Drugs, Health Technologies, Health Systems
Health Technology Review
Crushed Buprenorphine-Naloxone Tablets
Key Messages
What Is the Issue?
Opioid agonist therapy (OAT), including methadone and buprenorphine-naloxone, is the primary approach for managing opioid use disorder (OUD) in Canada and has been shown to reduce withdrawal symptoms and opioid use. Recent Canadian clinical guidelines prioritize buprenorphine-naloxone as the first-line treatment for OUD.
Buprenorphine-naloxone formulations, available as transmucosal tablets or films, are effective for OUD treatment. However, there is a risk of diversion of the tablet formulation; that is, it can be distributed and used by individuals other than those for whom the drugs were prescribed. Crushing buprenorphine-naloxone tablets before administration has been proposed as a potential strategy to mitigate diversion.
What Did We Do?
We sought to identify, summarize, and critically appraise available studies, as well as review evidence-based guideline recommendations on the administration of sublingual crushed buprenorphine-naloxone tablets for the treatment of opioid dependency.
We searched key resources, including journal citation databases, and conducted a focused internet search for relevant evidence published since 2016.
One reviewer screened articles for inclusion based on predefined criteria.
What Did We Find?
We did not find any evidence regarding the clinical effectiveness and safety of sublingual crushed buprenorphine-naloxone tablets for treating opioid dependency.
We did not find any evidence-based guidelines regarding sublingual crushed buprenorphine-naloxone tablets for treating opioid dependency.
What Does It Mean?
We identified no relevant literature on whether crushing buprenorphine-naloxone tablets effectively prevents misuse and diversion in adults with opioid dependence. As a result, no conclusions could be drawn regarding its effectiveness and safety, and no recommendations could be made.
Additional research is needed to assess the impact of crushing buprenorphine-naloxone tablets on efficacy, bioavailability, and adverse effects to determine the clinical implications of this practice.
Abbreviations
OAT
opioid agonist therapy
OUD
opioid use disorder
Context and Policy Issues
The opioid crisis, a complex health and social issue, claimed an estimated 12,800 lives in Canada from opioid-related overdoses between January 2016 and March 2019.1 OUD is a chronic condition with significant consequences for society and individuals, including increased mortality, risk of disease transmission, and poor social functioning.2 The primary approach for treating OUD in Canada is OAT, which includes methadone- and buprenorphine-based formulations, including the buprenorphine-naloxone combination. OAT is an effective form of treatment for people with opioid dependency, reducing withdrawal symptoms and associated risks while curbing opioid use. Recent Canadian clinical guidelines prioritize buprenorphine-naloxone–based OAT as the first choice for OUD treatment.3 Buprenorphine, a partial opioid agonist, produces mild euphoria and other opioidlike effects, albeit less intensely. Naloxone, an opioid antagonist, blocks the brain receptors targeted by opioids like heroin and methadone. Buprenorphine-naloxone formulations are available as tablets or films and are usually taken daily or every other day by patients.4 These transmucosal formulations (tablet and film) are effective in treating OUD. Naloxone in transmucosal formulations is poorly absorbed when taken orally. However, if these formulations are crushed and injected, naloxone blocks the effect of buprenorphine (an opioid), helping deter misuse. Still, diversion of transmucosal tablets, such as selling, sharing, or misusing the prescribed tablets leading to its use by individuals other than those for whom the drugs were prescribed, presents significant challenges in ensuring patients adhere to their treatment.5,6
Why Is It Important to Do This Review?
Crushing buprenorphine-naloxone tablets before administration has been suggested as a potential method of reducing diversion, promoting safe and effective use of medication, and lowering the risk of untreated opioid dependence.7 A 2016 CADTH review8 addressing a similar research question identified 1 study on crushing buprenorphine tablets, but found no literature or evidence-based guidelines on the administration of crushed buprenorphine-naloxone tablets. Understanding the implications of administering crushed buprenorphine-naloxone tablets for preventing misuse and diversion in adults with opioid dependence along with its effects on efficacy, bioavailability, and adverse events is crucial.
Objective
To support decision-making about the clinical practice of crushing buprenorphine-naloxone before administration to prevent diversion, we have prepared this Rapid Review to summarize and critically appraise the available studies on the efficacy and safety of sublingual crushed buprenorphine-naloxone tablets for treating opioid dependency. This report also aims to review the evidence-based guideline recommendations on the administration of crushed buprenorphine-naloxone tablets for the treatment of opioid dependency.
Research Questions
What is the clinical effectiveness and safety of sublingual crushed buprenorphine-naloxone tablets for treating opioid dependency?
What are the evidence-based guidelines regarding the administration of sublingual crushed buprenorphine-naloxone tablets for the treatment of opioid dependency?
Methods
Literature Search Methods
An information specialist conducted a literature search on key resources including MEDLINE, Embase, the Cochrane Database of Systematic Reviews, the International HTA Database, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search approach was customized to retrieve a limited set of results, balancing comprehensiveness with relevancy. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. Search concepts were developed based on the elements of the research questions and selection criteria. The main search concepts were buprenorphine-naloxone, form of administration, and opioid dependence. The search was completed on December 18, 2024, and limited to English-language documents published since January 1, 2016.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. Articles were included if they were made available since the previous search date and were not included in the 2016 CADTH report.8 The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
|---|---|
Population | Adults with opioid dependency |
Intervention | Sublingual administration of crushed buprenorphine-naloxone combination tablets (Suboxone and generics) |
Comparator | Sublingual administration of uncrushed buprenorphine-naloxone combination tablets (Suboxone and generics) |
Outcomes | Clinical effectiveness, safety (including potential for misuse or diversion), evidence-based guidelines |
Study designs | Q1: SRs, HTAs, RCTs (phase II, III, IV), nonrandomized studies including single-arm trials Q2: Evidence-based guidelines |
HTA = health technology assessments; RCT = randomized controlled trials; SR = systematic reviews.
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1.
Summary of Evidence
Quantity of Research Available
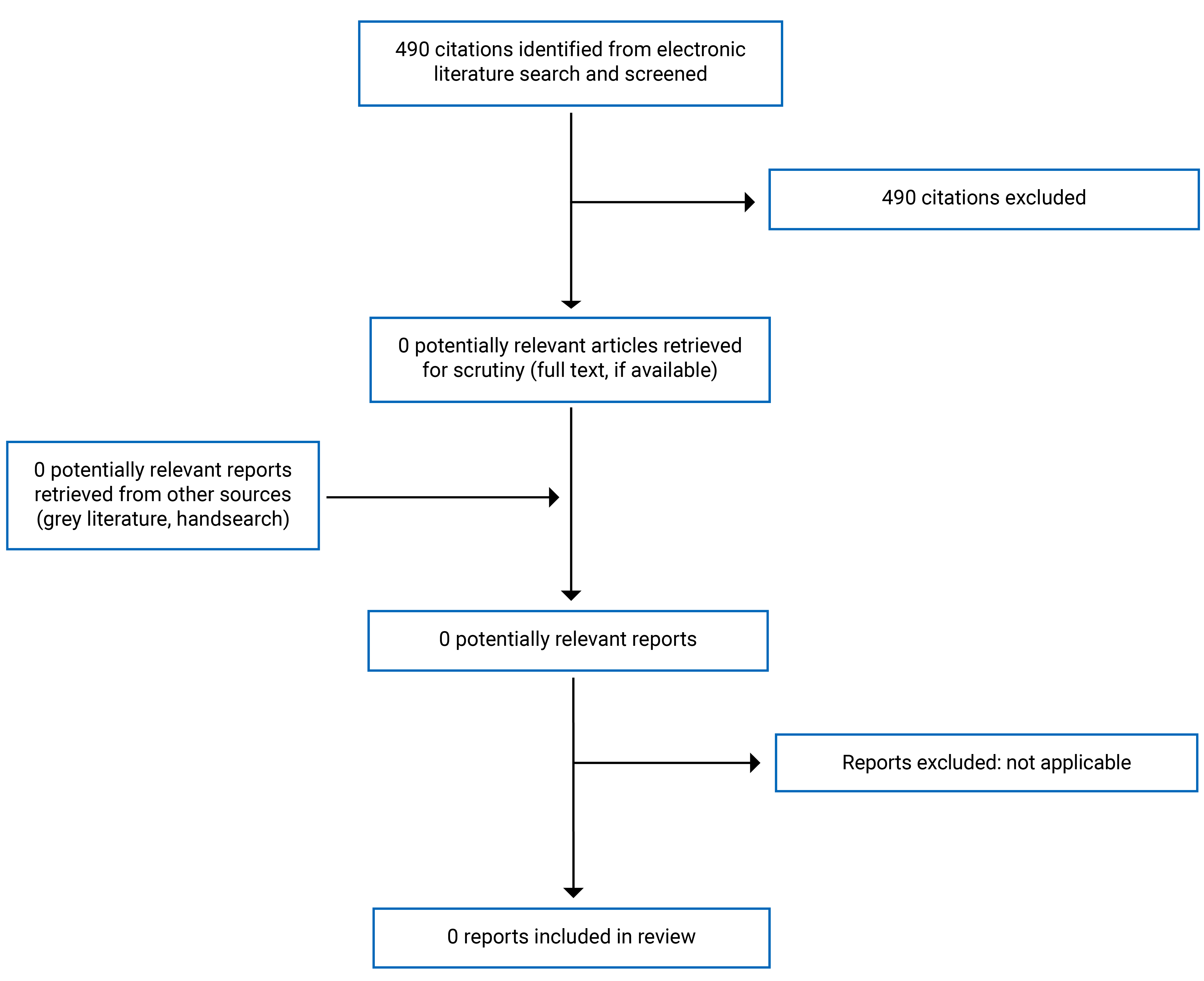
A total of 490 citations were identified in the literature search. Following the screening of titles and abstracts, all 490 citations were excluded. No potentially relevant publications were retrieved from the grey literature search for full-text review. Appendix 1 presents the PRISMA9 flow chart of the study selection.
Summary of Findings
We did not find any evidence regarding the clinical effectiveness and safety of sublingual crushed buprenorphine-naloxone tablets for treating opioid dependency. We also did not find any evidence-based guideline recommendations on sublingual crushed buprenorphine-naloxone tablets for treating opioid dependency.
Limitations
No evidence was identified regarding sublingual administration of crushed buprenorphine-naloxone tablets.
Conclusions and Implications for Decision- or Policy-Making
No relevant literature was identified to answer the research questions; therefore, conclusions could not be provided about clinical effectiveness and safety or recommendations on sublingual crushed buprenorphine-naloxone tablets. Similar to the 2016 report,8 no conclusion can be drawn regarding whether crushing buprenorphine-naloxone tablets could serve as an effective strategy to prevent misuse and diversion in adults with opioid dependence. Future areas of research may include examining the impact of crushing buprenorphine-naloxone tablets on the drug’s efficacy, bioavailability, and adverse effects to determine the clinical implications of this practice. Additional considerations for future research may include effective practices to deter and reduce opioid diversion.
References
1.Canadian Institute for Health Information. Opioids in Canada. 2024. Accessed February 10, 2025. https://www.cihi.ca/en/opioids-in-canada
2.Wright N, D'Agnone O, Krajci P, et al. Addressing misuse and diversion of opioid substitution medication: guidance based on systematic evidence review and real-world experience. J Public Health (Oxf). 2016;38(3):e368-e374. doi:10.1093/pubmed/fdv150 PubMed
3.Bruneau J, Ahamad K, Goyer M, et al. Management of opioid use disorders: a national clinical practice guideline. CMAJ. 2018;190(9):E247-e257. doi:10.1503/cmaj.170958 PubMed
4.BrightView. Sublocade vs. suboxone. 2023. Accessed February 10, 2025 https://www.brightviewhealth.com/latest-updates/sublocade-vs-suboxone/#:~:text=Suboxone%20has%20some%20potential%20for,only%20available%20during%20clinic%20visits
5.McCabe SE, West BT, Teter CJ, Ross-Durow P, Young A, Boyd CJ. Characteristics associated with the diversion of controlled medications among adolescents. Drug Alcohol Depend. 2011;118(2-3):452-8. doi:10.1016/j.drugalcdep.2011.05.004 PubMed
6.Rosenthal RN. Novel formulations of buprenorphine for treatment of opioid use disorder. Focus (Am Psychiatr Publ). 2019;17(2):104-109. doi:10.1176/appi.focus.20180043 PubMed
7.Reimer J, Wright N, Somaini L, et al. The impact of misuse and diversion of opioid substitution treatment medicines: Evidence review and expert consensus. Eur Addict Res. 2016;22(2):99-106. doi:10.1159/000438988 PubMed
8.Canadian Agency for Drugs and Technologies in Health. Crushed buprenorphine or buprenorphine-naloxone for opioid dependency: A review of the clinical effectiveness and guidelines. 2016. Accessed February 10, 2025. https://www.ncbi.nlm.nih.gov/books/NBK378983/
9.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-34. doi:10.1016/j.jclinepi.2009.06.006 PubMed
Appendix 1: Selection of Included Studies
Figure 1: PRISMA9 Flow Chart of Study Selection
ISSN: 2563-6596
Canada’s Drug Agency (CDA-AMC) is a pan-Canadian health organization. Created and funded by Canada’s federal, provincial, and territorial governments, we’re responsible for driving better coordination, alignment, and public value within Canada’s drug and health technology landscape. We provide Canada’s health system leaders with independent evidence and advice so they can make informed drug, health technology, and health system decisions, and we collaborate with national and international partners to enhance our collective impact.
Disclaimer: CDA-AMC has taken care to ensure that the information in this document was accurate, complete, and up to date when it was published, but does not make any guarantee to that effect. Your use of this information is subject to this disclaimer and the Terms of Use at cda-amc.ca.
The information in this document is made available for informational and educational purposes only and should not be used as a substitute for professional medical advice, the application of clinical judgment in respect of the care of a particular patient, or other professional judgments in any decision-making process. You assume full responsibility for the use of the information and rely on it at your own risk.
CDA-AMC does not endorse any information, drugs, therapies, treatments, products, processes, or services. The views and opinions of third parties published in this document do not necessarily reflect those of CDA-AMC. The copyright and other intellectual property rights in this document are owned by the Canadian Agency for Drugs and Technologies in Health (operating as CDA-AMC) and its licensors.
Questions or requests for information about this report can be directed to Requests@CDA-AMC.ca.