Drugs, Health Technologies, Health Systems
Health Technology Review
Voice Prostheses and Heat and Moisture Exchangers for Adults After Total Laryngectomy: An Updated Rapid Review
Key Messages
What Is the Issue?
Total laryngectomy is a surgical procedure that removes the larynx. During the surgery, the trachea is diverted to an opening in the neck called a stoma. This change in breathing pattern is permanent, significantly impacting the ability to swallow, breathe, and speak, greatly impacting overall quality of life.
Postlaryngectomy interventions include olfactory, voice, and swallowing rehabilitation and addressing the psychosocial aspects of patient recovery. Voice rehabilitation is an important aspect of postlaryngectomy care to restore vocal communication. An esophageal voice (EV), an artificial larynx (electrolarynx), and a tracheoesophageal voice (TEV) with voice prosthesis are options for restoring voice communication in adults following total laryngectomy.
The population of patients in Canada undergoing total laryngectomy is relatively small. There is reported to be well established clinical care for postlaryngectomy voice rehabilitation, yet the current evidence is limited. A request for a review of the evidence to inform policy decisions related to voice prostheses (indwelling and nonindwelling devices) and heat and moisture exchangers (HME) for adults following total laryngectomy was submitted to Canada’s Drug Agency (CDA-AMC).
What Did We Do?
This is an update of a Rapid Review report published in October 2024, It includes 1 additional systematic review and extends the Rapid Review methodology to include the engagement of clinical specialists and the lived experience of patients following a laryngectomy.
We aimed to identify and summarize related evidence and recommendations from systematic reviews, health economic evaluations, and evidence-based guidelines with a contextual evaluation of clinical and patient experiences. The clinical research questions were codeveloped with the project requester.
We searched journal databases and grey literature for relevant evidence published since January 2019. We used a 5-year search period for this review, considering that the identified systematic reviews had searched earlier periods. Three patients were interviewed to gain insight on their experience using these devices. One speech and language pathologist with experience working with patients following laryngectomy provided clinical expert review of this report.
What Did We Find?
The use of voice prostheses and HMEs for adults following total laryngectomy is reported by clinicians to be common practice across Canada. Both patients and the speech and language pathologist who reviewed this report underscore the importance of these devices in supporting voice restoration, pulmonary rehabilitation, infection prevention, and quality of life following surgery.
Nine eligible publications were identified, including 5 systematic reviews, 3 economic evaluations, and 1 evidence-based guideline. Owing to various methodological limitations, confidence in the evidence identified was determined to be very low.
Three patients reported that using voice prostheses and HMEs after total laryngectomy is critical to their ability to communicate, maintain independence, and prevent lung infection. While there are challenges with maintaining the devices and additional costs for the supplies needed to support use, the benefits of these devices were seen to outweigh these challenges.
Two systematic reviews compared TEV using voice prostheses with EV. Whereas 1 systematic review reported that TEV with voice prostheses may have a more positive impact on quality-of-life measures, 1 systematic review found no statistically significant differences in Voice Handicap Index (VHI) scores and voice-related quality of life (VRQoL). The speech and language pathologist who reviewed this report highlighted the difficulty associated with learning EV compared to voice prostheses. One of our patient partners agreed with this and mentioned they had not encountered patients within their community who used EV exclusively.
One systematic review with network meta-analysis compared 10 voice prostheses (8 indwelling and 2 nonindwelling). This review did not compare indwelling and nonindwelling devices as 2 distinct groups. Critical methodological flaws with this systematic review were identified. Most comparisons between various voice prostheses showed no statistically significant differences in device replacements, device lifetime, airflow resistance, leakage, speech rate, maximum phonation time, patient device preference, phonatory effort, fundamental frequency, voice loudness, speech intelligibility, dislodgement, fistula problems, granulation, prosthesis inaccurate size, prosthesis deterioration, and survival rate. Many effect estimates were imprecise — that is, the confidence intervals were wide, including the potential that either of the devices being compared could be favoured.
One systematic review reported that using HMEs, compared to no HMEs, significantly improved several clinical outcomes, including a decrease in mucus production, coughing, forced expectorations, the number of days requiring chest physiotherapy after surgery, tracheobronchitis or pneumonia episodes, and improved patient satisfaction.
No evidence regarding the cost-effectiveness of voice prostheses versus no prostheses, indwelling versus nonindwelling prostheses, or comparisons among different nonindwelling prostheses for adults following laryngectomy was identified. From a US perspective, HMEs were reported to be cost-effective compared to alternative stoma covers (ASCs). These findings may not be generalizable to Canada due to differences in health care systems.
One evidence-based guideline developed in Spain recommended replacing the prosthesis with a double-flanged one, such as Provox XtraSeal, adjusting the diameter and length, or placing a silicone sheet (or ring) on the tracheal side of the prosthesis to manage periprosthetic leakage. Our review did not identify any evidence-based guidelines regarding the use of HME for adults following total laryngectomy.
What Does It Mean?
The clinical and patient community we engaged with consider voice prostheses and HMEs to be essential devices. The evidence base related to their benefit and cost-effectiveness is limited. The perspectives of speech and language pathologists working with patients, and of patients who have lived experience with these devices, may supplement decision-making by contextualizing the evidence currently available.
Decisions regarding the choice of voice prosthesis should consider patients’ tracheoesophageal puncture (TEP) shape and size, patients’ values and preferences, accessibility, affordability, and other factors such as physical and mental capabilities, caregiver support, and patient motivation.
While the evidence is limited, patients and clinicians report that adding HMEs could be beneficial in several clinical outcomes, such as mucus reduction, infection prevention, and reported patient satisfaction.
Future systematic reviews should be planned and conducted in alignment with recognized methodological standards and should be transparently reported. As the certainty of evidence from high-quality systematic reviews relies, in part, on the risk of bias of their included studies, future primary studies should aim to draw from developed patient registries.
Abbreviations
ASC
alternative stoma cover
EV
esophageal voice
GRADE
Grading of Recommendations Assessment, Development and Evaluation
HME
heat and moisture exchanger
ICER
incremental cost-effectiveness ratio
NMA
network meta-analysis
QALY
quality-adjusted life-years
QoL
quality of life
SF-36
36-item short form survey instrument
TEP
tracheoesophageal puncture
TEV
tracheoesophageal voice
VHI
Voice Handicap Index
VRQoL
voice-related quality of life
Context and Policy Issues
What Is a Total Laryngectomy?
A laryngectomy is a surgical procedure involving the partial or total removal of the larynx.1,2 A total laryngectomy is indicated for several reasons, including neck injuries and advanced squamous cell carcinomas of the larynx or hypopharynx that have not metastasized distantly.2,3 In Canada, from 2003 to 2007, approximately 900 new laryngeal cancer cases were diagnosed in males and 195 in females, representing roughly 1.1% and 0.3% of all new cancer cases, respectively.4 The total laryngectomy procedure impacts a patient’s ability to swallow, breathe, and speak, and it necessitates breathing through a surgically created stoma. Following surgery, there is a need for specialized care and rehabilitation to restore essential functions.5,6
Postlaryngectomy interventions include olfactory, voice, and swallowing rehabilitation and addressing the psychosocial aspects of patient recovery.7-9 For patients who have undergone laryngectomy, interdisciplinary collaboration and personalized care plans are essential to optimize outcomes and improve the quality of life.7,8 Voice rehabilitation is an important aspect of postlaryngectomy care to restore vocal communication. Ensuring there is sufficient heat and moisture in the airway, often using HMEs, is also important because the disconnection of the upper and lower airways results in the loss of natural conditioning of inhaled air (humidification, filtration, and heating). Therefore, HMEs may support improved patient outcomes.10-12
What Are Commonly Used Approaches for Voice Restoration?
The commonly used approaches to restore voice and communication for patients who have undergone a total laryngectomy include EV, an artificial larynx (electrolarynx), and/or TEV restoration using a voice prosthesis.13 Successful voice restoration has a wide-ranging positive effect, improving quality of life, enhancing employment prospects, strengthening family relationships, and facilitating access to essential services.14,15
EV involves introducing and expelling air from the esophagus to produce sound.13 EV provides the benefit of hands-free verbal communication without the need for devices.13 EV, for which air is “swallowed” or “injected” and then “released” or “burped” for voice production, differs from lung-powered voice. Due to a limited air supply, it is often quieter, requires more effort, and has reduced utterance length than a lung-powered voice.16,17 EV often has a lower pitch and a “wet” quality, which can reduce intelligibility.16 Anatomical-physiological, patient-related, and treatment- and rehabilitation-related factors could impact a patient’s ability to use EV effectively.18 Mastering EV can be difficult, often requiring 4 to 6 months or more to achieve proficiency. Furthermore, there is a significant shortage of skilled EV trainers, and less than 30% of patients use EV as their primary method of communication.13
The electrolarynx is a battery-powered device used for voice, also offering communication. It has a mechanical sound and typically requires one-handed operation.13 To achieve more natural-sounding speech, some modern electrolarynx models offer pitch features.13 Choosing the best electrolarynx requires careful consideration of factors such as sufficient sound transfer to ensure clear speech and the individual's personal preference.13
TEV restoration, either performed during (primary TEP) or after (secondary TEP) laryngectomy, provides the most comparable speech alternative to natural, fluent speech and ease of voice production.13 Typically, TEV with voice prosthesis is reported to result in better voice quality and intelligibility than EV and electrolarynx voice.19 However, TEV with voice prosthesis requires considerable financial resources and time to learn.13
What Are Voice Prostheses and HMEs?
A voice prosthesis is a small medical device that incorporates a one-way valve, allowing patients to produce sounds by directing air from their lungs through the valve and into their vocal cavity. Typically, the voice prosthesis is placed in a surgically created fistula in the tracheoesophageal wall. Speakers can move air from the trachea through the pharyngoesophageal segment either by manually obstructing the stoma or by using a laryngectomy speaking valve. Subsequently, the movement of the vocal cavity structures shapes the sound into words for speech production.13
Voice prostheses can be classified as either indwelling or nonindwelling based on whether they can be removed and managed by the patient. Nonindwelling prostheses are removable by patients and can be changed, yet this requires the stoma to be easily accessible and for patients to have sufficient cognitive capacity, eyesight, and dexterity to remove and reinsert the device.20 Indwelling prostheses are exclusively changed by health care professionals (e.g., a physician or speech-language pathologist) and often have a longer lifespan than nonindwelling prostheses.13,20 Device life or durability significantly impacts patient satisfaction and quality of life.21 The median device life before leakage has been reported to be generally longer for indwelling prostheses (70 days) compared to nonindwelling prostheses (38 days).21 On average, TEV speakers require 4 to 6 voice prosthesis replacements annually, making management and replacement potentially costly.13
Ensuring there is sufficient heat and moisture supplied to the airway — often using HMEs or, alternatively, an external humidification system — is also important because the disconnection of the upper and lower airways results in the loss of natural conditioning of inhaled air (humidification, filtration, and heating).10-12 In the 1990s, HME devices were introduced for patients following total laryngectomy.10 These devices help compensate for the loss of the upper airway's natural humidifying and filtering functions after laryngectomy. Although some studies have shown that HMEs could potentially improve pulmonary function, reduce respiratory symptoms, and enhance overall quality of life compared with the conventional external humidification system, these potential benefits are limited in the short term (e.g., within approximately 12 days or 6 weeks) and are not consistently observed across all clinical outcomes.10-12 It is important to note that voice prostheses and HMEs can be used independently, and patients who use an electrolarynx following a total laryngectomy can still benefit from HMEs for pulmonary rehabilitation.22
Why Is It Important to Do This Review?
This report was conducted in response to a request from a provincial payer seeking to identify the evidence regarding the effectiveness and costs of, as well as any evidence-based recommendations on, these devices for adults following total laryngectomy.
Given the impact on quality of life that a total laryngectomy has for patients, it is important to evaluate the clinical and cost-effectiveness of these devices to inform decision-making. Earlier reviews have noted that the evidence to inform postlaryngectomy voice rehabilitation is limited. For instance, a previous Rapid Review by CADTH published in 2017 indicated that studies of the effectiveness and lifespan of different indwelling voice prostheses for adults following laryngectomy had inconsistent results and, at that time, did not identify any cost-effectiveness studies or clinical practice guidelines.20 Expenses may be a barrier to patients accessing the devices they need, and this issue deserves to be explored.
Objective
This Rapid Review collates evidence regarding the clinical and cost-effectiveness of voice prostheses (indwelling and nonindwelling devices) and HMEs for adults following total laryngectomy. It summarizes the related guideline recommendations available for this patient population. To contextualize the clinical and economic evidence, this Rapid Review incorporates the perspectives and experiences of patient partners. The research questions and the inclusion and exclusion criteria (scope of the review) are outlined in the following sections.
Research Questions
What is the clinical effectiveness of voice prostheses versus no voice prostheses for adults following total laryngectomy?
What is the comparative clinical effectiveness of various indwelling and nonindwelling voice prostheses for adults following total laryngectomy, specifically comparing indwelling versus other indwelling devices, nonindwelling versus other nonindwelling devices, and indwelling versus nonindwelling devices?
What is the clinical effectiveness of using a heat and moisture exchanger compared to no heat and moisture exchanger for adults following total laryngectomy?
What is the cost-effectiveness of voice prostheses versus no voice prostheses for adults following total laryngectomy?
What is the comparative cost-effectiveness of various indwelling and nonindwelling voice prostheses for adults following total laryngectomy, specifically comparing indwelling devices versus other indwelling devices, nonindwelling devices versus other nonindwelling devices, and indwelling versus nonindwelling devices?
What is the cost-effectiveness of heat and moisture exchangers compared to no heat and moisture exchangers for adults following total laryngectomy?
What are the evidence-based guidelines regarding the use of voice prostheses or heat and moisture exchangers for adults following total laryngectomy?
Methods
An information specialist conducted a customized literature search, balancing comprehensiveness with relevancy, of databases and grey literature on July 18, 2024. This search was updated on November 19, 2024. One reviewer screened citations and selected studies based on the inclusion criteria presented in Table 1. One reviewer extracted data from the included studies and completed critical appraisals.
No changes to the report objectives or research questions or literature search strategy were made to this updated review. The updated Rapid Review has been augmented to incorporate independent clinical review from an experienced speech and language pathologist and lived experiences from 3 patient partners who had undergone a laryngectomy (inputs gathered via 1 written input and 2 semistructured interviews).
Appendix 1 presents a detailed description of methods along with the search strategy.
Criteria | Description |
|---|---|
Population | Adults following total laryngectomy |
Intervention | Q1, Q2, Q4, Q5, Q7 Voice prostheses including:
Q3, Q6, Q7 Heat and moisture exchanger, with or without voice prostheses |
Comparator | Q1, Q4 No voice prostheses (i.e., esophageal voice) Q2, Q5 Compared to indwelling or nonindwelling voice prosthesis types, inclusive of the following comparisons:
Q3, Q6 No HME Q7 NA |
Outcomes | Q1 to Q3 Clinical benefits and harms (e.g., quality of life, patient satisfaction, depression, anxiety, self-esteem changes, device lifespan, safety) Q4 to Q6 Cost-effectiveness (e.g., cost per QALY gained, ICER) Q7 Recommendations regarding the use of voice prostheses (indwelling or nonindwelling) and HMEs |
Study designs | Health technology assessments, systematic reviews, primary clinical studies, economic evaluations, evidence-based guidelines Q1 to Q3 Prioritized evidence from systematic reviews over primary studies, as available Excluded primary studies contained within included systematic reviews, reporting data for the same comparison outcome were excluded. Single-arm studies were also excluded. |
Exclusion criteria | Articles focused on alternatives to voice prostheses (e.g., electrolarynx) |
HME = heat and moisture exchanger; ICER = incremental cost-effectiveness ratio; NA = not applicable; QALY = quality-adjusted life-year; vs. = versus.
Findings
We identified 9 publications eligible for inclusion, including 5 systematic reviews,23-27 3 economic evaluations,28-30 and 1 evidence-based guideline.31 Figure 1 (Appendix 1) presents the PRISMA32 flow chart of the study selection. Appendix 2 presents additional characteristics of the included studies. This is a relatively small patient population, which inhibits traditional approaches and the highest standards of methodology in primary research. Owing to various methodological limitations, confidence in the evidence identified was assessed as very low. Appendix 3 provides additional details regarding the strengths and limitations of the included publications. Appendix 4 presents results by different outcomes and clinical questions. Appendix 5 presents the GRIPP2 (SF) table, and Appendix 6 presents the list of excluded studies.
Patient Profiles
We engaged 3 patients who have had a laryngectomy. All patients interviewed were patients who had been fitted with a voice prosthesis and use HMEs. Two patients use an indwelling voice prosthesis device, and 1 uses a nonindwelling voice prosthesis device because they require the ability to replace the device themselves because they live far from the hospital. All patients use HMEs on a daily basis. Two of the patients interviewed were female, and the other male. All are now retired and all currently live in British Columbia, with 1 being initially diagnosed and treated in Ontario. The 3 patients interviewed are 1 year, 7 years, and 10 years postlaryngectomy.
Research Question 1: The Clinical Effectiveness of Voice Prostheses Versus No Voice Prostheses for Adults Following Total Laryngectomy
Two systematic reviews assessed the impact of TEV using voice prostheses on quality of life compared to EV without using voice prostheses.23,27
One systematic review (Maniaci, 2024) examined 15 observational studies (11 retrospective controlled studies and 4 uncontrolled retrospective studies) involving 1,085 patients who had undergone total laryngectomy for advanced laryngeal cancer. Most of the participants were male (89.38%) with a mean age of 65.38 years. The intervention group (TEV) consisted of 869 patients who received voice prosthesis rehabilitation (80.1%) and 216 patients (19.9%) who were treated with EV. The clinical outcomes assessed included the VHI score, VRQoL, and the 36-item short form survey instrument (SF-36). Our patient partners stated that voice prostheses are helpful for communicating with others and are important for their physical, mental, and emotional well-being, which closely relates to these quality-of-life measures.
The second systematic review (Plotas, 2024) included 9 observational studies. The sample size of participants with total laryngectomy ranged from 18 to 133, with all participants being 45 years or older.27 This review evaluated the impact of EV on various quality of life measures, such as VHI score, VRQoL, and the SF-36, comparing it to baseline measures or other voice restoration methods (e.g., TEV). The systematic review presented data at the individual study level but did not perform meta-analyses to pool the results.27 This systematic review found that patients who received voice rehabilitation with either TEV or EV had significant improvements in their quality of life and communication compared to those who did not.27
The details of the outcome measures (e.g., score range and minimal important difference), duration of disease, details on radiotherapy, and the length of follow-up were not reported for both systematic reviews (Maniaci, 2024; Plotas, 2024).23,27
VHI (2 Systematic Reviews)
Two systematic reviews evaluated the effectiveness of TEV compared to EV in improving VHI scores:
In 1 systematic review (Maniaci, 2024; 9 studies), the TEV group demonstrated a statistically significant improvement in VHI score compared to the EV group based on the mean scores.23 Details of the statistical analysis methods were not reported.
In 1 systematic review (Maniaci, 2024; 5 studies), the meta-analysis using random-effect models indicated that the mean differences in VHI scores between the 2 groups was not statistically significant.23 The 95% confidence interval was wide and included the potential that either of the treatments compared could be favoured.
In a second systematic review (Plotas, 2024), the number of studies contributing to the outcome was unclear). The authors indicated that TEV may perform better than EV in VHI scores according to a summary of individual studies.27
VRQoL (2 Systematic Reviews)
Two systematic reviews evaluated the effectiveness of TEV compared to EV in improving VRQoL.
In 1 systematic review (Maniaci, 2024; 7 studies), the TEV group showed a statistically nonsignificant difference compared to the EV group based on the mean scores.23 Details of the statistical analysis methods were not reported.
In 1 systematic review (Maniaci, 2024; 3 studies), the meta-analysis using random-effect models also indicated that the mean differences between the 2 groups was not statistically significant.23
In a second systematic review (Plotas, 2024), the number of studies contributing to the outcome was unclear). The authors indicated that TEV may perform better than EV in VRQoL scores according to a summary of individual studies.27
SF-36 (2 Systematic Reviews)
Two systematic reviews23 evaluated the effectiveness of TEV compared to EV in improving SF-36 scores.
In 1 systematic review (Maniaci 2024, 4 studies), the TEV group demonstrated a statistically significant better improvement in SF-36 compared to the EV group based on the mean scores.23 Details of the statistical analysis methods were not reported.
In 1 systematic review (Maniaci 2024, 4 studies), no meta-analysis was performed for SF-36.23
In the second systematic review (Plotas, 2024; the number of studies contributing to the outcome was unclear), the authors indicated that TEV may perform better than EV in SF-36 scores, according to a summary of individual studies.27
The 2 overlapping systematic reviews (Maniaci, 2024; Plotas, 2024)23,27 present differing conclusions about the comparative effects, highlighting inconsistency in findings. The 2 systematic reviews included some of the same studies, although they used the data from these studies differently and presented different summaries relevant to the research question.
Both systematic reviews had critical flaws, leading to critically low confidence in their results. For both reviews, the objective was clearly described, keywords of the search strategies were provided, and the study selection processes were reported. Searches were conducted in multiple databases. No systematic review provided the list of excluded studies, which prevented assessing whether any relevant studies had been inappropriately excluded. It was unclear how article selection and data extraction were conducted. The possibility of inappropriate inclusion or exclusion or errors in data extraction cannot be ruled out. Authors conducted risk of bias assessments of the included studies, yet the reviews did not explore the potential impact of risk of bias on result interpretations. Plotas (2024)27 reported excluding studies with a high risk of bias in their method section but noted that most of the included studies in this review had weak methodologies and high bias in their results section. Maniaci (2024)23 reported that most of the studies had a low risk of bias and assessed the quality of evidence using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) framework. The details of the GRADE assessment were unclear, and their assessment did not adhere completely to the GRADE principles in that the certainty of evidence was stated to be very low for evidence from observational studies and the certainty of evidence was not assessed for each outcome. The accuracy of the overall certainty of evidence appraisals was uncertain and difficult to interpret in this review.
Research Question 2: The Clinical Effectiveness of Indwelling and Nonindwelling Voice Prostheses for Adults Following Total Laryngectomy, Specifically Comparing Indwelling Devices Versus Other Indwelling Devices, Nonindwelling Versus Other Nonindwelling Devices, and Indwelling Versus Nonindwelling Devices
Two systematic reviews comparing the effectiveness of different voice prostheses on clinical outcomes were identified (Mayo-Yáñez 2023; Tawfik 2021).25,26
One systematic review (Mayo-Yáñez, 2023)25 included 4 observational studies involving 55 patients who underwent laryngectomy (87.27% male, mean age 62.71 years) who used a voice prosthesis. The studies compared the Provox Vega XtraSeal prosthesis (n = 94) to control voice prostheses (Vega and ActiValve Light, n = 221) and focused on voice prosthesis duration.
One systematic review (Tawfik, 2021) with network meta-analysis (NMA)26 included 120 studies with 11,918 patients who underwent laryngectomy (71.7% male, aged 17 to 90 years). The analysis evaluated 10 voice prostheses including 8 indwelling prostheses (Provox-1, Provox-2, Provox ActiValve, Provox Vega, Sound-Producing Voice Prosthesis, Nijdam, Groningen Low Resistance, Groningen Ultra Low Resistance) and 2 nonindwelling prostheses (Provox NiD and Blom-Singer Low Pressure) on multiple clinical outcomes, such as voice prosthesis replacement, voice prosthesis duration, airflow resistance, leakage rates, and patient device preference, with follow-up durations ranging from 0.5 to 133 months (about 11 years). This systematic review (Tawfik, 2021) also evaluated the use of HMEs in the NMA and compared different voice prostheses to HMEs for some outcomes.26 This systematic review did not clarify whether the voice prosthesis arm included patients with or without an HME.26 The results related to the comparisons of HMEs were not included in this report.
Comparisons Among 10 Voice Prostheses (8 Indwelling and 2 Nonindwelling)
One systematic review (201 studies) and NMA (120 studies) 26 compared the effectiveness of 10 voice prostheses (8 indwelling and 2 nonindwelling devices): Provox-1, Provox-2, Provox AV, Provox Vega, Sound-Producing Voice Prosthesis, Nijdam, Groningen Low Resistance, Groningen Ultra Low Resistance, Provox NiD, and Blom-Singer Low Pressure). For most comparisons across most clinical outcomes, the NMA was insufficient to show a difference between the devices being compared.26 Many effect estimates were imprecise. The 95% confidence intervals were wide, including the potential that either treatment being compared could be favoured.
Provox Vega XtraSeal Compared to a Control Voice Prosthesis (Vega and ActiValve Light)
One systematic review (Mayo-Yáñez, 2023; 4 studies)25 compared the lifespan of the Provox Vega XtraSeal and with that of control voice prostheses (Vega and ActiValve Light) and reported that the Provox Vega XtraSeal had a numerically longer mean lifespan than the control voice prostheses. However, the review (Mayo-Yáñez, 2023) did not perform statistical tests to compare the 2 groups, and the 95% confidence intervals overlapped.
Both systematic reviews had critical flaws, leading to critically low confidence in their results. The review objectives were clearly described, keywords of the search strategies were provided, and study selection processes were described. Both systematic reviews conducted their searches in multiple databases. One systematic review reported performing a grey literature search.26 Neither provided the list of excluded studies. These limitations may result in missing some eligible studies. At least 2 reviewers independently performed or verified the article selection and data extraction in 1 systematic review.24,26 Two reviewers independently conducted data extraction in 1 systematic review (Mayo-Yáñez, 2023), but it was unclear how the article selection was performed.25 The possibility of inappropriate inclusion or exclusion or errors in data extraction cannot be ruled out.
One systematic review (Mayo-Yáñez, 2023) assessed the risk of bias in the included individual studies and reported study quality, yet it did not provide an overall summary of the risk of bias. Neither review explored the potential impact of the risk of bias on the interpretation of the results. Tawfik (2021)26 stated that all 32 included RCTs had either low (n = 9) or unclear (n = 23) risk of bias. However, this review (Tawfik, 2021) also included approximately 169 observational studies, of which 32 were ranked as good, 107 as fair, and 30 as poor.26 The findings of some of these systematic reviews may be driven by studies with a high risk of bias.
Tawfik (2021)26 conducted a frequentist NMA comparing 10 voice prostheses: Provox-1, Provox-2, Provox AV, Provox Vega, Sound-Producing Voice Prosthesis, Nijdam, Groningen Low Resistance, Groningen Ultra Low Resistance, Provox NiD, and Blom-Singer Low Pressure. The NMA presented a range of results, including network plots, point estimates, 95% confidence intervals, and P scores. Intervention rankings were based solely on P scores without considering the results of statistical tests or the certainty of the evidence. This approach means that voice prostheses with top rankings may have low-certainty evidence or may not show statistically significant differences compared to other voice prostheses. The systematic review (Tawfik, 2021) noted some variability, or heterogeneity, among the included studies. However, it did not adequately assess potential treatment effect modifiers or how these factors could influence the assumption of exchangeability. This may introduce bias into the results of the NMA due to the insufficient evaluation of the validity of the exchangeability assumption. Additionally, the inclusion of nonrandomized studies in the NMA could have introduced bias due to the inherent limitations of observational studies, such as selection bias and confounding factors. We also compared the registered systematic review protocol in PROSPERO (CRD42017080110) with the published reviews and identified several discrepancies. For instance, the protocol specified the inclusion of only RCTs, but the published review also included observational studies. Additionally, while the protocol focused solely on voice prostheses, the review incorporated the HME devices in the NMA for certain outcomes, such as patient preference. The authors did not address these deviations between the review protocol and their actual work. In addition, a commentary on this review raised concerns about the accuracy and completeness of the findings, citing errors in data extraction, the exclusion of relevant studies, and the absence of crucial clinical outcomes, such as quality of life.33
Research Question 3: The Clinical Effectiveness of Heat and Moisture Exchangers for Adults Following Total Laryngectomy
One systematic review (Ahmed, 2023; 10 studies)24 evaluated the effectiveness of HMEs compared to no HME use or an external humidifier on various outcomes.
This review (Ahmed, 2023) identified 1 mixed methods study24 that included a rapid review, which met our criteria for systematic reviews. For the purpose of this Rapid Review, we refer to the rapid review as a systematic review in our report. The review (Ahmed, 2023) compared the effectiveness of HMEs with no HME use or an external humidifier. The review (Ahmed, 2023) included 10 studies comprising 3 RCTs, 3 time-series studies, 2 retrospective studies, 1 case-control study, and 1 study with an unclear design. The review (Ahmed, 2023) included 550 patients who underwent total laryngectomy. Age and sex data were not reported. The intervention involved the use of HMEs, compared to baseline, no HME use, an external humidifier, or another HME. This report only summarized the comparisons between HMEs compared to no HME use or external humidifier use. The review (Ahmed, 2023) summarized several clinical outcomes, including mucus production, coughing, forced expectorations, the number of days requiring chest physiotherapy after surgery, tracheobronchitis or pneumonia episodes, patient satisfaction, quality of life, sleep quality, speech quality, and social contacts. The follow-up duration for these outcomes was either 3 months or not reported.
HMEs were reported to statistically reduce various outcomes:24 mucus production, coughing, forced expectorations, the number of days requiring chest physiotherapy after surgery, tracheobronchitis, and pneumonia episodes. HMEs were reported to statistically significantly improve patient satisfaction.24 The difference between HME and control (no HME or external humidifier) is not statistically significant in the following outcomes:24 quality of life, sleep quality, speech quality, and social contacts.
This review had multiple critical flaws, leading to critically low confidence in results. The objective was clearly described, keywords of the search strategies were provided, and study selection processes were described. PubMed was searched, and no grey literature search was reported. The review did not provide a list of excluded studies and, therefore, some eligible studies may be missing. Two reviewers independently performed or verified the article selection and data extraction. This review did not assess the risk of bias in the included studies.24
Summary of Patient Experience Using Voice Prostheses and HMEs
The following section provides an overview of the patient experience collected from 3 patient partners. This section reports examples of individual experiences of using voice prostheses and HMEs. Head-to-head comparisons of voice prostheses and HMEs are outside of the scope of this Rapid Review. Given the small sample of interviewed patients, these reported examples are not indicative of device superiority.
All 3 patient partners engaged in this project used different models of voice prosthesis and HMEs and described trying and using different device models to find those that best aligned with their needs and preferences. Patients emphasized the importance of selecting device models that could best accommodate their physical comfort and needs (e.g., limited leakage), their budget, the geographical location of their residence, and their unique circumstances, such as physical changes due to radiation therapy, wildfire smoke, special occasions, and susceptibility to airborne pathogen exposure. For example, 1 patient used the indwelling Atos brand Provox VP, after trying the Blom-Singer prosthesis, because it best suited them and did not cause inner barrel leakage. Another patient found that the Provox Tru-Tone Emote electrolarynx enabled them to speak after radiation therapy and was cheaper than the Provox Vega 17Fr VP they previously used. Another patient used a nonindwelling voice prosthesis (Provox NiD), which they changed themselves to avoid travelling more than 3.5 hours to reach the hospital. This patient described travelling long distances to change the device as impractical, noting that other updated models need to be changed by the speech and language pathologist. Patients also used different HME models. They reported using “Atos Extra flow” and “Provox ExtraMoist,” switching to other HME models in unique circumstances, such as the hands-free HME from InHealth Technologies on “special occasions,” and the Provox Micron HME when the wildfire smoke was bad or in situations with a high risk of airborne pathogen exposure. One patient reported that a speech and language pathologist demonstrated EV, but the patient did not describe detailed personal experiences with it. The patient mentioned TEV was easier to learn than EV, and they never encountered 1 who used EV exclusively.
Patients reported 3 benefits from using their voice prostheses and HMEs, including improved communication, independence, and infection control. Patients described being able to live life and communicate with family and friends as the most important benefit. The patients talked about the isolation and frustration they experienced when they were unable to communicate and when using “type to speak” apps, which caused breaks in conversation and missed opportunities to communicate. Having a voice prosthesis and HME allowed patients to be independent — allowing them to communicate in person and on the phone. They mentioned that being independent is important for their physical, mental, and emotional well-being. Whereas the voice prosthesis allows patients to communicate, which some patients commented was a basic human right, they also felt that the HMEs were vital in preventing infection.
Patients described 3 challenges with using their voice prostheses and HMEs, including device limitations, environmental impact on use (i.e., weather and wildfires), and maintenance. Device limitations included several considerations, such as not being able to change the volume of their voices with a voice prosthesis, which makes it difficult to communicate in loud or quiet places, and not being able to change the pitch of the voice, with 1 patient emphasizing that their voice no longer sounded like themselves. However, they noted that being able to communicate far outweighed these limitations. Patients noted that their ability to communicate and engage with others in public was limited; they reflected that the need to obscure their stoma to talk meant they needed to avoid touching others (i.e., shaking hands) or touching surfaces to help prevent any potential infection. One patient mentioned being allergic to the adhesive on the hands-free HME and wearing a HME that they had to occlude themselves. Another patient mentioned that the softer silicone design of the 1 voice prosthesis device (Blom-Singer prosthesis) caused their fistula to distort out of shape, causing inner barrel leakage. Additionally, talking while eating or drinking was not possible (or recommended) — and some patients commented that they often drink privately, away from family and friends, to avoid leakage through their stoma.
Patients reported that the weather had a significant impact on being able to effectively use a voice prosthesis and HME. Patients reported that cold air feels painful, causes irritation, and causes the HME to be saturated, which can feel like it is dripping into their lungs. One patient mentioned that the negative impact of cold weather was a large driving factor for moving to a different province with warmer annual temperatures. The hot air can be an irritant as well, and the moist air can cause coughing, resulting in pain. Wildfires create additional challenges, with the HMEs getting frequently blocked and the need to use more or different devices to prevent infection.
Device maintenance was another challenge. Changing the voice prosthesis can be a problem, especially when living far from the hospital. One patient living 3.5 hours from the nearest hospital chose a nonindwelling voice prosthesis that they could change themselves. However, their experience with this device caused problems with leakage when drinking. Keeping the devices clean can also be a challenge. Patients mentioned needing to clean the voice prosthesis from once every other day to as much as 4 times per day due to food buildup. Patients also mentioned needing to replace their device as frequently as every 5 weeks for 1 patient and on average 3 times per year for another. This issue changed their eating habits and limited their eating. Patients noted that having a voice prosthesis that needs to be replaced by the specialist meant that replacing the voice prosthesis in case of a problem felt like a sense of emergency — 1 patient reported that, in their case, “you need to order yourself and then travel to the appointment and hope the new device fits.” Patients mentioned that when they went out, they needed to take a bag of supplies with them to help them maintain their device or manage any challenges (e.g., additional HMEs, adhesive tape, tissues). They also noted that sneezing and coughing can cause a large amount of mucus to get stuck in the HME, resulting in it needing to be thrown away. Patients commented on how challenging it is to try to remove the device before coughing and sneezing.
Research Question 4: The Cost-Effectiveness of Voice Prostheses Versus No Voice Prostheses for Adults Following Total Laryngectomy
No eligible studies were identified.
Research Question 5: The Cost-Effectiveness of Indwelling and Nonindwelling Voice Prostheses for Adults Following Total Laryngectomy, Specifically Comparing Indwelling Versus Other Indwelling Devices, Nonindwelling Versus Other Nonindwelling Devices, and Indwelling Versus Nonindwelling Devices
No evidence was found comparing the cost-effectiveness of indwelling versus nonindwelling voice prostheses, or between different nonindwelling voice prostheses for adults following laryngectomy.
Two cost-effectiveness studies28,29 that compared a regular indwelling voice prosthesis (Provox Vega) and its modified versions designed to prevent leakage (Provox XtraSeal and Provox ActiValve) were identified.
One study (Rodriguez-Lorenzana, 2023)28 compared the cost-effectiveness of Provox Vega against the Provox XtraSeal. The study used data on 551 voice prostheses (483 Provox Vega, 68 Provox XtraSeal) from 38 patients (35 men, 3 women), with a mean age of 66 years, from 2015 to 2023.28 The incremental cost-effectiveness ratio (ICER) was calculated from the Spanish National Health System's perspective, based on the difference in costs and the number of annual prosthesis replacements.28
One study (Mayo-Yáñez 2022)29 compared the Provox Vega to the Provox ActiValve, which features a magnet-based valve to prevent leakage. The study included 159 voice prostheses (150 Provox Vega, 9 Provox ActiValve) used in 5 men with a mean age of 64 years.29 The ICER was calculated based on the number of annual prosthesis replacements during the observational study from the perspective of the Spanish Public National Health System.29
Reported results comparing a regular indwelling voice prosthesis (Provox Vega) and its modified versions in patients who had undergone a laryngectomy and who are experiencing leakage with Provox Vega, based on Spanish National Health System perspective, are as follows:28,29
Switching to Provox XtraSeal is cost-effective if the cost of Provox XtraSeal remains less than €551.63.28
ICER (€/effectiveness): −0.01
Lower-cost scenario: −€291.80
Higher-cost scenario: €93.07
Switching to Provox ActiValve is also cost-effective:29
ICER (€/effectiveness): −133.97.
Both studies clearly defined their research questions, study design, data collection parameters, outcome measures, analysis perspectives, and rationale for selecting the study alternatives. The rationale for the chosen form of economic analysis could have been further elaborated. Each study’s effectiveness measures were derived from a single prospective study with small patient samples (5 and 38 users of voice prostheses, 40 users of HMEs, 22 users of ASCs). Both studies28,29 focused on the cost-effectiveness of different indwelling voice prostheses based on crossover studies. These studies involved users of Provox Vega who experienced 3 or more consecutive changes due to leakage, which affected the prosthesis’s theoretical lifespan. The patients then switched from the Provox Vega to its alternatives (Provox XtraSeal or Provox ActiValve). This transition introduced variability in the background care, or surgical interventions received, making comparisons between the devices less consistent. Both studies28,29 also lacked details on currency adjustments for inflation or conversion and did not include sensitivity analyses. These studies28,29 were conducted from the payer’s perspective within the Spanish National Health System, and their findings may not be applicable to the health care system in Canada.
Research Question 6: The Cost-Effectiveness of Heat and Moisture Exchangers for Adults Following Total Laryngectomy
This review included 1 study30 that compared the cost-effectiveness of HMEs versus ASCs in patients after they underwent laryngectomy at a clinic in Massachusetts, US. The study (Beck, 2020), conducted from September 2018 to December 2018, included 40 users of HMEs and 22 users of ASCs, mostly male (71%).30 Quality of life (QoL) data were collected via a study-specific questionnaire, and the utility index scores were derived using the EQ-5D and the US tariff.30 A Markov model calculated the ICER by dividing the total cost difference by the difference in quality-adjusted life-years (QALYs) from a US health care and societal perspective.30
This review included 1 study30 that compared the cost-effectiveness of HMEs versus ASCs in patients after laryngectomy from the US health care and societal perspective. The study found that HME use is cost-effective compared to ASCs:30
QALYs were slightly higher for users of HMEs compared to users of ASCs
Total lifetime costs per patient were higher for users of ASCs compared to users of HMEs
ICER (US$/QALY): health care perspective: −11,833; societal perspective: −306,551
Annual budget saving (US$): health care perspective: 1,551,083; societal perspective: 40,183,593.
The research questions, study design, data collection parameters, outcome measures, analysis perspectives, and rationale for selecting the study alternatives were clearly defined in the study. This study provided a comprehensive economic evaluation, justifying its choice of economic model, clearly defining effectiveness estimates and outcome measures, and including appropriate sensitivity analyses. This study was conducted from both US health care and societal perspectives, and findings may not be generalizable to the context in Canada due to differences in health care systems.
Summary of Patient Experiences Related to Device Costs
Costs associated with device use were reported as a significant challenge for all 3 patients interviewed. Patients reported being impacted by the cost of the voice prosthesis and HME devices, and also by the cost of maintenance items, such as medical tape, tissues, infection prevention cream, and cleaning materials. Patients mentioned that there was varying coverage for the costs of the voice prosthesis, HMEs, and associated supplies across the country. For example, in British Columbia, where all the patients lived, there is currently no funding for supplies, and this was seen as the biggest frustration for patients. One patient who previously lived in Ontario noted that, in that province, there was some financial funding to support the purchase of supplies for patients who have had a laryngectomy. Some patients mentioned that those who have a lower income would struggle to afford the voice prosthesis, HMEs, and additional supplies needed to appropriately manage and maintain the device.
High costs are associated with the voice prosthesis and the HMEs, which need to be changed often. Patients commented that voice prostheses need to be changed 3 to 4 times per year, and HMEs need to be replaced daily or more if the patient is coughing or sneezing or if the air quality is bad.
All 3 patients used an HME; however, due to the cost of these, they tried to minimize its use in the home. Sneezing and coughing can cause a large amount of mucus to get stuck in the HME, and it then needs to be thrown away. Patients commented on having to try to remove the HME before coughing and sneezing, with 1 patient referring to this as a “$5 sneeze.” One patient very generously provided a breakdown of the personal expenses for yearly maintenance of his laryngectomy, which totalled $7,844 per year: 3 voice prostheses = $1,540; HME = $1,656; adhesive patches = $2,640; foam patches = $168; liquid calcium = $832; Atos cleaning brushes = $480, hydrogen peroxide = $96, Polysporin cream = $192; tissues = $240.
Research Question 7: The Evidence-Based Guidelines Regarding the Use of Voice Prostheses or Heat and Moisture Exchangers for Adults Following Total Laryngectomy
One evidence-based guideline that provided recommendations regarding the use of voice prostheses for adults following laryngectomy in managing periprosthetic leakage was identified.31 No evidence-based guidelines regarding the use of HME for adults following laryngectomy were identified; therefore, no summary can be provided.
The guideline was developed in Spain focused toward health care professionals, including otorhinolaryngology specialists, speech therapists, nursing staff, and other specialists, with a focus on patients who had undergone a laryngectomy.31 The evidence was collected and synthesized through a systematic review of 91 studies on primary or secondary TEP (which does not address the same research questions as the current report), assessed using the Oxford Levels of Evidence system (2011), ranging from level 1a (systematic reviews of RCTs) to level 5 (mechanism-based reasoning). The guideline development group reviewed recent research on benefits, side effects, and risks to make recommendations with a grade of recommendation (B or C); however, the meaning of these recommendation grades was not specified.31
The guideline recommended replacing the prosthesis with a double-flanged one, such as the Provox Vega XtraSeal, or adjusting the diameter and length, or placing a silicone sheet (or ring) on the tracheal side of the prosthesis. It also mentioned that the Blom-Singer large esophageal and tracheal flange voice prosthesis is a useful solution for managing periprosthetic leakage. However, the guideline did not provide clear recommendations regarding the initial use of voice prostheses.
The included evidence-based guideline had clear objectives, guideline questions, and target populations (e.g., patients undergoing total laryngectomy).31 The guideline development group searched multiple databases (MEDLINE, Embase, Scopus, Web of Science, PubMed, Science Citation Index, and the Cochrane Library) for relevant evidence and then achieved consensus to formulate recommendations.31 The guideline panel included otolaryngologists, head and neck surgeons, and expert speech therapists.31 However, it is uncertain whether at least 1 methodology expert was involved in the development of the guideline and whether the perspectives or preferences of the target populations were sought or had an influence on the recommendations. Therefore, the recommendations may not adequately reflect the values and preferences of patients or other invested parties.
The guideline31 proposed using either B or C for the grade of recommendations; the meaning of recommendation grades was not specified, limiting the interpretation of the recommendations. The links between the recommendations and the supporting evidence were unclear. The guideline was funded by Atos Medical, and all guideline authors disclosed no competing interests. The included guideline discussed the potential facilitators to implementing some recommendations and considered some cost-effective evidence.31 The guideline did not discuss the related barriers regarding the use of a voice prosthesis, such as accessibility and affordability for the voice prosthesis, which could be a barrier to implementing related recommendations.
Limitations
Our Rapid Review has several limitations. The patient engagement component included 3 patient partners, all of whom were residents of British Columbia, with 1 having relocated from Ontario. Feedback obtained during these engagement activities revealed potential jurisdictional variations in coverage policies for voice prostheses, HMEs, and related supplies. The findings from engagement with patients may not be fully representative of the broader spectrum of patient perspectives across Canada. Furthermore, the patient engagement activities did not yield information regarding patient experiences with EV; therefore, a comparison between the experiences of users of vocal prostheses and those using EV remains unexplored.
Patient and clinician engagement occurred after the first version of this Rapid Review was complete and did not influence the formulation of research questions or outcomes of interest, which may limit the relevance and applicability of the findings. Research questions addressed only a subset of this broader clinical topic regarding care for adults following total laryngectomy, potentially overlooking important factors such as patient values, preferences, and accessibility. Our Rapid Review did not directly compare different types of head and neck management techniques or investigate other critical comparisons (e.g., TEV versus electrolarynx), which affects its comprehensiveness and utility for decision-making. Our search is limited to the past 5 years despite the search dates for the included literature dating back to the 1980s, it is possible that some relevant literature has not been identified.
Our report relies on systematic reviews; however, our confidence in their results was very low, making them unreliable for providing an accurate and comprehensive summary of the available evidence. Two systematic reviews (Maniaci, 2024; Plotas, 2024) included overlapping individual primary studies, which may lead to potential aggregate biases. Although this report included 5 systematic reviews23-27 addressing the clinical effectiveness of voice prostheses compared to no voice prostheses or another alternative voice prosthesis and considering many primary studies, due to various methodological flaws, again, our confidence in the results of these reviews is very low. These systematic reviews also did not directly address the same research questions as the current report. As such, these reviews should not be relied on to provide an accurate and comprehensive summary of the available studies answering the research questions.
The body of evidence identified has substandard reporting. None of the included systematic reviews focus on adverse outcomes associated with different voice restoration methods. The details of the QoL outcome measures (e.g., score range and minimal important difference) and the length of follow-up were not reported.23,27 This review identified evidence gaps — no high-quality systematic reviews that directly address our research questions were available. We based our conclusions on statistical significance, and it is important to note that statistically significant results may lack practical clinical importance, and nonsignificant results do not necessarily indicate no difference. In some systematic reviews, the effect estimates were challenging to interpret due to nonreporting of outcome definitions, the range and direction of scores on measurement scales, and units of measurement.
We did not limit voice prosthesis or HME devices by product. As such, some of the devices detailed in identified systematic reviews may not be available in Canada. The included economic evaluation studies were conducted from the perspectives of the US health system and Spanish National Health System.28-30 No evidence-based guidelines or economic evaluations were identified that focused on the context in Canada. The included guidelines were conducted in Spain,31 and no guideline authors were from Canadian institutions; therefore, the generalizability of the findings to settings in Canada is unclear.
Conclusions and Implications for Decision- or Policy-Making
This Rapid Review summarizes evidence on the effectiveness and cost-effectiveness of voice prostheses and HMEs compared to no voice prosthesis and/or HME for adults following total laryngectomy. According to feedback from clinicians, use of voice prostheses and HMEs following total laryngectomy is reported to have been in common clinical practice in Canada for many years. The impact of total laryngectomy on patients’ QoL is significant. Both the literature and our interviews with 3 patients revealed that voice prostheses and HMEs significantly benefit postlaryngectomy QoL, primarily by restoring communication and social engagement. HMEs are reported to be necessary for infection prevention. Although these devices are reported to enhance independence, social engagement, and overall QoL, there are reported challenges with their use, including device limitations (e.g., fixed volume and pitch, interference with voicing during mealtimes that impedes the ability to speak and drink simultaneously), environmental sensitivities to extreme temperatures or forest fire smoke, and the need for frequent maintenance (voice prosthesis replacements 2 to 3 times per year, daily HME changes). Patients reported that out-of-pocket costs related to the use of voice prostheses, HMEs, and related supplies are a major barrier, causing significant financial strain and frustration.
Potential inequities were observed. For example, patients who live in rural or remote locations may have a limited choice of devices because some voice prostheses can only be fitted by a speech and language pathologist. If a patient lives far from hospital facilities, it becomes challenging when there is a fault with the device or if it needs to be routinely changed. One of the patients interviewed chose a nonindwelling voice prosthesis device to be able to change themselves and not travel to the hospital. Similarly, a patient’s ability to change the HME and voice prosthesis as needed requires adequate cognitive capacity, physical mobility, and function to maintain their devices appropriately to ensure effective operation. Patients with comorbidities may need additional routine access to care.
Five systematic reviews,24-27 3 cost-effectiveness studies,28-30 and 1 evidence-based guideline31 were identified to answer our research questions. No evidence of the cost-effectiveness of voice prostheses versus no prostheses, indwelling versus nonindwelling prostheses, or comparisons among different nonindwelling prostheses for adults following laryngectomy was identified. This is a relatively small patient population and, as such, achieving the highest standards of methodology (i.e., large randomized controlled trials) in primary research is infeasible. Population size and primary evidence quality subsequently impacts the quality of a rapid review. Owing to various methodological limitations, confidence in the evidence identified was assessed as very low.
Two systematic reviews, for which we had critically low confidence results, suggest that TEV may positively impact QoL measures compared to EV.23,27 However, the available meta-analyses found no statistically significant differences between TEV and EV in VHI and VRQoL scores,23 with a wide 95% confidence interval, including the possibility of either intervention being favoured. One systematic review indicated that patients undergoing voice rehabilitation with either EV or TEV experienced significant improvements in their QoL and communication compared to those who did not receive voice restoration.27 The review highlights the challenges associated with EV, including the need for extensive training and the potential of the device to increase fear and anxiety and reduce self-confidence and self-esteem, which may impact the ability of the user to communicate effectively and the overall functionality of the device.27 The limited evidence emphasizes the importance of shared decision-making when selecting between TEV and EV. This process should incorporate patient values, preferences, lifestyle, and cost considerations. People should also consider a range of factors that can impact patient well-being, such as learning difficulties and anxieties about technologies.
The effectiveness of 1 model of voice prosthesis compared with others requires further investigation due to the critically low confidence in results from 1 included systematic review (Tawfik, 2021).26 This suggests that decision-makers should consider patient-centred factors such as individual values, preferences, lifestyle, cost, and ease of maintenance. Other factors influencing the decision to use a voice prosthesis or select a specific type include postoperative health and anatomic status, physical and mental capabilities, level of independent functioning, caregiver support, and patient motivation.13 The clinical expert we engaged noted that choices between indwelling and nonindwelling voice prostheses are often determined by patient and environmental factors. Due to the typically lower cost of nonindwelling voice prosthesis, these options are frequently considered more suitable for cognitively intact patients living in remote settings or within provinces where voice prostheses are not covered under health plans. The patient engagement findings support the feedback from the clinical expert.
For patients who underwent a total laryngectomy and experience leakage with Provox Vega, it may be reasonable to switch to a modified version to prevent further leakage, such as Provox XtraSeal for periprosthetic leakage or Provox ActiValve or Provox ActiValve for endoprosthesis leakage.28,29,31 It is important to note that eligible studies included in the review only examined and mentioned the Provox brand for managing voice prosthesis leakage, the switch from a single-valved to a dual-valved voice prosthesis is driven by the need to address device malfunction in individual patients rather than a specific brand.34 Patients could switch among different devices to find the most effective option. Alternatively, clinicians or patients can manage leakage by adjusting the diameter and length of the prosthesis or placing a silicone sheet (or ring) on the tracheal side of the prosthesis.31
One systematic review (Ahmed, 2023) for which we had critically low confidence in its results24 suggests the potential benefits of HMEs. This review concludes that HMEs significantly improve several clinical outcomes, including mucus production, coughing, forced expectorations, the number of days requiring chest physiotherapy after surgery, tracheobronchitis or pneumonia episodes, and patient satisfaction. No difference between HME use and the control was observed for QoL, sleep quality, speech quality, and social contacts. HMEs were reported to be cost-effective compared to ASCs from the US perspective.30
Future systematic reviews should be planned and conducted in alignment with recognized methodological standards and be transparently reported.35,36 As the certainty of evidence even from high-quality systematic reviews relies in part on the risk of bias in their included studies, future primary studies should also be robustly planned and conducted and transparently reported. For example, due to the size of this population, primary studies using data from patient registries of individuals who have undergone laryngectomy may help answer these research questions. Future cost-effectiveness analyses should include sensitivity analyses to test the robustness of their findings. Future evidence-based guidelines should conduct comprehensive literature reviews, have diversity in panel composition, and formulate recommendations through established consensus processes that involve patient partners or panel members from Canada to enhance the generalizability of recommendations to the context in Canada. Development of a living clinical practice guideline housing evidence and consensus-based recommendations on the use of voice prostheses and HMEs focused on the context in Canada would be optimal.
In conclusion, postlaryngectomy interventions include olfactory, voice, pulmonary, and swallowing rehabilitation and addressing the psychosocial aspects of patient recovery. Voice rehabilitation is an important aspect of postlaryngectomy care to restore vocal communication, and options include the use of EV, an artificial larynx (electrolarynx), or TEV with voice prosthesis. The use of voice prostheses and HMEs is highly valued by the clinical and patient community we engaged for this review. The evidence base related to their benefit and cost-effectiveness is limited. The perspectives of speech and language pathologists working with patients, and patients with lived experience of these devices, may supplement decision-making by contextualizing the evidence currently available. When choosing a voice prosthesis, decision-makers should consider the patient’s TEP shape and size, the patient’s values and preferences, accessibility, affordability, and other factors such as physical and mental capabilities, caregiver support, and patient motivation. Limited evidence aligns with reporting from patients and clinicians that adding HMEs could be beneficial in terms of several clinical outcomes, such as mucus reduction, reduced tracheobronchitis or pneumonia episodes, and reported patient satisfaction. Additionally, our patient partners highlighted the importance of HMEs in preventing infection. Geographical considerations, patient comorbidities, and financial barriers for this population of patients should also be carefully considered. Policy-makers should take into consideration the limited quantity and quality of the current evidence available for this small population of patients.
Acknowledgements
Patient Contributors
We sincerely thank Hilda Lily Hopp, Janice Haggart, and Peter Cassey for the time and energy they spent sharing their lived experiences of using voice prostheses and HMEs following their laryngectomy. Their contributions have been invaluable to this report.
Clinical Reviewer
We thank our content expert reviewer, Jennifer Cameron-Turley, MSc, S-LP(C), Reg SK, for her consultation on this report.
References
1.Crosetti E, Fantini M, Bertotto I, et al. Current Status of partial laryngeal surgery for advanced laryngeal cancer: when and why? Curr Oncol Rep. 2024;26(6):614-624. doi:10.1007/s11912-024-01516-7 PubMed
2.Hans S, Baudouin R, Circiu MP, et al. One hundred fifty years of total laryngectomies. Front Oncol. 2024;14:1351549. doi:10.3389/fonc.2024.1351549 PubMed
3.Hoffmann TK. Total Laryngectomy-Still Cutting-Edge? Cancers (Basel). 2021;13(6):19. doi:10.3390/cancers13061405 PubMed
4.Xie L, Semenciw R, Mery L. Cancer incidence in Canada: trends and projections (1983-2032). Health Promot Chronic Dis Prev Can. 2015;35(Suppl 1):2-186. doi:10.24095/hpcdp.35.S1.02 PubMed
5.Babin E, Blanchard D, Hitier M. Management of total laryngectomy patients over time: from the consultation announcing the diagnosis to long term follow-up. Eur Arch Otorhinolaryngol. 2011;268(10):1407-19. doi:10.1007/s00405-011-1661-4 PubMed
6.Brisson-McKenna M, Jefferson GD, Siddiqui SH, et al. Swallowing function after treatment of laryngeal cancer. Otolaryngol Clin North Am. 2023;56(2):371-388. doi:10.1016/j.otc.2022.11.004 PubMed
7.Rosa VM, Fores JML, da Silva EPF, et al. Interdisciplinary interventions in the perioperative rehabilitation of total laryngectomy: an integrative review. Clinics (Sao Paulo). 2018;73(suppl 1):e484s. doi:10.6061/clinics/2018/e484s PubMed
8.Sharpe G, Camoes Costa V, Doube W, Sita J, McCarthy C, Carding P. Communication changes with laryngectomy and impact on quality of life: a review. Qual Life Res. 2019;28(4):863-877. doi:10.1007/s11136-018-2033-y PubMed
9.Öztürk A, Mollaoğlu M. Determination of problems in patients with post-laryngectomy. Scand J Psychol. 2013;54(2):107-111. doi:10.1111/sjop.12025 PubMed
10.Kearney A, Norris K, Bertelsen C, et al. Adoption and Utilization of Heat and Moisture Exchangers (HMEs) in the Tracheostomy Patient. Otolaryngol Head Neck Surg. 2023;169(5):1374-1381. doi:10.1002/ohn.368 PubMed
11.Mérol JC, Charpiot A, Langagne T, Hémar P, Ackerstaff AH, Hilgers FJ. Randomized controlled trial on postoperative pulmonary humidification after total laryngectomy: external humidifier versus heat and moisture exchanger. Laryngoscope. 2012;122(2):275-81. doi:10.1002/lary.21841 PubMed
12.Parrilla C, Minni A, Bogaardt H, et al. Pulmonary Rehabilitation After Total Laryngectomy: A Multicenter Time-Series Clinical Trial Evaluating the Provox XtraHME in HME-Naïve Patients. Ann Otol Rhinol Laryngol. 2015;124(9):706-13. doi:10.1177/0003489415579219 PubMed
13.Lewin JS, Hoffman HT, Sperry SM. Post TW, ed. Alaryngeal speech rehabilitation. UpToDate; 2024. Accessed July 17, 2024. http://www.uptodate.com/
14.Attieh AY, Searl J, Shahaltough NH, Wreikat MM, Lundy DS. Voice restoration following total laryngectomy by tracheoesophageal prosthesis: effect on patients' quality of life and voice handicap in Jordan. Health Qual Life Outcomes. 2008;6:26. doi:10.1186/1477-7525-6-26 PubMed
15.Costa JM, López M, García J, León X, Quer M. Impact of total laryngectomy on return to work. Acta Otorrinolaringol Esp (Engl Ed). 2018;69(2):74-79. doi:10.1016/j.otorri.2017.02.006 PubMed
16.Doyle PC, Finchem EA. Teaching Esophageal Speech: A Process of Collaborative Instruction. In: Doyle PC, ed. Clinical Care and Rehabilitation in Head and Neck Cancer. Springer International Publishing; 2019:145-161.
17.Xi S. Effectiveness of voice rehabilitation on vocalisation in postlaryngectomy patients: a systematic review. Int J Evid Based Healthc. 2010;8(4):256-8. doi:10.1111/j.1744-1609.2010.00177.x PubMed
18.Uzelac J, Dragičević D, Glamočak S. Factors that may affect the success of the esophageal voice and speech education in laryngectomized patients. Timočki medicinski glasnik. 2022;47(1):23-31. Accessed December 03, 2024. https://tmg.org.rs/v470103e.htm
19.van Sluis KE, van der Molen L, van Son R, Hilgers FJM, Bhairosing PA, van den Brekel MWM. Objective and subjective voice outcomes after total laryngectomy: a systematic review. Eur Arch Otorhinolaryngol. 2018;275(1):11-26. doi:10.1007/s00405-017-4790-6 PubMed
20.Wells C, Adcock L. Indwelling voice prostheses for adults following laryngectomy: a review of clinical effectiveness, cost-effectiveness, and guidelines (CADTH Rapid response report: summary with critical appraisal). CADTH; 2017. Accessed August 20, 2024. https://pubmed.ncbi.nlm.nih.gov/30260608/
21.Lewin JS, Baumgart LM, Barrow MP, Hutcheson KA. Device Life of the Tracheoesophageal Voice Prosthesis Revisited. JAMA Otolaryngol Head Neck Surg. 2017;143(1):65-71. doi:10.1001/jamaoto.2016.2771 PubMed
22.Hilgers FJ, Aaronson NK, Ackerstaff AH, Schouwenburg PF, van Zandwikj N. The influence of a heat and moisture exchanger (HME) on the respiratory symptoms after total laryngectomy. Clin Otolaryngol Allied Sci. 1991;16(2):152-6. doi:10.1111/j.1365-2273.1991.tb01966.x PubMed
23.Maniaci A, Lechien JR, Caruso S, et al. Voice-Related Quality of Life After Total Laryngectomy: Systematic Review and Meta-Analysis. J Voice. 2024;38(2):539 e11-539 e19. doi:10.1016/j.jvoice.2021.09.040
24.Ahmed A, Mewes JC, Boot IWA, Vrijhoef HJM. New Heat and Moisture Exchangers for Laryngectomized Patients in Germany: Mixed Methods Study on the Expected Effectiveness. JMIR Form Res. 2023;7:e36401. doi:10.2196/36401 PubMed
25.Mayo-Yáñez M, Cabo-Varela I, Calvo-Henriquez C, Chiesa-Estomba C, Herranz Gonzalez-Botas J. Prevention of periprosthetic leakage with double flange voice prosthesis: a systematic review and management protocol proposal. Logoped Phoniatr Vocol. 2023;48(3):129-136. doi:10.1080/14015439.2022.2042595 PubMed
26.Tawfik GM, Makram OM, Zayan AH, et al. Voice Rehabilitation by Voice Prostheses After Total Laryngectomy: A Systematic Review and Network Meta-Analysis for 11,918 Patients. J Speech Lang Hear Res. 2021;64(7):2668-2681. doi:10.1044/2021_JSLHR-20-00597 PubMed
27.Plotas P, Mastronikolis SN, Papadopoulos A, et al. Quality of Life of Patients Using Esophageal Speech after Total Laryngectomy: A Systematic Review Study. J Pers Med. 2024;14(8):817. doi:10.3390/jpm14080817 PubMed
28.Rodríguez-Lorenzana P, Mayo-Yanez M, Chiesa-Estomba CM, et al. Cost-Effectiveness Study of Double-Flange Voice Prostheses in the Treatment of Periprosthetic Leakage in Laryngectomized Patients. J Pers Med. 2023;13(7):29. doi:10.3390/jpm13071064 PubMed
29.Mayo-Yáñez M, Chiesa-Estomba C, Lechien JR, Calvo-Henriquez C, Vaira LA, Cabo-Varela I. Long-term outcomes and cost-effectiveness of a magnet-based valve voice prosthesis for endoprosthesis leakage treatment. Eur Arch Otorhinolaryngol. 2022;279(8):4167-4172. doi:10.1007/s00405-022-07313-x PubMed
30.Beck ACC, Retel VP, Bunting G, et al. Cost-effectiveness analysis of using the heat and moisture exchangers compared with alternative stoma covers in laryngectomy rehabilitation: US perspective. Head Neck. 2020;42(12):3720-3734. doi:10.1002/hed.26442 PubMed
31.Mayo-Yáñez M, Klein-Rodriguez A, Lopez-Eiroa A, Cabo-Varela I, Rivera-Rivera R, Parente-Arias P. Evidence-Based Recommendations in Primary Tracheoesophageal Puncture for Voice Prosthesis Rehabilitation. Healthcare (Basel). 2024;12(6):14. doi:10.3390/healthcare12060652 PubMed
32.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. doi:10.1016/j.jclinepi.2009.06.006 PubMed
33.Mayo-Yáñez M, Chiesa-Estomba CM, Lechien JR, Maniaci A, van den Brekel M. Commentary on “Voice Rehabilitation by Voice Prostheses After Total Laryngectomy: A Systematic Review and Network Meta-Analysis for 11,918 Patients”. J Speech Lang Hear Res. 2022;65(9):3452-3455. doi:10.1044/2022_JSLHR-22-00137 PubMed
34.Brownlee B, Ahmad S, Grammer T, Krempl G. Selective patient experience with the Blom-Singer Dual Valve voice prosthesis. Laryngoscope. 2018;128(2):422-426. doi:10.1002/lary.26803 PubMed
35.Higgins JPT, Thomas J, Chandler J, et al. Cochrane Handbook for Systematic Reviews of Interventions version 6.5 (updated August 2024). The Cochrane Collaboration; 2024. Accessed December 11, 2024. www.training.cochrane.org/handbook
36.Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. doi:10.1136/bmj.n71 PubMed
37.CADTH Health Technology Review: Care for Adults Following Laryngectomy. Can J Health Technol. 2024;4(9). Accessed December 23, 2024. www.cda-amc.ca/voice-prostheses-and-heat-moisture-exchangers-adults-following-total-laryngectomy
38.Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. doi:10.1136/bmj.j4008 PubMed
39.Jansen JP, Trikalinos T, Cappelleri JC, et al. Indirect treatment comparison/network meta-analysis study questionnaire to assess relevance and credibility to inform health care decision making: an ISPOR-AMCP-NPC Good Practice Task Force report. Value Health. 2014;17(2):157-73. doi:10.1016/j.jval.2014.01.004. PubMed
40.Higgins JPT, Green S, eds. Figure 15.5.a: Drummond checklist (Drummond 1996). The Cochrane Collaboration; 2011. Accessed August 22, 2024. http://handbook-5-1.cochrane.org/chapter_15/figure_15_5_a_drummond_checklist_drummond_1996.htm
41.Agree Next Steps Consortium. The AGREE II Instrument. AGREE Enterprise; 2017. Accessed August 22, 2024. https://www.agreetrust.org/wp-content/uploads/2017/12/AGREE-II-Users-Manual-and-23-item-Instrument-2009-Update-2017.pdf
42.Staniszewska S, Brett J, Simera I, et al. GRIPP2 reporting checklists: tools to improve reporting of patient and public involvement in research. BMJ. 2017;358:j3453. doi:10.1136/bmj.j3453 PubMed
Appendix 1: Detailed Methods and Selection of Included Studies
Please note that this appendix has not been copy-edited.
Literature Search Methods
The literature search strategy used in this report is an update of 1 developed for a previous CDA-AMC report.37 For the current report, an information specialist conducted a literature search on key resources including MEDLINE, the Cochrane Database of Systematic Reviews, the International HTA Database, the websites of health technology assessment agencies in Canada and major international HTA agencies, as well as a focused internet search. The search approach was customized to retrieve a limited set of results, balancing comprehensiveness with relevance. The initial search was limited to English-language documents published between January 1, 2019 and July 18, 2024. For the current report, database searches were rerun on November 19, 2024 to capture any articles published or made available since the initial search date. The search of major HTA agencies was also updated to include documents published since July 2024. The strategy for MEDLINE follows; the search strategies for grey literature are available upon request.
Clinical Literature Search
Overview
Interface: Ovid
Databases:
MEDLINE All (1946-present)
Date of search: July 18, 2024; updated November 19, 2024
Search filters applied: Guidelines (for supplemental search only)
Limits:
Publication date limit: 2019 to present for initial search; July 2024 to present for updated search
Language limit: English language
Syntax | Description |
|---|---|
/ | At the end of a phrase, searches the phrase as a subject heading |
MeSH | Medical Subject Heading |
* | Before a word, indicates that the marked subject heading is a primary topic; or, after a word, a truncation symbol (wildcard) to retrieve plurals or varying endings |
adj# | Requires terms to be adjacent to each other within # number of words (in any order) |
.ti | Title |
.kf | Keyword heading word |
.ab | Abstract |
.au | Author name |
.pt | Publication type |
.sh | Subject heading |
.dt | Date the citation was added to PubMed (used for records beginning December 15, 2008) |
.ez | Date the citation was added to PubMed |
.da | Date MeSH terms were added to the citation |
Database Strategy
Note: Lines 21 and 22 of the search strategy were included only in the search update; these lines limit the original search to July 2024 onwards. The original search instead limited the date to 2019 onwards.
(heat adj2 moisture adj2 exchanger*).ti,ab.
Larynx, Artificial/
((Voice* or laryn*) adj4 (artificial* or prosthe* or replace* or replacing)).ti,ab.
((Voice* or larynx* or vocal* or speech) and (indwelling or in-dwelling)).ti,ab.
(Provox* or blom-singer* or blom singer).ti,ab.
1 or 2 or 3 or 4 or 5
Laryngectomy/ or (laryngectom* or post-laryngectom* or postlaryngectom*).ti,ab.
(guideline or practice guideline or consensus development conference or consensus development conference, NIH).pt.
(guideline* or standards or consensus* or recommendat*).ti.
(practice parameter* or position statement* or policy statement* or CPG or CPGs or best practice*).ti.
(care adj2 (path or paths or pathway or pathways or map or maps or plan or plans or standard)).ti.
((critical or clinical or practice) adj2 (path or paths or pathway or pathways or protocol*)).ti.
(algorithm* and (pharmacotherap* or chemotherap* or chemotreatment* or therap* or treatment* or intervention*)).ti.
(algorithm* and (screening or examination or test or tested or testing or assessment* or diagnosis or diagnoses or diagnosed or diagnosing)).ti.
(guideline* or standards or consensus* or recommendat*).au.
systematic review.ti,pt,kf,sh. and (practice guideline* or treatment guideline* or clinical guideline* or guideline recommendation*).ti,ab,kf.
or/8-16
7 and 17
6 or 18
limit 19 to English language
(202407* or 202408* or 202409* or 20241* or 2025*).dt,ez,da.
20 and 21
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1. Figure 1 presents the PRISMA32 flow chart of the study selection.
Exclusion Criteria
We excluded publications that did not meet the selection criteria outlined in Table 1, as well as duplicate publications. Additionally, we also excluded expert opinions or guidelines with unclear methods or recommendations, single-arm primary studies, and primary studies already included in at least 1 eligible systematic review for the same comparison outcome.
Definitions of “Systematic Review” and “Evidence-Based Guideline”
A review is considered systematic if it includes the following: a) an objective and/or research question(s); b) indications that evidence was searched for in a systematic way (e.g., information on 1 or more of the following provided: names of databases, search platforms/engines, search date, keywords or search strategy), and c) inclusion and exclusion criteria. An evidence-based clinical practice guideline is defined as a systematically developed statement or set of statements to assist practitioner- and patient decisions about appropriate health care for specific clinical circumstances. A guideline is considered evidence-based if a systematic search of the literature was undertaken and a guideline panel was involved to inform the recommendations.
Critical Appraisal of Included Studies
The included studies were critically appraised by 1 reviewer using the following tools as a guide: A Measurement Tool to Assess systematic Reviews 2 (AMSTAR 2)38 for systematic reviews and the “Questionnaire to assess the relevance and credibility of a network meta-analysis”39 for systematic review and network meta-analyses, Drummond checklist40 for economic evaluations, and the Appraisal of Guidelines for Research and Evaluation (AGREE) II instrument41 for guidelines. Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Engagement Process
Clinical Expert
This Rapid Review has been updated to augment findings of the rapid literature review with clinical and patient experience. A clinical reviewer was sourced via Speech-Language and Audiology Canada and contracted to provide detailed peer review of the drafted report, specifically to review any potential clinical misunderstandings and to supplement the clinical context for this relatively small population of patients.
Public Feedback
A draft version of this report was posted on the CDA-AMC website for open feedback from March 3 to March 14, 2025. Feedback from 1 external group was received, carefully reviewed and changes integrated into this version of the report.
Patient Engagement
We included the perspectives of 3 patients with lived experience of using a voice prosthesis and HMEs after having a laryngectomy.
Invitation to Participate and Consent
We reached out through email directly to patient advocacy groups. The preliminary engagement request included an overview of this project, the purpose of engagement, and the nature of engagement activities. Members of a patient group identified themselves as being interested in sharing their experiences. The CDA-AMC Patient Engagement Officer obtained the person’s informed consent to share their lived experiences regarding their voice prosthesis and HME.
Engagement Activities
They were provided with a brief background to the project via email and in a Zoom call when requested. Two patients preferred to meet via a 1-hour Zoom call to share their experience and 1 patient chose to respond to the questions via email. We reported the patient involvement results using the Guidance for Reporting Involvement of Patients and the Public (version 2) Short Form reporting checklist,42 which is outlined in Appendix 5.
All feedback received will be carefully considered by the research team and addressed within the report. Both clinical experts and patient partners will be invited to review the finalized version of the updated Rapid Review before publication.
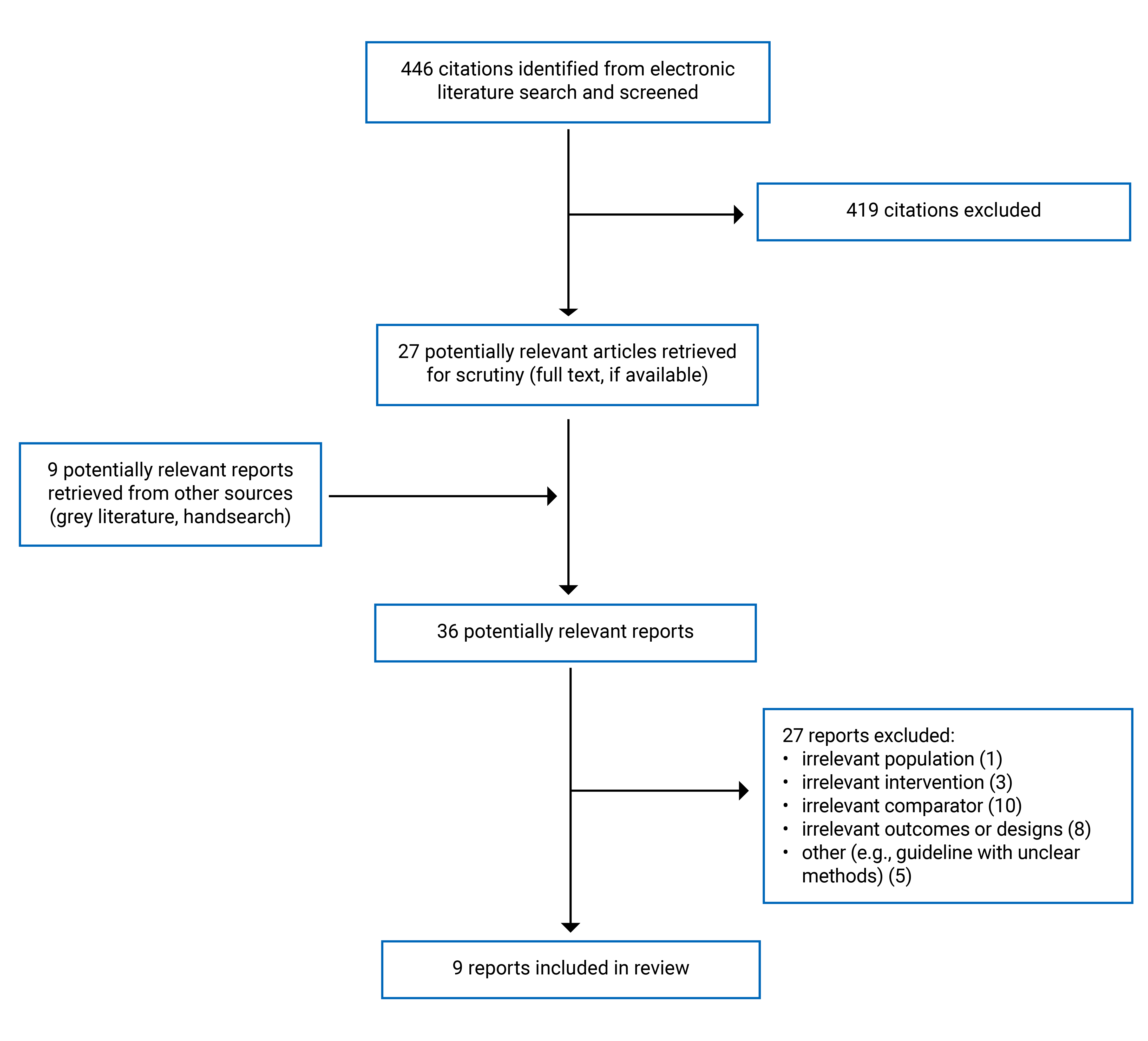
Appendix 2: Characteristics of Included Publications
Table 3: Characteristics of Included Systematic Reviews
Study citation, country, funding source | Study designs and numbers of primary studies included | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Plotas et al. (2024)27 Greece Funding source: Research Council of the University of Patras | Study design: systematic review of observational studies Number of included studies: 9 Country: NR Search: up to May 2023 | Patients after total laryngectomy Number of participants: from 18 to 133 Mean age: NR Age range: 45 years or older Sex: NR Disease duration: NR Radiotherapy: NR | Intervention: Esophageal voice without VPs Comparator: Voice prosthesis rehabilitation | Outcomes:
Follow-up: NR |
Maniaci et al. (2024)23 Belgium Funding source: NR | Study design: systematic review of observational studies Number of included studies: 15 Country: NR Search: from December 1, 2001, to June 1, 2021 | Patients after total laryngectomy for advanced laryngeal cancer Number of participants: 1,085 Mean age: 65.38 years Sex: male, 89.38% Disease duration: NR Radiotherapy: NR | Intervention: Voice prosthesis (indwelling and nonindwelling devices) rehabilitation (n = 869, 80.1%) Comparator: esophageal voice without VPs (n = 216, 19.9%) | Outcomes:
Follow-up: NR |
Ahmed et al. (2023)24 Netherlands Funding source: Atos Medical | Study design: mixed methods study with a rapid review Number of included studies: 10: 3 RCTs, 3 time-series studies, 1 retrospective cohort study, 3 studies with unclear design Country: US, Canada, France, Italy, Spain, the Netherlands, and Poland Search: from January, 2010 to February, 2021 | Patients who underwent total laryngectomy Number of participants: 550 (number in the individual studies ranged from 30 to 89) Age: NR Sex: NR Disease duration: NR Radiotherapy: NR | Intervention: HMEs (Assumption: HMEs were used in combination with VPs) Comparator: no HME use, an external humidifier, or a previous generation HME | Outcomes:
Follow-up: 3 months or NR |
Mayo-Yáñez et al. (2023)25 Spain Funding source: No funding support and the authors declared no conflict of interest | Study design: systematic review of observational studies Number of included studies: 4: 2 prospective case series, 1 prospective case-crossover, 1 case report Country: Germany, Netherlands, and Spain Search: from January, 2016 (year of the intervention commercialization) to February, 2020 (the paper was submitted in 2020 and was published in 2023) | Patients with laryngectomy and users of VP Number of participants: 55 patients (315 VP) Mean age: 62.71 Sex: male: 87.27% Disease duration: NR Radiotherapy: 55% to 100% when reported. | Intervention: PVX (n = 94) Comparator: control VP (Vega and ActiValve Light, n = 221) | Outcomes: VP duration Follow-up: NR |
Tawfik et al. (2021)26 Egypt Funding source: NR | Study design: systematic review and network meta-analysis Number of included studies: 120 in network meta-analysis; 27 in meta-analysis only Country: Australia, Belgium, Brazil, Canada, China, Croatia, Czech Republic, Denmark, UK, Egypt, Finland, France, Germany, Slovakia, Greece, India, Italy, Japan, Netherlands, Norway, Pakistan, Poland, South Africa, Spain, Sweden, Switzerland, Turkey, US. Search: up to May 11, 2019 | Patients who underwent total laryngectomy Number of participants: 11,918 Mean age: 17 to 90 years Sex: male: 71.7% Disease duration: NR Radiotherapy: 71.7%. | Intervention and comparators: various VPs that include Provox-1, Provox-2, Provox AV, Provox NiD, Provox Vega, SPVP, Nijdam, Groningen LR, Groningen ULR, BS-LP, | Outcomes: Devices replacements; Devices lifetime; Airflow resistance; MPT; Leakage rates; Speech rate; Patient device Preference; Phonatory effort; Voice speech quality; Fundamental frequency; Voice loudness; Speech intelligibility; Dislodgement; Fistula problems; Granulation; Prosthesis inaccurate size; Prosthesis deterioration; Survival rate; Aspiration pneumonia; Fungal colonization; Experience with speaking; Skin irritation; Chemoprophylaxis. Follow-up: from 0.5 to 133 months |
AV = ActiValve; BS-LP = Blom-Singer Low Pressure; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire-C30; EORTC QLQ-H&N35 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Head and Neck CANCER35; FACT-G = Functional Assessment of Cancer Therapy-General; GESQ = Groningen Enjoyment of Speech Questionnaire; HADS = Hospital Anxiety and Depression Scale; HMEs = heat and moisture exchangers; LR = low resistance; MPT = maximum phonation time; NR = not reported; P-SECEL = Portuguese Self Evaluation of Communication Experiences after Laryngectomy Cancer Questionnaire; PVX = Provox Vega XtraSeal; QoL = quality of life; RCT = randomized controlled trial; SF-36 = 36-item short form survey instrument; SPVP = sound-producing voice prosthesis; ULR = ultra low resistance; UW-QoL = University of Washington Quality of Life; VHI = Voice Handicap Index; VP = voice prostheses; VRQoL = voice-related quality of life.
Note: This table has not been copy-edited.
Table 4: Characteristics of Included Economic Evaluation
Study citation country, funding source | Type of analysis, time horizon, perspective | Population characteristics | Intervention and comparator(s) | Approach | Source of clinical, cost, and utility data used in analysis | Main assumptions |
|---|---|---|---|---|---|---|
Rodriguez-Lorenzana et al. (2023)28 Spain Funding source: covered by Fundación Profesor Nóvoa Santos (Hospital Teresa Herrera, 1ª Planta) | Type of analysis: Cost-effective analysis based on a crossover prospective observational study Time horizon: NR, but likely within study Perspective: Spanish national health system | Inclusion criteria: Patients who were laryngectomized, 18+, at least 3 months after total laryngectomy, at least 3 months after radiotherapy or chemotherapy, at least 3 years of follow-up, treated with proton-pump inhibitors, and had at least 3 months’ experience using the Provox Vega® 38 patients, 35 men and 3 women Mean age: 66.26 ± 9.36 years old | Intervention: Provox XtraSeal® Comparator: Provox Vega® | Outcome measures: The ICER was calculated | The study included the direct medical costs, such as the cost of the prostheses, which were obtained from the hospital’s economic department. The cost of each Provox Vega® was EUR 363 and, for Provox XtraSeal, a range between EUR 400 and EUR 600 was selected depending on the health centre assessed. | The anticipated change rate for Provox Vega® and Provox XtraSeal® was estimated at 3.5 changes per year. The predicted price for Provox Vega® was €1,269.08 and €1,928.55 for Provox XtraSeal®. The cost-effectiveness analysis aimed to achieve equal costs between the 2 devices. |
Miguel Mayo-Yáñez et al. (2022)29 Spain Funding source: Information not available | Type of analysis: CEA based on prospective case-crossover study Time Horizon: NR, but likely within study (mean follow-up: 5.24 years, from 4.04 years to 6.57 years) Perspective: Spanish Public National Health System | Total laryngectomized patients with Provox Vega® and endoprosthesis leakage to whom a Provox ActiValve® was placed. 5 Caucasian men, with a mean follow-up of 5.24 years (range 4.04 to 6.57), were selected. Mean age: 63.84 ± 0.38 years. | Intervention: Provox ActiValve Comparator: Provox Vega | Outcome measures:
| Cost of each Provox Vega: 363€, Cost of each Provox ActiValve:1,757.47€. The effectiveness of the treatment was estimated based on number of annual VP replacements and according to follow-up length. | The anticipated change rate for Provox Vega® and Provox ActiValve was estimated at 2.94 changes per year. The predicted price for Provox Vega® was €1,067.60 and €5,168.82 for Provox ActiValve. |
Beck et al. (2020)30 US Funding source: information not available | Type of analysis: cost-effectiveness and budget impact analysis Perspective: The model was based on a US health care and societal perspective. Time horizon: 20 years | Participants:
Mean age: HME patients 65.4 (37.9 to 88.9); ASC patients 67.7 (40.7 to 88.6) | Intervention: HME Comparator: alternative stoma cover | Study questionnaire was based on the Ackerstaff-Hilgers questionnaire A Markov decision model was developed with 3 mutually exclusive health states, reflecting the disease trajectory. Outcome measures: The ICER was used to evaluate the cost-utility of the HME system; represents the additional costs of HME use per QALY gained. | Utilities were obtained from the EQ-5D-5L (US tariff was used) Model inputs; clinical variables: device/equipment use, occurrence of pulmonary events, symptoms, productivity loss, treated with medication Costs: annual device costs, cost of accessories and equipment were included in the model. Hospital costs and medication costs were also obtained. All costs were calculated in US dollars Health effects: QALYs - survival probabilities after laryngectomy were derived from literature and assumed to be similar for both groups. In this analysis, disutilities were applied for progressive disease, daily extensive coughing, and mucus production per week. | The Markov model has a hypothetical cohort of 5,000 patients and all simulated patients in both groups start at disease-free survival. |
ASC = alternative stoma cover; CEA = cost-effectiveness analysis; HME = heat and moisture exchanger; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; NR = not reported; RCT = randomized controlled trial; VP = voice prosthesis.
Note: This table has not been copy-edited.
Table 5: Characteristics of Included Guidelines
Intended users, target population | Intervention and practice considered | Major outcomes considered | Evidence collection, selection, and synthesis | Evidence quality assessment | Recommendations development and evaluation | Guideline validation |
|---|---|---|---|---|---|---|
Mayo-Yáñez et al. (2024)31 | ||||||
Intended users: health care professionals: otorhinolaryngology specialists (physicians and residents), speech therapists, nursing staff, and other specialists Target population: Laryngectomized patients Country: Spain | Laryngectomized patients who are or could be users of voice prostheses | Vocal outcomes, quality of life, and complications. | The guideline authors searched MEDLINE, Embase, Scopus, Web of Science, PubMed, Science Citation Index, and the Cochrane Library between 1980 to 2023 and conducted a systematic review with 91 studies. | The Oxford Levels of Evidence system 2011: 1a: systematic review of RCTs or n-of-1 trials; to 5 (mechanism-based reasoning). | The recommendations were developed after reviewing and analyzing the most recent research: benefits, side effects, and risks. Grade of Recommendation: B or C, but the meaning of the grade of recommendation is not specified. The authors drafted and reviewed the recommendations. They used a mini-Delphi method with 2 meetings to define them. | The recommendations were then sent to the entire working group for anonymous feedback and reviewed in subsequent meetings. The guideline panel included otolaryngologists, head and neck surgeons, and expert speech therapists. The guideline was published in a peer-reviewed journal. |
RCT = randomized controlled trials.
Note: This table has not been copy-edited.
Appendix 3: Critical Appraisal of Included Publications
Please note that this appendix has not been copy-edited.
Table 6: Strengths and Limitations of Systematic Reviews Using AMSTAR 238 and the ISPOR Questionnaire39
Strengths | Limitations |
|---|---|
Plotas et al. (2024)27 | |
|
|
Maniaci et al. (2024)23 | |
|
|
Ahmed et al. (2023)24 | |
|
|
Mayo-Yáñez et al. (2023)25 | |
|
|
Tawfik et al. (2021)26 | |
|
|
AMSTAR 2 = A MeaSurement Tool to Assess systematic Reviews 2; CCAT = Crowe Critical Appraisal Tool; CINAHL = Cumulative Index to Nursing and Allied Health Literature; GRADE = Grading of Recommendations Assessment, Development and Evaluation; ISPOR = Questionnaire to assess the relevance and credibility of a network meta-analysis; mRCT = metaRegister of Controlled Trials; POPLINE = Population Information Online; RCTs = randomized controlled trials; RoB = risk of bias; SIGLE = System for Information on Grey Literature in Europe; VHL = Virtual Health Library; WHO GHL = WHO Global Health Library.
Table 7: Strengths and Limitations of Economic Evaluation Using the Drummond Checklist40
Strengths | Limitations |
|---|---|
Rodriguez-Lorenzana et al. (2023)28 | |
Study design:
Data Collection:
Analysis and interpretation:
|
|
Mayo-Yáñez et al. (2022)29 | |
Study design
Data Collection
Analysis and interpretation:
|
|
Beck et al. (2020)30 | |
Study design:
Data collection:
Analysis and interpretation:
|
|
Table 8: Strengths and Limitations of Guidelines Using AGREE II41
Item | Mayo-Yáñez et al. (2024)31 |
|---|---|
Domain 1: Scope and purpose | |
1. The overall objective(s) of the guideline is (are) specifically described. | Yes |
2. The health question(s) covered by the guideline is (are) specifically described. | Yes |
3. The population (patients, public, and so on) to whom the guideline is meant to apply is specifically described. | Yes |
Domain 2: Stakeholdera involvement | |
4. The guideline development group includes individuals from all relevant professional groups. | Yes |
5. The views and preferences of the target population (patients, public, and so on) have been sought. | No |
6. The target users of the guideline are clearly defined. | Yes |
Domain 3: Rigour of development | |
7. Systematic methods were used to search for evidence. | Yes |
8. The criteria for selecting the evidence are clearly described. | Yes |
9. The strengths and limitations of the body of evidence are clearly described. | Yes |
10. The methods for formulating the recommendations are clearly described. | Yes |
11. The health benefits, side effects, and risks have been considered in formulating the recommendations. | To some extent but lacked details |
12. There is an explicit link between the recommendations and the supporting evidence. | No |
13. The guideline has been externally reviewed by experts before its publication. | NR |
14. A procedure for updating the guideline is provided. | No |
Domain 4: Clarity of presentation | |
15. The recommendations are specific and unambiguous. | No |
16. The different options for management of the condition or health issue are clearly presented. | No |
17. Key recommendations are easily identifiable. | Yes |
Domain 5: Applicability | |
18. The guideline describes facilitators and barriers to its application. | Partially mentioned facilitators |
19. The guideline provides advice and/or tools on how the recommendations can be put into practice. | No |
20. The potential resource implications of applying the recommendations have been considered. | No |
21. The guideline presents monitoring and/or auditing criteria. | No |
Domain 6: Editorial independence | |
22. The views of the funding body have not influenced the content of the guideline. | Unclear (Atos Medical funded this guideline, and 1 of the co-authors is an employee of Atos Medical) |
23. Competing interests of guideline development group members have been recorded and addressed. | Yes (the authors declare no conflicts of interest) |
AGREE II = Appraisal of Guidelines for Research and Evaluation II; NR = not reported.
aThe term “stakeholder” is from the original source.
Appendix 4: Main Study Findings
Please note that this appendix has not been copy-edited.
Table 9: Summary of Findings by Outcome — Quality of Life for TEV Versus EV
Author (year) and study design | Results | ||||
|---|---|---|---|---|---|
Group (number of studies or participants) or variables | Effect measure | Effect estimate | I2 (%) | Notes | |
VHI (the range and direction of total scores were not reported) | |||||
Maniaci et al. (2024)23 Systematic review with 15 studies | TEV (9 studies) | Pooled Mean (SD), points | 31.93 (12.11) | NA | P = 0.003 |
EV (9 studies) | Pooled Mean (SD), points | 35.39 (20.6) | NA | ||
Comparison between TEV and EV (5 studies) | MD (95% CI), points | −1.90 (−14.83 to 11.02) | 97% | Random-effects model | |
VRQOL (the range and direction of total scores were not reported) | |||||
Maniaci et al. (2024)23 Systematic review with 15 studies | TEV (7 studies) | Pooled Mean (SD), points | 8.27 (5.98) | NA | NS |
EV (7 studies) | Pooled Mean (SD), points | 9.27 (2.02) | NA | ||
Comparison between TEV and EV (3 studies) | MD (95% CI), points | −0.74 (−2.85 to 1.38) | 71% | Random-effects model | |
SF-36 (the range and direction of total scores were not reported) | |||||
Maniaci et al. (2024)23 Systematic review with 15 studies | TEV (4 studies) | Pooled Mean (SD), points | 58.7(2.94) | NA | P < 0.001 |
EV (4 studies) | Pooled Mean (SD), points | 61.84 (8.33) | NA | ||
CI = confidence interval; EV = esophageal voice; NA = not applicable; NS = not statistically significant; SD = standard deviation; SF-36 = 36-item short form survey instrument; TEV = tracheoesophageal voice; VHI = Voice Handicap Index; VP = voice prostheses; VRQoL = voice-related quality of life.
Table 10: Summary of Findings — Various Clinical Outcomes for HMEs Versus Non-HMEs
Author (year) and study design | Results | ||||
|---|---|---|---|---|---|
Number of studies | Outcome/effect measure | Effect estimate | P | Notes | |
QOL (the range and direction of total scores were not reported) | |||||
Ahmed et al. (2023)24 Study design: mixed methods study with a rapid review with 10 studies | QOL (Shortness of breath) | ||||
1 study (Brook et al. 2013) | QOL questionnaire (unclear tool), points | Non-HME: 4.6 Provox Micron HMEs (first-generation): 4.9 Provox HME (first-generation): 4.3 | 0.363 | NS | |
QOL (sleep quality) | |||||
1 study (Brook et al. 2013) | QOL questionnaire (unclear tool), points | Non-HME: 4.5 Provox Micron HMEs (first-generation): 4.8 Provox HME (first-generation): 4.6 | 0.913 | NS | |
QoL (speech quality) | |||||
1 study (Brook et al. 2013) | QOL questionnaire (unclear tool), points | Non-HME: 7.6 Provox Micron HMEs (first-generation): 9.4 Provox HME (first-generation): 8.0 | 0.396 | NS | |
QOL (psychosocial aspects) | |||||
1 study (Brook et al. 2013) | QOL questionnaire (unclear tool), points | Non-HME: 5.8 Provox Micron HMEs (first-generation): 6.5 Provox HME (first-generation): 6.6 | 0.688 | NS | |
QoL (social contacts) | |||||
1 study (Brook et al. 2013) | QOL questionnaire (unclear tool), points | Non-HME: 9.6 Provox Micron HMEs (first-generation): 8.4 Provox HME (first-generation): 9.7 | 0.438 | NS | |
Mucus production | |||||
Ahmed et al. (2023)24 Study design: mixed methods study with a rapid review with 10 studies | 1 study (Ebersole et al. 2020) | Rate of mucus production | XtraHME: 0.13 per 10 inpatient days EH:0.38 per 10 inpatient days | P = 0.02 | Statistically lower in the XtraHME group |
1 study (Ebersole et al. 2020) | Proportion of patients with ≥ 1 mucus plug events | XtraHME: 11% EH: 50% | P = 0.01 | Statistically reduced in the XtraHME group | |
1 study (Foreman et al. 2016) | Proportion of patients experiencing mucus plugging | HME: 12.5% EH: 87.5% | P = 0.002 | Odds ratio of a mucus plug event when not using HME: 8.27 (confidence interval not reported) | |
Coughing | |||||
Ahmed et al. (2023)24 Study design: mixed methods study with a rapid review with 10 studies | 1 study (Dassonville et al. 2016) | Coughing (an analogue scale ranging from 0 to 10), points | “At 3 months, there was a significant decrease in coughing in the HME group versus the no-HME control group.” (p. 5) | P = 0.00174 | Statistically decreased in the HME group |
1 study (Bień et al. 2010) | Frequency of coughing | HME: week 1: 48 times; week 12: 30 times Control: week 1: 60 times; week 12: 56 times | < 0.001 | Statistically decrease in the HME group | |
1 study (Mérol et al.) | Number of coughing episodes | “In the EH group, 73% of the patients had 2 to 10 spontaneous coughing episodes per day, whereas 8% had 20, another 8% had 30, and 4% had 72 episodes a day (for 8%, this information was missing). In the HME group, most patients (90%) had 1 to 5 spontaneous coughing episodes per day, whereas 4.3% had 10 and another 4.3% had 20 such episodes per day” (p.6) | < 0.001 | Significantly lower in the HME group | |
Forced expectorations | |||||
Ahmed et al. (2023)24 Study design: mixed methods study with a rapid review with 10 studies | 1 study (Bień et al. 2010) | Frequency of forced expectorations | HME: week 1: 56 times; week 12: 27 times Control: week 1: 59 times; week 12: 53 times | < 0.001 | Statistically decreased in the HME group |
Sleep quality | |||||
Ahmed et al. (2023)24 Study design: mixed methods study with a rapid review with 10 studies | 1 study (Foreman et al. 2016) | Sleep quality (unclear tool) | “No significant difference was reported between the HME group and EH group in sleep quality” (p.6) | NR | NS |
1 study (Bień et al. 2010) | Frequency of patients who had sleeping problems | “In the control group, almost all the patients (97.5%) had sleeping problems, and this did not change over time. In the full compliance HME group (first-generation), 79% of the patients had sleeping problems at baseline, and 72% had this problem after 3 months of HME use.” (p. 6) | NR | NS | |
Speech quality | |||||
Ahmed et al. (2023)24 Study design: mixed methods study with a rapid review with 10 studies | 1 study (Brook et al. 2013) | Speech quality (unclear tool) | “The HME users and Micron users reported a better voice than did the non-HME users (not statistically significant)” (p.6) | NR | NS |
Physiotherapy | |||||
Ahmed et al. (2023)24 Study design: mixed methods study with a rapid review with 10 studies | 1 study (Foreman et al. 2016) | The number of days requiring chest physiotherapy after surgery | Provox XtraHME: 1.75 days EH: 3.20 days | 0.034 | Significantly reduced in the HME group |
Tracheobronchitis or pneumonia episodes | |||||
Ahmed et al. (2023)24 Study design: mixed methods study with a rapid review with 10 studies | 1 study (van den Boer et al. 2014) | Tracheobronchitis or pneumonia episodes | HME (first-generation): 0.066 episodes per patient per year Non-HME: 0.285 episodes per patient per year | 0.047 | Statistically lower in the HME group |
1 study (van den Boer et al. 2014) | Pulmonary infections (tracheobronchitis and pneumonia together) | HME (first-generation): 0.092 episodes per patient per year Non-HME: 0.129 episodes per patient per year | 0.33 | NS | |
Social contacts | |||||
Ahmed et al. (2023)24 Study design: mixed methods study with a rapid review with 10 studies | 1 study (Parrilla et al. 2015) | Unclear tool (after 12 weeks), points | “A statistically nonsignificant improvement in social contacts, with a baseline value of 8.1 versus a value 8.3 after 12 weeks (P =.728), was reported in the structured questionnaires when comparing no HME use with HME (second generation) use.” (p. 7) | 0.728 | NS |
Patient satisfaction | |||||
Ahmed et al. (2023)24 Study design: mixed methods study with a rapid review with 10 studies | 1 study (Mérol et al., 2012) | Unclear tool | “Patients’ satisfaction showed a significant improvement of first-generation HME over EH (P<.001). Patient satisfaction with the EH was quite low: 11% of the patients reported that they were satisfied with it, 8% reported they somewhat liked it, and 81% reported that they did not like it. All the patients (100%) in the HME (first-generation) group were satisfied with the device” (p. 7) | < 0.001 | Statistically improvement in the HME group over EH |
EH = external humidifier; HME = heat and moisture exchanger; NR = not reported; NS = not statistically significant; QOL = quality of life.
Table 11: Summary of Findings by Outcome — Device Replace Frequency
Author (year) and study design | Results | |||
|---|---|---|---|---|
VP device | Comparator VP | Effect estimate: RR (95% CI) | Notes | |
Tawfik et al. (2021)26 Systematic review with network meta-analysis (27 studies with 5,724 patients) | Provox-1 | BS-LP | 0.69 (0.19 to 2.51) | NS |
Nijdam | BS-LP | 0.78 (0.09 to 6.73) | NS | |
Groningen ULR | BS-LP | 0.81 (0.07 to 9.14) | NS | |
Provox AV | BS-LP | 0.96 (0.09 to 10.74) | NS | |
Provox NiD | BS-LP | 1.24 (0.17 to 9.07) | NS | |
Provox Vega | BS-LP | 1.24 (0.17 to 9.11) | NS | |
Provox 2 | BS-LP | 1.30 (0.30 to 5.58) | NS | |
Groningen LR | BS-LP | 1.44 (0.30 to 7.03) | NS | |
SPVP | BS-LP | 10.10 (0.71 to 144.07) | NS | |
AV = ActiValve; BS-LP = Blom-Singer Low Pressure; CI = confidence interval; LR = Low Resistance; NS = not statistically significant; RR = relative risk; SPVP = Sound-Producing Voice Prosthesis; VP = voice prosthesis.
Table 12: Summary of Findings by Outcome — Device Lifetime
Author (year) and study design | Results | |||
|---|---|---|---|---|
Comparisons | Effect measure | Effect estimate (years) | Notes | |
Tawfik et al. (2021)26 Systematic review with network meta-analysis (33 studies with 4,777 patients) | Provox AV vs. BS Advantage | MD (95% CI) | 17.25 (0.40 to 34.09) | Statistically significant (P value was not reported) |
Nijdam vs. BS Advantage | MD (95% CI) | 9.87 (−6.67 to 26.42) | NS | |
Provox 1 vs. BS Advantage | MD (95% CI) | 9.00 (−7.24 to 25.25) | NS | |
Groningen LR vs. BS Advantage | MD (95% CI) | 8.44 (−7.76 to 24.65) | NS | |
Groningen ULR vs. BS Advantage | MD (95% CI) | 7.45 (−9.18 to 24.09) | NS | |
BS DV vs. BS Advantage | MD (95% CI) | 6.30 (−19.12 to 31.72) | NS | |
Provox 2 vs. BS Advantage | MD (95% CI) | 6.82 (−9.26 to 22.91) | NS | |
Provox Vega vs. BS Advantage | MD (95% CI) | 5.24 (−10.87 to 21.36) | NS | |
BS-LP vs. BS Advantage | MD (95% CI) | 4.97 (−11.09 to 21.03) | NS | |
Mayo-Yáñez et al. (2023)25 Systematic review with 4 studies | PVX vs. Control VP (Vega or ActiValve light) | Mean ± SD (95% CI) | PVX: 114.28 ± 73.2 (98.29 to 130.26) days Control: 102.98 ± 17.74 (100.6 to 105.35) days | No statistical test performed |
AV = ActiValve; BS-LP = Blom-Singer Low Pressure; CI = confidence interval; DV = dual valve; LP = low pressure; LR = Low Resistance; MD = mean difference; NR = not reported; NS = not statistically significant; PVX = Provox Vega XtraSeal; ULR = ultra low resistance.
Table 13: Summary of Findings by Outcome — Air Flow Resistance
Author (year) and study design | Results | |||
|---|---|---|---|---|
VP device | Comparator VP | Effect estimate: RR (95% CI) | Notes | |
Tawfik et al. (2021)26 Systematic review with network meta-analysis (8 studies with 1,850 patients) | Provox 2 | Groningen LR | 0.42 (0.08 to 2.11) | NS |
Provox 1 | Groningen LR | 0.84 (0.18 to 3.95) | NS | |
Nijdam | Groningen LR | 1.31 (0.22 to 7.67) | NS | |
CI = confidence interval; LR = low resistance; NS = not statistically significant; RR = relative risk.
Table 14: Summary of Findings by Outcome — Maximum Phonation Time
Author (year) and study design | Results | |||
|---|---|---|---|---|
VP device | Comparator VP | Effect estimate: MD (95% CI), Seconds | Notes | |
Tawfik et al. (2021)26 Systematic review with network meta-analysis (13 studies with 639 patients) | Provox HME | BS Advantage | 6.30 (3.34 to 9.26) | Statistically significant (P value was not reported) |
BS ATV | BS Advantage | 3.00 (−0.35 to 6.35) | NS | |
Provox FreeHands HME | BS Advantage | −2.90 (−6.07 to 0.27) | NS | |
Provox 2 | BS Advantage | −3.60 (−7.55 to 0.35) | NS | |
Provox 1 | BS Advantage | −5.63 (−8.99 to −2.27) | Statistically significant (P value was not reported) | |
BS-LP | BS Advantage | −5.90 (−9.26 to −2.53) | Statistically significant (P value was not reported) | |
Panje | BS Advantage | −7.90 (−12.14 to −3.65) | Statistically significant (P value was not reported) | |
Groningen LR | BS Advantage | −12.38 (−22.69 to −2.07) | Statistically significant (P value was not reported) | |
ATV = Adjustable Tracheostoma Valve; BS = Blom-Singer; CI = confidence interval; HME = heat and moisture exchanger; LR = low resistance; MD = mean difference; NS = not statistically significant; VP = voice prostheses
Table 15: Summary of Findings by Outcome — Leakage
Author (year) and study design | Results | |||
|---|---|---|---|---|
VP device | Comparator VP | Effect estimate: RR (95% CI) | Notes | |
Tawfik et al. (2021)26 Systematic review with network meta-analysis (40 studies with 1,493 patients) | Provox Vega | BS-LP | 1.87 (0.97 to 3.60) | NS |
Provox 2 | BS-LP | 2.08 (1.11 to 3.88) | Statistically significant (P value was not reported) | |
Nijdam | BS-LP | 2.23 (1.27 to 3.90) | Statistically significant (P value was not reported) | |
Groningen LR | BS-LP | 2.39 (1.37 to 4.15) | Statistically significant (P value was not reported) | |
Provox 1 | BS-LP | 3.25 (1.89 to 5.60) | Statistically significant (P value was not reported) | |
BS-LP = Blom-Singer Low Pressure; CI = confidence interval; LR = low resistance; NS = not statistically significant; RR = relative risk; VP = voice prosthesis.
Table 16: Summary of Findings by Outcome — Speech Rate
Author (year) and study design | Results | |||
|---|---|---|---|---|
VP device | Comparator VP | Effect estimate: MD (95% CI) (units not reported) | Notes | |
Tawfik et al. (2021)26 Systematic review with network meta-analysis (40 studies with 1,493 patients) | Groningen LR | BS-LP | −1.75 (−24.67 to 21.17) | NS |
BS-LP = Blom-Singer Low Pressure; CI = confidence interval; LR = low resistance; MD = mean difference; NS = not statistically significant; VP = voice prostheses.
Table 17: Summary of Findings by Outcome — Patient Device Preference
Author (year) and study design | Results | |||
|---|---|---|---|---|
VP device | Comparator VP | Effect estimate: OR (95% CI) | Notes | |
Tawfik et al. (2021)26 Systematic review with network meta-analysis (21 studies with 932 patients) | Provox 2 | BS-LP | 33.88 (0.65 to 1,762.24) | NS |
Provox 1 | BS-LP | 12.04 (0.27 to 538.08) | NS | |
Provox XtraHME | BS-LP | 13.09 (0.18 to 974.17) | NS | |
Provox HME | BS-LP | 10.27 (0.54 to 194.25) | NS | |
Provox Stomafilter HME | BS-LP | 2.91 (0.03 to 266.18) | NS | |
Groningen LR | BS-LP | 1.46 (0.03 to 65.10) | NS | |
Provox FreeHands | BS-LP | 0.67 (0.01 to 61.92) | NS | |
Provox FreeHands HME | BS-LP | 0.19 (0.00 to 12.38) | NS | |
VoiceMaster | BS-LP | 0.10 (0.00 to 23.37) | NS | |
External Humidifier | BS-LP | 0.04 (0.00 to 1.22) | NS | |
BS-LP = Blom-Singer Low Pressure; CI = confidence interval; HME = heat and moisture exchanger; LR = low resistance; NS = not statistically significant; OR = odds ratio; VP = voice prostheses.
Table 18: Summary of Findings by Outcome — Increase Phonatory Effort
Author (year) and study design | Results | |||
|---|---|---|---|---|
VP device | Comparator VP | Effect estimate: OR (95% CI) | Notes | |
Tawfik et al. (2021)26 Systematic review with network meta-analysis (4 studies with 75 patients) | Provox Vega | BS-LP | 4.11 (1.29 to 13.06) | Statistically significant (P value was not reported) |
BS-LP = Blom-Singer Low Pressure; CI = confidence interval; NS = not statistically significant; OR = odds ratio; VP = voice prostheses.
Table 19: Summary of Findings by Outcome — Voice Speech Quality
Author (year) and study design | Results | |||
|---|---|---|---|---|
VP device | Comparator VP | Effect estimate: OR (95% CI) | Notes | |
Tawfik et al. (2021)26 Systematic review with network meta-analysis (6 studies with 620 patients) | Provox Vega | BS-LP | 16.41 (4.33 to 62.22) | Statistically significant (P value was not reported) |
Panje | BS-LP | 1.00 (0.16 to 6.08) | NS | |
BS-LP = Blom-Singer Low Pressure; CI = confidence interval; NS = not statistically significant; OR = odds ratio; VP = voice prostheses.
Table 20: Summary of Findings by Outcome — Fundamental Frequency
Author (year) and study design | Results | |||
|---|---|---|---|---|
VP device | Comparator VP | Effect size: MD (95% CI) (units not reported) | Notes | |
Tawfik et al. (2021)26 Systematic review with network meta-analysis (8 studies with 148 patients) | SPVP | Groningen LR | 96.33 (17.29 to 175.37) | Statistically significant (P value was not reported) |
Provox 1 | Groningen LR | 0.08 (−4.21 to 4.36) | NS | |
BS-LP = Blom-Singer Low Pressure; CI = confidence interval; LR = low resistance; MD = mean difference; NS = not statistically significant; SPVP = sound-producing voice prosthesis; VP = voice prosthesis.
Table 21: Summary of Findings by Outcome — Voice Loudness
Author (year) and study design | Results | |||
|---|---|---|---|---|
VP device | Comparator VP | Effect estimate: MD (95% CI) (units not reported) | Notes | |
Tawfik et al. (2021)26 Systematic review with network meta-analysis (7 studies with 247 patients) | Staffieri | BS-LP | 0.03 (−11.75 to 11.81) | NS |
Provox 1 | BS-LP | −0.50 (−5.48 to 4.48) | NS | |
Provox NiD | BS-LP | −1.00 (−4.62 to 2.62) | NS | |
BS-LP = Blom-Singer Low Pressure; CI = confidence interval; LR = low resistance; MD = mean difference; NS = not statistically significant; VP = voice prosthesis.
Table 22: Summary of Findings by Outcome — Speech Intelligibility
Author (year) and study design | Results | |||
|---|---|---|---|---|
VP device | Comparator VP | Effect estimate: OR (95% CI) | Notes | |
Tawfik et al. (2021)26 Systematic review with network meta-analysis (7 studies with 692 patients) | Nijdam | Groningen LR | 3.02 (0.12 to 74.99) | NS |
Provox 1 | Groningen LR | 0.10 (0.02 to 0.55) | Statistically significant (P value was not reported) | |
CI = confidence interval; LR = low resistance; NS = not statistically significant; OR = odds ratio; VP = voice prosthesis.
Table 23: Summary of Findings by Outcome — Stoma Stenosis
Author (year) and study design | Results | |||
|---|---|---|---|---|
VP device | Comparator VP | Effect estimate: RR (95% CI) | Notes | |
Tawfik et al. (2021)26 Systematic review with network meta-analysis (8 studies with 437 patients) | Provox Vega | BS-LP | 5.25 (2.06 to 13.40) | Statistically significant (P value was not reported) |
BS-LP = Blom-Singer Low Pressure; CI = confidence interval; RR = relative risk; VP = voice prosthesis.
Table 24: Summary of Findings by Outcome — Dislodgement
Author (year) and study design | Results | |||
|---|---|---|---|---|
VP device | Comparator VP | Effect estimate: RR (95% CI) | Notes | |
Tawfik et al. (2021)26 Systematic review with network meta-analysis (31 studies with 2,977 patients) | Provox 2 | Provox 1 | 0.27 (0.13 to 0.57) | Statistically significant (P value was not reported) |
Provox Vega | Provox 1 | 0.28 (0.12 to 0.67) | Statistically significant (P value was not reported) | |
CI = confidence interval; RR = relative risk; VP = voice prosthesis.
Table 25: Summary of Findings by Outcome — Fistula Problems
Author (year) and study design | Results | |||
|---|---|---|---|---|
VP device | Comparator VP | Effect estimate: RR (95% CI) | Notes | |
Tawfik et al. (2021)26 Systematic review with network meta-analysis (13 studies with 1,767 patients) | Groningen LR | ESKA-Herrmann | 0.76 (0.50 to 1.18) | NS |
Provox 1 | ESKA-Herrmann | 0.87 (0.66 to 1.15) | NS | |
Nijdam | ESKA-Herrmann | 0.96 (0.61 to 1.51) | NS | |
CI = confidence interval; LR = low resistance; NS = not statistically significant; RR = relative risk; VP = voice prosthesis.
Table 26: Summary of Findings by Outcome — Granulation
Author (year) and study design | Results | |||
|---|---|---|---|---|
VP device | Comparator VP | Effect estimate: RR (95% CI) | Notes | |
Tawfik et al. (2021)26 Systematic review with network meta-analysis (23 studies with 3,474 patients) | Provox 2 | BS-LP | 0.73 (0.02 to 26.32) | NS |
Provox 1 | BS-LP | 0.95 (0.13 to 7.03) | NS | |
Provox Vega | BS-LP | 0.87 (0.01 to 63.18) | NS | |
VoiceMast | BS-LP | 0.96 (0.06 to 15.20) | NS | |
Groningen LR | BS-LP | 0.97 (0.05 to 18.26) | NS | |
Nijdam | BS-LP | 1.93 (0.10 to 36.18) | NS | |
BS-LP = Blom-Singer Low Pressure; CI = confidence interval; LR = low resistance; NS = not statistically significant; RR = relative risk; VP = voice prosthesis.
Table 27: Summary of Findings by Outcome — Prosthesis Inaccurate Size
Author (year) and study design | Results | |||
|---|---|---|---|---|
VP device | Comparator VP | Effect estimate: RR (95% CI) | Notes | |
Tawfik et al. (2021)26 Systematic review with network meta-analysis (4 studies with 388 patients) | Provox 2 | Provox 1 | 0.77 (0.23 to 2.61) | NS |
CI = confidence interval; NS = not statistically significant; RR = relative risk; VP = voice prosthesis.
Table 28: Summary of Findings by Outcome — Prosthesis Deterioration
Author (year) and study design | Results | |||
|---|---|---|---|---|
VP device | Comparator VP | Effect estimate: RR (95% CI) | Notes | |
Tawfik et al. (2021)26 Systematic review with network meta-analysis (3 studies with 200 patients) | Provox 2 | Provox 1 | 2.62 (0.88 to 7.81) | NS |
CI = confidence interval; NS = not statistically significant; RR = relative risk; VP = voice prosthesis.
Table 29: Summary of Findings by Outcome — Survival Rate
Author (year) and study design | Results | |||
|---|---|---|---|---|
VP device | Comparator VP | Effect estimate: RR (95% CI) | Notes | |
Tawfik et al. (2021)26 Systematic review with network meta-analysis (3 studies with 135 patients) | Provox 1 | BS-LP | 1.99 (0.49 to 8.15) | NS |
BS-LP = Blom-Singer Low Pressure; CI = confidence interval; NS = not statistically significant; RR = relative risk; VP = voice prosthesis.
Table 30: Summary of Findings by Outcome — Other Outcomes
Author (year) and study design | Results | ||||
|---|---|---|---|---|---|
Group (number of studies) | Effect measure | Effect estimate (percentage) | I2 (%) | Notes | |
Aspiration pneumonia | |||||
Tawfik et al. (2021)26 Systematic review with network meta-analysis (4 studies with 274 patients) | Provox 2 (1 study) | Event rate (95% CI) | 0.063 (0.016 to 0.218) | NA | — |
Provox 1 (1 study) | Event rate (95% CI) | 0.034 (0.011 to 0.102) | NA | — | |
BS-LP (2 studies) | Event rate (95% CI) | 0.041 (0.019 to 0.089) | NR | — | |
Fungal colonization | |||||
Tawfik et al. (2021)26 Systematic review with network meta-analysis (6 studies with 213 patients) | Provox 2 (1 study) | Event rate (95% CI) | 0.810 (0.663 to 0.902) | NA | — |
Provox 1 (2 studies) | Event rate (95% CI) | 0.652 (0.552 to 0.741) | NR | — | |
BS-LP (2 studies) | Event rate (95% CI) | 0.500 (0.350 to 0.650) | NR | — | |
Rate of patients who were fluent in speaking | |||||
Tawfik et al. (2021)26 Systematic review with network meta-analysis (4 studies with 274 patients) | Provox Hands-free HME ENB (1 study) | Event rate (95% CI) | 0.792 (0.587 to 0.911) | NA | — |
Provox HME (1 study) | Event rate (95% CI) | 0.500 (0.342 to 0.658) | NA | — | |
BS-LP (2 studies) | Event rate (95% CI) | 0.480 (0.370 to 0.592) | NR | — | |
Groningen LR (1 Study) | Event rate (95% CI) | 0.352 (0.237 to 0.587) | NA | — | |
Provox 1 (1 study) | Event rate (95% CI) | 0.222 (0.056 to 0.579) | NA | — | |
Provox Hands-free HME (1 study) | Event rate (95% CI) | 0.208 (0.089 to 0.413) | NA | — | |
Skin irritation rate | |||||
Tawfik et al. (2021)26 Systematic review with network meta-analysis (6 studies with 213 patients) | Overall | Event rate (95% CI) | 0.189 (0.113 to 0.300) | NA | — |
Provox StabiliBase (1 study) with the highest rate | Event rate (95% CI) | 0.571 (0.316 to 0.794) | NA | — | |
BS-LP (1 studies) with the lowest rate | Event rate (95% CI) | 0.019 (0.005 to 0.074) | NA | — | |
BS-LP = Blom-Singer Low Pressure; CI = confidence interval; ENB = external neck brace; HME = heat and moisture exchanger; LR = low resistance; NA = not applicable; NR = not reported NS = not statistically significant.
Table 31: Summary of Findings of the Included Economic Evaluations
Main study findings | Authors’ conclusion |
|---|---|
Rodriguez-Lorenzana et al. (2023)28 | |
| “ By reducing the number of changes needed, the Provox XtraSeal® prosthesis offers a cost-effective alternative. The positive cost-effectiveness relationship of the Provox XtraSeal® prosthesis implies that the benefits gained from using this prosthesis outweigh the associated costs” (p. 10) |
Mayo-Yáñez et al. (2022)29 | |
| “The results proved the significant differences in terms of prosthesis duration between Provox Vega and Provox ActiValve, as week as its use is more effective and less expensive. These findings support the use of Provox ActiValve in patients with increased prosthesis replacements due to endoprosthesis leakage, to reduce the number of changes and cost.” (p. 4171 to 4172) |
Beck et al. (2020)30 | |
Health care perspective:
Social Perspective:
| “HME use scores favorably on cost-effectiveness compared with the ASC use in the pulmonary rehabilitation after laryngectomy in the US healthcare and societal setting.” (p. 3732) |
ASC = alternative stoma cover; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; VP = voice prosthesis.
Table 32: Summary of Recommendations in the Included Guidelines
Recommendations and supporting evidence | Quality of evidence and strength of recommendations |
|---|---|
Mayo-Yáñez (2024)31 | |
“For the management of periprosthetic leakage, the replacement of the prosthesis with a double-flanged one, such as the Provox® Vega™ XtraSeal™, is recommended.” (p. 8) (Recommendation 15) Relevant supporting evidence: “Replacement with a double-flanged prosthesis (Provox® Vega™ XtraSeal™) has shown a reduction in periprosthetic leakage (9.62% with XtraSeal vs. 22.43% in the control group) and has been shown to be a cost-effective procedure in the long term (3a, B). The Blom-Singer large oesophageal and tracheal flange VP is also a useful solution for the management of periprosthetic leakage, ensuring similar voice quality and an identical lifespan to that of other voice prostheses.” (p. 9) | Recommendation: B; based on 3b evidence. |
“For the management of periprosthetic leakage, VP replacement with the adjustment of diameter and length, or the placement of a silicone sheet on the tracheal side of the prosthesis, is also recommended.” (p. 8) (Recommendation 16) Relevant supporting evidence: “The management of this complication is usually conservative (4, C). Initially, techniques such as adjusting the size of the prosthesis or placing a silicone ring around the tracheal face of the prosthesis are used.” (p. 8) | Recommendation: C; based on C evidence. |
VP = voice prosthesis.
Appendix 5: Patient Involvement
Please note that this appendix has not been copy-edited.
Table 33: Summary of Patient Involvement Using the Guidance for Reporting Involvement of Patients and the Public (Version 2) Short Form Reporting Checklist42
Topic | Item | Section(s) |
|---|---|---|
Aim | To better understand the benefits and challenges of living with a voice prosthesis and the use of heat and moisture exchangers from the perspective of those with lived experience as a laryngectomee. | Key messages |
Methods | In December 2024 following feedback from external interested parties regarding our initial draft report we reached out to patient groups to better understand and gather insights from patients who had undergone a laryngectomy and are living with a voice prosthesis and heat and moisture exchangers. Three patients were identified through the Laryngectomee Association of British Columbia and accepted invitations to share their experiences. CDA-AMC Engagement staff offered all patients the opportunity to participate in a 30-minute introductory call to learn more about the details and context of the project, which 1 accepted (held on January 9, 2025). All 3 patients who had undergone a laryngectomy were provided a set of questions. Two patients opted for a 1-hour Zoom call (January 25), 1 of the patients interviewed also provided their written responses to the questions in addition to the call. One patient provided their written answers via email only. CDA-AMC offers a $100 gift card to select retailers as a gesture of thanks to patient participants. All patient contributors engaged in this project provided their consent for participating and all identified that they wanted to be publicly acknowledged by name in the report. | Methods |
Results of Engagement | Speaking to the patients helped to highlight when and why a device might work (or not) in 1 context and not another (for example, in extreme cold or hot weather, or living in rural and remote locations). The patient partner input also provided insights into important outcomes (i.e., communication, independence, and social engagement) and challenges of using the device, highlighting how the benefits outweigh the device’s limitations. It also helped to identify equity considerations, highlighting how the maintenance costs related to VP and HME as well as maintenance supplies was considered a barrier, particularly disadvantaging those with middle- or lower incomes. | Key messages, summary of finding |
Discussion and Conclusions | The insights and experience provided by patients who had undergone a laryngectomy was used to supplement the understanding of the impact of using a voice prostheses and heat and moisture exchangers following a laryngectomy. This opportunity to directly engage with someone with experience allowed the authors of our report to better understand the subject and contextualize the limited clinical and cost-effectiveness findings from the literature to provide a comprehensive picture of the benefits and challenges of using VP and HME devices for patients following a laryngectomy. Having a voice prosthesis and health moisture exchangers for patients following a laryngectomy is critical to their ability to live a fulfilled life, communicate with friends and family, maintain their independence, and prevent lung infection. While there are challenges with maintaining the devices and additional costs for the supplies needed, the benefits of these devices were seen to far outweigh these challenges. | Conclusion and implications |
Reflections and Critical Perspective | The patient contributors were highly engaged in their participation with Canada’s Drug Agency. Patient engagement occurred after the Rapid Review was complete, it did not influence the formulation of research questions or outcomes of interest, which may limit the relevance and applicability of the findings. All of the patients were supported by CDA-AMC Engagement Officers, and the interview was attended by 2 Engagement Officers. The introductory and engagement calls were scheduled at the patient’s convenience, and the patients were sent the questions in advance so that they could prepare. A choice of honorarium or gift card was offered as a gesture of thanks for their time and expertise. One limitation was our method. While our virtual approach enabled participation from individuals across Canada, the need for patients to have reliable technology and internet access to participate in a Zoom or telephone call potentially excluded some voices. Another limitation in our method would be that all the participating patients live in the same province (British Columbia). We did reach out to patient groups across Canada however we only received a response from 1 patient group based in British Columbia that were already aware of the project and keen to provide their perspective. | Limitations |
Appendix 6: List of Excluded Studies
Please note that this appendix has not been copy-edited.
Excluded for Single-Arm Primary Study
Heirman AN, Tellman RS, van der Molen L, et al. The acceptance and voice quality of a new voice prosthesis 'Vega High performance' - a feasibility study. Acta Otolaryngol. 2023;143(8):721-729. PubMed
Excluded for the Primary Study Already Included by at Least 1 Systematic Review
Ebersole B, Moran K, Gou J, et al. Heat and moisture exchanger cassettes: results of a quality/safety initiative to reduce postoperative mucus plugging after total laryngectomy. Head Neck. 2020;42(9):2453-2459. PubMed
Mayo-Yáñez M, Cabo-Varela I, Suanzes-Hernandez J, Calvo-Henriquez C, Chiesa-Estomba C, Herranz Gonzalez-Botas J. Use of double flange voice prosthesis for periprosthetic leakage in laryngectomised patients: a prospective case-crossover study. Clin Otolaryngol. 2020;45(3):389-393. PubMed
Petersen JF, Lansaat L, Timmermans AJ, van der Noort V, Hilgers FJM, van den Brekel MWM. Postlaryngectomy prosthetic voice rehabilitation outcomes in a consecutive cohort of 232 patients over a 13-year period. Head Neck. 2019;41(3):623-631. PubMed
Other Publications
Graville DJ, Palmer AD, Andersen PE, Cohen JI. Determining the efficacy and cost-effectiveness of the ActiValve: results of a long-term prospective trial. Laryngoscope. 2011;121(4):769-776. PubMed
Soolsma J, van den Brekel MW, Ackerstaff AH, Balm AJ, Tan B, Hilgers FJ. Long-term results of Provox ActiValve, solving the problem of frequent candida- and “underpressure”-related voice prosthesis replacements. Laryngoscope. 2008;118(2):252-257. PubMed
Retèl VP, van den Boer C, Steuten LM, Okla S, Hilgers FJ, van den Brekel MW. Cost-effectiveness of heat and moisture exchangers compared to usual care for pulmonary rehabilitation after total laryngectomy in Poland. Eur Arch Otorhinolaryngol. 2015;272(9):2381-2388. PubMed
van Sluis KE, van der Molen L, van Son R, Hilgers FJM, Bhairosing PA, van den Brekel MWM. Objective and subjective voice outcomes after total laryngectomy: a systematic review. Eur Arch Otorhinolaryngol. 2018;275(1):11-26. PubMed
ISSN: 2563-6596
Canada’s Drug Agency (CDA-AMC) is a pan-Canadian health organization. Created and funded by Canada’s federal, provincial, and territorial governments, we’re responsible for driving better coordination, alignment, and public value within Canada’s drug and health technology landscape. We provide Canada’s health system leaders with independent evidence and advice so they can make informed drug, health technology, and health system decisions, and we collaborate with national and international partners to enhance our collective impact.
Disclaimer: CDA-AMC has taken care to ensure that the information in this document was accurate, complete, and up to date when it was published, but does not make any guarantee to that effect. Your use of this information is subject to this disclaimer and the Terms of Use at cda-amc.ca.
The information in this document is made available for informational and educational purposes only and should not be used as a substitute for professional medical advice, the application of clinical judgment in respect of the care of a particular patient, or other professional judgments in any decision-making process. You assume full responsibility for the use of the information and rely on it at your own risk.
CDA-AMC does not endorse any information, drugs, therapies, treatments, products, processes, or services. The views and opinions of third parties published in this document do not necessarily reflect those of CDA-AMC. The copyright and other intellectual property rights in this document are owned by the Canadian Agency for Drugs and Technologies in Health (operating as CDA-AMC) and its licensors.
Questions or requests for information about this report can be directed to Requests@CDA-AMC.ca.