Drugs, Health Technologies, Health Systems
Health Technology Review
Dual Therapy for Initial Treatment of Adult Patients With Pulmonary Arterial Hypertension
Key Messages
What Is the Issue?
Pulmonary arterial hypertension (PAH) is a progressive disease characterized by increases in pulmonary vascular resistance and pulmonary arterial pressure, which eventually lead to right-sided heart failure and death if left untreated.
Decision-makers are interested in understanding the clinical effectiveness and safety of initial dual therapy in the treatment of patients with newly diagnosed PAH.
What Did We Do?
We identified and summarized the literature published since 2015 on the evidence of the clinical effectiveness and safety of initial dual therapy in the treatment of patients with newly diagnosed or previously untreated PAH.
What Did We Find?
We identified 3 relevant clinical studies. Two studies compared initial dual therapy with initial monotherapy, and 1 study compared initial triple therapy with initial dual therapy.
Initial dual therapy with an endothelin-1 receptor antagonist (ERA) and a phosphodiesterase type 5 (PDE5) inhibitor had significant advantages in improving various clinical outcomes compared with monotherapy, particularly for patients at low to intermediate risk with idiopathic PAH or connective tissue disease (CTD)–associated PAH and WHO functional class (FC) II or III symptoms.
Tolerability (withdrawal from the study due to adverse events [AEs]) was similar among patients receiving dual therapy or monotherapies, and the safety profile of dual therapy was consistent with the safety profiles of each monotherapy.
Initial triple therapy and initial dual therapy each improved various clinical outcomes in patients with newly diagnosed PAH, with no difference between groups.
What Does This Mean?
Initial combination therapy with 2 oral medications, an ERA and a PDE5 inhibitor, may provide better treatment outcomes in patients with PAH compared to monotherapy. However, there are limitations to the evidence that should be considered.
Abbreviations
6MWD
6-minute walk distance
AE
adverse event
CTD
connective tissue disease
ERA
endothelin-1 receptor antagonist
FC
functional class
HRQoL
health-related quality of life
NT-proBNP
N-terminal pro–brain natriuretic peptide
PAH
pulmonary arterial hypertension
PDE5
phosphodiesterase type 5
PH
pulmonary hypertension
PVR
pulmonary vascular resistance
RCT
randomized controlled trial
SAE
serious adverse event
SSc
systemic sclerosis
Context and Policy Issues
What Is PAH?
PAH is a rare, persistent, progressive disease characterized by high blood pressure in the arteries of the lungs. If left untreated, it can lead to difficulty breathing, fatigue, edema, dizziness, chest pain, heart failure, and ultimately death.1 It is 1 of the 5 pulmonary hypertension (PH) subgroups, group 1 PH,2 which is a specific type of PH where the pulmonary arteries become narrowed, thickened, or blocked.2 The cause in many cases is unknown (i.e., idiopathic).2 It can also be inherited (heritable), caused by drugs or toxins, or associated with other medical conditions such as CTD, congenital heart disease, or HIV infection.2
The annual incidence of PAH is estimated to be 7.6 cases per million adults in Canada, with a prevalence up to 26 to 100 cases per million adults in Canada.3 The average age of people who are newly diagnosed with PAH is 53 years, with more females diagnosed than males.1
The WHO FC system categorizes the severity of PAH and groups patients with PAH into 4 classes (I to IV) based on their symptoms and physical limitations, with higher classes representing more severe disease and greater functional impairment:4
WHO FC I: No limitations in physical activity. People with PAH have no symptoms.
WHO FC II: Slight limitations in physical activity. People with PAH may experience shortness of breath, fatigue, or chest pain with moderate exertion.
WHO FC III: Marked limitations in physical activity. People with PAH experience symptoms even with mild exertion.
WHO FC IV: People with PAH have symptoms even at rest and are unable to carry out any physical activity without discomfort.
The 2015 European Society of Cardiology and the European Respiratory Society guidelines classified patients with PAH into low-risk, intermediate-risk, and high-risk groups based on various clinical and hemodynamic factors, including clinical manifestations, symptom progression, WHO FC categories, 6-minute walk distance (6MWD) measures, cardiopulmonary exercise test results, plasma N-terminal pro–brain natriuretic peptide (NT-proBNP) levels, and other hemodynamic parameters.5 These classifications help predict patients’ 1-year mortality rates, with patients at low risk having a less than 5% estimated mortality risk, patients at intermediate risk having a 5% to 10% estimated mortality risk, and patients at high risk having a more than 10% estimated mortality risk.5
In addition, there are other recommended risk stratification assessment scales that are applicable to adults with PAH.2 These include the French Pulmonary Hypertension Network Risk Assessment Equation,6 the REVEAL risk score,7 the Pulmonary Hypertension Connection Equation,8 the Comparative, Prospective Registry of Newly Initiated Therapies for Pulmonary Hypertension (COMPERA) abbreviated risk assessment tool from the European Society of Cardiology and the European Respiratory Society,9 the Scottish composite score for PAH,10 and the COMPERA 2.0 risk assessment tool.11
What Are the Medications for Treatment of Patients With PAH?
Oral medications used for PAH targeted therapy include ERAs (e.g., ambrisentan, bosentan, macitentan), PDE5 inhibitors (e.g., sildenafil, tadalafil, vardenafil), soluble guanylate cyclase (e.g., riociguat), prostacyclin (PGI2) analogues (e.g., epoprostenol, iloprost, treprostinil, beraprost), and PGI2 receptor agonists (e.g., selexipag).2,12 Medications for the treatment of patients with PAH are also available as inhaled or parenteral formulations of prostanoids and as parenteral formulations of activin signalling inhibitors (e.g., sotatercept).12
Why Is It Important to Do This Review?
Pharmacologic monotherapy may not be consistently effective in treating all patients with PAH. Combination therapy with medications that target different pathways may potentially increase overall therapeutic effects. Evidence has shown that combination therapy with 2 oral medications (i.e., an ERA and a PDE5 inhibitor) is more effective than monotherapy.2 However, most studies have investigated sequential add-on therapies, while fewer studies have examined the effects of initial combination therapy on clinical outcomes.2
Objective
To support decision-making about the relative effects of initial dual therapy on clinical outcomes in patients with PAH, we prepared this Rapid Review to summarize and critically appraise the available studies on the clinical effectiveness and safety of dual therapy for the initial treatment of adult patients with previously untreated PAH.
Research Question
What is the clinical effectiveness and safety of pharmacologic dual therapy for the initial treatment of adult patients with newly diagnosed or previously untreated PAH?
Methods
Literature Search Methods
An information specialist conducted a literature search on key resources (i.e., MEDLINE, Embase, the Cochrane Database of Systematic Reviews, the International HTA Database, and the websites of health technology assessment agencies in Canada and internationally) as well as a focused internet search. The search approach was customized to retrieve a limited set of results, balancing comprehensiveness with relevance. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. Search concepts were developed based on elements of the research questions and selection criteria. The main search concepts were dual therapy and pulmonary arterial hypertension. Search filters were applied to limit retrieval to health technology assessments, systematic reviews, meta-analyses, indirect treatment comparisons, randomized controlled trials (RCTs), or controlled clinical trials. The search was completed on August 6, 2025, and was limited to English-language documents published since January 1, 2015, as CDA-AMC had previously conducted a Therapeutic Review entitled Drugs for Pulmonary Arterial Hypertension: Comparative Efficacy, Safety, and Cost-Effectiveness in 2015.13 The search strategy is available on request.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. Articles were included if they were made available after the publication of the 2015 CDA-AMC Therapeutic Review.13 The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
|---|---|
Population | Adults (aged ≥ 18 years) with newly diagnosed or previously untreated PAH Subgroups: 1. adults with idiopathic PAH 2. adults with heritable PAH 3. adults with drug- or toxin-induced PAH 4. adults with PAH associated with various conditions including connective tissue diseases, HIV infection, portal hypertension, and congenital heart disease 5. adults with PAH who are long-term responders to calcium channel blockers 6. adults with PAH with venous and/or capillary involvement Risk groups: Low risk, intermediate risk, high risk |
Interventions | Initial pharmacologic dual therapy |
Comparators | Pharmacologic monotherapy, pharmacologic combination therapy, or placebo |
Outcomes | Clinical effectiveness (e.g., disease progression, hospitalization for worsening PAH, need for transplant or septostomy, overall survival) Safety (e.g., AEs, SAEs, contraindications, deaths, treatment discontinuations due to AEs) |
Study designs | SRs, RCTs |
AE = adverse event; PAH = pulmonary arterial hypertension; RCT = randomized controlled trial; SAE = serious adverse event; SR = systematic review.
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1 or were published before 2015. Studies with sequential add-on combination therapy were excluded.
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the Downs and Black checklist14 for randomized studies.
Summary of Evidence
Quantity of Research Available
A total of 523 citations were identified in the literature search. Following the screening of titles and abstracts, 491 citations were excluded and 32 potentially relevant reports from the electronic search were retrieved for full-text review. No potentially relevant publications were found in the grey literature search. Of the potentially relevant articles, 27 were excluded for various reasons and 5 (of which 3 reported on the same study) met the inclusion criteria and were included in this report. These articles reported results from RCTs. Appendix 1 presents the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA)15 flow chart of the study selection.
Summary of Study Characteristics
Appendix 2 provides details regarding the characteristics of the included studies16-18 (Table 2).
Study Design
Three RCTs16-18 were included to answer the research question. These were the AMBITION study by Galie et al.,16 the TRITON study by Chin et al.,17 and the A DUE study by Grunig et al.18 Two subgroup analysis studies19,20 of the AMBITION study were also included.
The AMBITION study16 was a multicentre, randomized, double-blind, parallel, placebo-controlled trial conducted over a 24-week period. Patients were randomized in a 2:1:1 ratio to combination therapy with ambrisentan plus tadalafil, ambrisentan plus placebo, or tadalafil plus placebo. The study was published in 2015.
The TRITON study17 was a multicentre, randomized, double-blind, parallel, placebo-controlled trial conducted over a 26-week period. Patients were randomized in a 1:1 ratio to triple therapy (macitentan, tadalafil, and selexipag) or dual therapy (macitentan, tadalafil, and placebo). The study was published in 2021.
The A DUE study18 was a multicentre, randomized, double-blind, parallel, placebo-controlled trial conducted over a 16-week period. Patients were randomized in a 2:1:1 ratio to a fixed-dose combination of macitentan and tadalafil, macitentan, or tadalafil. The study was published in 2024.
Country of Origin
All 3 RCTs16-18 had study sites in multiple countries, including Canada. The AMBITION study16 was conducted in 14 countries, the TRITON study17 in 15 countries, and the A DUE study18 in 16 countries.
Patient Population
In the included RCTs,16-18 the mean age of patients ranged from 50 to 54 years, most patients were female (ranging from 76% to 78%), and most had idiopathic PAH (ranging from 47% to 53%) or CTD-associated PAH (ranging from 34% to 38%). About 75% of CTD-associated PAH cases are related to systemic sclerosis (SSc), with these patients having a poorer prognosis compared with other CTD cases.16 All patients in both the AMBITION study16 and the TRITON study17 were those with newly diagnosed PAH, while patients in the A DUE study18 were either naive to PAH-specific treatment (53%) or were receiving a stable therapeutic dose of an ERA or PDE5 inhibitor as monotherapy (47%) for at least 3 months. Patients in the AMBITION study16 had WHO FC II (31%) or III (69%) symptoms of PAH, and those in the TRITON study17 had WHO FC I or II (20%) or III or IV (80%; numbers of FC IV patients were 1 in the triple therapy group and 5 in the dual therapy group) symptoms of PAH. In the A DUE study,18 patients in the combination therapy group were more commonly classified as WHO FC II (60.7%), while those in the macitentan group and tadalafil group were more commonly classified as WHO FC III (68.6% and 58.6%, respectively).
With respect to race, most patients were white in the AMBITION study (89.0%),16 the TRITON study (85.0%),17 and the A DUE study (62.0%).18
Interventions and Comparators
In the AMBITION study,16 patients were randomized to receive once-daily initial combination therapy with ambrisentan 10 mg plus tadalafil 40 mg, ambrisentan 10 mg plus placebo, or tadalafil 40 mg plus placebo.
In the TRITON study,17 patients were randomized to receive initial triple therapy (macitentan 10 mg once daily, tadalafil 20 mg once daily, and selexipag 200 mcg to 1,600 mcg twice daily) or initial dual therapy (macitentan 10 mg once daily, tadalafil 20 mg once daily, and placebo).
In the A DUE study,18 patients were randomized to receive a fixed-dose combination of macitentan and tadalafil (single tablet), macitentan 10 mg once daily, or tadalafil 40 mg once daily. Patients were given matching relevant placebos for the combination, macitentan, or tadalafil to maintain blinding.
Outcomes
The primary clinical outcome of the AMBITION study16 was first event of clinical failure, a time-to-event analysis, while the primary outcome of the TRITON study17 and the A DUE study18 was pulmonary vascular resistance (PVR), expressed as a ratio of baseline. Secondary clinical outcomes in all 3 RCTs included changes in 6MWD, absence of worsening of WHO FC categorization from baseline, changes in NT-proBNP levels, and changes in other hemodynamic variables. Other secondary clinical outcomes included satisfactory clinical response, disease progression event, and changes in cardiopulmonary and cardiovascular symptom domain scores in the AMBITION study,16 the TRITON study,17 and the A DUE study,18 respectively. Safety outcomes in all 3 studies16-18 were AEs, serious AEs (SAEs), tolerability (withdrew from the study due to AEs), and death. Definitions and descriptions of the outcome measures are as follows:
First event of clinical failure: First occurrence of death, hospitalization for worsening PAH, disease progression, or unsatisfactory long-term clinical response.
Satisfactory clinical response: An increase of 10% from baseline in the 6MWD, with a reduction in symptoms to, or maintenance of, WHO FC I or II, and no events of worsening clinical condition before or at the week 24 visit.
Disease progression event: First occurrence of all-cause death; hospitalization for worsening PAH; initiation of prostacyclin, a prostacyclin analogue, or prostacyclin receptor agonist for worsening PAH; or clinical worsening, defined as a postbaseline decrease in 6MWD of more than 15% from the highest 6MWD obtained at or after screening and FC III or IV (both conditions confirmed at 2 consecutive postbaseline visits 1 to 21 days apart).
PVR: Measured by right heart catheterization, expressed as a ratio of baseline.
Absence of worsening of WHO FC from baseline: Assessment and classification of severity of PAH based on a patient’s functional limitations during physical activity.
PAH–Symptoms and Impact questionnaire: A questionnaire designed to assess the symptoms and impacts of PAH in patients. It includes 23 items: 11 symptom items and 11 impact items, plus 1 item on oxygen use. It measures symptoms experienced in the past 24 hours and impacts experienced in the past 7 days, with higher scores indicating more severe symptoms or impacts.
6MWD: Having a patient walk back and forth along a 30-metre (100-foot) corridor for 6 minutes, with the total distance covered recorded in metres.
NT-proBNP and other hemodynamics variables: Measured by blood test.
Summary of Critical Appraisal
Reporting
The authors of the included studies16-18 clearly described the objective of each study, the intervention of interest, the main outcomes, patient characteristics at baseline, and the main findings of the study. Actual P values and AEs of the intervention were reported. Protocols of these studies16-18 were published with no major changes while conducting the study, suggesting that reporting bias was low.
External Validity
Patients included in all 3 studies16-18 were from multiple countries, mostly in Europe and North America, including Canada. They mainly had idiopathic PAH or CTD-associated PAH and were of WHO FC II and III. The treatment settings (i.e., hospitals) appeared to be representative of the treatment received by most patients. As such, the patient populations and treatment settings were generalizable to the Canadian context.
Internal Validity: Bias
Each included study16-18 was a randomized, double-blind, placebo-controlled trials in which all patients were followed for the same period of time, suggesting a low risk of selection bias. Although the studies16-18 were double-blinded, there is recognition that specific AEs related to treatment with ERAs (ambrisentan, macitentan), PDE5 inhibitor (tadalafil), and prostacyclin receptor agonists (selexipag) could jeopardize the blinding and may have led to some risk of detection bias. Statistical tests were used appropriately, and the main outcome measures were accurate and reliable. However, there was no adjustment for multiple testing of the secondary outcomes in any of the included studies,16-18 which means there is a higher probability of statistical significance by chance alone, increasing the risk a false-positive result (type I error). In the AMBITION study,16 adherence with interventions was relatively moderate, as 83%, 76%, and 77% of patients in the dual therapy group, ambrisentan group, and tadalafil group completed the study, respectively, suggesting a risk of attrition bias. Adherence was relatively high in the TRITON study17 and the A DUE study18 as 94% and 95% of patients completed the studies, respectively. The primary end points in all included studies16-18 were measured accurately.
Internal Validity: Confounding
In each included study,16-18 patients in the intervention groups appeared to have been recruited from the same populations and over the same periods of time, and methods of randomization and allocation concealment (using the Interactive Response Technology system) were described. There were no group differences in demographic characteristics of the randomized patients in the AMBITION study16 or the TRITON study.17 In the A DUE study,18 differences between groups classified as WHO FC class II and III may have contributed to confounding the findings that favoured the combination therapy over monotherapies. Sample size calculation was performed in all included studies.16-18 Primary and secondary outcomes were analyzed using the full analysis set, which consisted of all randomized patients who received at least 1 dose of study treatment.16-18 The safety set included all randomized patients who received at least 1 dose of study treatment, and patients were evaluated according to study treatment received.16-18
Additional details regarding the strengths and limitations of included studies are provided in Appendix 3.
Summary of Findings
Appendix 4 presents the main study findings, which are summarized by outcome.
Pulmonary Vascular Resistance
In the TRITON study,17 PVR decreased from baseline to week 26 by 54% in the initial triple therapy (macitentan, tadalafil, and selexipag) group and by 52% in the initial dual therapy (macitentan, tadalafil, and placebo) group. The corresponding treatment effect showed no statistically significant difference between groups (Table 4).
In the A DUE study,18 PVR decreased in all groups from baseline to week 16, with a decrease of similar magnitude in the macitentan (23%) and tadalafil (22%) groups, and a greater decrease in the initial dual therapy (44%) group. The treatment effects showed that the reduction in PVR in the dual therapy group was statistically significantly greater compared to reductions in PVR in groups receiving monotherapies. The findings were consistent between patients who were treatment-naive and those receiving prior monotherapy (an ERA or a PDE5 inhibitor) at baseline (Table 4).
6-Minute Walk Distance
In the TRITON study,17 the mean 6MWD between baseline and week 26 increased by 55.0 m for the triple therapy (macitentan, tadalafil, and selexipag) group and by 56.4 m for the dual therapy (macitentan, tadalafil, and placebo) group. The treatment effect showed no statistically significant difference between groups (Table 5).
In the AMBITION study,16 dual therapy (ambrisentan and tadalafil) was associated with greater improvement in the median 6MWD between baseline and week 24 (49.0 m) compared to monotherapies (27 m for the ambrisentan group and 23 m for the tadalafil group). The differences between dual therapy and monotherapies were statistically significant (Table 5).
Subgroup analyses in the AMBITION study19 by FC symptoms at baseline revealed that patients with FC III symptoms assigned to dual therapy had a larger increase in median 6MWD compared to the pooled monotherapy group (52 m versus 22 m; P < 0.001). In patients with FC II symptoms at baseline, the difference between groups for improvement in median 6MWD was not statistically significant (40 m versus 32 m; P = 0.37) (Table 12).
Subgroup analyses in the AMBITION study20 by disease etiology showed that increases in median 6MWD between baseline and week 24 were greater in patients receiving dual therapy than in those receiving monotherapy in the CTD-PAH (41 m versus 23 m) and SSc-associated PAH (34 m versus 8 m) populations (Table 12). Statistical comparisons between groups were not reported.
In the A DUE study,18 the group receiving a fixed-dose combination dual therapy (macitentan and tadalafil) showed greater improvement in mean 6MWD between baseline and week 16 compared to groups receiving monotherapies (53.0 m versus 39.0 m for dual therapy versus macitentan, and 43.4 m versus 16.0 m for dual therapy versus tadalafil). However, the differences between groups receiving dual therapy or macitentan monotherapy and between those receiving dual therapy or tadalafil monotherapy were not statistically significant (Table 5).
Composite End Point: First Event of Clinical Failure
In the AMBITION study,16 fewer patients (18%) in the combination therapy (ambrisentan and tadalafil) group had a primary end point event up to the time of the final assessment visit compared to the ambrisentan monotherapy group (34%) or the tadalafil monotherapy group (28%). The hazard ratios for dual therapy versus monotherapies were statistically significant (Table 6). Hospitalization rates for worsening PAH were the main contributor, with the largest observed difference occurring between the dual therapy group and pooled monotherapy group (4% versus 12%) (Table 11). Nine patients (4%) died in the dual therapy group and 8 patients (3%) died in the pooled monotherapy group (Table 11). Disease progression occurred in 10 patients (4%) and 16 patients (6%) in the dual therapy group and the pooled monotherapy group, respectively (Table 11).
Subgroup analyses in the AMBITION study19 by WHO FC symptoms at baseline showed that the risk of clinical failure events was reduced by 79% for patients in WHO FC II and by 42% for patients in WHO FC III in the dual therapy group compared with those in the pooled monotherapy group (Table 12).
Subgroup analyses in the AMBITION study20 by disease etiology showed that the risk of clinical failure events was 52% lower with dual therapy compared with pooled monotherapy in patients with CTD-PAH and 54% lower with dual therapy compared with pooled monotherapy in patients with SSc-related PAH (Table 12).
Risk stratification in the AMBITION study20 classified patients into low-risk (27 patients, 12.5%), intermediate-risk (179 patients, 82.9%), and high-risk (10 patients, 4.6%) categories at baseline. In the group at low risk, there were no clinical failure events in the dual therapy group. Most clinical failure events occurred in the group at intermediate risk, for whom the risk of clinical failure was 48% lower with dual therapy compared with pooled monotherapy. The result in the group at high risk was uncertain due to small sample size (4 patients with dual therapy and 6 patients with pooled monotherapy) (Table 12).
Composite End Point: Satisfactory Clinical Response
In the AMBITION study,16 the percentage of patients with satisfactory clinical response was statistically significantly different between the dual therapy and tadalafil monotherapy groups, but not between the dual therapy and ambrisentan monotherapy groups (Table 6).
Composite End Point: First Event of Disease Progression
In the TRITON study,17 fewer patients (13.0%) in the triple therapy group had a first event of disease progression compared to 21.8% in the dual therapy group. The difference was driven by the proportions of patients hospitalized for PAH worsening (8.1% versus 15.3%) and all-cause deaths (0% versus 3.2%). However, the hazard ratio in a time-to-event analysis showed no statistically significant difference between groups receiving triple therapy or dual therapy (Table 6).
Absence of Worsening in WHO FC
In all included studies,16-18 the percentages of patients without worsening of WHO FC (i.e., with improved or no change in FC level) at the end of treatment were not different between groups (Table 7).
Cardiopulmonary and Cardiovascular Symptoms Domain Scores
In the A DUE study,18 there were no differences between fixed-dose combination dual therapy (macitentan and tadalafil) and monotherapies in improvements in cardiopulmonary and cardiovascular symptoms domain scores assessed using the PAH–Symptoms and Impact questionnaire (Table 8).
NT-proBNP Levels
In the AMBITION study16 and the A DUE study,18 reductions in NT-proBNP levels were observed in all groups, with the largest reductions found in the dual therapy (ambrisentan and tadalafil, or macitentan and tadalafil) groups compared with monotherapy groups. Differences in treatment effects were statistically significant between groups (Table 9).
Subgroup analyses in the AMBITION study19 by FC symptoms at baseline showed that NT-proBNP levels from baseline to week 24 decreased by 43% in patients with FC III symptoms who were randomized to dual therapy compared with those in the pooled monotherapy group. The reductions in NT-proBNP for patients with FC II symptoms were similar between groups (Table 12).
Subgroup analyses in the AMBITION study20 by disease etiology showed that the decrease in NT‑proBNP levels from baseline to week 24 was greater in patients receiving dual therapy than those receiving monotherapy in the CTD-PAH (58% versus 44%) and SSc-associated PAH (58% versus 40%) populations (Table 12). Statistical comparisons between groups were not reported.
In the TRITON study,17 there was no difference in the reduction of NT-proBNP levels between groups receiving triple therapy or dual therapy (Table 9).
Other Hemodynamic Parameters
In the TRITON study,17 there were no differences between groups receiving triple therapy or dual therapy in the reduction of hemodynamic parameters (Table 10).
In the A DUE study,18 dual therapy was associated with greater reductions in other hemodynamic parameters, concordant with the findings of the primary outcome of PVR, compared with monotherapies. However, the differences between groups were not subjected to statistical comparisons (Table 10).
Safety
In the AMBITION study16 and the A DUE study,18 peripheral edema, headache, nasal congestion, anemia, dizziness, and hypotension occurred more frequently in the dual therapy group than in either monotherapy group. There were no differences between groups in the rates of SAEs and the rates of discontinuation of study drug due to AEs. PH and pneumonia were the most common SAEs reported in the AMBITION study.16 Dyspnea and peripheral edema were the most common AEs leading to treatment discontinuation reported in the AMBITION study.16 Seventeen patients died in the AMBITION study16 (9 patients [4%] receiving dual therapy, 2 patients [2%] receiving ambrisentan monotherapy, and 6 patients [5%] receiving tadalafil monotherapy). Three deaths were reported in the A DUE study,18 and all occurred among patients receiving dual therapy (Table 11).
In the TRITON study,17 headache, diarrhea, nausea, pain in extremities, pain in jaw, vomiting, and dyspnea occurred more frequently in the triple therapy group than in the dual therapy group. The rates of AEs leading to treatment discontinuation were similar in both groups. The rates of SAEs were higher in the triple therapy group than in the dual therapy group. Common SAEs that occurred more frequently in the triple therapy group than in the dual therapy group included infections and infestations; respiratory, thoracic, and mediastinal disorders; gastrointestinal disorders; and blood and lymphatic system disorders. Two patients (1.7%) and 9 patients (7.1%) died in the triple therapy group and dual therapy group, respectively (Table 11).
Limitations
Evidence Gaps
Most outcomes assessed by the included studies16-18 focused mainly on clinical efficacy and safety of dual therapy versus monotherapy, or of triple therapy versus dual therapy. Evidence on the effect of initial combination therapy on health-related quality of life (HRQoL), an outcome important to patients with PAH, was not reported in the included studies. As such, a conclusion regarding the effect of dual therapy or triple therapy on HRQoL of patients with PAH could not be made.
Generalizability
The included studies16-18 compared initial dual therapy of an ERA (ambrisentan or macitentan) and a PDE5 inhibitor (tadalafil) versus monotherapy in patients with newly diagnosed PAH. It was unclear whether the findings in the AMBITION study16 and the A DUE study18 can be extrapolated to the use of other drugs in the same classes. It was also not known if dual therapy with drugs from other classes of approved therapies for PAH would produce similar results. Regarding the study population, the findings have limited generalizability to patients with WHO FC IV PAH symptoms or to those patients with rare PAH etiologies, such as heritable disease, drug- or toxin-induced PAH, HIV infection, corrected congenital heart disease, or portal hypertension. The findings of the included studies also had limited generalizability to patients who are not white, as other racial groups were underrepresented in the study populations.
Certainty of Evidence
The main study limitation of the findings in all included studies16-18 was the lack of adjustment for multiple testing of the secondary outcomes, which means there is a higher probability of statistical significance by chance alone, increasing the risk a false-positive result (type I error).
The A DUE study18 was designed and powered for the changes in the primary outcome (PVR) that limited the number of patients in treatment groups with a relatively short time of treatment duration. The study was not powered to detect statistically significant differences in secondary outcomes.
Despite the improvements with dual therapy demonstrated across various outcomes, the non–statistically significant differences for the changes in WHO FC among study groups in the AMBITION study16 and the A DUE study18 at end of treatment prevented the drawing of a meaningful conclusion.
Conclusions and Implications for Decision- or Policy-Making
This review included 3 RCTs16-18 that were relevant to the research question.
Both initial triple therapy (macitentan, tadalafil, and selexipag) and initial dual therapy (macitentan and tadalafil) improved patients’ hemodynamic parameters (including PVR) and other clinical variables by the end of treatment in patients with newly diagnosed PAH, with no differences between groups.
Initial treatment with dual therapy with ambrisentan and tadalafil, or fixed-dose combination therapy with macitentan and tadalafil, had significant advantages over monotherapy in various clinical outcomes including PVR and the risk of the composite outcome of clinical failure for patients who were treatment-naive at low to intermediate risk with idiopathic PAH or CTD-associated PAH with WHO FC II or III symptoms.
Tolerability was similar among patients receiving dual therapy or monotherapies, and the safety of dual therapy was consistent with the safety profiles of each monotherapy. Some common AEs such as peripheral edema, headache, nasal congestion, anemia, dizziness, and hypotension occurred more frequently in the dual therapy group than either monotherapy group.
Considerations for Future Research
Future studies could be conducted to evaluate dual therapy with other ERAs and PDE5 inhibitors or additional drug classes to explore whether higher efficacy and fewer side effects can be achieved. The long-term efficacy and safety of initial dual therapy should also be assessed through long-term extension studies.
Implications for Clinical Practice
The findings in this review suggest that combination therapy with 2 oral medications, an ERA and a PDE5 inhibitor, provides better treatment outcomes for patients with previously untreated or newly diagnosed PAH.
References
1.Maron BA, Abman SH, Elliott CG, et al. Pulmonary Arterial Hypertension: Diagnosis, Treatment, and Novel Advances. Am J Respir Crit Care Med. 2021;203(12):1472-1487. PubMed
2.Jin Q, Chen D, Zhang X, et al. Medical Management of Pulmonary Arterial Hypertension: Current Approaches and Investigational Drugs. Pharmaceutics. 2023;15(6). PubMed
3.Hirani N, Brunner NW, Kapasi A, et al. Canadian Cardiovascular Society/Canadian Thoracic Society Position Statement on Pulmonary Hypertension. Can J Cardiol. 2020;36(7):977-992. PubMed
4.PAH EUROPE. 2020; https://www.phaeurope.org/about-ph/classification-and-who-functional-class/#:~:text=The%20World%20Health%20Organization%20(WHO,affecting%20a%20patient's%20daily%20life. Accessed 20 August, 2025.
5.Galiè N, Humbert M, Vachiery JL, et al. 2015 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension: The Joint Task Force for the Diagnosis and Treatment of Pulmonary Hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS): Endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC), International Society for Heart and Lung Transplantation (ISHLT). Eur Respir J. 2015;46(4):903-975. PubMed
6.Humbert M, Sitbon O, Yaïci A, et al. Survival in incident and prevalent cohorts of patients with pulmonary arterial hypertension. Eur Respir J. 2010;36(3):549-555. PubMed
7.Benza RL, Miller DP, Gomberg-Maitland M, et al. Predicting survival in pulmonary arterial hypertension: insights from the Registry to Evaluate Early and Long-Term Pulmonary Arterial Hypertension Disease Management (REVEAL). Circulation. 2010;122(2):164-172. PubMed
8.Thenappan T, Glassner C, Gomberg-Maitland M. Validation of the pulmonary hypertension connection equation for survival prediction in pulmonary arterial hypertension. Chest. 2012;141(3):642-650. PubMed
9.Hoeper MM, Kramer T, Pan Z, et al. Mortality in pulmonary arterial hypertension: prediction by the 2015 European pulmonary hypertension guidelines risk stratification model. Eur Respir J. 2017;50(2). PubMed
10.Kylhammar D, Kjellström B, Hjalmarsson C, et al. A comprehensive risk stratification at early follow-up determines prognosis in pulmonary arterial hypertension. Eur Heart J. 2018;39(47):4175-4181. PubMed
11.Hoeper MM, Pausch C, Olsson KM, et al. COMPERA 2.0: a refined four-stratum risk assessment model for pulmonary arterial hypertension. Eur Respir J. 2022;60(1). PubMed
12.Chin KM, Gaine SP, Gerges C, et al. Treatment algorithm for pulmonary arterial hypertension. Eur Respir J. 2024;64(4). PubMed
13.CDA-AMC. Drugs for Pulmonary Arterial Hypertension. 2015; https://www.cda-amc.ca/drugs-pulmonary-arterial-hypertension. Accessed 10 September, 2025.
14.Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377-384. PubMed
15.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
16.Galie N, Barbera JA, Frost AE, et al. Initial Use of Ambrisentan plus Tadalafil in Pulmonary Arterial Hypertension. N Engl J Med. 2015;373(9):834-844. PubMed
17.Chin KM, Sitbon O, Doelberg M, et al. Three- Versus Two-Drug Therapy for Patients With Newly Diagnosed Pulmonary Arterial Hypertension. J Am Coll Cardiol. 2021;78(14):1393-1403. PubMed
18.Grunig E, Jansa P, Fan F, et al. Randomized Trial of Macitentan/Tadalafil Single-Tablet Combination Therapy for Pulmonary Arterial Hypertension. J Am Coll Cardiol. 2024;83(4):473-484. PubMed
19.White RJ, Vonk-Noordegraaf A, Rosenkranz S, et al. Clinical outcomes stratified by baseline functional class after initial combination therapy for pulmonary arterial hypertension. Respir Res. 2019;20(1):208. PubMed
20.Kuwana M, Blair C, Takahashi T, Langley J, Coghlan JG. Initial combination therapy of ambrisentan and tadalafil in connective tissue disease-associated pulmonary arterial hypertension (CTD-PAH) in the modified intention-to-treat population of the AMBITION study: post hoc analysis. Ann Rheum Dis. 2020;79(5):626-634. PubMed
Appendix 1: Selection of Included Studies
Please note that this appendix has not been copy-edited.
Figure 1: PRISMA15 Flow Chart of Study Selection
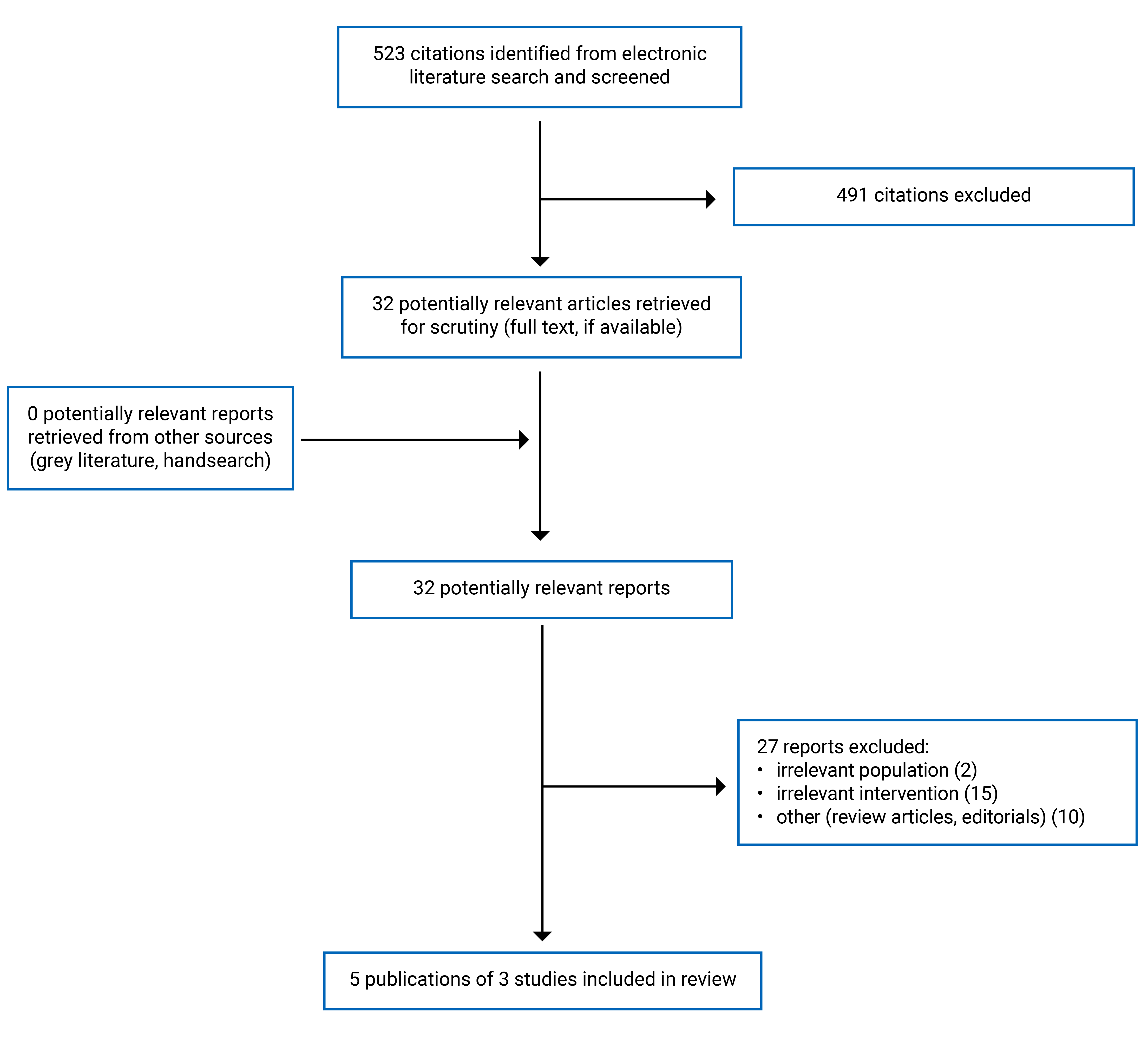
PRISMA = Preferred Reporting Items for Systematic reviews and Meta-Analyses.
Appendix 2: Characteristics of Included Publications
Table 2: Characteristics of Included Primary Clinical Studies
Study citation, country, funding source | Study design | Population characteristics | Intervention and comparator(s) | Clinical outcomes, treatment period |
|---|---|---|---|---|
Galie et al. (2015)16 Multinational (14 countries including Canada) Funding source: Gilead Sciences and GlaxoSmithKline Additional studies of subgroup analyses: White et al. (2019)19 Kuwana et al. (2020)20 | AMBITION study: Multicentre, randomized, double-blind, phase III to IV study | Adult patients (≥ 18 years) with newly diagnosed PAH Sex, %:
Mean age (SD), years: 54.4 (14.6) Race, n (%):
Median time from diagnosis of PAD, days: 22.5 PAH etiology, %:
Mean (SD) PAP, mm Hg: 48.7 (12.5) Mean (SD) 6MWD, m: 352.6 (89.9) WHO FC, %:
Mean PVR (SD), dynes.sec/cm5: 824.9 (435) Median (range) NT-proBNP, ng/L: 978.0 (331 to 2,187) | Intervention:
Comparator:
Maintenance period: Dual therapy: 10 mg ambrisentan once daily; 40 mg tadalafil once daily Monotherapy:
| Primary end point:
Secondary end points:
Safety:
Treatment period: 24 weeks |
Chin et al. (2021)17 Multinational (15 countries including Canada) Funding source: Actelion Pharmaceuticals Ltd. | TRITON study: Multicentre, double-blind, randomized, placebo-controlled phase IIIb study | Adult patients (≥ 18 years) with newly diagnosed PAH Sex, %:
Mean age (SD), years: 51.9 (13.7) Race, n (%):
Mean time (SD) from diagnosis of PAD, days: 21.9 (29.8) PAH etiology, %:
Mean (SD) PAP, mm Hg: 52.1 (10.6) Mean (SD) 6MWD, m: 346 (118.7) WHO FC, %:
Mean PVR (SD), Wood unitsi: 12.0 (4.7) | Intervention: Triple therapy (macitentan, tadalafil, selexipag) (n = 123) Comparator: Dual therapy (macitentan, tadalafil, placebo) (n = 124) Maintenance period: Triple therapy: 10 mg macitentan once daily; 40 mg tadalafil once daily; 200 mcg to 1,600 mcg selexipag twice daily Dual therapy: 10 mg macitentan once daily; 40 mg tadalafil once daily | Primary end point: PVR (expressed as ratio of baseline) Secondary end points:
Safety:
Treatment period: 26 weeks |
Grunig et al. (2024)18 Multinational (16 countries/ territories including Canada) Funding source: Actelion Pharmaceuticals Ltd., a Janssen Pharmaceutical company of Jonhson and Jonhson | A DUE study: Multicentre, double-blind, randomized, active-controlled, triple-dummy, parallel group, group sequential, adaptive phase III study | Adult patients (≥ 18 years) with PAH Sex, %:
Mean age (SD), years: 50.4 (15.1) Race, n (%):
Mean time (SD) from diagnosis of PAH, years:
PAH etiology, %:
Mean (SD) 6MWD, m: 353.8 (85.1) WHO FC group II, %:
WHO FC group III, %:
Mean PVR (SD), dynes.sec/cm5: 840.4 (463.4) Median (range) NT-proBNP, ng/L:
PAH therapy at baseline, %:
| Intervention: Dual therapy (n = 107) Comparator:
Maintenance period:
| Primary end point: PVR (expressed as ratio of baseline) Secondary end points:
Exploratory end points:
Safety:
Treatment period: 16 weeks |
6MWD = 6-minute walk distance; AE = adverse event; CTD = connective tissue disease; ERA = endothelin receptor antagonist; FC = functional class; NT-proBNP = N-terminal pro–brain natriuretic peptide; PAD = peripheral artery disease; PAH = pulmonary arterial hypertension; PAP = pulmonary artery pressure; PDE5 = phosphodiesterase 5; PVR = pulmonary vascular resistance; SAE = serious adverse event; SD = standard deviation.
Note: This table has not been copy-edited.
aDefined as the first occurrence of a composite end point of death, hospitalization for worsening PAH, disease progression, or unsatisfactory long-term clinical response.
bDefined as an increase of 10% from baseline in the 6-minute walk distance, with a reduction in symptoms to, or maintenance of, WHO FC I or II and no events of worsening clinical condition before or at the week 24 visit.
cDefined as first occurrence of all-cause death; hospitalization for worsening PAH; initiation of prostacyclin, a prostacyclin analogue, or prostacyclin receptor agonist for worsening PAH; or clinical worsening, defined as a postbaseline decrease in 6MWD of > 15% from the highest 6MWD obtained at or after screening and FC III or IV (both conditions confirmed at 2 consecutive postbaseline visits 1 to 21 days apart)
dA questionnaire designed to assess the symptoms and impacts of PAH in patients. It includes 23 items: 11 symptom items and 11 impact items, plus an item on oxygen use. It measures symptoms experienced in the past 24 hours and impacts experienced in the past 7 days, with higher scores indicating more severe symptoms or impacts.
eIncluded heritable (3%), drug- or toxin-induced (3%), associated with HIV infection (2%), and associated with corrected congenital heart disease (2%).
fIncluded heritable (6.5%), drug- or toxin-induced (8.1%), associated with HIV infection (3.2%), and associated with corrected congenital heart disease (1.2%).
gIncluded heritable (4.8%), drug- or toxin-induced (1.6%), associated with HIV infection (3.2%), associated with corrected congenital heart disease (3.2%), and associated with portal hypertension (1.6%).
hPreviously received a stable dose of an ERA or a PDE5 inhibitor for at least 3 months before baseline right heart catheterization.
iTo convert from Wood units to dynes·sec/cm5, multiply by 80.
jNumber of FC IV patients: 1 triple, 5 double.
Appendix 3: Critical Appraisal of Included Publications
Please note that this appendix has not been copy-edited.
Table 3: Strengths and Limitations of Clinical Studies Using the Downs and Black Checklist14
Strengths | Limitations |
|---|---|
Galie et al. (2015)16 | |
Reporting:
External validity:
Internal validity – bias:
Internal validity – confounding:
| Internal validity – bias:
|
Chin et al. (2021)17 | |
Reporting:
External validity:
Internal validity – bias:
Internal validity – confounding:
| Internal validity – bias:
|
Grunig et al. (2024)18 | |
Reporting:
External validity:
Internal validity – bias:
Internal validity – confounding:
| Reporting:
Internal validity – bias:
Internal validity – confounding:
|
AE = adverse event; FC = functional class; PAH = pulmonary arterial hypertension; PVR = pulmonary vascular resistance.
Appendix 4: Main Study Findings
Please note that this appendix has not been copy-edited.
Table 4: Summary of Findings by Outcome — PVR
Study citation and study design | Method of measurement | Intervention vs. comparator | Results |
|---|---|---|---|
Chin et al. (2021)17 TRITON study RCT | Right heart catheterization Expressed as a ratio of baseline | Triple therapy (macitentan, tadalafil, selexipag) vs. dual therapy (macitentan, tadalafil, placebo) | Decreased from baseline to week 26:
Geometric LS Means Ratioa (95% CI); P value = 0.96 (0.86 to 1.07); 0.42 |
Grunig et al. (2024)18 A DUE study RCT | Right heart catheterization Expressed as a ratio of baseline | Dual therapy vs. macitentan | Decreased from baseline to week 16:
Geometric LS Means Ratioa (95% CL):
|
Dual therapy vs. tadalafil | Decreased from baseline to week 16:
Geometric LS Means Ratio (95% CL):
|
CI = confidence interval; CL = confidence limit; ERA = endothelin-1 receptor antagonist; LS = least squares; PDE5 = phosphodiesterase type 5; PVR = pulmonary arterial resistance; RCT = randomized controlled trial; vs. = versus.
aValues less than 1 favour intervention.
Table 5: Summary of Findings by Outcome — 6MWD
Study citation and study design | Method of measurement | Intervention vs. comparator | Results |
|---|---|---|---|
Galie et al. (2015)16 AMBITION study RCT | Having a patient walk back and forth along a 30-metre (100-foot) corridor for 6 minutes, with the total distance covered recorded in metres | Dual therapy vs. ambrisentan | Median (IQR) change from baseline; P value:
|
Dual therapy vs. tadalafil | Median (IQR) change from baseline; P value:
| ||
Chin et al. (2021)17 TRITON study RCT | Having a patient walk back and forth along a 30-metre (100-foot) corridor for 6 minutes, with the total distance covered recorded in metres | Triple therapy (macitentan, tadalafil, selexipag) vs. dual therapy (macitentan, tadalafil, placebo) | Increased from baseline to week 26:
LS Mean Change (95% CI) = −1.4 (−19.4 to 16.5) |
Grunig et al. (2024)18 A DUE study RCT | Having a patient walk back and forth along a 30-metre (100-foot) corridor for 6 minutes, with the total distance covered recorded in metres | Dual therapy vs. macitentan | Increased from baseline to week 16:
LS Mean Change (95% CL); P value:
|
Dual therapy vs. tadalafil | Increased from baseline to week 16:
LS Mean Change (95% CL); P value:
|
6MWD = 6-minute walk distance; CI = confidence interval; CL = confidence limit; IQR = interquartile range; LS = least squares; RCT = randomized controlled trial; vs. = versus.
Table 6: Summary of Findings by Outcome — Composite End Points
Study citation and study design | Method of measurement | Intervention vs. comparator | Results |
|---|---|---|---|
Galie et al. (2015)16 AMBITION study RCT | First event of clinical failurea | Dual therapy vs. ambrisentan | Patients with events, n (%):
HR (95% CI) = 0.48 (0.31 to 0.72); P < 0.001 |
Dual therapy vs. tadalafil | Patients with events, n (%):
HR (95% CI) = 0.53 (0.34 to 0.83); P = 0.005 | ||
Galie et al. (2015)16 AMBITION study RCT | Satisfactory clinical responseb | Dual therapy vs. ambrisentan | Patients with events, n (%):
OR (95% CI) = 1.42 (0.88 to 2.31); P = 0.15 |
Dual therapy vs. tadalafil | Patients with events, n (%):
OR (95% CI) = 1.72 (1.05 to 2.83); P = 0.03 | ||
Chin et al. (2021)17 TRITON study RCT | First event of disease progressionc | Triple therapy (macitentan, tadalafil, selexipag) vs. dual therapy (macitentan, tadalafil, placebo) | Patients with events, n (%):
HR (95% CI) = 0.59 (0.32 to 1.09) |
6MWD = 6-minute walk distance; CI = confidence interval; FC = functional class; HR = hazard ratio; OR = odds ratio; PAH = pulmonary arterial hypertension; RCT = randomized controlled trial; vs. = versus.
aDefined as the first occurrence of a composite end point of death, hospitalization for worsening PAH, disease progression, or unsatisfactory long-term clinical response.
bDefined as an increase of 10% from baseline in the 6-minute walk distance, with a reduction in symptoms to, or maintenance of, WHO FC I or II and no events of worsening clinical condition before or at the week 24 visit.
cDefined as first occurrence of all-cause death; hospitalization for worsening PAH; initiation of prostacyclin, a prostacyclin analogue, or prostacyclin receptor agonist for worsening PAH; or clinical worsening, defined as a postbaseline decrease in 6MWD of > 15% from the highest 6MWD obtained at or after screening and FC III or IV (both conditions confirmed at 2 consecutive postbaseline visits 1 to 21 days apart).
Table 7: Summary of Findings by Outcome — Absence of Worsening in WHO FC
Study citation and study design | Method of measurement | Intervention vs. comparator | Results |
|---|---|---|---|
Galie et al. (2015)16 AMBITION study RCT | Assessment and classification on severity of pulmonary hypertension based on a patient's functional limitations during physical activity | Dual therapy vs. ambrisentan | n (%); P value:
|
Dual therapy vs. tadalafil | n (%); P value:
| ||
Chin et al. (2021)17 TRITON study RCT | Assessment and classification on severity of pulmonary hypertension based on a patient's functional limitations during physical activity | Triple therapy (macitentan, tadalafil, selexipag) vs. dual therapy (macitentan, tadalafil, placebo) | Triple therapy: 99.2% Dual therapy: 97.5% OR (95% CI) = 3.2 (0.3 to 31.8) |
Grunig et al. (2024)18 A DUE study RCT | Assessment and classification on severity of pulmonary hypertension based on a patient's functional limitations during physical activity | Dual therapy vs. macitentan | Dual therapy: 30 (93.8) Macitentan: 17 (100) OR (95% CL); P value: All patients: 0.20 (0.00, 1.73); 0.216 |
Dual therapy vs. tadalafil | Dual therapy: 35 (89.7) Tadalafil: 21 (95.5) OR (95% CL); P value: All patients: 0.99 (0.08, 7.74); 1.000 |
CI = confidence interval; CL = confidence limit; LS = least squares; FC = functional class; OR = odds ratio; RCT = randomized controlled trial; vs. = versus.
Table 8: Summary of Findings by Outcome — Cardiopulmonary and Cardiovascular Symptoms Domain Scores
Study citation and study design | Method of measurement | Intervention vs. comparator | Results |
|---|---|---|---|
Grunig et al. (2024)18 A DUE study RCT | Cardiopulmonary Symptom Domain Score | Dual therapy vs. macitentan | Mean (SD) change from baseline: Dual therapy: −0.20 (0.39) Macitentan: −0.14 (0.48) LS Mean Change (95% CL); P value:
|
Dual therapy vs. tadalafil | Mean (SD) change from baseline: Dual therapy: −0.15 (0.40) Tadalafil: −0.13 (0.55) LS mean change (95% CL); P value:
| ||
Cardiovascular Symptom Domain Score | Dual therapy vs. macitentan | Mean (SD) change from baseline: Dual therapy: −0.15 (0.35) Macitentan: −0.14 (0.47) LS mean change (95% CL); P value:
| |
Dual therapy vs. tadalafil | Mean (SD) change from baseline: Dual therapy: −0.10 (0.32) Tadalafil: −0.18 (0.61) LS mean change (95% CL); P value:
|
CL = confidence limit; LS = least squares; RCT = randomized controlled trial; SD = standard deviation; vs. = versus.
Table 9: Summary of Findings by Outcome — NT-proBNP Levels
Study citation and study design | Method of measurement | Intervention vs. comparator | Results |
|---|---|---|---|
Galie et al. (2015)16 AMBITION study RCT | Blood test Expressed as % change from baseline | Dual therapy vs. ambrisentan | % change in geometric mean; P value: −67.2 vs. −56.2; 0.01 |
Dual therapy vs. tadalafil | % change in geometric mean; P value: −67.2 vs. −43.8; < 0.001 | ||
Chin et al. (2021)17 TRITON study RCT | Blood test Expressed as a ratio of baseline | Triple therapy (macitentan, tadalafil, selexipag) vs. dual therapy (macitentan, tadalafil, placebo) | Geometric LS means ratioa (95% CI) = 1.03 (0.77 to 1.37) |
Grunig et al. (2024)18 A DUE study RCT | Blood test Expressed as a ratio of baseline | Dual therapy vs. macitentan | Geometric LS means ratioa (95% CL); P value:
|
Dual therapy vs. tadalafil | Geometric LS means ratioa (95% CL); P value:
|
CI = confidence interval; CL = confidence limit; LS = least squares; NT-proBNP = N-terminal pro–brain natriuretic peptide; RCT = randomized controlled trial; vs. = versus.
aValues less than 1 favour intervention.
Table 10: Summary of Findings by Outcome — Other Hemodynamic Parameters
Study citation and study design | Outcomes | Intervention vs. comparator | Results |
|---|---|---|---|
Chin et al. (2021)17 TRITON study RCT | mPAP, mm Hg | Triple therapy (macitentan, tadalafil, selexipag) vs. dual therapy (macitentan, tadalafil, placebo) | LS mean change (95% CI): −0.72 (−2.8 to 1.4) |
Cardiac index, L/min/m2 | Triple therapy (macitentan, tadalafil, selexipag) vs. dual therapy (macitentan, tadalafil, placebo) | LS mean change (95% CI): 0.13 (−0.07 to 0.33) | |
TPR, mean (SD), Wood units | Triple therapy (macitentan, tadalafil, selexipag) vs. dual therapy (macitentan, tadalafil, placebo) | LS mean change (95% CI): 0.03 (−0.87 to 0.93) | |
mRAP, mean (SD), mm Hg | Triple therapy (macitentan, tadalafil, selexipag) vs. dual therapy (macitentan, tadalafil, placebo) | LS mean change (95% CI): −0.09 (−1.00 to 0.83) | |
SvO2, mean (SD), % | Triple therapy (macitentan, tadalafil, selexipag) vs. dual therapy (macitentan, tadalafil, placebo) | LS mean change (95% CI): −1.2 (−2.7 to 0.3) | |
Grunig et al. (2024)18 A DUE study RCT | SBP, mean (SD), Expressed as change from baseline | Dual therapy vs. macitentan | −7.2 (18.7) vs. −5.4 (17.5) |
Dual therapy vs. tadalafil | −6.6 (16.8) vs. −2.1 (19.1) | ||
mRAP, mean (SD), Expressed as change from baseline | Dual therapy vs. macitentan | −1.4 (5.0) vs. −0.3 (5.7) | |
Dual therapy vs. tadalafil | −0.5 (5.2) vs. 0.4 (3.3) | ||
mPAP, mean (SD), Expressed as change from baseline | Dual therapy vs. macitentan | −10.0 (8.6) vs. −3.6 (8.2) | |
Dual therapy vs. tadalafil | −9.2 (8.2) vs. −3.0 (6.1) | ||
PAWP, mean (SD), Expressed as change from baseline | Dual therapy vs. macitentan | 0.8 (4.0) vs. 0.6 (5.2) | |
Dual therapy vs. tadalafil | 1.3 (4.0) vs. 0.9 (4.0) | ||
PVR, mean (SD), dynes.s/cm5 Expressed as change from baseline | Dual therapy vs. macitentan | −370.5 (428.8) vs. −162.0 (240.3) | |
Dual therapy vs. tadalafil | −384.5 (396.2) vs. −180.8 (237.5) | ||
SVR, mean (SD), dynes.s/cm5 Expressed as change from baseline | Dual therapy vs. macitentan | −516.6 (586.2) vs. −367.3 (523.0) | |
Dual therapy vs. tadalafil | −577.7 (454.4) vs. −178.4 (628.7) | ||
TPR, mean (SD), dynes.s/cm5 Expressed as change from baseline | Dual therapy vs. macitentan | −443.1 (504.4) vs. −166.7 (290.3) | |
Dual therapy vs. tadalafil | −456.4 (452.8) vs. −180.4 (451.5) | ||
Cardiac index, mean (SD), (L/min/m2) Expressed as change from baseline | Dual therapy vs. macitentan | 0.52 (0.58) vs. 0.16 (0.62) | |
Dual therapy vs. tadalafil | 0.60 (0.5) vs. 0.15 (0. 6) | ||
SvO2, mean (SD), % Expressed as change from baseline | Dual therapy vs. macitentan | 4.8 (7.3) vs. 1.8 (7.1) | |
Dual therapy vs. tadalafil | 4.0 (7.0) vs. 2.4 (5.6) |
CI = confidence interval; LS = least squares; FC = functional class; mPAP = mean pulmonary arterial pressure; PAWP = pulmonary artery wedge pressure; PVR = pulmonary vascular resistance; mRAP = mean right atrial pressure; RCT = randomized controlled trial; SBP = systolic blood pressure; SD = standard deviation; SvO2 = mixed venous oxygen saturation; SVR = systemic vascular resistance; TPR = total pulmonary resistance; vs. = versus.
Table 11: Summary of Findings by Outcome — Safety
Study citation and study design | Outcomes | Intervention vs. comparator | Results (n, %) |
|---|---|---|---|
Galie et al. (2015)16 AMBITION study RCT | AEs leading to treatment discontinuation | ||
Any | Dual therapy vs. ambrisentan vs. tadalafil | 31 (12) vs. 14 (11) vs. 14 (12) | |
Dyspnea | Dual therapy vs. ambrisentan vs. tadalafil | 5 (2) vs. 0 vs. 1 (< 1) | |
Peripheral edema | Dual therapy vs. ambrisentan vs. tadalafil | 4 (2) vs. 3 (2) vs. 1 (< 1) | |
Common AEs | |||
Peripheral edema | Dual therapy vs. ambrisentan vs. tadalafil | 115 (45) vs. 41 (33) vs. 34 (28) | |
Headache | Dual therapy vs. ambrisentan vs. tadalafil | 107 (42) vs. 41 (33) vs. 42 (35) | |
Nasal congestion | Dual therapy vs. ambrisentan vs. tadalafil | 54 (21) vs. 19 (15) vs. 15 (12) | |
Anemia | Dual therapy vs. ambrisentan vs. tadalafil | 37 (15) vs. 8 (6) vs. 14 (12) | |
Dizziness | Dual therapy vs. ambrisentan vs. tadalafil | 50 (20) vs. 24 (19) vs. 14 (12) | |
Syncope | Dual therapy vs. ambrisentan vs. tadalafil | 13 (5) vs. 7 (6) vs. 10 (8) | |
Hypotension | Dual therapy vs. ambrisentan vs. tadalafil | 20 (8) vs. 9 (7) vs. 9 (7) | |
SAEs | |||
Any | Dual therapy vs. ambrisentan vs. tadalafil | 92 (36) vs. 45 (36) vs. 50 (41) | |
Pulmonary hypertension | Dual therapy vs. ambrisentan vs. tadalafil | 11 (4) vs. 11 (9) vs. 9 (7) | |
Pneumonia | Dual therapy vs. ambrisentan vs. tadalafil | 11 (4) vs. 7 (6) vs. 4 (3) | |
Death, n (%) | Dual therapy vs. ambrisentan vs. tadalafil | 9 (4) vs. 2 (2) vs. 6 (5) | |
Hospitalization for worsening PAH, n (%) | Dual therapy vs. ambrisentan vs. tadalafil | 10 (4) vs. 18 (14) vs. 12 (10) | |
Disease progression, n (%) | Dual therapy vs. ambrisentan vs. tadalafil | 10 (4) vs. 12 (10) vs. 4 (3) | |
Chin et al. (2021)17 TRITON study RCT | AEs, n (%) | Triple therapy vs. dual therapy | 119 (100) vs. 123 (96.9) |
AEs leading to treatment discontinuation, n (%) | Triple therapy vs. dual therapy | 19 (16.0) vs. 17 (14.2) | |
Common AEs | |||
Headache | Triple therapy vs. dual therapy | 82 (68.9) vs. 77 (60.6) | |
Diarrhea | Triple therapy vs. dual therapy | 64 (53.8) vs. 40 (31.5) | |
Nausea | Triple therapy vs. dual therapy | 57 (47.9) vs. 32 (25.2) | |
Edema peripheral | Triple therapy vs. dual therapy | 44 (37.0) vs. 46 (36.2) | |
Pain in extremity | Triple therapy vs. dual therapy | 36 (30.3) vs. 20 (15.7) | |
Pain in jaw | Triple therapy vs. dual therapy | 35 (29.4) vs. 14 (11.0) | |
Vomiting | Triple therapy vs. dual therapy | 30 (25.2) vs. 15 (11.8) | |
Dyspepsia | Triple therapy vs. dual therapy | 27 (22.7) vs. 16 (12.6) | |
SAEs | |||
Any | Triple therapy vs. dual therapy | 51 (42.9) vs. 40 (31.5) | |
Infections and infestations | Triple therapy vs. dual therapy | 18 (15.1) vs. 10 (7.9) | |
Respiratory, thoracic, and mediastinal disorders | Triple therapy vs. dual therapy | 18 (15.1) vs. 15 (11.8) | |
Gastrointestinal disorders | Triple therapy vs. dual therapy | 13 (10.9) vs. 6 (4.7) | |
Cardiac disorders | Triple therapy vs. dual therapy | 11 (9.2) vs. 12 (9.4) | |
Blood and lymphatic system disorders | Triple therapy vs. dual therapy | 8 (6.7) vs. 3 (2.4) | |
Nervous system disorders | Triple therapy vs. dual therapy | 0 vs. 7 (5.5) | |
Death, n (%) | Triple therapy vs. dual therapy | 2 (1.7%) vs. 9 (7.1%) | |
Grunig et al. (2024)18 A DUE study RCT | AEs, n (%) | Dual therapy vs. macitentan vs. tadalafil | 88 (82.2) vs. 25 (71.4) vs. 35 (79.5) |
SAEs, n (%) | Dual therapy vs. macitentan vs. tadalafil | 15 (14.0) vs. 3 (8.6) vs. 4 (9.1) | |
AEs leading to treatment discontinuation, n (%) | Dual therapy vs. macitentan vs. tadalafil | 9 (8.4) vs. 0 (0) vs. 2 (4.5) | |
Common AEs | |||
Headache, n (%) | Dual therapy vs. macitentan vs. tadalafil | 18 (16.8) vs. 6 (17.1) vs. 6 (13.6) | |
Edema and fluid retention, n (%) | Dual therapy vs. macitentan vs. tadalafil | 22 (20.6) vs. 5 (14.3) vs. 7 (15.9) | |
Peripheral edema, n (%) | Dual therapy vs. macitentan vs. tadalafil | 14 (13.1) vs. 4 (11.4) vs. 5 (11.4) | |
Anemia, n (%) | Dual therapy vs. macitentan vs. tadalafil | 20 (18.7) vs. 1 (2.9) vs. 1 (2.3) | |
Hypotension, n (%) | Dual therapy vs. macitentan vs. tadalafil | 8 (7.5) vs. 0 vs. 0 | |
Death, n (%) | Dual therapy vs. macitentan vs. tadalafil | 3 (2.8) vs. 0 vs. 0 | |
AE = adverse event; PAH = pulmonary arterial hypertension; RCT = randomized controlled trial; SAE = serious adverse event; vs. = versus.
Table 12: Summary of Secondary Analyses of the AMBITION Study
Study citation and study design | Outcomes | Category (dual vs. monotherapy[pooled]) | Results |
|---|---|---|---|
White et al. (2019)19 AMBITION study RCT | First event of clinical failurea | WHO FC II (76 patients vs. 79 patients) | HR (95% CI) = 0.21 (0.07 to 0.63) |
WHO FC III (177 patients vs. 168 patients) | HR (95% CI) = 0.58 (0.39 to 0.86) | ||
NT-proBNP | WHO FC II | P = 0.380 | |
WHO FC III | Geometric mean ratio expressed as difference (95% CI) = −43% (−54 to −29); P < 0.001 | ||
6MWD | WHO FC II | Median increase from baseline to Week 24, m: 40 vs. 32; P = 0.366 | |
WHO FC III | Median increase from baseline to Week 24, m: 52 vs. 22; P < 0.001 | ||
Kuwana et al. (2020)20 AMBITION study RCT | First event of clinical failurea | CTD-PAH (117 patients vs. 99 patients) | HR (95% CI) = 0.48 (0.29 to 0.82) |
SSc-PAH (81 patients vs. 26 patients) | HR (95% CI) = 0.46 (0.24 to 0.90) | ||
Low risk at baseline (14 patients vs. 13 patients) | No events | ||
Intermediate risk at baseline (99 patients vs. 80 patients) | HR (95% CI) = 0.52 (0.30 to 0.91) | ||
High-risk group at baseline (4 patients vs. 6 patients) | HR (95% CI) = 0.20 (0.02 to 1.80) | ||
NT-proBNP | CTD-PAH (91 patients vs. 78 patients) | Reduction in geometric mean from baseline to Week 24 (%): 58.3 vs. 44.0 | |
SSc-PAH (64 patients vs. 46 patients) | Reduction in geometric mean from baseline to Week 24 (%): 58.2 vs. 40.2 | ||
6MWD | CTD-PAH (113 patients vs. 97 patients) | Median increase from baseline to Week 24, m: 40.5 vs. 23.0 | |
SSc-PAH (77 patients vs. 55 patients) | Median increase from baseline to Week 24, m: 34.0 vs. 8.0 |
CI = confidence interval; CTD-PAH = connective tissue disease-associated pulmonary arterial hypertension; FC = functional class; HR = hazard ratio; NT-proBNP = N-terminal pro–brain natriuretic peptide; OR = odds ratio; PAH = pulmonary arterial hypertension; RCT = randomized controlled trial; SSc-PAH = systemic sclerosis-related pulmonary arterial hypertension; vs. = versus.
aDefined as the first occurrence of a composite end point of death, hospitalization for worsening PAH, disease progression, or unsatisfactory long-term clinical response.
ISSN: 2563-6596
Canada’s Drug Agency (CDA-AMC) is a pan-Canadian health organization. Created and funded by Canada’s federal, provincial, and territorial governments, we’re responsible for driving better coordination, alignment, and public value within Canada’s drug and health technology landscape. We provide Canada’s health system leaders with independent evidence and advice so they can make informed drug, health technology, and health system decisions, and we collaborate with national and international partners to enhance our collective impact.
Disclaimer: CDA-AMC has taken care to ensure that the information in this document was accurate, complete, and up to date when it was published, but does not make any guarantee to that effect. Your use of this information is subject to this disclaimer and the Terms of Use at cda-amc.ca.
The information in this document is made available for informational and educational purposes only and should not be used as a substitute for professional medical advice, the application of clinical judgment in respect of the care of a particular patient, or other professional judgments in any decision-making process. You assume full responsibility for the use of the information and rely on it at your own risk.
CDA-AMC does not endorse any information, drugs, therapies, treatments, products, processes, or services. The views and opinions of third parties published in this document do not necessarily reflect those of CDA-AMC. The copyright and other intellectual property rights in this document are owned by the Canadian Agency for Drugs and Technologies in Health (operating as CDA-AMC) and its licensors.
Questions or requests for information about this report can be directed to Requests@cda-amc.ca.