Drugs, Health Technologies, Health Systems
Health Technology Review
Virtual Mental Health Counselling
Key Messages
What Is the Issue?
The rate of mental illnesses, such as major depressive disorder and generalized anxiety disorder, has significantly increased among people aged 15 and older living in Canada.
In Canada, more than 1 in 3 of those with mental illnesses do not receive adequate mental health (MH) services, with notable geographic disparities in the availability and quality of services. Specialized MH services remain particularly scarce in remote and rural areas.
Providing MH counselling through virtual platforms has the potential to enhance the accessibility of MH services and reduce the stigma associated with in-person services.
A review of the clinical effectiveness and evidence-based guidelines is required to help understand the potential role of virtual MH counselling in clinical practice.
What Did We Do?
To inform decisions regarding the use of virtual MH counselling for people with depression, anxiety, obsessive-compulsive disorder (OCD) or posttraumatic stress disorder (PTSD), we conducted a rapid review and summarized evidence that compared the clinical effectiveness of MH counselling provided in a virtual setting versus in person. We also sought to identify evidence-based guidelines regarding the use of virtual MH counselling for these populations.
We searched key resources, including journal citation databases, and conducted a focused internet search for relevant evidence published since 2019. One reviewer screened articles for inclusion based on predefined criteria, critically appraised the included studies, and narratively summarized the findings.
What Did We Find?
We found 6 systematic reviews (SRs) relevant to the present review that evaluated the clinical effectiveness of MH counselling provided through virtual versus in-person settings. Most SRs and their included randomized controlled trials (RCTs) reported results on the reduction of depression and anxiety, followed by PTSD and OCD.
For depression, PTSD and specific anxiety outcomes (generalized anxiety disorder, social anxiety disorder, and panic disorder), the effectiveness of virtual MH counselling in improving these outcomes was comparable to in-person settings. For OCD, results were inconsistent, suggesting virtual MH counselling can be an alternative treatment where in-person MH counselling is not readily available.
We found 5 evidence-based guidelines that provide recommendations on the use of virtual MH counselling for adults with depression, anxiety, and PTSD, based mostly on low-quality evidence or expert opinion. We did not find any evidence-based guidelines or relevant recommendations regarding the use of virtual MH counselling for people of any age with OCD nor children and youth with depression, anxiety, and PTSD.
Virtual MH counselling is recommended as a first-line intervention for adults with mild depression and for reducing symptoms of anxiety in older adults.
Virtual MH counselling is recommended as second-line adjunctive or alternative intervention for adults with moderate-severe depression, certain anxiety disorders, and PTSD.
What Does This Mean?
Virtual MH counselling may improve clinical outcomes for people with depression, anxiety, OCD, or PTSD and can be used as a comparable or alternative treatment to in-person MH counselling.
Virtual MH counselling may address equity issues regarding access to evidence-based MH services where in-person MH counselling is not readily available.
Clinicians and health care decision-makers can use the evidence summarized in this review to inform decisions regarding the implementation of virtual MH counselling for adults with depression, anxiety, OCD, or PTSD.
Abbreviations
BA
behavioural activation
CBT
cognitive behavioural therapy
HTA
health technology assessment
MH
mental health
iBA
internet-based behavioural activation
iCBT
internet-based cognitive behavioural therapy
MA
meta-analysis
MDD
major depressive disorder
OCD
obsessive-compulsive disorder
PRISMA
Preferred Reporting Items for Systematic Reviews and Meta-Analyses
PTSD
posttraumatic stress disorder
RCT
randomized controlled trial
SR
systematic review
Research Questions
What is the comparative clinical effectiveness of MH counselling (i.e., psychotherapy or clinical counselling) provided in a virtual setting versus in person for people with depression, anxiety, OCD, or PTSD?
What are the evidence-based guidelines regarding the use of MH counselling (i.e., psychotherapy or clinical counselling) in a virtual setting for people with depression, anxiety, OCD, or PTSD?
Context and Policy Issues
What Is MH?
MH is a state of well-being in which individuals can cope with the normal stresses of life, work productively, and contribute to their community.1 In contrast, mental illness can be defined as a range of conditions that significantly affect a person’s thinking, mood, behaviour, and ability to function in daily life.2 Four of the most prevalent mental illnesses include depressive disorders, anxiety disorders, OCD, and PTSD.2
The rate of mental illnesses, such as major depressive disorder (MDD) and generalized anxiety disorder, has significantly increased among people aged 15 and older living in Canada.3 More than 1 in 3 (36.6%) of people living in Canada with mental illnesses do not receive adequate MH services, with notable geographic disparities in the availability and quality of services.3 Specialized MH services remain particularly scarce in remote and rural areas.4 The COVID-19 pandemic further affected access to MH services in Canada as well as other countries.3
What Is the Current Practice?
In-person MH counselling is widely recognized as the standard of care, offering a structured, face-to-face environment that fosters trust, rapport, and effective communication between clients and therapists.5,6 In-person setting allows for real-time observation of nonverbal cues, immediate feedback, and personalized interventions tailored to the client’s unique needs.6 In-person MH counselling ensures access to a controlled and confidential space which is critical for addressing sensitive issues.5 Services offered may include individual therapy, group therapy and support groups, family and couples counselling, crisis intervention and suicide prevention, and psychoeducation.7
Cognitive behavioural therapy (CBT) has been the most studied approach of psychotherapy.7 However, the effectiveness of other psychotherapy approaches such as behavioural activation (BA), prolonged exposure (PE) therapy, psychodynamic approaches, interpersonal psychotherapy, and acceptance and commitment therapy has also been explored.7
What Is Virtual MH Counselling?
In an effort to increase access, many health care systems and organizations developed platforms to deliver MH services virtually.8 Virtual MH counselling refers to providing psychological support and therapy services through digital platforms, allowing individuals to access MH services remotely.8 These services can be delivered synchronously or asynchronously and differ based on the timing of communication between the client and the therapist.8 Synchronous counselling refers to real-time communication between a client and a therapist whereby both parties are actively engaging in the session at the same time (e.g., video calls, phone calls, or live chat).9 In contrast, asynchronous counselling does not require real-time interaction; clients and therapists communicate at their convenience through written messages, audio recordings, or video clips.10 For this review, virtual MH counselling delivered synchronously is of particular interest as it mirrors the dynamic of traditional in-person therapy; the therapist and client can engage in immediate dialogue, allowing the therapist to respond to the client’s concerns as they are expressed, enabling instant clarification and emotional support.9 Moreover, the use of verbal and nonverbal cues, especially in video sessions, helps build rapport and fosters a sense of connection.
What Are Its Potential Benefits and Challenges?
Virtual MH counselling offers several benefits. It increases accessibility, especially for people in rural areas, individuals with disabilities, or those with demanding schedules.11 It is also more affordable than in-person therapy.12 Virtual MH counselling can also reduce stigma by providing a private space for seeking help and reducing concerns about being seen visiting a therapist's office.13 Finally, it can help individuals with mental illnesses to maintain therapy even when travelling or during public health emergencies like the COVID-19 pandemic.14 Despite these benefits, MH counselling delivered via virtual settings has challenges such as technical barriers, the need for reliable internet access and familiarity with digital tools, which might exclude some populations.15,16 In addition, ensuring the confidentiality of sensitive information is critical and may depend on the platform's security measures.16 Therapists may find it harder to observe body language or subtle emotional cues, particularly in telephone-based formats.17 Finally, the effectiveness of virtual MH counselling in some conditions, such as severe psychiatric disorders, may be limited.18
Why Is It Important to Do This Review?
Virtual MH counselling is a rapidly evolving field. Conducting a review of clinical studies and guidelines on virtual MH is crucial for several reasons, as it helps establish a robust foundation for understanding its effectiveness, limitations, and best practices. A review helps evaluate the effectiveness of virtual MH interventions. By analyzing existing studies, practitioners and policy-makers can determine whether these services are as effective as in-person MH counselling for different populations and conditions. Understanding these findings is critical to building trust in virtual MH services and guiding clinicians and clients in their decision-making. Reviewing guidelines ensures adherence to ethical standards and best practices. A review of the available evidence is essential for adapting to changing client needs and emerging technologies. Evaluating these treatment modalities through rigorous studies ensures that their adoption is based on evidence. Moreover, as client expectations evolve, it may help ensure that services remain relevant and client-centred.
Objectives
The purpose of this rapid review is to identify, summarize, and critically appraise evidence on clinical effectiveness of MH counselling (i.e., psychotherapy or clinical counselling) provided in a virtual setting versus in-person for people with depression, anxiety, OCD, or PTSD. The second objective of this rapid review is to identify, summarize, and critically appraise the evidence-based guidelines regarding the use of MH counselling in a virtual setting for people with depression, anxiety, OCD, or PTSD.
Methods
An information specialist conducted a customized literature search, balancing comprehensiveness with relevancy, of multiple sources and grey literature on November 15, 2024. One reviewer screened citations and selected studies and guidelines based on the inclusion criteria presented in Table 1, and critically appraised included publications and guidelines using established critical appraisal tools. Appendix 1 presents a detailed description of methods and selection criteria for included studies.
Criteria | Description |
|---|---|
Population | People of any age requiring MH counselling services for depression, anxiety, OCD, or PTSD. |
Intervention | Psychotherapy or clinical counselling services provided through virtual settings (e.g., over a video call, telephone) by a registered psychologist, psychotherapist, psychiatric nurse, licensed counselling therapist, or social worker. |
Comparator | Q1: Psychotherapy or clinical counselling services provided in-person by a registered psychologist, psychotherapist, psychiatric nurse, licensed counselling therapist, or social worker. Q2: No comparator necessary |
Outcomes | Q1: Clinical effectiveness (e.g., psychological or psychosocial function or symptoms [e.g., mood, depression, anxiety], health-related quality of life) Q2: Recommendations regarding the use of psychotherapy or clinical counselling provided through virtual settings (e.g., appropriate populations) |
Study designs | HTAs, SRs, MAs, evidence-based guidelines |
Publication date | Q1: Since November 15, 2021 Q2: Since January 1, 2019 |
HTA = health technology assessment; MA = meta-analysis; MH = mental health; OCD = obsessive-compulsive disorder; PTSD = posttraumatic stress disorder; SR = systematic review.
Summary of Evidence
Quantity of Research Available
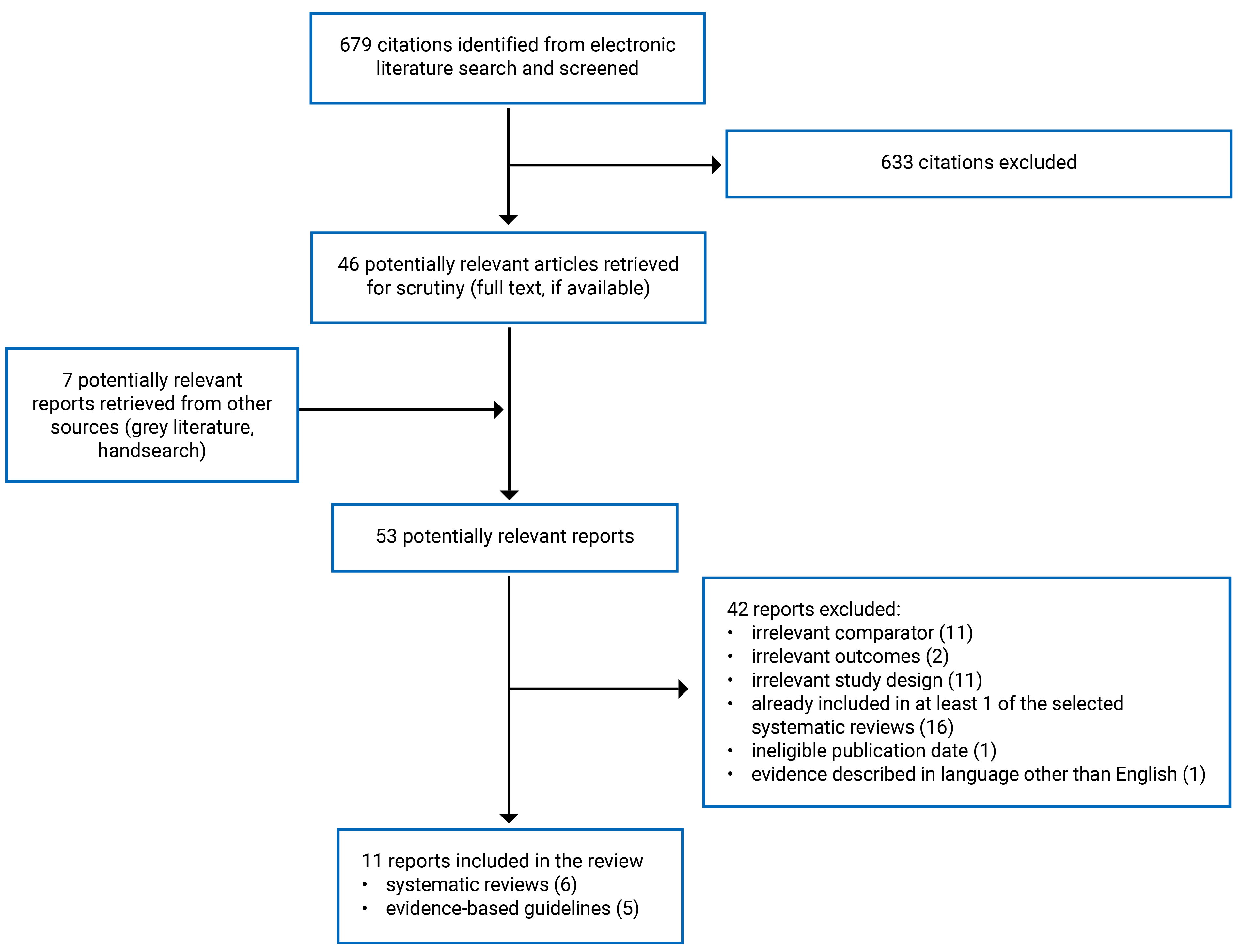
This report includes 6 SRs19-24 and 5 evidence-based guidelines.18,25-28 Appendix 1 presents the PRISMA29 flow chart of the study selection. Additional references of potential interest are provided in Appendix.
Summary of Study Characteristics
Summaries of study characteristics are organized by research question. Additional details regarding the characteristics of included publications are provided in Appendix 2.
Included Studies for Question 1: Clinical Effectiveness of MH Counselling Provided Through Virtual Versus In-Person Settings
We identified 6 SRs,19-24 4 of them20,22-24 with meta-analyses (MAs) that addressed this research question. These 4 SRs20,22-24 included data from 42 unique primary RCTs; however, there was considerable overlap among their included primary studies. As a result, the pooled effect estimates from separate reviews are based on some of the same data, although not all reviews reported the same outcomes. A citation matrix illustrating the degree of primary study overlap is presented in Appendix 5.
All SRs except for 121 limited their search to RCTs; the 6 SRs19-24 searched for studies published from inception, with the last search date being reported as March 2024.22
One SR19 included studies on children and adolescents, aged 0 to 19 years old, 1 SR22 included studies with participants aged over 5 years, and 4 SRs20,21,23,24 included studies on adults (aged ≥ 18 yr). Four SRs19,21-23 provided information on the age of participants from their included primary studies. Three SRs19,21,23 provided information on the sex of participants from their included primary studies; however, they did not report how sex was defined or measured. Authors of the SRs included number or percentage of female and/or male participants; other sexes or genders were not reported.
Four SRs20-22,24 included studies on any form of psychotherapies, such as CBT, BA, cognitive therapy, psychodynamic psychotherapy, PE therapy, or family therapy, which was delivered by a provider via videoconferencing technology (audio and/or video). Two SRs19,23 limited the included studies to CBT delivered via videoconferencing technology by a provider (therapist-guided). One SR21 focused on online group treatments that involved the presence or mediation of a therapist within the group and required active participation of group members. Two SRs22,24 included individual psychotherapy delivered via videoconferencing technology. Three SRs19,20,23 included a mix of individual and group therapies. One SR24 specified a duration of 6 sessions or longer for the length of interventions. Length of follow-up was reported in 4 SRs,19,21-23 which ranged from 0 to 6 months.
The included 6 SRs19-24 assessed several clinical outcomes to address research question 1. Four SRs20,22-24 included eligible MAs on various depression outcomes (e.g., depressive symptoms and severity), and 1 SR22 included eligible MA on anxiety symptoms. One SR24 conducted 2 MAs on depressive symptoms; the first 1 was based on posttreatment scores of 11 RCTs on depressive symptoms measures of all participants with a variety of primary diagnoses (PTSD [n = 5], depression [n = 3], insomnia [n = 1], bulimia nervosa [n = 1], and a combination of mood and anxiety disorders [n = 1]). The second 1 was focused on depressive symptoms measures of 3 RCTs of participants with depression.
Four SRs19-21,23 included eligible RCTs on depression (depressive symptoms or episodes and MDD), anxiety (generalized anxiety disorder, social anxiety disorder, panic disorder, and specific phobia), OCD outcomes (e.g., OCD symptoms and severity), and PTSD outcomes (e.g., PTSD symptoms and severity). One SR24 was limited to studies reporting depressive symptoms as the clinical outcome, 2 SRs19,22 reported on depression and anxiety symptoms, and 3 SRs reported on a mix of various clinical outcomes (e.g., anxiety, obsessive-compulsive, and trauma-related disorders).20,21,23 A variety of additional clinical outcomes were evaluated across the included SRs,20,21 including quality of life, satisfaction with treatment, therapeutic alliance (refers to the strength of the relationship between a therapist and a client), anger, and psychiatric and social functioning.
Included Studies for Question 2: Recommendations Regarding the Psychotherapy or Clinical Counselling Provided Through Virtual Settings
The 5 included guidelines18,25-28 all had specific sections providing recommendations on virtual MH counselling or psychotherapy. There were no guidelines that exclusively focused on virtual MH counselling or psychotherapy.
Two guidelines18,25 provide recommendations for adults with depression: 1 guideline was commissioned by the Canadian Network for Mood and Anxiety Treatments (CANMAT; an academic group)25 and 1 guideline was commissioned by the German National Disease Management Guideline Group (NDGM; in German: Nationale VersorgungsLeitlinie, a national medical association).18 Two guidelines26,27 provide recommendations for older adults and adults with anxiety, which were conducted by the Canadian Coalition for Seniors’ Mental Health (CCSMH; a not-for-profit organization)26 and the German Guidelines for Anxiety Disorders (GGAD) (an academic group).27 The final guideline was commissioned by the Phoenix Australia Centre for Posttraumatic Mental Health (a not-for-profit public company),28 and provides recommendations for children and adults with trauma-related symptoms and PTSD (virtual MH recommendations were specific to adults). No guidelines were found regarding virtual psychotherapy or counselling for OCD.
The guidelines considered and included recommendations on the use of several types of virtual MH interventions, including CBT (4 guidelines),25-28 trauma-focused CBT (1 guideline),28 psychodynamic therapy (1 guideline),27 and internet-based BA (iBA) (1 guideline).25 One guideline18 provides recommendations on internet- and mobile device–based interventions broadly.
Summary of Critical Appraisal
Critical appraisal summaries are organized by study design. Additional details regarding the strengths and limitations of included publications are provided in Appendix 3.
Systematic Reviews
The authors of all 6 SRs19-24 clearly defined their objectives and eligibility criteria, conducted comprehensive literature searches across multiple databases, and provided details on key search terms and search dates. They also included flow charts illustrating study selection, along with reasons for excluding studies. These methodological strengths increase the reproducibility of the SRs. The review methods for all 6 SRs were established before conducting the reviews (e.g., they were documented in published protocols), reducing the risk of reporting bias. In all 6 SRs,19-24 at least 2 independent reviewers conducted study selection and quality assessment. The quality of the included primary studies was assessed using transparent and satisfactory techniques in all 6 SRs. In 3 SRs,20,21,23 subject matter experts were consulted to ensure the search captured relevant studies. Four SRs19-21,23 reported the characteristics of included studies in sufficient detail (e.g., study design, number of participants, intervention). Five SRs19,20,22-24 conducted MAs; all used appropriate statistical methods for the MA. Publication bias was assessed by the authors of 3 SRs.20,23,24 Three SRs19,20,23 used appropriate methods for the statistical combination of results and assessing statistical heterogeneity (e.g., the I2 statistic). The authors of all 6 SRs stated their potential conflicts of interest and the sources of funding.19-24
As for methodological limitations, 3 SRs19,21,24 did not conduct a grey literature search, increasing the risk of missing relevant studies that are not published commercially and that may be inaccessible by bibliographic databases (i.e., non-indexed studies). Although the types of study designs included in the reviews are stated, none of the 6 SRs19-24 provided an explanation for including them. Three SRs19,20,24 limited included studies to those published in English, potentially introducing language bias and omitting relevant data from non-English studies. In 2 SRs,19,21 the data extraction was conducted by a single reviewer or was unclear, creating a risk for inaccuracies in these processes. Two SRs22,24 did not report adequate details on characteristics of included studies (e.g., study design, number of participants, study location, follow-up). One SR21 did not conduct a MA without providing an explanation. Two SRs19,22 did not assess the potential impact of risk of bias on MA findings or adequately investigate publication bias or discussed its likely impact on the results. In 1 SR,22 the authors did not provide an explanation for the considerable statistical heterogeneity observed in the MAs. Not all findings relevant to this review reported relative effects21,23 and actual P values.19,20,22-24 Finally, none of the 6 SRs19-24 reported funding sources for the included primary studies. Although reasons for exclusion were provided, none of the 6 SRs provided a list of excluded studies after full-text review.
Guidelines
All 5 guidelines18,25-28 reported seeking views and preferences of the target population. Three guidelines25,26,28 clearly outlined their scope and purpose. The target users and intended population of the guideline were clearly stated for 4 guidelines.18,25,26,28 All guidelines18,25-28 conducted SRs and had a grading system for assessing the quality of evidence used to make recommendations. Two guidelines conducted additional SRs and/or a rapid review where no recent high-quality SR was available,26,28 and 2 guidelines conducted literature searches of RCTs and other methods of searching (e.g., cross-referencing bibliographies, handsearching pre-existing international guidelines).25,27 Four guidelines25-28 presented each recommendation in an easily identifiable way (e.g., recommendation statements separated from explanatory text, tables within body of guideline to organize statements).
Two guidelines did not specifically describe the health questions.18,25 One guideline did not clearly define their target users.27 For 1 guideline, the methods for formulating the recommendations (e.g., voting, consensus) and an explicit link between the recommendations and the supporting evidence were not clearly described.18 Three guidelines18,27,28 were not externally reviewed by experts before their publication. Two guidelines18,27 did not report supporting documents or tools to aid readers in understanding or implementing recommendations. For 3 guidelines,18,25,27 it is unclear whether the views of the funding body have not influenced the content of the guideline. For 1 guideline, the conflicts of interest in guideline development were not recorded.28 None of the guidelines provided a procedure for updating the guideline.18,25-28
Summary of Findings
Appendix 4 presents the main study findings.
Clinical Effectiveness of MH Counselling Provided Through Virtual Versus In-Person Settings
Evidence regarding the clinical effectiveness of MH counselling provided through virtual versus in-person settings were available from 6 SRs,19-24 4 of them20,22-24 with MAs relevant to the present review. There was considerable overlap in the primary studies that were included in these SRs; the pooled estimates from separate reviews thus contain much of the same data (refer to Appendix 5 for details regarding overlap). Most SRs and their included RCTs reported results on reduction of depression and anxiety, followed by PTSD and OCD. In general, the effectiveness of MH counselling in the reduction of depression, PTSD and various anxiety outcomes was similar in both virtual and in-person settings. However, the results on OCD were inconclusive across intervention modalities.
Depression
Five SRs19,20,22-24 evaluated the effectiveness of MH counselling provided through virtual versus in-person settings on reduction of depression.
The results from 3 SRs, including 4 MAs,22-24 indicated that virtual MH counselling demonstrates comparable efficacy to in-person interventions in reducing the symptoms of depression.
Two SRs with MAs22,23 on depressive symptoms showed no difference in effectiveness of CBT delivered either virtually or in-person.
One SR conducted 2 MAs24 on RCTs comparing multiple video-based versus in-person MH counselling modalities (e.g., CBT and PE) in reducing depressive symptoms for people with various primary diagnoses (11 RCTs) and a subgroup of participants specifically based on depressive diagnoses (3 RCTs). Both MAs showed no evidence that video-based psychotherapy is inferior to in-person psychotherapy in the reduction of depressive symptoms. There was no significant difference between the pooled efficacy effect size estimate of the primary depression subgroup and the pooled estimate of the studies with primary diagnoses of other psychological diagnoses. Prespecified subgroup analyses assessing whether video-based MH counselling might be more effective than in-person counselling for people with a diagnosis of depression found no evidence of differences between the 2 approaches in reducing depressive symptoms or in the risk of participants’ attrition.
Results from 1 SR20 with MAs of 2 RCTs, including veterans and active-duty military participants, indicated that for those with symptoms or diagnosis of depression, in-person delivery was associated with better outcomes compared to video teleconference. The quality of evidence for this comparison was rated as low because of study-specific risk of bias and imprecision.
Results from 1 SR20 that included 1 RCT on telephone-based versus in-person CBT indicated a comparable reduction in depressive symptoms in both groups.
One SR19 including 2 relevant RCTs indicated that virtual CBT was not inferior to in-person CBT in terms of its effectiveness for reducing depressive symptoms in children and youth populations.
Anxiety
Two SRs22,23 evaluated the effectiveness of MH counselling provided through virtual versus in-person settings on reduction of anxiety. All RCTs included in these 2 SRs focused on CBT.
One SR with MA22 indicates that virtual CBT was comparable to in-person CBT in reducing symptoms of anxiety with a follow-up of more than 12 weeks.
One SR23 evaluated the effectiveness of therapist-guided virtual versus in-person CBT on various anxiety outcomes, including health anxiety (1 RCT), social anxiety disorder (1 RCT), panic disorder (4 RCTs) and social phobia (1 RCT). Results of these RCTs indicated that both forms of CBT were comparable and equally effective in improving these various anxiety outcomes of participants.
Obsessive-Compulsive Disorder
Two SRs19,23 including 3 RCTs described the clinical effectiveness of virtual MH counselling, with a focus on CBT, versus in-person counselling for OCD.
One SR19 included 1 RCT on the effectiveness of telephone-based CBT for adolescents (aged 11 to 18 years old) with OCD compared to standard clinic-based, in-person CBT. The results indicated that telephone-based CBT was not inferior to in-person CBT at posttreatment, 3-month, and 6-month follow-up and was similarly effective in reducing OCD symptoms.
One SR23 included 2 RCTs on the effectiveness of telephone-based CBT and therapist-guided internet-based CBT (iCBT) versus in-person CBT for adults with OCD. The clinical outcomes including reduction in OCD symptoms and level of satisfaction with treatment were equivalent for telephone-based CBT and in-person CBT. However, the findings on therapist-guided internet-based CBT versus in-person CBT for adults with OCD were less conclusive, as the primary noninferiority results favoured in-person CBT. SR authors concluded that the therapist-guided iCBT could be an alternative to in-person CBT for adults with OCD where traditional in-person CBT is not readily accessible.
Posttraumatic Stress Disorder
Two SRs20,21 including 12 RCTs provided results for the use of virtual MH counselling on PTSD. Two RCTs were included in both SRs.
Moderate quality of evidence from 1 SR,20 which included 10 relevant RCTs on the use of various interventions for PTSD, indicated that video teleconference is comparable to in-person delivery for people with PTSD. However, this body of literature is mostly focused on evaluating PE (in 3 RCTs) and cognitive processing therapy (CPT and CPT- cognitive only version in 5 RCTs).
One SR,21 including 4 RCTs (2 overlapping with other SR)20 explored the efficacy of online group therapies on PTSD and found evidence supporting the efficacy of video teleconference group therapies for populations with PTSD. These interventions included CPT-C in 2 RCTs and CBT and anger management therapy in the other 2 RCTs. In all 4 RCTs, both video teleconference and in-person group therapies showed significant reductions in PTSD. No significant differences were reported between the groups.
Other Clinical Outcomes
Three SRs20,21,23 reported on the effectiveness of virtual MH counselling versus in-person counselling on other clinical outcomes. They included studies investigating quality of life (1 RCT), satisfaction with treatment (5 RCTs), therapeutic alliance (5 RCTs), anger (1 RCT) and psychiatric and social functioning (1 RCT each). In general, participants who received virtual versus in-person MH counselling reported comparative degrees of therapeutic alliance and satisfaction with treatment. However, the results were inconclusive for other types of functioning and quality of life. Further, participants who received virtual MH counselling showed a similar reduction of anger symptoms as those who received in-person MH counselling.
Guidelines Regarding the Use of Psychotherapy or Clinical Counselling Provided Through Virtual Settings
Depression
Based on limited, low to moderate level quality or unclear evidence, NDGM (2022)18 and CANMAT (2023)25 guidelines provide recommendations for the use of MH counselling through a virtual setting for the treatment of depression. Both guidelines18,25 include recommendations based on the severity of depressive symptoms and/or MDD in adults. The CANMAT (2023)25 guideline provides recommendations on specific types of internet-based psychotherapy (i.e., guided iCBT and guided iBA). The NDGM (2022)18 guideline includes recommendations on the use of internet- and mobile device-based interventions. The NDGM (2022)18 and CANMAT (2023)25 guidelines recommend virtual MH counselling as first-line intervention for mild depression in adults. The NDGM (2022)18 recommends that it is embedded in an overall therapeutic plan. The NDGM (2022)18 guideline recommends virtual MH counselling as second-line adjunctive intervention for moderate-severe depression in addition to other psychotherapy or antidepressants and for adults with moderate depressive episodes who refuse both psychotherapy and antidepressants.
Anxiety
Based on limited and low-quality evidence, the CCSMH (2024)26 and GGAD (2022)27 guidelines include strong or positive recommendations for the use of MH counselling through virtual settings for the treatment of anxiety. The CCSMH (2024)26 guideline provides strong recommendations on the use of remote CBT for reducing symptoms of anxiety in older adults. The GGAD (2022)27 guideline provides positive recommendations on the use of virtual MH counselling for adults with 3 types of anxiety disorders, as an adjunctive intervention to other standard treatments or for adults waiting for initiation of in-person psychotherapy.27 This includes internet-based CBT for adults with generalized anxiety disorder, social anxiety disorder (SAD) or panic disorder with or without agoraphobia (PDA) (refers to an anxiety disorder characterized by recurrent unexpected panic attacks with or without a fear of being in situations where escape might be difficult), and virtual psychodynamic therapy for people with SAD.27
Obsessive-Compulsive Disorder
No guideline or recommendation on the use of virtual MH counselling was found for OCD.
Posttraumatic Stress Disorder
The Phoenix Australia (2021) guideline28 provides recommendations on the use of MH counselling through virtual setting for treatment of trauma-related symptoms and PTSD in adults.28 Based on insufficient evidence, the guideline28 does not recommend internet-based CBT for treatment of PTSD symptoms in adults within the first 3 months of trauma. Based on low-quality evidence, the guideline28 also includes conditional recommendations for use of trauma-focused iCBT and trauma-focused CBT delivered via telehealth (videoconferencing) for adults with PTSD, where face-to-face trauma-focused CBT or Eye Movement Desensitization and Reprocessing (EMDR) are unavailable or unacceptable. Based on insufficient evidence, the Phoenix Australia (2021) guideline28 was not able to make a recommendation on telephone-based CBT for adults within the first 3 months of trauma. Similarly, the guideline28 was not able to make recommendations on BA, Therapeutic Exposure, or group non–trauma-focused CBT delivered via telehealth (videoconferencing) for adults with PTSD.28
Limitations
Limitations to SRs
Evidence Gaps
Across the 6 SRs,19-24 significant gaps in evidence were identified. Mental illnesses such as OCD, or specific types of anxiety and depressive disorders were either included in very few studies or not studied at all. Similarly, virtual group counselling for common conditions were notably limited, restricting our understanding of their potential scalability and effectiveness. There is also a lack of long-term follow-up data to assess the sustained efficacy of these interventions. Most studies focused on immediate or short-term outcomes, leaving a critical knowledge gap about the durability of treatment effects over time. Furthermore, site-specific differences in virtual settings (e.g., home-based versus clinic-based delivery) were not adequately explored, even though such factors may influence treatment outcomes and people’s experiences.
Another critical gap involves the range of interventions studied under virtual CBT. Reviews often grouped diverse modalities, such as telephone-based, therapist-guided internet-based, and video-based therapy, under a broad umbrella. Still, there was insufficient evidence to clarify the differences in effectiveness among these approaches. For example, while therapist-guided, internet-based CBT showed comparable outcomes to in-person therapy, findings for telephone-based CBT were inconclusive, suggesting a need for further investigation.
Risk of Bias of Included Studies in SRs
Several limitations related to the risk of bias were apparent across SRs. A common issue was the potential for publication bias, as some reviews excluded unpublished data, which may overestimate the effectiveness of interventions. Moreover, a heavy reliance on self-reported measures for assessing MH symptoms was noted. Self-report tools can introduce bias, as they may not fully capture the clinical outcomes compared to clinician-rated assessments, which are typically more rigorous.
The narrow inclusion criteria in some reviews also restricted the diversity of studies analyzed. For example, some MAs focused exclusively on direct comparison RCTs, excluding studies with other relevant control conditions. While this approach reduced between-study heterogeneity, it also limited the scope of the analysis and potentially excluded valuable insights. Another significant concern was the unexplained heterogeneity in the pooled estimates, such as compliance rates. In some cases, subgroup analyses were hindered by the small number of trials available for specific conditions, such as anxiety or depression.20,22 This limitation may obscure clinically meaningful effects within subgroups, further complicating interpretations of the data.
Generalizability
The generalizability of findings from these SRs was a recurring challenge. Most of the studies included were conducted in high-income, developed countries and involved participants from relatively affluent and well-educated backgrounds. This demographic profile limits the applicability of findings to low- and middle-income countries or populations with fewer resources. Similarly, populations who may face additional barriers to using technology, such as people with disabilities, were underrepresented in the studies, raising concerns about whether the findings extend to this group. One SR23 was conducted in Canada. However, of the 4 SRs19,21-23 that reported country of study for the included RCTs, 2 RCTs were conducted in Canada. The lack of studies from Canada may limit the generalizability of the evidence to health care settings in Canada.
Other limitations were the age range and sex and gender of participants, with adolescents or younger children (under 12 years old) rarely studied and sex and gender-diverse groups often not specified or included, making it difficult to generalize the results to these populations. However, 2 guidelines25,26 developed by organizations in Canada (i.e., CCSMH (2024) and CANMAT (2023) guidelines) may enhance their relevance to the health care context in Canada. In addition, the reviews grouped diverse delivery methods under broad terms, such as “technology-assisted CBT,” without addressing whether interventions like telephone-based therapy or internet-based therapy provide equivalent outcomes. This lack of distinction undermines the ability to generalize findings across different modalities. Furthermore, the variability in virtual delivery settings — such as home-based versus supervised environments like clinics — was not adequately addressed, even though these factors may significantly influence treatment outcomes.
Limitations to Guidelines
The limitations of the guidelines for virtual MH counselling primarily relate to the quality and scope of the evidence used to inform their recommendations, as well as gaps in addressing specific populations (i.e., children and youth, sex and gender-diverse groups) and conditions (e.g., OCD). Many recommendations were based on limited, low-quality, or unclear evidence, reducing the confidence in their generalizability and applicability. Some guidelines provided broad recommendations without specifying the strength of the evidence or detailing the optimal conditions for intervention.
The guidelines were based on evidence largely derived from studies in high-income countries, limiting their applicability to low- and middle-income settings and culturally diverse populations. Children, adolescents, and individuals in remote or underserved areas were underrepresented in the evidence base. While virtual MH counselling is recommended as an adjunctive or alternative treatment for moderate-to-severe conditions, the guidelines do not provide detailed guidance on how to effectively integrate these interventions with existing treatments (e.g., medication or in-person psychotherapy).
Conclusions and Implications for Decision- or Policy-Making
This review includes 6 SRs,19-24 with 4 including MAs,20,22-24 regarding the effectiveness of MH counselling provided through virtual versus in-person settings. It also includes 5 evidence-based guidelines18,25-28 with specific recommendations on the use of virtual MH counselling for people with depression, anxiety, or PTSD. The evidence summarized in this report is drawn from SRs with substantial overlap in primary studies, meaning that data from the same participants were included in more than 1 SR (refer to Appendix 5 for a citation matrix illustrating the degree of primary study overlap). As a result, some evidence may be disproportionally represented in the overall conclusions.
Summary of Evidence
The evidence summarized in this report indicates virtual MH counselling showed comparable clinical effectiveness to in-person counselling for PTSD and depressive and anxiety disorders. However, findings for OCD, specific clinical settings or subpopulations presented mixed results, highlighting areas where virtual counselling may serve as an alternative to in-person therapy when traditional services are unavailable. Virtual MH counselling may be especially valuable in settings where access to in-person services is limited, though further research is needed to explore long-term outcomes and applicability to diverse populations and contexts. Variability in results may have been due to differences in included populations in studies, study designs, and the specific MH intervention used. For example, 3 SRs with MAs,22-24 which included a large number of participants of diverse backgrounds with depressive symptoms, showed no difference in effectiveness of CBT delivered either virtually or in-person. In contrast, the SR by Kelber et al.,20 which included data from 2 RCTs on veterans and active-duty military participants in their MA, indicated that in-person delivery was associated with better depression outcomes compared to virtual delivery, highlighting certain populations may experience different outcomes than others.
The guidelines for virtual MH counselling provide recommendations for its use across conditions such as depression, anxiety, and PTSD, while no specific guidelines were identified for OCD. Overall, the recommendations reflect limited but generally positive evidence supporting virtual counselling, with suggestions for its use either as a first-line intervention for mild conditions or as an adjunctive or alternative treatment for moderate-to-severe cases or specific conditions when in-person therapy is not feasible.
Considerations for Future Research
More studies are needed to evaluate the efficacy of virtual interventions for conditions such as OCD and co-occurring psychiatric or medical conditions to assess the utility of virtual MH counselling in managing these conditions. It is also needed to evaluate the long-term effectiveness of virtual MH counselling, including symptom recurrence, maintenance of therapeutic gains, and functional outcomes. Future research may consider comparing different virtual delivery methods (e.g., telephone-based, internet-based, video teleconferencing) to identify which approaches work best for specific conditions, populations, and settings. Additional research will benefit from adopting consistent, validated clinical and functional outcome measures, including clinician-rated tools, to improve comparability across studies. In addition, larger and adequately powered trials are needed to strengthen the evidence base. Future research is needed to assess the effectiveness of blended MH counselling models, combining virtual and in-person interventions, and integration with other treatments (e.g., pharmacological treatment) to optimize flexibility and accessibility.
Additional research is needed to address the generalizability of findings to diverse populations and settings. Future studies may include underrepresented groups, such as children and adolescents, culturally diverse populations, and individuals in low- and middle-income countries. Few RCTs included in SRs were conducted on veterans from living in rural areas. Additional research is needed with other groups living in areas where access to in-person services is limited.
The guidelines reflect the evolving state of evidence on virtual MH counselling and its growing role in clinical practice. However, their limitations underscore the need for more robust and inclusive research, particularly in areas like long-term outcomes, diverse populations, and underrepresented conditions (e.g., OCD). Addressing these gaps will enhance future guidelines' relevance, specificity, and strength.
Implications for Clinical Practice and Policy-Making
The integration of virtual interventions into clinical practice and policy frameworks requires addressing various practical, systemic, and person-centred considerations. Virtual MH counselling has demonstrated comparable effectiveness to in-person therapy for conditions such as depression, anxiety, PTSD, and some forms of OCD. This emerging evidence suggests that it may be a valuable option for expanding access to MH counselling, particularly in underserved areas (e.g., rural and remote communities) and underserved populations, such as individuals with mobility issues or transportation constraints. Notwithstanding, assessing people’s preferences, comfort with technology, and specific MH needs are important considerations when determining the appropriateness of virtual versus in-person counselling.30 For conditions such as OCD or PTSD, where virtual therapy may be less effective in some modalities (e.g., internet-based CBT), it will be helpful to consider hybrid or stepped-care approaches.31 While virtual counselling has shown high levels of satisfaction and therapeutic alliance in people who received these services, clinicians may consider strategies to build rapport in virtual settings.32 Techniques may include maintaining regular contact through video or telephone check-ins, and ensuring a supportive environment for group therapies, which have shown comparable effectiveness for PTSD and other conditions.32 Virtual therapy delivery may necessitate clinicians requiring training to navigate technology and maintain engagement.33 This points to the consideration of policy-makers and organizations developing standardized training programs for delivering evidence-based virtual MH counselling and providing technical and psychological support for clinicians to reduce burnout in virtual MH delivery.33
References
1.Mental health and wellness. About mental health. Government of Canada. Accessed December 19, 2024. https://www.canada.ca/en/public-health/services/about-mental-health.html
2.Mental health and wellness. About mental illness. Government of Canada. Accessed December 19, 2024. https://www.canada.ca/en/public-health/services/about-mental-illness.html
3.Stephenson E. Mental disorders and access to mental health care. Statistics Canada. Accessed December 17, 2024. https://www150.statcan.gc.ca/n1/pub/75-006-x/2023001/article/00011-eng.pdf
4.Rural and Remote Mental Health in Canada: Evidence Brief on Best and Promising Practices. Mental Health Commission of Canada. Accessed December 16, 2024. https://mentalhealthcommission.ca/resource/rural-and-remote-mental-health-in-canada-evidence-brief-on-best-and-promising-practices/
5.Horvath AO, Symonds BD. Relation between working alliance and outcome in psychotherapy: A meta-analysis. J Couns Psychol. 1991;38(2):139-149. doi:10.1037/0022-0167.38.2.139
6.Norcross JC, Wampold BE. Evidence-based therapy relationships: research conclusions and clinical practices. Psychotherapy (Chic). 2011;48(1):98-102. doi:10.1037/a0022161 PubMed
7.Cook SC, Schwartz AC, Kaslow NJ. Evidence-Based Psychotherapy: Advantages and Challenges. Neurotherapeutics. 2017;14(3):537-545. doi:10.1007/s13311-017-0549-4 PubMed
8.McDonald A, Eccles JA, Fallahkhair S, Critchley HD. Online psychotherapy: trailblazing digital healthcare. BJPsych Bull. Apr 2020;44(2):60-66. doi:10.1192/bjb.2019.66 PubMed
9.Dhaliwal R, Yap S, Talarico F, et al. Synchronous Web-Based Psychotherapy for Mental Disorders From a Health Quality Perspective: Scoping Review. J Med Internet Res. Nov 3 2023;25:e40710. doi:10.2196/40710 PubMed
10.Chan S, Li L, Torous J, Gratzer D, Yellowlees PM. Review of Use of Asynchronous Technologies Incorporated in Mental Health Care. Curr Psychiatry Rep. Aug 28 2018;20(10):85. doi:10.1007/s11920-018-0954-3 PubMed
11.Andersson G, Titov N, Dear BF, Rozental A, Carlbring P. Internet-delivered psychological treatments: from innovation to implementation. World Psychiatry. 2019;18(1):20-28. doi:10.1002/wps.20610 PubMed
12.Hedman E, El Alaoui S, Lindefors N, et al. Clinical effectiveness and cost-effectiveness of Internet- vs. group-based cognitive behavior therapy for social anxiety disorder: 4-year follow-up of a randomized trial. Behav Res Ther. Aug 2014;59:20-9. doi:10.1016/j.brat.2014.05.010 PubMed
13.Mohammadi R, Tabanejad Z, Abhari S, et al. A Systematic Review of the Use of Telemedicine in the Military Forces Worldwide. Shiraz E-Medical Journal. 2020;21(11):e99343. doi:10.5812/semj.99343
14.Zangani C, Ostinelli EG, Smith KA, et al. Impact of the COVID-19 Pandemic on the Global Delivery of Mental Health Services and Telemental Health: Systematic Review. JMIR Ment Health. Aug 22 2022;9(8):e38600. doi:10.2196/38600 PubMed
15.Feijt M, de Kort Y, Bongers I, Bierbooms J, Westerink J, W IJ. Mental Health Care Goes Online: Practitioners' Experiences of Providing Mental Health Care During the COVID-19 Pandemic. Cyberpsychol Behav Soc Netw. Dec 2020;23(12):860-864. doi:10.1089/cyber.2020.0370 PubMed
16.Gajarawala SN, Pelkowski JN. Telehealth Benefits and Barriers. J Nurse Pract. Feb 2021;17(2):218-221. doi:10.1016/j.nurpra.2020.09.013 PubMed
17.Lin T, Anderson T. Reduced therapeutic skill in teletherapy versus in-person therapy: The role of non-verbal communication. Counselling & Psychotherapy Research. 2024;24(1):317-327. doi:10.1002/capr.12666
18.Harter M, Prien P, N. V. L. Guideline Group. Clinical Practice Guideline: The Diagnosis and Treatment of Unipolar Depression-National Disease Management Guideline. Dtsch Arztebl Int. May 19 2023;120(20):355-361. doi:10.3238/arztebl.m2023.0074 PubMed
19.Bevilacqua L, Fox-Smith L, Lampard O, et al. Effectiveness of technology-assisted vs face-to-face cognitive behavioural therapy for anxiety and depression in children and young people: A systematic review and meta-analysis. Clin Child Psychol Psychiatry. Oct 2024;29(4):1349-1364. doi:10.1177/13591045241259070 PubMed
20.Kelber MS, Smolenski DJ, Boyd C, et al. Evidence-based telehealth interventions for posttraumatic stress disorder, depression, and anxiety: A systematic review and meta-analysis. J Telemed Telecare. Jan 22 2024:1357633X231224491. doi:10.1177/1357633X231224491
21.Laurito LD, Dos Santos-Ribeiro S, Moreira-de-Oliveira ME, et al. Online group therapies for anxiety, obsessive-compulsive, and trauma-related disorders: a systematic review. Front Hum Neurosci. 2023;17:1286865. doi:10.3389/fnhum.2023.1286865 PubMed
22.Oliveira Machado Cecagno P, Donati Polesello N, Duque-Cartagena T, et al. Efficacy of Remote Psychological Interventions for Patients with Anxiety and Depression Symptoms: Systematic Review and Meta-Analysis. Telemed J E Health. Sep 20 2024;20:20. doi:10.1089/tmj.2024.0297 PubMed
23.Zandieh S, Abdollahzadeh SM, Sadeghirad B, et al. Therapist-guided remote versus in-person cognitive behavioural therapy: a systematic review and meta-analysis of randomized controlled trials. CMAJ. Mar 17 2024;196(10):E327-E340. doi:10.1503/cmaj.230274 PubMed
24.Giovanetti AK, Punt SEW, Nelson EL, Ilardi SS. Teletherapy Versus In-Person Psychotherapy for Depression: A Meta-Analysis of Randomized Controlled Trials. Telemed J E Health. 08 2022;28(8):1077-1089. doi:10.1089/tmj.2021.0294
25.Lam RW, Kennedy SH, Adams C, et al. Canadian Network for Mood and Anxiety Treatments (CANMAT) 2023 Update on Clinical Guidelines for Management of Major Depressive Disorder in Adults: Reseau canadien pour les traitements de l'humeur et de l'anxiete (CANMAT) 2023: Mise a jour des lignes directrices cliniques pour la prise en charge du trouble depressif majeur chez les adultes. Can J Psychiatry. Sep 2024;69(9):641-687. doi:10.1177/07067437241245384 PubMed
26.Canadian Guidelines for the Assessment and Treatment of Anxiety in Older Adults. Canadian Coalition for Senior's Mental Health (CCSMH). Accessed November 25, 2024. https://ccsmh.ca/areas-of-focus/anxiety/clinical-guidelines/
27.Bandelow B, Werner AM, Kopp I, Rudolf S, Wiltink J, Beutel ME. The German Guidelines for the treatment of anxiety disorders: first revision. Eur Arch Psychiatry Clin Neurosci. Jun 2022;272(4):571-582. doi:10.1007/s00406-021-01324-1 PubMed
28.Australian Guidelines for the Prevention and Treatment of Acute Stress Disorder, Posttraumatic Stress Disorder, and Complex Posttraumatic Stress Disorder. Phoenix Australia. Accessed November 25, 2024. https://www.phoenixaustralia.org/australian-guidelines-for-ptsd/
29.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
30.Abuyadek RM, Hammouda EA, Elrewany E, et al. Acceptability of Tele-mental Health Services Among Users: A Systematic Review and Meta-analysis. BMC Public Health. Apr 24 2024;24(1):1143. doi:10.1186/s12889-024-18436-7 PubMed
31.Jagayat JK, Kumar A, Shao Y, et al. Incorporating a Stepped Care Approach Into Internet-Based Cognitive Behavioral Therapy for Depression: Randomized Controlled Trial. JMIR Ment Health. Feb 9 2024;11:e51704. doi:10.2196/51704 PubMed
32.Norwood C, Moghaddam NG, Malins S, Sabin-Farrell R. Working alliance and outcome effectiveness in videoconferencing psychotherapy: A systematic review and noninferiority meta-analysis. Clin Psychol Psychother. Nov 2018;25(6):797-808. doi:10.1002/cpp.2315 PubMed
33.Hilty DM, Groshong LW, Coleman M, et al. Best Practices for Technology in Clinical Social Work and Mental Health Professions to Promote Well-being and Prevent Fatigue. Clin Soc Work J. Jun 1 2023:1-35. doi:10.1007/s10615-023-00865-3 PubMed
34.Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. PubMed
35.Agree Next Steps Consortium. The AGREE II Instrument. AGREE Enterprise. Accessed December 6, 2024. https://www.agreetrust.org/wp-content/uploads/2017/12/AGREE-II-Users-Manual-and-23-item-Instrument-2009-Update-2017.pdf
Appendix 1: Detailed Methods and Selection of Included Studies
Please note that this appendix has not been copy-edited.
Literature Search Methods
An information specialist conducted a literature search on key resources including MEDLINE, PsycInfo, the Cochrane Database of Systematic Reviews, the International HTA Database, the websites of health technology assessment agencies in Canada and major international HTA agencies, as well as a focused internet search. The search approach was customized to retrieve a limited set of results, balancing comprehensiveness with relevancy. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. Search concepts were developed based on the elements of the research questions and selection criteria. The main search concepts were virtual or remote care, psychotherapy or counselling, and anxiety, depression, posttraumatic stress disorder, or obsessive-compulsive disorder. Search filters were applied to limit retrieval to health technology assessments, systematic reviews, meta-analyses, indirect treatment comparisons, or guidelines. The search was completed on November 15, 2024, and limited to English-language documents published since January 01, 2019.
Selection Criteria and Methods
One reviewer screened citations and selected studies: the reviewer screened the health technology assessments, systematic reviews (SRs), and meta-analyses (MAs) from the past 3 years (published since November 15, 2021) and screened the guidelines from the past 5 years (published since January 1, 2019). In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Exclusion Criteria
Articles were excluded if they met any of the following criteria:
did not meet the selection criteria outlined in Table 1
were SRs in which all relevant studies were captured in other more recent or more comprehensive SR
were guidelines with unclear methodology.
In addition, articles with a focus on the following criteria were excluded:
people receiving counselling for neurodevelopmental conditions (e.g., autism)
psychotherapy or clinical counselling provided by other health care providers not listed in Table 1 (e.g., psychiatrists, medical doctors)
facilities-based or residential-based addictions treatment
non-clinical counselling (e.g., life skills coaching, vocational coaching)
asynchronous communication (text, email, secured messaging) and AI-based software, apps or bots.
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the following tools as a guide: A MeaSurement Tool to Assess systematic Reviews 2 (AMSTAR 2)34 for SRs, and the Appraisal of Guidelines for Research and Evaluation (AGREE) II instrument35 for guidelines. Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Appendix 2: Characteristics of Included Publications
Table 2: Characteristics of Included Systematic Reviews
Study citation, country, funding source | Study designs and numbers of primary studies included | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Bevilacqua et al. (2024)19 UK Funding source: No funding | Study design: SR and MA of English-language RCTs published up to 1 November 2023. Number of included studies: 10 RCTs in total; 2 relevant to the present review. | Young people aged 0 to 19 (studies which included slightly older participants were accepted if they still included adolescents). Sex: The number of male participants from included primary studies ranged from 13 to 66 (when reported) (20 and 38 for relevant RCTs); the number of female participants was reported for 1 study (25); other sexes or genders were NR. Diagnosis: Anxiety and/or depression. Comorbidities: NR Treatment history: NR Other criteria: Age range of participants in both control and intervention arms had to be 18 or lower. | Intervention:
Comparator: f2f CBT (if more than 2 control groups were present [e.g., online CBT vs. waitlist control vs. f2f CBT] then the study had to include data (e.g., mean and standard deviation at posttreatment) that allowed for a formal comparison between the intervention group and the f2f CBT group). | Outcomes: Anxiety and/or depression (measured by standardized instruments and/or clinical diagnosis) Length of Follow-up: NR |
Kelber et al. (2024)20 US Funding source: No funding | Study design: SR and MA of English-language RCTs published up to April 2022. Number of included studies: 29 RCTs in total; 10 relevant to the present review. | Adult patients with symptoms or diagnoses of PTSD, depression, or anxiety disorder Sex: NR Diagnosis: PTSD, depression, or anxiety disorder Comorbidities: NR Treatment history: NR Other criteria: NA | Intervention: Evidence-based telehealth psychotherapies for patients with symptoms or diagnoses of PTSD, depression, or anxiety disorder. The telehealth modality had to be delivered synchronously by a provider in real-time via telephone or video. Comparator:
| Outcomes: The efficacy of evidence-based behavioural health treatment for symptoms or diagnosis of PTSD, depression, or anxiety disorder. Length of Follow-up: NR |
Oliveira et al. (2024)22 Brazil Funding source: Rio Grande do Sul Research Support Foundation, the National Research Council of Brazil, and the Coordination for the Improvement of Higher Education Personnel. | Study design: SR and MA of any language RCTs published up to March 2024. Number of included studies: 6 RCTs in total; all relevant to the present review. | Patients diagnosed with symptoms of anxiety and or depression of both sexes and aged over 5 years. Sex: NR Diagnosis: Anxiety and/or depression Comorbidities: NR Treatment history: Other intervention received is presented (when reported). Other criteria: NA |
Comparator: The same treatment of remote psychological therapy administered f2f | Outcomes: Impact of remote therapy for the treatment of depression and anxiety symptoms. Length of Follow-up: Ranged between 4 and 48 weeks. |
Zandieh et al. (2024)23 Canada Funding source: Canadian Institutes of Health Research Canada Research Chair in the prevention and management of chronic pain (Jason Busse). | Study design: SR and MA of any language RCTs published up to 4 July 2023. Number of included studies: 54 RCTs in total; 30 relevant to the present review. | Adults (aged ≥ 18 years) presenting with any clinical condition. Sex: The percentage of female participants from included primary studies ranged from 0% to 100% (the same for relevant RCTs) (when reported); other sexes or genders were NR. Diagnosis: Any clinical condition Comorbidities: NR Treatment history: NR Other criteria: NA | Intervention: Therapist-guided remote CBT (e.g., teleconference, videoconference). Comparator: In-person CBT | Outcomes:
Length of Follow-up: Ranged between 42 and 1,095 days. |
Laurito et al. (2023)21 Brazil Funding source: No funding | Study design: SR of RCTs and non-RCTs, observational studies, and case series published in English, Portuguese, German, or Spanish up to 11 March 2023. Number of included studies: 2 Open label and 8 RCTs in total; 4 RCTs relevant to the present review. | Individuals aged 18 years or older who had received a formal diagnosis of anxiety disorder, OCD, and PTSD as per criteria outlined in the DSM or ICD. Sex: The percentage of female participants from included primary studies ranged from 20% to 61% (0% for relevant RCTs); other sexes or genders were NR. Diagnosis: anxiety disorder, OCD (tic disorders), and PTSD. Comorbidities: Major comorbidities are presented (when reported). Treatment history: NR. Other criteria: NA. | Intervention: Online group treatments that involved the presence or mediation of a therapist within the group and required active participation of group members. The interventions were required to emphasize interaction among the participants as a fundamental aspect of the protocol, rather than merely suggesting or encouraging their engagement. Comparator:
| Outcomes: Changes in symptoms related to anxiety disorder, OCD, and PTSD, as measured by formal or validated instruments, both before and after the intervention. Length of Follow-up: 0 to 6 months. |
Giovanetti et al. (2022)24 US Funding source: No funding | Study design: SR and MA of English-language RCTs published from 1 January 2000 to 1 February 2021 Number of included studies: 11 RCTs in total; all relevant to the present review | Individuals who were at least 18 years of age and receiving psychotherapy for depression. Sex: NR Diagnosis: PTSD, chronic insomnia disorder, (major) depressive disorder, bulimia nervosa, and mood or anxiety disorder. Comorbidities: NR Treatment history: NR Other criteria: NA | Intervention: Video-based individual psychotherapy for a duration of 6 sessions or longer. Comparator: in-person individual psychotherapy for a duration of 6 sessions or longer. | Outcomes: Depressive symptoms severity assessed and reported at pretreatment and posttreatment. Length of Follow-up: NR |
CBT = cognitive behavioural therapy; DSM = Diagnostic and Statistical Manual of Mental Disorders; f2f = face to face; ICD = International Classification of Diseases; MA = meta-analysis; NA = not applicable; NR = not reported; OCD = obsessive-compulsive disorder; PTSD = posttraumatic stress disorder; RCT = randomized controlled trial; SR = systematic review.
Note: This table has not been copy-edited.
Table 3: Characteristics of Included Guidelines
Intended users, target population | Intervention and practice considered | Major outcomes considered | Evidence collection, selection, and synthesis | Evidence quality assessment | Recommendations development and evaluation | Guideline validation |
|---|---|---|---|---|---|---|
CCSMH (2024)26 | ||||||
Intended users: health care providers caring for the MH of older adults, including primary care physicians, nurses and nurse practitioners, psychiatrists, psychologists, social workers, and other allied health professionals. Target population: older adults, defined as those 65 and older (a cut-off of 60 and older was included to ensure that all of the relevant evidence in older adults was captured). | Guidelines for prevention, diagnosis, and management of anxiety; recommendations on remote CBT, including iCBT and telephone CBT; virtual MH recommendations are relevant to the present review | Symptoms of anxiety and DSM-5 anxiety disorders in older adults, specifically GAD, panic disorder, agoraphobia, specific phobia, and social anxiety disorder (social phobia). Also included fear of falling, which can be a cause of anxiety later in life. | Systematic literature review of available SR. When no recent high-quality SR was available, conducted SRs and a rapid review. | GRADE | For recommendations addressed through SRs, the certainty of evidence was graded. Working group members met and voted on the direction and strength of recommendations, which reflected the extent to which the panel was confident that the desirable effects of an intervention outweighed the undesirable effects. For best practice recommendations and those which were not directly addressing an SR question, the available evidence was reviewed and its level classified based on its susceptibility to bias. Working group members voted on recommendations and their strength. | The draft recommendations were reviewed by the external expert guidance group, a panel of older adults and caregivers with lived experience of anxiety, and in consultation with health care providers and academic experts. |
CANMAT (2023)25 | ||||||
Intended users: community-based psychiatrists and MH providers Target population: adults with MDD | Guidelines for assessment and management of MDD; recommendations on iCBT and iBA; virtual MH recommendations are relevant to the present review | MDD, Severity of MDD: mild, moderate, and severe, based on the rating of symptom severity and degree of functional impairment, whichever is higher. | SR of SRs and MAs published since 2015, literature search of the CANMAT 2016 guidelines, RCTs and other studies when SRs/MAs were unavailable. Cross-referencing bibliographies, reviews of other major reports and guidelines, expert feedback to identify additional studies. Two independent reviewers selected relevant studies, with consensus adjudication by a third reviewer in cases of disagreement. Data from the included studies were extracted by research staff. | GRADE | Recommendations were organized by lines of treatment, which were informed by CANMAT-defined levels of evidence and supplemented by clinical support (consisting of expert consensus on safety, tolerability, and feasibility). Consensus was sought after each level of review, initially within the authors of each section, then by the core editorial group (consisting of the co-editors and the section editors), and finally by all co-authors. | Internal review, external peer review, review by patient partners |
NDGM (2022)18 | ||||||
Intended users: primary care physicians, psychiatrists, psychotherapists, and complementary care providers. Target population: adults with acute and chronic depressive disorders. | Guidelines on the diagnosis and treatment of acute and chronic depressive disorders; recommendations on internet- and mobile device-based interventions; virtual MH recommendations are relevant to the present review | Depressive disorders and depressive episodes based on their severity: acute mild, moderate, and severe; chronic depression. | SR | GRADE | Structured, formalized consensus process; also, clinical considerations and practical aspects of care provision, together with issues raised by the patient representatives. | A draft of the guideline was made available for public scrutiny, received comments were discussed by the guideline group and led to incorporation of several revisions in the final version |
GGAD (2022)27 | ||||||
Intended users: NR Target population: adults with anxiety disorders. | Guidelines on anxiety disorders; recommendations on internet-based psychological interventions, mostly iCBT; virtual MH recommendations are relevant to the present review | Any anxiety disorder. | Evidence was identified by a search of RCTs published between 16/09/2013 and 20/06/2019, handsearching pre-existing international guidelines on the treatment of anxiety disorders as well as from research identified by an expert panel. RCTs were screened and selected based on inclusion criteria. | SIGN Statement criteria | Voting of the group members, considerations of risks, e.g., adverse effects of drugs. | NR |
Phoenix Australia (2021)28 | ||||||
Intended users: general and MH practitioners planning and providing treatment across clinical settings; people affected by trauma making decisions about their treatment; and funding bodies making service purchasing decisions. Target population: children and adults who are exposed to trauma, people with PTSD symptoms. | Guidelines on acute stress disorder, PTSD and complex PTSD; recommendations on universal and indicated interventions; recommendation on internet-based trauma-focused CBT; virtual MH recommendations for adults are relevant to the present review | Experience of trauma, PTSD symptoms severity and diagnosis, increased recognition of acute stress disorder, PTSD and complex PTSD, increased uptake of evidence-based care, and ultimately, better outcomes for people affected by trauma. | Existing SRs published by ISTSS (inception to October 10, 2018), An update of the ISTSS SRs (October 10, 2018 to June 6, 2019), a new SR, search of trials published between June 2019 and December 31, 2020. Two independent reviewers screened the studies and extracted data from included studies. All available data addressing specific scoping questions were meta-analyzed. | GRADE | Consensus by Guideline Development Group with consideration of balance of benefits and harms, certainty of evidence, patients’ values and preferences, resources, equity, acceptability and feasibility. | These guidelines are under continual review, and recommendations are updated in response to new evidence. The most recent update was approved by the Chief Executive Officer of the National Health and Medical Research Council in December 2021 under Section 14A of the National Health and Medical Research Council Act 1992. |
CANMAT = Canadian Network for Mood and Anxiety Treatments; CBT = cognitive behavioural therapy; CCSMH = Canadian Coalition for Seniors’ Mental Health; DSM-5 = Diagnostic and Statistical Manual of Mental Disorders-5th edition; GAD = generalized anxiety disorder; GGAD = German Guidelines for Anxiety Disorders; GRADE = Grading of Recommendations, Assessment, Development, and Evaluations; iBA = internet-based behavioural activation; iCBT = internet-based cognitive behavioural therapy; ISTSS = International Society for Traumatic Stress Studies; MA = meta-analysis; MDD = major depressive disorder; MH = mental health; NDGM = German National Disease Management Guideline on Unipolar Depression; NR = not reported; Phoenix Australia = Phoenix Australia Centre for Posttraumatic Mental Health; PTSD = posttraumatic stress disorder; RCT = randomized controlled trial; SIGN = Scottish Intercollegiate Guidelines Network; SR = systematic review.
Note: This table has not been copy-edited.
Appendix 3: Critical Appraisal of Included Publications
Please note that this appendix has not been copy-edited.
Table 4: Strengths and Limitations of SRs Using AMSTAR 234
Strengths | Limitations |
|---|---|
Bevilacqua et al. (2024)19 | |
|
|
Kelber et al. (2024)20 | |
|
|
Oliveira Machado et al. (2024)22 | |
|
|
Zandieh et al. (2024)23 | |
|
|
Laurito et al. (2023)21 | |
|
|
Giovanetti et al. (2022)24 | |
|
|
AMSTAR 2 = A MeaSurement Tool to Assess systematic Reviews 2; CINAHL = Cumulative Index to Nursing and Allied Health Literature; GRADE = Grading of Recommendations, Assessment, Development, and Evaluations; MA = meta-analysis; NRSI = nonrandomized studies on interventions; PROSPERO = International Prospective Register of Systematic Reviews; RCT = randomized controlled trial; RoB = risk of bias.
Table 5: Strengths and Limitations of Guidelines Using AGREE II35
Item | CCSMH (2024)26 | CANMAT (2023)25 | NDGM (2022)a18 | GGAD (2022)27 | Phoenix Australia (2021)28 |
|---|---|---|---|---|---|
Domain 1: Scope and purpose | |||||
1. The overall objective(s) of the guideline is (are) specifically described. | Yes | Yes | Yes | Yes | Yes |
2. The health question(s) covered by the guideline is (are) specifically described. | Yes | Yes | No | No | Yes |
3. The population (patients, public, etc.) to whom the guideline is meant to apply is specifically described. | Yes | Yes | Yes | Yes | Yes |
Domain 2: Stakeholder involvement | |||||
4. The Guideline Development Group includes individuals from all relevant professional groups. | Yes | Yes | Yes | Yes | Yes |
5. The views and preferences of the target population (patients, public, etc.) have been sought. | Yes | Yes | Yes | Yes | Yes |
6. The target users of the guideline are clearly defined. | Yes | Yes | Yes | No | Yes |
Domain 3: Rigour of development | |||||
7. Systematic methods were used to search for evidence. | Yes | Yes | Yes | Yes | Yes |
8. The criteria for selecting the evidence are clearly described. | Yes | Yes | No | Yes | Yes |
9. The strengths and limitations of the body of evidence are clearly described. | Yes | Yes | No | Yes | Yes |
10. The methods for formulating the recommendations are clearly described. | Yes | Yes | No | Yes | Yes |
11. The health benefits, side effects, and risks have been considered in formulating the recommendations. | Yes | Yes | Yes | Yes | Yes |
12. There is an explicit link between the recommendations and the supporting evidence. | Yes | Yes | No | Yes | Yes |
13. The guideline has been externally reviewed by experts before its publication. | Yes | Yes | No | No | Unclear |
14. A procedure for updating the guideline is provided. | No | No | No | No | No |
Domain 4: Clarity of presentation | |||||
15. The recommendations are specific and unambiguous. | Yes | Yes | Yes | Yes | Yes |
16. The different options for management of the condition or health issue are clearly presented. | Yes | Yes | Yes | Yes | Yes |
17. Key recommendations are easily identifiable. | Yes | Yes | No | Yes | Yes |
Domain 5: Applicability | |||||
18. The guideline describes facilitators and barriers to its application. | Yes | Yes | Yes | No | Yes |
19. The guideline provides advice and/or tools on how the recommendations can be put into practice. | Yes | Yes | Unclear | No | Yes |
20. The potential resource implications of applying the recommendations have been considered. | Yes | Yes | Unclear | No | Yes |
21. The guideline presents monitoring and/or auditing criteria. | Yes | Yes | No | Yes | No |
Domain 6: Editorial independence | |||||
22. The views of the funding body have not influenced the content of the guideline. | Yes | Unclear | Unclear | Unclear | Yes |
23. Competing interests of Guideline Development Group members have been recorded and addressed. | Yes | Yes | Yes | Yes | No |
AGREE II = Appraisal of Guidelines for Research and Evaluation II; CANMAT = Canadian Network for Mood and Anxiety Treatments; CCSMH = Canadian Coalition for Seniors’ Mental Health; GGAD = German Guidelines for Anxiety Disorders; NDGM = German National Disease Management Guideline on Unipolar Depression; Phoenix Australia = Phoenix Australia Centre for Posttraumatic Mental Health.
Note: All materials related to this guideline (Harter et al., 2023) are available free of charge at www.leitlinien.de and at www.awmf.org. However, since the language of the documents is German, some materials or information may be presented that are not accounted in this evaluation.
Appendix 4: Main Study Findings
Table 6: Summary of Findings by Outcome — Depression
Citation | Evidence source, number of participants | Intervention and modality, outcome (measure) | Baseline M (SD) | Follow-up M (SD) | Relative effect (95% CI) | P value (between groups) | ||
|---|---|---|---|---|---|---|---|---|
Intervention group | Control group | Intervention group | Control group | |||||
Kelber et al. (2024)20 | SR with MA (2 RCTs); 362 participants | VTC BA vs. FtF BA, Depression (BDI) | NR | NR | NR | NR | SMD = 0.28 (0.03 to 0.54) | NR |
Oliveira Machado et al. (2024)22 | SR with MA (4 RCTs); 468 participants | Remote CBT vs. in-person CBT, depression (various measures) | NR | NR | NR | NR | SMD = −0.10 (−0.57 to 0.37) | NR |
Zandieh et al. (2024)23 | SR with MA (13 RCTs); 1,410 participants | Therapist-guided remote CBT vs. in-person CBT, depression (various measures) | NR | NR | NR | NR | SMD = 0.02 (−0.21 to 0.25) | NR |
Giovanetti et al. (2022)a24 | SR with MA (11 RCTs); 1,494 participants | Various virtual vs. in-person interventions, depressive symptoms (various measures) | NR | NR | NR | NR | SMD = 0.04 (−0.12 to 0.20) | 0.60 |
Giovanetti et al. (2022)b24 | SR with MA (3 RCTs); NR | Various virtual vs. in-person interventions, depressive symptoms (various measures) | NR | NR | NR | NR | SMD = −0.06 (−0.56 to 0.45) | NR |
Bevilacqua et al. (2024)19 | 1 RCT; Nelson et al. (2003); 28 participants | VCBT with child/parent vs. FtF CBT with child/parent, depression (CDI) | 14.36 (SD = 9.85) | 13.57 (SD = 8.75) | 6.71 (SD = 4.78) | 11.64 (SD = 11.63) | NR | NR |
1 RCT; Turner et al (2014); 72 participants | Telephone-based vs. FtF CBT, depression (BDI-Y) | 14.58 (SD = 8.73) | 14.44 (SD = 8.77) | 11.08 (SD = 11.28) | 10.98 (SD = 10.16) | NR | NR | |
Kelber et al. (2024)20 | 1 RCT; Mohr et al. (2012); 325 participants | Telephone CBT vs. FtF CBT, depression (PHQ9) | NR | NR | NR | NR | d = −0.02 (−0.24 to 0.20) | NR |
BA = behavioural activation; BDI = Beck Depression Inventory; BDI-Y = Beck Depression Inventory for youth; CBT = cognitive behavioural therapy; CDI = Children’s Depression Inventory; CI = confidence interval; d = Cohen’s d effect size; FtF = face to face; M = mean; MA = meta-analysis; NR = not reported; PHQ9: Patient Health Questionnaire; RCT = randomized controlled trial; SD = Standard Deviation; SMD = standardized mean difference; SR = systematic review; VCBT = video conferencing cognitive behavioural therapy; VTC = video teleconference.
Note: There was overlap in the primary studies that were included in the SRs; the pooled estimates from separate reviews presented in this table thus contain some of the same data. Refer to Appendix 5 for a citation matrix illustrating the degree of overlap.
aMeta-analysis based on posttreatment scores on depressive symptom measures. The primary diagnostic focus of the included studies in this analysis was listed as follows: PTSD (n = 5), depression (n = 3), insomnia (n = 1), bulimia nervosa (n = 1), and a combination of mood and anxiety disorders (n = 1).
bSubgroup meta-analysis focused on studies recruited participants specifically based on depressive diagnoses.
Note: This table has not been copy-edited.
Table 7: Summary of Findings by Outcome — Anxiety
Citation | Evidence source, number of participants | Intervention and modality, Outcome (measure) | Baseline M (SD) | Follow-up M (SD) | Relative effect (95% CI) | P value (between groups) | ||
|---|---|---|---|---|---|---|---|---|
Intervention group | Control group | Intervention group | Control group | |||||
Anxiety symptoms | ||||||||
Oliveira Machado et al. (2024)22 | SR with MA (3 RCTs). 201 participants | Remote CBT vs. in-person CBT, anxiety symptoms (various measures) | NR | NR | NR | NR | SMD = −0.06 (−0.34 to 0.21) | NR |
GAD | ||||||||
Zandieh et al. (2024)23 | 1 RCT; Axelsson et al. (2020); 204 participants | Therapist-guided iCBT vs. in-person CBT, Health anxiety (Health Anxiety Inventory) | NR | NR | 20.70 (SD = 9.3) | 18.00 (SD = 8.50) | NR | NR |
SAD | ||||||||
Zandieh et al. (2024)23 | 1 RCT; Hedman et al. (2011); 126 participants | Therapist-guided iCBT vs. in-person CBT, SAD (Liebowitz Social Anxiety Scale) | NR | NR | 32.10 (SD = 23.10) | 40.70 (SD = 23.70) | NR | NR |
PD | ||||||||
Zandieh et al. (2024)23 | 1 RCT; Bergstrom et al. (2010); 104 participants | Therapist-guided iCBT vs. in-person CBT, PD severity (Panic Disorder Severity Scale) | NR | NR | 4.10 (SD = 4.20) | 5.00 (SD = 5.3) | NR | NR |
1 RCT; Carlbring et al. (2005); 49 participants | Therapist-guided iCBT vs. in-person CBT, anxiety associated with physiologic sensations, PD (Body Sensations Questionnaire) | NR | NR | 32.10 (SD = 11.50) | 31.90 (SD = 10.70) | NR | NR | |
1 RCT; Kenardy et al. (2003); 95 participants | Therapist-guided computer-based CBT vs. in-person CBT, PD (panic-anxiety composite score) | NR | NR | −1.21 (SD = 0.76) | −1.52 (SD = 0.70) | NR | NR | |
1 RCT; Kiropoulos et al. (2008); 86 participants | Therapist-guided iCBT vs. in-person CBT, panic severity (Panic Disorder Severity Scale) | NR | NR | 9.92 (SD = 5.88) | 9.24 (SD = 5.65) | NR | NR | |
Specific phobia | ||||||||
Zandieh et al. (2024)23 | 1 RCT; Andrews et al. (2011); 37 participants | Therapist-guided iCBT vs. in-person CBT, social phobia score (Social Interaction Anxiety Scale) | NR | NR | 44.00 (SD = 15.9) | 31.50 (SD = 23.30) | NR | NR |
CBT = cognitive behavioural therapy; CI = confidence interval; GAD = generalized anxiety disorder; iCBT = internet-based cognitive behaviour therapy; M = mean; MA = meta-analysis; NR = not reported; PD = panic disorder; RCT = randomized controlled trial; SAD = social anxiety disorder; SD = standard deviation; SMD: standardized mean difference; SR = systematic review.
Note: There was overlap in the primary studies that were included in the SRs; the pooled estimates from separate reviews presented in this table thus contain some of the same data. Refer to Appendix 5 for a citation matrix illustrating the degree of overlap.
This table has not been copy-edited.
Table 8: Summary of Findings by Outcome — OCD
Citation | Evidence source, number of participants | Intervention and modality, Outcome (measure) | Baseline M (SD) | Follow-up M (SD) | Relative effect (95% CI) | P value (between groups) | ||
|---|---|---|---|---|---|---|---|---|
Intervention group | Control group | Intervention group | Control group | |||||
Bevilacqua et al. (2024)19 | 1 RCT; Turner et al (2014); 72 participants | Telephone-based vs. FtF CBT, OCD (CY-BOCS) | 25.64 (SD = 3.86) | 24.11 (SD = 4.2) | 12.99 (SD = 8.56) | 11.72 (SD = 7.06) | NR | NR |
Zandieh et al. (2024)23 | 1 RCT; Lovell et al. (2006); 72 participants | Telephone-based CBT vs. in-person CBT, OCD (Y-BOCS) | NR | NR | 14.20 (SD = 7.80) | 13.30 (SD = 8.60) | NR | NR |
1 RCT; Lundstrom et al. (2022); 80 participants | Therapist-guided iCBT vs. in-person CBT, OCD (Y-BOCS) | NR | NR | 10.80 (SD = 5.81) | 11.70 (SD = 5.49) | NR | NR | |
CBT = cognitive behavioural therapy; CI = confidence interval; CY-BOCS = Children’s Yale-Brown Obsessive-Compulsive Scale; FtF = face-to-face; iCBT = internet-based cognitive behaviour therapy; M = mean; NR = not reported; OCD = obsessive-compulsive disorder; RCT = randomized controlled trial; SD = Standard Deviation; Y-BOCS = Yale-Brown Obsessive-Compulsive Scale.
Note: There was overlap in the primary studies that were included in the SRs; the pooled estimates from separate reviews presented in this table thus contain some of the same data. Refer to Appendix 5 for a citation matrix illustrating the degree of overlap.
This table has not been copy-edited.
Table 9: Summary of Findings by Outcome — PTSD
Citation | Evidence source, number of participants | Intervention and modality, Outcome (measure) | Baseline M (SD) | Follow-up M (SD) | Relative effect (95% CI) | P value (between groups) | ||
|---|---|---|---|---|---|---|---|---|
Intervention group | Control group | Intervention group | Control group | |||||
Kelber et al. (2024)20 | 1 RCT; Acierno et al. (2016); 265 participants | VTC BA + Therapeutic Exposure vs. FtF BA + Therapeutic Exposure, PTSD (PCL) | NR | NR | NR | NR | d = 0.01 (−0.27 to 0.28) | NR |
1 RCT; Acierno et al. (2017); 150 participants | VTC PE vs. FtF PE, PTSD (PCL) | NR | NR | NR | NR | d = 0.29 (−0.06 to 0.63) | NR | |
1 RCT; Acierno et al. (2021); 136 participants | VTC PE vs. FtF PE, PTSD (PCL) | NR | NR | NR | NR | d = 0.37 (−0.04 to 0.77) | NR | |
1 RCT; Frueh et al. (2007); 38 participants | VTC Group CBT vs. FtF Group CBT, PTSD (PCL) | 67.00 (SD = 9.4)a | 62.30 (SD = 12.8)a | Posttreatment: 68.10 (SD = 11.0)a | Posttreatment: 56.50 (SD = 10.1)a | d = 0.38 (−0.49 to 1.25) | 0.39 | |
f/ub: 61.40 (SD = 14.6)a | f/ub: 60.50 (SD = 9.8)a | |||||||
1 RCT; Liu et al. (2020); 207 participants | VTC CPT vs. FtF CPT, PTSD (CAPS) | NR | NR | 56.60 (SD = 28.5)c | 57.30 (SD = 26.9)c | d = 0.55 (0.28 to 0.83) | NR | |
1 RCT; Maieritsch et al. (2016); 90 participants | VTC CPT vs. FtF CPT, PTSD (CAPS) | NR | NR | 50.02 (SD = 22)c | 48.24 (SD = 21.42)c | d = −0.16 (−0.71 to 0.39) | NR | |
1 RCT; Morland et al. (2014); 144 participants | VTC Group CPT-C vs. In-person group CPT-C, PTSD (CAPS) | 72.00 (SD = 14.60)a | 68.90 (SD = 13)a | Posttreatment: 55.60 (SD = 18.80)a | Posttreatment: 58.70 (SD = 21)a | d = −0.27 (−0.66 to 0.12) | NR | |
f/ub: 56.20 (SD = 18)a | f/ub: 57.80 (SD = 18.7d)a | |||||||
1 RCT; Morland et al. (2015); 98 participants | VTC CPT vs. FtF CPT, PTSD (CAPS) | NR | NR | NR | NR | d = −0.18 (−0.53 to 0.18) | NR | |
1 RCT; Morland et al. (2020); 175 participants | Home-Based VTC PE vs. Office-Based VTC PE, PTSD (CAPS) | NR | NR | NR | NR | d = 0.22 (−0.14 to 0.59) | NR | |
1 RCT; Peterson et al. (2020); 120 participants | VTC CPT vs. FtF (in-office) CPT vs. FtF (in-home) CPT, PTSD (CAPS) | NR | NR | 26.00 (SD = 10.26)c | 26.20 (SD = 17.02)c | d = −0.19 (−0.74 to 0.37) | NR | |
Laurito et al. (2023)21 | 1 RCT; Morland et al. (2010); 125 participants | VTC group AMT vs. In-person group AMT, PTSD (CAPS) | 64.50 (SD = 11.60) | 65.80 (SD = 10.80) | 59.20 (SD = 15) | 57.40 (SD = 16) | NR | NR |
1 RCT; Morland et al. (2011); 13 participants | VTC group CPT-C vs. In-person group CPT, PTSD (CAPS) | 82.50 (NRe) | 77 (NRe) | Posttreatment: 69 (NRe) | Posttreatment: 62 (NRe) | NR | Posttreatment: P > 0.05 6M f/u: P > 0.05 | |
AMT = anger management therapy; BA = behavioural activation; CAPS = Clinician-Administered PTSD Scale for DSM-5; CBT = cognitive behavioural therapy; d = Cohen’s d effect size; CI = confidence interval; CPT = cognitive processing therapy; CPT-C: cognitive processing therapy - cognitive only version; FtF = face-to-face; f/u = follow-up; M = mean; NR = not reported; PE = prolonged exposure; PCL = PTSD Checklist; PTSD = posttraumatic stress disorder; RCT = randomized controlled trial; SD = standard deviation; VTC = video teleconference.
Note: There was overlap in the primary studies that were included in the SRs; the pooled estimates from separate reviews presented in this table thus contain some of the same data. Refer to Appendix 5 for a citation matrix illustrating the degree of overlap.
This table has not been copy-edited.
aThese data are reported from another SR, Laurito et al. (2023).21
bLength of follow-up not reported.
cThese data are reported from another SR, Zandieh et al. (2024).23
dThe standard deviation is reported as 19.8 in Zandieh et al. (2024).23
ePresented data on median scores.
Table 10: Summary of Findings by Outcome — Additional Clinical Outcomes
Citation | Evidence source, number of participants | Baseline M (SD) | Follow-up M (SD) | Relative effect (95% CI) | P value (between groups) | ||
|---|---|---|---|---|---|---|---|
Intervention group | Control group | Intervention group | Control group | ||||
Quality of life | |||||||
Kelber et al. (2024)20 | 1 RCT; Egede et al. (2015); 141 participants | NR | NR | NR | NR | d = −0.12 (−0.37 to 0.13) | NR |
Satisfaction with treatment | |||||||
Kelber et al. (2024)20 | 1 RCT; Acierno et al. (2017); 150 participants | NR | NR | NR | NR | Appearance of facility: d = −0.14 (−0.63 to 0.35) | NR |
Convenience of facility: d = 0.11 (−0.38 to 0.60) | |||||||
Recommendation: d = 0.06 (−0.43 to 0.55) | |||||||
Respectful care: d = −0.06 (−0.55 to 0.43) | |||||||
1 RCT; Egede et al. (2015); 241 participants | NR | NR | NR | NR | d = −0.05 (−0.30 to 0.20) | NR | |
1 RCT; Luxon et al. (2016); 121 participants | NR | NR | NR | NR | d = 0.39 (−0.04 to 0.81) | NR | |
1 RCT; Morland et al. (2014); 144 participants | NR | NR | NR | NR | Convenience of facility: d = 0.25 (−0.13 to 0.64) | NR | |
1 RCT; Morland et al. (2015); 98 participants | NR | NR | NR | NR | d = −0.21 (−0.56 to 0.14) | NR | |
Therapeutic alliancea | |||||||
Kelber et al. (2024)20 | 1 RCT; Mohr et al. (2012); 325 participants | NR | NR | NR | NR | Client: d = −1.02 (−1.27 to −0.78) | NR |
Therapist: d = −0.36 (−0.59 to −0.12) | |||||||
1 RCT; Maieritsch et al. (2016); 90 participants | NR | NR | NR | NR | d = −0.12 (−0.67 to 0.44) | NR | |
1 RCT; Morland et al. (2014); 144 participants | NR | NR | NR | NR | Leaders: d = 0.00 (−0.38 to 0.38) | NR | |
Leader self: d = 0.25 (−0.14 to 0.63) | |||||||
Member: d = 0.18 (−0.20 to 0.56) | |||||||
Total: d = 0.25 (−0.14 to 0.63) | |||||||
1 RCT; Morland et al. (2015); 98 participants | NR | NR | NR | NR | Client: d = −0.03 (−0.38 to 0.32) | NR | |
Therapist: d = −0.04 (−0.39 to 0.31) | |||||||
Zandieh et al. (2024)23 | 1 RCT; Watts et al. (2020); 115 participants | NR | NR | 240.73 (SD = 16.05) | 233.96 (SD = 13.76) | NR | NR |
Anger | |||||||
Laurito et al. (2023)21 | 1 RCT; Morland et al. (2010); 125 participants | STAXI-2 (AE) | NR | NR | |||
56.70 (SD = 12) | 55 (SD = 10.3) | Posttreatment: 42.40 (SD = 16.20) f/u: 42 (SD = 15.60) | Posttreatment: 46.60 (SD = 12.20) f/u: 46.60 (SD = 15.30) | ||||
STAXI-2 (TA) | |||||||
28 (SD = 6) | 27.80 (SD = 5.60) | Posttreatment: 22.10 (SD = 6.20) f/u: 22.40 (SD = 7.30) | Posttreatment: 23.30 (SD = 6) f/u: 25.60 (SD = 8.20) | ||||
NAS-T | |||||||
109.30 (SD = 16.10) | 109.8 (SD = 14) | Posttreatment: 94.20 (SD = 19.10) f/u: 97.70 (SD = 20.20) | Posttreatment: 99.20 (SD = 17.10) f/u: 101 (SD = 22.50) | ||||
Psychiatric functioning | |||||||
Kelber et al. (2024)20 | 1 RCT; Frueh et al. (2007); 38 participants | NR | NR | NR | NR | d = 0.47 (−0.41 to 1.34) | NR |
Social functioning | |||||||
Kelber et al. (2024)20 | 1 RCT; Frueh et al. (2007); 38 participants | NR | NR | NR | NR | d = −0.70 (−1.59 to 0.19) | NR |
CI = confidence interval; d = Cohen’s d effect size; f/u = follow-up; M = mean; NAS-t = Novaco anger scale-total score; NR = not reported; RCT = randomized controlled trial; SD = Standard Deviation; STAXI-2 (AE) = State-Trait Anger Expression Inventory-2 (anger expression); STAXI-2 (TA) = State-Trait Anger Expression Inventory-2 (trait anger).
Note: This table has not been copy-edited.
aRefers to the strength of the relationship between a therapist and a client.
Table 11: Summary of Recommendations in Included Guidelines — Depression
Recommendations and supporting evidence | Quality of evidence and strength of recommendations |
|---|---|
CANMAT (2023)25 | |
“Guided iCBT is recommended as a first-line monotherapy for mild depression, and as a first-line adjunctive treatment for moderate severity MDD.” (p. 666)25 Evidence from an umbrella review of iCBT reported medium to large effect sizes across 4 MAs. The Good Days Ahead program, incorporating therapist or telephone support, demonstrated efficacy in 2 large RCTs. | Level of evidence: level 2a Line of treatment: first lineb |
“Guided iBA is recommended as a second-line adjunctive treatment for mild–moderate MDD when supported by clinicians.” (p. 666)25 Evidence from 1 MA indicated that iBA for depression was more effective than psychoeducation or treatment as usual, and noninferior in effectiveness to other behavioural therapy and mindfulness formats. One RCT of guided email support showed no differences when compared to a waitlist control group. | Level of evidence: level 3c Line of treatment: second lined |
NDGM (2022)18 | |
“Internet- and mobile device-based interventions (IMI) should be offered in mild depressive episodes, embedded in an overall therapeutic concept.” (p. 357)18 Supporting evidence: NR | NR |
“Internet- and mobile device-based interventions may be offered to patients with moderate depressive episodes in addition to treatment with antidepressants or psychotherapy, embedded in an overall therapeutic concept.” (p. 358)18 Supporting evidence: NR | NR |
“Internet- and mobile device-based interventions should be offered as an alternative treatment option to patients with moderate depressive episodes who refuse both psychotherapy and antidepressants.” (p. 358)18 Supporting evidence: NR | NR |
“Internet- and mobile device-based interventions may be offered to patients with severe depressive episodes in addition to treatment with antidepressants and/or psychotherapy.” (p. 358)18 Supporting evidence: NR | NR |
CANMAT = Canadian Network for Mood and Anxiety Treatments; iBA = internet-based behavioural activation; iCBT = internet-based cognitive behavioural therapy; MA = meta-analysis; MDD = major depressive disorder; RCT = randomized controlled trial; NDGM = German National Disease Management Guideline on Unipolar Depression; NR = not reported.
Note: This table has not been copy-edited.
aLower-quality MA with wide confidence intervals and/or 1 or more RCTs with adequate sample size.
bLevel 1 or 2 evidence, plus clinical support. Clinical support refers to the application of expert consensus by the CANMAT editorial group to ensure that evidence-supported interventions are feasible and relevant to clinical practice.
cSmall-sample RCTs or nonrandomized, controlled prospective studies or high-quality retrospective studies.
dLevel 3 evidence or higher, plus clinical support.
Table 12: Summary of Recommendations in Included Guidelines — Anxiety
Recommendations and supporting evidence | Quality of evidence and strength of recommendations |
|---|---|
CCSMH (2024)26 | |
“Remote CBT is effective and should be offered as a treatment option for anxiety in older adults.” (p. 3)26 Evidence from 5 studies indicated that remote CBT was effectively reduced anxiety symptoms in older adults compared to usual care. There was no difference between remote and in-person CBT for reduction of anxiety symptoms. | Quality of evidence: Low Strength of recommendation: Strong |
GGAD (2022)27 | |
For panic disorder with or without agoraphobia: “Patients can be offered CBT-based internet interventions for bridging the waiting period until standard CBT starts or as add-on measure to standard CBT.” (p. 580)27 “CBT-based internet interventions should not be offered as monotherapy.” (p. 580)27 Expert consensus based on CCPa | Level of evidence: expert consensus Recommendation grade: CCP +b |
For generalized anxiety disorder: “Patients can be offered CBT-based internet interventions for bridging the waiting period until standard CBT starts or as add-on measure to standard CBT.” (p. 580)27 “CBT-based internet interventions should not be offered as monotherapy.” (p. 580)27 Expert consensus based on RCTs and CCPa Evidence from RCTs showed that internet-based psychological interventions were more effective than a waitlist control. There is insufficient evidence showing that internet-based psychological interventions are as effective as individual face-to-face CBT. | Level of evidence: expert consensus Recommendation grade: CCP +b |
For social anxiety disorder: “Patients can be offered CBT- or PDT-based internet interventions for bridging the waiting period until standard CBT starts or as add-on measure to standard CBT.” (p. 580)27 “CBT-based internet interventions should not be offered as monotherapy.” (p. 580)27 Expert consensus based on RCTs and CCPa Evidence from RCTs showed that internet-based psychological interventions were more effective than a waitlist control. There is insufficient evidence showing that internet-based psychological interventions are as effective as individual face-to-face CBT. | Level of evidence: expert consensus Recommendation grade: CCP+b |
CBT = cognitive behavioural therapy; CCP = clinical consensus point; CCSMH = Canadian Coalition for Seniors’ Mental Health; GGAD = German Guidelines for Anxiety Disorders; PDT = psychodynamic therapy; RCT = randomized controlled trial.
Note: This table has not been copy-edited.
aClinical consensus point: if no unequivocal evaluation of a relevant clinical topic was possible, recommendations were formulated by expert consensus.
bPositive recommendation based on clinical consensus point.
Table 13: Summary of Recommendations in Included Guidelines — PTSD
Recommendations and supporting evidence | Quality of evidence and strength of recommendations |
|---|---|
Phoenix Australia (2021)28 | |
“For adults within the first 3 months of trauma, wea suggest usual practice in preference to iCBT.” (p. 16)28 Insufficient supporting evidence Evidence from 1 study indicated a small but clinically important benefit of iCBT on PTSD diagnosis rates and symptom severity in adults within the first 3 months following a serious injury. The Guideline Development Group agreed that the current evidence is insufficient to make a recommendation for iCBT. | Certainty (quality) of evidence: Low Strength of recommendation: NA |
“For adults within the first 3 months of trauma, there was insufficient evidence to make a recommendation on telephone-based CBT.” (p. 18)28 Insufficient supporting evidence. Evidence from 1 study indicated that telephone-based CBT may have minimal or no impact on PTSD symptom severity. The Guideline Development Group was uncertain whether telephone-based CBT increases or decreases PTSD symptom severity. | Certainty (quality) of evidence: Very low Strength of recommendation: NA |
“For adults with PTSD where trauma-focused CBT or EMDR are unavailable or unacceptable, trauma-focused iCBT is conditionally recommended.” (p. 23)28 Evidence from 3 RCTs demonstrated a large clinically important benefit of guided trauma-focused iCBT compared to waitlist or attention control. Evidence from 1 RCT indicated a modest clinically important advantage of guided trauma-focused iCBT over internet-based supportive counselling without a trauma focus. Evidence from 1 RCT found no significant difference between guided trauma-focused iCBT and internet-based psychotherapy. Evidence from 1 RCT indicated a moderate clinically important benefit of in-person present-centred therapy compared to guided internet-based prolonged exposure. | Certainty (quality) of evidence: low Strength of recommendation: Conditionalb |
“For adults with PTSD, where face-to-face trauma-focused CBT or EMDR are unavailable or unacceptable, trauma-focused CBT delivered via telehealth (videoconferencing) is conditionally recommended.” (p. 39)28 Evidence from 3 RCTs indicated large clinically important benefit from guided trauma-focused iCBT compared to waitlist or attention control. Evidence from 1 RCT indicated a small clinically important benefit of guided trauma-focused iCBT above that of internet-based supportive counselling without a trauma focus. Evidence from 1 RCT indicated no important difference between guided trauma-focused iCBT and internet-based psychotherapy. Evidence from 1 RCT showed a moderate clinically important benefit from present-centred therapy delivered in person compared to guided internet-based prolonged exposure. | Certainty (quality) of evidence: Low Strength of recommendation: Conditionalb |
“For adults with PTSD, there was insufficient evidence to make a recommendation on Behavioural Activation and Therapeutic Exposure delivered via telehealth (videoconferencing).” (p. 39)28 Insufficient supporting evidence. Evidence from 1 study; the Guideline Development Group was uncertain if there is a difference between BA and Therapeutic Exposure delivered via telehealth (videoconferencing) vs. in person on PTSD symptom severity. | Certainty (quality) of evidence: Very low Strength of recommendation: NA |
“For adults with PTSD, there was insufficient evidence to make a recommendation on group non–trauma-focused CBT delivered via telehealth (videoconferencing).” (p. 39)28 Insufficient supporting evidence. Evidence from 2 studies with small sample sizes; the Guideline Development Group was uncertain if there is a significant difference between group non–trauma-focused CBT delivered via telehealth (videoconferencing) vs. in person on PTSD symptom severity. | Certainty (quality) of evidence: very low Strength of recommendation: NA |
BA = behavioural activation; CBT = cognitive behavioural therapy; CBT-t = cognitive behavioural therapy with a trauma focus; EMDR = Eye Movement Desensitization and Reprocessing; iCBT = internet-based Cognitive behavioural therapy; NA = not applicable; Phoenix Australia = Phoenix Australia Centre for Posttraumatic Mental Health; PTSD = posttraumatic stress disorder; RCT = randomized controlled trial.
Note: This table has not been copy-edited.
aRefers to the Guideline Development Group.
bThere is lower certainty in the evidence and clinicians should provide the intervention to most people, but not all.
Appendix 5: Overlap Between Included SRs
Please note that this appendix has not been copy-edited.
Table 14: Overlap in Relevant Primary Studies Between Included Systematic Reviews
Primary study citation | Bevilacqua et al. (2024)19 | Kelber et al. (2024)20 | Oliveira Machado et al. (2024)22 | Zandieh et al. (2024) 23 | Laurito et al. (2023)19 | Giovanetti et al. (2022)24 |
|---|---|---|---|---|---|---|
Acierno R, et al. Depress Anxiety. 2016; 33: 415 to 423. | — | Yes | — | — | — | Yes |
Acierno R, et al. Behav Res Ther. 2017; 89: 57 to 65. | — | Yes | — | — | — | Yes |
Acierno R, et al. J Anxiety Disord. 2021; 83: 102461. | — | Yes | — | — | — | — |
Alegría M, et al. Med Care. 2014; 52: 989 to 97. | — | — | — | Yes | — | — |
Andersson G, et al. J Affect Disord. 2013; 151: 986 to 94. | — | — | — | Yes | — | — |
Andrews G, et al. Aust N Z J Psychiatry. 2011; 45: 337 to 40. | — | — | — | Yes | — | — |
Arnedt JT, et al. Sleep. 2021; 44: zsaa136. | — | — | — | — | — | Yes |
Axelsson E, et al. JAMA Psychiatry. 2020; 77: 915 to 24. | — | — | — | Yes | — | — |
Bergström J, et al. BMC Psychiatry. 2010; 10:54. | — | — | — | Yes | — | — |
Bouchard S, et al. J Clin Med. 2022; 11(19): 5924. | — | — | Yes | — | — | — |
Carlbring P, et al. Behav Res Ther. 2005; 43: 1321 to 33. | — | — | — | Yes | — | — |
Choi NG, et al. Depress Anxiety. 2014a; 31: 653 to 61. | — | — | — | Yes | — | — |
Choi NG, et al. Am J Geriatr Psychiatry. 2014b; 22: 263 to 271. | — | — | — | — | — | Yes |
Egede LE, et al. Lancet Psychiatry. 2015; 2: 693 to 701. | — | — | — | Yes | — | Yes |
Frueh BC, et al. J Telemed Telecare. 2007; 13: 142 to 7. | — | Yes | — | Yes | Yes | — |
Glueckauf RL, et al. Rehabil Psychol. 2012; 57: 124 to 39. | — | — | — | Yes | — | — |
Hedman E, et al. PLoS One. 2011; 6: e18001. | — | — | — | Yes | — | — |
Himelhoch S, et al. AIDS Behav. 2013; 17:2756 to 64. | — | — | — | Yes | — | — |
Kenardy JA, et al. J Consult Clin Psychol. 2003; 71: 1068 to 75. | — | — | — | Yes | — | — |
Kheirkhah F, et al. Heliyon. 2023; 9: e15760. | — | — | — | Yes | — | — |
Kiropoulos LA, et al. J Anxiety Disord. 2008; 22: 1273 to 84. | — | — | — | Yes | — | — |
Liu L, et al. J Telemed Telecare. 2020; 26 (9): 507 to 19. | — | Yes | — | Yes | — | Yes |
Lovell K, et al. BMJ. 2006; 333: 883. | — | — | — | Yes | — | — |
Lundström L, et al. JAMA Network Open. 2022; 5: e221967-e. | — | — | — | Yes | — | — |
Luxton DD, et al. J Consult Clin Psychol. 2016; 84(11): 923 to 934. | — | — | Yes | Yes | — | Yes |
Maieritsch KP, et al. J Telemed Telecare. 2016; 22 (4): 238 to 43. | — | Yes | — | Yes | — | Yes |
Milgrom J, et al. J Med Internet Res. 2021; 23:e17185. | — | — | — | Yes | — | — |
Mitchell JE, et al. Behav Res Ther. 2008; 46: 581 to 592. | — | — | — | — | — | Yes |
Mohr DC, et al. JAMA. 2012; 307(21): 2278 to 2285. | — | — | Yes | Yes | — | — |
Morland LA, et al. J Clin. Psychiatry. 2010; 71: 855 to 863. | — | — | — | — | Yes | — |
Morland LA, et al. J Trauma Stress. 2011; 24: 465 to 469. | — | — | — | — | Yes | — |
Morland LA, et al. J Clin Psychiatry. 2014; 75: 470 to 6. | — | Yes | — | Yes | Yes | — |
Morland LA, et al. Depress Anxiety. 2015; 32(11): 811 to 820. | — | Yes | — | — | — | — |
Morland LA, et al. Depress Anxiety. 2020; 37: 346 to 355. | — | Yes | — | — | — | Yes |
Nelson EL, et al. Telemed J E Health. 2003; 9(1): 49 to 55. | Yes | — | Yes | — | — | — |
Peterson AL, et al. BMC Psychiatry. 2022; 41: 22. | — | Yes | — | Yes | — | — |
Stubbings DR, et al. J Med Internet Res. 2013; 15(11): e258. | — | — | Yes | Yes | — | Yes |
Thase ME, et al. Am J Psychiatry. 2018; 175: 242 to 50. | — | — | — | Yes | — | — |
Turner CM, et al. JAACAP. 2014; 53(12): 1298 to 1307.e2. | Yes | — | — | — | — | — |
Wagner B, et al. J Affect Disord. 2014; 152 to 154:113 to 121. | — | — | Yes | Yes | — | — |
Watts S, et al. J Psychother Integration. 2020; 30: 208 to 25. | — | — | — | Yes | — | — |
Ying Y, et al. Psychol Med. 2023; 53: 3932 to 42. | — | — | — | Yes | — | — |
Appendix 6: References of Potential Interest
Please note that this appendix has not been copy-edited.
Previous CDA-AMC Reports
Internet-Delivered Cognitive Behavioural Therapy for Post-traumatic Stress Disorder or Acute Stress Disorder. Ontario Health. Accessed December 9, 2024. https://www.hqontario.ca/evidence-to-improve-care/health-technology-assessment/reviews-and-recommendations/internet-delivered-cognitive-behavioural-therapy-for-post-traumatic-stress-disorder-or-acute-stress-disorder
With Ontario Health
Internet-Delivered Cognitive Behavioural Therapy for Major Depression and Anxiety Disorders. Health Quality Ontario. Accessed December 9, 2024. https://www.hqontario.ca/evidence-to-improve-care/health-technology-assessment/reviews-and-recommendations/internet-delivered-cognitive-behavioural-therapy-for-major-depression-and-anxiety-disorders
With Health Quality Ontario
Additional References
Williams S, Bornstein S. Indigenous Tele-Psychiatry: A Jurisdictional Scan. Newfoundland and Labrador Centre for Applied Health Research. Accessed December 4, 2024. https://www.mun.ca/nlcahr/media/production/memorial/administrative/nl-centre-for-applied-health-research/media-library/chrsp/Indigenous_Telepsychiatry_March2020.pdf
ISSN: 2563-6596
Canada’s Drug Agency (CDA-AMC) is a pan-Canadian health organization. Created and funded by Canada’s federal, provincial, and territorial governments, we’re responsible for driving better coordination, alignment, and public value within Canada’s drug and health technology landscape. We provide Canada’s health system leaders with independent evidence and advice so they can make informed drug, health technology, and health system decisions, and we collaborate with national and international partners to enhance our collective impact.
Disclaimer: CDA-AMC has taken care to ensure that the information in this document was accurate, complete, and up to date when it was published, but does not make any guarantee to that effect. Your use of this information is subject to this disclaimer and the Terms of Use at cda-amc.ca.
The information in this document is made available for informational and educational purposes only and should not be used as a substitute for professional medical advice, the application of clinical judgment in respect of the care of a particular patient, or other professional judgments in any decision-making process. You assume full responsibility for the use of the information and rely on it at your own risk.
CDA-AMC does not endorse any information, drugs, therapies, treatments, products, processes, or services. The views and opinions of third parties published in this document do not necessarily reflect those of CDA-AMC. The copyright and other intellectual property rights in this document are owned by the Canadian Agency for Drugs and Technologies in Health (operating as CDA-AMC) and its licensors.
Questions or requests for information about this report can be directed to Requests@CDA-AMC.ca.