Drugs, Health Technologies, Health Systems
Health Technology Review
Troponin | Point of Care Testing in Rural and Remote Community Health Centres
Key Messages
What Is the Issue?
Acute coronary syndrome (ACS), including myocardial infarction (MI), is a leading cause of morbidity and mortality worldwide and survival rates for MI may be lower in rural and remote settings compared to urban settings.
While chest pain is a common symptom of ACS, most patients with this symptom will ultimately not be diagnosed with MI and diagnosis can be challenging. Recommendations for diagnosis include many factors, one of which is serial blood sampling to test for cardiac troponin (cTn), a biomarker for cardiac injury. High sensitivity, laboratory-based assays are typically recommended for cTn testing ideally within 60 minutes of a patient’s presentation.
In many rural and remote community health centres, including in Canada, laboratory services are not easily accessible, and results may not be available for hours or days. The current clinical practice in many of these regions is to transfer patients presenting with suspected ACS to the nearest hospital or tertiary care centre, sometimes over long distances and by aeromedical transfer, and often at a high cost. Given many of these patients will not ultimately be diagnosed with MI or require hospital-based care, this poses a concern for patients, staff, and resources.
Point-of-care tests (POCT) for cTn may offer an interesting opportunity in these settings. Efficient access to cTn results may potentially improve the ability for health care workers in community settings to more easily diagnose and triage patients at risk for MI and potentially avoid unnecessary patient transfers. However, cTn POCTs are generally less sensitive than laboratory-based assays with varied performance between devices and staff training is required for implementation and quality control. It is important to understand the clinical utility and recommendations regarding the use of cTn POCTs in remote and rural settings.
What Did We Do?
This rapid review has been conducted in response to a request from a jurisdictional service provider to help determine if implementation of POCTs for a cardiac biomarker, cardiac troponin I (cTnI), should be considered in rural and remote community health or primary care centres. The research questions were codeveloped in response to this request. We aimed to identify and summarize recent evidence on the current use, clinical utility, and guideline recommendations regarding cTnI POCTs to support patient diagnosis and triage in these settings, where access to laboratory-based cTn results may be limited.
We searched key resources including journal citation databases and conducted a focused internet search for relevant evidence published since January 2009. No critical appraisal of identified information was conducted.
What Did We Find?
We identified 2 point-of-care testing programs implemented in rural jurisdictions that include cTnI POCTs, 1 in Australia and 1 in New Zealand; no records met our eligibility criteria regarding cTnI POCT use in rural and remote settings in Canada. The included reports describe program-related processes and experiences, including approaches to structured governance and oversight, training, and quality control. We also identified 2 surveys of general practitioners’ (GPs) current and desired use of cTnI POCT, 1 from Germany and 1 from South Africa, with limited applicability to the setting in Canada.
We identified 2 health technology assessments (HTAs (with 3 eligible studies in 4 reports) and 2 primary observational studies examining the clinical utility of cTnI POCT in community health centres in rural and remote settings. One HTA, including 2 studies, and 1 primary observational study assessed cTnI POCT as part of an accelerated diagnostic protocol (ADP), a clinical decision algorithm, incorporating cTnI POCT results with electrocardiogram (ECG) results, clinical assessment, and patient history. The results suggest that cTnI POCTs, when used within the context of an ACS-ADP, have the potential to identify low-risk patients (high sensitivity and negative predictive value), and reduce unnecessary referrals or transfers when there is limited or no efficient access to laboratory-based results.
While the included HTAs appear to be well conducted, they identified few primary research studies, studies were focused primarily on 1 cTnI POCT used within specific ADPs, the studies lacked a control group, and no studies assessed high-sensitivity cTnI POCTs. The results cannot be translated to other cTnI POCT devices nor those used within other ADPs. We identified no studies conducted in rural or remote jurisdictions in Canada.
While some existing guidelines provide specific recommendations on components of our questions, we did not identify evidence-based guideline recommendations on the use of cTnI POCT in rural or remote community health centres.
What Does It Mean?
The studies we identified suggest that cTnI POCTs may be useful in rural and remote community care settings to help identify patients presenting with symptoms of ACS who may be at low risk for MI, potentially avoiding unnecessary patient transfers to hospital.
As the clinical utility of cTnI POCTs is dependent on the device used, patient-management protocols and contextual factors such as underlying community risk, social acceptability and resources — and we identified no studies conducted in rural and remote community care settings in Canada — the applicability of the results is unclear. To better understand their use, cTnl POCTs should be assessed within a suspected ACS-ADP in the context of interest to better understand their utility.
The experiences published about rural or remote community POCT programs outside of Canada highlight various factors that may inform decision-making in Canada including the importance of governance and oversight structures; continuing resources for training, accreditation and quality control; and the challenges with high staff turnover in rural and remote regions.
As high-sensitivity cTn POCTs become available, it will be important to assess their clinical utility in settings of interest.
Abbreviations
ACS
acute coronary syndrome
ADP
accelerated diagnostic protocol
AIHTA
Austrian Institute for Health Technology Assessment
cTn
cardiac troponin
cTnI
cardiac troponin I
cTnT
cardiac troponin T
ECG
electrocardiogram
ED
emergency department
EUnetHTA
European Network for Health Technology Assessment
GP
general practitioner
HTA
health technology assessment
MACE
major adverse cardiovascular events
MI
myocardial infarction
NSTEMI
non–ST-elevation myocardial infarction
POCT
point-of-care test
QoL
quality of life
RACPP
Rural Accelerated Chest Pain Pathway
SR
systematic review
Context and Policy Issues
Acute Coronary Syndrome
In Canada, approximately 2.6 million people live with heart disease1 and it is the second leading cause of death.2 ACS refers to multiple forms of coronary artery disease where blood flow to the heart is suddenly reduced and includes acute MI, heart attack, and unstable angina. ACS is one of the leading causes of morbidity and mortality worldwide; more than 63,000 adults in Canada are diagnosed with their first heart attack annually3 and approximately 2% of patients have had a previous heart attack. In rural and remote settings, the risk of death due to MI may be higher than in urban settings.4
Diagnosis of Acute Coronary Syndrome
Prompt recognition and treatment of ACS is critical. Patients experiencing ACS often present with chest pain and this is one of the top reasons for emergency department (ED) visits in Canada,5 yet only a small proportion of patients presenting with chest pain will ultimately be diagnosed with ASC.6 Symptoms of ACS can vary by sex and other factors, and chest pain is neither a necessary nor a specific symptom for diagnosis.6,7 Diagnosis and triage of ACS includes multiple assessments, one of which is serial blood sampling to test and monitor levels of a cardiac injury biomarker, cTn — specifically cTnI or cardiac troponin T (cTnT). Other factors (e.g., injury) can also elevate or change cTn levels, thus triage and prompt diagnosis of ACS also includes relevant patient history, physical examination, and an ECG within 10 minutes of presentation. Patients with suspected ST-elevated MI (based on ECG results) require emergent intervention irrespective of cTn levels. For patients with suspected non–ST-segment elevation MI (NSTEMI), cTn testing is recommended as a component of a suspected ACS-ADP (i.e., a rapid MI rule in-rule out strategy).7-9
High-sensitivity laboratory assays are generally recommended for cTn measurement, with results recommended within 60 minutes of initial presentation.7-9 However, regular and efficient access to laboratory services is not available for many community care centres in rural and remote settings, where more than one-third of the population in many of Canada’s provinces and territories reside.10 Wait times for results can range from hours to days, inhibiting the ability to efficiently diagnose and triage patients onsite. These centres also do not typically have cardiologists or other specialist services. As such, reported standard practice is to transfer patients with suspected ACS to the nearest hospital or tertiary care centre for assessments including repeated laboratory-based cTn measurements. Transportation can include long-distance travel, in some cases by air ambulance or helicopter. In the northern territories in Canada, for example, much of the population lives greater than 100 km from, and often without road access to, the nearest hospital; thus, there is a high reliance on expensive, aeromedical evacuations.11,12 As many patients presenting with symptoms of possible ACS will not require hospital-based care, these potentially unnecessary patient transfers challenge finite health system and hospital resources; may cause avoidable hardship to patients; and may put patients, flight crews, and paramedics at risk in Canada’s often challenging geographic and weather conditions.
POCT for cTn pose an interesting opportunity to triage patients presenting with potential ACS in remote and rural community health care centres. These tests can be conducted close to the patient, often with handheld or desktop devices, provide results quickly (typically within 10 to 20 minutes),13 can be used without need for extensive medical-technical training, and many are approved for use in Canada.14 However, POCTs for cTn have been found to be less sensitive compared to laboratory-based assays,14 performance varies between devices, and staff training is required for implementation and quality control. A 2016 CADTH HTA14 of cTn POCTs in patients with symptoms suggestive of ACS in any setting concluded that cTn POCTs are not recommended when immediate access to central laboratory testing is available, but, in settings without immediate access to central laboratory testing, including rural or remote settings, cTn POCTs can be considered. A CADTH rapid response update (search date up to 2020),15 specific to cTnI POCTs, identified no new evidence.15
Why Is It Important to Do This Review?
Research and development in this field is rapidly evolving, including the availability of high-sensitivity cTn POCTs. As testing evolves, decision-makers are interested in understanding how cTnI POCTs may be used in community health care in rural and remote settings in Canada. Previous HTAs have identified limited research conducted in rural or remote settings. Most evidence and guideline recommendations have focused on cTn POCT use in EDs or hospitals in urban centres which differ in important ways in terms of patient demographics and efficient access to subsequent care. The 2023 European Society of Cardiology guidelines acknowledges that the clinical availability of validated high-sensitivity POCTs may alter the clinical utility of cTn POCT devices.7 As cTn testing is recommended as a component of suspected ACS-ADPs,7-9and guidelines recommend validating ADPs within their intended context,9 reviewing the current research on clinical utility of these devices in community health care in rural and remote settings is important.
Objective
The objective of this rapid review is to examine recent research and evidence-based guidance on the use of cTnI POCTs within community health and primary care centres in rural and remote settings, where there may be limited or no efficient access to laboratory-based cTn measurements. Of particular interest for this review is whether and how cTnI POCTs can be used to help identify, in people presenting with symptoms of possible ACS, those who are likely to be at low risk for MI and for whom community care may be safe and effective.
Research Questions
What is the available information regarding the current use of point-of-care testing for cTnI in community health centres in rural or remote settings?
What is the clinical utility of point-of-care tests for cTnI when used in community health centres in rural or remote settings?
What are the evidence-based guidelines and best practices regarding the use of point of care tests for cTnI in community health centres in rural or remote settings?
Methods
An information specialist conducted a customized literature search of multiple sources and grey literature on November 28, 2024, balancing comprehensiveness with relevancy and limited to English-language documents published since January 1, 2009.
One reviewer screened citations, selected studies based on the inclusion criteria presented in Table 1, and extracted data from the included studies. We did not predefine the terms rural or remote and accepted definitions as employed by the study authors. This rapid review did not include a formal critical appraisal of included studies; if the results of such assessments were presented in included HTAs, this has been noted.
Appendix 1 presents a detailed description of methods.
Criteria | Description |
|---|---|
Population | Patients presenting with symptoms of a myocardial infarction at community or primary health centres in a rural or remote setting |
Intervention | Point-of-care testing for troponin I |
Comparator | NA |
Outcomes | Q1: Current use of point of care for troponin I including jurisdictions using it in rural or remote community settings; how patients are transported to tertiary care (e.g., ambulance, medical evacuation), distance to tertiary care Q2: Clinical outcomes (e.g., mortality), patient acceptability and satisfaction with care Q3: Recommendations, best practices and practice standards regarding the appropriate use of point of care for troponin I in rural or remote community health care settings (e.g., decision-making criteria for transport to a tertiary care centre, how care is provided following testing) |
Study designs | HTAs, SRs, RCTs, nonrandomized studies, evidence-based guidelines, institutional guidelines, program evaluations |
HTA = health technology assessment; RCT = randomized controlled trial; SR = systematic review.
Summary of Evidence
Quantity of Research Available
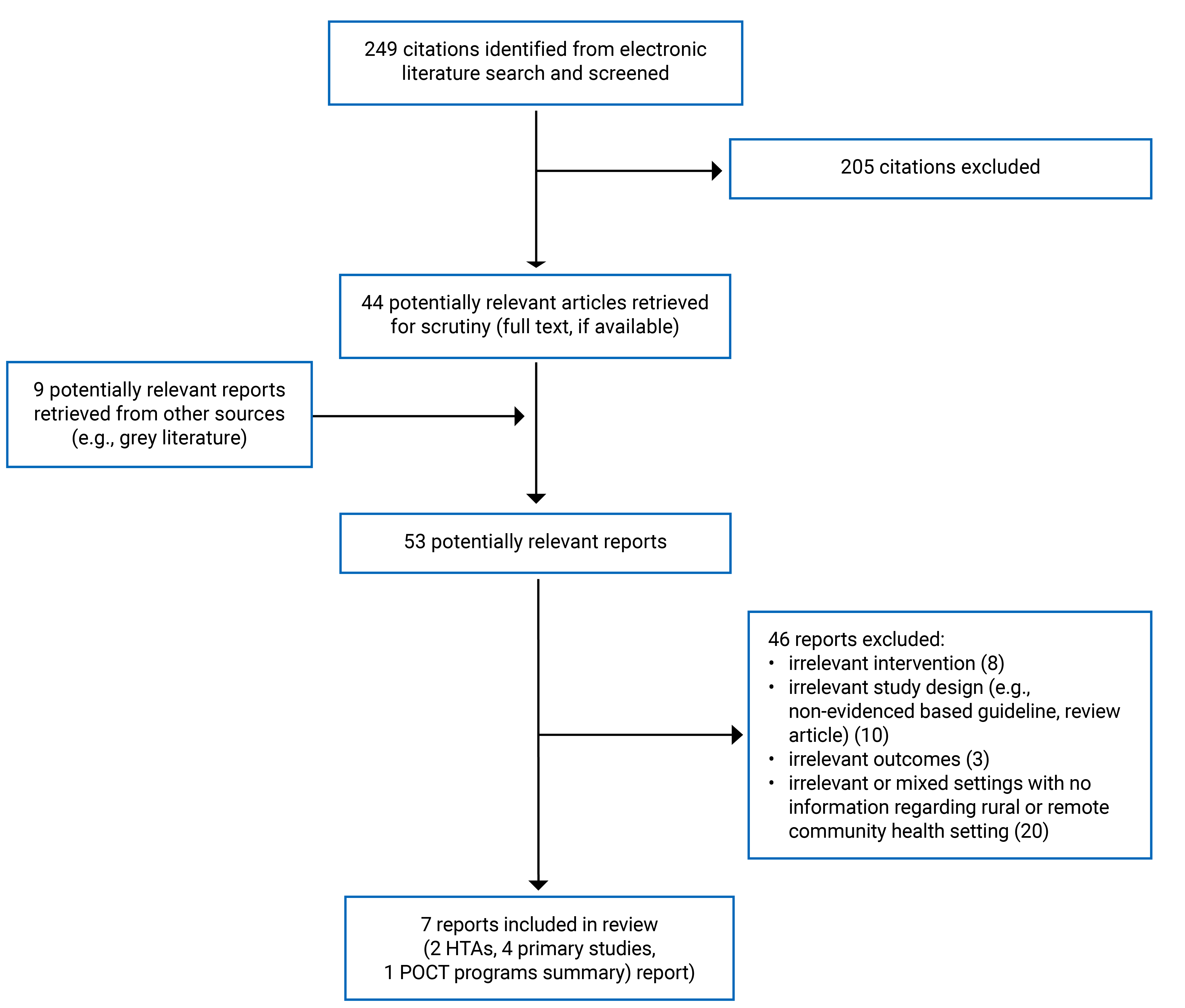
A total of 249 citations were identified in the literature search. Following screening of titles and abstracts, 205 citations were excluded and 44 potentially relevant reports from the electronic search were retrieved for full-text review. In addition, 8 potentially relevant publications were identified from the grey literature search and, 1 record referenced in a study. Of these potentially relevant articles, 46 publications were excluded. Appendix 1 presents the PRISMA16 flow chart of study selection.
This review includes 7 publications: 2 HTAs,17,18 4 primary studies including 2 surveys of current practice,19-22 and 1 report describing experiences with POCT programs.23 Other relevant records were identified in the search but were excluded as they were either included in 1 of the HTAs (24,25) or were systematic reviews (SRs) that did not provide additional relevant information.14,26,27 No evidence-based guidelines that provided recommendations on the use of cTnI POCT in rural or remote community health centres were identified within our search period.
Summary of Study Characteristics
Appendix 2 contains detailed characteristics of the included studies
Research Question 1: Current Use of cTnI Point-of-Care Testing in Community or Primary Health Centres in Rural and Remote Settings
Our search identified no information on the current use of cTnI POCT in rural or remote community health care settings in Canada. We identified 2 point-of-care testing programs that include cTnI POCT in rural and remote settings – 1 in Australia and 1 in New Zealand.19,20,23 Appendix 3 includes details of these programs extracted from the identified literature serve as examples of relevant programs. We also identified 2 surveys that assessed GPs’ current and desired use of cTnI POCT: 1 surveyed GPs from primary practices in 3 German federal states (n = 292 responses of 2,052 surveyed)21 with subgroup data for GPs from rural community practices (n = 84), and the other surveyed staff members (1 per site) from each one of 100 randomly selected primary health care clinics in KwaZulu-Natal, South Africa (100% response rate).23 Some respondent demographic information was provided in the publications yet is not detailed here due to the low applicability of these studies for this review.
Research Question 2: Clinical Use of cTnI Point-of-Care Testing in Community or Primary Health Centres in Rural and Remote Settings
Study Designs, Populations, and Settings
Two HTAs17,18 reporting 4 studies relevant to this review,24,25,28,29 and 2 primary observational studies19,20 examined the clinical utility of cTnI POCT in the settings of interest.
One HTA was conducted by the European Network for Health Technology Assessments (EUnetHTA)18 and the second, an update of the first with narrower eligibility criteria, was conducted by the Austrian Institute for Health Technology Assessment GmbH (AIHTA).17 Both had broader inclusion criteria than our rapid review: they assessed questions related to both cTn and another POCT (D-dimer to help rule-out deep vein thrombosis and pulmonary embolism); they included studies examining cTnT as well as cTnI, and they included settings beyond community care in rural and remote locations. Both searched for studies including adult patients with suspected non–ST-elevation acute MI. The EUnetHTA report included studies in both ambulatory and emergency settings, while the AIHTA report was limited to studies conducted in primary and community care. Both HTA teams used a stepwise approach to identify relevant evidence — first searching for SRs, HTAs, and clinical or diagnostic guidelines (published in English or German between 2009 and 2019,18 or 2019 and 202414), then supplementing the search, as needed, to identify primary studies. The EUnetHTA report18 identified 2 SRs, 1 of which was the 2016 CADTH HTA,14 and 8 guidelines that contributed to their assessment of cTn POCT. The AIHTA17 update identified no new relevant SRs or guidelines and included 3 primary studies in 4 publications. Only studies relevant to this rapid review, 2 from each HTA,24,25,28,29 will be described in this report.
The EUnetHTA report18 included 1 study reported in 2 publications assessing a POCT program implemented in 36 remote health or community service centres in Australia’s Northern Territory.25,29 Staff at the relevant health centres were invited to participate in a satisfaction survey (n = 127) regarding their perceptions before and after implementation of the POCT program.
The other 2 included primary observational studies19,20 also assessed Australia’s Northern Territory POCT Program, auditing clinical outcomes. Matthews et al. (2020)19 included data from up to 80 remote sites within this region, while Spaeth et al. (2017)20 included data from 6 remote health centres and limited participants to those with a primary presentation of chest pain, normal ECG, and clinical symptoms suggestive of NSTEMI. Time from onset of symptoms to presentation was not reported in either publication. In this region, patients can be transferred to 1 of 2 hospitals, typically by airplane or helicopter, and the average distance from practice to the hospital is 275 km (range, 100 to 700 km).
The AIHTA report17 included 2 relevant uncontrolled observational studies, both of which were conducted in New Zealand, and one28 is a pilot study of the other.24 These 2 studies had similar eligibility criteria: the pilot study28 included adult patients presenting to 1 of 12 rural family practices (n = 180 participants) for whom symptoms of suspected ACS began within 72 hours of presentation and transfer to hospital for serial cTn measurement was intended. The subsequent study24 recruited from up to 29 sites (n = 1,205 participants) and, while it recruited from rural hospitals and general and urgent care practices, it was included in this review as eligibility was limited to patients who would have required transfer for an urgent hospital-based assessment if they had presented to a general or urgent care practice. In both studies, practices do not include specialist care or central laboratory services and could be hours from the nearest metropolitan hospital. Participant baseline characteristics were similar between these 2 studies for most risk factors, although Norman et al. (2022)28 may have included a higher proportion of smokers and those with a family history of cardiovascular disease. Importantly, the study populations had different medians of time from pain onset to initial assessment: approximately 15 hours in Norman et al. (2022)28 and approximately 4.5 hours in Miller et al. (2022).24
Interventions and Comparators
Eligibility for inclusion in the 2 HTAs was limited to quantitative cTn POCT devices available in Europe. The AIHTA report17 intended to prioritize evidence from high-sensitivity cTn POCTs over non–high-sensitivity cTn POCTs but found no studies using the former. Both reviews considered all comparators of current diagnostic practice. Nearly all studies identified by the HTAs and this rapid review exclusively report using the i-STAT cTnI test and 3 studies specifically report using this as 1 component of a clinical decision pathway or ADP.20,24,28 All publications described study or program-specific training and quality control measures.
Two studies24,28 from the AIHTA report17 examined the use of cTnI POCT as part of the Rural Accelerated Chest Pain Protocol (RACPP), which was modified from a validated metropolitan ED chest pain ADP.24,28 This ADP includes, among other assessments, ECG and cTn POCT measurements at presentation and at 2 hours. Both studies used the i-STAT cTnI test and one24 also used the AQT90 FLEX cTnT test. To increase sensitivity, both used a lower test cut-off for i-STAT than the manufacturer’s upper recommended limit based on the 99th percentile. For a patient to be classified as low risk, the following was required: no red flags (e.g., crescendo angina, hemodynamic instability, or ongoing chest pain), absence of potentially significant ECG changes at 0 and 2 hours, an Emergency Department Assessment of Chest Pain Score30 of less than 16, and serial cTn concentrations below the lower rule-out threshold at 0 and 2 hours (i-STAT: 0.04 mcg/L; AQT90: 18 ng/L). If all criteria were met, the patients were discharged home with follow-up as appropriate based on the clinician’s assessment. If these criteria were not met or a change of 0.02 mcg/L or more in cTnI levels was observed on the i-STAT test, patients were transferred to a referral centre or admitted to hospital.
Spaeth et al. (2017)20 examined the use of cTnI as part of a modified standard care protocol similar to, but less specific than, that used in other studies (they state they used serial cTn measures at 0 and < 8 hours from presentation and did not state a cTnI concentration used to rule out MI).
Outcomes
The 2 HTAs17,18 included outcomes as eligibility criteria. They did not prespecify outcome definitions or methods of measurement other than for major adverse cardiovascular events (MACE). The outcomes assessed in the HTAs (with primary studies reporting these outcomes also referenced) include:
MACE,17,18 a composite outcome, was defined in the AIHTA report as ACS, percutaneous coronary intervention, coronary artery bypass grafting, coronary angiography revealing procedurally correctable stenosis managed conservatively, and all-cause mortality
other safety outcomes (adverse events,17,18 serious adverse events17)
measures of diagnostic accuracy (specifically: sensitivity, specificity, positive and negative predictive value)17
patient quality of life (QoL) or health-related quality of life17,18
patient satisfaction17
staff satisfaction17
treatment initiation18
time to discharge18
length of stay18
further diagnostic testing18
Additional relevant outcomes planned in the included primary studies were:
clinician adherence to pathway28
number of tests outside a defined critical action limit (i.e., a positive test) and clinical conditions of relevant patients.19
Research Question 3: Evidence-Based Guideline Recommendations on Use of cTnI Point-of-Care Testing in Community Health Care in Rural and Remote Settings
No evidence-based guidelines were identified that recommended best practices specific to cTnI POCTs in community health care and primary care settings in rural and remote locations.
Summary of Findings
Appendix 3 presents the main study findings.
Research Question 1: Current Use of cTnI Point-of-Care Testing in Community Health Centres in Rural and Remote Settings
Our search identified no information on the current use of cTnI POCT in rural or remote community health care settings in Canada. Appendix 3 (Table 5) includes details of 2 point-of-care testing programs in rural or remote settings that include cTnI POCTs; 1 in Australia and 1 in New Zealand.19,20,23 While not exhaustively searched and identified, these examples serve to provide approaches to structured governance and oversight, training and quality control, challenges experienced in these settings, and may inform the use of these devices in Canada. We also identified 2 surveys on GPs’ current and desired use of cTnI POCTs, in South Africa and Germany which, given health system and population dispersion differences, have limited applicability to the setting in Canada.
Current Use of cTn POC Devices
Data on the current use of cTn POCTs comes from 2 surveys and 1 program evaluation (Appendix 3, Table 6). Both surveys assessed the current and desired use of POCTs more generally, including specific questions regarding cTn POCTs. Matthes et al. (2023),21 mailed invitations to more than 2,000 GPs in urban and rural community practices in 3 German federal states in 2022; the total response rate was 14.5%. Thirty-nine percent of GPs from rural community practices reported regular use of cTn POCTs, 35.4% reported infrequent use, and 25.6% reported no use. The authors reported no statistically significant difference between rural and urban GPs’ use of cTn POCTs. Mashamba-Thompson et al. (2018)22 surveyed staff at 100 randomly selected rural primary health care clinics in KwaZulu-Natal, South Africa. Although the survey explicitly asked about current and desired use of cTn POCTs, the authors did not present responses about this test in the publication. The presentation of results was limited to the following: most frequently used tests, top 20 desired POCTs, and top 10 desirable POCTs by disease class, of which cTn POCTs were not rated. Based on the limited information, we can only conclude that cTn POCTs were not one of the most frequently used or desired tests, with less than 10% of respondents from this study indicating desired future need for cTn POCTs.
The 2020 report evaluating Australia’s Northern Territory POCT Program, implemented in 2008, showed a steady increase in cTnI POCT use over the first 4 years of the program.19
Context: Distance to Tertiary Care
In Australia’s Northern Territory POCT Program, 97.5% of remote health clinics are considered very remote. The region includes 2 tertiary care hospitals with an average distance of 275 km (range, 100 to 700 km) from practices to hospitals.19 Distances between centres of the various POCT programs in New Zealand were not described by Herd et al. (2021).23
The distance or time from study sites to specialist care and laboratory services was also described in the following included studies:
Miller et al. (2022):24 from 45 minutes to 4 hours and 20 minutes
Norman et al. (2022):28 0.01 km to 62.7 km (1 to 79 minutes) to a rural hospital and 32.0 to 178.4 km (30 to 152 minutes) to a base hospital
Mashamba-Thompson et al. (2018):22 the mean distance was 41.4 (standard deviation = 42.8) km, with 40% of practices within 10 km of the hospital.
Context: Method of Patient Transportation to Tertiary Care
We identified little information on transport methods from rural to tertiary care centres. Reports on Australia’s Northern Territory POCT Program state that patients can be transferred to 1 of 2 hospitals, typically by airplane or helicopter.19,20,25,29 Additionally, a report24 from a study included in 1 HTA17 noted that 1 study site may require transportation by helicopter or boat, but the mode of transportation was not specified for other sites.
Research Question 2: Clinical Use of cTnI Point-of-Care Testing in Community Health Centres in Rural and Remote Settings
We identified 2 HTAs17,18 and 2 primary observational studies19,20 examining the clinical utility of cTnI POCTs in community health or primary care centres in rural and remote settings. Three studies (224,28 included in 1 HTA17 and 1 primary study20) described cTnI POCT use as part of an ADP (i.e., a clinical decision algorithm) and the results suggest that a suspected ACS-ADP using cTnI POCTs may be beneficial to identify low-risk patients and safely avoid unnecessary referrals or patient transfers. However, the evidence of clinical utility in these settings comes from a few uncontrolled observational studies focused primarily on 1 cTnI POCT (i-STAT test) used within specific ADPs. As such, the results cannot be translated to other cTnI POCT devices nor those used within other ADPs. It is unclear if the results are valid in other rural and remote settings. Limited information was provided on patients’ acceptability and satisfaction with care.
Major Adverse Cardiovascular Events
One HTA17 identified 2 uncontrolled studies24,28 assessing MACE at 30 days. The HTA authors assessed these studies to be at serious and critical risk of bias. The 2 studies used similar ADPs, using the RACPP to stratify patient risk and guide patient transfer and hospital admission decisions. Both studies reported no MACE in patients designated as low risk and at least 1 MACE was experienced by 13%28 and 23%24 of participants designated as non–low risk.
Measures of Diagnostic Accuracy of RACPP
One HTA17 identified 2 uncontrolled studies24,28 assessing the diagnostic accuracy of the RACPP to predict 30-day MACE. The HTA authors assessed these studies to be at serious and critical risk of bias. The results for Miller et al. (2022)24 and Norman et al. (2022),28 respectively, are as follows:
sensitivity: 100% (95% confidence interval [CI], 97.3% to 100%) and 100.0% (95% CI, 70.1% to 100.0%)
negative predictive value: 100% (95% CI, 99.2% to 100%) and 100.0% (95% CI, 96.7% to 100.0%)
specificity: 50.7% (95% CI, 47.5% to 53.9%) and 63.8% (95% CI, 56.4% to 70.6%)
positive predictive value: 23.0% (95% CI, 19.8% to 26.6%) and 12.5% (95% CI, 6.7% to 22.1%).
Hospital Referrals, Admissions, Patient Evacuations
One HTA,17 including 2 uncontrolled studies,24,28 and 1 other primary study20 assessed hospital referrals, admissions, or patient evacuations (Appendix 3, Table 9). Miller et al. (2022)24 and Norman et al. (2022)28 reported that 91.8% (95% CI, 88.8% to 93.9%) and 100% of patients designated as low risk for MI, respectively, were never transferred or admitted to hospital (i.e., were discharged home). Spaeth et al. (2017)20 included 2 outcomes in this domain. The first outcome was defined as the number of patients designated as cTnI negative within the context of a POCT pathway (i.e., low risk) compared to those who were cTnI positive who were evacuated (10% versus 100%, respectively). The second outcome was based on a retrospective chart analysis by a senior rural medical practitioner who predicted whether patients would have been evacuated at the time of their assessment had cTnI POCTs not been available. The authors reported that cTnI POCTs might have helped avoid 38% of evacuations due to an inability, in their absence, to rule out cardiac involvement; all patients who were cTnI negative who were evacuated would still have been evacuated without cTnI POCTs due to their condition; and of those who were cTn-positive (n = 7), approximately one-half would not have been evacuated without cTnI POCT testing and would likely have experienced a poorer outcome.
Time to Diagnosis, Time to Treatment, and Door-to-Needle Time
One retrospective primary study20 reported both the time from cTnI POCT administration to diagnosis and to treatment. The authors presented summary measures based on whether patients received a single POCT or serial cTnI POCTs, had positive or negative results, and were evacuated or not. As the numbers are small within most groups and interquartile ranges are wide, conclusions cannot be drawn. Table 10 and Table 11 contain the summary measures by group.
Patient Satisfaction
One HTA17 identified 1 observational study28 assessing patient satisfaction with their care when care was guided by the RACPP that included cTnI POCT (Appendix 3, Table 12). Patient response rate was 75% (of 148 participants included in this analysis) and most patients reported “Good” or “Excellent” overall satisfaction with the service they received (94.0% of 67 low-risk patients and 95.5% of 44 non–low-risk patients, including 37 of the latter who were transferred to hospital).
Staff Satisfaction
The 2 HTAs17,18 identified 2 studies reported in 3 publications that assessed staff satisfaction (Appendix 3, Table 13).25,28,29 Norman et al. (2022)28 did not define this outcome and reported that “The pathway was considered feasible and acceptable by the general practices to the extent that it has been maintained as the standard of care in the participating centres.” Shephard et al. (2012, 2014)25,29 defined this outcome as “staff satisfaction with pathology services” and collected data using online questionnaires approximately 1 year after introducing the i-STAT POCT program. The results were based on recalled satisfaction for both before implementation and after implementation outcomes. The response rate was 31% (of 127 potential respondents) and results suggested perceived improvements between overall satisfaction of cTn testing in general and timeliness of acute test results before implementation (with laboratory-based assays) versus after implementation (with POCT-based assays). Each question had missing data and results should be interpreted with caution.
Adherence to Pathway
One HTA17 identified 1 uncontrolled observational pilot study28 assessing physicians’ and patients’ adherence to the RACPP (Appendix 3, Table 14). They reported adherence to the protocol for 95.5% of the 111 patients designated as low risk by the ADP and 81.2% of the 69 patients designated as non–low risk. In the low-risk group, 4 participants did not undergo the 2-hour assessment due to a diagnosis of non-cardiac chest pain and 1 refused to remain at the practice. In the non–low-risk group, 13 participants were not transferred for hospital assessment, against pathway guidance; none of these patients had elevated cTnI or experienced MACE within 30 days.
Proportion of cTnI Tests Outside the Defined Critical Action Limits and Corresponding Patient Clinical Condition
One study19 evaluating Australia’s Northern Territory POCT Program examined the number of tests outside the critical action limits (i.e., positive tests) and the diagnosis of corresponding patients (Appendix 3, Table 15). Three percent of 1,398 cTnI POCTs administered between September and December 2019 were outside the defined clinical limits (> 0.09 ng/m). Corresponding patient clinical conditions included MI (n = 34; 2.4%), chronic kidney disease related, (n = 4; 0.3%), atrial fibrillation (n = 3; 0.2%), respiratory related (n = 2; 0.1%), and hypokalemia (n = 2; 0.1%).
Outcomes Predefined in HTAs, Not Reported in Included Studies
The 2 HTAs sought evidence regarding the following outcomes and no relevant evidence was identified: treatment initiation, health or patient-related QoL, adverse events, and serious adverse events, turnaround time, time to discharge, length of stay, and further diagnostic testing.
Research Question 3: Evidence-Based Guideline Recommendations on Use of cTnI Point-of-Care Testing in Community Health Care in Rural and Remote Settings
Our electronic database and grey literature search did not identify evidence-based guideline recommendations specific to the use of cTnI POCTs in community health or primary care centres in rural or remote settings.
Limitations
Our search identified no information regarding the current use of cTnI POCTs in rural and remote settings in Canada. Surveys that were identified on current and desired use of cTnI POCTs, conducted in Germany and South Africa, are not directly applicable to the context in Canada due to population dispersion and health systems differences. We identified 2 POCT programs, 1 in Australia and 1 in New Zealand, that specifically reference cTnI POCT use in community and primary care centres in rural or remote jurisdictions. The applicability of these programs to the context in Canada, while promising, will need to be considered. Other POCT programs and implementation guidelines identified during this assessment (within or outside the context in Canada) either did not specifically mention or assess cTnI POCTs, did not describe the context as community health or primary care centres in rural and remote settings (e.g., mixed settings, rural hospitals), or did not meet other review eligibility criteria.
We also identified limited evidence to inform the clinical utility of cTnI POCTs in community health centres in remote and rural settings in Canada. The included HTAs appear to be well conducted yet few primary research studies were identified, they lacked a control group, and were assessed as having high risk of bias (by the authors of the HTA). The included studies primarily focused on 1 device, i-STAT, which is available in Canada. While the results of included studies are promising, the evidence is not applicable to other devices due to variations in diagnostic accuracy and recommended diagnostic cut-off values between devices. The included clinical utility studies also considered cTnI POCTs in the context of 2 ADPs and, given cTnI POCT clinical utility is dependent on the ADP guiding patient management, the results of the studies included in this review should not be considered applicable outside of the ADP within which they were tested. Importantly, no study assessed high-sensitivity cTnI POCT devices.
While some existing guidelines provide specific recommendations with respect to components of the review questions (e.g., recommendations on the use of cTn POCTs without a specific setting or not specific to rural and remote settings), we did not identify an evidence-based clinical guideline providing recommendations specific to community health care in rural and remote settings for this rapid review.
Conclusions and Implications for Decision-Making or Policy-Making
This rapid review evaluated the evidence on the current use, clinical utility, and guideline recommendations regarding cTnI POCTs in rural and remote community health settings. Seven publications were included in the review: 2 HTAs (from which 3 primary studies in 4 reports were applicable), 4 primary observational studies, and 1 report describing experiences with POCT programs in New Zealand. The overall evidence-base to inform the use of cTnI POCT in these settings is limited and no studies were conducted in Canada. The results suggest that cTnI POCTs, when used within the context of an ACS-ADP, have the potential to identify patients who were low-risk (high sensitivity and negative predictive value), reduce unnecessary referrals or transfers, and increase patient and staff satisfaction when there is limited or no efficient access to laboratory-based results. However, the studies we identified did not include control groups and have risks to their validity (as assessed by the authors of the HTA). As such, while promising, the results should be considered in this context.
Our search identified 2 current POCT programs that include cTnI testing — 1 implemented in Australia’s Northern Territory and 1 in New Zealand. These programs may be informative to the context in Canada given the similarities between health care systems and population dispersion. The experiences and challenges described in relation to these programs19,31 highlight the importance of strong governance and oversight structures; continuing resource needs for training, accreditation, and quality control; advantages of centralized data collection and monitoring; and the challenges with high staff turnover in rural and remote regions, the latter also noted in Canada.11,27
The limited evidence on the clinical utility of cTnI POCTs identified in this review comes from studies conducted in New Zealand and Australia and it is not clear whether the results may be applicable to rural and remote community health care in Canada. Research on cTnI POCTs is more established in other settings (EDs, prehospital care, or emergency medical services) and some studies conducted within rural hospitals (e.g., Dee et al.32) may also be informative; however, potential differences in the patient population, such as underlying patient risk4 and access to subsequent care, make it challenging to translate these results to rural and remote community care settings. We also acknowledge there are different levels of rurality and remoteness and that decisions and preferences concerning availability of POCTs may need to vary depending on the setting.
Importantly, cTnI testing is not assessed as an isolated intervention. Rather, it is assessed within the context of suspected ACS-ADPs, in alignment with current guideline recommendations.7-9 These typically incorporate ECG results, clinical risk scores (e.g., based on symptoms, age, sex, history), and time points and cut-off values for cTnI testing (often laboratory-based) to guide patient management. Guidelines recommend validating suspected ACS-ADPs within the intended context9 as numerous factors can affect their utility, including time from symptom onset to presentation and local prevalence of other risk factors, patient transport protocols, staff training, patient preferences, and staff and patient fidelity with the protocols. Both the authors of the most recent HTA17 and those of largest prospective patient-focused study24 conclude that further assessment is needed (e.g., larger studies, RCTs, longer follow-up, validation of ADPs in the settings of interest). Additionally, limited evidence was available on patient-focused outcomes such as QoL and satisfaction with care and these would be valuable additions to future research. The included evidence was almost all conducted using i-STAT cTnI, the results of which are not generalizable to other cTnI POCT devices, and no studies assessed a high-sensitivity cTnI POCT device; this evolving technology may affect POCT recommendations.7
Our initial search for evidence-based guidelines did not identify any specific recommendations regarding the use of cTnI POCTs in rural and remote community care centres. Some reports included evidence-based recommendations on cTn testing but not specific to the settings of interest,33 while others provided recommendations but did not describe both a systematic search for evidence and a defined consensus process.27,34 The 2023 European Society of Cardiology Guidelines acknowledged this is a rapidly evolving field and that an update of current recommendations may be required with the introduction of high-sensitivity cTn POCT devices in clinical settings.
Since completion of this rapid review, the anticipated 2025 update35 to the 2016 ACS guidelines9 by the National Heart Foundation of Australia and the Cardiac Society of Australia and New Zealand has been released. While no recommendation specifically guides the use of cTnI POCTs in community health or primary care centres in rural and remote settings, this guideline describes factors associated with all these variables separately and includes considerations for care of priority populations including those living in remote areas. Specifically, authors recommend use of high-sensitivity cTn assays, wherever possible, versus contemporary (non-high sensitivity) cTn assays and, as with previous guidance, they recommend the use of an evidence-based clinical decision pathway. The authors discuss considerations for testing and interpreting results based on other factors, including age, race, and the effect of sex hormones for transgender individuals. Authors note that cTn POCTs may lead to more timely management with comparable safety to laboratory-based assays and that emerging evidence supports rapid assessment using high-sensitivity cTn assays. They also acknowledge that the evidence-base is rapidly evolving and that the use of POCTs with ADPs, including in primary care, may become more common. No specific recommendation is provided regarding use of cTn POCTs in rural and remote settings. The authors recommend, more broadly, the establishment of centralized support systems for regional and remote health services to facilitate prompt assistance with ECG interpretation and access to cTn results when onsite access is not available.
Overall, while the results of this rapid review suggest that, when used within the context of an ACS-ADP, cTnI POCTs have the potential to identify patients who were considered at low-risk and reduce unnecessary referrals or transfers for people presenting with symptoms of ACS in community health care in rural and remote settings (with limited access to laboratory-based results), there are concerns about the validity and applicability of the evidence. We found no evidence from studies conducted in Canada, the evidence was limited primarily to 1 device, and it was assessed within uncontrolled observational studies. As such, when considering implementation of these devices, it would be advantageous to first assess them within the context of a suspected ACS-ADP in the settings of interest. This is important to account for variables such as the underlying community cardiac risk factors, patient experience, available resources, and availability of trained, qualified personnel. The advent of high-sensitivity cTn POCTs holds promise to help overcome some of the concerns with currently available non–high-sensitivity -cTnI POCTs and future research will be important to better understand their utility. Health care decision-makers will ultimately need to balance the limited existing and emerging evidence with the challenges of their current standard of care.
Acknowledgements
We thank our content expert reviewer, Alexander Hoechsmann, BA, BSc, MD, Emergency Physician, Island Health, for his consultation on this report.
References
1.Public Health Agency of Canada. Heart Disease in Canada. 2022. Accessed December 19, 2024. https://www.canada.ca/en/public-health/services/publications/diseases-conditions/heart-disease-canada.html
2.Statistics Canada. Table 13-10-0801-01: Leading causes of death, total population (age standardization using 2011 population). 2025. Accessed December 19, 2024. https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1310080101&pickMembers%5B0%5D=2.1&cubeTimeFrame.startYear=2023&cubeTimeFrame.endYear=2023&referencePeriods=20230101%2C20230101
3.Public Health Agency of Canada. Heart Disease in Canada: Highlights from the Canadian Chronic Disease Surveillance System. 2017. Accessed December 20, 2024. https://www.canada.ca/content/dam/phac-aspc/documents/services/publications/diseases-conditions/heart-disease-fact-sheet/heart-disease-factsheet-eng.pdf
4.Faridi B, Davies S, Narendrula R, et al. Rural-urban disparities in mortality of patients with acute myocardial infarction and heart failure: a systematic review and meta-analysis. Eur J Prev Cardiol. 2025;32(4):327-335. doi:10.1093/eurjpc/zwae351 PubMed
5.Canadian Institute for Health Information. NACRS emergency department visits and lengths of stay. 2024. Accessed December 20, 2024. https://www.cihi.ca/en/nacrs-emergency-department-visits-and-lengths-of-stay
6.Ko DT, Dattani ND, Austin PC, et al. Emergency Department Volume and Outcomes for Patients After Chest Pain Assessment. Circ Cardiovasc Qual Outcomes. 2018;11(11):e004683. doi:10.1161/CIRCOUTCOMES.118.004683 PubMed
7.Byrne RA, Rossello X, Coughlan JJ, et al. 2023 ESC Guidelines for the management of acute coronary syndromes. Eur Heart J. 2023;44(38):3720-3826. doi:10.1093/eurheartj/ehad191 PubMed
8.Gulati M, Levy PD, Mukherjee D, et al. 2021 AHA/ACC/ASE/CHEST/SAEM/SCCT/SCMR Guideline for the Evaluation and Diagnosis of Chest Pain: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2021;144(22):e368-e454. doi:10.1161/CIR.0000000000001029 PubMed
9.Chew DP, Scott IA, Cullen L, et al. National Heart Foundation of Australia & Cardiac Society of Australia and New Zealand: Australian Clinical Guidelines for the Management of Acute Coronary Syndromes 2016. Heart Lung Circ. 2016;25(9):895-951. doi:10.1016/j.hlc.2016.06.789 PubMed
10.Canadian Institute for Health Information. Your Health System. Accessed December 10, 2024, https://yourhealthsystem.cihi.ca/hsp/indepth?lang=en#/
11.Young TK, Tabish T, Young SK, Healey G. Patient transportation in Canada's northern territories: patterns, costs and providers' perspectives. Rural Remote Health. 2019;19(2):5113. doi:10.22605/RRH5113 PubMed
12.Oosterveer TM, Young TK. Primary health care accessibility challenges in remote indigenous communities in Canada's North. Int J Circumpolar Health. 2015;74:29576. doi:10.3402/ijch.v74.29576 PubMed
13.Lin YH, Zhang Y, Liu YT, Cui K, Kang JS, Zhou Z. How to choose a point-of-care testing for troponin. J Clin Lab Anal. 2020;34(7):e23263. doi:10.1002/jcla.23263 PubMed
14.CADTH. Point-of-Care Troponin Testing in Patients With Symptoms Suggestive of Acute Coronary Syndrome: A Health Technology Assessment. (CADTH Optimal Use Report). 2016.
15.CADTH. Troponin I Point of Care Testing for Patients with Suspected Acute Coronary Syndrome or Myocardial Infarction: Clinical Utility, Cost-Effectiveness and Guidelines. (CADTH rapid response report: summary of abstracts). 2020.
16.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
17.Huic M, Erdos J, Wild C. Point of Care Tests (POCT): D-Dimer and Troponin. HTA-Austria: Austrian Institute for Health Technology Assessment GmBH; 2024. Accessed December 4, 2024. https://eprints.aihta.at/1524/1/HTA-Projektbericht_Nr.124_Update_2024.pdf
18.EUnetHTA OCTCA22 Assessment Team. POCT/ Point of Care Test: D-dimer and Troponin. EUnetHTA; 2019. Accessed December 13, 2024. https://www.eunethta.eu/wp-content/uploads/2019/12/POCT_POCT_final.pdf
19.Matthews SJ, Spaeth B, Duckworth L, et al. Sustained Quality and Service Delivery in an Expanding Point-of-Care Testing Network in Remote Australian Primary Health Care. Arch Pathol Lab Med. 2020;144(11):1381-1391. doi:10.5858/arpa.2020-0107-OA PubMed
20.Spaeth BA, Shephard MDS, Omond R. Clinical Application of Point-of-Care Testing in the Remote Primary Health Care Setting. Quality in Primary Care 2017;25(3):164-175.
21.Matthes A, Wolf F, Schmiemann G, Gagyor I, Bleidorn J, Markwart R. Point-of-care laboratory testing in primary care: utilization, limitations and perspectives of general practitioners in Germany. BMC Prim Care. 2023;24(1):96. doi:10.1186/s12875-023-02054-0 PubMed
22.Mashamba-Thompson TP, Sartorius B, Drain PK. Operational assessment of point-of-care diagnostics in rural primary healthcare clinics of KwaZulu-Natal, South Africa: a cross-sectional survey. BMC Health Serv Res. 2018;18(1):380. doi:10.1186/s12913-018-3207-6 PubMed
23.Herd GCE, Musaad SMA. Point-of-Care Testing in Rural and Remote Settings to Improve Access and Improve Outcomes: A Snapshot of the New Zealand Experience. Arch Pathol Lab Med. 2021;145(3):327-335. doi:10.5858/arpa.2020-0104-RA PubMed
24.Miller R, Nixon G, Pickering JW, et al. A prospective multi-centre study assessing the safety and effectiveness following the implementation of an accelerated chest pain pathway using point-of-care troponin for use in New Zealand rural hospital and primary care settings. Eur Heart J Acute Cardiovasc Care. 2022;11(5):418-427. doi:10.1093/ehjacc/zuac037 PubMed
25.Shephard MD, Spaeth BA, Mazzachi BC, et al. Toward Sustainable Point-of-Care Testing in Remote Australia: the Northern Territory i-STAT Point-of-Care Testing. Point of Care. 2014;13(1):6-11.
26.Demandt JPA, Zelis JM, Koks A, et al. Prehospital risk assessment in patients suspected of non-ST-segment elevation acute coronary syndrome: a systematic review and meta-analysis. BMJ Open. 2022;12(4):e057305. doi:10.1136/bmjopen-2021-057305 PubMed
27.Pant Pai N, Grignon M, Bornstein S, Navarro P, Mackey S. Troponin Point-of-Care Testing in Smaller Hospital and Health Centre Emergency Departments in Newfoundland and Labrador Newfoundland & Labrador Centre for Applied Health Research, Memorial University; 2014. Accessed December 12, 2024. https://www.mun.ca/nlcahr/media/production/memorial/administrative/nl-centre-for-applied-health-research/media-library/chrsp/POCT_Full_Report_1224.pdf
28.Norman T, Young J, Scott Jones J, et al. Implementation and evaluation of a rural general practice assessment pathway for possible cardiac chest pain using point-of-care troponin testing: a pilot study. BMJ Open. 2022;12(4):e044801. doi:10.1136/bmjopen-2020-044801 PubMed
29.Shephard MD, Spaeth B, Mazzachi BC, et al. Design, implementation and initial assessment of the Northern Territory Point-of-Care Testing Program. Aust J Rural Health. 2012;20(1):16-21. doi:10.1111/j.1440-1584.2011.01243.x PubMed
30.Than M, Flaws D, Sanders S, et al. Development and validation of the Emergency Department Assessment of Chest pain Score and 2 h accelerated diagnostic protocol. Emerg Med Australas. 2014;26(1):34-44. doi:10.1111/1742-6723.12164 PubMed
31.New Zealand Point-of-Care Testing Advisory Group. New Zealand Best Practice Guidelines for Point-of-Care Testing. Royal College of Pathologists of Australasia; 2022. Accessed December 12, 2024. https://irp.cdn-website.com/102112c1/files/uploaded/2022%20NZPOCTAG%20Guidelines.pdf#:~:text=The%20New%20Zealand%20POCT%20Advisory%20Group%20%28NZPOCTAG%29%20was,by%20POCT%20services%20and%20providers%20in%20New%20Zealand.
32.Dee F, Savage L, Leitch JW, et al. Management of Acute Coronary Syndromes in Patients in Rural Australia: The MORACS Randomized Clinical Trial. JAMA Cardiol. 2022;7(7):690-698. doi:10.1001/jamacardio.2022.1188 PubMed
33.Collinson P, Aakre KM, Saenger A, et al. Cardiac troponin measurement at the point of care: educational recommendations on analytical and clinical aspects by the IFCC Committee on Clinical Applications of Cardiac Bio-Markers (IFCC C-CB). Clin Chem Lab Med. 2023;61(6):989-998. doi:10.1515/cclm-2022-1270 PubMed
34.Cardiac Care Network. Management of Acute Coronary Syndromes: Best Practice Recommendations for Remote communities. 2013. Accessed December 12, 2024. https://www.corhealthontario.ca/ACS-management-in-remote-communities-FINAL-Sept-2013.pdf
35.Brieger D, Cullen L, Briffa T, et al. National Heart Foundation of Australia & Cardiac Society of Australia and New Zealand: Comprehensive Australian Clinical Guideline for Diagnosing and Managing Acute Coronary Syndromes 2025. Heart Lung Circ. 2025;34(4):309-397. doi:10.1016/j.hlc.2025.02.102 PubMed
36.Spaeth BA, Kaambwa B, Shephard MD, Omond R. Economic evaluation of point-of-care testing in the remote primary health care setting of Australia's Northern Territory. Clinicoecon Outcomes Res. 2018;10:269-277. doi:10.2147/CEOR.S160291 PubMed
37.Health New Zealand, Te Whatu Ora. Rural alliance - Auckland and Waitematā: R-POCT (Rural Point of Care Testing Service). Accessed December 17, 2024, https://www.waitematadhb.govt.nz/about-us/rural-alliance/r-poct/
Appendix 1: Detailed Methods and Selection of Included Studies
Please note that this appendix has not been copy-edited.
Literature Search Methods
An information specialist conducted a literature search on key resources including MEDLINE, the Cochrane Database of Systematic Reviews, the International HTA Database, the websites of HTA agencies in Canada and major international HTA agencies, as well as a focused internet search. The search approach was customized to retrieve a limited set of results, balancing comprehensiveness with relevance. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (medical subject headings), and keywords. Search concepts were developed based on the elements of the research questions and selection criteria. The main search concepts were cTnI POCT and the rural or remote setting. To address question 3, search filters were applied to limit retrieval to HTAs, SRs, meta-analyses, or indirect treatment comparisons and guidelines; no filters were applied to limit the retrieval by study type for questions 1 and 2. The search was completed on November 28, 2024, and limited to English-language documents published since January 1, 2009. Internet links were provided, where available. We provide the search strategy for MEDLINE in Table 2.
Table 2: Search Strategy for Ovid MEDLINE (1946 to November 27, 2024)
Terms | Results |
|---|---|
1. exp “Point-of-Care Systems”/ | 21,753 |
2. (portable or hand-held or mobile or point of care or near patient or bedside or bed side or hand-held or POC or POCT or ambulatory or rapid test or rapid tests or rapid testing or rapid screen or rapid screening or remote test or remote tests or remote testing or rapid diagnostic test or rapid diagnostic tests or rapid diagnosis or rapid diagnoses or transportable or test kit or test kits).ti,ab,kf. | 409,330 |
3. (point adj4 care adj4 (test or testing or assay or assays)).ti,ab,kf. | 12,478 |
4. (portable adj4 (test or testing or assay or assays)).ti,ab,kf. | 1,332 |
5. ((rapid or bedside or bed side) adj4 (test or testing or assay or assays)).ti,ab,kf. | 43,049 |
6. 1 or 2 or 3 or 4 or 5 | 439,716 |
7. exp Troponin/ | 21,493 |
8. (troponin* or cTn* or TnI* or TnT*).ti,ab,kf. | 50,400 |
9. cardiac biomarker*.ti,ab,kf. | 4,083 |
10. 7 or 8 or 9 | 55,040 |
11. 6 and 10 | 1,704 |
12. (i?STAT or iSTAT or ISTATr or triage cardiac or cardio2 or cardio3 or Alfa Scientific or Instant View or (Vidas adj5 ultra) or miniVidas or LifeSign or Meritas or PathFast or Cardiac STATus or AQT90 or AQT90flex or (Response and RAMP) or Cobas h232 or “Cobas h 232” or Cardiac Reader or Stratus CS or (ZAP and troponin) or GEM Immuno or ReLIA TZ* or Radiometer AQ* or ATQ90* or Atellica?VTLi or Triage?True).ti,ab,kf. | 3,636 |
13. (triage and Alere).ti,ab,kf. | 36 |
14. (bioMerieux and Vidas).ti,ab,kf. | 226 |
15. (Roche and (“ Trop T” or “Troponin T” or TropT) and cardiac).ti,ab,kf. | 199 |
16. 12 or 13 or 14 or 15 | 4,067 |
17. 11 or 16 | 5,693 |
18. Rural Population/ or Rural Health/ or exp Rural Health Services/ or Hospitals, Rural/ or Regional Medical Programs/ or Medically Underserved Area/ or Health Services, Indigenous/ or exp Community Health Services/ or exp ambulatory care facilities/ | 499,627 |
19. (underserved or under-served or rural* or countryside* or country-side* or non-urban or nonurban or non-metropolitan or nonmetropolitan or remote* or mountain* or wilderness or outpost* or village* or resource-poor or resource limited or resource constrained or fly-in or Arctic or isolated communit* or community health centre* or community health centre* or primary care or general practition* or pre?hospital or (urgent adj3 care adj3 clinic*)).ti,ab,kf. | 639,911 |
20. 18 or 19 | 1,018,854 |
21. 17 and 20 | 219 |
22.limit 21 to (english language and yr = ”2009 -Current”) | 174 |
23. (systematic review or meta-analysis).pt. | 369,111 |
24. meta-analysis/ or systematic review/ or systematic reviews as topic/ or meta-analysis as topic/ or “meta-analysis (topic)”/ or “systematic review (topic)”/ or exp technology assessment, biomedical/ or network meta-analysis/ | 412,452 |
25. ((systematic* adj3 (review* or overview*)) or (methodologic* adj3 (review* or overview*))).ti,ab,kf. | 390,927 |
26. ((quantitative adj3 (review* or overview* or synthes*)) or (research adj3 (integrati* or overview*))).ti,ab,kf. | 18,632 |
27. ((integrative adj3 (review* or overview*)) or (collaborative adj3 (review* or overview*)) or (pool* adj3 analy*)).ti,ab,kf. | 44,666 |
28. (data synthes* or data extraction* or data abstraction*).ti,ab,kf. | 48,317 |
29. (handsearch* or hand search*).ti,ab,kf. | 11,834 |
30. (mantel haenszel or peto or der simonian or dersimonian or fixed effect* or latin square*).ti,ab,kf. | 40,009 |
31. (met analy* or metanaly* or technology assessment* or HTA or HTAs or technology overview* or technology appraisal*).ti,ab,kf. | 13,631 |
32. (meta regression* or metaregression*).ti,ab,kf. | 17,501 |
33. (meta-analy* or metaanaly* or systematic review* or biomedical technology assessment* or bio-medical technology assessment*).mp,hw. | 550,703 |
34. (medline or cochrane or pubmed or medlars or embase or cinahl).ti,ab,hw. | 406,400 |
35. (cochrane or (health adj2 technology assessment) or evidence report).jw. | 22,224 |
36. (comparative adj3 (efficacy or effectiveness)).ti,ab,kf. | 20,069 |
37. (outcomes research or relative effectiveness).ti,ab,kf. | 12,081 |
38. ((indirect or indirect treatment or mixed-treatment or bayesian) adj3 comparison*).ti,ab,kf. | 4,828 |
39. [(meta-analysis or systematic review).md.] | 0 |
40. (multi* adj3 treatment adj3 comparison*).ti,ab,kf. | 321 |
41. (mixed adj3 treatment adj3 (meta-analy* or metaanaly*)).ti,ab,kf. | 184 |
42. umbrella review*.ti,ab,kf. | 2,383 |
43. (multi* adj2 paramet* adj2 evidence adj2 synthesis).ti,ab,kf. | 15 |
44. (multiparamet* adj2 evidence adj2 synthesis).ti,ab,kf. | 19 |
45. (multi-paramet* adj2 evidence adj2 synthesis).ti,ab,kf. | 13 |
46. or/23 to 45 | 796,491 |
47. 17 and 46 | 76 |
48. limit 47 to (english language and yr = ”2009 -Current”) | 63 |
49. (guideline or practice guideline or consensus development conference or consensus development conference, NIH).pt. | 49,816 |
50. (guideline* or standards or consensus* or recommendat*).ti. | 208,203 |
51. (practice parameter* or position statement* or policy statement* or CPG or CPGs or best practice*).ti. | 20,162 |
52. (care adj2 (path or paths or pathway or pathways or map or maps or plan or plans or standard)).ti. | 9,787 |
53. ((critical or clinical or practice) adj2 (path or paths or pathway or pathways or protocol*)).ti. | 5,192 |
54. (algorithm* and (pharmacotherap* or chemotherap* or chemotreatment* or therap* or treatment* or intervention*)).ti. | 4,184 |
55. (algorithm* and (screening or examination or test or tested or testing or assessment* or diagnosis or diagnoses or diagnosed or diagnosing)).ti. | 5,055 |
56. (guideline* or standards or consensus* or recommendat*).au. | 11 |
57. [(guideline* or standards or consensus* or recommendat*).co.] | 0 |
58. (guideline* or standards or consensus* or recommendat*).ca. | 2,535 |
59. systematic review.ti,pt,kf,sh. and (practice guideline* or treatment guideline* or clinical guideline* or guideline recommendation*).ti,ab,kf. | 5,126 |
60. or/49 to 59 | 273,028 |
61. 17 and 60 | 40 |
62. limit 61 to (english language and yr = ”2009 -Current”) | 32 |
63. 48 or 62 | 93 |
64. 21 or 63 | 296 |
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, they were duplicate publications or were published before 2009. SRs in which all relevant studies were captured in other more recent or more comprehensive SRs were excluded. Primary studies retrieved by the search were excluded if they were captured in 1 or more included SRs. Guidelines with unclear methodology were also excluded. Studies conducted in urban settings, hospitals or EDs or mixed settings, unless results were reported separately for rural and remote settings, were not eligible.
Critical Appraisal of Individual Studies
We did not conduct a formal critical appraisal of individual studies for this review. The limitations of the included studies are discussed.
Appendix 2: Characteristics of Included Publications
Table 3: Characteristics of Included Health Technology Assessments
Study citation, country, funding source | Search, study designs, numbers of primary studies included | Population characteristics, settings | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Huic et al. (2024)17 Austria Funding source: Not directly stated – created by AIHTA | This review updated (with a narrower focus) the EUnetHTA (2019) HTA.18 This review aims to assess the clinical utility of troponin (in patients with suspected MI) and D-Dimer (in patients with suspected deep vein thrombosis or pulmonary embolism) POCT. The present summary is limited to the methods and results of troponin POCT. Search dates and limits: June 1, 2019, to March 1, 2024; German and English studies only Eligible study designs:
Included studies:
| Participants: Adult patients (≥ 18 years) with suspected NSTE-ASC (including signs/symptoms such as chest pain or breathlessness potentially indicative of acute MI) Exclusions: Specific high-risk groups (STEMI) Settings: Primary and community care (general practice, internal medicine or pulmonology in private practice) | Intervention: Quantitative D-dimer or troponin POCT with the intention to rule-out acute disease. For troponin, they favoured high-sensitivity (hs) tests but would consider non-hs POCT if the latter was not available. Comparator: Current diagnostic practice; all comparators eligible Intervention in 2 relevant included studies: Rural accelerated diagnostic chest pain pathway (RACPP) which included Abbott i-STAT troponin POCT to “rule out” MI | Outcomes:
Follow-up: None stated; 2 relevant studies included outcomes up to 30 days follow-up |
EUnetHTA OTCA22 Assessment Team. (2019)18 The Netherlands Funding source: European Union’s Health Programme | This review aims to assess the clinical utility of troponin and D-Dimer POCT. The present summary is limited to the methods and results for assessing troponin POCT. Search dates and limits: 2009 to 2019 for SRs and HTAs; up to 2019 for guidelines; 2016 to 2019 for primary studies; German and English studies only Eligible study designs:
Included studies: | Participants: Adult patients (≥ 18 years old) with signs or symptoms suggested of ACS, such as chest pain or breathlessness presenting in ambulatory or emergency settings in whom MI is suspected and has not been ruled out Settings: Ambulatory (primary or community) or emergency care | Interventions:
Comparator: Usual care – any (including central laboratory methods) Intervention in 2 relevant included studies: Abbott i-STAT | Outcomes:
Follow-up: None prespecified |
ACS = acute coronary syndrome; AE = adverse event; AIHTA = Austrian Institute for Health Technology Assessment; cTnI = cardiac troponin I; cTnT = cardiac troponin T; ED = emergency department; EUnetHTA = European Network for Health Technology Assessment; HTA = health technology assessment; hs = high sensitivity; MA = meta-analysis; MACE = major adverse cardiovascular events; MI = myocardial infarction; NSTE-ASC = non–ST-segment elevation acute coronary syndrome; POCT = point-of-care test; QoL = quality of life; RACPP = Rural Accelerated Chest Pain Pathway; RCT = randomized controlled trial; SAE = serious adverse event; SR = systematic review; STEMI = ST-elevation acute myocardial infarction.
Note: This table has not been copy-edited.
aMACE is defined as a combined end point of ACS, percutaneous coronary intervention, coronary artery bypass grafting, coronary angiography revealing procedurally correctable stenosis managed conservatively and all-cause mortality.
Table 4: Characteristics of Included Primary Clinical Studies
Study citation, country, funding source | Study design, Study setting, Study duration, Number of participants | Population characteristics, Inclusion criteria, Exclusion criteria | Intervention and comparator(s), POCT device/manufacturer, Troponin test, Test protocol | Health care professional(s) performing test, Training/Quality control | Outcomes, Length of follow-up |
|---|---|---|---|---|---|
Matthes et al. (2023)21 Germany Funding/support: Open Access funding by Projekt DEAL. The study is embedded in the project POCT-ambulant which is funded by the Bundesministerium für Bildung und Forschung (Ministry of Education and Research). “The funding source had no role in the design, conduct or reporting of this study; or in the decision to submit the manuscript for publication.” | Cross-sectional study; survey Settings/Sites: Outpatient general practices in Germany from 3 federal states; results for cTn POCT reported separately for rural and other settings Duration: NA Number of participants:
| Inclusion: General practitioners from 3 German federal states Exclusion: None Characteristics: Characteristics such as age, sex, work experience, practice type reported but this data not separated for practitioners in rural practice locations (n = 84 / 2014) Authors noted overrepresentation of GPs in rural settings (‘slightly over-represented’) and females (60% vs. 49%) compared to survey population characteristics | Intervention: Mailed survey; 12 questions on POCT utilization and limitations, and perspectives toward POCT use in general practice. Included specific question on current use of cTnI/cTnT POCTs. Device/manufacturer: Any; not stated | Training/Quality Control: NA | Outcomes:
|
From AIHTA (2024)17 (relevant study 1 of 2) Miller et al. (2022)24 New Zealand Funding: Heart Foundation of New Zealand; Abbott Diagnostics Point of Care investigator grant | Prospective observational study Settings/Sites: 27 to 29 (depending on reporting in paper) sites: 75.9% of patients presented to rural hospitals, 20.2% to general practices 3.8% to urgent care clinics. Sites were at least 45 minutes (up to 4 hours 20 minutes) drive from nearest metropolitan hospital with specialist care and central laboratory services. Means of transportation are not all described but include helicopter, boat and road. Duration: 30 days after presentation Number of participants; 1,205 enrolled; 132 (11%) excluded mostly due to protocol breaches. 1,073 included in primary analysis. Low risk: 474 (44%) Not low risk: 599 (56%) | Inclusion: Adults with symptoms suggestive of cardiac ischemia or AMI that began or worsened within the last 72 hour and ordinarily requiring transfer for an urgent hospital-based assessment if presenting to a primary care setting (GP or urgent care) Exclusion: Those who presented with STEMI; proven or suspected non-coronary artery cause; required transfer regardless of RACPP result; anticipated follow-up concern. Median time from pain onset to initial assessment: Low risk group: 4 hours and 36 minutes (IQR: 2 hours to 14 hours and 30 minutes) Not low-risk group: 4 hours and 20 minutes (IQR: 2 hours and 8 minutes to 10 hours and 9 minutes) Age (Mean (SD)): 63 (15) Sex: 48% Female; 52% Male Hypertension: 47% Dyslipidemia: 30% Diabetes: 15% Current smoker: 15% Family history of premature CAD: 14% Obesity: 11% | Intervention: RACPP including EDACS, ECG and 2 cTn POCTs – 1 at presentation and 1 at 2 hours Device/manufacturer:
RACPP:
High risk: i-STAT - any cTn concentration above URL or between thresholds but changes between tests of ≥ 0.02 mcg/L | Predominantly nurses Training/Quality Control: Manufacturers installed the necessary hardware, trained, and certified device users. Ongoing quality control included daily electronic and liquid quality control sampling. Study authors provided sites with education, training and support to implement the pathway. | Outcomes:
|
From AIHTA (2024)17 (relevant study 2 of 2) Norman et al. (2022)28 New Zealand Funding/support: Heart Foundation of New Zealand; Waikato Medical Research Foundation; Devices and training provided by Abbott Point of Care | Prospective observational study Settings/Sites: 12 rural general practices. Patients can be transferred to 1 metropolitan ED or 1 of 4 rural hospitals. Distance (time) from practice to rural hospital ranged from 0.01 km to 62.7 km (1 to 79 minutes) and distance from practice to base hospital ranged from 32.0 to 178.4 km (30 to 152 minutes) Duration: 30 days after presentation Number of participants:
| Inclusion: Patients ≥ 18 years old, presenting to rural general practice with suspected ischemic chest pain for whom the doctor intended transfer to hospital for serial troponin measurement Exclusion: Those who presented with STEMI; proven or suspected non-coronary artery cause; required transfer regardless of RACPP result; chest pain > 72 hours; re-presentation with chest pain during the evaluation period; anticipated follow-up concern Median time from pain onset to initial assessment:
Age (Mean years (SD)):
Sex (% Women):
Hypertension (%):
Dyslipidemia:
Diabetes mellitus:
Current smoker:
Family history of premature CAD:
Known ischemic heart disease:
| Intervention: RACPP adapted for management of suspected cardiac chest pain in rural practices including EDACS, ECG and 2 troponin POCTs – 1 at presentation and 1 at 2 hours. Device/manufacturer:
Reference laboratory diagnostic tests (duplicate samples at both time points):
RACPP:
| Training/Quality Control: Onsite training and performance were provided by an Abbott Point of Care representative to identify ‘primary users’ at each site who could train others and run quality control. Sites were given face-to-face education regarding the pathway. | Outcomes:
|
Matthews et al. (2020)19 Australia Funding: Northern Territory Department of Health’ Northern Territory Department of Health and no financial COI | Program evaluation – descriptive Settings/Sites: Up to 80 remote health centres Northern Territory POCT program. 97.5% are in ‘very remote locations’ and the remainder in ‘outer regional’ as described by Australia’s Remoteness Structure. Patients can be transferred to 1 of 2 hospitals typically by airplane or helicopter. Average distance from practice to hospital is 275 km (range: 100 to 700 km) Number of participants: Not stated. Total cTnI cartridges used for this study: 1,398 | Inclusion: clinical audit results from September 1 to December 31, 2019 Exclusion: NR | Intervention: i-STAT Point-of-Care Testing Program using 4 testing cartridges, 1 being cTnI Device/manufacturer: i-STAT 300 analyzer/Abbott Point of Care and the following cartridges: Chem8+, CG4+, PT/INR, cTnI | Training/Quality Control:
| Outcomes:
|
From EUnetHTA (2019)18 HTA (2 relevant studies) Shephard et al. (2014)25 and Shephard et al. (2012)29 Program also assessed in Matthews et al. (2020)19 (program evaluation, included separately in this table), Spaeth et al. (2018)36 (economic evaluation, excluded) and Spaeth et al. (2017)20 (included separately in this table) Australia Funding/support: Study 1:25 The authors declare no funding was received for this work and no COI Study 2:29 ‘Sources of support that require acknowledgement: Northern Territory Department of Health’ | Program description and evaluations with survey Settings/Sites: 33 remote health centres from the Northern Territory Department of Health and 3 Aboriginala Community Controlled Health Services of the Aboriginal Medical Services Alliance of the Northern Territory. Patients can be transferred to 1 of 2 hospitals typically by airplane or helicopter. Average distance from practice to hospital is 275 km (range: 100 to 700 km) Number of participants: The 2012 survey results seem to be repeated (in part) in 2014 publication: 39 respondents (31%) of 127 operators sent the questionnaire; other data captured electronically. Conducted 1 year after program inception. | Inclusion: Staff at all remote health centres participating in the POCT program Exclusion: NR | Intervention: i-STAT Point-of-Care Testing Program using 4 testing cartridges, 1 being cTnI Device/manufacturer: i-STAT 300 analyzer/Abbott Point of Care and the following cartridges: Chem8+, CG4+, PT/INR, cTnI | Training/Quality Control:
| Outcomes: Staff satisfaction |
Mashamba-Thompson et al. (2018)22 South Africa Funding/support: African Population and Health Research Center; University of KwaZulu-Natal College of Health Sciences; South African Centre of Excellence for Epidemiology and Modelling Analysis; and the National Institute of Allergy and Infectious Disease of the National Institutes of Health (K23 AI108293). Authors stated that funders played no role in study conduct. | Cross-sectional study; survey Settings/Sites: 100 randomly selected rural primary health care clinics of KwaZulu-Natal; selection method aimed to ensure uniform sampling across districts. The mean distance from each practice to the nearest emergency tertiary hospital was 41.4 km (SD = 42.8 km), with most (40%) being within 10 km. Duration: NA Number of participants: 100 sites contacted, 100 responded (100% response rate) | Inclusion: Staff (1 per clinic; including operations managers, primary health care specialist nurses, and staff nurses). Exclusion: None Characteristics: Respondent (year of qualification) and clinic (e.g., number of different staff, number of patients, clinic processes) characteristics were reported. | Intervention: Mailed survey. Pilot tested in 5 rural clinics Closed ended questions on demographics and current accessibility, availability, usage, and future needs for POCT tests in their practice. Included 2 questions on current use and potential use of troponin POCTs. Device/manufacturer: Any; not stated | Training/Quality Control: NA | Outcomes:
|
Spaeth et al.(2017)20 Australia Funding: supported by a grant provided by the Emergency Medicine Foundation (Emergency Medicine Foundation Ltd.) | Retrospective observational study Audit of clinical outcomes at selected centres “to determine the effectiveness of POCT as a decision support tool for triaging acutely ill patients”; 1 of 3 POCT tools, cTnI POCT was assessed to support triage of patients with acute chest pain. Our focus is limited to this research goal. Settings/Sites: 6 remote health centres in the Northern Territory with routinely available POCT. Within this region, a POCT network operates in 72 remotely located primary health care centres. Site selection was by study size and location to “eliminate any potential sources of bias” Duration: NA Number of participants: N = 147 | Inclusion: Patients who initially presented to 1 of 6 remote health centres over a 6-month period with a primary presentation of acute chest pain, normal ECG and clinical symptoms of non–ST elevation myocardial infarction (NSTEMI) with a completed troponin POCT identified by the i-STAT Central Data Station, a centrally administered repository of all de-identified results for each i-STAT device. Exclusion: Those with ST elevation on ECG (STEMI) Median time from pain onset to initial assessment: NR Age (Median):
Male Sex (n, (% in outcome group)):
| Intervention: Device/manufacturer:
Clinical ‘POCT pathway’; for patients with acute chest pain (without ST elevation on ECG). Based on defined ‘standard care’ protocols but adapted by the study team Low risk:
Not low risk:
| No information about staff conducting the test Training/Quality Control: Onsite training and competency assessment of i-STAT POCT. Centres conducted monthly quality control testing. | Outcomes:
Other data collected but not presented in this review: time to prepare for and perform test, time to initiate treatment, treatments given. Follow-up: NR |
ACS = acute coronary syndrome; AIHTA = Austrian Institute for Health Technology Assessment; AMI = acute myocardial infarction; CAD = cardiovascular disease; COI = conflict of interest; cTn = cardiac troponin; cTnI = cardiac troponin I; cTnT = cardiac troponin T; GP = general practitioner; ECG = electrocardiogram; ED = emergency department; EDACS = Emergency Department Assessment of Chest Pain Score; EUnetHTA = European Network for Health Technology Assessment; IQR = interquartile range; LR = likelihood ratio; MACE = major adverse cardiovascular events; NA = not applicable; NPV = negative predictive value; NR = not reported; NSTEMI = non–ST-elevation myocardial infarction; POCT = point-of-care test; PPV = positive predictive value; RACPP = Rural Accelerated Chest Pain Pathway; SD = standard deviation; STEMI = ST-elevation acute myocardial infarction; URL = upper reference limit.
Note: This table has not been copy-edited.
aTerminology from the original source.
Appendix 3: Main Study Findings
Please note that this appendix has not been copy-edited.
Table 5: Point of Care Testing Programs Identified in this Reviewa
Country, Region, Example of POCT program | Select notes from included publications |
|---|---|
Australia Northern Territory Northern Territory Department of Health and Community Point of Care Services Unit (Flinders University International Centre for Point-of-Care Testing)19,20,25,29,36 | Timeline: Initiated in 2008 Scope: For both acute and chronic conditions Settings/sites: As of 2020 the program had included at least 80 remotely located primary care centres which deliver general health services Staff:
Volume / population: Each centre services an average population of 523 Distance from hospitals: 2 Territorial hospitals - located on average 275 km (range:100 to 700km) from centres. Method of transport: Patients generally transported by airplane or helicopter to the nearest hospital emergency department Access to laboratory services: A 2007 internal Northern Territory government report noted most have regular access to pathology services twice a week or less (part of rationale for this program) Device(s) (Manufacturer) and Tests: i-STAT (Abbott Point of Care). Tests include Chem 8+ (Electrolytes, total CO2, urea, creatinine, glucose, ionized calcium, hemoglobin), CG4+ (Blood gas and lactate), PT/INR (prothrombin time / international normalized ratio), and cTnI (troponin I) Other: The program also includes an advanced web-based data manager (InfoHQ, Abbott), replacing the former Central Data Station (Abbott), electronically capturing deidentified patient and quality data from remote devices. Governance/Structure:
Training / Quality control:
Assessments: Most tests have met professional-based analytical goals and laboratory performance. Financial: “when used to aid medical decision-making in acutely ill patients, the NT POCT Program was estimated to save the Northern Territory health care system approximately A$21.75 million per annum by the prevention of unnecessary emergency medical retrievals for 3 common acute presentations.”19 Other notes: Staff turnover has been a significant issue (> 36% staff leaving program centres within 1 year) |
New Zealand has many POCT programs, some discussed in Herd and Musaad (2021)23 and are governed by practice guidelines.31 One example identified includes cTnI POCT: The Waitemata District Health Board (DHB) Rural Point of Care Testing Service37 | Scope: The Rural Alliance group of general practices identified the 4 most clinically valuable POCT tests for the management of people presenting acutely unwell in a rural setting. The rationale: to enable rapid decision-making and to reduce unnecessary ED presentations. Settings/sites: All rural general practices across both Auckland DHB and Waitemata DHB areas. Device(s) (Manufacturer) and Tests: Troponin I and INR on the Abbott i-STAT analyzer, D-dimer on the Roche h232 analyzer (Roche Diagnostics, F. Hoffmann-La Roche Ltd.), and a full blood count on the QBC STAR Hematology Centrifugal Analyzer (Drucker Diagnostics, Philipsburg, Pennsylvania). Governance/Structure:
Training / Quality control:
|
cTnI = cardiac troponin I; DHB = District Health Board; ED = emergency department; NT = Northern Territory; POCT = point-of-care test.
aIs not intended to be interpreted as a complete list of POCT programs.
bTerminology from the original source.
Table 6: Summary of Findings by Outcome — Rural GP Use or Desired Use of Troponin POCTs
Study citation, Design, Number of participants | POCT device/manufacturer, Troponin test, Test protocol | Outcome definition, Measurement, Time point | Outcome, n (%) |
|---|---|---|---|
Matthes et al. (2023)21 Survey 2,052 GPs surveyed and reached from 3 German federal states 292 responded (14.5%) 84 from rural community practice locations | Device/manufacturer: Any; not stated Test protocol: NR | Definition: Use of cTnI/cTnT POCTs Measurement: Mailed survey; responses to the question: “How often do you use POCTs for the following laboratory analyses in your routine work as a GP? Troponin I, Troponin T…” Response options included:
Time point: Survey conducted between April 2022 and June 2022 | GPs from practices in rural communities – responses from 81 / 84 respondents
The authors used Pearson’s Chi-square test to compare these responses to those from GPs from practices in towns (n = 130) and GPs from practices in urban centres (n = 66) and reported no significant difference (X2 = 9.222, df = 4, P = 0.056) |
Mashamba-Thompson et al. (2018)22 Survey Staff (1 per clinic) at 100 rural primary health care clinics of KwaZulu-Natal, South Africa; 100 clinics responded (100% response rate) | Device/manufacturer: Any; not stated Test protocol: NR | Definition: Current and potential desired use of specific POCTs, troponin being 1 of 50 included in specific questions. Measurement: Responses to the question: “Please select the answer that best matches your views about current or potential use of POCTs…Troponin” Time point: Survey conducted between April 2015 and August 2015 |
|
cTnI = cardiac troponin I; cTnT = cardiac troponin T; GPs = general practitioners; NR = not reported; POCT = point-of-care test.
Table 7: Summary of Findings by Outcome — Major Adverse Cardiovascular Events Within 30 days of Index Presentation and Diagnostic Accuracy of Accelerated Diagnostic Pathway
Study citation, design, number of patients | POCT device/manufacturer, troponin test, Test protocol | Outcome definition, measurement, time point | Outcomes per group | Pathway diagnostic accuracy for 30-day MACE (95% CI) | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
Low risk | Not-low risk | Sens | NPV | LR- | Spec | PPV | LR+ | |||
From AIHTA (2024)17 (relevant study 1 of 2) Miller et al. (2022):24 Prospective observational study; n = 1,205 enrolled; 1,073 included in primary analysis | Device/manufacturer:
Intervention:
| Definition: Death, cardiac arrest, emergency revascularization procedure, cardiogenic shock, ventricular arrhythmia, ventricular fibrillation, high-degree atrio-ventricular block needing intervention, or acute myocardial infarction Measurement: From National Minimal Dataset of public hospital admissions, NZ MOH and National Mortality Collection (MOH) Time point: up to 30 days after presentation | 0 of 474 (0%) 95% CI, 0 to 0.3% | 138 of 599 (23%) 124 / 236 (52.5%) of those identified as high risk had a 30-day MACE; 14 / 363 (3.9%) of those identified as intermediate risk had a 30-day MACE Included: 3 deaths, 125 patients with MI and 41 receiving emergency revascularization procedure | 100% (97.3% to 100%) | 100% (99.2% to 100%) | 0 (CI not estimable) | 50.7% (47.5% to 53.9%) | 23.0% (19.8% to 26.6%) | 2.0 (1.9 to 2.2) |
From AIHTA (2024)17 (relevant study 2 of 2) Norman et al. (2022)28 Prospective observational study; n = 186 identified, 180 included in analyses | Device/manufacturer: i-STAT cTnI/Abbott Point of Care Diagnostics) RACPP including EDACS, ECG and 2 troponin POCTs – 1 at presentation and 1 at 2 hours. Risk stratification to low risk and non-low risk | Definition: Death that was not known to be from non-cardiac causes, emergency coronary revascularization procedure, cardiac arrest, ventricular arrhythmia, cardiogenic shock, and high-degree atrioventricular block needing intervention Measurement: Electronic template in the practice management system. From National Health Index identifier event searches and nurse telephone follow-up at 30 days. Time point: up to 30 days after presentation | 0 of 111 (0.0%) | 9 of 69 (13.0%) 8 at index presentation; 2 during readmission (1 patient with 2 events) | 100.0% (70.1% to 100.0%) | 100.0% (96.7% to 100.0%) | NR | 63.8% (56.4% to 70.6%) | 12.5% (6.7% to 22.1%) | NR |
AIHTA = Austrian Institute for Health Technology Assessment; CI = confidence interval; cTnI = cardiac troponin I; ECG = electrocardiogram; EDACS = Emergency Department Assessment of Chest Pain Score; LR- = negative likelihood ratio; LR+ = positive likelihood ratio; MACE = major adverse cardiovascular events; MI = myocardial infarction; NPV = negative predictive value; NR = not reported; NZ MOH = New Zealand Ministry of Health; POCT = point-of-care test; PPV = positive predictive value; RACPP = Rural Accelerated Chest Pain Pathway; Sens = sensitivity; Spec = Specificity.
Table 8: Summary of Findings by Outcome — Agreement Between POCT and Laboratory Measured Cardiac Troponin Concentrations
Study citation, design, number of patients | POCT device/manufacturer, troponin test, test protocol | Outcome definition, measurement, time point | Outcomes per group |
|---|---|---|---|
From AIHTA (2024)17 (relevant study 2 of 2) Norman et al. (2022)28 Prospective observational study; n = 186 identified; 180 included in analyses | Device/manufacturer: i-STAT cTnI/Abbott Point of Care Diagnostics) Reference laboratory diagnostic tests (duplicate samples at both time points):
| Definition: Qualitative agreement between test results (positive or negative) Measurement: Pre-established cut points to define positive and negative tests (Refer to Table 7) Time point: 0 and 2 hours from presentation (samples stored for laboratory analysis) |
The authors noted that all discordant samples had measured concentration “very near the relevant cut-off and no patient with discordant troponin experienced a MACE within 30 days.” |
AIHTA = Austrian Institute for Health Technology Assessment; cTnI = cardiac troponin I; hs-troponin = high-sensitivity troponin; MACE = major adverse cardiovascular events; POCT = point-of-care test.
Table 9: Summary of Findings by Outcome — Hospital Referrals, Admissions, Evacuationsa
Study citation, design, number of patients | POCT device/manufacturer, troponin test, test protocol | Outcome definition, measurement, time point | Outcome |
|---|---|---|---|
Percentage of patients managed as low risk who were never transferred or admitted to hospital | |||
From AIHTA (2024)17 (relevant study 1 of 2) Miller et al. (2022):24 Prospective observational study; n = 1,205 enrolled; 1,073 included in primary analysis | Device/manufacturer:
Intervention:
| Definition: Percentage of patients managed as low risk who were never transferred or admitted to hospital Measurement: From National Minimal Dataset of public Hospital admissions, NZ MOH and National Mortality Collection (MOH) Time point: NR |
|
From AIHTA (2024)17 (relevant study 2 of 2) Norman et al. (2022)28 Prospective observational study; n = 186 identified; 180 included in analyses | Device/manufacturer: i-STAT cTnI/Abbott Point of Care Diagnostics) RACPP including EDACS, ECG and 2 troponin POCTs – 1 at presentation and 1 at 2 hours. Risk stratification to low risk and non-low risk | Definition: The proportion of patients identified as low-risk by the pathway, and managed in the community, without transfer to hospital, with no 30-day MACE. Measurement: Electronic template in the practice management system. From National Health Index identifier event searches and nurse telephone follow-up at 30 days. Time point: up to 30 days after presentation | 111 of 111 (100%) |
Patients requiring evacuation | |||
Spaeth et al. (2017):20 Retrospective observational study; n = 147 relevant to the current analysis | Intervention: “POCT Pathway” including ECG, clinical assessment and up to 2 troponin POCTs – 1 at presentation and 1 at > 8 hours after presentation Device/manufacturer:
| Definition: n (%) patients requiring evacuation Measurement: The Northern Territory’s Department of Health Primary Care Information System Time point: NR | cTnI negative: 14 of 140 (10%) patients evacuated cTnI positive: 7/7 (100%) patients evacuated |
Clinical judgment (retrospective) on patient evacuation status if troponin POCT had not been used | |||
Spaeth et al. (2017):20 Retrospective observational study; n = 147 relevant to the current analysis | Intervention: “POCT Pathway” including ECG, clinical assessment and up to 2 troponin POCTs – 1 at presentation and 1 at > 8 hours after presentation Device/manufacturer:
| Definition: Clinical judgment of likely outcome (evacuation or not) in hypothetical absence of POCT troponin i-STAT Measurement: Assessment by a clinical data by a Senior Rural Medical Practitioner with extensive experience in the decision-making of patient evacuations. Time point: NR | cTnI negative, not evacuated (n = 126): Clinical advisor stated that 48 (38%) of these patients would have been evacuated without i-STAT device availability (cardiac involvement could not be ruled out) cTnI negative, evacuated (n = 14): Clinical advisor stated that all 14 (100%) of these patients would have been evacuated without i-STAT device availability cTnI positive, evacuated (n = 7): Clinical advisor stated that 4 (57%) of these patients would have been evacuated without i-STAT device available and that those not evacuated would likely have had a poorer outcome. |
AIHTA = Austrian Institute for Health Technology Assessment; CDS = Central Data Station; CI = confidence interval; cTnI = cardiac troponin I; cTnT = cardiac troponin T; ECG = electrocardiogram; EDACS = Emergency Department Assessment of Chest Pain Score; MACE = major adverse cardiovascular events; NZ MOH = New Zealand Ministry of Health; NR = not reported; POCT = point-of-care test; RACPP = Rural Accelerated Chest Pain Pathway.
aIncludes both actual evacuation data or equivalent and clinical judgment of hypothetical evacuation status, depending on study.
Table 10: Summary of Findings by Outcome — Time to Diagnosis
Study citation, design, number of patients | POCT device/manufacturer, troponin test, test protocol | Outcome definition, measurement, time point | Outcome, group (n): median ± IQR |
|---|---|---|---|
Spaeth et al.(2017):20 Retrospective observational study; n = 146 relevant to the current analysis | Intervention: “POCT Pathway” including ECG, clinical assessment and up to 2 troponin POCTs – 1 at presentation and 1 at > 8 hours after presentation Device/manufacturer:
| Definition: Time from test to diagnosis Measurement: i-STAT CDS and Northern Territory’s Department of Health PCIS Time point: NR | Single Positive test + Evacuated (n = 3): 20 (± 68) minutes Single Negative test + Evacuated (n = 11): 50 (± 130) minutes Single Negative test + Not Evacuated (n = 97): 30 (± 34) minutes Serial Positive test + Evacuated (n = 4): 255 (± 570) minutes Serial Negative tests + Evacuated (n = 3): 100 (± 80) minutes Serial Negative + Not Evacuated (n = 28): 480 (± 630) minutes |
CDS = Central Data Station; cTnI = cardiac troponin I; ECG = electrocardiogram; IQR = interquartile range; NR = not reported; POCT = point-of-care test; PCIS = Primary Care Information System.
Table 11: Summary of Findings by Outcome — Time to Treatment
Study citation, design, number of patients | POCT device/manufacturer, troponin test, test protocol | Outcome definition, measurement, time point | Outcome, group (n): median ± IQR | ||
|---|---|---|---|---|---|
Spaeth et al.(2017):20 Retrospective observational study; n = 147 relevant to the current analysis | Intervention: “POCT Pathway” including ECG, clinical assessment and up to 2 troponin POCTs – 1 at presentation and 1 at > 8 hours after presentation Device/manufacturer:
| Definition: Time from test to treatment Measurement: i-STAT CDS and Northern Territory’s Department of Health PCIS Time point: NR | Single Positive test + Evacuated (n = 3): 20 (± 5) minutes Single Negative test + Evacuated (n = 6): 38 (± 64) minutes; missing data for 5 Single Negative test + Not Evacuated (n = 26): 15 (± 20) minutes; the remaining patients in this group did not require treatment Serial Positive test + Evacuated (n = 4): 40 (± 20) minutes Serial Negative tests + Evacuated (n = 2): 5 (± 0) minutes; missing data for 1 patient Serial Negative + Not Evacuated (n = 11): 30 (± 45) minutes; the remaining patients in this group did not require treatment | ||
CDS = Central Data Station; cTnI = cardiac troponin I; ECG = electrocardiogram; IQR = interquartile range; NR = not reported; POCT = point-of-care test; PCIS = Primary Care Information System.
Table 12: Summary of Findings by Outcome — Patient Satisfaction
Study citation, Design, Number of patients | POCT device/manufacturer, Troponin test, Test protocol | Outcome definition, Measurement, Time point | Outcome |
|---|---|---|---|
From AIHTA (2024)17 (relevant study 2 of 2) Norman et al. (2022)28 Prospective observational study; n = 186 identified; 180 included in analyses | Device/manufacturer: i-STAT cTnI/Abbott Point of Care Diagnostics) RACPP including EDACS, ECG and 2 troponin POCTs – 1 at presentation and 1 at 2 hours. Risk stratification to low risk and not-low risk | Definition: Patient responses (options Good-excellent, fair, poor) to questions about their satisfaction with:
Measurement: Telephone call from a research nurse Time point: 30 days after index presentation | Response rate: 111 of 148 (75%); 67 classified and managed as low risk; 44 classified as non-low risk of whom 37 were referred to the hospital Overall, 94.0% of low-risk and 95.5% of not low-risk respondents felt ‘good-excellent’ satisfaction with the service they received at the general practice. Refer to the study for more information. |
AIHTA = Austrian Institute for Health Technology Assessment; cTnI = cardiac troponin I; ECG = electrocardiogram; EDACS = Emergency Department Assessment of Chest Pain Score; POCT = point-of-care test; RACPP = Rural Accelerated Chest Pain Pathway.
Table 13: Summary of Findings by Outcome — Staff Satisfaction
Study citation, design, number of patients | POCT device/manufacturer, troponin test, test protocol | Outcome definition, measurement, time point | Outcome |
|---|---|---|---|
From AIHTA (2024)17 Norman et al. (2022):28 Prospective observational study; n = 186 identified; 180 included in analyses | Device/manufacturer: i-STAT cTnI/Abbott Point of Care Diagnostics RACPP including EDACS, ECG and 2 troponin POCTs – 1 at presentation and 1 at 2 hours. Risk stratification to low risk and not-low risk | Definition: NR Measurement: NR Time point: NR | Authors state: “The pathway was considered feasible and acceptable by the general practices to the extent that it has been maintained as the standard of care in the participating centres” |
From EUnetHTA (2019)18 Shephard et al. (2014)25 and Shephard et al. (2012):29
| Intervention: i-STAT Point-of-Care Testing Program using 4 testing cartridges, 1 being cTnI Device/manufacturer: i-STAT 300 analyzer/Abbott Point of Care and the following cartridges: Chem8+, CG4+, PT/INR, cTnI | Definition: Staff satisfaction with pathology services after introduction of i-STAT POCT program Measurement: Online questionnaires Time point: 2012 publication- Approximately 1 year after the start of program implementation | 39/127 (31%) response rate No information on characteristics of respondents and nonrespondents. cTnI POCT-relevant questions:
Note: the following is not specific to cTnI POCTs
|
AIHTA = Austrian Institute for Health Technology Assessment; cTnI = cardiac troponin I; ECG = electrocardiogram; EDACS = Emergency Department Assessment of Chest Pain Score; EUnetHTA = European Network for Health Technology Assessment; NR = not reported; NT POCT program: Northern Territory Point-of-Care Testing Program; POCT = point-of-care test; RACPP = Rural Accelerated Chest Pain Pathway.
Table 14: Summary of Findings by Outcome — Adherence to Pathway
Study citation, Design, Number of patients | POCT device/manufacturer, Troponin test, Test protocol | Outcome definition, Measurement, Time point | Outcome |
|---|---|---|---|
From AIHTA (2024)17 (relevant study 2 of 2) Norman et al. (2022):28 Prospective observational study; n = 186 identified; 180 included in analyses | Device/manufacturer:
| Definition: Adherence to the RACPP pathway (staff and patients) Measurement:
Time point: NR | Low-risk patients:
Non–low-risk patients:
|
AIHTA = Austrian Institute for Health Technology Assessment; cTnI = cardiac troponin I; ECG = electrocardiogram; EDACS = Emergency Department Assessment of Chest Pain Score; MACE = major adverse cardiovascular events; NR = not reported; POCT = point-of-care test; RACPP = Rural Accelerated Chest Pain Pathway.
Table 15: Summary of Findings by Outcome — Number (%) of cTnI Test Results Outside “Defined Critical Actions Limits” and Patient Clinical Conditions
Study citation, design, number of patients | POCT device/manufacturer, troponin test, test protocol | Outcome definition, measurement, time point | Outcome |
|---|---|---|---|
Matthews et al.(2020)19 Clinical audit / program evaluation Number of cTnI tests performed: 1,398 | Intervention: i-STAT Point-of-Care Testing Program using 4 testing cartridges, 1 being cTnI Device/manufacturer: i-STAT 300 analyzer/Abbott Point of Care and the following cartridges: Chem8+, CG4+, PT/INR, cTnI | Definition: Number (%) of tests conducted between September 1, 2019, and December 31, 2019, with POCT cTnI outside the defined clinical limit (critical range: 0.09 to 48.5 ng/mL; Median critical: 0.35 ng/mL; average critical: 3.08 ng/mL) and clinical condition of the relevant patients. Measurement: i-STAT 300 analyzer/Abbott Point of Care with cTnI cartridge Time point: NR |
|
cTnI = cardiac troponin I; NR = not reported; POCT = point-of-care test.
ISSN: 2563-6596
Canada’s Drug Agency (CDA-AMC) is a pan-Canadian health organization. Created and funded by Canada’s federal, provincial, and territorial governments, we’re responsible for driving better coordination, alignment, and public value within Canada’s drug and health technology landscape. We provide Canada’s health system leaders with independent evidence and advice so they can make informed drug, health technology, and health system decisions, and we collaborate with national and international partners to enhance our collective impact.
Disclaimer: CDA-AMC has taken care to ensure that the information in this document was accurate, complete, and up to date when it was published, but does not make any guarantee to that effect. Your use of this information is subject to this disclaimer and the Terms of Use at cda-amc.ca.
The information in this document is made available for informational and educational purposes only and should not be used as a substitute for professional medical advice, the application of clinical judgment in respect of the care of a particular patient, or other professional judgments in any decision-making process. You assume full responsibility for the use of the information and rely on it at your own risk.
CDA-AMC does not endorse any information, drugs, therapies, treatments, products, processes, or services. The views and opinions of third parties published in this document do not necessarily reflect those of CDA-AMC. The copyright and other intellectual property rights in this document are owned by the Canadian Agency for Drugs and Technologies in Health (operating as CDA-AMC) and its licensors.
Questions or requests for information about this report can be directed to Requests@CDA-AMC.ca.