Drugs, Health Technologies, Health Systems
Health Technology Review
Gabapentin for Seizures
Key Messages
What Is the Issue?
Gabapentin is 1 of many antiseizure medications available for the treatment of epilepsy in adults; however, there are potential risks associated with its use. Therefore, it is important to determine the place of therapy of gabapentin in the treatment of epilepsy.
What Did We Do?
To help determine the potential place in therapy for gabapentin in the treatment of epilepsy in adults, we sought to identify and summarize studies of the clinical- and cost-effectiveness of gabapentin as well as recommendations from evidence-based guidelines.
We searched key resources, including journal citation databases, and conducted a focused internet search for relevant evidence published since 2014. One reviewer screened articles for inclusion based on predefined criteria, critically appraised the included publications, and narratively summarized the findings.
What Did We Find?
We identified 1 systematic review and 1 randomized controlled trial (RCT) that evaluated the efficacy of gabapentin in adults with epilepsy. We identified 5 evidence-based guidelines that included recommendations on the use of gabapentin for epilepsy. We did not identify any studies that evaluated its cost-effectiveness.
Seizure-free retention at 3 months may be better in adults with epilepsy who were treated with lamotrigine than gabapentin or carbamazepine. There were no differences in other seizure outcomes (such as time to seizure, seizure freedom, or seizure-free retention) for adults with epilepsy treated with gabapentin versus lamotrigine or carbamazepine.
Adults with epilepsy treated with gabapentin were more likely to experience fair or poor health perception than those treated with oxcarbazepine. There were no differences in other quality of life outcomes (such as anxiety, depression, or worry about seizures) between those treated with gabapentin versus lamotrigine, carbamazepine, oxcarbazepine, or topiramate.
Withdrawals because of adverse events were similar between adults with epilepsy treated with gabapentin and lamotrigine. There were more systemic toxicities in adults treated with gabapentin than carbamazepine or lamotrigine but there were no differences in neurotoxicities between groups.
One guideline recommends against the use of gabapentin in people with myoclonic seizures or people with epilepsy with myoclonic-atonic seizures. One guideline states that there is insufficient evidence to consider gabapentin instead of carbamazepine in patients with new-onset focal epilepsy or unclassified generalized tonic-clonic seizures.
Three guidelines recommend the use of gabapentin in older adults with epilepsy. One guideline recommends the use of gabapentin in people with intellectual disability and epilepsy, if the benefits outweigh the risks or as a second-line option.
What Does It Mean?
There were few differences in outcomes between adults with epilepsy treated with gabapentin versus other active comparators in the studies we identified. The included guidelines recommended for or against the use of gabapentin depending on patient factors such as age and type of epilepsy or seizures.
Decision-makers may wish to consider individual patient factors such as age and type of epilepsy or seizures as well as the availability of other treatment options when making decisions on the use of gabapentin for the treatment of epilepsy.
Abbreviations
AAN
American Academy of Neurology
MPA
Medical Products Agency
NICE
National Institute for Health and Care Excellence
RCT
randomized controlled trial
SIGN
Scottish Intercollegiate Guidelines Network
Context and Policy Issues
What Is Epilepsy?
Epilepsy is a neurologic disorder that is characterized by recurrent seizures.1 A seizure is a burst of electrical activity in the brain that causes temporary abnormalities in muscle tone or movement, behaviours, sensations, and levels of consciousness.2 There are 2 types of seizures: focal seizures (seizures that begin in 1 area of the brain) and generalized-onset seizures (seizures that occur throughout the cortex of the brain).3 Epilepsy has been defined as 2 unprovoked seizures occurring 24 hours apart, a single seizure if the risk of recurrence is high, or the diagnosis of an epilepsy syndrome.4 Data from 2021 to 2022 show that approximately 1 in 100 people in Canada live with epilepsy. Among people with epilepsy in Canada, 63% are adults aged 20 to 64 years and 24% are older adults (aged 65 years and older).1
What Is the Current Practice?
The goal of epilepsy treatment is to limit or prevent seizures.1 Treatment options for epilepsy include medications, surgery, neuromodulation, and dietary therapy.1,4 There is a range of antiepileptic drugs available that have various mechanisms of action including acting on sodium channels, calcium channels, or gamma-aminobutyric acid type A receptors to reduce excitability in the brain.5 Many drugs can be used for both focal or generalized-onset seizures whereas some drugs are specific for a particular type of seizure (for example partial seizures) or epilepsy (for example, Dravet syndrome).4 Antiepileptic drugs include (but are not limited to) benzodiazepines, lamotrigine, levetiracetam, perampanel, phenobarbital, topiramate, sodium valproate, brivaracetam, carbamazepine, eslicarbazepine acetate, gabapentin, pregabalin, lacosamide, oxcarbazepine, phenytoin, vigabatrin, rufinamide, and stiripentol.4 The choice of medication is dependent on individual factors such as age, sex, comorbidities, tolerability issues, seizure type, and epileptic syndrome.4
What Is Gabapentin?
Gabapentin is a gabapentinoid that interacts with calcium channels in the brain and reduces excitability throughout the nervous system.6 Gabapentin is indicated as adjunctive therapy for the management of adults with epilepsy who are not satisfactorily controlled by conventional therapy.7 Gabapentin is available as capsules and tablets for oral administration.7 The starting dose for gabapentin is 300 mg 3 times per day and the dose may be increased depending on patient response and tolerance.7 Common adverse effects of gabapentin include sedation, dizziness, and vertigo.8
Why Is It Important to Do This Review?
There is reported nonmedical use of gabapentinoids (gabapentin and pregabalin) because of potentially desirable effects such as euphoria.8,9 Nonprescribed use of gabapentin, particularly when combined with opioids, is associated with increased risk of all-cause and drug-related hospitalization.10 The central nervous system depressant effects of both gabapentinoids and opioids (drowsiness, respiratory depression, and respiratory failure) have been implicated in drug-related deaths.9 Individuals who use gabapentinoids also have increased risks for suicidal ideation, unintentional overdoses, traffic accidents, and injuries.10 Because of the availability of many other antiepileptic medications as well as the potential risks associated with the use of gabapentin, decision-makers may be interested in determining the appropriate place in therapy of gabapentin for adults with epilepsy.
Research Questions
What is the clinical effectiveness and safety of gabapentin for treatment of adults with epilepsy?
What is the cost-effectiveness of gabapentin for the treatment of adults with epilepsy?
What are the evidence-based guidelines for the use of gabapentin for adults with epilepsy?
Methods
Literature Search Methods
An information specialist conducted a literature search on key resources including MEDLINE, Embase, the Cochrane Database of Systematic Reviews, the International HTA Database, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search approach was customized to retrieve a limited set of results, balancing comprehensiveness with relevancy. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. Search concepts were developed based on the elements of the research questions and selection criteria. The main search concepts were gabapentin and epilepsy or seizures. Conference abstracts were excluded. The search was completed on August 13, 2024, and limited to English-language documents published since January 1, 2014.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
|---|---|
Population | Adults aged ≥ 18 years who have seizures because of epilepsy |
Intervention | Gabapentin |
Comparator | Placebo; antiepileptics (e.g., phenytoin, phenobarbital, ethosuximide, carbamazepine, primidone, sodium valproate, vigabatrin, lamotrigine, benzodiazepines, topiramate, oxcarbazepine, levetiracetam, lacosamide, perampanel, eslicarbazepine, brivaracetam, rufinamide, stiripentol) |
Outcomes | Q1: Clinical benefits (e.g., seizure frequency emergency department visits, HRQoL) and harms (e.g., adverse events, myocardial infarction) Q2: Cost-effectiveness (e.g., cost per QALY gained) Q3: Guidelines regarding the use of gabapentin in adults with epilepsy |
Study designs | Health technology assessments, systematic reviews, randomized controlled trials, economic evaluations, evidence-based guidelines |
HRQoL = health-related quality of life; QALY = quality-adjusted life-year.
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, they were duplicate publications or were published before 2014. Systematic reviews in which all relevant studies were captured in other more recent or more comprehensive systematic reviews were excluded. Primary studies retrieved by the search were excluded if they were captured in 1 or more included systematic reviews. Guidelines with unclear methodology were also excluded.
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the following tools as a guide: A Measurement Tool to Assess Systematic Reviews 2 (AMSTAR 2)11 for systematic reviews, the Downs and Black checklist12 for randomized studies, and the Appraisal of Guidelines for Research and Evaluation (AGREE) II instrument13 for guidelines. Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Summary of Evidence
Quantity of Research Available
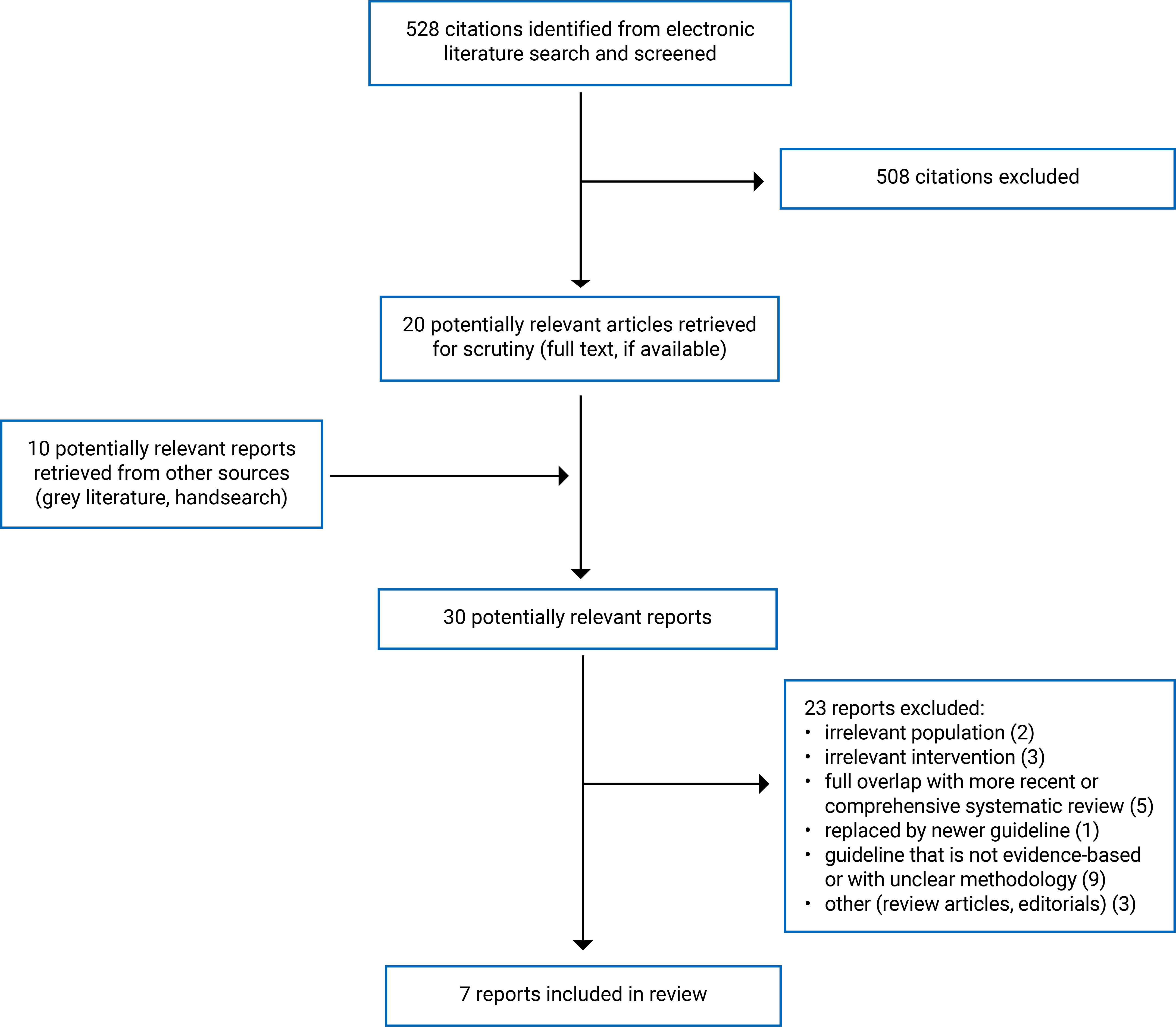
A total of 528 citations were identified in the literature search. Following screening of titles and abstracts, 508 citations were excluded and 20 potentially relevant reports from the electronic search were retrieved for full-text review. Ten potentially relevant publications were retrieved from the grey literature search for full-text review. Among these 30 potentially relevant articles, 23 publications were excluded for various reasons, and 7 publications met the inclusion criteria and were included in this report. These comprised 1 systematic review, 1 RCT, and 5 evidence-based guidelines. Appendix 1 presents the PRISMA14 flow chart of the study selection.
Additional references of potential interest are provided in Appendix 2.
Summary of Study Characteristics
We identified 1 systematic review15 and 1 RCT16 that evaluated the clinical effectiveness of gabapentin for the treatment of epilepsy in adults. We did not identify any studies that evaluated the cost-effectiveness of gabapentin for the treatment of epilepsy in adults. We identified 5 evidence-based guidelines17-21 that included recommendations on the use of gabapentin for epilepsy.
The included systematic review had broader inclusion criteria than the present report. Specifically, eligible interventions included a range of antiepileptic drugs, and the eligible population included children.15 Only the characteristics and results of the relevant studies (i.e., studies of gabapentin in adults) will be described in this report.
Additional details regarding the characteristics of included publications are provided in Appendix 3.
Study Design
The search time frame for the Nevitt et al. (2022)15 systematic review was from database inception to April 12, 2021. The systematic review included 89 RCTs in total, 2 of which are relevant to the present report.15
The Jacoby et al. (2015)16 study was a subgroup analysis of a randomized, unblinded, parallel-group trial that included both children and adults with epilepsy. The subgroup analysis was focused specifically on quality of life in adults.
The 5 included guidelines were developed by National Institute for Health and Care Excellence (NICE) in 2022,17 the Swedish Medical Products Agency (MPA) in 2020,18 American Academy of Neurology (AAN) in 2018,19 Scottish Intercollegiate Guidelines Network (SIGN) in 2018,20 and the Royal College of Psychiatrists in 2017.21 Systematic literature searches of RCTs and systematic reviews were conducted to inform the NICE (2022)17 guideline. The evidence was assessed using the Grading of Recommendations, Assessment, Development, and Evaluation methodology and assigned a rating from very low to high.17 A systematic review of RCTs, systematic reviews, meta-analyses, and guidelines was conducted to inform the Swedish MPA (2020)18 guideline. The evidence was evaluated using the International League Against Epilepsy template and assigned a level from F (lowest quality) to A (highest quality).18 A systematic review of RCTs and nonrandomized studies was conducted to inform the AAN (2018)19 guideline. Evidence was rated using the AAN therapeutic classification scheme with ratings that ranged from class IV (lowest quality) to class I (highest quality).19 Recommendations were assigned a level from U (lowest) to A (highest) based on the strength of supporting evidence.19 A systematic review was conducted to inform the SIGN (2018)20 guideline and evidence was given a level from 4 (lowest quality) to 1++ (highest quality) and the recommendations were assigned a grade from D (lowest) to A (highest). A focused literature review that included a grey literature search was conducted to inform the Royal College of Psychiatrists (2017)21 guideline and evidence was graded on a scale from V (lowest quality) to Ia (highest quality). Recommendations were rated using a traffic light system of red (lowest), amber, and green (highest).21
Country of Origin
The systematic review and RCT were conducted by authors in the UK.15,16 The NICE (2022)17 and Royal College of Psychiatrists (2017)21 guidelines are meant to apply to the UK, the Swedish MPA (2020)18 guideline is meant to apply to Sweden, the AAN (2018)19 guideline is meant to apply to the US, and the SIGN (2018)20 guideline is meant to apply to Scotland.
Patient Population
There were 2 relevant RCTs included in the Nevitt et al. (2022) systematic review. One of the relevant RCTs included participants older than 16 years with at least 2 focal seizures in the last 12 months who were either untreated in the previous 6 months or or who had never received antiepileptic drugs. The other relevant RCT included adults older than 60 years with newly diagnosed seizures with at least 1 seizure in the previous 3 months who were untreated or treated with subtherapeutic antiepileptic drug levels.
The Jacoby et al. (2015) included adults (aged 16 years or older at time of randomization) with a history of 2 or more clinically definite unprovoked seizures in the previous year.
The target population of the NICE (2022)17 guideline is children, young people and adults with epilepsy in primary and secondary care and the intended users are health care professionals in primary, secondary, and tertiary care; commissioners; providers and voluntary organizations; and people with epilepsy, their families and carers. The target population of the Swedish MPA (2020)18 guideline is people with newly diagnosed epilepsy and the intended users are doctors. The target population of the AAN (2018)19 guideline is people with new-onset focal or generalized epilepsy and the intended users were not specified. The target population of the SIGN (2018)20 guideline is adults with epilepsy and the intended users are health professionals in primary and secondary care involved in the management of people with epilepsy, those commissioning epilepsy services, public-health physicians, pharmacists, social-work staff, carers and relatives of people with epilepsy, and people with epilepsy themselves. The target population of the Royal College of Psychiatrists (2017)21 guideline is people with intellectual disability and epilepsy and the intended users are epileptologists, psychiatrists, doctors, and clinicians working with people with intellectual disability and epilepsy.
Interventions and Comparators
One of the relevant RCTs included in the Nevitt et al. (2022)15 systematic review compared gabapentin (dose range of 1,200 mg to 3,600 mg per day) and lamotrigine (dose range of 100 mg to 300 mg per day). The second relevant RCT included in the Nevitt et al. (2022)15 systematic review compared gabapentin (1,500 mg per day), carbamazepine (600 mg per day), and lamotrigine (150 mg per day).
Participants in the Jacoby et al. (2015)16 RCT received gabapentin, carbamazepine, lamotrigine, oxcarbazepine, or topiramate. The drug dosages were those used by the clinicians in their everyday practice. The rate of titration, initial maintenance dose, and any dose increases or decreases were decided by the clinician.
The interventions considered in 3 of the included guidelines were antiepileptic drugs.18,19,21 The SIGN (2018)20 guideline considered antiepileptic drugs as well as neurosurgical procedures. The NICE (2022)17 guideline considered antiseizure medications, ketogenic diets, surgical interventions, and vagus nerve stimulation.
Summary of Critical Appraisal
Additional details regarding the strengths and limitations of included publications are provided in Appendix 4.
Systematic Review
Overall, the systematic review by Nevitt et al. (2022)15 was well conducted. The research methods were established before conducting the review and the protocol was published. A comprehensive search strategy was used which reduces the likelihood that important studies were missed. The search was conducted in multiple databases, the full search strategy was provided, reference lists of included studies were hand searched for additional articles, experts in the field were contacted for details of ongoing or unpublished studies, and no language restrictions were used.15 Study selection was performed independently by 2 reviewers and the full list of excluded studies and reasons for exclusion was provided.15 These methods reduce the risk of bias in study selection.
RCT
The RCT by Jacoby et al. (2015)16 had several important limitations. The study participants and clinicians were not blind to the treatment interventions.16 This may have led to the differential treatment of intervention groups in the trial or the differential assessment of outcomes, which may have biased the estimates of treatment effects. Additionally, the outcomes assessed in the trial were subjective measures (i.e., quality of life) which are more prone to bias because of lack of blinding. Clinicians could switch trial participants to drugs other than the intervention they were assigned depending on treatment response.16,22 By the 2-year follow-up, approximately 45% of patients were no longer taking the drug they were randomized to.16 Therefore, any impact on outcomes may not be attributable to the intervention participants were randomized to. Further, a large proportion of participants were lost to follow-up. At 1 year, 68% of participants returned the questionnaire and at 2 years, 60% of participants returned the questionnaire.16 There were imbalances in baseline characteristics between those who responded to the questionnaires and those who did not, which may have impacted the study’s results.
Guidelines
The overall objectives and health questions were clearly described in all included guidelines.17-21 The views and preferences of the target population were sought in 3 of the guidelines.17,18,20 The AAN (2018)19 and Royal College of Psychiatrists (2017)21 guidelines did not report that they sought out the views and preferences of their target populations. Three of the included guidelines used systematic methods to search for evidence.17,19,20 The Swedish MPA (2020)18 guideline only searched a single database and therefore may have missed relevant literature. The Royal College of Psychiatrists (2017)21 guideline reported a very limited description of their search methods and therefore, it is unclear whether they were comprehensive. In 3 of the guidelines, there was an explicit link between the recommendations and supporting evidence.19-21 In the NICE (2022)17 guideline, it was not clear what evidence the gabapentin recommendations were based on. In the Swedish MPA (2020)18 guideline, they state that the gabapentin recommendation is based on a single study and provide an evidence rating; however, further details of the study were not provided. Four of the included guidelines reported their funding sources and potential conflicts of interest.17-20 The Royal College of Psychiatrists (2017)21 guideline did not report the funding source or the authors’ conflicts of interest. Conflicts of interest or influence from funders could lead to bias in the reporting of evidence or recommendations.
Summary of Findings
Appendix 5 presents the main study findings.
Clinical Effectiveness of Gabapentin
Seizures, study completion, compliance, and adverse events were evaluated in the systematic review by Nevitt et al. (2022).15 Quality of life was evaluated in the RCT by Jacoby et al. (2015).16
Seizures
There was no difference in the time to first seizure for adults treated with gabapentin versus lamotrigine (1 RCT).15 There was no difference in the time to first, second, fifth, or 10th seizure for adults treated with gabapentin, lamotrigine, or carbamazepine (1 RCT).15 There was no difference in seizure freedom at 12 months for adults treated with gabapentin, lamotrigine, or carbamazepine (1 RCT).15 There was a statistically significant difference in seizure-free retention at 3 months in favour of lamotrigine versus gabapentin and carbamazepine (1 RCT).15 There was no difference in seizure-free retention at 6 or 12 months between adults treated with lamotrigine, gabapentin, or carbamazepine (1 RCT).15 The percentage of participants who remained seizure-free during the final 12 weeks of the 30-week evaluation period was 76.1% for those treated with gabapentin and 76.8% for those treated with lamotrigine (1 RCT).15
Study Completion
There was no significant difference in median time to exit the study for adults treated with gabapentin versus lamotrigine (1 RCT).15 The proportion of participants completing the study was 71.6% for those treated with gabapentin and 67.1% for those treated with lamotrigine (1 RCT).15 There was no difference in time to withdrawal for any reason for participants treated with gabapentin versus lamotrigine (1 RCT).15 There was a significant difference in retention in trial for 12 months with the carbamazepine group having more early terminators than the gabapentin or lamotrigine groups (1 RCT).15
Compliance
There was no significant difference in treatment compliance between participants treated with gabapentin, lamotrigine, or carbamazepine (1 RCT).15
Quality of Life
In the Jacoby et al. (2015)16 RCT, participants assigned to gabapentin were more likely than those assigned to oxcarbazepine to experience fair or poor health perception rather than good or excellent. There was no significant difference in other quality of life outcomes (anxiety, depression, mastery [language retained from original source], adverse events profile, Aldenkamp-Baker Neuropsychological Assessment Schedule, stigma, worse health transition, worry about past seizure, or worry about future seizures) between participants treated with gabapentin versus lamotrigine, carbamazepine, oxcarbazepine, or topiramate.16
Adverse Events
During the titration period, there were 7 participants in the gabapentin group and 10 in the lamotrigine group that withdrew because of adverse events (1 RCT).15 After the titration period, there were 10 participants in the gabapentin group and 13 in the lamotrigine group that withdrew because of adverse events (1 RCT).15 There were more systemic toxicities with gabapentin than carbamazepine or lamotrigine (1 RCT).15 There were no significant differences in neurotoxicities between the gabapentin, carbamazepine, and lamotrigine groups over 12 months (1 RCT).15
Guidelines Regarding the Use of Gabapentin
The NICE (2022)17 guideline recommends against the use of gabapentin in people with myoclonic seizures or people with epilepsy with myoclonic-atonic seizures because it may exacerbate seizures. The NICE (2022)17 guideline also recommends being aware that gabapentin may exacerbate seizures in people with absence seizures, tonic or atonic seizures, Dravet syndrome, or Lennox-Gastaut syndrome.
The Swedish MPA (2022)18 guideline recommends gabapentin as a possible alternative to first-line options (lamotrigine and levetiracetam) for use as monotherapy for focal-onset seizures in older adults based on a single study with possible methodological flaws.
The AAN (2018)19 guideline states that gabapentin may be considered to decrease seizure frequency in patients aged 60 years or older with new-onset focal epilepsy. The strength of the recommendation is level C (possibly effective) based on Class II evidence.19 The AAN (2018)19 guideline also states that evidence is insufficient (level U, data inadequate) to consider gabapentin instead of carbamazepine in patients with new-onset focal epilepsy or unclassified generalized tonic-clonic seizures based on Class III evidence.
The SIGN (2018)20 guideline states that gabapentin may be used in adjunctive treatment of focal epilepsy. The recommendation was rated grade A (highest) based on high-quality evidence (1++ and 1+).20 The SIGN (2018)20 guideline also recommends gabapentin as an alternative option for monotherapy or adjunctive therapy in older people with epilepsy. The recommendation was rated grade C (low) based on high-quality evidence (1++ and 1+).20
The Royal College of Psychiatrists (2017)21 guideline states that gabapentin could be considered in people with intellectual disability and epilepsy if the benefits outweigh the risks or as a second-line option. The recommendation was rated as amber (moderate) based on moderate quality evidence (Level II).21
Limitations
This report is limited by the quantity of research identified that met our inclusion criteria. We did not identify any studies that evaluated the cost-effectiveness of gabapentin for the treatment of epilepsy in adults. Only 2 of the RCTs in the included systematic review were relevant to this report (i.e., evaluated gabapentin for epilepsy in adults). Additionally, the RCT we identified is at risk of bias because of several important limitations outlined in the critical appraisal section.
Conclusions and Implications for Decision- or Policy-Making
We included 1 systematic review,15 1 RCT,16 and 5 evidence-based guidelines17-21 on the use of gabapentin for the treatment of epilepsy in adults.
Results from the systematic review showed that when adults with epilepsy were treated with gabapentin versus other active comparators (i.e., lamotrigine or carbamazepine) there was no difference between groups in a range of seizure outcomes (time to first, second, fifth, or 10th seizure, seizure freedom at 12 months, seizure-free retention at 6 or 12 months).15 There was a statistically significant difference in seizure-free retention at 3 months in favour of lamotrigine versus gabapentin and carbamazepine (1 RCT).15 Results from the Jacoby et al. (2015)16 RCT showed that participants assigned to gabapentin were more likely than those assigned to oxcarbazepine to experience fair or poor health perception rather than good or excellent. There were no significant differences in other quality of life outcomes between participants treated with gabapentin versus lamotrigine, carbamazepine, oxcarbazepine, or topiramate.16
The systematic review reported that withdrawals because of adverse events were similar between adults with epilepsy treated with gabapentin and lamotrigine (1 RCT).15 The systematic review also reported that there were more systemic toxicities in participants treated with gabapentin than carbamazepine or lamotrigine but there were no significant differences in neurotoxicities between groups (1 RCT).15
The NICE (2022)17 guideline recommends against the use of gabapentin in people with myoclonic seizures or people with epilepsy with myoclonic-atonic seizures because it may exacerbate seizures. The AAN (2018)19 guideline states that there is insufficient evidence to consider gabapentin instead of carbamazepine in patients with new-onset focal epilepsy or unclassified generalized tonic-clonic seizures.
The Swedish MPA (2022)18 guideline recommends gabapentin as a possible alternative to first-line options for use as monotherapy for focal-onset seizures in older adults. The AAN (2018)19 guideline states that gabapentin may be considered to decrease seizure frequency in patients aged 60 years or older with new-onset focal epilepsy. The SIGN (2018)20 guideline states that gabapentin may be used in adjunctive treatment of focal epilepsy. The SIGN (2018)20 guideline also recommends gabapentin as an alternative option for monotherapy or adjunctive therapy in older people with epilepsy. The Royal College of Psychiatrists (2017)21 guideline states that gabapentin could be considered in people with intellectual disability and epilepsy if the benefits outweigh the risks or as a second-line option.
Based on the results of the clinical studies and guidelines identified in this report, decision-makers may wish to consider the availability of other treatment options as well as patient factors such as age and type of epilepsy or seizures when making decisions around the use of gabapentin for the treatment of epilepsy in adults.
References
1.Epilepsy in Canada. Ottawa (ON): Public Health Agency of Canada; 2024: https://www.canada.ca/en/public-health/services/publications/diseases-conditions/epilepsy.html. Accessed 2024 Sep 5.
2.Johns Hopkins Medicine. Seizures. [2024]; https://www.hopkinsmedicine.org/health/conditions-and-diseases/seizures. Accessed 2024 Sep 6.
3.Johns Hopkins Medicine. Types of Seizures. [2024]; https://www.hopkinsmedicine.org/health/conditions-and-diseases/epilepsy/types-of-seizures. Accessed 2024 Sep 6.
4.Thijs RD, Surges R, O'Brien TJ, Sander JW. Epilepsy in adults. Lancet. 2019;393(10172):689-701. PubMed
5.Sande R, Kale P, Godad A, Doshi G. An Update on the Pathways and Aspects of Epilepsy Treatment Targets. Current Signal Transduction Therapy. 2023;18(3):45-62.
6.McPherson D, Wick JY. Gabapentin: Change is in the Wind. Sr Care Pharm. 2019;34(8):490-498. PubMed
7.Neurontin (gabapentin): capsules, 100 mg, 300 mg and 400 mg, oral; tablets, 600 mg and 800 mg, oral [product monograph]. Etobicoke (ON): BGP Pharma ULC; 2023 Oct 16: https://pdf.hres.ca/dpd_pm/00072927.PDF. Accessed 2024 Sep 6.
8.Athavale A, Murnion B. Gabapentinoids: a therapeutic review. Aust Prescr. 2023;46(4):80-85. PubMed
9.Parsons G. Guide to the management of gabapentinoid misuse. Prescriber. 2018;29(4):25-30.
10.Baldwin DS, Masdrakis V. Non-prescribed use of gabapentinoids. Clinics in Integrated Care. 2023;21:100164.
11.Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. PubMed
12.Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377-384. PubMed
13.Agree Next Steps Consortium. The AGREE II Instrument. Hamilton (ON): AGREE Enterprise; 2017: https://www.agreetrust.org/wp-content/uploads/2017/12/AGREE-II-Users-Manual-and-23-item-Instrument-2009-Update-2017.pdf. Accessed 2024 Sep 6.
14.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
15.Nevitt SJ, Sudell M, Cividini S, Marson AG, Tudur Smith C. Antiepileptic drug monotherapy for epilepsy: a network meta-analysis of individual participant data. Cochrane Database Syst Rev. 2022;4(4):CD011412. PubMed
16.Jacoby A, Sudell M, Tudur Smith C, Crossley J, Marson AG, Baker GA. Quality-of-life outcomes of initiating treatment with standard and newer antiepileptic drugs in adults with new-onset epilepsy: findings from the SANAD trial. Epilepsia. 2015;56(3):460-472. PubMed
17.National Institute for Health and Care Excellence. Epilepsies in children, young people and adults. (NICE guideline NG217) 2022; https://www.ncbi.nlm.nih.gov/books/NBK581165/. Accessed 2024 Sep 6.
18.Compagno Strandberg M, Soderberg-Lofdal K, Kimland E, Dahlin M, Kallen K. Evidence-based anti-seizure monotherapy in newly diagnosed epilepsy: A new approach. Acta Neurol Scand. 2020;142(4):323-332. PubMed
19.Kanner AM, Ashman E, Gloss D, et al. Practice guideline update summary: Efficacy and tolerability of the new antiepileptic drugs I: Treatment of new-onset epilepsy: Report of the Guideline Development, Dissemination, and Implementation Subcommittee of the American Academy of Neurology and the American Epilepsy Society. Neurology. 2018;91(2):74-81. PubMed
20.Diagnosis and management of epilepsy in adults. (SIGN publication no. 143). Edinburgh (GB): Scottish Intercollegiate Guidelines Network (SIGN); 2018: https://www.sign.ac.uk/our-guidelines/diagnosis-and-management-of-epilepsy-in-adults/. Accessed 2024 Aug 27.
21.Prescribing anti-epileptic drugs for people with epilepsy and intellectual disability. (College Report CR206). London (GB): The Royal College of Psychiatrists; 2017: https://www.rcpsych.ac.uk/docs/default-source/improving-care/better-mh-policy/college-reports/college-report-cr206.pdf. Accessed 2024 Aug 28.
22.Marson AG, Appleton R, Baker GA, et al. A randomised controlled trial examining the longer-term outcomes of standard versus new antiepileptic drugs. The SANAD trial. Health Technol Assess. 2007;11(37):iii-iv, ix-x, 1-134.
Appendix 1: Selection of Included Studies
Figure 1: PRISMA14 Flow Chart of Study Selection
Appendix 2: References of Potential Interest
Please note that this appendix has not been copy-edited.
Previous CDA-AMC Reports
Gabapentin, Phenobarbital, Diazepam, and Lorazepam for the Treatment of Alcohol Withdrawal: Clinical Effectiveness and Guidelines. (CDA-AMC Rapid response report: summary of abstracts). Ottawa (ON): CDA-AMC; 2020 https://www.cda-amc.ca/sites/default/files/covid-19/RB1498%20Addiction%20Services%20during%20COVID%20Final.pdf. Accessed 2024 Sep 6.
Gabapentin for Adults With Neuropathic Pain: A Review. (In Brief: Summarizing the Evidence). Ottawa (ON): CDA-AMC; 2019 https://www.cda-amc.ca/gabapentin-adults-neuropathic-pain-review. Accessed 2024 Sep 6.
Guidelines That Are Not Evidence-Based or With Unclear Methodology
Updated Guidelines for the Management of Drug-resistant Epilepsy in Adults and Children who are not Candidates for Epilepsy Surgery. [Toronto (ON)]: Ontario Epilepsy Guidelines, Critical Care Services Ontario (CCSO) and EpLink – The Epilepsy Research Program of the Ontario Brain Institute; 2023: https://ontarioepilepsyguidelines.ca/updated-guidelines-for-the-management-of-drug-resistant-epilepsy-in-adults-and-children-who-are-not-candidates-for-epilepsy-surgery/. Accessed 2024 Sep 6.
Holtkamp, M., Krämer, G. Antiepileptic pharmacotherapy in old age: evidence-based approach versus clinical routine – English Version. Z Epileptol. 2022;35(Suppl 2):105-112. https://link.springer.com/article/10.1007/s10309-022-00492-x. Accessed 2024 Sep 6.
Clinical Guidelines for the Management of Epilepsy in Adults and Children. [Toronto (ON)]: Ontario Epilepsy Guidelines, Critical Care Services Ontario (CCSO) and EpLink – The Epilepsy Research Program of the Ontario Brain Institute; 2020: https://ontarioepilepsyguidelines.ca/updated-management-guidelines/. Accessed 2024 Sep 6.
Boon P, Ferrao Santos S, Jansen AC, Lagae L, Legros B, Weckhuysen S. Recommendations for the treatment of epilepsy in adult and pediatric patients in Belgium: 2020 update. Acta Neurol Belg. 2021 Feb;121(1):241-257. https://link.springer.com/article/10.1007/s13760-020-01488-y. Accessed 2024 Sep 6. PubMed: PM33048338.
Clinical Practice Guidelines for Epilepsy 2018. Japanese Society of Neurology; 2018: https://www.neurology-jp.org/guidelinem/epilepsy/index.html. Accessed 2024 Sep 6.
Liu G, Slater N, Perkins A. Epilepsy: Treatment Options. Am Fam Physician. 2017 Jul 15;96(2):87-96. https://www.aafp.org/pubs/afp/issues/2017/0715/p87.html. Accessed 2024 Sep 6. PubMed: PM28762701.
Mercadé Cerdá JM, Mauri Llerda JA, Becerra Cuñat JL, et al. Prognosis in epilepsy: initiating long-term drug therapy. Neurologia. 2015 Jul-Aug;30(6):367-74. https://www.elsevier.es/en-revista-neurologia-english-edition--495-articulo-prognosis-in-epilepsy-initiating-long-term-S2173580815000735. Accessed 2024 Sep 6. PubMed: PM24745309.
Nonrandomized Studies
Gremke N, Printz M, Moller L, Ehrenberg C, Kostev K, Kalder M. Association between anti-seizure medication and the risk of lower urinary tract infection in patients with epilepsy. Epilepsy Behav. 2022 10;135:108910. PubMed: PM36115082.
Cicekci F, Yuksekkavas D, Aydin A, Karaibrahimoglu A, Uca AU. The comparison of socio-demographic and clinical variables of inmates using gabapentin for medicinal purposes and those abusing the drug. Journal of Neurological Sciences. 2017;34(3):242-251.
Appendix 3: Characteristics of Included Publications
Please note that this appendix has not been copy-edited.
Table 2: Characteristics of Included Systematic Review
Study citation, country, funding source | Study design, outcomes | Intervention and comparator(s) | Included studies | Population characteristics |
|---|---|---|---|---|
Nevitt et al. (2022)15 UK Funding source: National Institute for Health Research | Systematic review and network meta-analysis of RCTs Outcomes: time to treatment failure, remission (6-month, 12-month), time to first seizure, adverse events | Interventions: carbamazepine, phenytoin, sodium valproate, phenobarbitone, oxcarbazepine, lamotrigine, gabapentin, topiramate, levetiracetam, zonisamide, eslicarbazepine acetate, and lacosamide | 89 RCTs in total; 2 RCTs relevant to the present report | Eligible population: Children or adults with focal-onset seizures or generalized-onset tonic-clonic seizures Brodie 2002: participants > 16 years with at least 2 focal seizures in the last 12 months who were untreated in the previous 6 months or AED naive
Rowan 2005: adults > 60 years with newly diagnosed seizures, untreated or treated with subtherapeutic AED levels, with at least 1 seizure in the previous 3 months
|
AED = antiepileptic drug; RCT = randomized controlled trial.
Table 3: Characteristics of Included Randomized Controlled Trial
Study citation, country, funding source | Study design | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Jacoby et al. (2015)16 UK Funding source: Health Technology Assessment program of the National Health Service in the UK, companies of the products assessed, Epilepsy Research UK | Randomized, unblinded, parallel-group trial | Adults (16 years or older at time of randomization) with a history of 2 or more clinically definite unprovoked seizures in the previous year (N = 1,267). Mean age (years):
| Intervention: gabapentin Comparators: carbamazepine, lamotrigine, oxcarbazepine, topiramate | Outcomes: quality of life Follow-up: 2 years |
Table 4: Characteristics of Included Guidelines
Intended users, target population | Intervention and practice considered | Major outcomes considered | Evidence collection, synthesis, and quality assessment | Recommendations development and evaluation | Guideline validation |
|---|---|---|---|---|---|
NICE (2022)17 | |||||
Intended users: Health care professionals in primary, secondary and tertiary care; commissioners, providers and voluntary organizations; people with epilepsy, their families and carers Target population: children, young people and adults with epilepsy in primary and secondary care | Antiseizure medications, ketogenic diets, surgical interventions, vagus nerve stimulation | Mortality, seizure freedom, seizure frequency, time to first seizure, time to withdrawal of treatment, quality of life, adverse events | Systematic literature searches were conducted in multiple databases to identify published clinical evidence (RCTs, systematic reviews) relevant to the review questions. Titles and abstracts were screened and full texts of relevant studies were obtained and screened based on prespecified inclusion and exclusion criteria. Relevant studies were critically appraised using the checklists specified in the NICE guidelines manual. Summaries of evidence were generated, and data were combined in meta-analysis where appropriate. Evidence was assessed using GRADE methodology (ratings range from very low to high). | The guideline development group drafted recommendations based on their interpretation of the relevant evidence. The considerations included the balance between benefits, harms, and costs between different options. | A draft version of the guideline was sent to interested parties. Revisions were made to the guideline based on the feedback received. |
Swedish MPA (2020)18 | |||||
Intended users: doctors Target population: people with newly diagnosed epilepsy | Drugs used as monotherapy in epilepsy | Seizure-free outcomes, drug retention | A systematic review of RCTs, SRs, meta-analyses, and guidelines was conducted in 1 database. The review methodology was prespecified. Screening of articles was conducted by 2 authors. Relevant studies were evaluated using the ILAE 2013 template. The evidence levels range from F (lowest quality) to A (highest quality). | A background draft was presented at an MPA epilepsy workshop. A draft of the guidelines was developed in collaboration with a national expert group. Further comments and revisions and the finalization of the guidelines were completed in a digital workspace. | The guideline underwent quality review by the MPA and was approved by the director general. |
AAN (2018)19 | |||||
Intended users: NR Target population: people with new-onset focal or generalized epilepsy | Second- and third-generation antiepileptic drugs | Seizure recurrence, seizure freedom, adverse events | A systematic review of RCTs and nonrandomized studies was conducted in multiple databases. Two guideline panel members reviewed the included studies using the 2004 AAN therapeutic classification of evidence scheme. The evidence ratings range from class IV (lowest quality) to class I (highest quality). | An expert panel formulated the recommendations based on the evidence identified to answer the guideline’s clinical questions. Recommendations were assigned a level based on the strength of supporting evidence.
| The draft guideline was reviewed by an internal committee as well as relevant external groups. |
SIGN (2018)20 | |||||
Intended users: health professionals in primary and secondary care involved in the management of people with epilepsy, those commissioning epilepsy services, public-health physicians, pharmacists, social-work staff, carers and relatives of people with epilepsy and people with epilepsy themselves Target population: adults with epilepsy | Antiepileptic drugs, neurosurgical procedures | Seizure frequency, seizure duration, quality of life, adverse events | A systematic literature review was conducted in multiple databases. Each of the selected articles was evaluated by 2 members of the guideline group using SIGN methodological checklists. The evidence supporting recommendations was given a level from 4 (lowest quality) to 1++ (highest quality). | The guideline development group drafted recommendations based on the evidence identified to answer each of the guideline’s key questions. Considerations included balance of benefits and harms, patient values, equity, and costs. Recommendations were assigned a grade from D (lowest) to A (highest). | A draft of the guideline was presented at a national open meeting attended by representatives of key specialties relevant to the guideline. The draft guideline was also available on the SIGN website for a limited period. The draft guideline was also reviewed by independent experts and the SIGN editorial group. |
Royal College of Psychiatrists (2017)21 | |||||
Intended users: epileptologists, psychiatrists, doctors and clinicians working with people with intellectual disability and epilepsy Target population: people with intellectual disability and epilepsy | Antiepileptic drugs | Seizure control, adverse events | A focused literature review that included a grey literature search was conducted. The quality of evidence was graded on a scale from V (lowest quality) to Ia (highest quality). | A draft report including recommendations was prepared and circulated to the advisory committee for feedback. Recommendations were formulated by integrating clinical experience, evidence of efficacy, and side effects. Recommendations used a traffic light system:
| A draft of the guidelines was submitted to the Royal College for feedback. The feedback received was incorporated to produce the final report. |
AAN = American Academy of Neurology; GRADE = Grading of Recommendations, Assessment, Development, and Evaluation; ILAE = International League Against Epilepsy; MPA = Medical Products Agency; NICE = National Institute for Health and Care Excellence; NR = not reported; RCT = randomized controlled trial; SIGN = Scottish Intercollegiate Guidelines Network; SR = systematic review.
Appendix 4: Critical Appraisal of Included Publications
Please note that this appendix has not been copy-edited.
Table 5: Strengths and Limitations of Systematic Review Using AMSTAR 211
Strengths | Limitations |
|---|---|
Nevitt et al. (2022)15 | |
Clear objective and inclusion criteria that included components of population, intervention, comparator, and outcomes The research methods were established before conducting the review and the protocol was published The choice of study designs included in the review (i.e., RCTs) was explained The literature search was conducted in multiple databases, the search strategy was provided, no language restrictions were used, reference lists of included studies were hand searched for additional articles, and experts in the field were contacted for details on ongoing or unpublished studies Study selection and data extraction were performed independently by 2 reviewers Full list of excluded studies and reasons for exclusion provided The included primary studies were described in adequate detail Risk of bias was assessed independently by 2 authors using a satisfactory technique Sources of funding for included primary studies were reported The source of funding for the systematic review and the authors’ potential conflicts of interest were reported | None |
AMSTAR 2 = A MeaSurement Tool to Assess systematic Reviews 2; RCT = randomized controlled trial.
Table 6: Strengths and Limitations of Randomized Controlled Trial Using the Downs and Black Checklist12
Strengths | Limitations |
|---|---|
Jacoby et al. (2015)16 | |
Objective, patient characteristics, interventions, and main findings clearly described Estimates of random variability (i.e., 99% confidence intervals) reported Patients, care providers, and care setting were representative of the population and setting of interest Statistical tests used to measure main outcomes were appropriate Patients in different intervention groups were recruited from the same population over the same time period Patients were randomized to treatment groups by telephone using minimization (with stratification by centre, sex, and drug use history) Funding source and potential conflicts of interest reported | Potential confounders not discussed or adjusted for Study participants and clinicians were not blind to the treatment interventions Study was a subgroup analysis of quality of life in adults and the authors do not state whether the subgroup analysis was preplanned Clinicians could switch patients to other drugs depending on treatment response and by the 2-year follow-up approximately 45% of patients were no longer taking the drug they were randomized to A large proportion of patients were lost to follow-up and there were some imbalances in baseline characteristics between responders and nonresponders There was no discussion of power or reporting of a power calculation Multiple outcomes were assessed; however, there was no adjustment for multiplicity |
Table 7: Strengths and Limitations of Guidelines Using AGREE II13
Item | NICE (2022)17 | Swedish MPA (2020)18 | AAN (2018)19 | SIGN (2018)20 | Royal College of Psychiatrists (2017)21 |
|---|---|---|---|---|---|
Domain 1: scope and purpose | |||||
1. The overall objective(s) of the guideline is (are) specifically described. | Yes | Yes | Yes | Yes | Yes |
2. The health question(s) covered by the guideline is (are) specifically described. | Yes | Yes | Yes | Yes | Yes |
3. The population (patients, public, and so on) to whom the guideline is meant to apply is specifically described. | Yes | Partially | Yes | Yes | Yes |
Domain 2: stakeholder involvement | |||||
4. The guideline development group includes individuals from all relevant professional groups. | Yes | Unclear | Yes | Yes | Yes |
5. The views and preferences of the target population (patients, public, and so on) have been sought. | Yes | Yes | No | Yes | No |
6. The target users of the guideline are clearly defined. | Yes | Partially | No | Yes | Yes |
Domain 3: rigour of development | |||||
7. Systematic methods were used to search for evidence. | Yes | Partially | Yes | Yes | Partially |
8. The criteria for selecting the evidence are clearly described. | Yes | Yes | Yes | Yes | No |
9. The strengths and limitations of the body of evidence are clearly described. | Yes | Yes | Yes | Yes | Yes |
10. The methods for formulating the recommendations are clearly described. | Yes | Yes | Yes | Yes | Yes |
11. The health benefits, side effects, and risks have been considered in formulating the recommendations. | Yes | Yes | Yes | Yes | Yes |
12. There is an explicit link between the recommendations and the supporting evidence. | No | Partially | Yes | Yes | Yes |
13. The guideline has been externally reviewed by experts before its publication. | Yes | No | Yes | Yes | Yes |
14. A procedure for updating the guideline is provided. | Yes | No | Yes | Yes | No |
Domain 4: clarity of presentation | |||||
15. The recommendations are specific and unambiguous. | Yes | Yes | Yes | Yes | Yes |
16. The different options for management of the condition or health issue are clearly presented. | Yes | Yes | Yes | Yes | Yes |
17. Key recommendations are easily identifiable. | Yes | Yes | Yes | Yes | Yes |
Domain 5: applicability | |||||
18. The guideline describes facilitators and barriers to its application. | Yes | No | No | Yes | No |
19. The guideline provides advice and/or tools on how the recommendations can be put into practice. | Yes | No | No | Yes | Yes |
20. The potential resource implications of applying the recommendations have been considered. | Yes | No | No | Yes | No |
21. The guideline presents monitoring and/or auditing criteria. | Yes | No | No | Partially | No |
Domain 6: editorial independence | |||||
22. The views of the funding body have not influenced the content of the guideline. | Yes | Yes | Yes | Yes | No |
23. Competing interests of guideline development group members have been recorded and addressed. | Yes | Yes | Yes | Yes | No |
AAN = American Academy of Neurology; AGREE II = Appraisal of Guidelines for Research and Evaluation II; MPA = Medical Products Agency; NICE = National Institute for Health and Care Excellence; SIGN = Scottish Intercollegiate Guidelines Network.
Appendix 5: Main Study Findings
Please note that this appendix has not been copy-edited.
Table 8: Summary of Findings from Included Systematic Review and RCT
Study citation and study design | Outcome | Results |
|---|---|---|
Nevitt et al. (2022)15 Systematic review (2 RCTs) | – | – |
Gabapentin vs. lamotrigine | ||
Brodie 2002 | Median time to exit |
|
Proportion of population completing the study |
| |
Time to withdrawal for any reason | No difference between groups. | |
Time to first seizure | No difference between groups. | |
Percentage who remained seizure-free during the final 12 weeks of the 30-week evaluation period |
| |
Withdrawals because of adverse events | Withdrawals during titration:
Withdrawals after titration:
| |
Gabapentin vs. lamotrigine vs. carbamazepine | ||
Rowan 2005 | Retention in trial for 12 months | Significant difference between 3 treatment groups (P = 0.00022)
|
Seizure freedom at 12 months | No significant difference between groups (P = 0.09)
| |
Time to seizures | No difference between groups for time to first, second, fifth and 10th seizure (P = 0.18, 0.13, 0.74, 0.95, respectively). | |
Drug toxicity | More systemic toxicities with gabapentin than carbamazepine or lamotrigine. No significant differences in neurotoxicities between treatment groups over 12 months. | |
Compliance | No significant differences between groups.
| |
Seizure-free retention at 3 months | Significant difference between groups (P = 0.02)
| |
Seizure-free retention at 6 months | No significant difference between groups (P = 0.22)
| |
Seizure-free retention at 12 months | No significant difference between groups (P = 0.33)
| |
Gabapentin vs. lamotrigine vs. carbamazepine vs. oxcarbazepine vs. topiramate | ||
Jacoby et al. (2015)16 RCT | Fair or poor health perception | Those assigned to gabapentin were more likely than those assigned to oxcarbazepine to experience fair or poor general health perception rather than good or excellent
|
Continuous QoL outcomes (anxiety, depression, mastery [language retained from original source], AEP, ABNAS, stigma) | No significant differences between gabapentin and other groups. | |
Binary QoL outcomes (worse health transition, worry about past seizure, worry about future seizures) | No significant differences between gabapentin and other groups. | |
ABNAS = Aldenkamp-Baker Neuropsychological Assessment Schedule; AEP = adverse events profile; CI = confidence interval; OR = odds ratio; QoL = quality of life; RCT = randomized controlled trial; vs. = versus.
Table 9: Summary of Recommendations in Included Guidelines
Recommendations and supporting evidence | Quality of evidence and strength of recommendations |
|---|---|
NICE (2022)17 | |
Be aware that gabapentin may exacerbate seizures in people with:
Supporting evidence: NR | Quality of evidence: NR Strength of recommendation: weak |
Do not use gabapentin in people with myoclonic seizures or people with epilepsy with myoclonic-atonic seizures because it may exacerbate seizures. Supporting evidence: NR | Quality of evidence: NR Strength of recommendation: strong |
Swedish MPA (2020)18 | |
Gabapentin is recommended as a possible alternative to first-line options (lamotrigine and levetiracetam) for use as monotherapy for focal-onset seizures in older adults. Supporting evidence: A single study with possible methodological flaws. | Quality of evidence: Level A Strength of recommendation: NR |
AAN (2018)19 | |
Gabapentin may be considered to decrease seizure frequency in patients aged 60 years or older with new-onset focal epilepsy. Supporting evidence: One double-blind randomized study compared efficacy and tolerability of gabapentin, lamotrigine, and carbamazepine in patients aged 60 years or older. Drug discontinuation was less common for lamotrigine than gabapentin or carbamazepine. The results suggest that gabapentin is possibly as effective and better tolerated than carbamazepine. | Quality of evidence: Class II Strength of recommendation: Level C (possibly effective) |
Evidence is insufficient to consider gabapentin instead of carbamazepine in patients with new-onset focal epilepsy or unclassified generalized tonic-clonic seizures. Supporting evidence: One randomized unblinded trial in children and adults with epilepsy that compared lamotrigine, gabapentin, carbamazepine, topiramate, and oxcarbazepine. | Quality of evidence: Class III Strength of recommendation: Level U (data inadequate) |
SIGN (2018)20 | |
Gabapentin may be used in the adjunctive treatment of focal epilepsy. Supporting evidence: Results from a meta-analysis suggest that gabapentin is effective as an adjunctive treatment for focal epilepsy. | Quality of evidence: 1++ and 1+ Strength of recommendation: Grade A (highest) |
Gabapentin is an alternative option for monotherapy or adjunctive therapy in older people with epilepsy. Supporting evidence: Studies found no significant difference in efficacy between carbamazepine, lamotrigine and gabapentin in older people. | Quality of evidence: 1++ and 1+ Strength of recommendation: Grade C (low) |
Royal College of Psychiatrists (2017)21 | |
Gabapentin could be considered in people with intellectual disability and epilepsy if the benefits outweigh the risks or as a second-line option. Supporting evidence: A comparative open-label study found no difference between gabapentin and lamotrigine. There are no definitive details of efficacy or potential for harm in people with intellectual disability and epilepsy. | Quality of evidence: Level II Strength of recommendation: Amber (moderate) |
AAN = American Academy of Neurology; ILAE = International League in Epilepsy; NR = not reported; SIGN = Scottish Intercollegiate Guidelines Network; MPA = Medical Products Agency.
ISSN: 2563-6596
Canada’s Drug Agency (CDA-AMC) is a pan-Canadian health organization. Created and funded by Canada’s federal, provincial, and territorial governments, we’re responsible for driving better coordination, alignment, and public value within Canada’s drug and health technology landscape. We provide Canada’s health system leaders with independent evidence and advice so they can make informed drug, health technology, and health system decisions, and we collaborate with national and international partners to enhance our collective impact.
Disclaimer: CDA-AMC has taken care to ensure that the information in this document was accurate, complete, and up to date when it was published, but does not make any guarantee to that effect. Your use of this information is subject to this disclaimer and the Terms of Use at cda-amc.ca.
The information in this document is made available for informational and educational purposes only and should not be used as a substitute for professional medical advice, the application of clinical judgment in respect of the care of a particular patient, or other professional judgments in any decision-making process. You assume full responsibility for the use of the information and rely on it at your own risk.
CDA-AMC does not endorse any information, drugs, therapies, treatments, products, processes, or services. The views and opinions of third parties published in this document do not necessarily reflect those of CDA-AMC. The copyright and other intellectual property rights in this document are owned by the Canadian Agency for Drugs and Technologies in Health (operating as CDA-AMC) and its licensors.
Questions or requests for information about this report can be directed to Requests@CDA-AMC.ca.