Drugs, Health Technologies, Health Systems
Health Technology Review
Myoelectric and Microprocessor-Enabled Prostheses
Key Messages
What Is the Issue?
Advanced prostheses offer people living with upper-limb or lower-limb amputations the potential for more complex movement compared to conventional or body-powered devices. However, advanced prostheses are expensive, require more training, and can require more maintenance than body-powered devices.
A review of the literature can inform health care decision-making regarding these devices by summarizing their clinical benefits and cost-effectiveness compared to body-powered devices.
What Did We Do?
To inform decisions regarding advanced prostheses for amputations, we conducted a Rapid Review to summarize evidence that compared the clinical effectiveness and cost-effectiveness of myoelectric and microprocessor-enabled prostheses to conventional or body-powered prostheses. We also sought to identify evidence-based guidelines regarding the use of myoelectric prostheses and microprocessor-enabled prostheses for this patient population.
We searched key resources, including journal citation databases, and conducted a focused internet search for relevant evidence published since January 1, 2015.
What Did We Find?
We found a total of 9 publications relevant for this review.
Three cross-sectional studies evaluated the clinical effectiveness of myoelectric prostheses compared to body-powered prostheses. The findings suggested that myoelectric prostheses do not provide additional clinical benefits in physical function, quality of life, or satisfaction when compared to body-powered prostheses for adults with upper-limb amputations. However, the studies had limited internal and external validity, and they were likely underpowered. The study populations consisted mostly of white, male veterans in the US, with potential overlap between some of the identified studies.
Two systematic reviews evaluated the clinical effectiveness of microprocessor-enabled prostheses (i.e., microprocessor knees) compared to body-powered prostheses. The findings suggested that, for above-the-knee amputations, microprocessor knees provide better or no additional clinical benefits in safety, physical function or mobility, quality of life, and satisfaction versus body-powered prostheses. However, there are many outcome measures used to assess safety and function across the literature, and results conflict depending on the measure used. Manufacturers were also involved in the conduct of 1 systematic review, while the other systematic review reported manufacturer involvement in the included studies.
We did not identify any studies on the cost-effectiveness of myoelectric prostheses compared to body-powered prostheses for upper-limb amputations.
One systematic review evaluated the cost-effectiveness of microprocessor-enabled prostheses (i.e., microprocessor knees). It concluded that microprocessor knees are cost-effective compared to nonmicroprocessor knees. However, the findings may not be generalizable to health systems in Canada, and there is considerable heterogeneity in willingness-to-pay thresholds and considered costs across the literature.
One guideline on upper-limb amputation recommends body-powered prostheses or externally-powered prostheses (including myoelectric prostheses) to improve independence and reduce disability for people with upper-limb amputation (a weak recommendation based on very low certainty of evidence). It did not identify evidence to recommend 1 type over another.
Two evidence-based guidelines recommend microprocessor knees based on evidence suggesting that they reduce falls, optimize function and mobility, enhance quality of life, and improve satisfaction. However, 1 guideline deemed the supporting evidence to be of very low quality and the recommendation to be weak, while the other guideline lacked a risk of bias assessment. The former guideline also recommends energy storing and return or microprocessor foot and ankle components over solid-ankle, cushioned-heel feet to improve ambulation and patient satisfaction (a weak recommendation based on very low-quality evidence).
What Does This Mean?
Microprocessor-enabled prostheses, specifically those with microprocessor knees, may provide more or no additional clinical benefits and may be more cost-effective than conventional prostheses for adults with above-the-knee amputations. However, the literature was assessed to be of low quality, with considerable heterogeneity in outcomes. It is unclear how generalizable these findings are to health systems in Canada.
Limited and low-quality evidence suggests that myoelectric prostheses and body-powered prostheses do not provide additional clinical benefits. Additionally, the comparative cost-effectiveness of these devices remains unclear.
Evidence-based guidelines underscore the importance of patient-centred care and shared decision-making for people living with an amputation. Clinicians may wish to account for patient factors — such as their activity levels and needs, preferences, and access to rehabilitation services — when prescribing a prosthesis.
Previous research has identified disproportionately higher rates of lower-limb amputations in remote areas, in neighbourhoods of low social capital or low socioeconomic status, and among Indigenous Peoples living in Canada, due to unmet health care needs. However, inadequate reporting of population characteristics in the included studies limited the ability to make conclusions about the applicability of findings for people with an amputation in these underserved populations.
Abbreviations
DOF
degree of freedom
GRADE
Grading of Recommendations Assessment, Development and Evaluation
QALY
quality-adjusted life-year
SF-36
Short Form (36) Health Survey
Key Terminology
Indigenous Peoples: People and communities who identify with and have historical claim as “First Peoples” who have been on these lands (colonially known as Canada and the US) since time immemorial. Indigenous Peoples within Canada often refers to people who belong to First Nations, Inuit, and Métis communities; however, we acknowledge that all Indigenous communities are widely heterogeneous, having distinct social, economic, and political systems, as well as distinct languages, cultures, and beliefs.1,2
Research Questions
What is the clinical effectiveness and safety of myoelectric prosthesis versus body-powered prosthesis for people with an upper-body amputation?
What is the clinical effectiveness and safety of microprocessor-enabled prosthesis versus body-powered prosthesis for people with a lower-body amputation?
What is the cost-effectiveness of myoelectric prosthesis versus body-powered prosthesis for people with an upper-body amputation?
What is the cost-effectiveness of microprocessor-enabled prosthesis versus body-powered prosthesis for people with a lower-body amputation?
What are the evidence-based guidelines regarding the use of myoelectric prosthesis or microprocessor-enabled prosthesis for people with upper-body or lower-body amputations, respectively?
Context and Policy Issues
Upper-Limb Amputations
In 2013, it was estimated that approximately 6,800 people in Canada had undergone an amputation proximal to the wrist.3 Trauma is the most common cause of upper-limb amputations.4 Other less common causes of upper-limb amputations in adults include infection (e.g., from diabetes or immunodeficiency), ischemic disease, and cancer.4 When replantation or reconstruction is not feasible, clinicians proceed with an upper-limb amputation.4 Levels of upper-limb amputation include interscapular thoracic (i.e., up to shoulder girdle), shoulder disarticulation (i.e., through the shoulder joint), transhumeral (i.e., above the elbow), elbow disarticulation (i.e., through the elbow joint), transradial (i.e., below the elbow), and hand and wrist disarticulation (at the wrist).5
Upper-Limb Prostheses
People with an upper-limb amputation may use a body-powered prosthesis or an externally-powered prosthesis. A body-powered prosthesis can be controlled using body motions, via a cable traversing from a harness, whereas externally-powered prostheses have at least 1 motorized joint powered by a battery.6 The most common type of externally-powered device is a myoelectric prosthesis.6 Myoelectric devices use electromyography surface electrodes embedded in the socket to convert signals from the muscle to control movement in the motorized joint.6,7 However, externally-powered prostheses can use other control inputs, such as force sensitive resistors, linear transducers, toggles, rocker switches, and inertial measurement units.6
Prostheses also include a terminal device, which is the end component that interacts with the environment.8 For upper-limb amputations, terminal devices function as the hand of the prosthesis. The ‘degrees of freedom’ (DOFs) describe the capabilities of terminal devices.7 Single-DOF myoelectric prostheses indicate that the terminal device can open and close, while multi-DOF myoelectric prostheses can perform more complex functions typical of the hand.7 Myoelectric prostheses are known to require more training for use than body-powered prostheses, given their potential for more complex function.7 They are also typically heavier, less durable (more susceptible to damage from moisture or vibration), and more expensive than body-powered prostheses.7 A 2013 budget impact analysis found that the average annual total cost, average annual cost of prosthesis components, and operation costs were higher for myoelectric devices compared to body-powered prostheses, based on data from 28 individuals in British Columbia.9 The annual average total prosthetic cost was more than $35,000 for myoelectric prostheses for the first year of use, while it was approximately $15,000 for body-powered prostheses.9 The first year of use represented more than 50% of the total cost of prosthesis use within the 5-year time frame of their analysis.9
Lower-Limb Amputations
Lower-limb amputations are largely caused by long-term and unresolved complications of peripheral artery disease and diabetes mellitus.10-14 The Canadian Institute of Health Information estimated that there were 7,720 lower-limb amputations per year associated with diabetes in adults living in Canada between 2020–2021 and 2022–2023.11 Lower-limb amputations in people with diabetes are typically preventable and reflect unmet health care needs.11 Health systems around the world, including Canada, use rates of leg amputations as a measure of diabetes care quality.11 Types of lower-limb amputation include hip disarticulation (through the hip joint), knee disarticulation (through the knee joint), transtibial (below the knee) or transfemoral (above the knee).15,16 Postoperative recovery rehabilitation for lower-limb amputations involving prosthesis can vary and involves many stages, such prosthesis fitting, prosthesis management, and prosthesis training so that individuals can resume daily activities and reintegrate into their community.15 The length of rehabilitation can vary by level of amputation and rehabilitation centre,17 but it can take up to 12 to 18 months.15
In 2024, the Canadian Institute of Health Information published a report highlighting considerable health inequities in diabetes-associated leg amputations.11 Their analysis found higher rates of diabetes-associated leg amputations in males, individuals living in the lowest-income neighbourhoods, individuals living in neighbourhoods with the lowest rates of high school completion, and individuals living in neighbourhoods with the highest social isolation.11 They also noted that rates of leg amputation increase with increasing remoteness.11 They attributed this phenomenon to lower access to health providers that deliver critical preventive services in remote areas.11 These health inequities remain significant after adjusting for diabetes prevalence (i.e., more prevalent among males and populations in neighbourhoods with lower incomes and areas with lower levels of education).11
Indigenous Peoples in Canada have disproportionately higher rates of lower-limb amputations compared to non-Indigenous populations.18-20 Authors of a study conducted in Saskatchewan reported that the rate of amputations is 1.7 times higher among First Nations individuals registered under the Indian Act compared to the non-Indigenous population.19 While diabetes-related foot complications are higher in Indigenous males than Indigenous females, both sexes are at higher risk of lower-limb amputations at a younger age compared to non-Indigenous populations in Canada.18 A scoping review reported that the mean age for lower-limb amputations in Indigenous Peoples is approximately 14 years younger than the non-Indigenous population.18 Disproportionate rates of lower-limb amputation and diabetes in Indigenous Peoples reflect their insufficient access to culturally-informed, specialized, and preventive care, as well as the documented barriers — including racism, discrimination, and marginalization — within the health care systems in Canada.18,21
Lower-Limb Prostheses
Lower-limb prostheses can include multiple components, such as a socket, knee, shin or pylon, foot, and ankle.15 The prosthesis can either be endoskeletal or exoskeletal. The former means that components may be left uncovered or hidden inside a cosmetic cover for easy replacement or alignment changes, whereas the latter has a rigid exterior.15 Microprocessor-enabled prostheses have microprocessor components, such as the knees. Microprocessor knees allow for faster knee adjustments and a more natural gait compared to other types of prosthetic knees.15,22 They can differ in which phases of gait are controlled and how the phase may be controlled.15 They also require regular maintenance and strict adherence, and have been reported to be heavier than nonmicroprocessor knees.15 Conventional prostheses without microprocessors move via mechanical adjustment or are weight-activated (e.g., single-axis knees, locking knees, stance-control “safety” knees, polycentric knees, and pneumatic or hydraulic knees).15,22 The cost of lower-limb prostheses can vary depending on the level of amputation and function. The US Department of Veterans Affairs estimates that the 5-year projected cost of lower-body prostheses ranges from US$82,251 to US$228,665 (inclusive of microprocessor and nonmicroprocessor knees).23 In general, microprocessor knees are more costly than nonmicroprocessor knees.24
Rehabilitation Services for Amputations and Prosthesis Coverage in Canada
The high cost of prostheses, especially those with more advanced technologies, is a considerable barrier to access for people living with amputations.23,25 In addition to the device itself, people need to consider costs associated with device maintenance and repairs, as well as rehabilitation and training (e.g., physical therapy and occupational therapy).26 Training can include balance and coordination training, gait training, muscle strengthening, cardiovascular training, and prosthesis education.17
Coverage for advanced prostheses, such as myoelectric and microprocessor knees, remains limited and varies across jurisdictions in Canada.23,25 While some coverage exists, people living with an amputation are still likely to rely on personal resources, private insurance, fundraising, or funding from nongovernmental organizations for access to a prosthesis and necessary care.23 Nongovernmental bodies include groups that represent people living with amputations, such as the Ottawa Amputee Society and the War Amps.17
An Environmental Scan identified that there are at least 36 regional sites that provide rehabilitation services for amputations in Canada.27 However, the findings suggest that people living with amputations may have different experiences between these centres because they can vary in clinician availability, access to prostheses (e.g., prosthesis fabrication, financial assistance benefits), and other services (e.g., mental health and peer support).27 Rehabilitation centres may also offer other types of therapy, such as aquatic therapy, stress management, phantom pain and body image education, and smoking cessation programs.17,27
Why Is It Important to Do This Review?
Clinicians and decision-makers may be uncertain about the clinical effectiveness and cost-effectiveness of advanced prostheses compared to body-powered prostheses, specifically myoelectric and microprocessor-enabled prostheses for upper-body and lower-body amputations, respectively. A review of the evidence can help inform decision-making regarding advanced prostheses for people with an upper-body or lower-body amputation compared to body-powered prostheses.
Objectives
In response to an external request, we prepared this Rapid Review that summarizes and critically appraises available evidence to inform decision-making regarding the clinical effectiveness and cost-effectiveness of:
myoelectric prostheses compared to body-powered prostheses for upper-body amputations
microprocessor-enabled prostheses compared to body-powered prostheses for lower-body amputations.
This review also summarizes recommendations from evidence-based guidelines regarding the use of myoelectric prostheses or microprocessor-enabled prostheses for this patient population.
Methods
An information specialist conducted a customized literature search, balancing comprehensiveness with relevance, of multiple sources and grey literature on July 14, 2025.
One reviewer screened citations and selected studies based on the inclusion criteria presented in Table 1, and critically appraised included publications using 3 critical appraisal tools. For this Rapid Review, systematic reviews must have a research question, reproducible strategy, inclusion and exclusion criteria, screening methods, critical appraisal or risk of bias assessment, and information about data analysis and synthesis.28 Additionally, health technology assessments must be informed by a systematic review. Of note, we did not conduct engagement with people living with amputations in Canada for this Rapid Review.
Appendix 1 presents a detailed description of methods and selection criteria for included studies.
Criteria | Description |
|---|---|
Population | Q1, Q3, Q5: People with upper-body amputation(s) Q2, Q4, Q5: People with lower-body amputation(s) |
Intervention | Q1, Q3, Q5: Myoelectric prosthesis Q2, Q4, Q5: Microprocessor-enabled prosthesis |
Comparator | Q1 to Q4: Body-powered prosthesis (or conventional prosthesis) Q5: Not applicable |
Outcomes | Q1, Q3: Clinical effectiveness (e.g., quality of life, function [e.g., activities of daily living, mobility], adverse events [e.g., falls], length of use, and acceptance rate of prosthesis) Q2, Q4: Cost-effectiveness (e.g., ICER) Q5: Recommendations regarding prosthetic use (e.g., appropriate type of prosthesis) |
Study designs | Health technology assessments, systematic reviews, randomized controlled trials, nonrandomized studies, economic evaluations, and evidence-based guidelines |
Publication date | Since January 1, 2015 |
ICER = incremental cost-effectiveness ratio.
Note: For research questions 1 to 4, we limited study designs of interest to systematic reviews, including those systematic reviews within health technology assessments. When no systematic reviews were available, we included primary studies that met the review’s eligibility criteria.
Summary of Evidence
Quantity of Research Available
This report includes 9 publications that met our inclusion criteria, including 3 systematic reviews,29-31 3 nonrandomized studies,32-34 and 3 guidelines.6,35,36
For question 1, we did not identify any relevant systematic reviews. To address this gap, we included the 3 nonrandomized studies identified from the search results.32-34
We identified 2 systematic reviews relevant to question 2.29,30 These systematic reviews overlapped on 3 primary studies, where 1 systematic review30 narratively summarized its findings and the other reported quantitative results.29 Hence, results from both systematic reviews are reported in this Rapid Review.29,30 A citation matrix describing the degree of overlap between primary studies is presented in Appendix 6.
We found 1 systematic review that aimed to address questions 3 and 4.31 It had broad selection criteria by including economic evaluations that evaluated the cost-effectiveness of any prosthesis-related devices for upper-limb or lower-limb amputations.31 This systematic review found no economic evaluations on devices for upper-limb amputations;31 however, the review identified literature on the cost-effectiveness of microprocessor-enabled prostheses (i.e., microprocessor knees) versus body-powered protheses, osseointegrated versus socket-suspended prostheses, and different types of transtibial sockets.31 Of the 6 economic evaluations on microprocessor knees, 4 met the inclusion criteria of this Rapid Review.31 Only the characteristics and results of these relevant studies are described in this report.
We identified 3 evidence-based guidelines relevant to question 5.6,35,36 We reported on the characteristics and results from the subset of relevant studies. Appendix 2 presents the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA)37 flow chart of the study selection.
Summary of Study Characteristics
Summaries of study characteristics are organized by research question. Appendix 3 provides details regarding the characteristics of included publications.
Included Studies for Question 1: Clinical Effectiveness of Myoelectric Prostheses Versus Body-Powered Prostheses
We identified 3 cross-sectional studies that evaluated the clinical effectiveness of myoelectric prostheses.32-34 We included these studies post hoc, given the lack of relevant systematic reviews for question 1. All 3 studies involved people with upper-limb amputations residing in the US. Of these 3 studies, 2 recruited veterans with at least 1 upper-limb amputation who received care from the US Department of Veterans Affairs or Department of Defense between 2010 and 2015.33,34 The remaining study recruited people with unilateral and bilateral upper-limb amputations seen at 5 US sites (85% were veterans).32 The US government, specifically the US army, funded all 3 cross-sectional studies.32-34
Across these 3 cross-sectional studies, the study population were mostly white, non-Hispanic, male veterans older than 50 years of age.32-34 Trauma was a major cause of amputations (i.e., combat, accident, and burn).32-34 None of the studies defined gender or sex and none reported population characteristics by socioeconomic status, place of residence, religion, occupation, social capital, or education.32-34
Two cross-sectional studies32,33 separated myoelectric prosthesis users into 2 subgroups for analysis: single-DOF and multi-DOF. DOF describes the terminal device used by the study arm.32,33 These 2 studies aligned in what they considered a single-DOF and multi-DOF terminal device.32,33 Additionally, 2 studies classified hybrid devices as myoelectric.32,34
One study compared the impact of the use of a prosthesis versus nonuse of a prosthesis on outcomes,33 while 2 studies also included cosmetic devices.33,34 These comparisons are beyond the scope of this report; thus, we reported results when the analysis included comparisons relevant for our review.
Two studies compared the impact on physical function and mobility (e.g., dexterity, activities of daily living, independence, and disability measures), as well as quality of life.32,33 Additionally, 2 studies compared user satisfaction between myoelectric and body-powered users.32,34 One study compared the impact of these devices on social wellness (via the Community Reintegration of Injured Service Members computer-adapted test) of the study population.32
Table 2 provides a detailed summary of the characteristics of the 3 cross-sectional studies for question 1.
Included Studies for Question 2: Clinical Effectiveness of Microprocessor-Enabled Versus Body-Powered Prostheses
We identified 2 systematic reviews that evaluated the clinical effectiveness of microprocessor-enabled prostheses versus body-powered prostheses, specifically microprocessor knees compared to nonmicroprocessor knees.29,30
One systematic review compared the impact of these devices on safety, function or performance, and satisfaction in people with above-the-knee amputations classified as Medicare functional classification level 2 (low mobility or limited community ambulator).29 Level 2 indicates that the individual using the prosthesis “has the ability or potential for ambulation with the ability to transverse low level environmental barriers such as curbs, stairs or uneven surfaces. This level is typical of the limited community ambulator.”38 The systematic review authors found a total of 15 studies (all relevant to the present review), with a total of 704 participants.29 The follow-up period ranged from 1 week to 6 months across the included studies.29 The study population was mostly male (76.9%), with a smaller proportion of females (22.9%).29 The systematic review included a meta-analysis with outcome measures reported in at least 3 primary studies, specifically:
safety (i.e., number of falls, fear of falling, Timed Up and Go test)
function and mobility (i.e., positive mobility grade change, walking speed, fast walking speed)
satisfaction-related questions from the General Prosthesis Evaluation Questionnaire (i.e., ambulation, utility, appearance, residual limb, sounds, utility, well-being).29
The other systematic review included studies on people with unilateral transfemoral amputation.30 This systematic review included 18 studies (17 relevant to the present review) with a total of 993 participants. Of the included studies, the study population was composed mostly of males (77.1%).30 However, this systematic review did not define or differentiate sex and gender. The mean age of the population ranged from 38.5 years to 69 years, and the follow-up period ranged from 1 week to 6 months across the included primary studies.30 The systematic review authors compared the impact of microprocessor knees to nonmicroprocessor knees on mobility and quality of life.30
None of the systematic reviews29,30 reported population characteristics by socioeconomic status, place of residence, religion, occupation, social capital, and education. It is unclear whether primary studies included in these systematic reviews reported on these characteristics.
Table 3 provides a detailed summary of the characteristics of included systematic reviews for question 2.
Included Studies for Question 3: Cost-Effectiveness of Myoelectric Versus Body-Powered Prostheses
We did not identify any publications that evaluated the cost-effectiveness of myoelectric versus body-powered prostheses. Therefore, we could not provide a summary.
Included Studies for Question 4: Cost-Effectiveness of Microprocessor Knees Versus Body-Powered Prostheses
We included 1 systematic review of economic evaluations that compared the cost-effectiveness of microprocessor knees versus mechanical knees (i.e., body-powered prostheses) in people with lower-extremity amputations.31 The systematic review authors included 12 economic evaluations (4 relevant to this Rapid Review).31 Of the relevant publications, 3 evaluations used a payer’s perspective in Italy, Sweden, and Denmark, and the remaining economic evaluation was conducted in the US with a societal perspective.31 Three of the included economic evaluations specifically evaluated the cost-effectiveness of microprocessor knees (C-Leg), whereas the remaining economic evaluation did not specify a specific brand or type of microprocessor knees.31
Direct and indirect costs varied across studies.31 Direct costs may include hospital stays, medications, rehabilitation-related visits, fitting time, diagnostics, and device service and maintenance.31 One of the included economic evaluations was limited to fitting time and service costs.31 Indirect costs can include transportation, lodging, patient and family or caregiver expenses, productivity losses, and lost wages. Additionally, the time horizon ranged from 5 years to 10 years across relevant economic evaluations.31
The systematic review did not describe the population characteristics of their study population.31 Table 3 provides a detailed summary of the characteristics of the systematic review for question 4.
Included Studies for Question 5: Guidelines Regarding the Use of Myoelectric Prostheses or Microprocessor-Enabled Prostheses
Table 4 provides a detailed summary of the characteristics of included guidelines for question 5.
Guidelines for Upper-Limb Amputations
The US Department of Veterans Affairs and Department of Defense published 1 evidence-based guideline in 2022 for adults with upper-limb amputations.6 They considered a variety of interventions for upper-limb amputations, such as prevention and treatment for residual limb pain, prostheses, and psychosocial interventions.6 They developed this guideline for health care providers, such as rehabilitation care providers, physicians, therapists, and prosthetists.6 Focus groups sought the perspectives of the population of interest receiving care from the Department of Veterans Affairs or the Department of Defense to inform the guideline.6
The guideline development group considered benefits and harms of interventions — such as functional status, quality of life, satisfaction, independence, pain, and mental health — from the literature.6 The quality of individual studies was determined using the US Preventive Services Task Force method.6 The overall quality of the body of evidence was determined using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach, which considers overall study quality or risk of bias, consistency of evidence, directness of evidence, and precision of evidence.6 The quality of the body of evidence is rated as high, moderate, low, or very low.6 The strength and direction of the recommendations was also determined using the GRADE approach, which considers the confidence in the quality of the evidence, the balance of desirable and undesirable outcomes, patient values and preferences, and other implications, such as feasibility and acceptability.6 The strength and direction of the recommendations is rated as strong for, weak for, neither for nor against, weak against, and strong against.6 It is unclear what process the guideline development group used to agree or resolve conflicts about decisions for this guideline.6
Guidelines for Lower-Limb Amputations
Two evidence-based guidelines published in 201936 and in 202435 for people with lower-limb amputations (acquired congenitally,35,36 from trauma,35,36 or from dysvascular issues36) were included in the current review.35,36 One guideline specifically focused on people with unilateral amputation at the knee disarticulation or transfemoral level.36 One guideline was developed for health care providers, community providers, and the US Department of Veterans Affairs or Department of Defense,35 while the other was developed for health care providers and policy-makers.36 Both guidelines were developed in the US,35,36 but 1 was specifically developed by the US Department of Veterans Affairs and Department of Defense.35 The same guideline was informed by findings from a focus group that gathered perspectives from people receiving care via the US Department of Veterans Affairs and Department of Defense.35 The other guideline lacked details about whether individuals were engaged in guideline development.36 The general outcomes of interest were the benefits and harms of rehabilitation or treatment strategies,35,36 such as functional status,35 quality of life,35 satisfaction,35 and falls.35
One guideline lacked assessment of the quality of individual studies, quality of the body of evidence, or the strength of the recommendations.36 The other guideline used the US Preventive Services Task Force method to assess the quality of individual studies.35 The same guideline used the GRADE approach to assess the quality of the body of evidence.35 The quality of the evidence is rated as high, moderate, low, or very low.35 The strength and direction of the recommendations was also determined using the GRADE approach.35 The strength and direction of the recommendations is rated as strong for, weak for, neither for nor against, weak against, and strong against.35
Summary of Critical Appraisal
Appendix 4 provides additional details about the strengths and limitations of the included publications.
Included Studies for Question 1: Clinical Effectiveness of Myoelectric Prostheses Versus Body-Powered Prostheses
All cross-sectional studies clearly reported their objective, main outcomes, population characteristics, interventions of interest, and findings.32-34
However, the included cross-sectional studies had limited internal validity due to their nonrandomized design, as well as the participants’ and researchers’ awareness of the intervention. The nature of intervention limited the ability to conceal treatment from participants.
One study used a convenience sample for participant recruitment, which put the study at risk of selection bias.32 The same study described potential confounders among the study population, but did not evaluate or investigate their impact on the study's findings (e.g., age, training for prosthesis, and terminal device type).32 The remaining 2 studies identified (via a regression model) and adjusted for confounding variables in their analysis of main outcomes.33,34 While researchers attempted to capture prosthesis use training as a potential confounding variable, they used a binary question with answers limited to “yes” or “no.”33,34 This binary question provided limited insight into an individual’s experience and comfort with their prosthesis. Both studies used a variety of outcomes, but researchers did not adjust for multiplicity.33,34
Furthermore, the findings of 1 study may have been impacted by misclassification bias.33 Researchers placed individuals with missing data on the number of the terminal device into the single-DOF group.33 It is possible that researchers included individuals using myoelectric prostheses in the single-DOF group. It is unclear how this may have impacted their findings for the myoelectric prostheses.33
All 3 studies had a small sample size and potentially lacked the power to detect a statistically significant effect.32-34 Additionally, these 3 cross-sectional studies recruited a study sample composed mostly of veterans that were white, non-Hispanic, male, and older than 50 years of age.32-34 While these studies were likely funded to inform decisions for this population of interest, their findings may not be generalizable to all individuals with upper-limb amputations, such as females and younger adults. It is also unclear how the study sample’s access to devices and experience with health care systems align with individuals seeking prosthesis-related care in Canada.32-34
Included Studies for Question 2: Clinical Effectiveness of Microprocessor-Enabled Prostheses Versus Body-Powered Prostheses
Both systematic reviews detailed their research questions and provided some details regarding primary studies.29,30 The systematic review by Hahn et al.29 did not have an explicit statement about established methods before the conduct of the review. The same systematic review mentioned a preparatory literature search, but did not detail their process or results, or how this was used to inform their search strategy.29 Neither systematic review justified its selection criteria.29,30 The systematic review by Thibaut et al.30 lacked details about their search time frame and limited inclusion criteria to studies with 20 or more participants without justification. Selection bias may have impacted the findings of both reviews.29,30
The systematic review by Thibaut et al.30 may also have been impacted by reporting bias. The systematic review lacked reporting of quantitative results from individual studies: the authors narratively summarized the main findings from each study.30 Additionally, the systematic review authors did not provide details on how they defined no difference, favourable results, or unfavourable results for most of their reported qualitative findings.30
The systematic review by Thibaut et al.30 described the findings of their risk of bias assessments. However, the systematic review by Hahn et al.29 did not consider the impact of confounding variables — such as amputation type, bilateral versus unilateral amputations, years of use, or user training and experience with devices — in their discussion of included studies and their meta-analysis. The same systematic review lacked exploration of the impact of publication bias,29 which was limited by the small number of studies included for outcomes in the meta-analysis. Additionally, Hahn et al.29 also acknowledged that the small number of studies pooled for meta-analysis limited the ability to identify sources of heterogeneity.
Both systematic reviews lacked details regarding the location of the included studies.29,30 Thus, it is unclear whether the findings of both reviews are generalizable to health settings and individuals with amputations in Canada. Further, the systematic review by Hahn et al.29 predominately evaluated microprocessor knees with specific functions. Their review findings may not be generalizable to all microprocessor knees.
Some authors of the systematic review by Hahn et al.29 were employees of manufacturers of microprocessor knees. Additionally, manufacturers also funded some of the primary studies included in the review by Thibaut et al.30 These findings should be interpreted with caution as study conduct and interpretation of results may have been influenced by these conflicts of interest.
Included Studies for Question 3: Cost-Effectiveness of Myoelectric Prostheses Versus Body-Powered Prostheses
We did not identify any publications that evaluated the cost-effectiveness of myoelectric versus body-powered prostheses. Therefore, we did not conduct a critical appraisal for question 3.
Included Studies for Question 4: Cost-Effectiveness of Microprocessor-Enabled Prostheses Versus Body-Powered Prostheses
The systematic review authors clearly detailed their objective, but they did not explicitly include a statement regarding established methods or provide their rationale for the exclusion criteria (e.g., studies conducted in languages other than English)31 Selection bias may have impacted findings of this review.31 Additionally, the publication did not provide details regarding funding sources. It is unclear whether funding sources may have influenced the study conduct.
The systematic review authors used a satisfactory technique to assess risk of bias, which included an assessment of funding sources of each included economic evaluation.31 However, they did not discuss their findings within the context of their bias assessment results.31 It is possible that findings were misleading without discussing the limitations of the included evaluations.
Most economic evaluations focused on the cost-effectiveness of the C-Leg microprocessor knee versus mechanical knees.31 It is unclear whether the findings of this systematic review apply to all microprocessor knees.31 There was also considerable heterogeneity across the economic evaluations, including time horizon, direct and indirect costs considered, and threshold of acceptability.31
It is likely that these findings may not be applicable to health settings in Canada. The relevant economic evaluations were conducted outside of Canada, and most were conducted with a payer’s perspective (3 of 4 relevant evaluations).31 Most economic evaluations did not consider indirect costs involved in the natural history of amputations and prosthesis use, such as rehabilitation and training costs.31 It is also unclear whether economic evaluations considered contexts of transitioning to new devices (i.e., from mechanical knees to microprocessor knees) or cases in which individuals discontinued an advanced prosthesis to return to their previous model (i.e., a mechanical knee).31
Included Studies for Question 5: Guidelines Regarding the Use of Myoelectric Prostheses or Microprocessor-Enabled Prostheses
Guidelines for Upper-Limb Amputations
The guidelines clearly described their scope and purpose, the health professionals involved in development, and the guidelines’ target users.6 They clearly detailed the methods of selecting articles based on inclusion and exclusion criteria.6 All recommendations were specific, unambiguous, and easily identifiable.6 The guidelines discussed the applicability of the recommendations with consideration of key factors such as facilitators, barriers, and monitoring and auditing criteria, when applicable.
The guideline development group conducted focus groups to help ensure relevance and incorporate patient perspectives.6 However, individuals in the focus group were those who had either received or were currently receiving care from the US Department of Veterans Affairs and Department of Defense.6 Therefore, the perspectives could be limited and not representative of the care or experience of all individuals with upper-limb amputations receiving care. Additionally, it is possible that the guidelines did not capture all patient considerations.
The guideline development group consisted of individuals from relevant professional groups.6 A systematic literature search was conducted to search for literature to develop the guidelines.6 However, the guidelines reported limited details about the development group’s decision-making process.6 Reporting these processes helps to understand how consensus was reached, and provides insight into how all members’ perspectives were considered. Additionally, there was no record of the competing interest disclosures of the development group members. It is unclear whether conflicts of interest influenced the recommendations.
Guidelines for Lower-Limb Amputations
Both guidelines clearly described their scope and purpose, partners in the development of the guidelines, and their target users.35,36 All recommendations are specific, unambiguous, and easily identifiable.35,36 One guideline retrieved relevant studies from multiple databases,35 while the other included 1 database.36 The latter guideline’s systematic search may have been impacted by selection bias, and may have missed relevant literature given that the search was limited to 1 database.36
The views and preferences of target users were sought through a focus group in 1 guideline, which helped to ensure relevance and incorporate patient-centred perspectives.35 The focus group included those who received or were currently receiving care from the US Department of Veterans Affairs and Department of Defense.35 Therefore, the perspectives could be limited and not representative of the care or experience of all individuals with lower-limb amputations. Additionally, it is possible that the guidelines did not capture all patient considerations. The other guideline did not consider patient perspectives, which could limit its relevance and applicability to its target population.36
While 1 guideline assessed the strength of evidence and the recommendation,35 the other guideline did not.36 It is unclear whether the latter guideline considered the biases and limitations of the literature to inform their recommendations.36 The same guideline lacked details about the clinical perspectives that were considered in guideline development.36 Neither guideline detailed the methods to reach consensus, which is necessary to understand how decision-making and members’ perspectives were considered.35,36 Further, the guideline by Stevens and Wurdeman36 did not discuss factors such as facilitators, barriers, monitoring, and auditing criteria that could impact the application of recommendations in practice.
The guideline by the US Department of Veteran Affairs35 provided no record of the competing interest disclosures from the guideline development group. However, they did report their processes to identify competing interests.35 It is unclear whether conflicts of interests influenced decision-making and the recommendations. While the other guideline stated “none” for funding sources, the authors worked in a prosthetics clinic, which could have influenced their recommendations.36
Summary of Findings
Appendix 5 presents additional details regarding the main study findings.
Question 1: Clinical Effectiveness of Myoelectric Prostheses Versus Body-Powered Prostheses
Physical Function and Mobility
For unilateral amputations, Resnik et al. (2020)33 found that both single-DOF and multi-DOF myoelectric prostheses resulted in no significant difference in physical function outcomes (i.e., Quick Disabilities of Arm, Shoulder, and Hand Score; help needed for activities of daily living) versus body-powered prostheses.
Another study aimed to identify whether there are differences in dexterity between users of single-DOF myoelectric prostheses, multi-DOF myoelectric prostheses, and body-powered prostheses, in people with transradial or transhumeral amputations.32 Of note, a significant difference in this study indicated a statistically significant difference between all devices, but it did not provide insight as to which device performed the best out of all prostheses considered via statistical methods.32 For unilateral transhumeral amputations, a significant difference remained after adjustment for multiple outcomes of the Jebsen-Taylor Hand Function assessment, specifically the small objects and 9-hole peg outcomes.32 However, no difference was detected for other dexterity outcomes within the Jebsen-Taylor Hand Function assessment.32 Additionally, no outcomes remained clinically significant after adjustment when considering unilateral and bilateral transhumeral amputations.32 Further, there were no differences identified in adults with transhumeral unilateral amputations for other measures of physical function (i.e., brief activities measure for upper limb amputations; activities measure for the upper-limb amputation; timed measure of activity performance for individuals; Quick Disabilities of the Arm, Shoulder, and Hand score; help needed for activities of daily living).32
The same study also identified a significant difference (after adjustment) in the 9-hole peg, box and blocks, and small objects outcomes for the Jebsen-Taylor Hand Function assessment between single-DOF myoelectric prostheses, multi-DOF myoelectric prostheses, and body-powered protheses, for bilateral and unilateral transradial amputations.32 For people with a unilateral transradial amputation, it also identified a significant difference in the heavy cans, 9-hole peg, and small objects outcomes.32 Additionally, it found a significant difference for the brief activities measure for upper limb amputations in people with unilateral transradial amputations.32 However, no significant difference was identified for other measures of physical function (i.e., activities measure for the upper limb; timed measure of activity performance for individuals; Quick Disabilities of the Arm, Shoulder, and Hand; help needed for activities of daily living) for individuals with unilateral transradial amputations.32
Quality of Life
For unilateral amputations, Resnik et al. (2020)33 found no significant difference in scores between body-powered prostheses and myoelectric devices, regardless of the number of DOFs, for the Veterans RAND 12-Item Health Survey physical and mental components. For the same components of the Veterans RAND 12-item Health Survey, another study found no statistically significant difference for people with transradial amputations or transhumeral amputations.32
Satisfaction
For bilateral and unilateral amputations, Resnik et al. (2020)34 found no significant difference in satisfaction levels between myoelectric and body-powered prosthesis users. Another study found no significant difference in satisfaction between users of single-DOF myoelectric prostheses, multi-DOF myoelectric prostheses, and body-powered prostheses, in people with unilateral transradial or unilateral transhumeral amputations (i.e., Community Reintegration of Injured Service Members computer-adapted test, Trinity Amputation and Prosthesis Experience Satisfaction Scale).32 Of note, the authors of the same study acknowledged that these measures focus on device attributes, and neither measures satisfaction with prosthesis function.34
Social Health
One study found a statistically significant difference in Community Reintegration of Injured Service Members computer-adapted test scores, specifically in perceived difficulty in participation, between users of single-DOF myoelectric prostheses, multi-DOF myoelectric prostheses, and body-powered prostheses, in people with transradial amputations.32 The same study found no significant difference for the same outcome in people with unilateral transhumeral amputations. Additionally, no statistically significant difference was identified for extent of participation for people with unilateral transhumeral or unilateral transradial amputation.32
Question 2: Clinical Effectiveness of Microprocessor-Enabled Prostheses Versus Body-Powered Prostheses
General Prosthesis Use
The systematic review by Thibaut et al.30 found 1 study that suggested there was no difference in Questionnaire for Persons with Transfemoral Amputations scores between those with microprocessor knees and those with nonmicroprocessor knees.
Safety
The meta-analysis results by Hahn et al.29 found statistically significant differences in favour of microprocessor knees versus nonmicroprocessor knees for all safety-related outcomes (11 studies), including number of falls (7 studies), fear of falling (6 studies), and Timed Up and Go (4 studies) in fixed-effects and random-effects models for limited community ambulators.
The systematic review by Hahn et al.29 found a favourable effect for microprocessor knees versus nonmicroprocessor knees (9 studies). Of the 12 outcome measures for safety:
7 resulted in a statistically significant difference
4 did not report statistically significant differences
2 did not report statistical significance (e.g., P values).
The same systematic review found that none of the included studies showed a decline in safety with the use of microprocessor knees in limited community ambulators.29
The systematic review by Thibaut et al.30 found 1 study that showed no difference in the number of falls between microprocessor knees versus nonmicroprocessor knees. However, it also found 2 studies that showed a reduction in falls from changing to a microprocessor knee from a nonmicroprocessor knee.30
Physical Function and Mobility
The systematic review by Hahn et al.29 found all outcomes evaluating physical function and mobility favoured microprocessor knees over nonmicroprocessor knees in limited community ambulators; however, not all reported statistically significant results (15 studies). Of the 91 outcome measures, 39 results were statistically significant, while 20 resulted in a nonsignificant difference between microprocessor versus nonmicroprocessor knees.29 Six measures resulted in nonsignificant and significant differences depending on the study.29 The remaining measures did not report statistical testing results (e.g., P values).29
Further, the results of their meta-analysis favoured microprocessor knees over nonmicroprocessor knees for walking speed (6 studies).29 However, the same meta-analysis found no statistically significant difference for positive mobility grade changes (6 studies) or fast walking speed (3 studies).29 The meta-analysis also found that satisfaction with ambulation was higher for microprocessor knees versus nonmicroprocessor knees in fixed and random models (4 studies).29 For the Activity-Specific Balance Confidence Scale, the fixed-effects model results demonstrated a statistically significant improvement for microprocessor knees versus nonmicroprocessor knees, whereas the findings from the random-effects model did not demonstrate significant differences (3 studies).29
The systematic review by Thibaut et al.30 found conflicting evidence for the 6-minute walk test (2 studies), and no difference between microprocessor and nonmicroprocessor knees for the 10 m walk test (1 study). The systematic review found evidence to suggest no difference in general efficacy scores (1 study).30 The same review found conflicting evidence regarding for the Locomotor Capabilities Index (3 studies) and mobility scores for the Prosthetic Limb Users Survey of Mobility (2 studies).30 However, it identified studies that indicate higher activity levels (1 study), shorter timed up and go scores (1 study), hill mobility (1 study), and less sitting time (1 study) for microprocessor knees compared to nonmicroprocessor knees.30
The same systematic review found no difference in results in the Assessment of Daily Activity Performance in Transfermoral Amputees Test between microprocessor and nonmicroprocessor knees in individuals living with transfemoral amputations classified to have low activity levels (1 study).30 However, it found that individuals with intermediate and high activity levels needed less time to complete the same test (1 study).30
One systematic review found faster gait speed with microprocessor versus nonmicroprocessor knees, but it also found no difference in stride length, knee extension and latency period, knee latency, and stance phase duration from 3D gait analysis (1 study).30 The other systematic review found no difference in gait profile scores (1 study), electromyography signals during gait (1 study), and 3D gait analysis (1 study).29
Satisfaction
The meta-analysis by Hahn et al.29 revealed better satisfaction with utility for microprocessor knees compared to nonmicroprocessor knees for both fixed and random effects models (3 studies). However, the same meta-analysis found no statistically significant difference in terms of satisfaction with sounds (3 studies) or appearance (3 studies), as well as perceived health of the residual limb (3 studies) between microprocessor and nonmicroprocessor knees.29
The same review29 found evidence showing significantly better satisfaction with walking in individuals with high and intermediate activity levels for microprocessor knees compared to nonmicroprocessor knees (2 studies), as well as significantly better outcomes from the Quebec User Evaluation of Satisfaction with Assistive Technology when comparing these devices (1 study). However, the systematic review found no statistically significant differences in perceived social burden, perceived response by others, and frustration between microprocessor and nonmicroprocessor knees (1 study).29
Quality of Life
Results of the meta-analysis by Hahn et al.29 found no statistically significant difference in how people perceive their well-being (subscale in the prosthesis evaluation questionnaire) with microprocessor knees versus nonmicroprocessor knees (3 studies).
The systematic review by Hahn et al.29 found significantly better scores for the mental component of the Short-Form (36) Health Survey (SF-36) with microprocessor knees versus nonmicroprocessor knees (1 study), but no difference in SF-36 physical component scores and overall scores (2 studies).29 The systematic review by Thibaut et al.30 found evidence to suggest that microprocessor knees improve overall SF-36 scores (2 studies), but found no difference in the following SF-36 subscales: general health, social role, emotional role, pain, vitality, mental, and physical component. For the SF-36 physical component summary, the same systematic review found conflicting evidence (2 studies).30 For EQ-5D-5L scores, both systematic reviews identified evidence suggesting better scores with microprocessor knees (a total of 2 studies between the 2 systematic reviews).30
Question 3: Cost-Effectiveness of Myoelectric Prostheses Versus Body-Powered Prostheses
We did not identify any relevant economic evaluations for question 3. Therefore, no summary could be provided.
Question 4: Cost-Effectiveness of Microprocessor-Enabled Prostheses Versus Body-Powered Prostheses
All 4 relevant economic evaluations in the systematic review found microprocessor knees to be cost-effective compared to nonmicroprocessor knees across different willingness-to-pay thresholds.31 The lowest incremental cost-effectiveness ratio reported from relevant economic evaluations was €3,218 per quality-adjust life-year (QALY) and the highest was €40,155 per QALY, with acceptability thresholds of €10,000 per QALY and €54,120 per QALY, respectively.31
Question 5: Guidelines Regarding the Use of Myoelectric Prostheses or Microprocessor-Enabled Prostheses
Guidelines for Upper-Limb Amputations
The US Department of Veterans Affairs and Department of Defense guidelines suggested that body-powered or externally-powered prostheses be used for patients with major upper-limb amputations to improve independence and reduce disability.6 Of note, the guideline considered myoelectric prostheses to be externally-powered prostheses.6 The guideline development group reported the strength of the recommendation as weak, and the strength of the evidence as very low.6 Of note, supporting evidence for this recommendation included the 3 cross-sectional studies32-34 regarding myoelectric prostheses in this Rapid Review (i.e., addressing research question 1).
Guidelines for Lower-Limb Amputations
The US Department of Veterans Affairs and Department of Defense provided several recommendations on the use of microprocessor knee units, ankle components, and foot components for lower-limb amputations.35 The recommendations, strength of the recommendations, and quality of the evidence are as follows:
Prescribing microprocessor knee units over nonmicroprocessor knee units in prosthetic ambulators to reduce falls, optimize functional mobility, and improve patient satisfaction is suggested (weak recommendation based on very low-certainty evidence).35
There is insufficient evidence to prescribe any specific energy-storing and return or microprocessor foot and ankle component over others for prosthetic ambulators (neither for nor against the recommendation based on very low certainty evidence).35
Energy-storing and return or microprocessor-controlled foot and ankle components are suggested over solid-ankle, cushioned-heel feet in prosthetic ambulators to improve ambulation and patient satisfaction (weak recommendation based on very low-certainty evidence).35
The guideline by Stevens and Wurdeman36 also provided recommendations on the use of microprocessor knee units for lower-limb amputations. They did not assess the strength of recommendations or the evidence. The recommendations align with the recommendations for lower-limb amputations by the US Department Veteran Affairs and Department of Defense.35 Compared to nonmicroprocessor knees, microprocessor knees re indicated:
to reduce falls, stumbles, and associated frustrations, as well as the cognitive demands of ambulation36
to increase confidence while walking, self-reported mobility, satisfaction, well-being, and quality of life36
to increase self-selected walking speed, walking speed on uneven terrain, and metabolic efficiency during gait36
for limited community ambulators to enable increases in level-ground walking speed and walking speed on uneven terrain while substantially reducing uncontrolled falls and increased measured and perceived balance.36
However, the same guideline found that microprocessor and nonmicroprocessor knees resulted in similar daily step counts, temporal spatial gait symmetry, self-reported general health, and total costs of prosthetic rehabilitation.36 Therefore, the guideline recommends against the use of these parameters as primary indicators for prosthesis knee joint selection.36
Limitations
Methodology and Engagement Approach
For research questions 1 to 4, we limited study designs of interest to systematic reviews published within the past 10 years, including systematic reviews within health technology assessments. When no systematic reviews were available, we mitigated this gap by including primary studies that met the Rapid Review’s eligibility criteria. Further, we included evidence-based guidelines if they were published within the past 10 years to answer research question 5. The approach helped to balance short timelines while ensuring we could report on evidence for each research question, when available.
Given the needs of the requestor and internal capacity limitations, we did not conduct patient engagement, which would include individuals from underserved groups with disproportionately higher amputation rates (e.g., Indigenous Peoples in Canada, individuals living in areas of social isolation or remote areas).11,18-20 We acknowledge this as a limitation of our work, and that this Rapid Review may not highlight or identify perspectives and evidence of relevance to these underserved groups. Of note, as part of CDA-AMC’s organizational commitment to reconciliation, we know it is important to consider and learn from Indigenous perspectives in our work. We also recognize that the research team consists of settler researchers, and we come to this work with our individual privileges and biases. Understanding the perspectives and priorities of Indigenous Peoples and other underserved groups as they relate to amputations and prostheses can support informed health care decision-making. It is possible that the perspectives and needs of individuals in these groups regarding prostheses and the research related to amputations and prostheses would differ.
Validity of Included Studies
Literature on Microprocessor Knees
For microprocessor knees, the 2 systematic reviews included outcomes with considerable heterogeneity. For example, the systematic reviews included more than 90 different measures of physical function and mobility.29,30 Similarly, 1 guideline on lower-limb amputations formed weak recommendations regarding microprocessor knees, supported by weak evidence.35 Using such a variety of outcomes increases the likelihood of finding statistically significant results, affects the ability to pool results, and limits the ability to make definitive conclusions about the clinical effectiveness of microprocessor-enabled prostheses (specifically microprocessor knees) versus body-powered prostheses.
The systematic reviews also focused on transfemoral amputations.29,30 These findings may not be generalizable to individuals with amputations at different locations of the lower limbs (e.g., knee or hip disarticulations). One systematic review focused on individuals classified as limited community ambulators, which limited the applicability of their findings to individuals with other mobility levels.29 One systematic review predominantly included studies evaluating specific microprocessor knees (i.e., C-Leg, C-Leg Compact, Genium, and Kenovo) with hydraulic units for comprehensive stance and swing phase.29 It is possible their findings may not be applicable to other microprocessor knees.29 Furthermore, the study sample consisted of mostly males in both systematic reviews.29,30 While rates of leg amputations are higher in males in Canada, these findings may not be generalizable to other sexes and genders.
The systematic review of economic evaluations did not include any relevant economic evaluations that were conducted in Canada.31 One economic evaluation conducted their analysis from a societal perspective, but remaining evaluations used a payer’s perspective.31 The economic evaluations also varied in the indirect and direct costs considered in their analysis.31 These limitations suggest that the findings of the cost-effectiveness systematic review may not be valid to the public health care systems of Canada. Furthermore, 3 of 4 included economic evaluations evaluated the cost-effectiveness of the C-Leg microprocessor.31 It is unclear if these findings are generalizable to all microprocessor knees.
Literature on Myoelectric Prosthesis
All 3 cross-sectional studies were limited in internal validity given the nature of the study designs and interventions.32-34 The literature on upper-limb amputations focused on informing clinical effectiveness in the US veteran population.32-34 The cross-sectional studies had samples composed of mostly white males older than 50 years of age.32-34 It is possible the findings may not be applicable to all people with upper-limb amputations, such as individuals of other races, sexes, genders, or ages.
Gaps in Evidence
We found no literature comparing the cost-effectiveness of myoelectric versus body-powered prostheses for upper-limb amputations. Future studies may wish to address this gap, specifically with a societal perspective in health care systems in Canada.
Evidence on microprocessor-enabled prostheses focused on the knee component of microprocessor-enabled prostheses. None of the clinical effectiveness studies seemed to consider the potential impact of other components of microprocessor-enabled prostheses, such as the socket, shin or pylon, and foot and ankle for transfemoral amputations.15 The design of the overall prostheses may influence clinical effectiveness in people with lower-limb amputations.15
Additionally, none of the studies in this Rapid Review investigated the clinical effectiveness or cost-effectiveness of advanced prostheses versus body-powered prostheses in groups of individuals who are typically underserved. As previously mentioned, rates of lower-limb amputations are disproportionately higher in remote areas, areas with lower levels of education, and areas of low social isolation. However, none of the studies for upper-limb amputations reported population characteristics based on socioeconomic status, education, place of residence, or social capital.29,30,33,34 The same studies were composed mostly of white male veterans living in the US.32-34 For question 2, the systematic reviews provided limited details about the study sample demographics.29,30 It is unclear if groups of individuals who are typically underserved are represented in the study sample.29
The cross-sectional studies in this Rapid Review described population characteristics, including race.32-34 These studies categorized their study populations into white, Black, or “mixed race/other,” as well as “unknown” or “missing” when the race was not reported in their data.32-34 Individuals classified as “unknown,” “missing,” or “other” may include individuals of diverse races or ethnicities. Of note, individuals categorized as “mixed/other” in included studies are described in this Rapid Review as racialized people. Two studies identified race as a potential confounding variable for the main outcome analysis via statistical methods. One study found Black individuals with upper limb amputations to had significantly lower health-related quality of life specific to mental health (SF-36 mental component summary scores) compared to white individuals with upper-limb amputations.33 Additionally, Black individuals and racialized people had lower scores for an outcome of function (i.e., Quick Disabilities of Arm, Shoulder, and Hand) compared to white individuals.33 The other cross-sectional study found that Black individuals had lower device satisfaction scores compared to white individuals.34 Of note, CDA-AMC recognizes that the term “Black” describes a heterogeneous community made up of a diversity of nations, cultures, beliefs, and languages with unique histories and experiences of oppression. However, none of the studies32-34 reported how they defined “Black.”
None of the identified studies or guidelines spoke to the clinical effectiveness, cost-effectiveness, or recommendations regarding the use of advanced prostheses in Indigenous Peoples. Rates of lower-limb amputations are disproportionately higher for Indigenous Peoples in Canada compared to the non-Indigenous population in Canada.18-20 Their experience accessing health care differs from the non-Indigenous populations in Canada due documented barriers including racism, discrimination, and marginalization within health care systems in Canada.39 Hence, research findings in this Rapid Review may not be generalizable to Indigenous Peoples in Canada.
Conclusions and Implications for Decision- or Policy-Making
This Rapid Review evaluated the literature regarding the clinical effectiveness and cost-effectiveness of myoelectric and microprocessor-enabled prostheses compared to body-powered prostheses for people with amputations. We also evaluated guidelines related to the use of myoelectric and microprocessor-enabled prostheses for upper-body and lower-body amputations, respectively. We identified a total of 9 relevant publications: 3 cross-sectional studies for question 1,32-34 2 systematic reviews for question 2,29,30 1 systematic review for question 4,31 and 3 evidence-based guidelines for question 5.6,35,36 We did not identify any relevant literature for question 3 of this Rapid Review.
The evidence summarized in this report was drawn from systematic reviews with some overlap in primary studies, meaning that data from the same participants from 3 of the studies were included in both systematic reviews (refer to Appendix 6 for a citation matrix illustrating the degree of primary study overlap). One included guideline6 was informed in part by the 3 cross-sectional studies32-34 included in this Rapid Review to address research question 1. As a result, some evidence may be disproportionally represented in the overall conclusions. Additionally, 2 cross-sectional studies recruited their study population from the same source and same period.33,34 It is possible that these individuals were disproportionally represented in this Rapid Review.
Summary of Evidence
Myoelectric Prosthesis for Upper-Limb Amputations
Overall, the cross-sectional studies suggested that myoelectric prostheses do not provide additional clinical benefits versus body-powered prostheses for adults with upper-limb amputations.32-34 No significant differences, regardless of DOF capabilities, were identified for physical function, quality of life, and satisfaction between myoelectric prosthesis users and body-powered prosthesis users.32-34 However, these cross-sectional studies had limited internal validity by design and methods used and were potentially underpowered (small sample size without power calculations).32-34 Furthermore, these studies included a sample of mostly older, white, male veterans,32-34 with potential overlap of the study population between studies.33,34 Therefore, these findings should be interpreted with caution given validity concerns; results may not be applicable to all people with an upper-limb amputation, including equity-deserving groups that are typically underrepresented and underserved.
Furthermore, the guideline from the US Department of Veteran Affairs and Department of Defense suggests that either body-powered or externally-powered prostheses (inclusive of myoelectric devices) be used for patients with upper-limb amputations to improve independence and reduce disability.6 This recommendation was graded as “weak for” based on a low certainty of evidence.6 The guideline development group assessed the supporting evidence comparing the clinical benefits of myoelectric and body-powered prosthesis to be limited and of low quality.6 They did not find sufficient evidence to recommend 1 type of prosthesis over another.6
Our conclusion also aligns with the findings of a review published in 2015.40 The review found conflicting evidence regarding functional performance and concluded that there is insufficient evidence to recommend myoelectric prostheses over body-powered prostheses for people with upper-limb amputations.40
Microprocessor-Enabled Prosthesis for Lower-Limb Amputations
Overall, the literature suggests that microprocessor knees result in better or no additional clinical benefits in safety, physical function or mobility, satisfaction, and quality of life compared to body-powered prostheses for people with transfemoral amputations.29,30 These findings align with the published 2009 report by CADTH regarding the clinical and cost-effectiveness of microprocessor knees (C-Leg) for above-the-knee amputations. The CADTH report found that microprocessor knees (C-Leg) improved balance and speed, as well as level and duration of activity.41However, the evidence identified to inform this Rapid Review used a wide variety of measures for safety and function, with some outcomes resulting in conflicting results in the literature. For example, the systematic review by Hahn et al.29 identified more than 90 measures involving a variety of tasks used to assess physical function (e.g., walking on uneven terrain, activities of daily living) across included studies. Both systematic reviews found small sample sizes, high attrition rates, and lack of consideration for confounding variables (e.g., training and learning, accommodation time) across included publications.29,30 Some of the authors of 1 systematic review were employees of relevant manufacturers,29 and another review identified that many of their included publications were funded by manufacturers.30 These conflicts of interest may have influenced review conduct. Hence, the findings of these systematic reviews should be interpreted with caution.
The US Department of Veteran Affairs and Department of Defense suggests prescribing microprocessor knees over nonmicroprocessor knees to reduce falls, optimize functional mobility, and improve satisfaction (weak recommendations based on very low certainty evidence).35 The same guideline suggests energy-storing and return or microprocessor-controlled foot and ankle components over solid-ankle, cushioned-heel feet to improve ambulation and patient satisfaction for prosthetic ambulators (based on very low certainty evidence).35 Additionally, they found insufficient evidence to prescribe any specific storing and return or microprocessor foot and ankle component over others (based on very low certainty of evidence).35 The guideline by Stevens and Wurdeman36 recommends that microprocessor knees be indicated over nonmicroprocessor knees to improve safety, walking capabilities and confidence, mobility, satisfaction, well-being, and quality of life, and to alleviate the cognitive burden of ambulation. However, the same guideline did not account for limitations of the evidence, and it also provided no details about the processes to develop the recommendations.36
One systematic review suggested that microprocessor knees were cost-effective compared to body-powered prostheses.31 The results reported an ICER range between €3,218 per QALY and €40,155 per QALY.31 However, there was considerable heterogeneity across economic evaluations, including time horizon, direct and indirect costs, and threshold of acceptability.31 None of the economic evaluations seemed to have considered the costs associated with stopping the use of microprocessor knees in their cost-effectiveness analysis. There is evidence suggesting some people will stop using their prostheses, which remains a concern in the field of prosthetics.7,42 In 2013, an investigation of upper-limb prosthesis users in British Columbia found that 20% of people with amputations stopped using their prostheses.9 Additionally, none of the economic evaluations were conducted in Canada, and most used a payer’s perspective (3 of 4 relevant economic evaluations included in the systematic review).31 Most economic evaluations evaluated a specific brand of microprocessor knee (i.e., C-Leg), specifically 3 of 4 relevant evaluations. Hence, it is unclear whether findings are applicable in the health care systems of Canada and to all microprocessor knees.31
Considerations for Future Research
Given the research gaps, future endeavours may consider evaluating the clinical effectiveness of advanced prostheses in a more diverse sample with adequate representation of groups of individuals who are typically underrepresented and underserved, including those who are disproportionately impacted, such as populations living in remote areas, in neighbourhoods of low social capital or low socioeconomic status, and Indigenous Peoples living in Canada.
There is evidence to suggest that sex and race may impact clinical outcomes for people with amputations.33-35 This phenomenon requires further investigation, especially within the context of the clinical benefits or harms of advanced prosthesis devices. Currently, the studies that identified race as a confounding variable account for Black, “mixed/other,” and white individuals. Additionally, future studies should ensure comprehensive reporting of their population characteristics to help inform the diversity and applicability of their findings.
Literature on microprocessor-enabled prostheses is limited to microprocessor knees, with no consideration of other components (e.g., sockets or osseointegrated implants, shin, and foot and ankle). Future studies can consider stratifying or adjusting their results by other components of the prostheses to evaluate whether these can influence the benefits of microprocessor knees.
There is some research investigating the potential for artificial intelligence (AI) in prosthetics. AI is being evaluated for its potential to enhance locomotion and control of prostheses.43-46 Additionally, AI may be leveraged to inform personalized treatment approaches for amputation care rehabilitation, including prosthesis prescription.47 However, the use of AI in prosthetics is outside the scope of this report, and requires future exploration.
Additionally, future research can consider evaluating the cost-effectiveness of myoelectric protheses, as we did not identify any relevant literature published in the past 10 years. In general, cost-effectiveness literature on myoelectric and microprocessor-enabled prostheses may consider use a societal perspective that includes direct (e.g., device, warranty) and indirect costs (e.g., training with prosthetists) to ensure applicability to health systems in Canada. They may also consider the cost implications of stopping prosthesis use. None of the studies in this Rapid Review compared prosthesis abandonment between advanced prostheses and body-powered prostheses. Another Rapid Review found that people may stop using their myoelectric prostheses due to function, weight, lack of durability, difficulty to control, lack of sensory feedback, and slow speed response.7 People with upper-limb amputations may stop using their body-powered prostheses due to lack of comfort and function.7
Considerations for Decision- or Policy-Making
An exploratory article on prosthesis design concluded that a device’s performance may not necessarily depend on design and prescription.48 It relies on individual needs, lifestyle, and preferences.48 A review suggested that activity-specific prostheses provide a function advantage for upper-limb amputations.40 Additionally, the same review found that benefits of myoelectric and body-powered prostheses compared to each other or other alternatives may depend on functional needs, control scheme familiarity, and user preference.40 The included evidence-based guidelines also underscored the importance of shared decision-making and patient-centred care in the rehabilitation of amputations.6,35
Health Technology Wales conducted focus groups to identify factors that can influence prosthesis preferences in people with upper-limb amputations.7 Some factors that influence prosthesis preference include activities and participation in life situations (e.g., school or work), their self-image with the prosthesis and their desire to fit in, their perceived need of prosthesis, appearance, costs, size, and functionality of the prosthesis.7 Some guidelines6,35 in this Rapid Review underscore that care should be sensitive to sex, gender, culture, ethnicity, and other dimensions of diversity.6,35 The guidelines highlight patient factors (e.g., sex, race) when discussing the literature on interventions or outcomes.6,35 The guideline on lower-limb amputation suggests “using patient-identified sex to inform individualized rehabilitation plans.”35 While the recommendation is considered weak, supporting evidence shows that the benefits of considering sex in the rehabilitation of lower-limb amputations outweigh the potential harms.35
One guideline stated that the process to receive a properly designed and fitting prosthesis can be burdensome, as it involves “patience, frequent visits, and establishment of realistic expectations based on appropriate patient education, and follow-up training.”6 A review found that body-powered prostheses require shorter training time, require fewer adjustments, and function with less sensitivity to fit.40 Clinicians may wish to consider an individual’s access to services for fitting and training, and willingness to participate, when deciding on an appropriate prosthesis.34,40 Travel may be a barrier, especially for patients who live in rural or remote areas with limited access to rehabilitation services.49 When clinicians consider these factors, it may help alleviate the likelihood that people will stop using their prostheses. In 2013, a cost-analysis on upper-limb prosthesis for adult workers in Canada suggested that there would be cost-savings of $305,922 if the appropriate prostheses are initially prescribed.9
Indigenous Peoples in Canada disproportionately experience nontraumatic lower-limb amputations from unmet health care needs.18-20 While it is recognized that an amputation is an appropriate option and the safest option in some cases, preventing avoidable nontraumatic lower-limb amputations may be a priority area for Indigenous health.36,50,51 Literature suggests that equitable access to Indigenous-focused and culturally appropriate preventive care and chronic disease management services can help prevent avoidable nontraumatic amputations.11,50,51
Clinicians and other decision-makers may use this Rapid Review to inform decision-making regarding advanced prostheses, specifically myoelectric prostheses and microprocessor-enabled prostheses via microprocessor knees. They may wish to consider providing patient-centred care that considers factors such as desired activity levels following amputation, preferences, access to rehabilitation services and prosthesis care, and costs, when providing a prosthesis to people living with amputations.
References
1.Public Health Ontario. Rapid review: Substance use services with, and for, Indigenous communities. 2023. Accessed August 11, 2025. https://www.publichealthontario.ca/-/media/Documents/S/2023/substance-use-services-indigenous-communities.pdf?rev=c50da5f26fea491caf6bfc937a0d9060&sc_lang=en
2.Health Standards Organization. British Columbia Cultural Safety and Humility standard (HSO 75000:2022). 2022. Accessed August 11, 2025. https://healthstandards.org/standard/cultural-safety-and-humility-standard/
3.Efanov JI, Tchiloemba B, Izadpanah A, Harris PG, Danino MA. A review of utilities and costs of treating upper extremity amputations with vascularized composite allotransplantation versus myoelectric prostheses in Canada. JPRAS Open. 2022;32:150-160. doi:10.1016/j.jpra.2022.03.003 PubMed
4.Chung KC, Yoneda H. Upper extremity amputation. UpToDate; 2025. Accessed July 18, 2025. https://www.uptodate.com/contents/upper-extremity-amputation/print?search=amputations&source=search_result&selectedTitle=3%7E78&usage_type=%E2%80%A6
5.War Amps. Amputation levels. Updated July 18, 2025. https://www.waramps.ca/ways-we-help/living-with-amputation/#Levels
6.Department of Veterans Affairs. VA/DoD clinical practice guideline for the management of upper limb amputation rehabilitation version 2. 2022. Accessed July 18, 2025. https://www.healthquality.va.gov/guidelines/Rehab/ULA/VADoDULACPG_Final_508.pdf
7.Health Technology Wales. Multi-grip myoelectric upper limb prosthetics. 2023. Accessed July 18, 2025. https://healthtechnology.wales/reports-guidance/multigrip-upper-limb-prosthetics/
8.Henson A. Terminal device overview. 2022. Updated August 18, 2025. https://www.armdynamics.com/upper-limb-library/terminal-device-overview
9.Chan A, Kwok E, Bhuanantanondh P. Cost of ownership of upper limb prostheses: A retrospective analysis. CMBES Proc. 2013;36. Accessed August 7, 2025. https://proceedings.cmbes.ca/index.php/proceedings/article/download/402/396
10.Kalapatu V. Lower extremity amputation. UpToDate; 2025. Accessed August 7, 2025. https://www.uptodate.com/contents/lower-extremity-amputation/print?search=amputations&source=search_result&selectedTitle=1%7E78&usage_type=%E2%80%A6
11.Canadian Institute of Health Information. Amputations signal opportunities to improve diabetes care and reduce system costs. 2024. Accessed July 18, 2025. https://www.cihi.ca/en/equity-in-diabetes-care-a-focus-on-lower-limb-amputation/amputations-signal-opportunities-to-improve-diabetes-care-and-reduce-system-costs
12.de Mestral C, Hussain MA, Austin PC, et al. Regional health care services and rates of lower extremity amputation related to diabetes and peripheral artery disease: an ecological study. CMAJ Open. 2020;8(4):E659-E666. doi:10.9778/cmajo.20200048 PubMed
13.Hussain MA, Al-Omran M, Salata K, et al. Population-based secular trends in lower-extremity amputation for diabetes and peripheral artery disease. Cmaj. 2019;191(35):E955-E961. doi:10.1503/cmaj.190134 PubMed
14.Imam B, Miller WC, Finlayson HC, Eng JJ, Jarus T. Incidence of lower limb amputation in Canada. Can J Public Health. 2017;108(4):e374-e380. doi:10.17269/cjph.108.6093 PubMed
15.Berke GM, Buell NC, Fergason JR, et al. Tranfemoral amputation: The basics and beyond 2008. Accessed July 18, 2025. http://www.oandplibrary.org/assets/pdf/Transfemoral_Amputation_the_Basics_and_Beyond.pdf
16.Medical center orthotics & prosthetics. Knee disarticulation. Updated August 7, 2025. https://mcopro.com/glossary/knee-disarticulation/
17.Imam B, Miller WC, Finalyson HC, Eng JJ, Jarus T. Lower limb prosthetic rehabilitation in Canada: A survey study. Physiother Can. 2019;71(1):11-21. doi:10.3138/ptc.2017-39 PubMed
18.Blanchette V, Patry J, Brousseau-Foley M, et al. Diabetic foot complications among Indigenous peoples in Canada: a scoping review through the PROGRESS-PLUS equity lens. Front Endocrinol (Lausanne). 2023;14:1177020. doi:10.3389/fendo.2023.1177020 PubMed
19.Essien SK, Linassi G, Larocque M, Zucker-Levin A. Incidence and trends of limb amputation in first nations and general population in Saskatchewan, 2006-2019. PLoS ONE. 2021;16(7):e0254543. doi:10.1371/journal.pone.0254543 PubMed
20.Isa D, Pace D. Is ethnicity an appropriate measure of health care marginalization? A systematic review and meta-analysis of the outcomes of diabetic foot ulceration in Aboriginal populations. Can J Surg. 2021;64(5):E476-E483. doi:10.1503/cjs.004619 PubMed
21.Asiniwasis R, Stonechild AB, Queen D, Sibbald RG. Indigenous Diabetic Foot-Related Lower Extremity Amputations: Integrating Traditional Indigenous and Western Health Models for Improved Outcomes. Adv Skin Wound Care. 2023;36(2):63. doi:10.1097/01.ASW.0000905664.97542.fd PubMed
22.War Amps. Prosthetic knees for adults. Updated August 7, 2025. https://www.waramps.ca/pdf/english-site/ways-we-help/artificial-limbs-and-devices/lower-limb/knees-for-adults.pdf
23.Howard CW, Saraswat DK, McLeod G, Yeung A, Jeong D, Lam J. Canada's Prosthetic Coverage: a Review of Provincial Prosthetic Policy. Can Prosthet Orthot J. 2019;2(2):33489. doi:10.33137/cpoj.v2i2.33489 PubMed
24.Dorset UH. The provision of microprocessor controlled prosthetic knees. Accessed August 8, 2025. https://www.uhd.nhs.uk/uploads/about/docs/our_publications/patient_information_leaflets/dpc/16_provision_of_microprocessor_controlled_prosthetic_knees.pdf
25.Petlock A, DiMario K. Access to artificial limbs: The patient's perspective according to the War Amps of Canada. Can Prosthet Orthot J. 2021;4(2):35972. doi:10.33137/cpoj.v4i2.35972 PubMed
26.Solomonov D. Prosthetic arm costs and financing: A comprehensive guide. 2021. Accessed August 7, 2025. https://groupenroll.ca/prosthetic-arm-costs-guide/#:~:text=Myoelectric%20arms%20fall%20into%20the,may%20cost%20less%20than%20%2420%2C000.
27.Hitzig SL, Zidarov D, MacKay C, et al. An environmental scan of limb loss rehabilitation centers across Canada. Prosthet Orthot Int. 2025;49(2):248-255. doi:10.1097/pxr.0000000000000405 PubMed
28.Martinic MK, Pieper D, Glatt A, Puljak L. Definition of a systematic review used in overviews of systematic reviews, meta-epidemiological studies and textbooks. BMC Med Res Methdol. 2019;19:203. doi:10.1186/s12874-019-0855-0 PubMed
29.Hahn A, Bueschges S, Prager M, Kannenberg A. The effect of microprocessor controlled exo-prosthetic knees on limited community ambulators: systematic review and meta-analysis. Disabil Rehabil. 2022;44(24):7349-7367. doi:10.1080/09638288.2021.1989504 PubMed
30.Thibaut A, Beaudart C, Maertens DENB, Geers S, Kaux JF, Pelzer D. Impact of microprocessor prosthetic knee on mobility and quality of life in patients with lower limb amputation: a systematic review of the literature. Eur J Phys Rehabil Med. 2022;58(3):452-461. doi:10.23736/s1973-9087.22.07238-0 PubMed
31.Donnelley CA, Shirley C, von Kaeppler EP, et al. Cost Analyses of Prosthetic Devices: A Systematic Review. Arch Phys Med Rehabil. 2021;102(7):1404-1415.e2. doi:10.1016/j.apmr.2021.02.010 PubMed
32.Resnik L, Borgia M, Cancio J, et al. Dexterity, activity performance, disability, quality of life, and independence in upper limb Veteran prosthesis users: a normative study. Disabil Rehabil. 2022;44(11):2470-2481. doi:10.1080/09638288.2020.1829106 PubMed
33.Resnik L, Borgia M, Clark M. Function and Quality of Life of Unilateral Major Upper Limb Amputees: Effect of Prosthesis Use and Type. Arch Phys Med Rehabil. 2020;101(8):1396-1406. doi:10.1016/j.apmr.2020.04.003 PubMed
34.Resnik L, Borgia M, Heinemann AW, Clark MA. Prosthesis satisfaction in a national sample of Veterans with upper limb amputation. Prosthet Orthot Int. 2020;44(2):81-91. doi:10.1177/0309364619895201 PubMed
35.Department of Veterans Affairs. VA/DOD clinical practice guideline for rehabilitation of individuals with lower limb amputation version 3. 2024. Accessed July 18, 2025. https://www.healthquality.va.gov/guidelines/Rehab/amp/LLA-CPG_2024-Guideline_final_20250110.pdf
36.Stevens PM, Wurdeman SR. Prosthetic Knee Selection for Individuals with Unilateral Transfemoral Amputation: A Clinical Practice Guideline. Jpo. 2019;31(1):2-8. doi:10.1097/jpo.0000000000000214 PubMed
37.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. doi:10.1016/j.jclinepi.2009.06.006 PubMed
38.Center for Medicare & Medicaid Services. Lower limb prosthetic workgroup consensus document. 2017. Accessed August 7, 2025. https://www.cms.gov/Medicare/Coverage/DeterminationProcess/downloads/LLP_Consensus_Document.pdf
39.Statistics Canada. Health care access and experiences among Indigenous people. 2024. Accessed August 8, 2025. https://www150.statcan.gc.ca/n1/daily-quotidien/241104/dq241104a-eng.htm
40.Carey SL, Lura DJ, Highsmith MJ. Differences in myoelectric and body-powered upper-limb prostheses: Systematic literature review. J Rehabil Res Dev. 2015;52(3):247-62. doi:10.1682/jrrd.2014.08.0192 PubMed
41.Ho C, Fitzsimmons H. Microprocessor-Controlled Prosthetic Knees (C-Leg) for Patients with AboveKnee Amputations: A Review of the Clinical- and Cost-Effectiveness. Canadian Agency for Drugs and Technologies in Health; 2009. Accessed August 20, 2025. https://www.cda-amc.ca/sites/default/files/pdf/L0101_C-Leg_Prostheses_final.pdf
42.Biddiss EA, Chau TT. Upper limb prosthesis use and abandonment: A survey of the last 25 years. Prosthet Orthot Int. 2007;31(3):236-257. doi:10.1080/03093640600994581 PubMed
43.Ahkami B, Kristoffersen MB, Ortiz-Catalan M. Real-time locomotion mode detection in individuals with transfemoral amputation and osseointegration. J Neuroengineering Rehabil. 2025;22(1):142. doi:10.1186/s12984-025-01672-2 PubMed
44.Ameri A, Akhaee MA, Scheme E, Englehart K. A Deep Transfer Learning Approach to Reducing the Effect of Electrode Shift in EMG Pattern Recognition-Based Control. IEEE Trans Neural Syst Rehabil Eng. 2020;28(2):370-379. doi:10.1109/tnsre.2019.2962189 PubMed
45.Bruni G, Marinelli A, Bucchieri A, et al. Object stiffness recognition and vibratory feedback without ad-hoc sensing on the Hannes prosthesis: A machine learning approach. Front. 2023;17:1078846. doi:10.3389/fnins.2023.1078846 PubMed
46.Edwards AL, Dawson MR, Hebert JS, et al. Application of real-time machine learning to myoelectric prosthesis control: A case series in adaptive switching. Prosthet Orthot Int. 2016;40(5):573-81. doi:10.1177/0309364615605373 PubMed
47.Carrasquillo C, Zhou S, Childers WL, Young A, Herrin K. A clinical decision-making algorithm for the personalized prescription of microprocessor-controlled prosthetic knees: An evidence-based approach based on a randomized trial. Prosthet Orthot Int. 2025;05:05. doi:10.1097/pxr.0000000000000462
48.Engdahl SM, Gonzalez MA, Lee C, Gates DH. Perspectives on the comparative benefits of body-powered and myoelectric upper limb prostheses. J Neuroengineering Rehabil. 2024;21(1):138. doi:10.1186/s12984-024-01436-4 PubMed
49.Smith LPR. Challenging health service delivery models to improve access to physical therapy in rural, remote, and northern communities. Front Rehabil Sci. 2022;3doi:10.3389/fresc.2022.892038
50.Maamwesying. Lower limb preservation. Updated July 18, 2025. https://maamwesyingontariohealthteam.com/key-initiatives/lower-limb-preservation
51.Wees T, Pandey M, Nicolay S, Windigo J, Bitternose A, Kopriva D. Identifying barriers to preventive care among First Nations people at risk of lower extremity amputation: a qualitative study. CMAJ Open. 2023;11(5):E906-E914. doi:10.9778/cmajo.20220150 PubMed
52.Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. doi:10.1136/bmj.j4008 PubMed
53.Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377-384. doi:10.1136/jech.52.6.377 PubMed
54.Agree Next Steps Consortium. The AGREE II Instrument. AGREE Enterprise; 2017. Accessed July 18, 2025. https://www.agreetrust.org/wp-content/uploads/2017/12/AGREE-II-Users-Manual-and-23-item-Instrument-2009-Update-2017.pdf
55.Cochrane methods. Progress-PLUS. Accessed July 18, 2025. https://methods.cochrane.org/equity/projects/evidence-equity/progress-plus
56.Canada's Drug Agency. Canada's Drug Agency style: A guide for Author's and Editor's. 2025. Accessed July 18, 2025. https://www.cda-amc.ca/style-guide
Appendix 1: Detailed Methods and Selection of Included Studies
Please note that this appendix has not been copy-edited.
What Is a Rapid Review?
Rapid reviews are based on accelerated and abbreviated systematic review methods, balancing timeliness with rigour, to allow for timely decision-making. Due to these abbreviated methods, rapid reviews have some limitations. For example, we included studies published from 2015, excluding older studies. We attempted to mitigate this by searching for and including relevant systematic reviews published in the past 10 years that included older studies. Focusing on more recently published articles may also be more reflective of current practices.
Literature Search Methods
An information specialist conducted a literature search on key resources including MEDLINE, the Cochrane Database of Systematic Reviews, the International HTA Database, the websites of health technology assessment agencies in Canada and major international HTA agencies, as well as a focused internet search. The search approach was customized to retrieve a limited set of results, balancing comprehensiveness with relevance. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. Search concepts were developed based on the elements of the research questions and selection criteria. The main search concepts were myoelectric prosthesis, microprocessor-enabled prosthesis, and amputation. The search was completed on July 14, 2025 and limited to English-language documents published since January 1, 2015. The full search strategy is available upon request.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1. For research questions 1 through 4, we limited study designs of interest to systematic reviews, including those systematic reviews within health technology assessments. When no systematic reviews were available, we included primary studies that met the review’s eligibility criteria.
Exclusion Criteria
Articles were excluded if they:
did not meet the selection criteria outlined in Table 1
were duplicate publications or were published before 2015
were systematic reviews in which all relevant studies were captured in other more recent or more comprehensive systematic reviews
were systematic reviews without a research question, a reproducible search strategy, selection criteria, screening methods, critical appraisal or risk of bias assessment, or information about data analysis and synthesis that allows for reproducibility28
were primary studies captured in 1 or more included systematic reviews
were guidelines with unclear methodology
were studies that evaluated the difference in kinetic or biomechanic outcomes between advanced prosthesis types and body-powered prostheses
were health technology assessments with abbreviated systematic review methods
Critical Appraisal of Individual Studies
The included publications were critically appraised 1 reviewer using the following tools as a guide: A MeaSurement Tool to Assess systematic Reviews 2 (AMSTAR 2)52 for systematic reviews and the Downs and Black checklist53 for randomized and nonrandomized studies. For guidelines, the included publications were critically appraised by 1 reviewer using Appraisal of Guidelines for Research and Evaluation (AGREE) II instrument.54 Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Data Extraction
One reviewer extracted data directly into standardized tables created in Microsoft Word, which were modified as necessary. The extracted information included study characteristics, methodology (e.g., study design), population, intervention, comparator, and results regarding the outcomes of interest.
One reviewer extracted information from the included systematic reviews and primary studies using the PROGRESS-Plus tool55 to describe different population groups. Each included study was checked to determine if PROGRESS-Plus55 criteria were reported by study authors to describe the participants; detailed characteristics, if available, were then extracted and reported in tables in Appendix 3. The main PROGRESS-Plus55 criteria include place of residence; race, ethnicity, culture, and/or language; occupation; gender and/or sex; religion; education; socioeconomic status; and social capital. As part of report writing, we discuss these characteristics across the evidence, where available, when presenting results within the text.
When reporting on sex, gender, race, or ethnicity in this Rapid Review, we planned to retain the language used by the original study authors, and, whenever possible, we referred to these groups based on guidance from Canada’s Drug Agency Style: A Guide for Authors and Editors56 at the time this Rapid Review was conducted, with an understanding that language is constantly evolving.
Patient Engagement
By understanding the needs of the requestor, internal capacity, and timeliness associated with this Rapid Review, we did not conduct any patient engagement with people living with an upper- or lower-body amputation to inform this work. We acknowledge this as a limitation of our report.
Appendix 2: Selection of Included Studies
Please note that this appendix has not been copy-edited.
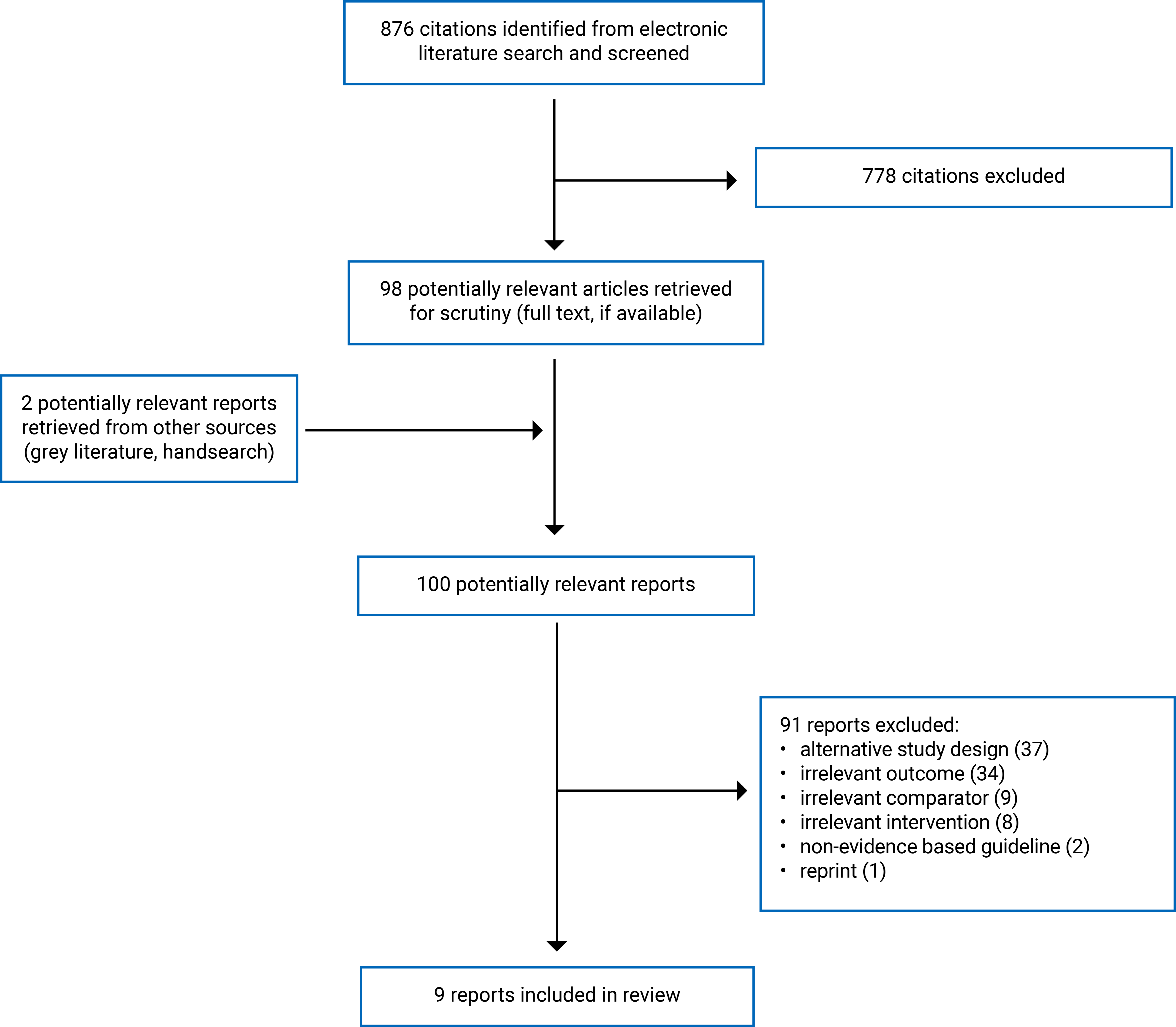
Appendix 3: Characteristics of Included Publications
Table 2: Characteristics of Nonrandomized Studies for Question 1
Study citation, country, funding source | Study design | Population characteristics | Relevant Interventions and comparators | Clinical outcomes |
|---|---|---|---|---|
Question 1: Clinical effectiveness of myoelectric prosthesis | ||||
Resnik et al. (2022)32 Country: US Funding source: Orthotics and Prosthetics Outcomes Research Program, Prosthetics Outcomes Research Award | Cross-sectional, observational study | People with unilateral and bilateral upper limb amputations recruited across 5 US sites. N = 127 Unilateral amputation: 112 (88.2%) Amputation type (unilateral only)
Age, mean (SD) = 56.9 (16.5) years Gender, males: 123 (96.9%)a Gender, females: 4 (3.2%)a Race White: 95 (74.8%) Black: 12 (11.0%) Mixed/other: 18 (14.2%) Ethnicity Hispanic: 16 (12.6%) Not Hispanic: 107 (84.3%) Unknown: 4 (3.2%) Military Status Veterans: 108 (85.0%) Active duty: 2 (1.6%) Civilians: 17 (13.4%) Etiology of Amputation Congenital: 4 (8.9%) Combat: 38 (35.9%) Accident: 58 (54.7%) Burn: 10 (9.4%) Cancer: 5 (4.7%) Diabetes: 1 (0.9%) Infection: 15 (14.2%) Prosthesis Training A quarter of the study population received prosthesis training for their device. Other PROGRESS-Plus Criteria SES: NR Place of residence: NR Education: NR Religion: NR Social Capital: NR | Interventions:
Comparator: Body-powered prosthesis (59% of study participants) Note: Researchers classified all hybrid devices as myoelectric | Outcomes:
|
Resnik et al. (2020)33 Country: US Funding source: Orthotics Research Program, Prosthetics Outcome Research Award | Cross-sectional survey | Veterans with unilateral upper limb amputation who received care in the Veterans Affairs between 2010 and 2015. N = 755b Users of prostheses relevant to this report: 427 (56.5%) Age Body-powered, mean (SD) = 65.8 (12.4) years Myoelectric prostheses (single-DOF), mean (SD) = 58.7 (15.9) years Myoelectric prostheses (multi- degrees of freedom), mean (SD) = 63.9 (10.4) years Sex, male: 422 (98.8%)a Sex, female: 21 (2.8%)a Time since initial amputation Body-powered prostheses, mean (SD) = 36.6 (17.4) years Myoelectric prostheses (single degree of freedom), mean (SD) = 25.7 (18.4) years Myoelectric prosthesis (multi- degrees of freedom), mean (SD) = 32.8 (17.8) years Race White: 328 (76.8%) Black: 42 (9.8%) Other, including mixed race: 19 (4.5%) Missing: 38 (8.9%) Ethnicity (Hispanic or Latino) Yes: 35 (8.2%) No: 373 (87.4%) Missing: 19 (4.4%) Etiology of Amputationc: Combat injury: 190 (44.5%) Accident: 268 (62.8%) Burn: 45 (10.5%) Cancer: 7 (1.6%) Diabetes: 3 (0.7%) Infection: 41 (9.6%) Amputation of dominant side: Yes: 227 (53.2%) No: 198 (46.4%) Missing: 2 (0.4%) Amputation level: Forequarter: 8 (1.9%) At the shoulder joint: 15 (3.5%) Above the elbow: 95 (22.2%) At the elbow: 19 (4.5%) Below the elbow: 197 (46.1%) At the wrist joint: 93 (21.8%) Prosthesis training Yes: 329 (77.1%) No: 95 (22.2%) Missing: 3 (0.7%) Other PROGRESS-Plus Criteria SES: NR Place of residence: NR Education: NR | Intervention:
Comparators: Body-powered prosthesis (n = 325) | Outcomes: Physical Function via measures of
Quality of Life
|
Resnik et al. (2020)34 Country: US Funding source: US army medical research acquisition activity | Cross-sectional survey | Veterans with major upper limb amputation who received any type of medical care from the Veterans Affairs between 2010 and 2015. N = 449b Users of prostheses relevant to this report: 427 (95.1%) Age Body-powered prostheses, mean (SD) = 65.5 (12.7) years Myoelectric or hybrid prostheses, mean (SD) = 55.7 (15.4) years Gender, male: 422 (98.8%)a Gender, female: 8 (1.8%)a Time since initial amputation Body-powered prostheses, mean (SD) = 36.3 (17.6) years Myoelectric or hybrid prostheses, mean (SD) = 23.5 (17.1) years Race White: 328 (76.8%) Black: 42 (9.8%) Other, including mixed race: 19 (4.5%) Unknown: 38 (8.9%) Ethnicity (Hispanic or Latino) Yes: 35 (8.2%) No: 373 (87.3%) Unknown: 19 (4.5%) Amputation level Forequarter: 8 (1.9%) At the shoulder joint: 15 (3.5%) Above the elbow: 95 (22.2%) At the elbow: 19 (4.5%) Below the elbow: 197 (46.1%) At the wrist joint: 93 (21.8%) Etiology of Amputationc Combat injury: 190 (44.5%) Accident: 268 (62.8%) Burn: 45 (10.5%) Cancer: 7 (1.6%) Diabetes: 3 (0.7%) Infection: 41 (9.6%) Other PROGRESS-Plus Criteria SES: NR Place of residence: NR Education: NR Religion: NR Social Capital: NR | Intervention: Myoelectric prostheses including hybrid devices (n = 93) Comparator: Body-powered prosthesis (n = 334) | Outcomes: Satisfaction (i.e., Modified Trinity Amputation and Prosthesis Experience Scales – Satisfaction Scale; Orthotics and Prosthetics Users’ Survey Client Satisfaction with devices Scale) |
DASH = disabilities of the arm, shoulder, and hand; DOF = degree of freedom; NR = not reported; RAND = research and development; SD = standard deviation; SES = socioeconomic status.
Note: This table has not been copy-edited.
Note: PROGRESS-Plus55 guided data extraction for population characteristics of primary studies included in this current review. DOF describes the terminal device of myoelectric prostheses.
aThe study did not define or differentiate between sex and gender.
bValue reported encompasses study participants not relevant to this report (i.e., nonusers or cosmetic devices).
cStudy participants can be included in more than 1 category.
Table 3: Characteristics of Included Systematic Reviews
Study citation, countries of eligible studies, funding source | Study designs, included studies, and search strategy | Population characteristics | Intervention and comparator(s) | Relevant outcomes, length of follow-up |
|---|---|---|---|---|
Question 2: Clinical effectiveness of microprocessor-enabled prosthesis | ||||
Hahn et al. (2022)29 Country: Authors did not report on the location of included primary studies. Funding source: None reported. | Study design: Systematic review with meta-analysis. Number of included studies: 15, including 13 NRS and 2 crossover RCT. (All are relevant to this current review) Search strategy: Electronic database search in MEDLINE, Cochrane Library, CINAHL Complete, Embase, Google Scholar, as well as Databases DARE, Cirrie, PEDro, and OTseeker with the search term logic adapted to their search. | People with transfemoral or amputations above the knee with a mobility grade equivalent to MCFL-2 or low mobility. N = 704 Sex, male (n): 542 (76.9%) Sex, female (n): 161 (22.9%) Age: Mean age ranged from 57.1 to 69 years across included studies. Etiology: Vascular disease: 255 Trauma: 202 Other: 225 Other PROGRESS-Plus criteria: NR; Review authors did not report on population characteristics by gender, SES, race or ethnicity, education, place of residence (urban, rural, or remote), religion. It is unclear if primary studies reported these characteristics for their sample. | Intervention: Microprocessor knees (e.g., C-Leg, C-Leg compact, Genium, K) Comparator: Nonmicroprocessor knees | Outcomes:
Follow-up: ranges from 1 week to 6 months Outcomes included in meta-analysis:
|
Thibaut et al. (2022)30 Country: Authors did not report on the location of included primary studies. Funding source: Author’s salary partially paid by Fonds Neurologic and Functional Rehabilitation Center | Study design: Systematic review. Number of included studies: 18, including 3 crossover RCTs and 12 NRS (17 studies are relevant to this review). Literature search strategy: Electronic database search on MEDLINE, Scopus, and SPORTDiscus for relevant publications from 1946 to February 15, 2021. They also conducted a manual search of bibliographies in relevant papers. | People with unilateral transfemoral limb loss N (range) = 993 (20 to 602). Age: mean age ranged from 38.5 to 69 years across included studies Sex and genderb, male (%) = 766 (77.1%) Sex and genderb, female: NR Etiology of limb loss: Review authors reported by study. The review includes people with vascular disease (including diabetes), arterial disease, tumours, infection, nonvascular diabetes, congenital limb loss. Other PROGRESS-Plus criteria: NR; Review authors did not report on population characteristics, such as SES, race or ethnicity, education, place of residence, religion, occupation and education. It is unclear if primary studies reported these characteristics for their sample. | Intervention: Microprocessor knees Comparator: Nonmicroprocessor knees | Outcome:
Follow-up: 1 week to 6 months |
Question 4: Cost-effectiveness of microprocessor-enabled prosthesis | ||||
Donnelley et al. (2021)31 Denmark, Italy, Sweden, and the US Funding source: Not reported. | Study design: Systematic review of economic evaluations. Number of included studies: 12 economic evaluations (4 are relevant to this current review) Literature search strategy: Electronic database search of PubMed, Embase, and Web of Science search engines for economic evaluations published before May 2, 2019. | People with upper- or lower- extremity amputation using a prosthesis (the 4 relevant economic evaluations were conducted considering people with a transfemoral amputation). n, relevant studiesc = Approximately 273 Other PROGRESS-Plus criteria: NR; Review authors did not report on population characteristics, such as age, sex, gender, SES, race or ethnicity, education, place of residence, religion, occupation, and education. It is unclear if included economic evaluations reported these characteristics for their sample. | Intervention: Prosthesis-related devices, inclusive of microprocessor knees Comparison: Other prosthesis-related devices, inclusive of nonmicroprocessor knees. | Outcomes: ICER Analysis type: cost-utility Perspective: payer (3 studies), societal (1 study) Time Horizon: ranges between 5 to 10 years across relevant included economic evaluations. |
CINAHL = Cumulative Index to Nursing and Allied Health Literature; Embase = Excerpta Medica Database; DARE = Database of Abstracts of Review of Effects; ICER = incremental cost-effectiveness ratio; PEDro = Physiotherapy Evidence Database; MCFL-2 = Medicare functional classification level 2; NA = not applicable; NR = not reported; NRS = nonrandomized studies; OT = occupational therapy; SES = socioeconomic status.
Note: This table has not been copy-edited.
Note: PROGRESS-Plus55 guided data extraction of systematic reviews included in this current review. We acknowledge that sex is assigned at birth and based on genetics, whereas gender refers to an individual’s social experience of being a man, woman, trans, or identifying outside gender confines. None of the studies defined how researchers identified sex or gender.
aMedicare functional classification level 2 means the individual was assessed with the ability or potential for ambulation with ability to traverse low level environmental barriers (e.g., curbs, stairs, uneven surfaces), which is typical of a “limited community ambulator.”38
bThe systematic review by Thibault et al.30 did not differentiate between sex and gender. It is unclear whether included studies in the systematic review defined or differentiated these terms.
cAn included economic evaluation included in the systematic review by Donnelley et al.31 did not disclose the total number of their sample population.
Table 4: Characteristics of Included Guidelines for Question 5
Intended users, target population | Intervention and practice considered | Major outcomes considered | Evidence collection, synthesis, and quality assessment | Recommendations development and evaluation | Guideline validation |
|---|---|---|---|---|---|
Department of Veterans Affairs and the Department of Defense (2024)35 | |||||
Intended users: Veterans Affairs or Department of Defense, community providers, and others involved in the health care team caring for adults with lower-limb amputation. Target population: Adults (ages 18+) who have had a lower-limb amputation, including those receiving care within the Veterans Affairs and Department of Defense health care delivery systems in the US. | An evidence-based framework for evaluating and managing the target population. Prosthetic interventions (e.g., microprocessor knees, rehabilitation interventions, surgical interventions, and behavioural health or psychosocial interventions). | Short, intermediate, and long-term clinical benefits and harms of relevant interventions (e.g., functional status, quality of life, satisfaction and falls), when available. | A systematic search conducted in multiple electronic databases for English-only systematic reviews and clinical studies published from July 6, 2016 to March 15, 2024. The results of the relevant studies were summarized qualitatively. A focus group was created through a convenience sample and consisted of 9 participants who received care from the Veterans Affairs and/or the Department of Defense for their amputation care or rehabilitation. The focus group was conducted to understand patient’s perspectives on their treatment and overall care to inform guideline development. The risk of bias of primary studies was assessed using the US Preventive Services Task Force method. | The Lower-Limb Amputation Work Group developed recommendations informed by the systematic review. They determined the strength and direction of each recommendation by assessing the quality of the overall evidence base, the associated benefits and harms, patient values and preferences, and other implications. The strength of the recommendation was determined by the GRADE approach. | The Lower-Limb Amputation Work Group internally reviewed the first 2 drafts. Experts identified from Veterans Affairs and Department of Defense health care systems reviewed the draft. The lower-limb Amputation Work Group presented the guidelines to the Veterans Affairs and Department of Defense Evidence-Based Practice Work Group for approval. |
Department of Veterans Affairs and the Department of Defense (2022)6 | |||||
Intended users: Health care providers caring for patients with an upper limb amputation, specifically rehabilitation care providers like physicians, therapists, and prosthetists. Target population: Adults with an upper limb amputation, including veterans, service members, military retirees, and beneficiaries. | Evidence-based practices on the target population. Prevention and treatment of phantom and residual limb pain, clinical assessments and outcome tools, psychosocial interventions, surgical procedures and medical interventions, and rehabilitation and prosthetic interventions. | Short, intermediate, and long-term clinical benefits and harms of rehabilitation strategies (e.g., functional status, independence, pain, mental health, and satisfaction), when available. | A systematic evidence review with a search involving multiple electronic databases of English-only systematic reviews and clinical studies published between February 1, 2013, and April 30, 2021. The results of relevant literature were qualitatively summarized. A focus group was created through a convenience sample and consisted of 9 participants, 6 of which were veterans who received care from Veterans Affairs and 4 were service members who received care from the Department of Defense. The focus group was conducted to understand patient’s perspectives on their treatment and overall care to inform guideline development. The risk of bias of relevant primary studies was assessed using the US Preventive Services Task Force method. | The Management of Upper Limb Amputation Rehabilitation Work Group (46 members) developed recommendations informed by the systematic review. They determined the strength and direction of each recommendation by assessing the quality of the overall evidence, the associated benefits and harms, patient values and preferences, and other implications. The strength of the evidence was determined by the GRADE approach. | The Management of the Upper Limb Amputation Work Group internally reviewed the first 2 drafts of the guidelines. Experts identified from Veterans Affairs and Department of Affairs were invited to provide feedback for the Work Group to consider The Management of the Upper Limb Amputation Work Group presented the guidelines to the Veterans Affairs and Department of Defense Evidence-Based Practice Work Group for approval. |
Stevens and Wurdeman (2019)36 | |||||
Intended users: Prosthetists, referring surgeons and physicians, treating physical therapists, and policy-makers. Target population: Adults with unilateral lower-limb absence whether congenital or acquired because of dysvascular, traumatic, or other etiology. | Present the highest level of evidence on prosthetic knee joint selection. Specifically, microprocessor-regulated knees were compared to nonmicroprocessor-regulated knees. Microprocessor knees in this guideline are specific to swing and stance | The outcomes considered were comparative effectiveness, and the benefits and harms of treatments. | A systematic literature search involving 1 electronic database of systematic reviews, meta-analyses, and published prescription guidelines published up to April 2017. Evidence statements or supported narrative statements were extracted from relevant literature. The quality and certainty of the evidence used to inform recommendations was not assessed. | Beyond being informed with a systematic review, the guideline did not provide additional details about recommendation development. Recommendations were not evaluated and lacked level of certainty or a grade. | The guidelines do not report any validation of recommendations. |
GRADE = Grading of Recommendations Assessment, Development and Evaluation.
Note: This table has not been copy-edited.
Appendix 4: Critical Appraisal of Included Publications
Please note that this appendix has not been copy-edited.
Table 5: Clinical Effectiveness of Myoelectric Prosthesis for Question 1: Strengths and Limitations of Cross-Sectional Studies Using the Downs and Black Checklist53
Strengths | Limitations |
|---|---|
Resnik et al. (2022)32 | |
Researchers clearly described the objective of the study. They also clearly described the interventions of interest and main outcomes, including how measures should be interpreted. Researchers provided a satisfactory description of study population demographics (e.g., gender, race, ethnicity, employment status, military status, etiology of amputation, training) and characteristics of prosthesis used (i.e., terminal device type). Additionally, they described demographics and prosthesis type by amputation type, specifically unilateral and bilateral amputations. No individuals lost to follow-up based on study design (i.e., cross-sectional design). All study participants were recruited from the same population. Researchers reported simple outcome data, estimates of random variability, and actual P values, when appropriate. The researchers used appropriate statistical tests to assess the main outcomes. The main outcome measures seem valid and reliable. Researchers conducted Benjamin-Hochberg method to adjust for false discovery rates from multiple comparisons. Researchers declared the source of funding and declared no conflict of interests. | The study did not measure adverse events from the interventions. Researchers used a convenience sample to recruit individuals for this study. The researchers described the distribution of potential confounders in the study population (e.g., age, training for prosthesis, terminal device type). However, they did not evaluate the differences in distribution between study groups, nor did they adjust for confounding variables (e.g., experience with prosthesis use and training) The recruitment strategy used a convenience sample without details regarding the period of recruitment. Hence, the study population may not be representative of the entire population from which the researchers recruited from. The study sample was mostly men. It is likely that the study sample is not representative of the entire population of interest. The staff, places, and facilities may not be representative of most of the population of interest may receive. The study recruited individuals from 6 US sites, which are not described. It is unclear how the findings apply to health settings and population of interest located in Canada. The research design (i.e., cross-sectional) and intervention limits the potential to randomize participants into study arms. Additionally, the nature of the study design and intervention limits the ability to conceal treatment from researchers and study participants involved in the study. Researchers did not calculate whether the study had sufficient power to detect a statistically significant effect. The study had a small sample size (n = 127). |
Resnik et al. (2020)33 | |
Researchers clearly described the objective of the study. They also clearly described the interventions of interest and main outcomes. Researchers published literature to describe the development and pilot testing of the survey instrument. Researchers provided a satisfactory description of study population demographics (e.g., sex, race, ethnicity, employment status, etiology of amputation, training) All study participants were recruited from the same population during the same period. Researchers reported estimates of random variability, and actual P values, when appropriate. The researchers used appropriate statistical tests to assess the main outcomes. The main outcome measures seem valid and reliable. It seems that researchers did not conduct any unplanned analysis. No individuals lost to follow-up based on study design (i.e., cross-sectional design). Researchers reported no conflicts of interest and disclosed funding sources. Researchers conducted a bivariate linear regression to identify potential confounders. They adjusted for identified confounders (P < 0.10) in their regression analysis for main outcomes. | The study did not measure adverse events from the interventions. It is unclear whether study participants are representative of the population from which researchers recruited from. Researchers did not describe individuals that opted out from participating in the study. It is unclear how they may have impacted findings. Researchers recruited the study population mostly of male (> 90%) US veterans. It is likely that this study population does not reflect the entire population of interest. Additionally, researchers used a sampling frame consisting of veterans receiving care from US Veterans Affairs. It is unclear how applicable these findings are to health settings in Canada, and if the staff, places, and facilities are representative of the population of interest experience when seeking care. The research design (i.e., cross-sectional) and intervention limits the potential to randomize participants into study arms. Additionally, the nature of study design and intervention limits the ability conceal the intervention from researchers and study participants involved in the study. Researchers did not provide details on how they addressed missing data. It is unclear how these may have impacted findings. The study lacks statistical analysis to adjust for multiplicity (there are multiple outcomes investigating function). Researchers suspect that the study may have been under powered to detect differences by certain prosthesis configuration subgroups due to their small size. Individuals with missing data on terminal devices were categorized as single-DOF myoelectric prostheses. It is unclear how the misclassification may have impacted findings. Overlap of study population with a cross-sectional study34 funded by US army included in this report is unclear. |
Resnik et al. (2020)34 | |
Researchers clearly described the objective of the study. They also clearly described the interventions of interest and main outcomes. Researchers provided a satisfactory description of study population demographics (e.g., gender, race, ethnicity, employment status, etiology of amputation, training). Researchers conducted general linear regression models to identify confounders (P < 0.20) for consideration in their analysis of main outcomes. Researchers reported estimates of random variability, and actual P values, when appropriate. All study participants were recruited from the same population during the same period. Researchers reported estimates of random variability, and actual P values, when appropriate. The researchers used appropriate statistical tests to assess the main outcomes. It seems that the main outcome measures used in the study were valid and reliable. It seems that researchers did not conduct any unplanned analysis. No individuals lost to follow-up based on study design (i.e., cross-sectional design). Researchers declared funding source and no conflicts of interest. | The study did not measure adverse events from the interventions. The research design (i.e., cross-sectional) and intervention limits the potential to randomize participants into study arms. Additionally, the nature of the study design and intervention limits ability to conceal the intervention from researchers and study participants involved in the study. It is unclear whether study participants are representative of the population from researchers recruited from. Researchers did not describe individuals that opted out from participating in the study. It is unclear how they may have impacted the findings. Researchers recruited the study population mostly of older male (> 90%) US veterans. It is likely that this study population does not reflect the entire population of interest. It is unclear how applicable these findings are to health settings in Canada, and if the staff, places, and facilities are representative of the experience seeking care for the population of interest. Researchers did not conduct any investigations to confirm that sufficient power to detect a clinically important effect. Researchers excluded missing data from analysis. It is unclear how these may have impacted findings. The study lacks statistical analysis to adjust for multiplicity (multiple outcomes for satisfaction). Overlap of study population with a cross-sectional study34 funded by US army included in this report is unclear. |
DOF = degree of freedom.
Note: We acknowledge that sex is assigned on birth and based on genetics, whereas gender refers to an individual’s social experience of being a man, women, trans, or identifying outside gender confines. None of the studies defined these terms in this Rapid Review.
Table 6: Clinical Effectiveness of Microprocessor Knees vs. Nonmicroprocessor Knees for Question 2: Strengths and Limitations of Systematic Reviews and Meta-Analyses Using AMSTAR 252
Strengths | Limitations |
|---|---|
Hahn et al. (2022)29 | |
The systematic review authors clearly defined their research questions and selection criteria. The systematic review authors provided satisfactory details regarding their literature search strategy. They also searched reference lists for relevant publications. Two systematic reviewers performed screening and critical appraisal in duplicate. The systematic review authors described the population, intervention, comparators, outcomes, research designs, time frame for follow-up, and results in adequate detail. The systematic review authors conducted a risk of bias assessment for included primary studies (i.e., State of the Science Evidence Report Guidelines). No funding was associated with the work featured in the systematic review. The meta-analysis included suitable parameters when it was identified in at least 3 independent studies. They reported the results of primary studies included in the review separately, including outcomes they were unable to include in the meta-analysis. The review authors used an appropriate weighted technique to combine study results. The systematic review authors presented the results of fixed and random effects models. Their justification was that the random-effects model accounts for different patient characteristics between the studies. | The publication lacks an explicit statement about established methods before the conduct of the systematic review or meta-analysis. The review authors conducted a preparatory systematic literature search with no details about the process. The systematic review authors did not justify their inclusion of both randomized controlled trials and nonrandomized studies. It is unclear if data extraction was performed in duplicate. It seems that the tool used to assess risk of bias lacked consideration of confounding variables (e.g., hip amputations, bilateral vs. unilateral amputations) The systematic review authors were unable to explore the possibility of publication bias due to relatively small number of studies that were pooled for the same outcome for the meta-analysis. The systematic review authors acknowledged that the small number of studies pooled for each outcome in the meta-analysis limited exploration of heterogeneity. Hence, it is unclear how sources of heterogeneity may have impacted effect sizes in the meta-analysis. Some systematic review authors were employees of the manufacturers of microprocessor knees during study conduct. The systematic review authors did not attempt to stratify for hip as an amputation or for bilateral amputations (potential confounders) in their meta-analysis The systematic review authors did not report specific values for nonsignificant results. External validity of the results to all microprocessor knees is unclear. The systematic review authors did not report where primary studies were conducted. The review authors did not provide a satisfactory discussion of the implications of the risk of bias in primary studies included in the systematic review. The systematic review did not report whether included studies described or provided information on dimensions of difference or diversity, such as ethnicity, race, place of residence, and gender. It is unclear how generalizable these results are to equity-deserving populations. |
Thibaut et al. (2022)30 | |
The systematic review authors clearly defined their research questions and selection criteria. The systematic review has an explicit statement of established methods with information about its registration. The systematic review authors described each study’s population, intervention, comparators, outcomes, research design, and time frame for follow-up. PRISMA table listed excluded studies with rationale. The systematic review authors provided satisfactory details regarding the funding and conflicts of interest as reported by each included study. The systematic review authors use a satisfactory technique to assess the risk of bias in individual studies, specifically Cochrane Risk of Bias tool for randomized controlled trials and NIH study quality assessment tools for NRS. No conflicts of interest declared by systematic review authors. Systematic reviews provided a satisfactory discussion about the risk of bias, specifically its impact on the internal validity of the report. | The systematic review authors did not justify their inclusion of both nonrandomized or randomized controlled trials, nor did they justify the inclusion of non-English and non-French publications and exclusion of studies with < 20 participants. The systematic review authors did not state their search time frame for their search strategy. The systematic review authors did not report quantitative results reported by included studies, including P values. It is unclear if risk of bias assessment was conducted in duplicate. It is unclear if any of the studies extracted data on people living in Canada or conducted in a health setting in Canada. Manufacturers of microprocessor knees funded some of the primary studies included in the systematic review. For 1 study, a manufacturer provided microprocessor knees, training sessions for ortho-prosthetists and rehabilitation knees, and support to monitor the multicentric study. The systematic review did not report whether included studies described or provided information on dimensions of difference or diversity, such as ethnicity, race, place of residence, and gender. It is unclear how generalizable these results are to equity-deserving populations. Most included studies had a small sample size. Except for a few cross-sectional studies, most studies had a sample size of 20. |
Donnelley et al. (2021)31 | |
The objective and exclusion criteria are clearly defined. The systematic review authors used a comprehensive literature search strategy. The systematic review authors conducted screening, and data extraction in duplicate. The systematic review provided detailed description of the intervention, comparators, and research designs of included economic evaluations. It seems that the systematic review authors used a satisfactory technique to assess risk of bias of included economic evaluations (i.e., Quality of Health Economic Studies instrument). The risk of bias instrument includes assessment of sources of funding for included studies. Overall health utility values (self-reported) were used to conduct economic evaluations. The review authors reported no conflicts of interest. | The systematic review authors did not explicitly include a statement that review methods were established prior the conduct of the review. Additionally, they did not clearly define the inclusion criteria, nor did they justify the inclusion of the types of economic evaluation. The systematic review authors did not provide a satisfactory list of excluded studies from full-text review. It is unclear if risk of bias assessment was conducted in duplicate. The systematic review authors did not provide a satisfactory detail about the population included in the relevant studies to this report (e.g., age, sex or gender, etiology of amputation). The systematic review authors also did not provide details regarding the type of model used by included economic evaluations. The systematic review authors did not discuss the impact of the risk of bias assessment on the findings of included economic evaluations. It is unclear if these studies are applicable to health settings as Canada, because of the following:
Most studies do not consider indirect costs associated with the natural history or progression of diseases, such as rehabilitation costs (e.g., physical therapist). It is unclear whether economic evaluations included in this review considered costs when adults have transitioned from mechanical knees to microprocessor knees (in such cases, costs should consider initial mechanical knees and costs from microprocessor knees). Included economic evaluations used general self-reported measures of overall health. However, relative clinical measures that provide in-depth investigation of function and mobility are outcomes of interest for clinical effectiveness. The systematic review authors did the source of funding for this study. |
AMSTAR 2 = A MeaSurement Tool to Assess systematic Reviews 2; NIH = National Institute of Health; NRS = nonrandomized study; vs. = versus.
Table 7: Strengths and Limitations of Guidelines Using AGREE II54
Item | Department of Veterans Affairs and the Department of Defense (2024)35 | Department of Veterans Affairs and the Department of Defense (2022)6 | Stevens and Wurdeman (2019)36 |
|---|---|---|---|
Domain 1: Scope and purpose | |||
1. The overall objective(s) of the guideline is (are) specifically described. | Yes | Yes | Yes |
2. The health question(s) covered by the guideline is (are) specifically described. | Yes | Yes | Yes |
3. The population (patients, public, and so on) to whom the guideline is meant to apply is specifically described. | Yes | Yes | Yes |
Domain 2: Stakeholder involvement [wording from original source]a | |||
4. The guideline development group includes individuals from all relevant professional groups. | Yes | Yes | No |
5. The views and preferences of the target population (patients, public, and so on) have been sought. | Yes | Yes | No |
6. The target users of the guideline are clearly defined. | Yes | Yes | Yes |
Domain 3: Rigour of development | |||
7. Systematic methods were used to search for evidence. | Yes | Yes | Yes |
8. The criteria for selecting the evidence are clearly described. | Yes | Yes | No |
9. The strengths and limitations of the body of evidence are clearly described. | Yes | Yes | No |
10. The methods for formulating the recommendations are clearly described. | No | No | No |
11. The health benefits, side effects, and risks have been considered in formulating the recommendations. | Yes | Yes | Yes |
12. There is an explicit link between the recommendations and the supporting evidence. | Yes | Yes | Yes |
13. The guideline has been externally reviewed by experts before its publication. | Yes | Yes | No |
14. A procedure for updating the guideline is provided. | Yes | Yes | No |
Domain 4: Clarity of presentation | |||
15. The recommendations are specific and unambiguous. | Yes | Yes | Yes |
16. The different options for management of the condition or health issue are clearly presented. | Yes | Yes | Yes |
17. Key recommendations are easily identifiable. | Yes | Yes | Yes |
Domain 5: Applicability | |||
18. The guideline describes facilitators and barriers to its application. | Yes | Yes | No |
19. The guideline provides advice and/or tools on how the recommendations can be put into practice. | Yes | Yes | No |
20. The potential resource implications of applying the recommendations have been considered. | Yes | Yes | No |
21. The guideline presents monitoring and/or auditing criteria. | Yes | Yes | No |
Domain 6: Editorial independence | |||
22. The views of the funding body have not influenced the content of the guideline. | Yes | Yes | Yes |
23. Competing interests of guideline development group members have been recorded and addressed. | Unclear | Unclear | No |
AGREE II = Appraisal of Guidelines for Research and Evaluation II.
aWe retained the domain names that are included in the original AGREE II checklist, which includes the term “stakeholder” (i.e., in domain 2), to be clear that we assessed the strengths and limitations of guidelines using AGREE II. However, Canda’s Drug Agency understands that language is constantly evolving and the word “stakeholder” has an association with colonialism; whenever possible, Canada’s Drug Agency does not use this word in our reports.
Appendix 5: Main Study Findings
Table 8: Clinical Effectiveness of Body-Powered vs. Myoelectric (With Single-DOF or Multi-DOF Terminal Devices) by Amputation Type for Question 1 From Resnik et al. (2022)32
Outcome, amputation | Transradial, mean (SD) | Transhumeral, mean (SD) | ||||||
|---|---|---|---|---|---|---|---|---|
Body-powered | Myoelectric, single | Myoelectric multi | P value | Body-powered | Myoelectric single | Myoelectric multi | P value | |
Physical function and mobility | ||||||||
Jebsen-Taylor Hand Function (dexterity)a, combinedb | ||||||||
Writing | 0.56 (0.33) | 0.47 (0.27) | 0.53 (0.29) | 0.53 | 0.38 (0.35) | 0.23 (0.20) | 0.25 (0.17) | 0.62 |
Page turning | 0.17 (0.13) | 0.15 (0.09) | 0.12 (0.07) | 0.29 | 0.07(0.06) | 0.04 (0.07) | 0.04 (0.04) | 0.24 |
Small objects | 0.13 (0.11) | 0.12 (0.12) | 0.08 (0.09) | 0.02 | 0.07 (0.06) | 0.03 (0.06) | 0.02 (0.02) | 0.01 |
Eating | 0.19 (0.11) | 0.17 (0.13) | 0.13 (0.09) | 0.13 | 0.09 (0.09) | 0.07 (0.08) | 0.04 (0.04) | 0.45 |
Checkers | 0.09 (0.08) | 0.13 (0.14) | 0.12 (0.08) | 0.29 | 0.07 (0.07) | 0.05 (0.07) | 0.03 (0.03) | 0.73 |
Light cans | 0.25 (0.19) | 0.23 (0.12) | 0.27 (0.15) | 0.68 | 0.14 (0.11) | 0.09 (0.10) | 0.11 (0.05) | 0.36 |
Heavy cans | 0.25 (0.22) | 0.27 (0.12) | 0.25 (0.13) | 0.24 | 0.09 (0.10) | 0.09 (0.10) | 0.15 (0.08) | 0.24 |
Box and blocks | 20.6 (9.2) | 15.1 (9.1) | 15.4 (6.0) | 0.02c | 11.8 (9.8) | 5.2 (5.7) | 7.6 (6.5) | 0.22 |
9 hole peg | 0.07 (0.06) | 0.06 (0.06) | 0.01 (0.01) | 0.0001c | 0.05 (0.06) | 0.01 (0.03) | 0 (0) | 0.03 |
Southampton Hand Assessment Procedure | 44.0 (19.6) | 41.0 (21.1) | 39.6 (14.8) | 0.57 | 14.4 (15.3) | 10.8 (16.6) | 12.8 (12.7) | 0.67 |
Jebsen-Taylor Hand Function (dexterity),a unilateral amputation | ||||||||
Writing | 0.49 (0.30) | 0.41 (0.26) | 0.52 (0.30) | 0.43 | 0.29 (0.26) | 0.21 (0.20) | 0.25 (0.17) | 0.83 |
Page turning | 0.13 (0.09) | 0.14 (0.10) | 0.12 (0.07) | 0.82 | 0.06 (0.05) | 0.02 (0.03) | 0.04 (0.04) | 0.15 |
Small objects | 0.11 (0.07) | 0.11 (0.11) | 0.07 (0.09) | 0.03 | 0.07 (0.06) | 0.01 (0.02) | 0.02 (0.02) | 0.005c |
Eating | 0.18 (0.12) | 0.17 (0.14) | 0.14 (0.09) | 0.42 | 0.08 (0.09) | 0.05 (0.06) | 0.04 (0.04) | 0.55 |
Checkers | 0.08 (0.06) | 0.08 (0.09) | 0.12 (0.08) | 0.1 | 0.06 (0.07) | 0.03 (0.05) | 0.03 (0.03) | 0.6 |
Light cans | 0.20 (0.13) | 0.22 (0.11) | 0.28 (0.15) | 0.3 | 0.12 (0.09) | 0.06 (0.07) | 0.11 (0.05) | 0.23 |
Heavy cans | 0.20 (0.17) | 0.26 (0.12) | 0.25 (0.14) | 0.048 | 0.08 (0.11) | 0.08 (0.09) | 0.15 (0.08) | 0.15 |
Box and blocks | 19.00 (8.73) | 14.27 (7.88) | 15.28 (6.19) | 0.06 | 10.5 (9.34) | 4.00 (4.47) | 7.60 (6.50) | 0.22 |
9 hole peg | 0.06 (0.05) | 0.06 (0.06) | 0.01 (0.01) | 0.0008c | 0.04 (0.04) | 0 (0) | 0 (0) | 0.02c |
Southampton Hand Assessment Procedure | 42.4 (18.4) | 39.3 (23.1) | 40.2 (15.0) | 0.83 | 13.4 (16.2) | 6.6 (10.3) | 12.8 (12.7) | 0.54 |
Activities Measure for Upper Limb Amputation (activity),a unilateral | 14.9 (5.3) | 14.9 (7.7) | 16.4 (6.5) | 0.68 | 12.3 (6.2) | 9.4 (4.2) | 11.9 (1.8) | 0.23 |
Brief Activities Measure for Upper Limb Amputation (activity),a unilateral | 6.6 (2.1) | 9.2 (1.0) | 9.2 (1.0) | 0.0023c | 4.5 (3.4) | 4.0 (NR) | 3.5 (0.7) | 0.83 |
Timed Measure of Activity Performance (activity),d unilateral | 5.0 (1.8) mins | 3.9 (0.6) mins | 3.9 (0.9) mins | 0.08 | 4.6 (1.7) mins | 4.9 (1.2) mins | 7.4 (3.0) mins | 0.18 |
Need for activities of daily living Health (n [yes], %)e unilateral | 7 (21.2) | 3 (37.5) | 2 (16.7) | 0.57 | 3 (25.0) | 2 (28.6) | 2 (28.6) | 1.0000 |
QuickDASH (disability), unilateral | 29.2 (19.4) | 30.9 (15.8) | 26.3 (18.1) | 0.7196 | 34.0 (20.7) | 28.2 (13.8) | 30.5 (13.3) | 0.85 |
Quality of life | ||||||||
Veterans RAND 12 item Mental Composite score (HRQoL)a unilateral | 53.5 (10.1) | 46.3 (12.8) | 52.4 (11.5) | 0.0854 | 50.4 (13.1) | 50.6 (14.6) | 52.9 (9.4) | 0.98 |
Veterans RAND 12 item Physical Composite score (HRQoL),a unilateral | 37.5 (8.9) | 43.2 (6.9) | 41.1 (8.2) | 0.09 | 34.7 (13.2) | 41.9 (5.6) | 44.0 (8.1) | 0.17 |
Social Health | ||||||||
CRISCAT (extent of participation in community),a unilateral | 50.1 (8.7) | 44.6 (9.6) | 49.5 (8.8) | 0.24 | 45.4 (8.3) | 50.1 (10.9) | 53.2 (8.6) | 0.13 |
CRISCAT (Perceived difficulty in participation),a unilateral | 49.4 (6.8) | 44.3 (4.7) | 51.1 (9.1) | 0.03 | 46.2 (5.0) | 48.3 (7.1) | 48.8 (7.9) | 0.87 |
Satisfaction | ||||||||
CRISCAT (satisfaction),a unilateral | 51.2 (9.2) | 46.9 (7.7) | 50.2 (10.5) | 0.37 | 45.6 (4.9) | 47.9 (5.8) | 47.7 (7.9) | 0.55 |
Trinity Amputation and Prosthesis Experience Satisfaction Scale (satisfaction),a unilateral | 4.0 (0.7) | 3.5 (0.7) | 3.8 (0.7) | 0.051 | 3.7 (0.9) | 3.5 (0.5) | 3.7 (0.5) | 0.64 |
CRISCAT = Community Reintegration of Injured Service Members-Computer Adapted-Test; DASH = disabilities of the arm, shoulder, and hand; DOF = degree of freedom; HRQoL = health-related quality of life; SD = standard deviation; vs. = versus.
Note: This table has not been copy-edited.
Note: Bolded P values denote statistical significance (P < 0.05).
aHigher scores indicate a better result.32
bCombined results include people with unilateral and bilateral amputations. Results for bilateral amputations consider the dominant side only.32
cFindings remain significant after Benjamin-Hochberg adjustment with false discovery rate = 0.1.
dLower scores indicate a better result.32
eParticipants responded yes or no. Individuals that respond “No” means that they do not require help and signifies greater independence.32
Table 9: Clinical Effectiveness of Body-Powered and Cosmetic Devices vs. Myoelectric (With Single-DOF or Multi-DOF Terminal Devices) for Question 1
Relevant outcome by study | Body-powered | Myoelectric, single-DOFc | P value | Myoelectric, multi-DOF | P value |
|---|---|---|---|---|---|
Resnik et al. (2020),33 unilateral amputations | |||||
Veteran’s RAND 12-item Health Survey, mental component summary (Beta, 95% CI) | reference | 2.07 (−1.73 to 5.87) | 0.29 | 2.59 (−2.14 to 7.32) | 0.28 |
Veteran’s RAND 12-item Health Survey, physical component summary (Beta, 95% CI) | reference | 0.17 (−2.26 to 2.59) | 0.89 | −0.97 (−3.99 to 2.05) | 0.53 |
Quick DASH (Beta, 95% CI)b | reference | −1.72 (−7.58 to 4.14) | 0.56 | 1.24 (−5.88 to 8.36) | 0.73 |
Help with activities of daily living | reference | 0.55 (0.24 to 1.23) | 0.14 | 1.75 (0.81 to 3.79) | 0.15 |
Resnik et al. (2020),34 combineda,b | |||||
Trinity Amputation and Prosthesis Experience Scales Satisfaction (beta)a | reference | −0.08a | 0.33a | NA | NA |
Orthotics and Prosthetics Users’ Survey – Client Satisfaction with Devices Scale (beta)a | reference | 1.19a | 0.59a | NA | NA |
CI = confidence interval; DASH = disabilities of the arm, shoulder, and hand; DOF = degree of freedom; NA = not applicable; RAND = research and development; SD = standard deviation; vs. = versus.
Note: This table has not been copy-edited.
Note: Results for cosmetic devices are only included in cases where it impacts P values. Resnik et al. (2020)34 did not separate results by DOF of terminal devices for myoelectric prostheses.
aThe study by Resnik et al.34 compared satisfaction between myoelectric (regardless of the DOF of terminal devices) and body-powered devices. Hence, the results under the “Myoelectric, single-DOF” column for Resnik et al. (2020)34 includes all myoelectric or hybrid devices.
bResults includes individuals with bilateral and unilateral amputations.
Table 10: Meta-Analysis by Hahn et al. (2022)29 – Clinical Effectiveness of Microprocessor vs. Nonmicroprocessor Knees for Question 2
Outcome | Microprocessor knees, total | Non- microprocessor knees, total | Standardized mean difference (95% CI) | P value | I2 |
|---|---|---|---|---|---|
Safety | |||||
Number of falls | — | — | — | — | 0% |
Fixed effect model | 117 | 114 | -0.59 (−0.85 to −0.21) | < 0.01 | NA |
Random-effects model | NA | NA | -0.59 (−0.85 to −0.21) | < 0.01 | NA |
Fear of falling | — | — | — | — | 80% |
Fixed effect model | 464 | 464 | 1.75 (1.60 to 1.90) | < 0.01 | NA |
Random-effects model | NA | NA | 1.20 (0.55 to 1.85) | < 0.01 | NA |
Timed up and go | — | — | — | — | 0% |
Fixed effect model | 45 | 45 | -0.45 (−0.87 to 0.02) | 0.04 | NA |
Random-effects model | NA | NA | -0.45 (−0.87 to 0.02) | 0.04 | NA |
Function, performance, and mobility | |||||
Positive mobility grade changea | — | — | — | — | 16% |
Fixed effect model | 519 | NA | 0.51 (0.47 to 0.55) | NA | NA |
Random-effects model | NA | NA | 0.51 (0.47 to 0.55) | NA | NA |
Walking speed | — | — | — | — | 0% |
Fixed effect model | 71 | 71 | 0.47 (−1.81 to 1.42) | < 0.01 | NA |
Random-effects model | NA | NA | 0.47 (−1.81 to 1.42) | < 0.01 | NA |
Fast walking speed | — | — | — | — | 0% |
Fixed effect model | 22 | 22 | 0.40 (−0.21 to 1.01) | 0.20 | NA |
Random-effects model | NA | NA | 0.40 (−0.21 to 1.01) | 0.20 | NA |
Activity-specific Balance Confidence Scale | — | — | — | — | 48% |
Fixed effect model | 40 | 40 | 7.90 (0.34 to 15.46) | 0.04 | NA |
Random-effects model | NA | NA | 7.55 (−7.03 to 22.14) | 0.31 | NA |
Perception and experience | |||||
Ambulation | — | — | — | — | 7% |
Fixed effect model | 78 | 78 | 9.24 (3.77 to 14.70) | < 0.01 | NA |
Random-effects model | NA | NA | 9.32 (3.61 to 15.03) | < 0.01 | NA |
Appearance | — | — | — | — | 1% |
Fixed effect model | 68 | 68 | 5.24 (−0.85 to 11.32) | 0.09 | NA |
Random-effects model | NA | NA | 5.24 (−0.85 to 11.35) | 0.13 | NA |
Residual limb | — | — | — | — | 4% |
Fixed effect model | 69 | 69 | 4.45(−1.15 to 10.05) | 0.12 | NA |
Random-effects model | NA | NA | 4.43 (−1.29 to 10.14) | 0.13 | NA |
Sounds | — | — | — | — | 0% |
Fixed effect model | 69 | 69 | 3.36 (−4.65 to 11.37) | 0.41 | NA |
Random-effects model | NA | NA | 3.36 (−4.65 to 11.37) | 0.41 | NA |
Utility | — | — | — | — | 0% |
Fixed effect model | 69 | 69 | 7.76 (2.05 to 13.47) | < 0.01 | NA |
Random-effects model | NA | NA | 7.76 (2.05 to 13.47) | < 0.01 | NA |
Well-being | — | — | — | — | 0% |
Fixed effect model | 68 | 68 | 4.97 (−1.01 to 10.96) | 0.10 | NA |
Random-effects model | NA | NA | 4.97 (−1.01 to 10.96) | 0.10 | NA |
NA = not applicable; vs. = versus.
Note: This table has not been copy-edited.
Note: This table details the results of a meta-analysis of patient reported outcomes by Hahn et al. (2022).29
aPositive grade change from changing to a microprocessor knee from nonmicroprocessor knee.
Table 11: Clinical Effectiveness of Microprocessor Knees vs. Nonmicroprocessor Knees for Question 2
Outcome | Hahn (2022),29 Systematic Review | Thibaut (2022),30 Systematic Review | |||
|---|---|---|---|---|---|
Absolute difference | Relative difference | P value | Results | P value | |
General prosthesis use | |||||
Questionnaire for Persons with Transfemoral Amputation | NA | NA | NA | One cross-sectional study found no difference between microprocessor knees and nonmicroprocessor knees. | NR |
Safety | |||||
Perception of safety on stops | 7.8 | 10.3% | 0.005 | NA | NA |
Perception on safety on sidesteps | 10.3 | 14.2% | 0.002 | NA | NA |
Perception on stability on stops | 10.8 | 14.7% | < 0.001 | NA | NA |
Perception on stability on side steps | 7.6 | 10% | 0.007 | NA | NA |
Perception on Obstacle clearance | 13.3 | 18.9% | 0.001 | NA | NA |
Number of nonstumblers | NR | 42% | 0.044 | NA | NA |
Number of stumblesa | NR | NR | ns | NA | NA |
−6 | −76% | 0.21 | NA | NA | |
Number of falls | NA | NA | NA | One crossover randomized study found no difference between microprocessor and nonmicroprocessor knees. Two before-and-after studies found a reduction in falls after changing to a microprocessor knee from a nonmicroprocessor knee. | NR |
Number of semicontrolled falls | NR | NR | ns | NA | NA |
Number of nonfallers | NR | NR | ns | NA | NA |
Fear of stumbles | 11.6 | 15.7% | 0.05 | NA | NA |
Observed fall events | NR | NR | ns | NA | NA |
Improved perception of safetya,b | 85% (95% CI, 84 to 90) | NA | NR | NA | NA |
100% (95% CI, 91.2 to 100) | NA | NR | NA | NA | |
Function, performance, or mobility | |||||
SSWS heel rise with the prosthetic limb | NR | NR | 0.33 | NA | NA |
FPWS heel rise with the prosthetic limb | NR | NR | 0.019 | NA | NA |
Activity-specific Balance Confidence Scalea | 15.6 | 26% | < 0.001 | NA | NA |
−41.1 | −118.7% | 0.09 | NA | NA | |
NR | NR | ns | NA | NA | |
Perceived improvements in standingb | 69% (95% CI, 46 to 92) | NA | NR | NA | NA |
SWSS level walking - Cadence | 7.0 | 9.2% | 0.001 | NA | NA |
SWSS level Walking – Stride Length | 0.1 m | 11.9% | 0.003 | NA | NA |
FPWS level walking - Cadence | 8.8 m | 10.1% | 0.002 | NA | NA |
FPWS level walking – Stride length | 0.13 m | 13.6% | < 0.001 | NA | NA |
SSWS level walking – Single Limb Support | NR | NR | 0.048 | NA | NA |
Perceived improvement in level walkingb | 79% (95%, CI 42 to 86) | NA | NR | NA | NA |
FPWS single limb support (prosthetic side) | NR | NR | ns | NA | NA |
FPWS (uneven terrain) | 0.14 m/s | 25.2% | 0.01 | NA | NA |
Confidence while walking | NR | NR | ns | NA | NA |
2 minute walk testa | 16.84 m | 18.1% | 0.001 | NA | NA |
NR | NR | ns | NA | NA | |
6 minute walk test | NR | NR | ns | One before-and-after study observed a decrease in time after changing to a microprocessor knees from nonmicroprocessor knees. A cross-sectional study found no difference between groups. | NR |
10 minute walk test | -2.6 second | 14.4% | 0.045 | NA | NA |
Speed 10-minute walk test | 0.1 m/s | 15.2% | 0.009 | NA | NA |
Perceived improvement in level walkingb | 64% (95% CI, 42 to 86) | NA | NR | NA | NA |
Confidence while walking | NR | NR | ns | NA | NA |
Improved ability to walk backwardb | 75.0% (95% CI, 58.7 to 91.3) | NA | NR | NA | NA |
Improved ability to do small stepsb | 65.0% (95% CI, 47.0 to 83.0) | NA | NR | NA | NA |
Stair mobilitya | -5.7 | 172.7% | 0.01 | NA | NA |
NR | NR | ns | NA | NA | |
Improved stair ambulationb | 41.3% (95% CI, 22.8 to 60) | NA | NR | NA | NA |
Improved descend on rampsb | 86.8% (95% CI, 74.0 to 99.6) | NA | NR | NA | NA |
Hill mobility | -2.1 | 38.9% | 0.01 | One before-and-after study found higher hill assessment index scores for microprocessor knees vs. nonmicroprocessor knees. | NR |
Hill speed | -0.46 m/s | 27.1% | 0.002 | NA | NA |
Speed in Slope Ascend | 0.13 m/s | 27.7% | 0.01 | NA | NA |
Cadence in Slope Ascend | 9.7 | 14.3% | 0.01 | NA | NA |
Stride Length in Slope Ascend | 0.10 m | 11.9% | 0.02 | NA | NA |
Speed in Slope Descend | 0.14 m | 36.2% | < 0.001 | NA | NA |
Cadence in Slope Descend | 10.9 | 16% | < 0.02 | NA | NA |
Stride length in Slope Descend | 0.13 m | 13.7% | 0.003 | NA | NA |
Obstacle course | -0.09 m/s | 11.3% | 0.02 | NA | NA |
Improved symmetryb | 95.5% (95% CI, 89.6 to 100) | NA | NR | NA | NA |
Improved relief sound sideb | 89.3% (95% CI, 77.6 to 100) | NA | NR | NA | NA |
95% (95% CI, 93 to 97) | NA | NR | NA | NA | |
Multitasking | -15.0 | 21.1% | 0.04 | NA | NA |
Activity level | NA | NA | NA | One before-and-after study observed higher activity levels with microprocessor knees vs. nonmicroprocessor knees | NR |
Activity time | 4% | 20% | 0.02 | NA | NA |
Siting time | 9% | 17% | 0.01 | One before-and-after study found that there is less sitting time for microprocessor knees vs. nonmicroprocessor knees. | NR |
Activity avoidance (VAS) | NR | NR | ns | NA | NA |
Attention accuracy (VAS) | NR | NR | ns | NA | NA |
Improved attentiona,b | 89.7% (95% CI, 78.2 to 100) | NA | NR | NA | NA |
90% (95% CI, 87 to 93) | NA | NR | NA | NA | |
Improved variability in speedb | 78.6%; (95% CI, 63.1 to 94.1) | NA | NR | NA | NA |
Improved gait harmonizationb | 93% (95% CI, 90 to 95) | NA | NR | NA | NA |
Improved level walkingb | 79% (95% CI, 42 to 86) | NA | NR | NA | NA |
Improved – uneven ground | 64% (95% CI, 42 to 85) | NA | NR | NA | NA |
Improved variability in gait speedb | 92.6%; (95% CI, 82.7 to 100) | NA | NR | NA | NA |
86% (95% CI, 83 to 89) | NA | NR | NA | NA | |
Improved overall effortb | 84% (95% CI, 81 to 87) | NA | NR | NA | NA |
85.7% (95% CI, 72.5 to 98.9) | NA | NR | NA | NA | |
Improved perceived exertionb | 84% (95% CI, 67 to 100) | NA | NR | NA | NA |
Improved ability to overcome obstaclesb | 84.0% (95% CI, 70.2 to 97.8) | NA | NR | NA | NA |
Improved rampsb | 86.8% (95% CI, 74 to 99.6) | NA | NR | NA | NA |
Improved ability to carry heavy loadsb | 78.2% (95% CI, 62.6 to 93.8) | NA | NR | NA | NA |
Improved ability to carry with visual obstructionb | 88.0% (95% CI, 75.7 to 100) | NA | NR | NA | NA |
Improved results for the “door test”b | 92.3% (95% CI 82.6 to 100) | NA | NR | NA | NA |
Improved mobility on standing rampsb | 92.0% (95% CI, 81.8 to 100) | NA | NR | NA | NA |
Improved toiletingb | 56.0% (95% CI,37.3 to 74.7) | NA | NR | NA | NA |
Mental energy expenditure | NR | NR | ns | NA | NA |
Difficulty with concentration | NR | NR | ns | NA | NA |
Improved concentrationb | 79% (95% CI, 61 to 97) | NA | NR | NA | NA |
Stair Ambulationb | 88.9% (95% CI, 77.0 to 100) | NA | NR | NA | NA |
Ambulation (PEQ) | 1.6 | 25.4% | 0.04 | NA | NA |
ADAPT circuit | NA | NA | NA | One randomized crossover study found that the time to complete ADAPT was shorter for “intermediate” and “high subgroups.” | NR |
ADAPT perceived difficulty (C-Leg compact) | NR | NR | ns | NA | NA |
ADAPT, low activity level | NR | NR | ns | One randomized crossover study found no difference between microprocessor and nonmicroprocessor knee. | NR |
ADAPT, AS1 (C-Leg) | NR | NR | 0.0001 | NA | NA |
ADAPT, AS1 (C-Leg compact) | NR | NR | 0.002 | NA | NA |
ADAPT, AS1 high activity level (C-Leg) | NR | NR | 0.01 | NA | NA |
ADAPT, AS1 high activity level (C-Leg Compact) | NR | NR | 0.019 | NA | NA |
ADAPT, AS1 intermediate activity level (C-Leg) | NR | NR | 0.004 | NA | NA |
ADAPT, AS1 intermediate activity level (C-Leg Compact) | NR | NR | 0.008 | NA | NA |
ADAPT, AS2 intermediate activity levela | NR | NR | ns | NA | NA |
ADAPT, AS2 intermediate activity level (C-Leg) | NR | NR | 0.0016 | NA | NA |
ADAPT, AS2 high activity level | NR | NR | ns | NA | NA |
ADAPT, perceived difficulty for AS2 | NR | NR | 0.023 | NA | NA |
ADAPT AS3 intermediate activity level | NR | NR | ns | NA | NA |
ADAPT, AS3 high activity level | NR | NR | 0.023 | NA | NA |
ADAPT, AS3 high activity level (C-Leg) | NR | NR | ns | NA | NA |
ADAPT, perceived difficulty for AS3 (C-Leg) | NR | NR | 0.0008 | NA | NA |
ADAPT, SAI intermediate activity level (C-Leg) | 5.5 | 171.9% | < 0.025 | NA | NA |
ADAPT, SAI high activity level(C-Leg) | 5.3 | 147.2% | < 0.025 | NA | NA |
ADAPT, SAI low activity level | NR | NR | ns | NA | NA |
ADAPT, SAI intermediate activity level (C-Leg Compact) | 4.6 | 143.8% | < 0.025 | NA | NA |
ADAPT, SAI high activity level (C-Leg Compact) | 5.2 | 144.4% | < 0.025 | NA | NA |
Wheelchair dependence | NR | 43% | 0.005 | NA | NA |
Locomotor Capabilities Indexa | 2.4 | 5.6% | 0.02 | One randomized crossover study found improvement was observed in the microprocessor vs. nonmicroprocessor group. Two before-and-after studies found an improvement in scores after changing to microprocessor from nonmicroprocessor knees | NR |
NR | NR | ns | NA | NA | |
NR | NR | ns | NA | NA | |
Prosthetic limb users survey of mobilitya | 4.67 | 10.6% | 0.004 | One study found mobility was greater for microprocessor knees compared to nonmicroprocessor knees. | NR |
NR | NR | ns | NA | NA | |
Amputee Mobility predictora | 3.49 | 9.6% | < 0.001 | NA | NA |
NR | NR | ns | NA | NA | |
The 4 square step test | NR | NR | ns | NA | NA |
L-test of functional mobility | -8.01 second | -21.1% | < 0.001 | NA | NA |
Montreal Rehabilitation Performance Profile | 2.7 | 38.8% | 0.03 | NA | NA |
Mobility grade change | NR | NR | ns | NA | NA |
Distance (10 m walk test) | NA | NA | NA | One cross-sectional study found no difference between microprocessor knees and nonmicroprocessor knees. | NR |
General Self-Efficacy Scale | NA | NA | NA | One cross-sectional study found no difference between microprocessor knees and nonmicroprocessor knees. | NR |
Timed up and go | 6.8s | 38.4% | < 0.02 | One randomized crossover study found that the microprocessor group had a shorter time vs. the nonmicroprocessor group. | NR |
Houghton’s Scalea | NR | NR | 0.058 | NA | NA |
2.75 | 100% | 0.19 | NA | NA | |
NR | NR | ns | NA | NA | |
NR | NR | ns | NA | NA | |
Berg Balance Scalea | −2.25 | −7.3 | 0.56 | NA | NA |
NR | NR | ns | NA | NA | |
NR | NR | ns | NA | NA | |
Satisfaction | |||||
Satisfaction with walking (high activity level)a | 10.6 | 15% | 0.04 | NA | NA |
Satisfaction with walking, (intermediate activity level) | 28.1 | 49.8% | 0.007 | NA | NA |
Preferenceb | 89% for microprocessors | NA | NA | NA | NA |
Satisfaction with prosthesis | NR | NR | ns | NA | NA |
Satisfaction (VAS) | NR | NR | Ns | NA | NA |
Quebec User Evaluation of Satisfaction with Assistive Technology | 0.8 | 17% | 0.001 | NA | NA |
Frustration (PEQ) | NR | NR | ns | NA | NA |
Perceived response (PEQ) | NR | NR | ns | NA | NA |
Social burden (PEQ) | NR | NR | ns | NA | NA |
Orthotics Prosthetics User Survey | NR | NR | ns | NA | NA |
Quality of Life | |||||
SF-36 | NR | NR | ns | One crossover randomized study and 1 before-and-after study found better SF-36 scores with microprocessor knees. | NR |
SF-36 vitality | NA | NA | NA | One before-and-after study found no improvement from changing to microprocessor from nonmicroprocessor knees. | NR |
SF-36 general health | NA | NA | NA | One before-and-after study found no improvement from changing to microprocessor from nonmicroprocessor knees | NR |
SF-36 social role | NA | NA | NA | One before-and-after study found no improvement from changing to microprocessor from nonmicroprocessor knees. | NR |
SF-36 emotional role | NA | NA | NA | One before-and-after study found no improvement from changing to microprocessor from nonmicroprocessor knees. | NR |
SF-36 pain | NA | NA | NA | One before-and-after study found no improvement from changing to microprocessor from nonmicroprocessor knees. | NR |
SF-36 mental component summary | 3.86 | 7.4% | 0.04 | One before-and-after study found no improvement from changing to microprocessor from nonmicroprocessor knees. | NR |
SF-36 physical component summary | NR | NR | ns | One before-and-after study found an improvement in scores after changing to microprocessor knees from nonmicroprocessor knees. Another before-and-after study found no difference in scores. | NR |
EQ-5D-5L | 0.08 | 12.1 | 0.01 | One cross-sectional study found higher scores for microprocessor knees (C-Leg) compared to nonmicroprocessor knees | NR |
Other | |||||
Frustration with falls | NR | NR | ns | NA | NA |
Embarrassment with falls | NR | NR | Ns | NA | NA |
Gait Analysis | |||||
Gait speed | NA | NA | NA | One cross-sectional study found faster gait speed with microprocessor knees compared to nonmicroprocessor knees. | NR |
Stride length | NA | NA | NA | One cross-sectional study found no difference between microprocessor knees and nonmicroprocessor knees. | |
Knee extension and latency period | NA | NA | NA | One cross-sectional study found no difference between microprocessor knees and nonmicroprocessor knees. | NR |
Knee latency | NA | NA | NA | One cross-sectional study found no difference between microprocessor knees and nonmicroprocessor knees. | NR |
Stance phase duration | NA | NA | NA | One cross-sectional study found no difference between microprocessor knees and nonmicroprocessor knees. | NR |
3D Gait analysis | NR | NR | ns | NA | NA |
Gait, entropy | NA | NA | NA | One before-and-after study found no improvement from changing to microprocessor from nonmicroprocessor knees | NR |
Gait profile score | NR | NR | ns | NA | NA |
Electromyography signals (various) | NR | NR | ns | NA | NA |
ADAPT = Assessment of Daily Activity Performance in Transfermoral Amputees Test; AS = activity set; FPWS = fastest possible walking speed; NA = not applicable; NR = not reported; ns = not statistically significant; SAI = stair assessment index; SPSS = self-selected walking speed; VAS = visual analogue scale; vs. = versus.
Note: This table has not been copy-edited.
Note: Bolded results denotes statistical significance. Outcomes from the systematic review by Hahn et al.29 were only included in this table if review authors were unable to include the results in meta-analysis. The systematic review by Thibault et al.30 used descriptive statistics only and did not report any quantitative results of included primary studies. Additionally, the systematic review by Thibault et al.30 did not report statistical significance for most outcomes, nor did they define how they decided on how to report favourable or unfavourable qualitative findings.
Note: A primary study included in the systematic review by Hahn et al.29 recruited a small number of participants with high heterogeneity. The primary study researchers used descriptive analysis only. The primary study’s result favours microprocessor knees over nonmicroprocessor knees, specifically for timed up and go, 2 minute walk test, self-selected walking speed, fastest possible walked speed, berg balance scale, mobility grade scale, observed fall events, Houghton’s scale, Orthotics Prosthetics Users Survey, Locomotors Capabilities Index, Activities-Specific Balanced Confidence Scale, 36-Item Short Form Survey, and 3D gait analysis.
aResults available for the outcome measure in more than1 included study in the systematic review by Hahn et al.29 current report.
bThe systematic review by Hahn et al.29 reported these results are presented by % of improved participants instead of absolute or relative difference between the effect of microprocessor knees and nonmicroprocessor knees.
Table 12: Economic Evaluations Included in the Systematic Review by Donnelley et al. (2021)31
Included study | Perspective | Time horizon (years) | Effect measure | Total costs | Utility | ICER | Discount rate | Acceptability threshold |
|---|---|---|---|---|---|---|---|---|
Brodtkobt TH, et al. Arch Phys Med Rehabil. 2008;89:24 to 30.a | Payer | 8 | EQ VAS | Microprocessor knee: €25,146 Mechanical knee: €17448 | Microprocessor knee: 6.98 Mechanical knee: 3.60 | €3,218 per QALY | 3% | €10,000 per QALY |
Chen C, et al. J Neuroeng Rehabil. 2018;15 (Suppl 1):62. | Societal | 10 | SF-36, PEQ, EQ-5D | Microprocessor knee: US$15,083/year Mechanical knee: US$13,382 | Microprocessor knee to mechanical knee: 0.91 | US$11,606 per QALY | 3% | US$50,000 to US$150,000 per QALY |
Cutti AG, et al. Prosthet Orthot. Int 2017;41:227 to 36.a | Payer | 5 | EQ-5D | Microprocessor knee: €22,656 Mechanical knee: €4,144 | Microprocessor knee: 3.84 Mechanical knee: 3.38 | €40,155 per QALY | None | €54,120 per QALY |
Gerzeli S, et al. Eur J Heal Econ. 2009;10:47 to 55a | Payer | 5 | EQ-5D | Microprocessor knee: €22,744 Mechanical knee: €7,449 | Microprocessor knee: 3.55 Mechanical knee: 3.14 | €35,971 per QALY | 3% | €30,000 to €100,000 per QALY |
EQ VAS = EQ visual analogue scale; ICER = incremental cost-effectiveness ratio; PEQ = Prosthesis evaluation questionnaire; QALY = Quality-adjusted life-year SF-36 = 36-Item Short Form Survey.
Note: This table has not been copy-edited.
Note: Bolded rows indicate cost-effectiveness based on the acceptability threshold. All included economic evaluations conducted a univariate sensitivity analysis and costs associated with transfemoral amputations. Included studies that did not use a relevant study design (e.g., budget impact analysis) were excluded from this table.
aIntervention is specific to the C-Leg microprocessor knee.
Table 13: Summary of Recommendations in Included Guidelines
Recommendations and supporting evidence | Quality of evidence and strength of recommendations |
|---|---|
Department of Veterans Affairs and the Department of Defense (2024)35 | |
“For prosthetic ambulators, we suggest prescribing microprocessor knee units over non-microprocessor knee units for reducing falls, optimizing functional mobility, and improving patient satisfaction.” (p. 31) Supporting evidence: Four studies found that microprocessor knees are favoured for motor and physical function in the stair assessment index, hill assessment index, locomotor capability index, and motor tests over a 1 to 3-month follow-up period as compared to nonmicroprocessor knees. In addition, 2 studies found that microprocessor knees were favoured over nonmicroprocessor knees for locomotor ability in longer term follow-up (6 months). In terms of specific microprocessor knees, 1 large study found no difference in the Prosthetic Limb Users Survey of Mobility scores between the C-Leg, Rheo, Orion, and Plie microprocessor knees. | Quality of evidence: Very low certainty of evidence Strength of recommendation: Weak for |
“For prosthetic ambulators, there is insufficient evidence to prescribe any specific energy storing and return (ESAR) or microprocessor foot and ankle component over another.” (p. 31) Supporting evidence: There was evidence to support the prescription of ESAR prosthetic feet or microprocessor-controlled foot and ankle components over solid ankle cushion heel, but there was no evidence to suggest which specific option was better than the other. | Quality of evidence: Very low certainty of evidence Strength of recommendation: Neither for nor against |
“For prosthetic ambulators, we suggest ESAR or microprocessor-controlled foot and ankle components over solid ankle cushioned heel (SACH) feet to improve ambulation and patient satisfaction.” (p. 31) Supporting evidence: Evidence from 1 systematic review found benefits in gait symmetry when comparing energy storing and returning prosthetic feet and a microprocessor-controlled foot and ankle with powered push-off with SACH. A randomized controlled trial found that energy storing and returning prosthetic feet outperformed SACH feet on all biomechanical measures. Another randomized controlled trial found that a novel energy storing and returning prosthetic foot performed comparatively to other energy storing and returning prosthetic feet for walking performance. Finally, a randomized controlled trial found that there was higher quality of life outcomes for energy storing and returning feet with micro-processor-controlled foot and ankle components compared to solely energy storing and returning feet. | Quality of evidence: Very low certainty of evidence Strength of recommendation: Weak for |
Department of Veterans Affairs and the Department of Defense (2022)6 | |
“For patients with major upper limb amputation (i.e., through or proximal to the wrist), we suggest use of a body-powered or externally-powereda prosthesis to improve independence and reduce disability.” (p. 23). Supporting evidence: One cross-sectional study33 found that the use of body-powered or externally-powered prostheses improves independence and reduces disability in patients with major unilateral upper limb amputation. The use of body-powered and externally-powered prostheses was associated with less difficulty performing activities, less disability, and higher physical function in most patients. There was no evidence to recommend 1 type of prosthetic over another. | Quality of evidence: Very low certainty of evidence Strength of recommendation: Weak for |
Stevens and Wurdeman (2019)36 | |
“Recommendation 2A: Microprocessor knee benefits: Compared with non-microprocessor knees: With respect to self-report indices and measures, microprocessor knees are indicated to reduce stumbles, falls, and associated frustrations as well as the cognitive demands of ambulation.” (p. 5) Supporting evidence: One trial found that transitioning from nonmicroprocessor knees to microprocessor knees resulted in a significant decrease in number of stumbles, semicontrolled falls, and uncontrolled falls. Another trial also found that microprocessor knee users experienced fewer stumbles and falls than those with a nonmicroprocessor knee. Frustration with falls was also reduced with the use of a microprocessor knee. A systematic review reporting evidence from 7 studies found that all studies supported the grade “B” recommendation that after moving from a nonmicroprocessor knee to a C-Leg, subjects will recall having reduced stumble and fall events. Another systematic review found that activities that require divided attention, like stair and hill descents, occur quicker with a microprocessor knee as compared to an nonmicroprocessor knee. | Quality of evidence: NR Strength of recommendation: NR |
“Recommendation 2B: Microprocessor knee benefits: Compared with non-microprocessor knees: With respect to self-report indices and measures, microprocessor knees are indicated to increase confidence while walking, self-reported mobility, satisfaction, well-being, and quality of life.” (p. 5) Supporting evidence: A cohort study reported that confidence in their microprocessor knees was observed in those who had switched from a nonmicroprocessor knee to a microprocessor knee. Self-reported mobility has increased with the use of a microprocessor knee compared to a nonmicroprocessor knee. Another study found increased energy burned over the course of a day with the use of a microprocessor knee despite having a nonsignificant decrease in oxygen consumption during ambulation. Two clinical trials have addressed both satisfaction and preference where participants were able to choose from either a microprocessor knee or a nonmicroprocessor knee after completion of the study and more chose microprocessor knees. Also, significantly higher satisfaction scores were observed with the use of a microprocessor knee. Two studies found that well-being scores increased when switching from a nonmicroprocessor knee to a microprocessor knee. In addition, 2 studies have found an increase In QALY values associated with the use of microprocessor knees. | Quality of evidence: NR Strength of recommendation: NR |
“Recommendation 2C: Microprocessor knee benefits: Compared with non-microprocessor knees: With respect to physical performance indices and measures, microprocessor knees are indicated to increase self-selected walking speed, walking speed on uneven terrain, and metabolic efficiency during gait.” (p. 6) Supporting evidence: Self-selected walking speed increases with the switch from nonmicroprocessor knees to microprocessor knees in 4 studies. Several trials found that walking speed increased with microprocessor knees when walking on uneven terrain. Increased walking speed downhill has also been found. There have been studies that found that microprocessor knees allowed for improved qualities of movement for stair descent and hill descent. Two studies found that there were no significant differences in oxygen cost when switching from nonmicroprocessor knees to microprocessor knees. Two other studies have found that there was a decreased oxygen cost with microprocessor knees. Oxygen rate generally decreases with the use of microprocessor knees and a single study reported reduced perceived exertion with microprocessor knees. | Quality of evidence: NR Strength of recommendation: NR |
“Recommendation 3: Microprocessor knee equivalence: Given the comparable values observed with the use of microprocessor and non-microprocessor knees with regard to daily step counts, temporal and spatial gait symmetry, self-reported general health, and total costs of prosthetic rehabilitation, these parameters may not be primary indications in prosthetic knee joint selection.” (p. 6) Supporting evidence: Two studies reported on step count, and number of and duration of activity bouts with microprocessor knees and nonmicroprocessor knees and found no significant difference in step-related activity outcomes. Two studies also found that general health with the use of microprocessor knees and nonmicroprocessor knees had nonsignificant improvements. When considering overall costs to society, including prosthetic acquisition costs, inpatient and outpatient care, hospital expenses, housekeeping, transportation, adaptive technology, and lost productivity, there was no significant difference when comparing microprocessor knees to nonmicroprocessor knees. | Quality of evidence: NR Strength of recommendation: NR |
“Recommendation 4. Microprocessor knees for limited community ambulators: Among limited community ambulators, microprocessor knees are indicated to enable increases in level ground walking speed and walking speed on uneven terrain while substantially reducing uncontrolled falls and increasing both measured and perceived balance.” (p. 6) Supporting evidence: A review on the effects of microprocessor knees for limited community ambulators found that there was increased self-selected walking velocity, ambulation across uneven surfaces, and an increase in descending slopes and hills. There was also a reduction in falls, and a significant decrease in the frequency of stumbles, uncontrolled falls, and frustration with falls in a similar population. Microprocessor knees were found to potentially enable community ambulators to perform activities that are typically for unlimited community ambulators. | Quality of evidence: NR Strength of recommendation: NR |
ESAR = energy storing and return; NR = not reported; QALY = quality-adjusted life-year.
Note: This table has not been copy-edited.
aExternally-powered prostheses include myoelectric prostheses. In this guideline document, an externally-powered prosthetic is “one characterized by at least one motorized joint, powered through a battery, and actuated by the user through one or more control inputs. The most common control inputs for externally-powered prostheses are electromyography (EMG) surface electrodes embedded into the socket. Externally-powered prostheses that utilize EMG electrodes are commonly referred to as ‘myoelectric’ prostheses.” (p. 81)6
Appendix 6: Overlap Between Included Systematic Reviews
Please note that this appendix has not been copy-edited.
Table 14: Overlap in Relevant Primary Studies Between Included Systematic Reviews
Primary study citation | Hahn et al. (2022)29 | Thibaut et al. (2022)30 |
|---|---|---|
Burçak B, et al. Ann Phys Rehabil Med. 2021;64(1):101405. | — | Yes |
Burnfield JM, et al. Prosthet Orthot Int. 2012;36(1):95 to 104. | Yes | — |
Campbell et al. J Rehabil Assist Technol Eng. 2020;7:2055668320968476. | — | Yes |
Davie-Smith F and Carse B. Prosthet Orthot Int. 2021;45(3):198 to 204. | Yes | — |
Eberly VJ, et al. Prosthet Orthot Int. 2014;38(6):447 to 455. | Yes | — |
Gerzeli S, et al. Eur J Health Econ. 2009;10(1):47 to 55 | — | Yes |
Hafner BJ and Smith DG. J Rehabil Res Dev. 2009;46(3):417 to 434. | Yes | — |
Hahn A and Lang M. J Prosthet Orthot. 2015;27(3):86 to 95. | Yes | — |
Hahn A, et al. Medicine. 2016;95(45):e5386. | Yes | — |
Hasenoehrl T, et al. Disabil Rehabil Assist Technol. 2017;95:1 to 9. | Yes | — |
Highsmith MJ, et al. J Rehabil Res Dev. 2016;53(6):753 to 66. | — | Yes |
Highsmith MJ, et al. Technol Innov. 2016;18(2 to 3):139 to 50. | — | Yes |
Highsmith MJ, et al. Technol Innov. 2016;18(2 to 3):151 to 7. | — | Yes |
Highsmith MJ, et al. Prosthet Orthot Int. 2013;37(5):362 to 8. | — | Yes |
Jayaraman C, et al. J Neuroeng Rehabil. 2021;18(1):88. | Yes | — |
Kahle JT, et al. J Rehabil Res Dev. 2008;45(1):1 to 14. | Yes | — |
Kaufman KR, et al. Clin Biomech. 2018;58:116 to 122. | Yes | Yes |
Lansade C, et al. Ann Phys Rehabil Med. 2021;64(1):101386. | — | Yes |
Lansade C, et al. Ann Phys Rehabil Med. 2018;61(5):278 to 85. | Yes | Yes |
Lura DJ, et al. Gait Posture. 2017;58:103 to 7. | — | Yes |
Lura DJ, et al. Clin Biomech. 2015;30:175 to 81. | — | Yes |
Maaref K, et al. Arch Phys Med Rehabil. 2010;91(6):919 to 25. | — | Yes |
Mileusnic MP, et al. J Prosthet Orthot. 2017;29(4):198 to 205. | Yes | — |
Moller S, et al. Prosthet Orthot Int. 2019;43(3):257 to 65. | — | Yes |
Moller S, et al. Disabil Rehabil Assist Technol. 2018;13(3):220 to 5. | — | Yes |
Sen M, et al. Acta Orthop Traumatol Turc. 2020;54(5):502 to 6. | — | Yes |
Theeven PJ, et al. J Rehabil Med. 2012;44(5):454 to 461. | Yes | — |
Theeven PJ, et al. J Rehabil Med. 2011;43(10):906 to 915. | Yes | Yes |
Wong K, et al. Arch Phys Med Rehabil. 2015;94(10): 804 to 810. | Yes | — |
Wurdeman SR, et al. Assist Technol. 2020;32(5):236 to 42. | — | Yes |
ISSN: 2563-6596
Canada’s Drug Agency (CDA-AMC) is a pan-Canadian health organization. Created and funded by Canada’s federal, provincial, and territorial governments, we’re responsible for driving better coordination, alignment, and public value within Canada’s drug and health technology landscape. We provide Canada’s health system leaders with independent evidence and advice so they can make informed drug, health technology, and health system decisions, and we collaborate with national and international partners to enhance our collective impact.
Disclaimer: CDA-AMC has taken care to ensure that the information in this document was accurate, complete, and up to date when it was published, but does not make any guarantee to that effect. Your use of this information is subject to this disclaimer and the Terms of Use at cda-amc.ca.
The information in this document is made available for informational and educational purposes only and should not be used as a substitute for professional medical advice, the application of clinical judgment in respect of the care of a particular patient, or other professional judgments in any decision-making process. You assume full responsibility for the use of the information and rely on it at your own risk.
CDA-AMC does not endorse any information, drugs, therapies, treatments, products, processes, or services. The views and opinions of third parties published in this document do not necessarily reflect those of CDA-AMC. The copyright and other intellectual property rights in this document are owned by the Canadian Agency for Drugs and Technologies in Health (operating as CDA-AMC) and its licensors.
Questions or requests for information about this report can be directed to Requests@CDA-AMC.ca.