Drugs, Health Technologies, Health Systems
Health Technology Review
Extracorporeal Shockwave Therapy for Erectile Dysfunction
Key Messages
What Is the Issue?
Sexual dysfunction, including erectile dysfunction (ED) is a common problem for males starting in their early 40s and increases with age.
ED may be caused by 1 or more reasons, including organic (e.g., vasculogenic, hormonal), psychogenic, or mixed psychogenic and organic reasons. ED is also common after pelvic trauma and penile fracture, surgery (e.g., prostatectomy), and radiation therapy (e.g., prostate cancer).
There are many nonsurgical treatment options for ED, including oral phosphodiesterase type 5 (PDE5) inhibitors, penile self-injections with vasoactive drugs, and extracorporeal shockwave therapy (ESWT). A review of the clinical effectiveness of ESWT could help clarify the potential role in clinical practice, in which populations and with which treatment protocols.
What Did We Do?
To inform decisions regarding the use of ESWT, we conducted a rapid review to identify and summarize evidence that compared the clinical effectiveness of ESWT to any comparators (e.g., sham or no treatment, pharmacological therapy, or platelet-rich plasma). We identified evidence-based guidelines that provided recommendations related to ESWT in males with ED.
We searched key resources, including journal citation databases, and conducted a focused internet search for relevant evidence published since 2014. One reviewer screened articles for inclusion based on predefined criteria, critically appraised the included studies, and narratively summarized the findings.
What Did We Find?
We found 1 health technology assessment (HTA), 1 overview of systematic reviews (SRs), and 7 SRs that evaluated the clinical effectiveness of ESWT for ED. We found 4 evidence-based guidelines that provided recommendations on the use of ESWT for ED.
Comparing ESWT to sham or no treatment, shockwave therapy (SWT) increases the mean International Index of Erectile Function – Erectile Function subscale (IIEF-EF) score and the proportion of males achieving a minimal clinically important difference (MCID) when compared to sham or no treatment. This differed when looking at subpopulations. Similarly, ESWT increases the mean Erectile Hardness Scale (EHS) score and the proportion of males with an improvement of 3 or more when compared to sham or no treatment. This differed when looking at subpopulations.
Comparing ESWT to pharmacological therapy, there was no statistical difference between groups for the IIEF-EF subscale (when reported) and the EHS. One observational study in an SR reported a statistically significant difference in the number of males who had an improved EHS score of 3 or more after treatment.
Comparing ESWT to platelet-rich plasma, there was no difference in any outcomes; however, this was poorly reported.
Comparing ESWT protocols, there was no difference in any outcomes; however, this was poorly reported.
One SR reported on treatment-related adverse effects, with few adverse effects reported. Two SRs reported on discontinuation from treatment, with no discontinuations.
International guidelines varied on recommending ESWT for ED, with 2 recommending it in specific populations, 1 not recommending it, and 1 guideline (published in 2019) stating there was insufficient evidence to make a recommendation.
What Does This Mean?
ESWT may improve clinical outcomes for males with ED when compared to sham or no treatment.
There may be differences in the effectiveness of ESWT treatment for subpopulations.
Data on the clinical effectiveness of different protocols of ESWT were limited.
ESWT is safe, with few treatment-related adverse events.
Abbreviations
ED
erectile dysfunction
EHS
Erectile Hardness Scale
ESWT
extracorporeal shockwave therapy
GRADE
Grading of Recommendations Assessment, Development and Evaluation
HTA
health technology assessment
IIEF-EF
International Index of Erectile Function – Erectile Function
Li-SWT
low-intensity shockwave therapy
Li-ESWT
low-intensity extracorporeal shockwave therapy
MCID
minimal clinically important difference
PDE5
phosphodiesterase type 5
RCT
randomized controlled trial
SEAR
self-esteem and relationship
SEP
sexual encounter profile
SD
standard deviation
SR
systematic review
SWT
shockwave therapy
Research Questions
What is the clinical effectiveness of ESWT for ED?
What are the evidence-based guidelines regarding the use of ESWT for ED?
Context and Policy Issues
What Is ED?
Sexual function in males requires an interaction between vascular, neurologic, hormonal, and psychological systems.1 Sexual dysfunction, which includes ED, diminished libido, and ejaculatory disorders, is a problem that becomes more common with increasing age.1 In a cross-sectional study of males aged 40 to 88 years, visiting primary care physicians’ offices from July 2001 to November 2002, 49.4% reported some degree of ED during the past 4 weeks or were taking oral medication for ED, with overall prevalence and severity of ED increasing with age.2 More recently, in a 2015 survey of 1,162 males between the ages of 40 and 59 years in Canada, 23.8% reported having erection problems, a significant contributor to their overall sexual happiness.3
ED is defined as “the consistent or recurrent inability to acquire or sustain an erection of sufficient rigidity and duration for sexual intercourse.”1 ED is classified as organic (i.e., vasculogenic, neurogenic, local penile [cavernous] factors, hormonal, drug-induced), psychogenic, or mixed psychogenic and organic.1 In addition to age, risk factors for ED are cardiovascular disease, diabetes mellitus, hypertension, obesity, dyslipidemia, hypogonadism, smoking, depression, and medication use.1 ED is also common after trauma (pelvic trauma and penile fracture), surgery (pelvic, penile, urethral, or prostatectomy), and radiation therapy.4
What Is the Current Practice?
There are several treatment options for ED, including nonsurgical and surgical treatment. Nonsurgical treatment options for ED include oral PDE5 inhibitors, penile self-injections with vasoactive drugs, intraurethral suppositories, vacuum erection devices, stem cell therapy, hyperbaric oxygen therapy, platelet-rich plasma injections, and ESWT, also referred to as low-intensity shockwave therapy (Li-SWT) or low-intensity extracorporeal shockwave therapy (Li-ESWT). Surgical options include penile prostheses and penile revascularization.5
What Is ESWT?
SWT, specifically extracorporeal shockwave lithotripsy, has been used by urologists since the 1980s for the noninvasive fragmentation of kidney stones. Within the realm of sexual medicine, Li-ESWT has been investigated for the treatment of ED. There are 3 types of Li-ESWT energy source generators available, electrohydraulic, electromagnetic, and piezoelectric, with similar mechanistic actions which produce acoustic waves that transfer energy to tissue, leading to potential improvement in microcirculation and vasodilation, a decrease in fibrosis, and nerve regeneration.6 Waves may be focused or radial, with differing tissue penetration depth and energy. Li-ESWT uses focused shockwaves which have a tissue penetration depth of 10 to 12 cm, compared to less than 3 cm depth from radial waves. Additionally, Li-ESWT has an energy of 0.09 to 1.5 mJ/mm2 compared to 0.02 to 0.06 mJ/mm2 of radial waves. For these reasons, it is said that radial therapy is not comparable to Li-ESWT for management of ED.7
Why Is It Important to Do This Review?
There are many nonsurgical treatment options for ED, including oral PDE5 inhibitors, penile self-injections with vasoactive drugs, and ESWT. A review of the clinical effectiveness of ESWT could help clarify the potential role in clinical practice, in which populations (e.g., mild ED or Peyronie disease) and with which treatment protocols.
Objective
The objectives of the report are to summarize the evidence regarding the clinical effectiveness of ESWT for the treatment of ED and to report on recommendations found in guidelines.
Methods
Literature Search Methods
An information specialist conducted a literature search on key resources including MEDLINE, Embase, the Cochrane Database of Systematic Reviews, the International HTA Database, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search approach was customized to retrieve a limited set of results, balancing comprehensiveness with relevancy. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s Medical Subject Headings (MeSH), and keywords. Search concepts were developed based on the elements of the research questions and selection criteria. The main search concepts were ED and shockwave. The search was completed on December 4, 2024, and limited to English-language documents published since January 1, 2014.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
|---|---|
Population | Adults (≥ 18 years) who experience erectile dysfunction |
Intervention | Extracorporeal shockwave therapy |
Comparator | Q1: Medication, placebo, no comparator (i.e., treatment as usual) Q2: NA |
Outcomes | Q1: Benefits (e.g., improvement in erectile function, patient-reported satisfaction) and harms (e.g., adverse events, visits to the emergency department) Q2: Recommendations regarding best practices (e.g., whether to use, frequency of treatment) |
Study designs | Health technology assessments, systematic reviews, evidence-based guidelines |
NA = not applicable.
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, they were duplicate publications or were published before 2014. SRs in which all relevant studies were captured in other more recent or more comprehensive SRs were excluded. Guidelines with unclear methodology or that were published before 2019 were also excluded. Due to the volume of included HTAs, SRs, and guidelines, primary studies were excluded.
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using A Measurement Tool to Assess Systematic Reviews 2 (AMSTAR 2)8 for SRs, the Downs and Black checklist9 for randomized and nonrandomized studies, and the Appraisal of Guidelines for Research and Evaluation (AGREE) II instrument10 for guidelines. Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Summary of Evidence
Quantity of Research Available
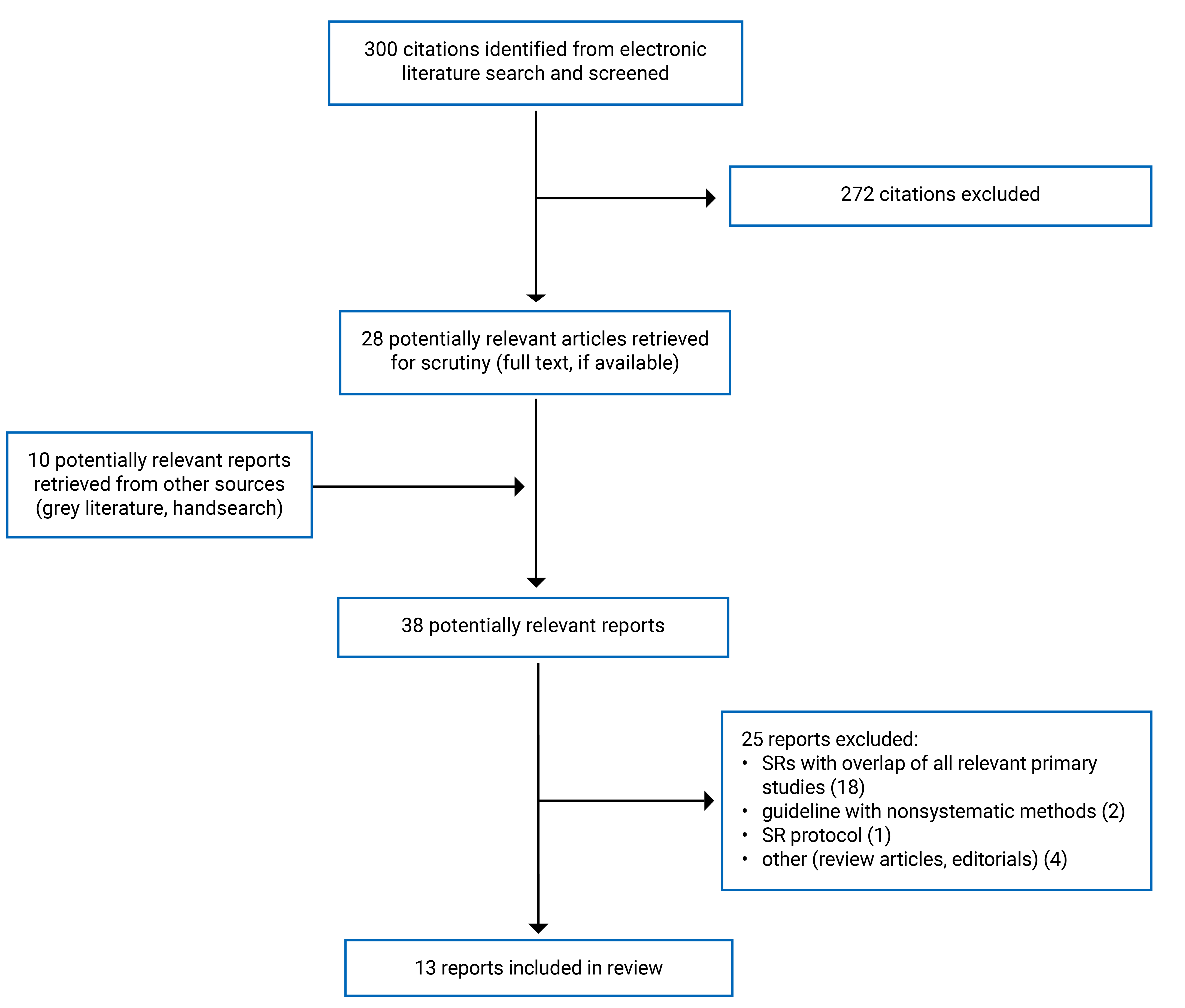
This report includes 1 HTA, 1 overview of SRs, 7 SRs, and 4 evidence-based guidelines. Appendix 1 presents the PRISMA11 flow chart of the study selection. Appendix 6 provides additional references of potential interest that did not meet our inclusion criteria.
Summary of Study Characteristics
Summaries of study characteristics are organized by research question. Appendix 2 provides detailed characteristics of the included publications.
Included Studies for Question 1: Clinical Effectiveness of ESWT for ED
We identified 1 HTA,12 published in 2023, which included males aged 18 years and older with vasculogenic, general, or diverse pathogeneses of ED. Six SRs, 3 randomized controlled trials (RCTs), and 2 nonrandomized studies in the HTA are relevant to this review. There was significant overlap of SRs and primary studies, with overlap addressed in Appendix 5. Therefore, only the 2 RCTs and 2 nonrandomized studies not reported in any other SRs, are reported in this review. The HTA compared Li-ESWT to several comparators including pharmacology therapy, medical devices, combination therapy, and placebo (sham).
We identified 1 overview of SRs,13 published in 2024, which included males with vascular-origin ED. This overview included 5 SRs, all of which were identified in this review and were evaluated for primary study overlap. As the overview of SRs only included studies that compared Li-ESWT to placebo specific to males with vascular-origin ED, not all primary studies were used in the reporting of the results. For this reason, we have not reported any of the results from this overview of SRs in this review, as they will be included in the SR section.
We identified 7 SRs, published between 2019 and 2024,14-20 of which 4 included meta-analyses.14,16,18,20 All SRs included males aged 18 years and older with ED.
Two SRs do not provide any outcomes for this review.15,19 Marchioni et al. (2020)19 summarized evidence about the efficacy of available treatment for ED after robotic assisted radical prostatectomy, and included conservative (e.g., pharmacological therapy, vacuum pump erectile devices, or ESWT) and surgical interventions. Eleven studies were included, with 1 primary study evaluating Li-ESWT; however, it is a noncomparative study and is therefore not relevant to this review. Bocchino et al. (2023)15 included males with ED according to the European guidelines diagnostic criteria, had a search date of August 2022, and identified 52 studies with 28 relevant to this review, evaluating Li-ESWT. However, they only reported the outcomes for the intervention group. As no data were extracted for this review, we did not assess overlapping primary studies.
Among the 5 SRs that provide data for this review, 2 had broader inclusion criteria than this review. Panunzio et al. (2024)14 included randomized and nonrandomized comparative studies published up to July 2023 (including in meeting abstract format) that evaluated platelet-rich plasma intracavernosal injections compared to other therapies (e.g., pharmacological, ESWT, or placebo) for the treatment of primary organic ED. One observational study, published in 2021, is relevant to this review. Sokolakis and Hatzichristodoulou (2019)20 included males with ED, not otherwise described, and had broader inclusion in terms of study design, as they included RCTs and single-arm studies. Search dates were from January 2010 to September 2018. A total of 28 studies were included: 14 single-arm studies and 14 RCTs. Their meta-analyses included 10 RCTs that compared Li-ESWT to sham therapy.
Two SRs included specific populations. Rosenberg et al. (2023)16 had narrower inclusion criteria related to the types of therapies evaluated as they included males with Peyronie disease. Although males with Peyronie disease may experience ED, the presence of ED was not an inclusion criterion. All nonsurgical therapies were included (e.g., ESWT, injections, and penile traction therapy). Two primary studies, published in 2009 and 2010, are relevant to this review. Sighinolfi et al. (2022)17 included randomized and nonrandomized comparative studies published between 2015 and 2022 (search date not reported), in patients after receiving prostatectomy. Three RCTs, 3 nonrandomized studies, and 1 conference abstract were included that compared Li-ESWT to delayed Li-ESWT, pharmacological therapy alone, sham, or no treatment. The 3 RCTs were also included in the meta-analysis in Yao et al. (2022)18; thus, only the data from the nonrandomized studies are reported in this review.
Yao et al. (2022)18 had similar inclusion criteria to this review, as they included males with ED not otherwise described, and compared Li-ESWT with or without pharmacological therapy to pharmacological therapy alone, sham, or no treatment. Sixteen RCTs published between 2010 and 2021 were included, all relevant to this review.
Across the primary studies in the SRs, the protocols for Li-ESWT varied in terms of energy density (e.g., 0.09, 0.15, and 0.16 mJ/mm2), frequency (e.g., 2 and 5 Hz), pulses per treatment (e.g., 600, 3000, and 4000), machine (e.g., RENOVA electromagnetic device, Omnispec ED1000, MT 2000H, Duolith SDI, Richard Wolf GmbH, Swiss Dolorclast, and Dornier Aries device), number of treatments per week (e.g., 1 and 2), number of treatment weeks (e.g., 3 weeks on, 3 weeks break, 3 weeks on or consecutive 4, 5, or 8 weeks).
Erection-related outcomes were patient-reported outcomes using the IIEF-EF subscale and the EHS. The IIEF-EF was reported as a mean (standard deviation [SD])12,14,17,18,20 as a proportion of those who reached an MCID,12,20 or as an increase since baseline.20 The IIEF-EF score determines the severity of ED, with a score of 26 to 30 as no ED, 22 to 25 as mild ED, 17 to 21 as mild to moderate ED, 11 to 16 as moderate ED, and 6 to 10 as severe ED. Achieving an MCID differs based on the baseline ED severity (e.g., an increase of 2 points for mild, 4 or 5 points for moderate, and 7 points for severe ED). The EHS score was reported as mean (SD)12,14,18 and as an improvement of 3 or more points.17,20 The EHS is a scale with 5 options ranging from 0 (penis does not enlarge) to 4 (penis is completely hard and fully rigid). Other outcomes were sparsely reported including self-esteem and relationship (SEAR),12,14 sexual encounter profile (SEP),18 the sexual bother score and the sexual function score from the Expanded Prostate Cancer Index Composite,17 quality of life,16 treatment-related adverse effects,16 and discontinuation from treatment.14,16
Included Studies for Question 2: Evidence-Based Guidelines Regarding the Use of ESWT for ED
Four guidelines published between 2019 and 2024 were identified. These guidelines were developed by the European Association of Urology,21 the Canadian Urological Association,4 the Asia-Pacific Society for Sexual Medicine,22 and the European Society for Sexual Medicine.23 Recommendations from 2 guidelines were specific for males with ED.4,22 Two guidelines provided recommendations for ED and other conditions; however, only recommendations related to ED were relevant to this report. The guideline by the European Association of Urology21 provided recommendations for male sexual dysfunction, infertility, and hypogonadism. The European Society for Sexual Medicine provided recommendations for ED, Peyronie disease, and chronic prostatitis or chronic pelvic pain syndrome.23 The guidelines looked at a variety of options for diagnosis and treatment, including pharmacological therapies, Li-ESWT, vacuum and pump devices, and surgery (e.g., prosthesis).
Guideline groups used different methods to identify their evidence base. The European Association of Urology guideline21 did not state the exact method; however, their guideline handbook states that they use a staged approach, first searching for SRs, then conducting a new SR, if required. The Canadian Urological Association4 did not state their method to identify the evidence base; however, they use the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach to evaluate the certainty of the evidence, which should be based on an SR. The Asia-Pacific Society for Sexual Medicine guideline22 based on a literature review, analyzed and summarized the evidence, and presented it at a scientific meeting. The European Society for Sexual Medicine23 performed a review which could be considered systematic based on their methodology description. Groups used consensus to develop recommendations, with some using a formal approach to evaluate the strength of the recommendations. The European Association of Urology guideline21 used a recommendations worksheet based on a modified GRADE approach, with strong recommendations typically indicating a high degree of evidence quality and/or a favourable balance of benefit to harm and patient preference and weak recommendations typically indicating availability of lower quality evidence, and/or equivocal balance between benefit and harm, and uncertainty or variability of patient preference. The Canadian Urological Association4 used the GRADE Evidence to Decision framework. The 2 other guidelines did not describe their process.
Two guidelines stated that the outcomes they considered included items such as benefits and harms, patient values and preferences, costs and resource use, equity, feasibility, and acceptability.4,21 One guideline looked at the treatment template and patient selection, clinical outcomes, and safety and tolerabilty,22 and 1 looked at the treatment efficacy, treatment protocol, clinical indications, and safety.23
Summary of Critical Appraisal
HTA and Overview of SRs
The HTA12 and the overview of SRs13 were assessed using AMSTAR 28 with additional questions specifically related to the overview of SRs (e.g., evaluating overlap of primary studies included in the SRs). Several strengths were identified. Both searched multiple electronic databases, sufficiently described the inclusion criteria, provided a PRISMA flow diagram, performed critical appraisal of the included studies, reported the source of funding, and declared conflicts of interest. The overview of SRs13 requested registration in PROSPERO (an open-access international prospective register of SRs) and reported on the overlap of the primary studies in the included SRs. Several limitations were identified. The HTA12 did not provide any details around a protocol. The HTA12 had 1 reviewer perform study selection, and the overview of SRs13 did not adequately describe how study selection was performed. Neither the HTA or the overview of SRs sufficiently described the process for data extraction and critical appraisal, provided a list of excluded studies, or reported on the source of funding on the included studies. These limitations can reduce the level of confidence that all relevant studies were identified and included, that all relevant data were extracted, and that critical appraisal was correctly and consistently performed.
Systematic Reviews
The 7 SRs were assessed using AMSTAR 2.8 All SRs provided a PRISMA flow diagram, which is a flow chart mapping the number of records identified, included and excluded, and the reasons for exclusion during the different levels of study selection, which increases the transparency of the SR process and may increase the reproducibility of the SR. All SRs also reported on conflicts of interest, which can help identify real or perceived author bias. There were several strengths identified in SRs; however, not across all reviews. Two SRs14,16 reported on a protocol developed before undertaking the review, which can reduce selection (of studies) and reporting (e.g., outcomes) bias. Four SRs14,16,19,20 provided sufficient details around inclusion criteria, with exclusion criteria much less explicitly defined, mainly reported for years of publication, study designs, and language. Six SRs searched multiple electronic databases, with Bocchino et al. (2023)15 searching only PubMed. Three SRs14,16,20 conducted supplemental searching (e.g., looking at the reference lists of included studies), which can identify studies not captured in the search of electronic databases. Three SRs16,18,20 did not limit language of publication. The methodological conduct of study selection, data extraction, and risk of bias assessment varied across reviews, with dual-independent selection, extraction, and critical appraisal increasing the likelihood that all studies, relevant data, and limitations were identified. Four SRs14,16,19,20 reported that 2 independent reviewers performed study selection, 4 SRs14-16,20 reported that 2 independent reviewers performed data extraction, and 5 SRs14,16-18,20 reported that 2 independent reviewers performed risk of bias assessment. Three SRs14,16,17 provided sufficient details around the included studies, which helped in identifying which ones were relevant to this review. Four SRs15-18 reported the source of funding. Four SRs performed meta-analyses,14,16,18,20 often resulting in high levels of heterogeneity, which can influence our trust in the generalizability of the results. Two SRs18,20 performed subgroup analyses (e.g., timing of outcome and severity of baseline ED), which may or may not have affected the levels of heterogeneity. Rosenberg et al. (2023)16 is a Cochrane review and followed rigorous methodological conduct and reporting of SRs. It was the only SR that provided a list of excluded studies and funding details of the included primary studies; however, it included studies in males with Peyronie disease, with only 2 studies relevant to this review.
Guidelines
The guidelines were assessed using the AGREE II tool.10 All guidelines provided a description of the scope and purpose of the guideline; clearly described the methods used for formulating the recommendations; considered the health benefits, side effects, and risks when formulating the recommendations; provided an explicit link between the recommendations of the supporting evidence; clearly presented recommendations that were specific; and provided a statement around the competing interests of the members of the guideline development group.
One guideline group21 referred to a guideline development handbook and an SR handbook, which provided additional details around incorporating views and preferences of the target population, searching for evidence, methods for formulating recommendations, and so forth. There were inconsistencies in reporting if the guideline was externally reviewed, a procedure for updating the guideline, description of facilitators and barriers to guideline application, and resource implications across the guidelines.
Additional details regarding the strengths and limitations of included publications are provided in Appendix 3.
Summary of Findings
Appendix 4 presents the main study findings.
There was some overlap in the primary studies that were included in the SRs; therefore, to avoid duplication of results, outcome data from an individual primary study were reported for most SRs. Yao et al. (2022)18 and Sokolakis and Hatzichristodoulou (2019)20 presented meta-analyzed results, thus there was overlap in these results. A citation matrix illustrating the degree of overlap is presented in Appendix 5.
Clinical Effectiveness of ESWT Versus Sham or No Treatment
International Index of Erectile Function – Erectile Function Subscale
Mean score: One RCT in the HTA by Syful Azlie and Izzuna (2023)12 reported a statistically significant difference between those who received ESWT and the sham group at 1-month, 3-months, and 6-months follow-up, with those in the ESWT reporting higher IIEF-EF scores (i.e., less ED). All meta-analyses in Yao et al. (2022)18 reported statistically significant differences in the mean difference, favouring the group who received ESWT. This was reported at 1-month, 3-months, and 6-months follow-up when combining studies of all severities of ED and when subgroup analysis was performed based on severity of ED at baseline (i.e., mild, moderate, or severe). Sokolakis and Hatzichristodoulou (2019)20 reported a statistically significant difference, favouring the group who received ESWT, when all populations were combined. However, when looking at the subgroups of those who responded to PDE5 inhibitors and kidney transplant recipients, there was no longer a statistically significant difference between those who received ESWT or sham. The difference remained statistically significant in those who did not respond to PDE5 inhibitors and in males after receiving radical cystectomy.
Proportion achieving MCID: When combining all populations, Sokolakis and Hatzichristodoulou (2019)20 reported a statistically significant difference in those who achieved an MCID in the IIEF-EF score in those who received ESWT compared to those who received sham. In subgroup analysis, this statistical difference remained in those who responded to PDE5 inhibitors, those who did not respond to PDE5 inhibitors, and in kidney transplant recipients, but not in males who had undergone radical cystectomy.
Erectile Hardness Scale
Mean score: One RCT in the HTA by Syful Azlie and Izzuna (2023)12 reported a statistically significant difference in those receiving ESWT reporting higher EHS means scores compared to the sham group at 1-month, 3-months, and 6-months follow-up.
Improvement in score to 3 or more: In a meta-analysis of 8 RCTs, Yao et al. (2022)18 reported that males in the ESWT group were more likely to go from an EHS score of 2 or less at baseline to a score of 3 or more after treatment when compared to those who received control. Sokolakis and Hatzichristodoulou (2019)20 also reported a statistically significant difference, with those receiving ESWT more likely to have improvement in EHS scores. This significant difference held in subgroups analysis for those who responded to PDE5 inhibitors, those who did not respond to PDE5 inhibitors, but not in kidney transplant recipients and not in males after receiving radical cystectomy.
Sexual Encounter Profile
Three RCTs in Yao et al. (2022)18 reported on those who answered yes to question 2 and question 3 on the SEP. Question 2 on the SEP asks, “Were you able to insert your penis into your partner’s vagina?” and question 3 asks, “Did your erection last long enough for you to have successful intercourse?” There was no statistical difference in the number of those who answered yes to either question.
Expanded Prostate Cancer Index Composite
Sexual bother score: One observational study from Sighinolfi et al. (2022)17 reported sexual bother scores, but did not provide a measure of statistical significance to determine if there was a difference between groups.
Sexual function score: One observational study from Sighinolfi et al. (2022)17 reported sexual bother scores, but did not provide a measure of statistical significance to determine if there was a difference between groups.
Quality of Life
Rosenberg et al. (2023)16 reported a statistically significant difference in the mean difference in quality of life, with those who received ESWT having higher scores.
Treatment-Related Adverse Effects
Two RCTs in the SR by Rosenberg et al. (2023)16 reported few treatment-related adverse events in both groups. The meta-analysis in the SR included studies not relevant to this review, thus, a measure of statistical significance was not provided for these 2 studies alone.
Discontinuation From Treatment
Two RCTs in the SR by Rosenberg et al. (2023)16 reported that no participants discontinued from treatment.
Clinical Effectiveness of ESWT Versus Pharmacological Therapy
International Index of Erectile Function – Erectile Function Subscale
Mean score: One RCT in the HTA by Syful Azlie and Izzuna (2023)12 reported a higher mean IIEF-EF score in the ESWT group compared to the pharmacological therapy group at 12-weeks follow-up but does not provide a measure of statistical significance. The 2 observational studies in this HTA12 reported no statistically significant difference between the 2 groups. One observational study in the SR by Sighinolfi et al. (2022)17 reported similar scores at 3-months follow-up, with higher scores in the ESWT group at 6-months and 12-months follow-up, but no measure of statistical significance was provided.
Proportion achieving MCID: One observational study in the HTA by Syful Azlie and Izzuna (2023)12 reported no difference in those who achieved an MCID in the IIEF-EF score between groups.
Erectile Hardness Scale
Mean score: One RCT in the HTA by Syful Azlie and Izzuna (2023)12 reported similar mean EHS scores in the ESWT group and the pharmacological therapy group at 12-weeks follow-up. One observational study in this HTA12 reports no statistically significant difference between the 2 groups.
Improvement in score to 3 or more: One observational study in the SR by Sighinolfi et al. (2022)17 reported no statistical difference in those who had an improvement in the EHS score to 3 or more between the ESWT group and the pharmacological therapy groups at 3-weeks, 1-month, and 3-months follow-up. However, at 6-months follow-up, those who received ESWT were more likely to have improved their EHS score to 3 or more.
Self-Esteem and Relationship
One observational study in Syful Azlie and Izzuna (2023)12 reported no statistical difference in SEAR score between those who received ESWT and those who received pharmacological therapy.
Clinical Effectiveness of ESWT Versus Platelet-Rich Plasma
International Index of Erectile Function – Erectile Function Subscale
Mean score: One observational study in the SR by Panunzio et al. (2023)14 reported that both groups had improvement in the mean IIEF score, “with no statistically significant difference” (p. 567). However, it is not clear if it was no significant difference improvement from baseline or between groups at follow-up.
Erectile Hardness Scale
Mean score: Mean EHS scores of 3.04 versus 3.89 were provided in Panunzio et al. (2023)14; however, no statistical test was provided to measure if there was a statistical difference between the 2 groups.
Self-Esteem and Relationship
One observational study in the SR by Panunzio et al. (2023)14 reported mean SEAR scores in ESWT and platelet-rich plasma groups, 45.25 and 48.33, respectively, but did not provide a measure of statistical significance.
Discontinuation From Treatment
One observational study in the SR by Panunzio et al. (2023)14 reported that no participants discontinued from treatment.
Clinical Effectiveness of ESWT Versus Different Protocol of ESWT
International Index of Erectile Function – Erectile Function Subscale
Increase in IIEF-EF score or proportion achieving MCID: The SR by Sokolakis and Hatzichristodoulou (2019)20 included 3 RCTs that evaluated different Li-ESWT treatment protocols. These RCTs were included only in Sokolakis and Hatzichristodoulou20 (i.e., no overlap with other SRs). One RCT had no statistically significant difference in those who had an IIEF-EF score increase by more than 5 when comparing 5 sessions versus 10 sessions. The other RCT reported that 62% of males who received 6 treatments (1 per week for 6 weeks) achieved MCID in the IIEF-EF score compared to 71% who received 12 treatments (2 per week for 6 weeks). Sokolakis and Hatzichristodoulou (2019)20 reported the increase of IIEF-EF scores since baseline, but did not report if these differences were statistically significant between groups.
Erectile Hardness Scale
Improvement in score to 3 or more: One RCT in Sokolakis and Hatzichristodoulou (2019)20 compared different ESWT protocols, 10 sessions versus 5 sessions. There was no statistically significant difference between protocols in the number of males who improved to a EHS score of 3 or more.
Sexual Encounter Profile
Two RCTs in Sokolakis and Hatzichristodoulou (2019)20 reported on the proportion of males who answered yes to question 3 in the SEP, but no statistical test was provided to measure if there was a statistical difference between the 2 groups.
Guidelines Regarding the Use of ESWT
Four evidence-based guidelines4,21-23 were identified providing recommendations for ESWT for the treatment of ED.
Recommendations for the use of Li-ESWT vary across the guidelines. The European Association of Urology guideline (2024)21 recommends the use of Li-SWT for ED in specific patients, including those with mild vasculogenic ED, as an alternative therapy in patients who were well-informed and who do not wish to have or are not suitable for oral vasoactive therapy, and in patients with vasculogenic ED who do not respond well to PDE5 inhibitors (quality of evidence: not reported; strength rating: weak). The Asia-Pacific Society for Sexual Medicine guideline (2021)22 has similar recommendations, stating that clinical adoption of Li-ESWT should be restricted to males with mild to moderate vasculogenic ED, who either responded or did not respond to PDE5 inhibitors, and Li-ESWT should ideally be performed in highly specialized centres with documented experience with Li-ESWT (based on SRs of RCTs or nonrandomized studies). Conversely, the Canadian Urological Association guideline (2021)4 suggests against the use of Li-SWT for patients with ED (quality of evidence: low; strength rating: conditional). Last, the European Society for Sexual Medicine guideline (2019)23 does not provide a recommendation as the current evidence is still controversial and more high-quality studies are needed.
The Asia-Pacific Society for Sexual Medicine guideline (2021)22 recommends that there is a need to define which subgroup of ED population is best suited and which Li-ESWT protocols to use (based on SRs of RCTs or nonrandomized studies). The European Society for Sexual Medicine guideline (2019)23 also states that there are only a few studies comparing different treatment protocol with the same shockwave generator, therefore a specific protocol cannot be suggested. Further, the European Society for Sexual Medicine guideline (2019)23 states that there are no studies that compared linear to focused SWT, thus, research is needed. Both the Asia-Pacific Society for Sexual Medicine guideline (2021)22 and the European Society for Sexual Medicine guideline (2019)23 states that Li-ESWT is a safe and well-tolerated procedure (based on SRs of RCTs).
Limitations
One HTA,12 1 overview of SRs,13 and 7 SRs14-20 were identified with primary studies that evaluated ESWT for ED. Overall, the quality of conduct and reporting for these reviews was mixed (e.g., no supplemental searching, lack of details around the methods of study selection, lack of details around the participants in the primary studies, no list of excluded studies), making it difficult to determine if all relevant primary studies were captured by the HTA, overview of SRs, and SRs. Additionally, SRs did not always report on the comorbid risk factors of the participants in the primary studies (e.g., diabetes mellitus, cardiovascular disease, or medication use), which may impact the reason for experiencing ED and the efficacy of ESWT in treating ED. One SR15 identified 28 relevant studies, which would be the most comprehensive SR; however, there were several limitations to the conduct and reporting of this SR. Only 1 electronic database was searched, there are no details around how study selection was performed, how the critical appraisal of the primary studies was not performed, there are no descriptors of the comparators, and they only report the results in the active treatment group. We have included this review; however, we have not reported the results, due to their significant limitations. There were 9 primary studies in this SR that were not captured by the other included SRs. References for these studies have been provided in Appendix 6.
Some SRs were conducted in specific populations, for example, in males with Peyronie disease, with chronic pelvic pain, and who had undergone prostatectomy. In these SRs, they were included for these reasons, and it is difficult to determine if the participants also had ED, as it is not always described in the inclusion criteria of the study or provided in the population characteristics in the SR. Therefore, it is possible that some primary study results in the included SRs were missed for these populations. Additionally, ESWT for chronic pelvic pain syndrome can be applied using a perineal approach and therefore may not be comparable to ESWT delivered on the penis.
There is variation in the ESWT protocols across primary studies in the SRs, in terms of the number of treatments, the number of weeks in which the treatments are given, the energy density of the treatment, the shockwave frequency (Hz), the number of pulses per treatment and overall, and the different types of shockwaves (e.g., linear or focused). Sokolakis and Hatzichristodoulou (2019)20 is the only SR that included studies (n = 3) that compared some of these protocols, with variation of the protocols compared.
There are several limitations in the outcomes and reporting of these outcomes in the SRs. First, reported outcomes are subjective and may be influenced by the knowledge of intervention received. RCTs with blinded participants would not be impacted, but outcomes from RCTs where blinding was not possible (e.g., ESWT versus PRP) and in observational studies where the participant knew they were receiving active treatment may be influenced by this knowledge. Second, adverse effects of treatment were poorly reported. One SR reported adverse effects of treatment,16 and 2 SRs reported on discontinuation from treatment.14,16 It is unclear if this is because they are not reported in the primary studies included in the SRs or if the SR authors did not extract these outcomes. Two international guidelines state that ESWT is safe and well-tolerated, with 1 of the guidelines providing 12 references of single-arm and sham-controlled trials23 and 1 guideline providing 8 references to clinical trials and SRs22 to support statements around safety and tolerability. Last, SRs did not always report on the variance (e.g., SD) or on the measure of difference between the groups (e.g., P value), making it difficult to determine if results were statistically significant or not.
The primary studies included in the SRs have a small number of participants. For example, in the 16 RCTs included in Yao et al. (2022),18 the range of participants in the primary studies is 20 to 118, with a median of 63 participants. Meta-analysis offers additional precision by increasing the number of participants contributing to the pooled estimate; however, the meta-analyses in the SRs had high heterogeneity. This was sometimes explained by conducting subgroup analyses (e.g., mild baseline severity of ED18), but heterogeneity in most subgroup analyses remained high. No SRs conducted a subgroup meta-analysis based on type of ED (e.g., vasculogenic, males who had undergone prostatectomy).
Follow-up for most primary studies are 1 month, 3 months, and 6 months, with few reporting at 12 months, and none of the relevant primary studies within the SRs reporting after 12 months. Guidelines have also highlighted this limitation and have stated the uncertainty of the clinical long-term significance of the improvement offered from treatment.22
Results from the primary studies included in the SRs may be generalizable to clinical practice in Canada, as they included males with vasculogenic ED and with ED with complications (e.g., prostatectomy); however, results from the primary studies included in the SRs in males with vasculogenic ED may not be generalizable to males with Peyronie disease, who had received radiotherapy for prostate cancer, or who had received prostatectomy, and vice versa. Guidelines provide recommendations on specific populations who should receive ESWT for ED (e.g., males with mild vasculogenic ED, those who did not respond well to PDE5 inhibitors), but also highlight the need to define which subgroup of the ED population is best suited to received ESWT.22 The Canadian Urology Association guideline (2021)4 suggested against the use of ESWT in males with ED; however, this was based on 4 RCTs (after removing 3 RCTs that were rated as high risk of bias) with low levels of certainty.
Conclusions and Implications for Decision-Making or Policy-Making
One HTA,12 1 overview of SRs,13 and 7 SRs14-20 were identified with primary studies that evaluated ESWT for ED. Four guidelines4,21-23 were identified that provided recommendations for the use of ESWT in males with ED. Overall, treatment with ESWT for ED increases the mean score of the IIEF-EF scale, when compared to sham or no treatment. However, ESWT when compared to sham or no treatment, may not be beneficial in all men, for example, in kidney transplant recipients.20 Further, SRs report a clinically meaningful improvement in the IIEF-EF score (i.e., those achieving an MCID) in most males who received ESWT compared to sham treatment.20 Poor reporting of patient populations and high heterogeneity leads to uncertainty in what population is best suited for ESWT. Most males also see an improvement (i.e., ≥ 3) on the EHS score,18,20 with the exception of kidney transplant recipients and males after receiving radical cystectomy20; however, there are few studies that report on these populations. There was little difference in other outcomes (e.g., SEAR score,12,14 SEP,18,20 sexual bother score, and sexual function score17); however, this was sparsely reported in the SRs and only in 1 to 3 primary studies in the SRs. There were few statistically significant differences in outcomes when comparing ESWT to pharmacological therapy, when compared to platelet-rich plasma, or when comparing different ESWT treatment protocols. Results should be interpreted with caution, as there were several limitations identified in the conduct and reporting of the HTA, overview of SRs, and SRs that were included. Limitations in conduct reduces our confidence that all relevant studies were captured, all relevant data were extracted, studies were properly critically appraised, and data were appropriately meta-analyzed. Limitations in reporting reduces transparency and confidence in the quality of conduct. Last, several included studies did not report a measure of statistical significance between groups, which limits interpretation if there were differences between the 2 groups.
Twenty-five SRs were identified and evaluated for overlap, with 7 SRs included in this review, showing significant overlap in the SRs that have been published. However, the quality of conduct and reporting of most of the included SRs highlights the need for a well-conducted and well-reported comprehensive review on the efficacy of ESWT for the treatment of ED. A new SR should be done to address the limitations identified in the existing HTA, overview of SRs, and SRs included, with the goal of increasing transparency, and improving the quality of conduct and reporting. It should include comparative studies (i.e., randomized and comparative observational studies) in all populations, which may allow for subgroup analysis and further evaluation of heterogeneity of the included studies, recognizing that the ability to conduct these subgroup analyses would be dependent on the quality of the conduct and reporting of the primary studies. The SR by Rosenberg et al. (2023),16 specific to males with Peyronie disease, was the only SR to provide summary of findings tables. This additional step should be taken in the new SR to determine the certainty of the evidence.
There is variation in recommending ESWT in the included guidelines. Two guidelines recommend ESWT in males with mild21 or mild to moderate22 vasculogenic ED, and in who do not wish or are not suitable for vasoactive therapy,21 and in patients with vasculogenic ED who are do not respond well to PDE5 inhibitors.21 The Canadian Urology Association4 suggests against the use of ESWT in males with ED; however, this is based on 4 RCTs and low levels of certainty in the evidence. The fourth guideline23 does not provide a recommendation, as “current evidence is promising but controversial.” It is important to highlight that this guideline was published in 2019 and does not include studies published since December 2018.
Transparency in conduct and reporting across SRs and guidelines may help identify differences in included studies, risk of bias assessments, conclusions, and recommendations. Lack of transparency leads to the inability to determine why differences occur. For example, although risk of bias assessment was undertaken in most SRs, there is a lack of transparency on how judgments were made (i.e., no explanatory statement) and there is variation in how primary studies were assessed between reviews and guidelines. The Canadian Urology Association guideline (2021)4 rated 3 primary studies as high risk and excluded them from the analysis that was used to provide the final recommendation (i.e., suggest against the use of Li-ESWT). However, in Yao et al. (2022),18 2 of these primary studies were rated as low risk for all domains, with the third study rated as low risk in 5 domains and unclear in 2 domains. With no explanatory statements on why these judgments were made, the reader has no context to the judgment. Future SRs should aim to be more transparent in their reporting.
For primary studies, clinical trials with longer term follow-up should be performed to determine how long the effects of ESWT last and if, and when, re-treatment with ESWT might be necessary.
Other implications to consider are the accessibility of the technology and the health care resources to administer the ESWT. This is highlighted in the Asia-Pacific Society for Sexual Medicine guideline (2021)22 that states ESWT should be administered in specialized centres with experience in administering this therapy. It is not mentioned in the included SRs who administered the ESWT and the length of time (e.g., in minutes) of treatment. Human resources and time allocated for treatment should be considered for decision-making and policy-making.
Acknowledgement: This document was externally reviewed by a content expert who has granted permission to be cited: Dr. Premal Patel, MD, FRSCS, with the University of Manitoba.
References
1.Rosen RC, Khera M. Epidemiology and etiologies of male sexual dysfunction. UpToDate; 2024.
2.Grover SA, Lowensteyn I, Kaouache M, et al. The Prevalence of Erectile Dysfunction in the Primary Care Setting. Importance of Risk Factors for Diabetes and Vascular Disease. Arch Intern Med. 2006;166:213-219. PubMed
3.Quinn-Nilas C, Milhausen RR, McKay A, Holzapfel S. Prevalence and Predictors of Sexual Problems Among Midlife Canadian Adults: Results from a National Survey. Journal of Sexual Medicine. 2018;15:873-879. PubMed
4.Domes T, Najafabadi BT, Roberts M, et al. Canadian Urological Association guideline: Erectile dysfunction. Can Urol Assoc J. 2021;15(10):310-322. PubMed
5.Khera M. Treatment of male sexual dysfunction. UpToDate; 2024.
6.Katz JE, Clavijo RI, Rizk P, Ramasamy R. The Basic Physics of Waves, Soundwaves, and Shockwaves for Erectile Dysfunction. Research Support, Non-U.S. Gov't Review. Sex Med Rev. 01 2020;8(1):100-105. doi:https://dx.doi.org/10.1016/j.sxmr.2019.09.004
7.Liu JL, Chu KY, Gabrielson AT, et al. Restorative Therapies for Erectile Dysfunction: Position Statement From the Sexual Medicine Society of North America (SMSNA). Review. Sex Med. Jun 2021;9(3):100343. doi:https://dx.doi.org/10.1016/j.esxm.2021.100343 PubMed
8.Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. NOT IN FILE. PubMed
9.Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. Journal of Epidemiology and Community Health. 1998;52(6):377-384. PubMed
10.Agree Next Steps C. The AGREE II Instrument. AGREE Enterprise; 2017. Accessed 1800 Jan 1. https://www.agreetrust.org/wp-content/uploads/2017/12/AGREE-II-Users-Manual-and-23-item-Instrument-2009-Update-2017.pdf
11.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. Journal of Clinical Epidemiology. 2009;62(10):e1-e34. PubMed
12.Syful Azlie M, Izzuna M. Extracorporeal shockwave therapy for the treatment of erectile dysfunction. Technology Review. 2023. 005-2023.
13.Medrano-Sanchez EM, Pena-Cantonero B, Candon-Ballester P, Blanco-Diaz M, Diaz-Mohedo E. Effectiveness of Low-Intensity Extracorporeal Shock Wave Therapy in Erectile Dysfunction: An Analysis of Sexual Function and Penile Hardness at Erection: An Umbrella Review. Review. J. Feb 04 2024;14(2):04. doi:https://dx.doi.org/10.3390/jpm14020177
14.Panunzio A, Labate C, Zacheo F, et al. Platelet-rich plasma intracavernosal injections for the treatment of primary organic erectile dysfunction: a systematic review and meta-analysis of contemporary controlled studies. Systematic Review Meta-Analysis Review. Int J Impot Res. Sep 2024;36(6):562-571. doi:https://dx.doi.org/10.1038/s41443-023-00798-y PubMed
15.Bocchino AC, Pezzoli M, Martinez-Salamanca JI, Russo GI, Lo Giudice A, Cocci A. Low-intensity extracorporeal shock wave therapy for erectile dysfunction: Myths and realities. Review. Investig Clin Urol. 03 2023;64(2):118-125. doi:https://dx.doi.org/10.4111/icu.20220327
16.Rosenberg JE, Ergun O, Hwang EC, et al. Non-surgical therapies for Peyronie's disease. Systematic Review Review Research Support, Non-U.S. Gov't. Cochrane Database Syst Rev. 07 17 2023;7:CD012206. doi:https://dx.doi.org/10.1002/14651858.CD012206.pub2
17.Sighinolfi MC, Eissa A, Bellorofonte C, et al. Low-intensity Extracorporeal Shockwave Therapy for the Management of Postprostatectomy Erectile Dysfunction: A Systematic Review of the Literature. Review. Eur Urol Open Sci. Sep 2022;43:45-53. doi:https://dx.doi.org/10.1016/j.euros.2022.07.003 PubMed
18.Yao H, Wang X, Liu H, et al. Systematic Review and Meta-Analysis of 16 Randomized Controlled Trials of Clinical Outcomes of Low-Intensity Extracorporeal Shock Wave Therapy in Treating Erectile Dysfunction. Meta-Analysis Research Support, Non-U.S. Gov't Systematic Review. Am J Mens Health. Mar-Apr 2022;16(2): 15579883221087532. doi:https://dx.doi.org/10.1177/15579883221087532 PubMed
19.Marchioni M, De Francesco P, Castellucci R, et al. Management of erectile dysfunction following robot-assisted radical prostatectomy: a systematic review. Systematic Review. Minerva Urol Nefrol. Oct 2020;72(5):543-554. doi:https://dx.doi.org/10.23736/S0393-2249.20.03780-7 PubMed
20.Sokolakis I, Hatzichristodoulou G. Clinical studies on low intensity extracorporeal shockwave therapy for erectile dysfunction: a systematic review and meta-analysis of randomised controlled trials. Meta-Analysis Systematic Review. Int J Impot Res. May 2019;31(3):177-194. doi:https://dx.doi.org/10.1038/s41443-019-0117-z PubMed
21.Salonia A, Bettocchi C, Capogrosso P, et al. EAU Guidelines on Sexual and Reproductive Health. Eur Urol; 2024.
22.Chung E, Lee J, Liu CC, Taniguchi H, Zhou HL, Park HJ. Clinical Practice Guideline Recommendation on the Use of Low Intensity Extracorporeal Shock Wave Therapy and Low Intensity Pulsed Ultrasound Shock Wave Therapy to Treat Erectile Dysfunction: The Asia-Pacific Society for Sexual Medicine Position Statement. Review. World j. Jan 2021;39(1):1-8. doi:https://dx.doi.org/10.5534/wjmh.200077
23.Capogrosso P, Frey A, Jensen CFS, et al. Low-Intensity Shock Wave Therapy in Sexual Medicine-Clinical Recommendations from the European Society of Sexual Medicine (ESSM). Review. J Sex Med. 10 2019;16(10):1490-1505. doi:https://dx.doi.org/10.1016/j.jsxm.2019.07.016
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Table 2: Characteristics of Included HTAs, Overview of Systematic Reviews, and Systematic Reviews
Study citation, country, funding source | Study designs and numbers of primary studies included | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Health technology assessment | ||||
Syful Azlie and Izzuna (2023)12 Malaysia Funding source: Ministry of Health Malaysia | 13 studies in total published up to April 2023; 6 SRs, 3 RCTs, and 2 nonrandomized studies relevant to the present review. To reduce overlap, 2 RCTs and 2 nonrandomized studies are reported in this review. | Men, 18 years and older with vasculogenic, general, or diverse pathogeneses (psychogenic, organic and mixed) ED. N in relevant studies = 251 | Intervention: Li-ESWT Comparator: pharmacologic therapy, medication refractory patients or in those with intolerable side effects, medical devices, combination therapy, placebo (sham) | Outcomes: effectiveness (e.g., IIEF-EF score, EHS, treatment satisfaction), safety, organizational issues (e.g., procedural time), economic implications Follow-up: up to 6 months |
Overview of systematic reviews | ||||
Medrano-Sanchez et al. (2024)13 Spain Funding source: none | 5 systematic reviews published up to June 2023; 5 relevant to the present review. All SRs have been evaluated for overlap of the SR and have either been excluded due to primary study overlap or have been reported separately in this review. | Males with vascular-origin ED | Intervention: Li-ESWT Comparator: placebo | Outcomes: sexual function (i.e., IIEF-EF), penile hardness at erection (EHS) Follow-up: NR |
Systematic reviews | ||||
Panunzio et al. (2024)14 Italy Funding source: NR | 7 studies in total published up to July 2023; 1 nonrandomized study relevant to this review. | Males 18 years and older with primary organic ED N in relevant study = 60 | Intervention: platelet-rich plasma intracavernosal injections alone or in combination with other therapies Comparator: pharma, ESWT, placebo | Outcomes: IIEF-5, EHS, SEAR, adverse events Follow-up: 3 months |
Bocchino et al. (2023)15 Italy Funding source: none | 52 studies in total published between 2012 and August 2022; 22 RCTs and 6 nonrandomized studies relevant to this review. No outcome data presented for comparator group, so no outcome data has been presented in this review. | Males with ED (according to European guideline diagnostic criteria) | Intervention: Li-ESWT Comparator: NR | Outcomes: Efficacy (e.g., IIEF-5, EHS, peak systolic velocity), safety (adverse events) Follow-up: up to 12 months |
Rosenberg et al. (2023)16 US Funding source: Internal salary support for members of investigator team, Minneapolis Veterans’ Administration Health Care System, Urology Section. External support: None | 14 RCTs in total published up to September 23, 2022; 2 RCTs relevant to this review | Males 18 years and older with a clinical diagnosis of Peyronie disease N in relevant studies = 136 | Intervention: oral therapies, injection therapies, mechanical therapies Relevant Intervention: mechanical therapy (i.e., ESWT) Comparator: placebo, no treatment | Outcomes: Patient-reported ability to have intercourse, quality of life, treatment-related adverse effects, penile curvature, discontinuation of treatment, subjective patient-reported change in penile curvature, improvement in penile pain Follow-up: up to 26 weeks after end of treatment |
Sighinolfi et al. (2022)17 Italy Funding source: none | 9 studies in total up to April 2022; 3 RCTs, 3 nonrandomized studies relevant to this review | Patients with postprostatectomy ED N in relevant studies = 583 | Intervention: Li-ESWT with or without pharmacological therapy Comparator: delayed Li-ESWT, pharmacological therapy, sham, no treatment | Outcomes: IIEF-5 score, EHS, sexual bother score from Expanded Prostate Cander Index Composite, sexual function score from Expanded Prostate Cander Index Composite, Sexual Health Inventory for Men (not reported in relevant studies) Follow-up: up to 12 months |
Yao et al. (2022)18 China Funding source: National Nature Science Foundation of China and Taishan Scholars Program of Shandong Province | 16 studies in total published between July 2011 to June 2021; 16 RCTs relevant to this review | Males with ED, with or without complications, any severity of ED, males who responded and did not respond to PDE5 inhibitors | Intervention: Li-ESWT with or without pharmacological therapy Comparator: sham, pharmacological therapy, no treatment | Outcomes: IIEF, EHS, sexual encounter profile (SEP) Follow-up: up to 6 months |
Marchioni et al. (2020)19 Italy Funding source: NR | 11 studies in total published up to November 2019; 0 relevant to the this review | Patients with ED after robot-assisted radical prostatectomy | Intervention: conservative (e.g., pharma, topical alprostadil, vacuum device, hyperbaric therapy, Li-ESWT) and surgical treatments (e.g., penile prosthesis) Relevant intervention: Li-ESWT Comparator: NR | Outcomes: erectile function recovery after conservative treatment, sexual function after prosthesis implant Follow-up: up to 24 months |
Sokolakis and Hatzichristodoulou (2019)20 Germany Funding source: NR | 28 studies in total published between January 2010 to September 2018; 14 RCTs relevant to this review (however, 1 RCT was retracted for plagiarized data) | Males with ED, including vasculogenic ED, males with ED after nerve-sparing radical cystectomy, and kidney transplant recipients. Males who responded and those who did not respond to PDE5 inhibitors | Intervention: Li-ESWT Comparator: sham, different protocol of Li-ESWT | Outcomes: IIEF, EHS, sexual encounter profile Follow-up: up to 12 months |
ED = erectile dysfunction; EHS = Erection Hardness Score; IIEF-EF = International Index of Erectile Function – Erectile Function; HTA = health technology assessment; Li-ESWT = low-intensity extracorporeal shockwave therapy; NR = not reported; PDE5 = phosphodiesterase type 5; RCT = randomized controlled trial; SEAR = self-esteem and relationship; SR = systematic review.
Note: This table has not been copy-edited.
Table 3: Characteristics of Included Guidelines
Intended users, target population | Intervention and practice considered | Major outcomes considered | Evidence collection, selection, and synthesis | Evidence quality assessment | Recommendations development and evaluation | Guideline validation |
|---|---|---|---|---|---|---|
Salonia et al. 202421 | ||||||
Intended users: NR Target Population: male sexual dysfunction, male infertility, and male hypogonadism | Screening, diagnosis, treatment, and/or management for late-onset hypogonadism, male sexual dysfunction (e.g., erectile dysfunction, premature ejaculation, other ejaculatory disorders), sexual desire, penile curvature, penile size abnormalities and dysmorphophobia, priapism, male infertility. | There are no details within this guideline around what outcomes were considered. | The European Association of Urology uses a staged approach to evidence review. First searching for existing systematic reviews, then conducting a new systematic review, if required, using gold standard methods. | Dependent on the study design, for example, the Cochrane risk of bias tool version 1 for randomized controlled trials. | Consensus, using a recommendations worksheet considering the overall certainty of the evidence, the balance of benefits and harms, differences in patient values and preferences, or uncertainty about them, and uncertainty about costs and resource utilization. | External review (no information on who provided this review). |
Domes et al. 20214 | ||||||
Intended users: learners and practitioners Target population: males with erectile dysfunction | Patient assessment including testing (e.g., laboratory) and treatment options (e.g., Li-SWT, pharmacological, vacuum and pump device). | Improvements in erectile function (measured by the IIEF-EF score), quality of life, and adverse events. | No description provided. | GRADE approach was used to evaluate the certainty in the evidence. | GRADE Evidence to Decision framework, considering the desirable effects, undesirable effects, balance of the effects (net benefit), certainty in estimates of effect, patients’ values and preferences, resources required, cost-effectiveness, equity, feasibility, and acceptability. | NR |
Chung et al. 202122 | ||||||
Intended users: NR Target population: males with erectile dysfunction | Li-ESWT and LIPUS (low-intensity pulsed ultrasound) | Effectiveness, treatment protocols, patient selection, safety | Available literature identified in MEDLINE and Embase. Literature review, analyzed and summarizes, and then presented at a scientific meeting. | “The quality of evidence was graded on the Oxford Centre for Evidence-Based Medicine recommendations.” (p. 2) | Clinical findings were internally discussed, and the quality of evidence was graded. “Any disagreements were resolved by consensus and the clinical principle was given when available data was insufficient or not suitable to draw conclusions.” (p. 2) | NR |
Capogrosso et al. 201923 | ||||||
Intended users: NR Target population: males with erectile dysfunction, Peyronie disease, and chronic prostatitis-chronic pelvic pain syndrome | Li-SWT for erectile dysfunction, Peyronie disease, and chronic prostatitis-chronic pelvic pain syndrome | Treatment efficacy (e.g., IIEF, Erection Hardness Scale), treatment protocol, clinical indications, safety | Abstracts reviewed, then full text for those relevant. Relevant studies were analyzed and summarized after an interactive peer-review process of the panel. When the evidence from RCTs was not enough to draw conclusions for clinical practice, data from nonrandomized cohort studies were assessed. | Cochrane risk of bias tool was used to evaluate randomized controlled trials. The quality of evidence was graded by applying the Oxford Centre for Evidence-Based Medicine recommendation. | The level of evidence was according to the Oxford 2011 criteria and graded using the Oxford Centre for Evidence-Based Medicine recommendations. No recommendations were given when the available data were insufficient to draw conclusions. Disagreements were resolved by consensus. | NR |
GRADE = Grading of Recommendations Assessment, Development and Evaluation; Li-ESWT = low-intensity extracorporeal shockwave therapy; Li-SWT = low-intensity shockwave therapy; NR = not reported; RCT = randomized controlled trial.
Note: This table has not been copy-edited.
Appendix 3: Critical Appraisal of Included Publications
Please note that this appendix has not been copy-edited.
Table 4: Strengths and Limitations of HTA, Overview of Systematic Reviews, and Systematic Reviews Using AMSTAR 28
Strengths | Limitations |
|---|---|
Health technology assessment | |
Syful Azlie and Izzuna (2023)12 | |
|
|
Overview of systematic reviews | |
Medrano-Sanchez et al. (2024)13 | |
|
|
Systematic reviews | |
Panunzio et al. (2024)14 | |
|
|
Bocchino et al. (2023)15 | |
|
|
Rosenberg et al. (2023)16 | |
| None |
Sighinolfi et al. (2022)17 | |
|
|
Marchioni et al. (2020)19 | |
|
|
Yao et al. (2020)18 | |
|
|
Sokolakis and Hatzichristodoulou (2019)20 | |
|
|
AMSTAR 2 = A Measurement Tool to Assess Systematic Reviews 2; ED = erectile dysfunction; HTA = health technology assessment; PICO = Participants, Intervention, Comparator, Outcomes.
Table 5: Strengths and Limitations of Guidelines Using AGREE II10
Item | Salonia et al. (2024)21 | Domes et al. (2021)4 | Chung et al. (2021)22 | Capogrosso et al. (2019)23 |
|---|---|---|---|---|
Domain 1: scope and purpose | ||||
1. The overall objective(s) of the guideline is (are) specifically described. | Yes | Yes | Yes | Yes |
2. The health question(s) covered by the guideline is (are) specifically described. | Yes | Yes | Yes | Yes |
3. The population (patients, public, and so forth) to whom the guideline is meant to apply is specifically described. | Yes | Yes | Yes | Yes |
Domain 2: stakeholder involvement | ||||
4. The guideline development group includes individuals from all relevant professional groups. | Yes | Yes | Yes, based on author affiliations | Yes, based on author affiliations |
5. The views and preferences of the target population (patients, public, and so forth) have been sought. | Yes, in Development handbooka | Unclear, not reported | Unclear, not reported | Unclear, not reported |
6. The target users of the guideline are clearly defined. | No, no explicit statement | Yes | No, no explicit statement | Yes, those in clinical practice |
Domain 3: rigour of development | ||||
7. Systematic methods were used to search for evidence. | Yes, in SR handbookb | Unclear, not well reported | Unclear, not well reported | Yes |
8. The criteria for selecting the evidence are clearly described. | No | Unclear, not reported | Unclear, not well reported | Yes |
9. The strengths and limitations of the body of evidence are clearly described. | No | Yes | No | Yes |
10. The methods for formulating the recommendations are clearly described. | Yes, in SR handbookb | Yes | Yes | Yes |
11. The health benefits, side effects, and risks have been considered in formulating the recommendations. | Yes, in Development handbooka | Yes | Yes | Yes |
12. There is an explicit link between the recommendations and the supporting evidence. | Yes | Yes | Yes | Yes |
13. The guideline has been externally reviewed by experts before its publication. | Yes, in Development handbooka | Unclear, not reported | Unclear, not reported | Unclear, not reported |
14. A procedure for updating the guideline is provided. | Yes, in Development handbooka | No | No | No |
Domain 4: clarity of presentation | ||||
15. The recommendations are specific and unambiguous. | Yes | Yes | Yes | Yes |
16. The different options for management of the condition or health issue are clearly presented. | Yes | Yes | Yes | Yes |
17. Key recommendations are easily identifiable. | Yes | Yes | Yes | Yes |
Domain 5: applicability | ||||
18. The guideline describes facilitators and barriers to its application. | Yes | Yes | No | No |
19. The guideline provides advice and/or tools on how the recommendations can be put into practice. | Yes | No | No | No |
20. The potential resource implications of applying the recommendations have been considered. | Yes, in Development handbooka | Yes | Yes, lack of published data on cost-effectiveness highlighted | No |
21. The guideline presents monitoring and/or auditing criteria. | Yes, in Development handbooka | No | No | No |
Domain 6: editorial independence | ||||
22. The views of the funding body have not influenced the content of the guideline. | Yes | Unclear, not reported | Unclear, not reported | Yes, no funding was received |
23. Competing interests of guideline development group members have been recorded and addressed. | Yes | Yes | Yes | Yes |
AGREE II = Appraisal of Guidelines for Research and Evaluation II; SR = systematic review.
aThe European Association of Urology have a Guidelines Development Handbook which provides a detailed approach to how their guidelines are developed (uroweb.org/eau-guidelines/methodology-policies).
bThe European Association of Urology have a Systematic Review Handbook which provides a detailed methodological approach to how the evidence base is identified (uroweb.org/eau-guidelines/methodology-policies).
Appendix 4: Main Study Findings
Please note that this appendix has not been copy-edited.
Table 6: Summary of Findings by Outcome — International Index of Erectile Function – Erectile Function: Mean (SD) Score
Study | Details (e.g., time point, population) | Intervention | Comparator | Difference between groups |
|---|---|---|---|---|
ESWT vs. sham | ||||
Syful Azlie and Izzuna (2023)12 | ||||
Ong 2022, RCT | 1 month follow-up | 14.1 (NR) | 9.3 (NR) | P < 0.001 |
Ong 2022, RCT | 3 months follow-up | 14.9 (NR) | 8.6 (NR) | P < 0.001 |
Ong 2022, RCT | 6 months follow-up | 14.2 (NR) | 7.9 (NR) | P < 0.001 |
Yao et al. (2022)18 | 1-month follow-up, all ED severities, 13 RCTs | Li-ESWT vs. control: MD = 3.18; 95% CI 1.38 to 4.98; P = 0.0005; I2 = 94% | ||
Yao et al. (2022)18 | 3-month follow-up, all ED severities, 8 RCTs | Li-ESWT vs. control: MD = 3.01; 95% CI 2.04 to 3.98; P < 0.00001; I2 = 57% | ||
Yao et al. (2022)18 | 6-month follow-up, all ED severities, 4 RCTs | Li-ESWT vs. control: MD = 3.20; 95% CI 2.49 to 3.92; P < 0.00001; I2 = 8% | ||
Yao et al. (2022)18 | any follow-up, all severities (baseline), 15 RCTs | Li-ESWT vs. control: MD = 4.02; 95%CI 2.74 to 5.30; P < 0.00001; I2 = 87% | ||
Yao et al. (2022)18 | any follow-up, severe ED at baseline, 6 RCTs | Li-ESWT vs. control: MD = 4.07; 95%CI 0.49 to 7.64; P = 0.03; I2 = 95% | ||
Yao et al. (2022)18 | any follow-up, moderate ED at baseline, 6 RCTs | Li-ESWT vs. control: MD = 4.24; 95%CI 2.88 to 5.59; P < 0.00001 I2 = 47% | ||
Yao et al. (2022)18 | any follow-up, mild ED at baseline, 3 RCTs | Li-ESWT vs. control: MD = 3.87; 95%CI 3.37 to 4.36; P < 0.00001; I2 = 0% | ||
Sokolakis and Hatzichristodoulou (2019)20 | last follow-up, all populations, 8 RCTs | Li-ESWT vs. sham: MD = 3.71; 95%CI 0.29 to 7.14; P = 0.03; I2 = 98% | ||
Sokolakis and Hatzichristodoulou (2019)20 | last follow-up, those who responded to PDE5 inhibitors, 5 RCTs | Li-ESWT vs. sham: MD = 4.33; 95%CI −0.90 to 9.55; P = 0.10; I2 = 98% | ||
Sokolakis and Hatzichristodoulou (2019)20 | last follow-up, those who did not respond to PDE5 inhibitors, 1 RCT | Li-ESWT vs. sham: MD = 5.00; 95%CI 4.01 to 5.99; P < 0.00001 | ||
Sokolakis and Hatzichristodoulou (2019)20 | last follow-up, those who responded to PDE5 inhibitors, kidney transplant recipients, 1 RCT | Li-ESWT vs. sham: MD = 0.69; 95%CI −4.01 to 5.39; P = 0.77 | ||
Sokolakis and Hatzichristodoulou (2019)20 | last follow-up, after receiving radical cystectomy (with bilateral nerve sparing) ED, 1 RCT | Li-ESWT vs. sham: MD = 1.80; 95%CI 1.06 to 2.54; P < 0.00001 | ||
ESWT vs. pharmacological therapy | ||||
Syful Azlie and Izzuna (2023)12 | ||||
Zanaty 2022, RCT | 12 weeks follow-up | 17.64 (4.01) | 15.72 (3.6) | NR |
Lei 2021, observational study | 3 months following initiation of treatment | 21.52 (NR) | 21.26 (NR) | P > 0.05 |
Wang 2023, observational study | 4 weeks after final session | 16.3 (5.5) | 18.3 (6.5) | P > 0.05 |
Sighinolfi et al. (2022)17 | ||||
Karakose 2021, observational study | 3 months follow-up | 7 (2.2) | 7 (2.8) | NR |
Karakose 2021, observational study | 6 months follow-up | 13 (3.3) | 7 (2.9) | NR |
Karakose 2021, observational study | 12 months follow-up | 18 (3) | 9 (3.4) | NR |
ESWT vs. platelet-rich plasma | ||||
Panunzio et al. (2023)14 | 3 months, 1 observational study (Sajjad 2021) | 20.21 (NR) | 21.26 (NR) | NR |
CI = confidence interval; ED = erectile dysfunction; Li-ESWT = low-intensity extracorporeal shockwave therapy; MD = mean difference; NR = not reported; RCT = randomized controlled trial; SD = standard deviation; vs. = versus.
Table 7: Summary of Findings by Outcome — International Index of Erectile Function – Erectile Function (Also Called IIEF-5): Proportion Achieving MCID
Study | Details (e.g., time point, population) | Intervention | Comparator | Difference between groups |
|---|---|---|---|---|
ESWT vs. sham | ||||
Sokolaski and Hatzichristodoulou (2019)20 | Last follow-up, all populations, 7 RCTs | 228/316 | 64/240 | OR = 8.54; 95%CI 2.64 to 27.63; P = 0.0003; I2 = 86% |
Sokolaski and Hatzichristodoulou (2019)20 | Last follow-up, those who responded to PDE5 inhibitors, 4 RCTs | 128/189 | 32/137 | OR = 7.26; 95%CI 1.44 to 36.54; P = 0.02; I2 = 88% |
Sokolaski and Hatzichristodoulou (2019)20 | Last follow-up, those who did not respond to PDE5 inhibitors, 1 RCT | 61/75 | 5/50 | OR = 39.21; 95%CI 13.17 to 116.79; P < 0.0001 |
Sokolaski and Hatzichristodoulou (2019)20 | Last follow-up, those who responded to PDE5 inhibitors, kidney transplant recipients, 1 RCT | 7/10 | 1/10 | OR = 21.00; 95%CI 1.78 to 248.1; P = 0.02 |
Sokolaski and Hatzichristodoulou (2019)20 | Last follow-up, after receiving radical cystectomy (with bilateral nerve sparing) ED, 1 RCT | 32/42 | 26/43 | OR = 2.09; 95%CI 0.82 to 5.34; P = 0.12 |
ESWT vs. pharmacological therapy | ||||
Syful Azlie and Izzuna (2023)12 | 3 months following initiation of treatment, 1 observational study (Lei 2021) | 52.2% | 59.4% | P > 0.05 |
ESWT vs. ESWT (different protocol) | ||||
Sokolakis and Hatzichristodoulou (2019)20 | 1 RCT (Fojecki 2018), IIEF-EF score > 5 | 54% | 47% | NS |
Sokolakis and Hatzichristodoulou (2019)20 | 1 RCT (Kalyvianakis 2018), MCID | 62% | 71% | NR |
CI = confidence interval; ED = erectile dysfunction; ESWT = extracorporeal shockwave therapy; IIEF-EF = International Index of Erectile Function – -Erectile Function; MCID = minimal clinically important difference; OR = odds ratio; RCT = randomized controlled trial; SD = standard deviation; NR = not reported; NS = not significant; PDE5 = phosphodiesterase type 5; vs. = versus.
Table 8: Summary of Findings by Outcome — International Index of Erectile Function – Erectile Function: Increase Since Baseline
Study | Details (e.g., time point, population) | Intervention | Comparator | Difference between groups |
|---|---|---|---|---|
ESWT vs. ESWT (different protocol) | ||||
Sokolakis and Hatzichristodoulou (2019)20 | 1 RCT (Kalyvianakis 2018), protocol A vs. protocol B | + 3.1 | + 5.1 | NR |
Sokolakis and Hatzichristodoulou (2019)20 | 1 RCT (Kalyvianakis 2018), protocol A + C vs. protocol B + D | + 1.8 | + 1.7 | NR |
Sokolakis and Hatzichristodoulou (2019)20 | 1 RCT (Katz 2018), protocol A Vs. protocol B | No significant difference from baseline | + 4.2 | NR |
ESWT = extracorporeal shockwave therapy; NR = not reported; RCT = randomized controlled trial; vs. = versus.
Table 9: Summary of Findings by Outcome — Erectile Hardness Scale: Mean (SD) Score
Study | Details (e.g., time point, population) | Intervention | Comparator | Difference between groups |
|---|---|---|---|---|
ESWT vs. sham | ||||
Syful Azlie and Izzuna (2023)12 | ||||
Ong 2022, RCT | 1 month follow-up | 2.4 (NR) | 1.8 (NR) | P = 0.001 |
Ong 2022, RCT | 3 months follow-up | 2.7 (NR) | 1.7 (NR) | P < 0.001 |
Ong 2022, RCT | 6 months follow-up | 2.7 (NR) | 1.6 (NR) | P < 0.001 |
ESWT vs. pharmacological therapy | ||||
Syful Azlie and Izzuna (2023)12 | ||||
Zanaty 2022, RCT | 12 weeks follow-up | 3.2 (0.76) | 3.1 (0.69) | NR |
Lei 2021, observational study | 3 months following initiation of treatment | NR | NR | P > 0.05 |
ESWT vs. platelet-rich plasma | ||||
Panunzio et al. (2023)14 | 3 months, 1 observational study (Sajjad 2021) | 3.04 (NR) | 3.89 (NR) | NR |
ESWT = extracorporeal shockwave therapy; RCT = randomized controlled trial; SD = standard deviation; NR = not reported; vs. = versus.
Table 10: Summary of Findings by Outcome — EHS: Improvement in EHS Score (≥ 3)
Study | Details (e.g., time point, population) | Intervention | Comparator | Difference between groups |
|---|---|---|---|---|
ESWT vs. sham | ||||
Yao et al. (2022)18 | 8 RCTs, improvement to ≥ 3 | Li-ESWT vs. control: OR = 5.07; 95% CI 1.78 to 14.44; P = 0.002; I2 = 80% | ||
Sokolakis and Hatzichristodoulou (2019)20 | Last follow-up, all populations, 8 RCTs | 186/363 | 61/273 | OR = 4.35; 95%CI 1.82 to 10.37; I2 = 69%; P = 0.002 |
Sokolakis and Hatzichristodoulou (2019)20 | Last follow-up, those who responded to PDE5 inhibitors, 5 RCTs | 129/274 | 30/202 | OR = 5.02; 95%CI 1.51 to 16.73; I2 = 75%; P = 0.003 |
Sokolakis and Hatzichristodoulou (2019)20 | Last follow-up, those who did not respond to PDE5 inhibitors, 1 RCT | 20/37 | 1/18 | OR = 20.00; 95%CI 2.41 to 166.27; P = 0.006 |
Sokolakis and Hatzichristodoulou (2019)20 | Last follow-up, those who responded to PDE5 inhibitors, kidney transplant recipients, 1 RCT | 5/10 | 4/10 | OR = 1.50; 95%CI 0.26 to 8.82; P = 0.65 |
Sokolakis and Hatzichristodoulou (2019)20 | Last follow-up, after receiving radical cystectomy (with bilateral nerve sparing) ED, 1 RCT | 32/42 | 26/43 | OR = 2.09; 95%CI 0.82 to 5.34; P = 0.12 |
ESWT vs. pharmacotherapy | ||||
Sighinolfi et al. (2022)17 | ||||
Jang 2022, observational study | 3 weeks follow-up | 14.6% (n = 41) | 0% | NS |
Jang 2022, observational study | 1 month follow-up | 12.2% (n = 41) | 5.1% (n = 39) | NS |
Jang 2022, observational study | 3 months follow-up | 14.6% (n = 41) | 5.1% (n = 39) | NS |
Jang 2022, observational study | 6 months follow-up | 29.3% (n = 41) | 10.3% (n = 39) | P = 0.034 |
ESWT vs. ESWT (different protocol) | ||||
Sokolakis and Hatzichristodoulou (2019)20 | 1 RCT (Fojecki), group A vs. group B | 34% | 24% | NS |
ED = erectile dysfunction; EHS = Erectile Hardness Scale; ESWT = extracorporeal shockwave therapy; Li-ESWT = low-intensity extracorporeal shockwave therapy; RCT = randomized controlled trial; SD = standard deviation; NR = not reported; NS = not significant; vs. = versus.
Table 11: Summary of Findings by Outcome — Other Patient-Related Outcomes
Study | Details (e.g., time point, population) | Intervention | Comparator | Difference between groups |
|---|---|---|---|---|
ESWT vs. sham | ||||
Sexual encounter profile (SEP) | ||||
Yao et al. (2022)18 | 3 RCTs, follow-up NR, Answered Yes to question 2 | 77/112 | 55/88 | OR = 1.27; 95% CI 0.70 to 2.30; P = 0.43; I2 = 78% |
Yao et al. (2022)18 | 3 RCTs, follow-up NR, Answered Yes to question 3 | 48/112 | 17/88 | OR = 4.24; 95%CI 0.67 to 26.83; P = 0.13; I2 = 84% |
Sexual bother score from Expanded Prostate Cancer Index Composite, mean (SD) score | ||||
Sighinolfi et al. (2022)17 | 6 monthsa,b, 1 observational study (Inoue 2020) | 46.3 (NR) | 54.2 (NR)c | NR |
Sexual function score from Expanded Prostate Cancer Index Composite, mean (SD) score | ||||
Sighinolfi et al. (2022)17 | 6 monthsb, 1 observational study (Inoue 2020) | 19.2 (NR) | 17.9 (NR)c | NR |
Quality of life | ||||
Rosenberg et al. (2023)16 | 1 RCT (Palmieri 2009) | 22.68 (4.5) | 19.62 (4.5) | MD = 3.06; 95%CI 1.30 to 4.82 |
Treatment-related adverse effects | ||||
Rosenberg et al. (2023)16 | 2 RCTs (Chitale 2010, Palmieri 2009), follow-up NR | 6/66 | 2/70 | NRd |
Discontinuation from treatment | ||||
Rosenberg et al. (2023)16 | 2 RCTs (Chitale 2010, Palmieri 2009), follow-up NR | 0/66 | 0/70 | NRd |
ESWT vs. pharmacological therapy | ||||
Self-esteem and relationship (SEAR) | ||||
Syful Azlie and Izzuna (2023)12 | 3 months following initiation of treatment, 1 nonrandomized study (Lei 2021) | NR | NR | P > 0.05 |
ESWT vs. platelet-rich plasma | ||||
Self-esteem and relationship (SEAR) mean (SD) score | ||||
Panunzio et al. (2023)14 | 3 months, 1 observational study (Sajjad 2021) | 45.25 (NR) | 48.33 (NR) | NR |
Discontinuation from treatment | ||||
Panunzio et al. (2023)14 | 1 observational study | 0/30 | 0/30 | |
ESWT vs. ESWT (different protocol) | ||||
Sexual encounter profile (SEP) | ||||
Sokolakis and Hatzichristodoulou (2019)20 | 1 RCT, protocol A vs. protocol B, Question 3 | 47.4% | 65.2% | NR |
Sokolakis and Hatzichristodoulou (2019)20 | 1 RCT, protocol A + C vs. protocol B + D, Question 3 | 61.9% | 68.4% | NR |
ESWT = extracorporeal shockwave therapy; Li- ESWT = low-intensity extracorporeal shockwave therapy; MD = mean difference; NR = not reported; SD = standard deviation; RCT = randomized controlled trial; SD = standard deviation;vs. = versus.
a3-month outcome data also reported but not extracted.
b9- and 12-month data also reported, but both groups had received Li-ESWT at these time points.
cThis group received delayed treatment with Li-ESWT 6 months after radical prostatectomy. There is a third group who did not receive Li-ESWT (data not extracted as they are similar to delayed ESWT group at 6 months).
dThe pooled results includes a study that is not relevant to the this review; therefore, the pooled results was not extracted.
Table 12: Summary of Recommendations in Included Guidelines
Recommendations and supporting evidence | Quality of evidence and strength of recommendations |
|---|---|
Salonia et al. 202421 | |
Use low-intensity shockwave treatment (Li-SWT) with or without PDE5 inhibitors in patients:
Single-arm trials, randomized controlled trials, and a meta-analysis formed the evidence base. However, authors of the meta-analysis outlined that the level of evidence was low, therefore, careful interpretation of the results is required. | Quality of evidence: not reported Strength rating: weak |
Domes et al. 20214 | |
We suggest against the use of Li-SWT for patients with ED. The panel reviewed 7 RCTs comparing Li-SWT to sham treatment. Combining these 7 RCTs there is a statistically significant mean increase in the IIEF-EF score; however, 3 RCTs were high risk of bias. When removing these studies from the meta-analysis, the mean increase in the IIEF-EF score was no longer statistically significant. | Quality of evidence: low levels of certainty in evidence Strength rating: conditional recommendation |
Chung et al. 202122 | |
“There is a need to define which subgroup of ED population is best suited and the LIESWT protocols including modality of shock waves energy, emission frequency and total energy delivery. The patient selection appears paramount to treatment success and patients with mild-moderate ED, younger age group, those with minimal cardiovascular comorbidities, and absence of diabetes or cavernous nerve are likely going to report high EF recovery and spontaneous erection.” (p. 4) Data from systematic reviews and randomized controlled trials were used for this recommendation. The guideline authors state that the outcomes should be interpreted with some caution due to heterogeneity and methodological flaws in the studies. | Level 2; grade B |
“LISWT improves EF scores and penile hemodynamic parameters in men with vasculogenic ED.” (p. 5) “Published literature suggests these positive effects of LIESWT to last up to 12 months after treatment.” (p. 5) Most published studies do not extend beyond 2 years follow-up, so there is some uncertainty of the clinical long-term significance of this improvement. | Level 1; grade B Level 2; grade B |
“The clinical adoption of Li-ESWT as an effective treatment option should be restricted to men with mild-moderate vasculogenic ED, either responder or non-responders to PDE5is, and ideally performed in the high specialized centres with documented experience with this type of therapy.” (p. 5) This recommendation is supported by multiple systematic reviews that reported on International Index of Erectile Function (IIEF) and Erectile Hardness Scale scores (EHS). | Level 2; grade B |
“LISWT is a safe and well-tolerated procedure without clinically significant adverse events.” (p. 6) Treatment-related adverse events and dropout rates due to treatment-related adverse events have been published in clinical trials and systematic reviews. | Level 1; grade A |
Capogrosso et al. 201923 | |
“Patient-reported outcomes (IIEF, EHS): Current evidence is promising but is still controversial; therefore, a clear clinical recommendation of LISWT for ED cannot be made, and more high-quality studies are needed.” (p. 1492) 11 RCTs were identified, but due to high risk of bias, 7 RCTs comparing Li-SWT to sham control were considered by the committee to assess treatment efficacy. Additionally, 5 meta-analyses were identified, 3 with heterogeneous populations, making it difficult to interpret the results on erectile function outcomes. | Not applicable |
“Penile hemodynamics: LISWT significantly improves penile hemodynamic parameters of patients with vasculogenic ED. However, the clinical long-term significance of this improvement is uncertain.” (p. 1492) Three sham-controlled trials were identified, all showing a significant improvement in penile blood flow in the actively treated group compared to the control group. | Level 2; grade C |
“Effect endurance: Current data suggest a variable effect of LISWT on EF up to 12 months after treatment. More data are needed to assess the longer term effects of LISWT.” (p. 1492) All studies suffer from short follow-up. One randomized controlled trial reported results at 6 months follow-up and 1 single-arm cohort study reported 2-year follow-up data. | Level 2; grade C |
“Energy source and type of SW (linear vs focused): Currently, there are no studies comparing the 2 treatment methods. Further research should address the possible differences between focused and linear SW.” (p. 1492) Only 2 RCTs used a linear generator, and 1 meta-analysis had a subgroup analysis according to type of generator used. Overall, current evidence is too limited to draw final conclusions on the best shockwave generator. | Not applicable |
“There are only few data comparing different treatment protocols with the same SW generator; therefore, a specific protocol cannot be suggested.” (p. 1492) Treatment protocols vary widely across the randomized controlled trials, in term of either energy flux density, number of sessions, and length of treatment. No studies directly compared different protocols. Four meta-analyses provided varied results. | Not applicable |
“LISWT for patients with vasculogenic ED, either treatment naïve, responders or non-responders to phosphodiesterase type 5 inhibitors (PDE5is), shows encouraging results, but unambiguous evidence for efficacy is lacking, pooled effect size is modest, and evidence quality is low. Patients should be informed about the conflicting results regarding efficacy of this treatment when discussing LISWT.” (p. 1492) Randomized controlled trials included vasculogenic ED with mild to severe levels, and only 1 trial included those who did not respond to PDE5 with another trial including both those who responded and those who did not respond. Two meta-analyses showed significant improvement in those with mild ED, with the use of PDE5 increasing the improvement. One of the 2 meta-analyses reported improvement in those with severe ED. | Level 2; grade D |
“Safety: LISWT is a safe and well-tolerated procedure without clinically significant adverse events.” (p. 1492) No adverse events have been reported in sham-controlled trials or single-arm cohort studies (referencing 12 studies). | Level 1; grade A |
ED = erectile dysfunction; EF = erectile function; IIEF-EF = International Index of Erectile Function – Erectile Function; Li-SWT = low-intensity shockwave therapy; PDE5 = phosphodiesterase type 5; RCT = randomized controlled trial.
Appendix 5: Overlap Between Included Systematic Reviews
Please note that this appendix has not been copy-edited.
Table 13: Overlap in Relevant Primary Studies Between Included HTA and Systematic Reviews
Primary study citation | Syful Azlie and Izzuna 202312 | Sighinolfi et al. 202217 | Sokolakis and Hatzichristodoulou 201920 | Yao et al. 202218 |
|---|---|---|---|---|
Baccaglini W, et al. J Sex Med. 2019;17(4);688–94. | — | Yes | — | Yes |
Fojecki GL, et al. J Sex Med. 2017;14:106–12. | — | — | Yes | Yes |
Kalyvianakis D, et al. J Sex Med. 2017;14:891–97. | — | — | Yes | Yes |
Kitrey ND. J Urol. 2016;195:1550–55. | — | — | Yes | Yes |
Ladegaard PBJ, et al. Sex Med. 2021;9(3):100338. | — | Yes | — | Yes |
Olsen AB, et al. Scand J Urol. 2015;49:329–33. | — | — | Yes | Yes |
Shendy WS, et al. Andrologia. 2021;53(4):e13997. | Yes | — | — | Yes |
Srini VS, et al. Can J Urol. 2015;22:7614–22. | — | — | Yes | Yes |
Vardi Y, et al. J Urol. 2012;187:1769–75. | — | — | Yes | Yes |
Yamacake KGR, et al. Int J Impot Res. 2019;31:195–203. | — | — | Yes | Yes |
Yee CH, et al. Int JUrol. 2014;21:1041–5. | — | — | Yes | Yes |
Zewin TS, et al. Int Urol Neph. 2018;50(11):2007–14. | — | Yes | Yes | Yes |
HTA = health technology assessment.
Appendix 6: References of Potential Interest
Please note that this appendix has not been copy-edited.
Randomized Controlled Trials
Li-ESWT Versus Sham
Kalyvianakis D, Mykoniatis I, Pyrgidis N, Kapoteli P, Zilotis F, Hatzichristou D. The effect of combination treatment with low-intensity shockwave therapy and daily tadalafil on severe erectile dysfunction: a double-blind, randomized, sham-controlled clinical trial. J Sex Med. 2024 May 28;21(6):533-538. PubMed
Kalyvianakis D, Mykoniatis I, Pyrgidis N, et al. The Effect of Low-Intensity Shock Wave Therapy on Moderate Erectile Dysfunction: A Double-Blind, Randomized, Sham-Controlled Clinical Trial. J Urol. 2022 08;208(2):388-395.
Motil I, Macik D, Sramkova K, Jarkovsky J, Sramkova T. Linear Low-Intensity Extracorporeal Shockwave Therapy as a Method for Penile Rehabilitation in Erectile Dysfunction Patients after Radical Prostatectomy: A Randomized, Single-Blinded, Sham-Controlled Clinical Trial. Urol Int. 2022;106(10):1050-1055. PubMed
Li-ESWT With Vacuum Device Versus Li-ESWT Versus Vacuum Device
Tao R, Chen J, Wang D, et al. The Efficacy of Li-ESWT Combined With VED in Diabetic ED Patients Unresponsive to PDE5is: A Single-Center, Randomized Clinical Trial. Front Endocrinol (Lausanne). 2022;13:937958. PubMed
ESWT Versus Exercise Versus Combine ESWT and Exercise
Salama AB, Abdrabo MS, Abouelnaga WA. Effect of physical exercise combined with shockwave therapy on erectile dysfunction in diabetic patients. Arch Med Sci. 2021;19(5):1207-1213. PubMed
Energy Flux Density and Frequency of Sessions
Kalyvianakis D, Mykoniatis I, Memmos E, Kapoteli P, Memmos D, Hatzichristou D. Low-intensity shockwave therapy (LiST) for erectile dysfunction: a randomized clinical trial assessing the impact of energy flux density (EFD) and frequency of sessions. Int J Impot Res. 2020 May;32(3):329-337. PubMed
Radial Wave
Sandoval-Salinas C, Saffon JP, Martinez JM, Corredor HA, Gallego A. Are Radial Pressure Waves Effective for the Treatment of Moderate or Mild to Moderate Erectile Dysfunction? A Randomized Sham Therapy Controlled Clinical Trial. J Sex Med. 2022 05;19(5):738-744.
Nonrandomized Studies
Dell'Atti L, Slyusar V, Cambise C. Multimodal treatments based on Tadalafil during acute phase of Peyronie's disease: experience at two referral academic centers. Ir J Med Sci. 2024 Oct;193(5):2301-2306. PubMed
Eryilmaz R, Kaplan S, Aslan R, Demir M, Taken K. Comparison of focused and unfocused ESWT in treatment of erectile dysfunction. Aging Male. 2020 Sep;23(3):206-209. PubMed
Ghahhari J, De Nunzio C, Lombardo R, et al. Shockwave Therapy for Erectile Dysfunction: Which Gives the Best Results? A Retrospective National, Multi-Institutional Comparative Study of Different Shockwave Technologies. Surg Technol Int. 2022 May 19;40:213-218. PubMed
Trishch VI, Mysak AI, Trishch AI, Mandzii AP. Assessment of the treatment effectiveness of men with mild and medium degree of erectile dysfunction. Pol Merkur Lekarski. 2024;52(1):79-86. PubMed
Zasieda Y. Combined Treatment with Focused Low-Intensity Shock-Wave Therapy and Androgen-Stimulation Therapy in Men with Corporal Veno-Occlusive Erectile Dysfunction on the Background of Hypogonadotropic Hypogonadism. Georgian Med News. 2020 Oct(307):49-53. PubMed
Guidelines and Recommendations
Guideline Published Before 2019
American Urological Association (AUA). Erectile dysfunction: AUA guideline. 2018. https://www.auanet.org/guidelines-and-quality/guidelines/erectile-dysfunction-(ed)-guideline
Additional References
Systematic Review Protocol
Ergun O, Kim K, Kim MH, Hwang EC, Blair Y, Gudeloglu A, Parekattil S, Dahm P. Low‐intensity shockwave therapy for erectile dysfunction [protocol]. Cochrane Database Syst Rev. 2023 Sep 20;2023(9):CD013166. doi: 10.1002/14651858.CD013166.pub2. PMCID: PMC10510023. https://www.cochranelibrary.com/cdsr/doi/10.1002/14651858.CD013166.pub2/full
Systematic Review With Questionable ED Among Participants in Primary Studies
Man L, Li G. Low-intensity Extracorporeal Shock Wave Therapy for Erectile Dysfunction: A Systematic Review and Meta-analysis. Urology. 2018 Sep; 119:97-103. PubMed: PM28962876.
Guideline With Nonsystematic Methodology to Identify Included Studies
Liu JL, Chu KY, Gabrielson AT, et al. Restorative Therapies for Erectile Dysfunction: Position Statement From the Sexual Medicine Society of North America (SMSNA). Sex. 2021 Jun;9(3):100343. PubMed: PM34000480.
Schoofs E, Fode M, Capogrosso P, Albersen M; for the European Association of Urology Young Academic Urologists (EAU - YAU) Men’s Health Group. Current guideline recommendations and analysis of evidence quality on low-intensity shockwave therapy for erectile dysfunction. Int J Impot Res. 2019 May;31(3):209-217. doi: 10.1038/s41443-019-0132-0. Epub 2019 Mar 25..PubMed
ISSN: 2563-6596
Canada’s Drug Agency (CDA-AMC) is a pan-Canadian health organization. Created and funded by Canada’s federal, provincial, and territorial governments, we’re responsible for driving better coordination, alignment, and public value within Canada’s drug and health technology landscape. We provide Canada’s health system leaders with independent evidence and advice so they can make informed drug, health technology, and health system decisions, and we collaborate with national and international partners to enhance our collective impact.
Disclaimer: CDA-AMC has taken care to ensure that the information in this document was accurate, complete, and up to date when it was published, but does not make any guarantee to that effect. Your use of this information is subject to this disclaimer and the Terms of Use at cda-amc.ca.
The information in this document is made available for informational and educational purposes only and should not be used as a substitute for professional medical advice, the application of clinical judgment in respect of the care of a particular patient, or other professional judgments in any decision-making process. You assume full responsibility for the use of the information and rely on it at your own risk.
CDA-AMC does not endorse any information, drugs, therapies, treatments, products, processes, or services. The views and opinions of third parties published in this document do not necessarily reflect those of CDA-AMC. The copyright and other intellectual property rights in this document are owned by the Canadian Agency for Drugs and Technologies in Health (operating as CDA-AMC) and its licensors.
Questions or requests for information about this report can be directed to Requests@CDA-AMC.ca.