Drugs, Health Technologies, Health Systems
Health Technology Review
BRAF and MEK Inhibitors for Active or Symptomatic Melanoma Brain Metastasis
Authors: Said Yousef Abdelrazeq, Shariq Najeeb, Shannon E. Kelly, Melissa Brouwers, Becky Skidmore, George A. Wells
This rapid review was conducted by the POst-Market Drug Evaluation Team (PODET) team through the Post-Market Drug Evaluation (PMDE) CoLab Network.
Key Messages
This rapid review examines the clinical efficacy, effectiveness, and safety of BRAF and MEK inhibitors as a treatment for patients with active or symptomatic melanoma brain metastasis (MBM).
Three primary studies and 4 clinical practice guidelines met the eligibility criteria for this rapid review. No systematic reviews (SRs) were found.
There are very few studies examining the effectiveness and safety of BRAF and MEK inhibitors in patients with active or symptomatic MBM.
The limited number of primary studies available are of low quality and are subject to significant risk of bias. Three single-arm, low-quality cohort studies published since 2019 were identified: 2 providing data on median progression-free survival (PFS) (approximately 5 months), 2 providing data on overall survival (OS) (approximately 7 to 9 months), and the third providing narrative descriptions only. Adverse effects were reported in 1 study. No comparative studies were located.
The 3 primary studies reported that patients may survive for up to 5 months without their symptoms worsening, and their OS rates were between 7.4 months to 9.5 months after receiving BRAF and MEK inhibitor combination therapy. In 1 study, common side effects included fever, rash, and fatigue, and some patients stopped treatment primarily because of fever and abnormal liver function.
The clinical practice guidelines considered our patient population, but the resulting recommendations did not differentiate between patients with and without active or symptomatic MBM or did not refer specifically to BRAF and MEK inhibitors. Instead, most recommendations focused on other treatments, such as surgery.
Abbreviations
AE
adverse event
AGREE II
Appraisal of Guidelines for Research and Evaluation II
ASCO
American Society of Clinical Oncology
ASTRO
American Society for Radiation Oncology
CCA
Cancer Council Australia
HR
hazard ratio
HTA
health technology assessment
MBM
melanoma brain metastasis
NCCN
National Comprehensive Cancer Network
OS
overall survival
PFS
progression-free survival
PICO
population, intervention, comparator, and outcome
SIGN
Scottish Intercollegiate Guidelines Network
SNO
Society for Neuro-Oncology
SR
systematic review
Introduction and Rationale
Background
Melanoma is a highly malignant neoplasm originating from melanocytes.1 It has been estimated that approximately 21 people (among 100,000 people) are diagnosed with melanoma every year in Canada.2 Melanoma typically presents as a skin lesion or evolves from a preexisting benign growth on the skin that is formed by a collection of melanocytes (i.e., nevus). It is characterized by an irregular border with a diameter exceeding 6 mm and varies in colour. Major risk factors for melanoma include prolonged exposure to UV radiation, fair skin colour, high count of nevi, genetic factors, and immunosuppression.3 If untreated, melanoma can metastasize to several sites. The brain is a common site for metastasis, leading to neurologic symptoms which include persistent and severe headaches, neurologic deficits such as weakness or numbness on 1 side of the body, speech difficulties, vision problems, and balance or coordination issues.4 In Canada, it has been estimated that approximately 7% of patients with skin melanoma progress to melanoma brain metastasis (MBM).5,6 Despite recent advancements in treatment, such as anti–PD-1 antibodies, the median survival rate of MBM remains just under 3 years.7
MBM can be classified based on the presence or absence of symptoms or disease activity. Symptomatic MBM refers to the presence of metastatic melanoma lesions in the brain that cause clinical symptoms such as headaches, seizures, neurologic deficits, or cognitive disturbances.8 These symptoms arise owing to the mass effect, edema, or hemorrhage associated with the metastatic lesions. Conversely, asymptomatic MBM involves metastatic brain lesions without any overt clinical symptoms and is typically identified incidentally through imaging studies performed for other reasons. Active MBM (both symptomatic and asymptomatic) specifically denotes metastases that are biologically active, showing growth, angiogenesis, or progression, in contrast to inactive or dormant lesions which remain stable without significant changes in size or activity. Active metastases also exhibit ongoing proliferation and the potential to cause symptoms as they grow and exert effects on surrounding brain tissue.
Mutations in genes such as BRAF and cell proliferation controlled by enzymes such as MEK play crucial roles in promoting cell survival, proliferation, and metastasis.9 BRAF and MEK inhibitors are targeted therapies used to treat metastatic melanoma, including cases where the cancer has metastasized to the brain.10 BRAF inhibitors, such as vemurafenib and dabrafenib, specifically target and inhibit the mutated BRAF V600E protein, a common mutation in melanoma that leads to uncontrolled cell proliferation, resulting in the reduction of cell proliferation.11 MEK inhibitors, such as trametinib and cobimetinib, target MEK1 and MEK2 and are downstream components of the same pathway, often used in combination with BRAF inhibitors to enhance efficacy and overcome resistance mechanisms.11,12 Two early studies demonstrated that this combination therapy has shown some clinical benefit in reducing tumour size and improving OS in patients with metastatic melanoma, including those with brain metastases, owing to its ability to penetrate the blood-brain barrier and target the oncogenic signalling pathways driving the malignancy.10,13 These studies included comparisons with monotherapy (e.g., dabrafenib-vemurafenib), although neither of these studies included a best supportive care or other comparison (e.g., surgery) as part of their study design. Currently, recommendations by Canada’s Drug Agency and the pan-Canadian Oncology Drug Review Expert Review Committee exclude BRAF and MEK inhibitors for patients with melanoma and symptomatic brain metastases.14 Recent limited data suggests that this patient population may benefit from BRAF and MEK inhibitors similar to those with asymptomatic brain metastases, with manageable toxicity.15
Policy Issue
The current pan-Canadian Oncology Drug Review Expert Review Committee recommendations are to exclude BRAF and MEK inhibitors for patients with active or symptomatic MBM; however, it has been suggested this patient population may experience benefits from BRAF and MEK inhibitors similar to those seen in patients with asymptomatic brain metastases with a manageable toxicity profile. Evidence in this space should be reviewed and appraised.
Policy Questions
Should BRAF and MEK inhibitors be funded for patients with melanoma and active or symptomatic brain metastases?
Purpose
To evaluate the efficacy, effectiveness, and safety of BRAF and MEK inhibitors in patients with melanoma and active or symptomatic brain metastases.
Research Questions
What is the efficacy and effectiveness of BRAF and MEK inhibitors for the treatment of patients with active or symptomatic MBM?
What is the safety of BRAF and MEK inhibitors for the treatment of patients with active or symptomatic MBM?
What are the evidence-based guidelines regarding the use of BRAF and MEK inhibitors for the treatment of patients with active or symptomatic MBM?
Methods
We conducted a rapid review of clinical efficacy, effectiveness, safety, and evidence-based guidelines.
Literature Search Methods
An experienced medical information specialist developed and tested the search strategies through an iterative process in consultation with the review team. Another senior information specialist peer-reviewed the MEDLINE strategy before execution using the PRESS Checklist.16 Using the multifile option and deduplication tool available on the Ovid platform, we searched Ovid MEDLINE ALL, Embase Classic+Embase, Cochrane Database of Systematic Reviews, and Cochrane Central Register of Controlled Trials. We performed all searches on June 26, 2024. We used a combination of controlled vocabulary (e.g., “neoplasm metastasis,” “vemurafenib,” “mitogen-activated protein kinase kinases/ai [antagonists & inhibitors]”) and keywords (e.g., “metastatic melanoma,” “BRAFI,” “MEK inhibitor”) and adjusted the vocabulary and syntax as necessary across the databases. We applied an SR filter and various primary study filters in MEDLINE and Embase (these filters are not required in the Cochrane databases), limiting all results to the English language and the publication years 2019 to the present and, where applicable, removing animal-only, conference abstracts, and opinion pieces. We downloaded and deduplicated the records using EndNote version 9.3.3 (Clarivate Analytics) and uploaded to Covidence (Veritas Health Innovation Ltd.).
We conducted a targeted search of various clinical guideline developers to identify reports related to melanoma published since 2019. Practice guideline developers specific to the cancer field (Canadian and international) and well-established generalist organizations were chosen. The targeted list of developers included the Scottish Intercollegiate Guidelines Network (SIGN), provincial guidelines (Cancer Care Ontario, British Columbia Cancer Agency, and Alberta Health Services), American Society of Clinical Oncology (ASCO), National Comprehensive Cancer Network (NCCN), Cancer Council Australia (CCA), European Society for Medical Oncology, and the National Institute for Health and Care Excellence in the UK. We searched the organizations’ websites to find the most current versions of the reports.
A targeted search was conducted for relevant reports on the websites of health technology assessment (HTA) agencies in the US, UK, Australia, and New Zealand using the Canada’s Drug Agency Grey Matters Checklist and keywords relevant to our research question. One reviewer screened relevant reports and publications on HTA websites and downloaded the full text of any relevant reports for additional review to check for eligibility.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
|---|---|
Population | Patients with active or symptomatic MBMa |
Intervention(s) | Any combination of BRAF and MEK inhibitorsb (e.g., vemurafenib-cobimetinib, dabrafenib-trametinib, encorafenib-binimetinib) |
Comparator(s) | Immune checkpoint inhibitors, other combination of BRAF and MEK inhibitors, brain radiation, no treatment, best supportive care, no comparator |
Outcome(s) | Any clinical benefits or harms |
Study design(s) | Health technology assessments, systematic reviews, randomized controlled trials, nonrandomized or observational studies, evidence-based guidelines |
MBM = melanoma brain metastasis.
aPatients with active or symptomatic MBM from any age group and country were included.
bInterventions of interest included combinations of BRAF and MEK inhibitors and were permitted to include nondrug interventions.
For all publications, we considered patients with active or symptomatic MBM from any age group and country. Interventions of interest included combinations of BRAF and MEK inhibitors and eligible nondrug interventions. The comparators considered eligible (where appropriate) were immune checkpoint inhibitors, other BRAF and MEK inhibitors, brain radiation, and no treatment. Outcomes of interest encompassed any clinical or safety outcomes.
Clinical Practice Guidelines: Guidelines were included if their objectives and scope included the possibility of recommendations for our patient population and treatments of interest.
Systematic Reviews: SRs, meta-analyses, and network meta-analyses were included, provided they met the PICO criteria and regardless of the primary study designs included in the review.
Primary studies: All comparative study designs were included, provided there were data specific to our patient population, and there was a comparison between BRAF and MEK inhibitors to a comparator of interest. All noncomparative study designs were also included, provided there were data specific to our patient population and treatment of interest.
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria specified in Table 1, were duplicate publications, or were published before 2019. Comparators involving different doses of the same BRAF and MEK inhibitor combination or the same BRAF and MEK inhibitor combination in patients with a different treatment history were excluded. Case reports and case series were excluded.
Critical Appraisal of Individual Studies
The included primary studies were critically appraised by 1 reviewer using a modified version of the Critical Appraisal Skills Programme checklist for cohort studies which focused on study validity (recruitment, exposure ascertainment, outcome ascertainment, confounding, and follow up).17 Evidence-based guidelines were appraised using the Appraisal of Guidelines for Research and Evaluation (AGREE) II instrument18 focusing on the rigour of development and editorial independence domains. Each included publication’s strengths and limitations were described narratively.
Summary of Evidence
Quantity of Research Available
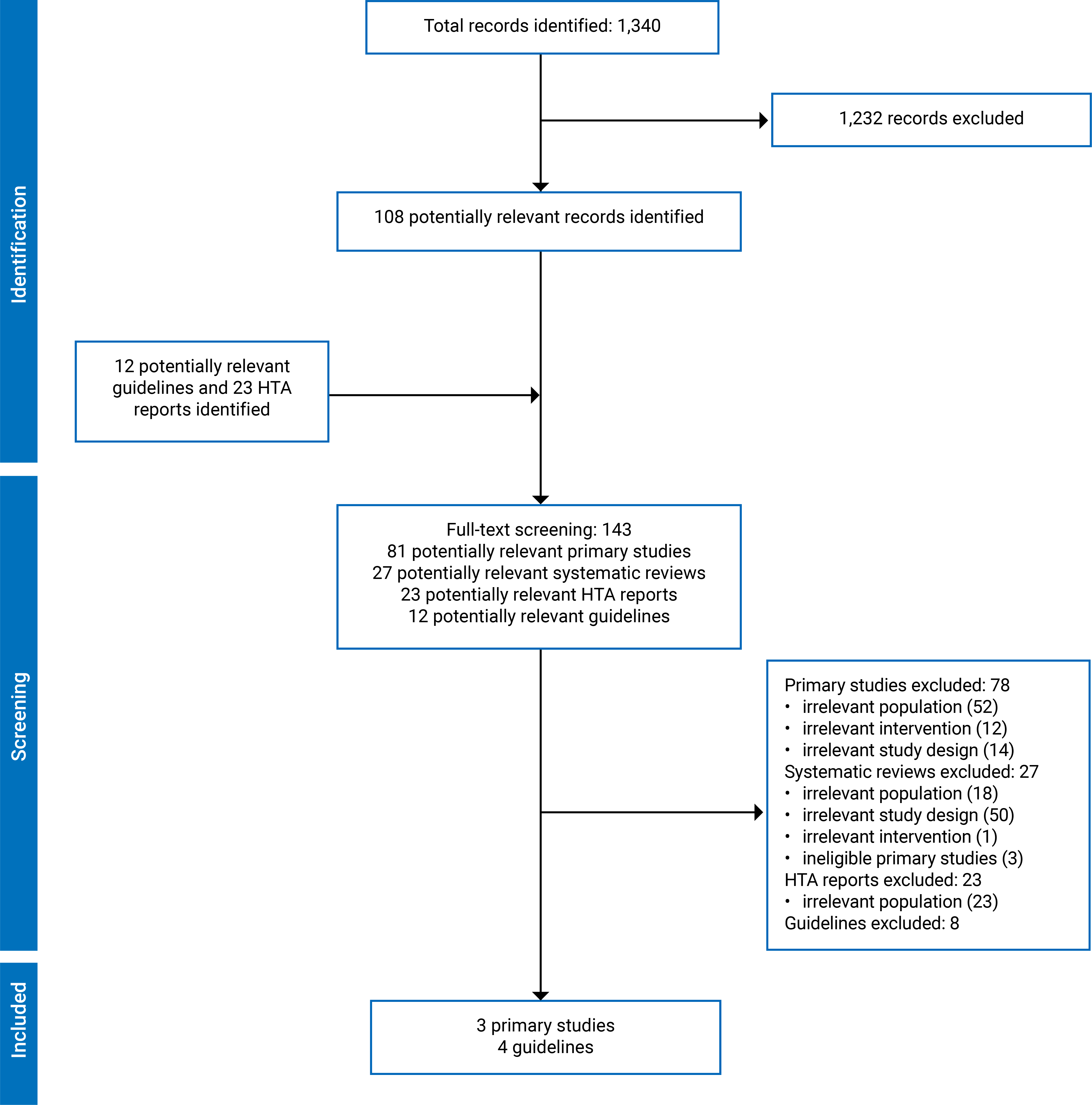
A total of 1,340 citations were identified in the literature search. Following the screening of titles and abstracts, 1,232 citations were excluded and 108 potentially relevant reports from the electronic search were retrieved for full-text review. In addition, 35 potentially relevant HTAs and guidelines were retrieved from the grey literature search for full-text review. Of these potentially relevant articles, 7 publications met the inclusion criteria and were included in this review. These comprised 3 single group intervention studies19-21 and 4 evidence-based guidelines.22-25 Appendix 1 presents the PRISMA flow chart of the study selection.
Study Characteristics
Additional details regarding the characteristics of included publications are provided in Appendix 2 (Table 2 and Table 3).
Three primary studies19-21 were identified that met the inclusion criteria. All potentially eligible SRs were excluded as they did not report data specific to patients with active or symptomatic MBM. Four evidence-based guidelines were identified that met the inclusion criteria.22-25
Primary Studies
Study Design
There were 3 descriptive observational cohort studies (1 prospective, 2 retrospective designs)19-21 published between 2019 and 2024 that evaluated BRAF and MEK inhibitors with no available comparator of interest. The BRAF and MEK inhibitor interventions reported were combinations of dabrafenib and trametinib,21 vemurafenib and cobimetinib,20,21 encorafenib and binimetinib,21 vemurafenib and trametinib,21 and 1 study reported unspecified BRAF and MEK inhibitor combinations19 collected from patient registry data.
Patient follow-up ranged from 18 months to 42.6 months.
One retrospective study19 aimed to assess the clinical effectiveness of rechallenge with BRAF inhibitors or combined BRAF and MEK inhibitors after treatment interruption among patients with advanced cutaneous melanoma, including identified populations with symptomatic or asymptomatic brain metastasis.
A second retrospective study explored the clinical course of patients with BRAF-mutated metastatic melanoma and brain metastases who received combination BRAF and MEK targeted therapy.21 A retrospective chart review was completed using data from 5 clinical centres based on patient receipt of dabrafenib-trametinib, vemurafenib-cobimetinib, encorafenib-binimetinib, or vemurafenib-trametinib.
The objective of included prospective, multicentre, noninterventional, postauthorization safety study was to examine the real-world effectiveness of cobimetinib and vemurafenib with a special focus on survival, safety, and utilization of combination therapy in 2 separate cohorts.20 The first cohort were patients with unresectable or metastatic BRAF V600 mutated melanoma without cerebral metastases and the second were patients with metastatic BRAF V600 mutated melanoma with cerebral metastases. Data were collected during routine clinical follow-up.
Country of Origin
One prospective cohort study was conducted in Germany at 30 sites. Of the 2 included retrospective cohort studies, 1 was conducted in the US21 and the other in the Netherlands.19
Patient Population
The 3 primary studies included 235 patients with symptomatic MBM from 2013 to 2022.19-21 One prospective cohort study20 considered the use of combined cobimetinib and vemurafenib in adult patients with histologically confirmed unresectable or MBM with a BRAF V600 mutation. Patient data were collected between 2017 and 2021. A total of 19 of the 41 patients had symptomatic MBM and were not analyzed separately. Data reported for patients who were symptomatic were for an exploratory post hoc subgroup analysis. No additional patient characteristics were reported. One retrospective cohort study21 considered BRAF and MEK combination use in 65 patients with biopsy-proven metastatic melanoma and active or symptomatic brain metastasis with BRAF V600 mutation. Patient data from 2013 to 2016 were studied. A total of 27 patients were female (41.5%). Patients were described as having American (40%) or European (60%) descent. Previous treatments received within the cohort were brain surgery (28%), anti–CTL-4 therapy (28%), anti–PD-1 therapy (19%), interferon (20%), and chemotherapy (5%). One retrospective study19 reported no additional descriptions of 468 patients with symptomatic MBM but did report treatment line according to the BRAF and MEK inhibitor combinations received for some patients. A total of 84 patients with symptomatic MBM received BRAF and MEK as initial therapy while 151 patients were retreated with BRAF and MEK combination therapy. No additional patient characteristics were reported.
Interventions and Comparators
None of the included observational studies were comparative. One prospective cohort study20 considered a combination of cobimetinib and vemurafenib. One study reported unspecified BRAF and MEK inhibitor combinations19 collected retrospectively from patient registry data in 468 patients with symptomatic MBM. One retrospective cohort study21 reported 4 different BRAF and MEK inhibitor combinations in 65 patients with active or symptomatic MBM including dabrafenib and trametinib (53 patients), vemurafenib and cobimetinib (10 patients), encorafenib and binimetinib (1 patient), and vemurafenib and trametinib (1 patient). No additional details are available for the interventions (e.g., dose or administration)
Clinical Outcomes
For patients with symptomatic MBM, 1 prospective cohort study20 and 1 retrospective cohort study21 reported both PFS and OS. One retrospective study provided only descriptive survival outcomes for patients of interest.19 Other outcomes reported were treatment response (1 retrospective cohort21) and disease progression (1 retrospective cohort21). Other clinical outcomes identified were not reported for patients with active or symptomatic MBM.
Safety and Tolerability
One retrospective cohort study21 of 65 patients with symptomatic MBM21 reported safety or tolerability outcomes. Reported outcomes were AEs, severe AEs, and discontinuation of interventions. No results were reported by the specific BRAF and MEK inhibitor combinations considered in the study, only for the entire patient population with symptomatic MBM receiving any BRAF and MEK inhibitor combination.21
Two eligible studies20,21 did not report safety outcomes for patients with symptomatic MBM.
Evidence-Based Guidelines
The 4 included evidence-based guidelines (NCCN Clinical Practice Guidelines in Oncology (2024),24 ASCO-SNO-ASTRO Guideline,23 CCA (2020),22 and SIGN146 (2023)25) offer comprehensive melanoma management options that encompass patients with brain metastases who are both symptomatic and asymptomatic. The guidelines were intended for a broad range of users, including health care professionals, payers, and patients.22-25 These guidelines serve to inform multidisciplinary teams in providing optimal care and support across various stages and manifestations of melanoma.
Critical Appraisal
Appendix 3 presents the critical appraisal summary of strengths and limitations by publication (Table 4 and Table 5).
Primary Studies
Each study addressed a clearly focused issue with transparent inclusion criteria and detailed descriptions of sex and ethnicity information in some cases.19-21 Drago et al. 21 and Van Not et al. 19 adjusted for several confounders in their analysis. Specifically, the authors used multivariable logistic regression and Cox proportional hazards models to assess factors associated with response to treatment with BRAK and MEK inhibitors and survival outcomes.19,21 However, Kahler et al. did not adjust for any covariates or confounding factors.20
These studies may have exhibited additional potential biases, such as detection bias owing to unmeasured outcomes in Drago et al. (2019)21 and Kahler et al. (2023),20 reporting bias in Van Not et al. (2024),19 for not reporting quantitative outcomes and attrition bias in Kahler et al. (2023),20 owing to inadequate follow-up. These biases highlight limitations in study design, data collection, and reporting, potentially affecting the validity and reliability of the study findings and conclusions.
Evidence-Based Guidelines
The strengths and limitations for each included guideline are presented in Appendix 4. The guidelines assessed using the AGREE II tool varied significantly in terms of rigour of development and editorial independence. The SIGN 146 Guideline 202325 had the highest rigour of development at 97% and complete editorial independence at 100%, indicating a high-quality guideline. The ASCO-SNO-ASTRO Guideline 202323 also showed high standards with an 87% rigour of development and 79% editorial independence. In contrast, the NCCN Guideline 202424 received poor ratings of 57% in rigour of development and 50% in editorial independence. Similarly, the CCA Guideline 202022 scored poorly, receiving 54% in rigour of development but 85% in editorial independence. While ASCO and SIGN guidelines demonstrated strong methodological robustness and editorial integrity, the NCCN guideline24 were not transparently reported, and the CCA guideline22 showed notable deficiencies in both evaluated criteria.
Findings
Appendix 4 presents the main study findings (Table 6, Table 7, and Table 8).
Clinical Effectiveness of BRAF and MEK Inhibitor Combinations
Progression-Free Survival
One retrospective cohort study reported a median PFS of 5.3 months.21 In an exploratory post hoc analysis of a prospective cohort study, PFS was reported to be 5.2 months in 19 patients with symptomatic MBM.20
Overall Survival
Two single cohort primary studies were identified that evaluated the clinical benefits of BRAF and MEK inhibitor combinations in patients with active or symptomatic MBM with BRAF V600 mutation. One retrospective cohort study reported a median OS of 9.5 months for all patients.21 Multivariable analysis revealed that OS was significantly related to age, location, and type of melanoma. Patients older than 49 years had hazards of death that were more than double those of patients younger than 49 years (hazard ratio [HR] = 2.18). The location of the primary lesion in a high-risk location such as the head, neck, or torso also increased the hazards of death in patients who were symptomatic more than 3 times compared with patients with a primary lesion in a lower risk location such as an upper or lower extremity (HR = 3.32). Patients with nodular melanoma had an increased hazard of death almost 5 times higher than patients with superficial spreading melanoma (HR = 4.95). In the same study, it is noted that 45 of 65 patients with symptomatic MBM did not survive to close of study.21
One prospective cohort study reported a post hoc exploration of 19 patients who were symptomatic with an OS of 7.4 months.20
Survival
One retrospective cohort study did not report outcomes according to OS or PFS. Rather, authors provided a descriptive summary of factors associated with hazard of progression or death and identified symptomatic MBM as a statistically significant variable (HR = 1.44). Descriptive results concluded that in patients with symptomatic MBM, retreatment with BRAF and MEK inhibitors resulted in worse survival outcomes.19
Disease Progression
One retrospective cohort study reported disease progression at study close according to no progression (11% of patients with symptomatic MBM) or progression (88% of patients with symptomatic MBM).21
Response Resulting in Reduction in Dose or Discontinuation of Other Medications
One retrospective cohort study reported response to combination therapy with BRAF and MEK inhibitors according to reductions in dose or discontinuation of steroids, anticonvulsants, or opioid medications.21 Patients with symptomatic MBM taking these medications reduced their dose of steroids (66.7%), anticonvulsants (19%), or opioids (33%) after introduction of BRAF and MEK inhibitor combinations. Patients discontinued steroids (33%) or opioids (33%) but not anticonvulsant medications.
Safety of BRAF and MEK Inhibitors
Discontinuation of Study Medications
In 1 retrospective cohort study, 20.8% of patients discontinued drugs owing to AEs, with fever (12.3%) and abnormal liver function tests (3%) being the leading causes.21 Other studies did not report discontinuation of study medications for any reason separately for patients with symptomatic MBM.
Adverse Events
Although, AEs were assessed in the overall population in all included 3 primary studies,19-21 the AEs within the cohort of patients who were symptomatic was assessed in only 1 study.21 Fever was the most common AE, occurring in 20% of patients with symptomatic MBM, followed by rash (13.8%), fatigue (10.8%), and creatinine kinase increase (9.2%).21 Other AEs included dizziness, central nervous system bleeding, myocardial infarction, hypertension, liver-related severe AEs, diarrhea, infection, palpitation, venous thrombosis, nausea, alopecia, and ocular complications, each with lower incidences.21 All other AEs were not reported separately for patients with symptomatic MBM.
Summary of the Recommendations from Evidence-Based Guidelines
The NCCN Guidelines 202424 favour brain-directed therapy over upfront systemic therapy for symptomatic MBM and surgery is preferred for large, symptomatic lesions or when diagnostic uncertainty exists. The ASCO-SNO-ASTRO Guideline 202323 lists local therapies (radiosurgery, radiation therapy, or surgery) regardless of systemic therapy for patients with symptomatic MBM. The CCA Guideline 2020 recommends surgery for patients with symptomatic MBM or causing mass effects. SIGN 146 Guideline 2023 provides no specific recommendations for patients with symptomatic MBM. These recommendations are described in Appendix 4, Table 8.
Overall, the 4 included guidelines provide varied approaches based on consensus, randomized trials, expert opinion, or specific recommendations.22-25 The level of strength and quality of the given recommendations varied, reflecting their respective methodologies and sources of evidence or expert consensus.22-25 Although some recommended surgery and other treatment options for patients with symptomatic MBM, none of the guidelines provided recommendations supporting or refuting the use of BRAF and MEK inhibitors in these patients.22-25
Limitations
There are no high-quality primary studies to support or refute the use of BRAF and MEK inhibitors for patients with active or symptomatic MBM. These studies were observational with no comparison arms and the sample sizes were small. Incomplete reporting was a common limitation. The generalizability of these studies to the Canadian context is uncertain. No SRs were identified that met our eligibility criteria. No clinical practice guidelines were identified that provided guidance specific to our target population and treatment.
The observational and noncomparative design and limited sample size of the included primary studies is a limitation as they cannot account for all known or unknown confounders and there is a potential for selection bias. None of the primary studies were testing a research hypothesis identified in advance and results may be considered purely exploratory. The lack of a formal comparison group limits any inferences that may be made regarding the effect of combined BRAF and MEK therapy on important outcomes in this symptomatic MBM population. It is not clear how these patients may progress without any treatment, on standard therapy, or otherwise. Patient characteristics were poorly described and none of the studies were conducted in Canada which limits our ability to consider the generalizability of the primary study findings to Canadian settings.
Conclusions and Implications for Decision- or Policy-Making
Three single-arm, low-quality cohort studies published since 2019 were identified; 2 studies provided data on median progression-free survival (approximately 5 months) and data on OS (approximately 7 to 9 months), and 1 study provided narrative descriptions only. Adverse effects were reported in 1 study. Incomplete reporting was a common source of bias across all studies.
There is little and low-quality evidence to assist in policy decisions about the role of BRAF and MEK inhibitors in the treatment of patients with active or symptomatic MBM, more research is required to provide higher quality, comparative evidence to inform knowledge gaps around the relative effects of BRAF and MEK inhibitors for patients with symptomatic MBM. Given the lower incidence of melanoma compared with other cancers, additional melanoma registries may be of benefit to identify prospective data about patients, their treatments, characteristics such as brain metastases, and related clinical and patient-relevant outcomes. Given the low-quality studies suggesting treatment responsiveness and relative safety, a special access or a compassionate care strategy to access BRAF and MEK inhibitors may be considered for select individual patients. This may be a reasonable policy option when recommended by a multidisciplinary care team, on a case-by-case basis.
References
1.Schadendorf D, van Akkooi ACJ, Berking C, et al. Melanoma. Lancet. 2018;392(10151):971-984. PubMed
2.Canadian Cancer Statistics Advisory Committee in collaboration with the Canadian Cancer Society, Statistics Canada and the Public Health Agency of Canada. Canadian cancer statistics 2021. Toronto (ON): Canadian Cancer Society 2021: https://cdn.cancer.ca/-/media/files/research/cancer-statistics/2021-statistics/2021-pdf-en-final.pdf. Accessed 2024 Jul 23.
3.Kibbi N, Kluger H, Choi JN. Melanoma: clinical presentations. Cancer Treat Res. 2016;167:107-129. PubMed
4.Chukwueke U, Batchelor T, Brastianos P. Management of brain metastases in patients with melanoma. J Oncol Pract. 2016;12(6):536-542. PubMed
5.Ernst DS, Petrella T, Joshua AM, et al. Burden of illness for metastatic melanoma in Canada, 2011-2013. Curr Oncol. 2016;23(6):e563-e570. PubMed
6.Liu JL, Walker EV, Paudel YR, Davis FG, Yuan Y. Brain metastases among cancer patients diagnosed from 2010–2017 in Canada: incidence proportion at diagnosis and estimated lifetime incidence. Curr Oncol. 2022;29(3):2091-2105. PubMed
7.Vosoughi E, Lee JM, Miller JR, et al. Survival and clinical outcomes of patients with melanoma brain metastasis in the era of checkpoint inhibitors and targeted therapies. BMC Cancer. 2018;18(1):490. PubMed
8.Davies MA, Liu P, McIntyre S, et al. Prognostic factors for survival in melanoma patients with brain metastases. Cancer. 2011;117(8):1687-1696. PubMed
9.Maraka S, Janku F. BRAF alterations in primary brain tumors. Discov Med. 2018;26(141):51-60. PubMed
10.Flaherty KT, Infante JR, Daud A, et al. Combined BRAF and MEK inhibition in melanoma with BRAF V600 mutations. N Engl J Med. 2012;367(18):1694-1703. PubMed
11.Robert C, Karaszewska B, Schachter J, et al. Improved overall survival in melanoma with combined dabrafenib and trametinib. N Engl J Med. 2015;372(1):30-39. PubMed
12.Larkin J, Ascierto PA, Dreno B, et al. Combined vemurafenib and cobimetinib in BRAF-mutated melanoma. N Engl J Med. 2014;371(20):1867-1876. PubMed
13.Menzies AM, Long GV. Dabrafenib and trametinib, alone and in combination for BRAF-mutant metastatic melanoma. Clin Cancer Res. 2014;20(8):2035-2043. PubMed
14.Provisional Funding Algorithm - Melanoma. Ottawa (ON): CADTH; 2023: https://www.cadth.ca/sites/default/files/DRR/2023/PH0022%20Rapid%20Algorithm%20Report%20for%20Melanoma_with%20CAPCA%20Endorsement_FINAL.pdf. Accessed 2024 Jul 23.
15.Davies MA, Saiag P, Robert C, et al. Dabrafenib plus trametinib in patients with BRAFV600-mutant melanoma brain metastases (COMBI-MB): a multicentre, multicohort, open-label, phase 2 trial. Lancet Oncol. 2017;18(7):863-873. PubMed
16.McGowan J, Sampson M, Salzwedel DM, Cogo E, Foerster V, Lefebvre C. PRESS Peer Review of Electronic Search Strategies: 2015 Guideline Statement. J Clin Epidemiol. 2016;75:40-46. PubMed
17.Long HA, French DP, Brooks JM. Optimising the value of the critical appraisal skills programme (CASP) tool for quality appraisal in qualitative evidence synthesis. Res Methods Med Health Sci. 2020;1(1):31-42.
18.Brouwers MC, Kho ME, Browman GP, et al. AGREE II: advancing guideline development, reporting, and evaluation in health care. Prev Med. 2010;51(5):421-424. PubMed
19.Van Not OJ, van den Eertwegh AJM, Haanen JB, et al. BRAF/MEK inhibitor rechallenge in advanced melanoma patients. Cancer. 2024;130(9):1673-1683. PubMed
20.Kähler KC, Debus D, Schley G, et al. Effectiveness, safety and utilization of cobimetinib and vemurafenib in patients with BRAF V600 mutant melanoma with and without cerebral metastasis under real-world conditions in Germany: the non-interventional study coveNIS. Melanoma Res. 2024;34(1):44-53. PubMed
21.Drago JZ, Lawrence D, Livingstone E, et al. Clinical experience with combination BRAF/MEK inhibitors for melanoma with brain metastases: a real-life multicenter study. Melanoma Res. 2019;29(1):65-69. PubMed
22.Hong AM, Waldstein C, Shivalingam B, et al. Management of melanoma brain metastases: evidence-based clinical practice guidelines by Cancer Council Australia. Eur J Cancer. 2021;142:10-17. PubMed
23.Vogelbaum MA, Brown PD, Messersmith H, et al. Treatment for brain metastases: ASCO-SNO-ASTRO guideline. Neuro Oncol. 2022;24(3):331–357. PubMed
24.NCCN Guidelines. Melanoma: cutaneous, version 2.2024. Plymouth Meeting (PA): National Comprehensive Cancer Network (NCCN); 2024: https://www.nccn.org/. Accessed 2024 Jul 23.
25.Cutaneous melanoma: a national clinical guideline. (SIGN publication no. 146). Edinburgh (UK): Scottish Intercollegiate Guidelines Network (SIGN); 2023: https://www.sign.ac.uk/media/2108/sign-146-cutaneous-melanoma-2023.pdf. Accessed 2024 Jul 23.
Authors and Contributors
Authors
Said Yousef Abdelrazeq contributed to the study’s conception and design, including data acquisition, screening, extraction, and analysis, interpretation of the results, and writing the final rapid review.
Shariq Najeeb contributed by screening studies, extracting data, analyzing, and interpreting results, figures, and tables; verifying and assessing risk of bias; and drafting and revising the report.
Shannon E. Kelly contributed to the conceptualization and design of the approach, provided research oversight, drafted portions of the report, contributed to the interpretation of results, and finalized the report in consultation with other authors.
Melissa Brouwers contributed to the study questions, protocol development, co-oversight of protocol implementation; data interpretation; drafting, editing, and refining the paper; and approval of final draft.
George A. Wells acted as the principal investigator by developing and leading the approach, and contributed to validation of results, interpretation of results, drafting, and finalizing the report.
Research Information Science
Becky Skidmore developed the search strategy in consultation with the review team; responded to PRESS feedback; translated and executed final strategies; deduped, packaged, and uploaded records to Covidence; and tracked PRISMA, provided search documentation, and wrote methods for final manuscript.
Contributors
We thank Kaitryn Campbell, MLIS, MSc (Hamilton, ON) for peer review of the MEDLINE search strategy.
Conflicts of Interest
George A. Wells disclosed the following:
VBI Vaccines Inc. (2020-Current): Coronavirus Vaccine. Data Safety Monitoring Board – Member.
Thermedical (2021-Current): Ablation system and catheter needle. Design and analysis advice for preparation of FDA Submission
VBI Vaccines Inc. (2020-Current): Coronavirus Vaccine. Design and Analysis Advice for preparation of FDA Submission
No other conflicts of interest were declared.
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Note that this appendix has not been copy-edited.
Table 2: Characteristics of Included Primary Studies
Study citation, country, funding source | Study design | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Drago et al. 201921 Country: US Funding source: NR | Retrospective cohort | Included patients: Active patients with biopsy-proven metastatic melanoma and symptomatic or active brain metastasis with BRAF V600 mutation. Date of inclusion: 2013 to 2016 Total: 65 Characteristics of symptomatic patients: Male: n = 38 (58.5%) Female: n = 27 (41.5%) Ethnic groups: European: n = 39 (60%) American: n = 26 (40%) Previous treatment:
| Intervention:
Comparator: None | Outcomes:
Follow-up: Median 19 months (95% CI 16 to 31) Subgroups by overall survival are also reported |
Kahler et al.202320 Country: Germany (30 sites) Funding source: Rocha Pharma, Germany | Prospective cohort | Inclusion criteria: Adult patients with histologically confirmed unresectable or MBM with a BRAF V600 mutation who received cobimetinib and vemurafenib according to the German label and summary of product characteristics. Study duration: 2017 to 2021 Total: 95 Characteristics of symptomatic patients (n = 19 [46.3%] of 41 patients with MBM) Male: NR Female: NR Ethnic groups: NR Previous treatment: NR | Intervention: Cobimetinib and vemurafenib Comparator: None | Outcomes:
Follow-up: 18 months posttreatment |
Van Not et al. 202419 Country: The Netherlands Funding source: None | Retrospective cohort (from patient registry) | Inclusion criteria: NR Date of inclusion: 2013 to 2022 Total: 468 Characteristics of symptomatic patients: Groups: Initial BRAF and MEK inhibitor therapy, n = 84 (17.9%) Retreatment with BRAF and MEK inhibitor, n = 151 (32.3%) Second retreatment, n NR Male: NR Female: NR Ethnic groups: NR Previous treatment: NR | Intervention: BRAF and MEK inhibitor combinations Comparator: None | Outcomes:
|
CI = confidence interval; CTL4 = Cytotoxic T-lymphocyte associated protein 4; MBM = melanoma brain metastasis; NR = not reported; PD-L1 = Programmed Death-Ligand 1.
aNot reported for symptomatic patients.
bName of drugs not reported.
cOnly descriptive outcomes reported.
Table 3: Characteristics of Included Evidenced-Based Guidelines
Intended users, target population | Intervention and practice considered | Major outcomes considered | Evidence collection, selection, and synthesis | Evidence quality assessment |
|---|---|---|---|---|
NCCN Clinical Practice Guidelines in Oncology: melanoma: cutaneous (Updated 2024)24 | ||||
Intended users: Oncologists and other health care professionals, health care institutions, insurance companies, and payers Target population: Patients with cutaneous melanoma, with and without metastases | Intervention: Any type of chemotherapy, immunotherapy, targeted drug therapy, surgery, radiation therapy, best supportive care, and surveillance | Overall survival, progression-free survival, objective response rate, intra- and extracranial response, and safety | PubMed literature searches to obtain key literature before creation or annual update of guidelines. No systematic review method reported | Evidence quality assessed using NCCN categories |
ASCO-SNO-ASTRO Guideline: treatment for brain metastases (updated 2023)23 | ||||
Intended users: Surgeons, oncologists, neurologists, and other health care providers engaged in caring for the target population Target population: Patients with brain metastases from cancer from nonhematologic solid tumours | Intervention: Any type of chemotherapy, immunotherapy, targeted drug therapy, surgery, radiation therapy, best supportive care, and surveillance | Overall survival, progression-free survival, objective, response rate, intra- and extracranial response, safety, and other outcomes | A comprehensive systematic review conducted with an appropriate PICO | Evidence graded according to the risk of bias within the reporting publication, clinical experience, and consensus |
Cancer Council Australia (CCA): management of melanoma brain metastases (2020)22 | ||||
Intended users: Oncologists and other health care professionals who manage patients with melanoma Target population: Patients with advanced melanoma brain metastases in Australia | Intervention: All types of systemic drug therapy reported in literature | Progression-free survival, overall survival, and intra- and extracranial response | Systematic and nonsystematic literature search carried out to find relevant literature. Wiki Platform used to support critical appraisal, data extraction, evidence assessment, and summary processes | GRADE approach used to rate evidence certainty as high, moderate, low, and very low |
SIGN146: cutaneous melanoma (2023)25 | ||||
Intended users: Primary care providers, dermatologists, surgeons, pathologists, oncologists, public health physicians, and other health care professionals Target population: Adult patients with all stages of cutaneous melanoma, including metastatic cutaneous melanoma | Interventions: Combination therapy using encorafenib with binimetinib or trametinib with dabrafenib. Interventions compared with any immunotherapies and targeted therapies, localized treatments for patients with locoregional disease | Progression-free survival, overall survival, and safety | A systematic review of the literature was carried out using an explicit search strategy devised by an information scientist. Databases searched included MEDLINE, Embase, Cinahl, PsycINFO, and the Cochrane Library. The year range covered: 2004 to 2016; updated in 2022. | Graded evidence according to the type of study reporting the treatment outcome and potential sources of bias within |
ASCO = American Society of Clinical Oncology; ASTRO = American Society for Radiation Oncology; CCA = Cancer Council Australia; GRADE = Grading of Recommendations, Assessment, Development and Evaluation; NCCN = National Comprehensive Cancer Network; PICO = Participants Intervention Control Outcome; SIGN = Scottish Intercollegiate Guidelines Network; SNO = Society for Neuro-Oncology.
Appendix 3: Critical Appraisal
Note that this appendix has not been copy-edited.
Table 4: Summary of the Critical Appraisal of Included Primary Studies Using the CASP Tool
Strengths | Limitations |
|---|---|
Drago et al. 201921 | |
|
|
Kahler et al. 202320 | |
|
|
Van Not et al. 202419 | |
|
|
CASP = Critical Appraisal Skills Programme; MBM = melanoma brain metastasis
Table 5: Summary of the Critical Appraisal of Included Evidence-based Guidelines Using the AGREE II Tool
Guidelines | Rigour of development (%) | Editorial independence (%) |
|---|---|---|
NCCN Guideline 202424 | 57 | 50 |
ASCO-SNO-ASTRO Guideline 202323 | 87 | 79 |
CCA Guideline 202022 | 54 | 85 |
SIGN Guideline 202325 | 97 | 100 |
AGREE II = Appraisal of Guidelines for Research and Evaluation II; ASCO = American Society of Clinical Oncology; ASTRO = American Society for Radiation Oncology; CCA = Cancer Council Australia; NCCN = National Comprehensive Cancer Network; SIGN = Scottish Intercollegiate Guidelines Network; SNO = Society for Neuro-Oncology
Appendix 4: Outcomes of Included Reports
Note that this appendix has not been copy-edited.
Table 6: Outcomes Reported in the Primary Studies
Outcomea | Drago et al. 201921 | Kahler et al. 202320 | Van Not et al. 202419 |
|---|---|---|---|
Progression-free survival | |||
Progression-free survival | Median 5.3 months (95% CI, 3.6 to 6.1) | Median 5.2 months (95% CI, 1.9 to 8.3)a | NR |
Progression-free survival following rechallenge with BRAF and MEK | NR | NR | HR 1.44 (95% CI, 1.08 to 1.94)b |
Overall survival | |||
Overall survival | Median 9.5 months (95% CI, 7.7 to 13.5)c | Median 7.4 months (95% CI, 2.6 to 16.0)a | NR |
Subgroups reported for overall survival | Age > 49 compared to age < 49: HR 2.18 (95% CI, 1.09 to 4.37) High-risk location compared to lower risk location of primary lesion: HR 3.32 (95% CI, 1.48 to 7.46) Nodular melanoma compared to superficial spreading melanoma: HR 4.95 (95% CI, 1.92 to 12.75) | NR | NR |
Mortality | |||
Mortality at study close | 45/65 (69%) | NR | NR |
Response leading to drug dose reduction or discontinuation | |||
Response leading to steroid dose reduction | 22/33 (66.7%) | NR | NR |
Response leading to steroid discontinuation | 11/33 (33.3%) | NR | NR |
Response leading to anticonvulsant dose reduction | 4/21 (19%) | NR | NR |
Response leading to anticonvulsant discontinuation | 0/21 (0%) | NR | NR |
Response leading to opioid dose reduction | 4/12 (33%) | NR | NR |
Response leading to opioid discontinuation | 4/12 (33%) | NR | NR |
Disease progression | |||
No progression at study close | 7/65 (10.8%) | NR | NR |
Progression at study close | 57/65 (87.7%) | NR | NR |
Unknown progression at study close | 1/65 (1.5%) | NR | NR |
CI = confidence interval; HR: hazard ratio; MBM = melanoma brain metastasis; NR = not reported.
aData only presented for patients with symptomatic MBM an exploratory post hoc result.
bData for HR were reported with little descriptive context for symptomatic patients with MBM (Refer to Figure 2 and page 1678).
cMultivariate analysis revealed that overall survival was significantly related to age, location, and type of melanoma. Patients older than 49 years had hazards of death that were more than double those of patients younger than 49 years (HR = 2.18, 95% CI, 1.09 to 4.37; P = 0.03).
dThis study only reported a descriptive outcome for symptomatic MBM. No quantitative outcomes for these patients were reported.
Table 7: Summary of the Adverse Event Outcomes for Symptomatic MBM Reported in the Included Primary Studies
Adverse event (n/N, %) | Drago et al. 201921 | Kahler et al. 202320 | Van Not et al. 202419,a |
|---|---|---|---|
Fever | 13/65 (20%) | 8/41 (19%)b | NR |
Fatigue | 7/65 (10.8%) | 9/41 (22%)b | NR |
Rash | 9/65 (13.8%) | 5/41 (12.2%)b,c | NR |
Dizziness | 1/65 (1%) | NR | NR |
CNS bleeding | 1/65 (1%) | NR | NR |
Myocardial infarction | 1/65 (1%) | NR | NR |
Creatinine kinase increase | 6/65 (9.2%) | NR | NR |
Hypertension | 2/65 (3.1%) | NR | NR |
Liver-related SAEs | 4/65 (6.2%) | NR | NR |
Diarrhea | 5/65 (7.7%) | 15/41 (36.6%)b | NR |
Infection | 5/65 (7.7%) | NR | NR |
Palpitation | 2/65 (3.1%) | NR | NR |
Venous thrombosis | 3/65 (4.6%) | NR | NR |
Nausea | 2/65 (3.1%) | NR | NR |
Alopecia | 1/65 (1.5%) | NR | NR |
Ocular complications | 1/65 (1.5%) | NR | NR |
Acute kidney SAE | NR | 3/41 (7.3%)b | NR |
Patients discontinuing drugs | 10/65 (20.8%) | NR | NR |
AEs leading to discontinuation | Fever (8/65, 12.3%) Abnormal LFTs (2/65, 3%) | 24/41 (58.5%)b,d | Toxicity: First BRAF and MEK (78/468, 16.7%) BRAF and MEK rechallenge (43/468, 9.2%) |
Total experiencing an AE | NR | 36/41 (87.8%)b | NR |
AE ≥ grade 3 | NR | 30/41 (73.2%)b,e | NR |
Any SAE | NR | 29/41 (70.7%)b | NR |
AE = adverse event; CNS = central nervous system; SAE = severe adverse event; LFT = liver function tests; NR = not reported
aSafety data includes entire study population.
bSafety data includes entire Cohort B population.
cAll were Cohort B patients taking cobimetinib and vemurafenib.
dIncludes 5 patients with diarrhea, 5 with pyrexia, 3 with fatigue, and 3 with nausea. Treatment discontinuation may have been temporary or permanent.
eIncludes 4 patients in Cohort B who died. Other SAEs were pyrexia (9.8%), acute kidney injury and seizure (both 7.3%).
Table 8: Description of the Recommendations and Their Supporting Evidence for the Management of Treatment of Patients With Symptomatic Melanoma Brain Metastasis Reported in Guidelines
Recommendations and supporting evidence | Strength of recommendations and quality of evidence |
|---|---|
NCCN Clinical Practice Guidelines in Oncology: melanoma: cutaneous (Updated 2024)24 | |
”Limited data supporting the efficacy of upfront systemic therapy in patients with symptomatic brain metastases, and brain-directed therapy is generally preferred.” ”Surgery is the preferred option for large, symptomatic lesions or single lesions in resectable areas, particularly when there is diagnostic uncertainty or when additional tissue sampling may drive future therapeutic decisions.” Evidence: Based on consensus. | Strength: Weak Quality: Low |
ASCO-SNO-ASTRO Guideline: treatment for brain metastases (Updated 2023)23 | |
”Patients with symptomatic brain metastases should be offered local therapy (radiosurgery and/or radiation therapy and/or surgery) as recommended in this guideline regardless of the systemic therapy used for the systemic disease.” Evidence: Randomized controlled trials. | Strength: Strong Quality: High |
Cancer Council Australia (CCA): management of melanoma brain metastases (2020)22 | |
”Brain metastases that are symptomatic or generate mass effect at presentation are best treated with surgery. – based on expert opinion and formulated by a consensus process.” Evidence: Based on expert opinion | Strength: Weak Quality: Low |
SIGN146: cutaneous melanoma (2023)25 | |
No specific recommendations for patients with symptomatic melanoma brain metastases provided. | Not applicable. |
ASCO = American Society of Clinical Oncology; ASTRO = American Society for Radiation Oncology; CCA = Cancer Council Australia; NCCN = National Comprehensive Cancer Network; SIGN = Scottish Intercollegiate Guidelines Network; SNO = Society for Neuro-Oncology.
ISSN: 2563-6596
This rapid review was conducted by the POst-Market Drug Evaluation Team (PODET) team through the through the Post-Market Drug Evaluation CoLab Network. This work was supported by Canada’s Drug Agency (CDA-AMC) and its Post-Market Drug Evaluation Program through funding provided by Health Canada.
CDA-AMC is a pan-Canadian health organization. Created and funded by Canada’s federal, provincial, and territorial governments, we’re responsible for driving better coordination, alignment, and public value within Canada’s drug and health technology landscape. We provide Canada’s health system leaders with independent evidence and advice so they can make informed drug, health technology, and health system decisions, and we collaborate with national and international partners to enhance our collective impact.
CoLab is a pan-Canadian network of experts in applied research, scientific methods, and data analysis. CoLab members work with the Post-Market Drug Evaluation Program to produce credible and timely evidence on postmarket drug safety and effectiveness.
Disclaimer: CDA-AMC has taken care to ensure that the information in this document was accurate, complete, and up to date when it was published, but does not make any guarantee to that effect. Your use of this information is subject to this disclaimer and the Terms of Use at cda-amc.ca.
The information in this document is made available for informational and educational purposes only and should not be used as a substitute for professional medical advice, the application of clinical judgment in respect of the care of a particular patient, or other professional judgments in any decision-making process. You assume full responsibility for the use of the information and rely on it at your own risk.
CDA-AMC does not endorse any information, drugs, therapies, treatments, products, processes, or services. The views and opinions of third parties published in this document do not necessarily reflect those of CDA-AMC. The copyright and other intellectual property rights in this document are owned by the Canadian Agency for Drugs and Technologies in Heath (operating as CDA-AMC) and its licensors.
This document is the property of PODET. CDA-AMC has a nonexclusive, limited, royalty-free, worldwide, nontransferable, fully paid-up, and irrevocable license to use the report in support of its objects, mission, and reasonable operational requirements.