CADTH Health Technology Review
Dental Bridges for Partial Tooth Loss
Rapid Review
Authors: Shannon Hill, Sharon Bailey, Angie Hamson
External Reviewer
This document was externally reviewed by a content expert who has granted permission to be cited.
Dr. Ronald Kelly, DDS
Territorial Dental Officer
Government of Nunavut
Acknowledgements
The authors would like to thank the anonymous individual with lived experience and their caregiver for their time and energy contributing to this report.
Abbreviations
CI
confidence interval
FDP
fixed dental prosthetic
MA
meta-analysis
SR
systematic review
Key Messages
This review identified limited evidence about the clinical effectiveness of dental bridges for partial tooth loss in adults. The identified studies had several limitations, including limited comparative data and concerns related to a lack of dental bridge specificity. Therefore, the findings related to effectiveness are uncertain.
In adults with partial tooth loss who have dental bridges supported by natural teeth, there may be minimal rates of dental bridge failure, high rates of dental bridge survival, and few complications.
Limited evidence from 1 study with a small number of patients that directly compared all-ceramic dental bridges with metal-ceramic dental bridges reported no failures in either group but suggested that patients with all-ceramic dental bridges may have more complications and changes in patient satisfaction, but the findings were uncertain.
One patient with lived experience shared clinical information related to the use of a dental bridge and reported that the dental bridge helped facilitate eating but they experienced issues with chipping which negatively affected function and satisfaction with the appearance of the bridge, which also had financial implications for repair and replacement of the damaged bridge. None of the studies in this report included direct measures related to the patient-identified outcomes, specifically financial implications.
We did not find any studies that compared dental bridges to partial dentures or different designs of dental bridges, nor did we find any studies on the cost-effectiveness of dental bridges that met the criteria for this review.
We did not find any evidence-based guidelines on the use of dental bridges for adults with partial tooth loss that met the criteria for this review.
Context and Policy Issues
Oral health is defined by WHO as a state of being free from mouth or facial pain, disease, infection, or tooth decay or loss.1 Globally, the most common forms of oral disease are attributed to dental caries (cavities or decay), periodontal disease, oral cancer, oral infection, and trauma from injuries.1 Dental caries are among the most common chronic diseases throughout the world and contribute to a major global public health challenge, despite being preventable.1 One key measure of oral health is the decayed, missing, and filled teeth index measure; the most recent decayed, missing, and filled teeth data reported in 2010 show that approximately 38.7% of 12-year-olds living in Canada had 1 or more permanent teeth affected by caries.1 Societal contexts may also contribute to access to oral health care and can have a subsequent impact on oral health and tooth loss.2 In 2020, approximately 27% of adults in Canada skipped dental care or check ups due to cost,2 and 1 in 6 Canadians with a oral health need cannot address their need due to cost.1 Overall, people in Canada from lower-income families were found to have approximately twice as many worse outcomes compared with higher-income families for any measure of oral health.1 Unaddressed oral diseases, such as dental caries and periodontal disease, can directly contribute to partial or complete tooth loss, known as edentulism.1
Partial tooth loss can often contribute to further oral health issues like periodontal disease or dental caries for surrounding teeth.3 A common intervention for partial tooth loss is the use of a fixed dental bridge. Fixed dental bridges are used to replace 1 or more missing teeth for the purpose of addressing a functional or cosmetic need.4 A fixed dental bridge typically extends across the area where teeth may be missing, and is made up of artificial teeth fused between 2 or more abutment crowns.5 Dental bridges are held in place by either natural teeth supports from leftover teeth on either side of the missing area or by dental implants that are inserted into the alveolar bone.5 Fixed dental bridges are a permanent dental procedure; as a result, they are often costly depending on the type of dental bridge.5 Fixed dental bridges are often susceptible to damage due to daily use and may need to be replaced; however, with adequate care, the estimated longevity of a fixed dental bridge is approximately 10 years.3
The purpose of this report is to summarize the evidence related to the clinical effectiveness, cost-effectiveness, and recommendations regarding the use of dental bridges for partial tooth loss in adults. This information is meant to inform and support decisions involved in the use and coverage of dental bridges for partial tooth loss.
Research Questions
What is the clinical effectiveness of dental bridges compared to partial dentures for partial tooth loss in adults?
What is the clinical effectiveness of dental bridges compared to no intervention for partial tooth loss in adults?
What is the clinical effectiveness of different types of dental bridges for partial tooth loss in adults?
What is the cost-effectiveness of dental bridges for partial tooth loss in adults?
What are the evidence-based guidelines regarding the use of dental bridges for partial tooth loss in adults?
Methods
Literature Search Methods
A limited literature search was conducted by an information specialist on key resources including MEDLINE, the Cochrane Database of Systematic Reviews, the International HTA Database, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were partial tooth loss and fixed dental bridges. Comments, newspaper articles, editorials, and letters were excluded. If possible, retrieval was limited to the human population. The search was also limited to English-language documents published between January 1, 2017, and December 1, 2022.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
|---|---|
Population | Adults (18 years and older) with partial tooth loss (e.g., 1 or more missing teeth, either arch, either subsection of the mouth, partial edentulism) |
Intervention | Dental bridges supported by natural teeth (any materials [e.g., metal ceramic or porcelain, all ceramic or porcelain, metal, zirconia ceramic, cobalt chromium] and any designs [e.g., traditional, Maryland or butterfly, cantilever]) |
Comparator | Q1, Q4: Partial dentures (any materials and designs) Q2, Q4: No intervention Q3, Q4: Dental bridges made with different materials or designs Q5: Not applicable |
Outcomes | Q1, Q2, Q3: Clinical benefits (e.g., longevity, masticatory function, quality of life, patient satisfaction) and harms (e.g., tooth complications, technical complications, and adverse events) Q4: Cost-effectiveness (e.g., cost per quality-adjusted life-year gained, incremental cost-effectiveness ratios) Q5: Recommendations regarding best practices (e.g., consideration for anterior and posterior bridges, number of missing teeth to be replaced by a bridge, appropriate patient populations, guidance related to how often dental bridges should be replaced, contraindications) |
Study designs | Health technology assessments, systematic reviews, randomized controlled trials, nonrandomized studies, economic evaluations, evidence-based guidelines |
Q = question.
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, they were duplicate publications, or were published before 2017. Systematic reviews (SRs) in which all relevant studies were captured in other more recent or more comprehensive SRs were excluded. Primary studies retrieved by the search were excluded if they were captured in 1 or more included SRs. Guidelines with unclear methodology were also excluded.
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the following tool as a guide: A Measurement Tool to Assess Systematic Reviews 2 (AMSTAR 2)6 for SRs. Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Patient Engagement
CADTH has adopted the CADTH Framework for Patient Engagement in Health Technology Assessment,7 which includes standards for patient involvement in individual health technology assessments and is used to support and guide CADTH activities involving patients. For this report, CADTH engaged a patient contributor with lived experience with dental bridges.
Invitation to Participate and Consent
People with lived experience were identified through CADTH’s connections to dental associations, patient groups, and through a media search. CADTH contacted the groups by email to ask that a recruitment email be disseminated to their patient partners. The preliminary request included the purpose and scope of this project, the purpose of engagement, and the nature of engagement activities. CADTH received responses from 3 interested parties. The Patient Engagement Officer contacted potential participants by email to set up an introductory call. Once an individual was selected, CADTH obtained the individual and their caregiver’s informed consent to share their lived experiences with a dental bridge with CADTH staff. Patient collaborators are recognized and thanked in the Acknowledgement section of this report. The participating individuals were offered an honorarium for their time and effort.
Engagement Activities
An individual with a dental bridge shared their personal experiences during drafting of the report. The engagement was a virtual dialogue between a CADTH Patient Engagement Officer, a CADTH Clinical Research Officer, the individual with a dental bridge, and their caregiver (a close family member). The caregiver provided translation and interpretation for the questions and conversation for the individual with a dental bridge. Perspectives gained through the engagement processes were used to ensure relevance of outcomes of interest and to provide insights, background, and context to the findings.
Patient involvement was guided by the Guidance for Reporting Involvement of Patients and the Public (version 2) Short Form reporting checklist, which is outlined in Appendix 6.8
Summary of Evidence
Quantity of Research Available
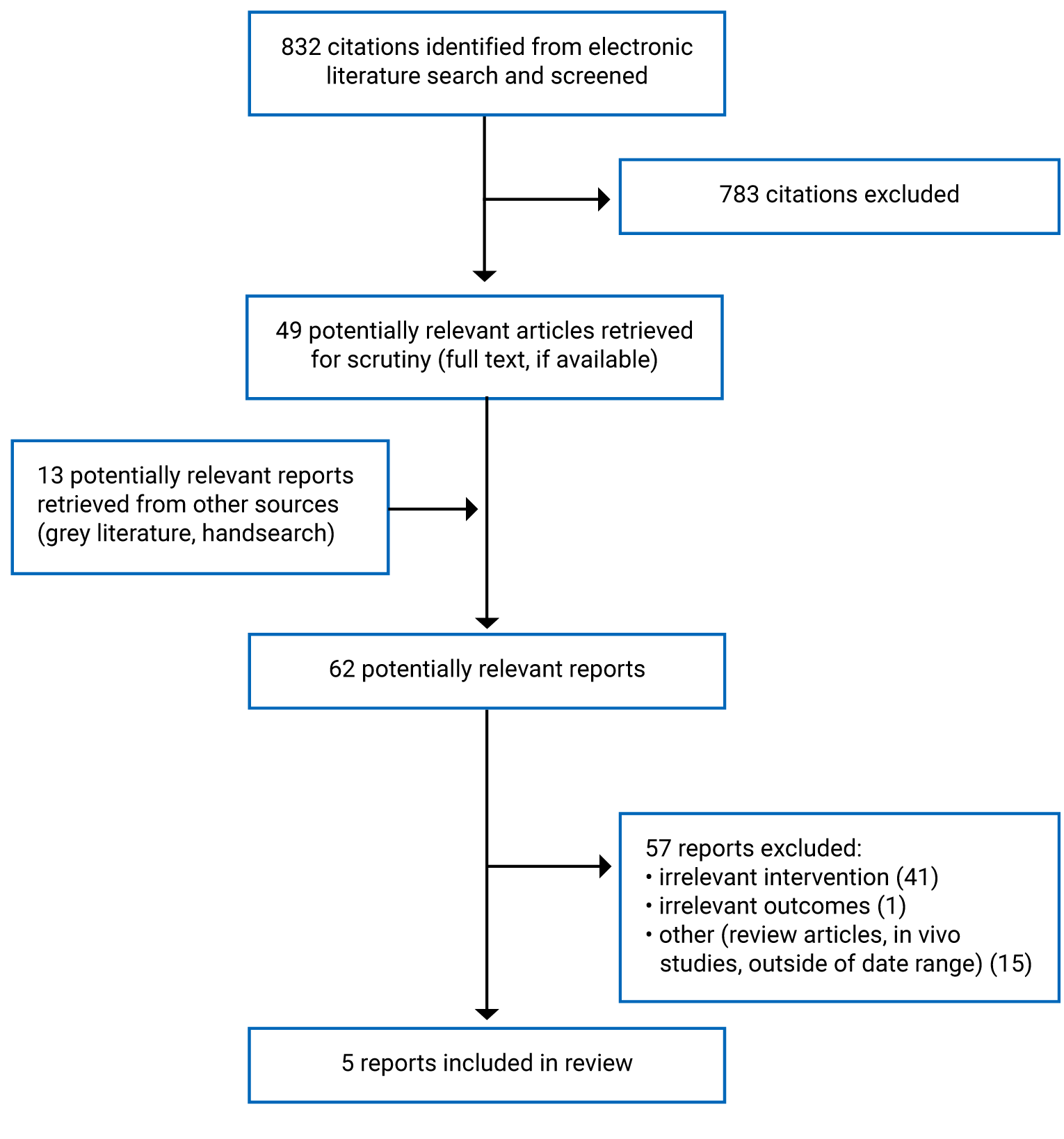
A total of 832 citations were identified in the literature search. Following screening of titles and abstracts, 783 citations were excluded and 49 potentially relevant reports from the electronic search were retrieved for full-text review. Thirteen potentially relevant publications were retrieved from the grey literature search for full-text review. Of these potentially relevant articles, 57 publications were excluded for various reasons, and 5 publications met the inclusion criteria and were included in this report. These comprised 5 SRs. Appendix 1 presents the PRISMA9 flow chart of the study selection.
Summary of Study Characteristics
Five SRs with meta-analyses (MAs)10-14 were included in this report. Four SRs had broader inclusion criteria than this report, which included fixed dental protheses (FDPs) that were not specifically described as dental bridges and implant-supported FDPs.10,12-14 Only studies that fit the inclusion criteria (i.e., studies that specified outcomes related to dental bridge use) are reported.
One of the identified SRs, conducted in Switzerland and published in 2018, did not include any relevant primary studies.12 This SR searched for primary studies that included adults with partial tooth loss that received a supported FDP; however, this SR only included studies that used an implant-supported dental bridge in their results despite searching for both implant-supported and natural tooth–supported fixed dental bridges.12 The authors conducted an MA, but the findings of the MA are not relevant to this report because there were no primary studies relevant to this report. Eligible study designs and the search time frame was not restricted for this SR, but the date of last search was not reported.12 Additional details regarding the characteristics of the included publications are provided in Appendix 2.
Study Design
One SR was published in 2022 and included studies published up to March 2020; however, only 2 relevant primary studies comprising case series were eligible to be included in this report.10 One SR with an MA was published in 2021 and included 17 primary studies comprised of 1 randomized controlled trial (RCT) and 16 nonrandomized studies published up to January 2020.11 One SR with an MA published in 2018 included 42 relevant primary studies published up to January 2017.13 One SR was published in 2017 and included 4 relevant primary studies including RCTs published up to May 2017.14 Three of the included SRs contained primary studies that overlapped with 1 or more SR.11,13,14 The degree of overlap is outlined in Appendix 5.
Country of Origin
The included SRs were conducted in Spain,10 Germany,11 the Netherlands,13 and the US.14
Patient Population
All 4 SRs included primary studies of adult patients in need of dental protheses due to edentulous complications.10,11,13,14 The total number of patients included in each SR ranged from 132 to 536.10,11,14 One SR did not report the total number of patients.13 The sample size of each included primary study ranged from 8 to 301.10,11,13,14
Interventions and Comparators
Consistent with the inclusion criteria for the current report, the identified SRs included primary studies that specifically described clinical effectiveness outcomes for dental bridges supported by natural teeth.10,11,13,14 One SR specified dental bridges consisting of all-ceramic material,11 whereas another SR specified any type of FDPs including dental bridges consisting of metal-free material.14 The comparators for the identified SRs included any alternative type of multiunit dental prosthetic,10,11 any metal ceramic or other all-metal material dental prosthetic,14 no intervention,10 or the comparator was not specified.11,13
Outcomes
The identified SRs reported outcomes related to the clinical effectiveness of dental bridges for patients with partial tooth loss. Four included SRs reported outcomes associated with dental bridge failure, including the number of failed prosthetics,10,11 the number of patients who experienced prosthetic failure,14 and prosthetic failure rate.11,13 Two SRs with MA reported outcomes associated with dental bridge survival rate.11,13 Three SRs reported outcomes associated with dental bridge complications, including complication rate,11 the number of biological and technical complications,10 and the number of patients who experienced a complication.14 One SR reported the number of patients who experienced a change in patient satisfaction with dental bridge use.14
Summary of Critical Appraisal
An overview of the critical appraisal of the included studies is summarized below, but additional details regarding the strengths and limitations of included publications are provided in Appendix 3. Only relevant items from the AMSTAR 2 tools were used to assess the SR that did not include any relevant primary studies.12
All 5 SRs provided clearly defined research questions, inclusion criteria, and adequate details of included studies,10-14 whereas 4 SRs also included population, intervention, comparators, and outcome components to support the literature search.10-12,14 Two SRs stated that review methods were established before the review was conducted;10,12 however, 3 SRs did not state that the review methods were established before the review was conducted, which created challenges for determining if there were any deviations in the methods used that could affect validity.11,13,14 All 5 SRs indicated that multiple databases were included in their search, and provided details related to search terms and search strategies that could help determine reproducibility.10-14 All 5 SRs studies did not restrict their search time frame,10-14 whereas 3 SRs did not restrict for study designs, which may reduce potential selection or publication bias.10-12 All 5 SRs indicated that literature search screening was done in duplicate,10-14 whereas 4 SRs also indicated that data extraction was done in duplicate thus minimizing potential errors in data collection and synthesis.10,12-14 Three SRs assessed risk of bias for the included primary studies using appropriate and validated techniques.10,11,14 In addition, 3 SRs indicated that potential effects of risk of bias for individual studies were accounted for when interpreting the results, which could help determine the internal validity of findings from the included primary studies.10,11,14 Two SRs assessed potential publication bias using appropriate methods.10,14 Four SRs indicated that appropriate statistical methods were used for primary outcomes and determining any measures of effect.10,11,13,14 Four of the SRs used appropriate methods for statistical combination of results and to determine heterogeneity across included primary studies, thus providing greater confidence for interpreting combined results.10,11,14 None of the SRs provided information related to funding sources for included primary studies.10-14 Four SRs disclosed if any funding was received for the review,10-12,14 whereas 4 SRs disclosed any conflict of interest implications for the review which could help determine if results of the review were affected by potential external influence.10,11,13,14
Summary of Findings
Four SRs were identified regarding the clinical effectiveness of dental bridges supported by natural teeth for individuals with partial tooth loss.10,11,13,14 Appendix 4 presents the relevant study findings by outcome, including dental bridge failure, dental bridge survival, complications associated with dental bridges, and patient satisfaction. Relevant primary study findings that specified outcomes related to dental bridge use are presented in this review. When feasible, the results outcome data from individual primary studies within SRs were only reported once to avoid duplication; however, some of the pooled estimates from separate reviews may contain overlapping data. A citation matrix illustrating the degree of overlap is presented in Appendix 5.
One SR with an MA included 1 primary study that presented findings for a direct comparison of all-ceramic dental bridge material compared with metal-ceramic dental bridge material.14 One SR specified that the outcomes are from dental bridges consisting of all-ceramic material.11 One SR included primary studies with no intervention comparators or single-arm data,10 whereas 2 SRs did not specify comparator outcomes for the MA findings.11,13 Outcomes from these 3 SRs were grouped as no intervention; however, there are a lack of comparative data because the included outcomes are specific to dental prosthetics, thus not applicable to individuals in a control arm who did not have a dental prosthetic.10,11,13
One additional SR searched for clinical effectiveness outcomes associated with the use of dental bridges supported by natural teeth, but no relevant primary studies were identified so no findings could be extracted.12
Clinical Effectiveness of Dental Bridges Compared to Partial Dentures
No evidence was identified regarding the clinical effectiveness of dental bridges for partial tooth loss in adults compared to partial dentures; therefore, no summary can be provided.
Clinical Effectiveness of Dental Bridges Compared to No Intervention
Dental Bridge Failure
One SR with 2 relevant case series that assessed the number of failed prosthetics and found approximately 45% (27 of 60) and 2.1% (7 of 332) of prosthetics failed, respectively.10 One case series was a single-arm study, whereas the other case series included a control arm with patients who did not have dental prosthetics; however, given that the individuals in the control arm did not have a dental prosthetic, dental bridge failure was not applicable for the control group, therefore no comparison was possible.10 Additional information from 1 case series stated that a failure was defined as a fracture in the bond or dislodging of the pontic, which required a new bridge.10 The other primary case series described the type of dental bridge that experienced a failure, which included a fracture in 1 bridge of unilateral extension, 3 bridges of cross-arch extension with distal abutment teeth, and 3 bridges of cross-arch extension involving cantilever units.10
One SR with an MA provided the combined overall number of failed prosthetics among 17 primary studies of all-ceramic dental bridges; however, the combined outcomes of the primary studies were grouped by similar mean follow-up times.11 Nine primary studies with a follow-up of approximately 4 years reported that approximately 4.5% (11 of 241) of prosthetics failed.11 Six primary studies with a follow-up of up to 7 years reported that approximately 5.7% (12 of 208) of prosthetics failed.11 Three primary studies with a follow-up of up to 10 years reported that approximately 18.8% (29 of 154) of prosthetics failed.11 In addition, the failure rate per 100 FDP years was estimated for each primary study group. The estimated failure rate was 1.78 (95% confidence interval [CI], 1.435 to 2.16), 2.07 (95% CI, 1.555 to 2.746), and 1.82 (95% CI, 1.716 to 1.935) for primary studies with a follow-up of approximately 4 years, up to 7 years, and up to 10 years, respectively.11 The authors of the SR described the common reasons for failure within the pooled analysis, which included secondary caries, chipping, and loss of retention leading to either dental bridge failure or replacement.11
One SR with an MA provided the combined overall dental bridge failure rate per year for 42 relevant primary studies and reported a 3.6% (95% CI, 2.7% to 4.7%) failure rate per year.13 The study reported that the weighted mean failure rate per year was 1.0% (95% CI, 0.7% to 1.5%) for the dental bridge supports, and the difference between the overall dental bridge failure rate and the weighted mean dental bridge support failure rate was not statistically significant (P = 0.34).13 The authors of this SR with an MA also collected information related to alternative FDPs supported by implants; however, it was unclear if any comparison was made between the 2 intervention groups, therefore no comparative information could be collected.13 The authors of the SR described the reasons for dental bridge failure, which was characterized as a failure in 1 of the supports because of a fracture or the framework or because of a defect in the material used.13
Dental Bridge Survival
One SR with an MA provided the combined estimated dental bridge survival rate at 3 years, 5 years, and 10 years across 3 groups of primary studies stratified by follow-up times for dental bridges consisting of all-ceramic material.11 The estimated 3-year dental bridge survival rate was reported to be 94.66, 93.80, and 94.53 (unit of measurement not provided) for primary studies with a follow-up of up to 4 years, 7 years, and 10 years, respectively.11 The estimated 5-year dental bridge survival rate was reported to be 91.10, 89.67, and 90.89 (unit of measurement not provided) for primary studies with a follow-up of up to 4 years, 7 years, and 10 years, respectively.11 The estimated 10-year dental bridge survival rate was reported to be 82.20, 79.33, and 81.78 (unit of measurement not provided) for primary studies with a follow-up of up to 4 years, 7 years, and 10 years, respectively.11 No measure of statistical significance, or measure of uncertainty were provided for these outcomes.
One SR with an MA provided the combined overall dental bridge survival rate per year for 42 relevant primary studies and reported an overall 96.4% survival rate per year.13 The study reported that the weighted mean survival rate for dental bridge supports per year was 99.0%; among studies with 5 or more years’ worth of follow-up, the survival rate per year was 97.9%.13 No measure of statistical significance or uncertainty was provided for these outcomes.
Complications Associated With Dental Bridge Use
One SR included 2 relevant case series that reported on complications associated with dental bridge use.10 One of the case series assessed the number of overall biological and technical complications, and reported that 8 abutment teeth were fractured attributing to the overall number of biological complications, whereas 18 (5.4%) technical complications were reported out of 332 included prosthetics.10 Technical complications included loss of retention and framework fractures. The other case study reported that no abutments were lost during their assessment.10
One SR with MA provided the combined estimated complication rate per 100 FDP years across 3 groups of primary studies stratified by follow-up times for dental bridges consisting of all-ceramic material.11 The authors of the SR with MA reported an estimated complication rate of 1.24 (95% CI, 0.932 to 1.661) (unit of measure not provided) for primary studies with approximately 4 years follow-up, 1.08 (95% CI, 0.759 to 1.523; unit of measure not provided) for primary studies with up to 7 years follow-up, and 1.8 (95% CI, 1.479 to 2.244; unit of measure not provided) for primary studies with up to 10 years follow-up.11 In addition, the authors reported the estimated success rate which was defined as complications with prostheses excluding failures. The authors reported that the estimated 3-year success rate ranged from 94.53 to 96.77 (unit of measure not provided) for different groups, the estimated 5-year success rate, which ranged from 90.89 to 94.62 (unit of measure not provided) for different groups, and the estimated 10-year success rate, which ranged from 81.78 to 89.25 (unit of measure not provided) for different groups.11 No statistical significance, or uncertainty was provided for these outcomes.
Clinical Effectiveness of Different Types of Dental Bridges
Dental Bridge Failure Between All-Ceramic Material and Metal-Ceramic Material
One SR included 1 RCT that assessed the number of patients who experienced a failed prosthetic at 1 year and at 3 years in patients with all-ceramic material and metal-ceramic material dental bridges.14 In both groups, no patients reported having a failed prosthetic at 1 year or at 3 years.14
Complications Associated with Dental Bridge Use Between All-Ceramic Material and Metal-Ceramic Material
One SR included 1 RCT that assessed the number of patients who experienced a complication associated with dental bridge use at 3 years in patients with all-ceramic material dental bridges and metal-ceramic material dental bridges.14 Five of 17 patients (29%) with all-ceramic material dental bridges reported a complication at 3 years, whereas 3 of 17 patients (18%) with metal-ceramic material dental bridges reported a complication at 3 years.14 The authors reported that patients with all-ceramic material dental bridges had an odds ratio of 1.94 (95% CI, 0.38 to 9.88) for experiencing a complication compared with patients with metal-ceramic material dental bridges; however, this was not statistically significant (P = 0.42).14 The estimated odds ratio is uncertain and should be interpreted with caution due to the large difference between the upper and lower limits of the confidence interval.
Patient Satisfaction Between All-Ceramic Material and Metal-Ceramic Material Dental Bridges
One SR included 1 RCT that assessed the number of patients who reported a change in aesthetic satisfaction in patients with all-ceramic material dental bridges and metal-ceramic material dental bridges.14 Satisfaction changes in oral health-related quality of life were measured using the Oral Health Impact Profile-14 model of assessment.14 Five patients (29%) with all-ceramic material dental bridges reported a change in aesthetic satisfaction, whereas no patients with metal-ceramic material dental bridges reported a change in aesthetic satisfaction.14 The authors reported that patients with all-ceramic material dental bridges had an odds ratio of 15.5 (95% CI, 0.78 to 304.61) for reporting a change in aesthetic satisfaction compared with patients with metal-ceramic material dental bridges; however, this was not statistically significant (P = 0.07).14 The estimated odds ratio should be interpreted with caution due to the large difference between the upper and lower limits of the confidence interval; this large degree of uncertainty and imprecision suggests there is insufficient evidence to show a difference between intervention groups.
Cost-Effectiveness of Dental Bridges for Partial Tooth Loss in Adults
No evidence was identified regarding the cost-effectiveness of dental bridges for partial tooth loss in adults; therefore, no summary can be provided.
Guidelines Regarding the Use of Dental Bridges for Partial Tooth Loss in Adults
No evidence-based guidelines were identified regarding the use of dental bridges for partial tooth loss in adults; therefore, no summary can be provided.
Limitations
The SRs identified in this report have limitations that should be considered when interpreting the results. Most notably, the quality of evidence included in the SRs is uncertain and the comparative evidence is unclear except for 1 primary study included in 1 SR with an MA.14 Limited information was available related to the study designs and availability of control groups for primary studies included in 3 of the SRs with MAs,10,11,13 so any interpretation of combined results from the MA findings may be uncertain and at high risk of bias. A concerted effort was made to include only data from primary studies that specified outcomes related to dental bridge use, which created challenges in controlling for information overlap from analyses that grouped large numbers of primary studies together and described outcomes associated with dental bridges as the intervention. There was also a large degree of heterogeneity within and across primary studies included in the SRs, specifically related to the type of intervention and population. Because of this heterogeneity, it is challenging to accurately compare outcomes across primary studies. In addition, some of the included SRs lacked sufficient information related to the outcomes presented (e.g., units of measure or measures of uncertainty), which created challenges in accurately interpreting findings with limited available data.
No evidence was identified regarding the cost-effectiveness or evidence-based guidelines of dental bridge use in patients with partial tooth loss, and no conclusions can be drawn related to funding considerations or recommendations for this treatment. No evidence was identified regarding the clinical effectiveness of dental bridges compared with partial dentures or between different designs of dental bridges, and no conclusions can be drawn related to comparative assessments of these different dental prosthetics. After speaking with an individual with lived experience using a dental bridge, an outcome that was identified as important to that individual was the burden of cost for replacing or repairing a chipped dental bridge. None of the identified literature in this report considered the cost of repairing or replacing a dental bridge and the direct impact that this may have on patients. Only 1 individual with lived experience was included in this report to share their experience with using a dental bridge, and the outcomes identified by this individual may not be representative of all patients who use a dental bridge.
The generalizability of findings specifically from the primary studies included in the SRs may be challenging to determine because the time frame of included primary studies extends to 1979 and it is unknown if older findings may be applicable to the modern treatment landscape. There was also a lack of information related to the setting in which interventions were applied, which may create challenges in generalizing results. No included studies were conducted in Canada or related to the Canadian dental context; thus, it is unclear how generalizable the findings may be to Canada. This should be considered because dental treatment outcomes may vary between country, especially when comparing public versus private payer systems for dental treatment, therefore findings may have different implications depending on the population and societal context.
Conclusions and Implications for Decision- or Policy-Making
This report identified 5 SRs related to the clinical effectiveness of dental bridges for patients with partial tooth loss.10-14 One of the identified SRs did not contain relevant primary studies so did not contribute to the findings of this report.12 Two SRs contained MA findings for clinical effectiveness outcomes related to dental bridges but did not specify comparative findings,11,13 whereas 1 SR contained findings from 2 relevant primary studies. These included a single-arm case series and a case series with a control arm; however, none of the outcomes relevant to this report were applicable to the control arm.10 One of the SRs reported findings from 1 RCT related to the clinical effectiveness of dental bridges using all-ceramic material compared to metal-ceramic material for patients with partial tooth loss.14 No evidence was identified regarding the clinical effectiveness of dental bridges compared to partial dentures or between different designs of dental bridges. No evidence was identified regarding the cost-effectiveness or recommendation of dental bridge use in patients with partial tooth loss; therefore, no conclusion can be drawn.
Each included study specified that the population of interest included adult patients in need of dental protheses due to edentulous complications.10-14 Studies were included in this report because the authors specified outcomes from included primary studies that were directly related to the use of dental bridges supported by natural teeth. Limited information was provided in each study regarding the specific dental bridge design or material. When reported, the follow-up time frame for each relevant study ranged from 12 months to 204 months.10,11,13,14 Additional supporting information was sought from 1 patient with lived experience using a dental bridge for partial tooth loss, which contributed to the clinical effectiveness outcomes associated with patient satisfaction.
Three SRs provided evidence related to dental bridge failure,10,11,13 2 SRs with MAs provided evidence related to dental bridge survival,11,13 and 2 SRs provided evidence related to complications associated with dental bridge use.10,11 However, comparative evidence to other dental prosthetics was not available for these SRs and the relevant outcomes were not applicable to the group that received no intervention. Evidence identified in this review found varying proportions of prosthetics had a failure, ranging from 2.1% to 45% of total prosthetics.10,11 When stratified by length of follow-up time from primary studies, 1 SR with an MA found that for primary studies with a follow-up of approximately 4 years or up to 7 years, 4.5% and 5.7% of prosthetics failed, respectively, whereas 18.8% of prosthetics failed in primary studies with a follow-up of approximately 10 years.11 This may indicate that dental bridge longevity may be impacted by length of use. Given the large increase in proportion of failed dental bridges between primary studies with a follow-up of 7 years and 10 years, this may provide context related to how long dental bridges may last and when a patient may expect to replace or repair their dental bridge. The estimated failure rate per 100 FDP years ranged from 1.78 to 2.07.11 Based on this evidence from studies with a follow-up of 4 to 10 years included in this SR, it is estimated that approximately 2 dental bridges may fail in a 100-year time frame.11 One SR with an MA assessed the combined failure rate for dental bridges and the failure rate for supports of dental bridges and found that the overall dental bridge failure rate per year was higher (approximately 4%) than the weighted mean dental bridge support failure rate per year (1%), but this difference was not statistically different.13
Evidence from 1 SR with an MA found that, based on findings from studies with follow-up times of up to 4 years, 7 years, and 10 years, the estimated 3-year dental bridge survival rate was approximately 94%, the estimated 5-year dental bridge survival rate ranged from 89% to 91%, and the estimated 10-year dental bridge survival rate was between 79% and 82%.11 Evidence from 1 SR with an MA assessed the combined survival rate for dental bridges and the survival rate of the dental bridge supports and found that the overall dental bridge survival rate per year was 96.4%, which was lower compared with the weighted mean dental bridge support survival rate of 99.0%.13
Evidence from 1 SR found that in 1 primary study a small number of patients experienced biological or technical complications, whereas in another primary study, no patients experienced complications associated with abutment loss.10 Evidence from another SR with an MA found that based on the findings from studies with follow-up times of up to 4 years, 7 years, and 10 years, the estimated complication rate per 100 FDP years ranged from 1.08 and 1.82; the estimate was highest among primary studies with the longest follow-up times of up to 10 years.11 Based on this evidence (studies with a follow-up of 4 to 10 years included in this SR), it is estimated that approximately 1 to 2 complications may occur in a 100-year time frame.11 Evidence from the same review found that the estimated 3-year success rate ranged between approximately 94% and 97%, the estimated 5-year success rate ranged between 90% and 95%, and the estimated 10-year success rate ranged between 81% and 89%. The estimates were highest among primary studies with medium follow-up times of up to 7 years.11
Comparing different materials, 1 SR that reported findings from 1 relevant RCT, found that no patients with all-ceramic dental bridges or metal-ceramic dental bridges experienced a failed prosthetic at 1 year and 3 years.14 Patients in this study with both types of dental bridges experienced complications at 3 years (i.e., 29% of patients with all-ceramic dental bridges and 18% of patients with metal-ceramic dental bridges), and patients with all-ceramic dental bridges may have higher odds of experiencing a complication at 3 years; however, this difference was not statistically significant and there is uncertainty in the finding.14 In terms of satisfaction, 29% of patients with an all-ceramic dental bridges reported a change in aesthetic satisfaction compared to none of the patients with the metal-ceramic dental bridges. Patients with all-ceramic dental bridges also may have higher odds of aesthetic satisfaction; however, this finding was not statistically significant, and there was substantial imprecision in this estimate.14 There were 17 patients in both groups in this study, which may contribute to the imprecision of the findings; more evidence may be needed to demonstrate a difference between these 2 types of dental bridges.
After speaking with an individual with lived experience with a dental bridge, the outcomes that were identified as important were function, durability (breaking or chipping), and the cost of treatment, repair, and replacement of a dental bridge. Outcomes related to function and durability may be relevant to findings identified from the literature related to dental bridge failure, dental bridge survival, and complications. The individual described feeling dissatisfied with the appearance of the bridge, which caused them distress at their own appearance. Feelings of distress and embarrassment can accompany damaged bridges. This outcome may provide context related to patient satisfaction. The financial implications of obtaining, repairing, and replacing a bridge were also a concern raised. This highlights equity issues for individuals without private insurance or with limited income. This outcome related to the potential personal financial burden of repairing or replacing a dental bridge was not reported within the studies in this report and may highlight a potential gap in the evidence.
The limitations of the included studies (e.g., uncertain quality of primary studies included in the SRs, heterogeneity of included primary studies, lack of clarity of included studies, potential high risk of bias, lack of statistical analyses, limited comparative evidence, lack of cost-effectiveness or evidence-based guidelines, and limited Canadian context) should be considered when interpreting the findings of this report. The evidence from this report may help stakeholders by providing limited evidence related to the use of dental bridges for patients with partial tooth loss. Further high-quality research that is specific to the use, design, and material of dental bridges within the Canadian context is needed to adequately assess the clinical effectiveness and cost-effectiveness of dental bridge use and inform recommendations that are relevant to Canadian users. In addition, future research on failure of dental bridges should consider other damage to bridges that result in cosmetic issues and the impact on mental health and satisfaction. Future work exploring the cost-effectiveness of dental bridges should consider the patient-borne costs (e.g., initial treatment and subsequent repairs or replacements) and the cost per quality-adjusted life-years.
References
1.Canadian Dental Association. The state of oral health in Canada. 2017; https://www.cda-adc.ca/stateoforalhealth/_files/TheStateofOralHealthinCanada.pdf. Accessed 2023 Jan 6.
2.Farmer J SS, Ghoneim A, Proaño D, Moharrami M, Kaura K, McIntyre J, Quiñonez C. Environmental scan of publicly financed dental care in Canada: 2022 update. 2022; https://caphd.ca/wp-content/uploads/2022/10/Canada-Dental-environmentscan-UofT-20221017.pdf. Accessed 2023 Jan 6.
3.Canadian Dental Association. Bridges & Dentures - Replacing Missing Teeth. 2023; https://www.cda-adc.ca/en/oral_health/talk/procedures/bridges_dentures/. Accessed 2023 Jan 6.
4.The British Society for Restorative Dentistry. Crowns, Fixed Bridges and Dental Implants. 2013; https://www.bsrd.org.uk/File.ashx?id=15191. Accessed 2023 Jan 6.
5.Canadian Dental Association. Bridges. 2023; https://www.cda-adc.ca/en/oral_health/talk/procedures/bridges_dentures/bridges.asp. Accessed 2023 Jan 6.
6.Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. PubMed
7.CADTH framework for patient engagement in health technology assessment. Ottawa (ON): CADTH; 2022: https://www.cadth.ca/cadth-framework-patient-engagement-health-technology-assessment. Accessed 2023 Jan 11.
8.Staniszewska S, Brett J, Simera I, et al. GRIPP2 reporting checklists: Tools to improve reporting of patient and public involvement in research. Res Involv Engagem. 2017;3:13. PubMed
9.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
10.Montero E, Molina A, Palombo D, Moron B, Pradies G, Sanz-Sanchez I. Efficacy and risks of tooth-supported prostheses in the treatment of partially edentulous patients with stage IV periodontitis. A systematic review and meta-analysis. J Clin Periodontol. 2022;49 Suppl 24:182-207. PubMed
11.Saravi B, Vollmer A, Hartmann M, et al. Clinical performance of CAD/CAM all-ceramic tooth-supported fixed dental prostheses: A systematic review and meta-analysis. Materials (Basel). 2021;14(10):20. PubMed
12.Wittneben JG, Wismeijer D, Bragger U, Joda T, Abou-Ayash S. Patient-reported outcome measures focusing on aesthetics of implant- and tooth-supported fixed dental prostheses: A systematic review and meta-analysis. Clin Oral Implants Res. 2018;29 Suppl 16:224-240. PubMed
13.Pol CWP, Raghoebar GM, Kerdijk W, Boven GC, Cune MS, Meijer HJA. A systematic review and meta-analysis of 3-unit fixed dental prostheses: Are the results of 2 abutment implants comparable to the results of 2 abutment teeth? J Oral Rehabil. 2018;45(2):147-160. PubMed
14.Poggio CE, Ercoli C, Rispoli L, Mairona C, Esposito M. Metal-free materials for fixed prosthodontic restorations. Cochrane Database Syst Rev. 2017;12(12):CD009606. PubMed
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Note that this appendix has not been copy-edited.
Table 2: Characteristics of Included Systematic Reviews
Study citation, country, funding source | Study designs and numbers of relevant primary studies included | Population characteristics | Relevant intervention and comparator(s) | Relevant clinical outcomes, length of follow-up |
|---|---|---|---|---|
Montero et al., (2022)10 Spain Funding source: This systematic review was self-funded | Study design: SR with MA Last search date: March 2020 Number of primary studies: 2 case series | Eligibility criteria: Partially edentulous adult patients diagnosed with periodontitis Total number of patients included in relevant primary studies: 342 Sample size: 301 and 41 | Intervention: Any type of multiunit dental prosthetic using teeth as abutments Comparator: Any type of multiunit dental prosthetic in patients without periodontitis or no intervention | Outcomes:
Follow-up (range): 36 to 204 months |
Saravi et al., (2021)11 Germany Funding source: Baden-Wuerttemberg Ministry of Science, Research and Art, and the University of Freiburg in the funding program Open Access Publishing. | Study design: SR with MA Last search date: January 2020 Number of primary studies: 17 (1 RCT, 16 nonrandomized studies) | Eligibility criteria: Patients using computer automated all-ceramic fixed dental protheses Total number of patients included in relevant primary studies: 563 Sample size (range): 15 to 75 | Intervention: Tooth–supported all-ceramic fixed dental protheses
Comparator: Alternative fixed dental protheses or not specified | Outcomes:
Follow-up (range): 18 to 120 months |
Pol et al., (2018)13 Netherlands Funding source: NR | Study design: SR with MA Last search date: January 2017 Number of primary studies: 42a | Eligibility criteria: Partially edentulous patients with 3-unit fixed dental protheses Total number of patients included in relevant primary studies: NR Sample size (range): 8 to 259b | Intervention: Tooth–supported 3-unit fixed dental protheses Comparator: Not specified | Outcomes:
Follow-up (range): 12 to 198 months |
Wittneben et al., (2018)12 Switzerland Funding source: No funding | Study design: SR with MA Last search date: NR Number of primary studies: 0 | Eligibility criteria: Partially edentulous patients with tooth–supported fixed dental protheses Total number of patients included in relevant primary studies: NA Sample size: NA | Intervention: Tooth–supported fixed dental protheses Comparator: NA | Outcomes: NA Follow-up: NA |
Poggio et al., (2017)14 US Funding source: National Institute for Health Research, UK; Cochrane Oral Health Global Alliance | Study design: SR with MA Last search date: May 2017 Number of primary studies: 4 RCTs | Eligibility criteria: RCTs with adult patients who received fixed prosthodontic restorative treatment Total number of patients included in relevant primary studies: 132 Sample size: 21 to 40 | Intervention: All types of metal-free material fixed dental protheses Comparator: Metal-ceramic or other conventional all-metal material fixed dental protheses | Outcomes:
Follow-up (range): 3 to 6 years |
MA = meta-analysis; NA = not applicable; NR = not reported; SR = systematic review.
aSpecific study design was NR.
bFrom studies that reported sample size.
Appendix 3: Critical Appraisal of Included Publications
Note that this appendix has not been copy-edited.
Table 3: Strengths and Limitations of Systematic Reviews Using AMSTAR 26
Strengths | Limitations |
|---|---|
Montero (2022)10 | |
|
|
Saravi (2021)11 | |
|
|
Pol (2018)13 | |
|
|
Wittneben (2018)12 | |
|
|
Poggio (2017)14 | |
|
|
AMSTAR 2 = A Measurement Tool to Assess Systematic Reviews 2; NA = not applicable; NR = not reported; RCT = randomized controlled studies; ROB 2.0 = Risk of Bias tool 2.0; ROBINS-I = Risk of Bias In Non-Randomized Studies of Interventions.
Appendix 4: Main Study Findings
Note that this appendix has not been copy-edited.
Table 4: Summary of Findings by Outcome — Dental Bridge Failure
Outcomes | Montero et al. (2022)10 SR | Saravi et al. (2021)11 SR with MA | Pol et al. (2018)13 SR with MA | Poggio et al. (2017)14 SRd | ||||
|---|---|---|---|---|---|---|---|---|
Quirynen et al. (1999) | Nyman et al. (1979) | Group 1a | Group 2b | Group 3c | — | All-ceramic material | Metal-ceramic material | |
Sample size | 41 | 251 | 242 | 199 | 150 | NR | 17 | 17 |
Number of failed prosthetics, n of Ne (%) | 27 of 60 (45%) | 7 of 332 (2.1%) | 11 of 241 (4.5%) | 12 of 208 (5.7%) | 29 of 154 (18.8%) | — | — | — |
Number patients with failed prosthetics at 1 year, n/N | — | — | — | — | — | — | 0 of 17 | 0 of 17 |
Number of patients with failed prosthetics at 3 years, n/N | — | — | — | — | — | — | 0/17 | 0/17 |
Estimated failure rate per 100 FDP years, rate (95% CI) | — | — | 1.78 (1.435 to 2.216) | 2.07 (1.555 to 2.746) | 1.82 (1.716 to 1.935) | — | — | |
Overall failure rate per year, % (95% CI) | — | — | — | — | — | 3.6% (2.7% to 4.7%) | — | |
Weighted mean dental bridge support failure rate per year, % (95% CI) | — | — | — | — | — | 1.0% (0.7% to 1.5%) | — | |
P valuef | — | — | — | — | — | 0.34 | — | |
CI = confidence interval; FDP = fixed dental prosthetic; NR = not reported.
aIncluded studies were divided in 3 groups depending on follow-up times. Group 1 consisted of 9 studies with a follow-up of approximately 4 years (mean = 34.6 months; range, 18 to 46 months).
bIncluded studies were divided in 3 groups depending on follow-up times. Group 2 consisted of 6 studies with a follow-up of up to 7 years (mean = 69.3 months; range, 60 to 84 months).
cIncluded studies were divided in 3 groups depending on follow-up times. Group 3 consisted of 3 studies with a follow-up of up to 10 years (mean = 118.2 months; range, 116.4 to 120 months).
dOutcomes based on 1 RCT (Nicolaisen et al. [2016]).
eOutcome is based on number of prosthetics.
fDifference in overall failure rate and weighted mean dental bridge support failure rate.
Table 5: Summary of Findings by Outcome — Dental Bridge Survival
Outcome | Saravi et al. (2021)11 SR with MA | Pol et al. (2018)13 SR with MA | ||
|---|---|---|---|---|
Group 1a | Group 2b | Group 3c | ||
Sample size | 242 | 199 | 150 | NR |
Estimated 3-year survival rate | 94.66 | 93.80 | 94.53 | — |
Estimated 5-year survival rate | 91.10 | 89.67 | 90.89 | — |
Estimated 10-year survival rate | 82.20 | 79.33 | 81.78 | — |
Overall survival rate per year, % | — | — | — | 96.4% |
Weighted mean dental bridge support survival rate per year, % | — | — | — | 99.0% |
Survival rate per year at ≥ 5 years of follow-up, % | — | — | — | 97.9% |
NR = not reported.
aIncluded studies were divided in 3 groups depending on follow-up times. Group 1 consisted of 9 studies with a follow-up of approximately 4 years (mean = 34.6 months; range, 18 to 46 months).
bIncluded studies were divided in 3 groups depending on follow-up times. Group 2 consisted of 6 studies with a follow-up of up to 7 years (mean = 69.3 months; range, 60 to 84 months).
cIncluded studies were divided in 3 groups depending on follow-up times. Group 3 consisted of 3 studies with a follow-up of up to 10 years (mean = 118.2 months; range, 116.4 to 120 months).
Table 6: Summary of Findings by Outcome — Complications Associated With Dental Bridge
Outcome | Montero et al. (2022)10 SR | Saravi et al. (2021)11 SR with MA | Poggio et al. (2017)14 SRd | ||||
|---|---|---|---|---|---|---|---|
Quirynen et al. (1999) | Nyman et al. (1979) | Group 1a | Group 2b | Group 3c | All-ceramic material | Metal-ceramic material | |
Sample size | 41 | 251 | 242 | 199 | 150 | 17 | 17 |
Overall biological complications, n (%) | NR | 8 (NR) | — | — | — | — | — |
Overall technical complications, n (%) | NR | 18 (5.4%) | — | — | — | — | — |
Number of abutments lost, n of N (%) | 0 of 82 | NR | — | — | — | — | — |
Estimated complication rate per 100 FDP years, rate (95% CI) | — | — | 1.24 (0.932 to 1.661) | 1.08 (0.759 to 1.523) | 1.82 (1.479 to 2.244) | — | — |
Estimated 3-year success ratee | — | — | 96.27 | 96.77 | 94.53 | — | — |
Estimated 5-year success ratee | — | — | 93.78 | 94.62 | 90.89 | — | — |
Estimated 10-year success ratee | — | — | 87.56 | 89.25 | 81.78 | — | — |
Number of patients with complications at 3 years, n/N | — | — | — | — | — | 5 of 17 | 3 of 17 |
P value | — | — | — | — | — | 0.42 | |
Odds ratio (95% CI) | — | — | — | — | — | 1.94 (0.38 to 9.88) | |
CI = confidence interval; FDP = fixed dental prostheses; NR = not reported.
aIncluded studies were divided in 3 groups depending on follow-up times. Group 1 consisted of 9 studies with a follow-up of approximately 4 years (mean = 34.6 months; range, 18 to 46 months).
bIncluded studies were divided in 3 groups depending on follow-up times. Group 2 consisted of 6 studies with a follow-up of up to 7 years (mean = 69.3 months; range, 60 to 84 months).
cIncluded studies were divided in 3 groups depending on follow-up times. Group 3 consisted of 3 studies with a follow-up of up to 10 years (mean = 118.2 months; range, 116.4 to 120 months).
dOutcome based on 1 RCT (Nicolaisen et al. [2016]).
eSuccess rates were considered complications with prostheses excluding failures.
Table 7: Summary of Findings by Outcome — Patient Satisfaction
Outcome | Poggio et al. (2017)14 SRa | |
|---|---|---|
All-ceramic material | Metal-ceramic material | |
Sample size | 17 | 17 |
Number of patient reported aesthetic satisfaction changes, n of N | 5 of 17 | 0 of 17 |
P value | 0.07 | |
Odds ratio (95% CI) | 15.4 (0.78 to 304.61) | |
CI = confidence interval.
aOutcome based on 1 RCT (Nicolaisen et al. [2016]).
Appendix 5: Overlap Between Included Systematic Reviews
Note that this appendix has not been copy-edited.
Table 8: Overlap in Relevant Primary Studies Between Included Systematic Reviews
Primary study citation | Montero et al. (2022)10 | Saravi et al. (2021)11 | Pol et al. (2018)13 | Poggio et al. (2017)14 |
|---|---|---|---|---|
Rinke et al. Int. J. Pros. 2018; 31: 35-42 | — | Yes | — | — |
Teichmann et al. Clin. Oral Investig. 2018; 22: 2905-2915 | — | Yes | — | — |
Nicolaisen et al. International Journal of Prosthodontics. 2016; 29(3): 259-64 | — | — | — | Yes |
Ioannidis et al. J. Dent. 2016; 47: 80-85 | — | Yes | — | — |
Chaar et al. J. Dent. 2015; 43: 512-517 | — | Yes | — | — |
Naenni et al. J. Dent. 2015; 43: 1365-1370 | — | Yes | Yes | Yes |
Selz et al. J. Dent. 2015; 43: 1428-1435 | — | Yes | — | — |
Solá-Ruíz et al. J. Pros. Dent. 2015; 113: 578-584 | — | Yes | — | — |
Reich et al. Clin. Oral Invest. 2014; 18: 2171-2178 | — | Yes | Yes | — |
Sasse et al. J Dent. 2014; 42: 373-376 | — | — | Yes | — |
Burke et al. J. Dent. 2013; 41: 992-999 | — | Yes | Yes | — |
Solá-Ruíz et al. Int J Prosthodont. 2013; 26: 175-180 | — | — | Yes | — |
Crisp et al. Dent Mater. 2012; 28: 229-236 | — | — | Yes | — |
Kern et al. J Am Dent Assoc. 2012; 143: 234-240 | — | — | Yes | — |
Kern et al. Int J Prosthodont. 2012; 25: 622-624 | — | — | Yes | — |
Ohlmann et al. Quintessence Int. 2012; 43: 643-648 | — | — | Yes | Yes |
Pelaez et al. Int J Prosthodont. 2012; 25: 451-458 | — | — | Yes | — |
Perry et al. Compend. Contin. Educ. Dent. 2012; 33: e1-e5 | — | Yes | — | — |
Raigrodski et al. J. Prosthet Dent. 2012; 108: 214-222 | — | Yes | Yes | — |
Schmitt et al. Int J Prosthodont. 2012; 25: 585-589 | — | — | Yes | — |
Sorrentino et al. Clin. Oral Investig. 2012; 16: 977-985 | — | Yes | Yes | — |
Cortellini et al. J Clin Periodontol. 2011; 38: 915-924 | — | — | Yes | — |
Makarouna et al. Int J Prosthodont. 2011; 24: 204-206 | — | — | Yes | Yes |
Sax et al. Int J Comput Dent. 2011; 14: 183-202 | — | — | Yes | — |
Boeckler et al. J Prosthodont. 2010; 19: 592-597 | — | — | Yes | — |
Christensen et al. J Am Dent Assoc. 2010; 141: 1317-1329 | — | — | Yes | — |
Gokcen-Rohlig et al. Int J Prosthodont. 2010; 23: 562-565 | — | — | Yes | — |
Ikai et al. J Prosthodont Res. 2010; 54:173-178 | — | — | Yes | — |
Philipp et al. Quintessence Int. 2010; 41: 313-319 | — | — | Yes | — |
Roediger et al. Int J Prosthodont. 2010; 23:141-148 | — | — | Yes | — |
Tsumita et al. J Prosthodont Res. 2010; 54: 102-105 | — | — | Yes | — |
Beuer et al. Clin. Oral Investig. 2009; 13: 445-451 | — | Yes | Yes | — |
Eschbach et al. Int J Prosthodont. 2009; 22: 490-492 | — | — | Yes | — |
Sailer et al. Clin Oral Implants Res. 2009; 20: 219-225 | — | — | Yes | — |
Schmitt et al. Int. J. Prosthod. 2009; 22: 597-603 | — | Yes | — | — |
Walton et al. Int J Prosthodont. 2009; 22: 260-267 | — | — | Yes | — |
Wolfart et al. Dent Mater. 2009; 25: e63-e71 | — | — | Yes | — |
Wolfart et al. Eur J Oral Sci. 2009; 117: 741-749 | — | — | Yes | — |
Zhang et al. Chin Med J. 2009; 122: 3007-3010 | — | — | Yes | — |
Edelhoff et al. Quint. Int. 2008; 39: 459-471 | — | Yes | — | — |
Esquivel-Upshaw et al. Int J Prosthodont. 2008; 21: 155-160 | — | — | Yes | — |
Molin et al. Int J Prosthodont. 2008; 21: 223-227 | — | — | Yes | — |
De Backer et al. Int J Prosthodont. 2006; 19: 567-573 | — | — | Yes | — |
Marquardt et al. Quintessence Int. 2006; 37:253-259 | — | — | Yes | — |
Sailer et al. Quint. Int. 2006; 37: 685-693 | — | Yes | — | — |
Taskonak et al. Dent Mater. 2006; 22: 1008-1013 | — | — | Yes | — |
Vult von Steyern et al. J. Oral Rehabil. 2005; 32: 180-187 | — | Yes | — | — |
Vult von Steyern et al. Int J Prosthodont. 2001; 14: 379-384 | — | — | Yes | — |
Quirynen et al. Journal of Periodontology. 1999; 70(2): 205-212 | Yes | — | — | — |
Sorensen et al. J Calif Dent Assoc. 1998; 26: 207-214 | — | — | Yes | — |
Chai et al. J Prosthet Dent. 1997; 77: 1-11 | — | — | Yes | — |
Fayyad et al. J Oral Rehabil. 1996; 23: 675-678 | — | — | Yes | — |
Jokstad et al. J Dent. 1996; 24: 309-315 | — | — | Yes | — |
Probster et al. Int J Prosthodont. 1993; 6: 259-263 | — | — | Yes | — |
Hochman et al. J Prosthet Dent. 1987; 58: 542-545 | — | — | Yes | — |
Nyman et al. Journal of Clinical Periodontology. 1979; 6(2): 98-105 | Yes | — | — | — |
Appendix 6: Guidance for Reporting Involvement of Patients and the Public (Version 2) Short-Form Reporting Checklist
Note that this appendix has not been copy-edited.
Table 9: Patient Involvement Dental Bridge Use
Section and topic | Item | Report section |
|---|---|---|
Aim | A patient contributor was involved in developing the report and commenting on outcomes. | Methods |
Methods | After giving informed consent, the contributor with lived experience participated in a dialogue with the Patient Engagement Officer and Research Officer, with their caregiver interpreting the conversation. The individual reported their experiences and perspectives on the outcomes via virtual meeting, with their caregiver sharing an update by email afterwards. | Methods |
Results of engagement | The researchers were made aware of the importance of several outcomes and themes. In particular, the relevance of the research question for patients and the connections between the quality-of-life outcomes (i.e., durability of the bridge and its connection to distress and dissatisfaction) were confirmed. There were also concerns about patient-borne costs, which speaks to equity issues in the community. | Conclusions and Implications for Decision- or Policy-Making |
Discussion and conclusions | Success of patient involvement in this report is related to several factors. First, the patient contributor was briefed on the objectives of the project and supported in their role, with interpretation services provided by their caregiver. The research team was receptive to this involvement and used it in their approach to the clinical evidence. Established processes are in place, and compensation was offered for their time to participate in the project. The patient preferred to remain anonymous in this report; therefore, they are not acknowledged by name. | Conclusions and Implications for Decision- or Policy-Making |
Reflections/critical perspective | The patient contributor was able to participate through the interpretation from their caregiver. However, their responses were limited to short answers, without significant elaboration. Their caregiver (a close family member) helped with explaining details. They reported patient concerns, family-borne costs, and burdens; for example, the financial cost to repairing and replacing damaged bridges. Ethical and equity issues are sometimes revealed in the telling of patient experiences. Financial costs were raised as an important consideration for people with limited income or without private insurance coverage. One limitation of our approach is that people need reliable access to phone and/or computer and internet to contribute to CADTH, which may exclude some voices. | Conclusions and Implications for Decision- or Policy-Making |
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca