Drugs, Health Technologies, Health Systems
Health Technology Review
Midline Catheters for Administering Intravenous Infusion Therapy
Key Messages
What Is the Issue?
Used to administer medications, nutrition, blood products, and other fluids, IV infusion therapy is an important part of clinical care across various health care settings.
Multiple types of venous access devices are available for IV therapy, including peripheral and central devices. Selecting the most appropriate venous access device is essential for ensuring patient safety and comfort.
Midline catheters, a type of peripheral venous access device, are increasingly used as an alternative to other peripheral catheters and central venous access devices. However, variations in clinical practice and uncertainty regarding their optimal use create challenges for clinicians and policy-makers in standardizing care.
What Did We Do?
We prepared this Rapid Review to summarize and critically appraise the available studies on the clinical effectiveness of midline catheters compared to other vascular access devices to support decision-making about the use of midline catheters for administering IV infusion therapy. We also sought to identify evidence-based guidelines regarding the use of midline catheters for administering IV infusion therapy.
We searched key resources, including journal citation databases, and conducted a focused internet search for relevant evidence published since 2020. Two reviewers screened articles for inclusion based on predefined criteria, critically appraised the included studies, and narratively summarized the findings.
What Did We Find?
We found 8 systematic reviews (SRs) that evaluated the clinical effectiveness of midline catheters compared to peripherally inserted central catheters (PICCs) (7 SRs) and central venous catheters (1 SR) for administrating IV infusion therapy, as well as 5 evidence-based guidelines that provide recommendations on the appropriate indications for midline catheter use.
Compared to PICCs, midline catheters may be associated with higher rates of total complications, catheter-related venous thromboembolism, catheter leakage, treatment discontinuation or premature catheter removals, infiltration, and shorter mean catheter dwell times. Midline catheters were also associated with lower rates of catheter-related bloodstream infection. None of the included SRs detected statistically significant differences between midline catheters and PICCs for phlebitis, catheter occlusion, catheter displacement, or mortality.
Compared to central venous catheters, midline catheters were associated with lower rates of total complications, catheter-related thrombosis, catheter-related infections, and catheter blockage. They also had longer mean catheter dwell times. The SR that examined this comparison did not find significant differences in phlebitis, catheter leakage, or catheter displacement.
Although some SRs reported statistically significant differences between midline catheters and other venous access devices, these findings were inconsistent across the included studies. Not all SRs detected statistically significant between-group differences for each of these outcomes.
The quality of the SRs described in this Rapid Review, as well as the quality of primary studies included in the SRs, was limited. Most of the clinical evidence summarized in this review is from low-to-moderate quality nonrandomized studies that may be influenced by selection bias, confounding bias, and performance bias.
We did not find any studies on the clinical effectiveness of midline catheters versus other peripheral venous access devices for administering IV infusion therapy that met our selection criteria for this review.
Evidence-based guidelines based mostly on low-quality evidence or expert opinion recommend considering midline catheters as an option in various clinical scenarios, including for children and adults who need longer-term peripheral venous access (e.g., up to 4 weeks). Guidelines also recommend avoiding the use of midline catheters for administering continuous vesicant therapy, parenteral nutrition, or solutions with extremes of pH or osmolarity and for patients with a history of thrombosis, hypercoagulability, decreased venous flow to the extremities, end-stage renal disease requiring vein preservation, or with planned or existing arteriovenous fistula or arteriovenous graft.
What Does This Mean?
Health care professionals and decision-makers can use this evidence to inform decisions around the appropriate use of midline catheters for administering IV infusion therapy.
Current evidence-based guidelines support the use of midline catheters in certain clinical scenarios after consideration for the type and anticipated duration of therapy and individual patient needs.
Further high-quality research from robustly conducted studies with improved reporting is needed to confirm the clinical effectiveness of midline catheters versus other vascular access devices.
Abbreviations
GRADE
Grading of Recommendations Assessment, Development and Evaluation
INS
Infusion Nurses Society
PICC
peripherally inserted central catheter
SR
systematic review
Research Questions
What is the clinical effectiveness of midline catheters versus other vascular access devices for administering IV infusion therapy?
What are the evidence-based guidelines regarding the use of midline catheters for administering IV infusion therapy?
Context and Policy Issues
What Is IV Infusion Therapy?
IV infusion therapy is a common medical technique used to administer medications, nutrition, blood products, or other fluids directly into the bloodstream through a vein. This is typically done using a catheter — a thin, flexible tube that can vary in design, size, length, material, and insertion site.1 Approximately 80% to 90% of patients who are hospitalized receive some form of IV infusion therapy, with more than 1 billion IV catheters inserted globally in patients who are hospitalized each year.2,3
Vascular access is broadly categorized into 2 main types: central and peripheral venous access. Central venous access occurs when the catheter’s tip is positioned in the inferior vena cava, superior vena cava, or right atrium.4 Central venous catheters are typically inserted at the internal jugular, subclavian, or femoral veins.4 For PICCs, a type of central venous access device, insertion sites include the basilic, brachial, or cephalic veins.5 In contrast, peripheral venous access is achieved when the catheter tip is located outside of the central veins.6 Peripheral venous access devices are usually inserted into the superficial veins of the upper limbs, such as those in the forearm or wrist.6
Many factors may influence the selection of a venous access device, including the type and duration of therapy, the risk of complications, and the patient’s medical history, vascular condition, and personal preferences.7
What Are Midline Catheters and What Are Their Potential Benefits?
Midline catheters are a type of peripheral venous access device that is longer than other peripheral IV catheters, but does not reach the central circulation.8 Introduced to clinical settings in the 1950s, midline catheters were developed as an alternative for patients requiring longer-term IV therapy without the need for central venous access.9 They are typically inserted into a vein in the upper arm (e.g., basilic, cephalic, or brachial veins) with the catheter tip positioned at or near the level of the axilla.8 Midline catheters are available with either a single or double lumen and range from 10 to 20 cm long, though some sources report variations in the accepted length range.10,11
Central lines can be technically challenging to place, pose a risk of serious complications, and are associated with considerable health care costs.12,13 Like other peripheral venous access devices, midline catheters are relatively easy to insert, yet they can potentially dwell longer than short peripheral IV catheters.14
Why Is It Important to Do This Review?
Selecting an appropriate vascular access device has implications for patient safety, treatment effectiveness, and health care costs.15 While the use of midline catheters in clinical practice is increasing, there remains uncertainty about their optimal indications and when they should be used as an alternative to central venous catheters or other peripheral venous access devices.9
Canada's Drug Agency previously conducted a review16 on the clinical effectiveness of midline catheters compared to extended dwell catheters for delivering peripherally compatible IV antibiotics to adults. A broader review of the available evidence, including other applications of midline catheters, could provide additional information to help guide informed decision-making on the appropriate use of midline catheters in patient care.
Objective
We prepared this Rapid Review to identify, summarize, and critically appraise the evidence regarding the clinical effectiveness of midline catheters compared to other vascular access devices for IV infusion therapy and to summarize and critically appraise the evidence-based guidelines that provide recommendations on the appropriate indications for midline catheter use.
Methods
An information specialist conducted a customized literature search, balancing comprehensiveness with relevance, of multiple sources and grey literature on January 13, 2025. Two reviewers screened citations and selected studies based on the inclusion criteria presented in Table 1, and critically appraised included publications using established critical appraisal tools. Appendix 1 presents a detailed description of methods and selection criteria for included studies.
Criteria | Description |
|---|---|
Population | People of any age undergoing IV infusion therapy |
Intervention | Midline catheters for administering IV infusion therapy |
Comparator | Q1: Other vascular access devices for administering IV infusion therapy, including:
Q2: Not applicable |
Outcomes | Q1: Clinical benefits (e.g., health-related quality of life, catheter dwell times) and harms (i.e., adverse events or complications) Q2: Recommendations regarding:
|
Study designs | Q1: Health technology assessments and SRs Q2: Evidence-based guidelines |
Publication date | Since January 1, 2020 |
PICC = peripherally inserted central catheter; SR = systematic review.
Summary of Evidence
Quantity of Research Available
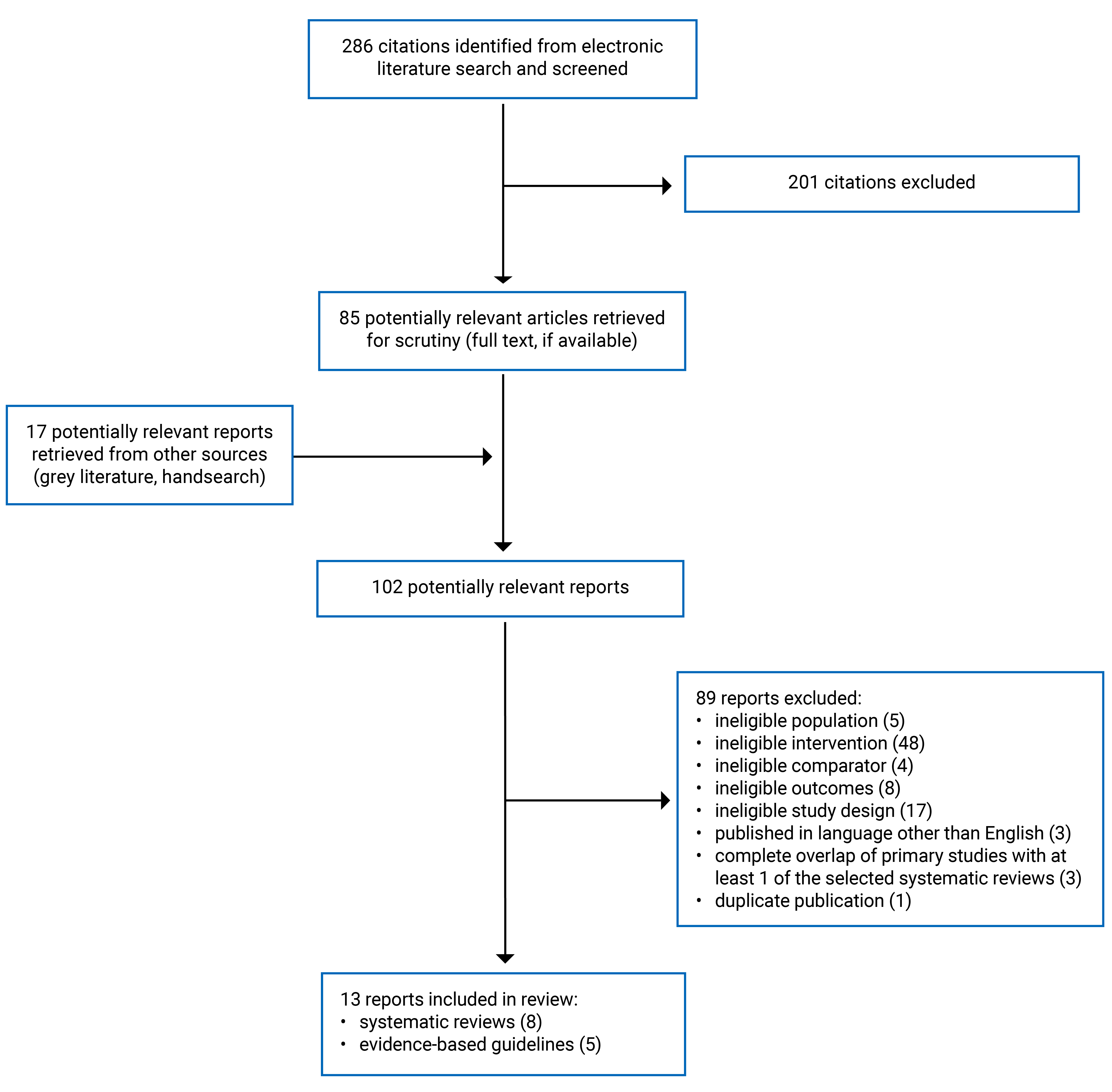
This report includes 13 publications that met the inclusion criteria, including 8 SRs17-24 and 5 evidence-based guidelines.25-29 Appendix 1 presents the PRISMA30 flow chart of the study selection.
Summary of Study Characteristics
Summaries of study characteristics are organized by research question. Appendix 2 provides detailed characteristics of the included publications.
Included Studies for Question 1: Clinical Effectiveness of Midline Catheters
Eight SRs (7 with meta-analyses)17-24 were included. Of these, 7 SRs17,18,20-24 compared midline catheters with PICCs. One SR19 compared midline catheters with central venous catheters, but the authors did not specify the types of central venous catheters that were eligible or examined in their included primary studies. Five SRs were conducted in China,19,20,22-24 1 in the US,21 1 in Taiwan,18 and 1 in Norway.17 These SRs17-24 were published between 2022 to 2024, and 5 stated that they received funding.17,19,20,23,24 Collectively, the 8 SRs17-24 evaluated data from 46 unique relevant primary studies. However, there was an overlap of 21 primary studies included in multiple SRs.17-24 On average, each overlapping primary study appeared in 3 SRs (range, 2 to 5). Therefore, estimates of clinical effectiveness are based on similar data, even though outcomes were not always the same across these publications. Appendix 5 describes the primary study overlap.
Comprehensive participant characteristics, including PROGRESS-Plus criteria,31,32 were not reported in any of the SRs.17-24 For example, gender or sex was not reported in 4 SRs.17,22-24 No included SRs described how gender or sex were defined and did not include gender identities, outside of male and female. The included primary studies across all SRs were a mix of randomized controlled trials and observational studies, while 1 SR17 did not specify the primary study design of included studies. The population reported among all SRs17-24 was from patients of any age who were not pregnant ranging from 1 to 101 years, receiving any IV infusion therapy administered via midline catheters, PICCs, or central venous catheters. Of note, 1 SR17 specifically evaluated data from patients with cancer receiving palliative care. When reported, the proportion of female participants ranged from 23% to 74%, while the proportion of male participants ranged from 31% to 76%. The relevant clinical outcomes reported across the 8 SRs17-24 were:
catheter-related complications
catheter dwell times
treatment discontinuation
mortality
participant satisfaction
pain.
Included Studies for Question 2: Guidelines Regarding the Use of Midline Catheters
Five evidence-based guidelines,25-29 published from 2023 to 2024, were relevant for this report. Four guidelines25,26,28,29 were developed for health care professionals, while 1 guideline27 was developed specifically for health care practitioners, patients, and hospital administrators involved in health care. Two guidelines were developed in the US, (1 by the American College of Radiology28 and 1 by the Infusion Nurses Society [INS]),25 2 guidelines were developed in Italy by the Catholic University Hospital ‘A. Gemelli,’26,29 and 1 guideline was developed by the WHO.27
Four guidelines25,26,28,29 used multiple electronic databases to conduct their literature search for English articles published between 2000 and 2024, and 1 guideline27 searched for articles published between 1980 and 2023 with no language restrictions. The included guidelines varied regarding their target population and approach to reporting: 1 did not specify the target population or clinical setting;25 1 targeted adults without specifying the clinical setting;29 1 targeted patients who were hospitalized and not hospitalized, but age was not specified;28 1 targeted children who were hospitalized and not hospitalized;26 and 1 targeted children (including neonates and adolescents) and adults regardless of the type of care settings.27 The guidelines were developed considering the selection, access, insertion, maintenance, and removal of venous access devices, including peripheral venous access devices (i.e., peripheral IV catheters, midline catheters, arm or chest ports, or short and long peripheral catheters) and central venous access devices (i.e., central catheters, totally implanted venous access devices, femoral inserted central catheters, tunneled and non-tunneled central venous catheters, and PICCs).25-29
The general outcomes of interest were patient safety,25,26,28,29 clinical efficacy and effectiveness,25,29 cost-effectiveness,25,29 acceptability,25 efficiency,25 and all-cause bloodstream infections related to venous access;27 no other clinical outcomes, such as hospital length of stay or mortality were considered among all guidelines.
Summary of Critical Appraisal
Overall, the level of quality from the included publications (8 SRs [7 with meta-analyses] and 5 evidence-based guidelines) was low to moderate. Appendix 3 presents additional details regarding the limitations and strengths of the included publications.
Systematic Reviews
All SRs17-24 clearly described their objectives, eligibility criteria (e.g., population, intervention, comparator, and outcome criteria) and all conducted literature searches using multiple databases, improving clarity, reproducibility, transparency and interpretability of findings. However, 7 SRs17,18,20-24 did not conduct a grey literature search, although they reported appropriate search terms and language restrictions (i.e., English17,18,20-24 and Chinese19,22). Excluding grey literature searches can lead to misleading treatment effects when key evidence from these sources is missed and can lead to an increased risk of bias. Limiting study eligibility based on the language of the publication affects the external validity and overall applicability, for example, it potentially excludes high-quality studies published in different languages from research groups or countries with similar or different health care systems. The rationale for not conducting grey literature searches and imposing language restrictions on eligible publications was not discussed in the included SRs.17,18,20-24
Study selection and data extraction were inconsistent across all studies,17-24 compromising the validity, reliability, and applicability of the findings:
one SR18 justified the inclusion of randomized controlled trials
one SR19 provided a list of studies excluded after full-text review with reasons for exclusion
two SRs17,20 adequately described included primary studies (e.g., study design, population, or outcomes of interest)
no SRs17-24 described the statistical methods of primary included studies.
All SRs17-24 assessed the quality of primary studies using a satisfactory tool and reported no conflict of interests. Seven SRs17-21,23,24 disclosed funding sources, while the authors of 1 SR22 did not. The funding sources of included primary studies were not reported in all SRs,17-24 affecting transparency and risk of funding bias. The authors of 4 SRs18-21 registered their study protocols in PROSPERO, and the completed reviews followed the outlined approaches without any major deviations. This helps reduce potential research duplication, publication bias, and selective reporting of outcomes. Appropriate statistical methods were used in 6 SRs.18,19,21-24 Four SRs18,22-24 reported low heterogeneity in their primary analysis, but discussion on this was limited. The authors of 1 SR17 indicated that meta-analysis was not possible due to the heterogeneity of primary studies. Publication bias was assessed in 5 SRs19,20,22-24 using funnel plots. However, most included studies had a variable risk of bias, and authors did not examine how risk of bias of the included primary studies could have impacted the results.17-21,23,24
Evidence-Based Guidelines
All guidelines25-29 clearly described their scope and purpose, outlining the involvement of relevant professional knowledge users and the target users. Relevant studies were retrieved from multiple databases in all guidelines.25-29 One guideline27 sought patient involvement, helping to ensure relevance and applicability and incorporate patient-centred perspectives. A high level of rigour in development was observed in 1 guideline.27 One guideline27 did not have geographical or lingual restrictions. However, 4 guidelines25,26,28,29 did not clearly report the methods of selecting articles (e.g., detailed inclusion and exclusion criteria) to inform their recommendations. All recommendations from all guidelines25-29 were specific, unambiguous, and were easily identifiable.
Assessment of quality of evidence differed across all guidelines: 3 did not report a tool used to assess the article’s quality,26,29,33 1 used the Grading of Recommendations Assessment, Development and Evaluation (GRADE) methodology,27 and 1 used the American College of Radiology Appropriateness Criteria Methodology.28 Transparent and consistent reporting of quality assessment tools is necessary to understand if, and how, quality of evidence was assessed. Three guidelines25,28,29 did not report the methods to achieve consensus, and 3 did not report a guideline validation method.26,28,29 The applicability of the guidelines was not uniform, and key factors such as facilitators, barriers, monitoring, and auditing criteria were not reported. In 3 guidelines,25,27,28 it was unclear whether funding influenced the content. However, all guidelines25-29 reported potential conflicts of interest.
Summary of Findings
Appendix 4 presents additional details regarding the main study findings.
Clinical Effectiveness of Midline Catheters Versus PICCs
Seven SRs (6 with meta-analyses)17,18,20-24 provided information on the clinical effectiveness of midline catheters versus PICCs for administering IV infusion therapy. There was considerable overlap in the primary studies that were included in these SRs; the pooled estimates from separate reviews thus contain much of the same data (refer to Appendix 5 for details regarding overlap).
Catheter-Related Complications
Total Complications
Two SRs with meta-analyses18,20 reported on the effect of midline catheters compared to PICCs on total complication rates. One SR,18 which pooled data from 4 studies, found that midline catheters were associated with a statistically significantly higher total complication rate compared to PICCs. In a separate analysis of a single study involving children, the increased risk of total complications remained significant. A third analysis of 3 studies focusing on adults found no statistically significant difference in total complication rates.
The second SR,20 based on a pooled analysis of 14 studies, found no statistically significant difference in total complications per patient. However, when analyzing per total catheter days (pooled data from 9 studies), there were statistically significantly more total complications observed in the midline catheter group.
Thrombosis
Four SRs with meta-analyses18,20,21,24 provided mixed results for the clinical effectiveness of midline catheters versus PICCs with respect to thrombosis-related outcomes:
One SR,24 based on a pooled analysis of 12 studies, reported that midline catheters were associated with statistically significantly higher rates of venous thromboembolism. The authors conducted additional analyses specific to adults (5 studies) and to other age groups (e.g., children and mixed age groups; 7 studies), and reported the difference remained statistically significant for both groups.
One SR21 reported that midline catheters were at a significantly increased risk for superficial vein thrombosis, based on a pooled analysis of 2 studies, but there were no statistically significant differences between midline catheters and PICCs with respect to risk for localized thrombosis (i.e., superficial vein thrombosis, deep vein thrombosis, or other thrombosis), deep vein thrombosis, and pulmonary embolism.
One SR18 assessed thrombosis rates in adults (pooled analysis of 4 studies), children (1 study), and in populations of any age (pooled analysis of 5 studies). In all 3 analyses, there were no statistically significant differences between midline catheters and PICCs.
Findings from the Wen et al. SR20 suggested that the proportion of patients with catheter-related superficial vein thrombosis and the rate of catheter-related deep vein thrombosis or superficial vein thrombosis (analyzed per total catheter days) was higher in patients who had a midline catheter. Rates of other thrombosis-related outcomes, including catheter-related deep vein thrombosis, contralateral and/or bilateral thrombosis, and pulmonary embolism were not statistically significantly different between the 2 groups.
Infection
Four SRs with meta-analyses18,20-22 described the risk of infection in participants who received IV therapy with midline catheters compared to PICCs:
One SR21 reported that midline catheters were associated with statistically significantly fewer patients with catheter-related bloodstream infections compared with PICCs, based on a pooled analysis of 9 studies. When analyzed per catheter, there was no significant difference between midline catheters and PICCs in risk for catheter-related bloodstream infections.
Based on a pooled analysis of 10 studies, the SR by Wen et al.20 reported participants who used midline catheters had a significantly lower incidence of catheter-related bloodstream infection compared to participants who used PICCs. When analyzed by total catheter days, there was no statistically significant difference between the 2 groups (7 studies).
One SR22 reported no differences in the proportion of participants with catheter-related bloodstream infection, based on a pooled analysis of 11 studies. However, findings from a sensitivity analysis that excluded low quality studies indicated that the incidence of catheter-related bloodstream infection in the midline catheter group was statistically significantly lower than that in the PICC group. There were no statistically significant differences in the number of participants with catheter-related bloodstream infection in 2 additional analyses that were specific to adults (6 studies) and studies that included children, mixed age groups, and those that did not report age (5 studies).
The fourth SR18 reported no differences in the number of catheter-related bloodstream infections, based on a pooled analysis of 5 studies. There were no differences in the number of catheter-related bloodstream infections in 2 additional analyses that were specific to children and adults.
Phlebitis
Pooled estimates from 3 SRs20,21,23 indicated no statistically significant difference in phlebitis rates between participants who received IV therapy using midline catheters and those using PICCs.
Catheter Occlusion
Two SRs with meta-analyses20,21 found no statistically significant difference in catheter occlusion rates between midline catheters and PICCs. These findings were consistent in analyses conducted both per participant and per catheter (e.g., the number of occlusions per total catheter days).
Catheter Leakage
One SR20 with meta-analysis compared the incidence of leakage between midline catheters and PICCs. The results indicated that midline catheters had a statistically significantly higher rate of leakage compared to PICCs, both when analyzed per participant (based on a pooled estimate from 5 studies) and per total catheter days (based on a pooled estimate from 4 studies).
Catheter Displacement
One SR20 with meta-analysis found no statistically significant difference in the rates of catheter displacement between the midline catheter and PICC groups.
Infiltration
One SR with meta-analysis20 evaluated the incidence of infiltrations among participants who received therapy with either midline catheters or PICCs. A pooled analysis of 6 studies found that participants with midline catheters had statistically significantly higher incidence of infiltration. When analyzed by total catheter days, there was no statistically significant difference in the number of catheters with infiltration between the 2 groups (based on a pooled estimate from 5 studies).
Catheter Fracture
The SR by Urtecho et al.21 found no statistically significant differences between the midline catheter and PICC groups in the number of participants with a fractured catheter or the number of catheters that fractured.
Catheter Dwell Time
Two SRs17,18 provided information on the effect of midline catheters versus PICCs on catheter dwell times. One SR,18 which pooled data from 4 studies, found that midline catheters were associated with statistically significantly shorter mean dwell time. Similarly, the authors’ analysis of a single study involving children indicated a significantly shorter mean dwell time for midline catheters. A third analysis of 3 studies focusing on adults found no statistically significant difference in mean catheter dwell time between midline catheters and PICCs.
The second SR17 included a prospective case series that reported catheter dwell times for participants who received a midline catheter or a PICC. The median dwelling time was 50.5 days in the midline group and 102 days in the PICC group; however, no statistical analysis was conducted to determine whether the between-group difference was significant.
Treatment Discontinuation
Three SRs with meta-analyses18,20,21 provided mixed results for measures of treatment discontinuation:
One SR18 reported that the mean number of premature catheter removals per 1,000 catheter days was statistically higher with midline catheters compared to PICCs based on their analyses of studies of any population age (3 studies) and studies of adults (2 studies), but that there was no statistically significant between-group difference in their analysis of studies specific to children (1 study).
Based on a pooled analysis of 6 studies, findings from the SR by Urtecho et al.21 indicated that the use of midline catheters was associated with more participants discontinuing therapy compared with PICCs. When evaluated per catheter, no difference was observed between the number of treatment discontinuations between the midline catheter and PICC groups (based on a pooled analysis of 3 studies).
One SR20 found no statistically significant difference between midline catheters and PICCs in the proportion of participants with premature catheter removal (based on a pooled estimate from 5 studies) and the number of premature catheter removals when analyzed by total catheter days (based on a pooled estimate from 4 studies).
Mortality
One SR with meta-analysis21 found no statistically significant difference in mortality between participants who received IV therapy with midline catheters versus PICCs, based on an analysis that included 1 primary study.
Other Outcomes
Based on an analysis of 1 primary study, the Wen et al. SR20 reported that participants treated with a PICC had a statistically significantly higher rate of dissatisfaction. Additionally, the authors of the SR20 found no statistically significant between-group differences in pain (whether assessed per participants or per catheter) or participant satisfaction rates. The authors did not provide information on how dissatisfaction, satisfaction, or pain were defined or measured.
Clinical Effectiveness of Midline Catheters Versus Central Venous Catheters
One SR19 provided information on the clinical effectiveness of midline catheters versus central venous catheters for administering IV infusion therapy.
Catheter-Related Complications
Total Complications
A pooled analysis of 10 studies from the SR19 found that the total complication rate was statistically significantly lower in the midline catheter group compared to the central venous catheter group.
Thrombosis
The SR,19 based on a pooled analysis of 8 studies, found that catheter-related thrombosis occurred less frequently in the midline catheter group than in the central venous catheter group, with a statistically significant difference.
Infection
Based on a pooled analysis of 8 studies,19 the incidence of catheter-related infection was statistically significantly lower in participants who received therapy with midline catheters compared to those with central venous catheters.
Phlebitis
The SR19 found no statistically significant difference in the occurrence of phlebitis between midline catheters and central venous catheters (meta-analysis of 8 studies).
Catheter Occlusion
The SR,19 based on a pooled analysis of 6 studies, found a statistically significant difference in catheter blockage between the 2 groups, with midline catheters having a lower incidence rate.
Catheter Leakage
Based on a pooled analysis of 7 studies, the SR19 found no statistically significant difference in the occurrence of leakage between the midline catheter and central venous catheter groups.
Catheter Displacement
A pooled analysis of 3 studies in the SR19 indicated that there was no statistically significant difference in the occurrence of catheter displacement between the midline catheter and central venous catheter groups.
Catheter Dwell Time
The SR,19 which pooled data from 3 studies, found that midline catheters were associated with statistically significantly longer mean catheter dwell times.
Guidelines Regarding the Use of Midline Catheters
We identified 5 evidence-based guidelines25-29 that provide recommendations on the appropriate use of midline catheters. Of these, 2 guidelines25,29 focus on adults, 1 guideline26 addresses children, 1 guideline27 applies to both adults and children, and 1 guideline28 does not specify the patient age to which its recommendations apply. Table 19 provides detailed recommendation statements and supporting evidence.
Recommendations for Adults
The INS guidelines25 recommend using midline catheters for adults who are hospitalized, require peripherally compatible therapy, and have an anticipated duration of therapy of 5 to 14 days. Additionally, the INS guidelines25 provide further guidance on the appropriate use of midline catheters:
Avoid using midline catheters as a strategy to prevent central line-associated bloodstream infections when central venous access is indicated.
Do not use midline catheters for continuous infusion of vesicant therapy, parenteral nutrition, or other infusates (i.e., fluids given through IV) with extreme pH or osmolarity (from original source).
Avoid midline catheters in patients with a history of thrombosis, hypercoagulability, decreased venous flow to the extremities, or end-stage renal disease requiring vein preservation.
For patients with a planned or existing arteriovenous fistula or arteriovenous graft, avoid inserting midline catheters and PICCs whenever possible due to an increased risk of thrombosis.
While midline catheters may be labelled for obtaining blood samples, further high-quality research is needed to establish a standard procedure for blood sampling with midline catheters.
Remove midline catheters in pediatric and adult patients based on site assessment and clinical signs or symptoms of systemic complications rather than solely on catheter dwell time.
Consider the risk for catheter-associated thrombosis when using midline catheters.
Do not use midline catheters for continuous infusions of antineoplastic vesicants.
Do not use midline peripheral catheters placed in deep peripheral vessels for continuous vesicant therapy.
The developers of the INS guidelines25 assigned a level of evidence to their recommendations based on study design, ranging from the highest level I (e.g., based on a meta-analysis) to the lowest level of V (e.g., based on case reports). However, they did not specify the strength of individual recommendations, and the process for achieving committee consensus for each recommendation was not reported.
The guidelines by Pittiruti et al. (2023)29 stated that the indications for specific peripheral venous access devices in adults are mainly based on the expected duration of treatment, and that midline catheters are appropriate when the expected duration is more than 4 weeks. This guideline did not report the strength of the recommendation, the quality of evidence informing the recommendation, or the methods for achieving committee consensus.
Recommendations for Children
The guidelines by Pittiruti et al. (2024)26 recommend that midline catheters may be taken into consideration in some selected cases of children who are not hospitalized and who need peripheral venous access for less than 4 weeks. This recommendation qualified as having strong agreement, as 19 of the 20 committee members voted in agreement (1 member was uncertain). The strength of the recommendation and the quality of evidence informing this recommendation were not reported.
Recommendations for Adults and Children
In adults and children requiring longer term IV access, the WHO guideline27 recommends the use of either a PICC or midline vascular catheter (conditional recommendation based on very low certainty evidence).
Without specifying patient age, the American College of Radiology28 guidelines state that midline catheters may be appropriate for patients who are acutely ill and are requiring infusion of an irritant medication, hemodynamic monitoring, or frequent blood draws for 2 weeks or less. The strength of the recommendation and the quality of evidence informing this were not reported.
Limitations
Evidence Gaps
We identified no evidence that examined the clinical effectiveness of midline catheters versus another type of peripheral venous access device (i.e., peripheral IV catheters), or versus specific types of central venous catheters, including tunneled and non-tunneled central venous catheters and totally implanted venous access devices. Therefore, no conclusions can be made on the clinical effectiveness of midline catheters compared to these devices.
The included studies provided limited information on the effect of midline catheters on patient-reported outcome measures, such as health-related quality of life, functional status, and patient experience of care. One SR20 provided data for pain, patient satisfaction, and patient dissatisfaction; however, information on how these outcomes were defined and measured was not reported, making it difficult to interpret their findings.
Although many clinical outcomes showed statistically significant differences between participants who used midline catheters and those who used other venous access devices, none of the included studies discussed minimum clinically important difference values for any of the reported outcomes. As a result, it remains unclear whether the observed differences are meaningful to patients, clinicians, or policy-makers in real-world practice.
Study Quality
In addition to the included SRs17-24 being of limited quality, the primary studies within these SRs also had several methodological limitations. In total, the 8 included SRs analyzed data from 46 relevant primary studies. Although we did not conduct our own critical appraisal of these primary studies, most were observational and may be influenced by selection bias, confounding bias, and performance bias. In the case of randomized controlled trials included in the SRs, the authors of the SRs often provided inadequate reporting of their methodology and other key considerations (e.g., randomization methods, masking of participants and care providers, and primary study authors’ potential conflicts of interest and funding sources). This lack of primary study information limits the reliability of the findings reported in the SRs.
The authors of the included SRs17-24 performed their critical appraisals using various tools, including the Downs and Black checklist, the Cochrane Risk of Bias tool, the Jadad scale, the Newcastle-Ottawa Scale, and the Effective Public Health Practice Project Quality Assessment Tool for quantitative studies. This variability in assessment methods limits comparability across studies. However, primary studies were generally rated as low to moderate in quality and at moderate to high risk of bias due to concerns related to external validity (e.g., the representativeness of study populations), confounding (e.g., the comparability between treatment groups), and reporting quality. Additionally, none of the included SRs reported the funding sources of individual primary studies, so the potential for sponsorship bias is unclear.
Generalizability
The authors of the included SRs17-24 analyzed data from a relatively large number of primary studies with high numbers of participants which were conducted in many different countries, including Australia, Canada, China, the Czech Republic, Denmark, England, Italy, South Korea, the UK, and the US. For example, the SR by Lu et al. (2022b)23 included data from 12 primary studies, comprising 40,871 participants, for their analysis of venous thromboembolism. Large participant numbers from studies conducted in various locations may increase the generalizability of the findings.
However, the reporting of primary study participants’ characteristics and care settings was generally poor across all 8 SRs. We used PROGRESS-Plus31,32 to guide data extraction and to provide insights into whether the analyses from the relevant SRs included data from diverse patient populations who could be representative of those in Canada. While some SRs provided basic demographic details, such as the mean age and the proportion of male or female participants, many important characteristics were not described.
Furthermore, when participant sex or gender were reported, the SRs17-24 did not include any information on how they were defined or measured, and it was unclear how gender diversity was considered. To improve generalizability to clinical practice settings in Canada, the analyses could have included participants with diversity across characteristics that stratify health opportunities and outcomes, such as race, ethnicity, place of residence, occupation, and socioeconomic status. Because these aspects were underreported in the included SRs, generalizability is uncertain.
In addition to participant characteristics, care indications and settings were also underreported. Apart from the SR by Gravdahl et al.,17 which focused on patients with cancer receiving palliative care, none of the included SRs clearly described the types of care indications that were examined across their included primary studies. The clinical effectiveness of catheters for IV infusion may vary depending on the types of medical conditions they are used to manage, as well as the availability of health care personnel and resources, such as clinicians who specialize in catheter insertion (e.g., PICC nurses), imaging equipment for guided placement (e.g., ultrasound or fluoroscopy), and infection control professionals.5,34,35 Without more detailed information, it is unclear whether the findings are generalizable to all care indications and settings, including less-resourced settings.
None of the included evidence-based guidelines were developed for use in Canada, which may limit the applicability of the recommendations summarized in this report in the health care context in Canada.
Conclusions and Implications for Decision- or Policy-Making
This Rapid Review evaluated the literature regarding the clinical effectiveness of midline catheters compared to alternative venous access devices for administering IV infusion therapy, as well as evidence-based guidelines related to the use of midline catheters for administering IV infusion therapy. The evidence summarized in this report is drawn from SRs17-24 with substantial overlap in primary studies, meaning that data from the same participants were included in more than 1 SR. Appendix 5 provides a citation matrix illustrating the degree of primary study overlap. As a result, some evidence may be disproportionally represented in the overall conclusions.
Summary of Evidence
Evidence from the 7 SRs (6 with meta-analyses)17,18,20-24 suggest that, compared to PICCs, midline catheters may be associated with lower rates of catheter-related bloodstream infections but higher rates of total complications, catheter-related venous thromboembolism, catheter leakage, infiltration, treatment discontinuation or premature catheter removals, and shorter mean catheter dwell times. There was no evidence to indicate any detected statistically significant differences between midline catheters and PICCs for phlebitis, catheter occlusion, catheter displacement, or mortality.
When compared to central venous access catheters, midline catheters were associated with lower rates of total complications, catheter-related thrombosis, catheter-related infections, catheter blockage, as well as longer mean catheter dwell times. The SR with meta-analysis19 that examined this comparison did not detect any statistically significant differences in phlebitis, catheter leakage, or catheter displacement.
The 5 evidence-based guidelines25-29 summarized in this review made recommendations on when midline catheters can be considered an appropriate option for administering IV infusion therapy. For example, guidelines support the use of midline catheters for both children and adults who need longer-term IV access (e.g., up to 4 weeks), after consideration for the type of therapy and individual patient needs. The guidelines25-29 also recommend against using midline catheters for administering continuous vesicant therapy, parenteral nutrition, or solutions with extremes of pH or osmolarity and for patients with a history of thrombosis, hypercoagulability, decreased venous flow to the extremities, end-stage renal disease requiring vein preservation, or with planned or existing arteriovenous fistula or arteriovenous graft.
The limitations of the included literature should be considered when interpreting the findings of this report. None of the included guidelines25-29 were specifically designed for use in Canada, and the SRs17-24 provided limited information on the characteristics of primary study participants and clinical settings. As a result, the applicability of the guidelines25-29 and generalizability of findings from the SRs17-24 is unclear. Additionally, the included SRs17-24 synthesized data from primary studies that evaluated midline catheters across a wide range of care indications and patient populations. While these analyses provide estimates for the overall effect of midline catheters, they do not clarify the specific clinical scenarios in which midline catheters may be most appropriate. Furthermore, the quality of studies included in the SRs and informing the evidence-based guidelines tended to be low, and there is uncertainty as to whether the statistically significant changes in outcome measures observed in the SRs translate into clinically meaningful differences.
We did not identify evidence on the clinical effectiveness of midline catheters versus other peripheral IV catheters. All comparative data within the included SRs compared midline catheters to central venous access devices. As a result, no conclusions can be drawn for this comparison.
Considerations for Future Research
To improve understanding of the role of midline catheters in patient care, robustly designed clinical studies with low risk of bias are needed. Future studies should apply methods to control for confounding factors, such as patient characteristics, severity of illness, infection control practices, and clinician expertise, through experimental design (e.g., randomization) or through statistical analysis. Standardizing how outcome measures are defined and reported could help reduce heterogeneity and improve the comparability of results across clinical studies. High-quality primary studies would enable the development of more robust guidelines and SRs that could provide stronger recommendations and more certain estimates of treatment effects.
Investigators of future primary studies and SRs could consider collecting and reporting patient-reported outcome data, which may provide unique information on the impact of midline catheters from the patients' perspective.36 Additionally, study authors may consider reporting detailed participant characteristics across dimensions of diversity such as age, religion, gender, ethnicity, mental and physical ability, place of residence (or other PROGRESS-Plus criteria)31,32 to provide a better understanding of how the results of their study may generalize to other populations.
Considerations for Decision-Making or Policy-Making
The findings of this Rapid Review suggest that midline catheters may be a suitable venous access device for people requiring IV infusion therapy. However, decision-makers should be aware that the evidence summarized in this review is of limited quality.
In addition to the relevant recommendations outlined in this Rapid Review, we identified 2 additional guidelines37,38 that provide information on the appropriate use of midline catheters. These guidelines were not included because their relevant guidance was not a part of the formal recommendations. However, the information may still be useful to clinicians and decision-makers.
The Registered Nurses' Association of Ontario guidelines37 indicate that midline catheters may be considered when the duration of therapy is less than 4 weeks and when the medications or solutions being administered are well tolerated by peripheral veins, such as antimicrobials, fluid replacement, and analgesics. They also state that midline catheters should not be used for continuous vesicant therapy, parenteral nutrition, or infusates with an osmolarity greater than 900 mOsm/L. The Agency for Clinical Innovation guidelines38 indicate that midline catheters can be used to infuse solutions with an osmolarity of less than 900 mOsm/L when the duration of therapy ranges from 14 days to 4 weeks. The guidelines38 advise against midline catheter use in patients with a history of thrombosis, hypercoagulability, end-stage renal disease requiring vein preservation, and decreased vascular flow to the extremities. The practice advice from both guidelines37,38 align with the recommendations from the evidence-based guidelines included in this Rapid Review.
Although it did not meet the inclusion criteria for our Rapid Review, we also identified an SR39 that examined the impact of midline catheter tip positioning on clinical outcomes. The authors concluded that, compared to placement in the axillary vein, placing the catheter tip in the subclavian vein was associated with lower complication rates and a reduced incidence of catheter-related thrombosis. However, the effect of tip location on catheter dwell time and the rates of other complications remained unclear.39 While these additional sources many provide useful information, the quality of the evidence informing these additional guidelines37,38 and the conclusions made by the authors of the SR39 were not assessed.
Clinicians and other decision-makers can use the evidence summarized in this review to inform their decisions about the appropriate use of midline catheters for administering IV infusion therapy. When making these decisions, careful consideration for factors such as the type of therapy, its physical and chemical properties (e.g., pH or osmolarity), the anticipated duration of therapy, the potential risk of complications, the availability of resources, and individual patient needs is needed.
References
1.Ojha V, Raju SN, Deshpande A, Ganga KP, Kumar S. Catheters in vascular interventional radiology: an illustrated review. Diagn Interv Radiol. 2023;29(1):138-145. doi:10.5152/dir.2022.21233 PubMed
2.Puolitaival A, Savola M, Tuomainen P, Asseburg C, Lundström T, Soini E. Advantages in Management and Remote Monitoring of Intravenous Therapy: Exploratory Survey and Economic Evaluation of Gravity-Based Infusions in Finland. Adv Ther. 2022;39(5):2096-2108. doi:10.1007/s12325-022-02093-6 PubMed
3.Alexandrou E, Ray-Barruel G, Carr PJ, et al. International prevalence of the use of peripheral intravenous catheters. J Hosp Med. 2015;10(8):530-3. doi:10.1002/jhm.2389 PubMed
4.Kolikof J, Peterson K, Baker AM. Central Venous Catheter Insertion. StatPearls Publishing; 2023. Accessed February 11, 2025. https://www.ncbi.nlm.nih.gov/books/NBK557798/
5.Gonzalez R, Cassaro S. Percutaneous Central Catheter. StatPearls Publishing; 2024. Accessed January 23, 2025. https://www.ncbi.nlm.nih.gov/books/NBK459338/
6.Beecham GB, Tackling G. Peripheral Line Placement. StatPearls Publishing; 2023. Accessed February 11, 2025. https://www.ncbi.nlm.nih.gov/books/NBK539795/
7.Fernández-Fernández I, Castro-Sánchez E, Blanco-Mavillard I. Determinants of the optimal selection of vascular access devices: A systematic review underpinned by the COM-B behavioural model. J Adv Nurs. 2024;doi:10.1111/jan.16202 PubMed
8.Adams DZ, Little A, Vinsant C, Khandelwal S. The Midline Catheter: A Clinical Review. J Emerg Med. 2016;51(3):252-8. doi:10.1016/j.jemermed.2016.05.029 PubMed
9.Chopra V, Kaatz S, Swaminathan L, et al. Variation in use and outcomes related to midline catheters: results from a multicentre pilot study. BMJ Qual Saf. 2019;28(9):714-720. doi:10.1136/bmjqs-2018-008554 PubMed
10.Jeon MH, Kim CS, Han KD, Kim MJ. Efficacy and Safety of Midline Catheters with Integrated Wire Accelerated Seldinger Technique. Vasc Specialist Int. 2022;38:2. doi:10.5758/vsi.210062 PubMed
11.Fabiani A, Aversana N, Santoro M, Sanson G. Complications associated to midline- and long peripheral catheters in adults. Systematic review of literature and proposal for a standardized model for data collection. Thromb Res. 2024;236:117-126. doi:10.1016/j.thromres.2024.02.022 PubMed
12.Johansson E, Hammarskjöld F, Lundberg D, Arnlind MH. Advantages and disadvantages of peripherally inserted central venous catheters (PICC) compared to other central venous lines: a systematic review of the literature. Acta Oncol. 2013;52(5):886-92. doi:10.3109/0284186x.2013.773072 PubMed
13.Roldan CJ, Paniagua L. Central Venous Catheter Intravascular Malpositioning: Causes, Prevention, Diagnosis, and Correction. West J Emerg Med. 2015;16(5):658-64. doi:10.5811/westjem.2015.7.26248 PubMed
14.Nickel B. Does the Midline Peripheral Intravenous Catheter Have a Place in Critical Care? Crit Care Nurse. 2021;41(6):e1-e21. doi:10.4037/ccn2021818 PubMed
15.Baldauf B, Cemin R, Hummel J, Bonnemeier H, Assadian O. Central Vascular Access Devices: Current Standards and Future Implications. J Vasc Dis. 2025;4(1):3. doi:10.3390/jvd4010003
16.Hao Q, Horton J. Midline and Extended Dwell Catheters for IV Antibiotics. Can J Health Technol. 2023;3(9):1-22. doi:10.51731/cjht.2023.738 PubMed
17.Gravdahl E, Haugen DF, Fredheim OM. Use of peripherally inserted central venous catheters and midline catheters for palliative care in patients with cancer: a systematic review. Support Care Cancer. 2024;32(7):464. doi:10.1007/s00520-024-08664-3 PubMed
18.Lai JY, Wu MJ, Gautama MSN, Huang TW. Comparison of complication rates between midline catheters and peripherally inserted central catheters: a systematic review and meta-analysis of randomized controlled trials. J Hosp Infect. 2024;151:131-139. doi:10.1016/j.jhin.2024.07.003 PubMed
19.Li X, Zhang H, Li H, Sun W. Comparison of complications and indwelling time in midline catheters versus central venous catheters: A systematic review and meta-analysis. Int J Nurs Pract. 2024;30(6):e13301. doi:10.1111/ijn.13301 PubMed
20.Wen J, Xiong S, Tu Z, et al. Which is the safer option for adult patients between peripherally inserted central catheters and midline catheters: a meta-analysis. Infect Control Hosp Epidemiol. 2024:1-8. doi:10.1017/ice.2024.190 PubMed
21.Urtecho M, Torres Roldan VD, Nayfeh T, et al. Comparing Complication Rates of Midline Catheter vs Peripherally Inserted Central Catheter. A Systematic Review and Meta-analysis. Open Forum Infect Dis. 2023;10(2):ofad024. doi:10.1093/ofid/ofad024 PubMed
22.Chen X, Liang M. A Meta-Analysis of Incidence of Catheter-Related Bloodstream Infection with Midline Catheters and Peripherally Inserted Central Catheters. J Healthc Eng. 2022;2022:6383777. doi:10.1155/2022/6383777 PubMed
23.Lu H, Yang Q, Tian B, Lyu Y, Zheng X, Xin X. A meta-analysis of the comparison of phlebitis between midline catheters and peripherally inserted central catheters in infusion therapy. Int J Nurs Pract. 2022;28(2):e12976. doi:10.1111/ijn.12976 PubMed
24.Lu H, Yang Q, Yang L, et al. The risk of venous thromboembolism associated with midline catheters compared with peripherally inserted central catheters: A systematic review and meta-analysis. Nurs Open. 2022;9(3):1873-1882. doi:10.1002/nop2.935 PubMed
25.Nickel B, Gorski L, Kleidon T, et al. Infusion Therapy Standards of Practice, 9th Edition. J Infus Nurs. 2024;47(1S Suppl 1):S1-s285. doi:10.1097/nan.0000000000000532
26.Pittiruti M, Crocoli A, Zanaboni C, et al. The pediatric DAV-expert algorithm: A GAVeCeLT/GAVePed consensus for the choice of the most appropriate venous access device in children. J Vasc Access. 2024:11297298241256999. doi:10.1177/11297298241256999 PubMed
27.World Health Organization. Guidelines for the prevention of bloodstream infections and other infections associated with the use of intravascular catheters. Part I: peripheral catheters. World Health Organization; 2024. Accessed January 23, 2025. https://www.who.int/publications/i/item/9789240093829
28.Massouh A, Kwan SW, Fidelman N, et al. ACR Appropriateness Criteria R Central Venous Access Device and Site Selection. J Am Coll Radiol. 2023;20(5S):S3-S19. doi:10.1016/j.jacr.2023.02.021 PubMed
29.Pittiruti M, Van Boxtel T, Scoppettuolo G, et al. European recommendations on the proper indication and use of peripheral venous access devices (the ERPIUP consensus): A WoCoVA project. J Vasc Access. 2023;24(1):165-182. doi:10.1177/11297298211023274 PubMed
30.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. doi:10.1136/bmj.n160 PubMed
31.Oliver S, Kavanagh J, Caird J, et al. Health Promotion, Inequalities and Young People's health: a Systematic Review of Research (EPPI-Centre report no. 161). EPPI-Centre, Social Science Research Unit, Institute of Education, University of London; 2008. Accessed January 23, 2025. https://eppi.ioe.ac.uk/cms/Portals/0/PDF%20reviews%20and%20summaries/Inequalities%20Young%20People%20R2008Oliver.pdf?ver=2010-12-22-123934-167
32.O'Neill J, Tabish H, Welch V, et al. Applying an equity lens to interventions: using PROGRESS ensures consideration of socially stratifying factors to illuminate inequities in health. J Clin Epidemiol. 2014;67(1):56-64. doi:10.1016/j.jclinepi.2013.08.005 PubMed
33.Nickel B. Does the Midline Peripheral Intravenous Catheter Have a Place in Critical Care? Crit Care Nurse. 2021;41(6):e1-e21. doi:10.4037/ccn2021818 PubMed
34.Montanarella MJ, Agarwal A, Moon B. Peripherally Inserted Central Catheter (PICC) Line Placement. StatPearls Publishing; 2025. Accessed January 23, 2025. https://www.ncbi.nlm.nih.gov/books/NBK573064/
35.Erskine B, Bradley P, Joseph T, Yeh S, Clements W. Comparing the accuracy and complications of peripherally inserted central catheter (PICC) placement using fluoroscopic and the blind pushing technique. J Med Radiat Sci. 2021;68(4):349-355. doi:10.1002/jmrs.533 PubMed
36.Mercieca-Bebber R, King MT, Calvert MJ, Stockler MR, Friedlander M. The importance of patient-reported outcomes in clinical trials and strategies for future optimization. Patient Relat Outcome Meas. 2018;9:353-367. doi:10.2147/prom.S156279 PubMed
37.Registered Nurses’ Association of Ontario (RNAO). Vascular access. 2nd ed. RNAO; 2021. Accessed January 23, 2025. https://rnao.ca/bpg/guidelines/Vascular_Access
38.Central venous access devices (CVAD): Clinical practice guide. NSW Agency for Clinical Innovation; 2021. Accessed January 23, 2025. https://aci.health.nsw.gov.au/__data/assets/pdf_file/0010/239626/ACI-CVAD-clinical-practice-guide.pdf
39.Zhang H, Li X, Sun W, Zhang R, Cai W. Comparison of complications and indwelling time of midline catheter at different tip locations: A systematic review and meta-analysis. J Vasc Access. 2024;25(6):1757-1766. doi:10.1177/11297298231199776 PubMed
40.Canada’s Drug Agency Style: A Guide for Authors and Editors. 8th ed. Canada’s Drug Agency; 2025. Accessed February 19, 2025. https://www.cda-amc.ca/sites/default/files/pdf/style_guide_2025_digital.pdf
41.Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. doi:10.1136/bmj.j4008 PubMed
42.The AGREE Next Steps Consortium. The AGREE II Instrument. AGREE Enterprise; 2017. Accessed January 23, 2025. https://www.agreetrust.org/wp-content/uploads/2017/12/AGREE-II-Users-Manual-and-23-item-Instrument-2009-Update-2017.pdf
Appendix 1: Detailed Methods and Selection of Included Studies
Please note that this appendix has not been copy-edited.
Literature Search Methods
An information specialist conducted a literature search on key resources including MEDLINE, the Cochrane Database of Systematic Reviews, the International HTA Database, the websites of health technology assessment agencies in Canada and major international health technology assessment agencies, as well as a focused internet search. The search approach was customized to retrieve a limited set of results, balancing comprehensiveness with relevance. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. Search concepts were developed based on the elements of the research questions and selection criteria. The main search concept was midline catheters. Search filters were applied to limit retrieval to health technology assessments, systematic reviews, meta-analyses, or indirect treatment comparisons. An additional search was also conducted with the search concept of venous catheters; for this search, search filters were applied to limit retrieval to guidelines. The searches were completed on January 13, 2025, and limited to English-language documents published since January 1, 2020.
Selection Criteria and Methods
Two reviewers screened citations and selected studies. In the first level of screening, they independently screened titles and abstracts of all retrieved citations for relevance following a liberal-accelerated approach, whereby a single reviewer was required to include a study and exclusion by both reviewers was needed to exclude a study. Full texts of titles and abstracts that were judged to be potentially relevant by at least 1 reviewer were retrieved and independently assessed by 2 reviewers for inclusion based on the inclusion criteria presented in Table 1. Discrepancies between reviewers at the full-text level were discussed until consensus was reached.
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1 or were duplicate publications. We excluded SRs in which all relevant studies were captured in other more recent or more comprehensive SRs. Guidelines with unclear methodology were also excluded.
Data Extraction
One reviewer extracted data directly into tables created in Microsoft Word, which were developed, piloted, and modified, as necessary. Two additional reviewers independently verified the study characteristics and outcomes data for accuracy and completeness. Disagreements were resolved through discussion.
Relevant information that was extracted included study characteristics, methodology (e.g., study design), population, intervention, comparator, and results regarding the outcomes of interest. When reporting on sex or gender in this Rapid Review, we retained the language used by the original study authors, and whenever possible, we referred to these groups based on guidance from Canada’s Drug Agency Style: A Guide for Authors and Editors40 at the time this Rapid Review was conducted, with an understanding that language is constantly evolving.
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the following tools as a guide: A Measurement Tool to Assess Systematic Reviews 2 (AMSTAR 2)41 for SRs and the Appraisal of Guidelines for Research and Evaluation (AGREE) II instrument42 for guidelines. A second reviewer verified the critical appraisal results for accuracy and consistency. Any disagreements were resolved through discussion. Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Appendix 2: Characteristics of Included Publications
Please note that this appendix has not been copy-edited.
Table 2: Characteristics of Included Systematic Reviews
Study citation, country, funding source | Study design, number of primary studies included | Population characteristicsa | Intervention and comparator(s) | Relevant clinical outcomes |
|---|---|---|---|---|
Gravdahl et al. (2024)17 Norway Funding source: The Akershus University Hospital and the South-Eastern Norway Regional Health Authority. | Study design: An SR of primary studies with experimental or quasi-experimental designs (e.g., clinical trials, cohort studies, case-control studies), case reports, cross-sectional studies, and literature reviews, with a literature search conducted up to December 23, 2022. Number of included studies: A total of 17 studies were included, of which, 2 were relevant to the current report (2 prospective case series). | Patients with cancer receiving IV palliative care interventions Age: NR Sex or gender: NR Other PROGRESS-Plus criteria: NRb | Relevant intervention: Any palliative care interventions (e.g., pain or other symptom treatment, transfusions, hydration, parenteral nutrition) administered using midline catheters. Relevant comparator: Any palliative care interventions administered using PICCs.c |
|
Lai et al. (2024)18 Taiwan Funding source: The authors reported that no financial support was received for the study. | Study design: SR and meta-analysis of RCTs published up to April 2024 Number of included studies: 5 RCTs | Patients of any age receiving IV therapies Age: The mean age of participants from included primary studies ranged from 6 years (SD = NR) to 72 years (SD = NR). Sex or gender: The proportion of male participants from included primary studies ranged from 31% to 63%; other sexes or genders were NR. BMI: The mean BMI of participants from included primary studies ranged from 26.3 kg/m2 (SD = 4.8) to 34.6 kg/m2 (SD = 11.7) (when reported). Other PROGRESS-Plus criteria: NRb | Intervention: Any IV therapies administered using midline catheters Comparator: Any IV therapies administered using PICCs.d |
|
Li et al. (2024)19 China Funding source: Plant Nursery Talent Project, The Beijing Tiantan Hospital, Capital Medical University | Study design: SR and meta-analysis of experimental and observational studies published up to May 2023 Number of included studies: 10 primary studies (primary study design was NR) | Adults who are not pregnant and are receiving IV therapies Age: The mean age of participants from included primary studies ranged from 40.3 years (SD = 6.4 years) to 65.0 years (SD = 16.0 years) (when reported).e Sex or gender: The proportion of male participants from included primary studies ranged from 40% to 68%; other sexes or genders were NR. Other PROGRESS-Plus criteria: NRb | Intervention: Any IV therapies administered using midline catheters. Comparator: Any IV therapies administered using central venous catheters. |
|
Wen et al. (2024)20 China Funding source: The Scientific and Technological Projects of Jiangxi Provincial Health Commission | Study design: SR and meta-analysis of RCTs and cohort studies. Databases were searched up to June 15, 2024. Number of included studies: 3 RCTs and 11 cohort studies | Adult patients who underwent catheter insertion for IV infusion therapy (without any contraindications for IV catheter insertion) Age: The mean age of participants from included primary studies ranged from 29 years (SD = NR) to 72 years (SD = NR). Sex or gender: The proportion of female participants from included primary studies ranged from 23.3% to 69.0%; the proportion of male participants from included primary studies ranged from 31.0% to 76.7% (when reported); other sexes or genders were NR. Other PROGRESS-Plus criteria: NRb | Intervention: Any IV therapies administered using midline catheters. Comparator: Any IV therapies administered using PICCs. |
|
Urtecho et al. (2023)21 US Funding source: The authors reported that no financial support was received for the study. | Study design: SR and meta-analysis of RCTs and comparative observational studies published up to June 24, 2022. Number of included studies: 1 RCT, 18 cohort studies, and 1 case series | Adult patients (≥ 18 years old) requiring venous access for > 24 hours Age: The mean age of participants from included primary studies ranged from 38 years (SD = 12.2 years) to 74 years (SD = 10.0 years) (when reported).e Sex or gender: The proportion of female participants from included primary studies ranged from 27% to 74%; other sexes or genders were NR. Race: Information on the race of primary study participants was available for 4 primary studies. Other PROGRESS-Plus criteria: NRb | Intervention: Venous access using midline catheters Comparator: Venous access using PICCs |
|
Chen and Liang (2022)22 China Funding source: NR | Study design: SR and meta-analysis of RCTs and observational studies. Databases were searched from inception to August 2022. Number of included studies: 2 RCTs and 9 cohort studies | Patients of any age receiving IV infusion therapy Age: The age of participants from included primary studies ranged from 1 year to 101 years (when reported). The mean or median ages were NR. Sex or gender: NR. Other PROGRESS-Plus criteria: NRb | Intervention: IV therapies administered using midline catheters. Comparator: IV therapies administered using PICCs. |
|
Lu et al. (2022a)23 China Funding source: Institutional Foundation of the First Affiliated Hospital of Xi’an Jiaotong University | Study design: A SR and meta-analysis of RCTs or observational studies published up to May 2020. Number of included studies: 4 RCTs and 3 cohort studies | Patients of any age receiving IV infusion therapy. Age: The age of participants from included primary studies ranged from 18 years to 95 years (when reported). The mean or median ages were NR. Sex or gender: NR Other PROGRESS-Plus criteria: NRb | Intervention: IV therapies administered using midline catheters. Comparator: IV therapies administered using PICCs. |
|
Lu et al. (2022b)24 China Funding source: The Fundamental Research Funds of the First Affiliated Hospital of Xi’an Jiao Tong University | Study design: An SR and meta-analysis of RCTs and observational studies. Databases were searched from inception to January 2020. Number of included studies: 2 RCTs and 10 cohort studies | Patients of any age receiving IV infusion therapy. Age: The age of participants from included primary studies ranged from 1 year to 101 years (when reported). The mean or median ages were NR. Sex or gender: NR Other PROGRESS-Plus criteria: NRb | Intervention: IV therapies administered using midline catheters. Comparator: IV therapies administered using PICCs. |
|
BMI = body mass index; NR = not reported; PICC = peripherally inserted central catheter; RCT = randomized controlled trial; SD = standard deviation; SR = systematic review.
aFor SRs with broader inclusion criteria than this report, participant characteristic data (e.g., age, sex) from the subset of studies relevant to the current report were summarized.
bThe main PROGRESS-Plus criteria include place of residence, race, ethnicity, culture, language, occupation, gender, sex, religion, education, socioeconomic status, social capital, personal characteristics associated with discrimination (e.g., age, disability), features of relationships, and time-dependent relationships.31,32
cThe scope of this SR was broader than that of this report and included additional interventions and comparators. Only the comparisons relevant to this report are included.
dThis SR included 1 primary study that used IV therapy administered using conventional catheters as the control group, which included peripheral venous catheters, central venous catheters, and PICCs.
eBased on the reporting in the SR, it was unclear whether the summary values for participant age in primary studies were reported as means, but they were assumed to be.
Table 3: Characteristics of Included Guidelines
Intended users, target population | Intervention(s) and practice considered | Major outcomes considered | Evidence collection, synthesis, and quality assessment | Recommendations development and evaluation | Guideline validation |
|---|---|---|---|---|---|
INS (2024)25 | |||||
Intended users: Infusion therapy clinicians in all care settings throughout the world. Target population: Patients undergoing infusion therapy for any indication. | Standards of practice were developed for the management of all patient infusion needs, including planning vascular access device and site selection, administering the patient’s therapeutic regimen, and monitoring and mitigating complications. | The primary outcome considered was patient safety. Other outcomes considered were clinical effectiveness, cost-effectiveness, acceptability, and efficiency. | The evidence informing this guideline was retrieved using comprehensive literature searches in multiple electronic databases for articles mainly in English, published between January 2017 and March 2023. Additional evidence was retrieved from the reference lists of relevant articles and through searching other sources of information (e.g., international health care-related agencies, manufacturers, and pharmaceutical organizations). Detailed study eligibility criteria (e.g., population, study design, outcomes) were NR. Studies considered relevant for informing standard statements and practice recommendations were classified by their study design and summarized. The methods for evaluating the quality of the evidence informing the recommendations were NR in detail but considered aspects such as sample size and threats to internal and external validity. | Standards and practice recommendations were drafted by committee members with subject-matter expertise, after reviewing the relevant evidence. All written content was reviewed weekly during virtual committee meetings to ensure all statements and verbiage had committee consensus. The details for achieving committee consensus were NR. Each referenced item cited in the Standards was assigned a level of evidence ranging from the highest level I (e.g., based on a meta-analysis) to the lowest level of V (e.g., based on case reports). | The first draft was externally reviewed by 144 interdisciplinary experts. The committee revised the draft to incorporate their feedback during a 6-week period with weekly virtual meetings. Once the second draft was completed, a final committee consensus was achieved for all standards. |
Pittiruti et al. (2024)26 | |||||
Intended Users: Health care professionals (e.g., physicians, nurses) who are involved in selecting venous access devices in pediatric patients. Target Population: Children who are hospitalized and who are not hospitalized and who require venous access during emergencies and elective conditions. | Venous access devices for children, including short peripheral catheters, long peripheral catheters, midline catheters, PICCs, centrally inserted central catheters, femorally inserted central catheters, and totally implanted venous access devices. | Not explicitly reported, though the included evidence-based recommendations are focused on measures of patient safety. | A systematic literature search was conducted in multiple databases to retrieve any relevant RCTs and observational studies on pediatric venous access published in English between January 2000 and April 2023. The references of articles, previous reviews, and meta-analyses were also reviewed for additional potentially relevant papers. The methods for selecting articles for consideration by the guideline panel were NR (e.g., detailed inclusion and exclusion criteria). The quality of articles deemed relevant for informing the panel’s recommendations was not assessed. | Recommendations were developed using the RAND-UCLA Appropriateness Method, which is a modification of the Delphi method. After reviewing the literature obtained from the systematic search, 3 coordinators drafted preliminary statements addressing 10 key questions regarding the choice of venous access devices. | Draft recommendation statements were shared with 17 panellists and 3 promoters, who rated their level of agreement with each statement and provided feedback. Live meetings were held to discuss opinions and revise the statements based on the panel’s suggestions. Following these discussions, the revised statements were distributed to panellists for a final vote. All statements that received agreement from at least 70% of the voting members were included in the final recommendations. |
WHO (2024)27 | |||||
Intended users: Health care practitioners (e.g., doctors, nurses, infection prevention and control professionals) involved in the management of patients who require PIVCs, hospital administrators, other professionals involved in health care, and patients. Target population: Adults and children in any type of care setting, including acute and long-term health care facilities and primary care settings. | The insertion, maintenance, access, and removal of intravascular catheters (e.g., peripheral IV catheters, PICCs, peripheral arterial catheters). | The primary outcome considered all-cause bloodstream infections and other infections associated or related to peripheral IV catheters. | A systematic literature search was conducted in several databases to retrieve relevant studies (e.g., RCTs, non-RCTs, controlled observational studies, controlled before-after studies, interrupted time series and repeated measures studies, before-and-after studies) published from January 1, 1980, to March 16, 2023. There were no restrictions for geographical areas, settings or publication language. The reference lists of selected SRs were also reviewed for additional potentially relevant citations. Qualitative syntheses were performed to summarize the results of relevant studies. When the data were sufficient, meta-analyses were performed to quantitatively synthesis the evidence for critical outcomes. The risk of bias of included primary studies was assessed using the Cochrane RoB 2 tool for RCTs, ROBINS-I for nonrandomized studies, and the EHHP tool for before-and-after studies. The overall certainty of the evidence for selected outcomes was assessed using the methods of the GRADE Working Group. | The recommendations were developed using the process described in the WHO Handbook for guideline development. A WHO Guideline Steering Group and a Guideline Development Group (21 external experts) were established to identify the primary critical outcomes, priority topics, and a series of questions to be addressed. Following a review of existing guidelines on the topic, SRs were performed to retrieve, assess, and synthesize the available evidence. The Guideline Development group then developed recommendations and assigned a strength to each recommendation using the GRADE approach. The development process included members of the WHO Guideline Steering Group, Guideline Development Group, and Systematic Reviews Expert Group (7 technical experts) who participated in the discussions. | An External Peer Review Group composed of 7 technical experts with relevant knowledge and experience reviewed the final guideline document, to identify inaccuracies or errors and provided comments on technical content and evidence, clarity of language, contextual issues and implications for implementation. All members of the External Peer Review Group agreed with each of the final recommendations. |
ACR (2023)28 | |||||
Intended users: Radiologists, radiation oncologists and referring physicians. Target population: Patients who require central venous access in various clinical settings (both inpatient and outpatient). | Central venous access device and site selection. Devices included non-tunneled central venous catheters, PICCs, midline catheters, tunneled central venous catheters, and arm and chest ports. | Not explicitly reported, though the included evidence is focused on measures of patient safety. | A systematic literature search was conducted on Ovid MEDLINE to retrieve any relevant articles published in English between January 1, 2017, and July 7, 2021. The methods for evidence selection and synthesis were NR (e.g., detailed inclusion and exclusion criteria). The quality of studies used to inform recommendations was assessed using a 5-category scale that is described in limited detail. | Recommendations were developed by the Expert Panel on Interventional Radiology following a review of the relevant literature. Nine clinical scenarios (referred to as variants) were drafted and a list of procedures that could be applied in each scenario were compiled. Details of the methods used to develop the clinical scenarios and potentially appropriate procedures were NR. | After each clinical scenario and a list of potential procedures were identified, the expert panel voted on each using a rating scale (range, 1 to 9). Final votes were tallied and were used to designate each procedure as usually appropriate, may be appropriate, or usually not appropriate for each clinical scenario. |
Pittiruti et al. (2023)29 | |||||
Intended users: Health care professionals who provide care for adults with peripheral venous access devices. Target population: Adults who require peripheral venous access. | The selection, insertion, maintenance, and removal of peripheral venous access devices, including short peripheral cannulas, long peripheral cannulas, and midline catheters. | Patient safety, clinical efficacy, and cost-effectiveness | The authors conducted a literature search to retrieve retrospective and prospective clinical studies, reviews, guidelines, and evidence-based documents on peripheral venous access devices published in English between January 2013 and January 2021. The methods for selecting articles for consideration by the guideline panel were NR (e.g., detailed inclusion and exclusion criteria). The quality of articles deemed relevant for informing the panel’s recommendations was not assessed. | Eleven panellists were divided into working groups that were each assigned a topic. Each working group developed a preliminary report on their topic with a discussion of the literature and a series of statements answering specific research questions that were previously developed by the whole panel. | The preliminary reports were merged into a single document and reviewed by all members of the panel. The statements were adjusted following feedback from the panel, and a vote was held to achieve consensus on the final recommendations. The methods for achieving consensus and consensus thresholds were NR. |
ACR = American College of Radiology; EHHP = Effective Public Health Practice Project; GRADE = Grading of Recommendations Assessment, Development and Evaluation; INS = Infusion Nurses Society; NR = not reported; PICC = peripherally inserted central catheter; PIVC = peripheral IV catheter; RAND = Research and Development; RCT = randomized controlled trial; RoB = Risk of Bias; ROBINS-I = Risk Of Bias In Nonrandomized Studies of Interventions; SR = systematic review; UCLA = University of California Los Angeles.
Appendix 3: Critical Appraisal of Included Publications
Please note that this appendix has not been copy-edited.
Table 4: Strengths and Limitations of Systematic Reviews Using AMSTAR 241
Strengths | Limitations |
|---|---|
Gravdahl et al. (2024)17 | |
|
|
Lai et al. (2024)18 | |
|
|
Li et al. (2024)19 | |
|
|
Wen et al. (2024)20 | |
|
|
Urtecho et al. (2023)21 | |
|
|
Chen and Liang (2022)22 | |
|
|
Lu et al. (2022a)23 | |
|
|
Lu et al. (2022b)24 | |
|
|
AMSTAR 2 = A Measurement Tool to Assess Systematic Reviews 2; GRADE = Grading of Recommendations Assessment, Development and Evaluation; PROSPERO = International Prospective Register of Systematic Reviews; RCT = randomized controlled trial; RoB = Risk of Bias.
Table 5: Strengths and Limitations of Guidelines Using AGREE II42
Item | INS (2024)25 | Pittiruti et al. (2024)26 | WHO (2024)27 | ACR (2023)28 | Pittiruti et al. (2023)29 |
|---|---|---|---|---|---|
Domain 1: scope and purpose | |||||
1. The overall objective(s) of the guideline is (are) specifically described. | Yes | Yes | Yes | Yes | Yes |
2. The health question(s) covered by the guideline is (are) specifically described. | Yes | Yes | Yes | Yes | Yes |
3.The population (patients, public, and so forth) to whom the guideline is meant to apply is specifically described. | Yes | Yes | Yes | Yes | Yes |
Domain 2: stakeholder involvementa | |||||
4. The guideline development group includes individuals from all relevant professional groups. | Yes | Yes | Yes | Yes | Yes |
5. The views and preferences of the target population (patients, public, and so forth) have been sought. | No | No | Yes | No | No |
6. The target users of the guideline are clearly defined. | Yes | Yes | Yes | No | Yes |
Domain 3: rigour of development | |||||
7. Systematic methods were used to search for evidence. | Yes | Yes | Yes | Yes | Yes |
8. The criteria for selecting the evidence are clearly described. | No | No | Yes | No | No |
9. The strengths and limitations of the body of evidence are clearly described. | No | No | Yes | No | No |
10. The methods for formulating the recommendations are clearly described. | No | Yes | Yes | No | Partially |
11. The health benefits, side effects, and risks have been considered in formulating the recommendations. | Yes | Yes | Yes | Yes | Yes |
12. There is an explicit link between the recommendations and the supporting evidence. | Yes | Yes | Yes | Yes | Yes |
13. The guideline has been externally reviewed by experts before its publication. | Yes | No | Yes | No | No |
14. A procedure for updating the guideline is provided. | Yes | No | Yes | No | No |
Domain 4: clarity of presentation | |||||
15. The recommendations are specific and unambiguous. | Yes | Yes | Yes | Yes | Yes |
16. The different options for management of the condition or health issue are clearly presented. | Yes | Yes | Yes | Yes | Yes |
17. Key recommendations are easily identifiable. | Yes | Yes | Yes | Yes | Yes |
Domain 5: applicability | |||||
18. The guideline describes facilitators and barriers to its application. | Yes | No | Partially | No | No |
19. The guideline provides advice and/or tools on how the recommendations can be put into practice. | Yes | Yes | Yes | Yes | Yes |
20. The potential resource implications of applying the recommendations have been considered. | Yes | Yes | Yes | Unclear | Yes |
21. The guideline presents monitoring and/or auditing criteria. | No | No | Yes | No | No |
Domain 6: editorial independence | |||||
22. The views of the funding body have not influenced the content of the guideline. | Unclear | Yes | Unclear | Unclear | Yes |
23. Competing interests of guideline development group members have been recorded and addressed. | Yes | Yes | Yes | Yes | Yes |
ACR = American College of Radiology; AGREE II = Appraisal of Guidelines for Research and Evaluation II.
aWe retained the domain names that are included in the original AGREE II checklist, which includes the terminology stakeholder (i.e., domain 2), to be clear that we assessed the strengths and limitations of guidelines using AGREE II.42 However, Canada’s Drug Agency understands that language is constantly evolving and the word stakeholder has association with colonialism; whenever possible, Canada’s Drug Agency does not use this word in our reports
Appendix 4: Main Study Findings
Please note that this appendix has not been copy-edited.
Table 6: Summary of Findings by Outcome — Total Complicationsa
Citation | Evidence source, sample size | Outcome | Outcome result | Effect estimate (95% CI) | P value | |
|---|---|---|---|---|---|---|
Midline catheter group | Control group | |||||
Midline catheter vs. PICC | ||||||
Lai et al. (2024)18 | SR with MA (4 studies); 488 participants (all ages) | Number of total complications, n/N | 46/244 | 23/244b | RR = 1.95 (1.23 to 3.08) | 0.005 |
SR with MA (3 studies); 382 adults | Number of total complications, n/N | 28/193 | 15/189b | RR = 1.70 (0.94 to 3.05) | 0.08 | |
SR with MA (1 study); 106 children | Number of total complications, n/N | 18/51 | 8/55 | RR = 2.43 (1.16 to 5.09) | 0.02 | |
Wen et al. (2024)20 | SR with MA (14 studies); 20,675 adults | Number of total complications, n/N | 1,221/9,841 | 1,753/10,834 | RR = 1.00 (0.71 to 1.43)c | 0.99 |
SR with MA (9 studies); 280,606 catheter days | Number of total complications, expressed as the number of events per total catheter days, n/N | 394/59,123 | 749/221,483 | RR = 1.96 (1.01 to 3.85)c | 0.05 | |
Midline catheter vs. central venous catheter | ||||||
Li et al. (2024)19 | SR with MA (10 studies); 1,722 adults | Number of total complications, n/N | 79/983 | 124/739 | OR = 0.36 (0.18 to 0.70) | 0.003 |
CI = confidence interval; DVT = deep vein thrombosis; MA = meta-analysis; NA = not applicable; NR = not reported; OR = odds ratio; PICC = peripherally inserted central catheter; RR = risk ratio; SD = standard deviation; SR = systematic review; SVT = superficial vein thrombosis; vs. = versus.
aThe specific types of complications included in this composite outcome were not explicitly defined in the included SRs18-20 and may vary across studies.
bOne primary study included in this analysis (Nielson et al. [2021]) used a conventional IV catheter control group, which included peripheral venous catheters, central venous catheters, and PICCs.
cThe findings from Wen et al.20 were calculated using PICC as the intervention compared to midline catheters. To align with the direction of this review (i.e., midline catheters compared to PICC) the effect estimates were inverted by taking the reciprocal of the risk ratio and the bounds of the confidence interval. The findings as reported in the SR were: number of total complications, RR = 1.00 (95% CI, 0.70 to 1.41); number of total complications, expressed as the number of events per total catheter days, RR = 0.51 (95% CI, 0.26 to 0.99).
Note: There was overlap in the primary studies that were included in the SRs; the pooled estimates from separate reviews presented in this table thus contain some of the same data. Refer to Appendix 5 for a citation matrix illustrating the degree of overlap.
Table 7: Summary of Findings by Outcome — Thrombosis
Citation | Evidence source, sample size | Outcome | Outcome result | Effect estimate (95% CI) | P value | |
|---|---|---|---|---|---|---|
Midline catheter group | Control group | |||||
Midline catheter vs. PICC | ||||||
Lai et al. (2024)18 | SR with MA (5 studies); 608 participants (all ages) | Participants with thrombosis, n (%) | 2 (0.66%) | 3 (0.99%)a | RR = 0.85 (0.18 to 4.07) | 0.84 |
SR with MA (4 studies); 502 adults | Participants with thrombosis, n (%) | 1 (0.40%) | 3 (1.2%)a | RR = 0.56 (0.09 to 3.36) | 0.53 | |
SR with MA (1 study); 106 children | Participants with thrombosis, n (%) | 1 (2.0%) | 0 (0%) | RR = 3.23 (0.13 to 77.56) | 0.47 | |
Wen et al. (2024)20 | SR with MA (14 studies); 20,675 adults | Participants with catheter-related DVT or SVT, n (%) | 313 (3.18%) | 349 (3.22%) | RR = 0.94 (0.62 to 1.45)b | 0.80 |
SR with MA (11 studies); 18,672 adults | Participants with catheter-related DVT, n (%) | 239 (2.69%) | 290 (2.96%) | RR = 0.92 (0.60 to 1.41)b | 0.69 | |
SR with MA (3 studies); 2,946 adults | Participants with catheter-related SVT, n (%) | 58 (4.70%) | 34 (1.98%) | RR = 2.38 (1.56 to 3.57)b | < 0.0001 | |
SR with MA (1 study); 2,577 adults | Participants with contralateral DVT or SVT, n (%) | 29 (2.65%) | 33 (2.23%) | RR = 1.19 (0.73 to 1.96)b | 0.49 | |
SR with MA (1 study); 2,577 adults | Participants with contralateral DVT, n (%) | 13 (1.19%) | 15 (1.01%) | RR = 1.18 (0.56 to 2.44)b | 0.67 | |
SR with MA (1 study); 2,577 adults | Participants with contralateral SVT, n (%) | 16 (1.46%) | 18 (1.21%) | RR = 1.20 (0.62 to 2.33)b | 0.58 | |
SR with MA (1 study); 2,577 adults | Participants with contralateral and/or bilateral DVT or SVT, n (%) | 60 (5.48%) | 62 (4.18%) | RR = 1.32 (0.93 to 1.85)b | 0.12 | |
SR with MA (1 study); 2,577 adults | Participants with contralateral and/or bilateral DVT, n (%) | 25 (2.29%) | 25 (1.69%) | RR = 1.35 (0.78 to 2.33)b | 0.28 | |
SR with MA (1 study); 2,577 adults | Participants with contralateral and/or bilateral SVT, n (%) | 44 (4.02%) | 42 (2.83%) | RR = 1.43 (0.93 to 2.17)b | 0.10 | |
SR with MA (3 studies); 13,755 adults | Participants with pulmonary embolism, n (%) | 27 (0.43%) | 40 (0.54%) | RR = 0.87 (0.54 to 1.41)b | 0.58 | |
SR with MA (9 studies); 280,606 catheter days | Number of catheter-related DVTs or SVTs, expressed as the number of events per total catheter days, n/N | 104/59,123 | 120/221,483 | RR = 2.44 (1.05 to 5.56)b | 0.04 | |
SR with MA (6 studies); 140,232 catheter days | Number of catheter-related DVTs, expressed as the number of events per total catheter days, n/N | 89/40,184 | 95/100,048 | RR = 2.50 (0.71 to 9.09)b | 0.15 | |
SR with MA (1 study); 111,242 catheter days | Number of pulmonary embolisms, expressed as the number of events per total catheter days, n/N | 8/30,630 | 14/80,612 | RR = 1.52 (0.63 to 3.57)b | 0.36 | |
Urtecho et al. (2023)21 | SR with MA (6 studies); 48,177 catheters | Catheters with localized thrombosis (i.e., SVT, DVT, other thrombosis), n (%) | 289 (2.2%) | 622 (1.8%) | OR = 1.05 (0.69 to 1.57) | NR |
SR with MA (9 studies); 14,555 adults | Participants with localized thrombosis (i.e., SVT, DVT, other thrombosis), n (%) | 227 (3.3%) | 207 (2.7%) | OR = 1.31 (0.74 to 2.30) | NR | |
SR with MA (2 studies); 2,892 catheters | Catheters with SVT, n (%) | 54 (4.5%) | 33 (2.0%) | OR = 2.30 (1.48 to 3.57) | NR | |
SR with MA (7 studies); 19,153 catheters | Catheters with DVT, n (%) | 227 (2.6%) | 279 (2.7%) | OR = 0.99 (0.70 to 1.41) | NR | |
SR with MA (2 studies); 13,440 adults | Participants with pulmonary embolism, n (%) | 26 (0.4%) | 38 (0.5%) | OR = 0.87 (0.53 to 1.44)c | NR | |
SR with MA (2 studies); 12,464 catheters | Catheters with pulmonary embolism, n (%) | 11 (0.2%) | 16 (0.2%) | OR = 0.80 (0.37 to 1.72) | NR | |
Lu et al. (2022b)24 | SR with MA (12 studies); 40,871 participants (all ages) | Participants with venous thromboembolism, n (%) | 310 (3.97%) | 758 (2.29%) | RR = 1.53 (1.33 to 1.76) | < 0.00001 |
SR with MA (5 studies); 3,772 adults | Participants with venous thromboembolism, n (%) | 149 (8.42%) | 110 (5.49%) | RR = 1.75 (1.38 to 2.22) | < 0.00001 | |
SR with MA (7 studies); 37,099 participants (children, mixed age groups, and studies that did not report age) | Participants with venous thromboembolism, n (%) | 161 (2.67%) | 648 (2.09%) | RR = 1.42 (1.19 to 1.69) | 0.0001 | |
Midline catheter vs. central venous catheter | ||||||
Li et al. (2024)19 | SR with MA (8 studies); 1,602 adults | Participants with catheter-related thrombosis, n (%) | 4 (0.43%) | 15 (2.21%) | OR = 0.28 (0.11 to 0.71) | 0.007 |
CI = confidence interval; DVT = deep vein thrombosis; MA = meta-analysis; NR = not reported; OR = odds ratio; PICC = peripherally inserted central catheter; RCT = randomized controlled trial; RR = risk ratio; SR = systematic review; SVT = superficial vein thrombosis; vs. = versus.
aOne primary study included in this analysis (Nielson et al. [2021]) used a conventional IV catheter control group, which included peripheral venous catheters, central venous catheters, and PICCs.
bThe findings from Wen et al.20 were calculated using PICC as the intervention compared to midline catheters. To align with the direction of this review (i.e., midline catheters compared to PICC) the effect estimates were inverted by taking the reciprocal of the risk ratio and the bounds of the confidence interval. The findings as reported in the SR were: participants with catheter-related DVT or SVT, RR = 1.06 (95% CI, 0.69 to 1.61); participants with catheter-related DVT, RR = 1.09 (95% CI, 0.71 to 1.68); participants with catheter-related SVT, RR = 0.42 (95% CI, 0.28 to 0.64); participants with contralateral DVT or SVT, RR = 0.84 (95% CI, 0.51 to 1.37); participants with contralateral DVT, RR = 0.85 (95% CI, 0.41 to 1.78); participants with contralateral SVT, RR = 0.83 (95% CI, 0.43 to 1.62); participants with contralateral and/or bilateral DVT or SVT, RR = 0.76 (95% CI, 0.54 to 1.08); participants with contralateral and/or bilateral DVT, RR = 0.74 (95% CI, 0.43 to 1.28); participants with contralateral and/or bilateral SVT, RR = 0.70 (95% CI, 0.46 to 1.07); participants with pulmonary embolism, RR = 1.15 (95% CI, 0.71 to 1.86); incidence of catheter-related DVT or SVT, expressed as the number of events per catheter day, RR = 0.41 (95% CI, 0.18 to 0.95); incidence of catheter-related DVT, expressed as the number of events per catheter day, RR = 0.40 (95% CI, 0.11 to 1.41); incidence of pulmonary embolism, expressed as the number of events per catheter day, RR = 0.66 (95% CI, 0.28 to 1.58).
cThis value was reported as OR = 0.87 (95% CI, 0.53 to 31.44) in the main text of the SR by Urtecho et al.,21 but as OR = 0.87 (95% CI, 0.53 to 1.44) in the supplementary materials.
Note: There was overlap in the primary studies that were included in the SRs; the pooled estimates from separate reviews presented in this table thus contain some of the same data. Refer to Appendix 5 for a citation matrix illustrating the degree of overlap.
Table 8: Summary of Findings by Outcome — Infection
Citation | Evidence source, sample size | Outcome | Outcome result | Effect estimate (95% CI) | P value | |
|---|---|---|---|---|---|---|
Midline catheter group | Control group | |||||
Midline catheter vs. PICC | ||||||
Lai et al. (2024)18 | SR with MA (5 studies); 608 participants (all ages) | Number of catheter-related bloodstream infections, n/N | 3/304 | 3/304a | RR = 0.77 (0.16 to 3.74) | 0.74 |
SR with MA (4 studies); 502 adults | Number of catheter-related bloodstream infections, n/N | 3/253 | 2/249a | RR = 0.95 (0.11 to 7.82) | 0.96 | |
SR with MA (1 study); 106 children | Number of catheter-related bloodstream infections, n/N | 0/51 | 1/55 | RR = 0.36 (0.01 to 8.62) | 0.53 | |
Wen et al. (2024)20 | SR with MA (10 studies); 17,431 adults | Participants with catheter-related bloodstream infection, n (%) | 591 (7.04%) | 840 (9.30%) | RR = 0.51 (0.30 to 0.87)b | 0.01 |
SR with MA (7 studies); 273,937 catheter days | Catheters with an associated bloodstream infection, expressed as the number of events per total catheter days, n/N (%) | 29/53,953 (0.05%) | 113/219,984 (0.05%) | RR = 1.12 (0.43 to 2.86) | 0.82 | |
Urtecho et al. (2023)21 | SR with MA (9 studies); 12,478 adults | Participants with catheter-related bloodstream infection, n (%) | 20 (0.3%) | 103 (1.6%) | OR = 0.24 (0.15 to 0.38) | NR |
SR with MA (9 studies); 49,426 catheters | Catheters with an associated bloodstream infection, n (%) | 649 (4.6%) | 1,204 (3.4%) | OR = 0.70 (0.39 to 1.27) | NR | |
Chen and Liang (2022)22 | SR with MA (11 studies); 33,809 participants (all ages) | Participants with catheter-related bloodstream infection, n (%) | 43 (0.60%) | 133 (0.50%) | OR = 0.72 (0.48 to 1.08) | 0.11 |
SR with MA (10 studies); 33,779 participants (all ages) (studies of moderate or good quality) | Participants with catheter-related bloodstream infection, n (%) | 36 (0.50%) | 131 (0.49%) | OR = 0.60 (0.39 to 0.93) | 0.02 | |
SR with MA (6 studies); 2,373 adults | Participants with catheter-related bloodstream infection, n (%) | 20 (1.25%) | 13 (1.69%) | OR = 0.64 (0.27 to 1.49) | 0.30 | |
SR with MA (5 studies); 31,436 participants (children, mixed age groups, and studies that did not report age) | Participants with catheter-related bloodstream infection, n (%) | 23 (0.41%) | 120 (0.46%) | OR = 1.52 (0.26 to 8.92) | 0.64 | |
Midline catheter vs. central venous catheter | ||||||
Li et al. (2024)19 | SR with MA (8 studies); 1,462 adults | Participants with catheter-related infection, n (%) | 7 (0.82%) | 18 (2.96%) | OR = 0.36 (0.16 to 0.78) | 0.007 |
CI = confidence interval; MA = meta-analysis; OR = odds ratio; PICC = peripherally inserted central catheter; RR = risk ratio; SR = systematic review; vs. = versus.
aOne primary study included in this analysis (Nielson et al. [2021]) used a conventional IV catheter control group, which included peripheral venous catheters, central venous catheters, and PICCs.
bThe findings from Wen et al.20 were calculated using PICC as the intervention compared to midline catheters. To align with the direction of this review (i.e., midline catheters compared to PICC) the effect estimates were inverted by taking the reciprocal of the risk ratio and the bounds of the confidence interval. The findings as reported in the SR were: participants with catheter-related bloodstream infection, RR = 1.95 (95% CI, 1.15 to 3.32); catheters with an associated bloodstream infection, expressed as the number of events per total catheter days, RR = 0.89 (95% CI, 0.35 to 2.31).
Note: There was overlap in the primary studies that were included in the SRs; the pooled estimates from separate reviews presented in this table thus contain some of the same data. Refer to Appendix 5 for a citation matrix illustrating the degree of overlap.
Table 9: Summary of Findings by Outcome — Phlebitis
Citation | Evidence source, sample size | Outcome | Outcome result | Effect estimate (95% CI) | P value | |
|---|---|---|---|---|---|---|
Midline catheter group | Control group | |||||
Midline catheter vs. PICC | ||||||
Wen et al. (2024)20 | SR with MA (5 studies); 1,530 adults | Participants with phlebitis, n (%) | 9 (1.04%) | 9 (1.35%) | RR = 0.82 (0.34 to 1.96)a | 0.66 |
SR with MA (4 studies); 13,761 catheter days | Number of phlebitis complications, expressed as the number of events per total catheter days, n/N | 4/8,359 | 6/5,402 | RR = 0.55 (0.15 to 2.00) | 0.36 | |
Urtecho et al. (2023)21 | SR with MA (5 studies); 659 adults | Participants with phlebitis, n (%) | 13 (3.3%) | 11 (4.2%) | OR = 0.91 (0.39 to 2.15) | NR |
SR with MA (1 study); 406 catheters | Catheters with phlebitis, n (%) | 5 (2.5%) | 3 (1.5%) | OR = 1.74 (0.41 to 7.36) | NR | |
Lu et al. (2022a)23 | SR with MA (7 studies); 1,377 participants (unspecified age) | Participants with phlebitis, n (%) | 12 (1.52%) | 20 (3.41%) | RR = 0.53 (0.27 to 1.07) | 0.08 |
Midline catheter vs. central venous catheter | ||||||
Li et al. (2024)19 | SR with MA (8 studies); 1,353 adults | Participants with phlebitis, n (%) | 20 (2.65%) | 10 (1.67%) | OR = 1.60 (0.74 to 3.48) | 0.23 |
CI = confidence interval; MA = meta-analysis; OR = odds ratio; PICC = peripherally inserted central catheter; RR = risk ratio; SR = systematic review; vs. = versus.
aThe findings from Wen et al.20 were calculated using PICC as the intervention compared to midline catheters. To align with the direction of this review (i.e., midline catheters compared to PICC) the effect estimates were inverted by taking the reciprocal of the risk ratio and the bounds of the confidence interval. The findings as reported in the SR were: participants with phlebitis, RR = 1.22 (95% CI, 0.51 to 2.92); number of phlebitis complications, expressed as the number of events per total catheter days, RR = 1.82 (95% CI, 0.50 to 6.56).
Note: There was overlap in the primary studies that were included in the SRs; the pooled estimates from separate reviews presented in this table thus contain some of the same data. Refer to Appendix 5 for a citation matrix illustrating the degree of overlap.
Table 10: Summary of Findings by Outcome — Catheter Occlusion
Citation | Evidence source, sample size | Outcome | Outcome result | Effect estimate (95% CI) | P value | |
|---|---|---|---|---|---|---|
Midline catheter group | Control group | |||||
Midline catheter vs. PICC | ||||||
Wen et al. (2024)20 | SR with MA (7 studies); 13,827 adults | Participants with catheter occlusion, n (%) | 128 (1.94%) | 436 (6.03%) | RR = 0.59 (0.28 to 1.23)a | 0.16 |
SR with MA (7 studies); 280,027 catheter days | Number of catheters with occlusion, expressed as the number of events per total catheter days, n/N (%) | 128/58,861 (0.22%) | 436/221,166 (0.20%) | RR = 1.72 (0.69 to 4.35)a | 0.24 | |
Urtecho et al. (2023)21 | SR with MA (5 studies); 11,515 adults | Participants with catheter occlusion, n (%) | 115 (2.1%) | 413 (6.9%) | OR = 0.46 (0.18 to 1.18) | NR |
SR with MA (4 studies); 43,220 catheters | Catheters with occlusion, n (%) | 149 (1.3%) | 484 (1.5%) | OR = 2.28 (0.19 to 27.58) | NR | |
Midline catheter vs. central venous catheter | ||||||
Li et al. (2024)19 | SR with MA (6 studies); 706 adults | Participants with catheter blockage, n (%) | 10 (2.48%) | 22 (7.28%) | OR = 0.21 (0.09 to 0.51) | 0.0005 |
CI = confidence interval; MA = meta-analysis; OR = odds ratio; PICC = peripherally inserted central catheter; RR = risk ratio; SR = systematic review; vs. = versus.
aThe findings from Wen et al.20 were calculated using PICC as the intervention compared to midline catheters. To align with the direction of this review (i.e., midline catheters compared to PICC) the effect estimates were inverted by taking the reciprocal of the risk ratio and the bounds of the confidence interval. The findings as reported in the SR were: participants with catheter occlusion, RR = 1.69 (95% CI, 0.81 to 3.53); number of catheters with occlusion, expressed as the number of events per total catheter days, RR = 0.58 (95% CI, 0.23 to 1.44).
Note: There was overlap in the primary studies that were included in the SRs; the pooled estimates from separate reviews presented in this table thus contain some of the same data. Refer to Appendix 5 for a citation matrix illustrating the degree of overlap.
Table 11: Summary of Findings by Outcome — Leakage
Citation | Evidence source, sample size | Outcome | Outcome result | Effect estimate (95% CI) | P value | |
|---|---|---|---|---|---|---|
Midline catheter group | Control group | |||||
Midline catheter vs. PICC | ||||||
Wen et al. (2024)20 | SR with MA (5 studies); 1,143 adults | Participants with leakage, n (%) | 28 (4.42%) | 2 (0.39%) | RR = 6.25 (1.89 to 20.00)a | 0.003 |
SR with MA (4 studies); 13,427 catheter days | Number of catheters with leakage, expressed as the number of events per total catheter days, n/N (%) | 26/7,905 (0.33%) | 2/5,522 (0.04%) | RR = 5.88 (1.56 to 20.00)a | 0.009 | |
Midline catheter vs. central venous access | ||||||
Li et al. (2024)19 | SR with MA (7 studies); 886 adults | Participants with leakage, n (%) | 11 (2.20%) | 15 (3.89%) | OR = 0.50 (0.22 to 1.12)b | 0.09 |
CI = confidence interval; MA = meta-analysis; OR = odds ratio; PICC = peripherally inserted central catheter; SR = systematic review; vs. = versus.
aThe findings from Wen et al.20 were calculated using PICC as the intervention compared to midline catheters. To align with the direction of this review (i.e., midline catheters compared to PICC) the effect estimates were inverted by taking the reciprocal of the risk ratio and the bounds of the confidence interval. The findings as reported in the SR were: participants with leakage, RR = 0.16 (95% CI, 0.05 to 0.53); number of catheters with leakage, expressed as the number of events per total catheter days, RR = 0.17 (95% CI, 0.05 to 0.64).
bThis value was reported as OR = 0.50 (95% CI, 0.22 to 0.12) in the main text of the SR by Li et al.,19 but as OR = 0.50 (95% CI, 0.22 to 1.12) in the associated figure.
Table 12: Summary of Findings by Outcome — Catheter Displacement
Citation | Evidence source, sample size | Outcome | Outcome result | Effect estimate (95% CI) | P value | |
|---|---|---|---|---|---|---|
Midline catheter group | Control group | |||||
Midline catheter vs. PICC | ||||||
Wen et al. (2024)20 | SR with MA (6 studies); 1,602 adults | Participants with catheter displacement, n (%) | 22 (2.44%) | 15 (2.15%) | RR = 1.19 (0.63 to 2.22)a | 0.60 |
SR with MA (6 studies); 33,357 catheter days | Number of catheters with displacement, expressed as the number of events per total catheter days, n/N (%) | 22/11,334 (0.19%) | 15/22,023 (0.07%) | RR = 1.92 (0.53 to 7.14)a | 0.32 | |
Midline catheter vs. central venous access | ||||||
Li et al. (2024)19 | SR with MA (3 studies); 391 adults | Participants with catheter displacement, n (%) | 8 (3.35%) | 3 (1.97%) | OR = 0.73 (0.19 to 2.84) | 0.65 |
CI = confidence interval; OR = odds ratio; MA = meta-analysis; PICC = peripherally inserted central catheter; SR = systematic review; vs. = versus.
aThe findings from Wen et al.20 were calculated using PICC as the intervention compared to midline catheters. To align with the direction of this review (i.e., midline catheters compared to PICC) the effect estimates were inverted by taking the reciprocal of the risk ratio and the bounds of the confidence interval. The findings as reported in the SR were: participants with catheter displacement, RR = 0.84 (95% CI, 0.45 to 1.58); number of catheters with displacement, expressed as the number of events per total catheter days, RR = 0.52 (95% CI, 0.14 to 1.89).
Table 13: Summary of Findings by Outcome — Infiltration
Citation | Evidence source, sample size | Outcome | Outcome result | Effect estimate (95% CI) | P value | |
|---|---|---|---|---|---|---|
Midline catheter group | Control group | |||||
Midline catheter vs. PICC | ||||||
Wen et al. (2024)20 | SR with MA (6 studies); 1,167 adults | Participants with infiltration, n (%) | 24 (3.72%) | 3 (0.58%) | RR = 3.70 (1.61 to 8.33)a | 0.002 |
SR with MA (5 studies); 13,656 catheter days | Number of catheters with infiltration, expressed as the number of events per total catheter days, n/N (%) | 15/7,993 (0.19%) | 3/5,663 (0.05%) | RR = 3.45 (0.55 to 20.00)a | 0.18 | |
CI = confidence interval; MA = meta-analysis; PICC = peripherally inserted central catheter; RR = risk ratio; SR = systematic review; vs. = versus.
aThe findings from Wen et al.20 were calculated using PICC as the intervention compared to midline catheters. To align with the direction of this review (i.e., midline catheters compared to PICC) the effect estimates were inverted by taking the reciprocal of the risk ratio and the bounds of the confidence interval. The findings as reported in the SR were: participants with infiltration, RR = 0.27 (95% CI, 0.12 to 0.62); number of catheters with infiltration, expressed as the number of events per total catheter days, RR = 0.29 (95% CI, 0.05 to 1.81).
Table 14: Summary of Findings by Outcome — Catheter Fracture
Citation | Evidence source, sample size | Outcome | Outcome result | Effect estimate (95% CI) | P value | |
|---|---|---|---|---|---|---|
Midline catheter group | Control group | |||||
Midline catheter vs. PICC | ||||||
Urtecho et al. (2023)21 | SR with MA (1 study); 328 adults | Participants with fractured catheters, n (%) | 2 (0.9%) | 1 (1.0%) | OR = 0.84 (0.08 to 9.36) | NR |
SR with MA (1 study); 30,987 catheters | Catheters that fractured, n (%) | 89 (1.6%) | 381 (1.5%) | OR = 1.11 (0.88 to 1.40) | NR | |
CI = confidence interval; MA = meta-analysis; NR = not reported; OR = odds ratio; PICC = peripherally inserted central catheter; SR = systematic review; vs. = versus.
Table 15: Summary of Findings by Outcome — Catheter Dwell Time
Citation | Evidence source, sample size | Outcome | Outcome result | Effect estimate (95% CI) | P value | |
|---|---|---|---|---|---|---|
Midline catheter group | Control group | |||||
Midline catheter vs. PICC | ||||||
Lai et al. (2024)18 | SR with MA (4 studies); 488 participants (all ages) | Mean catheter dwell time, days (SD) | NR | NR | MD = −1.91 (−3.26 to −0.56) | 0.006 |
SR with MA (3 studies); 382 adults | Mean catheter dwell time, days (SD) | NR | NR | MD = −1.11 (−2.45 to 0.24) | 0.11 | |
SR with MA (1 study); 106 children | Mean catheter dwell time, days (SD) | NR | NR | MD = −2.90 (−4.03 to −1.77) | < 0.00001 | |
Gravdahl et al. (2024)17 | Prospective case series; Bortolussi et al. (2015); 48 adults | Median catheter dwell time, days (range) | 50.5 (8 to 231) | 102 (13 to 462) | NA | NA |
Midline catheter vs. central venous catheter | ||||||
Li et al. (2024)19 | SR with MA (3 studies); 236 adults | Mean catheter dwell time, days (SD) | NR | NR | MD = 0.90 (0.33 to 1.46)a | 0.002 |
Midline catheter vs. conventional IV catheterb | ||||||
Lai et al. (2024)18 | RCT; Nielsen et al. (2021); NR | Median catheter dwell time, days (range) | 7 (0 to 60) | 4 (0 to 84) | NR | 0.002 |
CI = confidence interval; DVT = deep vein thrombosis; MA = meta-analysis; MD = mean difference; NA = not applicable; NR = not reported; PICC = peripherally inserted central catheter; RR = risk ratio; SD = standard deviation; SR = systematic review; SVT = superficial vein thrombosis; vs. = versus.
aThis value was reported as an odds ratio in the main text of the SR by Li et al.,19 but as a MD in the associated figure.
bConventional IV catheters included peripheral venous catheters, central venous catheters, and PICCs.
Table 16: Summary of Findings by Outcome — Treatment Discontinuation
Citation | Evidence source, sample size | Outcome | Outcome result | Effect estimate (95% CI) | P value | |
|---|---|---|---|---|---|---|
Midline catheter group | Control group | |||||
Midline catheter vs. PICC | ||||||
Lai et al. (2024)18 | SR with MA (3 studies); 434 participants (all ages) | Incidence of premature catheter removals per 1,000 catheter days (SD) | NR | NR | MD = 7.30 (2.37 to 12.23) | 0.004 |
SR with MA (2 studies); 328 adults | Incidence of premature catheter removals per 1,000 catheter days (SD) | NR | NR | MD = 6.52 (1.24 to 11.80) | 0.02 | |
SR with MA (1 study); 106 children | Incidence of premature catheter removals per 1,000 catheter days (SD) | 18.1 (45.18) | 5.52 (22.55) | MD = 12.58 (−1.18 to 26.34) | 0.07 | |
RCT; Nielsen et al. (2021); NR | Incidence of premature catheter removals per 1,000 catheter days (SD) | 49.0 (NR) | 11.6 (NR) | NR | NR | |
Wen et al. (2024)20 | SR with MA (5 studies); 2,261 adults | Participants with premature catheter removal, n (%) | 58 (5.24%) | 66 (5.71%) | RR = 1.23 (0.62 to 2.50)a | 0.54 |
SR with MA (4 studies); 148,855 catheter days | Number of premature catheter removals, expressed as the number of events per total catheter days, n/N (%) | 55/24,802 (0.22%) | 62/124,053 (0.05%) | RR = 3.33 (2.22 to 4.76)a | 0.23 | |
Urtecho et al. (2023)21 | SR with MA (6 studies); 13,653 adults | Participants who discontinued therapy, n (%) | 415 (5.4%) | 307 (5.1%) | OR = 1.92 (1.01 to 3.66) | NR |
SR with MA (3 studies); 31,071 catheters | Catheters with treatment discontinuation, n (%) | 124 (2.3%) | 264 (1.0%) | OR = 2.08 (0.53 to 8.15) | NR | |
CI = confidence interval; MA = meta-analysis; MD = mean difference; NR = not reported; OR = odds ratio; PICC = peripherally inserted central catheter; RR = risk ratio; SR = systematic review; vs. = versus.
aThe findings from Wen et al.20 were calculated using PICC as the intervention compared to midline catheters. To align with the direction of this review (i.e., midline catheters compared to PICC) the effect estimates were inverted by taking the reciprocal of the risk ratio and the bounds of the confidence interval. The findings as reported in the SR were: participants with premature catheter removal, RR = 0.81 (95% CI, 0.40 to 1.62); number of premature catheter removals, expressed as the number of events per total catheter days, RR = 0.30 (95% CI, 0.21 to 0.45).
Note: There was overlap in the primary studies that were included in the SRs; the pooled estimates from separate reviews presented in this table thus contain some of the same data. Refer to Appendix 5 for a citation matrix illustrating the degree of overlap.
Table 17: Summary of Findings by Outcome — Mortality
Citation | Evidence source, sample size | Outcome | Outcome result | Effect estimate (95% CI) | P value | |
|---|---|---|---|---|---|---|
Midline catheter group | Control group | |||||
Midline catheter vs. PICC | ||||||
Urtecho et al. (2023)21 | SR with MA (1 study); 406 adults | Mortality, n (%) | 16 (8.0%) | 9 (4.4%) | OR = 1.90 (0.82 to 4.41) | NR |
CI = confidence interval; MA = meta-analysis; NR = not reported; OR = odds ratio; PICC = peripherally inserted central catheter; SR = systematic review; vs. = versus.
Table 18: Summary of Findings by Outcome — Other Outcomes
Citation | Evidence source, sample size | Outcome | Outcome result | Effect estimate (95% CI) | P value | |
|---|---|---|---|---|---|---|
Midline catheter group | Control group | |||||
Midline catheter vs. PICC | ||||||
Wen et al. (2024)20 | SR with MA (4 studies); 1,013 adults | Participants with pain, n (%)a | 15 (2.65%) | 6 (1.35%) | RR = 1.30 (0.60 to 2.86)b | 0.51 |
SR with MA (3 studies); 11,175 catheter days | Number of catheters with pain, expressed as the number of events per total catheter days, n/N (%)a | 12/7,112 (0.17%) | 6/4,063 (0.15%) | RR = 1.54 (0.18 to 12.50)b | 0.69 | |
SR with MA (2 studies); 511 adults | Participant satisfaction rate, %a | 70.8% | 54.5% | RR = 1.09 (0.66 to 1.79)b | NR | |
SR with MA (1 study); 487 adults | Participant dissatisfaction rate, %a | 3.2% | 15.4% | RR = 0.21 (0.10 to 0.43)b | NR | |
CI = confidence interval; MA = meta-analysis; NR = not reported; OR = odds ratio; PICC = peripherally inserted central catheter; RR = risk ratio; SR = systematic review; vs. = versus.
aThe SR by Wen et al.20 included no information on how pain, patient satisfaction, and dissatisfaction were measured (e.g., the types of scales, questionnaires, surveys, or other tools used).
bThe findings from Wen et al.20 were calculated using PICC as the intervention compared to midline catheters. To align with the direction of this review (i.e., midline catheters compared to PICC) the effect estimates were inverted by taking the reciprocal of the risk ratio and the bounds of the confidence interval. The findings as reported in the SR were: participants with pain, RR = 0.77 (95% CI, 0.35 to 1.68); number of catheters with pain, expressed as the number of events per total catheter days, RR = 0.65 (95% CI, 0.08 to 5.42); participant satisfaction rate, RR = 0.92 (95% CI, 0.56 to 1.51); participant dissatisfaction rate, RR = 4.77 (95% CI, 2.33 to 9.77).Table 19: Summary of Recommendations in Included Guidelines
Table 19: Summary of Recommendations in Included Guidelines
Recommendations and supporting evidence | Quality of evidence and strength of recommendations |
|---|---|
INS (2024)25 | |
“Use all available resources, including, but not limited to, evidence-based drug monograph warnings, precautions, and toxicology, and interprofessional collaboration to identify medications that should and should not be given through peripheral veins. Peripheral infusion therapy should be isotonic and of physiological pH. When this is not achievable, peripheral intravenous infusion of extremes of pH and osmolarity should be avoided to reduce vascular endothelial damage. In clinical practice, many parameters, including administration site, number of infusion therapies, vein selected, related venous blood flow, infusion volume, infusion time, and planned duration of therapy contribute to vessel damage. There is no well-defined or generally recognized pH or osmolarity limit. Furthermore, some infusates with physiological pH and osmolarity can be cytotoxic, potentiating cell damage or death. Factors to consider include, but are not limited to: 1. The final osmolarity of the infusion, which is influenced by the diluent (refer to Standard 61, Parenteral Nutrition; Standard 43, Phlebitis) 2. Infusate pH 3. Method of administration (e.g., continuous or intermittent infusion or manual injection [i.e., IV push]), including infusion durations and frequency of administration. 4. Infusion rate and pressure (e.g., power injections) 5. Number of infusion therapies (single vs multiple) 6. Pharmacological effect of the medication on the vein (e.g., vasodilation vs vasoconstriction) (see Standard 65, Vasopressor Administration) 7. Anticipated duration of therapy (as a guide see below): 7.1. (≤ 4 days): Insert a peripheral IV catheter (PIVC) when all the above elements indicate peripherally compatible therapy. 7.2. (5 to 14 days): Insert a midline catheter in hospitalized adult patients when all the above elements indicate peripherally compatible therapy. A long PIVC may remain appropriate if patient’s vasculature, patient’s preference, and local health care outcomes support this practice. More high-quality clinical trials are needed to confirm the safety and efficacy of midline catheter use in neonates and infants. 7.3. (> 15 days): Consider insertion of a peripherally inserted central catheter (PICC). Midline catheters or PIVCs may remain appropriate when all the above elements indicate peripherally compatible therapy and if patient’s vasculature, patient preference, and local health care outcomes support this practice. More high-quality clinical trials are needed to confirm the appropriate use (e.g., single vs multiple therapies) and duration of these catheters” (p. S85-S86).25 Supporting evidence: 11 studies (additional details were NR) | Quality of evidence: Level I (i.e., based on a meta-analysis, SR, guideline based on RCTs, or at least 3 well-designed RCTs) Strength of recommendation: NR |
“Avoid insertion of a peripheral intravenous catheter or midline catheter as a central line-associated bloodstream infection prevention strategy when central venous access is indicated” (p. S86).25 Supporting evidence: Based on committee consensus | Quality of evidence: NA Strength of recommendation: NR |
“Do not use a midline for continuous infusion of vesicant therapy, parenteral nutrition, or other infusates with extremes of pH or osmolarity … Further clinical trials evaluating the appropriate use of midlines for vasopressors (drug type and duration) are needed” (p S87).25 Supporting evidence: 1 study (additional details were NR) | Quality of evidence: Level IV (i.e., based on a well-designed quasi-experimental study, case-control study, cohort study, correlational study, time series study, SR of descriptive and qualitative studies, narrative literature review, or psychometric study) Strength of recommendation: NR |
“Avoid the use of a midline when the patient has a history of thrombosis, hypercoagulability, decreased venous flow to the extremities, or end-stage renal disease requiring vein preservation” (p. S87).25 Supporting evidence: 4 studies (additional details were NR) | Quality of evidence: Level III (i.e., based on 1 well-designed RCT, several well-designed clinical trials without randomization, or several studies with quasi-experimental designs) Strength of recommendation: NR |
“If an arteriovenous fistula or arteriovenous graft is planned or existing … avoid insertion of midline and PICC whenever possible due to an increased risk of thrombosis” (p. S88).25 Supporting evidence: NR | Quality of evidence: NR Strength of recommendation: NR |
“Midline catheters may be labeled for obtaining blood samples; however, limited evidence is available regarding the techniques or outcomes of this procedure. A prospective observational study noted a low hemolysis rate of 0.69% in 1,021 blood samples drawn from midline catheters. Further high-quality research is needed to establish a standard procedure for blood sampling via the midline catheter” (p. S143).25 Supporting evidence: 2 studies (additional details were NR) | Quality of evidence: Level IV (i.e., based on a well-designed quasi-experimental study, case-control study, cohort study, correlational study, time series study, SR of descriptive and qualitative studies, narrative literature review, or psychometric study) Strength of recommendation: NR |
“Remove peripheral intravenous catheters and midline catheters in pediatric and adult patients when clinically indicated, based on findings from site assessment and/or clinical signs and symptoms of systemic complications and not solely on dwell time” (p. S147).25 Supporting evidence: NR | Quality of evidence: NR Strength of recommendation: NR |
“Consider the risk for catheter-associated thrombosis with midline catheters. The utilization of midline catheters has increased rapidly, with an urgent need for high quality research to guide optimal use” (p. S182).25 Supporting evidence: A SR and meta-analysis that included 40,871 patients found that the prevalence of venous thromboembolism with midline catheters was significantly higher than with PICCs. Findings from 2 additional studies also informed this recommendation (additional details were NR) | Quality of evidence: Level II (i.e., based on 2 well-designed RCTs, 2 or more well-designed, multicentre clinical trials without randomization, or an SR of varied prospective study designs) Strength of recommendation: NR |
“Do not use long peripheral intravenous catheters or midline catheters for continuous infusions of antineoplastic vesicants” (p. S220).25 Supporting evidence: 1 study (additional details were NR) | Quality of evidence: Level V (i.e., based on a clinical article, clinical/professional book, consensus report, case report, guideline based on consensus, descriptive study, well-designed quality improvement project, theoretical basis, recommendations by accrediting bodies and professional organizations, or manufacturer recommendations for products or services) Strength of recommendation: NR |
“Do not use midline catheters for continuous vesicant therapy, parenteral nutrition, or solutions with extremes of pH or osmolarity; the use of midline catheters for peripheral parenteral nutrition is not established; the location of midline catheters in a deeper vein may mask early signs of phlebitis, extravasation, and thrombosis” (p. S229).25 Supporting evidence: NR | Quality of evidence: NR Strength of recommendation: NR |
“Do not use the midline peripheral catheter or long peripheral intravenous catheter placed in deep peripheral vessels for continuous vesicant therapy, as there is insufficient evidence to support this practice and there is an increased risk of extensive tissue damage due to the depth of the catheter … Further high-quality, prospective research is needed to establish the safety of the use of the midline peripheral intravenous catheter for vasopressor administration” (p. S242).25 Supporting evidence: Findings from a secondary analysis of an RCT that compared 2 midline catheters suggest the administration of norepinephrine was associated with an increased risk of midline catheter failure. Findings from 2 additional studies also informed this recommendation (additional details were NR) | Quality of evidence: Level IV (i.e., based on a well-designed quasi-experimental study, case-control study, cohort study, correlational study, time series study, SR of descriptive and qualitative studies, narrative literature review, or psychometric study) Strength of recommendation: NR |
Pittiruti et al. (2024)26 | |
“Midline catheters (midclavicular) may be taken into consideration in some selected cases of non-hospitalized children who need a peripheral venous access for a limited period of time (< 4 weeks)” (p. 6).26 Supporting evidence: NR | Quality of evidence: NR Strength of recommendation: Strong agreement (i.e., 90% to 100% of voting members of the panel agreed with the recommendation) |
WHO (2024)27 | |
“WHO suggests the use of either a PICC or midline vascular catheter in adults, adolescents and children requiring longer term intravenous access” (p. 74).27 Supporting evidence: The SR identified 11 studies (2 RCTs and 9 nonrandomized studies) comparing PICCs to midline vascular catheters in adults and children. In adults, the evidence suggested that PICCs may increase the risk of complications related to intravascular catheter insertion compared to midline catheters (3 cohort studies). The evidence was very uncertain about the effect of PICCs compared to midline catheters on catheter-associated bloodstream infections and catheter-related bloodstream infection (5 cohort studies), local infections (1 cohort study), all-cause mortality (2 cohort studies), and phlebitis/thrombophlebitis (3 cohort studies). In children, the evidence was very uncertain about the effect of PICCs compared to midline catheters on catheter-associated bloodstream infections and catheter-related bloodstream infections (1 RCT) and phlebitis/thrombophlebitis (1 RCT). | Quality of evidence: Very low certainty evidence Strength of recommendation: Conditional recommendation |
ACR (2023)28 | |
“Variant 1. Device selection: Acutely ill patient requiring infusion of an irritant medication, or hemodynamic monitoring, or frequent blood draws for 2 weeks or shorter … Midline catheter may be appropriate” (p. S55).28 Supporting evidence: A single-centre prospective RCT found no difference in complication rates between patients who underwent vancomycin infusions (an irritant solution) with a midline catheter or a PICC. Additionally, a prospective cohort study found a low adverse event rate among midline catheters used for prolonged administration (i.e., 6 to 30 days) of nonvesicant drugs in patients with difficult IV access. | Quality of evidence: NR Strength of recommendation: NR |
Pittiruti et al. (2023)29 | |
“The indications for specific peripheral venous access devices are mainly based on the expected duration of treatment:
Supporting evidence: NR | Quality of evidence: NR Strength of recommendation: NR |
ACR = American College of Radiology; INS = Infusion Nurses Society; NA = not applicable; NR = not reported; PICC = peripherally inserted central catheter; RCT = randomized controlled trial; SR = systematic review.
Appendix 5: Overlap Between Included Systematic Reviews
Please note that this appendix has not been copy-edited.
Table 20: Overlap in Relevant Primary Studies Between Included Systematic Reviews
Primary study citation | Gravdahl et al. (2024)17 | Lai et al. (2024)18 | Li et al. (2024)19 | Wen et al. (2024)20 | Urtecho et al. (2023)21 | Chen and Liang (2022)22 | Lu et al. (2022a)23 | Lu et al. (2022b)24 |
|---|---|---|---|---|---|---|---|---|
Bahl et al. Clin Appl Thromb Hemos. 2019;25:1 to 8. | — | — | — | Yes | Yes | — | — | Yes |
Barr et al. Eur J Clin Microbiol Infect Dis. 2012;31(10):2611 to 2619 | — | — | — | — | Yes | Yes | — | — |
Benali et al. Pediatr Radiol. 2013;43(S3): S541. | — | — | — | — | — | Yes | — | Yes |
Bing et al. Am J Surg. 2022; 223(5):983 to 987. | — | — | — | Yes | Yes | — | — | — |
Bortolussi et al. J Pain Symptom Manage. 2015;50(1):118 to 123. | Yes | — | — | — | — | — | — | — |
Caparas and Hu. J Vasc Access. 2014;15:251 to 256. | — | Yes | — | Yes | Yes | Yes | — | Yes |
Caserta et al. J Vasc Access. 2022;23(3):485 to 487. | — | — | — | — | Yes | — | — | — |
Chang et al. Ningxia Medicine Journal. 2022;44(3):267 to 269. | — | — | Yes | — | — | — | — | — |
Dickson et al. J Infus Nurs. 2019;42:203 to 208. | — | — | — | — | Yes | — | — | — |
Gu et al. Front Med. 2012;13(5):8 to 9. | — | — | Yes | — | — | — | — | — |
He et al. China Health Vision. 2018;19:26. | — | — | — | — | — | — | Yes | — |
Hu et al. China Modern Medicine. 2022;29(3). | — | — | Yes | — | — | — | — | — |
Kaatz et al. Res Pract Thromb Hemost. 2019;3:706. | — | — | — | — | — | — | — | Yes |
Khalidi et al. J Assoc Vasc Access. 2009;14:84 to 91. | — | — | — | — | Yes | — | — | — |
Kim et al. Vasc Interv Radiol. 2022;33:189 to 96. | — | — | — | — | Yes | — | — | — |
Kleidon et al. Paediatr Anaesth. 2021;31(9):985 to 995. | — | Yes | — | — | — | — | — | — |
Lescinskas et al. Infect Control Hosp Epidemiol. 2020;41:608 to 610. | — | — | — | Yes | Yes | — | — | — |
Li et al. Chin Nurs Res. 2018;32(24):3966 to 3989. | — | — | — | — | — | — | Yes | — |
Lisova et al. Br J Nurs. 2015;24:S4-S10. | — | — | — | Yes | — | Yes | — | Yes |
Liu et al. Nursing Practice and Research. 2018;15(7):143 to 145. | — | — | — | — | — | — | Yes | — |
Liu et al. Chinese and Foreign Medical Research. 2019;17(35):173 to 175. | — | — | — | — | — | — | Yes | — |
Ma et al. China Health Nutrition. 2021;31(33):87 to 88. | — | — | Yes | — | — | — | — | — |
Mao et al. Modern Hospital (China). 2018;18(9):1390 to 1392. | — | — | Yes | — | — | — | — | — |
Marsh et al. Infect Dis Health. 2023;28:259 to 264. | — | Yes | — | Yes | — | — | — | — |
Magnani et al. J Vasc Access. 2019;20:475 to 481. | Yes | — | — | — | Yes | — | — | — |
Moureau et al. J Vasc Interv Radiol. 2002;13:1009 to 1016. | — | — | — | — | Yes | Yes | — | Yes |
Mushtaq et al. Am J Infect Control. 2018;46:788 to 792. | — | — | Yes | — | Yes | — | — | — |
Nielsen et al. Int J Infect Dis. 2021;102:220 to 225. | — | Yes | Yes | — | — | — | — | — |
Sargent and Nixon. Br J Nurs. 1997;6:543 to 553. | — | — | — | — | Yes | Yes | — | — |
Seo et al. Ann Pharmacother. 2020;54:232 to 238. | — | — | — | Yes | Yes | Yes | — | Yes |
Sharma et al. Am J Respir Crit Care Med,197(Meeting Abstracts). 2018;A6817. | — | — | — | — | — | — | — | Yes |
Sharp et al. Int J Nurs Stud. 2014;51(5):694 to 702. | — | — | — | Yes | Yes | Yes | Yes | Yes |
Shen et al. Nursing of Integrated Traditional Chinese and Western Medicine (China). 2020;6(8):187 to 189. | — | — | Yes | — | — | — | — | — |
Snooks et al. J Neurosurg Anesthesiol. 2019;31(1): 92 to 93. | — | — | — | — | — | Yes | — | — |
Swaminathan et al. JAMA Intern Med. 2022;182:50 to 58. | — | — | — | Yes | Yes | — | — | — |
Tao et al. Journal of BUON. 2019;25(6):2546 to 2552. | — | — | — | Yes | — | Yes | Yes | — |
Thomsen et al. JAMA Netw Open. 2024;7:e2355716. | — | Yes | — | Yes | — | — | — | — |
Tokars et al. Ann Intern Med. 1999;131:340 to 347. | — | — | — | Yes | Yes | — | — | — |
Tso et al. Neurology. 2017;89:279 to 283. | — | — | — | — | Yes | — | — | Yes |
Vanek et al. J Intraven Nurs. 1997;20:23 to 27. | — | — | — | — | Yes | — | — | — |
Xu et al. Am J Infect Control. 2016;44:1458 to 1461. | — | — | — | Yes | Yes | Yes | — | Yes |
Yang et al. Laboratory Medicine and Clinic. 2018;16(6):729 to 731. | — | — | — | — | — | — | Yes | — |
Yin et al. Journal of Medical Aesthetics and Cosmetology (China). 2021;30(7):95 to 96. | — | — | Yes | — | — | — | — | — |
Zeng et al. Journal Modern Medicine Health (China). 2022;38(11):1812 to 1815. | — | — | Yes | — | — | — | — | — |
Zerla et al. J Vasc Access. 2015;20:169 to 176. | — | — | — | Yes | — | — | — | — |
Zohourian et al. J Vasc Access. 2019;24(1):38 to 44. | — | — | — | — | — | — | — | Yes |
ISSN: 2563-6596
Canada’s Drug Agency (CDA-AMC) is a pan-Canadian health organization. Created and funded by Canada’s federal, provincial, and territorial governments, we’re responsible for driving better coordination, alignment, and public value within Canada’s drug and health technology landscape. We provide Canada’s health system leaders with independent evidence and advice so they can make informed drug, health technology, and health system decisions, and we collaborate with national and international partners to enhance our collective impact.
Disclaimer: CDA-AMC has taken care to ensure that the information in this document was accurate, complete, and up to date when it was published, but does not make any guarantee to that effect. Your use of this information is subject to this disclaimer and the Terms of Use at cda-amc.ca.
The information in this document is made available for informational and educational purposes only and should not be used as a substitute for professional medical advice, the application of clinical judgment in respect of the care of a particular patient, or other professional judgments in any decision-making process. You assume full responsibility for the use of the information and rely on it at your own risk.
CDA-AMC does not endorse any information, drugs, therapies, treatments, products, processes, or services. The views and opinions of third parties published in this document do not necessarily reflect those of CDA-AMC. The copyright and other intellectual property rights in this document are owned by the Canadian Agency for Drugs and Technologies in Health (operating as CDA-AMC) and its licensors.
Questions or requests for information about this report can be directed to Requests@CDA-AMC.ca.