Drugs, Health Technologies, Health Systems
Health Technology Review
Ferric Derisomaltose for Heart Failure and Iron Deficiency
Summary
Main Take-Aways
There was insufficient evidence to strongly support the use of IV ferric derisomaltose for the treatment of patients with heart failure with reduced ejection fraction and iron deficiency.
It is not known how well ferric derisomaltose works or how safe it is compared with ferric carboxymaltose or other IV iron treatments in adults with heart failure and iron deficiency.
Key Messages
What Is the Issue?
Iron deficiency is a common comorbidity in patients with heart failure.
Decision-makers are interested in understanding the clinical efficacy and safety of ferric derisomaltose in the treatment of patients with heart failure and iron deficiency.
What Did We Do?
We searched key resources, including journal citation databases, and conducted a focused internet search for relevant evidence published since 2020.
What Did We Find?
Clinical evidence suggests that ferric derisomaltose results in limited improvement in health-related quality of life in the short-term, without any effect on mortality, hospitalization, or exercise capacity compared to usual care.
There was a reduction in the frequency of cardiovascular death or hospitalization for stroke, myocardial infarction, or heart failure in patients who received ferric derisomaltose compared to patients who received usual care, but the evidence was uncertain due to imprecision and risk of bias. Safety outcomes were similar in both groups of patients.
An evidence-based guideline suggests that clinicians may consider 1 of 3 IV iron products, including ferric derisomaltose, for the treatment of patients with heart failure with reduced ejection fraction and iron deficiency, despite a lack of sufficient evidence to support a strong recommendation for IV iron therapy.
We did not identify any evidence on the comparative clinical efficacy and safety of ferric derisomaltose compared to ferric carboxymaltose or other IV iron products in adult patients with heart failure and iron deficiency.
What Does It Mean?
There was insufficient evidence to strongly support the use of IV ferric derisomaltose for the treatment of patients with heart failure with reduced ejection fraction and iron deficiency.
It is not known how well ferric derisomaltose works or how safe it is compared with ferric carboxymaltose or other IV iron treatments in adults with heart failure and iron deficiency.
Additional evidence is necessary to inform decision-making regarding the use of ferric derisomaltose for the treatment of adults with heart failure and iron deficiency.
Abbreviations
6MWD
6-minute walk distance
CI
confidence interval
GRADE
Grading of Recommendations Assessment, Development and Evaluation
HRQoL
health-related quality of life
MID
minimal importance difference
MLHFQ
Minnesota Living With Heart Failure Questionnaire
NICE
National Institute for Health and Care Excellence
RCT
randomized controlled trial
SAE
serious adverse event
TSAT
transferrin saturation
VAS
visual analogue scale
Context and Policy Issues
What Is Iron Deficiency in Patients With Heart Failure?
Iron deficiency is a common comorbidity in patients with heart failure, affecting more than 30% to 50% of patients with chronic heart failure.1 In Canada, a population-based study reported that in patients with heart failure, iron deficiency was present in about 70% of patients, while iron deficiency anemia was present in 50% of patients.2 Iron deficiency in patients with heart failure is defined as a serum ferritin level of less than 100 mcg/L or between 100 mcg/L and 299 mcg/L if their transferrin saturation (TSAT) level is less than 20%.3 People with heart failure and iron deficiency often experience reduced exercise capacity, worse heart failure symptoms, and poorer quality of life and are at higher risk for hospitalization and other complications.4 Iron deficiency is associated with higher mortality in patients with heart failure.5 Causes of iron deficiency in patients with heart failure include gastrointestinal or genitourinary blood loss related to the use of antiplatelet drugs and/or oral anticoagulation, impaired nutrition, malabsorption due to congestion, and abnormal production of hepcidin.6
What Are Current Treatment Options for Iron Deficiency in Patients With Heart Failure?
Treatment for iron deficiency in patients with heart failure primarily involves IV iron formulations, including iron sucrose, ferric carboxymaltose, and ferric derisomaltose.7 Ferric carboxymaltose is approved by Health Canada for the treatment of iron deficiency in patients with heart failure and New York Heart Association class II/III to improve exercise capacity, as well as for the treatment of iron deficiency anemia in adult and pediatric patients 1 year of age and older when oral iron preparations are not tolerated or are ineffective.8 Health Canada has approved ferric derisomaltose for the treatment of iron deficiency anemia in adult patients who have intolerance or unresponsiveness to oral iron therapy.9 IV iron is preferred over oral iron supplements due to higher efficacy, faster repletion, and better tolerability, especially in patients who have impaired oral absorption.7
What Is Ferric Derisomaltose?
Ferric derisomaltose (also known as iron isomaltoside 1000) is indicated for the treatment of iron deficiency anemia in adult patients who have an intolerance or unresponsiveness to oral iron therapy.10 Ferric derisomaltose is used off-label in patients with heart failure and iron deficiency. Ferric derisomaltose is available in 100 mg/mL elemental iron solution for injection and may be administered as an IV drip infusion, an IV bolus injection, or an injection into a dialyzer.9 The dose and administration schedule for ferric derisomaltose are determined for each patient, typically based on the patient’s hemoglobin concentration and body weight, with allowance for clinical judgment.9
Why Is It Important to Do This Review?
IV iron therapies can substantially affect health care systems due to infusion-related requirements (e.g., dedicated infusion clinics), the need for multiple visits to receive infusions, and potentially lengthy infusion times. Canada’s Drug Agency issued 2 reimbursement recommendations for 2 IV iron preparations between 2020 and 2025. A 2025 recommendation was issued for ferric carboxymaltose (Ferinject) for the treatment of iron deficiency in patients with heart failure categorized as New York Heart Association functional class II or III to improve exercise capacity. A 2020 recommendation was issued for ferric derisomaltose in patients with iron deficiency anemia who are intolerant to or whose disease is unresponsive to oral iron therapy. Neither of these reimbursement reviews focused specifically on the use of ferric derisomaltose in patients with heart failure and iron deficiency, and they did not focus on the comparative efficacy and safety of ferric derisomaltose versus other IV iron preparations for the treatment of iron deficiency in patients with heart failure. Thus, a review is needed to understand the current evidence base for the use of ferric derisomaltose in this patient population and how ferric derisomaltose compares to ferric carboxymaltose and other IV iron products for the treatment of iron deficiency in patients with heart failure.
Research Questions
What are the clinical efficacy and safety of ferric derisomaltose for adult patients with heart failure and iron deficiency?
What are the evidence-based guidelines regarding the use of ferric derisomaltose for adult patients with heart failure and iron deficiency?
What are the comparative clinical efficacy and safety of ferric derisomaltose compared to ferric carboxymaltose or other IV iron products in adult patients with heart failure and iron deficiency?
Methods
Literature Search Methods
An information specialist conducted a literature search using key resources such as MEDLINE, Embase, the Cochrane Database of Systematic Reviews, the International HTA Database, the websites of health technology assessment agencies in Canada and major international health technology assessment agencies, as well as a focused internet search. The search approach was customized to retrieve a limited set of results, balancing comprehensiveness with relevance. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. Search concepts were developed based on elements of the research questions and selection criteria. The main search concepts were ferric derisomaltose, ferric carboxymaltose, iron sucrose, IV iron, and heart failure. The search was completed on November 20, 2025, and was limited to English-language documents published since January 1, 2020.
Selection Criteria and Methods
The screening occurred in 2 steps; first titles and abstracts were screened, then full text. Two reviewers participated in a pilot exercise using the same 50 abstracts to calibrate and validate the screening process. An agreement level of 100% was achieved. Thereafter, a single reviewer screened the remaining abstracts.
The process was repeated for full-text screening. Two reviewers participated in a pilot exercise using the same 10 full texts. An agreement level of 90% was reached, and discrepancies were resolved through discussion. Thereafter, a single reviewer screened the remaining full texts independently. The final selection of full-text articles was based on the inclusion criteria presented in Table 1. The screening and selection process was managed using Covidence software.
Criteria | Description |
|---|---|
Population | Adult patients with heart failure and iron deficiency |
Intervention | Ferric derisomaltose |
Comparator |
|
Outcomes |
|
Study designs |
|
AE = adverse event; HTA = health technology assessment; RCT = randomized controlled trial; SAE = serious adverse event.
aA guideline is defined as a systematically developed statement or set of statements designed to assist practitioners and patients in making decisions about appropriate health care for specific clinical circumstances. A guideline is considered evidence-based if a systematic search of the literature was undertaken to inform the recommendations.
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1 or if they were published before 2020. Duplicate publications and guidelines with unclear methodology were also excluded.
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the following tools for guidance: the Downs and Black checklist11 for randomized controlled trials (RCTs) and the Appraisal of Guidelines for Research and Evaluation (AGREE) II instrument for guidelines.12 Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Summary of Evidence
Quantity of Research Available
A total of 435 citations were identified in the database literature search and grey literature search. Following the screening of titles and abstracts, 381 citations were excluded and 54 potentially relevant reports from the electronic search were retrieved for full-text review. Of these 54 potentially relevant articles, 52 publications were excluded for various reasons and 2 publications met the inclusion criteria and were included in this report. The included publications were 1 RCT13 and 1 evidence-based guideline.14
Appendix 1 presents the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) flow chart of the study selection.
Summary of Study Characteristics
Appendix 2 provides details regarding the characteristics of included publications.
Included Studies for Research Question 1: What Are the Clinical Efficacy and Safety of Ferric Derisomaltose for Adult Patients With Heart Failure and Iron Deficiency?
Study Design
One RCT13 was included to answer research question 1.
The RCT by Kalra et al. (2022),13 also known as the IRONMAN trial, was a multicentre, prospective, randomized, open-label, blinded end point study. It investigated the efficacy of repeated administration of IV ferric derisomaltose in adults with heart failure with reduced ejection fraction and iron deficiency compared with usual care. The authors defined usual care as guideline indicated therapy. The study was conducted at 70 hospital sites in the UK between August 25, 2016, and October 15, 2021. Patients were randomized in a 1:1 ratio to receive IV ferric derisomaltose or usual care. The study was an investigator-initiated study supported by the British Heart Foundation and by an additional grant from Pharmacosmos, the manufacturer of iron isomaltoside (ferric derisomaltose).
Country of Origin
The IRONMAN trial13 was conducted by authors in the UK.
Patient Population
A total of 1,137 patients with heart failure with reduced ejection fraction (left ventricular ejection fraction ≤ 45%) and iron deficiency (ferritin levels < 100 mcg/L or TSAT levels < 20%) were enrolled in the IRONMAN trial.13 Patients had new or established symptomatic heart failure specified as New York Heart Association functional class II (57%), III (41%), or IV (2%). Approximately 6% of patients were Asian, 2% were Black, 92% were white, and 1% were “other” [wording of original source]. The median age of participants was 73 years (range, 63 years to 79 years). Approximately 26% of patients were female and 74% were male. While most patients (67%) were enrolled from outpatient clinics, approximately 14% of patients were enrolled during a hospital admission for heart failure, and 18% of patients were enrolled following a recent hospital admission for heart failure within the previous 6 months.
Interventions and Comparators
Patients were randomized to receive IV ferric derisomaltose (up to 20 mg/kg total dose replenishment, repeated if ferritin levels were < 100 mcg/L or TSAT levels were < 20% at 4 or 20 months, or if clinically indicated) versus usual care. Patients in both groups received other heart failure therapy according to contemporary guidelines. Patients in the usual care group were permitted to receive oral iron at the investigators’ discretion. Usual care was defined as guideline indicated therapy, and no specific iron therapy or medications that constituted usual care were reported in the study.
Outcomes
The primary outcome of the IRONMAN trial13 was recurrent hospitalization for heart failure or cardiovascular death. Secondary outcomes included hospitalization for worsening heart failure, cardiovascular hospitalization, all-cause hospitalization, cardiovascular mortality, all-cause mortality, 6-minute walk distance (6MWD), and health-related quality of life (HRQoL) assessed at 4 months and 20 months by the Minnesota Living With Heart Failure Questionnaire (MLHFQ) and the EQ-5D instrument.
Brief descriptions of the aforementioned outcome tests and scales are as follows:
The 6-minute walk test is a supervised test that measures the distance a patient can walk back and forth along a 30-metre (100-foot) hard, flat corridor in 6 minutes, with the total distance covered recorded in metres (6MWD).15 The 6-minute walk test is commonly used to evaluate global function of organ systems involved in exercise (i.e., the heart, lungs, peripheral circulation, nervous system, muscles, bones, and joints) during walking, a self-paced activity. The minimal important difference (MID) for improvement in 6MWD was estimated to be 14 m to 15 m in patients with heart failure and iron deficiency.16
The MLHFQ is a patient-reported outcome measure designed to assess the impact of heart failure on an individual’s daily life, including physical, emotional, and social dimensions.17 The MLHFQ has 21 questions and uses a 0 to 5 Likert scale to rate responses. Total scores range from 0 (not affected) to 105 (very much affected). The MID for MLHFQ varies by study, but average changes of 6.0 (range, 3.6 to 9.5), 2.0 (range, 2.0 to 2.5), and 10.0 (range, 7.4 to 13.0) on the physical domain, emotional domain, and total scores, respectively, are considered meaningful improvements for patients with heart failure.18
The EQ-5D assesses HRQoL in 5 dimensions (mobility, pain, self-care, usual activities, and anxiety or depression).19 The newer 5-level version of EQ-5D (EQ-5D-5L) consists of the EQ-5D descriptive system and the EQ visual analogue scale (VAS).20 Each dimension in the descriptive system has 5 levels of severity ranging from 1 (no problems) to 5 (extreme problems). In the EQ VAS, patients are asked to self-rate how good or bad their health is that day by writing down a number from 0 (worst imaginable health) to 100 (best imaginable health) on a 20 cm vertical VAS. Those values are combined to produce a single score (EQ-5D index score) representing a person’s HRQoL on a scale for which 1 is best health possible, 0 is death, and negative values indicate health states the person considers worse than death. There is no single universal MID for EQ-5D, which varies with treatment type and may decrease with increasing baseline scores.21
Included Studies for Research Question 2: What Are the Evidence-Based Guidelines Regarding the Use of Ferric Derisomaltose for Adult Patients With Heart Failure and Iron Deficiency?
Study Design
One evidence-based guideline from the National Institute for Health and Care Excellence (NICE),14 published in 2025, was included to answer research question 2.
The process and methods for developing NICE guidelines can be found in Developing NICE Guidelines: The Manual.22 Details on the evidence review conducted to inform the NICE guideline can be found in the Evidence Review for IV Iron Therapy for Heart Failure.23
Briefly, the committee conducted a systematic review to assess the clinical and cost-effectiveness of IV iron supplementation in adults with chronic heart failure and iron deficiency. The literature search was conducted for RCTs, systematic reviews, network meta-analyses, and individual participant data meta-analyses. The certainty of evidence for each outcome was rated using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) system. The strength of recommendations was not provided.
Country of Origin
The NICE guideline14 was developed in the UK.
Patient Population
The target patient population in the NICE (2025)14 guideline is adults with chronic heart failure with reduced ejection fraction who also have iron deficiency (defined as either serum ferritin levels < 100 mcg/L or serum ferritin levels between 100 mcg/L and 299 mcg/L if TSAT levels are < 20%). The intended users are health care professionals, people with heart failure, and these patients’ families and carers.
Interventions and Practice Considered
The NICE guideline14 was broad in scope and included recommendations for treating chronic heart failure in adults, including the use of specific heart failure medications, IV iron therapy for iron deficiency, and other advice for patients (e.g., related to vaccinations, contraception and pregnancy, alcohol, smoking, and travel). Only the recommendations relevant to IV iron therapy are discussed in this report.
Outcomes
The NICE guideline14 considered exercise tolerance, HRQoL, hospitalization, and cost-effectiveness in developing recommendations.
Included Studies for Research Question 3: What Are the Comparative Clinical Efficacy and Safety of Ferric Derisomaltose Compared to Ferric Carboxymaltose or Other IV Iron Products in Adult Patients With Heart Failure and Iron Deficiency?
We did not identify any studies that evaluated the comparative clinical efficacy and safety of ferric derisomaltose compared to ferric carboxymaltose or other IV iron products in adult patients with heart failure and iron deficiency that met the inclusion criteria for this review.
Summary of Critical Appraisal
Additional details on the critical appraisal of the included RCT13 and evidence-based guideline14 are provided in Appendix 3.
Randomized Controlled Trial
For reporting, the authors of the included RCT13 clearly described the objective of the study, the intervention of interest, the main outcomes, and the main findings of the study. The demographic characteristics of the randomized participants were clearly reported. As such, there is a low risk for potential differences in baseline characteristics between groups. Actual P values and adverse events of the intervention were reported in the RCT.13
In terms of external validity, the patients included in the RCT13 may be representative of the entire eligible population, as they were recruited from multiple centres. Most of the patients (67%) in the RCT13 were ambulatory and were recruited through outpatient clinics. The inclusion of older patients with a mean age older than 70 years and high comorbidity burdens (e.g., chronic kidney disease was common among these patients) appears to be representative of the treatment setting in which most patients would receive heart failure services. As most of the patients included in the trial13 were male, white, and had reduced ejection fraction, the findings of the trial13 may have limited generalizability to patients underrepresented in the study populations or those with preserved ejection fraction. As the RCT13 was conducted in the UK, the findings may be applicable to the Canadian health care setting.
For internal validity related to bias, the RCT13 was registered with ClinicalTrials.gov. As such, the risk of bias in the selection of the reported results was considered to be low. Statistical tests were used appropriately, and the main outcome measures were accurate and reliable. The primary efficacy end points were accurately assessed using appropriate outcome measures.
For internal validity related to confounding, patients in both the intervention and comparator groups appeared to have been recruited from the same population and over the same period of time. Also, methods of randomization and allocation concealment were described. These approaches help ensure comparability and minimize selection bias. Sample size calculation was performed that provided enough statistical power to detect a real effect. The intention-to-treat population was used in the efficacy analysis, and patients who received at least 1 dose of the ferric derisomaltose were included in the safety analysis, which provides the most realistic assessment of a treatment's effectiveness and safety in a real-world setting. However, adjustment for multiplicity in the analysis of secondary outcomes was not performed, which increases the risk of false-positive results (type I errors). Overall, the included RCT13 had certain weaknesses in external validity and internal validity related to confounding, which should be considered during the interpretation of the findings.
Guideline
In the NICE guideline,14 the scope, purpose, intended users, guideline development groups, and target populations were clearly described. The guideline14 reported that the views and preferences of patients were sought. The evidence review conducted to develop the guideline clearly reported comprehensive evidence synthesis methods, including the key research questions, search strategy, and criteria for selection based on the population, intervention, comparison, and outcome of interest (i.e., the PICO framework). The guideline14 was validated through public consultation on the scope and draft guidance, methodological quality assurance, and external review of the evidence review. There were partial links between recommendations and the supporting evidence. GRADE methodology was applied to access the certainty of evidence for IV iron versus placebo or usual care. The guideline authors14 considered health benefits, costs, and risks of side effects in formulating the recommendations. A plan for updating the guideline was indicated in the manual for developing NICE guidelines.22 Recommendations were presented clearly in the guideline14 (i.e., key recommendations were specific, unambiguous, and easy to find, with options for managing the different conditions or health issues). The authors of the guideline14 declared the competing interests of all members of the guideline development group and disclosed that the views of the funding body had no influence on the content of the guideline. Overall, the included guideline14 was robust in terms of scope and purpose, partner involvement, rigour of development, clarity of presentation, and editorial independence.
Summary of Findings
The study findings from all included publications are provided in Appendix 4.
Clinical Efficacy of Ferric Derisomaltose for Adult Patients With Heart Failure and Iron Deficiency
Mortality
There were no statistically significant differences in all-cause death or cardiovascular death between patients who received ferric derisomaltose and those who received usual care.
Hospitalization
There were no statistically significant differences in all-cause hospitalization, cardiovascular hospitalization, or hospitalization due to heart failure between groups.
Cardiovascular Death or Hospitalization
There was a reduction in cardiovascular death or hospitalization for stroke, myocardial infarction, or heart failure in the group receiving ferric derisomaltose compared to the group receiving usual care (RR = 0.83; 95% confidence interval [CI], 0.69 to 1.00; P = 0.045); however, the CI indicates uncertainty and includes the possibility of no effect.
6-Minute Walk Distance
The treatment effect did not show a statistically significant difference between the 2 patient groups for 6MWD at 4 months or at 20 months.
Health-Related Quality of Life
At 4 months, there was an improvement in overall MLHFQ scores in patients receiving ferric derisomaltose compared with patients receiving usual care (least squares mean = −3.33; 95% CI, −6.67 to 0.00; P = 0.05); however, this result is uncertain, as the CI includes the possibility of no true difference. In addition, the change was less than the average MID of 10 points on a total MLHFQ score for a meaningful improvement.
At 4 months, there was an improvement in the physical domain score on the MLHFQ among patients receiving ferric derisomaltose compared with patients receiving usual care (least squares mean = −1.98; 95% CI, −3.42 to −0.54; P = 0.007). However, the change was less than the average MID of 6 points on the physical domain score for a meaningful improvement.
At 20 months, there were no differences between patient groups in the overall score or the physical domain score on the MLHFQ.
No statistically significant difference was observed in EQ-5D scores at 4 months or at 20 months between the 2 patient groups.
Safety of Ferric Derisomaltose for Adult Patients With Heart Failure and Iron Deficiency
The frequency of overall serious adverse events (SAEs) was similar in both groups.
Fewer patients in the group receiving ferric derisomaltose (36%) reported serious adverse cardiac events compared with patients in the group receiving usual care (43%) (between-group difference = −7.00%; 95% CI, −12.69% to −1.32%; P = 0.016).
There were no differences in frequencies of other SAEs between the group receiving ferric derisomaltose and the group receiving usual care.
There were no differences in deaths or hospitalizations due to infection between the group receiving ferric derisomaltose and the group receiving usual care.
Evidence-Based Guideline Regarding the Use of Ferric Derisomaltose
The 2025 NICE guideline14 recommends that clinicians may consider IV iron sucrose, ferric carboxymaltose, or ferric derisomaltose as treatment options for people with heart failure with reduced ejection fraction and hemoglobin levels less than 150 g/L if they have iron deficiency (defined as TSAT levels less than 20% or serum ferritin levels less than 100 mcg/L). The guideline also recommends assessing iron status and checking for anemia with blood tests for TSAT, serum ferritin, and hemoglobin levels to support the recommendation on when to consider IV iron.
The rationale for the recommendation was based on evidence from 12 RCTs, whose meta-analysis findings showed that IV iron supplementation (including iron sucrose, ferric carboxymaltose, or ferric derisomaltose) improved exercise tolerance, improved HRQoL, and reduced hospitalization in the first year for people with heart failure with reduced ejection fraction and iron deficiency. Overall, confidence in the clinical evidence ranged from high to very low. The recommendation was made for the therapeutic drug class of IV iron and is not specific to ferric derisomaltose. The authors of the guideline reported that the strength of the evidence was not sufficient to support a strong recommendation for IV iron supplementation; therefore, they recommended that clinicians consider it.
Limitations
Evidence Gaps
This report is limited by the quantity of research identified that met the inclusion criteria. No studies were identified that evaluated the comparative clinical efficacy and safety of ferric derisomaltose compared to ferric carboxymaltose or other IV iron products in adult patients with heart failure and iron deficiency. The IRONMAN trial did not report on fatigue or iron levels as outcomes, thus no conclusions can be formed on the impact of ferric derisomaltose on these outcomes. The included guideline14 provided recommendations on the use of IV iron therapy (i.e., iron sucrose, ferric carboxymaltose, or ferric derisomaltose) in general, but it did not have specific recommendations on the use of ferric derisomaltose for the treatment of heart failure and iron deficiency.
Generalizability
The IRONMAN trial13 mainly enrolled participants who were white, ambulatory outpatients. As such, the findings may not be generalizable to people who are nonambulatory, inpatients, and other groups of patients. As the NICE guideline was developed in the UK, its recommendations may be applicable to the Canadian context.
Certainty of Evidence
In the IRONMAN trial,13 the magnitude of the effect may have been influenced by 17% of patients in the usual care group having received IV iron infusions (i.e., protocol deviations). The reduced and differential follow-up due to the COVID-19 pandemic may have also biased the estimated treatment effect. There was a risk of assessment bias for subjective outcome measures such as HRQoL and 6MWD, as the study participants and clinicians were aware of treatment interventions. Additionally, there was lack of clarity on the type of treatments given to the usual care group in the study, which limits the interpretation of the results. Therefore, the findings of the IRONMAN trial13 are uncertain due to the aforementioned risk of bias.
Although the included guideline14 was generally methodologically robust, it was not without limitations that could affect the recommendations. The guideline did not specifically focus on the use of ferric derisomaltose but rather developed recommendations for the therapeutic class of iron products, which included other IV iron products such as iron sucrose and ferric carboxymaltose. The evidence that supported the recommendations on IV iron therapy was derived from meta-analysis findings of 12 RCTs, of which only 1 RCT (the IRONMAN trial13) used IV ferric derisomaltose, while most of the RCTs used ferric carboxymaltose. The included RCTs in the guideline were heterogeneous in terms of interventions, comparators, populations, and outcomes. The level of evidence for different outcomes whose estimates were pooled from included RCTs varied from high to very low. The strength of recommendations was not reported, as the authors of the guideline indicated there was insufficient evidence to support a strong recommendation for IV iron supplementation. As such, the recommendation may not be directly applicable to specific iron products such as ferric derisomaltose for adults with heart failure with reduced ejection fraction and iron deficiency.
Conclusions and Implications for Decision- or Policy-Making
This review included 1 RCT13 and 1 evidence-based guideline.14
Clinical Efficacy and Safety of Ferric Derisomaltose for Adult Patients With Heart Failure and Iron Deficiency
The IRONMAN trial13 showed a reduction in the frequency of cardiovascular death or hospitalization for stroke, myocardial infarction, or heart failure in the ferric derisomaltose group compared to the usual care group, but the evidence was uncertain due to imprecision and risk of bias. The trial also showed short-term improvement in HRQoL as assessed by decreases in the total score and the physical domain score of the MLHFQ at 4 months. However, the changes in those scores did not meet the MIDs for a meaningful improvement. In addition, the clinical evidence was insufficient to show a statistically significant difference between patients who received ferric derisomaltose compared with patients in the usual care group for other outcomes such as mortality (all cause or due to cardiovascular events), hospitalization (all cause, due to heart failure, or due to cardiovascular events), exercise capacity, and HRQoL (assessed by MLHFQ at 20 months or by EQ-5D at 4 months and 20 months). Safety outcomes, particularly SAEs, were similar in both groups, except that patients who received ferric derisomaltose reported fewer cardiac SAEs. No evidence was identified on the comparative clinical efficacy or safety of ferric derisomaltose compared to ferric carboxymaltose or other IV iron products in adult patients with heart failure and iron deficiency.
Recommendations From the Included Evidence-Based Guideline
The 2025 NICE guideline14 recommends that clinicians may consider ferric derisomaltose or other iron products such as iron sucrose or ferric carboxymaltose for the treatment of heart failure and iron deficiency. However, the authors of the guideline noted that the strength of the evidence was not sufficient to support a strong recommendation for IV iron supplementation.
Considerations for Future Research
Additional clinical evidence from well-controlled studies is necessary to inform decision-making with respect to the use of ferric derisomaltose for the treatment of adults with heart failure and iron deficiency. Guidelines should be developed or updated to incorporate new evidence on the efficacy and safety of IV ferric derisomaltose for the treatment of heart failure and iron deficiency.
Implications for Clinical Practice
Evidence in this review is insufficient to strongly support the use of IV ferric derisomaltose for the treatment of patients with heart failure with reduced ejection fraction and iron deficiency.
References
1.Rocha BML, Cunha GJL, Menezes Falcão LF. The Burden of Iron Deficiency in Heart Failure: Therapeutic Approach. J Am Coll Cardiol. 2018;71(7):782-793. doi: 10.1016/j.jacc.2017.12.027 Medline
2.Wahid M, Islam S, Sepehrvand N, et al. Iron Deficiency, Anemia, and Iron Supplementation in Patients With Heart Failure: A Population-Level Study. Circ Heart Fail. 2024;17(4):e011351. doi: 10.1161/CIRCHEARTFAILURE.123.011351 Medline
3.McDonagh TA, Metra M, Adamo M, et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J. 2021;42(36):3599-3726. doi: 10.1093/eurheartj/ehab368 Medline
4.Lopez V, Chacon M, Arias MJ, et al. Intravenous Iron Therapy in Patients Admitted With Acute Heart Failure and Iron Deficiency: A Systematic Review and Meta-Analysis. Cureus. 2025;17(7):e88989. doi: 10.7759/cureus.88989 Medline
5.Klip IT, Comin-Colet J, Voors AA, et al. Iron deficiency in chronic heart failure: an international pooled analysis. Am Heart J. 2013;165(4):575-582 e3. doi: 10.1016/j.ahj.2013.01.017 Medline
6.Del Pinto R, Ferri C. Iron deficiency in heart failure: diagnosis and clinical implications. Eur Heart J Suppl. 2022;24(Suppl I):I96-I99. doi: 10.1093/eurheartjsupp/suac080 Medline
7.Messner M, Polzl G, Adlbrecht C, et al. Diagnosis and treatment of iron deficiency in chronic heart failure: Position statement of the heart failure working group of the Austrian Society of Cardiology. Wien Klin Wochenschr. 2025;137(Suppl 3):143-156. doi: 10.1007/s00508-025-02521-x Medline
8.FERINJECT® Ferric Carboxymaltose Injection. 2024. Accessed 08 January. https://pdf.hres.ca/dpd_pm/00074900.PDF
9.MONOFERRIC® Ferric Derisomaltose for Injection. 2021. Accessed 08 January. https://pdf.hres.ca/dpd_pm/00062976.PDF
10.Monoferric (ferric derisomaltose for injection): solution, 100 mg elemental iron/mL (as ferric derisomaltose [also known as iron isomaltoside 1000]), intravenous use [product monograph]. Pfizer Canada. 2025. Accessed December 17, 2025. https://pdf.hres.ca/dpd_pm/00078460.PDF
11.Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377-384. doi: 10.1136/jech.52.6.377 Medline
12.AGREE Next Steps Consortium. The AGREE II Instrument. AGREE Enterprise; 2017. Accessed January 1, 1800. https://www.agreetrust.org/wp-content/uploads/2017/12/AGREE-II-Users-Manual-and-23-item-Instrument-2009-Update-2017.pdf
13.Kalra PR, Cleland JGF, Petrie MC, et al. Intravenous ferric derisomaltose in patients with heart failure and iron deficiency in the UK (IRONMAN): an investigator-initiated, prospective, randomised, open-label, blinded-endpoint trial. Lancet (London, England). 2022;400(10369):2199-2209. doi: 10.1016/S0140-6736(22)02083-9 Medline
14.National Institute for Health and Care Excellence. Chronic heart failure in adults: diagnosis and management. (NICE guideline NG106). 2025. Accessed January 1, 1800. https://www.nice.org.uk/guidance/ng106
15.ATS Committee on Proficiency Standards for Clinical Pulmonary Function Laboratories. ATS statement: guidelines for the six-minute walk test. Am J Respir Crit Care Med. 2002;166:111-117. Medline
16.Khan MS, Anker SD, Friede T, et al. Minimal Clinically Important Differences in 6-Minute Walk Test in Patients With HFrEF and Iron Deficiency. J Card Fail. 2023;29(5):760-770. doi: 10.1016/j.cardfail.2022.10.423 Medline
17.Rector TS, Cohn JN. Assessment of patient outcome with the Minnesota Living with Heart Failure questionnaire: reliability and validity during a randomized, double-blind, placebo-controlled trial of pimobendan. Am Heart J. 1992;124(4):1017-1025. Medline
18.Zhu Y, Cong J, Lin L, et al. Minimum clinically important differences in the Minnesota Living with Heart Failure questionnaire: from a study of heart failure patients treated with integrated Chinese and Western medicine. Front Cardiovasc Med. 2023;10:1242216. doi: 10.3389/fcvm.2023.1242216 Medline
19.The EuroQol Group. EuroQol-a new facility for the measurement of health-related quality of life. Health Policy. 1990;16(3):199-208. Medline
20.EQ-5D-5L User Guide - Basic information on how to use the EQ-5D-5L instrument. 2015. Accessed 05 January. https://www.cric.nu/wp-content/uploads/2018/04/EQ-5D-5L_UserGuide_2015.pdf
21.Cheng LJ, Chen LA, Cheng JY, Herdman M, Luo N. Systematic review reveals that EQ-5D minimally important differences vary with treatment type and may decrease with increasing baseline score. J Clin Epidemiol. 2024;174:111487. doi: 10.1016/j.jclinepi.2024.111487 Medline
22.Developing NICE guidelines: the manual. 2025. Accessed 5 January. https://www.nice.org.uk/process/pmg20/resources/developing-nice-guidelines-the-manual-pdf-72286708700869
23.Chronic heart failure in adults: diagnosis and management [C] Evidence review for IV iron therapy for heart failure. 2025. Accessed 5 January. https://www.ncbi.nlm.nih.gov/books/NBK618734/pdf/Bookshelf_NBK618734.pdf
24.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. doi: 10.1016/j.jclinepi.2009.06.006 Medline
25.Lin DY, Wei LJ, Yang I, et al. Semiparametric regression for the mean and rate functions of recurrent events. J R Stat Soc Ser B Stat Methodol. 2002;62(4):711-730. doi: 10.1111/1467-9868.00259
Appendix 1: Selection of Included Studies
Please note that this appendix has not been copy-edited.
Figure 1: PRISMA Flow Chart of Study Selection
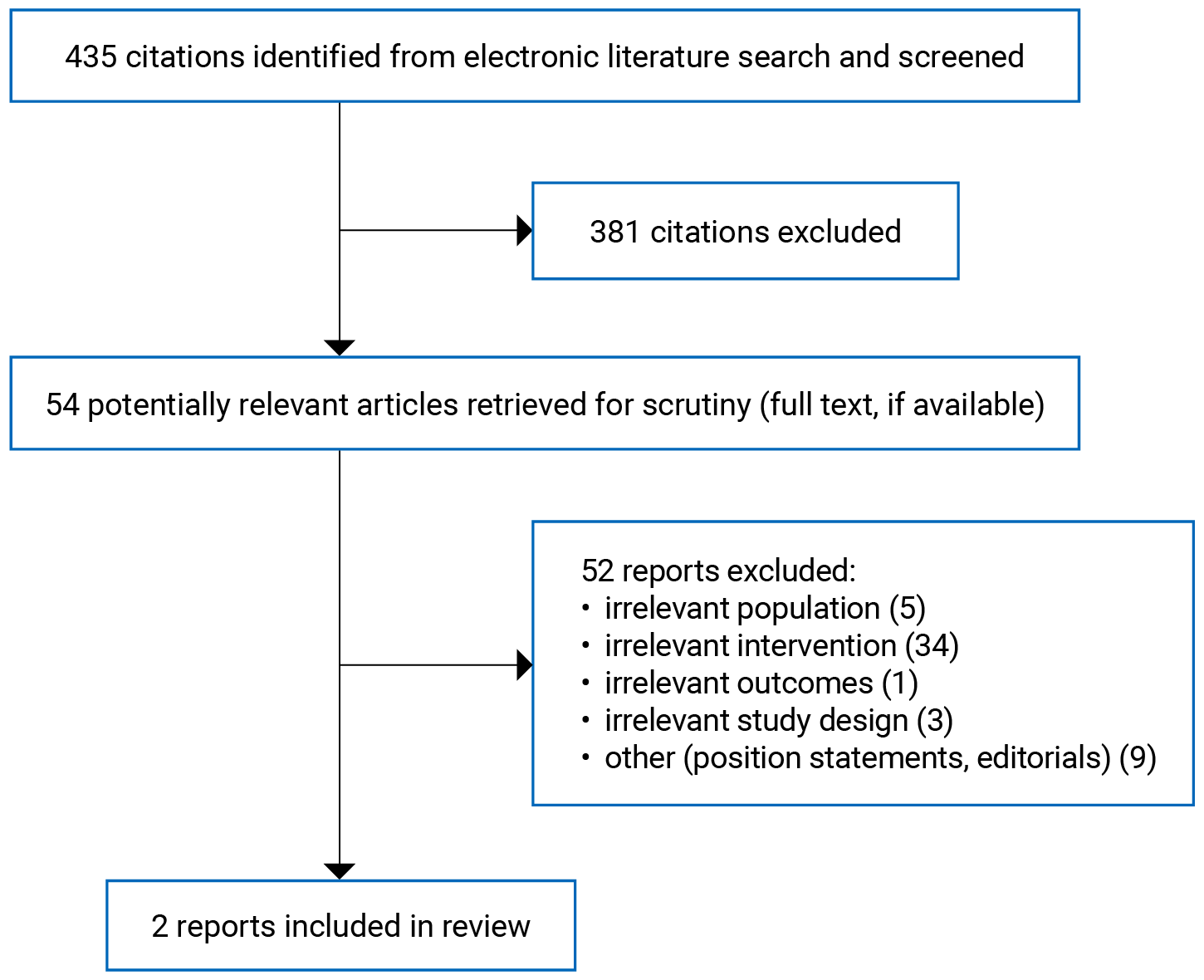
PRISMA = Preferred Reporting Items for Systematic reviews and Meta-Analyses.24
Appendix 2: Characteristics of Included Publications
Please note that this appendix has not been copy-edited.
Table 2: Characteristics of the Included RCT
Study citation, country, funding source | Study design | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Kalra et al. (2022)13 UK Funding sources: British Heart Foundation and Pharmacosmos | Prospective, randomized, open-label, blinded end point RCT | Adult patients with new or established symptomatic heart failure, evidence of iron deficiency (serum ferritin < 100 mcg/L or transferrin saturation < 20%), and a left ventricular ejection fraction of 45% or less within the preceding 24 months N = 1137 Median age: 73 years (IQR, 63 years to 79 years) Sex: Female 26%, male 74% Ethnicity:
| Intervention: Ferric derisomaltose Comparator: Usual care | Primary outcomes:
Secondary outcomes:
Trial duration/follow-up: Median 2.7 years (IQR, 1.8 years to 3.6 years). Maximum of 5.4 years. |
6MWD = 6-minute walk distance; IQR = interquartile range; MLHFQ = Minnesota Living With Heart Failure Questionnaire; RCT = randomized controlled trial.
aWording of original source.
Table 3: Characteristics of the Included Guideline
Intended users, target population | Intervention and practice considered | Major outcomes considered | Evidence collection, selection, and synthesis | Evidence quality assessment | Recommendations development and evaluation | Guideline validation |
|---|---|---|---|---|---|---|
NICE (2025)14 | ||||||
Intended users: Health care professionals, people with HF and their families and carers Target population: Adults with chronic HF |
| Exercise tolerance, quality of life, HF hospitalization, cost-effectiveness | Systematic review to identify and review evidence for 4 key review questions. One review question focused on clinical and cost-effectiveness of IV iron in adults with HF and iron deficiency. The review developed systematic search strategies, predefined eligibility criteria using a PICO framework, and structured data extraction across RCTs and economic evaluations. | The quality of evidence was appraised using GRADE methodology for intervention reviews. | Recommendations were drafted on the basis of the committee’s interpretation of the available evidence, taking account of the balance of benefits, harms, and costs between different courses of action. |
|
ACE = angiotensin-converting enzyme; ARB = angiotensin receptor blocker; ARNI = angiotensin receptor-neprilysin inhibitor; GRADE = Grading of Recommendations Assessment, Development and Evaluation; HF = heart failure; MRA = mineralocorticoid receptor antagonist; NICE = National Institute for Health and Care Excellence; PICO = population, intervention, comparison, outcome; RCT = randomized controlled trial; SGLT2 = sodium-glucose cotransporter-2.
Appendix 3: Critical Appraisal of Included Publications
Please note that this appendix has not been copy-edited.
Table 4: Strengths and Limitations of the RCT Using the Downs and Black Checklist11
Strengths | Limitations |
|---|---|
Kalra et al. (2022)13 | |
|
|
6MWD = 6-minute walk distance; HRQoL = health-related quality of life; RCT = randomized controlled trial; vs. = versus.
Table 5: Strengths and Limitations of the Guideline Using AGREE II12
Item | NICE (2025)14 |
|---|---|
Domain 1: Scope and purpose | |
1. The overall objective(s) of the guideline is (are) specifically described. | Yes |
2. The health question(s) covered by the guideline is (are) specifically described. | Yes |
3. The population (patients, public, etc.) to whom the guideline is meant to apply is specifically described. | Yes |
Domain 2: Stakeholdera involvement | |
4. The guideline development group includes individuals from all relevant professional groups. | Yes |
5. The views and preferences of the target population (patients, public, etc.) have been sought. | Yes |
6. The target users of the guideline are clearly defined. | Yes |
Domain 3: Rigour of development | |
7. Systematic methods were used to search for evidence. | Yes |
8. The criteria for selecting the evidence are clearly described. | Yes |
9. The strengths and limitations of the body of evidence are clearly described. | Yes |
10. The methods for formulating the recommendations are clearly described. | Yes |
11. The health benefits, side effects, and risks have been considered in formulating the recommendations. | Yes |
12. There is an explicit link between the recommendations and the supporting evidence. | Partial |
13. The guideline has been externally reviewed by experts before its publication. | Yes |
14. A procedure for updating the guideline is provided. | Yes |
Domain 4: Clarity of presentation | |
15. The recommendations are specific and unambiguous. | Yes |
16. The different options for management of the condition or health issue are clearly presented. | Yes |
17. Key recommendations are easily identifiable. | Yes |
Domain 5: Applicability | |
18. The guideline describes facilitators and barriers to its application. | Yes |
19. The guideline provides advice and/or tools on how the recommendations can be put into practice. | Yes |
20. The potential resource implications of applying the recommendations have been considered. | Yes |
21. The guideline presents monitoring and/or auditing criteria. | Unclear |
Domain 6: Editorial independence | |
22. The views of the funding body have not influenced the content of the guideline. | Yes |
23. Competing interests of guideline development group members have been recorded and addressed. | Yes |
AGREE II = Appraisal of Guidelines for Research and Evaluation II; NICE = National Institute for Health and Care Excellence.
aWording of original source.
Appendix 4: Main Study Findings
Please note that this appendix has not been copy-edited.
Table 6: Summary of Findings by Outcome — Clinical Efficacy in the IRONMAN Trial13
Outcome | Ferric derisomaltose (N = 569) | Usual care (N = 568) | Effect estimate (95% CI) | P value |
|---|---|---|---|---|
Cardiovascular death and hospitalization | ||||
Cardiovascular death and hospital admission for heart failure, number of events (rate per 100 patient-years) | 336 (22.4) | 411 (27.5) | 0.82 (0.66 to 1.02)a | 0.070 |
Hospitalizations | ||||
Heart failure hospital admission (rate per 100 patient-years) | 250 (16.7) | 313 (20.9) | 0.80 (0.62 to 1.03)a | 0.085 |
Cardiovascular hospital admission, n (%) | 254 (45) | 273 (48) | 0.90 (0.76 to 1.07)b | 0.24 |
All-cause hospital admission, n (%) | 351 (62) | 370 (65) | 0.91 (0.79 to 1.05)b | 0.21 |
Cardiovascular death or heart failure hospitalization | ||||
All-cause mortality, n (%) | 184 (32) | 193 (34) | 0.95 (0.78 to 1.17)b | 0·64 |
Cardiovascular death or hospital admission for heart failure, n (%) | 198 (35) | 231 (41) | 0.84 (0.70 to 1.02)b | 0.081 |
Cardiovascular death or hospital admission for stroke, myocardial infarction, or heart failure, n (%) | 209 (37) | 246 (43) | 0.83 (0.69 to 1.00)b | 0.045 |
All-cause mortality or all-cause unplanned hospital admission, n (%) | 365 (64) | 392 (69) | 0.90 (0.78 to 1.03)b | 0.13 |
6MWDc | ||||
At 4 months, least squares mean (SE) | 286.1 (9.6) | 287.7 (9.6) | –1.6 (–28.2 to 24.9)d,e | 0.90 |
At 20 months, least squares mean (SE) | 252.9 (13.7) | 288.8 (13.9) | –35.9 (–74.4 to 2.64)f | 0.068 |
HRQoL | ||||
Overall score of MLHFQ at 4 months, least squares mean (SE)g | 36.9 (1.2) | 40.2 (1.2) | –3.33 (–6.67 to 0.00)d | 0.050 |
Overall score of MLHFQ at 20 months, least squares mean (SD)g | 40.1 (1.5) | 42.7 (1.5) | –2.57 (–6.72 to 1.59)d | 0.23 |
Physical domain of MLHFQ at 4 months, least squares mean (SE)g | 18.2 (0.5) | 20.2 (0.5) | –1.98 (–3.42 to –0.54)d | 0.0071 |
Physical domain of MLHFQ at 20 months, least squares mean (SE)g | 19.4 (0.6) | 20.6 (0.6) | –1.16 (–2.93 to 0.62)d | 0.20 |
EQ-5D VAS score at 4 months, least squares mean (SE)h | 63.2 (0.9) | 63.0 (1.0) | 0.20 (–2.47 to 2.87)d | 0.88 |
EQ-5D VAS score at 20 months, least squares mean (SE)h | 59.9 (1.3) | 59.4 (1.3) | 0.54 (–2.86 to 3.94)d | 0.75 |
EQ-5D index score at 4 months, least squares mean (SE)h | 0.61 (0.01) | 0.60 (0.01) | 0.01 (–0.02 to 0.04)d | 0.64 |
EQ-5D index score at 20 months, least squares mean (SE)h | 0.57 (0.01) | 0.55 (0.01) | 0.01 (–0.03 to 0.05)d | 0.5 |
6MWD = 6-minute walk distance; CI = confidence interval; HRQoL = health-related quality of life; MLHFQ = Minnesota Living With Heart Failure Questionnaire; SD = standard deviation; SE = standard error; VAS = visual analogue scale.
aRate ratio (estimated using the method of Lin et al.).25
bHazard ratios are estimated from Cox proportional hazards models.
cHigher 6MWD over time indicates improved exercise capacity.
dEstimated mean difference using multiple imputation and Rubin’s rules.
eSample sizes after imputation were based on those able and willing to conduct the test at baseline and who could potentially have carried out the test at 4 months (n = 335 in the ferric derisomaltose group and n = 314 in the usual care group).
fEstimated mean difference based on limited data for 193 patients (n = 98 in the ferric derisomaltose group and n = 95 in the usual care group).
gLower scores on the MLHFQ mean fewer symptoms and improved quality of life.
hFor the EQ-5D index and the EQ VAS, higher values indicate improved health.
Table 7: Summary of Findings by Outcome — Safety in the IRONMAN Trial13
Outcome | Ferric derisomaltose (N = 559) | Usual care (N = 568) | Difference (95% CI) | P value |
|---|---|---|---|---|
SAEs | ||||
All, n (%) | 410 (73) | 435 (77) | –3.24 (–8.30 to 1.82) | 0.21 |
Cardiac, n (%) | 200 (36) | 243 (43) | –7.00 (–12.69 to –1.32) | 0.016 |
Infections and infestations, n (%) | 142 (25) | 162 (29) | –3.12 (–8.30 to 2.06) | 0.24 |
Surgical and medical, n (%) | 80 (14) | 74 (13) | 1.28 (–2.73 to 5.29) | 0.53 |
Gastrointestinal, n (%) | 56 (10) | 64 (11) | –1.25 (–4.85 to 2.35) | 0.50 |
Injury, poisoning, and procedural, n (%) | 59 (11) | 63 (11) | –0.54 (–4.16 to 3.09) | 0.77 |
Respiratory, thoracic, and mediastinal, n (%) | 48 (9) | 67 (12) | –3.21 (–6.74 to 0.32) | 0.074 |
Renal and urinary, n (%) | 55 (10) | 64 (11) | –1.43 (–5.01 to 2.16) | 0.43 |
General and administration site, n (%) | 57 (10) | 52 (9) | 1.04 (–2.41 to 4.49) | 0.55 |
Nervous system, n (%) | 54 (10) | 45 (8) | 1.74 (–1.57 to 5.04) | 0.30 |
Metabolism and nutrition, n (%) | 31 (6) | 49 (9) | –3.08 (–6.07 to –0.09) | 0.043 |
Vascular disorders, n (%) | 34 (6) | 42 (7) | –1.31 (–4.24 to 1.61) | 0.38 |
Neoplasms benign, malignant, and unspecified, n (%) | 22 (4) | 21 (4) | 0.24 (–2.00 to 2.48) | 0.83 |
Musculoskeletal and connective tissue, n (%) | 19 (3) | 25 (4) | –1.00 (–3.26 to 1.26) | 0.38 |
Deaths or hospitalizations due to AEs | ||||
Deaths due to infection, n (%) | 34 (6) | 28 (5) | 1.22 (0.74 to 2.02)a | 0.43 |
Hospitalizations due to infection, n (rate per 100 patient-years) | 175 (11.7) | 213 (14.2) | 0.82 (0.62 to 1.08)b | 0.16 |
AE = adverse event; CI = confidence interval; SAE = serious adverse event.
aHazard ratio estimated using a Cox proportional hazards model.
bRate ratio estimated using a negative binomial regression model.
Table 8: Summary of Recommendations in the Included Guideline
Recommendations and supporting evidence | Quality of evidence and strength of recommendations |
|---|---|
NICE (2025)14 | |
“Consider iron sucrose, ferric carboxymaltose or ferric derisomaltose for people with heart failure with reduced ejection fraction and haemoglobin of less than 150 g per litre if they have iron deficiency defined as:
Supporting evidence: 12 RCTs provided evidence of different IV iron formulations compared to either placebo or usual care. Rationale: Evidence showed IV iron supplementation (including iron sucrose, ferric carboxymaltose, or ferric derisomaltose) improved exercise tolerance and quality of life in the first year for people with HFrEF and iron deficiency. Reduced hospitalization for heart failure was a clinical benefit of IV iron in some trials, though the specific trials were not referenced. | Quality of evidence: High to very lowa Strength of recommendation: NRb |
GRADE = Grading of Recommendations Assessment, Development and Evaluation; HFrEF = heart failure with reduced ejection fraction; NICE = National Institute for Health and Care Excellence; NR = not reported; RCT = randomized controlled trial; TSAT = transferrin saturation.
aThe guideline authors used the GRADE criteria to assess confidence in the evidence for IV iron versus placebo.
bThe guideline authors reported that the strength of the evidence was not sufficient to support strong recommendation for IV iron supplementation; therefore, they recommended that clinicians consider it. However, the authors did not explicitly state the strength of the recommendation.
ISSN: 2563-6596
Canada’s Drug Agency (CDA-AMC) is a pan-Canadian health organization. Created and funded by Canada’s federal, provincial, and territorial governments, we’re responsible for driving better coordination, alignment, and public value within Canada’s drug and health technology landscape. We provide Canada’s health system leaders with independent evidence and advice so they can make informed drug, health technology, and health system decisions, and we collaborate with national and international partners to enhance our collective impact.
Disclaimer: CDA-AMC has taken care to ensure that the information in this document was accurate, complete, and up to date when it was published, but does not make any guarantee to that effect. Your use of this information is subject to this disclaimer and the Terms of Use at cda-amc.ca.
The information in this document is made available for informational and educational purposes only and should not be used as a substitute for professional medical advice, the application of clinical judgment in respect of the care of a particular patient, or other professional judgments in any decision-making process. You assume full responsibility for the use of the information and rely on it at your own risk.
CDA-AMC does not endorse any information, drugs, therapies, treatments, products, processes, or services. The views and opinions of third parties published in this document do not necessarily reflect those of CDA-AMC. The copyright and other intellectual property rights in this document are owned by the Canadian Agency for Drugs and Technologies in Health (operating as CDA-AMC) and its licensors.
Questions or requests for information about this report can be directed to Requests@CDA-AMC.ca.