Drugs, Health Technologies, Health Systems
Health Technology Review
Review of Guidelines on Bupropion for Depression
Key Messages
What Is the Issue?
Bupropion is a drug used in the treatment of depression. Bupropion is 1 of many treatment options available for depression and is associated with several side effects as well as the potential for misuse. Some patients continue to experience symptoms of depression despite trying multiple medications (known as treatment-resistant depression). Therefore, it is important to determine the place in therapy of bupropion for the treatment of depression.
What Did We Do?
To help determine the potential place in therapy for bupropion for the treatment of major depressive disorder (MDD) and treatment-resistant depression in adults, we sought to identify and summarize recommendations in evidence-based guidelines.
We searched key resources, including journal citation databases, and conducted a focused internet search for relevant evidence published since 2019. One reviewer screened articles for inclusion based on predefined criteria, critically appraised the included publications, and narratively summarized the findings.
What Did We Find?
We identified 4 evidence-based guidelines that included recommendations on the use of bupropion for MDD. We identified 1 evidence-based guideline that included a recommendation on the use of bupropion for difficult-to-treat depression (defined as persistent depression despite several standard treatments).
All 4 included guidelines recommend bupropion for the treatment of adults with MDD. Two of the guidelines recommend bupropion as a first-line treatment option. One guideline suggests bupropion as an option for initial pharmacologic treatment or for patients who have previously responded well to pharmacotherapy. One guideline suggests bupropion as an option for adjunctive treatment for patients in the acute phase of moderate to severe MDD who did not respond to treatment with a second-generation antidepressant.
One guideline suggests bupropion as a second-line adjunctive option for adults with difficult-to-treat depression.
What Does It Mean?
The included evidence-based guidelines consistently recommend bupropion as an option for the treatment of adults with MDD. Additional factors such as the availability of other options, costs, and patient preferences may also be important to decision-making around the use of bupropion for MDD.
Only 1 of the included guidelines included a recommendation on the use of bupropion for patients with difficult-to-treat depression. Future evidence-based guidelines that include recommendations on the use of bupropion for treatment-resistant depression would help fill the gaps identified in this report.
Abbreviations
ACP
American College of Physicians
CANMAT
Canadian Network for Mood and Anxiety Treatments
DoD
US Department of Defense
MDD
major depressive disorder
RANZCP
Royal Australian and New Zealand College of Psychiatrists
VA
US Department of Veterans Affairs
Context and Policy Issues
What Are MDD and Treatment-Resistant Depression?
MDD is defined by a depressed mood or loss of pleasure or interest for at least 2 weeks.1 For a diagnosis it must be accompanied by 4 additional symptoms including weight loss or change in appetite, insomnia or hypersomnia, slowing down or speeding up of physical movements, fatigue or loss of energy, feelings of worthlessness, indecisiveness or diminished ability to concentrate or think, and recurrent thoughts of death or suicide.1,2 MDD causes disability, impairs functioning, impacts quality of life, and can adversely affect the prognosis of physical illnesses.3 In 2022, 7.6% of people aged 15 years and older in Canada experienced a major depressive episode in the previous 12 months.4 Treatment-resistant depression is a subset of MDD in which patients do not respond to 2 or more adequate trials of medication.5 Treatment-resistant depression is estimated to affect approximately 2% of people in Canada (around 700,000 individuals).5
What Is the Current Practice?
There are a range of treatment options used for depression including pharmacotherapy, psychoeducation, psychotherapy, and brain stimulation therapies (for example electroconvulsive therapy).6 Different treatments for depression can be used alone or in combination. The goals for treatment of depression are symptom remission and return to baseline functioning.7 Common classes of medications used in the treatment of depression include selective serotonin reuptake inhibitors (for example, fluoxetine, paroxetine, or fluvoxamine), serotonin and norepinephrine reuptake inhibitors (for example, venlafaxine or duloxetine), norepinephrine and dopamine reuptake inhibitors (for example, bupropion), nonselective cyclics (for example, amitriptyline, imipramine, or desipramine), and monoamine oxidase inhibitors (for example, phenelzine or moclobemide).8 The choice of medication for depression treatment is usually individualized based on efficacy and tolerability.7
What Is Bupropion?
Bupropion is a drug that is used in the treatment of depression. Its mechanism of action is not fully understood; however, it inhibits the reuptake of norepinephrine and dopamine.9 Bupropion is indicated for the treatment of major depressive illness and the prevention of major depressive illness with an autumn to winter seasonal pattern.10 It is available as extended-release tablets in 150 mg and 300 mg doses.10 The starting dose is 150 mg per day and the usual target dose is 300 mg per day, given once daily in the morning.10 Potential side effects of bupropion include increased heart rate, rhinitis, throat inflammation, insomnia, headache, agitation, dizziness, excessive sweating, weight loss, constipation, dry mouth, nausea, tremor, and blurred vision.9
Why Is It Important to Do This Review?
Intentional misuse of bupropion has been reported.11 Bupropion overdose is frequently associated with seizures, tachycardia (increased heart rate), and agitation.11 Because of the availability of many other treatment options for depression as well as the potential for misuse, an overview of recommendations in evidence-based guidelines on the use of bupropion may aid decision-making. Additionally, guidelines on bupropion may help decision-makers determine the place in therapy for bupropion for patients with treatment-resistant depression. Since patients with treatment-resistant depression have not responded to multiple medications, the availability of treatment options with different mechanisms of action may be important for these patients.
Research Question
What are the evidence-based guidelines for the use of bupropion for MDD and treatment-resistant depression?
Methods
Literature Search Methods
An information specialist conducted a literature search on key resources including MEDLINE, Embase, PsycInfo, as well as a focused internet search. The search approach was customized to retrieve a limited set of results, balancing comprehensiveness with relevancy. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. Search concepts were developed based on the elements of the research questions and selection criteria. The main search concepts were bupropion and depression. Search filters were applied to limit retrieval to guidelines. Conference abstracts were excluded. The search was completed on September 6, 2024, and limited to English-language documents published since January 1, 2019.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
|---|---|
Population | Adults aged ≥ 18 years with major depressive disorder or treatment-resistant depression |
Intervention | Bupropion |
Comparator | NA |
Outcomes | Guidelines regarding the use of bupropion for the treatment of major depression disorder or treatment-resistant depression |
Study designs | Evidence-based guidelines |
NA = not applicable.
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, they were duplicate publications, or were published before 2019. Guidelines with unclear methodology were also excluded.
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the Appraisal of Guidelines for Research and Evaluation (AGREE) II instrument12 as a guide. Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Summary of Evidence
Quantity of Research Available
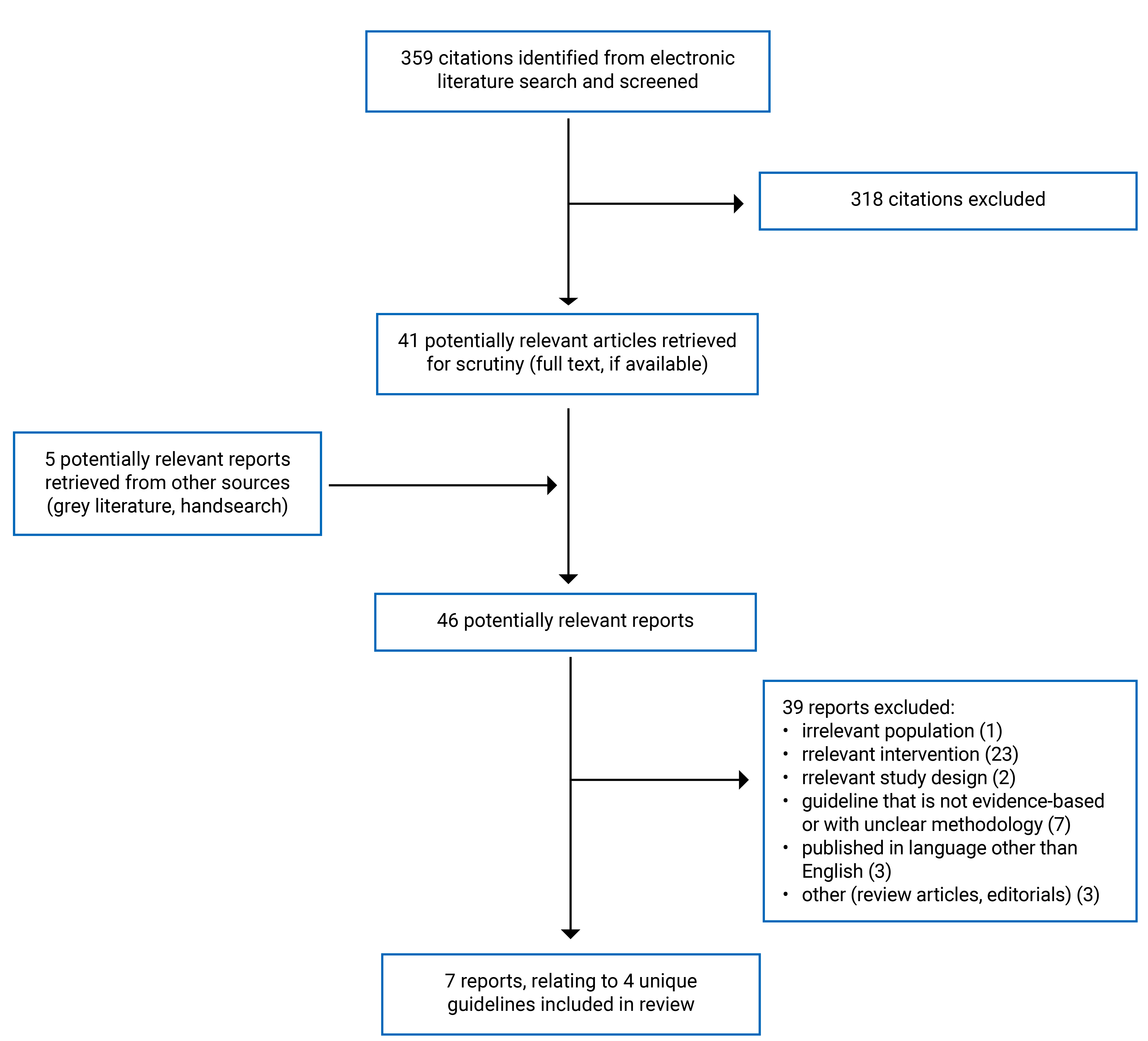
A total of 359 citations were identified in the literature search. Following screening of titles and abstracts, 318 citations were excluded and 41 potentially relevant reports from the electronic search were retrieved for full-text review. Five potentially relevant publications were retrieved from the grey literature search for full-text review. Of these potentially relevant articles, 39 publications were excluded for various reasons, and 7 publications met the inclusion criteria and were included in this report. These 7 publications were related to 4 unique evidence-based guidelines. Appendix 1 presents the PRISMA13 flow chart of the study selection.
Additional references of potential interest are provided in Appendix 2.
Summary of Guideline Characteristics
This report included 4 evidence-based guidelines14-17 that included recommendations on bupropion for the treatment of MDD or treatment-resistant depression. The US Department of Veterans Affairs (VA), the US Department of Defense (DoD) (2022),16 and the Royal Australian and New Zealand College of Psychiatrists (RANZCP) (2020)17 guidelines also published guideline summaries18,19 that were captured by our search. The systematic review20 supporting the American College of Physicians (ACP) (2023)15 guideline was published separately and captured by our search.
The authors of all of the included guidelines conducted literature reviews to inform their recommendations. The authors of the Canadian Network for Mood and Anxiety Treatments (CANMAT) (2024)14 guideline conducted a review that was focused on systematic reviews and meta-analyses. The systematic review20 for the ACP (2023)15 guideline focused on randomized controlled trials and nonrandomized studies. Additionally, 2 rapid reviews were conducted for the ACP (2023)15 guideline. The systematic literature review for the VA-DoD (2022)16 guideline included systematic reviews and randomized controlled trials. The literature review for the RANZCP (2020)17 guideline prioritized systematic reviews and meta-analyses.
Within the CANMAT (2024)14 guideline, the included evidence was assigned a level between 1 (high-quality studies) and 4 (expert opinion-consensus). Treatments were recommended as first, second, or third line, or were not recommended depending on the level of supporting evidence.14 Within the ACP (2023)15 and VA-DoD (2022)16 guidelines the certainty of evidence was assessed using the Grading of Recommendations, Assessment, Development, and Evaluation methodology as very low, low, moderate, or high. The ACP (2023)15 guideline rated recommendations as either strong or conditional. The VA/DoD (2022)16 guideline rated recommendations as either strong or weak. The RANZCP (2020)17 guideline assigned the included evidence a level from I (highest quality) to IV (lowest quality). Within the RANZCP guideline, interventions were classified as actions (treatments that are essential in all cases), choices (treatments available if actions are not sufficient), or alternatives (remaining treatments that may be considered).17
The target population for 3 of the guidelines were adults with MDD.14-16 The target population for the RANZCP (2020)17 guideline were people of any age with mood disorders.
The guideline development groups were from Canada,14 the US,15,16 and Australia.17
Additional details regarding the characteristics of included publications are provided in Appendix 3.
Summary of Critical Appraisal
The CANMAT (2024),14 ACP (2023),15 and VA-DoD (2022)16 guidelines were well conducted overall. The RANZCP (2020)17 guideline had some important limitations. All the included guidelines had clear objectives, guideline questions, and target populations.14-17 Three of the guidelines sought the views and preferences of the target population. The RANZCP (2020)17 guideline did not state that they sought the views and preferences of the target population and therefore the recommendations may not be reflective of the views of people with mood disorders. Three of the guidelines used comprehensive methods to search for evidence and reported details of their search strategy.14-16 The RANZCP (2020)17 guideline did not report the search strategy or key search terms used, search dates, or inclusion or exclusion criteria. Including details on these elements of the search strategy increases its reproducibility and helps the reader determine if the search was comprehensive or if important evidence may have been missed. Three of the guidelines included an explicit link between the supporting evidence and recommendations.14-16 The RANZCP (2020)17 guideline reported on the evidence supporting some of the recommendations; however, limited details of the evidence supporting the bupropion recommendation were provided and the rating for the quality of the evidence was not reported. Providing clear descriptions of the evidence used to support the recommendations increases transparency in the recommendation development process. The funding sources and competing interests of authors were reported in all guidelines.14-17
Additional details regarding the strengths and limitations of included publications are provided in Appendix 4.
Summary of Recommendations
Appendix 5 presents the guideline recommendations.
Guidelines Regarding the Use of Bupropion
The CANMAT (2024)14 guideline recommends bupropion as a first-line treatment option for adults with MDD. The guideline also recommends bupropion as a second-line adjunctive treatment option for adults with difficult-to-treat depression.14 Difficult-to-treat depression was defined as persistent with numerous unsuccessful standard treatments.14 Both recommendations were based on high-quality evidence.14 The ACP (2023)15 guideline suggests augmentation with a second pharmacologic treatment such as bupropion as an option for patients in the acute phase of moderate to severe MDD who did not respond to initial treatment with an adequate dose of a second-generation antidepressant (conditional recommendation based on low certainty evidence). The VA-DoD (2022)16 guideline suggests bupropion as an option for adults with MDD when choosing an initial pharmacotherapy, or for patients who have previously responded well to pharmacotherapy (weak recommendation based on very low-quality evidence). The RANZCP (2020)17 guideline recommends bupropion as an option for first-line pharmacotherapy for patients with MDD. Bupropion was classified by the RANZCP (2020)17 guideline as a choice (treatment available if initial options [actions] are not sufficient). The quality of evidence supporting the recommendation was not reported.
Limitations
This report is limited by the quantity of available evidence. Four evidence-based guidelines were identified that included recommendations on the use of bupropion for MDD. Only 1 guideline included a recommendation on the use of bupropion for difficult-to-treat depression (defined as persistent depression with numerous unsuccessful standard treatments).14 Additionally, the quality of evidence supporting the recommendations was rated as low or very low for 2 of the guidelines and was not reported for 1 guideline. Only the recommendations included in the CANMAT (2024)14 guideline were based on evidence that was rated by the authors as high quality.
Conclusions and Implications for Decision- or Policy-Making
We included 4 evidence-based guidelines on the use of bupropion for the treatment of MDD and treatment-resistant depression.
All 4 guidelines recommend bupropion for MDD. The CANMAT (2024)14 and RANZCP (2020)17 guidelines recommend bupropion as a first-line treatment option for MDD. The VA-DoD (2022)16 guideline suggests bupropion as an option for MDD as initial pharmacotherapy or for patients who have previously responded well to pharmacotherapy. The ACP (2023)15 guideline suggests bupropion as an option for adjunctive treatment for patients in the acute phase of moderate to severe MDD who did not respond to treatment with a second-generation antidepressant.
The CANMAT (2024)14 guideline recommends bupropion as a second-line adjunctive treatment option for adults with difficult-to-treat depression (defined as persistent depression with numerous unsuccessful standard treatments).
Future evidence-based guidelines that include recommendations on the use of bupropion for treatment-resistant depression would help fill the gaps identified in this report. The identified guidelines consistently recommend bupropion as an option for patients with MDD; however, other factors such as the availability of other options, costs, and patient preferences may also be important to decision-making around the use of this drug.
References
1.Clinical Practice Guideline for the Treatment of Depression Across Three Age Cohorts. Washington (DC): American Psychological Association; 2019: https://www.apa.org/depression-guideline. Accessed 2024 Oct 3.
2.Anxiety and Depression Association of America. Clinical Practice Review for Major Depressive Disorder. 2020; https://adaa.org/resources-professionals/practice-guidelines-mdd. Accessed 2024 Oct 3.
3.Lyness JM, Gaynes BN. Depression in adults: Clinical features and diagnosis. In: Post TW, ed. UpToDate. Waltham (MA): UpToDate; 2024: https://www.uptodate.com/. Accessed 2024 Sept 3.
4.Stephenson E. Mental disorders and access to mental health care. Insights on Canadian Society. Ottawa (ON): Statistics Canada; 2023: https://www150.statcan.gc.ca/n1/pub/75-006-x/2023001/article/00011-eng.htm. Accessed 2024 Oct 3.
5.Downar J, Blumberger DM, Daskalakis ZJ. Repetitive transcranial magnetic stimulation: an emerging treatment for medication-resistant depression. CMAJ. 2016;188(16):1175-1177. PubMed
6.CAMH. Depression. [2024]; https://www.camh.ca/en/health-info/mental-illness-and-addiction-index/depression. Accessed 2024 Oct 4.
7.CAMH. Depression: Psychopharmacology. [2024]; https://www.camh.ca/en/professionals/treating-conditions-and-disorders/depression/depression—treatment/depression—psychopharmacology. Accessed 2024 Oct 4.
8.CAMH. Antidepressant Medications. [2024]; https://www.camh.ca/en/health-info/mental-illness-and-addiction-index/antidepressant-medications. Accessed 2024 Oct 4.
9.Huecker MR, Smiley A, Saadabadi A. Bupropion. StatPearls. Treasure Island (FL): StatPearls Publishing; 2024: https://www.ncbi.nlm.nih.gov/books/NBK470212/. Accessed 2024 Oct 4.
10.Wellbutrin XL (bupropion hydrochloride): extended-release tablets, 150 mg and 300 mg, for oral use [product monograph]. Laval (QC): Bausch Health, Canada Inc.; 2022: https://pdf.hres.ca/dpd_pm/00066655.PDF. Accessed 2024 Oct 4.
11.Alberter AA, Chambers AJ, Wills BK. Bupropion Toxicity. StatPearls. Treasure Island (FL): StatPearls Publishing; 2022: https://www.ncbi.nlm.nih.gov/books/NBK580478/. Accessed 2024 Oct 7.
12.Agree Next Steps Consortium. The AGREE II Instrument. Hamilton (ON): AGREE Enterprise; 2017: https://www.agreetrust.org/wp-content/uploads/2017/12/AGREE-II-Users-Manual-and-23-item-Instrument-2009-Update-2017.pdf. Accessed 2024 Oct 7.
13.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
14.Lam RW, Kennedy SH, Adams C, et al. Canadian Network for Mood and Anxiety Treatments (CANMAT) 2023 Update on Clinical Guidelines for Management of Major Depressive Disorder in Adults: Reseau canadien pour les traitements de l'humeur et de l'anxiete (CANMAT) 2023: Mise a jour des lignes directrices cliniques pour la prise en charge du trouble depressif majeur chez les adultes. Can J Psychiatry. 2024;69(9):641-687. PubMed
15.Qaseem A, Owens DK, Etxeandia-Ikobaltzeta I, Tufte J, Cross JT, Wilt TJ. Nonpharmacologic and Pharmacologic Treatments of Adults in the Acute Phase of Major Depressive Disorder: A Living Clinical Guideline From the American College of Physicians. Ann Intern Med. 2023;176(8):239-252. PubMed
16.VA/DoD Clinical Practice Guideline: The Management of Major Depressive Disorder (MDD) Version 4.0 – (2022). Washington (DC): U.S. Department of Veterans Affairs; 2022: https://www.healthquality.va.gov/guidelines/MH/mdd/. Accessed 2024 Sep 18.
17.Royal Australian & New Zealand College of Psychiatrists. Mood disorders clinical practice guideline. 2020; https://www.ranzcp.org/clinical-guidelines-publications/clinical-guidelines-publications-library/mood-disorders-cpg. Accessed 2024 Sep 18.
18.McQuaid JR, Buelt A, Capaldi V, et al. The Management of Major Depressive Disorder: Synopsis of the 2022 U.S. Department of Veterans Affairs and U.S. Department of Defense Clinical Practice Guideline. Ann Intern Med. 2022;175(10):1440-1451. PubMed
19.Malhi GS, Bell E, Singh AB, et al. The 2020 Royal Australian and New Zealand College of Psychiatrists clinical practice guidelines for mood disorders: Major depression summary. Bipolar Disorders. 2020;22(8):788-804. PubMed
20.Gartlehner G, Dobrescu A, Chapman A, et al. Nonpharmacologic and Pharmacologic Treatments of Adult Patients With Major Depressive Disorder: A Systematic Review and Network Meta-analysis for a Clinical Guideline by the American College of Physicians. Ann Intern Med. 2023;176(2):196-211. PubMed
Appendix 1: Selection of Included Studies
Figure 1: PRISMA13 Flow chart of Study Selection
Appendix 2: References of Potential Interest
Note that this appendix has not been copy-edited.
Previous CDA-AMC Reports
CADTH Health Technology Review: Bupropion for Treatment Resistant Depression. Can J Health Technol. 2021;1(4). https://www.cda-amc.ca/bupropion-treatment-resistant-depression. Accessed 2024 Oct 8.
CADTH Health Technology Review: Bupropion for Major Depressive Disorder or Persistent Depressive Disorder (Dysthymia). Can J Health Technol. 2021;1(4). https://www.cda-amc.ca/bupropion-major-depressive-disorder-or-persistent-depressive-disorder-dysthymia. Accessed 2024 Oct 8.
Drugs for Major Depressive Disorder. (CADTH technology review: focused critical appraisal; no. 24). Ottawa (ON): CDA-AMC; 2020: https://www.cda-amc.ca/major-depressive-disorder-focused-critical-appraisal-network-meta-analysis. Accessed 2024 Oct 8.
Guidelines That Are Not Evidence-Based or With Unclear Methodology
Yrondi A, Javelot H, Nobile B, et al. French Society for Biological Psychiatry and Neuropsychopharmacology (AFPBN) guidelines for the management of patients with partially responsive depression and treatment-resistant depression: Update 2024. Encephale. 2024;17:17. PubMed
Corral R, Bojorquez E, Cetkovich-Bakmas M, et al. Latin American consensus recommendations for the management and treatment of patients with treatment-resistant depression (TRD). Span J Psychiatry Ment Health. 2023;22:22. PubMed
Hogan R. Depression in Adults and Older Adults: Oxford Health, Berkshire Healthcare Foundation Trust and BOB ICB Primary Care Treatment Guidelines. [Oxford (GB)]: Buckinghamshire, Oxfordshire and Berkshire West Integrated Care Board (BOB ICB); 2023: https://www.oxfordhealthformulary.nhs.uk/docs/BOB%20ICB%20depression%20guideline.pdf. Accessed 2024 Oct 8.
Iljes AP, Radobuljac MD, Plesnicar BK, et al. Recommendations for treatment of unipolar depressive disorder. Zdravniski Vestnik. 2023;92(7-8):D9-D24.
Villanueva V, Artal J, Cabeza-Alvarez CI, et al. Proposed Recommendations for the Management of Depression in Adults with Epilepsy: An Expert Consensus. Neurol Ther. 2023;12(2):479-503. PubMed
Chin T, Huyghebaert T, Svrcek C, Oluboka O. Individualized antidepressant therapy in patients with major depressive disorder: Novel evidence-informed decision support tool. Can Fam Physician. 2022 Nov;68(11):807-814. https://www.cfp.ca/content/68/11/807. Accessed 2024 Oct 8. PubMed
Treatment of Adult Major Depressive Disorder (MDD) Tool. Toronto (ON): Centre for Effective Practice; 2019: https://cep.health/media/uploaded/CEP_MDD_2019.pdf. Accessed 2024 Oct 8.
Review Articles
Dominiak M, Antosik-Wojcinska AZ, Baron M, Mierzejewski P. Screening and treatment of depression - recommendations for Polish health professionals. Prz Menopauzalny. 2021;20(1):1-13. PubMed
Appendix 3: Characteristics of Included Publications
Table 2: Characteristics of Included Guidelines
Intended users, target population | Intervention(s) and major outcomes considered | Evidence collection, synthesis, and quality assessment | Recommendations development and evaluation | Guideline validation |
|---|---|---|---|---|
CANMAT (2024)14 | ||||
Intended users: community-based psychiatrists and mental health providers Target population: adults with major depressive disorder | Interventions: psychotherapies, pharmacotherapies, lifestyle interventions (for example exercise, nutrition, sleep hygiene) Outcomes: symptom remission, functional improvement, quality of life, recurrence, adverse events | A systematic literature review focused on systematic reviews and meta-analyses was conducted in multiple databases. Where systematic reviews and meta-analyses were unavailable, RCTs and other studies were included. The search was focused on articles published since the previous version of the guidelines in 2016. Relevant studies were selected by 2 independent reviewers. Each article’s quality and risk of bias were assessed using the modified global rating from the GRADE classification. Evidence was assigned a level from 1 to 4:
| All recommendations were made by consensus of the entire guidelines author group. The consensus process occurred at several levels of review of the guideline. Treatment recommendations were organized by lines of treatment based on the strength of evidence and clinical support. Clinical support represents expert consensus by the CANMAT editorial group on tolerability, safety, and feasibility. Lines of treatment:
| Drafts of the guideline were reviewed by patient partners and underwent external peer review |
ACP (2023)15 | ||||
Intended Users: clinicians caring for adult patients in the acute phase of major depressive disorder in ambulatory care Target Population: adults in the acute phase of major depressive disorder | Interventions: nonpharmacologic (psychotherapy, complementary and alternative medicine, exercise) and pharmacologic interventions Outcomes: reduction of suicidal ideation or behaviours, remission, response to treatment, functional capacity, quality of life, reduction of mental suffering (from original source), and serious adverse events | A systematic review and network meta-analysis and 2 rapid reviews were conducted. The systematic review was focused on the comparative benefits and harms of the evaluated pharmacologic and nonpharmacologic treatments. The systematic review was conducted in multiple databases and RCTs were eligible for benefits outcomes and RCTs and nonrandomized studies were eligible for harms outcomes.20 The rapid reviews were focused on patient values and preferences and cost-effectiveness. The certainty of the evidence was assessed using GRADE with possible ratings of very low, low, moderate, and high. | Recommendations were developed by the guideline committee based on the evidence. Findings on patient values and preferences and costs were incorporated when determining the value of interventions. Recommendations were assessed using GRADE methodology. Recommendations were rated as either strong or conditional. | The guideline underwent a public panel that included patient perspectives and peer review process. |
VA-DoD (2022)16 | ||||
Intended Users: health care providers caring for patients with major depressive disorder Target Population: adults who have a diagnosis of major depressive disorder who are eligible for care in the VA or DoD health care delivery systems | Interventions: pharmacotherapies, psychotherapies, complementary and integrative health interventions, physical activity, somatic interventions (for example transcranial magnetic stimulation) Outcomes: symptom improvement, remission, quality of life, functional status, relapse, adverse events | A systematic evidence review was conducted in multiple databases. Systematic reviews and RCTs were eligible for inclusion. The risk of bias of included studies was assessed using the USPSTF method. The overall quality of the body of evidence supporting each outcome was assessed using the GRADE approach with ratings of very low, low, moderate, and high. | A 4-day recommendation development meeting was held to develop the evidence-based recommendations based on the systematic review findings. New recommendations were developed or when appropriate, recommendations were carried forward or modified from the previous version of the guidelines. The strength and direction of each recommendation were determined by assessing the quality of the evidence, benefits and harms, patient values and preferences, and other implications. Recommendations were rated as either strong or weak. | Draft versions of the guideline were posted online for feedback and sent to experts for external peer review. |
RANZCP (2020)17 | ||||
Intended Users: psychiatrists, psychologists, primary care physicians, and others with an interest in mental health care Target Population: people with mood disorders | Interventions: lifestyle changes, psychoeducation, psychological interventions, pharmacotherapies Outcomes: NR | A literature review was conducted in multiple databases. Recent evidence, systematic reviews and meta-analyses were prioritized. Evidence was assigned a level of I (highest quality), II, III-1, III-2, III-3, or IV (lowest quality). | The guideline committee developed a draft that was informed by regular teleconferences and a full day face-to-face meeting. Evidence-based recommendations were developed where possible. Where this was not possible (for example due to insufficient evidence), consensus-based recommendations were developed. Interventions were classified as actions, choices, or alternatives.
| The guideline underwent review by College committees and a peer review conducted by the Australian and New Zealand Journal of Psychiatry. |
ACP = American College of Physicians; CANMAT = Canadian Network for Mood and Anxiety Treatments; DoD = US Department of Defense; GRADE = Grading of Recommendations, Assessment, Development, and Evaluation; NR = not reported; RANZCP = Royal Australian and New Zealand College of Psychiatrists; USPSTF = US Preventive Services Task Force; VA = US Department of Veterans Affairs.
Note: This table has not been copy-edited.
Appendix 4: Critical Appraisal of Included Publications
Note that this appendix has not been copy-edited.
Table 3: Strengths and Limitations of Guidelines Using AGREE II12
Item | CANMAT (2024)14 | ACP (2023)15 | VA-DoD (2022)16 | RANZCP (2020)17 |
|---|---|---|---|---|
Domain 1: scope and purpose | ||||
1. The overall objective(s) of the guideline is (are) specifically described. | Yes | Yes | Yes | Yes |
2. The health question(s) covered by the guideline is (are) specifically described. | Yes | Yes | Yes | Yes |
3. The population (patients, public, and so on) to whom the guideline is meant to apply is specifically described. | Yes | Yes | Yes | Yes |
Domain 2: stakeholder involvement | ||||
4. The guideline development group includes individuals from all relevant professional groups. | Yes | Yes | Yes | Yes |
5. The views and preferences of the target population (patients, public, and so on) have been sought. | Yes | Yes | Yes | No |
6. The target users of the guideline are clearly defined. | Yes | Yes | Yes | Yes |
Domain 3: rigour of development | ||||
7. Systematic methods were used to search for evidence. | Yes | Yes | Yes | Partially |
8. The criteria for selecting the evidence are clearly described. | Yes | Yes | Yes | No |
9. The strengths and limitations of the body of evidence are clearly described. | Yes | Yes | Yes | Partially |
10. The methods for formulating the recommendations are clearly described. | Yes | Yes | Yes | Yes |
11. The health benefits, side effects, and risks have been considered in formulating the recommendations. | Yes | Yes | Yes | Yes |
12. There is an explicit link between the recommendations and the supporting evidence. | Yes | Yes | Yes | Partially |
13. The guideline has been externally reviewed by experts before its publication. | Yes | Yes | Yes | Yes |
14. A procedure for updating the guideline is provided. | Yes | Yes | Yes | No |
Domain 4: clarity of presentation | ||||
15. The recommendations are specific and unambiguous. | Yes | Yes | Yes | Yes |
16. The different options for management of the condition or health issue are clearly presented. | Yes | Yes | Yes | Yes |
17. Key recommendations are easily identifiable. | Yes | Yes | Yes | Partially |
Domain 5: applicability | ||||
18. The guideline describes facilitators and barriers to its application. | Yes | Yes | Partially | No |
19. The guideline provides advice and/or tools on how the recommendations can be put into practice. | Yes | Partially | Yes | Partially |
20. The potential resource implications of applying the recommendations have been considered. | Yes | Yes | Yes | Yes |
21. The guideline presents monitoring and/or auditing criteria. | Yes | No | Partially | No |
Domain 6: editorial independence | ||||
22. The views of the funding body have not influenced the content of the guideline. | Yes | Yes | Yes | Yes |
23. Competing interests of guideline development group members have been recorded and addressed. | Yes | Yes | Yes | Yes |
AGREE II = Appraisal of Guidelines for Research and Evaluation II; ACP = American College of Physicians; CANMAT = Canadian Network for Mood and Anxiety Treatments; DoD = US Department of Defense; RANZCP = Royal Australian and New Zealand College of Psychiatrists; VA = US Department of Veterans Affairs.
Appendix 5: Summary of Recommendations
Note that this appendix has not been copy-edited.
Table 4: Summary of Recommendations in Included Guidelines
Recommendations and supporting evidence | Quality of evidence and strength of recommendations |
|---|---|
CANMAT (2024)14 | |
Bupropion is recommended as a first-line treatment option for adults with major depressive disorder. Supporting evidence: NMA that confirmed bupropion is more effective than placebo. Evidence from meta-analyses for superior response of bupropion vs. comparator medications. | Quality of evidence: Level 1 (high quality) Line of treatment: First line |
Bupropion is recommended as a second-line adjunctive treatment option for adults with difficult-to-treat depression. Supporting evidence: Large RCTs have shown evidence of the effectiveness of adjunctive bupropion; however, meta-analyses were inconclusive. | Quality of evidence: Level 1 (high quality) Line of treatment: Second line |
ACP (2023)15 | |
“ACP suggests one of the following options for patients in the acute phase of moderate to severe major depressive disorder who did not respond to initial treatment with an adequate dose of a second-generation antidepressant:
The informed decision on the options should be personalized and based on discussion of potential treatment benefits, harms, adverse effect profiles, cost, feasibility, patients’ specific symptoms (such as insomnia, hypersomnia, or fluctuation in appetite), comorbidities, concomitant medication use, and patient preferences. Rationale: If a clinically satisfactory response or remission of symptoms is not achieved with initial monotherapy with an SGA (including dose optimization), switching to monotherapy with CBT or to a different SGA or augmenting SGA monotherapy with CBT or with a second pharmacologic treatment (such as mirtazapine, bupropion, or buspirone) are reasonable approaches, as these second-line treatment strategies showed similar efficacy when compared with each other (p. 242).”15 Supporting evidence: Evidence from an RCT showed similar response and remission rates when augmentation of a second-generation antidepressant with cognitive therapy was compared to pharmacologic augmentation (with bupropion or buspirone). | Certainty of evidence: Low Strength of recommendation: Conditional |
VA-DoD (2022)16 | |
“When choosing an initial pharmacotherapy, or for patients who have previously responded well to pharmacotherapy, we suggest offering one of the following (not rank ordered):
Supporting evidence: NMA of 522 RCTs showed similar effect between bupropion, mirtazapine, trazodone, nefazodone, serotonin-norepinephrine reuptake inhibitors, selective serotonin reuptake inhibitor, MAOIs, and TCAs in terms of symptom improvement and remission rates, with all being significantly more effective than placebo. NMA of 53 RCTs showed similar frequency of adverse events between these agents. | Quality of evidence: Very low Strength of recommendation: Weak |
RANZCP (2020)17 | |
Bupropion is an option for first-line pharmacotherapy for patients with major depressive disorder. Supporting evidence: NMAs that showed antidepressants are more effective than placebo. | Quality of evidence: NR Strength of recommendation: Choice (treatments available if actions are not sufficient) |
ACP = American College of Physicians; CANMAT = Canadian Network for Mood and Anxiety Treatments; CBT = cognitive behavioural therapy; DoD = US Department of Defense; MAOI = monoamine oxidase inhibitors; NMA = network meta-analysis; NR = not reported; RANZCP = Royal Australian and New Zealand College of Psychiatrists; RCT = randomized controlled trial; SGA = second-generation antidepressant; TCAs = tricyclic antidepressants; VA = US Department of Veterans Affairs.
ISSN: 2563-6596
Canada’s Drug Agency (CDA-AMC) is a pan-Canadian health organization. Created and funded by Canada’s federal, provincial, and territorial governments, we’re responsible for driving better coordination, alignment, and public value within Canada’s drug and health technology landscape. We provide Canada’s health system leaders with independent evidence and advice so they can make informed drug, health technology, and health system decisions, and we collaborate with national and international partners to enhance our collective impact.
Disclaimer: CDA-AMC has taken care to ensure that the information in this document was accurate, complete, and up to date when it was published, but does not make any guarantee to that effect. Your use of this information is subject to this disclaimer and the Terms of Use at cda-amc.ca.
The information in this document is made available for informational and educational purposes only and should not be used as a substitute for professional medical advice, the application of clinical judgment in respect of the care of a particular patient, or other professional judgments in any decision-making process. You assume full responsibility for the use of the information and rely on it at your own risk.
CDA-AMC does not endorse any information, drugs, therapies, treatments, products, processes, or services. The views and opinions of third parties published in this document do not necessarily reflect those of CDA-AMC. The copyright and other intellectual property rights in this document are owned by the Canadian Agency for Drugs and Technologies in Health (operating as CDA-AMC) and its licensors.
Questions or requests for information about this report can be directed to Requests@CDA-AMC.ca.