CADTH Health Technology Review
Screening for Colorectal Cancer in Individuals Younger Than 50 Years
Rapid Review With Expert Input
Authors: Sara D. Khangura, Carolyn Spry
Key Messages
What Is the Issue?
Incidence of colorectal cancer in individuals younger than 50 years in Canada is rising, despite existing recommendations in Canada advising that colorectal cancer screening be initiated at 50 years.
In response to the also increasing incidence of colorectal cancer observed in other jurisdictions, screening for colorectal cancer in individuals of average risk younger than 50 years has been recommended.
These factors have prompted reconsideration of current Canadian guidelines regarding the age at which colorectal cancer screening should be initiated.
What Did We Do?
To inform considerations about the age at which colorectal cancer screening should best be initiated, CADTH identified and summarized studies comparing colorectal cancer screening in individuals of average risk younger than 50 years with either no screening or screening in individuals of average risk aged 50 years and older.
An information specialist conducted a search of peer-reviewed and grey literature sources. Recommendations from evidence-based guidelines for screening individuals of average risk younger than 50 years were also sought and summarized.
What Did We Find?
Data from 1 retrospective cohort study in the US conducted in a large sample across 13 years suggested there is higher incidence of colorectal cancer among individuals between the ages of 45 and 49 years who underwent screening colonoscopy than in those between the ages of 50 and 54 years.
Data from a retrospective cohort study conducted in Greece with a limited sample size across 1 year of observation demonstrated no difference in the cumulative incidence of colorectal cancer in individuals of average risk younger than 50 years or 50 years and older.
Estimates from 4 modelling studies (1 of which was Canadian) that investigated screening in individuals younger than 50 years indicate that life-years may be gained, colorectal cancer cases and deaths may be reduced, but that numbers of lifetime colonoscopies and complications from screening would likely increase.
One economic evaluation conducted in Portugal concluded that there is no cost-utility for colorectal cancer screening in individuals of average risk younger than 50 years at a willingness-to-pay threshold of €39,760, given current estimates of incidence in this age cohort.
Seven evidence-based guidelines identified recommend that colorectal cancer screening be initiated in individuals of average risk at age 45 years, whereas 1 guideline recommends against screening in individuals of average risk beginning at 45 years and 1 guideline recommends against screening beginning at age 40 years. Most evidence-based guidelines highlight the lack of empirical evidence describing clinical effectiveness and cost-effectiveness as limitations when developing recommendations.
What Does It Mean?
Empirical data describing the effectiveness of colorectal cancer screening in individuals of average risk younger than 50 years remain limited, although a preponderance of evidence-based guidelines identified by this review recommend in favour of doing so.
Modelled data estimate that colorectal cancer screening in individuals younger than 50 years may produce benefits, although these estimates are vulnerable to model inputs and assumptions (perfect adherence to screening protocols, for instance), and may not adequately account for the potential harms of screening.
Additional opportunities for maximizing the benefits of colorectal cancer screening may include targeting increased uptake among disadvantaged and high-risk groups, including those 50 years and older.
Broader considerations that address societal benefit and costs — including health equity and implementation — are essential to inform decision-making concerning colorectal cancer screening in individuals of average risk younger than 50 years.
Acknowledgement
This document was externally reviewed by a content expert who has granted permission to be cited.
Linda Rabeneck, MD MPH FRCPC
Professor of Medicine
University of Toronto
Abbreviations
CRC
colorectal cancer
FIT
fecal immunochemical test
LYG
life-years gained
Context and Policy Issues
What Is Colorectal Cancer?
Colorectal cancer (CRC) has been described as 1 of the most common types of cancer and causes of death from cancer in the world.1-3 In Canada, CRC is the third most common cancer, with an estimated 24,100 Canadians expected to be diagnosed in 2023.4
CRC is usually asymptomatic in its early stages, with symptoms developing as the disease progresses.5 Symptoms and signs occurring in later stages of the disease may include abdominal pain, anemia, rectal bleeding, and bowel obstruction.5 It is believed that CRC generally develops across what is known as the adenoma-carcinoma sequence, during which initially noncancerous lesions, known as adenomatous polyps, develop into cancer.6-8 This sequence can take years or decades.8 It is during this time that an opportunity for detection of precancerous lesions in the colon and rectum is available, allowing for early treatment, which can reduce morbidity and mortality.9 Survival rates for CRC are closely associated with the stage of cancer at detection, with earlier stages resulting in higher survival and later-stage cancers resulting in lower survival rates.10-12
What Is the Current Practice for CRC Screening?
There are 2 types of tests available to screen for CRC: stool based (including fecal immunochemical testing) and direct visualization techniques (including colonoscopy).13 The fecal immunochemical test (FIT) is a measure of hemoglobin detected in stool samples,14 which can indicate the presence of adenomatous polyps or CRC. A positive FIT is followed up with a diagnostic colonoscopy.15 Colonoscopy is an endoscopic procedure used for diagnosis and treatment (i.e., colonoscopy can be used to identify precancerous polyps or lesions and remove them from the colon).15 The benefit of colonoscopy is the opportunity to both identify and remove adenomatous polyps before they develop into invasive CRC.6,8,12,16 However, due to its invasiveness, colonoscopy can also cause harm, such as perforation or bleeding.15,17,18 Although other screening tests for CRC are available,6 this report is limited to a focus on FIT and colonoscopy.
Many current recommendations — including those in Canada19 — advise that people 50 years and older be screened for CRC.20-22 Generally, this is supported in part by evidence indicating that the incidence of CRC is higher in individuals 50 years and older compared with younger individuals.19
Why Is It Important to Do This Review?
The incidence of CRC in people younger than 50 years has been on the rise in Canada and other countries, prompting reconsideration of the recommended age for initiation of CRC screening to include those younger than 50 years.6,7,17,18,23-27 CRC in younger populations has been characterized as more aggressive and resulting in more deleterious outcomes compared with disease identified in older populations.26 Nonetheless, the potential for harm caused by CRC screening, as well as the cost-benefit implications, give pause when considering the optimal age for initiation of CRC screening in younger populations.11,17,18,26
Objective
To help inform decisions concerning policy and practice for CRC screening, this report sought to assemble and summarize available evidence describing the clinical benefits, harms, and recommendations concerning CRC screening in individuals of average risk younger than 50 years.
Research Questions
What is the effectiveness of colorectal cancer screening in average-risk individuals younger than 50 years versus those aged 50 to 75 years on the incidence of and mortality from colorectal cancer?
What is the effectiveness of colorectal cancer screening versus no screening in average-risk individuals younger than 50 years on the incidence of and mortality from colorectal cancer?
What is the cost-effectiveness of screening average-risk individuals younger than age 50 years for colorectal cancer?
What are the evidence-based guidelines regarding screening average-risk individuals younger than age 50 years for colorectal cancer?
Methods
Literature Search Methods
An information specialist conducted a literature search on key resources, including MEDLINE, the Cochrane Database of Systematic Reviews, the International HTA Database, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search approach was customized to retrieve a limited set of results, balancing comprehensiveness with relevancy. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. Search concepts were developed based on the elements of the research questions and selection criteria. The main search concepts were fecal immunochemical test, colonoscopy, and colorectal cancer screening.
CADTH-developed search filters were applied to limit retrieval to health technology assessments, systematic reviews, meta-analyses, indirect treatment comparisons, any type of clinical trial, observational studies, economic studies, and guidelines. Comments, newspaper articles, editorials, and letters were excluded. The search was completed on September 5, 2023, and limited to English-language documents published since January 1, 2017. The search was supplemented by reviewing bibliographies of key papers and through contacts with experts.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
|---|---|
Population | Adult individuals with average riska of developing colorectal cancer |
Intervention | Colorectal cancer screening at age younger than 50 years using colonoscopy or FIT as initial screening test |
Comparator | Q1: Colorectal cancer screening at age 50 to 74 years using colonoscopy or FIT as initial screening test. Q2: No colorectal cancer screening Q3: No colorectal cancer screening Q4: Not applicable |
Outcomes | Q1 and Q2: Clinical benefits (i.e., CRC incidence, CRC mortality) and harms (e.g., test complications [bleeding, perforation], unplanned admission) Q3: Incremental cost per clinical benefit Q4: Recommendations regarding best practices |
Study designs | Health technology assessments, systematic reviews, randomized controlled trials, nonrandomized studies, clinical modelling studies, economic evaluations, evidence-based guidelines |
CRC = colorectal cancer; FIT = fecal immunochemical testing.
aAverage risk was defined as “individuals with no first-degree relative who has been diagnosed with CRC or those with no personal history of colorectal neoplasia or inflammatory bowel disease.”
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, were duplicate publications, or were published before 2017. Guidelines with unclear methodology were also excluded.
Although studies addressing issues of health equity and/or implementation that were not otherwise eligible according to the selection criteria were not included for full summary in this report, they were given consideration, with some information of relevance being summarized.
Critical Appraisal of Individual Studies
The eligible and included publications were critically appraised by 1 reviewer using the following tools as a guide: the Downs and Black checklist28 for nonrandomized studies, the Drummond checklist29 for economic evaluations, and the Appraisal of Guidelines for Research and Evaluation (AGREE) II instrument30 for guidelines. Summary scores were not calculated for the included studies and guidelines; rather, the strengths and limitations of each included publication were described narratively.
Modelling studies for which some data were summarized were not scrutinized using formal critical appraisal tools; rather, key limitations relevant to the methods were highlighted. Sources describing health equity and/or implementation issues of relevance that were not otherwise eligible for this report did not undergo critical appraisal or consideration of methodological approach.
Summary of Evidence
Quantity of Research Available
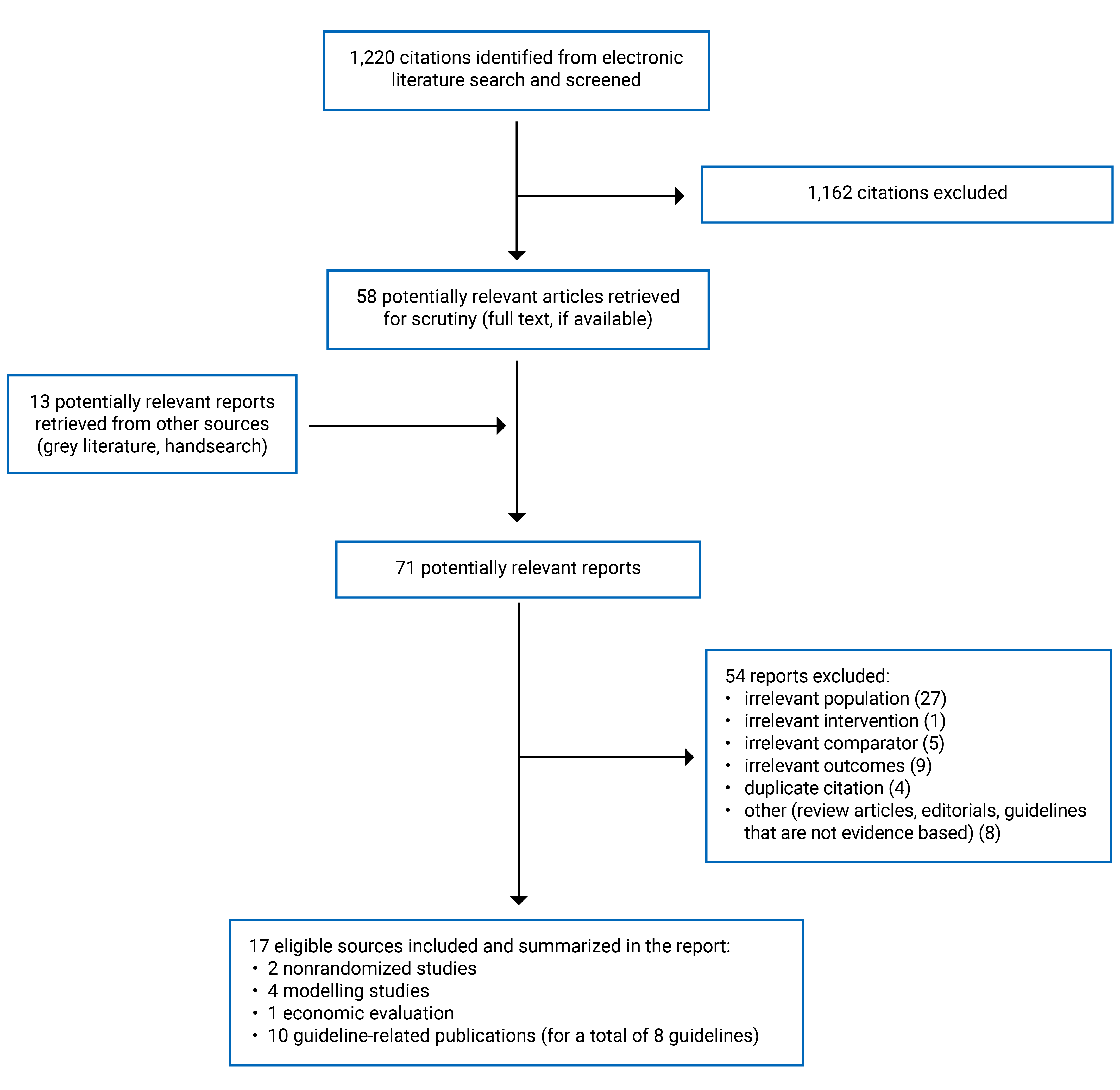
A total of 1,220 citations were identified in the literature search. Following screening of titles and abstracts, 1,162 citations were excluded and 58 potentially relevant reports from the electronic search were retrieved for full-text review. Thirteen potentially relevant publications were retrieved from the grey literature search and hand searches for full-text review. Of these potentially relevant articles, 54 publications were excluded for various reasons, and 17 publications met the inclusion criteria and were included in this report.31-47 The included publications comprised 2 nonrandomized studies,34,46 4 modelling studies,32,36,44,45 1 economic evaluation,33 and 8 evidence-based guidelines (2 of which had 2 related publications: the original full guideline published in 2017 as well as updated recommendations of relevance to this report published in 2022 or 2023).31,35,37-43,47 Appendix 1 presents the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA)48 flow chart of the study selection outlining the inclusion of eligible studies.
Additional references of potential interest are provided in Appendix 5.
Summary of Study Characteristics
Two nonrandomized studies (NRS),34,46 4 microsimulation modelling studies,32,36,44,45 1 economic evaluation,33 and 8 evidence- based guidelines (2 of which had original guidelines published in 2017 with focused updates published in 2022 and 2023) met the eligibility criteria and were summarized in this report.31,35,37-43,47
Details regarding the characteristics of these eligible publications are provided in Appendix 2.
Study Design
Two nonrandomized studies met the review’s eligibility criteria, both of which were retrospective cohort studies published in 202146 and 2020.34
The 4 modelling studies used similar methods, including modifications to existing models. One modelling study used the OncoSim model,45 1 used the CRC Simulated Population Model for Incidence and Natural History (CRC-SPIN),32 1 used the Microsimulation Screening Analysis-Colon (MISCAN-Colon),44 and 1 used the CRC-SPIN, MISCAN-Colon, and Simulation Model of CRC (SimCRC).36 Inputs for the extant Canadian model were based on data from Canada,45 and based on data from the US for the other 3 models.32,36,44 The modelling studies aimed to estimate benefits and/or harms of CRC screening given estimated incidence, natural history, and/or birth cohort effects, with updated incidence data incorporated to account for more recent trends in populations younger than 50 years.32,36,44,45 Two modelling studies were published in 2023,32,45 1 in 2021,36 and 1 in 2018,44 with all using a lifetime time horizon. Three studies assumed complete or perfect adherence to screening protocols and/or follow-up,32,36,44 whereas the Canadian study assumed screening participation based on published data describing this variable.45
One economic evaluation met the review's eligibility criteria, describing a cost-utility analysis published in 2021 and conducted from a societal perspective.33 Data were sourced from reviews of published literature, national statistical data sources, and registries. The time horizon of the cost-utility study was not reported, and a decision tree model was used. The analyses assumed a willingness-to-pay threshold of €39,760 and assumed that screening for CRC is cost-effective for individuals aged 50 years and older.33
The 8 evidence-based guidelines were produced by the American College of Physicians,43 Austrian National Committee for Cancer Screening,31 Kaiser Permanente (2022),42 US Multi-Society Task Force on Colorectal Cancer (which published a full guideline in 2017 and an updated recommendation of relevance in 2022),35,40 American College of Gastroenterology,38 US Preventive Services Task Force,37 American Cancer Society,39 and Cancer Council Australia (i.e., which published a full guideline in 2017 and an updated chapter in 2023).41,47 Guidelines were published between 2017 and 2023, with 3 published in 2023,31,43,47 1 published in 2022,35 2 published in 2021,37,38 1 published in 2018,39 and 2 published in 2017.40,41 All the evidence-based guidelines reported literature searches with some systematic methods used to identify evidence.31,35,37-43,47 All of the guidelines report critical appraisal of the evidence used to inform development of the recommendations,31,37-43,47 with 3 guidelines including a standardized method to assign the quality level of the evidence supporting their recommendations,31,35,38 whereas 3 of the guidelines include some acknowledgement of the quality of the evidence supporting the relevant recommendations,37,39,43 and 2 guidelines did not make an explicit acknowledgement concerning quality of the supporting evidence.42,47 Five of the guidelines assigned strength to the relevant recommendation(s),31,35,37-39 whereas 3 did not.42,43,47
Country of Origin
One of the 2 retrospective cohort studies was conducted in the US46 and the other in Greece.34 The economic evaluation was undertaken in Portugal.33 One of the modelling studies was conducted in Canada45 and the remaining 3 were conducted in the US.32,36,44
Six of the guidelines (1 with a full published guideline in 2017 and updated recommendations of relevance published in 2022) were developed by groups based in the US,35,37,38,40,42,43 1 was developed by an Austrian group,31 and 1 guideline (with a separately published updated chapter) by an Australian group.41,47
Patient Population
One retrospective cohort study included a large cohort of residents in the state of Florida who had a colonoscopy and had no evidence of a history of inflammatory bowel disease (IBD) or CRC, including 1 subgroup (some of whom underwent screening) between the ages of 45 and 49 years and another subgroup who underwent screening between the ages of 50 and 54 years.46 The other retrospective cohort study included asymptomatic individuals of average risk (i.e., excluding those with a personal or family history of CRC or adenomas, a positive screen for CRC, digestive symptoms [i.e., persistent abdominal pain, rectal blood, chronic diarrhea, weight loss], chronic IBD, or iron-deficiency anemia). The mean age of participants who underwent CRC screening was 63 years, including subgroups of those younger than 50 years (mean age = 42.5 years) and 50 years and older (mean age = 65.9 years).34
The Canadian modelling study considered 4 hypothetical birth cohorts, including those born from 1973 to 1977, 1978 to 1982, 1983 to 1987, and 1988 to 1992. However, it was unclear whether these individuals were all of average risk.45 The 3 US-based modelling studies considered hypothetical cohorts of individuals of average risk from 40 years.32,36,44 Although “average risk” was stated by these 3 modelling studies, 1 did not define average risk,32 1 defined average risk as asymptomatic and unscreened,36 and 1 described average risk as free from CRC.44
The economic evaluation’s base case examined population-level data from individuals between the ages of 45 and 50 years who had not previously undergone screening for CRC.33 No other information concerning the definition of average risk was reported.33
All the included guidelines were clear in their description of the target population of interest, which specified individuals at average risk for CRC. However, the definition of average risk was reported variably.31,35,37-43,47 One guideline did not provide a definition of average risk,38 the others included definitions that described no personal and/or family history of CRC,31,35,37,39,40,42,43,47 no diagnosis and/or clinical symptoms of CRC,31,35,37,41,43 no symptoms or history of IBD,31,35,37,39,42,43 and/or no known genetic disorders that may increase risk of CRC.31,37,39,43 Intended users of the guidelines were often described as clinicians and/or health care providers,35,38,39,41-43 although 2 of the guidelines were not explicit concerning the intended users.31,37
Interventions and Comparators
Most of the included publications evaluated CRC screening in individuals younger than 50 years using colonoscopy or FIT as the initial screening test.31-40,42-46 One guideline (with an original version published in 2017 and an updated chapter published in 2023) presented relevant recommendations that did not specify the screening intervention, but referred only to “screening.”47 Exceptions related to the indications for colonoscopy (i.e., indications for colonoscopy beyond screening; unclear indications for colonoscopy) are further described for individual studies as applicable.
One retrospective cohort study included subgroups of patients between the ages of 45 and 49 years or between the ages of 50 and 54 years for whom the colonoscopy indication was presumed to be screening (but also included those with other indications such as polyps or a history of polyps, or benign neoplasms).46 The other compared colonoscopy screening as the initial test for individuals younger than 50 years versus initial screening with colonoscopy in those who were 50 years and older.34
The 4 modelling studies considered CRC screening beginning at the age of 45 years,32,36,44,45 and 2 modelling studies also considered screening beginning at 40 years.44,45 Two of the modelling studies considered both FIT and colonoscopy as screening tests,36,44 whereas 1 considered biennial FIT only45 and 1 considered colonoscopy only.32
Of the 3 studies that modelled FIT screening:
1 assumed use of the OC-Sensor family of tests using a cut-off of 20 mcg of hemoglobin per gram of feces36
2 assumed the sensitivity of FIT to detect CRC at 75%19 or a range between 62.6% and 88.6%44
No screening was the hypothetical comparator for 3 of the modelling studies,32,36,44 with 2 modelling studies including comparisons with individuals initiating screening at 50 years.36,45
The economic evaluation compared CRC screening, with either FIT or colonoscopy as the initial test, to no screening in individuals starting at 45 years.33 Analyses were mutually exclusive (i.e., FIT as initial test versus no screening, or colonoscopy as the initial test versus no screening).
All the evidence-based guidelines made recommendations concerning CRC screening in individuals younger than 50 years.31,35,37-43,47 Although some guidelines addressed multiple testing interventions that were not relevant to this report, colonoscopy and FIT were explicitly considered in 7 of the included guidelines,31,35,37-40,42,43 with 1 guideline not specifying which intervention was recommended in the recommendations of relevance to this report (although, other recommendations that are not relevant to this report describe the use of the immunochemical fecal occult blood test).47
Outcomes
One retrospective cohort study investigated incidence rates of CRC per 100,000 person-years across a 13-year time frame from 2005 to 2017.46 The other investigated CRC cases that were detected cumulatively across the span of 1 year.34
Three of the modelling studies reported estimates of life-years gained (LYG).32,36,44 Other estimated benefits included CRC cases avoided and CRC deaths avoided, which were reported by 2 studies.36,45 Three of the modelling studies reported burdens and/or harms of screening, with all 3 describing estimates of lifetime number of colonoscopies,32,36,44 and 1 describing estimates of complications from screening tests.36 Complications from this 1 modelling study were reported aggregately, and described as serious and other gastrointestinal events (including perforations, bleeding, need for transfusion, paralytic ileus, nausea, and vomiting) and cardiovascular events (including myocardial infarction, angina, arrhythmia, congestive heart failure, cardiac or respiratory arrest, syncope, hypotension, and shock).36 Three of the modelling studies described a lifetime horizon across which the analyses were conducted,32,36,44 whereas the Canadian modelling study reported the use of a 40-year time horizon.45
The economic evaluation measured cost-utility, expressed using Euros per quality-adjusted life-year (€/QALY). Time horizon was not reported. Incremental cost-effectiveness ratios (ICERs) were also reported as outcomes of the cost-utility analysis.33
The evidence-based guidelines considered CRC incidence, CRC mortality, and/or harms of screening as major outcomes informing development of their recommendations.31,35,37-43,47 Two guidelines (1 with 2 publications) also considered LYG with screening younger than 50 years.39,41,47
Summary of Critical Appraisal
Nonrandomized Studies
Strengths of the retrospective cohort studies included clarity of reporting, appropriate statistical methods, and valid and reliable outcome measures, which support the internal validity of the findings.34,46 One retrospective cohort study included a large sample size, drawing from a state-wide data source across a 13-year time frame, which supported its external validity.46 Limitations included a lack of reporting on harms of screening and limited clarity concerning the representativeness of the study population, intervention, and/or setting.34,46 In particular, it was not clear whether the study populations were representative of the source population from which they were selected. In 1 study, it was unclear whether the group of patients younger than 50 years was representative of individuals of average risk because indications for colonoscopy included those other than screening (i.e., history of polyps or benign neoplasm).46 Similarly, in the other nonrandomized study, it was reported that screening was provided at the request of the patient, which may not support the representativeness of the group to an average-risk population.34 Both the studies described information on the race or ethnicity of study participants, but no other details that may be relevant to health equity considerations (e.g., socioeconomic status or rurality of residence). However, outcome data were not reported by race or ethnicity.34,46 Notably, 1 study reported that all participants were of “white-Caucasian” ethnicity, which may limit the representativeness of the findings outside of these groups.34 In addition, it was not clear whether the 1 study centre at which the screening was provided was representative of the care received among the source population.34 This lack of clarity concerning representativeness may indicate limitations to the external validity of the studies, which is critical to demonstrating that the findings are likely to be applicable across populations and settings.49
Considerations for Modelling Studies
The research objectives and their importance were made clear in the 3 modelling studies.32,36,44,45 Each of these studies used and modified existing models, describing the rationale and methods for doing so and including published sources for incidence and mortality data that were incorporated.32,36,44,45 One of the modelling studies assumed screening participation rates in accordance with published data,45 whereas 3 of the modelling studies assumed perfect or complete adherence to screening and/or follow-up. This is a notable limitation given that adherence to screening protocols is not perfect in real-world scenarios.43 Three of the studies addressed both estimated benefits and burdens of screening32,36,44 and 1 also reported on estimated harms of screening,36 but 1 reported on estimated benefits of screening only.45 The limited investigation and reporting of estimated harms of screening may have limited the interpretation of the findings (i.e., emphasis on the estimated benefits of screening in the analyses may not have adequately characterized the balance against estimated harms from screening). One of the modelling studies accounted for uncertainty in its estimates using credible intervals,32 but the other 3 did not.36,44,45 Characterizing uncertainty statistically is important for clarifying the accuracy and potential validity of reported estimates.29
Given the research objectives and methods described, as well as the estimates generated, the conclusions reported for the 3 modelling studies appeared balanced and reasonable.32,36,44,45
Economic Evaluation
Strengths of the economic evaluation included a clearly stated research objective, viewpoint, and main outcomes. Data inputs for incidence, mortality, cost, and utilities were drawn from published sources.33 Key limitations included the lack of a reported time horizon, preventing the reader from understanding the duration over which the model estimates were generated. Although variables and transition probabilities were provided in a supplementary file to the published report, details describing the methods used for the decision tree model were not reported.33 An important limitation was the source of incidence estimates, which authors explained were only available from 1993 until 2010.33 This limits the model estimates from consideration of more recent trends in CRC incidence and could affect the cost-utility findings and conclusions (i.e., incorporation of more recent data that may demonstrate increasing incidence may generate estimates that favour cost-utility).
Evidence-Based Guidelines
The scope and purpose of the included guidelines are generally clear,31,35,37-43 although the overall objectives of the guidelines are not stated or are not clear in 3 guidelines,37,38,42 and the questions being addressed by the guidelines are not clearly stated in 2 of the guidelines (1 with 2 publications).35,40,43 Stakeholder involvement is well represented in 4 guidelines, which describe involvement of relevant professional groups,31,39,42,43 whereas 4 guidelines (2 with 2 publications each) do not make this clear.35,37,38,40,41,47 Efforts to consult with members of the target population are described in 5 of the guidelines (1 with 2 publications),31,37,39,41,43,47 but not clear in the remaining 3 (1 with 2 publications).35,38,40,42
Rigour of development was supported by a systematic literature review in 7 guidelines,37-43 whereas details of the systematic review methods were not reported in 1 guideline.31 A link between the evidence and the recommendations is made clear in 7 of the guidelines,31,35,37-39,43,47 whereas the association is unclear in 1 guideline.42 There is evidence of external peer review for 7 of the guidelines,31,37-41,43 although external review is not clear for 1 guideline.42
The recommendations are clear and easily identifiable in all 8 included guidelines.31,35,37-39,42,43,47 The applicability of the recommendations is generally not clearly reported, with 6 (1 with 2 publications) not describing barriers and facilitators to applying the guidelines31,35,37,38,40,42,43 and 4 of the guidelines (1 with 2 publications) not providing advice or tools to support putting recommendations into practice.38,41-43,47 Similarly, the potential influence of funding on the development of the guidelines is not reported or not clearly reported in 6 of the guidelines (1 with 2 publications),37-39,41-43,47 and potential conflicts of interest are not reported or not clearly reported in 4 of the guidelines (1 with 2 publications).37,38,41,42,47
Additional details regarding the strengths and limitations of included publications are provided in Appendix 3.
Summary of Findings
Effectiveness of CRC Screening in Individuals of Average Risk Younger Than 50 Years Versus Those Older Than 50 Years
Empirical Data From Observations
Colonoscopy Screening
In 1 retrospective study, 38,586 individuals between the ages of 45 and 49 years were analyzed across a 13-year time frame. Some of these individuals underwent colonoscopy for an indication of screening producing a CRC incidence rate of 23.7 per 100,000 person-years.46 In the same study, 365,152 individuals between the ages of 50 and 54 years were analyzed, producing a CRC incidence rate of 15.7 per 100,000 person-years.46 No statistical comparisons were made between these 2 groups; however, the 95% confidence intervals (CIs) for the 2 rates did not overlap (45 to 49 years: 95% CI, 18.4 to 30.2; 50 to 54 years: 95% CI, 14.1 to 17.5).46 This finding suggests there is a significant difference between the groups (i.e., a higher incidence rate of CRC observed in the younger group).
Of 47 individuals younger than 50 years (mean = 42.5 years; SD = 5.9 years) who were screened for CRC in the other retrospective cohort study, 1 CRC case (2.1%) was detected over the course of 1 year.34 In 333 individuals who were 50 years or older (mean = 65.9 years; SD = 8.3 years), 7 cases (2.1%) of CRC were detected by first-time colonoscopy screening. The odds ratio (OR) between the groups indicated a non–statistically significant difference in CRC cases detected between groups (OR = 1.01; 95% CI, 0.12 to 8.4; P = 0.9).34
Table 9 provides tabulated details for these findings.
Modelled Data: Estimated Benefits
Colonoscopy Screening: Life-Years Gained
One modelling study estimated that 27 LYG may be observed with colonoscopy every 10 years initiated at 45 years compared to 50 years in 1,000 individuals of average risk across a lifetime horizon.36
FIT Screening: Life-Years Gained
One modelling study estimated that 26 LYG may be observed with annual FIT as the initial screening test initiated at 45 years compared to 50 years in 1,000 individuals of average risk across a lifetime horizon.36
Colonoscopy Screening: CRC Incidence
One modelling study estimated that 3 CRC cases would be avoided across a lifetime horizon with colonoscopy every 10 years initiated at 45 years compared to 50 years in 1,000 individuals of average risk.36
FIT Screening: CRC Incidence
The Canadian modelling study estimated that 18,135 fewer CRC cases may occur across a 40-year interval among 4 birth cohorts if biennial FIT screening was initiated at 40 years compared to 50 years.45 The same study estimated that if screening was initiated at 45 years versus 50 years, 12,188 CRC cases may be avoided.45
Another modelling study estimated that 3 CRC cases would be avoided across a lifetime horizon with annual FIT initiated at 45 years compared to 50 years in 1,000 individuals of average risk.36
Colonoscopy Screening: CRC Mortality
One modelling study estimated that 1 death caused by CRC would be avoided across a lifetime horizon with colonoscopy every 10 years initiated at 45 years compared to 50 years in 1,000 individuals of average risk.36
FIT Screening: CRC Mortality
The Canadian modelling study estimated that 7,988 fewer deaths caused by CRC may occur across a 40-year interval among 4 birth cohorts if biennial FIT screening was initiated at 40 years compared to 50 years.45 The same study estimated that if biennial FIT screening was initiated at 45 years versus 50 years, 5,261 deaths caused by CRC may be avoided.45
Another modelling study estimated that 1 death caused by CRC would be avoided across a lifetime horizon with annual FIT initiated at 45 years compared to 50 years in 1,000 individuals of average risk.36
Modelled Data: Estimated Burden and Harms
Colonoscopy Screening: Number of Lifetime Colonoscopies
One modelling study estimated that an additional 784 lifetime colonoscopies would occur with colonoscopy every 10 years initiated at 45 years compared to 50 years in 1,000 individuals of average risk.36
FIT Screening: Number of Lifetime Colonoscopies
One modelling study estimated that an additional 186 colonoscopies would be performed with annual FIT as the initial screening test initiated at 45 years compared to 50 years in 1,000 individuals of average risk across a lifetime horizon.36
Colonoscopy Screening: Number of Lifetime Complications From Screening
One modelling study estimated that more than 2 complications (which could include gastrointestinal and/or cardiovascular events but were reported aggregately only) may occur with colonoscopy every 10 years initiated at 45 years compared to 50 years in 1,000 individuals of average risk across a lifetime horizon.36
FIT Screening: Number of Lifetime Complications From Screening
With annual FIT as the initial screening test initiated at 45 years compared to 50 years in 1,000 individuals of average risk, 1 modelling study estimated that more than 0.2 complications may occur across a lifetime horizon. Complications were reported aggregately but may have included gastrointestinal and/or cardiovascular events.36
Table 10 provides tabulated details for these findings.
Effectiveness of CRC Screening Versus No Screening in Individuals of Average Risk Younger Than 50 Years
Empirical Data From Observations
No eligible studies were identified, so no summary of the evidence could be provided.
Modelled Data: Estimated Benefits
Colonoscopy Screening: Life-Years Gained
The 3 modelling studies32,36,44 estimated a range of 33736 to 43844 LYG with colonoscopy screening every 10 years starting at age 40 or 45 versus no screening in 1,000 individuals of average risk across a lifetime horizon.36,44
FIT Screening: Life-Years Gained
With annual FIT as the initial screening test, 3 modelling studies32,36,44 estimated a range of 31836 to 41744 LYG per 1,000 individuals of average risk across a lifetime horizon.
Colonoscopy Screening: CRC Incidence
Compared to no screening:
One modelling study estimated that a mean of 61 CRC cases may be averted with colonoscopy initiated at 45 years.36
One modelling study estimated that 36 or 37 CRC cases may be expected in patients undergoing colonoscopy when screening is initiated at age 40 or 45 years, respectively, compared with 108 expected CRC cases in an unscreened population younger than 50 years.44
FIT Screening: CRC Incidence
Compared to no screening:
One modelling study estimated that a mean of 50 CRC cases may be averted with annual FIT initiated at 45 years.36
One modelling study estimated that 52 or 54 CRC cases may be expected in patients undergoing FIT when screening is initiated at age 40 or 45 years, respectively, versus 108 expected CRC cases in an unscreened population younger than 50 years.44
Colonoscopy Screening: CRC Mortality
Compared to no screening:
One modelling study estimated that a mean of 28 CRC deaths may be averted with colonoscopy initiated at 45 years.36
One modelling study estimated that 8 CRC deaths may be observed in patients undergoing colonoscopy at either age 40 or 45 years, whereas 45 CRC deaths may be expected in an unscreened population.44
FIT Screening: CRC Mortality
Compared to no screening:
One modelling study estimated that a mean of 26 CRC deaths may be averted with annual FIT initiated at 45 years.36
Another modelling study estimated that 11 CRC deaths may be observed in patients undergoing FIT starting at either age 40 or 45 years, whereas 45 CRC deaths may be expected in an unscreened population.44
Modelled Data: Estimated Burden and Harms
Colonoscopy Screening: Number of Lifetime Colonoscopies
The 3 modelling studies32,36,44 estimated expected lifetime colonoscopies for 1,000 individuals aged 40 years with average risk. These individuals received either colonoscopy testing every 10 years beginning at either age 40 or 45 years or no screening, with an estimated range of expected lifetime colonoscopies from between 3,96132 to 6,08344 for the screened groups receiving colonoscopy.
FIT Screening: Number of Lifetime Colonoscopies
Two modelling studies estimated expected lifetime colonoscopies for 1,000 individuals aged 40 years with average risk who received either annual FIT initiated at 45 years or no screening, with estimates of between 1,68236 and 2,69844 lifetime colonoscopies expected in the screened groups.
Colonoscopy Screening: Number of Lifetime Complications From Screening
One modelling study estimated that more than 16 lifetime complications (reported aggregately but may have included gastrointestinal and/or cardiovascular events) may occur from CRC screening with colonoscopy testing every 10 years in 1,000 individuals of average risk younger than 50 years versus no screening.36
FIT Screening: Number of Lifetime Complications From Screening
One modelling study estimated that more than 10.2 lifetime complications (reported aggregately but may have included gastrointestinal and/or cardiovascular events) may occur from CRC screening with annual FIT screening in 1,000 individuals of average risk younger than 50 years versus no screening.36
Table 10 provides tabulated details for these findings.
Cost-Effectiveness of CRC Screening Versus No Screening in Individuals of Average Risk Younger Than 50 Years
Assuming a willingness-to-pay threshold of €39,760, neither a CRC screening strategy using FIT nor colonoscopy as the initial test in adults starting at 45 years demonstrated cost-utility across an unreported time horizon. Assuming the cost of colonoscopy at €150, FIT generated an ICER of €84,304, with an assumed 50% screening participation rate, and colonoscopy had an ICER of €3,112,244 with an assumed 38% participation rate, compared with no screening until age 50 years.33 Analyses assuming the cost of colonoscopy at €397 generated ICERs of €176,213 for FIT screening and €6,620,987 for colonoscopy screening.33 Authors emphasized that the findings were most sensitive to the estimated incidence of CRC, which would have to rise from 30 to 47.5 cases per 100,000 individuals of average risk younger than 50 years to demonstrate cost-utility.33
Table 11 provides tabulated detail for these findings.
Evidence-Based Guidelines Regarding CRC Screening in Individuals of Average Risk Younger Than 50 Years
Seven of the guidelines (1 developed by an Austrian group, 5 developed by groups in the US, and 1 developed by an Australian group) make recommendations in favour of screening individuals of average risk beginning at the age of 45 years,31,35,37-39,42,47 whereas 2 guidelines make recommendations against the initiation of screening in individuals at 40 years 47 or 45 years.43 Recommendations with supporting evidence and rationale were summarized, when provided in the guidelines, and are reported in Table 12.
Of the 7 guidelines that make recommendations in favour of CRC screening for individuals from 45 years, 2 indicated that the evidence is of low or very low quality,35,38 1 indicated that the evidence is of moderate quality,31 and 4 were not explicit about the quality of the evidence informing the relevant recommendation(s).37,39,42,47 Three of the guidelines assigned a grade to the recommendations, with weak, conditional or qualified recommendations favouring screening in younger populations.35,38,39
Of the 2 guidelines that make recommendations against screening for individuals younger than 50 years (1 Australian and 1 from the US), 1 did not describe the quality of the evidence used to inform the relevant recommendation against screening initiation at age 40 (but did specify an unfavourable “benefits-to-burden balance” for this age group in its rationale).47 The other evidence-based guideline, which recommends against the initiation of screening at 45 years, was clear about important limitations of the evidence reviewed, which was deemed to not support a recommendation in favour of screening in this population.43 Neither of these guidelines are explicit about assigning a grade to the relevant recommendations indicating their strength.43,47
Appendix 4 presents tabulated details about the study findings and evidence-based guidelines.
Limitations
As has been highlighted in many published sources on the topic, empirical data describing the clinical benefits and harms of CRC screening in individuals of average risk younger than 50 years are scarce.50 Whereas 4 modelling studies reporting microsimulated estimates were included and summarized, 2 eligible retrospective cohort studies and 1 economic evaluation published since 2017 were identified for inclusion. The limitations of available empirical data are also highlighted in the 9 included guidelines,31,35,37-43,47 several of which are explicit about the scarcity of relevant, available evidence to inform decisions and practice regarding CRC screening in populations younger than 50 years.38,40,43 The dearth of available evidence may have resulted in no eligible studies of relevance identified using observed, empirical data in answer to the second of this report’s research questions regarding the effectiveness of colorectal cancer screening versus no screening in individuals of average risk younger than 50 years.
Eligible primary clinical and cost-effectiveness data informing this report are scarce, although modelling studies were included which provided estimates of relevance to the research questions regarding effectiveness of CRC screening.32,36,44,45 However, because these studies are not based on observed outcomes following CRC screening in individuals of average risk, the inferences and conclusions that can be drawn from their findings are limited to the validity and quality of the assumptions and inputs of the models. For instance, 3 of the modelling studies assumed perfect adherence to screening protocols, which is a limitation because perfect adherence to screening and follow-up testing is not observed in real-world settings.43 This limitation could overestimate the projected benefits, burdens, and harms of CRC screening. The Canadian modelling study reported on estimated benefits without accounting for the potential burdens and/or harms of screening and was not clear about analyzing an average-risk population,45 which could overestimate the estimated benefits of screening. Regarding complications, 1 of the modelling studies reported on this outcome, but did not specify types of harms. It reported complications aggregately as gastrointestinal and/or cardiovascular events.36 This lack of specificity limits the interpretation of the findings regarding complications from colonoscopy that can occur because the severity of different types of complications is variable. Several of the evidence-based guidelines included in this report relied on some of these and other modelling studies,31,35,39,41,47 most of which emphasize the limitations of relying on modelled data for informing decision-making and clinical practice.
The potential utility of some, or all, of the recommendations in the included evidence-based guidelines may also be limited. Seven of the guidelines made recommendations favouring CRC screening in individuals of average risk younger than 50 years,31,35,37-39,42,47 whereas 2 made recommendations that do not favour CRC screening in this age group, specifically in individuals starting at the age of 45 years43 or in individuals starting at the age of 40 years.47 The discordance among some of the recommendations made in the evidence-based guidelines is particularly notable given the similar evidence sources used across the included guidelines, and the agreement among them concerning the availability and quality of evidence. For instance, it is not clear whether other factors in addition to the available evidence may have accounted for the lack of agreement across all the included guidelines.
Of the eligible and included studies summarized in this report, some data may be limited in their potential applicability, utility, and/or generalizability, including that of relevance to the Canadian context. Four of the included sources did not clearly state or define whether the population of interest was of average risk,32,33,38,45 which may limit the applicability of their findings and/or recommendations to the population of interest. One retrospective cohort study was conducted using health administrative data in a US context,46 and the other was conducted on a limited sample size in a Greek population and health system,34 which may bear limited representativeness to Canadian populations and health care systems. In addition, 1 retrospective cohort study may have included study patients who were not of average risk.,46 The other study compared younger study participants to those older than 50 years, including those who were 75 years and older,34 neither of which are relevant to this report or to the Canadian context. Further, because the Canadian modelling study did not clearly limit its analyses to individuals of average risk,45 its findings may be limited in their generalizability to an average-risk population.
The cost-utility analyses were conducted in Portugal and incorporated incidence data from 1993 until 2010.33 This may also bear limited relevance to the Canadian context and may not adequately consider more recent trends in CRC incidence among individuals of average risk younger than 50 years. In addition, the lack of clarity about the CRC risk of included participants and the lack of a reported time horizon limited the interpretation of the findings.
Six of the included guidelines (1 with 2 publications) were developed in the US, which has a health system that is distinct from Canada’s health systems.35,37-40,42,43 The remaining 2 guidelines (1 with 2 publications) were produced in Austria31 and Australia,41,47 which have distinct social, cultural, economic, and geographic contexts, thus may have limited generalizability within Canada.
Conclusions and Implications for Decision- or Policy-Making
This review identified 2 retrospective cohort studies, 1 economic evaluation, 3 modelling studies, and 8 evidence-based guidelines (2 of which also published updates in 2022 and 2023) reporting data and information relevant to CRC screening in individuals of average risk younger than 50 years.31-44,47
Empirical data describing observations of the effectiveness of screening regarding CRC incidence, mortality, and harms were limited. One retrospective cohort study reported rates that are suggestive of a higher incidence of CRC in individuals between the ages of 45 and 49 years compared with those between the ages of 50 and 54 years (although the authors concede that the younger group may not be representative of an average-risk population).46 The other retrospective cohort study found no statistically significant difference in the cumulative incidence in Greece of CRC among 380 individuals of average risk who underwent colonoscopy for the first time, 47 of whom were younger than 50 years, compared with 333 who were 50 years or older.34 Differences in the methods and other study features may account for this apparent difference in observed direction of effect (e.g., the US study did not clearly limit study participants to those of average risk, or to colonoscopy for screening alone,46 whereas the Greek study used a small sample size that may not be generalizable to a larger population34).
It is likely that the limited empirical data available that answers the research questions posed in this report are a function of the widespread and longstanding recommendations in most jurisdictions limiting CRC screening to those aged 50 years and older (i.e., where screening for individuals of average risk younger than 50 years is not practised, generating data on its effectiveness is challenging to produce). Consequently, this report and many of its included evidence-based guidelines have looked to modelled data to help inform questions about CRC screening in individuals of average risk younger than 50 years. The estimated benefit generated by modelled data highlight opportunities for increased LYG, reductions in CRC cases, and mortality, alongside estimated burdens and harms that include increased testing and potential adverse events that screening in individuals of average risk younger than 50 years are anticipated to produce.32,36,44 These limited findings may be interpreted as supportive of CRC screening strategies that initiate in populations younger than 50 years, and are corroborated by observed and broadly acknowledged increases in CRC incidence among individuals younger than 50 years across the world.6,7,24,25,51 Nonetheless, modelled screening scenarios that assumed the initiation of screening in individuals at 40 or 45 years compared to 50 years and older also produce higher estimates of lifetime colonoscopies and potential harms from this increased number of endoscopic interventions across the lifespan.32,36,44 Finally, 1 modelling study included in this report accounted for imperfect participation in screening,45 but 3 did not.32,36,44 Future modelling studies may also consider incorporating assumptions and inputs that are more consistent with real-world observations (e.g., that adherence to CRC screening protocols are not perfect, which will impact the estimates of benefits and harms).
One economic evaluation determined there was no cost-utility of CRC screening in individuals of average risk younger than 50 years in Portugal based on current estimates of incidence.33 Nonetheless, incidence data used in the decision tree model covered the time period up until 2010,33 rendering its findings limited in their applicability to more current trends in CRC incidence.33 Further, sensitivity analyses demonstrated that CRC incidence would have to rise from its current rate of 30 to 47.5 per 100,000 individuals of average risk younger than 50 years to render cost-utility, assuming the lowest cost test option (i.e., FIT at €150).33 Although screening for CRC in populations younger than 50 years has been described elsewhere in the literature as not being cost-effective,26 the rising trends in incidence of the disease among younger people may impact the findings for this outcome. In 2 economic evaluations that did not meet the eligibility criteria for this review, the authors concluded that CRC screening for those younger than 50 years compared to those 50 years and older demonstrated cost-effectiveness.45,52 However, 1 of these also reported greater benefits at lower costs were estimated with CRC screening strategies that targeted uptake among higher-risk and older populations.52
Seven of the 8 included evidence-based guidelines made recommendation(s) in favour of CRC screening for individuals of average risk younger than 50 years, specifically starting at age 45.31,35,37-39,42,47 Nonetheless, a recurring assertion among the evidence-based guidelines included in this report was the lack of empirical data available to inform recommendations for CRC screening in individuals of average risk younger than 50 years.31,35,37-39,41-43,47 Evidence describing the effectiveness of CRC screening relies almost solely on nonrandomized methods, which are arguably unavoidable due to the nature of the disease and the diagnostic process, but which render less robust findings than randomized studies (e.g., CRC screening studies may be vulnerable to self-selection and other biases).12 Similarly, a recent review of Canadian recommendations and practices for CRC screening in individuals of average risk younger than 50 years concluded that the balance of costs and benefits remains unclear.19
Further, a preponderance of data from modelling studies has been used to inform recommendations in favour of CRC screening for younger individuals,31,35,37-40,42 And although modelling studies are common and can be useful for estimating long-term outcomes of CRC screening, the data are also vulnerable to variability and uncertainty according to model inputs. For example, various existing models assume variable durations for the adenoma-carcinoma sequence that range from 6 to 23 years.8 These and other differences in model assumptions and inputs can account for important differences in the estimates that they generate concerning the benefits of CRC screening. Lastly, a more extensive and robust assessment of the estimated harms of screening may provide a more fulsome perspective on the balances of benefits and harms, which could better inform decision-making concerning policy and practice for CRC screening in individuals of average risk younger than 50 years.
Considerations for Health Equity and Implementation
In addition to the evidence relevant to clinical effectiveness and cost-effectiveness, considerations that address health equity, implementation, and broader impacts of CRC screening for younger individuals of average risk are critical. One Canadian guidance document highlighted the importance of prioritizing CRC screening outreach interventions for adults between the ages of 45 and 75 years who are experiencing disadvantage.53 Another analysis concluded that CRC screening in younger individuals would likely be cost-effective, but a strategy focused on increasing uptake among those 50 years and older, as well as among those at highest risk, would produce greater societal benefits.52
Some information addressed the need for increased uptake among higher-risk and/or underserved communities as a strategy for improving the effectiveness of CRC screening. One of the modelling studies summarized in this report generated estimates by race and sex subgroups, reporting that life expectancy, CRC cases, and deaths were unlikely to differ by race in a hypothetical population of 40 year olds that had not previously undergone CRC screening.36 Based on this, and their supporting work of a review of the literature, the authors posited that disparities by race and sex in CRC outcomes are more likely to be caused by differences in screening uptake than by differences in natural history of the disease by racial group.36 Accordingly, 1 of the evidence-based guidelines summarized in this report made a qualifying statement concerning race (i.e., that while CRC incidence rates are higher in Black, American Indian, and Alaskan Native adults, screening should be offered to all adults beginning at the age of 45 years).37 Similarly, another of the evidence-based guidelines incorporated good practice points highlighting the importance of health care human resources availability and upskilling to support the uptake of screening — particularly among potentially disadvantaged communities.47 CRC screening strategies that prioritize improving uptake among higher-risk and/or underserved communities have been studied as well, with 2 studies identified by this review investigating implementation techniques for screening programs in racialized populations.54,55 One US-based study of a FIT mailed outreach intervention found that an enhanced envelope with what was intended to be a more “eye catching” appearance produced statistically significantly higher return rates than a plain envelope in adults between the ages of 45 and 49 years.54 Return rates were not statistically significantly different between envelope types among non-Hispanic white and Hispanic groups, a statistically significant higher return rate for enhanced envelopes was observed among the non-Hispanic Black population in the study.54 Another US-based study describing health equity and implementation considerations found that the completion rate of a mailed FIT kit in a previously unscreened African American population who were between the ages of 45 and 50 years was statistically significantly higher than those of previously unscreened African American, white, and Hispanic groups between the ages of 51 and 56 years (although, there was no statistically significant difference with Asian and Pacific Islanders between the ages of 51 and 56 years).55 Completion rates of colonoscopy among FIT-positive African Americans aged 45 to 50 years did not differ versus those of African American, white, and Hispanic groups (although rates were higher compared to the Asian and Pacific Islander group aged 51 to 56 years).55 CRC cases among FIT-positive African American, white, and Asian and Pacific Islander groups between the ages of 51 and 56 years were statistically significantly higher than those among African Americans aged 45 to 50 years (with no cases observed among FIT-positive Hispanics aged 51 to 56 years).55 These findings appear to support analyses indicating that strategies focused on increasing CRC screening uptake in older and/or higher-risk populations may yield greater overall benefit than strategies focused on universal screening in individuals of average risk younger than 50 years.52
Finally, while considering implementation of CRC screening programs in individuals of average risk younger than 50 years and/or optimizing uptake among higher-risk and disadvantaged communities is important, barriers and facilitators to buy-in among health care providers is also essential. One US-based survey of health care providers reported that a majority of respondents did not believe that CRC screening (using colonoscopy or FIT) was effective for individuals younger than 50 years.56 Similarly, a large majority of respondents indicated that they would not routinely recommend CRC screening with colonoscopy or FIT in individuals younger than 50 years.56For CRC screening programs to be optimally effective in any population, the support of clinicians who provide health care and requisition CRC screening tests is critical. Changes to CRC screening recommendations and policy must carefully consider outreach and education for health care providers.
Findings from relevant sources describing health equity and/or implementation considerations are provided in Table 13.
Opportunities for Future Research and Conclusion
Given the limited empirical data available to inform policy and practice for CRC screening among individuals of average risk, future research efforts may benefit from a focus on rigorous observational studies of populations in which CRC screening for younger populations has been recommended (e.g., in the US). Real-world observations — using pilot programs, for instance — and comparisons with no screening in younger individuals as well as comparisons with outcomes in older individuals, will better support consideration of the benefits, harms, costs, and implementation considerations of a CRC screening approach in individuals of average risk younger than 50 years. In addition, adjustments for potentially confounding factors (e.g., sex, race and/or ethnicity, as well as lifestyle risk factors such as overweight or obesity, excessive alcohol, and/or tobacco use), will support more accurate estimates of the effectiveness of screening in younger individuals of average risk. Importantly, broader considerations addressing the potential for other screening strategies — including increasing uptake in older, higher-risk, and disadvantaged populations — will also be essential to informing decisions concerning optimal approaches to CRC screening in the future.57
References
1.Colorectal cancer. Global Cancer Observatory factsheet. Lyon (FR): WHO International Agency for Research on Cancer (IARC); 2020: https://gco.iarc.fr/today/data/factsheets/cancers/10_8_9-Colorectum-fact-sheet.pdf. Accessed 2023 Nov 22.
2.Morgan E, Arnold M, Gini A, et al. Global burden of colorectal cancer in 2020 and 2040: incidence and mortality estimates from GLOBOCAN. Gut. 2023;72(2):338-344. PubMed
3.Arnold M, Sierra MS, Laversanne M, Soerjomataram I, Jemal A, Bray F. Global patterns and trends in colorectal cancer incidence and mortality. Gut. 2017;66(4):683-691. PubMed
4.Canadian Cancer Statistics Advisory Committee, the Canadian Cancer Society, Statistics Canada, and the Public Health Agency of Canada. Canadian Cancer Statistics 2023. Toronto (ON): Canadian Cancer Society; 2023: https://cdn.cancer.ca/-/media/files/research/cancer-statistics/2023-statistics/2023_PDF_EN.pdf. Accessed 2023 Nov 8.
5.Macrae FA, Parikh AR, Ricciardi R. Clinical presentation, diagnosis, and staging of colorectal cancer. In: Post TW, ed. UpToDate. Waltham (MA): UpToDate; 2023: http://www.uptodate.com. Accessed 2023 Oct 20.
6.Gong Y, Zheng Y, Wu R, Liu M, Li H, Zeng Q. Detection rates of adenomas, advanced adenomas, and colorectal cancers among the opportunistic colonoscopy screening population: a single-center, retrospective study. Chin Med J. 2023;136(2):159-166. PubMed
7.Ambe PC, Jansen S, Zirngibl H. New trend in colorectal cancer in Germany: are young patients at increased risk for advanced colorectal cancer? World J Surg Oncol. 2017;15(1):159. PubMed
8.Prakash MK, Lang B, Heinrich H, et al. CMOST: an open-source framework for the microsimulation of colorectal cancer screening strategies. BMC Med Inform Decis Mak. 2017;17(1):80. PubMed
9.Nguyen LH, Goel A, Chung DC. Pathways of colorectal carcinogenesis. Gastroenterology. 2020;158(2):291-302. PubMed
10.Alduraywish SA, Altamimi LA, Almajed AA, et al. Barriers of colorectal cancer screening test among adults in the Saudi population: a cross-sectional study. Prev Med Rep. 2020;20:101235. PubMed
11.Vermeer NC, Snijders HS, Holman FA, et al. Colorectal cancer screening: systematic review of screen-related morbidity and mortality. Cancer Treat Rev. 2017;54:87-98. PubMed
12.Zhang J, Chen G, Li Z, et al. Colonoscopic screening is associated with reduced colorectal cancer incidence and mortality: a systematic review and meta-analysis. J Cancer. 2020;11(20):5953-5970. PubMed
13.Lauby-Secretan B, Vilahur N, Bianchini F, Guha N, Straif K. The IARC perspective on colorectal cancer screening. N Engl J Med. 2018;378(18):1734-1740. PubMed
14.Robertson DJ, Lee JK, Boland CR, et al. Recommendations on fecal immunochemical testing to screen for colorectal neoplasia: a consensus statement by the US Multi-Society Task Force on colorectal cancer. Gastrointest Endosc. 2017;85(1):2-21.e23. PubMed
15.Doubeni C. Tests for screening for colorectal cancer. In: Post TW, ed. UpToDate. Waltham (MA): UpToDate; 2022: http://www.uptodate.com. Accessed 2023 Oct 20.
16.Sarakarn P, Promthet S, Vatanasapt P, et al. Preliminary results: colorectal cancer screening using fecal immunochemical test (FIT) in a Thai population aged 45-74 years: a population-based randomized controlled trial. Asian Pac J Cancer Prev. 2017;18(10):2883-2889. PubMed
17.Huffstetler AN, Fraiman J, Brownlee S, Stoto MA, Lin KW. An estimate of severe harms due to screening colonoscopy: a systematic review. J Am Board Fam Med. 2023;36(3):493-500. PubMed
18.Jung YS, Park CH, Kim NH, Park JH, Park DI, Sohn CI. Colorectal cancer screening with the fecal immunochemical test in persons aged 30 to 49 years: focusing on the age for commencing screening. Gastrointest Endosc. 2017;86(5):892-899. PubMed
19.Kalyta A, De Vera MA, Peacock S, et al. Canadian colorectal cancer screening guidelines: do they need an update given changing incidence and global practice patterns? Curr Oncol. 2021;28(3):1558-1570. PubMed
20.American Cancer Society guideline for colorectal cancer screening. Atlanta (GA): American Cancer Society; 2020: https://www.cancer.org/cancer/types/colon-rectal-cancer/detection-diagnosis-staging/acs-recommendations.html. Accessed 2023 Nov 22.
21.Colorectal cancer: screening. (Final recommendation statement). Rockville (MD): U.S. Preventive Services Task Force; 2021: https://www.uspreventiveservicestaskforce.org/uspstf/recommendation/colorectal-cancer-screening. Accessed 2023 Nov 22.
22.Colorectal cancer (2016). Montreal (QC): Canadian Task Force on Preventive Health Care (CTFPHC); 2016: https://canadiantaskforce.ca/guidelines/published-guidelines/colorectal-cancer/. Accessed 2023 Nov 22.
23.Brenner DR, Heer E, Sutherland RL, et al. National trends in colorectal cancer incidence among older and younger adults in Canada. JAMA Netw Open. 2019;2(7):e198090. PubMed
24.Kim I, Lee HH, Ko YJ, et al. Factors associated with the risk of colorectal neoplasia in young adults under age 40. Korean J Intern Med. 2022;37(5):969-978. PubMed
25.Park YM, Kim HS, Park JJ, et al. A simple scoring model for advanced colorectal neoplasm in asymptomatic subjects aged 40-49 years. BMC Gastroenterol. 2017;17(1):7. PubMed
26.Kim NH, Park JH, Park DI, Sohn CI, Choi K, Jung YS. The fecal immunochemical test has high accuracy for detecting advanced colorectal neoplasia before age 50. Dig Liver Dis. 2017;49(5):557-561. PubMed
27.Wong JC, Lau JY, Suen BY, et al. Prevalence, distribution, and risk factor for colonic neoplasia in 1133 subjects aged 40- 49 undergoing screening colonoscopy. J Gastroenterol Hepatol. 2017;32(1):92-97. PubMed
28.Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377-384. PubMed
29.Higgins JPT, Green S, editors. Figure 15.5.a: Drummond checklist (Drummond 1996). Cochrane handbook for systematic reviews of interventions. London (GB): The Cochrane Collaboration; 2011: http://handbook-5-1.cochrane.org/chapter_15/figure_15_5_a_drummond_checklist_drummond_1996.htm. Accessed 2023 Oct 20.
30.Agree Next Steps Consortium. The AGREE II Instrument. [Hamilton, ON]: AGREE Enterprise; 2017: https://www.agreetrust.org/wp-content/uploads/2017/12/AGREE-II-Users-Manual-and-23-item-Instrument-2009-Update- 2017.pdf. Accessed 2023 Oct 20.
31.Gartlehner G, Schernhammer E, Lax SF, et al. Screening for colorectal cancer: a recommendation statement of the Austrian National Committee for Cancer Screening. Wien Klin Wochenschr. 2023;135(17-18):447-455. PubMed
32.de Lima PN, Rutter CM, Maerzluft C, Ozik J, Collier N. Robustness analysis of colorectal cancer colonoscopy screening strategies [preprint]. medRxiv. 2023.
33.Currais P, Mao de Ferro S, Areia M, Marques I, Mayer A, Dias Pereira A. Should colorectal cancer screening in Portugal start at the age of 45 years? A cost-utility analysis. Port J Gastroenterol. 2021;28(5):311-318. PubMed
34.Panteris V, Vasilakis N, Demonakou M, et al. Alarming endoscopic data in young and older asymptomatic people: Results of an open access, unlimited age colonoscopic screening for colorectal cancer. Mol Clin Oncol. 2020;12(2):179-185. PubMed
35.Patel SG, May FP, Anderson JC, et al. Updates on age to start and stop colorectal cancer screening: recommendations from the U.S. Multi-Society Task Force on Colorectal Cancer. Am J Gastroenterol. 2022;117(1):57-69. PubMed
36.Knudsen AB, Rutter CM, Peterse EFP, et al. Colorectal cancer screening: an updated modeling study for the US Preventive Services Task Force. JAMA. 2021;325(19):1998-2011. PubMed
37.Davidson KW, Barry MJ, Mangione CM, et al. Screening for colorectal cancer: US Preventive Services Task Force recommendation statement. JAMA. 2021;325(19):1965-1977. PubMed
38.Shaukat A, Kahi CJ, Burke CA, Rabeneck L, Sauer BG, Rex DK. ACG clinical guidelines: colorectal cancer screening 2021. Am J Gastroenterol. 2021;116(3):458-479. PubMed
39.Wolf AMD, Fontham ETH, Church TR, et al. Colorectal cancer screening for average-risk adults: 2018 guideline update from the American Cancer Society. CA Cancer J Clin. 2018;68(4):250-281. PubMed
40.Rex DK, Boland CR, Dominitz JA, et al. Colorectal cancer screening: recommendations for physicians and patients from the U.S. Multi-Society Task Force on Colorectal Cancer. Am J Gastroenterol. 2017;112(7):1016-1030. PubMed
41.Cancer Council Australia Colorectal Cancer Guidelines Working Party. Clinical practice guidelines for the prevention, early detection and management of colorectal cancer. Short form summary of NHMRC approved recommendations. Sydney (AU): Cancer Council Australia; 2017: https://wiki.cancer.org.au/australia/Guidelines:Colorectal_cancer. Accessed 2023 Sep 12.
42.Colorectal cancer screening guideline. Oakland (CA): Kaiser Permanente; 2022: https://wa.kaiserpermanente.org/static/pdf/public/guidelines/colon.pdf. Accessed 2023 Sep 12.
43.Qaseem A, Harrod CS, Crandall CJ, et al. Screening for colorectal cancer in asymptomatic average-risk adults: a guidance statement from the American College of Physicians (version 2). Ann Intern Med. 2023;176(8):1092-1100. PubMed
44.Peterse EFP, Meester RGS, Siegel RL, et al. The impact of the rising colorectal cancer incidence in young adults on the optimal age to start screening: microsimulation analysis I to inform the American Cancer Society colorectal cancer screening guideline. Cancer. 2018;124(14):2964-2973. PubMed
45.Kalyta A, Ruan Y, Telford JJ, et al. Association of reducing the recommended colorectal cancer screening age with cancer incidence, mortality, and costs in Canada using OncoSim. JAMA Oncol. 2023;9(10):1432-1436. PubMed
46.Sehgal M, Ladabaum U, Mithal A, Singh H, Desai M, Singh G. Colorectal cancer incidence after colonoscopy at ages 45– 49 or 50–54 years. Gastroenterology. 2021;160(6):2018-2028.e2013.
47.Clinical practice guidelines for the prevention, early detection, and management of colorectal cancer: population screening. Sydney (AU): Cancer Council Australia; 2023: https://app.magicapp.org/#/guideline/j1Q1Xj. Accessed 2023 Nov 22.
48.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
49.Steckler A, McLeroy KR. The importance of external validity. Am J Public Health. 2008;98(1):9-10. PubMed
50.Lee JA, Chang Y, Kim Y, et al. Colonoscopic screening and risk of all-cause and colorectal cancer mortality in young and older individuals. Cancer Res Treat. 2023;55(2):618-625. PubMed
51.Kim KO, Yang HJ, Cha JM, et al. Risks of colorectal advanced neoplasia in young adults versus those of screening colonoscopy in patients aged 50 to 54 years. J Gastroenterol Hepatol. 2017;32(11):1825-1831. PubMed
52.Ladabaum U, Mannalithara A, Meester RGS, Gupta S, Schoen RE. Cost-effectiveness and national effects of initiating colorectal cancer screening for average-risk persons at age 45 years instead of 50 years. Gastroenterology. 2019;157(1):137-148. PubMed
53.Persaud N, Sabir A, Woods H, et al. Preventive care recommendations to promote health equity. Can Med Assoc J. 2023;195(37):E1250-E1273. PubMed
54.O'Leary MC, Reuland DS, Correa SY, et al. Uptake of colorectal cancer screening after mailed fecal immunochemical test (FIT) outreach in a newly eligible 45-49-year-old community health center population. Cancer Causes Control. 2023;10:10. PubMed
55.Levin TR, Jensen CD, Chawla NM, et al. Early screening of African Americans (45-50 years old) in a fecal immunochemical test-based colorectal cancer screening program. Gastroenterology. 2020;159(5):1695-1704.e1691.
56.Ghai NR, Jensen CD, Merchant SA, et al. Primary care provider beliefs and recommendations about colorectal cancer screening in four healthcare systems. Cancer Prev Res. 2020;13(11):947-958. PubMed
57.Hyams T, Mueller N, Curbow B, King-Marshall E, Sultan S. Screening for colorectal cancer in people ages 45–49: research gaps, challenges and future directions for research and practice. Transl Behav Med. 2021;12(2):198-202. PubMed
58.Qaseem A, Kansagara D, Lin JS, et al. The development of clinical guidelines and guidance statements by the Clinical Guidelines Committee of the American College of Physicians: update of methods. Ann Intern Med. 2019;170(12):863-870. PubMed
59.Lin JS, Perdue LA, Henrikson NB, Bean SI, Blasi PR. Screening for colorectal cancer: updated evidence report and systematic review for the US Preventive Services Task Force. JAMA. 2021;325(19):1978-1998. PubMed
60.Standards for guideline development. Rockville (MD): U.S. Preventive Services Task Force; 2021: https://www.uspreventiveservicestaskforce.org/uspstf/sites/default/files/inline-files/standards-guideline- dev%20%281%29.pdf. Accessed 2023 Oct 3.
61.Knudsen MD, Botteri E, Holme O, et al. Association between lifestyle and site-specific advanced colorectal lesions in screening with faecal immunochemical test and sigmoidoscopy. Dig Liver Dis. 2021;53(3):353-359. PubMed
62.Jahn B, Sroczynski G, Bundo M, et al. Effectiveness, benefit harm and cost effectiveness of colorectal cancer screening in Austria. BMC Gastroenterol. 2019;19(1):209. PubMed
63.Cancer Council Australia Colorectal Cancer Screening Working Party. Clinical practice guidelines for the prevention, early detection and management of colorectal cancer: population screening. Appendix E. Sydney (AU): Cancer Council Australia; 2023: https://www.cancer.org.au/assets/pdf/population-screening-appendix-e. Accessed 2023 Nov 22.
64.Lew J-B, St John DJG, Macrae FA, et al. Benefits, harms and costs of potential age-extensions to the National Bowel Cancer Screening Program in Australia: impact of inviting people aged 40-49 years and 75-84 years. Modelling report: PSC1d. Sydney (AU): Cancer Council Australia; 2017: https://wiki.cancer.org.au/australiawiki/images/b/b6/CRC_PSC1d_modelling_report.pdf. Accessed 2023 Oct 11.
65.Siegel RL, Fedewa SA, Anderson WF, et al. Colorectal cancer incidence patterns in the United States, 1974-2013. J Natl Cancer Inst. 2017;109(8):djw322. PubMed
66.Grade definitions. Rockville (MD): U.S. Preventive Services Task Force; 2018: https://www.uspreventiveservicestaskforce.org/uspstf/about-uspstf/methods-and-processes/grade-definitions. Accessed 2023 Oct 3.
67.Knudsen AB, Zauber AG, Rutter CM, et al. Estimation of benefits, burden, and harms of colorectal cancer screening strategies: modeling study for the US Preventive Services Task Force. JAMA. 2016;315(23):2595-2609. PubMed
68.Meester RGS, Peterse EFP, Knudsen AB, et al. Optimizing colorectal cancer screening by race and sex: microsimulation analysis II to inform the American Cancer Society colorectal cancer screening guideline. Cancer. 2018;124(14):2974-2985. PubMed
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Note that this appendix has not been copy-edited.
Table 2: Characteristics of Included Primary Clinical Studies
Study citation, country, funding source | Study design | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Sehgal et al. (2021)46 Country: US Funding source: NR | Retrospective cohort | Individuals residing in Florida with no data indicating a history of IBD or CRC Individuals < 50 years of age: N = 38,586 Age in years, range: 45 to 49 Individuals ≥ 50 years of age: N = 365,152 Age in years, range: 50 to 54 | Intervention: Exposure colonoscopy for screeninga in individuals < 50 years of age Comparator: Exposure colonoscopy for screeninga in individuals ≥ 50 years of age | Outcome: Incidence rate per 100,000 person-years Time period: 13 years (2005 to 2017) |
Panteris et al. (2020)34 Country: Greece Funding source: Reported as none | Retrospective cohort (described by the authors as ‘cross- sectional’) | Average-risk, asymptomatic individuals (excluding those with a personal or family history of CRC or adenomas, positive screen for CRC, digestive symptoms [i.e., persistent abdominal pain, rectal blood, chronic diarrhea, weight loss], chronic IBD or iron-deficiency anemia) Individuals < 50 years of age: Age in years, range: 30 to 49 Age in years, mean (SD): 42.5 (5.9) Sex, male (%): 42.6 Individuals ≥ 50 years of age: Age in years, range: NR Age in years, mean (SD): 65.9 (8.3) Sex, male (%): 54.7 | Intervention: Colorectal cancer screening in individuals < 50 years of age using colonoscopy as the initial test Comparator: Colorectal cancer screening in individuals ≥ 50 years of ageb using colonoscopy as the initial test | Outcome: Cumulative incidence Time period: 1 year (2017) |
NR = not reported; SD = standard deviation
aExposure colonoscopy was defined as the occurrence of colonoscopy without evidence of a subsequent CRC diagnosis within 6 months; the screening group was defined as inclusive of those who were presumably undergoing screening, or had polyps, benign neoplasms, or a history of polyps.
bThe comparator group was not limited to individuals between the ages of 50 and 75 years of age, with some individuals included who were older than 75 years of age. Nonetheless, the mean age fell between 50 and 75 years, and so, the data were retained for inclusion and summary.
Table 3: Characteristics of Relevant Modelling Studies
Study citation country, funding source | Type of analysis, time horizon | Population characteristics | Relevant intervention(s) and comparator(s) | Relevant variables considered | Data sources | Relevant outcomes |
|---|---|---|---|---|---|---|
Kalyta (2023)45 Country: Canada Funding source: BC Cancer Foundation | Analysis: Microsimulation using the OncoSim model, updated to incorporate recent observed trends in incidence of CRC Time horizon: 40 years | 4 population- based birth cohorts i.e., individuals born between: 1973 and 1977 1978 and 1982 1983 and 1987 1988 and 1992 | Intervention: Colorectal cancer screening starting at 40 or 45 years of age and ending at 74 years of age using biennial FIT (or colonoscopy for high-risk individuals) Comparator: Colorectal cancer screening starting at 50 years of age and ending at 74 years of age using biennial FIT (or colonoscopy for high-risk individuals) | Natural history i.e., rate of adenoma development Screening i.e., sensitivity (75% for cancer), specificity (96%), interval Screening participation was assumed to be 43% in response to the initial invitation (as per existing data) | Published clinical and statistical sources | Benefits of screening, expressed as CRC cases and deaths avoided |
de Lima (2023)32 Country: US Funding source: NR | Analysis: Modification of the CRC-SPIN model to incorporate potential natural history and birth cohort effects Time horizon: Lifetime | Simulated cohort of average-risk (not defined) individuals at 40 years of age | Intervention: Colorectal cancer screening starting at 45 years of age using colonoscopy Comparator: No screening | Natural history i.e., age at adenoma development Screening i.e., sensitivity, interval, and age at which screening ends Perfect adherence to screening was assumed | Published clinical and statistical sources | Benefits of screening, expressed as life-years gained per 1,000 individuals Burden of screening, expressed as estimated lifetime number of colonoscopies per 1,000 individuals |
Knudsen (2021)36 Country: US Funding sources: AHRQ (HHSA- 290 to 2015 to 00007-I-EPC5), US Department of Health and Human Services | Analysis: Microsimulation using SimCRC, CRC-SPIN and MISCAN models, updated to incorporate observed trends in population risk of CRC Time horizon: Lifetime | Hypothetical cohort of average-risk (i.e., asymptomatic, unscreened) individuals at 40 years of age who were unscreened and free of CRC | Intervention: Colorectal cancer screening starting at 45 years of age using FIT or colonoscopy Comparator: No screening; colorectal cancer screening starting at 50 years of age using FIT or colonoscopy | Natural history i.e., adenoma and CRC development Screening i.e., sensitivity, interval, and age at which screening ends; FIT was modelled assuming use of the OC-Sensor family of tests (Polymedco) with a cut-off of 20 mcg of hemoglobin per gram of feces Full adherence to screening and colonoscopy follow-up for non-colonoscopy tests were assumed | Published clinical and statistical sources | Benefits of screening, expressed as estimated life- years gained, CRC cases avoided and CRC deaths averted per 1,000 individuals Burden/harms of screening, expressed as estimated lifetime number of colonoscopies and complications of screening (GI and/or CV events) per 1,000 individuals |
Peterse (2018)44 Country: US Funding sources: American Cancer Society, National Cancer Institute (grant U01-CA199335), grant P30- CA008748 | Analysis: Microsimulation using the MISCAN-Colon model, updated to incorporate observed increases in CRC risk in populations younger than 50 years of age Time horizon: Lifetime | Simulated cohort of average-risk (i.e., free of CRC) 40-year-old individuals who were free of CRC | Intervention: Colorectal cancer screening starting at 40 or 45 years of age using FIT or colonoscopy Comparator: No screening | Updated CRC incidence, age at which screening ends Screening i.e., sensitivity (range between 62.6 to 88.6% for CRC), specificity (96.4%) Complete adherence to screening, follow-up and surveillance were assumed | Published clinical and statistical sources | Benefits of screening, expressed as estimated life- years gained per 1,000 individuals Burden of screening, expressed as estimated lifetime number of colonoscopies |
AHRQ = Agency for Health care Research and Quality; CRC = colorectal cancer; CRC-SPIN = Colorectal Cancer Simulated Population model for Incidence and Natural history; CV = cardiovascular; FIT = fecal immunochemical test; GI = gastrointestinal; mcg = microgram(s); MISCAN = Microsimulation Screening Analysis; SimCRC = Simulation Model of CRC; NR = not reported
Table 4: Characteristics of Included Economic Evaluation
Study citation country, funding source | Type of analysis, time horizon, perspective | Population characteristics | Intervention and comparator(s) | Approach | Source of clinical, cost, and utility data used in analysis | Main assumptions |
|---|---|---|---|---|---|---|
Currais (2021)33 Portugal Funding source: Reported as none | Analysis: Cost utility Time horizon: NR Perspective: Societal | Individuals between 45 and 50 years of age who had not undergone screening for colorectal cancer | Intervention: Colorectal cancer screening starting at 45 years of age using FIT or colonoscopy as the initial test Comparator: No screening | Decision tree model | Incidence, mortality clinical and utility data were taken from national statistical data sources, registries, and reviews of published literature Cost data were taken from national data and published literature sources | WTP threshold = EUR39,760 Screening participation rates of 50% for FIT and 38% for colonoscopy |
EUR = Euro(s); FIT = fecal immunochemical test; NR = not reported; WTP = willingness-to-pay
Table 5: Characteristics of Included Guidelines
Intended users, target population | Intervention and practice considered | Major outcomes considered | Evidence collection, selection, and synthesis | Evidence quality assessment | Recommendations development and evaluation | Guideline validation |
|---|---|---|---|---|---|---|
Intended users: Clinicians Target population: Asymptomatic adults at an average risk for colorectal cancer (i.e., no prior diagnosis of CRC, adenomatous polyps, or inflammatory bowel disease; no personal diagnosis or family history of known genetic disorders that could increase risk for CRC) | CRC screening, including colonoscopy and FIT | CRC incidence, opportunity costs, and resource implications | Database search and critical review of existing guidelines and associated evidence | Included guidelines were assessed using AGREE II | Guidance statements were developed by evaluating and either adopting or adapting recommendations from included guidelines using discussion and consensus | Internal review and external peer review before journal publication |
Austrian National Committee for Cancer Screening (2023)31 | ||||||
Intended users: Unclear Target population: Asymptomatic adults at an average risk for colorectal cancer (i.e., no prior diagnosis of CRC, adenomatous polyps, or IBD; no personal diagnosis or family history of colorectal cancer; no genetic disorder that could increase CRC risk) | A nationwide organized colorectal cancer screening program in Austria using colonoscopy and/or FIT | Patient- relevant outcomes i.e., CRC incidence, mortality, and harms of screening | An evidence review guided by an analytic framework, explicit research questions and selection criteria | GRADE | Recommendations were drafted in consideration of the evidence, its quality, the acceptability of the screening interventions in the population and the USPSTF grading system to indicate the strength of each recommendation | The draft recommendatio ns were reviewed by stakeholders external to the guideline development group |
Cancer Council Australia Colorectal Cancer Guidelines: Updated chapter (2023)47 and Full Guideline (2017)41 | ||||||
Intended Users: Health care providers and policy-makers Target population: Australian populations including people with average risk (i.e., no history or diagnosis of CRC or family history of CRC) and who are at risk of CRC | CRC prevention, screening and diagnosis, clinical care, follow-up, and psychosocial care | Clinical benefits (i.e., reduction in morbidity and mortality) | Systematic review and modelling analyses | NHMRC Evidence Statement form was used to assess and appraise the body of evidence in 201841 The updated chapter used a hybrid approach combining the 2018 approach and GRADE47 | Guideline development was guided by the NHMRC handbook which outlined the protocol for developing research questions and search strategies, conducting a systematic review and modelled analyses, summarizing, and assessing the literature, and formulation and grading recommendations | The draft guideline recommendations were circulated internally;41 released for expert consultation and public review; all feedback was considered and incorporated in accordance with consensus among the Working Group, which endorsed the final recommendations41,47 |
Kaiser Permanente (2022)42 | ||||||
Intended Users: Health care providers Target population: Patients at average risk (i.e., no personal or family history of CRC; no IBD) for CRC between the ages of 45 and 75 | CRC screening, including colonoscopy and FIT | CRC mortality | Systematic literature search and evidence synthesis (methods NR) | Critical appraisal (methods NR) | Recommendations were adapted from existing evidence- based guidelines as identified evidence did not impact existing recommendations (methods NR) | No review was described other than internal approval from a Guideline Oversight Group |
US Multi-Society Task Force on Colorectal Cancer: Focused Update (2022)35 and Full Guideline (2017)40 | ||||||
Intended users: Clinicians Target population: Asymptomatic adults at an average risk for CRC (i.e., no personal or family history of CRC; no clinical symptoms of CRC) | CRC screening, including colonoscopy and FIT The focused update was “restricted to addressing the age to start and stop CRC screening in average-risk individuals”35 | CRC incidence, mortality, potential harms of screening | Systematic review | GRADE | An evidence review was used to develop draft statements that are moved to consensus guidance statements through a series of deliberations | Draft updated consensus guidance statements were reviewed and approved by the American College of Gastroenterology, American Gastroenterological Association, and American Society for Gastrointestinal Endoscopy35 The original full guideline underwent internal review and journal peer review40 |
American College of Gastroenterology (2021)38 | ||||||
Intended users: Clinicians in the US Target population: Individuals at average risk (not defined) for CRC | CRC screening, including colonoscopy and FIT | CRC incidence (including precursors of cancer), CRC mortality and harms of screening | Systematic review | GRADE | NR | NR (though, the guidance is published in a peer-reviewed journal) |
The US Preventive Services Task Force (2021)37 | ||||||
Intended Users: Likely clinicians (though not clearly stated) Target population: Asymptomatic adults 45 years or older who are at average risk of CRC (i.e., no prior diagnosis of CRC, adenomatous polyps, or IBD; no personal diagnosis or family history of known genetic disorders that could increase the risk of CRC) | CRC screening, including colonoscopy and FIT | CRC incidence, mortality, harms of screening | Systematic review59 | Adapted criteria from the NOS (for cohort studies), QUADAS (for diagnostic test accuracy studies), USPSTF criteria (for RCTs)59 | Not specifically stated with respect to this particular guidance; an online document describes general standards for development which indicate the composition of guideline development groups (i.e., consultation with experts) but no detail on the methods for development of recommendations.60 | Not specifically stated with respect to this particular guidance; an online document describes general standards for development which indicate that external review is standard practice.60 |
American Cancer Society Guideline for CRC Screening (2018)39 | ||||||
Intended users: Individuals at average risk for CRC, clinicians, and health care providers Target population: Adults at average risk of CRC (i.e., no history of adenomatous polyps or CRC; no family history; no confirmed or suspected hereditary CRC syndrome (such as familial adenomatous polyposis or Lynch syndrome); no personal history of IBD) | CRC screening, including stool-based tests and structural examination s | Clinical benefits (i.e., life-years gained), CRC incidence, mortality rates, and adverse events | Systematic review and report of simulation modelling | GRADE and GRADE Evidence-to-Decision frameworks | A subcommittee of 6 Guideline Development Group members were responsible for reviewing the evidence, drafting recommendation, and preparing the manuscript, but all members of the Guideline Development Group were included in the review, formulation of proposed guidelines and voting to approve final guidelines | Before guideline finalization, the proposed manuscript was submitted to the ACS Mission Outcomes Committee and Board of Directors for review and approval of recommendations |
ACS = American Cancer Society; CRC = colorectal cancer; FIT = fecal immunochemical testing; GRADE = Grading of Recommendations, Assessment, Development, and Evaluations; NHMRC = National Health and Medical Research Council; NOS = Newcastle Ottawa Scale; QUADAS = Quality Assessment of Diagnostic Accuracy Studies; RCT = randomized controlled trial; USPSTF = US Preventive Services Task Force.
Appendix 3: Critical Appraisal of Included Publications
Note that this appendix has not been copy-edited.
Table 6: Strengths and Limitations of Clinical Studies Using the Downs and Black Checklist28
Strengths | Limitations |
|---|---|
Sehgal (2021)46 | |
Reporting: Reporting was clear, with the study objective, main outcomes, patient characteristics, main findings and estimates of variability using actual values External validity: Given the source of data and the sample size, it is likely that the staff, places, and facilities where the patients were screened is representative of the treatment that the majority of patients receive Internal validity:
| Reporting: Adverse events were not reported External validity
|
Panteris (2020)34 | |
Reporting: Reporting was clear, with the study objective, main outcomes, patient characteristics, main findings and estimates of variability using actual values described Internal validity:
| Reporting: Adverse events were not reported External validity:
|
Table 7: Strengths and Limitations of Economic Evaluation Using the Drummond Checklist29
Strengths | Limitations |
|---|---|
Currais (2021)33 | |
|
|
Table 8: Strengths and Limitations of Guidelines Using AGREE II30
Item | ANCCS (2023)31 | ACP (2023)43 | Kaiser Permanente (2022)42 | USPSTF (2021)37 | ACG (2021)38 | ACS (2018)39 | ||
|---|---|---|---|---|---|---|---|---|
Domain 1: Scope and purpose | ||||||||
1. The overall objective(s) of the guideline is (are) specifically described. | Yes | Yes | Yes | Unclear | Unclear | Yes | No | Yes |
2. The health question(s) covered by the guideline is (are) specifically described. | Yes | No | Yes | Yes | Yes | No | Yes | Yes |
3. The population (patients, public, etc.) to whom the guideline is meant to apply is specifically described. | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
Domain 2: Stakeholder involvement | ||||||||
4. The guideline development group includes individuals from all relevant professional groups. | Yes | Yes | Unclear | Yes | Unclear | Unclear | Unclear | Yes |
5. The views and preferences of the target population (patients, public, etc.) have been sought. | Yes | Yes | Yes | Unclear | Yes | Unclear | Unclear | Yes |
6. The target users of the guideline are clearly defined. | Unclear | Yes | Yes | Yes | Unclear | Yes | Yes | Yes |
Domain 3: Rigour of development | ||||||||
7. Systematic methods were used to search for evidence. | Unclear | Yes | Yes | Yes | Yesa | Yes | Yes | Yes |
8. The criteria for selecting the evidence are clearly described. | Yes | No | No | No | Yes | Yes | Yes | No |
9. The strengths and limitations of the body of evidence are clearly described. | No | Unclear | No | No | Yes | Unclear | No | No |
10. The methods for formulating the recommendations are clearly described. | Yes | Yes | Yes | No | No | Yes | No | Yes |
11. The health benefits, side effects, and risks have been considered in formulating the recommendations. | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
12. There is an explicit link between the recommendations and the supporting evidence. | Yes | Yes | Unclear | No | Yes | Yes | Yes | Yes |
13. The guideline has been externally reviewed by experts before its publication. | Yes | Yes | Yes | Unclear | Yes | Yes | Yes | Yes |
14. A procedure for updating the guideline is provided. | No | No | Yes | No | Yes | No | No | No |
Domain 4: Clarity of presentation | ||||||||
15. The recommendations are specific and unambiguous. | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
16. The different options for management of the condition or health issue are clearly presented. | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes |
17. Key recommendations are easily identifiable. | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
Domain 5: Applicability | ||||||||
18. The guideline describes facilitators and barriers to its application. | No | No | Yes | No | No | No | No | Yes |
19. The guideline provides advice and/or tools on how the recommendations can be put into practice. | Yes | No | No | No | Yes | Yes | No | Yes |
20. The potential resource implications of applying the recommendations have been considered. | No | Yes | Unclear | Yes | Unclear | Yes | Unclear | Yes |
21. The guideline presents monitoring and/or auditing criteria. | No | No | No | No | No | Yes | No | Unclear |
Domain 6: Editorial independence | ||||||||
22. The views of the funding body have not influenced the content of the guideline. | Yes | Unclear | Unclear | Unclear | Unclear | Yes | Unclear | Unclear |
23. Competing interests of guideline development group members have been recorded and addressed. | Yes | Yes | Unclear | No | Unclear | Yes | Unclear | Yes |
ACG = American College of Gastroenterology; ACP = American College of Physicians; ACS = American Cancer Society; AGREE II = Appraisal of Guidelines for Research and Evaluation II; ANCSS = Austrian National Committee for Cancer Screening; USMSTF = US Multi-Society Task Force on Colorectal Cancer; USPSTF = US Preventive Services Task Force
aAll methods for the systematic review are described in a separate report.59
Appendix 4: Main Study Findings
Note that this appendix has not been copy-edited.
Table 9: Colorectal Cancer Incidence
Study, outcome | Colonoscopy screening group | Group difference | |
|---|---|---|---|
< 50 years | ≥ 50 years | ||
Sehgal 202146 | |||
Incidence rate per 100,000 person-years (95% CI) | 23.7 (18.4 to 30.2) | 15.7 (14.1 to 17.5) | NR |
Panteris 202034 | |||
Individuals screened, n | 47 | 333 | OR 1.01 (95% CI 0.12 to 8.4), P = 0.9 |
Colorectal cancer cases, n (%) | 1 (2.1) | 7 (2.1) | |
CI = confidence interval; OR = odds ratio
Table 10: Findings From Relevant Modelling Studies
Main study findings | Authors’ conclusion |
|---|---|
Kalyta (2023)45 | |
Benefits of biennial FIT screening Estimated cumulative CRC cases avoided across a 40-year interval in all birth cohorts, n:
Estimated cumulative CRC deaths avoided across a 40-year interval in all birth cohorts, n:
| “…earlier screening may reduce CRC disease burden and add life-years to the Canadian population at a modest cost. Guideline changes suggesting earlier CRC screening in Canada may be justified, but evaluation of the resulting effects on colonoscopy capacity is necessary.” (p. 1432) |
de Lima (2023)32 | |
Benefits of colonoscopy screening every 10 years from ages 45 to 75 years vs. no screening Estimated life-years gained per 1,000 people, n (95% CrI):
Burden of colonoscopy screening every 10 years from ages 45 to 75 years vs. no screening Estimated lifetime number of colonoscopies per 1,000 people screened, n (95% CrI):
| “We find that model projections of screening benefit are highly dependent on natural history and test sensitivity assumptions… Our results demonstrate that current USPSTF recommendations are robust under a wide range of conditions.” (pp. 1, 20) |
Knudsen (2021)36 | |
Benefits of colonoscopy screening every 10 years initiated at 45 years of age vs. no screening Estimated mean life-years gained per 1,000 people screened, n (95% CI): 337 (NR) Estimated mean CRC cases averted per 1,000 people screened, n (95% CI): 61 (NR) Estimated mean CRC deaths avoided per 1,000 people screened, n (95% CI): 28 (NR) Benefits of annual FIT screening initiated at 45 years of age vs. no screening Estimated mean life-years gained per 1,000 people screened, n (95% CI): 318 (NR) Estimated mean CRC cases averted per 1,000 people screened, n (95% CI): 50 (NR) Estimated mean CRC deaths avoided per 1,000 people screened, n (95% CI): 26 (NR) Benefits of colonoscopy screening every 10 years initiated at 45 years of age vs. 50 years of age Estimated mean life-years gained per 1,000 people screened, n (95% CI): 27 (NR) Estimated mean CRC cases averted per 1,000 people screened, n (95% CI): 3 (NR) Estimated mean CRC deaths avoided per 1,000 people screened, n (95% CI): 1 (NR) Benefits of annual FIT screening initiated at 45 years of age vs. 50 years of age Estimated mean life-years gained per 1,000 people screened, n (95% CI): 26 (NR) Estimated mean CRC cases averted per 1,000 people screened, n (95% CI): 3 (NR) Estimated mean CRC deaths avoided per 1,000 people screened, n (95% CI): 1 (NR) Harms/burden of colonoscopy screening every 10 years initiated at 45 years of age vs. no screening Estimated mean excess complications per 1,000 people screened, n (95% CI): 16 (NR)Estimated lifetime mean number of additional colonoscopies per 1,000 people screened, n (95% CI): 4,248 (NR) Estimated lifetime mean number of additional non-colonoscopy tests per 1,000 people screened, n (95% CI): 0 (NR) Harms/burden of annual FIT screening initiated at 45 years of age vs. no screening Estimated mean excess complications per 1,000 people screened, n (95% CI): 10.2 (NR) Estimated lifetime mean number of additional colonoscopies per 1,000 people screened, n (95% CI): 1,682 (NR) Estimated lifetime mean number of additional non-colonoscopy tests per 1,000 people screened, n (95% CI): 19,412 (NR) Harms/burden of colonoscopy screening every 10 years initiated at 45 years of age vs. 50 years of age Estimated mean excess complications per 1,000 people screened, n (95% CI): 2 (NR) Estimated lifetime mean number of additional colonoscopies per 1,000 people screened, n (95% CI): 784 (NR) Estimated lifetime mean number of additional non-colonoscopy tests per 1,000 people screened, n (95% CI): 0 (NR) Harms/burden of annual FIT screening initiated at 45 years of age vs. 50 years of age Estimated mean excess complications per 1,000 people screened, n (95% CI): 0.2 (NR) Estimated lifetime mean number of additional colonoscopies per 1,000 people screened, n (95% CI): 186 (NR) Estimated lifetime mean number of additional non-colonoscopy tests per 1,000 people screened, n (95% CI): 3,472 (NR) | “This microsimulation modeling analysis suggests that screening for colorectal cancer with stool tests, endoscopic tests, or computed tomography colonography starting at age 45 years provides an efficient balance of colonoscopy burden and life-years gained.” (p. 11) |
Peterse (2018)44 | |
Potential benefits of colonoscopy screening every 10 years vs. no screening Estimated life-years gained per 1,000 people screened, n (95% CI):
Estimated CRC cases per 1,000, n (95% CI):
Potential benefits of annual FIT screening vs. no screening Estimated life-years gained per 1,000 people screened, n (95% CI):
Estimated CRC cases per 1,000, n (95% CI):
Estimated CRC deaths per 1,000, n (95% CI):
Burden of colonoscopy screening every 10 years Estimated lifetime number of colonoscopies per 1,000 people, n (95% CI):
Burden of annual FIT screening Estimated lifetime number of colonoscopies per 1,000 people, n (95% CI):
| “A well-established decision-analytic modeling approach that incorporates the increase in CRC incidence among those of younger ages suggests that screening from ages 45 to 75 years is recommended for the current generation of 40-year-olds. Colonoscopy screening every 10 years, annual FIT screening… are screening strategies with similar benefits and acceptable colonoscopy burdens. If the gradual increase in CRC incidence in more recent birth cohorts continues, even earlier start ages for screening should be considered in the future.” (p. 2972) |
CI = confidence interval; CrI = credible interval; FIT = fecal immunochemical test; NR = not reported; USPSTF = US Preventive Services Task Force; vs. = versus Footnote:
aBaseline sensitivity was assumed to be 0.75 for adenomas of ≤ 5 mm; 0.85 for adenomas of 6 to 9 mm; 0.95 for adenomas of ≥ 10 mm.
Table 11: Summary of Findings of Included Economic Evaluation
Main study findings | Authors’ conclusion |
|---|---|
Currais (2021)33 | |
Cost utility (EUR/QALY)
ICUR
| CRC screening starting at the age of 45 years demonstrated no cost utility in a Portuguese population, assuming an annual incidence of 30/100,000 CRC cases and a WTP threshold of EUR39,760. Incidence in this population would have to rise to 47.5/100,000 CRC cases to demonstrate cost utility. |
CRC = colorectal cancer; EUR = Euro(s); FIT = fecal immunochemical test; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; ref = referent; WTP = willingness-to-pay
Table 12: Summary of Recommendations in Included Guidelines
Relevant recommendation(s) | Evidence supporting the recommendation(s) | Summary of rationale for recommendation(s) | Quality of evidence and strength of recommendations |
|---|---|---|---|
American College of Physicians (2023)43 | |||
“Guidance Statement 2: Clinicians should consider not screening asymptomatic average-risk adults between the ages of 45 to 49 years. Clinicians should discuss the uncertainty around benefits and harms of screening in this population.” (p. 1097) | Lin JS, Perdue LA, Henrikson NB, et al. Screening for colorectal cancer: an evidence update for the US Preventive Services Task Force. Agency for Health care Research and Quality; 2021.59 Lin JS, Perdue LA, Henrikson NB, et al. Screening for colorectal cancer: updated evidence report and systematic review for the US Preventive Services Task Force. JAMA. 2021;325:1978 to 1998.59 Knudsen AB, Rutter CM, Peterse EFP, et al. Colorectal cancer screening: an updated decision analysis for the US Preventive Services Task Force. Agency for Health care Research and Quality; 2021.61 | No available studies of effectiveness and harms were limited to individuals younger than 50 years of age, and diagnostic test accuracy in this population remains unknown. Health care disparities could be exacerbated by shifting limited resources to a screening strategy that is not yet supported by evidence. Recommendations favouring screening in younger populations are largely based on modelled data, which rely on assumptions that may have limited accuracy. The estimated benefit of screening in individuals younger than 50 years of age is lower than that in older populations. | Limitations of the evidence are summarized narratively in support of the guidance statement, but the guidance statement was not assigned a strength and the quality of evidence was not assigned an overall summary score, rating, or value. |
Austrian National Committee for Cancer Screening (2023)31 | |||
“The ANCCS recommends the implementation of an organized colorectal cancer screening program for all adults aged 45–75 years.” (p. 451)a | Lin JS, Perdue LA, Henrikson NB et al. Screening for colorectal cancer: an evidence update for the US preventive services task force. Rockville: Agency for Health care Research and Quality; 2021.59 Knudsen AB, Rutter CM, Peterse EFP, et al. Colorectal cancer screening: an updated decision analysis for the US Preventive Services Task Force. Agency for Health care Research and Quality; 2021.61 Jahn B, Sroczynski G, Bundo M, et al. Effectiveness, benefit harm and cost-effectiveness of colorectal cancer screening in Austria. BMC Gastroenterol. 2019;19(1):209.62 | Based on modelled data, screening initiated at 45 years of age compared to 50 years of age:
| Both recommendations are graded as “A”b and the quality of the evidence is indicated as moderate. (p. 451) |
Cancer Council Australia (2023)47 | |||
“The recommended age range for organised population screening is 45–74 years.” (p. 7 of 168) “Although modelling indicated that it may be cost-effective, starting screening at age 40 is not recommended for population screening because at this age range there is a less favourable benefits to burden balance compared to screening for 45-74 years.” (p. 7 of 168) | “Screening from age 50-74 (the NBCSP target age range as of 2023) program has a very favourable benefits-to burden balance and is highly cost-effective (even cost- saving). None of the alternative screening age ranges performed better than screening from age 50-74 in terms of benefits-to-burden and cost-effectiveness. However, if extending the screening age range is considered, of all the alternative screening age ranges considered in the analysis, screening at 45 to 74, and 40 to 74 years were found to have a more favourable benefits-and-burden balance, were potentially cost- effective, and have the smallest increase in lifetime colonoscopy utilization and associated serious adverse events.” (p. 36) | Grade of evidence: NR; strength of recommendation NR | |
Kaiser Permanente (2022)42 | |||
Routine CRC screening with annual FIT or colonoscopy (every 10 years) is recommended for patients between the ages of 45 and 75 years at average risk i.e., no history of CRC, adenomas, IBD and no family history of CRC. | Relevant sources of supporting evidence were not linked to the recommendation. | None reported. | The quality of the evidence and strength of the recommendation is not reported. |
US Multi-Society Task Force on Colorectal Cancer (2022)35 | |||
“We suggest that clinicians offer CRC screening to all average-risk individuals ages 45 to 49” (p. 65) | Relevant sources of supporting evidence included multiple NRS and modelling studies. | “Although there is no literature demonstrating that CRC screening in individuals under age 50 improves health outcomes such as CRC incidence or CRC-related mortality, sufficient data support the U.S. Multi-Society Task Force to suggest average-risk CRC screening begin at age 45.” (p. 57) | Weak recommendation; low- quality evidence |
The US Preventive Services Task Force (2021)37 | |||
“The USPSTF recommends screening for colorectal cancer in adults aged 45 to 49 years” (p. 1965) Relevant supporting statement (applicable to FIT and colonoscopy, as well as other tests not relevant to this report): “The USPSTF concludes with moderate certainty that screening for colorectal cancer in adults aged 45 to 49 years has moderate net benefit.” (p. 1966) | Knudsen AB, Rutter CM, Peterse EF, et al. Colorectal cancer screening: an updated decision analysis for the US Preventive Services Task Force. Agency for Health care Research and Quality; 2021.61 Knudsen AB, Rutter CM, Peterse EFP, et al. Colorectal cancer screening: an updated modelling study for the US Preventive Services Task Force. JAMA. 2021 05 18;325(19):1998 to 201136 Siegel RL, Fedewa SA, Anderson WF, et al. Colorectal cancer incidence patterns in the United States, 1974 to 2013. J Natl Cancer Inst. 2017;109 (8):djw322.65 | With regard to potential benefits of screening: “Although no studies report on the benefits of screening specifically in adults younger than 50 y, some studies reporting an association of fewer colorectal cancer deaths with screening colonoscopy… included patients younger than 50 y” (p. 1969) With regard to potential harms of screening: “Although fewer studies include persons younger than 50 y, overall findings suggest risk for bleeding and perforation with colonoscopy… may be lower at younger ages” (p. 1969) | The recommendation is described as “B” which is defined as: “The USPSTF recommends the service. There is high certainty that the net benefit is moderate or there is moderate certainty that the net benefit is moderate to substantial.”66 |
American College of Gastroenterology (2021)38 | |||
“We suggest CRC screening in average-risk individuals between ages 45 and 49 years to reduce incidence of advanced adenoma, CRC, and mortality from CRC.” (p. 459) | Comment on available sources of evidence: The guideline summarizes modelling studies used in other guidelines, relevant epidemiologic data, and the overall lack of available, empirical evidence, concluding that: “There are few empirical data regarding the effectiveness of screening in younger average-risk individuals, and the most appropriate screening modality in this age group is not known.” (p. 464) | Epidemiological data indicating a significant rise in the incidence of CRC among individuals younger than 50 years of age. Advantages of CRC screening in individuals younger than 50 years of age include reduced CRC cases and deaths. Disadvantages of CRC screening in individuals younger than 50 years of age include resource implications that may limit the potential of other screening strategies e.g., increasing uptake in individuals 50 years of age and older. “There are few empirical data regarding the effectiveness of screening in younger average-risk individuals, and the most appropriate screening modality in this age group is not known.” (p. 464) | Very low-quality evidence; conditional recommendation. |
American Cancer Society (2018)39 | |||
“The ACS recommends that adults aged 45 y and older with and average risk of CRC undergo regular screening with either high-sensitivity stool-based test or a structural (visual) examination, depending on patient preference and test availability. As part of the screening process, all positive results on noncolonoscopy screening should be followed up with timely colonoscopy.” (p. 255) | Knudsen AB, Zauber AG, Rutter CM, et al. Estimation of benefits, burden, and harms of colorectal cancer screening strategies: modelling study for the US Preventive Services Task Force. JAMA. 2016;315:2595 to 2609.67 Meester RGS, Peterse EFP, Knudsen AB, et al. Optimizing colorectal cancer screening by race and sex: microsimulation analysis II to inform the American Cancer Society colorectal cancer screening guideline. Cancer. 2018 Jul 15;124(14):2974 to 2985.68 Peterse EFP, Meester RGS, Siegal RL, et al. The impact of the rising colorectal cancer incidence in young adults on the optimal age to start screening: microsimulation analysis I to inform the American Cancer Society colorectal cancer screening guideline. Cancer. 2018;124(14):2964 to 2973.44 | “Results from modeling analyses identified efficient and model-recommendable strategies that started screening at age 45 years.” (p. 250) “The recommendation to begin screening at age 45 years is based on disease burden, results from microsimulation modeling, and the reasonable expectation that screening will perform similarly in adults aged 45 to 49 years as in persons for whom screening is currently recommended.” (p. 255) | The recommendation to begin screening at age 45 is a “qualified recommendation,” which is defined as: “…clear evidence of benefit or harm but less certainty either about the balance of benefits and harms or about patient’s values and preferences, which could lead to different individual decisions.” |
ACS = American Cancer Society; ANCSS = Austrian National Committee for Cancer Screening; CRC = colorectal cancer; FIT = fecal immunochemical test; IBD = inflammatory bowel disease; NA = not applicable; NBCSP = National Bowel Cancer Screening Program; NR = not reported. NRS = nonrandomized study; USPSTF = US Preventive Services Task Force
aAdults aged 45 to 75 years refers to: “Persons who do not have signs or symptoms of colorectal cancer and who are at average risk for colorectal cancer” (p. 451).31
bA grading of “A” indicates that: “The ANCCS recommends this service. There is a high certainty of evidence that the net benefit is substantial” (p. 450).31
Table 13: Health Equity and Implementation Considerations From Eligible and Otherwise Relevant Studies
Main study findings | Authors’ conclusion | |
|---|---|---|
Cancer Council Australia (2023)47 | ||
Implementation and health equity relevant good practice statements concerning CRC screening for disadvantaged populations: “18. Practice Point Encouragement by health care professionals (including general practitioners (GPs), Aboriginal Health Workers (AHWs), Aboriginal Health Practitioners (AHPs), nurses and other primary health care professionals substantially boosts participation in colorectal cancer screening. Health care professionals play a key role in providing patients with screening advice. GP or clinic endorsement messages in advance of receiving a test kit, the use of GP or clinic reminder systems, leadership of AHWs and AHPs in health promotion activities and practice audits can improve participation rates (Dodd et al. 2019[107], Goodwin et al. 2020[114], Lee et al. 2021[119]).” (p. 9 of 168) “22. Practice Point Local access to culturally safe, targeted advice and support for colorectal cancer screening, diagnostic services and treatment should be provided through health care professionals to improve equity for Aboriginal and Torres Strait Islander peoples.” (p. 10 of 168) | “Increased participation in the National Bowel Cancer Screening Program (NBCSP) through encouragement and access through a variety of NBCSP kit distribution avenues will increase the program's effectiveness and cost-effectiveness.” (p. 9 of 168) | |
O’Leary (2023)54 | ||
Implementation and health equity relevant information: uptake of FIT screening among a racially diverse population of 45 to 49 years of age:
| “In conclusion, our study suggests that mailed FIT outreach could be used to accelerate the uptake of CRC screening in the newly eligible age group of 45–49-year-old patients. Identifying opportunities to increase the effectiveness of these interventions in this younger population will be important to ensure equitable screening outcomes in response to the updated screening recommendation.” (p. 8/9) | |
Persaud (2023)53 | ||
Health equity and implementation relevant recommendation and supporting statements concerning CRC screening outreach interventions for disadvantaged populations: “We recommend prioritizing colorectal cancer screening outreach efforts for adults aged 45–74 years experiencing disadvantages (strong recommendation, high-certainty evidence)” (p. E1252) | “Because screening starting at age 45 years is effective in general for colorectal cancer (1 additional colorectal cancer death avoided for every 1000 in general population screened starting at age 45 yr rather than 50 yr),70,75 and because people experiencing disadvantages may not be immediately reached by outreach efforts, it is reasonable to start outreach for people experiencing disadvantages at the age of 45 years rather than 50 years, as recommended for Black people by the US Multi-Society Task Force.76” (pp. E1252, E1254) | |
Knudsen (2021)36 | ||
Health equity relevant variable: Race (reported as Black/White, subgrouped by sex) Estimated mean life expectancy at 40 years of age per 1,000 people with no CRC screening, n years:
Estimated mean lifetime CRC cases at 40 years of age per 1,000 people with no CRC screening, n:
Estimated mean CRC deaths at 40 years of age per 1,000 people with no CRC screening, n:
| “[These and other] analyses found that starting screening at age 45 years provided an efficient balance of colonoscopies and LYG for the asymptomatic average-risk population as a whole and by race.” (p. 9)36 | |
The US Preventive Services Task Force (2021)37 | ||
Health equity relevant statement concerning race (described as Black, white) as it pertains to the relevant recommendation (summarized above): “Rates of colorectal cancer incidence are higher in Black adults and American Indian and Alaskan Native adults... However, all adults 45 years or older should be offered screening, even if these risk factors are absent.” (p. 1966) | “Based on the limited available empirical evidence, the USPSTF is not able to make a separate, specific recommendation on colorectal cancer screening in Black adults... The current USPSTF statement recommends starting screening for everyone at age 45 years, including Black adults.” (p. 1970) | |
Ghai (2020)56 | ||
Implementation relevant findings of beliefs of 1,887 health care providers concerning CRC screening in individuals younger than 50 years of age Beliefs concerning effectiveness of colonoscopy for reducing CRC mortality, % providers:
Beliefs concerning effectiveness of FIT for reducing CRC mortality, % providers
Provider recommendations for colonoscopy screening interval, % providers
Provider recommendations for FIT screening interval, % providers
| “Most providers believed screening was of unproven effectiveness for persons younger or older than conventional screening ages and few recommended it for these populations. If screening recommendations are extended to older and younger age groups, as recommended by some guidelines, targeting providers with relevant evidence-based screening test information should be evaluated as a strategy for increasing provider beliefs in test effectiveness and patient uptake of CRC screening.” (p. 10) | |
Levin (2020)55 | ||
Health equity and implementation relevant variables: Uptake of screening and CRC cases by race (reported as African American (subgrouped by age, 45 to 50 years [n = 10,232] and 51-56 years [n = 3,603]), White 51 to 56 years (n = 22,832), Hispanic 51 to 56 years (n = 10,930), Asian/Pacific Islander 51 to 56 years (n = 8,893) Completion of FIT in response to mailout, % patients, OR vs. African American 45 to 50 years (95% CI)
Completion of colonoscopy, % patients with positive FIT, OR vs. African American 45 to 50 years (95% CI)
CRC cases, % patients with positive FIT, OR vs. African American 45 to 50 years (95% CI)
| “In conclusion, guidelines recommend early CRC screening in African Americans, but have lacked evidence of screening uptake and test yield. We demonstrated that implementation of FIT-based CRC screening in African Americans ages 45 to 50 is feasible in a large integrated health care setting, and that FIT positivity, colonoscopy follow-up after a positive FIT, and the detection of… cRc in this population subgroup who completed screening was at least comparable to that seen in other racial/ethnic groups 51 to 56 years of age.” (p. 11) | |
CI = confidence interval; CRC = colorectal cancer; FIT = fecal immunochemical test; LYG = life-years gained; OR = odds ratio; USPSTF = US Preventive Services Task Force; vs. = versus
aIndicates an observation that is statistically significantly lower than the African American (45 to 50 years) group b: indicates an observation that is statistically significantly higher than the African American (45 to 50 years) group.
Appendix 5: References of Potential Interest
Note that this appendix has not been copy-edited.
Guidelines and Recommendations
Clinical Practice Guidelines (Insufficient Supporting Evidence)
American Cancer Society guideline for colorectal cancer screening. Atlanta (GA): American Cancer Society; 2020: https://www.cancer.org/cancer/types/colon- rectal-cancer/detection-diagnosis-staging/acs-recommendations.html. Accessed 2023 Sep 12.
Colorectal cancer screening and surveillance: clinical guideline and rationale. Bannockburn (IL): American Society of Colon and Rectal Surgeons: https://fascrs.org/healthcare-providers/education/clinical-practice-guidelines/colorectal-cancer-screening-and-surveillance-clini. Accessed 2023 Sep 12.
Contributors: Elizabeth Carson, Shannon Hill, Camille Santos, Anusree Subramonian
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy- makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third- party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec. Questions or requests for information about this report can be directed to Requests@CADTH.ca