Drugs, Health Technologies, Health Systems
Health Technology Review
Artificial Intelligence–Assisted Colonoscopy for Detecting Polyps, Adenomas, Precancerous Lesions, and Colorectal Cancer
Key Messages
What Is the Issue?
Colorectal cancer is 1 of the most common cancers globally. In Canada, it is estimated that more than 25,000 people will be diagnosed with colorectal cancer in 2024 and that more than 9,000 people will die of it.
To reduce the incidence and mortality of colorectal cancer, screening programs across various jurisdictions in Canada have implemented screening strategies involving routine fecal testing and colonoscopy. While colonoscopy is often considered the gold standard for colorectal cancer screening, missed polyps remain a challenge with this modality.
In recent years, many artificial intelligence (AI)–enabled polyp detection systems have been developed for use during colonoscopy. A review of the clinical and cost-effectiveness of these systems could help clarify their potential role in clinical practice.
What Did We Do?
To inform decisions regarding the use of AI-assisted colonoscopy, we conducted a rapid review to identify and summarize evidence that compared the clinical and cost-effectiveness of AI-assisted colonoscopy to conventional colonoscopy and among different AI-assisted colonoscopy systems.
We searched key resources, including journal citation databases, and conducted a focused internet search for relevant evidence published since 2019. One reviewer screened articles for inclusion based on predefined criteria, critically appraised the included studies, and narratively summarized the findings.
What Did We Find?
We found 1 health technology assessment (HTA), 3 systematic reviews (SRs), and 1 randomized controlled trial (RCT) that evaluated the clinical and cost-effectiveness of AI-assisted colonoscopy for detecting polyps, adenomas, precancerous lesions, and colorectal cancer.
AI-assisted colonoscopy may improve clinical outcomes compared to conventional colonoscopy, including adenoma detection rates, the number of adenomas detected per procedure, and adenoma miss rates, although it may also lead to longer withdrawal times. However, not all studies included in this report demonstrated statistically significant differences between the groups for each of these outcomes.
The included RCT allocated participants to receive AI-assisted colonoscopy with either Deep-GI or CAD EYE, but the authors did not perform statistical testing to compare the outcomes between these 2 treatment groups.
Findings from 6 economic evaluations summarized in the HTA suggest that AI-assisted colonoscopy is likely to be cost-effective or dominant — meaning it is less costly and more effective — compared to conventional colonoscopy.
We did not find any studies on the relative cost-effectiveness of different AI-assisted colonoscopy systems that met our selection criteria for this review.
None of the included studies reported long-term outcomes, such as colorectal cancer incidence and mortality; therefore, the impact of AI-assisted colonoscopy on these outcomes is unknown.
What Does This Mean?
AI-assisted colonoscopy may improve clinical outcomes and be more cost-effective than conventional colonoscopy for detecting polyps, adenomas, precancerous lesions, and colorectal cancer.
The clinical and cost-effectiveness of different types of AI-assisted colonoscopy systems compared to each other is unknown.
Clinicians and decision-makers can use the evidence summarized in this review to inform decisions regarding the implementation of AI-assisted colonoscopy.
Abbreviations
AI
artificial intelligence
HTA
health technology assessment
NHS
UK National Health Service
RCT
randomized controlled trial
SR
systematic review
Research Questions
What is the clinical effectiveness of AI-assisted colonoscopy versus conventional colonoscopy for the detection of polyps, adenomas, precancerous lesions, and colorectal cancer?
What is the clinical effectiveness of different AI-assisted colonoscopy systems versus each other for the detection of polyps, adenomas, precancerous lesions, and colorectal cancer?
What is the cost-effectiveness of AI-assisted colonoscopy versus conventional colonoscopy for the detection of polyps, adenomas, precancerous lesions, and colorectal cancer?
What is the cost-effectiveness of different AI-assisted colonoscopy systems versus each other for the detection of polyps, adenomas, precancerous lesions, and colorectal cancer?
Context and Policy Issues
What Is Colorectal Cancer?
Colorectal cancer is a type of cancer that develops in the cells that line the inside of the colon or rectum, which are parts of the large intestine. In 2024, an estimated 25,200 new cases will be diagnosed in Canada, making it the fourth most common cancer.1 It is also the second leading cause of cancer-related mortality in Canada, with approximately 9,400 deaths projected this year.2
Most cases of colorectal cancer begin as small, noncancerous growths called polyps. Over time, some of these polyps can develop into cancer.3 Symptoms of colorectal cancer include diarrhea, constipation, blood in the stool, abdominal pain or discomfort, unexplained weight loss, fatigue, and anemia (low iron levels).4,5 Factors that may affect an individual’s risk for developing colorectal cancer include age, family history, race, inflammatory bowel disease, physical activity levels, diet, and alcohol or tobacco use.6
Colorectal cancers tend to develop slowly and are often highly treatable when detected early, while the disease is localized to the bowel. For stage I colorectal cancers, the 5-year net survival rate exceeds 90%.7 However, because many people show no symptoms in the early stages of the disease, identifying individuals who could benefit from early intervention is challenging.8
What Is the Current Practice?
Over the past 20 years, provinces and territories across Canada have established organized colorectal cancer screening programs. While screening guidelines vary between jurisdictions, they generally recommend screening asymptomatic, average-risk individuals between the ages of 50 and 74 or 75 every 12 to 24 months using a fecal test, such as the fecal immunochemical test or the guaiac fecal test, as the primary screening method.9 These guidelines align with recommendations from the Canadian Task Force on Preventive Health Care.10
Individuals who receive abnormal results from a fecal test are typically referred for further evaluation with a colonoscopy.9,11 In some jurisdictions, individuals may also be referred directly for colonoscopy by a primary care provider or through self-referral, depending on their risk level.9,12,13 Colonoscopy is a medical procedure used to examine the large intestine. It is performed using a colonoscope, a flexible, hand-held, tube-like device equipped with a high-definition camera at its tip. The colonoscope is inserted into the large intestine, and the camera provides a real-time video feed that allows clinicians to inspect the colon and rectum for abnormalities. During the procedure, polyps, adenomas, or other suspicious tissues can be sampled or removed as necessary.14 Though colonoscopy has been established as a highly sensitive and definitive test, it may not detect polyps or colorectal neoplasia if they are small or located in hard-to-see areas.15,16 Colonoscopies are usually performed in hospitals, clinics, or doctors’ offices, and they take about 30 to 45 minutes.17
Data from the 2017 cycle of the Canadian Community Health Survey suggest that there are disparities in access to colorectal cancer screening programs, with newcomers to Canada and members of racialized groups experiencing inequities.18 To help address these challenges, many colorectal screening programs have implemented strategies to increase and improve screening in different populations, including rural and remote populations; groups that are underserved; 2SLGBTQ+ populations; and First Nations, Inuit, and Métis Peoples. For example, the Alberta Colorectal Cancer Screening Program has worked with Indigenous partners to develop and provide culturally appropriate information and has piloted nurse practitioner–led integrated mobile screening services to increase community outreach.9
When it comes to treatment, how colorectal cancer is managed depends on the location and stage of the disease. Surgical resection is the primary form of treatment, but additional options include chemotherapy (e.g., capecitabine, irinotecan), radiotherapy, targeted therapy (e.g., bevacizumab, cetuximab), and immunotherapy (e.g., ipilimumab, pembrolizumab).19-21
What Is AI-Assisted Colonoscopy and What Are Its Potential Benefits?
AI is a branch computer science, statistics, and engineering that uses algorithms or models to perform tasks and exhibit behaviours such as learning, making decisions, and making predictions.22 In recent years, AI has driven significant technological advancements in health care. AI-enabled technologies have been developed to assist with decision-making in patient diagnosis and treatment, transcribe medical documents, aid in drug discovery and development, and streamline clinical workflows by automating administrative tasks.23-25
AI-assisted colonoscopy systems have been developed to analyze real-time images generated during the procedure, identifying areas of concern. These systems typically highlight suspicious regions of the large intestine with a visual marker, such as a box, to indicate potential mucosal abnormalities. In real-time, the clinician can then assess these flagged regions as part of their evaluation and make a final decision on whether to remove or biopsy the identified abnormality.26 The first AI-assisted colonoscopy system to receive Health Canada licensing for sale was introduced in 2021.26,27 Since then, AI-assisted colonoscopy has been implemented in various clinical settings across Canada.28-30 Globally, there are many different types of AI-assisted colonoscopy systems currently available or under development, many of which are compatible with any colonoscope and do not require specialized infrastructure to implement.31 The potential benefits of AI-assisted colonoscopy may include increased detection rates of polyps and other abnormalities, reduced adenoma miss rates, and improved inter-reader or inter-centre variability in colonoscopy, which could lead to earlier intervention and improved patient outcomes.32
Why Is It Important to Do This Review?
Colonoscopy plays a critical role in colorectal cancer screening programs across Canada, yet the issue of missed polyps and colorectal neoplasia during the procedure remains a significant concern.33,34 AI-assisted colonoscopy systems have the potential to increase detection rates and improve patient outcomes. A review of the available evidence is important to understand how these systems may impact the effectiveness of colonoscopy and to guide informed decision-making regarding their implementation into clinical practice.
Objective
The purpose of this rapid review is to identify, summarize, and critically appraise evidence comparing the clinical and cost-effectiveness of AI-assisted colonoscopy to conventional colonoscopy, as well as make comparisons among different AI-assisted systems, for detecting polyps, adenomas, precancerous lesions, and colorectal cancer.
Methods
An information specialist conducted a customized literature search, balancing comprehensiveness with relevancy, of multiple sources and grey literature on October 9, 2024. One reviewer screened citations and selected studies based on the inclusion criteria presented in Table 1 and critically appraised included publications using established critical appraisal tools. Appendix 1 presents a detailed description of methods and selection of included studies.
Criteria | Description |
|---|---|
Population | People undergoing colonoscopy for the screening, diagnosis, or surveillance of polyps, adenomas, precancerous lesions, or colorectal cancer |
Intervention | Real-time AI-assisted colonoscopy |
Comparator | Q1 and Q3: Conventional colonoscopy (i.e., performed without AI assistance) Q2 and Q4: Real-time AI-assisted colonoscopy with alternative systems |
Outcomes | Q1 and Q2: Clinical benefits (e.g., detection rates, miss rates, polyps per procedure, procedure time) and harms (e.g., adverse events) Q3 and Q4: Cost-effectiveness (e.g., cost per quality-adjusted life-year gained) |
Study designs | Q1: HTAs and SRs Q2: HTAs, SRs, RCTs, and nonrandomized studies Q3 and Q4: HTAs, SRs, and economic evaluations |
Publication date | Since January 1, 2019 |
AI = artificial intelligence; HTA = health technology assessment; RCT = randomized controlled trial; SR = systematic review.
Summary of Evidence
Quantity of Research Available
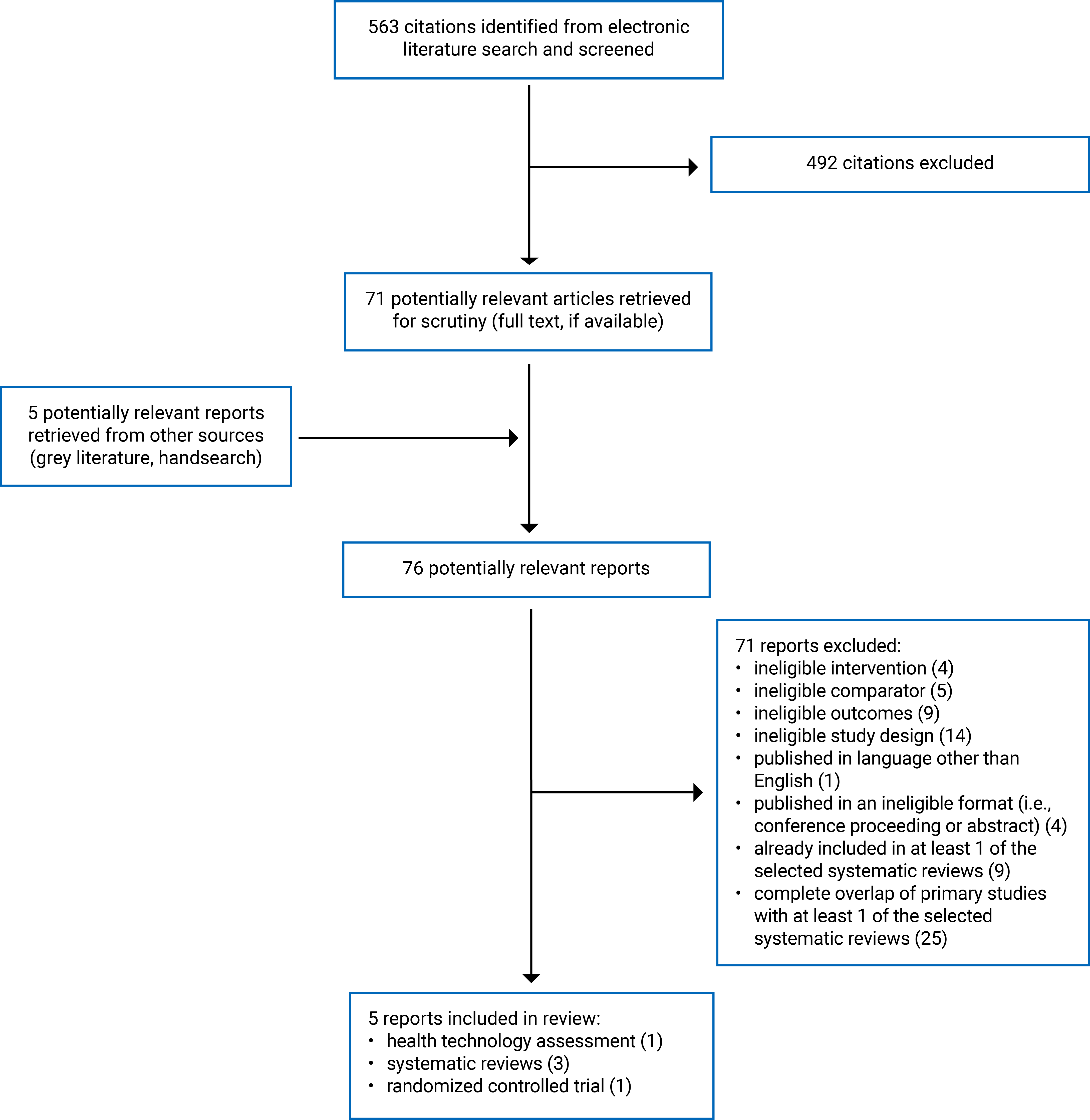
This report includes 1 HTA,35 3 SRs,36-38 and 1 RCT.39 Appendix 1 presents the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA)40 flow chart of the study selection. Appendix 6 provides additional references of potential interest that did not meet our inclusion criteria.
Summary of Study Characteristics
Summaries of study characteristics are organized by research question. Appendix 2 provides detailed characteristics of the included publications.
Included Studies for Question 1: Clinical Effectiveness of AI-Assisted Colonoscopy Versus Conventional Colonoscopy
We identified 4 SRs with meta-analyses,35-38 1 of which was conducted as part of an HTA,35 to address this research question. These SRs35-38 included data from a total of 54 unique primary clinical studies; however, there was considerable overlap among the included primary studies. As a result, the pooled effect estimates from separate reviews are based on much of the same data, although not all reviews reported the same outcomes. A citation matrix illustrating the degree of primary study overlap is presented in Appendix 5.
The authors of the SR and meta-analysis conducted as part of the HTA by Health Technology Wales35 searched for studies published between January 2010 and March 2024. The authors included 4 SRs with meta-analyses of RCTs and 7 further RCTs that were published after the latest search in their included SRs. In total, their analysis included evidence from 39 RCTs.
In the 2 included SRs with meta-analyses36 study design was limited to RCTs. The SR by Lee et al.36 included 26 RCTs published up to March 2023, while the SR by Aslam et al.38 included 11 RCTs published up to April 21, 2022.
The authors of the fourth SR with meta-analysis37 searched for nonrandomized studies published between January 1, 2020, and April 1, 2023, and identified 12 relevant nonrandomized studies.
Two SRs with meta-analyses35,36 provided information on the age and sex of participants from the included primary studies; however, the authors did not report how sex was defined or measured. None of the included SRs35-38 provided participant information for other PROGRESS-Plus criteria,41,42 such as place of residence, race, ethnicity, culture, language, occupation, religion, education, socioeconomic status, or social capital.
A variety of AI-enabled colonoscopy systems were evaluated across the included SRs and meta-analyses,35-38 including CAD EYE, Deep-GI, Eagle-Eye, ENDO-AID, EndoAngel, EndoScreener, EndoVigilant, GI Genius, MAGENTIQ-COLO, SKOUT, and other self-developed or unnamed systems.
Clinical outcomes assessed across the 4 SRs with meta-analyses35-38 to address research question 1 included:
detection rates for adenomas, polyps, sessile serrated lesions, or carcinomas
the number of adenomas, polyps, or sessile serrated lesions detected per colonoscopy
miss rates for adenomas or sessile serrated lesions
withdrawal time
procedure time
adverse events (e.g., polypectomies of non-neoplastic lesions per colonoscopy).
Included Studies for Question 2: Clinical Effectiveness of Different AI-Assisted Colonoscopy Systems Versus Each Other
We found 1 RCT39 that evaluated the clinical effectiveness of 2 different AI-assisted colonoscopy systems. This parallel-group RCT39 included 1,200 participants between the ages of 50 and 75 years who were randomized to receive colonoscopy performed with Deep-GI, CAD EYE, or conventional white-light endoscopy (1:1:1 ratio). Only data from the Deep-GI and CAD EYE groups were considered relevant for addressing research question 2. The study39 was conducted at 5 endoscopy referral centres in Thailand between February 2022 and May 2023. The mean age of participants was 62.7 years, and the proportion of male participants was 39.8% (other sexes or genders were not reported). The authors also provided the following information on study participants: body mass index, family history of colorectal cancer, and smoking status. No other PROGRESS-Plus criteria41,42 were reported.
Clinical outcomes assessed included adenoma, proximal adenoma, and advanced adenoma detection rates; the number of adenomas, proximal adenomas, and advanced adenomas detected per colonoscopy; and adverse events.
Though the authors of this study39 provided results for each of the AI-assisted colonoscopy groups separately, their statistical analysis compared outcomes of either AI-assisted colonoscopy group to the control group (i.e., conventional white-light colonoscopy) rather than against each other, limiting the applicability of their findings to our research question.
Included Studies for Question 3: Cost-Effectiveness of AI-Assisted Colonoscopy Versus Conventional Colonoscopy
We identified 1 HTA35 that provided information on the cost-effectiveness of AI-assisted colonoscopy versus conventional colonoscopy. The HTA35 included an SR of economic evidence that summarized findings from 5 relevant economic evaluations. Appendix 2 (Table 5) details the characteristics of these 5 economic evaluations, as reported in Health Technology Wales (2024).35
In addition to the SR,35 Health Technology Wales researchers developed their own cost-utility analysis to evaluate the cost-effectiveness of AI-assisted colonoscopy compared with conventional colonoscopy for the detection of cancer and precancerous lesions from the perspective of the UK National Health Service (NHS). They used a decision tree model to capture the effects of each screening approach. Everyone entering the model had undergone either AI-assisted colonoscopy or conventional colonoscopy and were then assigned to various health states (e.g., nothing detected, low-risk adenoma, high-risk adenoma, colorectal cancer). Costs and benefits (i.e., quality-adjusted life-years) were evaluated over a lifetime horizon and discounted at an annual rate of 3.5%.
Clinical model inputs (e.g., cohort characteristics, adenoma detection rates, consequences of missed polyps) were drawn from meta-analyses conducted as part of the HTA35 and various sources of published literature. Cost inputs were sourced from NHS Supply Chain, 2021–2022 NHS reference costs, manufacturers of AI-assisted colonoscopy systems, and various sources of published literature and unpublished data. Costs were inflated to 2021–2022 prices using the NHS cost inflation index. Quality-adjusted life-year inputs and model-state transition probabilities were sourced from unpublished data or a previous National Institute for Health and Care Excellence assessment of fecal immunochemical testing to guide colorectal cancer pathway referral in primary care, or they were based on assumptions.35
Included Studies for Question 4: Cost-Effectiveness of Different AI-Assisted Colonoscopy Systems Versus Each Other
We found no relevant studies that addressed research question 4; therefore, no summary can be provided.
Summary of Critical Appraisal
Critical appraisal summaries are organized by study design. Appendix 3 presents additional details regarding the strengths and limitations of the included publications.
Systematic Reviews
The authors of all 4 SRs,35-38 including the SR from the HTA,35 clearly defined their objectives and eligibility criteria, conducted comprehensive literature searches across multiple databases, and provided details on key search terms and search dates. They also included flow charts illustrating the study selection along with their reasons for excluding studies. These methodological strengths increase the reproducibility of the SRs. The review methods for all 4 SRs35-38 were established before conducting the reviews (e.g., they were documented in published protocols), reducing the risk of reporting bias. The quality of the included primary studies was assessed using transparent and satisfactory techniques in 3 SRs,36-38 and the authors of 2 SRs35,36 reported the sources of funding for the included primary studies. Publication bias was assessed by the authors of 2 SRs37,38 using funnel plots. In both cases, the authors suggested that the risk for publication bias was low. All 4 SRs35-38 reported the characteristics of included studies in sufficient detail (e.g., study design, number of participants, study location) and used appropriate methods for the statistical combination of results and assessing statistical heterogeneity (e.g., the I2 statistic).
As for methodological limitations, the authors of all 4 SRs35-38 did not conduct a grey literature search, increasing the risk of missing relevant studies that are not published commercially and that may be inaccessible via bibliographic databases (i.e., nonindexed studies). Three SRs35-37 limited included studies to those published in English or did not specify which languages were eligible for inclusion, potentially introducing language bias and omitting relevant data from non-English studies. In 3 SRs,35,36,38 it was unclear if study selection, data extraction, or critical appraisal were conducted by a single reviewer or multiple reviewers, creating a risk for inaccuracies in these processes. The authors of all 4 SRs35-38 included primary studies in pooled analyses regardless of their study quality and did not assess the potential impact of risk of bias on the meta-analysis findings. As such, it is unclear whether results from primary studies with a low risk of bias might have differed from the overall pooled estimates. In 2 SRs,35,36 the authors did not provide an explanation for the considerable statistical heterogeneity observed in the meta-analyses. The generalizability of findings from all 4 SRs35-38 to settings in Canada was unclear because of limited reporting on the characteristics of primary study participants (e.g., across PROGRESS-Plus criteria).41,42 Finally, the authors of 1 SR35 did not state their potential conflicts of interest, and the sources of funding for 1 SR36 was unclear.
Randomized Controlled Trial
The authors of the RCT39 provided clear descriptions of the study’s aim, interventions, comparator, participant eligibility criteria, and main outcomes. The methods for randomization and allocation concealment were appropriate, which reduced the risk of selection bias. Additional methodological strengths were that compliance with the assigned intervention was reliable, outcome measures were valid, and authors reported estimates of random variability (e.g., confidence intervals) and actual P values. Procedural adverse events were recorded, and care providers and settings appeared to be representative of those of interest. The authors declared that they had no potential conflicts of interest related to this work and reported their sources of funding, which were unrelated to industry and considered unlikely to have influenced the study’s findings.
Several factors affected the internal and external validity of this RCT.39 Because of the nature of the intervention, endoscopists (i.e., outcome assessors) were aware of the intervention each participant received. This could have led to differential treatment across treatment arms, potentially introducing bias into the estimates of treatment effects. Additionally, endoscopists may have modified their approach to colonoscopy, knowing that the results of their examination were being recorded for the study (i.e., the Hawthorne effect), potentially influencing study findings. Although the authors reported some relevant baseline participant characteristics (e.g., age, sex, body mass index), many important characteristics that stratify health opportunities and outcomes were not reported, such as race, ethnicity, culture, language, place of residence, socioeconomic status, and other PROGRESS-Plus criteria.41,42 As a result, it remains unclear whether the study population is representative and whether the findings of this RCT39 conducted in Thailand can be generalized to settings in Canada.
Economic Evaluation
The authors of the economic evaluation35 clearly stated their research question, objectives, the economic importance of the research question, the screening strategies compared, and rationale for conducting the analysis from the perspective of the NHS and Personal Social Services using a lifetime horizon. They provided detailed information on the sources of the effectiveness estimates, utility values, and treatment costs. The authors recorded the currency and price data used and the methods for adjusting prices for inflation, described their approach to sensitivity analyses, reported incremental analyses, provided an answer to the study question, and summarized the findings with conclusions accompanied by appropriate caveats.
The primary limitation of the economic evaluation35 is the uncertain generalizability of its findings to settings in Canada. Key model inputs were mainly derived from UK data. Results from deterministic scenario analyses conducted as part of the economic evaluation suggest that changes to several model inputs (e.g., cost of non-neoplastic lesion removal) could lead to different conclusions about the cost-effectiveness of AI-assisted colonoscopy. Any differences in adenoma prevalence, colorectal cancer screening strategies, consequences of missed polyps, and the costs associated with implementing AI-assisted colonoscopy between health care systems in the UK and Canada could impact the relevance of the cost-effectiveness findings.
Summary of Findings
Appendix 4 presents additional details regarding the main study findings.
Clinical Effectiveness of AI-Assisted Colonoscopy Versus Conventional Colonoscopy
Evidence regarding the clinical effectiveness of AI-assisted colonoscopy versus conventional colonoscopy for the detection of polyps, adenomas, precancerous lesions, and colorectal cancer was available from 4 SRs with meta-analyses.35-38 There was considerable overlap in the primary studies that were included in these SRs; the pooled estimates from separate reviews thus contain much of the same data (refer to Appendix 5 for details regarding overlap).
Detection Rates
The results from all 4 SRs with meta-analyses35-38 indicate that AI-assisted colonoscopy has statistically significantly higher adenoma detection rates than conventional colonoscopy. Similarly, pooled analyses from 2 SRs35,38 suggest that AI-assisted colonoscopy results in statistically significantly higher polyp detection rates than conventional colonoscopy.
For advanced adenoma detection rates, pooled estimates from 2 SRs35,36 indicate no difference between AI-assisted colonoscopy and conventional colonoscopy.
Findings for sessile serrated lesion detection rates were mixed. One SR,35 based on a pooled analysis of 19 RCTs, reported that AI-assisted colonoscopy was associated with statistically significantly higher sessile serrated lesion detection rates. Another SR,36 based on a pooled analysis of 12 RCTs, found no statistically significant difference in sessile serrated lesion detection rates.
One SR35 provided a narrative summary of 13 RCTs that evaluated carcinoma detection rates of AI-assisted colonoscopy versus conventional colonoscopy. There was no evidence of a difference in carcinoma detection rates between the groups in any of these primary studies. The confidence intervals for many of these comparisons were wide, indicating imprecision in the effect estimates. This imprecision may have been because of the low event rates for carcinoma detection, which ranged from 0% to 4% in AI-assisted colonoscopy groups and between 0% to 3.2% for conventional colonoscopy groups across the 13 RCTs.
Abnormalities Detected Per Colonoscopy
Two SRs with meta-analyses36,37 reported mixed evidence on the effect of AI-assisted colonoscopy on the number of abnormalities detected per colonoscopy. AI-assisted colonoscopy was associated with statistically significant increases in the number of adenomas detected per colonoscopy based on a pooled analysis of 23 RCTs by Lee et al.36 The other SR37 found no statistically significant difference in adenomas per colonoscopy, based on a pooled analysis of 6 nonrandomized studies.
One SR with meta-analysis36 compared the number of advanced adenomas and the number of sessile serrated lesions detected per colonoscopy with and without AI assistance. For both outcomes, there was no statistically significant difference between AI-assisted colonoscopy and conventional colonoscopy. The findings for advanced adenomas were based on a pooled analysis of 13 RCTs, while those for sessile serrated lesions were based on pooled data from 16 RCTs.
Miss Rates
Two SRs with meta-analyses35,36 described the clinical effectiveness of AI-assisted colonoscopy versus conventional colonoscopy with respect to miss rates:
Both SRs found that AI-assisted colonoscopy led to statistically significantly lower adenoma miss rates, based on pooled analyses of 6 RCTs35 and 24 RCTs.36
One SR35 reported no differences in advanced adenoma miss rates, based on a pooled analysis of 3 RCTs.
One SR35 reported that AI-assisted colonoscopy resulted in statistically significantly lower sessile serrated lesion miss rates, based on a pooled analysis of 4 RCTs.
Withdrawal Times
Three SRs with meta-analyses35,36,38 provided mixed results for withdrawal times:
One SR35 provided a narrative summary of a previous SR with meta-analysis (Lou et al. [2023]), which included a pooled analysis of 18 RCTs. The authors of this analysis estimated that withdrawal times excluding biopsy were statistically significantly longer for patients who received AI-assisted colonoscopy. The mean difference of 20 seconds was considered clinically unimportant by experts contacted by Health Technology Wales. The authors of the SR35 also conducted a narrative review of 10 further RCTs that reported withdrawal time excluding biopsy; 3 RCTs reported a small but clinically unimportant increase in withdrawal time for AI-assisted colonoscopy, while the remaining 7 RCTs studies reported no difference between groups. For withdrawal times including biopsy, the SR35 summarized the findings from a previous SR with meta-analysis of 4 RCTs (Huang et al. [2022]) and a 4 further RCTs, which suggested that AI-assisted colonoscopy was associated with small statistically significant increases in time. The clinical importance of these increases was not specified.
Two SRs,36,38 without distinguishing withdrawal times with or without biopsy, found that AI-assisted colonoscopy led to statistically significantly longer withdrawal times. These findings were based on pooled analyses of 18 RCTs in 1 review36 and 8 RCTs in the other.38
Procedure Times
The authors of 1 SR35 conducted a narrative synthesis of 6 RCTs that provided information on procedure times. Among these, 1 RCT found a statistically significant increase in procedure times with AI-assisted colonoscopy compared to conventional colonoscopy, with the difference being less than 1 minute. Experts contacted by Health Technology Wales considered this difference not clinically important. There was no evidence of a difference in procedure times between the groups in any of the remaining 5 RCTs.
Adverse Events
One included SR35 provided a narrative synthesis of adverse event data from 2 previous SRs with meta-analysis (Lou et al. [2023]; Hassan et al. [2023b]) and 5 additional RCTs. Findings from 2 SRs, based on pooled estimates from 18 RCTs and 12 RCTs, and 1 additional RCT suggest that AI-assisted colonoscopy leads to statistically significant increases in the number of polypectomies of non-neoplastic lesions per colonoscopy.
Findings for non-neoplastic lesion resection rates were mixed.35 One SR (Lou et al. [2023]) found no statistically significant difference in non-neoplastic lesion resection rates between AI-assisted colonoscopy and conventional colonoscopy. One RCT summarized in the SR35 reported statistically significantly higher non-neoplastic lesion resection rates in the AI-assisted colonoscopy group compared to the conventional colonoscopy group.
The SR35 summarized data from 22 RCTs on overall adverse event rates. Of these, 18 RCTs reported no adverse events, while 4 RCTs reported that at least 1 adverse event occurred. There was no evidence of a difference in adverse event rates between the groups in any of these studies (i.e., P values were insignificant or were not reported).
Clinical Effectiveness of Different AI-Assisted Colonoscopy Systems Versus Each Other
One included RCT39 provided information on the clinical effectiveness of 2 different AI-assisted colonoscopy systems, Deep-GI and CAD EYE.
Detection Rates
The RCT39 reported adenoma detection rates of 54.8% for the Deep-GI group and 50.0% for the CAD EYE group, proximal adenoma detection rates of 38.8% for the Deep-GI group and 32.3% for the CAD EYE group, advanced adenoma detection rates of 9.5% for the Deep-GI group and 10.3% for the CAD EYE group, and sessile serrated lesion detection rates of 3.0% for the Deep-GI group and 2.3% for the CAD EYE group. The authors of the RCT39 did not perform statistical testing to assess whether differences in any of the detection rates between the groups were significant.
Abnormalities Detected Per Colonoscopy
The RCT39 reported 1.16 adenomas per colonoscopy in the Deep-GI group and 1.04 in the CAD EYE group, 0.64 proximal adenomas per colonoscopy in the Deep-GI group and 0.53 in the CAD EYE group, and 0.10 advanced adenomas per colonoscopy in the Deep-GI group and 0.12 in the CAD EYE group. The authors of the RCT39 did not perform statistical testing to assess whether the between-group differences in the mean number of abnormalities detected per colonoscopy were statistically significant.
Withdrawal Times
The RCT39 reported median withdrawal times, excluding the time spent on fecal debris irrigation and polypectomy, of 10 minutes (interquartile range, 7 to 12) for both the Deep-GI group and the CAD EYE group.
Adverse Events
The authors of the RCT39 reported that there were no procedural adverse events.
Cost-Effectiveness of AI-Assisted Colonoscopy Versus Conventional Colonoscopy
Evidence regarding the cost-effectiveness of AI-assisted colonoscopy was available from 5 economic evaluations summarized in an SR and 1 additional economic evaluation. The SR and primary economic evaluation were both conducted as part of the included HTA.35
The findings from 4 analyses, including 1 study that was conducted from the perspective of a health care system in Canada, suggest that AI-assisted colonoscopy is less costly and more effective than conventional colonoscopy (i.e., dominant). The 2 other economic evaluations indicate that AI-assisted colonoscopy is cost-effective versus conventional colonoscopy at their specified willingness-to-pay thresholds, which were £20,000 and ¥5 million per quality-adjusted life-year gained.
Cost-Effectiveness of Different AI-Assisted Colonoscopy Systems Versus Each Other
We found no relevant evidence regarding the cost-effectiveness of different AI-assisted colonoscopy systems versus each other for the detection of polyps, adenomas, precancerous lesions, and colorectal cancer; therefore, no summary can be provided.
Limitations
Evidence Gaps
Evidence comparing the clinical effectiveness of different AI-assisted colonoscopy systems was limited to 1 RCT.39 This RCT39 included 2 different AI-assisted colonoscopy treatment arms: 1 group received colonoscopy with the Deep-GI system, and the other with the CAD EYE system. However, the authors’ statistical analysis did not directly compare outcomes between these 2 groups; instead, each was individually compared to a control group that received conventional colonoscopy. As of November 2024, neither the Deep-GI system nor the CAD EYE system appear to be available for clinical use in Canada. Furthermore, we found no evidence comparing the cost-effectiveness of different AI-assisted colonoscopy systems for detecting polyps, adenomas, precancerous lesions, and colorectal cancer. Consequently, no conclusions can be drawn regarding the relative clinical or cost-effectiveness of different AI-assisted colonoscopy systems.
None of the included clinical studies reported long-term outcomes, such as colorectal cancer incidence and mortality; therefore, the impact of AI-assisted colonoscopy on these outcomes is unknown.
Risk of Bias of Included Studies in SRs
The evidence on the clinical effectiveness of AI-assisted colonoscopy compared to conventional colonoscopy summarized within this report is from 4 SRs35-38 that included data from a total of 54 unique primary clinical studies. Though we did not conduct our own critical appraisal of each primary study, the authors of the SRs35-38 noted that some studies had methodological limitations affecting the validity and reliability of their results. For example, many studies were at risk for performance bias because participants, endoscopists, and outcome assessors were aware of the treatment allocation. Some RCTs were also at risk for selection bias because of their methods for random sequence generation and allocation concealment. Pooled estimates from the meta-analyses in each of these SRs35-38 included data from all relevant studies, regardless of their risk of bias. These potential biases may influence the robustness of the findings.
Generalizability
The primary clinical studies included in the 4 SRs35-38 summarized in this report took place across a variety of locations, including China, France, Germany, Hong Kong, Israel, Italy, Japan, Latvia, Singapore, Spain, Sweden, Switzerland, Thailand, the UK, the US, and Vietnam. However, because none of these clinical studies were conducted in Canada, differences in colonoscopy practices or patient populations between these locations and Canada may limit the generalizability of this evidence to settings in Canada.
We used PROGRESS-Plus41,42 to guide data extraction and to provide insights into whether the clinical studies conducted to date included diverse patient populations who could be representative of those in Canada. However, the literature we reviewed for this report provided limited information on participant characteristics, often not reporting any participant demographics or clinical characteristics, or only reporting a few factors such as age or sex. In cases where participant sex or gender were reported, the authors did not provide any information on how they were defined or measured.
AI systems that are trained, validated, and tested using diverse datasets are more likely to be generalizable to new populations and settings, reducing the risk of issues like overfitting bias.43-46 Because of the limited information available on the patient populations used to test the performance of AI-assisted colonoscopy, we cannot comment on whether the study populations were representative of the clinical settings in which they are intended to be deployed. As such, it is uncertain if the effects of AI-assisted colonoscopy are generalizable, consistent, and robust across diverse patient populations.
Conclusions and Implications for Decision- or Policy-Making
This review includes 1 HTA (which included 1 SR with meta-analyses and 1 economic evaluation),35 3 SRs with meta-analyses,36-38 and 1 RCT39 regarding the clinical or cost-effectiveness of AI-assisted colonoscopy for detecting polyps, adenomas, precancerous lesions, or colorectal cancer. The evidence summarized in this report is drawn from SRs with substantial overlap in primary studies, meaning that data from the same participants were included in more than 1 SR (refer to Appendix 5 for a citation matrix illustrating the degree of primary study overlap). As a result, some evidence may be disproportionally represented in the overall conclusions.
Summary of Evidence
The evidence summarized in this report indicates that AI-assisted colonoscopy has the potential to improve clinical outcomes compared to conventional colonoscopy. For most outcomes, including detection rates, the number of abnormalities detected per colonoscopy, and miss rates, there were some mixed findings, with some estimates suggesting that AI-assisted colonoscopy led to significant improvements, while other studies suggest there is no evidence to indicate that 1 method is superior to the other. Variability in results may have been due to differences in patient populations, clinical settings, study designs, and the specific AI-assisted colonoscopy systems used. For example, the SR by Lee et al.,36 which included data from 23 RCTs, reported that AI-assisted colonoscopy was associated with statistically significant increases in the number of adenomas detected per colonoscopy. In contrast, the SR by Wei et al.,37 which only included data from nonrandomized real-world studies, found no statistically significant difference in adenomas detected per colonoscopy.
Among the 6 economic evaluations summarized, 4 reported that AI-assisted colonoscopy was less costly while generating more quality-adjusted life-years than conventional colonoscopy.35 The authors of the remaining 2 studies estimated that AI-assisted colonoscopy was more costly and generated more benefits than conventional colonoscopy and was likely to be cost-effective at willingness-to-pay thresholds of £20,000 and ¥5 million per quality-adjusted life-year gained.35
Evidence comparing the clinical and cost-effectiveness of different AI-assisted colonoscopy systems was limited. One included RCT39 allocated participants to receive AI-assisted colonoscopy using either the Deep-GI system or the CAD EYE system. However, the authors did not perform statistical testing to determine whether there were any significant differences between the groups. Additionally, we did not identify any relevant studies that evaluated the relative cost-effectiveness of different AI-assisted colonoscopy systems.
Considerations for Future Research
Numerous AI-assisted colonoscopy systems have been developed by different manufacturers, yet evidence from head-to-head trials remains limited. Future research that directly compares different AI-assisted colonoscopy systems could be informative for decision-makers who are looking to implement specific technologies.
The current evidence is highly focused on procedure-related outcomes, such as adenoma detection rates, the number of adenomas detected per colonoscopy, adenoma miss rates, and withdrawal times. Future studies that evaluate long-term outcomes, such as colorectal cancer incidence and mortality, could provide a more comprehensive understanding of the clinical effectiveness of AI-assisted colonoscopy and help reduce uncertainty in future economic evaluations.
In Canada, disparities in colorectal cancer incidence, mortality, and treatment outcomes exist among various demographic groups.18 To provide insights into how AI-assisted colonoscopy could mitigate or exacerbate these health inequities, future studies should collect and report equity-relevant population characteristics, such as place of residence, race, ethnicity, culture, language, occupation, gender, sex, religion, education, socioeconomic status, and social capital. This information would help determine whether equity-deserving groups were represented and whether study findings are likely to be generalizable to other settings.
The literature we reviewed as part of this report did not provide any information on the methods used to develop, train, and refine machine learning models that are used by various AI-enabled polyp detection systems.35-39 Transparent reporting of these aspects may improve the explainability and intelligibility of these systems; help to build trust and accountability; and empower patients, clinicians, and policy-makers to make informed decisions regarding their use.47,48
Implications for Clinical Practice and Policy-Making
The findings of this report suggest that AI-assisted colonoscopy may improve clinical outcomes and be cost-effective compared to conventional colonoscopy. However, there is some uncertainty as to whether these findings are generalizable to settings in Canada. AI-enabled medical devices often face significant challenges in achieving generalizability across new populations and clinical settings.49 Differences in observed treatment effects between controlled clinical trials and real-world clinical practice may arise because of many factors, including implementation and workflow challenges and mismatches between the patient data used to train and validate machine learning models and the target population.50,51 For example, clinicians in clinical trials may receive specialized training on how to use the intervention being studied, whereas clinicians in real-world settings may have limited training or support.52,53 Decision-makers who intend to implement AI-assisted colonoscopy systems as a part of routine clinical care should consider conducting ongoing monitoring to determine whether the system’s performance is meeting their expectations.
Our literature search identified an ongoing assessment54 of AI software to help detect and characterize colorectal polyps by the National Institute for Health and Care Excellence, which could offer additional insights for decision-makers. Although the project does not yet have an expected publication date, the final protocol55 and scope documents56 suggest that this assessment may address some of the evidence gaps highlighted in this report. For example, it plans to evaluate the impact of AI software on long-term outcomes (e.g., rates of colorectal cancer diagnosis and mortality) and provide information on other key considerations, including the impact of endoscopist skill and experience, workforce capacity, equality issues, and implementation challenges.
Potential implementers of AI-assisted colonoscopy systems may also wish to reflect on the interoperability of these systems with existing colonoscopy equipment and workflows. The included HTA35 noted that not all AI-assisted colonoscopy systems are compatible with all colonoscopes from all manufacturers.
The limitations of the included literature, such as the lack of evidence comparing different types of AI-assisted colonoscopy systems, the variable quality of primary studies included in identified SRs, uncertainties in the economic models, and concerns regarding the generalizability of findings to settings in Canada, should be considered when interpreting the conclusions of this report.
References
1.Canadian Cancer Society. Colorectal cancer statistics. 2024; https://cancer.ca/en/cancer-information/cancer-types/colorectal/statistics. Accessed 2024 Oct 24.
2.Canadian Cancer Statistics 2024. Canadian Cancer Statistics Advisory Committee in collaboration with the Canadian Cancer Society Statistics Canada and the Public Health Agency of Canada; 2024: https://cdn.cancer.ca/-/media/files/research/cancer-statistics/2024-statistics/2024-cmaj/2024_cancer-specific-stats.pdf?rev=-1&hash=AB4A55266C9E3E89F32D4B921451F446&_gl=1*1guf9i4*_gcl_au*NDA5OTUyMTExLjE3MjU1MzMzNTc. Accessed 2024 Nov 7.
3.Government of Ontario. Colon cancer testing and prevention. 2024; https://www.ontario.ca/page/colon-cancer-testing-and-prevention?gad_source=1&gclid=EAIaIQobChMIpLGN1vfdiAMV2TfUAR05GgfVEAMYAiAAEgLRYvD_BwE&gclsrc=aw.ds. Accessed 2024 Oct 23.
4.Canadian Cancer Society. Symptoms of colorectal cancer. 2024; https://cancer.ca/en/cancer-information/cancer-types/colorectal/signs-and-symptoms. Accessed 2024 Oct 23.
5.World Health Organization. Colorectal cancer. 2023; https://www.who.int/news-room/fact-sheets/detail/colorectal-cancer. Accessed 2024 Oct 23.
6.Menon G, Recio-Boiles A, Lotfollahzadeh S, Cagir B. Colon Cancer. StatPearls 2024: https://www.ncbi.nlm.nih.gov/books/NBK470380/#:~:text=Age%3A%20The%20median%20age%20of,a%20person's%20colon%20cancer%20risk. Accessed 2024 Nov 7.
7.Ellison F, Saint-Jacques N. Five-year cancer survival by stage at diagnosis in Canada. Ottawa (ON): Statistics Canada; 2023: https://www150.statcan.gc.ca/n1/pub/82-003-x/2023001/article/00001-eng.htm. Accessed 2024 Oct 24.
8.Duan B, Zhao Y, Bai J, et al. Colorectal Cancer: An Overview. In: Morgado-Diaz JA, ed. Gastrointestinal Cancers 2022.
9.Colorectal Screening in Canada: 2021/2022 Environmental Scan. Toronto (ON): Canadian Partnership Against Cancer; 2022: https://www.partnershipagainstcancer.ca/topics/colorectal-cancer-screening-in-canada-2021-2022/summary/. Accessed 2024 Oct 24.
10.Recommendations on screening for colorectal cancer in primary care. Can Med Assoc J. 2016;188(5):340-348. PubMed
11.Mohl JT, Ciemins EL, Miller-Wilson L-A, Gillen A, Luo R, Colangelo F. Rates of Follow-up Colonoscopy After a Positive Stool-Based Screening Test Result for Colorectal Cancer Among Health Care Organizations in the US, 2017-2020. JAMA Netw. 2023;6(1):e2251384-e2251384. PubMed
12.Health PEI. Colorectal Cancer Screening Program. 2024; https://www.princeedwardisland.ca/en/information/health-pei/colorectal-cancer-screening-program. Accessed 2024 Nov 6.
13.BC Cancer. Get Screened. 2024; http://www.bccancer.bc.ca/screening/colon/get-screened. Accessed 2024 Nov 6.
14.Stauffer CM, Pfeifer C. Colonoscopy. StatPearls 2023: https://www.ncbi.nlm.nih.gov/books/NBK559274/. Accessed 2024 Oct 24.
15.Kumar R, Lewis CR. Colon Cancer Screening. StatPearls 2024: https://www.ncbi.nlm.nih.gov/books/NBK559064/. Accessed 2024 Nov 7.
16.Lin JS, Perdue LA, Henrikson NB, Bean SI, Blasi PR. Screening for Colorectal Cancer: Updated Evidence Report and Systematic Review for the US Preventive Services Task Force. JAMA. 2021;325(19):1978-1998. PubMed
17.Canadian Cancer Society. Colonoscopy. 2024; https://cancer.ca/en/treatments/tests-and-procedures/colonoscopy. Accessed 2024 Oct 24.
18.Adefemi K, Knight JC, Zhu Y, Wang PP. Racial and sociodemographic distribution of colorectal cancer screening in Canada: A cross-sectional study. Can J Public Health. 2024;115(3):371-383. PubMed
19.PDQ Adult Treatment Editorial Board. Colon Cancer Treatment (PDQ®): Patient Version. PDQ Cancer Information Summaries. Bethesda (MD): National Cancer Institute; 2024: https://www.ncbi.nlm.nih.gov/books/NBK65880/. Accessed 2024 Nov 7.
20.Canadian Cancer Society. Treatments for colon cancer. 2024; https://cancer.ca/en/cancer-information/cancer-types/colorectal/treatment/colon-cancer. Accessed 2024 Oct 24.
21.Canadian Cancer Society. Treatments for rectal cancer. 2024; https://cancer.ca/en/cancer-information/cancer-types/colorectal/treatment/rectal-cancer. Accessed 2024 Oct 24.
22.Artificial Intelligence Medical Devices (AIMD) Working Group. Machine Learning-enabled Medical Devices: Key Terms and Definitions. 2022: https://www.imdrf.org/sites/default/files/2022-05/IMDRF%20AIMD%20WG%20Final%20Document%20N67.pdf. Accessed 2024 Oct 23.
23.Paul D, Sanap G, Shenoy S, Kalyane D, Kalia K, Tekade RK. Artificial intelligence in drug discovery and development. Drug Discov Today. 2021;26(1):80-93. PubMed
24.Alowais SA, Alghamdi SS, Alsuhebany N, et al. Revolutionizing healthcare: the role of artificial intelligence in clinical practice. BMC Med Educ. 2023;23(1):689. PubMed
25.Bajwa J, Munir U, Nori A, Williams B. Artificial intelligence in healthcare: transforming the practice of medicine. Future Healthc J. 2021;8(2):e188-e194. PubMed
26.Roshan A, Byrne MF. Artificial intelligence in colorectal cancer screening. Can Med Assoc J. 2022;194(43):E1481-E1484. PubMed
27.Medtronic Canada ULC. Medtronic receives Health Canada licence for GI Genius™ intelligent endoscopy module with artificial intelligence system for colonoscopy. 2021; https://canadanews.medtronic.com/2021-11-30-Medtronic-receives-Health-Canada-licence-for-GI-Genius-TM-intelligent-endoscopy-module-with-artificial-intelligence-system-for-colonoscopy. Accessed 2024 Nov 6.
28.Mazenes S. UHN using artificial intelligence to help prevent colon cancer. 2024; https://uhnfoundation.ca/stories/uhn-using-artificial-intelligence-to-help-prevent-colon-cancer/. Accessed 2024 Nov 6.
29.Collingwood G&M Hospital. [Advancements in CGMH's colon cancer screening program]. 2024; https://cgmh.on.ca/news-article/cgmh-drives-colorectal-cancer-screening-forward-with-cutting-edge-technology. Accessed 2024 Nov 6.
30.Ryan H. N.S. hospital will be first in Canada to screen for colon cancer with AI machine. CBC News 2022; https://www.cbc.ca/news/canada/nova-scotia/n-s-hospital-first-in-canada-to-screen-for-colon-cancer-with-ai-machine-1.6396618. Accessed 2024 Nov 6.
31.Hassan C, Repici A, Sharma P. Incorporating Artificial Intelligence Into Gastroenterology Practices. Clin Gastroenterol Hepatol. 2023;21(7):1687-1689. PubMed
32.Lou S, Du F, Song W, et al. Artificial intelligence for colorectal neoplasia detection during colonoscopy: a systematic review and meta-analysis of randomized clinical trials. EClinicalMedicine. 2023;66. PubMed
33.Lee J, Park SW, Kim YS, et al. Risk factors of missed colorectal lesions after colonoscopy. Medicine (Baltimore). 2017;96(27):e7468. PubMed
34.Cha JM. Colonoscopy Quality is the Answer for the Emerging Issue of Interval Cancer. Intest Res. 2014;12(2):110-116. PubMed
35.Artificial intelligence assisted endoscopy in the detection of lower gastrointestinal cancer and pre-cancerous lesions. Cardiff (UK): Health Technology Wales; 2024: https://healthtechnology.wales/wp-content/uploads/EAR055-AIAE-WEB.pdf. Accessed 2024 Oct 21.
36.Lee MCM, Parker CH, Liu LWC, Farahvash A, Jeyalingam T. Impact of study design on adenoma detection in the evaluation of artificial intelligence-aided colonoscopy: a systematic review and meta-analysis. Gastrointest Endosc. 2024;99(5):676-687.e616. PubMed
37.Wei MT, Fay S, Yung D, Ladabaum U, Kopylov U. Artificial Intelligence-Assisted Colonoscopy in Real-World Clinical Practice: A Systematic Review and Meta-Analysis. Clin Transl Gastroenterol. 2024;15(3):e00671. PubMed
38.Aslam MF, Bano S, Khalid M, et al. The effectiveness of real-time computer-aided and quality control systems in colorectal adenoma and polyp detection during colonoscopies: a meta-analysis. Ann Med Surg (Lond). 2023;85(2):80-91. PubMed
39.Tiankanon K, Aniwan S, Kerr SJ, et al. Improvement of adenoma detection rate by two computer-aided colonic polyp detection systems in high adenoma detectors: a randomized multicenter trial. Endoscopy. 2024;56(4):273-282. PubMed
40.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
41.O'Neill J, Tabish H, Welch V, et al. Applying an equity lens to interventions: using PROGRESS ensures consideration of socially stratifying factors to illuminate inequities in health. J Clin Epidemiol. 2014;67(1):56-64. PubMed
42.Oliver S, Kavanagh J, Caird J, et al. Health Promotion, Inequalities and Young People's health: a Systematic Review of Research. EPPI-Centre report no. 161. London (GB): University of London; 2008: https://eppi.ioe.ac.uk/cms/Portals/0/PDF%20reviews%20and%20summaries/Inequalities%20Young%20People%20R2008Oliver.pdf?ver=2010-12-22-123934-167. Accessed 2024 Oct 29.
43.Antonelli G, Badalamenti M, Hassan C, Repici A. Impact of artificial intelligence on colorectal polyp detection. Best Pract Res Clin Gastroenterol. 2021;52-53:101713. PubMed
44.Goetz L, Seedat N, Vandersluis R, van der Schaar M. Generalization-a key challenge for responsible AI in patient-facing clinical applications. NPJ Digit Med. 2024;7(1):126. PubMed
45.Kwong JCC, Khondker A, Lajkosz K, et al. APPRAISE-AI Tool for Quantitative Evaluation of AI Studies for Clinical Decision Support. JAMA Netw. 2023;6(9):e2335377-e2335377. PubMed
46.Nazer LH, Zatarah R, Waldrip S, et al. Bias in artificial intelligence algorithms and recommendations for mitigation. PLOS Digit Health. 2023;2(6):e0000278. PubMed
47.Amann J, Blasimme A, Vayena E, Frey D, Madai VI. Explainability for artificial intelligence in healthcare: a multidisciplinary perspective. BMC Med Inform Decis Mak. 2020;20(1):310. PubMed
48.Steerling E, Siira E, Nilsen P, Svedberg P, Nygren J. Implementing AI in healthcare-the relevance of trust: a scoping review. Front Health Serv. 2023;3:1211150. PubMed
49.Eche T, Schwartz LH, Mokrane FZ, Dercle L. Toward Generalizability in the Deployment of Artificial Intelligence in Radiology: Role of Computation Stress Testing to Overcome Underspecification. Radiol Artif Intell. 2021;3(6):e210097. PubMed
50.Plana D, Shung DL, Grimshaw AA, Saraf A, Sung JJY, Kann BH. Randomized Clinical Trials of Machine Learning Interventions in Health Care: A Systematic Review. JAMA Netw. 2022;5(9):e2233946-e2233946. PubMed
51.Huisman M, Hannink G. The AI Generalization Gap: One Size Does Not Fit All. Radiol Artif Intell. 2023;5(5):e230246. PubMed
52.Neugebauer EAM, Rath A, Antoine S-L, et al. Specific barriers to the conduct of randomised clinical trials on medical devices. Trials. 2017;18(1):427. PubMed
53.Govindarajulu US, Stillo M, Goldfarb D, Matheny ME, Resnic FS. Learning curve estimation in medical devices and procedures: hierarchical modeling. Stat Med. 2017;36(17):2764-2785. PubMed
54.National Institute for Health and Care Excellence. Artificial intelligence software to help detect and characterise colorectal polyps. 2024; https://www.nice.org.uk/guidance/indevelopment/gid-dg10118. Accessed 2024 Nov 7.
55.National Institute for Health and Care Excellence. Artificial intelligence software to help detect and characterise colorectal polyps [DAP78]. 2024; https://www.nice.org.uk/guidance/gid-dg10118/documents/final-protocol. Accessed 2024 Nov 7.
56.National Institute for Health and Care Excellence. Artificial intelligence software to help detect and characterise colorectal polyps: final scope. 2024; https://www.nice.org.uk/guidance/gid-dg10118/documents/final-scope. Accessed 2024 Nov 7.
57.Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. PubMed
58.Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377-384. PubMed
59.Higgins JPT, Green S, editors. Figure 15.5.a: Drummond checklist (Drummond 1996). Cochrane handbook for systematic reviews of interventions. London (GB): The Cochrane Collaboration; 2011: http://handbook-5-1.cochrane.org/chapter_15/figure_15_5_a_drummond_checklist_drummond_1996.htm. Accessed 2024 Oct 24.
60.CADTH Style Guide. 7th ed: https://www.cda-amc.ca/sites/default/files/pdf/cadth_style_guide_7th_edition_v1.3.pdf. Accessed 2024 Nov 7.
Appendix 1: Detailed Methods and Selection of Included Studies
Please note that this appendix has not been copy-edited.
Literature Search Methods
An information specialist conducted a literature search on key resources including MEDLINE, the Cochrane Database of Systematic Reviews, the International HTA Database, the websites of major international health technology agencies and health technology agencies in Canada, as well as a focused internet search. The search approach was customized to retrieve a limited set of results, balancing comprehensiveness with relevance. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. Search concepts were developed based on the elements of the research questions and selection criteria. The main search concepts were colonoscopy and artificial intelligence. Search filters were applied to limit retrieval to HTA, SRs, meta-analyses, or indirect treatment comparisons, any types of clinical trials or observational studies, or economic studies. The search was completed on October 9, 2024 and limited to English-language documents published since January 1, 2019.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Exclusion Criteria
Articles were excluded if they met any of the following criteria:
did not meet the selection criteria outlined in Table 1
were duplicate publications
were SRs in which all relevant studies were captured in other more recent or more comprehensive SRs
were primary studies captured in 1 or more included SRs
were studies on AI systems that evaluate the quality of bowel preparation before colonoscopy
were preclinical studies that assessed the performance of AI systems using still images or prerecorded colonoscopy videos (e.g., video-based benchmarking)
only reported on outcomes related to diagnostic accuracy (e.g., sensitivity, specificity).
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the following tools as a guide: A MeaSurement Tool to Assess systematic Reviews 2 (AMSTAR 2)57 for SRs, the Downs and Black checklist58 for RCTs, and the Drummond checklist59 for economic evaluations. Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Equity Considerations
We used PROGRESS-Plus,41,42 1 tool to describe equity-deserving groups, to guide data extraction and report writing. Each included publication was checked to determine if relevant PROGRESS-Plus criteria were reported by study authors to describe the participants. When available, detailed participant characteristics were then extracted and reported in tables in Appendix 2. The main PROGRESS-Plus criteria include place of residence, race, ethnicity, culture, language, occupation, gender, sex, religion, education, socioeconomic status, social capital, personal characteristics associated with discrimination (e.g., age, disability), features of relationships, and time-dependent relationships.41,42
When reporting on sex or gender in this rapid review, we retained the language used by the original study authors and whenever possible we referred to these groups based on guidance from the CDA-AMC style guide60 at the time this rapid review was conducted, with an understanding that language is constantly evolving.
Appendix 2: Characteristics of Included Publications
Please note that this appendix has not been copy-edited.
Table 2: Characteristics of Included HTA and SRs
Study citation, country, funding | Study designs and numbers of primary studies included | Population characteristics | Intervention and comparator(s) | Relevant outcomes |
|---|---|---|---|---|
HTAs | ||||
Health Technology Wales (2024)35 Wales Funding: Health Technology Wales is funded by the Welsh government. | Study design: An SR of clinical and economic evidence published between January 2010 and March 2024. The HTA also included a de novo cost-utility analysis, which is described in Appendix 2, Table 4 Number of included studies: Four SRs with meta-analyses (which included 32 unique English-language RCTs), 7 additional RCTs, and 6 economic studies (5 relevant to the current review) were included | People who were referred for identification of precancerous lesions, polyps, adenomas, or lower gastrointestinal cancer Age: The mean age of participants from included primary studies within the SRs and the included RCTs ranged from 41.3 years to 67.0 years (when reported) Sex: The proportion of female participants from included primary studies ranged from 23.2% to 68.0%; the proportion of male participants from included primary studies ranged from 32.0% to 76.8% (when reported); other sexes or genders were NR Other PROGRESS-Plus criteria: NRa | Intervention: AI-assisted endoscopy with video images reviewed in real-time, used as an adjunct to standard care. Comparator: Endoscopy with video images reviewed in real-time, without AI assistance (i.e., standard care) |
|
SRs | ||||
Lee et al. (2024)36 Canada Funding: NR | Study design: SR and meta-analysis of RCTs published up to March 2023 Number of included studies: 26 RCTs | Patients who underwent colonoscopy for screening, surveillance, or diagnostic purposes Age: The mean age of participants from included primary studies ranged from 46.0 years to 66.3 years (when reported) Sex: The proportion of female participants from included primary studies ranged from 23.5% to 57.0% (when reported); other sexes or genders were NR Other PROGRESS-Plus criteria: NRa | Intervention: Colonoscopy performed with an AI-aided polyp detection system Comparator: Routine high-definition white-light colonoscopy, without AI assistance |
|
Wei et al. (2024)37 US Funding: No funding | Study design: SR and meta-analysis of nonrandomized studies published between January 1, 2020, and April 1, 2023 Number of included studies: 12 nonrandomized studies | Adults who underwent a colonoscopy for detecting colorectal cancer Age: NR Sex: NR Other PROGRESS-Plus criteria: NRa | Intervention: Colonoscopy performed with AI-augmented real-time detection systems Comparator: Conventional colonoscopy (i.e., without AI assistance) |
|
Aslam et al. (2023)38 Pakistan Funding: No funding | Study design: SR and meta-analysis of RCTs published up to April 21, 2022 Number of included studies: 11 RCTs | Patients who underwent colonoscopy to detect adenomas or polyps Age: NR Sex: NR Other PROGRESS-Plus criteria: NRa | Intervention: Colonoscopy performed with AI-assisted detection systems Comparator: Conventional colonoscopy (i.e., without AI assistance) |
|
AI = artificial intelligence; HTA = health technology assessment; ICER = incremental cost-effectiveness ratio; NR = not reported; QALY = quality-adjusted life-year; RCT = randomized controlled trial; SR = systematic review.
aThe main PROGRESS-Plus criteria include place of residence, race, ethnicity, culture, language, occupation, gender, sex, religion, education, socioeconomic status, and social capital, personal characteristics associated with discrimination (e.g., age, disability), features of relationships, and time-dependent relationships.41,42
Table 3: Characteristics of Included RCT
Study citation, country, funding | Study design and setting | Population characteristics | Intervention and comparator(s) | Relevant clinical outcomes |
|---|---|---|---|---|
Tiankanon et al. (2024)39 Thailand Funding: Chulalongkorn University, the National Research Council of Thailand, and King Chulalongkorn Memorial Hospital | Multicentre, parallel-group, 3-arm RCT conducted between February 2022 and May 2023 at 5 endoscopy referral centres in Thailand. Data from 2 of the 3 treatment arms, specifically the Deep-GI and CAD EYE arms, were relevant to the current report | Inclusion criteria: Asymptomatic participants, between the ages of 50 and 75 years, who underwent routine screening colonoscopy or were screened after a positive fecal immunochemical test Excluded: Those with a personal history of colorectal cancer, inflammatory bowel diseases, familial polyposis syndrome, or prior colonic resection Number of participants: 400 in the Deep-GI group; 400 in the CAD EYE group Age, mean (SD): 62.7 (7.7) years in the Deep-GI group; 63.2 (6.5) years in the CAD EYE group Sex: 45.3% male in the Deep-GI group; 35.8% male in the CAD EYE group; other sexes or genders were NR BMI, mean (SD): 23.8 (4.3) kg/m2 in the Deep-GI group; 23.6 (3.8) kg/m2 in the CAD EYE group Family history of colorectal cancer: 8.0% in the Deep-GI group; 7.5% in the CAD EYE group Smoking status: 11.0% in the Deep-GI group; 9.3% in the CAD EYE group Other PROGRESS-Plus criteria: NRa | Intervention: AI-assisted colonoscopy performed with either the Deep-GI system or the CAD EYE system Comparator: Conventional white-light colonoscopy Only data for the Deep-GI group and the CAD EYE group were considered relevant for addressing research question 2. Data comparing either intervention group with the control group are summarized in an included SR35 |
|
AI = artificial intelligence; BMI = body mass index; NR = not reported; RCT = randomized controlled trial; SD = standard deviation; SR = systematic review.
aThe main PROGRESS-Plus criteria include place of residence, race, ethnicity, culture, language, occupation, gender, sex, religion, education, socioeconomic status, and social capital, personal characteristics associated with discrimination (e.g., age, disability), features of relationships, and time-dependent relationships.41,42
Table 4: Characteristics of Included Economic Evaluation
Study citation country, funding | Type of analysis, time horizon, perspective | Population characteristics | Intervention and comparator | Approach | Source of clinical, cost, and utility data used in analysis | Main assumptions |
|---|---|---|---|---|---|---|
Health Technology Wales (2024)35 Wales Funding: Health Technology Wales is funded by the Welsh government. | Analysis: Cost-utility analysis conducted as part of an HTA Time horizon: A lifetime horizon Perspective: UK NHS and Personal Social Services | The modelled cohort characteristics reflected study populations from the 39 RCTs included in the SR of clinical evidence conducted as part of the HTA Age, mean (SE): 57.4 (5.8) years Sex: 49% female; other sexes or genders were NR Other PROGRESS-Plus criteria: NRa | Intervention: Colonoscopy performed with AI assistance Comparator: Conventional colonoscopy (i.e., without AI assistance) | A decision tree model that captured the short-term outcomes of each colonoscopy screening strategy | Clinical model inputs were drawn from meta-analyses conducted as part of the HTA and various sources of published literature. Cost inputs were sourced from NHS Supply Chain, 2021/22 NHS reference costs, manufacturers, and various sources of published literature and unpublished data. QALY estimates and model-state transition probabilities were sourced from assumptions, unpublished data, or a previous NICE assessment of fecal immunochemical testing to guide colorectal cancer pathway referral in primary care |
|
AI = artificial intelligence; HTA = health technology assessment; NHS = UK National Health Service; NICE = National Institute for Health and Care Excellence; NR = not reported; QALY = quality-adjusted life-year; RCT = randomized controlled trial; SE = standard error; SR = systematic review.
aThe main PROGRESS-Plus criteria include place of residence, race, ethnicity, culture, language, occupation, gender, sex, religion, education, socioeconomic status, and social capital, personal characteristics associated with discrimination (e.g., age, disability), features of relationships, and time-dependent relationships.41,42
Table 5: Characteristics of Economic Evaluations Included in the SR by Health Technology Wales (2024)35
Study citation country, funding | Type of analysis, time horizon, perspective | Population characteristics | Intervention and comparator | Approach | Source of clinical, cost, and utility data used in analysis | Main assumptions |
|---|---|---|---|---|---|---|
Barkun et al. (2023) as reported in Health Technology Wales (2024)35 Canada Funding: The intervention manufacturer. | Analysis: Cost-utility analysis Time horizon: A lifetime horizon Perspective: Health care system | People undergoing colonoscopy following a positive FIT result, aged 50 years or older Age: 50 years Sex: 54.5% male; other sexes or genders were NR Other PROGRESS-Plus criteria: NRa | Intervention: Colonoscopy performed with AI assistance (using GI Genius) Comparator: Conventional colonoscopy (i.e., without AI assistance) | A Markov model captured the incidence of small adenomas and progression through medium and large adenoma to colorectal cancer | Disease prevalence data were retrieved from an Ontario screening program and were adjusted using adenoma miss rates from a meta-analysis. Transition probabilities were sourced from previous modelling studies. Cost data were retrieved from the manufacturer, Canadian schedules, and the literature. Utility data were sourced from a previous cost-utility study or from the literature | NR |
Hassan et al. (2023a) as reported in Health Technology Wales (2024)35 Italy Funding: The intervention manufacturer | Analysis: Cost-utility analysis Time horizon: A lifetime horizon Perspective: Health care system | People undergoing colonoscopy following a positive FIT result Age: 50 years Sex: NR Other PROGRESS-Plus criteria: NRa | Intervention: Colonoscopy performed with AI assistance (using GI Genius) Comparator: Conventional colonoscopy (i.e., without AI assistance) | A Markov model captured the incidence of small adenomas and progression through medium and large adenoma to colorectal cancer | Disease prevalence data were retrieved from an Italian screening program and were adjusted using adenoma miss rates from a meta-analysis. Transition probabilities were sourced from previous modelling studies. Cost data came from Italian national tariffs and the literature | NR |
Sekiguchi et al. (2023) as reported in Health Technology Wales (2024)35 Japan Funding: NR | Analysis: Cost-utility analysis Time horizon: A lifetime horizon Perspective: Health care payer | People at average risk of colorectal cancer between the ages of 40 to 74 years Age: NR Sex: NR Other PROGRESS-Plus criteria: NRa | Intervention: Colonoscopy performed with AI assistance after positive FIT Comparator: Conventional colonoscopy (i.e., without AI assistance) after positive FIT | A Markov model captured the incidence of adenomas and progression to advanced adenomas and colorectal cancer | Population characteristics, disease incidence data, and utilization of FIT screening and colonoscopy came from Japanese data. Diagnostic accuracy of AI-assisted colonoscopy came from previous Japanese cost-effectiveness studies. Cost data were from Japanese national reimbursement tables. The source of quality of life data was NR | NR |
Thiruvengadam et al. (2023) as reported in Health Technology Wales (2024)35 US Funding: NR | Analysis: Cost-utility analysis Time horizon: A lifetime horizon (to age 100 years) Perspective: Health care payer | People aged 45 to 75 years undergoing screening colonoscopy Age: 45 years Sex: NR Other PROGRESS-Plus criteria: NRa | Intervention: Colonoscopy performed with AI assistance Comparator: Conventional colonoscopy (i.e., without AI assistance) | A semi-Markov microsimulation captured the natural history incidence of adenomas and colorectal cancer, with progression from low-risk to high-risk adenomas, and local to metastatic colorectal cancer | Clinical inputs were derived from multiple literature sources. The natural history model was based on cohort data from the US, Australia, and Germany. Effectiveness inputs were sourced from the literature. Cost data were obtained from analyses of Medicare, Medicaid, and commercial insurer payment data. Utility data for local, regional, and metastatic colorectal cancer were from the literature | NR |
Areia et al. (2022) as reported in Health Technology Wales (2024)35 US Funding: NR | Analysis: Cost-effectiveness and cost-utility analysis Time horizon: A lifetime horizon (to age 100 years) Perspective: Societal | Screening-eligible populations at average risk for colorectal cancer Age: 50 years (primary analysis) Sex: NR Other PROGRESS-Plus criteria: NRa | Intervention: Colonoscopy performed with AI assistance Comparator: Conventional colonoscopy (i.e., without AI assistance) | A Markov microsimulation captured the natural incidence of adenomas and progression from low-risk to high-risk adenomas, stage I to stage IV colorectal cancer, and death | Population characteristics were retrieved from 2008 US Census data. Data on the prevalence of polyps, incidence of colorectal cancer, and survival were derived primarily from studies in the US. Transition probabilities were sourced from the literature. The natural history model was calibrated to historical US data collected before the widespread adoption of colorectal cancer screening programs. Cost inputs were sourced from US manufacturer prices and from analyses of Medicare, Medicaid, and commercial insurer payment data | NR |
AI = artificial intelligence; FIT = fecal immunochemical test; HTA = health technology assessment; NR = not reported; QALY = quality-adjusted life-year; SE = standard error; SR = systematic review.
aThe main PROGRESS-Plus criteria include place of residence, race, ethnicity, culture, language, occupation, gender, sex, religion, education, socioeconomic status, and social capital, personal characteristics associated with discrimination (e.g., age, disability), features of relationships, and time-dependent relationships.41,42
Appendix 3: Critical Appraisal of Included Publications
Please note that this appendix has not been copy-edited.
Table 6: Strengths and Limitations of SRs Using AMSTAR 257
Strengths | Limitations |
|---|---|
Health Technology Wales (2024)35 | |
|
|
Lee et al. (2024)36 | |
|
|
Wei et al. (2024)37 | |
|
|
Aslam et al. (2023)38 | |
|
|
AMSTAR 2 = A MeaSurement Tool to Assess systematic Reviews 2; INAHTA = International Network of Agencies for Health Technology Assessment; PROSPERO = International Prospective Register of Systematic Reviews; RCT = randomized controlled trial; RoB = Risk of Bias; SR = systematic review.
Table 7: Strengths and Limitations of the RCT Using the Downs and Black Checklist58
Strengths | Limitations |
|---|---|
Tiankanon et al. (2024)39 | |
Reporting
External validity
Internal validity – bias
Internal validity – confounding
Power
Other
| External validity
Internal validity – bias
Other
|
BMI = body mass index; CI = confidence interval; RCT = randomized controlled trial.
Table 8: Strengths and Limitations of Economic Evaluation Using the Drummond Checklist59
Strengths | Limitations |
|---|---|
Health Technology Wales (2024)35 | |
Study design
Data collection
Analysis and interpretation of results
Other
| Data collection
Other
|
HTW = Health Technology Wales; QALY = quality-adjusted life-year; SR = systematic review.
Appendix 4: Main Study Findings
Please note that this appendix has not been copy-edited.
Table 9: Summary of Findings by Outcome — Adenoma Detection Ratea
Citation | Evidence source, number of participants | Outcome result | Relative effect (95% CI) | P value | |
|---|---|---|---|---|---|
Intervention group | Control group | ||||
AI-assisted colonoscopy vs. conventional colonoscopy | |||||
Health Technology Wales (2024)35 | SR with MA (36 RCTs); 27,870 participants | 44.3% | 37.1% | RR = 1.23 (1.16 to 1.29) | < 0.001 |
Lee et al. (2024)36 | SR with MA (24 RCTs); 17,413 participants | 39.3% | 33.1% | RR = 1.24 (1.17 to 1.31) | < 0.001 |
Wei et al. (2024)37 | SR with MA (12 NRSs); 11,655 participants | 36.3% | 35.8% | RR = 1.13 (1.01 to 1.28) | 0.04 |
Aslam et al. (2023)38 | SR with MA (11 RCTs); 6,856 participants | 41.7% | 35.3% | OR = 1.51 (1.15 to 1.99) | 0.003 |
Deep-GI vs. CAD EYE | |||||
Tiankanon et al. (2024)39 | RCT; 800 participants | 54.8% | 50.0% | NR | NR |
AI = artificial intelligence; CI = confidence interval; MA = meta-analysis; NR = not reported; NRS = nonrandomized study; OR = odds ratio; RCT = randomized controlled trial; RR = risk ratio; SR = systematic review; vs. = versus.
Note: There was overlap in the primary studies that were included in the SRs; the pooled estimates from separate reviews presented in this table thus contain some of the same data. Refer to Appendix 5 for a citation matrix illustrating the degree of overlap.
aDefined as the percentage of patients who underwent colonoscopy and had 1 or more adenomas detected.
Table 10: Summary of Findings by Outcome — Proximal Adenoma Detection Ratea
Citation | Evidence source (for SRs), number of participants | Outcome result | Relative effect (95% CI) | P value | |
|---|---|---|---|---|---|
Intervention group | Control group | ||||
Deep-GI vs. CAD EYE | |||||
Tiankanon et al. (2024)39 | RCT; 800 participants | 38.8% | 32.3% | NR | NR |
CI = confidence interval; NR = not reported; RCT = randomized controlled trial; SR = systematic review; vs. = versus.
aDefined as the percentage of patients who underwent colonoscopy and had 1 or more proximal adenomas detected.
Table 11: Summary of Findings by Outcome — Advanced Adenoma Detection Ratea
Citation | Evidence source, number of participants | Outcome result | Relative effect (95% CI) | P value | |
|---|---|---|---|---|---|
Intervention group | Control group | ||||
AI-assisted colonoscopy vs. conventional colonoscopy | |||||
Health Technology Wales (2024)35 | SR with MA (16 RCTs); 15,639 participants | 13.3% | 12.2% | RR = 1.06 (0.98 to 1.15) | 0.134 |
Lee et al. (2024)36 | SR with MA (9 RCTs); 6,906 participants | 9.0% | 8.1% | RR = 1.12 (0.96 to 1.30) | 0.16 |
Deep-GI vs. CAD EYE | |||||
Tiankanon et al. (2024)39 | RCT; 800 participants | 9.5% | 10.3% | NR | NR |
AI = artificial intelligence; CI = confidence interval; MA = meta-analysis; NR = not reported; RCT = randomized controlled trial; RR = risk ratio; SR = systematic review; vs. = versus.
Note: There was overlap in the primary studies that were included in the SRs; the pooled estimates from separate reviews presented in this table thus contain some of the same data. Refer to Appendix 5 for a citation matrix illustrating the degree of overlap.
aDefined as the percentage of patients who underwent colonoscopy and had 1 or more advanced adenomas detected.
Table 12: Summary of Findings by Outcome — Polyp Detection Ratea
Citation | Evidence source, number of participants | Outcome result | Relative effect (95% CI) | P value | |
|---|---|---|---|---|---|
Intervention group | Control group | ||||
AI-assisted colonoscopy vs. conventional colonoscopy | |||||
Health Technology Wales (2024)35 | SR with MA (30 RCTs); 24,073 participants | 55.5% | 47.7% | RR = 1.20 (1.14 to 1.27) | < 0.001 |
Aslam et al. (2023)38 | SR with MA (10 RCTs); 6,685 participants | 55.0% | 41.8% | OR = 1.89 (1.66 to 2.15) | < 0.00001 |
AI = artificial intelligence; CI = confidence interval; MA = meta-analysis; OR = odds ratio; RCT = randomized controlled trial; RR = risk ratio; SR = systematic review; vs. = versus.
Note: There was overlap in the primary studies that were included in the SRs; the pooled estimates from separate reviews presented in this table thus contain some of the same data. Refer to Appendix 5 for a citation matrix illustrating the degree of overlap.
aDefined as the percentage of patients who underwent colonoscopy and had 1 or more polyps detected.
Table 13: Summary of Findings by Outcome — Sessile Serrated Lesion Detection Ratea
Citation | Evidence source, number of participants | Outcome result | Relative effect (95% CI) | P value | |
|---|---|---|---|---|---|
Intervention group | Control group | ||||
AI-assisted colonoscopy vs. conventional colonoscopy | |||||
Health Technology Wales (2024)35 | SR with MA (19 RCTs); 18,050 participants | 11.1% | 9.1% | RR = 1.21 (1.06 to 1.38) | 0.006 |
Lee et al. (2024)36 | SR with MA (12 RCTs); 10,045 participants | 5.5% | 5.7% | RR = 0.95 (0.81 to 1.11) | 0.51 |
Deep-GI vs. CAD EYE | |||||
Tiankanon et al. (2024)39 | RCT; 800 participants | 3.0% | 2.3% | NR | NR |
AI = artificial intelligence; CI = confidence interval; MA = meta-analysis; NR = not reported; RCT = randomized controlled trial; RR = risk ratio; SR = systematic review; vs. = versus.
Note: There was overlap in the primary studies that were included in the SRs; the pooled estimates from separate reviews presented in this table thus contain some of the same data. Refer to Appendix 5 for a citation matrix illustrating the degree of overlap.
aDefined as the percentage of patients who underwent colonoscopy and had 1 or more sessile serrated lesions detected.
Table 14: Summary of Findings by Outcome — Carcinoma Detection Ratea
Citation | Evidence source, number of participants | Outcome result | Relative effect (95% CI) | P value | |
|---|---|---|---|---|---|
Intervention group | Control group | ||||
AI-assisted colonoscopy vs. conventional colonoscopy | |||||
Health Technology Wales (2024)35 | 1 RCT; Engelke et al. (2023); 232 participants | 2.5% | 0.9% | RR = 2.70 (0.29 to 25.62) | > 0.05 |
1 RCT; Wang et al. (2023); 1,261 participants | 0% | 0% | NR | NR | |
1 RCT; Yamaguchi et al. (2024); 321 participants | 0.9% | 2.5% | RR = 0.35 (0.04 to 3.30) | 0.638 | |
1 RCT; Hüneburg et al. (2023); 96 participants | 4.0% | 0% | RR = 0.35 (0.04 to 3.30) | 0.52 | |
1 RCT; Wang et al. (2019); 1,058 participants | 0% | 0% | NR | NR | |
1 RCT; Repici et al. (2020); 685 participants | 2.9% | 0.9% | RR = 3.36 (0.93 to 12.11) | 0.067 | |
1 RCT; Wang et al. (2020b); 962 participants | 0% | 0% | NR | NR | |
1 RCT; Repici et al. (2022); 660 participants | 0% | 0.9% | NR | 0.247 | |
1 RCT; Liu et al. (2020a); 790 participants | 0% | 0% | NR | NR | |
1 RCT; Gimeno-García et al. (2023); 312 participants | 1.9% | 2.5% | RR = 0.76 (0.06 to 1.22) | 0.99 | |
1 RCT; Xu et al. (2023); 2,527 participants | 0.2% | 0.6% | RR = 0.26 (0.06 to 1.22) | 0.109 | |
1 RCT; Nakashima et al. (2023); 415 participants | 0.5% | 0% | NR | NR | |
1 RCT; Mangas-Sanjuan et al. (2023); 3,213 participants | 3.7% | 3.2% | RR = 1.15 (0.80 to 1.66) | 0.46 | |
AI = artificial intelligence; CI = confidence interval; MA = meta-analysis; NR = not reported; RCT = randomized controlled trial; RR = risk ratio; SR = systematic review; vs. = versus.
aDefined as the percentage of patients who underwent colonoscopy and had 1 or more carcinomas detected.
Table 15: Summary of Findings by Outcome — Adenomas Per Colonoscopy
Citation | Evidence source, number of participants | Outcome result | Relative effect (95% CI) | P value | |
|---|---|---|---|---|---|
Intervention group | Control group | ||||
AI-assisted colonoscopy vs. conventional colonoscopy | |||||
Lee et al. (2024)36 | SR with MA (23 RCTs); 17,013 participants | NR | NR | MD = 0.19 (0.15 to 0.24); favours AI group | < 0.001 |
Wei et al. (2024)37 | SR with MA (6 NRSs); NR | NR | NR | RR = 1.12 (0.95 to 1.33) | 0.18 |
Deep-GI vs. CAD EYE | |||||
Tiankanon et al. (2024)39 | RCT; 800 participants | 1.16 (SD = 1.63) | 1.04 (SD = 1.51) | NR | NR |
AI = artificial intelligence; CI = confidence interval; MA = meta-analysis; MD = mean difference; NR = not reported; NRS = nonrandomized study; RCT = randomized controlled trial; RR = rate ratio; SD = standard deviation; SR = systematic review; vs. = versus.
Table 16: Summary of Findings by Outcome — Proximal Adenomas Per Colonoscopy
Citation | Evidence source, number of participants | Outcome result | Relative effect (95% CI) | P value | |
|---|---|---|---|---|---|
Intervention group | Control group | ||||
Deep-GI vs. CAD EYE | |||||
Tiankanon et al. (2024)39 | RCT; 800 participants | 0.64 (SD = 1.06) | 0.53 (SD = 1.03) | NR | NR |
CI = confidence interval; NR = not reported; RCT = randomized controlled trial; vs. = versus.
Table 17: Summary of Findings by Outcome — Advanced Adenomas Per Colonoscopy
Citation | Evidence source, number of participants | Outcome result | Relative effect (95% CI) | P value | |
|---|---|---|---|---|---|
Intervention group | Control group | ||||
AI-assisted colonoscopy vs. conventional colonoscopy | |||||
Lee et al. (2024)36 | SR with MA (13 RCTs); 9,217 participants | NR | NR | MD = 0.00 (−0.01 to 0.01) | 0.63 |
Deep-GI vs. CAD EYE | |||||
Tiankanon et al. (2024)39 | RCT; 800 participants | 0.10 (SD = 0.34) | 0.12 (SD = 0.36) | NR | NR |
AI = artificial intelligence; CI = confidence interval; MA = meta-analysis; MD = mean difference; NR = not reported; RCT = randomized controlled trial; SD = standard deviation; SR = systematic review; vs. = versus.
Table 18: Summary of Findings by Outcome — Sessile Serrated Lesions Per Colonoscopy
Citation | Evidence source, number of participants | Outcome result | Relative effect (95% CI) | P value | |
|---|---|---|---|---|---|
Intervention group | Control group | ||||
AI-assisted colonoscopy vs. conventional colonoscopy | |||||
Lee et al. (2024)36 | SR with MA (16 RCTs); 11,740 participants | NR | NR | MD = 0.01 (−0.01 to 0.03) | 0.19 |
AI = artificial intelligence; CI = confidence interval; MA = meta-analysis; MD = mean difference; NR = not reported; RCT = randomized controlled trial; SR = systematic review; vs. = versus.
Table 19: Summary of Findings by Outcome — Adenoma Miss Ratea
Citation | Evidence source, number of participants | Outcome result | Relative effect (95% CI) | P value | |
|---|---|---|---|---|---|
Intervention group | Control group | ||||
AI-assisted colonoscopy vs. conventional colonoscopy | |||||
Health Technology Wales (2024)35 | SR with MA (6 RCTs); 2,012 participants | 15.3% | 34.1% | RR = 0.46 (0.36 to 0.58) | 0.004 |
Lee et al. (2024)36 | SR with MA (24 RCTs); NR | 15.1% | 34.8% | RR = 0.44 (0.35 to 0.56) | < 0.00001 |
AI = artificial intelligence; CI = confidence interval; MA = meta-analysis; NR = not reported; RCT = randomized controlled trial; RR = risk ratio; SR = systematic review; vs. = versus.
Note: There was overlap in the primary studies that were included in the SRs; the pooled estimates from separate reviews presented in this table thus contain some of the same data. Refer to Appendix 5 for a citation matrix illustrating the degree of overlap.
aAdenoma miss rates are obtained from tandem colonoscopy studies (i.e., in which patients undergo 2 consecutive colonoscopies). They are defined as the number of additional adenomas detected during the second colonoscopy divided by the total number of adenomas detected during both colonoscopies.
Table 20: Summary of Findings by Outcome — Advanced Adenoma Miss Ratea
Citation | Evidence source, number of participants | Outcome result | Relative effect (95% CI) | P value | |
|---|---|---|---|---|---|
Intervention group | Control group | ||||
AI-assisted colonoscopy vs. conventional colonoscopy | |||||
Health Technology Wales (2024)35 | SR with MA (3 RCTs); 938 participants | 12% | 40% | OR = 1.07 (0.17 to 6.70) | 0.45 |
AI = artificial intelligence; CI = confidence interval; MA = meta-analysis; OR = odds ratio; RCT = randomized controlled trial; SR = systematic review; vs. = versus.
aAdvanced adenoma miss rates are obtained from tandem colonoscopy studies (i.e., in which patients undergo 2 consecutive colonoscopies). They are defined as the number of additional advanced adenomas detected during the second colonoscopy divided by the total number of advanced adenomas detected during both colonoscopies.
Table 21: Summary of Findings by Outcome — Sessile Serrated Lesion Miss Ratea
Citation | Evidence source, number of participants | Outcome result | Relative effect (95% CI) | P value | |
|---|---|---|---|---|---|
Intervention group | Control group | ||||
AI-assisted colonoscopy vs. conventional colonoscopy | |||||
Health Technology Wales (2024)35 | SR with MA (4 RCTs); 1,168 participants | 9% | 16% | OR = 0.22 (0.08 to 0.65) | 0.01 |
AI = artificial intelligence; CI = confidence interval; MA = meta-analysis; NR = not reported; OR = odds ratio; RCT = randomized controlled trial; SR = systematic review; vs. = versus.
aSessile serrated lesion miss rates are obtained from tandem colonoscopy studies (i.e., in which patients undergo 2 consecutive colonoscopies). They are defined as the number of additional sessile serrated lesions detected during the second colonoscopy divided by the total number of sessile serrated lesions detected during both colonoscopies.
Table 22: Summary of Findings by Outcome — Withdrawal Times
Citation | Outcome | Evidence source, number of participants | Outcome result | Relative effect (95% CI) | P value | |
|---|---|---|---|---|---|---|
Intervention group | Control group | |||||
AI-assisted colonoscopy vs. conventional colonoscopy | ||||||
Health Technology Wales (2024)35 | Withdrawal time excluding biopsy, minutes (mean [SD] or median [IQR]) | SR with MA (18 RCTs); Lou et al. (2023); 13,740 participants | NR | NR | MD = 0.33 (0.09 to 0.57); longer in AI group | 0.012 |
1 RCT; Desai et al. (2024); 1,112 participants | 11.3 (SD = 4.6) | 10.8 (SD = 4.8) | NR | 0.11 | ||
1 RCT; Lau et al. (2024); 766 participants | 14.9 (SD = 8.1) | 13.7 (SD = 8.7) | NR | 0.048 | ||
1 RCT; Lui et al. (2024); 452 participants | 7.5 (SD = 1.7) | 7.5 (SD = 1.9) | NR | NR | ||
1 RCT; Maas et al. (2024); 916 participants | 6.5 (IQR = 4.0) | 6.5 (IQR = 4.1) | NR | 0.86 | ||
1 RCT; Mangas-Sanjuan et al. (2023); 3,213 participants | 10.6 (SD = 5.3) | 9.8 (SD = 4.3) | NR | NR | ||
1 RCT; Repici et al. (2022); 660 participants | 8.2 (SD = 1.6) | 8.0 (SD = 0.2) | NR | 0.176 | ||
1 RCT; Rondonotti et al. (2022); 800 participants | 9.0 (IQR, 8.0 to 11.0) | 9.0 (IQR, 7.6 to 10.0) | NR | 0.40 | ||
1 RCT; Schöler et al. (2024); 240 participants | 13.9 (SD = 7.3) | 12.3 (SD = 9.4) | NR | 0.98 | ||
1 RCT; Tiankanon et al. (2024); 1,200 participants | AI Group 1: 10.0 (IQR, 7.0 to 12.0) AI Group 2: 10.0 (IQR, 7.0 to 12.0) | 9.0 (IQR, 7.0 to 11.0) | NR; longer in both AI groups | NR | ||
1 RCT; Yao et al. (2023); 456 participants | 7.4 (SD = 3.4) | 7.3 (SD = 2.9) | NR | NR | ||
Withdrawal time including biopsy, minutes (mean [SD] or median [IQR]) | SR with MA (4 RCTs); Huang et al. (2022); 3,836 participants | NR | NR | MD = 0.35 (0.15 to 0.55); longer in AI group | 0.02 | |
1 RCT; Glissen Brown et al. (2022); 223 participants | 9.5 (IQR, 7.8 to 13.8) | 8.5 (IQR, 7.0 to 11.0) | NR | 0.01 | ||
1 RCT; Karsenti et al. (2023); 2,015 participants | 8.0 (IQR, 6.0 to 10.8) | 7.3 (IQR, 6.0 to 9.7) | NR | 0.0013 | ||
1 RCT; Schöler et al. (2024); 240 participants | 21.4 (SD = 13.5) | 17.4 (SD = 13.1) | NR | 0.03 | ||
1 RCT; Mangas-Sanjuan et al. (2023); 3,213 participants | 16.9 (SD = 10.3) | 15.7 (SD = 9.4) | NR | < 0.05 | ||
Lee et al. (2024)36 | Withdrawal time, minutes (mean [SD])a | SR with MA (18 RCTs); 14,783 participants | NR | NR | MD = 0.34 (0.11 to 0.56); longer in AI group | 0.004 |
Aslam et al. (2023)38 | Withdrawal time, minutes (mean [SD])a | SR with MA (8 RCTs); 5,773 participants | 6.94 (SD = NR) | 6.57 (SD = NR) | SMD = 0.25 (0.2 to 0.31) | < 0.0001 |
Deep-GI vs. CAD EYE | ||||||
Tiankanon et al. (2024)39 | Withdrawal time excluding the time spent on fecal debris irrigation and polypectomy, minutes (median [IQR]) | RCT; 800 participants | 10 (IQR, 7 to 12) | 10 (IQR, 7 to 12) | NR | NR |
AI = artificial intelligence; CI = confidence interval; IQR = interquartile range; MA = meta-analysis; MD = mean difference; NR = not reported; RCT = randomized controlled trial; SD = standard deviation; SMD = standardized mean difference; SR = systematic review; vs. = versus.
Note: There was overlap in the primary studies that were included in the SRs; the pooled estimates from separate reviews presented in this table thus contain some of the same data. Refer to Appendix 5 for a citation matrix illustrating the degree of overlap.
aThe authors did not specify whether the reported withdrawal times included biopsy.
Table 23: Summary of Findings by Outcome — Procedure Time
Citation | Outcome | Evidence source, number of participants | Outcome result | Relative effect (95% CI) | P value | |
|---|---|---|---|---|---|---|
Intervention group | Control group | |||||
AI-assisted colonoscopy vs. conventional colonoscopy | ||||||
Health Technology Wales (2024)35 | Procedure time, minutes (mean [SD] or median [IQR]) | 1 RCT; Ahmad et al. (2023); 614 participants | 24.9 (IQR, 19.7 to 32.5) | 24.3 (IQR, 18.5 to 32.0) | NR | 0.18 |
1 RCT; Hüneburg et al. (2023); 96 participants | 22.0 (SD = 5.3) | 21.1 (SD = 5.8) | NR | 0.425 | ||
1 RCT; Liu et al. (2020a); 790 participants | 13.37 (SD = 5.15) | 13.01 (SD = 4.64) | NR | 0.315 | ||
1 RCT; Shaukat et al. (2022); 1,359 participants | 15.82 (SD = 5.1) | 15.41 (SD = 5.1) | NR | 0.41 | ||
1 RCT; Wang et al. (2019); 1,058 participants | 12.52 (SD = 4.38) | 12.10 (SD = 4.08) | NR | 0.11 | ||
1 RCT; Wei et al. (2023); 769 participants | 20.8 (SD = 8.1) | 19.1 (SD = 6.7) | NR | 0.00013 | ||
AI = artificial intelligence; CI = confidence interval; IQR = interquartile range; NR = not reported; RCT = randomized controlled trial; SD = standard deviation; vs. = versus.
Table 24: Summary of Findings by Outcome — Adverse Events
Citation | Outcome | Evidence source, number of participants | Outcome result | Relative effect (95% CI) | P value | |
|---|---|---|---|---|---|---|
Intervention group | Control group | |||||
AI-assisted colonoscopy vs. conventional colonoscopy | ||||||
Health Technology Wales (2024)35 | Polypectomies of non-neoplastic lesions per colonoscopy (mean) | SR with MA (18 RCTs); Lou et al. (2023); NR | NR | NR | IRR = 1.63 (1.39 to 1.93); favours conventional group | < 0.001 |
SR with MA (12 RCTs); Hassan et al. (2023b); 12,943 participants | 0.52 (95% CI, 0.41 to 0.63) | 0.34 (95% CI, 0.23 to 0.46) | MD = 0.18 (0.11 to 0.26) | < 0.001 | ||
1 RCT; Lau et al. (2024); 766 participants | 1.17 (SD = 1.65) | 0.61 (SD = 1.13) | FC = 1.92 (1.54 to 2.41) | < 0.001 | ||
Non-neoplastic lesion resection rate | SR with MA (7 RCTs); Lou et al. (2023); NR | NR | NR | RR = 1.16 (0.98 to 1.39) | 0.079 | |
1 RCT; Lau et al. (2024); 766 participants | 52.1% | 35.0% | RR = 1.70 (1.37 to 2.11) | 0.001 | ||
Adverse event ratea | 1 RCT; Engelke et al. (2023); 232 participants | 0.8% | 4.5% | NR | > 0.05 | |
1 RCT; Karsenti et al. (2023); 2,015 participants | 0.1% | 0.0% | NR | NR | ||
1 RCT; Wallace et al. (2022); 230 participants | 5.0% | 3.9% | NR | NR | ||
1 RCT; Zhang et al. (2023); 1,293 participants | 0.2% | 0.0% | NR | NR | ||
Deep-GI vs. CAD EYE | ||||||
Tiankanon et al. (2024)39 | Procedural adverse events (mean) | RCT; 800 participants | 0 | 0 | NR | NR |
AI = artificial intelligence; CI = confidence interval; FC = fold change; IRR = incident rate ratios; MA = meta-analysis; MD = mean difference; NR = not reported; RCT = randomized controlled trial; RR = risk ratio; SD = standard deviation; SR = systematic review; vs. = versus.
aThe authors did not specify which adverse events were included or how they were defined.
Table 25: Summary of Main Findings of Included Economic Evaluation
Citation | Main study findings | Authors’ conclusion |
|---|---|---|
Health Technology Wales (2024)35 | Base case results Incremental cost per person (AI-assisted vs. conventional colonoscopy):
Incremental QALYs per person (AI-assisted vs. conventional colonoscopy):
ICER (incremental costs/incremental QALYs):
Probability of cost-effectiveness: In probabilistic sensitivity analyses, AI-assisted colonoscopy was cost-effective at a willingness-to-pay threshold of £20,000 per QALY in 83% of estimates The authors used deterministic sensitivity analyses to assess the impact of alternative assumptions and inputs on the findings of the analyses. The modelled scenarios included changes to the life span of AI-assisted polyp detection systems, disease prevalence, adenoma detection rates, and the cost of AI-assisted polyp detection systems. The results of these deterministic sensitivity analyses are available in the publication35 | “Overall costs and QALYs were similar for the strategies modelled. However, computer-aided detection was estimated to provide very small QALY gains at a slightly higher cost than the comparator. The ICER of £4,197 per QALY gained indicates that computer-aided detection may be cost effective compared with standard colonoscopy. Computer-aided detection was cost effective in most deterministic sensitivity analyses, but the conclusion did change in a few scenarios tested (p. 39).”35 |
AI = artificial intelligence; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; vs. = versus.
Table 26: Summary of Main Findings of Economic Evaluations Included in the SR by Health Technology Wales (2024)35
Primary study | Main study findings |
|---|---|
Barkun et al. (2023) as reported in Health Technology Wales (2024)35 | Base case results Cost per person:
QALYs:
AI-assisted colonoscopy was less costly and more effective than conventional colonoscopy (i.e., dominant) Probability of cost-effectiveness: In probabilistic sensitivity analyses, AI-assisted colonoscopy was cost-effective at a willingness-to-pay threshold of CA$50,000 per QALY in 63% of estimates |
Hassan et al. (2023a) as reported in Health Technology Wales (2024)35 | Base case results Cost per person:
QALYs:
AI-assisted colonoscopy was less costly and more effective than conventional colonoscopy (i.e., dominant) Probability of cost-effectiveness: In probabilistic sensitivity analyses, AI-assisted colonoscopy was cost-effective at willingness-to-pay thresholds of around €3,000 per QALY in almost 80% of estimates |
Sekiguchi et al. (2023) as reported in Health Technology Wales (2024)35 | Base case results Cost per person:
QALYs:
ICER (incremental costs/incremental QALYs):
Probability of cost-effectiveness: In probabilistic sensitivity analyses, AI-assisted colonoscopy was cost-effective at willingness-to-pay thresholds of ¥5 million per QALY in 51% of estimates (using an incremental cost of ¥4,000 per colonoscopy) |
Thiruvengadam et al. (2023) as reported in Health Technology Wales (2024)35 | Base case results Cost per person:
QALYs:
AI-assisted colonoscopy was less costly and more effective than conventional colonoscopy (i.e., dominant) Probability of cost-effectiveness: In probabilistic sensitivity analyses, AI-assisted colonoscopy was cost-effective at a willingness-to-pay threshold of US$50,000 per QALY in 79% of estimates |
Areia et al. (2022) as reported in Health Technology Wales (2024)35 | Base case results Cost per person:
Colorectal cancer cases per 100,000 people:
Colorectal cancer deaths per 100,000 people:
AI-assisted colonoscopy was less costly and more effective than conventional colonoscopy (i.e., dominant) Probability of cost-effectiveness: In probabilistic sensitivity analyses, AI-assisted colonoscopy was cost-effective at a willingness-to-pay threshold of US$50,000 per QALY in 90% of estimates |
AI = artificial intelligence; ICER = incremental cost-effectiveness ratio; FIT = fecal immunochemical test; QALY = quality-adjusted life-year; SR = systematic review.
Appendix 5: Overlap Between Included SRs
Please note that this appendix has not been copy-edited.
Table 27: Overlap in Relevant Primary Studies Between Included SRs
Primary study citation | Health Technology Wales (2024)35 | Lee et al. (2024)36 | Wei et al. (2024)37 | Aslam et al. (2023)38 |
|---|---|---|---|---|
Agazzi et al. United Eur Gastroenterol J. 2021;813-814. | — | — | Yes | — |
Ahmad et al. Endoscopy. 2023;55(4):313-319. | Yes | Yes | — | — |
Ahmad et al. Gut. 2021;70:A42. | — | — | Yes | — |
Aniwan et al. Gastrointest Endosc. 2023;97(3):507-516. | Yes | Yes | — | — |
Areia et al. Lancet Digit Health. 2022;4(6):e436-e444. | Yes | — | — | — |
Barkun et al. J Can Assoc Gastroenterol. 2023;6(3):97-105. | Yes | — | — | — |
Desai et al. Am J Gastroenterol. 2024;119(7):1383-1391. | Yes | — | — | — |
Engelke et al. Scand J Gastroenterol. 2023;58(10):1194-1199. | Yes | — | — | — |
Glissen Brown et al. Clin Gastroenterol Hepatol. 2022;20(7):1499-1507.e4. | Yes | Yes | — | — |
Gimeno-García et al. Gastrointest Endosc. 2023;97(3):528-536.e1. | Yes | Yes | — | — |
Gong et al. Lancet Gastroenterol Hepatol. 2020;5(4):352-361. | Yes | Yes | — | Yes |
Hassan et al. Endosc Int Open. 2023;11(11):E1046-E1055. | Yes | — | — | — |
Hüneburg et al. United European Gastroenterol J. 2023;11(1):60-68. | Yes | — | — | — |
Ishiyama et al. Gastrointest Endosc. 2022;95(1):155-163. | — | — | Yes | — |
Kamba et al. J Gastroenterol. 2021;56(8):746-757. | Yes | Yes | — | Yes |
Karsenti et al. Lancet Gastroenterol Hepatol. 2023;8(8):726-734. | Yes | — | — | — |
Koh et al. Surg Endosc. 2022;37(1):165-171. | — | — | Yes | — |
Ladabaum et al. Gastroenterology. 2023;164(3):481-483.e6. | — | — | Yes | — |
Lau et al. Clin Gastroenterol Hepatol. 2024;22(3):630-641.e4. | Yes | — | — | — |
Levy et al. Am J Gastroenterol. 2022;117(11):1871-1873. | — | — | Yes | — |
Liu et al. Saudi J Gastroenterol. 2019;26(1):13-19. | Yes | Yes | — | Yes |
Liu et al. Therap Adv Gastroenterol. 2020;13:1756284820979165. | Yes | Yes | — | — |
Lui et al. Am J Gastroenterol. 2024;119(7):1318-1325. | Yes | — | — | — |
Lui et al. Gastrointest Endosc. 2023;97:325-334.e1. | — | Yes | — | — |
Luo et al. J Gastrointest Surg. 2021;25(8):2011-2018. | Yes | — | — | — |
Maas et al. Lancet Digit Health. 2024;6(3):e157-e165. | Yes | — | — | — |
Mangas-Sanjuan et al. Ann Intern Med. 2023;176(9):1145-1152. | Yes | — | — | — |
Misawa et al. Gastroenterology. 2018;154(8):2027-2029.e3. | — | — | — | Yes |
Mori et al. Gastrointest Endosc. 2020;92(4):905-911.e1. | Yes | — | — | — |
Nakashima et al. Digestion. 2023;104(3):193-201. | Yes | Yes | — | — |
Nehme et al. Gastrointest Endosc. 2023;98(1):100-109.e6. | — | — | Yes | — |
Quan et al. Sci Rep. 2022;12(1):6598. | — | — | Yes | — |
Repici et al. Gastroenterology. 2020;159(2):512-520.e7. | Yes | Yes | — | Yes |
Repici et al. Gut. 2022;71(4):757-765. | Yes | Yes | — | — |
Richter et al. Dig Dis. 2023;41(4):615-619. | — | — | Yes | — |
Rondonotti et al. Endoscopy. 2022;54(12):1171-1179. | Yes | Yes | — | — |
Schauer et al. N Z Med J. 2022 Sep 2;135(1561):22-30. | — | — | Yes | — |
Schöler et al. BMJ Open Gastroenterol. 2024;11(1):e001247. | Yes | — | — | — |
Sekiguchi et al. Dig Endosc. 2023;35(7):891-899. | Yes | — | — | — |
Shaukat et al. Endosc Int Open. 2021;9(2):E263-E270. | — | — | Yes | — |
Shaukat et al. Gastroenterology. 2022;163(3):732-741. | Yes | Yes | — | — |
Shen et al. J Dig Dis. 2021;22(5):256-262. | Yes | — | — | — |
Su et al. Gastrointest Endosc. 2020;91(2):415-424.e4. | Yes | Yes | — | Yes |
Thiruvengadam et al. Gastroenterology. 2023;164(6):906-920. | Yes | — | — | — |
Tiankanon et al. Endoscopy. 2024;56(4):273-282. | Yes | — | — | — |
Vilkoite et al. Diagnostics (Basel). 2023;13(4):701. | Yes | Yes | — | — |
Wallace et al. Gastroenterology. 2022;163(1):295-304.e5. | Yes | Yes | — | — |
Wang et al. Gastroenterol Rep (Oxf). 2023:11:goac081. | Yes | Yes | — | — |
Wang et al. Gastroenterology. 2020;159(4):1252-1261.e5. | Yes | Yes | — | Yes |
Wang et al. Gut. 2019;68(10):1813-1819. | Yes | Yes | — | Yes |
Wang et al. Lancet Gastroenterol Hepatol. 2020;5(4):343-351. | Yes | Yes | — | Yes |
Wei et al. Am J Gastroenterol. 2023;118(10):1841-1847. | Yes | Yes | — | — |
Wong et al. Surg Pract. 2022;26(2):115-119. | — | — | Yes | — |
Xu et al. Cancer Med. 2021;10(20):7184-7193. | Yes | — | — | — |
Xu et al. Clin Gastroenterol Hepatol. 2023;21(2):337-346.e3. | Yes | Yes | — | — |
Yamaguchi et al. Dig Endosc. 2024;36(1):40-48. | Yes | Yes | — | — |
Yao et al. Endoscopy. 2022;54(8):757-768. | Yes | Yes | — | Yes |
Yao et al. Gastrointest Endosc. 2024;99(1):91-99.e9. | Yes | — | — | — |
Zhang et al. Front Med (Lausanne). 2024;10:1341259. | Yes | — | — | — |
Zippelius et al. Endoscopy. 2022;54(5):465-472. | — | — | — | Yes |
SR = systematic review.
Appendix 6: References of Potential Interest
Please note that this appendix has not been copy-edited.
Systematic Reviews
Alternative Intervention: Computer-Aided Diagnosis for Colorectal Polyps
Hassan C, Misawa M, Rizkala T, et al. Computer-Aided Diagnosis for Leaving Colorectal Polyps In Situ: A Systematic Review and Meta-analysis. Ann Intern Med. 2024;177(7):919-928. PubMed: PM38768453.
Hassan C, Rizkala T, Mori Y, et al. Computer-aided diagnosis for the resect-and-discard strategy for colorectal polyps: a systematic review and meta-analysis. Lancet Gastroenterol Hepatol. 2024;17:17. PubMed: PM39303733.
ISSN: 2563-6596
Canada’s Drug Agency (CDA-AMC) is a pan-Canadian health organization. Created and funded by Canada’s federal, provincial, and territorial governments, we’re responsible for driving better coordination, alignment, and public value within Canada’s drug and health technology landscape. We provide Canada’s health system leaders with independent evidence and advice so they can make informed drug, health technology, and health system decisions, and we collaborate with national and international partners to enhance our collective impact.
Disclaimer: CDA-AMC has taken care to ensure that the information in this document was accurate, complete, and up to date when it was published, but does not make any guarantee to that effect. Your use of this information is subject to this disclaimer and the Terms of Use at cda-amc.ca.
The information in this document is made available for informational and educational purposes only and should not be used as a substitute for professional medical advice, the application of clinical judgment in respect of the care of a particular patient, or other professional judgments in any decision-making process. You assume full responsibility for the use of the information and rely on it at your own risk.
CDA-AMC does not endorse any information, drugs, therapies, treatments, products, processes, or services. The views and opinions of third parties published in this document do not necessarily reflect those of CDA-AMC. The copyright and other intellectual property rights in this document are owned by the Canadian Agency for Drugs and Technologies in Health (operating as CDA-AMC) and its licensors.
Questions or requests for information about this report can be directed to Requests@CDA-AMC.ca.