Drugs, Health Technologies, Health Systems
Health Technology Review
Cryoneurolysis for Patients Undergoing Surgical Stabilization of Rib Fractures
Key Messages
What Is the Issue?
Rib fractures pose a substantial clinical burden in patients with blunt trauma and result in significant pain and morbidity. Pain from rib fractures is often intense and prolonged, frequently lasting for several weeks following the injury. The adoption of surgical stabilization of rib fractures (SSRF) has emerged as a key therapeutic option for patients with severe rib fractures.
Cryoneurolysis is a technology that delivers prolonged analgesia by applying a cryoablation probe at temperatures ranging from −40°C to −70°C for approximately 2 minutes to the intercostal nerves corresponding to the fractured rib levels. Cryoneurolysis has been used as an adjunct to SSRF to improve pain management and other outcomes after surgery.
A comprehensive assessment of the comparative clinical effectiveness and cost-effectiveness of cryoneurolysis as an adjunct to SSRF through a rapid review is essential to examine potential benefits and harms compared with the existing pain management strategies.
What Did We Do?
To inform decisions regarding the use of cryoneurolysis for pain management for people undergoing SSRF, we conducted a rapid review to summarize evidence that compared the clinical effectiveness and cost-effectiveness of cryoneurolysis to alternative pain management interventions not involving cryoneurolysis for people undergoing SSRF.
We searched key resources, including journal citation databases, and conducted a focused internet search for relevant evidence published since 2020.
What Did We Find?
We identified 6 retrospective cohort studies addressing the clinical effectiveness of cryoneurolysis in people undergoing SSRF:
Cryoneurolysis used as an adjunct to SSRF was associated with statistically significantly lower or similar postsurgery patient-reported pain intensity, opioid consumption, resource use, in-hospital complications, and adverse events compared to SSRF without cryoneurolysis or with alternative pain management strategies.
The statistically significant differences between cryoneurolysis and noncryoneurolysis groups were more evident in reduced postsurgery opioid consumption, and intensive care unit (ICU) and postoperative length of stay (LOS).
The certainty of evidence was limited, as all studies had a nonrandomized retrospective design.
We did not find any studies on the relative cost-effectiveness of cryoneurolysis in people undergoing SSRF.
What Does This Mean?
Cryoneurolysis may improve clinical outcomes in people undergoing SSRF by reducing postsurgery opioid consumption and resource use without increasing hospital complications and adverse events.
Widespread implementation should be balanced against current evidence limitations, resource implications, and equity considerations.
Because cryoneurolysis is typically available in specialized centres with established SSRF expertise, there is a risk of uneven access across regions and populations. Mechanisms such as referral pathways, training, or regional planning may be needed to support equitable access.
Abbreviations
EIP
elastomeric infusion pump
ICU
intensive care unit
LOS
length of stay
MME
morphine milliequivalents
MMPR
multimodal pain regimen
NPS
numeric pain score
SSRF
surgical stabilization of rib fractures
Research Questions
What is the clinical effectiveness of cryoneurolysis compared to pain management interventions not involving cryoneurolysis for patients undergoing surgical stabilization of rib fractures?
What is the cost-effectiveness of cryoneurolysis compared to pain management interventions not involving cryoneurolysis for patients undergoing surgical stabilization of rib fractures?
Context and Policy Issues
Pain Management After Rib Fractures
Rib fractures are common among patients with blunt trauma1 and represent a significant subset of thoracic injuries treated in emergency care.2 Rib fractures are a significant source of morbidity and mortality, especially among older adults.3 Pain from rib fractures, particularly with movement and breathing, is often intense and prolonged, frequently lasting for several weeks following the injury.4,5 Inadequate pain management can result in less coughing, retained secretions, and increased bacterial colonization, which consequently elevate the risk of pneumonia.6 In addition, chest wall injuries and rib fractures may lead to long-term consequences, including persistent disability and reduced quality of life, commonly driven by chronic pain and respiratory fatigue.7
Addressing pain in this population remains a critical challenge and includes both surgical and nonsurgical strategies.4,8 Standard nonoperative care worldwide typically consists of analgesia, pulmonary hygiene, and early mobilization.4,6 Although the use of opioids remains a significant pain management strategy, their use has been linked to numerous adverse effects, including nausea, vomiting, respiratory depression, constipation, prolonged hospitalization, opioid tolerance, and substance use disorder.6 In addition, high doses of opioids for patients with rib fractures are associated with increased risks contributing to mortality, as opioids reduce respiratory drive and secretion clearance.8,9 Consequently, there is a need for more effective pain management strategies that reduce dependence on short-term opioid-based therapies while improving pain control and overall patient outcomes.
What Is Surgical Stabilization of Rib Fractures?
Surgical stabilization of rib fractures (SSRF) has emerged as a safe and effective method for treatment of patients with severe rib injuries.10,11 SSRF has been evaluated as an intervention to stabilize rib fractures and support pulmonary function.10,11 Evidence from recent studies suggests that SSRF may be associated with improved pain control and reduced analgesic requirements, as well as shorter hospital and intensive care unit (ICU) length of stay (LOS), fewer days of mechanical ventilation, and a lower likelihood of tracheostomy. Some studies have also reported lower rates of pneumonia incidence and mortality among patients undergoing SSRF.10,11 These observed effects are hypothesized to be related to improved chest wall stability and respiratory mechanics; however, the magnitude and consistency of these associations vary in the year following surgery.12
Pain management after SSRF is typically multimodal, combining regional anesthesia (e.g., epidural, paravertebral, erector spinae plane blocks, or cryoneurolysis), systemic nonopioid and opioid medications, and supportive pulmonary care.10 The primary objectives are to optimize analgesia, support pulmonary function, and minimize opioid-related harms. Management strategies are generally tailored to injury severity, patient comorbidities, and institutional expertise, and often evolve over the postoperative course.
What Is Cryoneurolysis?
Cryoneurolysis — also known as cryoneuroablation, cryoanalgesia, and intercostal nerve cryoablation (INCA) — was first introduced in the 1960s and has since emerged as a strategy for pain management, particularly for pain associated with specific surgeries.13 This technique delivers prolonged analgesia by applying a cryoablation probe to the intercostal nerves corresponding to the fractured rib levels at temperatures of approximately −70°C for about 2 minutes.13
Cryoneurolysis produces a localized and reversible injury to the targeted nerve while preserving the endoneurial, perineurial, and epineurial structures. Thermal neurolytic techniques are intended to interrupt peripheral pain signal transmission to the central nervous system, thereby reducing pain perception.14 Available evidence suggests that nerve conduction is temporarily reduced following treatment, with sensory function typically recovering over several months, commonly reported as occurring within 6 to 12 months.13
Cryoneurolysis has been associated with pain relief without permanent nerve injury and may avoid adverse effects on lower-extremity sensory or motor function.14 Some studies have also reported a lower incidence of complications such as urinary retention, infection, and opioid-related adverse effects.14 The technique has been evaluated in a range of chronic or refractory pain conditions, particularly when a discrete peripheral nerve can be identified as the primary pain source.13,15
Cryoneurolysis for Management of Rib Fracture Pain
Cryoneurolysis for rib fracture pain may be delivered either during SSRF or as a separate procedure after SSRF.16 When performed during SSRF, it is typically done intraoperatively under direct visualization of the nerve, often through an open or thoracoscopic approach, allowing targeted ablation at the time of fixation.16 Cryoneurolysis may be performed after SSRF or independently of surgery for pain management after rib fractures, using a percutaneous, image-guided technique (most commonly ultrasound or CT), enabling treatment of ongoing pain without returning to the operating room.16 The choice of approach varies by institutional protocols, surgical workflow, and clinical context.16
Cryoneurolysis in Canada
In Canada, practice patterns for pain management after rib fractures — including after SSRF — are variable across trauma centres, but generally emphasize multimodal analgesia and individualized care.8
SSRF has historically been concentrated in higher-level trauma centres in Canada.17 In the context of Canada, level I and II trauma centres are typically the sites where advanced interventions (e.g., SSRF, cryoneurolysis, complex regional anesthesia), comprehensive access to trauma surgeons, subspecialty services, and trauma research are provided. Lower-level centres (levels III to IV) generally focus on initial assessment, resuscitation, stabilization, and transferring patients requiring SSRF to level I or II centres.18 Cryoneurolysis in Canada is currently in the early phase of clinical research use and limited to specialized practice for rib fracture pain.19 It has not yet been widely adopted as a standard treatment, with most activity taking place in select academic trauma centres and research settings, rather than as part of routine provincial health care delivery.19
Why Is It Important to Do This Review?
Cryoneurolysis offers prolonged analgesia for people undergoing SSRF.16,20 However, its impact on patient outcomes — such as respiratory complications, LOS, functional limitations, and chronic pain — remains insufficiently established. In addition, this technique requires specialized equipment, training, and operating room resources, raising important questions about value for money within a publicly funded health system.20 There is a need to synthesize evidence from studies evaluating clinical effectiveness and cost-effectiveness of cryoneurolysis, compared with alternative noncryoneurolysis pain management approaches, for people undergoing SSRF. A comprehensive assessment of cryoneurolysis through a rapid review is essential to evaluate potential benefits and harms compared with the existing pain management strategies, while balancing cost-effectiveness, within the health care context in Canada.
In mid-2025, policy decision-makers requested evidence to inform decisions regarding cryoneurolysis. To assess the available literature, Canada’s Drug Agency compiled a preliminary reference list of relevant research, which was used to prioritize 2 rapid reviews: cryoneurolysis for total knee arthroplasty and cryoneurolysis for SSRF.
Objectives
In response to an external request to support decision-making about cryoneurolysis, we prepared this rapid review to summarize and critically appraise available evidence regarding the clinical effectiveness and cost-effectiveness of cryoneurolysis compared to alternative pain management interventions not involving cryoneurolysis for people undergoing SSRF.
Methods
An information specialist conducted a customized literature search, balancing comprehensiveness with relevance, of multiple sources and grey literature on November 10, 2025.
One reviewer screened citations and selected studies based on the inclusion criteria presented in Table 1, and critically appraised the included publications using 1 critical appraisal tool.21 Appendix 1 presents a detailed description of methods and selection criteria for included studies.
Criteria | Description |
|---|---|
Population | Participants (all ages) undergoing surgical stabilization of rib fractures |
Intervention | Cryoneurolysis delivered using any device or system, alone or with background therapy |
Comparator | Alternative pain management interventions not involving cryoneurolysis (e.g., pharmacotherapy, physical therapy, psychological therapy, multimodal pain management strategies), sham cryoneurolysis, or no additional treatment (e.g., pain management protocol per institution) |
Outcomes | Q1: Pain, physical function, self-efficacy, quality of life, hospital length of stay, analgesic use, adverse events Q2: Cost-effectiveness (e.g., cost per quality-adjusted life-year gained) |
Study designs | Q1: HTAs, SRs, RCTs, and nonrandomized studies Q2: HTAs, SRs, and economic evaluations |
Publication date | January 1, 2020, to November 10, 2025 |
HTA = health technology assessment; RCT = randomized controlled trial; SR = systematic review.
Summary of Evidence
Quantity of Research Available
This report includes 6 publications22-27 that met our inclusion criteria, all of which were nonrandomized studies and addressed question 1 (clinical effectiveness). No studies were identified that addressed question 2 (cost-effectiveness). We reported on the characteristics and results from the subset of relevant studies. Appendix 2 presents the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA)28 flow chart of the study selection.
Summary of Study Characteristics
Summaries of study characteristics are organized by research question. Appendix 3 provides details regarding the characteristics of included publications.
Included Studies for Question 1: Clinical Effectiveness of Cryoneurolysis for Patients Undergoing SSRF
We identified 6 clinical studies addressing this question.22-27 All studies were retrospective cohort studies.22-27 Of these, 3 reported data from 1 centre,24,25,27 2 from multiple centres,23,26 and 1 from a national deidentified database.22 All studies were conducted in the US.22-27
Across all studies, populations included adult participants older than 18 years of age undergoing SSRF for rib fractures described as blunt trauma (2 studies),22,23 acute rib fractures (1 study),24 traumatic rib fractures (2 studies),25,27 and traumatic chest wall injury (1 study).26 Comorbidities of other medical disorders were reported in 3 studies,22,25,26 smoking in 3 studies,22,25,27 and substance use disorders in 2 studies.22,27 Two studies excluded participants with histories of opioid dependence.24,26
All included clinical studies22-27 provided information on the age and sex of participants; the authors did not report how sex was defined or measured. One study25 reported on the race of participants. The authors of 2 studies25,27 also provided information on body mass index. None of the included studies22-27 provided participant information for other PROGRESS-Plus criteria,29 such as place of residence, ethnicity, culture, language, occupation, religion, education, socioeconomic status, or social capital.
The study setting was described as level II or higher designated trauma centres located in urban settings in 1 study,23 a level I trauma centre in 2 studies,24,25 level I and III trauma centres in 1 study,26 and a level II trauma centre in 1 study.27 The setting was not reported in 1 study.22
Five23-27 out of 6 studies reported on the professional role of the person who administered cryoneurolysis; 4 studies23,25-27 reported that the cryoneurolysis was conducted by surgeons, and 1 study reported that a single faculty member with trainee surgeons24 administered the cryoneurolysis. All included studies22-27 implemented cryoneurolysis during the SSRF.
Interventions and comparators included:
cryoneurolysis versus standard multimodal pain regimen (MMPR) (1 study)26
cryoneurolysis versus elastomeric infusion pump (EIP) (1 study).27
All 6 studies reported more than 1 outcome on the clinical effectiveness of cryoneurolysis, including:
pain intensity, including patient-reported postsurgery changes as well as pre- and postsurgery changes in numeric pain score (NPS) (4 studies)24-27
analgesic use, including postsurgery changes as well as pre- and postsurgery changes in opioid consumption in oral morphine milliequivalents (MME) (5 studies)23-27
in-hospital complications (4 studies),22,24-26 including:
intubation after surgery (4 studies)24-263
Four studies24-27 reported on outcomes at follow-up after SSRF, which ranged from 30 days to 490 days.
Three studies conducted subgroup analyses on patients with flail chest,22 participants who were not sedated with opioid infusion,26 and patients who were opioid-naive.27
Included Studies for Question 2: Cost-Effectiveness of Cryoneurolysis for Patients Undergoing SSRF
This rapid review did not identify relevant studies that addressed research question 2; therefore, no summary can be provided.
Summary of Critical Appraisal
Appendix 4 provides additional details about the strengths and limitations of the included publications.
Included Studies for Question 1: Clinical Effectiveness of Cryoneurolysis for Patients Undergoing SSRF
The authors of the 6 included studies22-27 provided clear descriptions of study aims, interventions, participant eligibility criteria, and main outcomes. Reporting quality was generally good, with clear descriptions of interventions and clinically relevant outcomes. Additional methodological strengths included the use of valid outcome measures and reporting estimates of random variability (e.g., confidence intervals) and exact P values across all studies.22-27
Several factors affected the internal and external validity of the included studies. All studies22-27 were observational and retrospective, with no randomized or prospective comparative designs, which increases the risk of confounding and selection bias and limits causal inference. Many important patient-centred and safety outcomes were not consistently reported.323 Because of the nature of the intervention (surgeon’s familiarity with the procedure, absence of contraindications), the decision to conduct the cryoneurolysis was left at the discretion of the operating surgeon performing SSRF in 423,25-27 out of 6 studies (1 study22 did not report on the person conducting the surgery). This could have resulted in systematic differences between intervention and comparator groups, potentially introducing bias into the estimates of treatment effects.
Although authors reported some relevant baseline participant characteristics (e.g., age, sex, body mass index), many important characteristics that stratify health opportunities and outcomes were not reported in the included studies, such as race, ethnicity, culture, language, place of residence, socioeconomic status, and other PROGRESS-Plus criteria.29 As a result, it remains unclear whether the study population is representative and whether the findings of these studies conducted in the US can be generalized to settings in Canada. In addition, none of the included studies22-27 included formal power calculations.
Across all studies,22-27 authors reported their potential conflicts of interest related to their work; the authors of 3 studies23,26,27 reported that they had paid affiliations with related medical device companies. Importantly, the authors of 2 studies23,27 were paid to educate faculty by the medical company developing the cryoneurolysis probe used in these studies. This may have influenced the study’s findings. The authors of 4 studies22,25-27 reported receiving no financial support for their studies, whereas sources of funding were not disclosed in 2 studies.23,24
Overall, the studies varied in scope and strength. Smaller single-centre studies24,25,27 contributed valuable information on feasibility, patient-reported pain intensity, opioid consumption, and postsurgery adverse outcomes, but were limited by small sample sizes, limited adjustment for confounders, and restricted generalizability. Larger multicentre and national database studies22,23,26 improved external validity and assessment of system-level outcomes such as ICU LOS and in-hospital complications, although contextual details of interventions in various settings and patient-centred outcomes were often lacking.
Included Studies for Question 2: Cost-Effectiveness of Cryoneurolysis for Patients Undergoing SSRF
This rapid review did not identify relevant studies that addressed research question 2; therefore, no appraisal can be provided.
Summary of Findings
Appendix 5 presents additional details regarding the main study findings.
Question 1: Clinical Effectiveness of Cryoneurolysis for Patients Undergoing SSRF
Evidence regarding the clinical effectiveness of cryoneurolysis versus alternative pain management interventions for patients undergoing SSRF was available from 6 primary clinical studies.22-27
Pain Intensity
Four studies24-27 reported on the patient-reported postsurgery changes25,26 as well as pre- and postsurgery changes24,27 in pain intensity. One study27 showed that receiving cryoneurolysis was associated with a statistically significant reduction in postoperative pain in NPS compared to the EIP group. The other 3 studies24-26 did not show statistically significant differences in NPS for cryoneurolysis versus comparators (noncryoneurolysis24,25 and MMPR26).
Analgesic Use
Five studies23-27 reported on analgesic use, including postsurgery changes23,25,26 as well as pre- and postsurgery changes24,27 in opioid consumption, in oral MME. Two studies indicated a statistically significant reduction in total23,25 and daily25 MME in those receiving cryoneurolysis compared to those not receiving cryoneurolysis after SSRF. One study27 showed that receiving cryoneurolysis was associated with statistically significantly lower inpatient opioid use after SSRF compared to receiving EIP. One study26 comparing cryoneurolysis to MMPR after SSRF indicated statistically significantly lower total and daily MME in the cryoneurolysis group, whereas differences in discharge MME were not statistically significant between groups. One study24 comparing changes in opioid requirements in oral MME, between 12 hours before SSRF and the last 24 admission hours before discharge, did not show statistically significant differences between those receiving cryoneurolysis compared to those not receiving cryoneurolysis after SSRF.
Resource Use
All 6 included studies22-27 reported on total hospital LOS after SSRF. Of these, 2 studies23,26 showed statistically significantly shorter total hospital LOS with cryoneurolysis versus noncryoneurolysis23 and MMPR26 after SSRF.
Three studies reported on postoperative LOS after SSRF.23,24,27 Of these, 2 studies showed statistically significantly shorter postoperative LOS with cryoneurolysis compared to EIP27 and noncryoneurolysis.23 The difference in postoperative LOS in 1 study24 comparing cryoneurolysis to noncryoneurolysis was not statistically significant.
Four studies reported on ICU admission24 or ICU LOS.22,25,26 Three studies indicated that receiving cryoneurolysis after SSRF was associated with statistically significantly shorter ICU LOS compared to noncryoneurolysis24,25 and MMPR.26 The 1 study reporting on rate of ICU admission24 showed no statistically significant differences for cryoneurolysis versus noncryoneurolysis.
One study24 on operation time showed no statistically significant differences between those who received cryoneurolysis and those who did not receive cryoneurolysis for patients undergoing SSRF.
Three studies22,25,26 reported on duration of mechanical ventilation: 1 study26 indicated statistically significantly lower duration of mechanical ventilation in the group that received cryoneurolysis compared to those who received MMPR, whereas the differences in 2 studies comparing cryoneurolysis versus noncryoneurolysis were not statistically significant.
Other than these outcomes, none of the included studies reported on factors or outcomes related to human health resources, such as staff time, workflow impacts, or training and credentialing requirements for cryoneurolysis use.
In-Hospital Complications
Four studies22,24-26 reported on outcomes related to in-hospital complications. Of the 2 studies22,26 that reported on overall in-hospital complications, 1 study22 showed statistically significantly fewer complications in the cryoneurolysis group than in the noncryoneurolysis group, whereas the other study26 did not report statistically significant differences between the cryoneurolysis and MMPR groups.
Out of the 3 studies22,24,25 reporting on the incidence of pneumonia in those receiving cryoneurolysis versus those not receiving cryoneurolysis after SSRF, 1 study22 showed statistically significantly lower rates of ventilator-associated pneumonia in the cryoneurolysis group compared to the noncryoneurolysis group. The group differences in the other 2 studies24,25 were not statistically significant.
Three studies reported on tracheostomy rates in groups receiving cryoneurolysis versus noncryoneurolysis24,25 and MMPR.26 Of these, 1 study25 showed statistically significantly lower rates of tracheostomy in the cryoneurolysis group than in the noncryoneurolysis group.
Of the 2 studies22,26 reporting on return to the operating room after SSRF, neither showed a statistically significant difference with cryoneurolysis versus comparators (i.e., noncryoneurolysis22 or MMPR26).
Three studies22,26,27 reported on pulmonary complications after SSRF. One study22 indicated statistically significantly fewer pulmonary complications with cryoneurolysis versus noncryoneurolysis; however, the differences between cryoneurolysis and MMPR26 or EIP27 were not statistically significant in 2 studies.
Four studies22,24-26 reported on intubation after surgery. Two studies showed that a statistically significantly lower percentage of patients who received cryoneurolysis were intubated compared with those in the noncryoneurolysis25 or MMPR groups.26 The differences in 2 studies22,24 comparing cryoneurolysis to noncryoneurolysis were not statistically significant.
Two studies22,26 reported on other in-hospital complications after SSRF. In 1 study26 reporting on unplanned reintubation, hardware removal, chest tube reinsertion, COVID+ [as reported by the study authors], and postoperative nerve block, authors did not find any statistically significant differences between those who received cryoneurolysis versus MMPR after surgery. The other study22 reported on cerebrovascular accidents, extremity compartment syndrome, delirium, acute respiratory distress syndrome, myocardial infarction, cardiac arrest, acute kidney injury, deep vein thrombosis, sepsis, and various infections (superficial, deep, and organ space surgical site infection, central line-associated bloodstream infection, and catheter-associated urinary tract infection). Participants who received cryoneurolysis showed a statistically significant reduction in extremity compartment syndrome and cerebrovascular accident events compared to those in the noncryoneurolysis group.22 Other group differences were not statistically significant in this study.22
Postdischarge Adverse Events
Four studies24-27 reported on short-term and long-term adverse events after SSRF, which ranged from 30 days to 490 days.
No statistically significant group differences were shown in 2 studies26,27 reporting on post-discharge adverse events, including 30-day readmission and incidence of chest wall neuralgia at a 1-year follow-up.
One study24 that reviewed long-term adverse events, to assess long-term safety, reported that patients who underwent SSRF with cryoneurolysis did not experience any functional limitations or other complications of cryoneurolysis, except for 1 patient (6%) who reported mild lateral chest wall paresthesia at a 6-month follow-up. Of those who did not receive cryoneurolysis, 1 patient reported difficulty sleeping due to chest wall pain at a 1-month follow-up. No statistical comparison was reported between groups for these adverse events. Authors did not find statistically significant differences in the proportion of patients requiring opioids or other pain medications at a follow-up of 2 weeks after discharge.24
One study25 reported on short-term (0 to 3 months) and long-term (3 to 6 months) follow-up of patients who received cryoneurolysis versus noncryoneurolysis after SSRF. The authors reported that short-term adverse events occurred in 86.3% of the patients receiving cryoneurolysis and 87.5% of patients in the noncryoneurolysis group. No statistical comparison was reported between groups for these adverse events.25
Other Outcomes
All 6 included studies22-27 reported on other outcomes. Of the 2 studies24,25 that reported on discharge disposition, 1 study25 found that those who received cryoneurolysis versus noncryoneurolysis after SSRF had a statistically significantly higher likelihood of being discharged to their home. The group differences in the other study24 reporting on the percentage of people being discharged to home, long-term care hospitals, or skilled nursing and other facilities were not statistically significant.
Four studies22,24-26 reported on mortality rate between those received cryoneurolysis versus noncryoneurolysis22,24,25 or cryoneurolysis versus MMPR.26 None of the group differences related to these outcomes were statistically significant.
Two studies23,27 reported on hospital charges. One study23 indicated statistically significantly lower postoperative hospital charges, and charges related to the day of surgery among those receiving cryoneurolysis versus the noncryoneurolysis group, despite similar total hospital charges. The other study27 observed lower mean hospital costs in the cryoneurolysis group compared to the EIP group; however, this difference did not reach statistical significance.
Subgroup Analyses
Three studies22,26,27 conducted subgroup analyses related to data from their research participants.
One study22 performed a subgroup analysis of patients with flail chest. The decreased ICU LOS in the cryoneurolysis versus noncryoneurolysis groups remained a statistically significant outcome in the flail chest subset.
One study26 conducted analyses excluding participants who were sedated with opioid infusion. Total MME, hospital LOS, and ICU LOS remained statistically significant in both univariate and multivariable analyses.26
The third study evaluated opioid dependence at 1 year following surgery for patients who were opioid-naive.27 At discharge, patients who were opioid-naive and received cryoneurolysis were prescribed a statistically significantly lower median opioid dose than those who received EIP.
Question 2: Cost-Effectiveness of Cryoneurolysis for Patients Undergoing SSRF
We found no relevant evidence regarding the cost-effectiveness of cryoneurolysis for patients undergoing SSRF; therefore, no summary can be provided.
Limitations
Evidence Gaps
Despite a growing number of studies evaluating cryoneurolysis during SSRF, important gaps remain in the evidence base. No randomized controlled trials or well-designed prospective comparative studies were identified, limiting the ability to draw firm conclusions about comparative clinical effectiveness. Evidence is particularly limited for head-to-head comparisons with established analgesic modalities, such as thoracic epidural analgesia or paravertebral blocks.8
Several clinically relevant outcomes were either inconsistently reported or not reported, including long-term pain intensity, functional recovery, quality of life, return to work, and patient satisfaction.22,23 Evidence is also lacking for many populations of interest, such as older adults with frailty, individuals with multiple comorbidities, and those with chronic pain or opioid use disorder, for whom analgesic strategies may have different risk and benefit profiles. An additional evidence gap is the lack of evidence on the effectiveness and other considerations for postoperative cryoneurolysis, as all included studies22-27 applied cryoneurolysis intraoperatively during SSRF, leaving its impact when delivered after surgery unknown. Another limitation of the literature is the absence of data on human health resource implications of cryoneurolysis, as included studies did not assess staff time, workflow impacts, or training and credentialing requirements, limiting understanding of its feasibility and scalability in routine clinical practice.
Evidence on long-term outcomes remains sparse. Although cryoneurolysis is intended to provide analgesia for several months, few studies reported on long-term outcomes, such as postdischarge opioid use or pneumonia beyond the index hospitalization.22-27 In addition, the available follow-up data were limited in duration, incomplete, and not systematic. Two single-centre studies24,27 that included limited postdischarge follow-up data did not identify persistent neuropathic pain or long-term complications. However, these findings were based on small samples and were not powered to detect uncommon or delayed adverse events.
Large database studies22 and multicentre cohorts23,26 did not capture outcomes related to long-term pain, opioid use, pulmonary complications, functional recovery, or quality of life. As a result, substantial uncertainty remains regarding the durability of analgesic benefit and long-term safety, highlighting an important gap in the evidence base.
The overall quantity of evidence is limited to a small number of observational studies conducted in a narrow range of settings. While findings are directionally consistent, the limited number of studies and their overlapping designs reduce confidence in the robustness of conclusions. The conclusions from findings rely heavily on outcomes such as opioid consumption and LOS rather than patient-reported outcomes. As a result, there is limited certainty regarding the strength of conclusions that can be drawn about the magnitude of benefit associated with cryoneurolysis for SSRF.
This rapid review did not identify any relevant evidence regarding the cost-effectiveness of cryoneurolysis in people undergoing SSRF. This limits the ability to evaluate their economic value. Without evidence on costs relative to health and/or social outcomes, policy-makers may face challenges in how to allocate scarce resources and how to prioritize cryoneurolysis implementation over other alternative pain management after SSRF.
Generalizability
Generalizability of findings is constrained by the clinical and institutional contexts in which the studies were conducted. Most studies were performed in high-volume trauma centres with established SSRF programs and access to specialized surgical and anesthetic expertise.23-25,27 Patients included in these studies often had injury patterns and clinical trajectories that may not reflect those seen in smaller or rural hospitals.22,23 The lack of standardization across centres regarding both the number of nerves cryoablated and the ablation technique limits comparability across studies.22,23,26 It remains unclear whether similar outcomes would be achieved in settings without comparable resources, experience, or multidisciplinary pain management infrastructure.
Applicability to Clinical Practice in Health Care Context in Canada
The applicability of the findings to clinical practice in Canada is uncertain, as none of the included studies were conducted in Canada. Differences in trauma system organization, access to SSRF, availability of cryoneurolysis technology, and postoperative pain management pathways may influence both feasibility and effectiveness in the context of Canada. System-level considerations in publicly funded care — such as operating room time, staffing, and costs — are particularly relevant, and without evidence from hospitals in Canada, findings should be interpreted cautiously.
Equity Considerations
Equity considerations are largely absent from the current literature. None of the studies reported outcomes stratified by sex, gender, race, ethnicity, socioeconomic status, or rurality, nor did they address barriers to accessing SSRF or cryoneurolysis. This limits understanding of whether the benefits of cryoneurolysis are equitably distributed or whether certain groups may face disproportionate barriers to access. Additionally, because cryoneurolysis is typically available in specialized centres,23-25,27 there are concerns that its adoption could exacerbate existing disparities in trauma care, particularly for patients living in rural or remote communities and those with limited access to tertiary trauma services. The absence of patient engagement data further limits insight into patient-valued outcomes and equity-related impacts.
Conclusions and Implications for Decision- or Policy-Making
This rapid review evaluated the literature regarding the clinical effectiveness and cost-effectiveness of cryoneurolysis compared with alternative noncryoneurolysis pain management interventions for people undergoing SSRF. We identified 6 retrospective cohort studies22-27 addressing clinical effectiveness and no studies evaluating the cost-effectiveness of cryoneurolysis.
Summary of Evidence
Results from the 6 included studies22-27 suggest that cryoneurolysis used during SSRF is generally associated with improved postoperative pain-related outcomes compared with SSRF without cryoneurolysis or with alternative pain management strategies (i.e., MMPR26 or EIP27). Benefits were most consistently observed for reduced opioid consumption, lower pain scores, and shorter postoperative and ICU LOS, with no evidence of increased complications. Subgroup analyses across 3 studies showed that cryoneurolysis was associated with shorter ICU or hospital LOS and reduced opioid use.22,26,27 Among patients who were opioid-naive, cryoneurolysis was linked to lower opioid prescribing at discharge and no reported long-term opioid use at 1 year.27
Earlier research24 established the technical feasibility and short-term safety of cryoneurolysis used during SSRF, whereas subsequent single-centre and multicentre cohort studies demonstrated consistent reductions in opioid consumption, as well as shorter postoperative or ICU LOS compared with SSRF without cryoneurolysis23,25 or with other analgesic strategies.26,27 Importantly, the national database analysis22 extended these findings to a system level, suggesting that improved analgesia may result in fewer serious in-hospital complications and reduced ICU utilization.
Although causality cannot be established, the convergence of findings across diverse settings and outcomes strengthens confidence that cryoneurolysis may provide incremental clinical benefit within SSRF pathways. However, limitations in the evidence base highlight the need for randomized and longitudinal research.
Despite the review’s intention to assess economic evidence, no studies evaluating cost-effectiveness were identified. However, all included studies provided direct23,27 and indirect22-27 information on cost and resource use about the economic implications of cryoneurolysis used during SSRF. Across studies that reported financial outcomes, cryoneurolysis was not associated with higher overall hospital costs27 and, in some cases, was linked to lower postoperative charges23 and resource use.22,23,27 Importantly, no study reported increased LOS or complication-related costs attributable to cryoneurolysis.
Overall, while the available evidence suggests cryoneurolysis is unlikely to increase costs and may be cost-neutral or cost-saving in some settings, economic conclusions remain uncertain. There is a need for robust cost-effectiveness analyses incorporating procedural costs, human health resource implications, downstream resource use, and longer-term outcomes.
Considerations for Future Research
Future research should focus on generating comparative evidence to clarify the independent effectiveness of cryoneurolysis during SSRF. Prospective and, where feasible, randomized controlled trials comparing cryoneurolysis with established analgesic strategies are needed to reduce uncertainty and better define its role within multimodal pain management pathways.
Research should also prioritize patient-reported and longer-term outcomes, including functional recovery, chronic pain, and sustained opioid use, while improving representation across care settings and equity-deserving populations. Finally, integrating robust economic evaluations into future studies is essential to determine the value of cryoneurolysis within publicly funded health care systems.
Considerations for Clinical Practice or Considerations for Decision- or Policy-Making
Cryoneurolysis may offer meaningful benefits in postoperative pain management, particularly through opioid-sparing effects and potential reductions in postoperative and ICU LOS. These benefits appear to be achieved without an observed increase in complications, which supports the consideration of cryoneurolysis as an adjunct within specialized SSRF programs. However, decisions about adoption should be made in the context of limited certainty, as the evidence is derived entirely from observational studies conducted in a limited number of high-volume trauma centres. Cryoneurolysis should therefore be viewed as a potentially beneficial option for pain management; however, its use may be most appropriate in centres with established SSRF expertise, multidisciplinary pain management teams, and the technical capacity to perform the procedure safely.
In addition, the generalizability of findings to the context of Canada and its health care systems is limited, as none of the included studies were conducted in Canada. The absence of robust cost-effectiveness evidence warrants a cautious and context-sensitive approach. While available data suggest that cryoneurolysis is unlikely to increase overall hospital costs and may reduce downstream resource use, these findings are indirect and dependent on the setting and country. Phased or selective implementation approaches, along with the systematic collection of data on clinical outcomes, resource use, and patient-reported experiences, could help inform future decision-making.
Because cryoneurolysis is typically available in specialized or high-level trauma centres with established SSRF programs, experienced surgical teams, and advanced pain management infrastructure, findings may not be directly generalizable to lower-level trauma centres where SSRF is less common and access to cryoneurolysis expertise and resources may be limited. As a result, there is a risk of uneven access across regions and populations.13 Targeted strategies, such as referral pathways, training, or regional planning, may be required to support equitable access.
Overall, cryoneurolysis may be considered a beneficial adjunct for pain management for individuals undergoing SSRF within appropriate clinical contexts; however, broader implementation should be balanced against current evidence limitations, resource implications, and equity considerations, with ongoing evaluations to reduce uncertainty over time.
References
1.Mayberry JC, Trunkey DD. The fractured rib in chest wall trauma. Chest Surg Clin N Am. 1997;7(2):239-61. PubMed
2.Racine S, Émond M, Audette-Côté JS, et al. Delayed complications and functional outcome of isolated sternal fracture after emergency department discharge: a prospective, multicentre cohort study. CJEM. 2016;18(5):349-57. doi:10.1017/cem.2016.326 PubMed
3.Bergeron E, Lavoie A, Clas D, et al. Elderly trauma patients with rib fractures are at greater risk of death and pneumonia. J Trauma. 2003;54(3):478-85. doi:10.1097/01.Ta.0000037095.83469.4c PubMed
4.Stopenski S, Binkley J, Schubl SD, Bauman ZM. Rib fracture management: A review of surgical stabilization, regional analgesia, and intercostal nerve cryoablation. Surg Pract Sci. 2022;10:100089. doi:10.1016/j.sipas.2022.100089 PubMed
5.Fabricant L, Ham B, Mullins R, Mayberry J. Prolonged pain and disability are common after rib fractures. Am J Surg. 2013;205(5):511-5. doi:10.1016/j.amjsurg.2012.12.007 PubMed
6.Hammal F, Chiu C, Kung JY, Bradley N, Dillane D. Pain management for hospitalized patients with rib fractures: A systematic review of randomized clinical trials. J Clin Anesth. Feb 2024;92:111276. doi:10.1016/j.jclinane.2023.111276 PubMed
7.Marasco S, Lee G, Summerhayes R, Fitzgerald M, Bailey M. Quality of life after major trauma with multiple rib fractures. Injury. 2015;46(1):61-5. doi:10.1016/j.injury.2014.06.014 PubMed
8.Yu S, Patton P, Vogt K, et al. Examining Canadian trauma centres' analgesic protocols for rib fractures. West J Emerg Med. 2025;26(5):1367-73. doi:10.5811/westjem.24945 PubMed
9.Karmakar MK, Ho AM. Acute pain management of patients with multiple fractured ribs. J Trauma. Mar 2003;54(3):615-25. doi:10.1097/01.Ta.0000053197.40145.62 PubMed
10.Fokin AA, Hus N, Wycech J, Rodriguez E, Puente I. Surgical stabilization of rib fractures: indications, techniques, and pitfalls. JBJS Essent Surg Tech. 2020;10(2):e0032. doi:10.2106/jbjs.St.19.00032 PubMed
11.Shaban Y, Frank M, Schubl S, et al. The History of surgical stabilization of rib fractures (SSRF). Surg Pract Sci. 2022;10:100084. doi:10.1016/j.sipas.2022.100084 PubMed
12.Caragounis EC, Fagevik Olsén M, Pazooki D, Granhed H. Surgical treatment of multiple rib fractures and flail chest in trauma: a one-year follow-up study. World J Emerg Surg. 2016;11:27. doi:10.1186/s13017-016-0085-2 PubMed
13.Law L, Rayi A, Hendrix JM, Derian A. Cryoanalgesia. StatPearls Publishing LLC. Accessed December 22, 2025, https://www.ncbi.nlm.nih.gov/books/NBK482123/
14.Biel E, Aroke EN, Maye J, Zhang SJ. The applications of cryoneurolysis for acute and chronic pain management. Pain Pract. 2023;23(2):204-215. doi:10.1111/papr.13182 PubMed
15.Huang J, Delijani K, El Khudari H, Gunn AJ. Intercostal cryoneurolysis. Semin Intervent Radiol. 2022;39(2):167-171. doi:10.1055/s-0042-1745763 PubMed
16.Muldiiarov V, Bauman ZM. Role of intercostal nerve block and cryoneurolysis in the management of rib fractures: a narrative review. Current Challenges in Thoracic Surgery. 2025;7
17.Kane ED, Jeremitsky E, Pieracci FM, Majercik S, Doben AR. Quantifying and exploring the recent national increase in surgical stabilization of rib fractures. J Trauma Acute Care Surg. 2017;83(6):1047-1052. doi:10.1097/ta.0000000000001648 PubMed
18.Caminsky NG, Wong EG. Trauma systems in Canada: striving for quality across an expansive landmass. Emergency and Critical Care Medicine. 2023;3(3):89-93. doi:10.1097/ec9.0000000000000102
19.Jew MK, Evtushevski B, Liang J, Wang KH. Ultrasound-guided, percutaneous cryoneurolysis of intercostal nerves in high-risk, traumatic rib fracture patients. Reg Anesth Pain Med. 2025;05:05. doi:10.1136/rapm-2025-106973
20.Cha PI, Min JG, Patil A, Choi J, Kothary NN, Forrester JD. Efficacy of intercostal cryoneurolysis as an analgesic adjunct for chest wall pain after surgery or trauma: Systematic review. Review. Trauma Surgery and Acute Care Open. 2021;6(1)e000690. doi:10.1136/tsaco-2021-000690 PubMed
21.Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377-384. doi:10.1136/jech.52.6.377 PubMed
22.Aryan N, Nahmias J, Grigorian A, et al. Inpatient outcomes of intercostal nerve cryoablation with surgical rib fixation. Journal of Surgical Research. 2024;303:105-110. doi:10.1016/j.jss.2024.08.022 PubMed
23.Bauman ZM, Loftus J, Raposo-Hadley A, et al. Surgical stabilization of rib fractures combined with intercostal nerve cryoablation proves to be more cost effective by reducing hospital length of stay and narcotics. Injury. 2021;52(5):1128-1132. doi:10.1016/j.injury.2021.02.009 PubMed
24.Choi J, Min JG, Jopling JK, Meshkin S, Bessoff KE, Forrester JD. Intercostal nerve cryoablation during surgical stabilization of rib fractures. Conference Paper. Journal of Trauma and Acute Care Surgery. 2021;91(6):976-980. doi:10.1097/ta.0000000000003391 PubMed
25.Fernandez CA, Narveson JR, Niu F, et al. In-hospital outcomes of intercostal nerve cryoablation and surgical stabilization of rib fractures. Journal of Trauma and Acute Care Surgery. 2022;93(5):695-701. doi:10.1097/ta.0000000000003623 PubMed
26.Marturano MN, Thakkar V, Wang H, et al. Intercostal nerve cryoablation during surgical stabilization of rib fractures decreases post-operative opioid use, ventilation days, and intensive care days. Injury. 2023;54(9)110803. doi:10.1016/j.injury.2023.05.034 PubMed
27.O'Connor LA, Houseman B, Cook T, Quinn CC. Intercostal cryonerve block versus elastomeric infusion pump for postoperative analgesia following surgical stabilization of traumatic rib fractures. Injury. 2023;54(11) 111053. doi:10.1016/j.injury.2023.111053 PubMed
28.Page MJ, Moher D, Bossuyt PM, et al. PRISMA 2020 explanation and elaboration: updated guidance and exemplars for reporting systematic reviews. BMJ. 2021;372:n160. doi:10.1136/bmj.n160 PubMed
29.O'Neill J, Tabish H, Welch V, et al. Applying an equity lens to interventions: using PROGRESS ensures consideration of socially stratifying factors to illuminate inequities in health. J Clin Epidemiol. 2014;67(1):56-64. doi:10.1016/j.jclinepi.2013.08.005 PubMed
30.Canada’s Drug Agency. Canada's Drug Agency Style: A Guide for Authors and Editors. 2025. Accessed December 22, 2025. https://www.cda-amc.ca/sites/default/files/pdf/style_guide_2025_digital.pdf
Appendix 1: Detailed Methods and Selection of Included Studies
Please note that this appendix has not been copy-edited.
What Is a Rapid Review?
Rapid reviews are based on accelerated and abbreviated systematic review methods, balancing timeliness with rigour, to allow for timely decision-making. Due to these abbreviated methods, rapid reviews have some limitations. For example, following full-text review, the research questions and eligibility criteria were refined to align with project timelines and to focus the rapid review on SSRF, the priority area identified by the customer. This decision was informed by the review’s initial aim to examine chest wall surgery more broadly, with SSRF identified as the highest-priority topic for the customer. In addition, unlike in systematic reviews, for which at least 2 independent reviewers are needed to screen studies to reduce selection bias, a single reviewer was required to include, extract the data, and appraise a study. Similarly, we included studies published from 2020, excluding older studies. Albeit, focusing on more recently published articles may be more reflective of current practices. Our rapid review intends to summarize the available evidence, rather than provide recommendations. These findings should not be interpreted as prescriptive guidance.
Literature Search Methods
An information specialist conducted a literature search on key resources including MEDLINE, the Cochrane Database of Systematic Reviews, the International HTA Database, the websites of health technology assessment (HTA) agencies in Canada and major international HTA agencies, as well as a focused internet search. The search approach was customized to retrieve a limited set of results, balancing comprehensiveness with relevance. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. Search concepts were developed based on the elements of the research questions and selection criteria. The main search concepts were cryoneurolysis and chest surgery. Search filters were applied to limit retrieval to health technology assessments, systematic reviews, meta-analyses, or indirect treatment comparisons, randomized controlled trials, controlled clinical trials, or any other type of clinical trial, observational studies, economic studies, and citations related to health utilities or quality of life. Conference reviews, conference abstracts, and clinicaltrials.gov records were excluded. Retrieval was limited to the human population. The search was completed on November 10, 2025, and limited to English-language documents published since January 1, 2020. The search strategy is available on request.
Selection Criteria and Methods
One reviewer screened citations and selected studies examining the clinical effectiveness and cost-effectiveness of cryoneurolysis for patients undergoing chest wall surgery. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. Following full-text review, the scope of the review was further refined to focus on SSRF, reflecting a modification of the original research questions and inclusion criteria to align with project timelines and the priority area. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Exclusion Criteria
Articles were excluded if they:
did not meet the selection criteria outlined in Table 1
were focused on using cryoneurolysis for chest surgeries other than SSRF
were duplicate publications or were published before 2020
were of any design published only as abstracts, conference proceedings, presentations, thesis documents, or preprints
were single-arm before-and-after studies, case studies, and case reports
were published in languages other than English (for feasibility reasons).
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the Downs and Black checklist21 for randomized and nonrandomized studies as a guide. Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Data Extraction
One reviewer extracted data directly into standardized tables created in Microsoft Word, which were modified as necessary. The extracted information included study characteristics, methodology (e.g., study design), population, intervention, comparator, and results regarding the outcomes of interest.
One reviewer extracted information from the included studies using the PROGRESS-Plus29 tool to describe different population groups. Each included study was checked to determine if PROGRESS-Plus29 criteria were reported by study authors to describe the participants; detailed characteristics, if available, were then extracted and reported in tables in Appendix 2. The main PROGRESS-Plus29 criteria include place of residence; race, ethnicity, culture, and/or language; occupation; gender and/or sex; religion; education; socioeconomic status; and social capital. As part of report writing, we discuss these characteristics across the evidence, where available, when presenting results within the text.
When reporting on sex, gender, race, or ethnicity in this rapid review, we planned to retain the language used by the original study authors, and, whenever possible, we referred to these groups based on guidance from Canada’s Drug Agency Style: A Guide for Authors and Editors30 at the time this rapid review was conducted, with an understanding that language is constantly evolving.
Appendix 2: Selection of Included Studies
Please note that this appendix has not been copy-edited.
Figure 1: Selection of Included Studies — PRISMA28 Flow Chart of Selected Reports
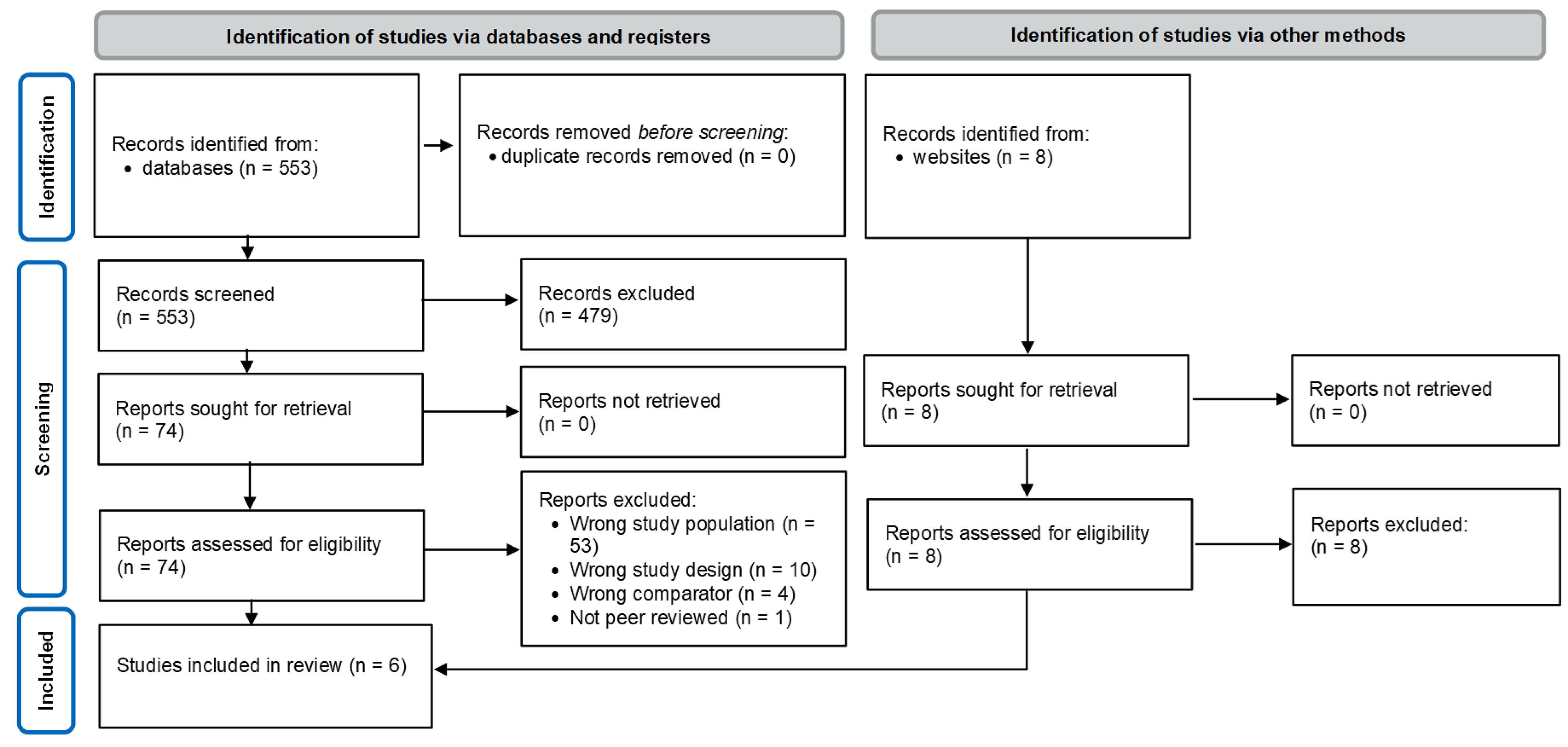
PRISMA = Preferred Reporting Items for Systematic reviews and Meta-Analyses.
Appendix 3: Characteristics of Included Publications
Please note that this appendix has not been copy-edited.
Table 2: Characteristics of Included Primary Clinical Studies
Study citation, country, funding source | Study design and period | Population characteristics and setting | Injury profile | Operation characteristics | Intervention, manufacturer, and comparator(s) | Clinical outcomes, length of follow-up, subgroup analysis |
|---|---|---|---|---|---|---|
Aryan et al. (2024)22 US Funding source: None | Retrospective cohort Trauma Quality Improvement Program database (a national deidentified database) from 2017 to 2021 | Participants: 15,784 participants ≥ 18 years old with blunt trauma undergoing SSRF. Of these, 750 (4.8%) received cryoneurolysis. Diagnosis: blunt trauma Comorbiditiesa:
Age, median (IQR)a: 59 (47 to 67) years vs.57 (46 to 67) years Sex or gender:
Other PROGRESS-Plus criteriac: NR Setting: NR | Mechanism of injurya
Vitals on arrivala:
Injury characteristica:
Head: 4.9% vs. 5.2% Thorax: 27.1% vs. 34.0%b Abdomen: 6.0% vs. 7.6% Traumatic brain injury: 13.1% vs. 15.2%
Single rib fracture: 2.8% vs. 3.4% Multiple rib fractures: 66.3% vs. 63.5% Sternum fracture: 10.8% vs. 11.5% Flail chest: 38.5% vs. 43.1%b Thoracic vessels: 2.5% vs. 2.8% Esophagus: 0% vs. 0%
Pneumothorax: 36.3% vs. 39.1% Hemothorax: 19.1% vs. 17.1% Hemopneumothorax: 39.1% vs. 42.1% Lung NOS: 46.8% vs. 52.5%b
Liver: 8.9% vs. 11.8%b Spleen: 13.7% vs. 14.3% Stomach: 0% vs. 0.3% Small bowel: 0.9% vs. 1.2% Colon: 1.2% vs. 1.2% Rectum: 0.1% vs. 0% Pain management during hospitalization: NR | Number of ribs fixateda: NR Number of nerves cryoablated: NR Cryoneurolysis conducted by: NR Time of cryoneurolysis administration: during SSRF; specific timing NR Time to surgery: during the hospitalization after injury; exact timing NR | Intervention: cryoneurolysis
Comparator: No cryoneurolysis | Outcomes:
Follow-up: NR Subgroup analysis: flail chest participants |
Marturano et al. (2023)26 US Funding source: None | Multicentre retrospective cohort January 2015 to September 2021 | Participants: 241 participants ≥ 18 years old undergoing SSRF. Of these, 51 (21.2%) received cryoneurolysis. Diagnosis: traumatic chest wall injury Comorbiditiesa:
Age, mediana (IQR): 60.0 (51.0 to 70.0) vs. 55.0 (42.0 to 65.0)b Sex or gendera:
Other PROGRESS-Plus criteriac: NR Setting: 2 trauma centres within the same system (Level I and III) | Mechanism of injurya: NR Vitals on arrivala: NR Injury characteristica:
Pain management during hospitalization: peripheral nerve block within 48 hours of admission | Number of ribs fixateda, median (IQR): 4.0 (3.0 to 5.0) vs. 4.0 (3.0 to 6.0) Number of nerves cryoablated, median (IQR): 6 (5 to 6) vs. NA Cryoneurolysis conducted by: surgeons Time of cryoneurolysis administration: during SSRF; during drainage of any hemothorax and before fracture reduction and fixation Time from admission to surgery: within 72 hours of admission | Intervention: cryoneurolysis
Comparator: Standard MMPR (MMPR included scheduled acetaminophen, ibuprofen, gabapentin, methocarbamol, and/or topical lidocaine as first-line agents. A combination of short acting opioids in both IV and oral forms was used as second-line options) | Outcomes:
Follow-up: 30 days Subgroup analysis: excluding participants who were sedated with opioid infusion |
Fernandez et al. (2022)25 US Funding source: None | Single-centre retrospective cohort September 28, 2015 to January 9, 2021 | Participants: 68 participants ≥ 18 years old undergoing SSRF. Of these, 44 (64.7%) received cryoneurolysis. Diagnosis: multiple traumatic rib fractures Comorbiditiesa:
Age, mediana (IQR): 59 (52 to 69) vs. 57 (50 to 68) Sex or gendera:
other sexes or genders NR Racea:
BMI, mediana (IQR): 27.3 (24.9 to 30.0) vs. 26.8 (25.8 to 32.3) Other PROGRESS-Plus criteriac: NR Setting: Level I trauma centre | Mechanism of injurya:
Vitals on arrivala: NR Injury characteristica:
Pain management during hospitalization: All patients received rib fracture multimodal pain management according to standardized protocols at the institution: Patient-controlled analgesia: 11.4% vs. 20.8% Intercostal nerve block: 29.5% vs. 8.3% Epidural: 29.5% vs. 41.7% | Number of ribs fixateda, median (IQR): 4 (3 to 5) vs. 5 (4 to 5) Number of nerves cryoablated, median (IQR): 5 (4 to 6) vs. NA Cryoneurolysis conducted by: an attending surgeon with the assistance of residents Time of cryoneurolysis administration: during SSRF; at the end of surgery Time from admission to surgery, median (IQR): 3 days (2 to 4) vs. 3 days (2 to 6) | Intervention: cryoneurolysis
Comparator: No cryoneurolysis | Outcomes:
Follow-up: 0 to 3 months, 3 to 6 months Subgroup analysis: none |
O'Connor et al. (2022)27 US Funding source: None | Single-centre retrospective cohort October 2017 to November 2020 | Participants: 26 participants ≥ 18 years old undergoing SSRF. Of these, 14 (53.8%) received cryoneurolysis. Diagnosis: traumatic rib fractures Comorbiditiesa:
Age, meana (SD): 54 (12.3) vs. 52 (20.5) Sex or gendera:
BMI, meana (SD): 30.8 (7.2) vs. 33.1 (8.8) Other PROGRESS-Plus criteriac: NR Setting: level II trauma centre | Mechanism of injurya: NR Vitals on arrivala:
Injury characteristica:
Pain management during hospitalization: standard multimodal pain management protocol per institution’s rib fracture pathway, including scheduled and as-needed medications | Number of ribs fixateda, median (range): 4 (1 to 5) vs. 4 (3 to 5) Number of nerves cryoablated: NR Cryoneurolysis conducted by: surgeons Time of cryoneurolysis administration: during SSRF; at the beginning of the rib fixation procedure Time from admission to surgery, (days), mean (SD): 3.1 (1.4) vs. 3.6 (2.5) | Intervention: cryoneurolysis
Comparator: ropivacaine 0.2% EIP | Outcomes:
Follow-up: 30 days Subgroup analysis: opioid-naive patients |
Bauman et al. (2021)23 US Funding source: NR | Multicentre, retrospective cohort Eight-year period | Participants: 136 participants ≥ 18 years undergoing SSRF during the index hospitalization over an 8-year period. Of these, 44 (32.4%) received cryoneurolysis. Diagnosis: blunt trauma Comorbiditiesa: NR Age, meana (SD): 58.9 (13.6) vs. 56.8 (15.7) Sex or gendera:
Other PROGRESS-Plus criteriac: NR Setting: Level II or higher designated trauma centres located in urban settings | Mechanism of injurya: NR Vitals on arrivala: NR Injury characteristica:
Pain management during hospitalization: all patients were placed on MMPR (oral and IV narcotics as needed, scheduled acetaminophen and ibuprofen, scheduled gabapentin 300 mg 3 times daily, and as-needed muscle relaxants), and some form of regional anesthesia | Number of ribs fixated, meana (± SD): 4.73 (1.66) vs. 4.78 (1.64) Number of nerves cryoablated: NR Cryoneurolysis conducted by: surgeons Time of cryoneurolysis administration: during SSRF; specific timing NR Time from admission to surgery: within 72 hours of injury, less than 14 days | Intervention: cryoneurolysis
Comparator: No cryoneurolysis | Outcomes:
Follow-up: NR Subgroup analysis: none |
Choi et al. (2021)24 US Funding source: NR | Single-centre retrospective cohort September 1, 2019, to September 30, 2020 | Participants: 34 participants ≥ 18 years old undergoing SSRF. Of these, 22 (64.7%) received cryoneurolysis. Diagnosis: acute rib fractures Comorbidities: NR Age, mediana (IQR): 55.0 (45.0 to 67.3) vs. 55.0 (37.0 to 60.8) Sex or gendera:
Other PROGRESS-Plus criteriac: NR Setting: Level I trauma centre | Mechanism of injurya: NR Vitals on arrivala: NR
Pain management during hospitalization: All patients without contraindications receive around-the-clock acetaminophen, celecoxib, and gabapentin throughout hospitalization | Number of ribs fixated, mediana (IQR): 4 (3 to 5) vs. 4 (4 to 6) Number of nerves cryoablated, median (IQR): 6 (6 to 7) vs. NA Cryoneurolysis conducted by: single faculty with trainee surgeons Time of cryoneurolysis administration: during SSRF; after rib fixation Time from admission to surgery: NR | Intervention: cryoneurolysis
Comparator: No cryoneurolysis | Outcomes:
Follow-up: 2-weeks, 6-months, and 1-year follow-up visits
Subgroup analysis: none |
AIS = abbreviated injury scale; BMI = body mass index; bpm = beats per minute; CAUTI = catheter-associated urinary tract infection; CLABSI = central line-associated bloodstream infection; COPD = chronic obstructive pulmonary disease; EIP = elastomeric infusion pump; GCS = Glasgow coma score; HLOS = hospital length of stay; ICU = intensive care unit; IQR = interquartile range; ISS = injury severity score; LOS = length of stay; MME = morphine milliequivalents; MMPR = multimodal pain regimen; NA = not applicable; NOS = not otherwise specified; NPS = numeric pain score; NR = not reported; SD = standard deviation; SSI = surgical site infection; SSRF = surgical stabilization of rib fractures; vs. = versus.
aIntervention group vs. comparator group, respectively.
bSignificant differences between groups (defined as P < 0.05).
cThe main PROGRESS-Plus criteria include place of residence, race, ethnicity, culture, language, occupation, gender, sex, religion, education, socioeconomic status, and social capital, personal characteristics associated with discrimination (e.g., age, disability), features of relationships, and time-dependent relationships.29
dMore than 22 breaths per minute.
eSystolic blood pressure less than 90 mm Hg.
fOpioid tolerance was defined as daily use within 2 weeks before presentation and duration of use more than 4 weeks, illicit drug use with positive urine or serum toxicology results.
gChange was recorded at baseline (24 hours before surgery) and on postoperative days 1 to 3.
hChange measured by generalized estimating equation comparing 12 hours before SSRF and the last 24 admission hours.
Appendix 4: Critical Appraisal of Included Publications
Please note that this appendix has not been copy-edited.
Table 3: Strengths and Limitations of Primary Clinical Studies Using the Downs and Black Checklist21
Strengths | Limitations |
|---|---|
Aryan et al. (2024)22 | |
Authors clearly described the objectives and hypotheses of the study, main outcomes, interventions, and main findings. Standardized outcome definitions were provided. Authors provided comprehensive reporting of patients’ injury profile, comorbidities, and in-hospital complications. Appropriate statistical analyses for large observational data were reported. For outcomes, the authors reported simple outcome data (n [%]), or measures of variability (IQRs, medians) for intervention and comparator groups, and actual P values. A separate subgroup analysis of flail chest patients was reported. Adverse events were reported. The study was conducted using a large national database, which enhances generalizability. The presented data reflected practice across diverse trauma centres (i.e., multiple sites). Statistical adjustment improved comparability. The author(s) received no financial support for the research, authorship, and/or publication of this article. The authors declared that they had no potential conflicts of interest. | The details on technique or timing of the intervention (cryoneurolysis) were not explained. The details on the comparator (noncryoneurolysis) were not specified. There was limited reporting of the characteristics of study participants (e.g., across PROGRESS-Plus criteria).29 The study was completed in highly specialized settings, limiting generalizability to lower-Level trauma care. Retrospective registry data are prone to coding and misclassification errors. Retrospective design with no blinding introduces risk of selection bias. There was a lack of patient-centred outcomes (e.g., pain scores, opioid use). There were unmeasured confounding factors (e.g., centre expertise, analgesia protocols). It was not reported how participants were selected to receive the intervention (cryoneurolysis). Small effect sizes may reach statistical significance because of large sample size. |
Marturano et al. (2023)26 | |
Authors clearly described the objectives and hypotheses of the study, main outcomes, participant eligibility criteria, intervention, comparator, and main findings. A subgroup analysis excluding participants who were sedated with opioid infusion was reported. Inclusion criteria were well defined. Findings are likely applicable to similar trauma centres with SSRF capability. Outcomes were generally objective. Sample size may be insufficient for reporting uncommon complications. The authors received no financial support for the research, authorship, and/or publication of this article. The authors declared potential conflicts of interest. Two authors had affiliations with related medical device companies. | There was limited reporting of the characteristics of study participants (e.g., across PROGRESS-Plus criteria).29 Some outcomes reported without full adjustment details. Single trauma centre was included, limiting generalizability. Appropriate presentation of participants at follow-up were not provided. Retrospective registry data are prone to coding and misclassification errors. Retrospective design with no blinding introduces risk of selection bias. Pain intensity scores were subjective and susceptible to reporting bias. Potential selection bias for intervention (surgeon discretion determined cryoneurolysis use) was present. There was limited ability to control for factors such as COVID-19 complications, and evolving care pathways (e.g., change in culture regarding opioid use). No power calculation was reported. |
Fernandez et al. (2022)25 | |
Authors clearly described the objectives and hypotheses of the study, main outcomes, participant eligibility criteria, interventions, and main findings. Measures of variability and exact P values reported. Appropriate statistical methods were described, including regression modelling and sensitivity analyses. Appropriate presentation of participants at follow-up was provided. Inclusion criteria were clearly defined. Clinically relevant outcomes were used. Baseline differences (e.g., chest-AIS distribution) were acknowledged and partially addressed via sensitivity analyses. Outcomes were largely objective (MME, LOS, intubation, tracheostomy). The authors received no financial support for the research, authorship, and/or publication of this article. The authors declared that they had no potential conflicts of interest. | The details on the comparator (noncryoneurolysis) were not specified. There was limited reporting of the characteristics of study participants (e.g., across PROGRESS-Plus criteria).29 Results were most applicable to similar trauma centres with SSRF expertise. Retrospective registry data are prone to coding and misclassification errors. Retrospective design with no blinding introduces risk of selection bias. Historical control groups introduce high risk of temporal bias. Residual confounding is likely present (e.g., surgeon discretion determined cryoneurolysis use), limiting generalizability. Pain intensity scores were subjective and susceptible to reporting bias. No formal power calculation was reported. Small sample size may limit ability to detect significant clinically meaningful differences. |
O'Connor et al. (2022)27 | |
Authors clearly described the objectives and hypotheses of the study, main outcomes, participant eligibility criteria, interventions, comparator, and main findings. Effect sizes and confidence intervals were presented for key outcomes. Appropriate presentation of participants at follow-up was presented. The long-term outcomes of opioid-naive patients was reported separately. Clinically relevant outcomes were used. Opioid use and LOS are objective outcomes. Clinically meaningful comparison was conducted against another active pain-control strategy. The authors received no financial support for the research, authorship, and/or publication of this article. The authors declared potential conflicts of interest. Three authors had affiliations with related medical device companies. | There was limited reporting of the characteristics of study participants (e.g., across PROGRESS-Plus criteria).29 Single-centre study was included, limiting generalizability. Specialized surgical and pain-management expertise may not reflect typical practice. Comparator reflected local standards rather than universal care. Retrospective registry data are prone to coding and misclassification errors. Retrospective design with no blinding introduces risk of selection bias. Pain intensity scores were subjective and susceptible to reporting bias. Small sample size limited ability to control for confounders. Differences in analgesic pathways beyond cryoneurolysis may exist. Potential selection bias for Intervention (surgeon discretion determined cryoneurolysis use) was present. The study was likely underpowered for complications and cost outcomes. No power calculation was reported. Two authors were paid educating faculty members for AtriCure (their cryoneurolysis probe was used in the study). |
Bauman et al. (2021)23 | |
Authors clearly described the objectives and hypotheses of the study, main outcomes, participant eligibility criteria, and main findings. Participant characteristics, intervention details, and main outcomes (opioid use, LOS, hospital charges) were reported. Measures of variability (IQRs, medians) reported for key outcomes. Appropriate statistical tests were reported. The study used a multi-institutional design, which improves generalizability. Findings are likely applicable to similar trauma centres with SSRF capability. Authors conducted appropriate statistical analyses. Outcome measures were valid. Opioid use measured objectively (MME), limiting measurement bias. The authors declared that their potential conflicts of interest. Two authors had affiliations with related medical device companies. | The details on the comparator (noncryoneurolysis) were not specified. There was no reporting of key safety or complication outcomes. There was limited reporting of the characteristics of study participants (e.g., across PROGRESS-Plus criteria).29 Retrospective registry data are prone to coding and misclassification errors. Retrospective design with no blinding introduces risk of selection bias. Groups may differ systematically (e.g., injury severity, institutional practices). Limited adjustment was done for confounders related to analgesia protocols. Choice of cryoneurolysis use likely influenced by surgeon preference and centre-level factors. Power calculation was not reported. Sources of funding were not disclosed. One author is a paid educating faculty for AtriCure (their cryoneurolysis probe was used in the study). |
Choi et al. (2021)24 | |
Authors clearly described the objectives and hypotheses of the study, main outcomes, participant eligibility criteria, intervention, and main findings. Careful description of surgical technique was provided. Appropriate framing was provided as exploratory/pilot work. The study provided appropriate presentation of participants at follow-up. The study included longer-term follow-up for adverse effects. Adequate inclusion criteria were used (e.g., patients tolerating single-lung ventilation). Objective outcomes were reported. Time-series analysis was appropriate for repeated measures. The authors declared that they had no potential conflicts of interest. | The details on the comparator (noncryoneurolysis) were not specified. There was limited reporting of the characteristics of study participants (e.g., across PROGRESS-Plus criteria).29 The study was completed in a highly specialized setting (thoracoscopic IC, single institution), limiting generalizability. Retrospective registry data are prone to coding and misclassification errors. Retrospective design with no blinding introduces risk of selection bias. Pain intensity scores were subjective and susceptible to reporting bias. The study had small sample size and small comparison groups. There were baseline injury differences between groups (e.g., pulmonary contusions, fracture complexity). Limited adjustment was done for confounders due to small sample size. The study was a pilot study. No power calculation was conducted. Sources of funding were not disclosed. |
AIS = abbreviated injury scale; CI = confidence interval; IQR = interquartile range; LOS = length of stay; MME = morphine milliequivalents; SSRF = surgical stabilization of rib fractures.
Appendix 5: Main Study Findings
Please note that this appendix has not been copy-edited.
Table 4: Summary of Findings by Outcome — Pain Intensity
Author (year) and intervention | With cryoneurolysis | Without cryoneurolysis | P value |
|---|---|---|---|
Postsurgery NPS, median (IQR) | |||
Marturano et al. (2023)26 Cryo vs. MMPR | Score at discharge: 4.0 (1.0 to 5.0) | 2.0 (1.0 to 5.0) | 0.27 |
Fernandez et al. (2022)25 Cryo vs. noncryo | Daily score: 3.4 (2.7 to 4.2) | 3.0 (2.1 to 3.8) | 0.409 |
Change in NPS, mean (SE) | |||
Choi et al. (2021)24,a Cryo vs. noncryo | −0.2 (1.5) | Reference group | 0.91 |
Cryo = cryoneurolysis; IQR = interquartile range; MMPR = multimodal pain regimen; NPS = numeric pain score; SE = standard error; SSRF = surgical stabilization of rib fractures.
Note: Bold numbers are representing significant P values, defined as P < 0.05.
aChange measured by generalized estimating equation comparing 12 hours before SSRF and last 24 admission hours.
Table 5: Summary of Findings by Outcome — Association of Cryo vs. EIP and Patient-Reported NPS
Author (year) and intervention | Point estimate (SE) | Estimated df | t value | 95% CI | P value |
|---|---|---|---|---|---|
O'Connor et al. (2022)27,a Cryo vs. EIP | −1.51 (0.61) | 73.14 | −2.47 | −2.722 to −0.290 | 0.02 |
CI = confidence interval; Cryo = cryoneurolysis; df = degrees of freedom; EIP = elastomeric infusion pump; SE = standard error.
aA linear mixed-effects model was used to estimate the association of Cryo and EIP on patients’ outcomes while controlling for other covariates, including opioid tolerance, sex, age, number of ribs fractured, number of ribs fixed, rib injury severity score (ISS), trauma ISS, presence of flail segment, smoking status, and postoperative length of stay.
Table 6: Summary of Findings by Outcome — Analgesic Use
Author (year) and intervention | With cryoneurolysis | Without cryoneurolysis | P value |
|---|---|---|---|
Postsurgery opioid consumption in oral MME, median (IQR) | |||
Marturano et al. (2023)26 Cryo vs. MMPR | Total use: 144.5 (55.5 to 301.5) Daily use: 16.3 (8.0 to 36.7) Discharge use: 135 (45 to 180) | 262.5 (129.5 to 464.5) 32.8 (15.2 to 57.6) 150 (45 to 225) | 0.001 0.01 0.22 |
Fernandez et al. (2022)25 Cryo vs. noncryo | Total use: 332 (209 to 528) Daily use: 28.5 (19.8 to 41.1) | 1,148 (613 to 2,149) 62.2 (37.9 to 102.0) | 0.002 0.014 |
Bauman et al. (2021)23 Cryo vs. noncryo | Total use: 88.6 (33.5 to 125.5) | 113.7 (67.5 to 254.6) | 0.026 |
Change in opioid consumption in oral MME (mg) | |||
Choi et al. (2021)24,a Cryo vs. noncryo | Mean (rSE): + 43.9 (86.1) | Reference group | 0.61 |
Cryo = cryoneurolysis; EIP = elastomeric infusion pump; IQR = interquartile range; MME = morphine milliequivalents; MMPR = multimodal pain regimen; rSE = robust standard error; SSRF = surgical stabilization of rib fractures.
Note: Bold numbers are representing significant P values, defined as P < 0.05.
aChange measured by generalized estimating equation comparing 12 hours before SSRF and the last 24 admission hours.
Table 7: Summary of Findings by Outcome — Association of Cryo vs. EIP and Opioid Consumption in Oral MME (mg)
Author (year) and intervention | Point estimate (SE) | Estimated df | t value | 95% CI | P value |
|---|---|---|---|---|---|
O'Connor et al. (2022)27,a Cryo vs. EIP | −1.37 (0.52) | 68.8 | −2.64 | −2.411 to −0.335 | 0.01 |
CI = confidence interval; Cryo = cryoneurolysis; df = degrees of freedom; EIP = elastomeric infusion pump; MME = morphine milliequivalents; SE = standard error; vs. = versus.
aA linear mixed-effects model was used to estimate the association of Cryo and EIP on patients’ outcomes while controlling for other covariates, including opioid tolerance, sex, age, number of ribs fractured, number of ribs fixed, rib injury severity score (ISS), trauma ISS, presence of flail segment, smoking status, and postoperative length of stay.
Table 8: Summary of Findings by Outcome — Resource Use
Author (year) and intervention | With cryoneurolysis | Without cryoneurolysis | P value |
|---|---|---|---|
Total hospital LOS (days), median (IQR) or 95%CI | |||
Aryan et al. (2024)22 Cryo vs. noncryo | 12 (8 to 18) | 12 (9 to 19) | 0.10 |
Marturano et al. (2023)26 Cryo vs. MMPR | 9.0 (6.0 to 14.0) | 11.0 (8.0 to 18.0) | 0.02 |
Fernandez et al. (2022)25 Cryo vs. noncryo | 10 (95% CI, 8 to 11) | 12 (95% CI, 7 to 24) | 0.072 |
O'Connor et al. (2022)27 Cryo vs. EIP | 9 (7 to 10) | 11 (9 to 15.5) | 0.09 |
Bauman et al. (2021)23 Cryo vs. noncryo | 9 (7 to 11) | 10 (8 to 13) | 0.018 |
Choi et al. (2021)24 Cryo vs. noncryo | 6.0 (4.8 to 11.0) | 7.5 (5 to 15.8) | 0.19 |
Postoperative LOS (days), median (IQR) | |||
O'Connor et al. (2022)27 Cryo vs. EIP | 4 (4 to 5) | 6 (5 to 9.5) | 0.04 |
Bauman et al. (2021)23 Cryo vs. noncryo | 4 (2 to 5.75) | 6 (4 to 8) | < 0.001 |
Choi et al. (2021)24 Cryo vs. noncryo | 4 (3 to 8) | 4 (3 to 5) | 0.84 |
ICU admission or ICU LOS (days) | |||
Aryan et al. (2024)22 Cryo vs. noncryo | Median (IQR): 6 (4 to 11) | 7 (4 to 13) | < 0.001 |
Marturano et al. (2023)26 Cryo vs. MMPR | Median (IQR): 2 (0 to 4) | 4 (2 to 8) | 0.001 |
Fernandez et al. (2022)25 Cryo vs. noncryo | Median (95% CI): 8 (6 to 9) | 9 (6 to 22) | 0.027 |
Choi et al. (2021)24 Cryo vs. noncryo | n (%): 16 (80) | 12 (86) | 0.99 |
Operative times (minutes), median (IQR) | |||
Choi et al. (2021)24 Cryo vs. noncryo | 148.5 (122.5 to 180.5) | 131.5 (124.5 to 138.8) | 0.26 |
Duration of mechanical ventilation, median (IQR) | |||
Aryan et al. (2024)22 Cryo vs. noncryo | Days, 6 (3 to 13) | 7 (3 to 13) | 0.23 |
Marturano et al. (2023)26 Cryo vs. MMPR | Days, 0.0 (0.0 to 0.0) | 0.0 (0.0 to 3.0) | 0.002 |
Fernandez et al. (2022)25 Cryo vs. noncryo | Hours, 8 (3 to 13) | 10 (2 to 18) | 0.687 |
CI = confidence interval; Cryo = cryoneurolysis; EIP = elastomeric infusion pump; ICU = intensive care unit; IQR = interquartile range; LOS = length of stay; MMPR = multimodal pain regimen; noncryo = no cryoneurolysis.
Note: Bold numbers are representing significant P values, defined as P < 0.05.
Table 9: Summary of Findings by Outcome — In-Hospital Complications
Author (year) and intervention | With cryoneurolysis | Without cryoneurolysis | P value |
|---|---|---|---|
Overall in-hospital complications, n (%) | |||
Aryan et al. (2024)22 Cryo vs. noncryo | 153 (20.4) | 3670 (24.4) | 0.01 |
Marturano et al. (2023)26 Cryo vs. MMPR | 10 (19.6) | 38 (20) | 1.0 |
Incidence of pneumonia | |||
Aryan et al. (2024)22 Cryo vs. noncryo | n (%): 16 (2.1%) | 572 (3.8%) | 0.02 |
Fernandez et al. (2022)25 Cryo vs. noncryo | % (95% CI): 15.9 (8.0 to 31.8) | 33.3 (18.7 to 59.3) | 0.106 |
Choi et al. (2021)24 Cryo vs. noncryo | n (%): (0)0 | 2 (14) | 0.16 |
Tracheostomy rates | |||
Marturano et al. (2023)26 Cryo vs. MMPR | n (%): 3 (5.9) | 7 (3.7) | 0.88 |
Fernandez et al. (2022)25 Cryo vs. noncryo | % (95% CI): 4.6 (1.1 to 18.1) | 25.0 (12.3 to 50.6) | 0.032 |
Choi et al. (2021)24 Cryo vs. noncryo | n (%): 1 (5) | 1 (7) | 0.99 |
Return to operation room, n (%) | |||
Aryan et al. (2024)22 Cryo vs. noncryo | 21 (2.8) | 465 (3.1) | 0.66 |
Marturano et al. (2023)26 Cryo vs. MMPR | 2 (3.9) | 14 (7.4) | 1.0 |
Pulmonary complications, n (%) | |||
Aryan et al. (2024)22 Cryo vs. noncryo | 5 (0.7) | 263 (1.8) | 0.02 |
Marturano et al. (2023)26 Cryo vs. MMPR | 38 (20.0) | 10 (19.6) | 0.693 |
Intubated after surgery, n (%) | |||
Aryan et al. (2024)22 Cryo vs. noncryo | 47 (6.3) | 1151 (7.3) | 0.15 |
Marturano et al. (2023)26 Cryo vs. MMPR | 9 (17.7) | 74 (39.0) | 0.01 |
Fernandez et al. (2022)25 Cryo vs. noncryo | (NR) 22.7 | (NR) 62.5 | 0.002 |
Choi et al. (2021)24 Cryo vs. noncryo | 4 (20) | 4 (29) | 0.69 |
Unplanned reintubation, n (%) | |||
Marturano et al. (2023)26 Cryo vs. MMPR | 5 (9.8) | 5 (2.6) | 0.08 |
Hardware removal, n (%) | |||
Marturano et al. (2023)26 Cryo vs. MMPR | 0 (0.0) | 7 (3.7) | 0.70 |
Chest tube reinsertion, n (%) | |||
Marturano et al. (2023)26 Cryo vs. MMPR | 2 (3.9) | 14 (7.4) | 1.0 |
COVID+ [as reported by the study authors], n (%) | |||
Marturano et al. (2023)26 Cryo vs. MMPR | 2 (3.9) | 0 (0.0) | 0.08 |
Postoperative nerve block, n (%) | |||
Marturano et al. (2023)26 Cryo vs. MMPR | 2 (3.9) | 3 (1.6) | 0.58 |
Cerebrovascular accident, n (%) | |||
Aryan et al. (2024)22 Cryo vs. noncryo | 12 (1.6) | 123 (0.8) | 0.02 |
Extremity compartment syndrome, n (%) | |||
Aryan et al. (2024)22 Cryo vs. noncryo | 2 (0.3) | 9 (0.1) | 0.04 |
Delirium, n (%) | |||
Aryan et al. (2024)22 Cryo vs. noncryo | 21 (5.5) | 204 (5.5) | 1.0 |
Acute respiratory distress syndrome, n (%) | |||
Aryan et al. (2024)22 Cryo vs. noncryo | 9 (1.2) | 282 (1.9) | 0.18 |
Myocardial infarction, n (%) | |||
Aryan et al. (2024)22 Cryo vs. noncryo | 6 (0.8) | 61 (0.4) | 0.11 |
Cardiac arrest, n (%) | |||
Aryan et al. (2024)22 Cryo vs. noncryo | 13 (1.7) | 311 (2.1) | 0.52 |
Acute kidney injury, n (%) | |||
Aryan et al. (2024)22 Cryo vs. noncryo | 23 (3.1) | 363 (2.4) | 0.27 |
Deep vein thrombosis, n (%) | |||
Aryan et al. (2024)22 Cryo vs. noncryo | 22 (2.9) | 512 (3.4) | 0.47 |
Sepsis, n (%) | |||
Aryan et al. (2024)22 Cryo vs. noncryo | 10 (1.3) | 235 (1.6) | 0.61 |
Superficial SSI, n (%) | |||
Aryan et al. (2024)22 Cryo vs. noncryo | 1 (0.1) | 79 (0.5) | 0.14 |
Deep SSI, n (%) | |||
Aryan et al. (2024)22 Cryo vs. noncryo | 2 (0.3) | 71 (0.5) | 0.41 |
Organ space SSI, n (%) | |||
Aryan et al. (2024)22 Cryo vs. noncryo | 3 (0.4) | 50 (0.3) | 0.76 |
CLABSI, n (%) | |||
Aryan et al. (2024)22 Cryo vs. noncryo | 0 (0) | 32 (0.2) | 0.21 |
CAUTI, n (%) | |||
Aryan et al. (2024)22 Cryo vs. noncryo | 3 (0.4) | 116 (0.8) | 0.25 |
CAUTI = catheter-associated urinary tract infection; CLABSI = central line-associated bloodstream infection; Cryo = cryoneurolysis; IQR = interquartile range; MMPR = multimodal pain regimen; noncryo = no cryoneurolysis; NR = not reported; SSI = surgical site infection; vs. = versus.
Note: Bold numbers are representing significant P values, defined as P < 0.05.
Table 10: Summary of Findings by Outcome — Association of Cryo vs. EIP With In-Hospital Complications Related to Pulmonary Functiona
Author (year) and intervention | Point estimate (SE) | Estimated df | t value | 95% CI | P value |
|---|---|---|---|---|---|
O'Connor et al. (2022)27,b Cryo vs. EIP | −48.84 (131.84) | 58.42 | −0.37 | −312.74 to 215.01 | 0.71 |
CI = confidence interval; Cryo = cryoneurolysis; df = degrees of freedom; EIP = elastomeric infusion pump; SE = standard error; vs. = versus.
aPulmonary function is reflected by incentive spirometry (IS) effort in mL.
bA linear mixed-effects model was used to estimate the association of Cryo and EIP on patients’ outcomes while controlling for other covariates, including opioid tolerance, sex, age, number of ribs fractured, number of ribs fixed, rib injury severity score (ISS), trauma ISS, presence of flail segment, smoking status, and postoperative length of stay.
Table 11: Summary of Findings by Outcome — Postdischarge Adverse Events
Author (year), intervention, duration of follow-up | With cryoneurolysis | Without cryoneurolysis | P value |
|---|---|---|---|
Pain medications, n (%) | |||
Fernandez et al. (2022)25 Cryo vs. noncryo | |||
0 to 3 months | Opioids use: 12 (31.6) | 13 (61.9) | NR |
3 to 6 months | Opioids use: 1 (25) | 3 (50) | NR |
Choi et al. (2021)24 Cryo vs. noncryo | |||
2 weeks | Opioids use: 3 (27) | 0 (0) | 0.51 |
2 weeks | Other pain medications: 4 (36) | 3 (60) | 0.60 |
Minor medical complications,a n (%) | |||
Fernandez et al. (2022)25 Cryo vs. noncryo | |||
0 to 3 months | 5 (13.2) | 7 (33.3) | NR |
3 to 6 months | 1 (25) | 1 (16.7) | NR |
Functional limitations, n (%) | |||
Fernandez et al. (2022)25 Cryo vs. noncryo | |||
0 to 3 monthsb | 1 (2.6) | 2 (9.5) | NR |
3 to 6 monthsc | 0 (0) | 1 (16.7) | NR |
Choi et al. (2021)24 Cryo vs. noncryo | |||
2 weeks | 0 | 0 | NA |
30-day readmission, n (%) | |||
Marturano et al. (2023)26 Cryo vs. MMPR | 3 (5.9) | 7 (3.7) | 0.88 |
O'Connor et al. (2022)27 Cryo vs. EIP | 1 (7) | 1 (8) | > 0.99 |
Chest wall neuralgia or paresthesia, n (%) | |||
Fernandez et al. (2022)25 Cryo vs. noncryo | |||
0 to 3 months | 4 (10.5) | 6 (28.6) | NR |
3 to 6 months | 0 (0) | 3 (50) | NR |
O'Connor et al. (2022)27 Cryo vs. EIP | |||
1 year | 0 (0) | 2 (17) | 0.11 |
Choi et al. (2021)24 Cryo vs. noncryo | |||
6 months | 1 (6) | 0 | NR |
Difficulty sleeping due to chest wall pain, n (%) | |||
Choi et al. (2021)24 Cryo vs. noncryo | |||
1 month | 0 | 1 | NR |
Cryo = cryoneurolysis; EIP = elastomeric infusion pump; MMPR = multimodal pain regimen; NA = not applicable; noncryo = no cryoneurolysis; NR = not reported; vs. = versus.
Note: Bold numbers are representing significant P values, defined as P < 0.05.
aMinor medical complications included incisional infection, delayed wound healing, small pleural effusion, residual pneumothorax, and seroma formation.
bShort-term (0 to 3 months) functional limitations included vocal cord paralysis, scapular winging, and scapular or clavicular pain.
cLong-term (3 to 6 months) functional limitations included hardware infection (n = 1), neuropathic pain (n = 3), and functional limitations associated with winging scapula.
Table 12: Summary of Findings by Outcome — Other
Author (year) and Intervention | With cryoneurolysis | Without cryoneurolysis | P value |
|---|---|---|---|
Discharge disposition | |||
Fernandez et al. (2022)25 Cryo vs. noncryo | % (95% CI) | ||
Home: 81.8 (71.0 to 94.3) | 54.2 (37.2 to 78.8) | 0.044 | |
Choi et al. (2021)24 Cryo vs. noncryo | n (%) | ||
Home: 13 (65) | 9 (64) | 0.80 | |
Long-term care hospital 3: (15) | 2 (14) | NR | |
Skilled nursing facility: 30 (15) | 2 (14) | NR | |
Other: 0 (0) | 1 (7) | NR | |
Mortality rate, n (%) | |||
Aryan et al. (2024)22 Cryo vs. noncryo | 18 (2.4) | 359 (2.4) | 0.98 |
Marturano et al. (2023)26 Cryo vs. MMPR | 1 (2.0) | 5 (2.6) | 1.0 |
Fernandez et al. (2022)25 Cryo vs. noncryo | 1 (NR) | 0 (0) | 1.000 |
Choi et al. (2021)24 Cryo vs. noncryo | 1 (5) | 0 (0) | 0.99 |
Hospital charges | |||
O'Connor et al. (2022)27 Cryo vs. EIP | Mean (SD) | ||
$90,224 (34,633) | $131,498 (73,072) | 0.07 | |
Bauman et al. (2021)23 Cryo vs. noncryo | Median (IQR) | ||
Postoperative: $10,556 (4,481 to 23,026) | $20,269 (10,445 to 43,430) | 0.001 | |
Total: $153,908 (118,820 to 213,823) | $143,196 (109,183 to 212,318) | 0.734 | |
The day of surgery: $93,932 (79,384 to 114,292) | $71,143 (52,401 to $86,611) | < 0.001 | |
Cryo = cryoneurolysis; EIP = elastomeric infusion pump; IQR = interquartile range; MMPR = multimodal pain regimen; noncryo = no cryoneurolysis; NR = not reported; SD = standard deviation; vs. = versus.
Note: Bold numbers are representing significant P values, defined as P < 0.05.
Table 13: Summary of Findings — Subgroup Analysis
Outcomes | With cryoneurolysis | Without cryoneurolysis | P value |
|---|---|---|---|
Aryan et al. (2024):22 Cryo vs. noncryo — Analysis for patients with flail chest | |||
ICU LOSa (days), median (IQR) | 7 (NR) | 8 (NR) | 0.02 |
Marturano et al. (2023):26 Cryo vs. MMPR — Analysis excluding patients sedated with opioid infusions | |||
Average daily MME, median (IQR) | 26.5 (12.2 to 44.4) | 33.0 (15.9 to 59.2) | Univariate: 0.081 Multivariableb: 0.260 |
Total MME, median (IQR) | 132.3 (48 to 275.3) | 226.0 (109 to 362) | Univariate: 0.038 Multivariableb: 0.016 |
Discharge MME, median (IQR) | 150.0 (90.0 to 210.0) | 150.0 (90 to 225) | Univariate: 0.367 Multivariableb: 0.575 |
Discharge NPS, median (IQR) | 4.0 (1.0 to 5.0) | 2.0 (1.0 to 5.0) | Univariate: 0.547 Multivariableb: 0.427 |
Hospital LOS (days), median (IQR) | 7.0 (6.0 to 10.0) | 9.0 (7.0 to 13.0) | Univariate: 0.020 Multivariableb: 0.005 |
ICU admission (days), median (IQR) | 0.0 (0.0 to 3.0) | 3.0 (0.0 to 5.0) | Univariate: 0.004 Multivariableb: 0.002 |
Ventilator duration (days), median (IQR) | 0.0 (0.0 to 0.0) | 0.0 (0.0 to 0.0) | Univariate: 0.093 Multivariableb: 0.181 |
Pulmonary complications, n (%) | 4 (9.8%) | 17 (13.7%) | Univariate: 0.700 Multivariablec: 0.449 |
O'Connor et al. (2022):27 Cryo vs. EIP — Analysis for patients who were opioid-naive | |||
Discharge opioid prescription (mg), median (IQR) | 41.25 (37.5 to 45) | 175 (150 to 200) | 0.03 |
No discharge opioid prescription, n (%) | 3 (38) | 1 (13) | 0.56 |
Opioid prescription refill 30 days after discharge, n (%) | 1 (13) | 1 (13) | > 0.99 |
Patients on opioids 1-year after surgery, n (%) | 0 | 1 (13) | > 0.99 |
Cryo = cryoneurolysis; EIP = elastomeric infusion pump; ICU = intensive care unit; IQR = interquartile range; LOS = length of stay; MME = morphine milliequivalents; MMPR = multimodal pain regimen; noncryo = no cryoneurolysis; NPS = numeric pain score; NR = not reported; SD = standard deviation; vs. = versus.
Note: Bold numbers are representing significant P values, defined as P < 0.05.
aOnly this outcome was reported from the subgroup analysis on patients with flail chest.
bAnalyses were adjusted for age, underlying lung disease, number ribs broken, injury severity score, and preoperative peripheral nerve block.
cAnalysis was adjusted for age.
ISSN: 2563-6596
Canada’s Drug Agency (CDA-AMC) is a pan-Canadian health organization. Created and funded by Canada’s federal, provincial, and territorial governments, we’re responsible for driving better coordination, alignment, and public value within Canada’s drug and health technology landscape. We provide Canada’s health system leaders with independent evidence and advice so they can make informed drug, health technology, and health system decisions, and we collaborate with national and international partners to enhance our collective impact.
Disclaimer: CDA-AMC has taken care to ensure that the information in this document was accurate, complete, and up to date when it was published, but does not make any guarantee to that effect. Your use of this information is subject to this disclaimer and the Terms of Use at cda-amc.ca.
The information in this document is made available for informational and educational purposes only and should not be used as a substitute for professional medical advice, the application of clinical judgment in respect of the care of a particular patient, or other professional judgments in any decision-making process. You assume full responsibility for the use of the information and rely on it at your own risk.
CDA-AMC does not endorse any information, drugs, therapies, treatments, products, processes, or services. The views and opinions of third parties published in this document do not necessarily reflect those of CDA-AMC. The copyright and other intellectual property rights in this document are owned by the Canadian Agency for Drugs and Technologies in Health (operating as CDA-AMC) and its licensors.
Questions or requests for information about this report can be directed to Requests@CDA-AMC.ca.