the review authors account for RoB in primary studies when interpreting/discussing the results of the review? | Yes |
14. Did the review authors provide a satisfactory explanation for, and discussion of, any heterogeneity observed in the results of the review? | Yes |
15. If they performed quantitative synthesis did the review authors carry out an adequate investigation of publication bias (small study bias) and discuss its likely impact on the results of the review? | Yes |
16. Did the review authors report any potential sources of conflict of interest, including any funding they received for conducting the review? | Yes |
AMSTAR = A Measurement Tool to Assess Systematic Reviews; NMA = network meta-analysis; PICO = population, intervention, comparator, and outcome; RoB = risk of bias; SR = systematic review.
Table 14: Risk of Bias for the RCT Using a Modified Cochrane Risk of Bias Tool
Outcome | Sequence generation | Allocation concealment | Blinding of patients | Blinding of health care providers | Blinding of data collectors | Blinding of outcome assessors/ adjudicators | Blinding of data analysts | Incomplete outcome data | Selective outcome reporting | Other bias |
|---|---|---|---|---|---|---|---|---|---|---|
Total effective rate | Low | Low | Low | Probably low | Probably low | Low | Probably low | Low | Low | Low |
Time to alleviation of symptoms | Low | Low | Low | Probably low | Probably low | Low | Probably low | Low | Low | Probably low |
Emergence of resistance | Low | Low | Low | Low | Low | Low | Low | High | High | High |
SAEs | Low | Low | Low | Probably high | Probably high | Low | Probably low | Low | Low | Low |
RCT = randomized controlled trial; SAE = serious adverse event.
Appendix 4: Study and Population Characteristics From the Landmark SR and NMA
Table 15: Study Characteristics of Relevant Included RCTs From the Landmark SR and NMA
Study | Publication status | Country or region | Patients randomized, N | Confirmed influenza, % | Time from onset of symptoms to treatment or randomization, days | Treatments | Outcomes |
|---|---|---|---|---|---|---|---|
Watanabe 2019 | Peer-reviewed publication | Japan | 400 | 100 | ≤ 2 |
|
|
Portsmouth 2021 | Peer-reviewed publication | US, Japan | 1,436 | 74.93 | ≤ 2 |
|
|
Ison 2020, Takazono 2021 | Peer-reviewed publication | 17 countries | 2,184 | 100 | ≤ 2 |
|
|
Baker 2020 | Peer-reviewed publication | US, Poland, Spain, Costa Rica, Mexico, Russia | 176 | 67.05 | ≤ 2 |
|
|
Beigel 2020 | Peer-reviewed publication | Thailand, US, Argentina | 556 | 90.11 | 1.21 |
|
|
Butler 2020, Li 2021 (a) | Peer-reviewed publication | 15 European countries | 3,266 | 51.34 | ≤ 3 |
|
|
Dharan 2012 | Peer-reviewed publication | US | 19 | 100 | 2.90 |
|
|
Fan 2019 | Peer-reviewed publication | China | 129 | 100 | < 2 |
|
|
Fry 2014 | Peer-reviewed publication | Bangladesh | 1,190 | 100 | mean 2; < 2 for 66.7% of participants |
|
|
Heinonen 2010 | Peer-reviewed publication | Finland | 409 | 23.96 | 0.40 |
|
|
Johnston 2005, WV15759/WV15871 | Peer-reviewed publication | Argentina, Australia, Belgium, Canada, Chile, Finland, Germany, China, Israel, New Zealand, Spain, South Africa, Sweden, UK, US | 334 | 53.59 | 1.13 |
|
|
Kashiwagi 2000, JV15823 | Peer-reviewed publication | Japan | 316 | 80.50 | 0.98 |
|
|
Li 2004 | Peer-reviewed publication | China | 273 | 100 | ≤ 1.50 |
|
|
Lin 2006 | Peer-reviewed publication | China | 118 | 47.46 | < 2 |
|
|
Nicholson 2000, WV15670 | Peer-reviewed publication | Europe, Canada, China | 726 | 66.06 | 1.00 |
|
|
McLean 2015 | Peer-reviewed publication | US | 165 | 100 | < 5 |
|
|
Roberts 2019 | Peer-reviewed publication | Australia, South Africa, US | 14 | 100 | < 2 |
|
|
Treanor 2000, WV15671 | Peer-reviewed publication | US | 627 | 59.65 | 1.07 |
|
|
Whitley 2001 | Peer-reviewed publication | US, Canada | 695 | 65.04 | 1.41 |
|
|
M76001 2000 | Clinical study report | US | 1,447 | 73.46 | ≤ 1.50 |
|
|
WV15707 1999 | Clinical study report | Australia, South Africa, South America | 27 | 46.15 | ≤ 1.50 |
|
|
WV15730 1999 | Clinical study report | Australia, South Africa | 58 | 65.51 | ≤ 1.50 |
|
|
WV15758 2000 | Clinical study report | US, Canada | 695 | 64.76 | < 2 |
|
|
WV15812/WV15872 2000 | Clinical study report | Belgium, Canada, Denmark, Finland, France, Israel, New Zealand, Norway, Sweden, UK, US, Australia, Netherlands, Russia | 401 | 62.44 | ≤ 1.50 |
|
|
WV15819/WV15876/WV15978 2000 | Clinical study report | France, Netherlands, Belgium, Germany, Switzerland, UK, Norway, Sweden, Denmark, Israel, US, Canada, South Africa, New Zealand, Australia, Finland, Lithuania, Estonia, Poland | 736 | 64.67 | ≤ 1.50 |
|
|
WV16277 2003 | Clinical study report | Belgium, Denmark, Estonia, Finland, France, Germany, Lithuania, Norway, Sweden | 454 | 51 | ≤ 1.50 |
|
|
NV16871 2004 | Clinical study report | Czech Republic, Estonia, Germany, Israel, Latvia, Poland, Russia, Slovakia, Sweden, Ukraine | 329 | 28.57 | 0.81 |
|
|
Hirotsu 2017 | Peer-reviewed publication | Japan | 123 | 100 | ≤ 2 |
|
|
Duval 2010 | Peer-reviewed publication | France | 541 | 100 | < 1.50 |
|
|
Escuret 2012 | Peer-reviewed publication | France | 24 | 100 | 1.02 |
|
|
Hsieh 2021 | Peer-reviewed publication | US | 180 | 100 | < 4 |
|
|
Kato 2021 | Peer-reviewed publication | Japan | 208 | 100 | < 2 |
|
|
Nakamura 2017 | Peer-reviewed publication | Japan | 92 | 100 | 1.13 |
|
|
Kohno 2011 | Peer-reviewed publication | Japan, South Korea, China | 1,099 | 100 | < 2 |
|
|
NCT02369159 2015 | Trial registration | US, South Africa | 137 | 70.80 | ≤ 3 |
|
|
Kohno 2010 | Peer-reviewed publication | Japan | 296 | 100 | < 2 |
|
|
NCT00419263 2007 | Trial registration | US, Canada | 344 | 100 | ≤ 2 |
|
|
NCT00705406 20095406 | Trial registration | US, Australia, New Zealand, South Africa | 405 | 99.26 | ≤ 1.50 |
|
|
NCT00610935 2008 | Trial registration | US | 82 | 97.56 | ≤ 2 |
|
|
MIST 1998, NAIB3001 | Peer-reviewed publication | Australia, New Zealand, South Africa | 455 | 70.55 | ≤ 1.50 |
|
|
Hedrick 2000, NAI30009 | Peer-reviewed publication | US, Canada, UK, Belgium, Finland, Spain, Russia, Sweden, France, Germany, Israel | 471 | 73.46 | 0.84 |
|
|
Makela 2000, NAIB3002 | Peer-reviewed publication | Belgium, Denmark, Finland, France, Germany, Holland, Italy, Norway, Spain, Sweden, UK | 356 | 77.81 | < 2 |
|
|
Matsumoto 1999 | Peer-reviewed publication | Japan | 116 | 62.93 | < 1.50 |
|
|
Monto 1999, NAIA/B2008 | Peer-reviewed publication | Belgium, Canada, Denmark, Finland, France, Germany, Italy, Netherlands, Norway, Spain, Sweden, US, UK | 1,256 | 57 | 1.21 |
|
|
Murphy 2000, NAI30008 | Peer-reviewed publication | US, Canada, Europe, Australia, Chile, South Africa | 525 | 59.62 | ≤ 1.50 |
|
|
Puhakka 2003, NAI30015 | Peer-reviewed publication | Finland | 588 | 73.98 | 1 |
|
|
Hayden 2000, NAI30010 | Peer-reviewed publication | US, Canada, UK, Finland | 321 | 48.91 | < 1.50 |
|
|
JNAI-01 2000 | Clinical study report | Japan | 116 | 48.28 | ≤ 1.50 |
|
|
JNAI-04 1999 | Clinical study report | Japan | 49 | 45.83 | ≤ 1.50 |
|
|
JNAI-07 1999 | Clinical study report | Japan | 329 | 73.04 | ≤ 1.50 |
|
|
NAI30011 2001 | Clinical study report | US | 466 | 45.28 | 1.18 |
|
|
NAI30012 2002 | Clinical study report | Australia, Canada, Chile, Czech Republic, Denmark, Finland, France, Germany, Israel, Italy, Lithuania, Netherlands, Norway, Romania, Russia, Slovakia, South Africa, Spain, UK, US | 358 | 57.54 | < 2 |
|
|
NAI30020 2002 | Clinical study report | Germany | 331 | 100 | < 2 |
|
|
NAI30028 2003 | Clinical study report | Germany | 266 | 100 | < 2 |
|
|
NAIA2005 1998, Hayden 1997 | Clinical study report | Canada, US | 220 | 50.45 | 1.26 |
|
|
NAIA3002 1998 | Clinical study report | Canada, US | 777 | 73.23 | < 2 |
|
|
NAIB2005 1998, Hayden 1997 | Clinical study report | Belgium, Finland, France, Germany, Italy, Netherlands, Norway, Spain, Sweden, UK | 197 | 79.70 | 1.29 |
|
|
NAIB2007 1998 | Clinical study report | Australia, New Zealand, South Africa | 554 | 100 | 1.23 |
|
|
AE = adverse event; COPD = chronic obstructive pulmonary disease; ICU = intensive care unit; NMA = network meta-analysis; NR = not reported; SAE = serious adverse event; SR = systematic review.
Notes: This table has not been copy-edited.
The study and population characteristics are only presented for RCTs relevant to this review (n = 58).
Table 16: Patient Characteristics of Relevant Included RCTs From the Landmark SR and NMA
Study | Treatments | Patients randomized, N | Mean age, years | Age range, years | Male / female, % | High risk, %a | Comorbidities, % | Type of influenza (%) | Confirmed influenza % | Influenza vaccination % |
|---|---|---|---|---|---|---|---|---|---|---|
Hayden 2018 (a), Watanabe 2019 |
| 400 | 36.88 | 20 to 64 | 61.75 / 38.25 | 0 | None |
| 100 | 30.50 |
Hayden 2018 (b), Portsmouth 2021 |
| 1,436 | 33.33 | 12 to 64 | 50 / 50 | 0 | None |
| 74.93 | 21.62 |
Ison 2020, Takazono 2021 |
| 2,184 | 51.77 | 12 to 89 | 48.5 / 51.5 | 100 |
|
| 100 | 25.28 |
Baker 2020 |
| 176 | 6.10 | 1 to 12 | 46.8 / 53.2 | NR | NR |
| 67.05 | 49.13 |
Beigel 2020 |
| 556 | 36.67 | 18 to 64 | 37.59 / 62.41 | 0 | NR |
| 90.11 | 10.25 |
Butler 2020, Li 2021 (a) |
| 3,266 | 35.45 | ≥ 1 | 44.12 / 55.88 | NR |
|
| 51.34 | 9.42 |
Dharan 2012 |
| 19 | 9.00 | 1 to 54 | 52.63 / 47.37 | NR | NR |
| 100 | NR |
Fan 2019 |
| 129 | 32.05 | 15 to 68 | 38.76 / 61.24 | NR | NR | NR | 100 | NR |
Fry 2014 |
| 1,190 | 5.00 | > 1 | 52.69 / 47.31 | NR | NR |
| 100 | NR |
Heinonen 2010 |
| 409 | 2.40 | 1 to 4 | 62.2 / 37.8 | NR | 13.30 (asthma) |
| 23.96 | 13.27 |
Johnston 2005, WV15759/WV15871 |
| 334 | 9.00 | 6 to 12 | 64.52 / 35.48 | 100 | 100 (asthma) | NR | 53.59 | 19.46 |
Kashiwagi 2000, JV15823 |
| 316 | 34.09 | 16 to 89 | 48.24 / 51.76 | NR | NR |
| 80.50 | 0 |
Li 2004 |
| 273 | 31.04 | 18 to 65 | 49.82 / 50.18 | NR | NR |
| 100 | NR |
Lin 2006 |
| 118 | 50.28 | NR | 58.93 / 41.07 | 100 |
| NR | 47.46 | 0 |
Nicholson 2000, WV15670 |
| 726 | 37.43 | 18 to 65 | 51.01 / 48.99 | NR | NR |
| 66.06 | 0 |
McLean 2015 |
| 165 | 17.69 | 1 to 79 | 40 / 60 | 11.52 | NR |
| 100 | NR |
Roberts 2019 |
| 14 | 34.85 | 18 to 64 | 78.57 / 21.43 | NR | NR |
| 100 | 0 |
Treanor 2000, WV15671 |
| 627 | 32.63 | 18 to 65 | 49.28 / 50.72 | 0 | NR |
| 59.65 | 0 |
Whitley 2001 |
| 695 | 5.00 | 1 to 12 | 50.36 / 49.64 | 0 | NR |
| 65.04 | 3 |
M76001 2000 |
| 1,447 | 35.00 | 13 to 80 | 44.16 / 55.84 | 3.87 |
|
| 73.46 | NR |
WV15707 1999 |
| 27 | 71.62 | 65 to 84 | 53.85 / 46.15 | 100 |
|
| 46.15 | 65.38 |
WV15730 1999 |
| 58 | 35.17 | 18 to 65 | 51.72 / 48.28 | NR |
|
| 65.51 | 0 |
WV15758 2000 |
| 695 | 5.34 | 1 to 12 | 50.36 / 49.64 | NR |
|
| 64.76 | 3.02 |
WV15812/WV15872 2000 |
| 401 | 51.82 | 13 to 88 | 44.14 / 55.86 | 100 |
|
| 62.44 | 27.68 |
WV15819/WV15876/WV15978 2000 |
| 736 | 72.95 | 65 to 97 | 42.99 / 57.01 | 100 |
|
| 64.67 | 42.86 |
WV16277 2003 |
| 454 | 34.92 | 13 to 86 | 49.67 / 50.33 | NR |
|
| 51 | 6.87 |
NV16871 2004 |
| 329 | 11.00 | 6 to 17 | 65.35 / 34.65 | 100 | 100 (asthma) |
| 28.57 | 6.08 |
Hirotsu 2017 |
| 123 | NR | 4 to 12 | 51.75 / 48.25 | NR | No |
| 100 | 57.89 |
Duval 2010 |
| 541 | 39.34 | 18 to 84.2 | 49.72 / 50.28 | NR | NR |
| 100 | 0 |
Escuret 2012 |
| 24 | 34.40 | 19.10 to 55.20 | 41.67 / 58.33 | NR | NR |
| 100 | 0 |
Hsieh 2021 |
| 180 | 50.00 | ≥ 18 | 40.8 / 59.2 | 67.60 |
|
| 100 | 43.60 |
Kato 2021 |
| 208 | NR | 16 to 79 | 44.71 / 55.29 | 100 |
|
| 100 | 37.80 |
Nakamura 2017 |
| 92 | 71.15 | ≥ 20 | 46.74 / 53.26 | 100 |
|
| 100 | 50 |
Kohno 2011 |
| 1,099 | 35.13 | 20 to 80 | 51.52 / 48.48 | NR | NR |
| 100 | 16.77 |
NCT02369159 2015 |
| 137 | 8.32 | 0 to 17 | 46.72 / 53.28 | 0 | No | NR | 70.80 | NR |
Kohno 2010 |
| 296 | 34.17 | 20 to 64 | 50.68 / 49.32 | NR | No |
| 100 | NR |
NCT004192632007 |
| 344 | 35.43 | ≥ 18 | 46.49 / 53.51 | 0 | NR | NR | 100 | 0 |
NCT00705406 |
| 405 | 35.00 | ≥ 18 | 49.14 / 50.86 | 0 | No | NR | 99.26 | 0 |
NCT00610935 2008 |
| 82 | 33.00 | 18 to 75 | 48.78 / 51.22 | 0 | No |
| 97.56 | 0 |
MIST 1998, NAIB3001 |
| 455 | 36.95 | ≥ 12 | 52.97 / 47.03 | 16.70 |
|
| 70.55 | 5.71 |
Hedrick 2000, NAI30009 |
| 471 | 8.71 | 5 to 12 | 54.78 / 45.22 | NR | 7.64 (respiratory diseases) |
| 73.46 | 2.34 |
Makela 2000, NAIB3002 |
| 356 | 37.20 | 12 to 81 | NR / NR | 8.99 | NR |
| 77.81 | NR |
Matsumoto 1999 |
| 116 | 29.74 | 16 to 65 | 37.07 / 62.93 | NR | NR |
| 62.93 | 0.86 |
Monto 1999, NAIA/B2008 |
| 1,256 | 35.01 | ≥ 13 | 44.03 / 55.97 | 12.56 | NR |
| 57 | 1.51 |
Murphy 2000, NAI30008 |
| 525 | 38.00 | ≥ 12 | 42.48 / 57.52 | 100 |
|
| 59.62 | 23.24 |
Puhakka 2003, NAI30015 |
| 588 | 19.25 | 17 to 29 | 99.15 / 0.84999 | NR | NR |
| 73.98 | 0.51 |
Hayden 2000, NAI30010 |
| 321 | 19.46 | ≥ 5 | 42.37 / 57.63 | NR | 6.54 (underlying respiratory conditions) |
| 48.91 | 10.28 |
JNAI-01 2000 |
| 116 | NR | 16 to 65 | NR / NR | NR | NR | NR | 48.28 | NR |
JNAI-04 1999 |
| 49 | 38.38 | ≥ 16 | 52.08 / 47.92 | NR | NR |
| 45.83 | 0 |
JNAI-07 1999 |
| 329 | 34.17 | ≥ 16 | 50 / 50 | NR | NR |
| 73.04 | 1.30 |
NAI30011 2001 |
| 466 | 36.15 | 18 to 99 | 43.35 / 56.65 | NR |
|
| 45.28 | 9.01 |
NAI30012 2002 |
| 358 | 73.35 | > 65 | 41.06 / 58.94 | 100 |
|
| 57.54 | 45.81 |
NAI30020 2002 |
| 331 | 50.01 | ≥ 18 | 49.3 / 50.7 | 100 |
|
| 100 | NR |
NAI30028 2003 |
| 266 | 7.00 | 5 to 14 | 61.28 / 38.72 | NR |
|
| 100 | NR |
NAIA2005 1998, Hayden 1997 |
| 220 | 32.00 | ≥ 13 | 60.91 / 39.09 | 0 | NR |
| 50.45 | 0 |
NAIA3002 1998 |
| 777 | 35.00 | 12 to 86 | 48.13 / 51.87 | 14.03 |
|
| 73.23 | 14 |
NAIB2005 1998, Hayden 1997 |
| 197 | 33.67 | ≥ 18 | 52.55 / 47.45 | 0 |
|
| 79.70 | 0 |
NAIB2007 1998 |
| 554 | 30.00 | ≥ 13 | 52 / 48 | 11.91 |
|
| 100 | 1.62 |
COPD = chronic obstructive pulmonary disease; NMA = network meta-analysis; NR = not reported; RCT = randomized controlled trial; SR = systematic review.
Notes: This table has not been copy-edited.
The study and population characteristics are only presented for RCTs relevant to this review (n = 58).
aPatients considered to be at risk for severe influenza.
bFor children younger than 13 years, oseltamivir was given in oral suspension according to weight; children weighing 10 to 15 kg received 30 mg, > 15 to 23 kg received 45 mg, > 23 to 40 kg received 60 mg, and > 40 kg received 75 mg.
ISSN: 2563-6596
This work was conducted by the PODET through the Post-Market Drug Evaluation CoLab Network. It was supported by Canada’s Drug Agency (CDA-AMC) and its Post-Market Drug Evaluation Program through funding provided by Health Canada.
CDA-AMC is a pan-Canadian health organization. Created and funded by Canada’s federal, provincial, and territorial governments, we’re responsible for driving better coordination, alignment, and public value within Canada’s drug and health technology landscape. We provide Canada’s health system leaders with independent evidence and advice so they can make informed drug, health technology, and health system decisions, and we collaborate with national and international partners to enhance our collective impact.
CoLab is a pan-Canadian network of experts in applied research, scientific methods, and data analysis. CoLab members work with the Post-Market Drug Evaluation Program to produce credible and timely evidence on postmarket drug safety and effectiveness.
Disclaimer: CDA-AMC has taken care to ensure that the information in this document was accurate, complete, and up to date when it was published, but does not make any guarantee to that effect. Your use of this information is subject to this disclaimer and the Terms of Use at cda-amc.ca.
The information in this document is made available for informational and educational purposes only and should not be used as a substitute for professional medical advice, the application of clinical judgment in respect of the care of a particular patient, or other professional judgments in any decision-making process. You assume full responsibility for the use of the information and rely on it at your own risk.
CDA-AMC does not endorse any information, drugs, therapies, treatments, products, processes, or services. The views and opinions of third parties published in this document do not necessarily reflect those of CDA-AMC. The copyright and other intellectual property rights in this document are owned by the Canadian Agency for Drugs and Technologies in Health (operating as CDA-AMC) and its licensors.
This document is the property of PODET. CDA-AMC has a nonexclusive, limited, royalty-free, worldwide, nontransferable, fully paid-up, and irrevocable licence to use the report in support of its objects, mission, and reasonable operational requirement.