CADTH Health Technology Review
Lenvatinib for the Treatment of Hepatocellular Carcinoma After Liver Transplant
Rapid Review
Key Messages
What Is the Issue?
Liver transplant is 1 of the main curative therapies for liver cancer; however, hepatocellular carcinoma (HCC) recurrence presents in 10% to 20% of patients after liver transplant.
Lenvatinib, an oral multikinase inhibitor drug, was approved for use in Canada as a first-line standard therapy for unresectable HCC, based on a pivotal trial that excluded patients who underwent a prior liver transplant.
Data were scarce on the efficacy and safety of lenvatinib for treatment of HCC recurrence in patients who received a liver transplant and were limited to a few case series and case reports.
What Did We Do?
We identified and summarized the literature on the evidence of the clinical effectiveness and safety of lenvatinib for the first-line treatment of patients with unresectable HCC recurrence after liver transplant.
We searched key resources, including journal citation databases and conducted a focused internet search for relevant evidence published since 2019. One reviewer screened citations for inclusion based on predefined criteria, critically appraised the included studies, and narratively summarized the findings.
What Did We Find?
We identified a multinational, multicentre, retrospective, single-arm chart review study evaluating the efficacy and safety of lenvatinib in patients with HCC recurrence after liver transplant. Lenvatinib was primarily used as a first-line treatment for most patients (n = 42; 93.3%) and as a second-line treatment for 3 patients (6.7%).
The single-arm chart review study showed lenvatinib treatment had an overall response rate (ORR) of 20.0%, a median overall survival (OS) of 14.5 months, and a median progression-free survival (PFS) of 7.6 months. These findings were similar to those randomized to lenvatinib in the pivotal phase III REFLECT trial, which excluded patients who had a prior liver transplant.
What Does This Mean?
The findings of this report suggest that lenvatinib has a potential role as a first-line treatment for patients with HCC recurrence after liver transplant.
As the current evidence is limited to a retrospective single-arm chart review study, which had several limitations (e.g., lack of sample size calculation, noncomparative, and retrospective design), further investigations are needed to establish the clinical efficacy and safety of lenvatinib as a first-line treatment for unresectable HCC recurrence after liver transplant.
Abbreviations
AE
adverse event
ALBI
albumin-bilirubin
BCLC
Barcelona Clinic Liver Cancer
CI
confidence interval
DCR
disease control rate
HCC
hepatocellular carcinoma
ORR
overall response rate
OS
overall survival
PFS
progression-free survival
RTK
receptor tyrosine kinase
Context and Policy Issues
What Is Liver Cancer?
HCC is the most common form of primary liver cancer, representing approximately 80% to 90% of patients.1 HCC is the sixth most common cancer and fourth leading cause of cancer-related death worldwide.1 In 2024, an estimated 4,700 people were diagnosed with liver cancer in Canada, and of these, 3,700 were expected to die from the disease.2 Men are more likely to be diagnosed with liver cancer and will die from it than women.2
Although it is rare, liver cancer is quite common in people with underlying liver disease.3 Many risk factors leading to the development of liver cancer include chronic liver disease, chronic viral infection with either hepatitis B or hepatitis C, certain types of inherited liver disease (e.g., hemochromatosis, alpha-1 antitrypsin deficiency, and tyrosinemia), liver cirrhosis, excessive alcohol intake, non-alcoholic fatty liver disease, tobacco use, and long-term use of anabolic steroids.3
Liver cancer is generally asymptomatic in the early stages.3 Most signs and symptoms (e.g., weight loss, loss of appetite, abdominal pain, yellow colouration of skin or eyes, and fluid in the abdomen) begin to appear when the disease has reached an advanced stage.3 Liver cancer can be diagnosed by ultrasound of the abdomen, blood test (check for increased levels of alpha-fetoprotein), CT scan, MRI, and liver biopsy.3
What Are the Treatment Approaches for HCC?
The treatment approaches of HCC is based on the extent of tumour spread (stage), the speed of tumour growth, and the patient’s overall health.3 There is a global consensus among clinicians to decide how HCC should be treated based on the Barcelona Clinic Liver Cancer (BCLC) staging system.1,4,5 There are 5 BCLC stages of HCC: very early (stage 0), early (stage A), intermediate (stage B), advanced (stage C), and end stage (stage D). Patients with stage 0 or stage A (localized liver cancer has not spread outside the liver, single tumour, and tumour size is less than 2 cm or 3 cm) are candidates for treatment with surgical resection, ablation, or liver transplant. Patients with stage B (many tumours in the liver, but the liver is still working well) are treated with local regional therapies such as transarterial chemoembolism, transarterial radioembolism, or systemic therapy. Patients with stage C (advanced HCC, liver cancer has not spread beyond the liver) are treated with systemic therapies. Certain patients with stage B or stage C with adequate downstaging can be candidates for liver transplant. There is no treatment for stage D liver cancer (liver cancer has spread from the liver to distant parts of the body).6 At this stage, treatment is focused on easing a patient’s pain and symptoms (palliative care).6
What Is Systemic Treatment?
Systemic treatment is reserved for certain patients with HCC in stages B and C, who will not benefit from regional treatment approaches.7 Recent approval of current systematic therapies and future potential combination approaches include tyrosine kinase inhibitors, immunotherapy, and combinations of targeted drugs with immunotherapy.7
Receptor tyrosine kinases (RTKs) are key regulators in many cellular processes, including differentiation, proliferation, and survival.7 Abnormal activation of RTKs (e.g., autocrine activation, amplification, mutations, or chromosomal rearrangements) would lead to the pathogenesis of HCC.7 Targeted therapy using monoclonal antibodies or tyrosine kinase inhibitors have been developed to inhibit those pathways.7 Sorafenib and lenvatinib are multitargeted tyrosine kinase inhibitors that inhibit various RTKs.8
Sorafenib (brand name Nexavar) was discovered in the late 1990s and approved for first-line treatment of advanced HCC in the US in 2007 and later worldwide.8 It was approved in Canada in 2014 for treatment of patients with unresectable HCC.9 For more than a decade, sorafenib was the only systemic drug proven to extend survival when used as a first-line treatment for advanced unresectable HCC compared with placebo.10
Lenvatinib (brand name Lenvima) was approved in 2018 for first-line treatment of advanced HCC initially in Japan and later in various countries including Canada.8,11 After multiple failed trials, lenvatinib was the first drug to show noninferiority to sorafenib in terms of OS for the treatment of patients with unresectable or metastatic HCC in the randomized, open-label, phase III, REFLECT trial in 2018.12 Lenvatinib showed statistically significant improvement for all secondary efficacy end points (PFS, time to progression, and objective response) across subgroups.12 The comparative efficacy and safety of lenvatinib compared with sorafenib in first-line treatment for unresectable HCC was later evaluated in a series of systematic reviews and meta-analyses.13-17 In 2019, the CADTH recommendation for lenvatinib for first-line treatment of unresectable HCC specifically excluded patients after liver transplant, based on the exclusion criteria of the REFLECT trial.18
Why Is It Important to Do This Review?
Although liver transplant offers the possibility of curing liver cancer, it has been reported that HCC recurrence presents in 10% to 20% of patients after liver transplant.19,20 The median time from liver transplant to HCC recurrence was 13 months (range, 2 months to 132 months).19 Patients with HCC recurrence after liver transplant represent a special subgroup among those with HCC, but were excluded from prospective studies of lenvatinib including the REFLECT trial.12,21,22 Data were scarce on the efficacy and safety of lenvatinib in patients with HCC recurrence after liver transplant and were limited to a few case series and case reports.23-25 Most studies of systemic therapy in patients with HCC recurrence after liver transplant involved sorafenib.26 The main limitation of sorafenib in patients with liver transplant was toxicity, often leading to dose reduction.27 As lenvatinib has been shown to be noninferior to sorafenib,12 it is therefore important to determine if there is any evidence that lenvatinib can be used as a first-line treatment option for patients with HCC recurrence after liver transplant.
Objective
To support decision-making about the role of lenvatinib after liver transplant, we prepared this Rapid Review to summarize and critically appraise the available studies on the clinical efficacy and safety of lenvatinib for the first-line treatment of patients with unresectable HCC recurrence after liver transplant.
Research Question
What is the clinical effectiveness and safety of lenvatinib for the first-line treatment of patients with unresectable HCC recurrence after liver transplant?
Methods
Literature Search Methods
An information specialist conducted a literature search on key resources including MEDLINE, Embase, the Cochrane Database of Systematic Reviews, the International HTA Database, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search was customized to retrieve a limited set of results, balancing comprehensiveness with relevancy. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. Search concepts were developed based on the elements of the research questions and selection criteria. The main search concepts were lenvatinib and HCC. Search filters were applied to limit retrieval to health technology assessments, systematic reviews, meta-analyses, indirect treatment comparisons, randomized controlled trials or controlled clinical trials, and guidelines. A second search was conducted using the concepts of lenvatinib and liver transplant, with no search filters applied. Conference abstracts were excluded from both searches. The searches were completed on July 23, 2024, and limited to English-language documents published since January 1, 2019.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
|---|---|
Population | Patients with unresectable hepatocellular carcinoma recurrence after liver transplant |
Intervention | Lenvatinib as first-line treatment |
Comparator | Sorafenib; radiofrequency ablation; transarterial chemoembolization; surgical resection; no treatment |
Outcomes | Clinical outcomes (e.g., objective response rate, progression-free survival, overall survival), safety outcomes (e.g., treatment-related adverse events), and patient-reported outcomes (e.g., health-related quality of life) |
Study designs | Health technology assessments, systematic reviews, randomized controlled trials, nonrandomized studies |
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1 or were published before 2019.
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the Downs and Black checklist28 for nonrandomized study. Summary scores were not calculated for the included study; rather, the strengths and limitations of the included publication were described narratively.
Summary of Evidence
Quantity of Research Available
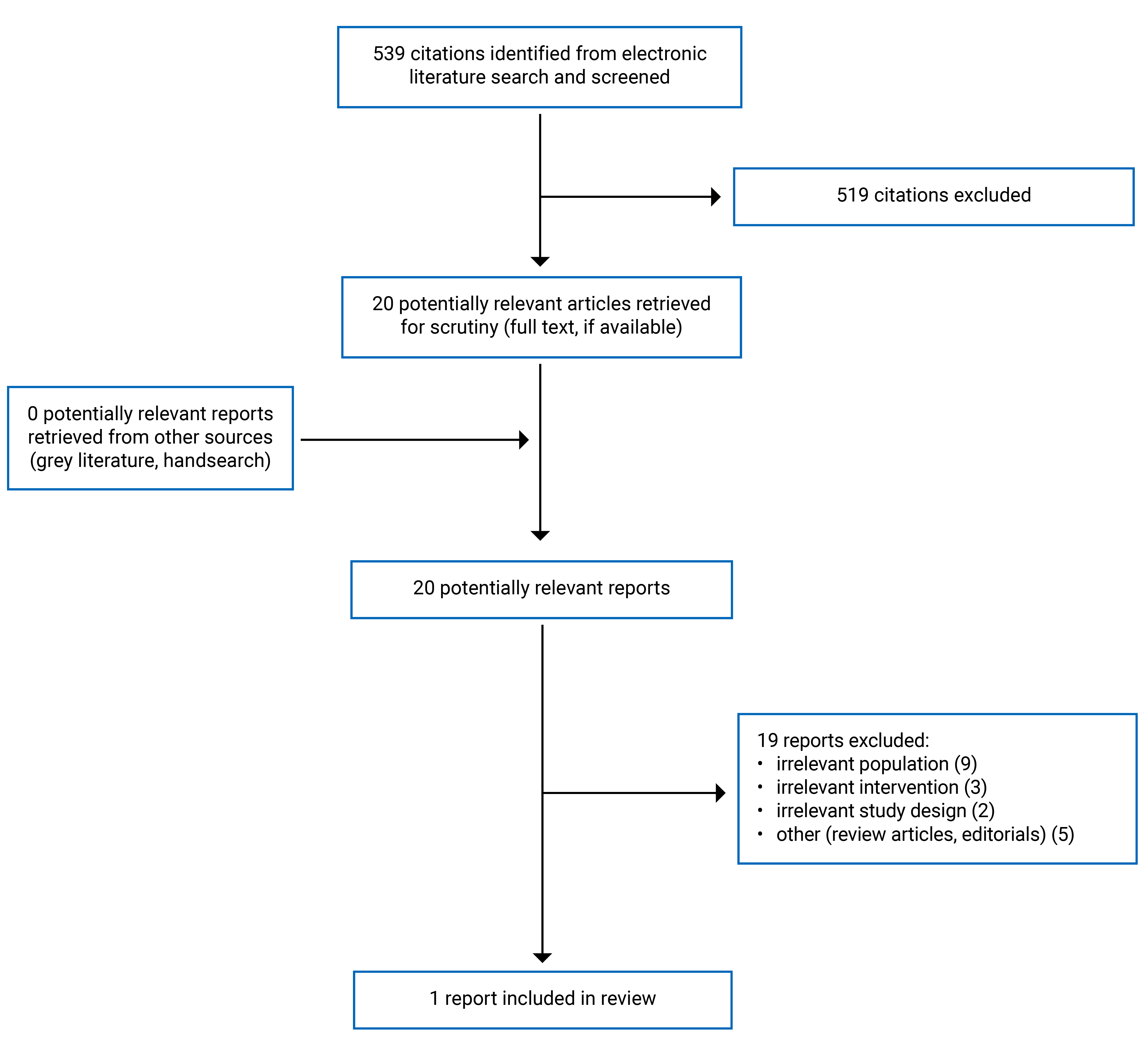
We identified a total of 539 citations from the literature search. Following screening of titles and abstracts, we excluded 519 citations and retrieved 20 potentially relevant reports from the electronic search for full-text review. We found no potentially relevant publications from the grey literature search. Of the 20 potentially relevant articles, we excluded 19 publications for various reasons and included 1 publication that met the inclusion criteria. Appendix 1 shows the PRISMA29 flow chart of the study selection (Figure 1).
Summary of Study Characteristics
Appendix 2 provides details regarding the characteristics of the included primary study (Table 2).30
Study Design
The included primary study was a multinational, multicentre, retrospective, single-arm chart review study.30
Country of Origin
The included study was conducted by authors in South Korea, Italy, and Hong Kong.30
Patient Population
The study retrospectively reviewed the electronic medical records of 45 patients with HCC recurrence or metastasis after receiving liver transplant; most patients were male (95.6%) and the median age was 59 years (range, 20 to 87 years). Patients had an Eastern Cooperative Oncology Group performance status of 0 (42.2%) or 1 (57.8%). Most patients had the least severe form of liver disease (95.4% Child-Pugh score A), the lowest mortality risk (77.8% albumin-bilirubin [ALBI] grade 1), and advanced HCC (91.1% BCLC stage C). The most common etiology was hepatitis B (55.6%) and hepatitis C (24.4%). The median time to recurrence of HCC after liver transplant was 22.4 months (range, 4.2 months to 231.9 months).
Intervention
The median time between liver transplant and the initiation of lenvatinib was 28.1 months (range, 4.2 months to 231.9 months). Most patients (99.3%) received lenvatinib as first-line treatment. Three patients (6.7%) received lenvatinib as second-line treatment after progression on sorafenib. The dosage of lenvatinib was 12 mg/day or 8 mg/day for patients with a body weight of at least 60 kg or less than 60 kg, respectively, as described in the REFLECT trial.12 Dose reduction (8 mg/day or 4 mg/day) was allowed at the discretion of the attending physicians. The median duration of lenvatinib treatment was 6.6 months (range, 0.1 months to 20.0 months).
Outcomes
Efficacy outcomes included best responses to treatment (e.g., complete response, partial response, stable disease, or progressive disease), ORR, disease control rate (DCR), time to response, PFS, and OS. Tumour response was assessed according to the Response Evaluation Criteria in Solid Tumors version 1.1 (RECIST v1.1). ORR is defined as the proportion of patients who have a complete or partial response to therapy. DCR is defined as the proportion of patients with advanced or metastatic cancer who have experienced complete response, partial response, or stabilized disease with a therapeutic intervention.
For safety outcomes, all treatment-related adverse events (AEs) were graded according to the National Cancer Institute Common Terminology Criteria for Adverse Events version 5.0.
Summary of Critical Appraisal
Appendix 3 provides details regarding the strengths and limitations of the included primary study30 (Table 3).
The study by Bang et al.30 was explicit in terms of reporting (i.e., objectives, intervention of interest, main outcomes, main findings, and characteristics of the participants). AEs of the intervention and actual P values for the main outcomes were reported. For external validity, the study was conducted in a hospital setting, where all patients with cancer were treated. Patients in the study may not be representative of the entire population from which they were recruited, owing to the small sample size. For internal validity related to bias, the included study had a high risk of selection bias owing to the retrospective design. For internal validity related to confounding, despite that electronic medical records of all patients were reviewed from multiple centres within the same period, limitations included lack of sample size calculation and lack of identification and adjustment for potential confounders in the analyses. Overall, the included study had several limitations related to external validity, internal validity related to bias, and internal validity related to confounding that may reduce the certainty of the findings.
Summary of Findings
Appendix 4 presents the main study findings, which were summarized as efficacy of lenvatinib (Table 4), and safety profiles of lenvatinib (Table 5) for the first-line treatment of patients with HCC recurrence after liver transplant.
Clinical Efficacy of Lenvatinib
The proportions of patients treated with lenvatinib experiencing partial response, stable disease, and progressive disease were 20%, 68.9%, and 6.7%, respectively. None of the patients experienced complete response. Thus, the ORR was 20% and the DCR was 88.9%. Among patients who experienced a response (in this case was partial response), the median time to response was 2.4 months (range, 1.5 months to 7.4 months).
With a median follow-up duration of 12.9 months (95% confidence interval [CI], 11.2 months to 14.7 months), the median OS was 14.5 months (95% CI, 0.8 months to 28.2 months), and the median PFS was 7.6 months (95% CI, 5.3 months to 9.8 months). The 6-month OS rate and 6-month PFS rate were 86.0% and 60.1%, respectively.
Exploratory analysis revealed that patients with ALBI grade 1 had a statistically significant higher median OS (52.3 months; 95% CI not assessable) compared with patients with ALBI grade 2 (11.1 months; 95% CI, 0.0 months to 30.4 months; P = 0.003). Patients with ALBI grade 1 had numerically higher median PFS (8.0 months; 95% CI, 5.2 months to 10.8 months) compared with patients with ALBI grade 2 (3.0 months; 95% CI, 0.0 months to 7.5 months; P = 0.078).
During lenvatinib therapy, 31 patients (68.9%) had HCC progression, and 22 patients (71.0%) received subsequent treatment with second-line systemic therapy, mostly sorafenib.
Safety Profiles of Lenvatinib
The most common AEs of all grades associated with lenvatinib treatment were hypertension (n = 25, 55.6%), fatigue (n = 17, 37.8%), elevation of liver enzymes (n = 17, 37.8%), and anorexia (n = 14, 31.1%). The most common grade 3 to 4 AEs were hypertension (n = 9, 20.0%), neutropenia (n = 4, 8.9%), and fatigue (n = 4, 8.9%). Four patients (8.9%) discontinued lenvatinib owing to AEs (2 patients with grade 3 hypertension, 1 patient with grade 3 proteinuria, and 1 patient with grade 3 fatigue).
Twenty-two patients (48.9%) had lenvatinib therapy interruption or dose reduction. The most common reasons for dose reduction were fatigue (7 of 22, 31.8%), hypertension (4 of 22, 18.2%), and proteinuria (2 of 22, 9.1%).
Limitations
Evidence Gaps
No evidence was found for the clinical effectiveness and safety of lenvatinib compared with placebo or active comparators such as sorafenib, radiofrequency ablation, transarterial chemoembolism, or surgical resection as first-line treatments of patients with unresectable HCC recurrence after liver transplant. No conclusions can be formed on these aspects.
Generalizability
Most patients (95.6%) were male, which limited the generalizability of the results. Although patients were identified from 6 centres in 3 countries (i.e., South Korea, Italy, and Hong Kong), with 24 patients (53.3%) identifying as East Asian and 21 patients (46.7%) identifying as Caucasian [wording from original source], it is unclear if the findings could be generalized to the population in Canada.
Heterogeneity
Patients were heterogeneous in terms of sites of HCC recurrence or metastasis, mostly liver (64.4%) and lung (53.3%), followed by peritoneum (24.4%), bone (20.0%), and lymph nodes (17.8%). This may impact the overall findings.
Certainty of Evidence
Evidence on lenvatinib as first-line treatment of patients with HCC recurrence or metastasis after liver transplant remains uncertain as only 1 single-arm retrospective study was identified. The study design was a main limitation and included a high risk of bias. As 3 patients (6.7%) who received lenvatinib as second-line treatment after sorafenib were included in the study population, the current findings could not be considered as the results of first-line treatment with lenvatinib. Results for those 3 patients might not have a significant impact on the overall findings. The findings based on an exploratory analysis of ALBI grade remain to be determined as most patients (n = 35, 77.8%) were ALBI grade 1, while only 10 patients (22.2%) were ALBI grade 2. The findings based on ALBI grade should be considered as exploratory. Although the study had the largest number of patients with prior liver transplant so far in the literature, the current sample size may have insufficient power to perform multivariate analysis to define the prognostic factors from first-line therapy with lenvatinib.
Conclusions and Implications for Decision- or Policy-Making
This review included 1 single-arm retrospective study30 and evaluated the efficacy and safety of lenvatinib for first-line treatment of patients with unresectable HCC recurrence after liver transplant. Treatment with lenvatinib in this patient population showed an ORR and DCR of 20% and 88.9%, respectively. Moreover, the median OS and PFS were 14.5 months and 7.6 months, respectively. The most common AEs associated with lenvatinib treatment were hypertension, followed by elevation of liver enzyme, fatigue, and anorexia. Grade 3 to 4 AEs included hypertension, fatigue, and neutropenia.
The clinical efficacy and safety of lenvatinib were comparable with those of the pivotal phase III REFLECT trial, which excluded patients who had prior liver transplant. In the REFLECT trial, the ORR was 18.8%, and the median OS and median PFS for lenvatinib were 13.6 months and 7.4 months, respectively. Although it is not feasible to compare studies, the findings by Bang et al.30 suggested that lenvatinib might be effective as first-line treatment in patients with unresectable HCC recurrence after liver transplant.
Considerations for Future Research
Well-controlled, multicentre, prospective studies with larger patient populations are needed to establish the clinical efficacy and safety of lenvatinib as first-line treatment for unresectable HCC recurrence after liver transplant. It is also important to establish an optimal strategy for systemic therapy in patients with HCC recurrence following liver transplant. Further investigations are also needed to ascertain the correlation between better liver function (ALBI grade 1) with better survival outcomes in first-line treatment with lenvatinib for patients with HCC recurrence after liver transplant.
Implications for Clinical Practice
Although the current evidence is limited to a retrospective single-arm study, with several limitations, the findings suggest that lenvatinib has a potential role for first-line treatment of patients with HCC recurrence after liver transplant. Until stronger evidence is available, decision-makers should consider that the current findings from the included study are just preliminary experience that may form the basis for further investigation with well-controlled trials in the setting of liver transplant. Decision-makers may wish to consider other therapeutic strategies for patients with HCC recurrence after liver transplant that depend on location, multifocality, and clinical presentation of recurrence.27 The role of adjuvant lenvatinib for preventing HCC recurrence after liver transplant has also started to appear in the literature.31,32
References
1.Sankar K, Gong J, Osipov A, et al. Recent advances in the management of hepatocellular carcinoma. Clin Mol Hepatol. 2024;30(1):1-15. PubMed
2.Canadian Cancer Society. Liver cancer statistics. 2024; https://cancer.ca/en/cancer-information/cancer-types/liver/statistics. Accessed 2024 Jul 30.
3.Canadian Liver Foundation. Liver cancer and tumours. 2024; https://www.liver.ca/patients-caregivers/liver-diseases/liver-cancer/. Accessed 2024 Jul 30.
4.EASL Clinical Practice Guidelines: Management of hepatocellular carcinoma. J Hepatol. 2018;69(1):182-236. PubMed
5.Marrero JA, Kulik LM, Sirlin CB, et al. Diagnosis, staging, and management of hepatocellular carcinoma: 2018 practice guidance by the American Association for the Study of Liver Diseases. Hepatology. 2018;68(2):723-750. PubMed
6.Canadian Cancer Society. Treatments for stage D liver cancer. 2019; https://cancer.ca/en/cancer-information/cancer-types/liver/treatment/stage-d. Accessed 2024 Jul 30.
7.Becht R, Kiełbowski K, Wasilewicz MP. New opportunities in the systemic treatment of hepatocellular carcinoma - today and tomorrow. Int J Mol Sci. 2024;25(3). PubMed
8.Doycheva I, Thuluvath PJ. Systemic therapy for advanced hepatocellular carcinoma: An update of a rapidly evolving field. J Clin Exp Hepatol. 2019;9(5):588-596. PubMed
9.Nexavar (sorafenib): 200 mg tablets [product monograph]. Mississauga (ON): Bayer Inc.; 2014 Dec 17: https://pdf.hres.ca/dpd_pm/00028744.PDF. Accessed 2024 Jul 30.
10.Dipasquale A, Marinello A, Santoro A. A comparison of lenvatinib versus sorafenib in the first-line treatment of unresectable hepatocellular carcinoma: Selection criteria to guide physician's choice in a new therapeutic scenario. J Hepatocell Carcinoma. 2021;8:241-251. PubMed
11.Lenvima (lenvatinib): 4mg and 10mg capsules [product monograph]. Mississauga (ON): Eisai Limited; 2018 Dec 19: https://pdf.hres.ca/dpd_pm/00048812.PDF. Accessed 2024 Jul 31.
12.Kudo M, Finn RS, Qin S, et al. Lenvatinib versus sorafenib in first-line treatment of patients with unresectable hepatocellular carcinoma: A randomised phase 3 non-inferiority trial. Lancet. 2018;391(10126):1163-1173. PubMed
13.Hua X, Yin Z, Liang J, Chen W, Gong H. Efficacy and safety comparison between lenvatinib and sorafenib in hepatocellular carcinoma treatment: A systematic review and meta-analysis of real-world study. Eur J Gastroenterol Hepatol. 2024;36(1):120-128. PubMed
14.Hu L, Zheng Y, Lin J, Shi X, Wang A. Comparison of the effects of lenvatinib and sorafenib on survival in patients with advanced hepatocellular carcinoma: A systematic review and meta-analysis. Clin Res Hepatol Gastroenterol. 2023;47(1):102061. PubMed
15.Jaiswal V, Hameed M, Naz S, et al. Efficacy of lenvatinib versus sorafenib in the primary treatment of advanced hepatocellular carcinoma: A meta-analysis. JGH Open. 2023;7(12):832-840. PubMed
16.Luo J, Gao B, Lin Z, et al. Efficacy and safety of lenvatinib versus sorafenib in first-line treatment of advanced hepatocellular carcinoma: A meta-analysis. Front Oncol. 2022;12:1010726. PubMed
17.Wang S, Wang Y, Yu J, Wu H, Zhou Y. Lenvatinib as first-line treatment for unresectable hepatocellular carcinoma: A systematic review and meta-analysis. Cancers (Basel). 2022;14(22):10. PubMed
18.Drug Reimbursement Review clinical guidance report: Lenvatinib (Lenvima) for hepatocellular carcinoma. Ottawa (ON): CADTH; 2019 Jul 24: https://www.cda-amc.ca/sites/default/files/pcodr/Reviews2019/10175LenvatinibHCC_inCGR_NOREDACT_EarlyConv_Post_24Jul2019_final.pdf. Accessed 2024 Aug 13.
19.de'Angelis N, Landi F, Carra MC, Azoulay D. Managements of recurrent hepatocellular carcinoma after liver transplantation: A systematic review. World J Gastroenterol. 2015;21(39):11185-11198. PubMed
20.Fernandez-Sevilla E, Allard MA, Selten J, et al. Recurrence of hepatocellular carcinoma after liver transplantation: Is there a place for resection? Liver Transpl. 2017;23(4):440-447. PubMed
21.Ikeda K, Kudo M, Kawazoe S, et al. Phase 2 study of lenvatinib in patients with advanced hepatocellular carcinoma. J Gastroenterol. 2017;52(4):512-519. PubMed
22.Ikeda M, Okusaka T, Mitsunaga S, et al. Safety and pharmacokinetics of lenvatinib in patients with advanced hepatocellular carcinoma. Clin Cancer Res. 2016;22(6):1385-1394. PubMed
23.Pinero F, Thompson M, Marin JI, Silva M. Lenvatinib as first-line therapy for recurrent hepatocellular carcinoma after liver transplantation: Is the current evidence applicable to these patients? World J Transplant. 2020;10(11):297-306. PubMed
24.Chen YY, Chen CL, Lin CC, et al. Efficacy and safety of lenvatinib in hepatocellular carcinoma patients with liver transplantation: A case-control study. Cancers (Basel). 2021;13(18):12. PubMed
25.Ichida A, Akamatsu N, Nagata R, et al. Efficacy and safety of lenvatinib for the treatment of recurrent hepatocellular carcinoma after living donor liver transplantation: A report of two cases. Anticancer Res. 2022;42(2):1161-1167. PubMed
26.Mancuso A, Mazzola A, Cabibbo G, et al. Survival of patients treated with sorafenib for hepatocellular carcinoma recurrence after liver transplantation: A systematic review and meta-analysis. Dig Liver Dis. 2015;47(4):324-330. PubMed
27.Sposito C, Citterio D, Virdis M, et al. Therapeutic strategies for post-transplant recurrence of hepatocellular carcinoma. World J Gastroenterol. 2022;28(34):4929-4942. PubMed
28.Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377-384. PubMed
29.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
30.Bang K, Casadei-Gardini A, Yoo C, et al. Efficacy and safety of lenvatinib in patients with recurrent hepatocellular carcinoma after liver transplantation. Cancer Medicine. 2023;12(3):2572-2579. PubMed
31.Han B, Ding H, Zhao S, et al. Potential role of adjuvant lenvatinib in improving disease-free survival for patients with high-risk hepatitis B virus-related hepatocellular carcinoma following liver transplantation: a retrospective, case control study. Front Oncol. 2020;10:562103. PubMed
32.Guo DZ, Cheng JW, Yan JY, et al. Efficacy and safety of lenvatinib for preventing tumor recurrence after liver transplantation in hepatocellular carcinoma beyond the Milan criteria. Ann Transl Med. 2022;10(20):1091. PubMed
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Table 2: Characteristics of Included Primary Clinical Study
Study citation, country, funding source | Study design | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Bang et al. (2023)30 Korea, Italy, Hong Kong Funding source: No funding from any sources | Multinational, multicentre, retrospective, single-arm chart review study | Patients (N = 45) with recurrence HCC after LT Sex, n (%):
Median age (range), years: 59 (20 to 87) Etiology, n (%):
ECOG performance statusa, n (%):
Child-Pugh score,b n (%):
ALBI grade,c n (%):
Site of recurrence or metastasis, n (%):
BCLC stage,d n (%):
Treatment line with lenvatinib, n (%):
Median interval (range) between liver transplantation and initiation of lenvatinib, months:28.1 (4.2 to 231.9) | Intervention: Lenvatinib (12 or 8 mg/day for patients with body weight ≥ 60 kg or < 60 kg, respectively) Dose modification was 8 to 4 mg/day. Median (range) time between liver transplantation and the initiation of lenvatinib: 28.1 months (4.2 months to 231.9 months). Median (range) duration of lenvatinib treatment: 6.6 months (0.1 months to 20.0 months) Comparator: NA | Outcomes:
Median follow-up: 12.9 months (95% CI 11.2 to 14.7 months) (ORR is defined as the proportion of patients who have a complete or partial response to therapy.) (DCR is defined as the proportion of patients with advanced or metastatic cancer who have experienced complete response, partial response, and stable disease to a therapeutic intervention.) |
AE = adverse event; ALBI = albumin-bilirubin; BCLC = Barcelona Clinic Liver Cancer; CI = confidence interval; DCR = disease control rate; ECOG = Eastern Cooperative Oncology Group; HCC = hepatocellular carcinoma; LT = liver transplantation; NA = not applicable; ORR = overall response rate; OS = overall survival; PFS = progression-free survival; TTR = time to response.
aThe ECOG performance status scale indicates an increasing level of disability. 0 = fully active; 1 = restricted in strenuous activity; 2: restricted in work activity but ambulatory and capable of self-care.
bThe Child-Pugh score is a system for assessing the prognosis — including the required strength of treatment and necessity of liver transplant — of chronic liver disease, primarily cirrhosis. It provides a forecast of the increasing severity of your liver disease and your expected survival rate. A score of 1, 2, or 3 is given to each of the clinical measures of liver disease, including total bilirubin, serum albumin, prothrombin time, ascites, hepatic encephalopathy.
Class A: 5 to 6 points; least severe liver disease; 1- to 5-year survival rate: 95%
Class B: 7 to 9 points; moderately severe liver disease; 1- to 5-year survival rate: 75%
Class C: 10 to 15 points; most severe liver disease; 1- to 5-year survival rate: 50%
cThe ALBI score is an index of liver function that was developed to assess prognosis in patients with HCC, irrespective of the degree of underlying liver fibrosis.
Formula: (log10 bilirubin [μmol/L] × 0.66) + (albumin [g/L] × −0.0852)
Grade 1: −2.60 or lower
Grade 2: −2.60 to −1.39
Grade 3: −1.39 or higher
dThe BCLC staging system is used to predict the patient’s chance of recovery and to plan treatment based on the following: whether the cancer has spread within the liver or other parts of the body; how well the liver is working; the general health and wellness of the patient; the symptoms caused by the cancer
Stage 0: very early
Stage A: early
Stage B: intermediate
Stage C: advanced
Stage D: end-stage
Note: This table has not been copy-edited.
Appendix 3: Critical Appraisal of Included Publications
Please note that this appendix has not been copy-edited.
Table 3: Strengths and Limitations of Clinical Study Using the Downs and Black Checklist28
Strengths | Weaknesses |
|---|---|
Bang et al. (2023)30 | |
Reporting:
External validity:
Internal validity – bias:
Internal validity – confounding:
| Reporting:
External validity:
Internal validity – bias:
Internal validity – confounding:
|
Appendix 4: Main Study Findings
Please note that this appendix has not been copy-edited.
Table 4: Efficacy of Lenvatinib
Study citation and study design | Outcomes | Results | Notes |
|---|---|---|---|
Bang et al. (2023)30 Multinational, multicentre, retrospective, single-arm chart review study | Best response, n (%) |
| None of the patients experienced complete response. These were combined results from 93.3% of patients receiving lenvatinib as 1st line and 6.7% of patients receiving lenvatinib as 2nd line. The findings in the REFLECT trial for complete response, partial response, stable disease, progressive disease, and not evaluable were 1%, 23%, 51%, 15%, and 10%, respectively. |
ORR, % | 20 | Comparable with the REFLECT trial (18.8%) | |
DCR, % | 88.9 | Comparable with the REFLECT trial (75.5%) | |
Median TTR (range), months | 2.4 (1.5 to 7.4) | In patients who experienced PR | |
Median PFS, months (95% CI) | 7.6 (5.3 to 9.8) | Median follow-up: 12.9 months (95% CI 11.2 to 14.7 months) Comparable with the REFLECT trial (median OS 13.6 month; median PFS 7.4 months) | |
Median OS, months (95% CI) | 14.5 (0.8 to 28.2) | ||
6-month PFS rate, % | 60.1 | ||
6-month OS rate, % | 86.0 | ||
Median PFS, months (95% CI) by ALBI grade | ALBI grade 1: 8.0 (5.2 to 10.8) ALBI grade 2: 3.0 (0.0 to 7.5); P = 0.078 | Patients with ALBI grade 1 showed better OS and PFS. | |
Median OS, months (95% CI) by ALBI grade | ALBI grade 1: 52.3 (not assessable) ALBI grade 2: 11.1 (0.0 to 30.4); P = 0.003 | ||
Subsequent therapy, n (%) |
| Of 31 patients with HCC progression with lenvatinib, 22 (71.0%) received subsequent systemic therapy. |
ALBI = albumin-bilirubin; CI = confidence interval; DCR = disease control rate; ORR = overall response rate; OS = overall survival; PFS = progression-free survival; PR = partial response; TTR = time to response.
Table 5: Safety Profiles of Lenvatinib
Study citation and study design | Safety profiles | Results | Notes |
|---|---|---|---|
Bang et al. (2023)30 Multinational, multicentre, retrospective, single-arm chart review study | Therapy interruption or dose reduction, n (%) | 22 (48.9) | Reasons: fatigue (7 of 22, 31.8%); hypertension (4 of 22, 18.2%); and proteinuria (2 of 22, 9.1%) |
Discontinued lenvatinib due to AEs, n (%) | 4 (8.9) | AEs: grade 3 hypertension (n = 2); grade 3 proteinuria (n = 1); grade 3 fatigue (n = 1) | |
AEs occurred in > 5% of patients, n (%) | Any grade: 44 (97.8) Grade 1: 36 (80.0) Grade 2: 27 (60.0) Grade 3: 16 (25.6) | The most common AEs were hypertension (55.6%), followed by fatigue (37.8%), liver enzyme elevation (38.8%) and anorexia (31.1%). | |
Neutropenia, n (%) | Any grade: 7 (15.6) Grade 1: 1 (2.2) Grade 2: 2 (4.4) Grade 3: 4 (8.9) | ||
Anemia, n (%) | Any grade: 7 (15.6) Grade 1: 5 (11.1) Grade 2: 2 (4.4) Grade 3: 0 (0.0) | ||
Thrombocytopenia, n (%) | Any grade: 8 (17.8) Grade 1: 7 (15.6) Grade 2: 1 (2.2) Grade 3: 0 (0.0) | ||
Elevated AST/ALT, n (%) | Any grade: 17 (37.8) Grade 1: 14 (31.1) Grade 2: 3 (6.7) Grade 3: 0 (0.0) | ||
Elevated bilirubin, n (%) | Any grade: 4 (8.9) Grade 1: 4 (8.9) Grade 2: 0 (0.0) Grade 3: 0 (0.0) | ||
Hypothyroidism, n (%) | Any grade: 10 (22.2) Grade 1: 7 (15.6) Grade 2: 3 (6.7) Grade 3: 0 (0.0) | ||
Hypertension, n (%) | Any grade: 25 (55.6) Grade 1: 9 (20.0) Grade 2: 7 (15.6) Grade 3: 9 (20.0) | ||
Proteinuria, n (%) | Any grade: 10 (22.2) Grade 1: 3 (6.7) Grade 2: 5 (11.1) Grade 3: 2 (4.4) | ||
Fatigue, n (%) | Any grade: 17 (37.8) Grade 1: 8 (17.8) Grade 2: 5 (11.1) Grade 3: 4 (8.9) | ||
Anorexia, n (%) | Any grade: 14 (31.1) Grade 1: 9 (20.0) Grade 2: 4 (8.9) Grade 3: 1 (2.2) | ||
Diarrhea, n (%) | Any grade: 12 (26.7) Grade 1: 7 (15.6) Grade 2: 5 (11.1) Grade 3: 0 (0.0) | ||
Hand-foot syndrome, n (%) | Any grade: 7 (15.6) Grade 1: 6 (13.3) Grade 2: 1 (2.2) Grade 3: 0 (0.0) | ||
Oral mucositis, n (%) | Any grade: 6 (13.3) Grade 1: 6 (13.3) Grade 2: 0 (0.0) Grade 3: 0 (0.0) |
AE = adverse event; ALT = alanine aminotransferase; AST = aspartate aminotransferase.
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up to date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca