Drugs, Health Technologies, Health Systems
Health Technology Review
Early Biologic Treatment for Inflammatory Bowel Disease
Authors: Shu-Ching Hsieh, Xiaoqin Wang, Zemin Bai, Becky Skidmore, Shannon E. Kelly, Melissa Brouwers, George Wells
This rapid review was conducted by the Post-Market Drug Evaluation Team (PODET) through the Post Market Drug Evaluation CoLab Network.
Key Messages
This rapid review updates the evidence for early biologic treatment versus conventional step-up therapy for patients with luminal Crohn disease, fistulizing Crohn disease, or ulcerative colitis.
Findings are based on 4 systematic reviews, 2 randomized controlled trials, and 3 updated clinical guidelines.
Luminal Crohn Disease
Three systematic reviews showed that early biologic treatment, initiated within 36 months of diagnosis, significantly improved clinical remission, mucosal healing, and reduced relapse rates, surgery needs, and disease progression compared to conventional strategies. Two randomized controlled trials found that early infliximab treatment led to better remission rates, quality of life, and safety outcomes compared with conventional treatment for both adults and children with newly diagnosed moderate-to-severe Crohn disease. These results are consistent with previous evidence suggesting that early biologic drugs improve clinical benefits compared with conventional strategies.
Clinical guidelines generally recommend biologic drugs as third-line treatment. One guideline targets adults and children with severe, active Crohn disease, and another focuses on children and adolescents with luminal Crohn disease regardless of severity. Of these, 1 guideline recommends first-line biologics for high-risk pediatric patients.
Fistulizing Crohn Disease
One guideline recommends third-line infliximab for patients with active fistulizing Crohn disease who did not respond, did not tolerate or had a contraindication to conventional therapy. First-line anti–tumour necrosis factor therapy was only recommended for children and adolescents with fistulizing perianal Crohn disease. No evidence was identified for this population.
Ulcerative Colitis
In 1 systematic review, early biologics were found to be associated with a higher risk of colectomy. However, these findings should be interpreted with caution as they are based on evidence from 3 observational studies. One guideline recommends infliximab as a third-line option for acute severe cases contraindicated to or clinically inappropriate with ciclosporin.
Abbreviations
AE
adverse event
AGREE II
Appraisal of Guidelines for Research and Evaluation II
CD
Crohn disease
ECCO-ESPGHAN
European Crohn’s and Colitis Organization-European Society for Paediatric Gastroenterology Hepatology and Nutrition
FL-IFX
first-line infliximab
HTA
health technology assessment
IBD
inflammatory bowel disease
IFX
infliximab
NICE
National Institute for Health and Care Excellence
PICO
patient, intervention, comparison, and outcome
RCT
randomized controlled trials
SR
systematic review
TNF alpha
tumour necrosis factor alpha
UC
ulcerative colitis
Introduction and Rationale
Background
Inflammatory bowel disease (IBD) results in inflammation of the gastrointestinal tract lining, impairing the body's ability to digest food, absorb nutrients, and eliminate waste effectively. Crohn disease (CD) and ulcerative colitis (UC) are the 2 distinct types of IBD, both causing inflammation and functional disruption. In Canada, the prevalence of IBD in 2023 is estimated at 825 per 100,000 individuals, with 410 per 100,000 for Crohn disease and 414 per 100,000 for UC and IBD-unclassified.1 This translates to approximately 322,600 people in Canada living with IBD in 2023, with half of these cases comprising either UC or CD. By 2035, the prevalence is expected to increase to 1.1% of the population, or 1 in 91 people living in Canada.2
CD is a type of IBD that may affect any portion of the gastrointestinal tract from the mouth to the anus. Patients with CD have a higher risk of developing strictures, fistulas, and abscesses due to transmural inflammation, which is painful, reduces quality of life and causes other chronic or severe symptoms. It is estimated that 33% of CD patients may develop a fistula within 10 years of initial diagnosis, increasing to up to 50% within 20 years.3 Approximately one-quarter of the global Crohn disease population may develop perianal lesions, with 18% presenting as penetrating lesions such as fistulas or abscesses.3 The prevalence of perianal fistulas in Crohn disease varies according to disease location, being least common in isolated ileal disease (12%) or ileocolonic disease (15%) and most common in colonic disease (41%), particularly with rectal involvement (92%).4 Consequently, patients with Crohn disease typically experience periods of remission and relapse over time.5,6 For the subtype of fistulizing Crohn disease, surgical interventions, such as bowel resection, are often necessary.5,7 In contrast, UC is confined to the colon and rectum, with inflammation confined to the mucosal layer, though it presents a higher risk of colorectal cancer after 8 to 10 years of disease progression.8
According to the Crohn and Colitis Canada,2 the economic burden of IBD is substantial. In 2023, approximately $5.38 billion was spent on IBD care, with $2.05 billion in indirect and out-of-pocket costs and $3.33 billion in direct health care costs. Health care utilization for IBD has shifted from inpatient to outpatient management, leading to fewer hospital admissions and surgeries but an increase in outpatient visits. Effective pharmacotherapy remains crucial, including treatment options such as aminosalicylates, corticosteroids, immunomodulators, Janus kinase (JAK) inhibitors, antibiotics, and biologics.
Biologics, despite their high cost, have undergone continuous evaluation for efficacy and safety within the constraints of limited health resources. In Canada, approved biologics for IBD include 3 tumour necrosis factor (TNF) antagonists (infliximab, adalimumab, and golimumab), 2 IL-12/IL-23 inhibitors (risankizumab, ustekinumab), and 1 anti-integrin drug (vedolizumab). In 2017, biologics accounted for approximately 50% of IBD-related health care costs, a proportion that has likely increased since then.2 Reports from several provinces in Canada indicate a rapid rise in the use of biologics for both Crohn disease and UC.9
In the conventional treatment approach for IBD, medication follows a therapeutic hierarchy: starting with tier I 5-aminosalicylic acid, followed sequentially by tier II corticosteroids (prednisone or budesonide), tier III immunomodulators (azathioprine, 6-mercaptopurine, or methotrexate), and finally tier IV biologic drugs (infliximab, adalimumab, or certolizumab pegol).10 Alternatively, the top-down or accelerated step-up approach administers more potent drugs early in patient care, often immediately after diagnosis. As evidence supporting the benefits of biologics continues to grow, the top-down approach with early biologic intervention has become increasingly central in IBD management. Two distinct treatment protocols have emerged: 1) early use of biologics alone, and 2) a combined top-down approach with early use of both immunomodulators and biologics.11 Given that the top-down approach with biologics is relatively new and involves debates concerning its safety, efficacy, and cost, updated evidence is critical for informing stakeholders.
Policy Issue
To support decision-making about the current role of biologics in treating IBD, this rapid review provides an update to the 2019 CADTH Technology Review,12 which summarized findings from 3 related rapid reviews13-15 on the appropriate use of biologics in IBD management.
Policy Questions
Is there a role for earlier biologic therapy in IBD treatment:
For patients with moderate-to-severe luminal Crohn disease who have not received adequate trials of both corticosteroids and immunomodulators?
For patients with fistulizing Crohn disease who have not received a course of antibiotics and adequate trial of immunomodulators?
For patients with moderate-to-severe UC who have not received prior immunomodulating therapy?
Purpose
This Rapid Review aims to update and summarize evidence since 2018 on the earlier use of biologics for IBD to address the previously stated policy questions.
Research Questions
What is the clinical efficacy and safety of early biologic treatment compared with conventional step-up treatment for luminal Crohn disease?
What is the clinical efficacy and safety of early biologic treatment compared with conventional step-up treatment for fistulizing Crohn disease?
What is the clinical efficacy and safety of early biologic treatment compared with conventional step-up treatment for UC?
What are the evidence-based guidelines on the position of biologics in the sequencing of pharmacological treatments for Crohn disease and UC?
Methods
We conducted a rapid review on the efficacy and safety of early biologic treatment for IBD and sought updates to existing evidence-based guidelines.
Literature Search Methods
An experienced medical information specialist developed and refined the search strategies through an iterative process in consultation with the review team. The specialist then executed the searches in Ovid MEDLINE ALL (Ovid platform) and the Cochrane Library (Wiley) on July 19, 2024. The strategies utilized a combination of controlled vocabulary (e.g., “Colitis, Ulcerative,” “Crohn Disease,” “Biological Therapy”) and keywords (e.g., “colitis gravis,” “biosimilar,” “top-down”), adjusting the vocabulary and syntax as necessary across the databases. We limited results to citations published after November 1, 2018, and, where applicable, removed animal-only studies and opinion pieces. We downloaded and deduplicated the records using EndNote version 9.3.3 (Clarivate Analytics) and uploaded to Covidence (Veritas Health Innovation Ltd.).
We conducted a targeted search for relevant health technology assessments (HTAs) on the websites of HTA agencies in Canada, US, UK, Australia, and New Zealand via the CDA Grey Matters Checklist using keywords relevant to our research questions. One reviewer screened relevant reports and publications on HTA websites and downloaded the full text of any relevant reports for additional review to check for eligibility.
We did not search for evidence-based guidelines. Rather, we consulted the websites of clinical guideline developers with guidelines on the position of biologic drugs cited in the previous CDA report12 to check for updated guidelines or recommendations. One reviewer checked relevant websites and downloaded the full text or link to any relevant guideline updates to check for eligibility.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first-level screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1. Where necessary, the criteria were aligned with research questions Q1 to Q4.
Criteria | Description |
|---|---|
Populations | Q1: Individuals with luminal Crohn diseasea Q2: Individuals with fistulizing Crohn diseasea Q3: Individuals with ulcerative colitis Q4: Individuals with Crohn disease or ulcerative colitis |
Interventions | Biologics (e.g., adalimumab, infliximab, vedolizumab, ustekinumab, golimumab) as first-line or early therapy; or Biologics combined with conventional therapyb (This is also called the top-down approach.) |
Comparators | Q1 to Q3: Conventional management sequence (“step-up”) typically consisting of giving steroids, then switching to or adding immunosuppressants when remitting or not responding, and then switching to or adding biologics if not responding to previous drugs. Q4: NA |
Outcomes | Q1 to Q3: Clinical benefits (e.g., clinical response rate, clinical remission, surgery, hospitalization, need for steroids) and harms (e.g., adverse events, infections, malignancies) Q4: Guidelines regarding the place in therapy of biologics for the treatment of patients with Crohn disease or ulcerative colitis |
Study designs | Health technology assessments, systematic reviews, randomized controlled trials,c and evidence-based guidelines |
NA = not applicable.
aDuring screening, we included any relevant literature focusing on Crohn disease. During data extraction, we assessed eligibility and baseline information to differentiate between luminal and fistulizing subgroups of Crohn disease and identify any available subgroup analysis results. This same methodology was applied to identify evidence for the moderate-to-severe group within each subgroup.
bInclude tier I to III medications for conventional therapy sequentially:10 5-aminosalicylic acid, corticosteroids (prednisone or budesonide), and immunomodulators (azathioprine, 6-mercaptopurine, or methotrexate).
cEligible randomized controlled trials in the included health technology assessment or systematic review were excluded.
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria specified in Table 1, were duplicate reports as separate publications, or were published before November 2018. Additionally, we excluded non-English records, meeting abstracts, protocols, and studies in-progress.
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the following tools as a guide: A MeaSurement Tool to Assess systematic Reviews 2 (AMSTAR 2)16 for systematic reviews, the Cochrane Risk of Bias tool (RoB v2)17 for randomized controlled trials (RCT), and 2 domains of the Appraisal of Guidelines for Research and Evaluation (AGREE II) instrument (rigour of development and editorial independence)18 for guidelines. Summary ratings were not assessed for the included studies; rather, the strengths and limitations of each included article were described narratively.
Summary of Evidence
Quantity of Research Available
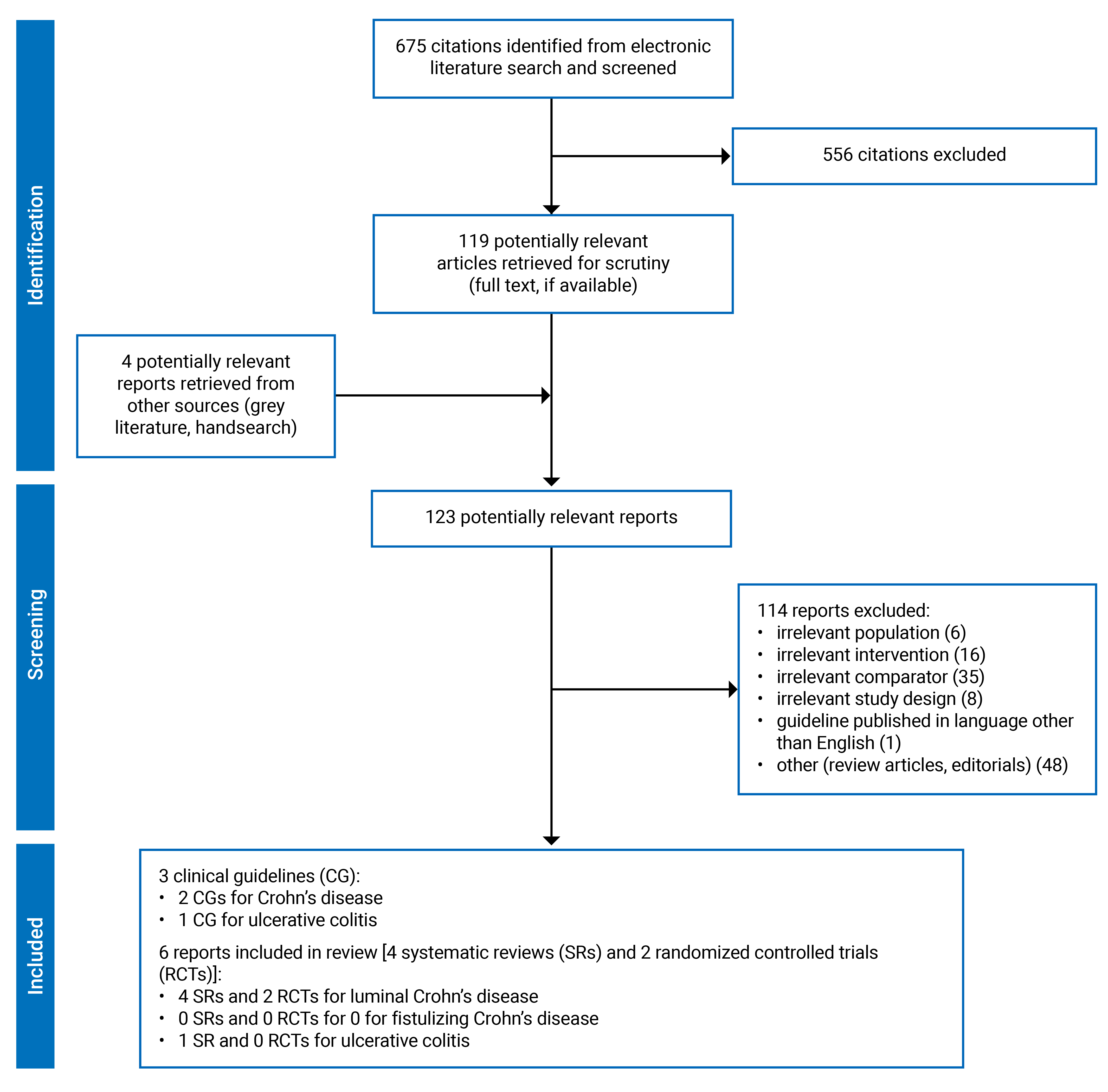
A total of 675 citations were identified in the literature search. After screening the titles and abstracts, 556 citations were excluded, and 119 potentially relevant reports from the electronic search were retrieved for full-text review. Additionally, 4 potentially relevant guideline updates were retrieved from the grey literature search for full-text review. In total, 9 publications met the inclusion criteria and were included in this review. These comprised of 4 systematic reviews, 2 RCTs, and 3 updated evidence-based guidelines. Appendix 1 presents the PRISMA flow chart of the study selection.
Appendix 6 provides several references for records which may be of potential interest but were not included in the review.
We searched 40 websites of 38 HTA agencies for relevant reports including 19 websites in Canada, 6 in Australia, 7 in the UK, 7 websites for 5 organizations in the US, and 1 in New Zealand. Six reports were reviewed and no eligible HTAs were located.
Study Characteristics
Further details regarding the characteristics of included systematic reviews, RCTs, and evidence-based guidelines are provided in Table 2 and Table 3 in Appendix 2, respectively.
Four SRs, 2 RCTs, and 3 updated evidence-based guidelines were identified that met the inclusion criteria.
Systematic Reviews
Four SRs11,19-21 were included. All 4 SRs included RCTs and observational studies.
Systematic Reviews of Patients With Luminal Crohn Disease
While the scope of the 4 SRs considered populations broader than luminal CD, they provided relevant evidence for the research questions in this review. All 4 SRs included studies in patients with Crohn disease without distinguishing between luminal and fistulizing Crohn disease. We included these SRs as more than 80% of the populations were considered to have luminal Crohn disease while less than 20% had penetrating lesions (fistulas or abscesses) requiring medical treatment based on baseline disease descriptions.7,22
All of the included SRs considered RCTs though a large proportion of the primary studies included were observational studies. Specifically, 2 of the 18 studies in the review by Law et al. (2024),20 2 of the 13 studies in the review by Zhang et al. (2023),21 3 of the 11 studies in the review by Hamdeh et al. (2020),19 and 6 of the 19 studies in the review by Tsui, et al. (2018)11 were either RCTs or posthoc analyses of RCTs. The 4 included SRs included primary studies published up to 2021.
Additional details on the included studies, including an assessment of overlap among the included primary studies across the 4 SRs is provided in Appendix 5.
Country of Origin
Two SRs were conducted by researchers from the US,19,20 1 from Canada11 and 1 from China.21
Patient Population
All 4 SRs focused on patients with Crohn disease. One SR20 also considered UC as an indication. One of the reviews focused on adult populations,19 another on children and adolescents,21 and 2 addressed both children and adults.11,20 One review20 briefly described the included study populations as “moderate-to-severe Crohn disease,” 2 reviews summarized the characteristics of included studies where some were classified as having moderate-to-severe disease,19,21 and 1 review11 did not report any relevant details on disease severity.
Interventions and Comparators
Three systematic reviews compared early versus late administration of biologic drugs, with 2 explicitly defining early biologic drugs20 and early anti–TNF-alpha19 as those administered within 3 years of disease onset. The third review21 did not provide a clear definition for the timing of prescribed biologics or what they considered to be early use. A time frame of “18-24 months” was inferred from the included studies. The comparators were generally referred to as late biologics,20,21 late anti–TNF-alpha,19 or late/conventional treatment, which could include a placebo control group or standard care. A fourth SR11 conducted a descriptive review and critical appraisal of the current literature on top-down therapy. The top-down therapy included 3 distinct treatment protocols: early use of biologics, such as infliximab, adalimumab, and certolizumab pegol; early use of immunomodulators, such as azathioprine, 6-mercaptopurine, and methotrexate; and early combined use of both immunomodulators and biologics. In contrast, traditional step-up approaches commence with locally acting oral steroids, followed by systemic steroids, and subsequently immunomodulators and biologic drugs for steroid-dependent or resistant patients. The review did not specify the timing of early use, but it was inferred from the treatment timing of included studies, ranging from week 0 to within 3 years of diagnosis for adult patients and from week 0 to within 3 months for pediatric patients.
Efficacy Outcomes
Three SRs19-21 reported clinical outcomes of interest and conducted meta-analyses where feasible including:
One SR by Tsui (2018)11 did not conduct any quantitative analysis and summarized the result for outcomes including remission and need for surgery narratively.
Safety Outcomes
None of the SRs reported any of the safety outcomes of interest.
Systematic Reviews of Patients With Fistulizing Crohn Disease
None of the included systematic reviews considered patients with fistulizing CD.
Systematic Reviews of Patients With UC
A single SR by Law et al. (2024),20 considered UC in addition to Crohn disease. Three observational studies, 2 in adults and 1 in children, were included for UC with disease duration less than 3 years.
Country of Origin
The SR20 was conducted by researchers in the US.
Patient Population
This SR20 included studies of both CD and UC in both children and adults.
Interventions and Comparators
The included SR20 compared early versus late administration of biologics, defining early biologic drugs as those administered within 3 years of disease onset.
Efficacy Outcomes
The included SR20 reported a single clinical outcome — need for surgery.
Safety Outcomes
This included SR did not report any safety outcomes of interest.
Primary Studies
Two RCTs23,24 were included. Neither RCT was included the SRs included in this review. We considered both to primarily support the evidence for luminal Crohn disease, given the disease characteristics and severity of the patients included in these studies. This included a low prevalence of patients with penetrating lesions (fistulas or abscesses) requiring medical treatment (less than 20%),7,22 trial eligibility and/or a small portion of patients who were categorized with penetrating (classified as B3) disease behaviour at baseline. Specifically, Noor et al. (2024)23 included only 1% (3/382) of patients with penetrating disease behaviour, while Jongsma et al. (2022)24 excluded patients with active perianal fistulas and none classified as having penetrating disease behaviour.
RCTs of Patients With Luminal Crohn Disease
Country of Origin
One multicentre RCT23 was conducted in 40 hospitals in the UK. A second multicentre RCT24 was conducted in 12 hospitals located in the Netherlands, Croatia, and Finland.
Patient Population
The PROFILE trial (PRedicting Outcomes For Crohn disease using a moLecular biomarker)23 included 386 adults with newly diagnosed active Crohn disease between December 29, 2017, and January 5, 2022. To be eligible, patients were required to have a Harvey-Bradshaw Index score of at least 7, elevated C-reactive protein, fecal calprotectin, or both, and endoscopic evidence of active inflammation. Participants were randomized into 2 groups: the top-down group (n = 193) and the accelerated step-up group (n = 193), with stratification by a blood-based prognostic biomarker subgroups [IBDhi (poor prognosis) versus IBDlo (better prognosis)], disease location (colon only versus other), and mucosal inflammation severity (mild, moderate, or severe). The mean age of participants was 33.6 years (SD 13.2), with 179 females (46%) and 207 males (54%). The median time from diagnosis to trial enrollment and initiation of treatment with the index course of steroids was 12 days (range 0 to 191). At baseline, the prevalence of penetrating (B3) disease behaviour was 1% in both the top-down group (1/192) and the accelerated step-up group (2/190). Patient characteristics and baseline disease activity were similar across both groups. After the 48-week study duration, primary outcome data were available for 379 participants (189 in the top-down group and 190 in the accelerated step-up group).
A second trial24 included 100 newly diagnosed pediatric patients with moderate-to-severe CD between April 7, 2015, and November 19, 2018. These patients, aged 3 to 17 years, presented with untreated Crohn disease according to the revised Porto criteria, had a weighted Pediatric Crohn Disease Activity Index (wPCDAI) of more than 40, and weighed more than 10 kg at baseline. Patients with active perianal fistulas were excluded. Eligible patients were stratified by centre and equally randomized into 2 groups: the first-line infliximab (FL-IFX) group (n = 50) and the conventional treatment group (n = 50). The mean age of participants was 14.6 years (SD 3.5), with 48 females (48%) and 52 males (52%). The median time between diagnostic endoscopy and the start of treatment was 8 days (IQR 4 to 14). At baseline, 10% of patients in both the FL-IFX group and the conventional treatment group had perianal disease, such as inactive fistulas, skin tags, or anal fissures, but none were classified with penetrating (B3) disease behaviour. The other baseline characteristics were similar between treatment groups. After the 52-week study duration, primary outcome data were available for 94 participants (46 in the FL-IFX group and 48 in the conventional treatment group). Safety analyses included 97 patients who received actual treatment per protocol (50 in the FL-IFX group and 47 in the conventional treatment group).
Interventions and Comparators
Both trials23,24 employed infliximab (IFX) as the investigated biologic, utilizing different comparative designs.
The PROFILE trial23 aimed to compare 2 treatment strategies: top-down versus accelerated step-up. Both groups initiated steroid induction during the screening period (−2 weeks) and followed different medication algorithms at weeks 4, 16, 32, and 48 after randomization:
In the top-down group, IV IFX and an immunomodulator were started, and the steroid taper was continued. The treatment protocol was as follows:
If in remission, continue IFX and the immunomodulator.
If flare 1 occurred, administer an additional course of steroid medication.
If flare 2 occurred, consider nonresponse and withdraw from the trial.
IFX was administered at a dose of 5 mg/kg with standard induction at 0, 2, and 6 weeks, followed by maintenance infusions every 8 weeks. Patients who did not respond after induction had early treatment withdrawal and returned to standard care with their local clinical team.
In the accelerated step-up group, the steroid taper was continued with the following protocol:
If in remission, continue the current step of treatment.
If flare 1 occurred, start steroids and an immunomodulator.
If flare 2 occurred, start IFX alongside the immunomodulator.
For participants starting on an immunomodulator, the choice was at the local investigator's discretion among azathioprine, low-dose mercaptopurine with allopurinol, or methotrexate.
In the trial by Jongsma et al. (2022),24 FL-IFX was compared to a conventional treatment strategy. Patients in the FL-IFX group received 5 IV infusions of IFX (Inflectra, CT-P13) at a dose of 5 mg/kg for induction at weeks 0, 2, and 6, followed by 2 maintenance infusions every 8 weeks. This regimen was combined with oral azathioprine as maintenance treatment, administered once daily at a dose of 2 to 3 mg/kg, starting on the day the induction treatment began. In the conventional strategy group patients received standard induction treatment with either exclusive enteral nutrition (polymeric feeding for 6 to 8 weeks, after which normal diet was gradually reintroduced within 2 to 3 weeks) or oral prednisolone (for 4 weeks 1 mg/kg daily with a maximum of 40 mg, followed by tapering down to 5 mg per week until stop). Induction treatment with enteral nutrition or prednisolone was based on patient preference. Ultimately, 27 patients (56%) received enteral nutrition, while 20 patients (42%) received prednisolone.
Efficacy Outcomes
The PROFILE trial23 reported sustained steroid-free and surgery-free remission at week 48 as the primary outcome. It also assessed 7 secondary outcomes, including endoscopic remission, health-related quality of life (HRQoL, IBD-Q) numerical score, number of flares, number of steroid courses, number of hospital admissions, and number of surgeries. Additionally, 37 tertiary outcomes were detailed in an accompanying appendix (these outcomes were not exacted for this review).
The Jongsma et al. (2022)24 trial reported clinical remission without the need for treatment escalation at week 52 as the primary outcome. Secondary outcomes were assessed at 2 time points: 10 weeks for the efficacy of induction therapy and 52 weeks after the treatment course. At 10 weeks, the study evaluated clinical remission, endoscopic remission, and fecal calprotectin levels. At 52 weeks, it assessed additional corticosteroid use, the need for treatment escalation, linear growth, clinical remission, endoscopic remission, and fecal calprotectin levels. HRQoL was measured with the validated IMPACT III questionnaire at week 14.
Safety Outcomes
Both included RCTs23,24 reported safety outcomes, including any adverse events and serious adverse events.
RCT of Patients With Fistulizing Crohn Disease
No RCTs were identified.
RCT of Patients With UC
No RCTs were identified.
Evidence-Based Guidelines for Patients With Crohn Disease or UC
Three updated guidelines were identified, including 2 for CD25,26 and 1 for UC.27 Two versions of 1 updated guideline for UC published in Spanish are listed in Appendix 6.
Critical Appraisal
Additional details regarding the strengths and limitations of included publications are provided in Appendix 3.
Critical Appraisal of Included Systematic Reviews
Although the 4 SRs11,19-21 had broader scopes in terms of study design, participants, interventions and comparators, they clearly defined the patient, intervention, comparison and outcome (PICO) questions according to their specific research interests. Except for Tsui et al. (2018),11 which conducted a qualitative systematic review, the remaining 3 SRs19-21 performed independent screening and data extraction in duplicate and employed appropriate statistical methods. Zhang et al. (2023)21 and Hamdeh et al. (2020)19 used robust techniques for assessing the RoB in both RCTs and observational studies; whereas Law et al. (2024)20 and Tsui et al. (2018)11 assessed the RoB solely in RCTs. Common limitations across all SRs included the lack of information on preplanned protocols, no search for grey literature, and failure to list and justify excluded studies. Additionally, only Zhang et al. (2023)21 and Hamdeh et al. (2020)19 disclosed sources of conflict of interest, including any funding. Based on the critical appraisal, all included SRs were considered to have more than 1 critical flaw. According to guidance from AMSTAR2, more than 1 critical flaw in a SR indicates that the review should not be relied on to provide an accurate and comprehensive summary of the available studies.
Critical Appraisal of Included Primary Studies
Both RCTs23,24 were judged to have good internal validity concerning randomization, outcome data analysis, and reporting. However, due to the complex nature of IBD care, blinding of researchers and participants (carers) was not feasible, and the assignment of interventions was transparent to all involved parties. This lack of blinding might have introduced bias due to deviations from intended interventions and the measurement of outcomes. Consequently, some concerns were raised regarding the evidence provided.
Critical Appraisal of Included Evidence-Based Guidelines
The 3 updated guidelines25-27 were developed with high quality, demonstrating rigorous guideline development and editorial independence. They defined clear PICO criteria and employed systematic search strategies and formal methods for grading evidence and formulating recommendations, such as GRADE and the Oxford Centre approach. However, it is challenging to identify explicit links between recommendations and their supporting evidence. Specifically, 2 NICE guidelines26,27 presented the evidence reviews separately from their recommendation documents, while the European Crohn and Colitis Organization-European Society for Paediatric Gastroenterology Hepatology and Nutrition (ECCO-ESPGHAN) guideline25 included supporting evidence under each recommendation but did not provide evidence tables. Extensive external review was reported in ECCO-ESPGHAN guideline while it was not found in the 2 updated NICE guidelines and their evidence review documents. The NICE methodology manual outlines a procedure for updating guidelines, but no future updating information was reported in the ECCO-ESPGHAN guideline.25 All 3 guidelines were developed by internal teams of the funding organizations, with established disclosure policies and declaration forms.
Findings
Appendix 4 presents findings for all included records (Table 7, Table 8, and Table 9).
Systematic Reviews
Effect estimates and findings for the included SRs are presented in Appendix 4 (Table 7).
Findings from Systematic Reviews of Patients With Luminal Crohn Disease
Based on the evidence from 4 SRs, the early use of biologics in CD (within 3 years after disease diagnosis), presents notable benefits to patients. Hamdeh (2020)19 indicated benefits of early biologics specifically on adult patients. Compared to late anti–tumour necrosis factor alpha (TNF-alpha), where biologics are used following the sequential failure of steroids and immunomodulators, early anti–TNF-alpha administration is associated with a statistically significant improvement in clinical remission rates, particularly in early remission (within 12 weeks). Early biologics also enhance mucosal healing and reduce relapse rates, disease progression, and the need for surgery.
In pediatric patients, Zhang et al. (2023)21 demonstrated that early biologic treatment is more effective than late or conventional therapy in achieving clinical remission, promoting mucosal healing, and reducing relapse rates in children and adolescents with CD.
Regarding evidence that combines both adult and pediatric populations, Tsui, et al. (2018)11 summarized the findings of included studies and found that 4 studies reported overall positive outcomes with top-down therapy, while 1 study showed less favourable results compared to conventional treatment. Law et al. (2024)20 concluded that early biologic therapy was associated with a lower likelihood of requiring surgery compared to late treatment.
Findings From Systematic Reviews of Patients With UC
Based on limited evidence presented for UC, early biologic therapy is associated with increased odds of colectomy, although this finding may be confounded by baseline disease severity.
Primary Studies
Findings From RCT With Luminal Crohn Disease
One RCT focused on pediatric patients,24 while the other targeted adults.23 The findings for these 2 populations were presented separately.
For Pediatric Patients
Results from a single RCT24 show that 10 weeks after start of therapy, the proportion of children in clinical and endoscopic remission is significantly higher in the group treated with first-line infliximab than in the group that received exclusive enteral nutrition or prednisolone (conventional treatment). For maintenance, first-line IFX combined with azathioprine is also superior in achieving clinical remission at 1 year without the need for corticosteroids or further biologics. Contrarily, a significant proportion of children in the conventional treatment group received an additional course of corticosteroids. Despite the possibility to escalate to treatment with IFX, the group that received conventional treatment shows poorer growth at 1 year.
For safety, first-line IFX resulted in fewer adverse events and serious adverse events when compared to conventional treatment.
For Adults
Results from a single RCT23 show that top-down treatment with combination infliximab and immunomodulator was significantly better than accelerated step-up (conventional) treatment in maintaining steroid-free and surgery-free remission throughout 48 weeks of follow-up. Top-down treatment also showed greater efficacy in achieving endoscopic remission.
The top-down treatment also improved HRQoL, reduced number of flares requiring treatment escalation, and reduced need for urgent abdominal surgery. Although not powered to show a difference in safety end points, there were fewer adverse events or serious adverse events in the top-down group than in the accelerated step-up group. There was no difference in risk of serious infection between treatment strategies and no reported malignancies or deaths during the trial.
Evidence-Based Guidelines
Findings From Evidence-Based Guidelines of Patients With Luminal Crohn Disease
Two updated guidelines25,26 recommend the use of biologics for patients with CD. The NICE guideline26 encompasses all CD populations, while the ECCO-ESPGHAN guideline25 specifically addresses children and adolescents with luminal CD.
For Pediatric Patients
For children and adolescents with luminal CD, biologics use is recommended as the third-line pharmacotherapy for induction or maintenance. For induction, anti-TNF drugs are recommended in patients who fail to achieve or maintain remission with an immunomodulator. Specifically, the guidelines suggest using infliximab in combination with an immunomodulator, or adalimumab either as monotherapy or in combination therapy. Ustekinumab and vedolizumab are recommended only for patients who have not responded to anti-TNF drugs. However, for maintenance therapy, anti-TNF drugs are recommended solely for postoperative patients at high risk of recurrence.
The early use of anti-TNF drugs in pediatric patients with luminal CD is recommended only for children and adolescents who are newly diagnosed and with high risk.
For Adults
We consider the following recommendations from the NICE CD guideline26 to focus on luminal CD, as it specifically addresses fistulizing CD separately.
For induction therapy, it recommends the use of biologics based on the patient's age, disease severity, and specific subgroups of CD:
Adults with severe active CD: Infliximab or adalimumab monotherapy or combined with an immunosuppressant if not responded, not tolerated or contraindicated to conventional therapy.
People (6 to 17 years) with severe active CD: Infliximab if not responded, not tolerated or contraindicated to conventional therapy (including corticosteroids, immunomodulators and primary nutrition therapy).
Adults with moderate-to-severe active CD after previous treatment: Ustekinumab or vedolizumab, if inadequate response with, lost response to, intolerant or contraindicated to either conventional therapy or a TNF-alpha inhibitor.
For maintenance therapy, only infliximab or adalimumab is recommended, with reassessment every 12 months or restarting treatment upon relapse. Specifically, for patients who have completed macroscopic resection of ileocolonic CD, it is recommended not to offer biologics for maintenance of remission and to opt for azathioprine and metronidazole instead.
Findings From Evidence-Based Guidelines of Patients With Fistulizing Crohn Disease
For Pediatric Patients
The ECCO-ESPGHAN guideline25 recommends first-line anti-TNF therapy for children and adolescents with fistulizing perianal CD, both for induction (in combination with antibiotic therapy, surgical intervention, or both) and for maintenance (in combination with antibiotic therapy).
For Adults
The NICE guideline26 recommends infliximab as a third-line pharmacotherapy for patients with active fistulizing CD who do not respond to, not tolerate, or contraindicate to conventional therapies, including antibiotics, drainage, and immunosuppressants.
Findings From Evidence-Based Guidelines of Patients With UC
The NICE guideline27 recommends infliximab as a third-line pharmacotherapy for patients with acute severe UC who are contraindicated or clinically inappropriate for ciclosporin, and otherwise only for experimental use in clinical trials of patients with acute severe UC.
Limitations
The SRs included in the review has several limitations. Three of the 4 SRs had broad scopes and included populations and study designs that extended beyond our research questions, resulting in limited retrievable evidence for the populations of interest. The timing of early biologic treatment was broadly 3 years postdiagnosis; however, the definitions provided were not clear. As such, we were unable to determine whether the patients included in these reviews might have been exposed sufficiently to conventional treatments. Whereas 3 systematic reviews compared early versus late administration of biologics, the only SR comparing top-down treatment strategies to step-up therapy did not provide any quantitative results. There was no safety data reported in the included SRs. Therefore, there was limited evidence in the included SRs to inform the research questions.
The 2 included RCTs may provide more relevant insight into the research questions on clinical efficacy and safety, as they involved newly diagnosed Crohn disease patients. However, both trials were conducted in Europe, which may limit their external validity due to variations in clinical practices and health care settings. This issue is particularly pertinent in 1 RCT focused on pediatric Crohn disease, where 56% of patients in the conventional treatment group received exclusive enteral nutrition, an intervention not commonly regarded as a standard component of conventional therapy. In addition, both RCTs used infliximab as the investigated biologic, so the findings may not be generalizable to other biologic drugs, particularly those with different molecular structures or mechanisms of action that target the immune system to inflammation.
Conclusions and Implications for Decision- or Policy-Making
In CD, early use of biologics within 3 years from diagnosis improves remission rates, mucosal healing, and reduces relapse rates and surgery needs. Specific findings relevant to fistulizing CD are unclear. At least 1 guideline recommended early use of biologic drugs in high-risk populations of children and adolescents with luminal or fistulizing disease. Findings in CD patients are generally consistent with those reported in the previous CADTH Technology Review.12
In UC, limited evidence from 3 observational studies included in 1 systematic review suggest a higher associated risk of colectomy. This finding should be interpreted with caution due to the paucity of available evidence. Guidelines do not recommend early use of biologics in these patients.
While additional studies, especially RCTs, focusing on specific patient subgroups would strengthen the evidence base, it is difficult to adequately capture patient subgroups in an RCT due to challenges of designing and implementing a trial to overcome potential bias from nonblinding/concealment of treatment, especially when dealing with sequences of therapies with different means of administration and side effect profiles.
The definition of early use of biologic drugs was unclear. It should include newly diagnosed patients or those naive to specific drugs. A clearer definition would ensure decisions are based on practical and precise criteria. Additionally, further such studies comparing biologics other than infliximab and corresponding treatment regimens would be beneficial.
References
1.Coward S, Benchimol EI, Kuenzig ME, et al. The 2023 Impact of Inflammatory Bowel Disease in Canada: Epidemiology of IBD. J Can Assoc Gastroenterol. 2023;6(Suppl 2):S9-S15. PubMed
2.2023 Impact of inflammatory bowel disease in Canada. Toronto (ON): Crohn's and Colitis Canada; 2023: https://crohnsandcolitis.ca/Crohns_and_Colitis/documents/reports/2023-IBD-Report-English-LR.pdf?ext=.pdf. Accessed 2024 Jul 24.
3.Schwartz DA, Loftus EV, Jr., Tremaine WJ, et al. The natural history of fistulizing Crohn's disease in Olmsted County, Minnesota. Gastroenterology. 2002;122(4):875-880. PubMed
4.Hellers G, Bergstrand O, Ewerth S, Holmstrom B. Occurrence and outcome after primary treatment of anal fistulae in Crohn's disease. Gut. 1980;21(6):525-527. PubMed
5.Feuerstein JD, Cheifetz AS. Crohn Disease: Epidemiology, Diagnosis, and Management. Mayo Clin Proc. 2017;92(7):1088-1103. PubMed
6.Kalla R, Ventham NT, Satsangi J, Arnott ID. Crohn's disease. BMJ. 2014;349:g6670. PubMed
7.Gecse KB, Bemelman W, Kamm MA, et al. A global consensus on the classification, diagnosis and multidisciplinary treatment of perianal fistulising Crohn's disease. Gut. 2014;63(9):1381-1392. PubMed
8.Burri E, Maillard MH, Schoepfer AM, et al. Treatment Algorithm for Mild and Moderate-to-Severe Ulcerative Colitis: An Update. Digestion. 2020;101 Suppl 1:2-15. PubMed
9.Kuenzig ME, Coward S, Targownik LE, et al. The 2023 Impact of Inflammatory Bowel Disease in Canada: Direct Health System and Medication Costs. J Can Assoc Gastroenterol. 2023;6(Suppl 2):S23-S34. PubMed
10.Aloi M, Nuti F, Stronati L, Cucchiara S. Advances in the medical management of paediatric IBD. Nat Rev Gastroenterol Hepatol. 2014;11(2):99-108. PubMed
11.Tsui JJ, Huynh HQ. Is top-down therapy a more effective alternative to conventional step-up therapy for Crohn's disease? Ann Gastroenterol. 2018;31(4):413-424. PubMed
12.de Léséleuc L, McGolrick D. Appropriate Pharmacotherapy for Inflammatory Bowel Disease. (CADTH Technology review optimal use 360 report no. 22). Ottawa (ON): CADTH; 2019 Jun: https://www.cadth.ca/sites/default/files/hta-he/ho0003-he0018-ibd-ou360.pdf. Accessed 2024 Jul 30.
13.Thompson W, Argáez C. Early Biologic Treatment versus Conventional Treatment for the Management of Crohn’s Disease: A Review of Comparative Clinical Effectiveness and Cost-Effectiveness. (CADTH Rapid response report: peer-reviewed summary with critical appraisal). Ottawa (ON): CADTH; 2019 Feb: https://www.ncbi.nlm.nih.gov/books/NBK543466/. Accessed 2024 Jul 30.
14.Young C, Campbell K. Biologics versus Immunomodulators or Antibiotics for the Management of Fistulizing Crohn’s Disease: A Review of Comparative Clinical Effectiveness and Cost-Effectiveness. (CADTH Rapid response report: summary with critical appraisal). Ottawa (ON): CADTH; 2019 Mar: https://www.ncbi.nlm.nih.gov/books/NBK544684/. Accessed 2024 Jul 30.
15.Chao Y-S, Loshak H. Biologics versus Immunomodulators for the Treatment of Ulcerative Colitis: A Review of Comparative Clinical Effectiveness and Cost-Effectiveness. (CADTH Rapid response report: peer-reviewed summary with critical appraisal). Ottawa (ON): CADTH; 2019 Apr: https://www.ncbi.nlm.nih.gov/books/NBK549363/. Accessed 2024 Jul 30.
16.Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. PubMed
17.Higgins J, Savović J, Page M, Elbers R, Sterne J. Chapter 8: Assessing risk of bias in a randomized trial. In: Higgins JPT, Thomas J, Chandler J, et al (eds). Cochrane Handbook for Systematic Reviews of Interventions version 6.4 (updated August 2023). Cochrane; 2023: https://training.cochrane.org/handbook. Accessed 2024 Aug 5.
18.Brouwers MC, Kho ME, Browman GP, et al. AGREE II: advancing guideline development, reporting, and evaluation in health care. Prev Med. 2010;51(5):421-424. PubMed
19.Hamdeh S, Aziz M, Altayar O, Olyaee M, Murad MH, Hanauer SB. Early vs Late Use of Anti-TNFa Therapy in Adult Patients With Crohn Disease: A Systematic Review and Meta-Analysis. Inflamm Bowel Dis. 2020;26(12):1808-1818. PubMed
20.Law CCY, Tkachuk B, Lieto S, et al. Early Biologic Treatment Decreases Risk of Surgery in Crohn's Disease but not in Ulcerative Colitis: Systematic Review and Meta-Analysis. Inflamm Bowel Dis. 2024;30(7):1080-1086. PubMed
21.Zhang L, Jin Z, Hao J. Efficacy of early biologic therapy versus late/conventional therapy in children and adolescents with Crohn's disease: A systematic review and meta-analysis. Saudi J Gastroenterol. 2023;29(5):259-268. PubMed
22.Feuerstein JD, Ho EY, Shmidt E, et al. AGA Clinical Practice Guidelines on the Medical Management of Moderate to Severe Luminal and Perianal Fistulizing Crohn's Disease. Gastroenterology. 2021;160(7):2496-2508. PubMed
23.Noor NM, Lee JC, Bond S, et al. A biomarker-stratified comparison of top-down versus accelerated step-up treatment strategies for patients with newly diagnosed Crohn's disease (PROFILE): a multicentre, open-label randomised controlled trial. Lancet Gastroenterol Hepatol. 2024;9(5):415-427. PubMed
24.Jongsma MME, Aardoom MA, Cozijnsen MA, et al. First-line treatment with infliximab versus conventional treatment in children with newly diagnosed moderate-to-severe Crohn's disease: an open-label multicentre randomised controlled trial. Gut. 2022;71(1):34-42. PubMed
25.van Rheenen PF, Aloi M, Assa A, et al. The Medical Management of Paediatric Crohn's Disease: an ECCO-ESPGHAN Guideline Update. J Crohns Colitis. 2020. PubMed
26.National Institute for Health and Care Excellence. Crohn’s disease: management. (NICE guideline NG129) 2019; https://www.nice.org.uk/guidance/ng129. Accessed 2024 Aug 1.
27.National Institute for Health and Care Excellence. Ulcerative colitis: management. (NICE guideline NG130) 2019; https://www.nice.org.uk/guidance/ng130. Accessed 2024 Aug 1.
Authors and Contributors
Authors
Shu-Ching Hsieh contributed to the conception and design of the review, conducted literature screening and study selection, data abstraction and risk of bias assessment for primary studies, interpretation, and writing of the final report.
Xiaoqin Wang contributed to the conception and design of the review, conducted literature screening and study selection, data abstraction, risk of bias assessment, and interpretation for systematic reviews, prepared the result materials, and review the final report.
Zemin Bai contributed to the conception and design of the review, conducted literature screening and study selection, data abstraction, risk of bias assessment, and interpretation for clinical guidelines, prepared the result materials, and review the final report.
Shannon E. Kelly contributed to the conception and design of the review, provided oversight to the research process, provided feedback on the implementation process and methods, and reviewed and provided feedback on the final report.
Melissa Brouwers contributed to study questions, protocol development, co-oversight of protocol implementation, data interpretation, drafting, editing, and refining paper, and approval of final draft.
George Wells provided oversight and was involved in the conception, design, and implementation of the review, as well as the review of the final report.
Research Information Science
Becky Skidmore designed and executed search strategies in consultation with the review team (data acquisition), provided search documentation and wrote the literature search methods
Contributors
We thank Kaitryn Campbell, MLIS, MSc (Hamilton, ON) for peer review of the MEDLINE search strategy.
Conflicts of Interest
George A. Wells disclosed the following:
VBI Vaccines Inc. (2020-Current): Coronavirus Vaccine. Data Safety Monitoring Board — Member.
Thermedical (2021-Current): Ablation system and catheter needle. Design and analysis advice for preparation of FDA Submission
VBI Vaccines Inc. (2020-Current): Coronavirus Vaccine. Design and Analysis Advice for preparation of FDA Submission
No other conflicts of interest were declared.
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Table 2: Characteristics of Included Systematic Reviews
Study citation, country, funding source | Study designs and numbers of primary studies included | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Law et al. (2024)20 US Funding source: National Institutes of Health K23 Career Development Award (K23 KD111995 to 01A1). | 18 studies included: 16 were observational studies and 2 were posthoc analysis of RCTs |
Sample sizes ranged from 16 to 1253 | Intervention: Early biologics, within 3 years of treatment Comparator: Late biologic, step-up treatment. | Outcomes: Risk of inflammatory bowel disease-related surgery Follow-up: varied by studies, ranging from 24 months to 172 months |
Zhang et al. (2023)21 China Funding source: None | 13 studies: 11 cohort studies, 2 RCTs | Children and adolescents patients were included. Three included studies specified that the participants were of moderate-to-severe spectrum. Two studies focused on patients with luminal Crohn disease. Sample sizes ranged from 26 to 199. | Intervention: Early biologics Comparator: Late biologics No definition for “early” administration of widely prescribed biologics was provided. However, the time frame of “18-24 months” was inferred from the included studies. | Outcomes:
Follow-up: varied by studies, ranging from 2 months to 2 years |
Hamdeh et al. (2020)19 US Funding Source: NR | 11 studies: 8 non-RCTs, 3 RCTs | Adult patients Average age: 4 studies reported the average age range of 30 to 43 years old Gender: 4 studies reported with male account for 35% to 71%. One study recruited moderate-to-severe CD patients Sample sizes ranged from 45 to 942. | Intervention: early anti–TNF-alpha therapy, less than 3 years from disease diagnosis Comparator: Late anti–TNF-alpha therapy. | Outcomes:
Follow-up: varied by studies, ranging from 2 weeks to 10 years (or > 36 months) |
Tsui et al. (2018)11 Canada Funding source: NR | 19 studies: 6 RCTs, 13 cohort studies | Five studies for pediatric, 14 for adults. | Intervention: Top-down therapy, including the following 3 distinct treatment protocol designs: 1. Early use of biologics, such as infliximab, adalimumab, and certolizumab pegol; 2. Early use of immunomodulators, such as azathioprine, 6-mercaptopurine, and methotrexate; and 3) top-down / early combined (early use of both immunomodulators and biologics). Comparator: Step-up therapy, the traditional “step-up” approaches, which start with topically acting oral steroids, followed by systemic steroids, and by immunomodulators and biologic agents in steroid-dependent or resistant patients. The treatment timing of “early use,” was inferred as within 3 years of diagnosis. (The “treatment timing” of included studies ranged from “week 0 to within 3 years of diagnosis” for adult patients and “from week 0 to within 3 months for pediatric patients.”) | Outcomes:
Follow-up: varied by studies, ranging from 1 to 39 years |
CD = Crohn disease; NR = not reported; RCT = randomized controlled trial; TNF-alpha = tumour necrosis factor alpha; UC = ulcerative colitis.
Note: This table has not been copy-edited.
Table 3: Characteristics of Included Primary Clinical Studies- RCTs
Study citation, country, funding source | Study design | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Noor et al. (2024)23 40 hospitals in the UK Funding source: Wellcome and PredictImmune Ltd. | A multicentre, open-label, biomarker-stratified, randomized controlled trial to compare top-down vs. accelerated step-up treatment strategies for patients with newly diagnosed CD. The authors used sealed Envelope version 17.2.1 for randomization and patient allocation. | Eligibility criteria: aged 16 to 80 years; newly diagnosed active CD required all of (1) CD diagnosed within 6 months using standard clinical, endoscopic, histological, and radiological methods; (2) active, symptomatic disease (corresponding to Harvey-Bradshaw symptomatic disease (corresponding to HBI ≥ 7); (3) biochemical evidence of active inflammation with either serum above the ULN, fecal calprotectin of 200 mcg/g or more, or both; (4) endoscopic evidence of active CD ([SES-CD] ≥ 4 for ileal-only disease or ≥ 6 for ileocolonic/colonic disease); and (5) naive to immunomodulator and biologic therapy. Patients with clinically significant obstructive or peri-anal disease were excluded. Top-down (N = 193) vs Accelerated step-up (N = 193)
Author’s conclusions: Patient characteristics and baseline disease activity were similar across both groups. | Both groups start steroid induction at screening period (−2 weeks). Intervention: Top-down Start IFX and immunomodulator, and continue steroid taper:
Comparator: Accelerated step-up Continue steroid taper:
| Primary Outcomes: Sustained steroid-free and surgery-free remission Follow-up: 48 weeks Secondary Outcomes:
Tertiary Outcomes: 37 outcomes are listed in Appendix 1 of the main publication. |
Jongsma 202224 Netherlands, Croatia, and Finland Funding source: ZonMw (The Netherlands Organisation for Health Research and Development) under project number 113202001, Crocokids (a Dutch fundraising organization to support research on IBD in children) and an Investigator-Sponsored Research Award from Pfizer (Study ID WI213008). | An investigator-initiated international open-label randomized controlled trial to compare the first-line use of IFX and remission than conventional treatment in achieving and maintaining remission. The authors employed a web-based block randomization model for stratified randomization. Allocation was concealed from all participants and health care providers. | Eligibility criteria: Patient presents with new-onset untreated CD according to the revised Porto criteria; both wPCDAI > 40 and Body weight > 10 kg at baseline First-line IFX (N = 49) vs Conventional (N = 50)
Author’s conclusions: Patient and disease characteristics at baseline were similar between treatment groups | Intervention: First-line IFX Patients received 5 IV IFX (Inflectra, CT-P13) infusions of 5 mg/kg induction at weeks 0, 2, and 6, followed by 2 maintenance infusions every 8 weeks. This was combined with oral AZA as maintenance treatment (once daily, dosed 2 to 3 mg/kg), which was initiated on the day induction treatment was started. Comparator: Conventional Patients received standard induction treatment with either EEN (polymeric feeding for 6 to 8 weeks, after which normal diet was gradually reintroduced within 2 to 3 weeks) or oral prednisolone (for 4 weeks 1 mg/kg daily with a maximum of 40 mg, followed by tapering down to 5 mg per week until stop). Induction treatment with EEN or prednisolone was based on patient preference. Ultimately, 27 patients (56%) received EEN, while 20 patients (42%) received prednisolone. | Primary Outcomes: Clinical remission without need for treatment escalation Follow-up: 52 weeks Secondary Outcomes: Follow-up: 52 weeks
Follow-up: 10 weeks
Follow-up: 14 weeks
|
AZA = azathioprine; CD = Crohn disease; CRP = C-reactive protein; EEN = exclusive enteral nutrition; HRQoL = health-related quality of life; IFX = infliximab; HBI = Harvey-Bradshaw Index; IQR = interquartile range; MTX = methotrexate; SD = standard deviation; SES-CD = Simple Endoscopic Score for Crohn disease; TNF = tumour necrosis factor; ULN = upper limit of normal; wPCDAI = weighted Paediatric CD Activity Index score.
aIBDhi (IBD2) = poor prognosis subgroup and IBDlo (IBD1) = better prognosis subgroup), both are blood-based prognostic biomarker (classifier) developed and validated by a whole blood qPCR assay.
Note: This appendix has not been copy-edited.
Appendix 3: Critical Appraisal of Included Publications
Please note that this appendix has not been copy-edited.
Table 4: Strengths and Limitations of Systematic Reviews Using AMSTAR 216
Strengths | Limitations |
|---|---|
Law et al. (2024)20 | |
This systematic review clearly defined the PICO question and did independent screening and extraction. | The systematic review did not have preplanned protocol or registration, lack search for grey literature, did not justify for excluded studies, did not account for risk of bias when interpret the result and failed to provide publication bias assessment result even conducted. Moreover, authors included both RCT and observational studies without explaining the rationale, and pooled data from both observational studies without mentioning adjusted or non-adjusted result. At last, this review failed to report statement on conflict of interest. |
Zhang et al. (2023)21 | |
This systematic review clearly defined the PICO question, did independent screening and extraction, used appropriate methods to assess the risk of bias for included studies and discussed the impact on the result. | The systematic review did not have preplanned protocol or registration, lacked search for grey literature, did not justify excluded studies, and did not report funding source of included studies. For analysis methods, authors used I2 to decide using a fixed model or not, which is not appropriate. Moreover, authors included both RCT and observational studies without explaining the rationale. Also, authors identified potential publication bias but did not discuss the impact on the results. |
Hamdeh et al. (2020)19 | |
This systematic review clearly defined the PICO question, did independent screening and extraction, and used appropriate methods to assess the risk of bias. | The systematic review mentioned protocol a priori but nothing was linked or reported, lack search for grey literature, did not justify for excluded studies, did not report funding source of included studies, did not account for risk of bias when interpret the result and did not provide satisfactory explanation on heterogeneity. For analysis methods, authors pooled data from both observational studies without mentioning adjusted or nonadjusted result. Moreover, included both RCT and observational studies without explaining the rationale. Also, authors identified potential publication bias but did not discuss the impact on the results. |
Tsui et al. (2018)11 | |
This systematic review summarized evidence on top-down therapy compared to conventional step-up therapy for Crohn disease. | This is a qualitative review without a preplanned protocol or registration. No search for grey literature, did not justify for excluded studies and did not report funding source of included studies. Moreover, authors included both RCT and observational studies without explaining the rationale. Authors assessed risk of bias for randomized trials but did interpret the result in discussion. |
AMSTAR 2 = A MeaSurement Tool to Assess systematic Reviews 2; RCT = randomized controlled trial; CD = Crohn disease; PICO = population, intervention, comparator, outcomes.
Table 5: Strengths and Limitations of Clinical Studies Using RoB v217
Strengths | Limitations |
|---|---|
Noor et al. (2024)23 | |
The authors utilized the secure online software Sealed Envelope version 17.2.1 for randomization. Patients were stratified based on biomarker levels, disease location (colon only vs. other), and mucosal inflammation (mild vs. moderate vs. severe) to ensure even distribution across both groups. The allocation sequence was properly concealed. The authors used regression analyses adjusting for covariates or multiple imputation to account for missing baseline values. They also performed testing procedures over the primary and 5 secondary analyses. The analyses estimated for the main effect of the biomarker and treatment, and the interaction between the biomarker and treatment, adjusting for baseline variables. In addition, 94 (181/193) in top-down group and 89% (172/193) in conventional group completed the 52-week study. The attrition bias was judged to be modest. All outcome variables were in align with the protocol and reported properly. | An open-label study comparing top-down and accelerated step-up treatment strategies relies on clinical judgment based on patient signs and symptoms. The knowledge of treatment assignment by both researchers and patients(carers) may have influenced their intervention performance and outcome assessment. This study compared 2 strategies for IBD care. The conclusion was only limited to infliximab-based top-down strategy, which may not necessarily apply to all biologics. In the conventional group, patients experiencing flare 2 could start infliximab with an immunomodulator, both of which were used in the top-down group. The potential influence of infliximab use in this subgroup on the comparison of the 2 strategies was not addressed. |
Jongsma 202224 | |
The authors employed a validated variable block randomization model for centre-stratified randomization, integrated into the trial's web-based database (Castor Electronic Data Capture). Although the concealment method was not detailed, it was confirmed that allocation was concealed for all participants and health care providers. Baseline patient and disease characteristics were similar between treatment groups. The authors used an intention-to-treat approach for efficacy outcomes and the safety analyses were based on the actual treatment patients received (i.e., per protocol). Statistical methods, including descriptive and exploratory, were clearly described and adhered to. Most patients were likely hospitalized and carefully followed, with 98% (49/50) in the infliximab group and 100% (50/50) in the conventional group completing the 52-week study. Any bias from missing outcome data was considered minor. All outcome variables were in align with the protocol and reported properly. | An open-label study compared the safety and efficacy of IV infliximab with conventional treatments (EEN or prednisolone at 1 mg/kg, up to 40 mg). The distinct differences between the regimens likely revealed the treatment assignment to researchers and patients, potentially influencing intervention performance, and outcome assessment. In the conventional group, induction treatment with EEN or prednisolone was based on patient preference. Ultimately, 27 patients (56%) chose EEN, and 20 patients (42%) chose prednisolone. Thus, the evidence may not fully represent medication-based conventional treatment. |
EEN = exclusive enteral nutrition; IBD = inflammatory bowel disease.
Table 6: Strengths and Limitations of Guidelines Using AGREE II18
AGREE II item | ECCO-ESPGHAN guideline update of pediatric CD (2021)25 | NICE guideline for CD (2019)26 ,a,b | NICE guideline for UC (2019)27,b,c |
|---|---|---|---|
Domain 3: Rigour of development | |||
7. Systematic methods were used to search for evidence. | 5 (p172) - no search terms and strategies | 7 (Appendix C – search strategies) | 7 (Appendix C – search strategies) |
8. The criteria for selecting the evidence are clearly described. | 6 (p172 and suppl. 1) – mentioned PICO format but didn't provide specific PICO table | 7 (PICO table, Appendix A - protocol) | 7 (PICO table, Appendix A – protocol) |
9. The strengths and limitations of the body of evidence are clearly described. | 6 (p172-Oxford Centre for Evidence-Based Medicine 2011 Levels of Evidence) + quality of evidence in main text - > no evidence table: not easy to find | 7 (Table 9, Appendix F – ROB table, H - GRADE tables) | 7 (Table 9, Appendix F – clinical evidence table, H – GRADE tables) |
10. The methods for formulating the recommendations are clearly described. | 6 (P172 – panel and ECCO standard operating procedures) – didn't have clear outcome development | 6 (p50 to 3.9 Making group decisions and reaching consensus- guideline manual) – not easy to find | 6 (p50 to 3.9 Making group decisions and reaching consensus- guideline manual) – not easy to find |
11. The health benefits, side effects, and risks have been considered in formulating the recommendations. | 6 (main text – practical guidance) – not easy to find | 6 (p39 – evidence review, p191- guideline manual) – not easy to find | 6 (p39 -evidence review, p191 – guideline manual) – not easy to find |
12. There is an explicit link between the recommendations and the supporting evidence. | 6 (main text - evidence under each recommendation) – no evidence table: not easy to find | 4 (p33-evidence review) – show clinical evidence statements related to recommendations but didn't show clear link with recommendations; published recommendations without the link to evidence | 4 (p180 results, 256 results, 315 discussion-evidence review) – didn't have a clear link between evidence and recommendations; published recommendations without the link to evidence |
13. The guideline has been externally reviewed by experts before its publication. | 5 (p187) – no methods, info gathered, and how to use that info to inform guideline development. | 3 (p209 – guideline manual, not routinely commission), didn't have an external peer review in publication and in an evidence review | 3 (p209 – guideline manual, not routinely commission), didn't have an external peer review in publication and an evidence review |
14. A procedure for updating the guideline is provided. | 0 (no info on the future update) | 6 (p229 – updating procedure in guideline manual) – no update plan specific to this guideline | 6 (p229 – updating procedure in guideline manual) – no update plan specific to this guideline |
Domain 6: Editorial independence | |||
22. The views of the funding body have not influenced the content of the guideline. | 7 (Funding info provided, funder-their own organizations) | 7 (Appendix A – protocol in evidence review -The NICE Guideline Updates Team is an internal team within NICE). | 7 (p49 – Sources of funding/support – The NICE Guideline Updates Team is an internal team within NICE-evidence review) |
23. Competing interests of guideline development group members have been recorded and addressed. | 7 (disclosure policy and declaration forms) | 7 (p43-CoI- guideline manual). | 7 (p43 – CoI – guideline manual) |
Summary of strengths and limitations | |||
Strengths discussed in the evidence review report. | None reported. | The main strength of this analysis is that it made use of all available data to compare as many treatments as possible using the outputs of the network meta-analyses. This analysis used data on endoscopic relapse in the base case. The committee felt this reflected an important shift in clinical practice toward more emphasis on earlier intervention to promote mucosal healing rather than symptom relief alone. In our analysis, we were able to include a number of trials with longer-term follow-up and adopted a 3-year time horizon for the base-case analysis. (p241- evidence review). | The main strength of this analysis is that it incorporates new RCT evidence that has emerged since the 2013 guideline was produced, expands the number of treatment sequences under comparison, updates the assumptions about rescue therapy to reflect current practice and produces separate cost-effectiveness results for each extent of disease. The model makes use of all available data by drawing on evidence synthesized using network meta-analysis to estimate the relative effects of all treatments of interest in terms of both withdrawal due to adverse events and probability of achieving remission. (p316) |
Limitations discussed in the evidence review report. | None reported. | An insufficient amount of data was available to test alternative assumptions. In addition, some of the estimates of relative effects from the NMA were subject to considerable uncertainty due to sparseness of the network and small sample sizes of a number of trials. We were unable to explicitly model the impact of treatment-specific adverse events in the cost-effectiveness model in the absence of this info. The committee noted that in clinical practice, a number of other treatment options would be considered before reoperation, including dose escalation or switching between TNF inhibitors and other biologic therapies (vedolizumab and ustekinumab). However, there was uncertainty about the optimal strategy and consistency in clinical practice with respect to these options, so they were not explicitly modelled as part of the downstream pathway. The committee noted the high drug costs for infliximab and adalimumab in the base-case model and felt that these do not necessarily reflect locally negotiated prices. (p241 to 242). | Sparseness of data and small sample sizes resulted in high levels of uncertainty in the estimates of relative effectiveness for a number of comparisons. The duration of follow-up in trials for some of the drugs did not match the committee’s experience regarding duration of treatment in practice. This resulted in a mismatch between the time point at which remission was reported in some RCTs for some drugs and the assumption about duration (and therefore cost) of treatment in the cost-effectiveness model. In clinical practice, an assessment of response to treatment would generally take place approximately halfway through a full course of treatment so that people whose disease was not responding to treatment could be switched to another treatment. There was no evidence to suggest different treatments would have any impact on mortality rates. (p316) |
AGREE II = Appraisal of Guidelines for Research and Evaluation II; CD = Crohn disease; ECCO = European Crohn and Colitis Organization; ESPGHAN = European Society for Pediatric Gastroenterology, Hepatology and Nutrition; GRADE = Grading of Recommendations Assessment, Development and Evaluation; NICE = National Institute for Health and Care Excellence; NMA = network meta-analysis; RCT = randomized controlled trial; ROB = risk of bias; TNF = tumour necrosis factor; UC = ulcerative colitis.
aCrohn disease: management. Evidence review for postsurgical maintenance of remission. NICE guideline NG129, Evidence review, May 2019 https://www.nice.org.uk/guidance/ng129/evidence/postsurgical-maintenance-of-remission-pdf-6777581006
bDeveloping NICE guidelines: the manual. NICE process and methods. Published: 31 October 2014. Last updated: 29 May 2024 www.nice.org.uk/process/pmg20
cUlcerative colitis. Evidence reviews for induction of remission in mild-to-moderate ulcerative colitis. NICE guideline NG130, Evidence review, May 2019 https://www.nice.org.uk/guidance/ng130/evidence/may-2019-evidence-review-pdf-6777260893
Appendix 4: Main Study Findings
Please note that this appendix has not been copy-edited.
Table 7: Outcomes Reported in the Systematic Reviews- for Luminal Crohn Disease
First author, year | Description | Findings | Author’s conclusions |
|---|---|---|---|
Remission | |||
Zhang et al. (2023)21 | Thirteen studies comparing early biologics and late biologics reported clinical remission, with the follow-up time ranging from 2 months to 2 years. Among them, 11 studies (2 RCTs and 9 cohort studies) provided available data for clinical remission. | Early biologics vs. late biologics: a pooled RR 1.30 (95% CI, 1.10 to 1.54, I2 = 56.6%). | Early biologic treatment, known as the “top-down approach,” was associated with a statistically significant improvement in clinical remission rates. There was no single specific cut-off for defining early biological therapy, thus for our review, we followed the definition as start of biologicals within 18 to 24 months of diagnosis of CD. |
Hamdeh et al. (2020)19 | Remission within 12 weeks: Three studies comparing early anti–TNF-alpha and late anti–TNF-Alpha were included in this analysis. | Early anti–TNF-alpha and late anti-TNF: a pooled RR 1.94 (95% CI, 1.54 to 2.46; I2 = 0%). | Early anti–TNF-alpha use was associated with a statistically significant increase in the rate of early remission when compared with late use. The certainty in evidence was very low because of the observational nature of 1 of the 3 studies and imprecision (a small number of events). |
Remission beyond 12 weeks: Four studies comparing early anti–TNF-alpha and late anti–TNF-alpha were included in this analysis. | Early anti–TNF-alpha and late anti-TNF: a pooled RR was 1.39 (95% CI, 0.94 to 2.05; I2 = 65%). | Early anti–TNF-alpha use was not associated with a statistically significant increase in the rate of late remission compared with late anti–TNF-alpha use. The certainty in evidence was very low because of the observational nature of 1 of the 4 studies and imprecision (a small number of events). | |
Tsui et al. (2018)11 | Remission, unclear follow-up ranging from 1 to 39 years. Seven studies on adult patients comparing top-down vs. step-up therapy were included. | NAa | Two studies showed an overall positive result from the use of top-down therapy, and 4 showed an overall negative result. With the pediatric cases, 4 studies showed an overall positive result from the use of top-down therapy and 1 study showed an overall negative result. The last study showed a tiered result in which early biologic therapy was superior to early immunomodulators, superior to step-up therapy. |
Relapse | |||
Zhang et al. (2023)21 | Remission, unclear follow-up, ranging from 2 months to 2 years. Five among 13 included studies comparing early biologics and late biologics (1 RCTs + 4 cohort studies) provided relapse data for analysis. | Early biologics vs. late biologics: a pooled RR 0.33 (95% CI, 0.21 to 0.53, I2 = 0.0%). | Regarding relapse rates, the early biologic treatment was associated with a 65% reduction in relapse rates among pediatric CD cases compared to conventional therapy. |
Surgery | |||
Law et al. (2023)20 | For Luminal CD, risk of IBD-related surgery ranging from 24 months to 172 months. | Early biologics vs. late biologics: a pooled OR 0.63 (95% CI, 0.48 to 0.84, I2 = 0.0%). | In patients with CD, early biologic therapy was associated with lower odds of surgery compared with late treatment. |
For UC, risk of IBD-related surgery ranging from 24 months to 172 months | Early biologics vs. late biologics: a pooled OR 2.86 (95% CI, 1.30 to 6.30, I2 = 0.0%). | In patients with UC, the odds of colectomy were increased in early biologics compared with late biologics. | |
Hamdeh et al. (2020)19 | Need for surgery (related to underlying CD including bowel and/or perianal disease surgeries). Five studies comparing early anti–TNF-alpha and late anti–TNF-alpha reported the data for analysis. | Early anti–TNF-alpha vs. late anti-TNF: a pooled RR 0.43 (95% CI, 0.26 to 0.69; I2 = 68%). | The early use of anti–TNF-alpha was associated with a statistically significant decreased risk of the need for surgery The certainty in evidence was very low because of the observational nature of the studies and imprecision (a small number of events). |
Tsui et al. (2018)11 | Surgery, unclear follow-up, ranging from 1 to 39 years Four studies comparing top-down vs. set-up therapy reported data for analysis. | NA | Results from 4 of the studies found that top-down therapy was associated with a decrease in rates for surgery. The remaining 2 studies did not associate top-down therapy with better surgical outcomes. |
Mucosal healing | |||
Zhang et al. (2023)21 | Mucosal healing, unclear follow-up, ranging from 2 months to 2 years Three among 13 included studies comparing early biologics and late biologics (all cohort studies) provided data for analysis. | Early biologics vs. late biologics: a pooled RR 1.47 (95% CI, 1.10 to 1.97, I2 = 0.0%). | The results showed that early biologics were associated with increased mucosal healing compared to conventional therapy for treating pediatric CD. |
Tsui et al. (2018)11 | Mucosal healing– follow-up 26 to 41 weeks Two studies evaluated mucosal healing: 1 assessed at 26 weeks, and another 1 at up to 41 weeks after anti–TNF-alpha treatment. | Early biologics vs. conventional therapy: a pooled RR 1.10 (95% CI, 0.63 to 1.91, I2 = 0.0%). | The early use of anti–TNF-alpha was not associated with a statistically significant increased rate of mucosal healing. The certainty in evidence was very low because of the observational nature of the studies and imprecision (a small number of events). |
Disease progression | |||
Hamdeh et al. (2020)19 | Disease progression was defined as a lack of clinical response leading to either escalation of medication dosages, hospitalizations, or complications of the disease). Five studies comparing early anti–TNF-alpha and late anti–TNF-alpha reported the data. | Early anti–TN-alpha vs. late anti-TNF: a pooled RR 0.51 (95% CI, 0.35 to 0.75; I2 = 61%). | Early anti–TNF-alpha use was associated with a significant decrease in the rate of disease progression compared with late use. The certainty in evidence was very low because of the observational nature of 1 of the studies and imprecision (a small number of events). |
Clinical response | |||
Hamdeh et al. (2020)19 | Clinical response, defined as a significant decrease in the CD activity index by more than 100. Two studies comparing early anti–TNF-alpha and late anti–TNF-alpha reported the data. | No meta-analysis was conducted due to wide variation in the timing of clinical response. RRs (early anti–TNF-alpha vs. late anti–TNF-alpha) from individual studies:
RR1.40 (95% CI, 1.08to 1.82) and RR1.38 (95% CI, 1.01 to 1.88) at weeks 26 and 52 | The certainty in evidence was very low because of the observational nature of the studies and imprecision (a small number of events). |
CD = Crohn disease; IBD = inflammatory bowel disease; NA = not applicable; RR = relative risk; TNF alpha = tumour necrosis factor alpha; UC = ulcerative colitis.
aNo quantitative findings reported.
Table 8: Outcomes Reported in the Primary Studies- Randomized Controlled Trials
Outcome | Noor et al. (2024)23 | Jongsma et al. (2022)24 |
|---|---|---|
Remission | ||
Sustained steroid-free and surgery-free remission- completion of steroid induction course (≤ 8 weeks) through to week 48 | Top-down: 79% (149/189) Accelerated step-up: 15% (29/190) Difference between groups: 64% (95% CI, 57% to 72%), P < 0.0001 | NR |
Endoscopic remission- completion of steroid induction course (≤ 8 weeks) through to week 48 | Top-down vs. accelerated step-up, difference between groups: 23% (95% CI, 11% to 36%), P < 0.0001 | NR |
Endoscopic remission – week 10 | NR | First-line IFX: 16/27 (59%) Conventional: 5/30 (17%) P = 0.001 |
Endoscopic remission – week 52 | NR | First-line IFX: 5/18 (28%) Conventional: 5/14 (36%) P = 0.001 |
Clinical remission without need for treatment escalation – week 52 | NR | First-line IFX: 19/46 (41%) Conventional: 7/48 (15%) First-line IFX vs Conventional, absolute difference: 26% (95% CI, 0.18% to 0.35%), P = 0.004 |
Clinical remission, % – week 10 | NR | First-line IFX: 24/41(59%) Conventional: 15/44 (34%) P = 0.021 |
Clinical remission, % – week 52 | NR | First-line IFX: 33/47 (70%) Conventional: 26/46 (57%) P = 0.420 |
Simple Endoscopic Score for Crohn disease at week 10, median (IQR) | NR | First-line IFX: 3 (0 to 5) Conventional: 9 (3 to 19) |
Simple Endoscopic Score for Crohn disease at week 52, median (IQR) | NR | First-line IFX: 7 (2 to 7) Conventional: 6 (0 to 10) P = 0.961 |
Disease severity scores | ||
Weighted Paediatric CD Activity Index score- week 52, median (IQR) | NR | First-line IFX: 7.5 (0 to 15) Conventional: 10 (0 to 17.5) P = 0.476 |
Health-Related Quality of life | ||
HRQoL by IBD-Q numerical score – week 48 | Top-down vs. accelerated step-up, difference between groups: 8.54 (95% CI, 3.51 to 13.60), P < 0.0001 | NR |
HRQoL by IMPACT III questionnaire (range from 0 to 100, with a higher score indicating a better HRQoL) – week 14, median (IQR) | NR | First-line IFX:
P < 0.001 Conventional:
P < 0.001 |
Corticosteroid use / treatment escalation | ||
Number of steroid courses- week 48 | Top-down vs. accelerated step-up, difference between groups: –0·87 (95% CI, –0·97 to –0·76), P < 0.0001 | NR |
Treatment escalation (type)- week 52, n (%) | NR | First-line IFX: NR:
Conventional: 36 patients needed treatment escalation:
|
Negative outcome of CD | ||
Number of flares | Top-down vs. accelerated step-up, difference between groups: −1.29 (95% CI, −1.42 to −1.16), P < 0.0001 | NR |
Time-to-treatment escalation from start of induction, %- week 52 | NR | Patients needed treatment escalation First-line IFX: 43% (95% CI, 30% to 57%) Conventional: 75% (95% CI, 60% to 86%) P = 0.001 |
Hospitalization and surgery | ||
Number of hospital admissions and surgeries, difference between groups | Top-down vs. accelerated step-up: –0·12 (95% CI, –0·23 to –0·02), P < 0.023 | NR |
Laboratory levels | ||
Fecal calprotectin level, mcg/g, median (IQR) – week 10 | NR | First-line IFX: 286 (62 to 596) Conventional: 545 (279 to 1108) P = 0.004 |
Patients with a fecal calprotectin (Fcal) level < 100 mcg/g – week 10, n (%) | NR | First-line IFX: 13/39 (33%) Conventional: 8.4 (2.0 to 23.8) P < 0.036 |
Fcal < 100 mcg/g – week 52, n (%) | NR | First-line IFX: 17/48 (35%) Conventional: 9/47 (19%) P = 0.120 |
C-reactive protein (mg/L), median (IQR) – week 10 | NR | First-line IFX: 2.0 (0.8 to 3.2) Conventional: 8.4 (2.0 to 23.8) P < 0.001 |
Erythrocyte sedimentation rate (mm/hour), median (IQR) – week 10 | NR | First-line IFX: 6.5 (3.0 to 17.3) Conventional: 17 (8.0 to 33.0) P = 0.003 |
Total leucocyte count (109/L), median (IQR) – week 10 | NR | First-line IFX: 5.5 (4.8 to 7.1) Conventional: 7.3 (5.9 to 9.3) P = 0.001 |
Others | ||
Change in SDS height-for-age – week 52 | NR | First-line IFX: 0.08 (−0.05 to 0.21) Conventional: −0.08 (−0.23 to 0.04) P = 0.002 |
Serious adverse events (SAE) | ||
Any SAE, n | Top-down: 15 Accelerated step-up: 42 No reported malignancies or deaths during the trial in both groups. | First-line IFX: 6 Conventional: 9 |
List of SAE- week 48, number of events, number of patients (%) | List of SAE- week 52, number of patients | |
Hospitalization | For flare of CD Top-down: 3, 3 (2%) Accelerated step-up: 15, 12 (6%) | NR |
Surgery | For disease complication Top-down: 2, 2 (1%) Accelerated step-up: 11, 10 (5%) | For Ileocecal resection First-line IFX: 1 Conventional: 2 |
Abdominal surgery | Top-down: 1, 1 (1%) Accelerated step-up: 10, 9 (5%) | NR |
Perianal surgery | Top-down: 1, 1 (1%) Accelerated step-up: 1, 1 (1%) |
|
Medication related | Top-down: 1, 1 (1%) Accelerated step-up: 1, 1 (1%) | NR |
Serious infection | Top-down: 3, 3 (2%) Accelerated step-up: 8, 4 (2%) | NR |
Hospitalization | NR | First-line IFX: 2 Conventional: 3 |
Psychosis | NR | First-line IFX: 1 Conventional: 0 |
Safety (adverse events) | ||
Any AE | Top-down: 168 Accelerated step-up: 315 | NR |
Flare of CD, number of events, number of patients (%) | Top-down: 30, 26 (13%) Accelerated step-up: 225, 132 (68%) | NR |
Infection | Top-down: 23, 16 (8%) Accelerated step-up: 20, 12 (6%) | NR |
Thiopurine intolerance | Top-down: 87, 62 (32%) Accelerated step-up: 59, 48 (25%) | NR |
Methotrexate intolerance | Top-down: 8, 6 (3%) Accelerated step-up: 9, 4 (2%) | NR |
AE = adverse events; CD = Crohn disease; IBD-Q = Inflammatory Bowel Disease Questionnaire; CI = confidence interval; IFX = infliximab; IQR = interquartile range; L = litres; n = number of participants; NR = not reported; HRQoL = health-related quality of life; SAE = severe adverse event; SES-CD = Simple Endoscopic Score for Crohn Disease; wPCDAI = weighted Paediatric CD Activity Index score.
Table 9: Summary of Recommendations in Included Guidelines
Population relevant to the recommendations | First-line pharmacotherapy for the induction of remission | First-line pharmacotherapy for the maintenance of remission | Second-line pharmacotherapy for the maintenance of remission | Third-line pharmacotherapy for the maintenance of remission |
|---|---|---|---|---|
NICE guideline [NG129] (2019)26 for Crohn disease | ||||
Adults, children, and young people with CD | First presentation or a single inflammatory exacerbation of CD in a 12-month period:
| Azathioprine or mercaptopurine, particularly for those with adverse prognostic factors such as early age of onset, perianal disease, glucocorticosteroid use at presentation and severe presentations (p13) No budesonide after completing macroscopic resection of ileocolonic CD (p15) | Induction Two or more inflammatory exacerbations in a 12-month period or glucocorticosteroid dose cannot be tapered:
Maintenance: Methotrexate if inducing remission, not tolerated or contraindicated to azathioprine or mercaptopurine (p13) | Induction Adults with severe active CD: Infliximab or adalimumab monotherapy or combined with an immunosuppressant if not responded, not tolerated, or contraindicated to conventional therapy (including immunosuppressive and/or corticosteroid) (p9 to 10) People (6 to 17 years) with severe active CD: Infliximab if not responded, not tolerated, or contraindicated to conventional therapy (including corticosteroids, immunomodulators, and primary nutrition therapy) (p11) Active fistulizing CD: Infliximab if not responded, not tolerated, or contraindicated to conventional therapy (including antibiotics, drainage and immunosuppressive treatments) (p10) Adults with moderate-to-severe active CD after previous treatment: Ustekinumab (https://www.nice.org.uk/guidance/ta456/chapter/1-Recommendations) or Vedolizumab (https://www.nice.org.uk/guidance/ta352/chapter/1-Guidance), if inadequate response with, lost response to, intolerant, or contraindicated to either conventional therapy or a TNF-alpha inhibitor Maintenance:
|
For CD: ECCO-ESPGHAN Guideline Update (2020)25 for Crohn disease | ||||
Children and adolescents with luminal CD | Active luminal CD:
New-onset with high risk:
| Methotrexate as a first-choice immunomodulator or after thiopurine failure or intolerance (Statement12, LoE: 3 | Agreement: 96%) thiopurines [azathioprine or 6-mercaptopurine] (Statement 13, LoE: 3 | Agreement: 88%) Low risk:
| Induction Thiopurnes monotherapy should not be used. (Statement 10, LoE: 4 | Agreement:100%) | Induction
Maintenance postoperative use of anti-TNF drugs in patients with high risk of recurrence (Statement 15, LoE: 3 | Agreement: 100%) |
Children and adolescents with fistulizing perianal CD | anti-TNF therapy in combination with antibiotic therapy, surgical treatment, or both. (Statement 11, LoE: 3 | Agreement: 100%) | anti-TNF therapy in combination with antibiotic therapy (Statement 11, LoE: 3 | Agreement: 100%) | NA | NA |
NICE guideline [NG130] (2019)27 for ulcerative colitis | ||||
Adults, children, and young people with UC | Mild-to-moderate:
Acute severe:
|
| INDUCTION Acute severe: IV ciclosporine added to IV corticosteroids or surgery if no improvement or symptoms worsen despite corticosteroid treatment (p10) | INDUCTION Acute severe: Infliximab if ciclosporin contraindicated or clinically inappropriate, or in clinical trials (p10) |
CD = Crohn disease; ECCO- ESPGHAN = European Crohn and Colitis Organization-European Society for Paediatric Gastroenterology Hepatology and Nutrition; EEN = exclusive enteral nutrition; IBD = inflammatory bowel disease; IV = IV; LoE = level of evidence; NA = not applicable; NICE = National Institute for Health and Care Excellence; TNF = tumour necrosis; UC = ulcerative colitis.
Appendix 5: Overlap Between Included Systematic Reviews
Please note that this appendix has not been copy-edited.
Table 10: Overlap in Relevant Primary Studies Between Included Systematic Reviews
Primary study citation | Law et al. (2023)20 | Zhang et al. (2023)21 | Hamdeh (2020)19 | Tsui (2018)11 |
|---|---|---|---|---|
Ma C, et al. Can J Gastroenterol Hepatol. 2016;2016:2079582. | Yes | — | — | — |
De Caro G, et al. Am J Gastroenterol. 2015;110: S823 | Yes | — | — | — |
Pineton de Chambrun G, et al. Gastroenterology. 2015;148(4): S-864. | Yes | — | — | — |
Dulai PS, et al. J Crohns Colitis. 2020;15(2):195 to 202. | Yes | — | — | — |
Han M, et al. Yonsei Med J. 2020;61(5):382 to 390. | Yes | — | — | — |
Hoekman DR, et al. J Crohns Colitis. 2018;12(5):517 to 524. | Yes | — | — | — |
Jung YS, et al. Korean J Intern Med. 2020;35(5):1104 to 1113. | Yes | — | — | — |
Ma C, et al. Inflamm Bowel Dis. 2016;22(4):870 to 879. | Yes | — | Yes | Yes |
Mantzaris GJ, et al. Crohns Colitis 360. 2021;3(4):otab064. | Yes | — | — | — |
Markowitz J, et al. Gastroenterology. 2012;142(5 suppl 1):S-600. | Yes | — | — | — |
Minhas A, et al. Am J Gastroenterol. 2010;105:S439. | Yes | — | — | — |
Mir SAV, et al. J Clin Gastroenterol. 2014;48(3):248 to 252. | Yes | — | — | — |
Oh EH, et al. PLoS One. 2017;12(5):e0177479. | Yes | — | — | — |
Patel H, et al. Am J Gastroenterol. 2018;113:S8. | Yes | — | — | — |
Schnitzler F, et al. Crohns Colitis 360. 2021;3(3):otab060. | Yes | — | — | — |
Seitz T, et al. United Eur Gastroenterol J. 2018;6(8):A108. | Yes | — | — | — |
Singh H, et al. Scand J Gastroenterol. 2021;56(4):397 to 402. | Yes | — | — | — |
Zhu M, et al. BMC Gastroenterol. 2020;20(1):421. | Yes | — | — | — |
Schreiber S, et al. J Crohns Colitis. 2013;7:213 to 221. | — | — | Yes | — |
Nuij V, et al. J Crohns Colitis. 2015;9:997 to 1003. | — | — | Yes | — |
Harper J and Zisman T. Inflamm Bowel Dis. 2012;18:S31–S32. | — | — | Yes | — |
Colombel JF, et al. Aliment Pharmacol Ther. 2015;41:734 to 746. | — | — | Yes | — |
Matsumoto T, et al. Dis Colon Rectum. 2008;51:916 to 923. | — | — | Yes | — |
Miyoshi J, et al. Digestion. 2014;90:130 to 136. | — | — | Yes | — |
Colombel JF, et al. Clin Gastroenterol Hepatol. 2014;12:414 to 422.e5. | — | — | Yes | — |
Frei R, et al. J Crohns Colitis. 2019;13:1292 to 1301. | — | — | Yes | — |
De Chambrun GP, et al. Gastroenterology. 2015;148:S–864. | — | — | Yes | — |
Oh EH, et al. Plos One. 2017;12:e0177479. | — | — | Yes | — |
Markowitz J, et al. 2000;119(4):895 to 902. | — | Yes | — | Yes |
Punati J, et al. Inflamm Bowel Dis. 2008;14(7):949 to 54. | — | Yes | — | Yes |
Hyams JS, et al. Inflamm Bowel Dis 2009;15:816 to 22. | — | Yes | — | — |
Lee JS, et al. World J Gastroenterol 2010;16:1776 to 81. | — | Yes | — | Yes |
Kim MJ, et al. Acta Paediatr 2011;100:451 to 5. | — | Yes | — | |
Walters TD, et al. Gastroenterology 2014;146:383 to 91 | — | Yes | — | Yes |
Nuti F, et al. J Crohns Colitis 2016;10:5 to 12 | — | Yes | — | — |
Kang B, et al. J Crohns Colitis 2016;10:1279 to 86 | — | Yes | — | — |
Lee D, et al. Inflamm Bowel Dis 2015;21:1786 to 93 | — | Yes | — | — |
Assa A, et al. Gastroenterology 2019;157:985 to 96 | — | Yes | — | — |
Lee YM, et al. J Pediatr Gastroenterol Nutr 2015;60:737 to 43. | — | Yes | — | — |
Lee YS, et al. Pediatr Gastroenterol Hepatol Nutr 2012;15:243 to 9. | — | Yes | — | Yes |
Olbjørn C, et al. Scand J Gastroenterol 2014;49:1425 to 31. | — | Yes | — | Yes |
D’Haens G, et al. Lancet 2008;371:660 to 667. | — | — | — | Yes |
Fan R,et al. World J Gastroenterol 2014;20:14479 to 14487. | — | — | — | Yes |
Panés J, et al. Gastroenterology 2013;145:766 to 774.e1. | — | — | — | Yes |
Cosnes J, et al. Gastroenterology 2013;145:758 to 765.e2. | — | — | — | Yes |
Khanna R, et al. Lancet 2015;386:1825 to 1834. | — | — | — | Yes |
Ghazi LJ, et al. Inflamm Bowel Dis 2013;19:1397 to 1403. | — | — | — | Yes |
Kim NH, et al. Intest Res 2014;12:281 to 286. | — | — | — | Yes |
Kwak MS, et al. BMC Gastroenterol 2014;14:85. | — | — | — | Yes |
Chatu S, et al. Am J Gastroenterol 2014;109:409 to 416. | — | — | — | Yes |
Ramadas AV, et al. Gut 2010;59:1200 to 1206. | — | — | — | Yes |
Kariyawasam VC, et al. Inflamm Bowel Dis 2014;20:1382 to 1390. | — | — | — | Yes |
Lakatos PL, et al. Am J Gastroenterol 2012;107:579 to 588. | — | — | — | Yes |
Appendix 6: References of Potential Interest
Please note that this appendix has not been copy-edited.
Evidence-Based Guideline
Published in Spanish
Sicilia B, García-López S, González-Lama Y, et al. GETECCU 2020 guidelines for the treatment of ulcerative colitis. Developed using the GRADE approach. Gastroenterol Hepatol. 2020 Aug;43 Suppl 1:1-57. PubMed
Fuxman C, Sicilia B, Linares ME, et al. GADECCU 2022 Guideline for the treatment of Ulcerative Colitis. Adaptation and updating of the GETECCU 2020 Guideline. Gastroenterol Hepatol. 2023 Mar;46 Suppl 1:S1-S56. PubMed
Systematic Reviews
Alternate Comparator
Avedillo-Salas A, Corral-Cativiela S, Fanlo-Villacampa A, Vicente-Romero J. The Efficacy and Safety of Biologic Drugs in the Treatment of Moderate-Severe Crohn's Disease: A Systematic Review. Pharmaceuticals (Basel). 2023;16(11). PubMed
Shehab M, Alrashed F, Heron V, Restellini S, Bessissow T. Comparative Efficacy of Biologic Therapies for Inducing Response and Remission in Fistulizing Crohn's Disease: Systematic Review and Network Meta-Analysis of Randomized Controlled Trials. Inflamm Bowel Dis. 2023;29(3):367-375. PubMed
Yin J, Li Y, Chen Y, Wang C, Song X. Adalimumab for induction of remission in patients with Crohn's disease: a systematic review and meta-analysis. Eur J Med Res. 2022;27(1):190. PubMed
Rui M, Fei Z, Wang Y, et al. Will the Inducing and Maintaining Remission of Non-biological Agents and Biological Agents Differ for Crohn's Disease? The Evidence From the Network Meta-Analysis. Front Med (Lausanne). 2021;8:679258. PubMed
Singh S, Murad MH, Fumery M, et al. Comparative efficacy and safety of biologic therapies for moderate-to-severe Crohn's disease: a systematic review and network meta-analysis. Lancet Gastroenterol Hepatol. 2021;6(12):1002-1014. PubMed
Singh S, Murad MH, Fumery M, Dulai PS, Sandborn WJ. First- and Second-Line Pharmacotherapies for Patients With Moderate to Severely Active Ulcerative Colitis: An Updated Network Meta-Analysis. Clin Gastroenterol Hepatol. 2020;18(10):2179-2191 e2176. PubMed
Singh S, Facciorusso A, Dulai PS, Jairath V, Sandborn WJ. Comparative Risk of Serious Infections With Biologic and/or Immunosuppressive Therapy in Patients With Inflammatory Bowel Diseases: A Systematic Review and Meta-Analysis. Clin Gastroenterol Hepatol. 2020;18(1):69-81 e63. PubMed
Abbass M, Cepek J, Parker CE, et al. Adalimumab for induction of remission in Crohn's disease. Cochrane Database Syst Rev. 2019;2019(11). PubMed
Trigo-Vicente C, Gimeno-Ballester V, Garcia-Lopez S, Lopez-Del Val A. Systematic review and network meta-analysis of treatment for moderate-to-severe ulcerative colitis. Int J Clin Pharm. 2018;40(6):1411-1419. PubMed
Nelson SM, Nguyen TM, McDonald JW, MacDonald JK. Natalizumab for induction of remission in Crohn's disease. Cochrane Database Syst Rev. 2018;8(8):CD006097. PubMed
Lee MJ, Parker CE, Taylor SR, et al. Efficacy of Medical Therapies for Fistulizing Crohn's Disease: Systematic Review and Meta-analysis. Clin Gastroenterol Hepatol. 2018;16(12):1879-1892. PubMed
Alternate Definition for “Early Use” of Biologics (Not in Scope)
Attauabi M, Steenholdt C, Poulsen A, et al. Network meta-analysis: Comparative onset of early effect of biologics and small molecules in moderately to severely active luminal Crohn's disease. Aliment Pharmacol Ther. 2024;60(2):124-143. PubMed
Gordon M, Sinopoulou V, Akobeng AK, Sarian A, Moran GW. Infliximab for maintenance of medically-induced remission in Crohn's disease. Cochrane Database Syst Rev. 2024;2(2):CD012609. PubMed
Gao J, Nie R, Chen Y, Yang W, Ren Q. Comparative of the effectiveness and safety of biological agents, small molecule drugs, and microbiome therapies in ulcerative colitis: Systematic review and network meta-analysis. Medicine (Baltimore). 2023;102(43):e35689. PubMed
Gordon M, Sinopoulou V, Akobeng AK, et al. Infliximab for medical induction of remission in Crohn's disease. Cochrane Database Syst Rev. 2023;11(11):CD012623. PubMed
ISSN: 2563-6596
This appraisal was conducted by the by the POst-Market Drug Evaluation Team (PODET) through the Post-Market Drug Evaluation CoLab Network. This work was supported by Canada’s Drug Agency (CDA-AMC) and its Post-Market Drug Evaluation Program through funding provided by Health Canada.
CDA-AMC is a pan-Canadian health organization. Created and funded by Canada’s federal, provincial, and territorial governments, we’re responsible for driving better coordination, alignment, and public value within Canada’s drug and health technology landscape. We provide Canada’s health system leaders with independent evidence and advice so they can make informed drug, health technology, and health system decisions, and we collaborate with national and international partners to enhance our collective impact.
CoLab is a pan-Canadian network of experts in applied research, scientific methods, and data analysis. CoLab members work with the Post-Market Drug Evaluation Program to produce credible and timely evidence on postmarket drug safety and effectiveness.
Disclaimer: CDA-AMC has taken care to ensure that the information in this document was accurate, complete, and up to date when it was published, but does not make any guarantee to that effect. Your use of this information is subject to this disclaimer and the Terms of Use at cda-amc.ca.
The information in this document is made available for informational and educational purposes only and should not be used as a substitute for professional medical advice, the application of clinical judgment in respect of the care of a particular patient, or other professional judgments in any decision-making process. You assume full responsibility for the use of the information and rely on it at your own risk.
CDA-AMC does not endorse any information, drugs, therapies, treatments, products, processes, or services. The views and opinions of third parties published in this document do not necessarily reflect those of CDA-AMC. The copyright and other intellectual property rights in this document are owned by the Canadian Agency for Drugs and Technologies in Heath (operating as CDA-AMC) and its licensors.
This document is the property of PODET. CDA-AMC has a nonexclusive, limited, royalty-free, worldwide, nontransferable, fully paid-up, and irrevocable license to use the report in support of its objects, mission, and reasonable operational requirements.