Drugs, Health Technologies, Health Systems
Health Technology Review
Midazolam Compared With Lorazepam in Adults to Control Seizures
Key Messages
What Is the Issue?
The emergency treatment of prolonged seizures or status epilepticus is required to be rapid and efficient to prevent permanent brain damage or death.
Benzodiazepines, such as midazolam, lorazepam, diazepam, and clonazepam, are established as first-line treatment medications for acute treatments of seizures.
Various administration routes of delivery for these drugs have become available, but the comparative clinical effectiveness and safety among administration routes are still unclear.
Decision-makers are interested in whether the current use of intramuscular (IM) midazolam for treatment of seizures by paramedics in a prehospital environment can be switched to IV lorazepam as normally used by nurses and physicians in clinic settings.
What Did We Do?
We identified and summarized the literature on the evidence of the clinical effectiveness and safety of midazolam compared to lorazepam in adults to control seizures.
We searched key resources, including journal citation databases, and conducted a focused internet search for relevant evidence published since 2019. One reviewer screened citations for inclusion based on predefined criteria, critically appraised the included studies, and narratively summarized the findings.
What Did We Find?
We identified 1 systematic review (SR) that included 4 randomized controlled trials (RCTs), only 1 was relevant to this review. This double-blind RCT determined the efficacy of IM midazolam as noninferior to IV lorazepam for treatment of seizures by paramedics in a mixed population of adults (89%) and children (11%).
The authors of the SR conducted a subanalysis of a dataset of participant-level data and showed that IM midazolam was as effective and safe as IV lorazepam in adult patients for prehospital seizure cessation. The findings of the adult population were similar to those of the whole randomized population of both adults and children.
What Does This Mean?
With the shorter time required to administration of midazolam by the IM route compared to administration of lorazepam by the IV route, and the comparable efficacy and safety between the 2 active treatments, the use of IM midazolam may be a better option in the prehospital environment when IV access in patients with seizures is not readily established.
Switching of IM midazolam to IV lorazepam for treatment of seizures by paramedics may not be practical.
Abbreviations
AE
adverse event
CI
confidence interval
ED
emergency department
ICU
intensive care unit
IM
intramuscular
ITT
intention to treat
RCT
randomized controlled trial
RR
relative risk
SR
systematic review
Context and Policy Issues
What Is Seizure?
A seizure is a period of symptoms caused by sudden, uncontrolled, and abnormal electrical activity between nerve cells in the brain that causes temporary changes in behaviour, feelings, movements (sudden stiffening and jerking of the arms and legs), and levels of consciousness.1-3 Seizures are classified into 2 major classes (i.e., focal onset and generalized onset) that are based on how and where seizures begin.1-3 Focal onset seizures, the most common type of seizure in adults, start with electrical activity in 1 area of the brain and can occur with or without impaired awareness.1-3 There are 2 types of focal seizures: focal aware seizure (the person is aware of what is happening) and focal unaware seizure (the person may appear confused and cannot respond to questions or directions).1-3 Generalized onset seizures involve all areas of the brain where abnormal nerve discharges surge more or less at the same time.1-3 Generalized seizures commonly develop during childhood and may have a genetic component.1-3 There are 6 main types of generalized seizures: tonic-clonic, tonic, clonic, myoclonic, absence, and atonic seizures.2,3
Seizures may be either provoked or unprovoked.4,5 Provoked seizures may result from various causes such as electrolyte disturbances (e.g., hypoglycemia, hyponatremia, hypernatremia, or hypocalcemia), acute toxic effects, withdrawal syndromes (e.g., alcohol or benzodiazepines), infections (e.g., sepsis or central nervous system infection), brain injury (e.g., hypoxic or trauma), stroke, neoplasm, inflammation, fever, or sleep deprivation.5 Unprovoked seizures occur without provocative causes or more than 7 days after an acute injury of the brain such as a stroke (ischemic or hemorrhagic).5 Epilepsy is defined as 2 or more unprovoked seizures.1 Also, when a seizure lasts more than 5 minutes or when seizures occur closely together without returning to a normal level of consciousness between episodes, this is a medical emergency known as status epilepticus, or prolonged seizures, and a treatment is required immediately to prevent permanent brain damage or death.6
Data from fiscal year 2021–2022 showed that about 1 out of 100 people living in Canada live with epilepsy.7 Among those with epilepsy, 13% were children and adolescents (aged 1 to 19 years), 63% were adults (aged 20 to 64 years), and 24% were older adults (aged 65 years and older).7 The proportions are similar for both sexes.7 However, new cases are more frequent among younger and older people (i.e., 66 new cases per 100,000 in children and adolescents, 51 new cases per 100,000 in adults, and 87 new cases per 100,000 in older adults).7
What Is the Current Practice?
Initial response to a person having a seizure involves ensuring the person is protected from potential harms from objects nearby, and managing their airway, breathing, and circulation.1,8 The person should be placed on their side to prevent choking.1,8 There are many approaches for treatment of seizures including medication, surgery, electrical stimulation, dietary therapy, and lifestyle changes.9 For medication, benzodiazepines such as midazolam, lorazepam, or diazepam are recommended as first-line treatment medications for continuing seizures.1,10 Second-line treatment medications include fosphenytoin, valproate, and levetiracetam.1,10
The choice of a drug depends on many factors including seizure type, seizure frequency, lifestyle, age, drug side effects, other health conditions, and pregnancy.9 An antiseizure medication is usually started with a low dose, which is slowly titrated upward to determine an optimal dose that gives the best seizure control with minimal side effects.9 All benzodiazepines can cause amnesia, sedation, respiratory depression, and coma.11 As side effects depend on dose and duration of action, choices of an adequate dose and of a short half-life drug are important factors.11 Underdosing of benzodiazepines is therefore common for fear of respiratory depression.11
What Are the Characteristics of Midazolam and Lorazepam?
Midazolam is a short-acting benzodiazepine with a relatively rapid onset of action (within 2 minutes after IM injection) and a relatively short half-life of 1 to 4 hours.11 The duration of action is 1 to 2 hours.12 This drug exhibits anxiolytic, muscle relaxant, anticonvulsant, sedative, hypnotic, and amnesic properties.11 Midazolam formulations are available by oral (tablet or syrup), rectal, intranasal, IM, IV, or buccal.11 Midazolam injection (solution, 1 mg/mL and 5 mg/mL, IV and IM) has been approved for use in various biomedical applications, including surgical or diagnostic procedures, endoscopic procedures, anesthesia, and sedation during intubation for mechanical ventilation in the intensive care unit (ICU).13 Midazolam administered through IM route has been recommended for adult status epilepticus in the prehospital setting or where obtaining IV access is not available or challenging in patients with ongoing convulsions.10
Lorazepam is a benzodiazepine with a fast onset of action (1 to 3 minutes after IV injection) and a relatively intermediate half-life of 8 to 25 hours. The duration of action is about 10 to 20 hours.11 This drug has anticonvulsant, sedative, hypnotic, and anti-anxiety properties.11 Available routes of delivery of lorazepam include oral, sublingual, IM, and IV.11 Lorazepam injection (solution, 4 mg/mL, IM and IV) has been approved for use in adults for anxiety relief, in patients with anxiety neurosis or before surgical intervention, and as an anticonvulsant drug for the control of status epilepticus.14
Why Is It Important to Do This Review?
The American Epilepsy Society guideline has a treatment algorithm for status epilepticus, which starts with a stabilizing phase (0 to 5 minutes), followed by an initial therapy phase (5 to 20 minutes) using a benzodiazepine as first choice in children and adults in a prehospital setting or in-hospital setting.15 One of the 3 equivalent first-line options is IM midazolam (10 mg for > 40 kg, 5 mg for 13 to 40 kg, single dose), IV lorazepam (0.1 mg/kg, a maximum single dose of 4 mg, may repeat dose once), or IV diazepam (0.15 to 0.2 mg/kg, a maximum single dose of 10 mg, may repeat dose once).15 If the abovementioned 3 options are not available, the guideline recommends using IV phenobarbital, rectal diazepam, or intranasal midazolam.15
In the prehospital setting, many emergency paramedic services routinely use IM midazolam rather than IV lorazepam, although IV lorazepam is the most effective treatment and commonly used to treat seizures in the emergency department (ED).10,16,17 The preferred use of IM midazolam by paramedics in the prehospital setting highlights that IM administration is faster and easier to attain than IV administration, and lorazepam solution has a shorter shelf-life in the absence of refrigeration.16,18 Decision-makers want to know whether IM midazolam is as effective and safe as IV lorazepam for terminating seizures before arriving at the hospital, and whether paramedic protocols can be switched to using IV lorazepam to align with protocols in the in-hospital settings.
Objective
To support decision-making about whether paramedics should switch their protocols from using IM midazolam to IV lorazepam, we prepared this Rapid Review to summarize and critically appraise the available studies on the comparative clinical effectiveness and safety of midazolam and lorazepam in adults to control seizures.
Research Question
What are the clinical effectiveness and safety of midazolam compared to lorazepam in adults to control seizures?
Methods
Literature Search Methods
An information specialist conducted a literature search on key resources including MEDLINE, Embase, the Cochrane Database of Systematic Reviews, the International HTA Database, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search approach was customized to retrieve a limited set of results, balancing comprehensiveness with relevancy. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. Search concepts were developed based on the elements of the research questions and selection criteria. The main search concepts were midazolam and lorazepam and seizures. The search was completed on September 19, 2024, and limited to English-language documents published since January 1, 2019.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
|---|---|
Population | Adult patients experiencing seizures: First Nations, Inuit, and Métis populations, patients in remote or nursing station settings, patients without IV or IO access, patients with a risk of respiratory depression (prior use of barbiturates) |
Intervention | Midazolam in the treatment of seizures (acute, emergency setting) |
Comparator | Lorazepam in the treatment of seizures (acute, emergency setting) |
Outcomes | Effectiveness: time to seizure cessation (time from administration of the medication to the cessation of seizure activity); seizure recurrence rate (proportion of patients who experience seizure recurrence within a defined period [e.g., 24 hours] after initial treatment); need for additional dosing (percentage of patients requiring a second dose or additional rescue medication due to ongoing or recurrent seizures); Glasgow Outcome Scale (neurologic function and overall recovery postseizure) Safety: adverse effects, respiratory depression, hypotension, bradycardia following administration, rates of hospitalization or intensive care admission |
Study designs | HTAs, SRs with or without MA or NMA, RCTs |
HTA = health technology assessment; IO = intraosseous; MA = meta-analysis; NMA = network meta-analysis; RCT = randomized controlled trial; SR = systematic review.
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1 or were published before 2019.
Critical Appraisal of Individual Studies
The included publication was critically appraised by 1 reviewer using A Measurement Tool to Assess Systematic Reviews 2 (AMSTAR 2)19 for SR. Summary scores were not calculated for the included studies; rather, the strengths and weaknesses of the included publication were described narratively.
Summary of Evidence
Quantity of Research Available
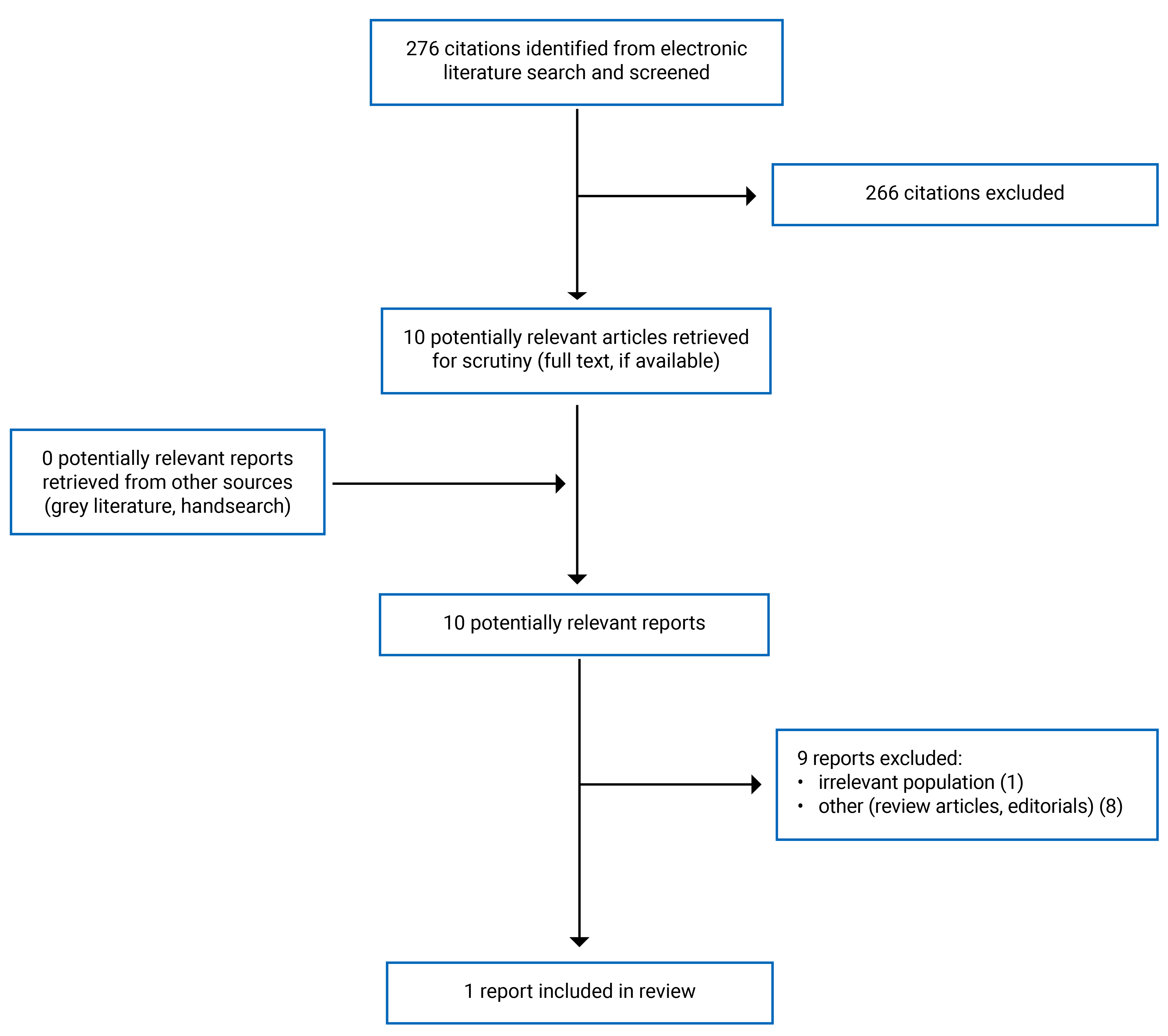
We identified a total of 276 citations from the literature search. Following screening of titles and abstracts, we excluded 266 citations and retrieved 10 potentially relevant reports from the electronic search for full-text review. We found no potentially relevant publications from the grey literature search. Of the 10 potentially relevant articles, we excluded 9 publications for various reasons, and included 1 publication (i.e., SR) that met the inclusion criteria. Appendix 1 presents the PRISMA20 flow chart of the study selection.
Summary of Study Characteristics
Table 2 provides details regarding the characteristics of the included SR.21
Included studies for the research question: what are the clinical effectiveness and safety of midazolam compared to lorazepam in adults to control seizures?
Study Design
The identified SR21 included 4 RCTs, of which only 1 RCT was relevant for this review.
Country of Origin
The SR21 was conducted by authors in the UK.
Patient Population
The interested patient population included in the SR21 were adults with convulsive status epilepticus from the RAMPART trial by Silbergleit et al., who recruited adults (89%) and children (11%) with a body weight of at least 13 kg.22 The authors of the SR21 obtained a dataset of participant-level data by contacting the authors of the RAMPART trial,22 and extracted data of 782 participants aged older than 16 years. Mean age was 48 years in the IM midazolam group and 49 years in the IV lorazepam group. The proportion of male to female was similar in both groups. Most patients in both groups (about 90%) had status epilepticus.
Intervention and Comparator
The RAMPART trial22 was a double-blind, randomized, noninferiority trial comparing the efficacy and safety of IM midazolam with IV lorazepam for children and adults with status epilepticus treated by paramedics. Patients with an estimated body weight of more than 40 kg received either 10 mg IM midazolam followed by IV placebo or IM placebo followed by IV lorazepam.
Outcomes
The outcomes presented in the SR21 were seizure cessation, recurrence of seizure, and adverse events (AEs). Seizure cessation was reported as the proportion of people with cessation of seizure activity and time to seizure cessation from administration of the study drug. Recurrence of seizures was reported as proportion of people with recurrence of seizures. AEs were reported as mortality rates of the adult population and respiratory depression rates of the whole population of the RAMPART trial.22 In addition to the outcomes for adults as reported in the SR,21 we also referred to the pivotal RAMPART trial22 to extract all primary and secondary outcomes for the intention to treat (ITT) population that were not reported in the SR. Additional outcomes included endotracheal intubation, hypotension, hospital admission, ICU admission, hospital length of stay, and ICU length of stay.
Summary of Critical Appraisal
Table 3 provides details regarding the strengths and weaknesses of the included SR.21
The included SR21 was explicit in its objective, inclusion criteria for the review, literature search strategy, and selection of the study designs for inclusion. The authors of the SR registered the research protocol (PROSPERO) before conducting the review. The study selection, data extraction, and critical appraisal of the included studies were performed independently by 2 reviewers. Disagreements were resolved by discussion or consultation with a third review author. Critical appraisal was conducted using a revised Cochrane risk of bias tool for randomized trials. The characteristics of the included studies were described in adequate details, including study design, intervention, control, and outcomes. Patient characteristics were adequately described. The authors of the SR provided a list of excluded studies and the reasons for exclusion. The review authors declared that they had no conflicts of interest related to this work. Overall, the methodology of the included SR was robust.
Summary of Findings
Table 4 presents the main study findings, which were summarized as clinical outcomes and safety outcomes.
Clinical Effectiveness Outcomes of Midazolam Compared to Lorazepam in Adults to Control Seizures
Table 4 presents the summary of clinical outcomes of the adult population and the ITT population.
Seizure Cessation
Seizures were terminated without rescue therapy before arrival in the ED in 73.9% (289 of 391) of adult patients treated with IM midazolam and in 62.4% (244 of 391) of patients treated with IV lorazepam. Statistical comparisons were not reported. The results were similar to those of the entire ITT population (i.e., 73.4% versus 63.4% for IM midazolam versus IV lorazepam, respectively; P < 0.001).
Among adult patients whose seizures ceased before arrival in the ED, the median time from administration of the study drug to seizure cessation (i.e., onset of action) was 3 minutes (range, 2 minutes to 6.3 minutes) for IM midazolam and 2 minutes (range, 1 minute to 4.4 minutes) for IV lorazepam. Similarly, the onset of action of the study drugs in the ITT population occurred longer after IM than after IV administration (3.3 minutes versus 1.6 minutes), but the median time required to administration of active treatment was shorter by the IM route than by the IV route (1.2 minutes versus 4.8 minutes). However, the overall interval from the start of drug administration to the termination of seizures was similar in both groups (data shown in a graphical form).
Recurrence of Seizures
Within 12 hours after ED arrival, seizures reoccurred in 12.0% (47 of 391) of adult patients in the IM midazolam group and in 10.7% (42 of 391) of those in the IV lorazepam group. The results were similar to the entire ITT population (i.e., 11.4% versus 10.6% for IM midazolam versus IV lorazepam, respectively). Statistical comparisons were not reported.
Safety Outcomes of Midazolam Compared to Lorazepam in Adults to Control Seizures
Table 5 presents the summary of safety outcomes mostly of the ITT population obtained from the RAMPART trial.22 The SR21 only reported the mortality rates of the adult population.
Respiratory Depression
Among all patients who were enrolled and underwent randomization, respiratory depression occurred in 6.4% (33 of 514) of patients who received IM midazolam and in 10.0% (47 of 509) of patients who received IV lorazepam. Statistical comparisons were not reported.
Mortality
Mortality rates among adult patients receiving IM midazolam and IV lorazepam were 2.8% (11 of 391) and 2.0% (8 of 391), respectively. Statistical comparisons were not reported. No mortality rates for the ITT population were reported.22
Endotracheal Intubation
The frequencies of endotracheal intubation were similar in the 2 study groups of the ITT population. The relative risk (RR) was 0.98 with a 95% confidence interval (CI) of 0.70 to 1.34.
Hypotension
The frequencies of hypotension were similar in the 2 study groups of the ITT population (RR = 0.92; 95% CI, 0.42 to 1.98).
Hospitalization
The proportion of patients in the ITT population admitted to the hospital was statistically significantly lower in the IM midazolam group than in the IV lorazepam group (RR = 0.88; 95% CI, 0.79 to 0.98).
ICU Admission
The proportion of patients in the ITT population admitted to the ICU was statistically significantly lower in the IM midazolam group than in the IV lorazepam group (RR = 0.79; 95% CI, 0.65 to 0.95).
Length of Stay in the Hospital
The length of stay in the hospital did not statistically significantly differ between groups of the ITT population (P = 0.11).
Length of Stay in the ICU
The length of stay in the ICU did not statistically significantly differ between groups of the ITT population (P = 0.09).
Limitations
Evidence Gaps
No actual trials were found for the comparison of the efficacy and safety of midazolam versus lorazepam in adults with seizures. The authors of the included SR21 were able to access the individual participant data of the RAMPART trial,22 and conduct the analysis of the 782 participants aged older than 16 years. However, the authors of the SR21 that performed the subanalysis for the adult population did not have a statistical plan for the comparisons of outcomes between groups.
Generalizability
Subanalysis of data from a single trial (RAMPART) published in 2012 limited the generalizability of the findings to the general adult patient population. However, evidence from the RAMPART trial22 suggested that IM midazolam is as safe and effective as IV lorazepam for prehospital seizure cessation in both children and adults.
Certainty of Evidence
It remains uncertain regarding the comparative clinical efficacy and safety of midazolam and lorazepam in adults with seizures, as the sample size of adults extracted from the RAMPART trial may have inadequate power to detect clinically important differences between midazolam and lorazepam.
Conclusions and Implications for Decision- or Policy-Making
This review included 1 SR21 that included 4 RCTs, but only 1 was relevant to the research question. The RAMPART trial22 was a double-blind, randomized, noninferiority trial comparing the efficacy and safety of IM midazolam with IV lorazepam for children and adults with seizures treated by paramedics. The authors of the SR obtained the available dataset of participant-level data, extracted data for the 782 participants aged older than 16 years, and narratively summarized each outcome without performing any statistical comparisons. We therefore referred to the RAMPART trial22 to present the outcomes that were not reported in the SR.
Among the adult population, seizures were stopped without rescue therapy at the time of arrival in the ED in 73.9% of the IM midazolam group and in 62.4% of the IV lorazepam group. The findings were similar with the ITT population showing that prehospital treatment with IM midazolam was as effective as IV lorazepam (73.4% versus 63.4%; P < 0.001). The noninferiority of IM midazolam compared with IV lorazepam in the ITT population was supported by highlighting that the frequencies of recurrence of seizures, endotracheal intubation, and other safety outcomes such as respiratory depression, and hypotension were similar between the 2 treatment groups. The proportion of patients of the ITT population admitted to the hospital or the ICU was statistically significantly lower in the IM midazolam group than the IV lorazepam group, but there were no differences in the length of stay. Given that the overall interval from the starting of drug administration to the termination of seizures was similar in both groups, the time required to deliver midazolam intramuscularly was shorter compared to IV lorazepam, lorazepam was less stable when not refrigerated, and IM midazolam was as effective and safe as IV lorazepam. Switching of IM midazolam to IV lorazepam for treatment of seizures by paramedics may not be practical.
Considerations for Future Research
Future clinical trials comparing midazolam to lorazepam using different administration routes would provide useful information to inform the management of seizures in adults, especially for prehospital settings when IV access is not feasible.
Implications for Clinical Practice
Although the onset of action was more rapid after IV administration than after IM administration, the longer time required to administration of lorazepam by the IV route versus administration of midazolam by the IM route suggested that establishing IV access in the prehospital setting can be challenging and time-consuming. Since IM administration is more readily accessible and has comparable efficacy with IV administration, the use of IM midazolam may be a better option for treatment of seizures in the prehospital environment.
References
1.Huff JS, Murr NI. Seizure. StatPearls. Treasure Island (FL): StatPearls Publishing LLC.; 2024.
2.Johns Hopkins Medicine. Types of Seizures. 2024; https://www.hopkinsmedicine.org/health/conditions-and-diseases/epilepsy/types-of-seizures. Accessed 2024 Sep 25.
3.Mayo Clinic. Seizures. 2023; https://www.mayoclinic.org/diseases-conditions/seizure/symptoms-causes/syc-20365711. Accessed 2024 Sep 25.
4.Cleveland Clinic. Seizure: What it is, Causes, Symptoms, Treatment & Types. 2024; https://my.clevelandclinic.org/health/diseases/22789-seizure. Accessed 2024 Sep 25.
5.Fisher RS, Acevedo C, Arzimanoglou A, et al. ILAE official report: a practical clinical definition of epilepsy. Epilepsia. 2014;55(4):475-482. PubMed
6.The Epilepsies and Seizures: Hope Through Research. Bethesda (MD): National Institute of Neurological Disorders and Stroke; 2018: https://eabb.org/wp-content/uploads/2023/01/epilepsies-seizures-hope-through-research.pdf. Accessed 2024 Sep 25.
7.Epilepsy in Canada. Ottawa (ON): Public Health Agency of Canada; 2024: https://www.canada.ca/en/public-health/services/publications/diseases-conditions/epilepsy.html. Accessed 2024 Sep 25.
8.Betjemann JP. Current Trends in Treatment of Status Epilepticus and Refractory Status Epilepticus. Semin Neurol. 2015;35(6):621-628. PubMed
9.National Institute of Neurological Disorders and Stroke. Epilepsy and Seizures. 2024; https://www.ninds.nih.gov/health-information/disorders/epilepsy-and-seizures. Accessed 2024 Sep 25.
10.Bannouvong K, Coons C, Len S, Johnson K, Bhimji H. An overview of benzodiazepines for adult status epilepticus and the role of the emergency medicine pharmacist. J Emerg Crit Care Med. 2024;8:10.
11.Kienitz R, Kay L, Beuchat I, et al. Benzodiazepines in the Management of Seizures and Status Epilepticus: A Review of Routes of Delivery, Pharmacokinetics, Efficacy, and Tolerability. CNS Drugs. 2022;36(9):951-975. PubMed
12.Olkkola KT, Ahonen J. Midazolam and other benzodiazepines. Handb Exp Pharmacol. 2008(182):335-360. PubMed
13.Midazolam Injection USP (midazolam): solution, 1 mg / ml and 5 mg / ml, intramuscular, intravenous [product monograph]. Kirkland (QC): Pfizer Canada ULC; 2023: https://pdf.hres.ca/dpd_pm/00069010.PDF. Accessed 2024 Sep 25.
14.Lorazepam Injection USP (lorazepam): sterile solution (4 mg/mL) [product monograph]. Kirkland (QC): Pfizer Canada ULC; 2019: https://pdf.hres.ca/dpd_pm/00052835.PDF. Accessed 2024 Sep 25.
15.Glauser T, Shinnar S, Gloss D, et al. Evidence-Based Guideline: Treatment of Convulsive Status Epilepticus in Children and Adults: Report of the Guideline Committee of the American Epilepsy Society. Epilepsy Curr. 2016;16(1):48-61. PubMed
16.Billington M, Kandalaft OR, Aisiku IP. Adult Status Epilepticus: A Review of the Prehospital and Emergency Department Management. J Clin Med. 2016;5(9). PubMed
17.Silverman EC, Sporer KA, Lemieux JM, et al. Prehospital Care for the Adult and Pediatric Seizure Patient: Current Evidence-based Recommendations. West J Emerg Med. 2017;18(3):419-436. PubMed
18.Alldredge BK, Gelb AM, Isaacs SM, et al. A comparison of lorazepam, diazepam, and placebo for the treatment of out-of-hospital status epilepticus. N Engl J Med. 2001;345(9):631-637. PubMed
19.Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. PubMed
20.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
21.Cruickshank M, Imamura M, Counsell C, et al. Management of the first stage of convulsive status epilepticus in adults: a systematic review of current randomised evidence. J Neurol. 2022;269(7):3420-3429. PubMed
22.Silbergleit R, Durkalski V, Lowenstein D, et al. Intramuscular versus intravenous therapy for prehospital status epilepticus. N Engl J Med. 2012;366(7):591-600. PubMed
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publication
Note that this appendix has not been copy-edited.
Table 2: Characteristics of Included Systematic Review
Study citation, country, funding source | Study design, outcomes | Intervention and comparators | Included studies | Population characteristics |
|---|---|---|---|---|
Cruickshank et al. (2022)21 UK Funding source: National Institute for Health Research | SR Outcomes:
| Intervention: IM MDZ (N = 391) Comparator: IV LZP (N = 391) | 4 RCTs, but only 1 relevant RCT – the RAMPART trial (double-blind, randomized, noninferiority trial)22 Setting: paramedics Number of centres: NR (4,314 paramedics, 33 emergency medical services, and 79 receiving hospitals) Country: US Duration of follow-up: NR (participants were followed for duration of hospital stay, an average of 6 days) | The RAMPART trial recruited adults and children with body weight at least 13 kg (N = 893). The authors of the SR obtained a publicly available dataset of participant-level data and extracted data for the 782 participants over 16 years of age. Mean age (SD), years:
Gender (M/F), n (%)
Diagnosis, n (%):
|
AE = adverse event; F = female; IM = intramuscular; IV = IV; LZP = lorazepam; M = male; MDZ = midazolam; NE = nonepileptic; NR = not reported; RCT = randomized controlled trial; SE = status epilepticus; SD = standard deviation; UD = undetermined.
Appendix 3: Critical Appraisal of Included Publication
Note that this appendix has not been copy-edited.
Table 3: Strengths and Weaknesses of Systematic Review Using AMSTAR 219
Strengths | Weaknesses |
|---|---|
Cruickshank et al. (2022)21 | |
|
|
AMSTAR 2 = A MeaSurement Tool to Assess systematic Reviews 2; PICO = population, intervention, comparator, and outcome; RCT = randomized controlled trial; SR = systematic review.
Appendix 4: Main Study Findings
Note that this appendix has not been copy-edited.
Table 4: Summary of Clinical Outcomes
Study Citation and Study Design | Outcomes | Results | Notes |
|---|---|---|---|
Cruickshank et al. (2022)21 SR Included study:
ITT population:
Adult population:
| Seizure cessation | ||
Number of people experiencing seizure cessation, n/N (%) | Adults only:
Entire population (ITT):
| Seizures were terminated before arrival in the ED without the need for rescue therapy. No statistical comparison was performed for the adult population. | |
Median time needed to administer the medication, minutes | Adults only:
Entire population (ITT):
| Among patients whose seizures ceased before arrival in the ED. The median time to administration of active treatment was shorter by the IM route (1.2 vs. 4.8 minutes), but the onset of action (i.e., termination of seizures) occurred sooner after IV than after IM administration (1.6 vs. 3.3 minutes). However, the overall interval until termination of seizures was similar in both groups (data were shown in a graphical form). | |
Median time (IQR) to seizure cessation from administration of study drug, minutes | Adults only:
Entire population (ITT):
| ||
Recurrence of seizures | |||
Number of people with recurrence of seizures, n/N (%) | Adults only:
Entire population (ITT):
| Within 12 hours after ED arrival | |
ED = emergency department; IM = intramuscular; IQR = interquartile range; ITT = intention to treat; IV = IV; MDZ = midazolam; LZP = lorazepam; SR = systematic review.
Table 5: Summary of Safety Outcomes
Study Citation and Study Design | Outcomes | Results | Notes |
|---|---|---|---|
Cruickshank et al. (2022)21 SR Included study:
ITT population:
Adult population:
| Respiratory depression, n/N (%) | Adults only:
Total randomized enrolments:
| Data for adult population were not reported in the SR. The SR reported data of all enrolled participants. |
Mortality, n/N (%) | Adults only:
Entire population (ITT):
| Data for adult population were reported in the SR. Data for ITT population were not reported in the pivotal trial.22 | |
Endotracheal intubation, n/N (%) | Adults only:
Entire population (ITT):
| Data for adult population were not reported in the SR. Data for ITT population were obtained from the pivotal trial.22 Within 30 minutes after ED arrival | |
Hypotension, n/N (%) | Adults only:
Entire population (ITT):
| Data for adult population were not reported in the SR. Data for ITT population were obtained from the pivotal trial.22 | |
Hospitalization, n/N (%) | Adults only:
Entire population (ITT):
| Data for adult population were not reported in the SR. Data for ITT population were obtained from the pivotal trial.22 | |
Mean (SD) length of hospital stay, days | Adults only:
Entire population (ITT):
| Data for adult population were not reported. Data for ITT population were obtained from the pivotal trial.22 Number of patients with length of stay data:
| |
ICU admission, n/N (%) | Adults only:
Entire population (ITT):
| Data for adult population were not reported in the SR. Data for ITT population were obtained from the pivotal trial.22 | |
Mean (SD) length of ICU stay, days | Adults only:
Entire population (ITT):
| Data for adult population were not reported. Data for ITT population were obtained from the pivotal trial.22 Number of patients with length of stay data:
|
ED = emergency department; ICU = intensive care unit; IM = intramuscular; IQR = interquartile range; ITT = intention to treat; IV = IV; MDZ = midazolam; LZP = lorazepam; NR = not reported; RAMPART = Rapid Anticonvulsant Medication Prior to Arrival Trial; RR = relative risk; SD = standard deviation; SR = systematic review.
ISSN: 2563-6596
Canada’s Drug Agency (CDA-AMC) is a pan-Canadian health organization. Created and funded by Canada’s federal, provincial, and territorial governments, we’re responsible for driving better coordination, alignment, and public value within Canada’s drug and health technology landscape. We provide Canada’s health system leaders with independent evidence and advice so they can make informed drug, health technology, and health system decisions, and we collaborate with national and international partners to enhance our collective impact.
Disclaimer: CDA-AMC has taken care to ensure that the information in this document was accurate, complete, and up to date when it was published, but does not make any guarantee to that effect. Your use of this information is subject to this disclaimer and the Terms of Use at cda-amc.ca.
The information in this document is made available for informational and educational purposes only and should not be used as a substitute for professional medical advice, the application of clinical judgment in respect of the care of a particular patient, or other professional judgments in any decision-making process. You assume full responsibility for the use of the information and rely on it at your own risk.
CDA-AMC does not endorse any information, drugs, therapies, treatments, products, processes, or services. The views and opinions of third parties published in this document do not necessarily reflect those of CDA-AMC. The copyright and other intellectual property rights in this document are owned by the Canadian Agency for Drugs and Technologies in Health (operating as CDA-AMC) and its licensors.
Questions or requests for information about this report can be directed to Requests@CDA-AMC.ca.