Drugs, Health Technologies, Health Systems
Health Technology Review
Subtalar Joint Arthroereisis
Key Messages
What Is the Issue?
The subtalar joint enables the inversion and eversion of the feet. Excessive movement of the subtalar joint can lead to painful foot conditions that may require surgical treatment in severe cases.
Subtalar joint arthroereisis involves the insertion of an implant that limits excessive movement of the subtalar joint. It is considered a minimally invasive surgical procedure with a relatively fast healing period compared to alternative surgical procedures.
While this procedure is commonly used for children with pes planus, it is becoming a more common treatment for adults with foot conditions. There is uncertainty as to whether subtalar joint arthroereisis can be effective for adults.
What Did We Do?
We conducted a rapid review to identify, summarize, and critically appraise evidence regarding the clinical effectiveness and cost-effectiveness of subtalar joint arthroereisis for adults with pes planus (i.e., flatfoot, plantar fasciitis, and other foot conditions). Additionally, we aimed to identify, summarize, and critically appraise evidence-based guidelines regarding the use of subtalar joint arthroereisis for adults.
An information specialist conducted a customized literature search, balancing comprehensiveness with relevancy, of multiple sources and grey literature on November 20, 2024.
What Did We Find?
We identified 8 relevant studies (1 systematic review and 7 nonrandomized studies) that evaluated the clinical effectiveness of subtalar joint arthroereisis for adults with pes planus. Compared to baseline, the literature suggests that subtalar joint arthroereisis improves key clinical outcomes, such as overall foot and ankle condition, health-related quality of life, and pain relief (1 systematic review and 4 nonrandomized studies). One nonrandomized study found mixed results when comparing subtalar joint arthroereisis to lateral column lengthening for adults living with stage IIb adult-acquired flatfoot deformity.
We also found 2 relevant nonrandomized studies regarding the clinical effectiveness of subtalar joint arthroereisis for adults with other foot conditions (i.e., reducible talotarsal joint dislocation and partial talotarsal joint instability). Compared to baseline, the literature suggests that subtalar joint arthroereisis improves the function of the foot and ankle, pain relief, and ability to perform activities of daily living in the long term for adults with partial talotarsal joint issues (1 nonrandomized study).
For the studies in this report, sinus tarsi pain was the most reported adverse event and the cause of implant removal. Other adverse events included implant revision, surgical infection, stress fractures, insufficient deformity correction, reoccurrence of foot deformity, wound healing issues, and muscle and tendon complications (10 studies).
Overall, there is uncertainty in the identified evidence due to risk of bias and methodological limitations.
We did not identify relevant studies regarding the clinical effectiveness of subtalar joint arthroereisis for adults with plantar fasciitis. We also did not find any relevant cost-effectiveness studies or evidence-based guidelines regarding the use of subtalar joint arthroereisis for adults.
What Does This Mean?
These results should be interpreted with caution. Most studies included in this report were of low-quality and limited to comparing before-and-after outcomes. Additionally, most studies did not account for the impact of confounding variables (e.g., obesity) and heterogeneity within and between treatment arms (e.g., implant sizes, adjunct procedures, and implant type). Comparative evidence from robust studies is needed before definitive conclusions regarding the clinical effectiveness of subtalar joint arthroereisis can be made.
Future studies could consider evaluating the cost-effectiveness of subtalar joint arthroereisis with considerations of the implications of implant removals, as well as the clinical effectiveness of subtalar joint arthroereisis for individuals with plantar fasciitis. Given that subtalar joint arthroereisis is commonly provided in combination with other procedures, future research may also consider evaluating best practices with adjunctive treatments for adults with foot conditions.
Abbreviations
AOFAS
American Orthopaedic Foot & Ankle Society
BMI
body mass index
FADI
Foot and Ankle Disability Index
FAOS
Foot and Ankle Outcome Score
SF-36
Short Form (36) Health Survey
VAS
visual analogue scale
VAS-FA
visual analogue scale – foot and ankle
Research Questions
What is the clinical effectiveness of subtalar joint arthroereisis for adults with plantar fasciitis?
What is the clinical effectiveness of subtalar joint arthroereisis for adults with pes planus?
What is the clinical effectiveness of subtalar joint arthroereisis for adults with other foot conditions?
What is the cost-effectiveness of subtalar joint arthroereisis for adults with plantar fasciitis?
What is the cost-effectiveness of subtalar joint arthroereisis for adults with pes planus?
What is the cost-effectiveness of subtalar joint arthroereisis for adults with other foot conditions?
What are the evidence-based guidelines regarding the use of subtalar joint arthroereisis for adults?
Context and Policy Issues
What Is the Subtalar Joint?
Our feet use a complex mechanical system formed of many bones, joints, muscles, ligaments, and tendons that work together to support all steps of the human gait.1 The foot can be divided into 3 regions: the hindfoot, midfoot, and forefoot.1 In the hindfoot, the subtalar joint articulates the talus bone and calcaneus, and enables the inversion and eversion of the feet.1,2
Inversion, or pronation, refers to when feet roll inwards during motion.3,4 Eversion, or supination, refers to when the foot rolls outward.3 Abnormal eversion and inversion increases the risk of injury and can lead to painful conditions, such as pes planus and plantar fasciitis.3
What Is Pes Planus?
Pes planus involves the loss or absence of the longitudinal arch, which can present in combination with other foot deformities. Individuals with pes planus can be asymptomatic while others may experience pain along their foot.5,6 Other symptoms include difficulties in footwear fitting, as well as impaired gait and function.5,7 Pes planus can be congenital or acquired. In the first few years of life, pes planus is considered physiologically normal unless it is symptomatic.5 Typically, pes planus in childhood spontaneously corrects itself, but in some cases, it may persist through or be acquired during adulthood.5 Risk factors of acquired pes planus include age, obesity, diabetes, hypertension, and trauma.8,9
The severity of pes planus can be categorized into 4 stages: I, II (i.e., type a and type b), III, and IV.10 Stage I, the least severe stage, indicates loss of the longitudinal arch and is typically managed using conservative treatment.10,11 The additional stages increase in pain severity and foot deformity, moving beyond the loss of the longitudinal arch.10,11 Stage II indicates hindfoot deformity with (type b) or without (type a) forefoot abduction and loss of the longitudinal arch.10,11 Stage III indicates a hindfoot deformity, rigid forefoot abduction, and loss of the longitudinal arch.10,11 Stage IV indicates rigid hindfoot valgus, rigid forefoot abduction, deltoid ligament compromise, and loss of the longitudinal arch.10,11 A flexible deformity means the absence of the deformity when there is no weight on the foot, whereas a rigid deformity indicates that the deformity is present regardless of weight on the foot.12
Individuals with symptomatic pes planus will typically start treatment with conservative strategies, such as activity modifications, stretching, and muscle strengthening exercises as well as supportive footwear, orthotics, and over-the-counter pain medications.5,6,13,14 When conservative treatment is ineffective in relieving pain, surgical treatments can be considered, such as lateral column lengthening or Evan’s osteotomy (which involves inserting a bone graft),15 arthrodesis, and other types of osteotomies.5,6,11
What Is Plantar Fasciitis?
Individuals with plantar fasciitis experience inferior heel pain and local point tenderness near the plantar fascia.9,16 The plantar fascia is a band of tissues that connects your heel bone to the base of your toes. It also supports the longitudinal arch of the foot.9,16 It is believed that the etiology of plantar fasciitis is multifactorial.9 Risk factors may include weight and obesity, diabetes, physical trauma, pes planus, and reduced ankle dorsiflexion.9
Individuals with plantar fasciitis most often experience heel pain when initiating walking (e.g., in the morning or after long periods of rest).9,16 In severe cases, individuals may experience pain with any weight-bearing movement.16 Treatments for individuals with plantar fasciitis include avoiding potential triggers, cushioned footwear, and addressing underlying conditions (e.g., symptomatic pes planus).9 For more severe cases, more intensive treatments, such as glucocorticoid injections and surgical options, are available.9
What Is Subtalar Joint Arthroereisis?
Subtalar joint arthroereisis involves the surgical insertion of an implant in the subtalar joint to restore and maintain the physiologic alignment between the talus and calcaneus, while aiming to minimize pain and excessive pronation.4-6 The procedure is reversible, considered minimally invasive, has a relatively fast healing period, and is seen to have lower risks and complications compared to more invasive surgical procedures, such as arthrodesis and osteotomies.4 The procedure can be a standalone treatment or combined with other treatments.5 There are 3 different types of implants used for subtalar joint arthroereisis, including axis-altering prosthesis, impact-blocking devices, and self-locking implants.5 While they differ in design, all 3 types of implants are designed to limit subtalar joint movement.5
Why Is It Important to Do This Review?
The literature suggests that children and adolescents with pes planus benefit from subtalar joint arthroereisis, given their flexible skeletal structure and soft tissues that have yet to reach maturity.13,17 This surgical procedure is becoming a more common treatment for adults, especially for those with pes planus.10 However, there is uncertainty about the benefits and harms, cost-effectiveness, and best practices of subtalar joint arthroereisis in adults with foot conditions.
Objectives
The purpose of this rapid review is to summarize and critically appraise the evidence regarding the clinical effectiveness and cost-effectiveness of subtalar joint arthroereisis for adults with foot conditions, such as pes planus and plantar fasciitis. We also aimed to summarize and critically appraise evidence-based guidelines regarding the use subtalar joint arthroereisis in adults.
Methods
An information specialist conducted a customized literature search, balancing comprehensiveness with relevancy, of multiple sources and grey literature on November 20, 2024. One reviewer screened citations and selected studies based on the inclusion criteria presented in Table 1, and critically appraised included publications using established critical appraisal tools.
Appendix 1 presents a detailed description of methods and selection criteria for included studies.
Criteria | Description |
|---|---|
Population | Adults with plantar fasciitis, pes planus, or other foot conditions |
Intervention | Subtalar joint arthroereisis (may also be referred to as extraosseous talotarsal stabilization) |
Comparator | Q1 to Q6: Standard of care, any treatment, no treatment Q7: Not applicable |
Outcomes | Q1 to Q3: Clinical benefits (e.g., physical activity level, pain, function) and harms (e.g., adverse events) Q4 to Q6: Cost-effectiveness (e.g., cost per quality-adjusted life-year gained) Q7: Recommendations regarding best practices for subtalar joint arthroereisis |
Study designs | Systematic reviews, randomized controlled trials, nonrandomized studies, economic evaluations, evidence-based guidelines |
Publication date | Since January 1, 2014 |
Summary of Evidence
Quantity of Research Available
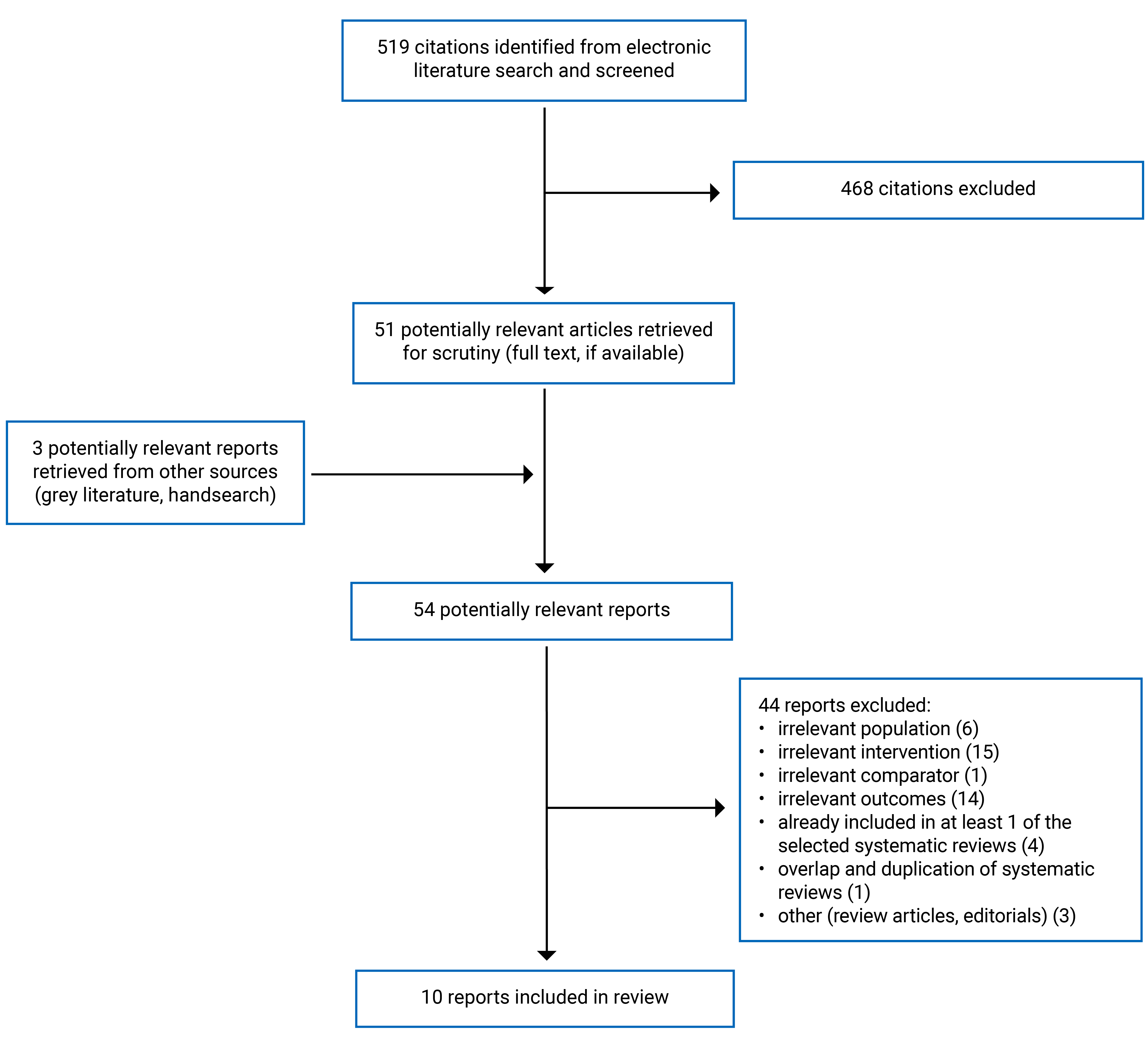
This rapid review includes a total of 10 relevant articles,10,11,13,18-24 specifically 1 systematic review10 and 9 nonrandomized studies.11,13,18-24 Of the 10 studies, 8 articles addressed question 2,10,11,13,19,20,22-24 while 2 articles addressed question 3.18,21
Appendix 1 presents the PRISMA25 flow chart of the study selection. Additional references of potential interest are provided in Appendix 5.
Summary of Study Characteristics
The summary of study characteristics is organized by research question. We did not identify any relevant articles for questions 1, 4, 5, 6, and 7; therefore, no summaries can be provided for these research questions. Additional details regarding the characteristics of included publications are provided in Appendix 2.
Included Studies for Question 2: Clinical Effectiveness of Subtalar Joint Arthroereisis for Pes Planus
We identified a total of 8 relevant articles to question 2, specifically 1 systematic review10 and 7 nonrandomized studies.11,13,19,20,22-24
Systematic Review
The systematic review by Baryeh and colleagues10 was conducted in the UK and published in 2022. The review authors limited the eligibility criteria to nonrandomized studies, specifically cohorts and case series, that focused on adults with adult-acquired flatfoot.10 The review had no search time frame limitations for their search strategy.10 Relevant to this review, they investigated clinical outcomes before-and-after subtalar joint arthroereisis, including both isolated and adjunct procedures.10 Baryeh and colleagues10 reported on the following clinical outcomes:
adverse events
general health and quality of life using the Short Form (36) Health Survey (SF-36)
overall foot and ankle condition using the American Orthopaedic Foot and Ankle Society (AOFAS) score and the Foot and Ankle Outcome Score (FAOS).
Nonrandomized Studies
Of the 7 nonrandomized studies, 2 studies evaluated the clinical effectiveness of subtalar joint arthroereisis and lateral column lengthening for adults with stage IIb adult flatfoot deformity.11,20 Both studies measured clinical outcomes of subtalar joint arthroereisis before and after the procedure, specifically, adverse events, general health and quality of life (i.e., SF-36 score), overall foot and ankle condition (i.e., AOFAS score), and pain (visual analogue scale [VAS] score).11,20 Additionally, both studies were conducted in Singapore.11,20
Silva et al. (2021)11 conducted a retrospective cohort study. They included 72 adults (79 feet) who underwent treatment at a single centre between 2007 and 2013.11 The researchers measured outcomes at 6- and 24-months postprocedure.11 Subtalar joint arthroereisis was an adjunct procedure to Achilles tendon lengthening or gastrocnemius release (dependent on their clinical needs).11 Participants who underwent a lateral column lengthening procedure also underwent a medializing calcaneal osteotomy, distraction osteotomy, flexor digitorum longus transfer, and either Achilles tendon lengthening or gastrocnemius release (dependent on their clinical needs).11 In addition to AOFAS score, SF-36, and VAS, Silva and colleagues11 compared changes in body mass index (BMI) within and between study groups at 24 months postprocedure. For this study, the mean age of individuals who underwent a subtalar joint arthroereisis was 46.3 years old, which did not significantly differ from those in the comparator group.11 Further, individuals who underwent a subtalar joint arthroereisis procedure did not differ in sex and race or ethnicity to individuals who underwent a lateral column lengthening procedure. However, the lateral column lengthening had a statistically significantly higher BMI at baseline compared to the subtalar joint arthroereisis group.11
The study by Fang Junxian and colleagues20 conducted a retrospective study that was published in 2015. They included 22 adults who underwent unilateral surgeries from a single centre.20 All study participants received the same adjunctive procedures regardless of whether they underwent subtalar joint arthroereisis or lateral column lengthening (i.e., gastrocnemius recession, tibialis posterior insertion site debridement, and a calcaneal osteotomy).20 Fang Junxian and colleagues20 compared clinical outcomes at baseline and at follow-up at a minimum of 12 months postprocedure. For this study, the mean age of individuals who underwent a subtalar joint arthroereisis was 52.7 years old.20 The study groups were comparable in age and sex.20 While the study compared before-and-after outcomes for each treatment arm, the researchers did not conduct any statistical tests to compare the before-and-after scores between subtalar joint arthroereisis and lateral column lengthening.20
The remaining 5 nonrandomized studies relevant to question 2 compared the clinical effectiveness of subtalar joint arthroereisis from baseline.13,19,20,22-24 Of which, 3 studies13,19,24 measured adverse events postprocedure as clinical outcomes relevant to this review. Fu et al. (2024)13 conducted their study in a hospital in Shanghai, and analyzed data of individuals who did not respond to 6 months of conservative treatment with no age limits.13 Of 732 study participants, 223 were adults (i.e., the relevant population for this report).13 Most adults (92.4%) in this study underwent an adjunct subtalar joint arthroereisis.13 Saxena and colleagues24 conducted a prospective study on 41 adults with symptomatic flexible pes planus in Poland.24 The mean age of the study population was 53.3 years.24 They measured the adverse events, specifically implant removals.24 The study population had a mean follow-up of 6.5 years.24 Bernasconi et al. (2022) conducted a single-centre, retrospective study in the UK.19 They analyzed data from 21 adults (22 feet) with stage IIb adult-acquired flexible flatfoot deformity. For inclusion, adults must have follow-up data regarding adverse events at least 6 months postprocedure.19 In addition to subtalar joint arthroereisis, study participants underwent medializing calcaneal osteotomy, flexor digitorum longus transfer, and spring ligament repair with or without cotton osteotomy.19 The mean age of adults included in the study was 55.2 years old.19
Lewis et al. (2024)22 and Ozan et al. (2015)23 evaluated the impact of subtalar joint arthroereisis using a single centre, before-and-after study design. Lewis and colleagues22 conducted a retrospective study involving 187 adults (212 feet) with Stage I pes planus who did not respond to 6 months of conservative treatment.22 The mean age of study participants was 59.7 years, and the mean follow-up was 2.5 years.22 The researchers compared postprocedure results from baseline, specifically foot and ankle condition using FAOS score and Foot and Ankle Disability Index (FADI), and quality of life using the EQ-5D-5L.22 Lewis and colleagues22 also measured adverse events (i.e., implant removal rate).22 The study by Ozan and colleagues23 compared the before-and-after outcomes of isolated subtalar joint arthroereisis on 16 adults (26 feet) with symptomatic flexible pes planus, specifically foot and ankle condition (i.e., AOFAS score) and pain (i.e., VAS score). The mean age was 24.5 years, and the mean follow-up is 15.1 months.23
Included Studies for Question 3: Clinical Effectiveness of Subtalar Joint Arthroereisis for Other Foot Conditions
Nonrandomized Studies
We identified 2 nonrandomized studies published in 2023 relevant to question 3.18,21
Kolodziej and colleagues21 conducted a single-centre, prospective, before-and-after study to evaluate the clinical effectiveness of extraosseous talotarsal stabilization (with the HyProCure implant) for adults with partial talotarsal joint instability. They included 41 adults (62 feet) who received the HyProCure implant from a surgical department in Poland between 2012 to 2015.21 The mean age of participants was 46.4 years.21 They measured the impact of extraosseous talotarsal stabilization on activity (i.e., the UCLA activity score, symptom-related activity scale score), function (i.e., Lower Extremity Functional Scale score), ability to partake in sports and exercise (i.e., sports frequency score, number of physical activity, and time on physical activity), and pain (i.e., VAS). The mean follow-up for study participants was 8.6 years.21
Agnew and colleagues18 conducted a multicentre, retrospective, before-and-after study in the US.18 Relevant to this review, they analyzed adverse event data (i.e., implant revision and implant removal rates) from 67 individuals who had subtalar joint arthroereisis, of which 53 (79.1%) were adults, with symptomatic talotarsal joint dislocation.18 These adults received a standalone type II extraosseous talotarsal stabilization implant (HyProCure).18 The median age is 41 years (ranging from 20 to 74 years). The mean follow-up was 7 years, 8 months, and 19 days.18
Summary of Critical Appraisal
Critical appraisal summaries are organized by research questions followed by study design. Additional details regarding the strengths and limitations of included publications are provided in Appendix 3.
Clinical Effectiveness Literature on Adults With Pes Planus (Question 2)
Systematic Review
Overall, the systematic review by Baryeh et al.10 lacks rigour and is at a high risk of selection bias. The review authors did not describe established methods before its conduct or rationale for limiting their eligibility to case series and cohort studies. While Baryeh and colleagues10 conducted a risk of bias assessment, they did not discuss or address the implications of their evidence assessment findings in their results and discussion. The review authors assessed some primary studies in their review as “some risk of bias” and “high risk of bias” in the areas of selection bias, performance bias, attrition bias, and detection bias of their assessment tool.10 The findings could be misleading without a clear explanation of how they should be interpreted.
Moreover, the review authors limited inclusion to before-and-after studies.10 Given the nature of before-and-after study designs, individual studies do not consider confounding variables, which may have implications for their results. Baryeh and colleagues10 reported averages of relevant outcomes across included studies without performing a meta-analysis. Thus, these averages did not account for heterogeneity and effect sizes. Additionally, Baryeh and colleagues10 did not conduct any tests for publication bias, and they did not state an intent to investigate sources of funding for included studies. It is unclear how confounding variables, bias, and funding may have affected the findings of their review.
Nonrandomized Studies
For question 2, all relevant nonrandomized studies clearly described the study objective and the main outcomes of interest.11,13,19,20,22-24 Additionally, 5 studies detailed their inclusion and exclusion criteria,11,13,19,22,24 and 2 studies did not.20,23 Saxena and colleagues24 did not describe the surgical process, unlike the other nonrandomized studies.
The included nonrandomized studies were mostly limited to before-and-after comparisons without comparative evidence against an alternative treatment.19,20,22-24 Considering the nature of the included nonrandomized studies, this study design is at a greater risk of threats to internal validity, whereas a control group would have limited such threats. In addition, there are further internal validity concerns given that the investigators did not report whether they concealed treatment to researchers or study participants.11,13,19,20,22-24 There was a minimal consideration of confounding variables and considerable heterogeneity across the studies and treatment arms within these studies.11,13,19,20,22-24 For example, most studies differed in adjunct procedures, implant types, and implant sizes within study arms.11,13,19,20,22,24 In addition, some studies included both isolated and adjunct procedures under the same treatment group.13,24
It appears that all nonrandomized studies used appropriate statistical methods and outcome measures.11,13,19,20,22-24 However, the Lewis et al. study22 used multiple outcome measures to assess foot condition, specifically pain and activity levels.22 Their statistical analysis did not adjust for multiplicity,22 and it increases the likelihood of favourable outcomes. Additionally, Lewis and colleagues22 conducted unplanned comparative analysis to evaluate the impact of age and operative FAOS, FADI, and EQ-5D-5L scores on implant removal.
All nonrandomized studies for question 2 provided little to no description of individuals lost to follow-up or those excluded.11,13,19,20,22-24 It is unclear how these individuals may have impacted their findings. The studies conducted by Silva et al.11 and Bernasconi et al.19 were adequately powered. The other nonrandomized studies that conducted statistical testing for outcome measures relevant for this report did not report whether they were adequately powered.13,20,22-24
Two studies measured the impact of subtalar joint arthroereisis and lateral column lengthening over the time intended for comparison.11,20 The study by Fang Junxian et al.20 did not use statistical methods to compare these 2 treatments. It is unclear if the subtalar joint arthroereisis and lateral column lengthening were comparable at baseline or if there was a clinically meaningful difference postprocedure. The same study provided minimal details about how they recruited the study population.20 Hence, it is unclear how selection bias may have impacted their findings. Additionally, the study by Silva et al.11 did not report their funding source. It is unclear if funding may have influenced their findings.
None of the nonrandomized studies for question 2 were conducted in Canada. Some studies provided minimal descriptions of their recruitment process.20,23,24 For these studies, it is unclear as to whether their study population is representative of their source population. It is also unclear how generalizable these studies are to other health settings, including those in Canada.
Clinical Effectiveness Literature on Adults With Other Foot Conditions (Question 3)
Nonrandomized Studies
The nonrandomized studies clearly described the researchers’ hypothesis, outcomes of interest, the intervention of interest, and main findings.18,21 When applicable, the researchers of both studies provided estimated of random variability and P values.18,21 Both studies reported no conflicts of interest for authors and no funding sources that may have introduced bias and affected the reporting of study findings.18,21
The included nonrandomized studies were limited to before-and-after comparisons without comparative evidence against an alternative treatment.18,21 Additionally, individuals involved in the study and participants had knowledge of the intervention. Both studies lack consideration of confounding variables that may have affected the findings of the study.18,21 For both studies, the researchers did not describe individuals excluded from the study due to lack of follow-up data.18,21 It is also unclear how excluded individuals differ from study participants, and how they may have affected the results. Hence, it is unclear to what extent the results can be attributed to the subtalar joint arthroereisis alone.
The study by Kolodziej and colleagues25 used a variety of outcome measures to evaluate the impact of the intervention on function and activities of daily living. By using multiple outcome measures, the researchers may have increased the risk of finding a significant result.
Both studies were conducted outside of Canada.18,21 It is unclear as to how their treatment facilities differ from health settings in Canada, and how applicable these findings are to adults living in Canada with foot conditions.
Summary of Findings
We summarized the results of relevant studies regarding the clinical effectiveness of subtalar joint arthroereisis for pes planus (question 2) and other foot conditions (question 3). No relevant evidence regarding the subtalar joint arthroereisis for plantar fasciitis was identified; therefore, no summary can be provided for question 1. Additionally, we did not find relevant economic evaluations or evidence-based guidelines; therefore, no summary of findings can be provided for questions 4 to 7.
Appendix 4 presents additional details regarding the main study findings.
Clinical Effectiveness of Subtalar Arthroereisis for Pes Planus (Before-and-After Outcomes)
Foot and Ankle Condition
The systematic review by Baryeh and colleagues10 found that subtalar joint arthroereisis improved AOFAS scores for adults with pes planus compared to baseline (P value not reported). These findings align with the Fang Junxian et al.20 and Ozan et al.23 studies, which reported a statistically significant improvement in AOFAS scores from baseline.
The systematic review by Baryeh and colleagues10 also reported that subtalar joint arthroereisis significantly improved total FAOS scores for adults with pes planus compared to baseline.
Health-Related Quality of Life
The study by Lewis and colleagues22 found a statistically significant improvement in EQ-5D-5L in adults who underwent a subtalar joint arthroereisis compared to baseline scores.
Pain
Compared to baseline, all studies that included the reporting of pain outcomes found a statistically significant decrease in pain due to pes planus after subtalar joint athroereisis.10,22,23 However, some studies reported that subtalar joint arthroereisis caused pain postprocedure, including sinus tarsi pain and complex regional pain syndrome.10,13,19 The prevalence of pain because of the procedure ranged from 0.6% to 57.1% of adults with pes planus.10,13,19
Symptoms
Lewis and colleagues also found an improvement of symptoms after subtalar joint arthroereisis for adults with pes plenus.22 They measured and reported pain scores separately using a subcomponent of FAOS.22
Activities of Daily Living or Activity
The study by Lewis and colleagues found a statistically significant improvement in the ability to partake in activities for adults with pes planus after subtalar joint arthroereisis (as measured by a subcomponent of the FADI).22 The same study found a statistically significant improvement in the ability to perform activities of daily living, as measured by a FAOS subcomponent.22
Adverse Events
Implant Removal and Revision
The prevalence of implant removals among adults with pes planus who underwent a subtalar joint arthroereisis varied across studies. It ranged from 7.6% to 48.1% of study participants.10,13,19,22-24 Most studies reported sinus tarsi pain as the most common cause of implant removals for this population.10,13,19,22 The study by Fu and colleagues reported that all individuals who had their implants removed experienced pain relief.13
Other Adverse Events and Complications
Studies reported adverse events and complications beyond pain and implant removals after subtalar joint arthroereisis for adults with pes planus. They reported the following complications:
surgical infection (2 studies with rates ranging from 0.6% to 10% of study participants)10
stress fracture (0.6% of feet from 1 systematic review)10
insufficient foot correction (0.6% of feet from 1 systematic review)10
recurrence of deformity (0.6% of feet from 1 systematic review and 3.8% of feet in a nonrandomized study)10
Achilles tendon tension (0.85% of feet from 1 study)13
peroneal spasm (0.85% of feet from 1 study)13
wound healing issues (0.42% of cases from 1 study)13
foreign body sensations (0.42% of cases from 2 study).13
Clinical Effectiveness of Subtalar Joint Arthroereisis Versus Lateral Column Lengthening for Pes Planus
Of note, the Fang Junxian et al. study20 does not use statistical methods to compare before-and-after scores between lateral column lengthening and subtalar joint arthroereisis (refer to Table 7 for further study results).20
Foot and Ankle Condition
The study by Fang Junxian and colleagues20 found subtalar joint arthroereisis and lateral column lengthening significantly improved the condition of the foot and ankle. Both procedures resulted in a statistically significant increase in AOFAS scores at follow-up compared to baseline.20 Silva and colleagues11 found that subtalar joint arthroereisis and lateral column lengthening increased AOFAS scores for the hindfoot and midfoot area at 6 and 24 months. Lateral column lengthening resulted in a statistically significant increase in AOFAS scores for the hindfoot area compared to subtalar joint arthroereisis at 24 months, which suggests that lateral column lengthening may result in greater sustained improvements in the hindfoot.11 The authors did not find any significant differences between groups for AOFAS scores for all other comparisons (i.e., hindfoot at 6 or 24 months, midfoot at 6 months).
General Health
Fang Junxian and colleagues20 found a statistically significant increase in the SF-36 general health subscale scores for subtalar joint arthroereisis and lateral column lengthening compared to baseline. These findings suggest that both procedures may improve overall health.20
Physical Health
Fang Junxian and colleagues20 reported a statistically significant increase in physical function and role limitation (physical health) subscale scores of the SF-36 compared to baseline. Additionally, the study by Silva and colleagues11 found an increase physical component summary of the SF-36 for subtalar joint arthroereisis and lateral column lengthening with no difference when comparing scores between treatments.11 These results suggest that both procedures may improve physical health for people with stage IIb adult-acquired flatfoot.
Mental Health
Silva and colleagues11 found an increase in SF-36 mental health component summary scores after subtalar joint arthroereisis and lateral column lengthening compared to baseline. However, there were no clinically meaningful differences between the treatments.11 The study by Fang Junxian and colleagues20 found a statistically significant increase in role limitation (emotional problems, subscale of SF-36) but no significant differences for emotional well-being (subscale of the SF-36) after subtalar joint arthroereisis compared to baseline.
Social Function
The study by Fang Junxian and colleagues20 reported an increase in the SF-36’s social functioning subscale scores after lateral column lengthening and subtalar joint arthroereisis compared to baseline. These findings suggest that both procedures can improve social function for people with stage IIb adult-acquired flatfoot.20
Energy
Fang Junxian and colleagues20 reported a statistically significant increase in the SF-36 energy and fatigue subscale scores for subtalar joint arthroereisis and lateral column lengthening compared to baseline, which suggests both procedures can improve energy for people with stage IIb adult-acquired flatfoot.20
Pain
Fang Junxian and colleagues20 found that, compared to baseline, both subtalar joint arthroereisis and lateral column lengthening significantly decreased pain caused by stage II adult-acquired flatfoot.20 Lateral column lengthening and subtalar joint arthroereisis resulted in a statistically significant increase in SF-36 pain scores and a statistically significant decrease in VAS scores postprocedure compared to baseline.20
Silva and colleagues11 found an improvement in VAS for midfoot and hindfoot pain, compared to baseline, in subtalar joint arthroereisis and lateral column lengthening groups at 6 and 24 months.11 Compared to baseline, they found decreased VAS scores for the midfoot and hindfoot.11 Lateral column lengthening resulted in statistically significantly lower midfoot VAS compared to subtalar joint arthroereisis at 24-months follow-up, but not 6-months follow-up. This suggests that lateral column lengthening results in better sustained pain relief in midfoot area.11 However, there were no statistically significant differences between groups for the hindfoot area for either follow-up period.
Adverse Events
The Silva et al. study11 found the lateral column lengthening group had fewer complications (4.4%, n = 2) than the subtalar joint arthroereisis group (20.6%, n = 7). For the lateral column lengthening group, the adverse events reported included wound breakdown and sural nerve entrapment. For subtalar joint arthroereisis, all implant removals were due to midfoot pain.11 Silva and colleagues11 reported that correction of flatfoot was maintained at 24 months despite removal. Fang Junxian and colleagues20 found that lateral column lengthening group had no implant removals (i.e., bone graft); whereas the subtalar joint arthroereisis group had 4 (33.3% of participants in this study group) implant removals.
Body Mass Index
Silva and colleagues11 found there was a statistically significant reduction in BMI for the lateral column lengthening group at 24 months postprocedure but not for the subtalar joint arthroereisis group.11 Of note, individuals in the lateral column lengthening arm of the study had a significantly higher BMI at baseline than individuals who underwent a subtalar joint arthroereisis. Silva and colleagues11 hypothesized that the lower complication rate in the lateral column lengthening allowed for reduced hospital stays and, thus, an earlier return to an active lifestyle.
Clinical Effectiveness of Subtalar Joint Arthroereisis for Talotarsal Joint Issues (Before-and-after Outcomes)
The study by Kolodziej and colleagues21 measured clinical outcomes, which are summarized in detail in Table 8. Relevant to this report, Agnew and colleagues18 reported adverse events (Table 9).
Function and Activities of Daily Living
Kolodziej and colleagues21 assessed the function of the foot and ankle, and activities of daily living before and after the subtalar joint arthroereisis using the UCLA activity score, Symptom-Related Activity Scale, and the Lower Extremity Functional Scale. The results were mixed: the Symptom-Related Ankle Activity Scale and Lower Extremity Functional Scale outcome measures showed a statistically significant improvement from baseline, whereas the UCLA activity score did not.21
Sports and Exercise
Compared to baseline, Kolodziej et al.21 did not find any statistically significant differences for participants after subtalar joint arthroereisis regarding sport frequency score and number of physical activities.
Pain
Subtalar joint arthroereisis resulted in statistically significant reduction of pain caused by partial talotarsal joint instability in the long-term, as indicated by the lower mean VAS after the procedure.21
Adverse Events
Overall, Kolodziej et al. (2023)21 reported 2 minor complications (4.9%) from subtalar joint arthroereisis.21 One participant experienced persistent pain that limited their activities, and another participant experienced wound healing issues that self-resolved without negatively affecting activity and function. None of the participants had their implants removed.21
Agnew and colleagues18 reported that 8 (15.1%) implants in their study experienced ongoing device issues. Within this category, they included a broad range of adverse events and complications, such as pain, stiffness, general discomfort, and ankle disability, that occurred postprocedure.18 Additionally, 3 (4.5%) implants needed device revision surgery.18 Of which, 2 implants from 1 adult (a bilateral case) received incorrect implant sizes; whereas the remaining case needed revision surgery as the patient believed their improvement had plateaued.18
Limitations
Limited Comparative Studies and Poor-Quality Evidence
Most studies in this report evaluated the clinical effectiveness of subtalar joint arthroereisis for adults with pes planus and talotarsal joint issues using before-and-after outcomes.10,13,18,19,21-24 Most studies lacked comparative evidence against an alternative treatment, randomization of study participants, detailed description of individuals lost to follow-up or excluded from the study, and consideration of confounding variables.10,13,18-24 It is possible that subtalar joint arthroereisis may have contributed to the positive findings of these studies, but the extent to which it can be attributed to the procedure alone remains unclear.
Adjunct Procedures With Subtalar Joint Arthroereisis
The nonrandomized studies conducted subtalar joint arthroereisis with other adjunct procedures for adults with indications of interest,11,13,19,20,22 except for 2 studies.18,21 Across these studies, adjunct procedures that may have been performed with subtalar joint arthroereisis include medializing calcaneal osteotomy, flexor digitorum longus, Achilles tendon lengthening, gastrocnemius release, tibialis posterior insertion site debridement, and other types of surgical procedures.10,11,13,19,22,24 Some procedures were performed at the discretion of clinicians, dependent on clinical needs.11,13,19,22,24 However, most nonrandomized studies did not account for the variations in procedures when applicable.11,13,19,22,24 Additionally, 1 systematic review reported that the heterogeneity of adjunct procedures across included studies was a limitation of their review.10
Two nonrandomized studies evaluated the clinical effectiveness of subtalar joint arthroereisis in insolation,18,21 with 1 study that reported on 1 relevant outcome for this report (i.e., adverse events).18 These 2 studies provided limited insight into the procedure's clinical effectiveness for pes planus, and may be influenced by other factors, such as the staff (i.e., surgeons) and staff experience at facilities. Moreover, there are some concerns for risk of bias for both studies, including threats to both internal and external validity, and these methodological limitations restrict the potential to understand the true effects of isolated subtalar joint arthroereisis for adults with indications of interest.
Types of Implant and Implant Sizes for Subtalar Joint Arthroereisis
In addition to the adjunct procedures used, participants across studies may have differed in the type of implant and implant size used for subtalar joint arthroereisis. Of the 7 included nonrandomized studies, 4 used HyProCure implants.11,13,18,21 The remaining nonrandomized studies did not specify the type of implant used for subtalar joint arthroereisis.19,20,22 The systematic review by Baryeh and colleagues found that the studies included in their review varied widely in implant type.10 It is unclear how the implant type may have affected the results.
Lack of Evidence for Adults With Plantar Fasciitis
We did not identify any studies regarding the clinical effectiveness of subtalar joint arthroereisis for adults with plantar fasciitis. Hence, it is unclear how effective subtalar joint arthroereisis is for this subpopulation.
Lack of Relevant Economic Evaluations and Guidelines
We did not identify any economic evaluations and evidence-based guidelines that met this report’s eligibility criteria. Hence, it is unclear whether performing subtalar joint arthroereisis is cost-effective for adults with plantar fasciitis, pes planus, and other foot conditions. Additionally, the standard and best practices to perform subtalar joint arthroereisis for adults with foot conditions remains unclear.
External Validity
All studies in this report were conducted outside of Canada. Most studies performed specific procedures at a single facility.11,13,19,20,22 It is unclear how these treatments and contexts align with facilities in Canada and how they apply to adults with pes planus or partial talotarsal joint instability living in Canada.
Additionally, most studies evaluated the clinical effectiveness of subtalar joint arthroereisis on adults with stage IIb adult-acquired flatfoot. It is unclear how generalizable these findings are to other stages of pes planus.
Conclusions and Implications for Decision- or Policy-Making
Summary of Evidence
Subtalar joint arthroereisis involves surgically inserting an implant to limit excessive movement of the subtalar joint that may cause painful foot conditions.4-6 We conducted a rapid review of the evidence on the clinical effectiveness and cost-effectiveness of subtalar joint arthroereisis for adults with foot conditions (e.g., plantar fasciitis, pes planus). We also searched for guidelines with recommendations for these populations. We identified 1 systematic review and 9 nonrandomized studies relevant to this report. Most of the evidence extracted from the included studies was from before-and-after study designs, which limits our ability to provide strong conclusions for questions where literature was identified.
Overall, the literature suggests that subtalar joint arthroereisis may provide adults with pes planus and flexible or reducible talotarsal dislocation with some clinical benefits over time. We did not identify any studies on adults with plantar fasciitis. Pain was a complication postprocedure and a common reason for implant removal. Rates of implant removal varied across studies, ranging from 0% to 48.1% of cases.10,11,13,19-21 Other adverse events reported in the identified literature include device revision (the need for),10 surgical infection,10 stress fracture,10 insufficient deformity correction,10 reoccurrence of foot deformity,13,21 wound healing issues,10 and muscle and tendon complications.10,11,13,19,20,22
We found 8 relevant studies that evaluated the clinical effectiveness of subtalar joint arthroereisis for adults with pes planus (question 2).10,11,13,19,20,22-24 The findings suggest that, compared to baseline, subtalar joint arthroereisis improves overall foot and ankle condition,22 function (overall, physical, social),20 energy,20 health-related quality of life,22 symptoms,22 pain,10,20,22 and ability to perform activities of daily living22 for adults with pes planus. One comparative study found mixed results when comparing lateral column lengthening to subtalar joint arthroereisis procedures: the findings varied depending on the outcome, duration of follow-up, and aspect of the foot involved (i.e., midfoot versus hindfoot).11
We also identified 2 relevant studies that evaluated the clinical effectiveness of subtalar joint arthroereisis for adults with flexible or reducible talotarsal joint dislocation (question 3).18,21 Compared to baseline, subtalar joint arthroereisis may improve function of the foot and ankle as well as pain outcomes.18
Considerations for Interpreting Evidence
These results should be interpreted with caution. The included systematic review lacked methodological rigour, given the absence of established methods before conduct, detailed reporting of processes, and consideration of risk of bias in reporting results.
The nonrandomized studies were mostly limited to comparing before-and-after clinical outcomes. Given the nature of these study designs, they are at high risk for internal bias (e.g., absence of randomization). Of the 9 nonrandomized studies, 6 studies11,13,19,20,22,24 evaluated adjunct subtalar joint arthroereisis or had a portion of their study population consisting of adjunct subtalar joint arthroereisis. The systematic review also discussed the amount of heterogeneity in the included studies regarding adjunct procedures.10 However, this may be consistent with how subtalar joint arthroereisis is used in clinical practice: the procedure is seldom performed in isolation, especially for adults.13,26 Moreover, the American College of Foot and Ankle Surgeons found limited evidence that demonstrates the effectiveness of isolated subtalar joint arthroereisis for a stage IIb adult-acquired flatfoot deformity during the development of their consensus statements on the clinical management of pes planus.17 Some literature suggests that isolated subtalar joint arthroereisis may be less successful in adults because their feet have matured and are less adaptable compared to the feet of children and adolescents.13,17 Interestingly, the Agnew et al.18 study included in this rapid review found no differences in outcomes between adults and children with talotarsal joint dislocation.
There was little to no consideration of confounding variables in the analysis or interpretation of findings for most studies in this review. For example, the literature suggests that obesity can increase the risk of sinus tarsi pain postprocedure in adults with pes planus.13 Most studies in this report did not account for such factors in their analysis or report the demographics of their study population. The true clinical effects of subtalar joint arthroereisis remains unclear without accounting for confounding factors that may have influenced results. Additionally, high heterogeneity across studies, beyond adjunct procedure, may have also affected the findings. For example, the sizes and types of implants specific for subtalar joint arthroereisis varied within and across some studies. There is some literature to suggest that implant size and implant type can impact the success of subtalar joint arthroereisis.5,27,28 Given the complexity of foot biomechanics, some researchers have begun evaluating the potential for customized implants as a potential solution to address the consequences of implant mismatch using computerized models.28
Clinical Implications and Considerations for Future Research
This rapid review may be used to understand how subtalar joint arthroereisis has been evaluated in the adult population. However, none of the studies in this report were conducted in Canada; therefore, it is unclear how generalizable these results are to health settings in Canada. In addition, robust and high-quality randomized studies are still needed to draw conclusions about the clinical effectiveness of subtalar joint arthroereisis in practice, especially studies that compare the intervention against a comparator, control for heterogeneity, and account for confounding variables. Future studies may ensure both treatment arms receive similar adjunct procedures and account for confounding variables, such as obesity, implant types, and implant size, in their analysis.
We did not identify any economic evaluations regarding subtalar joint arthroereisis. Bernasconi and colleagues19 raised concerns about the potential financial burden of implant removals, which can cost as much as the implant itself. Future economic evaluations may consider implant removals when developing their models. We also did not identify any evidence-based guidelines regarding subtalar joint arthroereisis. Hence, there is a gap in the literature about best practices and treatment standards when using subtalar joint arthroereisis as treatment for adult foot conditions. Future studies may wish to consider evaluating best adjunctive treatments with subtalar joint arthroereisis for adults with pes planus given that it is typically given in combination with other treatments in clinical practice.
References
1.Managanaro D, Dollinger B, Nezwek TA, Sadiq NM. Anatomy, Bony Pelvis and Lower Limb, Foot joints. StatPearls; 2023. Accessed January 13 2025. https://www.ncbi.nlm.nih.gov/books/NBK536941/#:~:text=The%20specific%20intertarsal%20joints%20of,joint%2C%20and%20the%20intercuneiform%20joint.
2.Krahenbuhl N, Horn-Lang T, Hintermann B, Knupp M. The subtalar joint: A complex mechanism. EFORT Open Rev. 2017;2(7):309-316. doi:10.1302/2058-5241.2.160050 PubMed
3.New York Bone & Joint Specialists. A podiatrist's guide to pronation versus supination. Accessed January 13 2025, https://nyboneandjoint.com/a-podiatrists-guide-to-foot-pronation-vs-supination/#:~:text=Whereas%20pronation%20refers%20to%20an,ankle%20to%20roll%20or%20sprain.
4.Ghali A, Mhapankar A, Momtaz D, Driggs B, Thabet AM, Abdelgawad A. Arthroereisis: Treatment of Pes Planus. Cureus. 2022;14(1):e21003. doi:10.7759/cureus.21003 PubMed
5.Bernasconi A, Lintz F, Sadile F. The role of arthroereisis of the subtalar joint for flatfoot in children and adults. EFORT Open Rev. 2017;2(11):438-446. doi:10.1302/2058-5241.2.170009 PubMed
6.Ortiz CA, Wagner E, Wagner P. Arthroereisis: What Have We Learned? Foot Ankle Clin. 2018;23(3):415-434. doi:10.1016/j.fcl.2018.04.010 PubMed
7.Toullec E. Adult flatfoot. Orthop Traumatol Surg Res. 2015;101(1 Suppl):S11-7. doi:10.1016/j.otsr.2014.07.030 PubMed
8.Knapp PW, Constant D. Posterior Tibial Tendon Dysfunction. StatPearls; 2024. Accessed January 15 2025. https://www.ncbi.nlm.nih.gov/books/NBK542160/
9.Buchbinder R. Post TW, ed. Plantar Fasciitis. UpToDate; 2024. Accessed January 13 2025. https://www.uptodate.com/contents/plantar-fasciitis/print?search=flatfoot&source=search_result&selectedTitle=6%7E82&usage_type=default&display_ra%E2%80%A6
10.Baryeh KW, Ismail H, Sobti A, Harb Z. Outcomes Following the Use of Subtalar Arthroereisis in the Correction of Adult Acquired Flatfoot: A Systematic Review. Foot ankle spec. 2022;15(4):384-393. doi:10.1177/1938640020987775 PubMed
11.Silva M, Koh DTS, Tay KS, Koo KOT, Singh IR. Lateral column osteotomy versus subtalar arthroereisis in the correction of Grade IIB adult acquired flatfoot deformity: A clinical and radiological follow-up at 24 months. J Foot Ankle Surg. 2021;27(5):559-566. doi:10.1016/j.fas.2020.07.010 PubMed
12.Atik A, Ozyurek S. Flexible flatfoot. North Clin Istanb. 2014;1(1):57-64. doi:10.14744/nci.2014.29292 PubMed
13.Fu S, Wu C, Wang C, Wang J, Shi Z. HyProCure for Flatfoot Deformity: A Clinical Characteristics Analysis in China. Orthopaedic Audio Synopsis Continuing Medical Education [Sound Recording]. 2024;06:06. doi:10.1111/os.14285
14.Stichnoth M, Luders KA, Hell AK, Stinus H. Comparative study of subtalar arthroereisis, medializing calcaneal osteotomy and the combination of both techniques for the treatment of symptomatic adult flatfeet. J Foot Ankle Surg. 2024;29:29. doi:10.1016/j.fas.2024.10.006 PubMed
15.BC Children's Hospital. Calcaneal (Lateral column lengthening). Accessed January 27 2025, http://www.bcchildrens.ca/our-services/clinics/orthopaedics/orthopaedic-cerebral-palsy/lower-extremity-surgery/calcaneal-lengthening-lateral-column-lengthening
16.Government of Canada. Plantar Fasciitis. Accessed November 29 2024, https://www.veterans.gc.ca/en/mental-and-physical-health/mental-health-and-wellness/compensation-illness-or-injury/disability-benefits/entitlement-eligibility-guidelines/az-index/plantar-fasciitis
17.Piraino JA, Theodoulou MH, Ortiz J, et al. American College of Foot and Ankle Surgeons Clinical Consensus Statement: Appropriate Clinical Management of Adult-Acquired Flatfoot Deformity. J Foot Ankle Surg. 2020;59(2):347-355. doi:10.1053/j.jfas.2019.09.001 PubMed
18.Agnew PS, Foster JD, Chariton J, et al. Clinical Outcomes Following Treatment of Recurrent Talotarsal Joint Dislocation Using a Type II Extraosseous Talotarsal Stabilization Implant-A Long-Term Follow-Up Study. J Foot Ankle Surg. 2023;62(5):877-882. doi:10.1053/j.jfas.2023.06.001 PubMed
19.Bernasconi A, Argyropoulos M, Patel S, et al. Subtalar Arthroereisis as an Adjunct Procedure Improves Forefoot Abduction in Stage IIb Adult-Acquired Flatfoot Deformity. Foot ankle spec. 2022;15(3):209-220. doi:10.1177/1938640020951031 PubMed
20.Fang Junxian C, Kunnasegaran R, Thevendran G. Surgical Management of Symptomatic Adult Pes Planovalgus Secondary to Stage 2B Posterior Tibial Tendon Dysfunction: A Comparison of Two Different Surgical Treatments. Indian J Orthop. 2020;54(1):22-30. doi:10.1007/s43465-019-00011-7 PubMed
21.Kolodziej L, Ciechanowicz D, Wojtowicz M, et al. Prospective, Long-Term Functional Outcomes of Extra-Osseous Talotarsal Stabilization (EOTTS) Using HyProCure in Adult Patients with Talotarsal Joint Instability: Assessment of Physical Activity and Patient Satisfaction. J Clin Med. 2023;12(14):24. doi:10.3390/jcm12144872 PubMed
22.Lewis TL, Goff TAJ, Ray R, Dhaliwal J, Carmody D, Wines AP. Clinical outcomes of subtalar arthroereisis for the treatment of stage 1 flexible progressive collapsing foot deformity. Eur J Orthop Surg Traumatol. 2024;34(6):2933-2940. doi:10.1007/s00590-024-04007-4 PubMed
23.Ozan F, Dogar F, Gencer K, et al. Symptomatic flexible flatfoot in adults: subtalar arthroereisis. Ther Clin Risk Manag. 2015;11:1597-602. doi:10.2147/TCRM.S90649 PubMed
24.Saxena A, Via AG, Maffulli N, Chiu H. Subtalar Arthroereisis Implant Removal in Adults: A Prospective Study of 100 Patients. J Foot Ankle Surg. 2016;55(3):500-3. doi:10.1053/j.jfas.2015.12.005 PubMed
25.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
26.Mattesi L, Ancelin D, Severyns MP. Is subtalar arthroereisis a good procedure in adult-acquired flatfoot? A systematic review of the literature. Orthop Traumatol Surg Res. 2021;107(6):103002. doi:10.1016/j.otsr.2021.103002 PubMed
27.Chen C, Shi Z. Letter to the editor regarding “Finite element analysis of subtalar joint arthroereisis on adult-acquired flexible flatfoot deformity using sinus tarsi implant”. J Orthop Translat. 2022;33:70-71. doi:10.1016/j.jot.2022.02.003 PubMed
28.Wong DW, Wang Y, Niu W, Zhang M. Finite element analysis of subtalar joint arthroereisis on adult-acquired flexible flatfoot deformity using customised sinus tarsi implant. J Orthop Translat. 2021;27:139-145. doi:10.1016/j.jot.2020.02.004 PubMed
29.Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. PubMed
30.Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377-384. PubMed
Appendix 1: Detailed Methods and Selection of Included Studies
Please note that this appendix has not been copy-edited.
An information specialist conducted a literature search on key resources including MEDLINE, the Cochrane Database of Systematic Reviews, the International HTA Database, the websites of health technology assessment agencies in Canada and major international health technology assessment agencies, as well as a focused internet search. The search approach was customized to retrieve a limited set of results, balancing comprehensiveness with relevance. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. Search concepts were developed based on the elements of the research questions and selection criteria. The main search concept was arthroereisis. Comments, newspaper articles, editorials, and letters were excluded. Retrieval was limited to the human population. The search was completed on November 20, 2024, and was limited to English-language documents published since January 1, 2014.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, were duplicate publications, or were published before 2014. Systematic reviews in which all relevant studies were captured in other more recent or more comprehensive systematic reviews were excluded. We identified another systematic review which had significant overlap in included primary studies as the systematic review included in this rapid review (Baryeh et al. study10), as well as a greater number of relevant studies included to this rapid review. However, we excluded this review considering comprehensiveness and the level of rigour between the systematic reviews and considerable overlap. Primary studies retrieved by the search were excluded if they were captured in 1 or more included systematic reviews. Guidelines with unclear methodology were also excluded.
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the following tools as a guide: A MeaSurement Tool to Assess systematic Reviews 2 (AMSTAR 2)29 for the systematic review and the Downs and Black checklist30 for nonrandomized studies. Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Appendix 2: Characteristics of Included Publications
Table 2: Characteristics of the Included Systematic Review
Study citation, country, funding source | Study design, Number of primary studies included | Population characteristics | Intervention and comparator | Relevant clinical outcomes, length of follow-up |
|---|---|---|---|---|
Baryeh et al. (2022)10 UK Funding source: The authors received no support for the research, authorship, and/or publication of the study. | Study Design: Systematic review of clinical and radiological outcomes from studies published from inception to December 2019. Included studies: 9 nonrandomized studies (case series or cohort studies) | Adults treated with subtalar joint arthroereisis for acquired flatfoot N = 167 adults (190 feet) Age, mean (SD): 47.4 (NR) years Sex: 2:1 ratio of female to male Bilateral surgery: NR Surgery on left foot: NR Ethnicity: NR BMI: NR Implant size: Varied across studies Implant type: Varied across studies | Intervention: Isolated or adjunct subtalar joint arthroereisis Comparator: Baseline |
Follow-up, mean (range): 31.9 (1.3 to 76.0) months |
AOFAS = American Orthopaedic Foot & Ankle Society; FAOS = Foot and Ankle Outcome Score; NR = not reported; SD = standard deviation; SF-36 = Short Form (36) Survey; VAS-FA = Visual Analogue Scale Foot and Ankle.
Note: This table has not been copy-edited.
Table 3: Characteristics of Included Nonrandomized Studies
Study citation, country, funding source | Study design | Population characteristics | Intervention and comparator | Relevant clinical outcomes, length of follow-up |
|---|---|---|---|---|
Indication: Pes planus | ||||
Fu et al. (2024)13 China Funding source: Shanghai Jiao Tong University, Science and Technology of Shanghai Municipality, and Shanghai Municipal Commission of Economy and Informatization. | Single-centre retrospective study | People with pes planus, admitted to Shanghai Sixth People’s Hospital from 2013 to 2015 who did not respond to 6 months of conservative treatment preoperatively. N = 508 Adults, n (%): 223 (43.9%) Age (adults): NR Sex (adults): 156 (69.9%) females Bilateral surgery (adults): NR Surgery on left foot (adults): 132 (59.1%) had implants inserted in their left foot Ethnicity (adults): NR BMI (adults), median (Q1, Q3): 22.9 (20.7, 25.4) kg/m2 Implant size (adults): Varied across the study population Implant type (adults): HyProCure | Intervention: Isolated or adjunct subtalar joint arthroereisis
Comparator: NA |
Follow-up: NR |
Lewis et al. (2024)22 Australia Funding Source: No funding received to support completing this study. | Single-centre, retrospective, before-and-after study | Adults with stage I flexible progressive collapsing foot deformity between 2010 and 2018, who did not respond to 6 months of non-operative treatment. N = 187 adults (212 feet) Age, mean (SD): 59.7(13.1) years Sex: 118 (63.1%) females Bilateral surgery: 26 feet (12.3%) Surgery on left foot = 126 (59.4%) implants were inserted in the left foot Ethnicity: NR BMI, mean (SD): 28.1 (4.3) kg/m2 Implant size: 90.6% of cases used a 9 mm implant. Implant type: NR | Intervention: Adjunct subtalar joint arthroereisis. Of 212 feet, 133 (62.7%) also underwent Achilles tendon lengthening as part of the procedure Comparator: Baseline |
Follow-up, mean (SD): 2.5 (1.3) years |
Bernasconi et al. (2022)19 UK Funding Source: Authors received no financial support for the research, authorship, and/or publication of this article. | Single-centre, retrospective, before-and-after study | Adults with stage IIb adult-acquired flexible flatfoot deformity (ICD 21.4) presenting to a single unit between July 2004 to January 2019 N = 21 adults (22 feet) Age, mean (SD): 55.2 (2.4) years Sex: 11 (50%) females Bilateral surgery: NR Surgery on left foot: NR Ethnicity: NR BMI, mean (SD): 31.4 (1.1) kg/m2 Implant size: Varied across study population. Implant type: NR | Intervention: Adjunct subtalar joint arthroereisis. All participants also underwent medializing calcaneal osteotomy, flexor digitorum longus transfer, spring ligament repair with or without cotton osteotomy Comparator: NA |
Follow-up: minimum 6 months postprocedure |
Silva et al. (2021)11 Singapore Funding Source: NR | Single-centre, retrospective cohort study | Adults with stage IIb acquired flatfoot deformity between January 2007 and 2013. N = 72 adults (79 feet) Age: The mean age for the intervention arm was 46.3 (SD 16.8) years. The mean age for intervention group was 46.9 (SD 25.1) years. Sex: 55 (76.4%) females Bilateral surgery: NR Surgery on left foot: NR Race or ethnicity: 61 (84.7%) adults were reported to be Chinese. BMI: The BMI at baseline significantly differed between the intervention and comparator groups. The mean BMI for the intervention group is 26.3 (SD 4.3) kg/m2. The mean BMI for the comparator group is 29.1 (SD 4.2) kg/m2. Implant size: Varied across the study population. Implant type: HyProCure Intervention and comparator groups did not differ in sex, age, and race or ethnicity. | Intervention: Subtalar joint arthroereisis (HyProCure implant) adjunct to tendo-Achilles lengthening or gastrocnemius release (dependent on clinical findings) Comparator: Lateral column lengthening with medializing calcaneal osteotomy, distraction osteotomy, flexor digitorum longus transfer, and tendo-Achilles lengthening or gastrocnemius release (dependent on clinical findings) |
Follow-up: 6 and 24 months after surgery |
Fang Junxian et al. (2020)20 Singapore Funding source: No funding was received for the completion of the study. | Single-centre, retrospective cohort study | Adults with symptomatic adult-acquired flatfoot disease (stage IIb posterior tibial tendon dysfunction) N = 22 adults (22 feet) Subtalar joint arthroereisis, n (%): 12 (54.5%) Age (subtalar joint arthroereisis group), mean (SD): 52.7 (NR) years Sex: 13 (59.0%) females Unilateral surgery: all cases (100%) Surgery on left foot: 6 (27.2%) implants were done on the left foot Ethnicity: NR BMI: NR Implant size: Varied across the study population. Implant type: NR Intervention and comparator groups were comparable in age and sex. | Intervention: Adjunct subtalar joint arthroereisis Comparators: Baseline, adjunct lateral column lengthening All study participants had an endoscopic gastrocnemius recession, tibialis posterior insertion site debridement, and a medializing calcaneal osteotomy. |
Follow-up: minimum of 12 months |
Saxena et al. (2016)24 US Funding Source: First author received royalties from Arthrex for the implants used. | Prospective study | Adults treated for symptomatic flexible flatfoot between 1996 and 2012. N = 100 adults Age, mean (SD): 53.3 (14.7) years Sex: NR Bilateral surgery: NR Surgery on left foot: NR Ethnicity: NR BMI: NR Implant size: NR Implant type: Varied across study population | Intervention: Subtalar joint arthroereisis
Comparator: NA |
Follow-up, mean (SD): 6.5 (3.2) years |
Ozan et al. (2015)23 Turkey Funding Source: NR | Single-centre, before-and-after study | Adults with symptomatic flexible flatfoot deformity treated between 2011 and 2013, who did not respond to 6 months of conservative treatment. N = 16 adults (26 feet) Age, mean (SD): 24.5 (5.24) years Sex: 12 (75%) females Bilateral surgery: NR Surgery on left foot: 13 (50%) implants were inserted in the left foot. Ethnicity: NR Implant size: Varied across study population Implant type: BioPro Horizon | Intervention: Isolated subtalar joint arthroereisis Comparator: Baseline |
Follow-up, mean (SD): 15.1 (4.7) months |
Indication: Other foot conditions | ||||
Agnew et al. (2023)18 US Funding Source: No funding was received for conducting this study. | Multicentre, retrospective, before-and-after study | Individuals with symptomatic, reducible talotarsal joint dislocation since 2009. N = 67 individuals (53 feet) Adults, n (%): 36 (53 feet) Age, median (range): 41 (20 to 74) years Sex (adults): 37 (69.8%) feet from female participants Bilateral surgery (adults), n (%): 17 (25.4%) Surgery on left foot (adults), n (%): 27 (50.9%) Ethnicity: NR BMI: NR Implant size: Varied across study population. Implant type: HyProCure and HyProCure II | Intervention: Standalone type II extraosseous talotarsal stabilization implant (HyProCure and HyProCure II implants) Comparator: NA |
Follow-up (adults), mean (range): 7 years, 8 months, 19 days (5 years, 2 days to 12 years, 2 months, 7 days) |
Kolodziej et al. (2023)21 Poland Funding Source: No external funding reported. | Single-centre, prospective, before-and-after study | Adults (> 18 years) with partial talotarsal joint instability between 2012 and 2015. N = 41 adults (62 feet) Age, mean (SD): 46.4 (15.6) years Sex: 36 (87.8%) females Bilateral surgery, n (%): 21 (51.2%) Surgery on left foot: NR Ethnicity: NR BMI, mean (SD): 24.2 (3.2) kg/m2 Implant size: Varied across study population Implant type: HyProCure implant | Intervention: Extraosseous talotarsal stabilization. Comparator: Baseline |
Follow-up, mean (range): 8.6 (7.3 to 10.3) years |
AOFAS = American Orthopaedic Foot & ankle Society; BMI = body mass index; FADI = Foot and Ankle Disability Index; FAOS = Foot and Ankle Outcome Score; ICD = international classification of diseases; NA = not applicable; NR = not reported; Q = quartile; SD = standard deviation; SF-36 = Short Form (36) Health Survey; VAS = visual analogue scale.
Note: This table has not been copy-edited.
Appendix 3: Critical Appraisal of Included Publications
Please note that this appendix has not been copy-edited.
Table 4: Strengths and Limitations of the Systematic Review Using AMSTAR 229
Strengths | Limitations |
|---|---|
Baryeh et al. (2022)10 | |
|
|
AMSTAR 2 = A MeaSurement Tool to Assess systematic Reviews 2; PRISMA = Preferred Reporting Items for Systematic Reviews and Meta-analyses.
Table 5: Strengths and Limitations of Clinical Studies Using the Downs and Black Checklist30
Strengths | Limitations |
|---|---|
Fu et al. (2024)13 | |
|
|
Lewis et al. (2024)22 | |
|
|
Agnew et al. (2023)18 | |
|
|
Kolodziej et al. (2023)21 | |
|
|
Bernasconi et al. (2022)19 | |
|
|
Silva et al. (2021)11 | |
|
|
Fang Junxian et al. (2020)20 | |
|
|
Saxena et al. (2016)24 | |
|
|
Ozan et al. (2015)23 | |
|
|
AOFAS = American Orthopaedic Foot & Ankle Society; BMI = body mass index; Version; FADI = Foot and Ankle Disability Index; FAOS = Foot and Ankle Outcome Score; SF-36 = Short Form (36) Health Survey; VAS = visual analogue scale.
Appendix 4: Main Study Findings
Table 6: Summary of Findings — Subtalar Joint Arthroereisis and Lateral Column Lengthening for Adults With Pes Planus From the Nonrandomized Study by Silva et al. (2021)11
Outcome measure | Baseline (mean score) | Follow-up at 6 months (mean score) | Follow-up at 24 months (mean score) | ||||||
|---|---|---|---|---|---|---|---|---|---|
Subtalar joint arthroereisis | Lateral column lengthening | P value | Subtalar joint arthroereisis | Lateral column lengthening | P value | Subtalar joint arthroereisis | Lateral column lengthening | P value | |
AOFAS hindfoot | 50.3 (SD 21.1) | 52.2 (SD 21.6) | ns | 75.3 (SD 18.6) | 71.4 (SD 17.5) | ns | 81.6 (SD 21.6) | 86.4 (SD 17.3) | ns |
AOFAS midfoot | 47.6 (SD 26.0) | 45.1 (SD 21.9) | 0.21 | 74.0 (SD 24.2) | 73.1 (SD 19.5) | 0.15 | 81.1 (SD 20.6) | 90.3 (SD 12.6) | < 0.001 |
SF-36 PCS | 47.8 (SD 21.2) | 48.3 (SD 19.2) | ns | 57.3 (SD 20.0) | 52.4 (SD 19.9) | ns | 65.3 (SD 21.1) | 65.2 (SD 23.3) | ns |
SF-36 MCS | 69.1 (SD 21.8) | 75.3 (SD 20.3) | ns | 76.6 (SD 19.9) | 74.8 (SD 20.7) | ns | 80.6 (SD 17.5) | 79.1 (SD 19.5) | ns |
VAS midfoot | 4.8 (SD 3.7) | 5.7 (SD 3.2) | ns | 1.7 (SD 2.7) | 1.5 (SD 2.2) | ns | 1.3 (SD 2.4) | 0.5 (SD 1.6) | < 0.001 |
VAS hindfoot | 6.1 (SD 3.0) | 5.6 (SD 3.3) | ns | 2.6 (SD 2.9) | 2.2 (SD 2.4) | ns | 1.4 (SD 2.5) | 1.2 (SD 2.6) | ns |
BMIa | 26.3 (SD 4.3) | 29.1 (SD 4.2) | < 0.01 | NA | NA | NA | 26.8 (SD 4.5) | 27.2 (SD 4.2) | ns |
Adverse eventsb [rate (%)] | NA | NA | NA | NA | NA | NA | 7 (20.6)b | 2 (4.4%)b | NA |
AOFAS = American Orthopaedic Foot & Ankle Society; BMI = body mass index; MCS = mental component summary; NA = not significant; ns = not significant; PCS = physical component summary; SD = standard deviation; SF-36 = Short Form (36) Health Survey; VAS = visual analogue scale.
Notes: Bolded outcome measures indicate a statistically significant difference.
Silva and colleagues11 did not report P values for any nonsignificant comparisons where P > 0.05, except for VAS midfoot score.
The study by Fang Junxian and colleagues20 compared and reported before-and-after outcomes for the subtalar joint arthroereisis group and the lateral column lengthening group. However, they did not use any statistical methods to compare the scores of the subtalar joint arthroereisis group vs. the scores of the lateral column lengthening group. Therefore, the findings relevant to this report are the before-and-after results for the subtalar joint arthroereisis group and presented in the before-and-after outcomes tables. Of note, this study found that lateral column lengthening significantly improved the overall foot and ankle condition (AOFAS), general health (SF-36), role limitation from physical health (SF-36), energy (SF-23), emotional well-being (SF-36), and pain relief (VAS) compared to baseline.
aThis outcome was only measured at 24 months.
bAdverse events were reported as a rate (% of cases) throughout the study. While it is reported under “follow-up at 24 months,” these adverse events may have started before the 6-months or 24-months follow-up.
Note: This table has not been copy-edited.
Table 7: Summary of Findings — Subtalar Joint Arthroereisis for Pes Planus (Before-and-after Outcomes)
Study, study design | Baseline mean score | Follow-Up mean score | P value | Notes |
|---|---|---|---|---|
Outcome measure: AOFAS score | ||||
Baryeh et al. (2022),10 SR | 50.7 (NR)a | 81.4 (NR)a | NA | Based on the findings of 5 included studies. Of which, 3 reported significant improvement at follow-up from baseline (P value < 0.001, < 0.00001, 0.0001). |
Fang Junxian et al. (2020),20 NRS | 54.9 (NR) | 83.8 (NR) | 0.004b | — |
Ozan et al. (2015),23 before-and-after study | 52 (SD 6.6) | 75 (SD 11.2) | 0.0001b | — |
Outcome measure: EQ-5D-5L score | ||||
Lewis et al. (2024),22 before-and-after study | 0.69 (SD 0.22) | 0.82 (SD 0.14) | < 0.05b | Of 187 participants, 21 had pre- and postoperative scores. |
Outcome measure: FAOS score | ||||
Baryeh et al. (2022)10 SR | 42.6 (NR) | 68.2 (NR) | < 0.05b | Based on the findings of 1 included study. |
Lewis et al. (2024),22 before-and-after study | — | — | Of 187 participants, 21 had pre- and postoperative scores. | |
Pain | 35.9a (SD 17.2) | 73.0a (SD 16.6) | < 0.001b | — |
Symptoms | 71.8a (SD 6.1) | 81.9a (SD 9.6) | < 0.001b | — |
Activities of daily living | 65.6a (SD 14.6) | 84.0a (SD 11.0) | < 0.001b | — |
Quality of life | 26.6a (SD 14.0) | 47.8a (SD 20.1) | 0.001b | — |
Outcome measure: FADI score | ||||
Lewis et al. (2024),22 before-and-after study | — | — | — | Of 187 participants, 21 had pre and postoperative scores. |
Pain | 52.0 (SD 18.6) | 22.4 (SD 16.9) | < 0.001b | — |
Activity | 49.8 (SD 22.0) | 23.8 (SD 18.9) | < 0.001b | — |
Outcome measure: SF-36 score | ||||
Baryeh et al. (2022),10 SR | NR | 75.4 | NA | — |
Fang Junxian et al. (2020),20 NRS | — | — | — | — |
Physical function | 40.3 (NR) | 72.1 (NR) | 0.006b | — |
Role limitation (physical health) | 16.1 (NR) | 82.1 (NR) | 0.001b | — |
Role limitation (emotional problems) | 38.1 (NR) | 90.5 (NR) | 0.006b | — |
Energy fatigue | 52.9 (NR) | 64.3 (NR) | 0.026b | — |
Emotional well-being | 72.7 (NR) | 77.1 (NR) | 0.573 | — |
Social functioning | 58.0 (NR) | 96.4 (NR) | 0.001b | — |
Pain | 43.4 (NR) | 83.4 (NR) | 0.001b | — |
General function | 58.6 (NR) | 66.8 (NR) | 0.009b | — |
Outcome measure: VAS-FA score | ||||
Baryeh et al. (2022),10 SR | 61.6 (range 25 to 86) | 83 (range 61 to 100) | < 0.0001b | Based on the findings of 1 included study, |
Outcome measure: VAS score | ||||
Baryeh et al. (2022),10 SR | 7.8 (NR) | 2.8 (NR) | NA | Based on the findings of 3 included studies. Of which, 2 studies reported a significant difference (< 0.05 and 0.0001). |
Fang Junxian et al. (2020),20 NRS | 7.6 (NR) | 2.9 (NR) | 0.002b | — |
Ozan et al. (2015),23 before-and-after study | 6.9 (SD 0.6) | 4.1 (SD 1.4) | 0.0001b | — |
AOFAS = American Orthopaedic Foot & Ankle Society; FA = foot and ankle; FAOS = Foot and Ankle Outcome Score; NA = not applicable; NR = not reported; SF-36 = Short Form (36) Health Survey; SR = systematic review; VAS = visual analogue scale; VAS-FA = visual analogue scale foot and ankle.
aReported as a mean by the respective study.
bP < 0.05.
Note: This table has not been copy-edited.
Table 8: Summary of Findings — Subtalar Joint Arthroereisis for Partial Talotarsal Joint Instability (before-and-after study by Kolodziej et al. [2023]21)
Outcome measure | Baseline, mean (SD) | Follow-up, mean (SD) | P value |
|---|---|---|---|
Function and activities of daily living | |||
Lower Extremity Functional Scale | 74.2 (23.7) | 88.6 (15.3) | 0.0006a |
Symptom-Related Ankle Activity Scale | 71.7 (20.0) | 82.9 (18.7) | 0.002a |
UCLA Activity Score | 6.02 (2.7) | 6.09 (2.5) | 0.787 |
Sports and exercise | |||
Number of physical activities (per week) | 1.95 (1.1) | 1.83 (1.0) | 0.37 |
Sport Frequency score | 2.1 (0.5) | 2.1 (0.4) | 0.11 |
Time of physical activity (minutes per week) | 153 (126.3) | 170 (102) | 0.15 |
Pain | |||
VAS | 4.6 (3.3) | 0.9 (1.5) | < 0.0001a |
SD = standard deviation; VAS = visual analogue scale.
aP value < 0.05.
Note: This table has not been copy-edited.
Table 9: Summary of Findings — Adverse Events or Complications
Study, study design | Result | Notes |
|---|---|---|
Implant removal | ||
Baryeh et al. (2022),10 SR | 40 of 175 (22.9%) implants | Based on 8 relevant studies involving 175 feeta Of the 40 removals, the main causes include:
3 implant removals had no reasons described (7.5%) |
Fu et al. (2024),13 NRS | 36 (15.3%) implants | Implant removals were caused by sinus tarsi pain that was not relieved by conservative treatment. After removal, all patients experienced pain relief. The most common cause of removal was sinus tarsi pain. |
Lewis et al. (2024),22 before-and-after study | 102 of 212 (48.1%) implants | Mean time for removal was 0.64 years (SD 0.41) postprocedure. Sinus tarsi pain or lateral hind foot pain was the reason for all implant removals. Lewis and colleagues found a statistically significant difference in age between participants who had their implant removed and those who did not. |
Agnew et al. (2023),18 before-and-after study | 2 of 53 (3.7%) implantsb | — |
Kolodziej et al. (2023),21 before-and-after study | 0 of 41 adultsb | — |
Bernasconi et al. (2022),19 before-and-after study | 4 of 21 (19.0%) adults | Implants were removed due to sinus tarsi pain. |
Silva et al. (2021),11 NRS | 7 of 31 (20.6%) adults | Implants were removed due to midfoot pain. For adults with removed implants, deformity correction was maintained at 24 months. |
Fang Junxian et al. (2020),20 NRS | 4 of 12 (33.3%) implants | All implants were removed because of sinus tarsi pain. They performed removals at a mean of 27 months after the intervention. Implant removal significantly improved all components of SF-26 (except for emotional being), AOFAS score, and VAS scores. |
Saxena et al. (2016),24 NRS | 23 of 103 (22.3%) implants | Most implants were removed at a mean of 12.9 months (SD 8.6) after the procedure. |
Ozan et al. (2015),23 before-and-after study | 3 of 26 (7.6%) implants | Of 3 implant removals, 2 were caused by sinus tarsi pain and 1 was caused by loss of deformity fixation. |
Pain | ||
Kolodziej et al. (2023),21 before-and-after study | 1 of 41 (2.4%) individuals experienced persistent painb | The individual experience pain up until their last follow-up (8 years from surgery), which also limited their activities. |
Bernasconi et al. (2022),19 before-and-after study | 12 of 21 (57.1%) adults experienced persistent sinus tarsi pain | — |
Baryeh et al. (2022),10 SR | 1 (0.6%) foot with complex regional pain syndrome | Based on 8 relevant studies involving 175 feet.a |
Baryeh et al. (2022),10 SR | 28 of 175 (16%) with sinus tarsi pain | Based on 8 relevant studies involving 175 feet.a |
Fu et al. (2024),13 NRS | 60 (25.42%) cases with sinus tarsi pain | Sinus tarsi pain was the most common complication and most common cause of implant removal. Of the 60 cases, 23 feet experienced symptom relief conservative treatment. |
Fang Junxian et al. (2020),20 NRS | 6 (27.3%) adults with sinus tarsi pain | — |
Ozan et al. (2015),23 before-and-after study | 3 of 26 (11.5%) feet with sinus tarsi pain | — |
Device revision | ||
Agnew et al. (2023),18 before-and-after study | 3 of 53 (5.6%) implantsb | — |
Infection | ||
Baryeh et al. (2022),10 SR | 1 (0.6%) foot with surgical site infection | Based on 8 relevant studies. |
Fractures | ||
Baryeh et al. (2022),10 SR | 1 of 175 (0.6%) feet experienced a stress fracture | Based on 8 relevant studies.a |
Insufficient foot correction | ||
Baryeh et al. (2022),10 SR | 1 of 175 (0.6%) feet experienced insufficient foot correct | Based on 8 relevant studies.a |
Recurrence of deformity | ||
Baryeh et al. (2022),10 SR | 1 of 175 (0.6%) feet experienced a reoccurrence of foot deformity | Based on 8 relevant studies.a |
Ozan et al. (2015),23 before-and-after study | 1 of 26 (3.8%) feet | — |
Muscle and tendon complications | ||
Fu et al. (2024),13 NRS | 2 (0.85%) cases had Achilles tendon tension | — |
Fu et al. (2024),13 NRS | 2 (0.85%) cases had peroneal spasm | — |
Fu et al. (2024),13 NRS | 2 (0.85%) cases experienced decline in muscle strength | — |
Wound healing issues | ||
Fu et al. (2024),13 NRS | 1 (0.42%) case had poor wound healing | — |
Kolodziej et al. (2023),21 before-and-after study | 1 of 41 (2.4%) individuals with a wound healing issueb | “The issue self-resolved without any negative impact on the outcome.” |
Other | ||
Fu et al. (2024),13 retrospective cohort | 1 (0.42%) case had a foreign body sensation | — |
Agnew et al. (2023),18 before-and-after study | 8 of 53 (15.1%) implants experienced “ongoing device related issues”b | For this study, this category includes pain, stiffness, general discomfort, feeling of weak ankle and instability, lack of correction or improvement, difficulty walking, difficulty wearing shoes, neuropathy, swelling, limited range of motion, and occasional feelings of cramps art night. |
NRS = nonrandomized study; SR = systematic review.
Note: Most studies in this table were conducted on adults with pes planus except for the Agnew et al. study18 and the Kolodziej et al. study.21
aFor the systematic review by Baryeh and colleagues,10 a total of 8 studies were included. They had difficulties ascertaining whether complications were from the interest group in 1 study.
bThe study was conducted on individuals with other foot conditions.
Note: This table has not been copy-edited.
Appendix 5: References of Potential Interest
Please note that this appendix has not been copy-edited.
Nonrandomized Studies
Mixed Population (Includes Pediatric Population)
Stichnoth M, Luders KA, Hell AK, Stinus H. Comparative study of subtalar arthroereisis, medializing calcaneal osteotomy and the combination of both techniques for the treatment of symptomatic adult flatfeet. J Foot Ankle Surg. 2024 Oct 29;29:29. PubMed: PM39523149.
Jain A, Gupta G, Gupta A. Short Term Clinico-Radiological Outcome of Extra Osseous Talo-Tarsal Stabilization (EOTTS) in Flat Foot: An Indian Perspective. Indian J Orthop. 2022 Jan;56(1):94-102. PubMed: PM35070148.
Case Series
Mercun A, Kovacic B, Suhodolcan L, Drobnic M. Patient Outcomes Following Extra-Osseous Talo-Tarsal Stabilization for Foot Hyperpronation. J Foot Ankle Surg. 2022 Mar-Apr;61(2):318-322. PubMed: PM34600818.
Guidelines and Recommendations
Unclear Methodology
College of Chiropodists of Ontario. Subtalar Joint Arthroereisis Procedure. Accessed November 21 2024, https://www.cocoo.on.ca/pdf/guidelines/subtalar_joint_arthroereisis.pdf.
Alternative Methods
Salga M, Gatin L, Deltombe T, et al. International Recommendations to Manage Poststroke Equinovarus Foot Deformity Validated by a Panel of Experts Using Delphi. Arch Phys Med Rehabil. 2023 03;104(3):372-379. PubMed: PM36030892.
Review Articles
Blue Shield of California. Subtalar Arthroereisis. Accessed November 21 2024, https://www.blueshieldca.com/content/dam/bsca/en/provider/docs/medical-policies/Subtalar-Arthroereisis.pdf.
ISSN: 2563-6596
Canada’s Drug Agency (CDA-AMC) is a pan-Canadian health organization. Created and funded by Canada’s federal, provincial, and territorial governments, we’re responsible for driving better coordination, alignment, and public value within Canada’s drug and health technology landscape. We provide Canada’s health system leaders with independent evidence and advice so they can make informed drug, health technology, and health system decisions, and we collaborate with national and international partners to enhance our collective impact.
Disclaimer: CDA-AMC has taken care to ensure that the information in this document was accurate, complete, and up to date when it was published, but does not make any guarantee to that effect. Your use of this information is subject to this disclaimer and the Terms of Use at cda-amc.ca.
The information in this document is made available for informational and educational purposes only and should not be used as a substitute for professional medical advice, the application of clinical judgment in respect of the care of a particular patient, or other professional judgments in any decision-making process. You assume full responsibility for the use of the information and rely on it at your own risk.
CDA-AMC does not endorse any information, drugs, therapies, treatments, products, processes, or services. The views and opinions of third parties published in this document do not necessarily reflect those of CDA-AMC. The copyright and other intellectual property rights in this document are owned by the Canadian Agency for Drugs and Technologies in Health (operating as CDA-AMC) and its licensors.
Questions or requests for information about this report can be directed to Requests@CDA-AMC.ca.