Drugs, Health Technologies, Health Systems
Health Technology Review
Antiviral Drugs for the Prevention or Treatment of Zoonotic Influenza
Authors: Jennifer Seida, Elham Barati, Dagmara Chojecki
This rapid review was conducted by the Alberta Drug and Therapeutic Evaluation Consortium (ADTEC) through the Post-Market Drug Evaluation CoLab Network.
Key Messages
What Is the Issue?
Zoonotic influenza may result in severe illness and death in individuals infected by sick animals. These influenza A viruses also pose a pandemic risk due to their adaptability and humans’ lack of existing immunity to them.
Antivirals, such as baloxavir marboxil, oseltamivir, peramivir, and zanamivir, may be used before or after exposure to infected animals to prevent symptomatic illness, or after infection to treat zoonotic influenza in humans. However, the effectiveness and safety of antivirals for zoonotic influenza is unknown.
What Did We Do?
We conducted a rapid review to identify and summarize evidence on the clinical efficacy, effectiveness, and safety of antivirals used for the prevention or treatment of zoonotic influenza.
We searched electronic databases and key online sources for studies published in English from January 1, 2019, to December 9, 2024 (for systematic reviews [SRs] and randomized controlled trials [RCTs]) and to January 8, 2025 (for observational studies). One researcher screened titles and abstracts of citations and 2 researchers reviewed full-text articles to identify studies that met the predefined criteria. We narratively summarized the study findings.
What Did We Find?
We identified 2 SRs on the efficacy and safety of antivirals for zoonotic influenza. One SR focused on preventing infection after exposure and the other SR focused on treating zoonotic influenza. Neither review identified relevant RCTs examining individuals with zoonotic influenza.
We did not identify any primary studies relevant to our review.
What Does It Mean?
There is a lack of evidence on the efficacy, effectiveness, and safety of various antivirals for the prevention and treatment of zoonotic influenza; therefore, we were not able to draw any conclusions.
Abbreviations
NAI
neuraminidase inhibitor
NMA
network meta-analysis
RCT
randomized controlled trial
SR
systematic review
Introduction and Rationale
Background
Zoonotic influenza refers to influenza A viruses found in wild birds and poultry and, less commonly, in mammals such as pigs, cattle, and horses, that cross the animal-human species barrier to infect humans.1,2 Transmission of zoonotic influenza usually occurs through close contact with infected animals or their environments, such as working on farms or in slaughterhouses, hunting, defeathering, butchering wild flock or mammals, or visiting live poultry markets.3 While zoonotic influenza viruses, such as avian influenza subtypes A(H5N1), A(H5N6), A(H7N9) or swine influenza subtypes A(H1N1) and A(H3N2), can infect and cause illness in humans, they are distinct from human influenza viruses and have not demonstrated sustained human-to-human transmission.3 However, influenza A viruses are susceptible to antigenic mutations and the emergence of a viral strain with the ability to spread easily among humans poses a significant pandemic risk.4-6 In particular, as human populations generally have little to no pre-existing immunity against these viruses, outbreaks could lead to high morbidity and mortality. Consequently, pandemic preparedness is essential.3,6,7
In humans, infection with zoonotic influenza viruses can have a range of presentations, from minor upper respiratory symptoms to severe, acute respiratory disease that may lead to death.3 Symptoms typically develop within 1 to 5 days after exposure, though the incubation period can sometimes extend beyond this range.8 Influenza can lead to a variety of complications that affect multiple body systems, including cardiovascular, hematologic, musculoskeletal, neurologic, ocular, pulmonary, and renal functions.5,9 The severity and frequency of the illness’s complications depends on the specific virus and the individual’s health.3 While vulnerable groups, such as individuals who are immunocompromised and those who have chronic underlying medical conditions, are at high risk of complications, healthy persons and younger adults are also at risk of severe illness and death with some zoonotic strains.8 Case fatality rates for avian influenza strains A(H5N1), A(H5N6), and A(H7N9) are higher than for seasonal influenza, estimated at 60%, 39%, and 40%, respectively.8-10 Conversely, the A(H9N2) strain generally causes milder illness, with very few cases leading to death.11
Diagnosis of infection with a zoonotic influenza strain is confirmed through laboratory testing with reverse transcription-polymerase chain reaction, which is prioritized for individuals with significant exposure history.3,9 Positive cases of strains such as H5N1 must undergo subsequent confirmation testing and analysis with the National Microbiology Laboratory to fulfill Canada’s obligation under International Health Regulations.9 However, confirmation of zoonotic influenza is not required to initiate treatment, which should not be delayed while awaiting test results.9
Prevention of Zoonotic Influenza
Efforts for preventing zoonotic influenza begin with animal health, including vaccinating animals and biosecurity.12,13 To prevent cross-species transmission, proper use of personal protective equipment is essential for those in close contact with animals or their environment.14,15 According to the WHO (2023), robust surveillance systems are also essential in both animal and human populations to detect and respond to zoonotic influenza outbreaks promptly.3 In addition, having a detailed response plan in place before a pandemic ensures preparedness, with strategies for quick response, effective communication, and resource allocation to protect public health.3
The development of human vaccines for zoonotic influenza faces unique challenges due to the genetic and antigenic diversity of influenza A viruses.8 Seasonal influenza vaccines do not offer protection against avian influenza and14 there are no human vaccines to protect against avian influenza available for public use in Canada.9
Antiviral drugs may be used prophylactically, either pre-exposure or post-exposure, in an effort to prevent the development of symptomatic influenza.8,9 The Association of Medical Microbiology and Infectious Disease Canada 2023 guidelines recommend the use of the neuraminidase inhibitor (NAI) oseltamivir for chemoprophylaxis after a discrete exposure event to poultry or other zoonotic source of avian influenza.16 The decision to initiate post-exposure antiviral chemoprophylaxis should rely on clinical judgment, taking into account factors such as the nature and duration of the exposure, the time elapsed since the exposure, and the infection status of the birds or animals involved.17
Treatment of Zoonotic Influenza
The treatment of zoonotic influenza primarily involves antiviral medications, with NAIs being the first-line therapy.8 Oseltamivir is the most widely used NAI and recommended as the primary antiviral drug for zoonotic influenza, particularly for H5N1 infections, based on animal data.8,16 Other NAIs authorized in Canada include zanamivir and peramivir.8,9 Baloxavir marboxil is also used in the treatment of zoonotic influenza, either as a standalone therapy or in combination with NAIs.18,19 Treatment should be initiated as early as possible, ideally within 48 hours of symptom onset, but it can still be beneficial when started later in moderate to severe cases.9,16 The Centers for Disease Control and Prevention recommend starting antiviral treatment immediately for confirmed, probable, or suspected cases, regardless of the time elapsed since symptoms began.19 In addition to antivirals, supportive care may be necessary, especially for patients who are severely ill and may require respiratory support.9
Policy Issue
This rapid review is 1 component of a broader project examining antiviral drugs for influenza. Evidence from this rapid review and other components will support multijurisdictional decisions on the appropriate and safe use of antiviral drugs for prophylaxis and treatment of influenza A or B for pandemic preparedness.
Policy Questions
The policy question examined in the rapid review is as follows:
Is there a need to stockpile antiviral drugs for prepandemic or pandemic preparedness for prophylaxis and treatment of zoonotic influenza strains?
Which influenza antivirals should be stockpiled for prepandemic or pandemic preparedness for prophylaxis and treatment?
What does each influenza antiviral offer in the prepandemic or pandemic context, considering relevant outcomes for specific populations?
Purpose
The purpose of this rapid review is to identify and describe the evidence examining the efficacy, effectiveness, and safety of antiviral drugs approved for use in Canada for pre-exposure prophylaxis, post-exposure prophylaxis, and treatment of zoonotic influenza.
Research Questions
The research questions are as follows:
What are the efficacy and effectiveness of antiviral drugs for pre-exposure prophylaxis in individuals at high risk of getting influenza A due to unprotected exposure to infected animals or an environment highly contaminated by infected animals?
What is the safety of antiviral drugs for pre-exposure prophylaxis in individuals at high risk of getting influenza A due to unprotected exposure to infected animals or an environment highly contaminated by infected animals?
What is the efficacy and effectiveness of antiviral drugs for post-exposure prophylaxis in individuals exposed to zoonotic influenza A due to unprotected exposure to infected animals or an environment highly contaminated by infected animals?
What is the safety of antiviral drugs for post-exposure prophylaxis in individuals exposed to zoonotic influenza A due to unprotected exposure to infected animals or an environment highly contaminated by infected animals?
What are the efficacy and effectiveness of antiviral drugs to treat zoonotic influenza A due to unprotected exposure to infected animals or an environment highly contaminated by infected animals?
What is the safety of antiviral drugs to treat zoonotic influenza A due to unprotected exposure to infected animals or an environment highly contaminated by infected animals?
Methods
Literature Search Methods
An information specialist conducted searches in the electronic databases Ovid Medline, Ovid Embase, and Web of Science for English-language literature published from January 1, 2019, to December 9, 2024 (for SRs and RCTs) and to January 8, 2025 (for observational studies). Articles were identified using a combination of controlled vocabulary; for example, MeSH and Embase subject heading terms and relevant keywords surrounding the topics of antivirals and zoonotic influenza. An RCT filter and an observational studies filter developed by Canada’s Drug Agency were also used to first limit the search to RCTs and then to observational studies. Grey literature searching was conducted in Chat GPT, Perplexity AI, Google Scholar, Google Advanced, the International Network of Agencies for Health Technology Assessment (INAHTA) HTA database, and the Centers for Disease Control and Prevention website. Reference lists of included articles were scanned to help identify additional relevant evidence.
Selection Criteria and Methods
One researcher screened titles and abstracts of the studies identified in the literature searches following pilot testing of a sample of the studies. The full-text articles of all potentially relevant studies were retrieved and 2 researchers independently assessed the full texts based on the predetermined eligibility criteria presented in Table 1. Disagreements were resolved through consensus.
Criteria | Description |
|---|---|
Population | Individuals at high risk of zoonotic influenza A, exposed to zoonotic influenza A, or infected with zoonotic influenza Aa |
Subgroups and priority populations |
|
Interventions | Baloxavir marboxil, oseltamivir, peramivir, zanamivir, combination therapyb |
Comparators | Active control(s) approved in Canada, placebo, no treatment, or standard of care |
Outcomes | Zoonotic PReP or PEP Primary outcomes:
Secondary outcomes:
Zoonotic Treatment
|
Study designs | SRs with or without NMAs, RCTs, controlled clinical trials, comparative observational studies |
NAI = neuraminidase inhibitor; NMA = network meta-analysis; PEP = post-exposure prophylaxis; PReP = pre-exposure prophylaxis; RCT = randomized controlled trial; SR = systematic review.
Note: PReP is an antiviral drug taken before exposure to the virus (for example, by at-risk workers) to prevent the risk of infection; PEP is an antiviral drug taken after exposure to the virus but before the development of symptoms or a positive laboratory test result to prevent illness; treatment is an antiviral drug taken to treat symptomatic influenza.
aZoonotic influenza was defined as resulting from unprotected exposure to infected animals or an environment highly contaminated by infected animals; or novel influenza A viruses that have been known to cross the animal-human species barrier and cause severe illness in humans, such as avian influenza subtypes A(H5N1), A(H5N6), A(H7N9).
bEligible combination treatment is an NAI with another NAI or an NAI with baloxavir marboxil.
Exclusion Criteria
Studies were excluded if they did not meet the study selection criteria (Table 1), they were duplicate publications, or they were published before 2019. Case reports, case series, and other noncomparative observational studies were excluded. Studies that examined patients with seasonal influenza or in which the effects of specific drugs or drug combinations of interest could not be isolated (for example, studies that reported the results for NAIs without specifying drugs or drug combinations) were excluded.
Critical Appraisal of Individual Studies
We did not conduct a critical appraisal because there were no relevant primary studies identified and the findings of the included SRs were based on data extrapolated from seasonal influenza.
Data Extraction
One reviewer extracted information from each article using a standardized data extraction form. Extracted information included the study characteristics (year of publication, country, funding source, study design), number of included studies (for SRs), number of participants, population characteristics, intervention(s), comparator(s), clinical outcomes, length of follow-up, and study findings, where reported.
Summary of Evidence
Quantity of Research Available
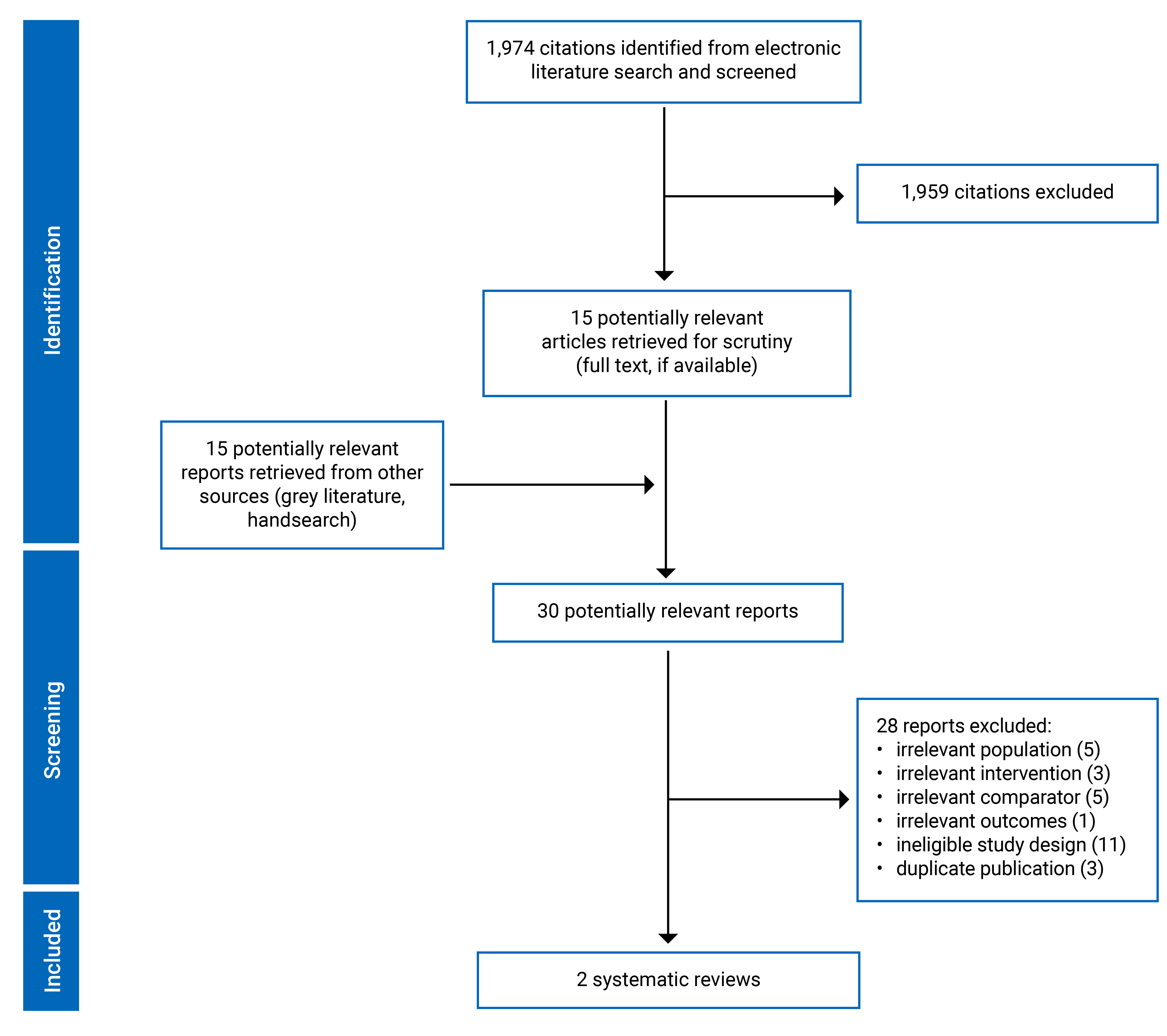
Of the 1,974 citations identified in the literature search, 15 were potentially relevant based on title and abstract screening and were retrieved for full-text review. The full-text articles of an additional 15 potentially relevant publications, identified through the grey literature search, were retrieved. Of these 30 articles, 28 were excluded, and 2 studies that met the eligibility criteria were included in this rapid review. Both included studies are SRs with network meta-analyses (NMAs).20,21 The PRISMA flow chart of the study selection is available in Appendix 1. A list of the excluded studies with reasons for exclusion are available in Appendix 2.
Study Characteristics
Two SRs20,21 with NMAs met the eligibility criteria for this rapid review. Both SRs were conducted to support an update of the WHO influenza guidelines,22 were published in 2024, and included RCTs published up to September 2023. The aims of the SRs were to examine the efficacy and safety of antiviral drugs for post-exposure prophylaxis21 and treatment20 of influenza, respectively. The reviews had broader inclusion criteria than the present rapid review as they examined both seasonal and zoonotic influenza and examined a wider range of available drugs than those approved in Canada. Neither of the SRs included any RCTs examining individuals with zoonotic influenza.
Zhao et al.21 examined the effectiveness of various direct-acting antivirals for post-exposure prophylaxis of influenza compared with placebo, standard care, or a different antiviral drug. A total of 33 RCTs assessing 6 antiviral drugs (zanamivir, oseltamivir, laninamivir, baloxavir, amantadine, and rimantadine) in individuals exposed to seasonal influenza met the inclusion criteria. The outcomes of interest included infection, hospital admission, mortality, and adverse events. NMAs were conducted and the certainty of the evidence was assessed using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach. No RCTs examining post-exposure prophylaxis following exposure to animals with novel influenza A virus were identified; therefore, the study extrapolated findings from seasonal influenza trials to infer the effects of antivirals in people exposed to zoonotic influenza.
Gao et al.20 assessed the effectiveness of direct-acting antivirals for the treatment of patients who were hospitalized with suspected or confirmed influenza compared with placebo, standard care, or another antiviral. All 8 included RCTs examined patients with severe seasonal influenza and compared various antiviral drugs (i.e., oseltamivir, peramivir, zanamivir, rimantadine, zanamivir plus rimantadine, and baloxavir plus NAIs). Six trials were included in NMAs for various outcomes, including mortality, intensive care admission, duration of hospitalization, and time to symptom alleviation. In the absence of trials examining zoonotic influenza, the authors used baseline risk data and network relative estimates from severe seasonal influenza to estimate the effects of antivirals for patients with severe zoonotic influenza.
Additional details regarding the characteristics of the included SRs are provided in Appendix 3.
Findings
No relevant evidence on the efficacy, effectiveness, or safety of antivirals for pre-exposure prophylaxis, post-exposure prophylaxis, or treatment of zoonotic influenza was identified. Two included SRs used extrapolated evidence from seasonal influenza to estimate the effects of antivirals for zoonotic influenza. Subgroups were not considered due to the lack of evidence for zoonotic influenza.
The effect of antiviral post-exposure prophylaxis in individuals exposed to zoonotic influenza was estimated using baseline risks and data from studies of seasonal influenza in 1 SR.21 Based on extrapolated evidence, baloxavir, oseltamivir, and zanamivir may decrease the risk of symptomatic influenza in individuals exposed to animals infected with novel influenza A viruses compared with placebo (low certainty of evidence).21 Baloxavir and zanamivir may reduce the risk of hospital admission and mortality (very low certainty of evidence).21 The authors inferred that the risk of adverse events from antivirals used for post-exposure prophylaxis of zoonotic influenza would be similar to that of seasonal influenza, with no significant difference between antivirals and placebo (low to high certainty of evidence).21
Similarly, Gao et al.20 estimated the impact of antiviral treatment for individuals with severe zoonotic influenza on mortality rates using extrapolated evidence of individuals with severe seasonal influenza. The authors found there is uncertainty as to whether oseltamivir, peramivir, or zanamivir reduce mortality in individuals with severe zoonotic influenza compared with placebo, standard care, or other antivirals (very low certainty of evidence).20
Limitations
No RCTs or comparative observational studies were found that examined the efficacy, effectiveness, or safety of antivirals for pre-exposure prophylaxis, post-exposure prophylaxis, or treatment of zoonotic influenza. The included SRs estimated the effect of antivirals for prevention of zoonotic influenza and treatment of severe zoonotic influenza based on data derived from trials of seasonal influenza. The utility of the efficacy estimates based on the data extrapolated from seasonal influenza is uncertain. Zoonotic influenza viruses are distinct from human influenza viruses, and it is unknown whether it is clinically appropriate to transfer the findings pertaining to seasonal influenza to zoonotic influenza. In addition, the mortality rate used to extrapolate the findings was based on influenza A viruses associated with severe illness; therefore, the effect estimates may not be generalizable to zoonotic influenza A viruses with lower disease severity.21
Conclusions and Implications for Decision- or Policy-Making
The objective of this rapid review was to describe the evidence examining the efficacy, effectiveness, and safety of antiviral drugs approved for use in Canada for pre-exposure prophylaxis, post-exposure prophylaxis, and treatment of zoonotic influenza. We did not identify any relevant RCTs or comparative observational studies focusing on zoonotic influenza. However, we did identify 2 SRs with NMAs that met the eligibility criteria of the review. These SRs estimated the effect and impact of antiviral post-exposure prophylaxis and treatment of individuals with zoonotic influenza using extrapolated evidence from individuals with seasonal influenza. The extrapolated estimates suggest that some antivirals may decrease the risk of influenza infection compared to placebo or standard care and have an acceptable safety profile (this is information that is inferred, and not explicitly known).
The policy question asked whether there is a need to stockpile antiviral drugs for prepandemic or pandemic preparedness for prophylaxis and treatment of zoonotic influenza strains. The evidence considered in this review cannot adequately answer this question. Due to the lack of evidence, no conclusions can be drawn about the efficacy, effectiveness, and safety of antiviral drugs for pre-exposure prophylaxis, post-exposure prophylaxis, and treatment of zoonotic influenza.
Authors
Jennifer Seida led the rapid review, conducted study selection, conducted the analysis, and wrote the report.
Elham Barati conducted title and abstract screening, study selection, and data extraction, and wrote sections of the report.
Dagmara Chojecki designed the literature search methodology, conducted the literature searches, and drafted the literature search methods section and description of search strategies in the final report.
Conflicts of Interest
Lesley Dunfield disclosed the following:
Worked at Canada’s Drug Agency from 2014 to May 2024 (former employee).
No other conflicts of interest were declared.
References
1.World Health Organization (WHO). Zoonotic influenza. 2025. Accessed January 23, 2025. https://www.who.int/news-room/spotlight/influenza-are-we-ready/zoonotic-influenza
2.Suarez DL. Influenza A virus. In: Swayne DE, ed. Animal Influenza. 3rd ed. John Wiley & Sons, Inc.; 2016:1-30.
3.World Health Organization (WHO). Influenza (avian and other zoonotic). 2023. Accessed January 16, 2025. https://www.who.int/news-room/fact-sheets/detail/influenza-(avian-and-other-zoonotic)
4.Reperant LA, Grenfell BT, Osterhaus AD. Quantifying the risk of pandemic influenza virus evolution by mutation and re-assortment. Vaccine. 2015;33(49):6955-6966. doi: 10.1016/j.vaccine.2015.10.056 PubMed
5.Public Health Agency of Canada. Flu (influenza): For health professionals. 2024. Accessed January 16, 2025. https://www.canada.ca/en/public-health/services/diseases/flu-influenza/health-professionals.html
6.Abdelwhab EM, Mettenleiter TC. Zoonotic animal influenza virus and potential mixing vessel hosts. Viruses. 2023;15(4):980. doi: 10.3390/v15040980 PubMed
7.Kessler S, Harder TC, Schwemmle M, Ciminski K. Influenza A viruses and zoonotic events-are we creating our own reservoirs? Viruses. 2021;13(11):2250. doi: 10.3390/v13112250 PubMed
8.Mehta K, Goneau LW, Wong J, L'Huillier AG, Gubbay JB. Zoonotic influenza and human health-part 2: Clinical features, diagnosis, treatment, and prevention strategies. Curr Infect Dis Rep. 2018;20(10):38. doi: 10.1007/s11908-018-0643-8 PubMed
9.Public Health Agency of Canada. Avian influenza A(H5N1): For health professionals. 2024. Accessed January 16, 2025. https://www.canada.ca/en/public-health/services/diseases/avian-influenza-h5n1/health-professionals.html
10.Sandhu S, Ferrante C, MacCosham A, Atchessi N, Bancej C. Epidemiological characteristics of human infections with avian influenza A(H5N6) virus, China and Laos: A multiple case descriptive analysis, February 2014 - June 2023. Can Commun Dis Rep. 2024;50:77-85. doi: 10.14745/ccdr.v50i12a09 PubMed
11.Public Health Agency of Canada. Influenza A virus subtypes H5, H7, and H9: Infectious substances pathogen safety data sheet. 2023. Accessed January 16, 2025. https://www.canada.ca/en/public-health/services/laboratory-biosafety-biosecurity/pathogen-safety-data-sheets-risk-assessment/influenza-a-virus-subtypes-h5-h7-h9.html
12.Lorbach JN, Nelson SW, Lauterbach SE, et al. Influenza vaccination of swine reduces public health risk at the swine-human interface. mSphere. 2021;6(3):e0117020. doi: 10.1128/mSphere.01170-20 PubMed
13.Charisis N. Avian influenza biosecurity: A key for animal and human protection. Vet Ital. 2008;44(4):657-669. PubMed
14.Public Health Agency of Canada. Avian influenza A(H5N1): Prevention and risks. 2025. Accessed January 16, 2025. https://www.canada.ca/en/public-health/services/diseases/avian-influenza-h5n1/prevention-risks.html
15.Ramirez A, Capuano AW, Wellman DA, Lesher KA, Setterquist SF, Gray GC. Preventing zoonotic influenza virus infection. Emerg Infect Dis. 2006;12(6):997-1000. doi: 10.3201/eid1206.051576 PubMed
16.Harrison R, Mubareka S, Papenburg J, et al. Ammi Canada 2023 update on influenza: Management and emerging issues. J Assoc Med Microbiol Infect Dis Can. 2023;8(3):176-185. doi: 10.3138/jammi-2023-07-12 PubMed
17.Centers for Disease Control and Prevention (CDC). Highly pathogenic avian influenza A(H5N1) virus: Interim recommendations for prevention, monitoring, and public health investigations. 2024. Accessed January 16, 2025. https://www.cdc.gov/bird-flu/prevention/hpai-interim-recommendations.html
18.Mishin VP, Patel MC, Chesnokov A, et al. Susceptibility of influenza A, B, C, and D viruses to baloxavir(1). Emerg Infect Dis. 2019;25(10):1969-1972. doi: 10.3201/eid2510.190607 PubMed
19.Centers for Disease Control and Prevention (CDC). Interim guidance on the use of antiviral medications for treatment of human infections with novel influenza A viruses associated with severe human disease. 2024. Accessed January 16, 2025. https://www.cdc.gov/bird-flu/hcp/novel-av-treatment-guidance/
20.Gao Y, Guyatt G, Uyeki TM, et al. Antivirals for treatment of severe influenza: A systematic review and network meta-analysis of randomised controlled trials. Lancet. 2024;404(10454):753-763. doi: 10.1016/S0140-6736(24)01307-2 PubMed
21.Zhao Y, Gao Y, Guyatt G, et al. Antivirals for post-exposure prophylaxis of influenza: A systematic review and network meta-analysis. Lancet. 2024;404(10454):764-772. doi: 10.1016/S0140-6736(24)01357-6 PubMed
22.World Health Organization. Clinical practice guidelines for influenza. 2024. Accessed February 26, 2025. https://iris.who.int/bitstream/handle/10665/378872/9789240097759-eng.pdf
Appendix 1: Selection of Included Studies
Appendix 2: List of Excluded Studies by Reason for Exclusion
Please note that this appendix has not been copy-edited.
Irrelevant Population (n = 5)
Chen HD, Wang X, Yu SL, Ding YH, Wang ML, Wang JN. Clinical effectiveness of intravenous peramivir compared with oseltamivir in patients with severe influenza a with primary viral pneumonia: A randomized controlled study. Open Forum Infect Dis 2021;8(1):562. PubMed
Gao R, Pascua PN, Chesnokov A, Nguyen H, Uyeki T, Mishin V, et al. Antiviral susceptibility of swine-origin influenza A viruses isolated from humans, United States. Emerg Infect Dis Journal 2024;30(11):2303. PubMed
Ikematsu H, Hayden FG, Kawaguchi K, Kinoshita M, de Jong MD, Lee N, et al. Baloxavir marboxil for prophylaxis against influenza in household contacts. N Engl J Med 2020;383(4):309-20. PubMed
Kumar D, Ison MG, Mira JP, Welte T, Hwan Ha J, Hui DS, et al. Combining baloxavir marboxil with standard-of-care neuraminidase inhibitor in patients hospitalised with severe influenza (FLAGSTONE): A randomised, parallel-group, double-blind, placebo-controlled, superiority trial. Lancet Infect Dis 2022;22(5):718-30. PubMed
Mishin VP, Patel MC, Chesnokov A, De La Cruz J, Nguyen HT, Lollis L, et al. Susceptibility of influenza A, B, C, and D viruses to baloxavir. Emerg Infect Dis 2019;25(10):1969-72. PubMed
Irrelevant Intervention (n = 3)
Cheng W, Pan A, Rathbun SL, Ge Y, Xiao Q, Martinez L, et al. Effectiveness of neuraminidase inhibitors to prevent mortality in patients with laboratory-confirmed avian influenza A H7N9. Int J Infect Dis 2021;103:573-8. PubMed
Lim JJ, Nilsson AC, Silverman M, Assy N, Kulkarni P, McBride JM, et al. A phase 2 randomized, double-blind, placebo-controlled trial of MHAA4549A, a monoclonal antibody, plus oseltamivir in patients hospitalized with severe influenza A virus infection. Antimicrob Agents Chemother 2020;64(7):23. PubMed
Yang Y, Wong G, Yang L, Tan S, Li J, Bai B, et al. Comparison between human infections caused by highly and low pathogenic H7N9 avian influenza viruses in wave five: Clinical and virological findings. J Infect 2019;78(3):241-8. PubMed
Irrelevant Comparator (n = 5)
Fu B, Wu Z, Huang L, Chai Z, Zheng P, Sun Q, et al. A comparison of demographic, epidemiological and clinical characteristics of hospital influenza-related viral pneumonia patients. BMC Infect Dis 2021;21(1). PubMed
Garg S, Reinhart K, Couture A, Kniss K, Davis CT, Kirby MK, et al. Highly pathogenic avian influenza A(H5N1) virus infections in humans. N Engl J Med 2024;31:31. PubMed
Hegde S, Thyagaraj V, Prabhu D. H1N1 influenza revisited: Our experience of the 2019 outbreak. Bangladesh J Med Sci 2022;21(2):426-31.
Yang Y, Li X, Birkhead GS, Zheng Z, Lu JH. Clinical indices and mortality of hospitalized avian influenza A (H7N9) patients in Guangdong, China. Chin Med J 2019;132(3):302-10. PubMed
Zheng S, Zou Q, Wang X, Bao J, Yu F, Guo F, et al. Factors associated with fatality due to avian influenza A(H7N9) infection in China. Clin Infect Dis 2020;71(1):125-32. PubMed
Irrelevant Outcome(s) (n = 1)
Wang WH, Erazo EM, Ishcol MRC, Lin CY, Assavalapsakul W, Thitithanyanont A, et al. Virus-induced pathogenesis, vaccine development, and diagnosis of novel H7N9 avian influenza A virus in humans: A systemic literature review. J Int Med Res 2020;48(1). PubMed
Ineligible Study Design (n = 11)
Centers for Disease Control and Prevention (CDC). Highly pathogenic avian influenza A(H5N1) virus: Interim recommendations for prevention, monitoring, and public health investigations. CDC; 2024. https://www.cdc.gov/bird-flu/prevention/hpai-interim-recommendations.html. Accessed 2025 Jan 16.
Centers for Disease Control and Prevention (CDC). Interim guidance on the use of antiviral medications for treatment of human infections with novel influenza A viruses associated with severe human disease. CDC; 2024. https://www.cdc.gov/bird-flu/hcp/novel-av-treatment-guidance/index.html#:~:text=Initiation%20of%20antiviral%20treatment%20with%20oral%20or%20enterically%20administered%20oseltamivir,of%20time%20since%20illness%20onset. Accessed 2025 Jan 16.
Center for Infectious Disease Research and Policy (CIDRAP). 3 new studies probe the efficacy of antivirals in preventing, treating flu. CIDRAP; 2024. https://www.cidrap.umn.edu/influenza-general/3-new-studies-probe-efficacy-antivirals-preventing-treating-flu#:~:text=Of%20three%20new%20studies%20on,death%20from%20flu%2Drelated%20pneumonia. Accessed 2025 Jan 16.
Center for Infectious Disease Research and Policy (CIDRAP). Study says baloxavir fights all 4 flu types, many animal flu viruses. CIDRAP; 2019. https://www.cidrap.umn.edu/influenza-general/study-says-baloxavir-fights-all-4-flu-types-many-animal-flu-viruses. Accessed 2025 Jan 16.
Guan W, Qu R, Shen L, Mai K, Pan W, Lin Z, et al. Baloxavir marboxil use for critical human infection of avian influenza A H5N6 virus. Med 2024;5(1):32-41. PubMed
Kumari R, Sharma Suresh D, Kumar A, Ende Z, Mishina M, Wang Y, et al. Antiviral approaches against influenza virus. Clin Microbiol Rev 2023;36(1):e00040-22. PubMed
Lafond KE, Praptiningsih CY, Mangiri A, Syarif M, Triada R, Mulyadi E, et al. Seasonal influenza and avian influenza A(H5N1) virus surveillance among inpatients and outpatients, East Jakarta, Indonesia, 2011-2014. Emerg Infect Dis 2019;25(11):2031-9. PubMed
Mehta K, Goneau LW, Wong J, L'Huillier AG, Gubbay JB. Zoonotic influenza and human health-part 2: Clinical features, diagnosis, treatment, and prevention strategies. Curr Infect Dis Rep 2018;20(10):38. PubMed
Mishra R. H1N1 infection complications and potential moieties for treatment: A systematic review. Int J Pharm Res 2020;12(Supplementary 1):905-9.
Public Health Agency of Canada. Guidance on human health issues related to avian influenza in Canada (HHAI). Government of Canada; 2024. https://www.canada.ca/en/public-health/services/publications/diseases-conditions/guidance-human-health-issues-avian-influenza.html. Accessed 2025 Jan 16.
United Nations Environment Programme (UNEP). Preventing the next pandemic - Zoonotic diseases and how to break the chain of transmission. Nairobi (KE): UNEP; 2020. https://www.unep.org/resources/report/preventing-future-zoonotic-disease-outbreaks-protecting-environment-animals-and. Accessed 2025 Jan 16.
Duplicate Study (n = 3)
Gao Y, Guyatt G, Uyeki TM, Liu M, Chen Y, Zhao Y, et al. Antivirals for treatment of severe influenza: A systematic review and network meta-analysis of randomised controlled trials. Lancet 2024;404(10454):753-63. PubMed
Guan W, Qu R, Shen L, Mai K, Pan W, Lin Z, et al. Baloxavir marboxil use for critical human infection of avian influenza A H5N6 virus. medRxiv 2023;05.
Zhao Y, Gao Y, Guyatt G, Uyeki TM, Liu P, Liu M, et al. Antivirals for post-exposure prophylaxis of influenza: A systematic review and network meta-analysis. Lancet 2024;404(10454):764-72. PubMed
Appendix 3: Characteristics of Included Publications
Please note that this appendix has not been copy-edited.
Table 2: Characteristics of Included Systematic Reviews
Study citation, country, funding source | Study designs and numbers of primary studies included | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Gao et al. (2024)20 Country: Canada Funding source: WHO | SR / NMA of RCTs 8 RCTs with 1,424 participants; 0 RCTs relevant to the present review | Eligible population: Hospitalized patients with any type of suspected or confirmed influenza; Relevant population: Patients with zoonotic influenza Age (years), range: 36 to 60 Sex (male), range (%): 43 to 78 Laboratory-confirmed influenza patients, range (%): 79 to 100 | Intervention: Antivirals for the treatment of severe influenza: Baloxavir, oseltamivir, laninamivir, zanamivir, peramivir, umifenovir, favipiravir, amantadine, rimantadine; Relevant intervention: Baloxavir, oseltamivir, zanamivir, peramivir Comparator: Placebo, standard care without placebo, or another antiviral for treatment of severe influenza | Outcomes: Duration of hospitalization, time to symptom relief, ICU admission, progression to invasive mechanical ventilation, length of mechanical ventilation, mortality, discharge destination, antiviral resistance emergence, adverse events, treatment-related adverse events, severe adverse events Follow-up: NR |
Zhao et al. (2024)21 Country: Canada Funding source: WHO | SR / NMA of RCTs 33 RCTs with 19,096 participants; 0 RCTs relevant to the present review | Eligible population: Individuals exposed to influenza viruses; Relevant population: Individuals exposed to zoonotic influenza viruses Age (years), mean: 6.75 to 81.15 Sex NR | Intervention: antiviral prophylaxis; Eligible interventions: viral polymerase complex inhibitors, NAIs, matrix protein 2 ion channel inhibitors, cap-dependent endonuclease inhibitors; Relevant intervention: Baloxavir, oseltamivir, zanamivir, peramivir. Comparator: placebo, standard care, or another antiviral for prevention of influenza | Outcomes: Time to symptom onset, infection, symptom duration, hospital admission, hospitalization length, progression to invasive mechanical ventilation, ICU admission, mechanical ventilation duration, disease severity progression, antiviral resistance emergence, all-cause mortality, antiviral-related adverse events, serious adverse events Follow-up: NR |
ICU = intensive care unit; NAI = neuraminidase inhibitor; NMA = network meta-analysis; NR = not reported; RCT = randomized control trial; SR = systematic review.
ISSN: 2563-6596
This work was conducted by the Alberta Drug and Therapeutic Evaluation Consortium (ADTEC) through the Post-Market Drug Evaluation CoLab Network. It was supported by Canada’s Drug Agency (CDA-AMC) and its Post-Market Drug Evaluation Program through funding provided by Health Canada.
CDA-AMC is a pan-Canadian health organization. Created and funded by Canada’s federal, provincial, and territorial governments, we’re responsible for driving better coordination, alignment, and public value within Canada’s drug and health technology landscape. We provide Canada’s health system leaders with independent evidence and advice so they can make informed drug, health technology, and health system decisions, and we collaborate with national and international partners to enhance our collective impact.
CoLab is a pan-Canadian network of experts in applied research, scientific methods, and data analysis. CoLab members work with the Post-Market Drug Evaluation Program to produce credible and timely evidence on postmarket drug safety and effectiveness.
Disclaimer: CDA-AMC has taken care to ensure that the information in this document was accurate, complete, and up to date when it was published, but does not make any guarantee to that effect. Your use of this information is subject to this disclaimer and the Terms of Use at cda-amc.ca.
The information in this document is made available for informational and educational purposes only and should not be used as a substitute for professional medical advice, the application of clinical judgment in respect of the care of a particular patient, or other professional judgments in any decision-making process. You assume full responsibility for the use of the information and rely on it at your own risk.
CDA-AMC does not endorse any information, drugs, therapies, treatments, products, processes, or services. The views and opinions of third parties published in this document do not necessarily reflect those of CDA-AMC. The copyright and other intellectual property rights in this document are owned by the Canadian Agency for Drugs and Technologies in Heath (operating as CDA-AMC) and its licensors.
This document is the property of ADTEC. CDA-AMC has a nonexclusive, limited, royalty-free, worldwide, nontransferable, fully paid-up, and irrevocable license to use the report in support of its objects, mission, and reasonable operational requirements.