CADTH Health Technology Review
Care for Adults Following Laryngectomy
Rapid Review
Key Messages
What Is the Issue?
Total laryngectomy is a surgical procedure to remove the larynx which significantly impacts a patient's ability to swallow, breathe and speak, thereby having a great impact on their overall quality of life (QoL).
Voice rehabilitation or using a voice prosthesis are options for restoring voice communication in adults following total laryngectomy. However, prostheses are usually expensive and require self-care and/or regular visits to health care personnel to maintain function.
The effectiveness and health economic evaluation of using voice prostheses (indwelling and non-indwelling devices) and heat moisture exchangers for adults following laryngectomy is unclear.
What Did We Do?
To inform decisions on the appropriate use of voice prostheses (indwelling and non-indwelling devices) and heat moisture exchangers for adults following laryngectomy, Canada’s Drug Agency sought to identify and summarize related evidence or recommendations from clinical studies, health economic evaluations, and evidence-based guidelines.
We searched key resources, including journal citation databases, and conducted a focused grey literature search for relevant evidence published since January 2019.
What Did We Find?
One systematic review compared tracheoesophageal voice (TEV) using voice prostheses and esophageal voice (EV) and that meta-analysis revealed that the mean difference between the 2 groups was not statistically significant for voice handicap index (VHI) and voice-related QoL. The overall quality of evidence was assessed as very low.
One systematic review compared 10 voice prostheses (8 indwelling and 2 non-indwelling) and ranked these devices based on P-scores. This review did not compare indwelling and non-indwelling devices as 2 distinct groups. Most comparisons between various VPs showed no statistically significant differences in device replacements, device lifetime, airflow resistance, leakage, speech rate, maximum phonation time, patient device preference, phonatory effort, fundamental frequency, voice loudness, speech intelligibility, stoma stenosis, dislodgement, fistula problems, granulation, prosthesis inaccurate size, prosthesis deterioration, and survival rate.
One systematic review reported using heat moisture exchangers significantly reduced several clinical outcomes including mucus production, coughing, forced expectorations, the number of days requiring chest physiotherapy after surgery, tracheobronchitis or pneumonia episodes and improved patient satisfaction. There were no statistically significant differences between heat moisture exchangers and control groups in quality of life (QoL), sleep quality, speech quality, or social contacts.
No evidence regarding cost-effectiveness of voice prostheses versus no prostheses, indwelling versus non-indwelling prostheses, or comparisons among different non-indwelling prostheses for adults following laryngectomy was identified.
Heat moisture exchangers were reported as cost-effective compared to alternative stoma covers (ASC) from the US perspectives.
For laryngectomized patients with periprosthetic leakage, switching from Provox Vega to its modified versions (Provox XtraSeal or Provox ActiValve) was reported as cost-effective.
One evidence-based guideline recommended replacing the prosthesis with a double-flanged one, such as Provox XtraSeal, adjusting the diameter and length, or placing a silicone sheet on the tracheal side of the prosthesis can be used to manage periprosthetic leakage. This report did not identify any evidence-based guidelines regarding the use of heat moisture exchanger (HME) for adults following laryngectomy.
What Does it Mean?
Initial decisions regarding the choice of voice prostheses should consider patients’ values and preferences, accessibility, affordability, and other factors such as physical and mental capabilities, caregiver support, and patient motivation.
For laryngectomy patients experiencing periprosthetic leakage, it may be reasonable to switch to a modified version.
Adding heat moisture exchangers might be beneficial in several clinical outcomes, such as mucus reduction and reported patient satisfaction yet some studies reported similar scores in QoL, sleep quality, speech quality, and social contacts compared to no heat moisture exchangers.
Further high-quality research is necessary to confirm whether voice prostheses (indwelling or non-indwelling devices) or heat moisture exchangers can be routinely used for adults following laryngectomy.
Abbreviations
ASC
alternative stoma cover
BS-LP
Blom-Singer low pressure
CI
confidence interval
EH
external humidification
EV
esophageal voice
GRADE
grading of recommendations, assessment, development, and evaluations
HME
heat moisture exchanger
ICER
incremental cost-effectiveness ratio
SF-36
36-Item short form survey instrument
QALY
quality-adjusted life-year
QoL
quality of life
TEP
tracheoesophageal puncture
TEV
tracheoesophageal voice
VHI
voice handicap index
VP
voice prosthesis
VRQoL
voice-related quality of life
Context and Policy Issues
What Is a Laryngectomy and Care Following Laryngectomy?
Laryngectomy is a surgical procedure involving the partial or total removal of the larynx, it is commonly performed to treat locoregionally advanced laryngeal and hypopharyngeal cancers.1,2 Total laryngectomy is often indicated for advanced squamous cell carcinomas of the larynx or hypopharynx that have not metastasized distantly.2,3 The total laryngectomy procedure impacts the patient's ability to swallow, breathe, speak and necessitates breathing through an opening stoma after the larynx is removed and creating a need for specialized postsurgical care and rehabilitation to restore essential functions.4,5
Care following laryngectomy involves comprehensive interventions that include olfactory, voice, swallowing rehabilitation and addressing the psychosocial aspects of patient recovery.6-8 For patients who have undergone laryngectomy surgery, interdisciplinary collaboration and personalized care plans are essential to optimize outcomes and improve the QoL.6,7 Voice or speech rehabilitation is an important aspect of care following laryngectomy to restore vocal communication. Ensuring sufficient localized heat and moisture, often with heat and moisture exchangers, can support improved patient outcomes.
What Are Commonly Used Approaches for Voice Restoration?
The commonly used approaches to restore voice and communication include the artificial larynx (electrolarynx), TEV restoration, and esophageal speech.9 The electrolarynx is a widely used, battery-powered device used for speech, offering immediate communication. However, it has a mechanical sound and typically requires one-hand operation. Esophageal speech, the traditional method, involves introducing and expelling air from the esophagus to produce sound. It is advantageous for hands-free verbal communication without any devices and closer to natural laryngeal vibrations but is difficult to learn, with less than 30% of patients using it as their primary communication method. Tracheoesophageal (TE) voice restoration, either performed during (primary tracheoesophageal puncture, TEP) or after (secondary TEP) laryngectomy, provides the most comparable speech alternative to natural, fluent speech and ease of production.9
What Are Voice Prostheses and Heat And Moisture Exchangers?
A voice prosthesis is a small medical device that incorporates a one-way valve, allowing patients to produce sounds by directing air from their lungs, through the valve, and into their mouth. Typically, the voice prosthesis is placed in a surgically created fistula in the tracheoesophageal wall. Speakers can move air from the trachea into the pharyngoesophageal either by manually obstructing the stoma or by using a tracheostoma breathing valve. Subsequently, the movement of oral cavity structures shapes the sound into words for speech production.9
Voice prostheses can be classified as either indwelling or non-indwelling based on whether they can be removed and managed by the patient. Non-indwelling prostheses are removable by the patient and can be changed but this requires the stoma to be easily accessible and the patient to have sufficient eyesight and dexterity to remove and reinsert the device.10 Indwelling prostheses are exclusively changed by health care professionals (e.g., physician or speech-language pathologist) and often have a longer lifespan than non-indwelling prostheses.9,10
HME devices were introduced in the total laryngectomy in the 1990s. It helps compensate for the loss of the upper airway's natural humidifying and filtering functions, which are compromised after laryngectomy. HMEs have been shown to improve pulmonary function, reduce respiratory symptoms, and enhance overall QoL compared with the conventional external humidification (EH) system.11
Why Is it Important To Do This Review?
Given the complexities of care following laryngectomy and voice restoration, there is a need to evaluate the clinical- and cost-effectiveness of these interventions or devices to ensure optimal outcomes for patients. The effectiveness, health economic evaluations, and recommendations from evidence-based guidelines regarding the use of voice prostheses (indwelling and non-indwelling devices) and HMEs for adults following laryngectomy remain unclear. For instance, a previous review indicated that the effectiveness and lifespan of different indwelling voice prostheses for adults following laryngectomy had inconsistent results and did not identify any cost-effectiveness studies or clinical practice guidelines.10
Objective
This review aimed to provide a foundation for evidence-based decision-making regarding the clinical effectiveness and cost-effectiveness of voice prostheses (indwelling and non-indwelling devices) and HMEs for adults following laryngectomy. This review also summarized the related guideline recommendations available for this patient population.
Research Questions
What is the clinical effectiveness of voice prostheses versus no voice prostheses for adults following laryngectomy?
What is the clinical effectiveness of indwelling and non-indwelling voice prostheses for adults following laryngectomy?
What is the clinical effectiveness of heat and moisture exchanger for adults following laryngectomy?
What is the cost-effectiveness of voice prostheses versus no voice prostheses for adults following laryngectomy?
What is the cost-effectiveness of indwelling and non-indwelling voice prostheses for adults following laryngectomy?
What is the cost-effectiveness of heat and moisture exchanger for adults following laryngectomy?
What are the evidence-based guidelines regarding the use of voice prostheses or heat and moisture exchanger for adults following laryngectomy?
Methods
An information specialist conducted a customized literature search, balancing comprehensiveness with relevancy, of multiple sources and grey literature on July 18, 2024. One reviewer screened citations and selected studies based on the inclusion criteria presented in Table 1.
Appendix 1 presents a detailed description of methods.
Criteria | Description |
|---|---|
Population | Adults following laryngectomy |
Intervention | Q1, Q2,Q4,Q5,and Q7: Voice prostheses including:
Q3,Q6,and Q7: Heat and moisture exchanger, with or without voice prostheses |
Comparator | Q1 and Q4: No voice prostheses Q2 and Q5: Compared to indwelling or non-indwelling voice prostheses types, inclusive of the following comparisons:
Q3 and Q6: No heat and moisture exchanger Q7: NA |
Outcomes | Q1 to Q3: Clinical benefits and harms (e.g., quality of life, patient satisfaction, depression, anxiety, self-esteem changes, device lifespan, safety) Q4 to Q6: Cost-effectiveness (e.g., cost per QALY gained, ICER) Q7: Recommendations regarding the use of voice prostheses (indwelling or non-indwelling) and heat moisture exchangers |
Study designs | Health technology assessments, systematic reviews, randomized controlled trials, nonrandomized studies, economic evaluations, evidence-based guidelines |
Exclusion criteria | Articles focused on alternatives to voice prostheses (e.g., electrolarynx) |
Publication date | Since January 1, 2019 |
Summary of Evidence
Quantity of Research Available
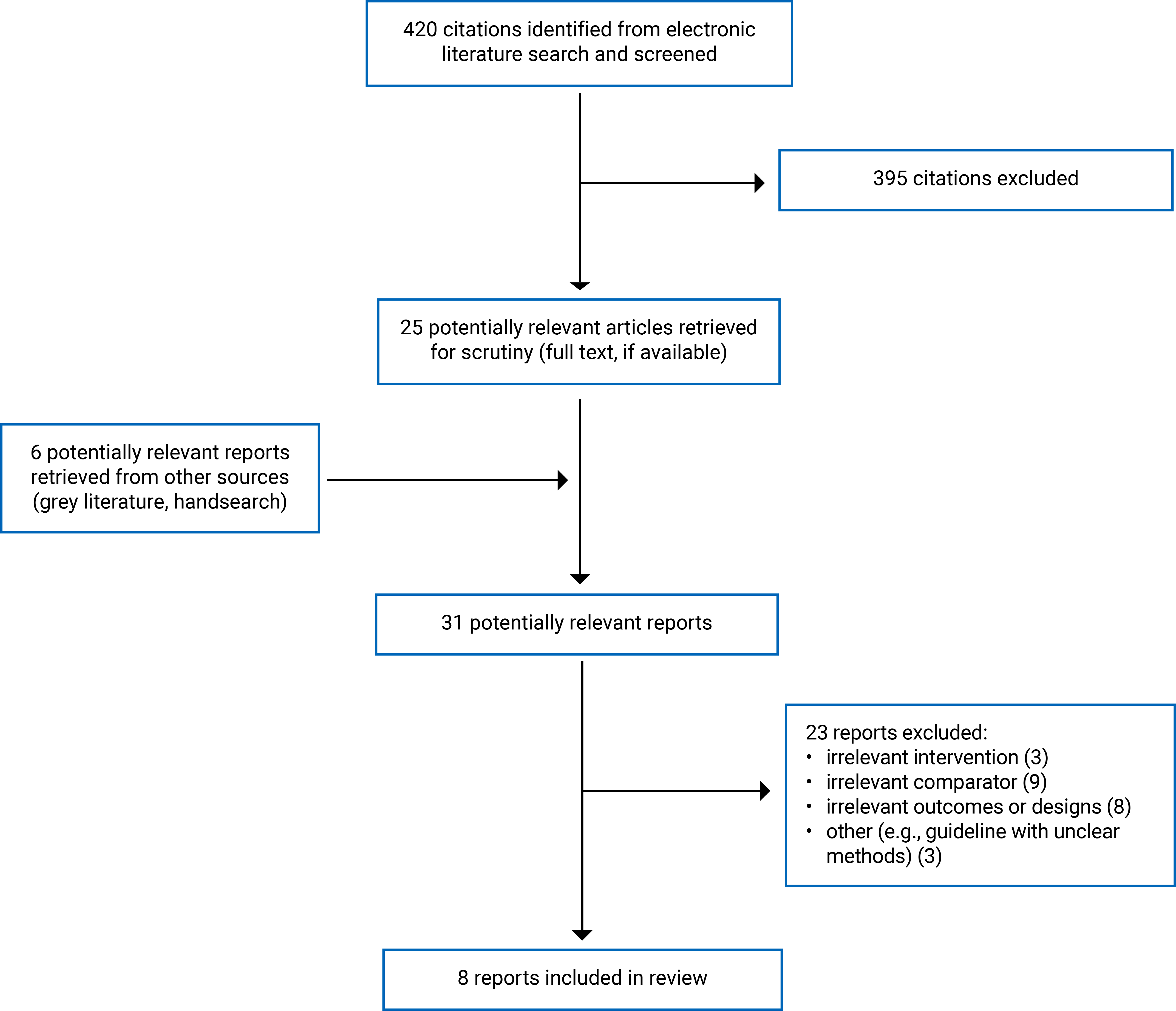
This review includes 8 publications, including 4 systematic reviews,12-15 3 economic evaluations,16-18 and 1 evidence-based guideline.19 Figure 1 (Appendix 1) presents the PRISMA20 flow chart of the study selection. Appendix 5 presents additional references of potential interest that were excluded due to single-arm design or because they were already included in at least 1 eligible systematic review.
Summary of Study Characteristics
Research Question 1: the clinical effectiveness of voice prostheses versus no voice prostheses for adults following laryngectomy
This review included 1 systematic review12 that compared the effectiveness of tracheoesophageal voice (TEV) rehabilitation using VP versus EV without VP. The systematic review conducted in Belgium, examined 15 observational studies (11 retrospective controlled studies and 4 uncontrolled retrospective studies) involving 1,085 patients who had undergone total laryngectomy for advanced laryngeal cancer. Most of the participants were male (89.38%), with a mean age of 65.38 years. The intervention group (TEV) consisted of 869 patients who received voice prosthesis rehabilitation (80.1%), while 216 patients (19.9%) were treated with EV. The clinical outcomes assessed included the VHI, Voice-Related Quality of Life (VRQoL), and the 36-Item short form survey instrument (SF-36). The duration of disease, details on radiotherapy, and the length of follow-up were not reported.12
Research Question 2: the clinical effectiveness of indwelling and non-indwelling voice prostheses for adults following laryngectomy
This review included 2 systematic reviews14,15 that compared the effectiveness of different voice protheses on clinical outcomes. One systematic review14 was conducted in Spain and included 4 observational involving 55 laryngectomy patients (87.27% male, mean age 62.71 years) who used VP. The studies compared the Provox Vega XtraSeal (PVX) prosthesis (n = 94) to control VPs (Vega and ActiValve Light, n = 221) and focused on VP duration.
The second systematic review with network meta-analysis (NMA)15 was conducted in Egypt and Japan, including 120 studies with 11,918 laryngectomy patients (71.7% male, aged 17 to 90 years) from 30 countries, including the US, UK, and Canada. The analysis evaluated 10 VPs that includes 8 indwelling prostheses [Provox-1, Provox-2, Provox ActiValve (AV), Provox Vega, Sound-Producing Voice Prosthesis (SPVP), Nijdam, Groningen Low Resistance, Groningen Ultra Low Resistance] and 2 non-indwelling prosthesis [Provox non-indwelling device (NID) and Blom-Singer low pressure (BS-LP)] on multiple clinical outcomes, such as VP replacement, VP duration, airflow resistance, leakage rates, and patient device preference, with follow-up durations ranging from 0.5 to 133 months. This systematic review also evaluated use of HMEs in the NMA and compared different VPs to HMEs for some outcomes.15 It is unclear whether the VP arm without any HME was included, and these comparisons were not the primary outcomes of the systematic review.15 The results related to the comparisons of HMEs were not included in this report.
Research Question 3: the clinical effectiveness of heat and moisture exchanger for adults following laryngectomy
This review included 1 mixed-methods study13 that included a rapid review that compared the effectiveness of HMEs compared to no HME use or external humidifier. This review was conducted in the Netherlands and funded by Atos Medical. The review included 10 studies comprising 3 RCTs, 3 time-series studies, 1 retrospective cohort study, and 1 study with an unclear design, from the US, Canada, France, Italy, Spain, the Netherlands, and Poland. The review included 550 patients who underwent total laryngectomy, age and sex data were not reported. The intervention involved the use of HMEs, compared to no HME use, an external humidifier or another HME. This report only summarized the comparisons between HMEs compared to no HME use or external humidifier. The review summarized several clinical outcomes including mucus production, coughing, forced expectorations, the number of days requiring chest physiotherapy after surgery, tracheobronchitis or pneumonia episodes, patient satisfaction, QoL, sleep quality, speech quality, and social contacts. The follow-up duration for these outcomes was either 3 months or not reported.
Research Question 4: the cost-effectiveness of voice prostheses versus no voice prostheses for adults following laryngectomy
No eligible studies were identified.
Research Question 5: the cost-effectiveness of indwelling and non-indwelling voice prostheses for adults following laryngectomy
This review included 2 cost-effectiveness studies compared a regular indwelling VP (Provox Vega) and its modified versions designed to prevent leakage (Provox XtraSeal and Provox ActiValve). One study compared the cost-effectiveness of Provox Vega against the Provox XtraSeal. The study used data on 551 VPs (483 Provox Vega, 68 Provox XtraSeal) from 38 patients (35 men, 3 women) with a mean age of 66 from 2015 to 2023. The incremental cost-effectiveness ratio (ICER) was calculated from the Spanish National Health System's perspective, based on the difference in costs and the number of annual prosthesis replacements. The other study compared the Provox Vega to the Provox ActiValve, which features a magnet-based valve to prevent leakage. The study included 159 VPs (150 Provox Vega, 9 Provox ActiValve) from 5 Caucasian men with a mean age of 64. The ICER was calculated based on the number of annual prosthesis replacements during the observational study from the perspective of the Spanish Public National Health System.
Research Question 6: the cost-effectiveness of heat and moisture exchanger for adults following laryngectomy
This review included 1 study that compared cost-effectiveness of HMEs versus alternative stoma covers (ASC) in patients after laryngectomy at a clinic in Massachusetts, US. The study, conducted from September to December 2018, included 40 HME users and 22 ASC users, mostly male (47 of 66). QoL data were collected via a study specific questionnaire and the utility index scores were derived using the EuroQol five-dimensional questionnaire (EQ-5D-5L) and the US tariff. A Markov model calculated the ICER by dividing the total cost difference by the difference in quality-adjusted life-years (QALYs) from a US health care and societal perspective.
Research Question 7: the evidence-based guidelines regarding the use of voice prostheses or heat and moisture exchanger for adults following laryngectomy
This review included 1 evidence-based guideline that provided the recommendation regarding the use of voice prostheses for adults following laryngectomy in managing the periprosthetic leakage. The guideline was developed in Spain aimed at health care professionals, including otorhinolaryngology specialists, speech therapists, nursing staff, and other specialists, with a focus on laryngectomized patients. The evidence was collected and synthesized through a systematic review of 91 studies on primary or secondary TEP (which does not address the same research questions as the current report), assessed using the Oxford Levels of Evidence system (2011), ranging from level 1a (systematic reviews of RCTs) to level 5 (mechanism-based reasoning). The guideline development group reviewed recent research on benefits, side effects, and risks to make recommendations with a grade of recommendation (B or C), however, the meaning of these recommendation grades was not specified.
Appendix 2 presents additional characteristics of the included studies.
Summary of Critical Appraisal
Systematic Reviews
In all included systematic reviews,12-15 the objective was clearly described, keywords of the search strategies, and study selection process were provided. Three systematic reviews conducted a search in multiple databases.12,14,15 One systematic review13 only searched PubMed and 3 systematic reviews12-14 did not report searching the Embase database. Only 1 systematic review reported performing a grey literature search.15 No systematic review provided the list of excluded studies. These limitations may result in missing some eligible studies.
At least 2 reviewers independently performed or verified the article selection and data extraction in 2 systematic reviews.13,15 Two reviewers independently conducted data extraction in 1 systematic review, but it was unclear how the article selection was performed.14 In 1 systematic review, it was unclear how article selection and data extraction were conducted.12 The possibility of inappropriate inclusion or exclusion or errors in data extraction cannot be ruled out.
Three systematic reviews12,14,15 assessed the risk of bias of included individual studies and reported study quality, however, 1 systematic review did not assess the risk of bias of included studies.13 No systematic reviews explored the potential impact of risk of bias on result interpretations. The findings of these systematic reviews may be driven by studies with high risk of bias. One systematic review12 assessed the quality of evidence using the GRADE framework, the details of the GRADE assessment were unclear and did not adhere completely to the GRADE principles as it started the certainty of evidence at very low for evidence from observational studies and did not assess the certainty of evidence at each outcome level. The accuracy of the overall quality evidence was uncertain and difficult to interpret in this review.
One systematic review15 conducted a frequentist network meta-analysis (NMA) comparing 10 VPs: Provox-1, Provox-2, Provox AV, Provox Vega, SPVP, Nijdam, Groningen Low Resistance, Groningen Ultra Low Resistance, Provox NID, and BS-LP. The NMA presented a range of results, including network plots, point estimates, 95% confidence intervals, and P-scores. Intervention rankings were based solely on P-scores without considering the results of statistical tests or the certainty of the evidence. This approach means that VPs with top rankings may have low-certainty evidence or may not show statistically significant differences compared to other VPs. Additionally, the inclusion of nonrandomized studies in the NMA could have introduced bias. We also compared the registered systematic review protocol in PROSPERO (CRD42017080110) with the published reviews and identified several discrepancies. For instance, the protocol specified the inclusion of only RCTs, but the published review also included observational studies. Additionally, while the protocol focused solely on VPs, the review incorporated the HME devices in the NMA for certain outcomes, such as patient preference. The authors did not address these deviations between the review protocol and their actual work, which may result in potential publication bias.
Evidence-Based Guidelines
The included evidence-based guidelines had clear objectives, guideline questions, and target populations (e.g., patients undergoing total laryngectomy).19 The guideline development group searched multiple databased (MEDLINE, Embase, Scopus, Web of Science, PubMed, Science Citation Index, and the Cochrane Library) for relevant evidence and then achieved consensus to formulate recommendations.19 The guideline panel included otolaryngologists, head and neck surgeons, and expert speech therapists.19 However, it is uncertain whether at least 1 methodology expert was involved in the development of the guideline and whether the perspectives or preferences of the target populations were sought or had an influence on the recommendations. Therefore, the recommendations may not adequately reflect the values and preferences of patients or other partners.
The guideline19 proposed using either B or C for the grade of recommendations; the meaning of recommendation grades was not specified, limiting the interpretation of the recommendations. The links between the recommendations and the supporting evidence were unclear. All guideline authors disclosed no competing interests. The guideline was funded by the Atos Medical and 1 author of the guideline was an employee of Atos Medical which potentially impacts the interval validity of the guideline. The included guideline discussed the potential facilitators to implementing some recommendations and considered some cost-effective evidence.19 The guideline did not discuss the related barriers regarding the use of VP, such as accessibility and affordability for the VP, which could be a barrier to implementing related recommendations.
Cost-Effectiveness Studies
All cost-effectiveness studies clearly defined their research questions, study design, data collection parameters, outcome measures, analysis perspectives, and rationale for selecting the study alternatives. The rationale for the chosen form of economic analysis could have been further elaborated. Each study's effectiveness measures were derived from a single prospective study with small patient samples (5 or 38 VP users, 40 HME users, 22 ASC users).
Two studies focused on the cost-effectiveness of different indwelling VPs based on crossover studies. These studies involved Provox Vega users who experienced 3 or more consecutive changes due to periprosthesis leakage, which affected the prosthesis's theoretical lifespan. The patients then switched from the Provox Vega to its alternatives (Provox XtraSeal or Provox ActiValve). This transition introduced variability in the background care, or surgical interventions received, making comparisons between the devices less consistent. Both studies also lacked details on currency adjustments for inflation or conversion and did not include sensitivity analyses. These studies were conducted from the payer’s perspective within the Spanish National Health System, their findings may not be applicable to the Canadian health care system.
One study provided a comprehensive economic evaluation, justifying its choice of economic model, clearly defining effectiveness estimates and outcome measures, and including appropriate sensitivity analyses. This study was conducted from both a US health care and societal perspectives and findings may not be generalizable to the context in Canada due to differences in health care systems.
Appendix 3 provides additional details regarding the strengths and limitations of included publications.
Summary of Findings
This report has summarized the effectiveness, cost-effectiveness and evidence-based recommendations regarding the use of VPs and HMEs based on 8 eligible publications. Appendix 3 presents the summary of findings by different outcomes and clinical questions.
Research Question 1: Clinical effectiveness of voice prostheses versus no voice prostheses for adults following laryngectomy
VHI (1 systematic review)
One systematic review evaluated the effectiveness of TEV compared to EV in improving VHI
TEV group demonstrated a statistically significant improvement in VHI than the EV group based on the mean scores.12
The meta-analysis using random-effect models indicated that the mean differences in VHI between the 2 groups was not statistically significant.12
VRQoL (1 systematic review)
One systematic review evaluated the effectiveness of TEV compared to EV in improving VRQOL.
TEV group showed a nonstatistically significant difference compared to the EV group based on the mean scores.12
The meta-analysis using random-effect models also indicated that the mean differences between the 2 groups was not statistically significant.12
SF-36 (1 systematic review)
One systematic review12 evaluated the effectiveness of TEV compared to EV in improving SF-36.
TEV demonstrated a statistically significant better improvement in SF-36 compared to the EV group based on the mean scores, but the TEV group had a lower SF-36 score than the EV group.12
The meta-analysis did not provide a comparison between the 2 groups on SF-36.12
Research Question 2: Clinical effectiveness of indwelling and non-indwelling voice prostheses for adults following laryngectomy
Comparisons Among 10 VPs (8 indwelling and 2 non-indwelling)
One systematic review and NMA15 compared the effectiveness of 10 VPs (8 indwelling and 2 non-indwelling devices): Provox-1, Provox-2, Provox AV, Provox Vega, SPVP, Nijdam, Groningen Low Resistance, Groningen Ultra Low Resistance, Provox NID, and BS-LP. The review ranked VPs based on P-scores across 18 clinical outcomes. However, the effect sizes for most comparisons between different VPs were not statistically significant across the majority of clinical outcomes.15
The systematic review also reported on the cost of VPs based on 3 studies, which showed significant variation across different VPs. It reported that Provox AV and Provox-2 were the most expensive devices, while BS-LP was the least expensive according to a single study. However, it is unclear which VPs were included for comparison on cost.
PVX Compared to Control VP (vega and ActiValve light)
One systematic review14 compared the lifespan of PVX and control voice prostheses (Vega and ActiValve Light) and reported that PVX had a numerically longer mean lifespan than the control VPs. However, the review did not perform statistical tests to compare the 2 groups, and the 95% confidence intervals overlapped.
Research Question 3: Clinical effectiveness of heat and moisture exchanger for adults following laryngectomy
One systematic review13 evaluated the effectiveness of HMEs compared to non-HME or external humidification (EH) on various outcomes.
HMEs were reported to statistically reduce various outcomes:13
mucus production
coughing
forced expectorations
the number of days requiring chest physiotherapy after surgery
tracheobronchitis or pneumonia episodes
HMEs were reported to statistically improve patient satisfaction.13
The difference between HME and control (non-HME or external humidifier) are not statistically significant in the following outcomes:13
QoL
Sleep Quality
Speech Quality
Social contacts.
Research Question 4: Cost-Effectiveness of voice prostheses versus no voice prostheses for adults following
No cost-effectiveness evidence was identified comparing the cost-effectiveness of voice prostheses versus no voice prostheses for adults following laryngectomy; therefore, no summary can be provided.
Research Question 5: Cost-effectiveness of indwelling and non-indwelling voice prostheses for adults following laryngectomy
This review included 2 cost-effectiveness studies compared a regular indwelling VP (Provox Vega®) and its modified versions for laryngectomized patients experiencing periprosthetic leakage with Provox Vega:16,17
Switching to Provox XtraSeal is cost-effective if the cost of Provox XtraSeal remains below EUR 551.63.16
ICER (EUR/Effectiveness): −0.01
Lower cost scenario: EUR −291.80
Higher cost scenario: EUR 93.07
Switching to Provox ActiValve is also cost-effective:17
ICER (EUR/Effectiveness): −133.97.
No evidence was found comparing the cost-effectiveness of indwelling versus non-indwelling voice prostheses, nor between different non-indwelling VPs for adults following laryngectomy.
Research Question 6: Cost-effectiveness of heat and moisture exchanger for adults following laryngectomy
This review included 1 study18 compared cost-effectiveness of HMEs versus ASCs in patients after laryngectomy from the US health care and societal perspective. The study found that HME use is cost-effective compared to ASCs:18
QALYs were slightly higher for HME users compared to ASCs.
Total lifetime costs per patients were higher for ASCs users compared to HME users.
ICER (US $/QALY): health care perspective: −11,833; societal perspective: −306,551.
Annual budget saving (US $): health care perspective: 1,551,083; societal perspective: 40,183,593.
Research Question 7: Evidence-based guideline recommendations regarding the use of voice prostheses or heat and moisture exchanger for adults following laryngectomy
We identified 1 evidence-based guideline19 that recommended the use of VPs in adults following laryngectomy to manage periprosthetic leakage. The guideline recommended replacing the prosthesis with a double-flanged one, such as PVX, or adjusting the diameter and length, or placing a silicone sheet on the tracheal side of the prosthesis. It also mentioned that the Blom-Singer large esophageal and tracheal flange VP is a useful solution for managing periprosthetic leakage. However, the guideline did not provide clear recommendations regarding the initial use of VPs.
No evidence-based guideline regarding the use of HME for adults following laryngectomy was identified; therefore, no summary can be provided.
Limitations
Although this report included 4 systematic reviews12-15 addressing the clinical effectiveness of VPs compared to no VPs or another alternative VP and considering many primary studies, these systematic reviews had various methodological limitations and did not address the same research questions as the current report; methodological limitations are present in the body of evidence presented which are outlined in the critical appraisal section. It is worth emphasizing that the results reported in the systematic review and NMA of 120 studies relies on P-scores and disregards comparative statistical test results, and the certainty of evidence; their results on the rankings were misleading.15 All these reviews12-15 included mainly observational studies, with a small number of RCTs. Therefore, the body of evidence may be influenced from selection bias, recall bias, or performance bias that skews findings.
Reporting of evidence is consistently unclear across the included evidence, as well as heterogeneity and inconsistency or discrepancies is evident in some reported is present. For example, 1 review12 compared the TEV using VPs to the EV on QoL outcomes yet failed to report the timing of outcome measures, which is a crucial consideration. Although the pooled mean score in VHI favoured the VP group, the meta-analysis did not find statistical significance.12 None of the included systematic reviews reported the funding sources of individual studies, raising concerns about potential publication bias. In addition, 1 systematic review12 did find substantial heterogeneity, they did not conduct a thorough assessment of the potential explanations for the heterogeneity, such as through subgroup analysis. Therefore, the observed pooled treatment effects may not be entirely reliable, and the interpretations of evidence were limited.
This review identified evidence gaps as no high-quality systematic reviews that directly address our research questions were available. There was no evidence on the cost-effectiveness of voice prostheses versus no prostheses, indwelling versus non-indwelling prostheses, or comparisons among different non-indwelling prostheses for adults following laryngectomy. The included economic evaluation studies conducted from the perspectives of the US and Spanish National Health System.16-18 No evidence-based guidelines or economic evaluations were identified focused on the context in Canada. The included guidelines were conducted in Spain,19 and no guideline authors were from institutions in Canada, as such, the generalizability of the findings to settings in Canada was unclear.
Conclusions and Implications for Decision- or Policy-Making
This review summarizes evidence on the effectiveness and cost-effectiveness of VPs and HMEs for adults following laryngectomy. Four systematic reviews,13-15 3 cost-effectiveness studies,16-18 and 1 evidence-based guideline19 were identified to answer these research questions. No evidence of cost-effectiveness of voice prostheses versus no prostheses, indwelling versus non-indwelling prostheses, or comparisons among different non-indwelling prostheses for adults following laryngectomy was identified. No evidence-based guidelines regarding the use of HME for adults following laryngectomy was identified.
VPs Versus no VPs: TEV Versus EV
This report identified 1 systematic review12 to answer this research question. Despite the statistically significant improvement in VHI and SF-36 mean scores for the TEV group using VPs compared to the EV group, the meta-analysis revealed that the mean difference between the 2 groups was not statistically significant for VHI and unavailable for SF-36.12 The study found no significant difference in VRQOL between the 2 groups.12
Indwelling and Non-Indwelling VPs
One systematic review and NMA of RCTs and observational studies,15 reported that the effect sizes for most comparisons between various voice prostheses (8 indwelling VPs and 2 non-indwelling VPs) were not statistically significant for the majority of clinical outcomes. The systematic review concluded that the best VP is Provox-2, the second best is Provox 1, and Groningen low resistance and Nijdam were identified as the least effective devices based on P-scores.15 The systematic review also reported that Provox AV and Provox-2 were the most expensive devices, while BS-LP was the least expensive, according to a single study.15 One systematic review reported that PVX had a numerically longer mean lifespan than the control VPs (Vega and ActiValve Light).14
HME Versus no HME
One systematic review13 reported that HMEs statistically reduce mucus production, coughing, forced expectorations, the number of days requiring chest physiotherapy after surgery, tracheobronchitis or pneumonia episodes and improve patient satisfaction. However, the difference between HME and control is not statistically significant in QoL, sleep or speech quality or social contacts.
Cost-Effectiveness of Indwelling VPs and HMEs
Based on 2 cost-effectiveness studies,16,17 it can be concluded that laryngectomized patients experiencing periprosthetic leakage with Provox Vega who switched to its modified versions (Provox XtraSeal or Provox ActiValve) was cost-effective. Based on 1 cost-effectiveness study,18 it was reported that the use of HME is cost-effective compared to ASCs.
Evidence-Based Recommendations Regarding the Use of VPs
One evidence-based guideline19 recommended replacing the prosthesis with a double-flanged one, such as PVX, adjusting the diameter and length, or placing a silicone sheet on the tracheal side of the prosthesis to manage periprosthetic leakage.
Considerations for Future Research
Future systematic reviews should prioritize appropriate methods and focus on RCTs. High-quality systematic reviews addressing the specific research questions in this report are necessary for decision-making. Further research is needed to fill the identified research gaps, the cost-effectiveness of voice prostheses versus no prostheses, indwelling versus non-indwelling prostheses, or comparisons among different non-indwelling prostheses for adults following laryngectomy to support optimal patient care. Future primary studies should have robust designs, adequate sample sizes and pro-active strategies to minimize selection bias. Future cost-effectiveness analyses should include sensitivity analyses to test the robustness of their findings. Any future evidence-based guidelines should involve patient partners or panel members from Canada to enhance the generalizability of recommendations to the context in Canada.
Implications for Clinical Practice
Based on low or very low-certainty evidence, TEV may have similar effectiveness to EV on QoL measures, and the effectiveness of these VPs is comparable across most clinical outcomes. Initial decisions regarding the choice of VPs should consider values and preferences, accessibility, and affordability. Other factors influencing the decision to use a VP or select a specific type include anatomic status, physical and mental capabilities, level of independent functioning, caregiver support, and patient motivation.9
For laryngectomy patients experiencing periprosthetic leakage with Provox Vega, it may be reasonable to switch to a modified version, such as Provox XtraSeal or Provox ActiValve, to prevent further leakage. Alternatively, clinicians or patients can manage leakage by adjusting the prosthesis's diameter and length or placing a silicone sheet on the tracheal side of the prosthesis.
HMEs significantly improve several clinical outcomes, except for QoL, sleep quality, speech quality, and social contacts, based on 1 systematic review. HMEs were cost-effective compared to ASCs from the US perspective. Clinicians and policy-makers should consider the local context and engage with potential HME users to make personalized decisions regarding HME use.
References
1.Crosetti E, Fantini M, Bertotto I, et al. Current Status of partial laryngeal surgery for advanced laryngeal cancer: when and why? Curr Oncol Rep. 2024;26(6):614-624. PubMed
2.Hans S, Baudouin R, Circiu MP, et al. One hundred fifty years of total laryngectomies. Front Oncol. 2024;14:1351549. PubMed
3.Hoffmann TK. Total laryngectomy-still cutting-edge? Cancers (Basel). 2021;13(6). PubMed
4.Babin E, Blanchard D, Hitier M. Management of total laryngectomy patients over time: from the consultation announcing the diagnosis to long term follow-up. Eur Arch Otorhinolaryngol. 2011;268(10):1407-1419. PubMed
5.Brisson-McKenna M, Jefferson GD, Siddiqui SH, et al. Swallowing function after treatment of laryngeal cancer. Otolaryngol Clin North Am. 2023;56(2):371-388. PubMed
6.Rosa VM, Fores JML, da Silva EPF, et al. Interdisciplinary interventions in the perioperative rehabilitation of total laryngectomy: an integrative review. Clinics. 2018;73(suppl 1):e484s. PubMed
7.Sharpe G, Camoes Costa V, Doubé W, Sita J, McCarthy C, Carding P. Communication changes with laryngectomy and impact on quality of life: a review. Qual Life Res. 2019;28:863-877. PubMed
8.Öztürk A, Mollaoğlu M. Determination of problems in patients with post-laryngectomy. Scand J Psychol. 2013;54(2):107-111. PubMed
9.Lewin JS, Hoffman HT, Sperry SM. Alaryngeal speech rehabilitation In: Post TW, ed. UpToDate. Waltham (MA): UpToDate; 2024: http://www.uptodate.com/. Accessed 2024 Jul 17.
10.Wells C, Adcock L. Indwelling voice prostheses for adults following laryngectomy: a review of clinical effectiveness, cost-effectiveness, and guidelines. (CADTH Rapid response report: summary with critical appraisal). Ottawa (ON): CADTH; 2017.
11.Kearney A, Norris K, Bertelsen C, et al. Adoption and utilization of Heat and Moisture Exchangers (HMEs) in the tracheostomy patient. Otolaryngol Head Neck Surg. 2023;169(5):1374-1381. PubMed
12.Maniaci A, Lechien JR, Caruso S, et al. Voice-related quality of life after total laryngectomy: systematic review and meta-analysis. J Voice. 2024;38(2):539.e511-539.e519. PubMed
13.Ahmed A, Mewes JC, Boot IWA, Vrijhoef HJM. New heat and moisture exchangers for laryngectomized patients in Germany: mixed- methods study on the expected effectiveness. JMIR Form Res. 2023;7:e36401. PubMed
14.Mayo-Yanez M, Cabo-Varela I, Calvo-Henriquez C, Chiesa-Estomba C, Herranz Gonzalez-Botas J. Prevention of periprosthetic leakage with double flange voice prosthesis: a systematic review and management protocol proposal. Logoped Phoniatr Vocol. 2023;48(3):129-136. PubMed
15.Tawfik GM, Makram OM, Zayan AH, et al. Voice rehabilitation by voice prostheses after total laryngectomy: a systematic review and network meta-analysis for 11,918 patients. J Pers Med. 2021;64(7):2668-2681. PubMed
16.Rodriguez-Lorenzana P, Mayo-Yanez M, Chiesa-Estomba CM, et al. Cost-effectiveness study of double-flange voice prostheses in the treatment of periprosthetic leakage in laryngectomized patients. J Pers Med. 2023;13(7):29. PubMed
17.Mayo-Yanez M, Chiesa-Estomba C, Lechien JR, Calvo-Henriquez C, Vaira LA, Cabo-Varela I. Long-term outcomes and cost-effectiveness of a magnet-based valve voice prosthesis for endoprosthesis leakage treatment. Eur Arch Otorhinolaryngol. 2022;279(8):4167-4172. PubMed
18.Beck ACC, Retel VP, Bunting G, et al. Cost-effectiveness analysis of using the heat and moisture exchangers compared with alternative stoma covers in laryngectomy rehabilitation: US perspective. Head Neck. 2020;42(12):3720-3734. PubMed
19.Mayo-Yanez M, Klein-Rodriguez A, Lopez-Eiroa A, Cabo-Varela I, Rivera-Rivera R, Parente-Arias P. Evidence-based recommendations in primary tracheoesophageal puncture for voice prosthesis rehabilitation. Healthcare (Basel). 2024;12(6):14. PubMed
20.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
21.Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. PubMed
22.Jansen JP, Trikalinos T, Cappelleri JC, et al. Indirect treatment comparison/network meta-analysis study questionnaire to assess relevance and credibility to inform health care decision making: an ISPOR-AMCP-NPC Good Practice Task Force report. Value Health. 2014;17(2):157-173. PubMed
23.Higgins JPT, Green S, editors. Figure 15.5.a: Drummond checklist (Drummond 1996). Cochrane handbook for systematic reviews of interventions. London (GB): The Cochrane Collaboration; 2011: http://handbook-5-1.cochrane.org/chapter_15/figure_15_5_a_drummond_checklist_drummond_1996.htm. Accessed 2024 Jul 11.
24.Agree Next Steps C. The AGREE II Instrument. Hamilton (ON): AGREE Enterprise; 2017: https://www.agreetrust.org/wp-content/uploads/2017/12/AGREE-II-Users-Manual-and-23-item-Instrument-2009-Update-2017.pdf. Accessed 2024 Jul 11.
Appendix 1: Detailed Methods and Selection of Included Studies
Please note that this appendix has not been copy-edited.
Literature Search Methods
An information specialist conducted a literature search on key resources including MEDLINE, the Cochrane Database of Systematic Reviews, the International HTA Database, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search approach was customized to retrieve a limited set of results, balancing comprehensiveness with relevancy. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. Search concepts were developed based on the elements of the research questions and selection criteria. The main search concepts were voice protheses and laryngectomy. A supplemental search was conducted with search filters applied to limit retrieval to guidelines. The search was completed on July 18, 2024 and limited to English-language documents published since January 1, 2019.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1. Figure 1 presents the PRISMA20 flow chart of the study selection.
Exclusion Criteria
We excluded publications that did not meet the selection criteria outlined in Table 1, as well as duplicate publications. Additionally, we also excluded expert opinions or guidelines with unclear recommendations, single-arm primary studies, and primary studies already included in at least 1 eligible systematic review.
Critical Appraisal of Evidence-Based Guidelines
The included studies were critically appraised by 1 reviewer using the following tools as a guide: A Measurement Tool to Assess systematic Reviews 2 (AMSTAR 2)21 for systematic reviews and the “Questionnaire to assess the relevance and credibility of a NMA”22 for systematic review and network meta-analyses, Drummond checklist23 for economic evaluations, and the Appraisal of Guidelines for Research and Evaluation (AGREE) II instrument24 for guidelines. Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Appendix 2: Characteristics of Included Publications
Please note that this appendix has not been copy-edited.
Table 2: Characteristics of Included Systematic Reviews
Study citation, country, funding source | Study designs and numbers of primary studies included | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Maniaci et al. (2024)12 Belgium Funding source: NR | Study design: systematic review of observational studies Number of included studies: 15 Country: NR | Patients after total laryngectomy for advanced laryngeal cancer Number of participants: 1085 Mean age: 65.38 years Sex: male, 89.38% Disease duration: NR Radiotherapy: NR | Intervention: Voice prosthesis (indwelling and non-indwelling devices) rehabilitation (n = 869, 80.1%) Comparator: esophageal speech without VPs (n = 216, 19.9%) | Outcomes:
Follow-up: NR |
Ahmed et al. (2023)13 Netherlands Funding source: Atos Medical | Study design: mixed- methods study with a rapid review Number of included studies: 10: 3 RCTs, 3 time-series studies, 1 retrospective cohort study, 1 study with unclear design Country: United States, Canada, France, Italy, Spain, the Netherlands, and Poland. | Patients who underwent total laryngectomy Number of participants: 550 (number in the individual studies ranged from 30 to 89) Age: NR Sex: NR Disease duration: NR Radiotherapy: NR | Intervention: HMEs (Assumption: HMEs were used in combination with VPs) Comparator: no HME use, an external humidifier or a previous generation HME | Outcomes:
Follow-up: 3 months or NR |
Mayo-Yanez et al. (2023)14 Spain Funding source: No funding support and the authors declared no conflict of interest | Study design: systematic review of observational studies Number of included studies: 4: 2 prospective case series, 1 prospective case-crossover, 1 case report Country: Germany, Netherlands, and Spain. | Patients with laryngectomy and users of VP Number of participants: 55 patients (315 VP) Mean age: 62.71 Sex: male: 87.27% Disease duration: NR Radiotherapy: 55% to 100% when reported. | Intervention: PVX (n = 94). Comparator: control VP (Vega and ActiValve Light, n = 221) | Outcomes:
Follow-up: NR |
Tawfik et al. (2021)15 Egypt Funding source: NR | Study design: systematic review and network meta-analysis Number of included studies: 120 in network meta-analysis; 27 in meta-analysis only Country: Australia, Belgium, Brazil, Canada, China, Croatia, Czech Republic, Denmark, UK, Egypt, Finland, France, Germany, Slovakia, Greece, India, Italy, Japan, Netherlands, Norway, Pakistan, Poland, South Africa, Spain, Sweden, Switzerland, Turkey, US. | Patients who underwent total laryngectomy Number of participants: 11,918 Mean age: 17 to 90 years Sex: male: 71.7% Disease duration: NR Radiotherapy: 71.7%. | Intervention and comparators: various VPs that include Provox-1, Provox-2, Provox AV, Provox NID, Provox Vega, SPVP, Nijdam, Groningen LR, Groningen ULR, BS-LP, | Outcomes: Devices replacements; Devices lifetime; Airflow resistance; MPT; Leakage rates; Speech rate; Patient device Preference; Phonatory effort; Voice speech quality; Fundamental frequency; Voice loudness; Speech intelligibility; Stoma Stenosis; Dislodgement; Fistula problems; Granulation; Prosthesis inaccurate size; Prosthesis deterioration; Survival rate; Aspiration pneumonia; Fungal colonization; Experience with speaking; Skin irritation; Chemoprophylaxis; Cost. Follow-up: from 0.5 to 133 months |
AV = ActiValve; BS-LP = Blom-Singer low pressure; HMEs = heat and moisture exchangers; LR = low resistance; MPT = maximum phonation time; NID = non-indwelling device; NR = not reported; PVX = Provox Vega XtraSeal; QoL = quality of life; RCT = randomized controlled trial; SF-36 = 36-Item short form survey instrument; SPVP = sound-producing voice prosthesis; ULR = ultra-low resistance; VHI = voice handicap index; VP = voice prostheses; VRQoL = voice-related quality of life.
Table 3: Characteristics of Included Economic Evaluation
Study citation country, funding source | Type of analysis, time horizon, perspective | Population characteristics | Intervention and comparator(s) | Approach | Source of clinical, cost, and utility data used in analysis | Main assumptions |
|---|---|---|---|---|---|---|
Rodriguez-Lorenzana et al. (2023)16 Spain Funding source: covered by Fundación Profesor Nóvoa Santos (Hospital Teresa Herrera, 1ª Planta) | Type of analysis: Cost-effective analysis based on a crossover prospective observational study Time Horizon: NR, but likely within study Perspective: Spanish national health system | Inclusion Criteria: Patients who were laryngectomized, 18+, at least 3 months after total laryngectomy, at least 3 months postradiotherapy or chemotherapy, at least 3 years of follow-up, treated with proton-pump inhibitors, and had at least 3 months’ experience using the Provox Vega® 38 patients, 35 men and 3 women Mean age: 66.26 ± 9.36 years old | Intervention: Provox XtraSeal® Comparator: Provox Vega | Outcome measures: The incremental cost-effectiveness ratio (ICER) was calculated. | The study included the direct medical costs, such as the cost of the prostheses, which were obtained from the hospital’s economic department. The cost of each Provox Vega® was EUR 363 and, for Provox XtraSeal, a range between EUR 400 and EUR 600 was selected depending on the health centre assessed. | The anticipated change rate for Provox Vega and Provox XtraSeal was estimated at 3.5 changes per year. The predicted price for Provox Vega® was 1269.08 EUR and 1928.55 EUR for Provox XtraSeal®. The cost-effectiveness analysis aimed to achieve equal costs between the 2 devices. |
Miguel Mayo-Yanez et al. (2022)17 Spain Funding source: Information not available | Type of analysis: CEA based on prospective case-crossover study Time Horizon: NR, but likely within study (mean follow-up: 5.24 years, from 4.04 years to 6.57 years) Perspective: Spanish Public National Health System | Total laryngectomized patients with Provox Vega® and endoprosthesis leakage to whom a Provox ActiValve® was placed. 5 Caucasian men, with a mean follow-up of 5.24 years (range 4.04 to 6.57), were selected. Mean age: 63.84 ± 0.38 years. | Intervention: Provox ActiValve Comparator: Provox Vega | Outcome measures: ICER was calculated A 4 quadrant cost-effectiveness plane was presented. | Cost of each Provox Vega: 363€, Cost of each Provox ActiValve: 1,757.47€. The effectiveness of the treatment was estimated based on number of annual VP replacements and according to follow-up length. | The anticipated change rate for Provox Vega and Provox ActiValve was estimated at 2.94 changes per year. The predicted price for Provox Vega was 1067.60 € and 5168.82 € for Provox ActiValve. |
Beck et al. (2020)18 US Funding source: information not available | Type of analysis: cost-effectiveness and budget impact analysis Perspective: The model was based on a US health care and societal perspective. Time horizon: 20 years | Participants: 40 HME users and 22 ASC users 47 males and 15 females Mean age: HME patients 65.4 (37.9 to 88.9); ASC patients 67.7 (40.7 to 88.6) | Intervention: heat moisture exchanger Comparator; alternative stoma cover | Study questionnaire was based on the Ackerstaff-Hilgers questionnaire A Markov decision model was developed with 3 mutually exclusive health states, reflecting the disease trajectory. Outcome measures: The ICER was used to evaluate the cost-utility of the HME system; represents the additional costs of HME use per QALY gained. | Utilities were obtained from the EQ-5D-5L (US tariff was used) Model inputs; Clinical variables: (device or equipment use, occurrence of pulmonary events, symptoms, productivity loss, treated with medication Costs: annual device costs, cost of accessories and equipment were included in the model. Hospital costs and medication costs were also obtained. All costs were calculated in US dollars Health effects: QALYs - survival probabilities after laryngectomy were derived from literature and assumed to be similar for both groups. In this analysis, disutilities were applied for progressive disease, daily extensive coughing, and mucus production per week. | The Markov model has a hypothetical cohort of 5,000 patients and all simulated patients in both groups start at disease-free survival. |
ASC = alternative stoma covers; CEA = cost-effectiveness analysis; EQ-5D-5L = EuroQol 5 Dimension 5 Level; HMEs = heat and moisture exchangers; ICER = incremental cost-effectiveness ratio; QALYs = quality-adjusted life-years; NR = not reported; RCT = randomized controlled trials; VP = voice prosthesis.
Table 4: Characteristics of Included Guidelines
Intended users, target population | Intervention and practice considered | Major outcomes considered | Evidence collection, selection, and synthesis | Evidence quality assessment | Recommendations development and evaluation | Guideline validation |
|---|---|---|---|---|---|---|
Mayo-Yanez et al. (2024)19 | ||||||
Intended users: health care professionals: otorhinolaryngology specialists (physicians and residents), speech therapists, nursing staff, and other specialists Target population: Laryngectomized patients Country: Spain | Laryngectomized patients who are or could be users of voice prostheses | Vocal outcomes, quality of life, and complications. | The guideline authors searched MEDLINE, Embase, Scopus, Web of Science, PubMed, Science Citation Index, and the Cochrane Library between 1980 to 2023 and conducted a systematic review with 91 studies. | The Oxford Levels of Evidence system 2011: 1a: systematic review of RCTs or n-of-1 trials; to 5 (mechanism-based reasoning). | The recommendations were developed after reviewing and analyzing the most recent research: benefits, side effects, and risks. Grade of Recommendation: B or C, but the meaning of the grade of recommendation is not specified. The authors drafted and reviewed the recommendations. They used a mini-Delphi method with 2 meetings to define them. | The recommendations were then sent to the entire working group for anonymous feedback and reviewed in subsequent meetings. The guideline panel included otolaryngologists, head and neck surgeons, and expert speech therapists. The guideline was published in a peer-reviewed journal. |
RCT = randomized controlled trials.
Appendix 3: Critical Appraisal of Included Publications
Please note that this appendix has not been copy-edited.
Table 5: Strengths and Limitations of Systematic Reviews Using AMSTAR 221 and the ISPOR Questionnaire22
Strengths | Limitations |
|---|---|
Maniaci et al. (2024)12 | |
The purpose of the study was clearly described. Multiple databases were searched (PubMed, Scopus, and Web of Science). The keywords in the search strategy were provided. The authors manually searched related references from the lists of identified full texts. A flow chart of study selection was provided. The details of the included studies were adequately described. The review authors assessed the studies’ RoB using the Joanna Briggs Institute critical appraisal checklist for observational studies. The intervention and study designs of the individual study for inclusion were clearly described. The authors used the GRADE framework to assess the overall certainty of evidence. | The authors did not search the Embase. A grey literature search was not reported. The list of excluded studies was not provided. It was unclear if the study selection, data extraction, and RoB assessments were conducted by at least 2 authors independently. The review authors did not report the funding sources and conflict of interest. The methods to pool all outcome measures were unclear. The follow-up of outcome measures was unclear. The review authors did not assess the potential impact of RoB in individual studies on result interpretations. The GRADE assessment details were unclear: the starting point of the certainty of evidence from observational studies should be “low” rather than “very low” and did not assess the certainty at the outcome level (Table 2) There is a discrepancy between the description in the main text (p. 539.e13) on SF-36 and figure 4C. |
Ahmed et al. (2023)13 | |
The purpose of the study was clearly described. The keywords in the search strategy were provided. The title and abstract screening were conducted by at least 2 authors independently. One reviewer performed the full-text screening and data extractions and verified them with a second reviewer. The study designs of the individual study for inclusion were provided. The review authors declared no conflicts of interest. | The authors only searched PubMed. A grey literature search was not reported. The list of excluded studies was not provided. The authors did not assess the RoB for eligible studies. The details of participants, intervention and control were not clearly reported. The follow-up of outcome measures was unclear for most outcomes. Atos Medical provided funding support for the study. |
Mayo-Yanez et al. (2023)14 | |
The purpose of the study was clearly described. The study designs of the individual study for inclusion were clearly described. Multiple databases (PubMed/MEDLINE, the Cochrane Library, Google Scholar, Scielo, and Web of Science) were searched. The keywords of the search strategy were provided. The authors manually searched related references from the lists of identified full texts. The data extraction was conducted independently by 2 authors. The review authors assessed the methodological quality of eligible studies, using the NICE public health guidance tool. A flow chart of study selection was provided. The review authors declared no conflicts of interest. | The review authors did not search the Embase. Preprint studies and grey literature were not considered. It was unclear if the study selection and RoB were conducted by at least 2 authors independently. The list of excluded studies was not provided. The details of participants, intervention and control were not clearly reported. The follow-up of outcome measures was unclear for most outcomes. |
Tawfik et al. (2021)15 | |
The purpose of the study was clearly described. The protocol of this review was prospectively registered in the PROSPERO (CRD42017080110). Multiple databases were searched (PubMed, Google Scholar,Scopus, Web of Science, Embase, VHL, WHO GHL, Cochrane, Clinical trials.gov, mRCT, Science Direct, WHO, CINAHL, POPLINE, and SIGLE). The search strategies were provided in supplemental Table S2. A manual search of possibly missed articles was conducted. The study selection process and data extraction were clearly described and conducted by 3 reviewers. The review authors assessed the RoB for RCTs using the Cochrane Collaboration RoB tool; for observational studies using the National Institutes of Health for observational cohort, cross-sectional studies, and case-series studies. A flow chart of study selection was provided. Publication bias assessments were conducted. The characteristics of the included studies were adequately described. Ranking probabilities were conducted. The network plot was presented in the appendix. The pointed estimates and 95% credible intervals were reported. | There are several discrepancies between the registered systematic review protocol in PROSPERO (CRD42017080110) and the published reviews. The review authors did not report the funding sources for eligible studies. The review authors did not assess the potential impact of RoB in individual studies on result interpretations. The ranks of the best interventions for each outcome were based on P-scores only, without considering the certainty of evidence. The review authors did not report the funding sources and conflict of interest. Publication bias was not assessed. This network included observational studies. The review did not report direct and indirect estimates. The authors did not assess the systematic differences in treatment effect modifiers across the different treatment comparisons in the network. The individual study results and the details of outcome measures were not reported. The impact of important patient characteristics (e.g., age or disease severity) on treatment effects were not reported. The conclusions were driven by the statistical tests (p-score) and did not consider the results of statistical tests and the certainty of evidence. |
AMSTAR 2 = A MeaSurement Tool to Assess systematic Reviews 2; CCAT = Crowe Critical Appraisal Tool; CINAHL = Cumulative Index to Nursing and Allied Health Literature; GRADE = Grading of Recommendations, Assessment, Development and Evaluation; ISPOR = questionnaire to assess the relevance and credibility of a network meta-analysis; mRCT = metaRegister of Controlled Trials; POPLINE = population information online; RCTs = randomized controlled trials; RoB = risk of bias; SIGLE = System for Information on Grey Literature in Europe; VHL = virtual health library; WHO GHL = WHO Global Health Library.
Table 6: Strengths and Limitations of Economic Evaluation Using the Drummond Checklist23
Strengths | Limitations |
|---|---|
Rodriguez-Lorenzana et al. (2023)16 | |
Study design
Data Collection
Analysis and interpretation:
|
|
Mayo-Yáñez et al. (2022)17 | |
Study design
Data Collection
Analysis and interpretation:
|
|
Beck et al. (2020)18 | |
Study design
Data Collection
Analysis and interpretation:
|
|
Table 7: Strengths and Limitations of Guidelines Using AGREE II24
Item | Mayo-Yanez et al. (2024)19 |
|---|---|
Domain 1: Scope and purpose | |
1. The overall objective(s) of the guideline is (are) specifically described. | Yes |
2. The health question(s) covered by the guideline is (are) specifically described. | Yes |
3. The population (patients, public, etc.) to whom the guideline is meant to apply is specifically described. | Yes |
Domain 2: Stakeholder involvement | |
4. The guideline development group includes individuals from all relevant professional groups. | Yes |
5. The views and preferences of the target population (patients, public, etc.) have been sought. | No |
6. The target users of the guideline are clearly defined. | Yes |
Domain 3: Rigour of development | |
7. Systematic methods were used to search for evidence. | Yes |
8. The criteria for selecting the evidence are clearly described. | Yes |
9. The strengths and limitations of the body of evidence are clearly described. | Yes |
10. The methods for formulating the recommendations are clearly described. | Yes |
11. The health benefits, side effects, and risks have been considered in formulating the recommendations. | To some extent but lacked details. |
12. There is an explicit link between the recommendations and the supporting evidence. | No |
13. The guideline has been externally reviewed by experts before its publication. | NR |
14. A procedure for updating the guideline is provided. | No |
Domain 4: Clarity of presentation | |
15. The recommendations are specific and unambiguous. | No |
16. The different options for management of the condition or health issue are clearly presented. | No |
17. Key recommendations are easily identifiable. | Yes |
Domain 5: Applicability | |
18. The guideline describes facilitators and barriers to its application. | Partially mentioned facilitators. |
19. The guideline provides advice and/or tools on how the recommendations can be put into practice. | No |
20. The potential resource implications of applying the recommendations have been considered. | No |
21. The guideline presents monitoring and/or auditing criteria. | No |
Domain 6: Editorial independence | |
22. The views of the funding body have not influenced the content of the guideline. | Unclear (Atos Medical funded this guideline, and one of the co-authors is an employee of Atos Medical). |
23. Competing interests of guideline development group members have been recorded and addressed. | Yes (the authors declare no conflicts of interest). |
AGREE II = Appraisal of Guidelines for Research and Evaluation II; NR = not reported.
Appendix 4: Main Study Findings
Please note that this appendix has not been copy-edited.
Table 8: Summary of Findings by Outcome — Quality of Life for TEV versus EV
Author (year) and study design | Results | ||||
|---|---|---|---|---|---|
Group (number of studies or participants) or variables | Statistics | Effect size | I2 (%) | Notes | |
VHI | |||||
Maniaci et al. (2024)12 Systematic review with 15 studies | TEV (8 studies) | Mean (SD) | 31.93 (12.11) | NR | P = 0.003 |
EV (8 studies) | Mean (SD) | 35.39 (20.6) | NR | ||
Comparison between TEV and EV (5 studies) | MD | −1.90 (−14.83 to 11.02) | 97% | Random-effects model | |
VRQOL | |||||
Maniaci et al. (2024)12 Systematic review with 15 studies | TEV (7 studies) | Mean (SD) | 8.27 (5.98) | NR | NS |
EV (7 studies) | Mean (SD) | 9.27 (2.02) | NR | ||
Comparison between TEV and EV (3 studies) | MD | −0.74 (−2.85 to 1.38) | 71% | Random-effects model | |
SF-36 | |||||
Maniaci et al. (2024)12 Systematic review with 15 studies | TEV (4 studies) | Mean (SD) | 58.7(2.94) | NR | P < 0.001 |
EV (4 studies) | Mean (SD) | 61.84 (8.33) | NR | ||
EV = esophageal voice; NR = not reported; NS = not statistically significant; SD = Standard deviation; SF-36 = 36-Item short form survey instrument; TEV = tracheoesophageal voice; VHI = Voice handicap index; VP = Voice prostheses; VRQOL = Voice-related quality of life.
Table 9: Summary of Findings- Various clinical outcomes for HMEs versus non-HMEs
Author (year) and study design | Results | ||||
|---|---|---|---|---|---|
Number of studies | Statistics/measures | Effect size/description | P | Notes | |
QoL | |||||
Ahmed et al. (2023)13 Study design: mixed-methods study with a rapid review with 10 studies | QOL (Shortness of breath) | ||||
1 study (Brook et al. 2013) | QOL questionnaire (unclear tool) | Non-HME: 4.6 Provox Micron HMEs (first generation): 4.9 Provox HME (first generation): 4.3 | 0.363 | NS | |
QoL (Sleep quality) | |||||
1 study (Brook et al. 2013) | QOL questionnaire (unclear tool) | Non-HME: 4.5 Provox Micron HMEs (first generation): 4.8 Provox HME (first generation): 4.6 | 0.913 | NS | |
QoL (Speech quality) | |||||
1 study (Brook et al. 2013) | QOL questionnaire (unclear tool) | Non-HME: 7.6 Provox Micron HMEs (first generation): 9.4 Provox HME (first generation): 8.0 | 0.396 | NS | |
QOL (Psychosocial aspects) | |||||
1 study (Brook et al. 2013) | QOL questionnaire (unclear tool) | Non-HME: 5.8 Provox Micron HMEs (first generation): 6.5 Provox HME (first generation): 6.6 | 0.688 | NS | |
QoL (social contacts) | |||||
1 study (Brook et al. 2013) | QOL questionnaire (unclear tool) | Non-HME: 9.6 Provox Micron HMEs (first generation): 8.4 Provox HME (first generation): 9.7 | 0.438 | NS | |
Mucus production | |||||
Ahmed et al. (2023)13 Study design: mixed-methods study with a rapid review with 10 studies | 1 study (Ebersole et al. 2020) | rate of mucus production | XtraHME: 0.13 per 10 inpatient days EH:0.38 per 10 inpatient days | P = 0.02 | Statistically lower in the XtraHME group. |
1 study (Ebersole et al. 2020) | proportion of patients with ≥ 1 mucus plug events | XtraHME: 11% EH: 50% | P = 0.01 | statistically reduced in the XtraHME group. | |
1 study (Foreman et al. 2016) | proportion of patients experiencing mucus plugging | HME: 12.5% EH: 87.5% | P = 0.002 | Odds ratio of a mucus plug event when not using HME: 8.27. | |
Coughing | |||||
Ahmed et al. (2023)13 Study design: mixed-methods study with a rapid review with 10 studies | 1 study (Dassonville et al. 2016) | Coughing (an analogue scale ranging from 0 to 10) | “At 3 months, there was a significant decrease in coughing in the HME group versus the no HME control group.” (p. 5) | P = 0.00174 | statistically decrease in the HME group. |
1 study (Bień et al. 2010) | frequency of coughing | HME: week 1: 48 times; week 12: 30 times Control: week 1: 60 times; week 12: 56 times | < 0.001 | statistically decrease in the HME group. | |
1 study (Mérol et al.) | number of coughing episodes | “In the EH group, 73% of the patients had 2 to 10 spontaneous coughing episodes per day, whereas 8% had 20, another 8% had 30, and 4% had 72 episodes a day (for 8%, this information was missing). In the HME group, most patients (90%) had 1 to 5 spontaneous coughing episodes per day, whereas 4.3% had 10 and another 4.3% had 20 such episodes per day” (p.6) | < 0.001 | significantly lower in the HME group. | |
Forced expectorations | |||||
Ahmed et al. (2023)13 Study design: mixed-methods study with a rapid review with 10 studies | 1 study (Bień et al. 2010) | frequency of forced expectorations | HME: week 1: 56 times; week 12: 27 times Control: week 1: 59 times; week 12: 53 times | < 0.001 | statistically decrease in the HME group. |
Sleep Quality | |||||
Ahmed et al. (2023)13 Study design: mixed-methods study with a rapid review with 10 studies | 1 study (Foreman et al. 2016) | Sleep quality (unclear tool) | “No significant difference was reported between the HME group and EH group in sleep quality” (p.6) | NR | NS |
1 study (Bień et al. 2010) | frequency of patients who had sleeping problems | “In the control group, almost all the patients (97.5%) had sleeping problems, and this did not change over time. In the full compliance HME group (first generation), 79% of the patients had sleeping problems at baseline, and 72% had this problem after 3 months of HME use.” (p. 6) | NR | NS | |
Speech Quality | |||||
Ahmed et al. (2023)13 Study design: mixed-methods study with a rapid review with 10 studies | 1 study (Brook et al. 2013) | Speech quality (unclear tool) | “The HME users and Micron users reported a better voice than did the non-HME users (not statistically significant)” (p.6) | NR | NS |
Physiotherapy | |||||
Ahmed et al. (2023)13 Study design: mixed-methods study with a rapid review with 10 studies | 1 study (Foreman et al. 2016) | the number of days requiring chest physiotherapy after surgery | Provox XtraHME: 1.75 days EH: 3.20 days | 0.034 | significantly reduced in the HME group. |
Tracheobronchitis or pneumonia episodes | |||||
Ahmed et al. (2023)13 Study design: mixed-methods study with a rapid review with 10 studies | 1 study (van den Boer et al. 2014) | tracheobronchitis or pneumonia episodes | HME (first generation): 0.066 episodes per patient per year Non-HME: 0.285 episodes per patient per year | 0.047 | statistically lower in the HME group. |
1 study (van den Boer et al. 2014) | Pulmonary infections (tracheobronchitis and pneumonia together) | HME (first generation): 0.092 episodes per patient per year Non-HME: 0.129 episodes per patient per year | 0.33 | NS | |
Social contacts | |||||
Ahmed et al. (2023)13 Study design: mixed-methods study with a rapid review with 10 studies | 1 study (Parrilla et al. 2015) | Unclear tool (after 12 weeks) | “A statistically nonsignificant improvement in social contacts, with a baseline value of 8.1 versus a value 8.3 after 12 weeks (P=.728), was reported in the structured questionnaires when comparing no HME use with HME (second generation) use.” (p. 7) | 0.728 | NS |
Patient Satisfaction | |||||
Ahmed et al. (2023)13 Study design: mixed-methods study with a rapid review with 10 studies | 1 study (Mérol et al. 2012) | Unclear tool | “Patients’satisfaction showed a significant improvement of first-generation HME over EH (P<.001). Patient satisfaction with the EH was quite low: 11% of the patients reported that they were satisfied with it, 8% reported they somewhat liked it, and 81% reported that they did not like it. All the patients (100%) in the HME (first generation) group were satisfied with the device” (p. 7) | < 0.001 | statistically improvement in the HME group over EH. |
EH = external humidifier; HME = heat and moisture exchanger; NR = not reported; NS = not statistically significant; QoL = quality of life.
Table 10: Summary of Findings by Outcome — Device replace frequency
Author (year) and study design | Results | ||||
|---|---|---|---|---|---|
VP device | Comparator VP | Effect size: RR (95% CI) | P-score | Notes | |
Tawfik et al. (2021)15 Systematic review with network meta-analysis (27 studies with 5724 patients) | Provox-1 | BS-LP | 0.69 (0.19 to 2.51) | 0.74 | NS |
Nijdam | BS-LP | 0.78 (0.09 to 6.73) | 0.64 | NS | |
Groningen ULR | BS-LP | 0.81 (0.07 to 9.14) | 0.62 | NS | |
Provox AV | BS-LP | 0.96 (0.09 to 10.74) | 0.57 | NS | |
Provox NID | BS-LP | 1.24 (0.17 to 9.07) | 0.49 | NS | |
Provox Vega | BS-LP | 1.24 (0.17 to 9.11) | 0.48 | NS | |
Provox 2 | BS-LP | 1.30 (0.30 to 5.58) | 0.44 | NS | |
Groningen LR | BS-LP | 1.44 (0.30 to 7.03) | 0.40 | NS | |
SPVP | BS-LP | 10.10 (0.71 to 144.07) | 0.05 | NS | |
AV = ActiValve; BS-LP = Blom-Singer low pressure; CI = confidence interval; LR = low resistance; NID = non-indwelling device; NS = not statistically significant; RR = relative risk; SPVP = sound-producing voice prosthesis; VP = voice prosthesis.
Table 11: Summary of Findings by Outcome — Device lifetime
Author (year) and study design | Results | ||||
|---|---|---|---|---|---|
Comparisons | Statistics | Effect size | P-score | Notes | |
Tawfik et al. (2021)15 Systematic review with network meta-analysis (33 studies with 4777 patients) | Provox AV vs. BS Advantage | MD (95% CI) | 17.25 (0.40 to 34.09) | 0.97 | Statistically significant (p value was not reported) |
Nijdam vs. BS Advantage | MD (95% CI) | 9.87 (−6.67 to 26.42) | 0.73 | NS | |
Provox 1 vs. BS Advantage | MD (95% CI) | 9.00 (−7.24 to 25.25) | 0.66 | NS | |
Groningen LR vs. BS Advantage | MD (95% CI) | 8.44 (−7.76 to 24.65) | 0.61 | NS | |
Groningen ULR vs. BS Advantage | MD (95% CI) | 7.45 (−9.18 to 24.09) | 0.49 | NS | |
BS DV vs. BS Advantage | MD (95% CI) | 6.30 (−19.12 to 31.72) | 0.46 | NS | |
Provox 2 vs. BS Advantage | MD (95% CI) | 6.82 (−9.26 to 22.91) | 0.40 | NS | |
Provox Vega vs. BS Advantage | MD (95% CI) | 5.24 (−10.87 to 21.36) | 0.25 | NS | |
BS-LP vs. BS Advantage | MD (95% CI) | 4.97 (−11.09 to 21.03) | 0.24 | NS | |
Mayo-Yáñez et al. (2023)14 Systematic review with 4 studies | PVX vs. Control VP (Vega or ActiValve light) | Mean ± SD (95% CI) | PVX: 114.28 ± 73.2 (98.29 to 130.26) days Control: 102.98 ± 17.74 (100.6 to 105.35) days | NR | No statistical test performed |
AV = ActiValve; BS-LP = Blom-Singer; CI = confidence interval; DV = dual valve; LP = low pressure; LR = low resistance; MD = mean difference; NR = Not reported; NS = not statistically significant; PVX = Provox Vega XtraSeal; ULR = ultra-low resistance.
Table 12: Summary of Findings by Outcome — Air flow resistance
Author (year) and study design | Results | ||||
|---|---|---|---|---|---|
VP device | Comparator VP | Effect size: RR (95% CI) | P-score | Notes | |
Tawfik et al. (2021)15 Systematic review with network meta-analysis (8 studies with 1850 patients) | Provox 2 | Groningen LR | 0.42 (0.08 to 2.11) | 0.84 | NS |
Provox 1 | Groningen LR | 0.84 (0.18 to 3.95) | 0.49 | NS | |
Nijdam | Groningen LR | 1.31 (0.22 to 7.67) | 0.28 | NS | |
CI = confidence interval; LR = low resistance; NS = not statistically significant; RR = relative risk.
Table 13: Summary of Findings by Outcome — Maximum phonation time
Author (year) and study design | Results | ||||
|---|---|---|---|---|---|
VP device | Comparator VP | Effect size: MD (95% CI) | P-score | Notes | |
Tawfik et al. (2021)15 Systematic review with network meta-analysis (13 studies with 639 patients) | Provox HME | BS Advantage | 6.30 (3.34 to 9.26) | 1.00 | Statistically significant (p value was not reported) |
BS ATV | BS Advantage | 3.00 (−0.35 to 6.35) | 0.87 | NS | |
Provox FreeHands HME | BS Advantage | −2.90 (−6.07 to 0.27) | 0.59 | NS | |
Provox 2 | BS Advantage | −3.60 (−7.55 to 0.35) | 0.52 | NS | |
Provox 1 | BS Advantage | −5.63 (−8.99 to −2.27) | 0.33 | NS | |
BS-LP | BS Advantage | −5.90 (−9.26 to −2.53) | 0.27 | NS | |
Panje | BS Advantage | −7.90 (−12.14 to −3.65) | 0.12 | NS | |
Groningen LR | BS Advantage | −12.38 (−22.69 to −2.07) | 0.06 | NS | |
ATV = adjustable tracheostoma valve; BS = Blom-Singer; CI = confidence interval; HME = heat and moisture exchanger; LR = low resistance; MD = mean difference; NS = not statistically significant; VP = voice prostheses.
Table 14: Summary of Findings by Outcome — Leakage rate
Author (year) and study design | Results | ||||
|---|---|---|---|---|---|
VP device | Comparator VP | Effect size: RR (95% CI) | P-score | Notes | |
Tawfik et al. (2021)15 Systematic review with network meta-analysis (40 studies with 1493 patients) | Provox Vega | BS-LP | 1.87 (0.97 to 3.60) | 0.72 | NS |
Provox 2 | BS-LP | 2.08 (1.11 to 3.88) | 0.53 | Statistically significant (p value was not reported) | |
Nijdam | BS-LP | 2.23 (1.27 to 3.90) | 0.47 | Statistically significant (p value was not reported) | |
Groningen LR | BS-LP | 2.39 (1.37 to 4.15) | 0.29 | Statistically significant (p value was not reported) | |
Provox 1 | BS-LP | 3.25 (1.89 to 5.60) | 0 | Statistically significant (p value was not reported) | |
BS-LP = Blom-Singer low pressure; CI = confidence interval; LR = low resistance; NS = not statistically significant; RR = relative risk; VP = voice prostheses.
Table 15: Summary of Findings by Outcome — Speech rate
Author (year) and study design | Results | ||||
|---|---|---|---|---|---|
VP device | Comparator VP | Effect size: MD (95% CI) | P-score | Notes | |
Tawfik et al. (2021)15 Systematic review with network meta-analysis (40 studies with 1493 patients) | Groningen LR | BS-LP | −1.75 (−24.67 to 21.17) | 0.44 | NS |
BS-LP = Blom-Singer low pressure; CI = confidence interval; LR = low resistance; MD = mean difference; NS = not statistically significant; VP = voice prostheses.
Table 16: Summary of Findings by Outcome — Patient device preference
Author (year) and study design | Results | ||||
|---|---|---|---|---|---|
VP device | Comparator VP | Effect size: OR (95% CI) | P-score | Notes | |
Tawfik et al. (2021)15 Systematic review with network meta-analysis (21 studies with 932 patients) | Provox 2 | BS-LP | 33.88 (0.65 to 1762.24) | 0.92 | NS |
Provox 1 | BS-LP | 12.04 (0.27 to 538.08) | 0.78 | NS | |
Provox XtraHME | BS-LP | 13.09 (0.18 to 974.17) | 0.78 | NS | |
Provox HME | BS-LP | 10.27 (0.54 to 194.25) | 0.76 | NS | |
Provox Stomafilter HME | BS-LP | 2.91 (0.03 to 266.18) | 0.55 | NS | |
Groningen LR | BS-LP | 1.46 (0.03 to 65.10) | 0.45 | NS | |
Provox FreeHands | BS-LP | 0.67 (0.01 to 61.92) | 0.36 | NS | |
Provox FreeHands HME | BS-LP | 0.19 (0.00 to 12.38) | 0.20 | NS | |
VoiceMaster | BS-LP | 0.10 (0.00 to 23.37) | 0.17 | NS | |
External Humidifier | BS-LP | 0.04 (0.00 to 1.22) | 0.09 | NS | |
BS-LP = Blom-Singer low pressure; CI = confidence interval; HME = heat and moisture exchanger; LR = low resistance; NS = not statistically significant; OR = odds ratio; VP = voice prostheses.
Table 17: Summary of Findings by Outcome — Increase phonatory effort
Author (year) and study design | Results | ||||
|---|---|---|---|---|---|
VP device | Comparator VP | Effect size: OR (95% CI) | P-score | Notes | |
Tawfik et al. (2021)15 Systematic review with network meta-analysis (4 studies with 75 patients) | Provox Vega | BS-LP | 4.11 (1.29 to 13.06) | 0.99 | Statistically significant (p value was not reported) |
BS-LP = Blom-Singer low pressure; CI = confidence interval; NS = not statistically significant; OR = odds ratio; VP = voice prostheses.
Table 18: Summary of Findings by Outcome — Voice speech quality
Author (year) and study design | Results | ||||
|---|---|---|---|---|---|
VP device | Comparator VP | Effect size: OR (95% CI) | P-score | Notes | |
Tawfik et al. (2021)15 Systematic review with network meta-analysis (6 studies with 620 patients) | Provox Vega | BS-LP | 16.41 (4.33 to 62.22) | 1.00 | Statistically significant (p value was not reported) |
Panje | BS-LP | 1.00 (0.16 to 6.08) | 0.25 | NS | |
BS-LP = Blom-Singer low pressure; CI = confidence interval; NS = not statistically significant; OR = odds ratio; VP = voice prostheses.
Table 19: Summary of Findings by Outcome — Fundamental Frequency
Author (year) and study design | Results | ||||
|---|---|---|---|---|---|
VP device | Comparator VP | Effect size: MD (95% CI) | P-score | Notes | |
Tawfik et al. (2021)15 Systematic review with network meta-analysis (8 studies with 148 patients) | SPVP | Groningen LR | 96.33 (17.29 to 175.37) | 0.99 | Statistically significant (p value was not reported) |
Provox 1 | Groningen LR | 0.08 (−4.21 to 4.36) | 0.26 | NS | |
BS-LP = Blom-Singer low pressure; CI = confidence interval; LR = low resistance; MD = mean difference; NS = not statistically significant; SPVP = sound-producing voice prosthesis; VP = voice prosthesis.
Table 20: Summary of Findings by Outcome — Voice Loudness
Author (year) and study design | Results | ||||
|---|---|---|---|---|---|
VP device | Comparator VP | Effect size: MD (95% CI) | P-score | Notes | |
Tawfik et al. (2021)15 Systematic review with network meta-analysis (7 studies with 247 patients) | Staffieri | BS-LP | 0.03 (−11.75 to 11.81) | 0.54 | NS |
Provox 1 | BS-LP | −0.50 (−5.48 to 4.48) | 0.48 | NS | |
Provox NID | BS-LP | −1.00 (−4.62 to 2.62) | 0.39 | NS | |
BS-LP = Blom-Singer low pressure; CI = confidence interval; LR = low resistance; MD = mean difference; NID = non-indwelling device; NS = not statistically significant; VP = voice prosthesis.
Table 21: Summary of Findings by Outcome — Speech Intelligibility
Author (year) and study design | Results | ||||
|---|---|---|---|---|---|
VP device | Comparator VP | Effect size: OR (95% CI) | P-score | Notes | |
Tawfik et al. (2021)15 Systematic review with network meta-analysis (7 studies with 692 patients) | Nijdam | Groningen LR | 3.02 (0.12 to 74.99) | 0.87 | NS |
Provox 1 | Groningen LR | 0.10 (0.02 to 0.55) | 0.62 | Statistically significant (p value was not reported) | |
CI = confidence interval; LR = low resistance; NS = not statistically significant; OR = odds ratio; VP = voice prosthesis.
Table 22: Summary of Findings by Outcome — Stoma stenosis
Author (year) and study design | Results | ||||
|---|---|---|---|---|---|
VP device | Comparator VP | Effect size: RR (95% CI) | P-score | Notes | |
Tawfik et al. (2021)15 Systematic review with network meta-analysis (8 studies with 437 patients) | Provox Vega | BS-LP | 5.25 (2.06 to 13.40) | 0 | Statistically significant (p value was not reported) |
BS-LP = Blom-Singer low pressure; CI = confidence interval; RR = relative risk; VP = voice prosthesis.
Table 23: Summary of Findings by Outcome — Dislodgement
Author (year) and study design | Results | ||||
|---|---|---|---|---|---|
VP device | Comparator VP | Effect size: RR (95% CI) | P-score | Notes | |
Tawfik et al. (2021)15 Systematic review with network meta-analysis (31 studies with 2977 patients) | Provox 2 | Provox 1 | 0.27 (0.13 to 0.57) | 0.79 | Statistically significant (p value was not reported) |
Provox Vega | Provox 1 | 0.28 (0.12 to 0.67) | 0.71 | Statistically significant (p value was not reported) | |
CI = confidence interval; RR = relative risk; VP = voice prosthesis.
Table 24: Summary of Findings by Outcome — Fistula problems
Author (year) and study design | Results | ||||
|---|---|---|---|---|---|
VP device | Comparator VP | Effect size: RR (95% CI) | P-score | Notes | |
Tawfik et al. (2021)15 Systematic review with network meta-analysis (13 studies with 1767 patients) | Groningen LR | ESKA-Herrmann | 0.76 (0.50 to 1.18) | 0.87 | NS |
Provox 1 | ESKA-Herrmann | 0.87 (0.66 to 1.15) | 0.79 | NS | |
Nijdam | ESKA-Herrmann | 0.96 (0.61 to 1.51) | 0.31 | NS | |
CI = confidence interval; LR = low resistance; NS = not statistically significant; RR = relative risk; VP = voice prosthesis.
Table 25: Summary of Findings by Outcome — Granulation
Author (year) and study design | Results | ||||
|---|---|---|---|---|---|
VP device | Comparator VP | Effect size: RR (95% CI) | P-score | Notes | |
Tawfik et al. (2021)15 Systematic review with network meta-analysis (23 studies with 3474 patients) | Provox 2 | BS-LP | 0.73 (0.02 to 26.32) | 0.60 | NS |
Provox 1 | BS-LP | 0.95 (0.13 to 7.03) | 0.53 | NS | |
Provox Vega | BS-LP | 0.87 (0.01 to 63.18) | 0.53 | NS | |
VoiceMast | BS-LP | 0.96 (0.06 to 15.20) | 0.52 | NS | |
Groningen LR | BS-LP | 0.97 (0.05 to 18.26) | 0.52 | NS | |
Nijdam | BS-LP | 1.93 (0.10 to 36.18) | 0.30 | NS | |
BS-LP = Blom-Singer low pressure; CI = confidence interval; LR = low resistance; NS = not statistically significant; RR = relative risk; VP = voice prosthesis.
Table 26: Summary of Findings by Outcome — Prosthesis inaccurate size
Author (year) and study design | Results | ||||
|---|---|---|---|---|---|
VP device | Comparator VP | Effect size: RR (95% CI) | P-score | Notes | |
Tawfik et al. (2021)15 Systematic review with network meta-analysis (4 studies with 388 patients) | Provox 2 | Provox 1 | 0.77 (0.23 to 2.61) | 0.66 | NS |
CI = confidence interval; NS = not statistically significant; RR = relative risk; VP = voice prosthesis.
Table 27: Summary of Findings by Outcome — Prosthesis deterioration
Author (year) and study design | Results | ||||
|---|---|---|---|---|---|
VP device | Comparator VP | Effect size: RR (95% CI) | P-score | Notes | |
Tawfik et al. (2021)15 Systematic review with network meta-analysis (3 studies with 200 patients) | Provox 2 | Provox 1 | 2.62 (0.88 to 7.81) | 0.04 | NS |
CI = confidence interval; NS = not statistically significant; RR = relative risk; VP = voice prosthesis.
Table 28: Summary of Findings by Outcome — Survival rate
Author (year) and study design | Results | ||||
|---|---|---|---|---|---|
VP device | Comparator VP | Effect size: RR (95% CI) | P-score | Notes | |
Tawfik et al. (2021)15 Systematic review with network meta-analysis (3 studies with 135 patients) | Provox 1 | BS-LP | 1.99 (0.49 to 8.15) | 0.83 | NS |
BS-LP = Blom-Singer low pressure; CI = confidence interval; NS = not statistically significant; RR = relative risk; VP = voice prosthesis.
Table 29: Summary of Findings by Outcome — Other outcomes
Author (year) and study design | Results | ||||
|---|---|---|---|---|---|
Group (number of studies) | Statistics | Effect size | I2 (%) | Notes | |
Aspiration pneumonia | |||||
Tawfik et al. (2021)15 Systematic review with network meta-analysis (4 studies with 274 patients) | Provox 2 (1 study) | Event rate (95% CI) | 0.063 (0.016 to 0.218) | NA | — |
Provox 1 (1 study) | Event rate (95% CI) | 0.034 (0.011 to 0.102) | NA | — | |
BS-LP (2 studies) | Event rate (95% CI) | 0.041 (0.019 to 0.089) | NR | — | |
Fungal colonization | |||||
Tawfik et al. (2021)15 Systematic review with network meta-analysis (6 studies with 213 patients) | Provox 2 (1 study) | Event rate (95% CI) | 0.810 (0.663 to 0.902) | NA | — |
Provox 1 (2 studies) | Event rate (95% CI) | 0.652 (0.552 to 0.741) | NR | — | |
BS-LP (2 studies) | Event rate (95% CI) | 0.500 (0.350 to 0.650) | NR | — | |
Rate of patients who were fluent in speaking | |||||
Tawfik et al. (2021)15 Systematic review with network meta-analysis (4 studies with 274 patients) | Provox Hands-free HME ENB (1 study) | Event rate (95% CI) | 0.792 (0.587 to 0.911) | NA | — |
Provox HME (1 study) | Event rate (95% CI) | 0.500 (0.342 to 0.658) | NA | — | |
BS-LP (2 studies) | Event rate (95% CI) | 0.480 (0.370 to 0.592) | NR | — | |
Groningen LR (1 Study) | Event rate (95% CI) | 0.352 (0.237 to 0.587) | NA | — | |
Provox 1 (1 study) | Event rate (95% CI) | 0.222 (0.056 to 0.579) | NA | — | |
Provox Hands-free HME (1 study) | Event rate (95% CI) | 0.208 (0.089 to 0.413) | NA | — | |
Skin irritation rate | |||||
Tawfik et al. (2021)15 Systematic review with network meta-analysis (6 studies with 213 patients) | Overall | Event rate (95% CI) | 0.189 (0.113 to 0.300) | NA | — |
Provox StabiliBase (1 study) with the highest rate | Event rate (95% CI) | 0.571 (0.316 to 0.794) | NA | — | |
BS-LP (1 studies) with the lowest rate | Event rate (95% CI) | 0.019 (0.005 to 0.074) | NA | — | |
Cost of device | |||||
Tawfik et al. (2021)15 Systematic review with network meta-analysis | 3 studies | Prices | Highest price: Provox AV or Pro Provox-2 Lowest price: BS-LP | NA | — |
BS-LP = Blom-Singer low pressure; CI = confidence interval; ENB = external neck brace; HME = heat and moisture exchanger; LR = low resistance; NA = not applicable; NR = not reported; NS = not statistically significant.
Table 30: Summary of Findings of Included Economic Evaluations
Main study findings | Authors’ conclusion |
|---|---|
Rodriguez-Lorenzana et al. (2023)16 | |
| “By reducing the number of changes needed, the Provox XtraSeal® prosthesis offers a cost-effective alternative. The positive cost-effectiveness relationship of the Provox XtraSeal® prosthesis implies that the benefits gained from using this prosthesis outweigh the associated costs” (p. 10) |
Mayo-Yáñez et al. (2022)17 | |
| “The results proved the significant differences in terms of prothesis duration between Provox Vega and Provox ActiValve, as week as its use is more effective and less expensive. These findings support the use of Provox ActiValve in patients with increased prosthesis replacements due to endoprosthesis leakage, to reduce the number of changes and cost.” (p. 4171 to 4172) |
Beck et al. (2020)18 | |
Health care perspective;
Social Perspective:
| “HME use scores favorably on cost-effectiveness compared with the ASC use in the pulmonary rehabilitation after laryngectomy in the US healthcare and societal setting.” (p. 3732) |
ASC = alternative stoma covers; ICER = incremental cost-effectiveness ratio; QALYs = quality-adjusted life-years; VP = voice prosthesis.
Table 31: Summary of Recommendations in Included Guidelines
Recommendations and supporting evidence | Quality of evidence and strength of recommendations |
|---|---|
Mayo-Yanez (2024)19 | |
“For the management of periprosthetic leakage, the replacement of the prosthesis with a double-flanged one, such as the Provox® Vega™ XtraSeal™, is recommended.” (p. 8) (Recommendation 15) Relevant supporting evidence: “Replacement with a double-flanged prosthesis (Provox® Vega™ XtraSeal™) has shown a reduction in periprosthetic leakage (9.62% with XtraSeal vs. 22.43% in the control group) and has been shown to be a cost-effective procedure in the long term (3a, B). The Blom-Singer large oesophageal and tracheal flange VP is also a useful solution for the management of periprosthetic leakage, ensuring similar voice quality and an identical lifespan to that of other voice prostheses.” (p. 9) | Recommendation: B; based on 3b evidence. |
“For the management of periprosthetic leakage, VP replacement with the adjustment of diameter and length, or the placement of a silicone sheet on the tracheal side of the prosthesis, is also recommended.” (p. 8) (Recommendation 16) Relevant supporting evidence: “The management of this complication is usually conservative (4, C). Initially, techniques such as adjusting the size of the prosthesis or placing a silicone ring around the tracheal face of the prosthesis are used. “(p. 8) | Recommendation: C; based on C evidence. |
VP = voice prosthesis.
Appendix 5: References of Potential Interest
Please note that this appendix has not been copy-edited.
<excluded for single-arm primary study>
Heirman AN, Tellman RS, van der Molen L, et al. The acceptance and voice quality of a new voice prosthesis 'Vega High performance' - a feasibility study. Acta Otolaryngol. 2023;143(8):721-729. PubMed
<excluded for the primary study already included by at least one systematic review>
Ebersole B, Moran K, Gou J, et al. Heat and moisture exchanger cassettes: results of a quality/safety initiative to reduce postoperative mucus plugging after total laryngectomy. Head Neck. 2020;42(9):2453-2459. PubMed
Mayo-Yanez M, Cabo-Varela I, Suanzes-Hernandez J, Calvo-Henriquez C, Chiesa-Estomba C, Herranz Gonzalez-Botas J. Use of double flange voice prosthesis for periprosthetic leakage in laryngectomised patients: a prospective case-crossover study. Clin Otolaryngol. 2020;45(3):389-393. PubMed
Petersen JF, Lansaat L, Timmermans AJ, van der Noort V, Hilgers FJM, van den Brekel MWM. Postlaryngectomy prosthetic voice rehabilitation outcomes in a consecutive cohort of 232 patients over a 13-year period. Head Neck. 2019;41(3):623-631. PubMed
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners' own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada's federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user's own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for noncommercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada's health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada's federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca