CADTH Health Technology Review
Continuous Diffused Oxygen Therapy for Wound Healing
Rapid Review
Key Messages
What Is the Issue?
Wounds are prevalent across health care settings, costing Canada an estimated $12 billion per year in wound care. Chronic wounds (wounds that do not heal in the typical amount of time, which can depend on the size and type of wound) can have a significant impact on a patient’s quality of life and health.
Healing tissue has a high need for oxygen. Oxygen can be delivered in several ways, including topical oxygen therapy, which delivers oxygen directly to the wound. One type of topical oxygen therapy is continuously diffused oxygen (CDO) therapy, which uses a device that takes oxygen from the air and then delivers pure, humidified oxygen to the wound.
We previously completed a Rapid Review on CDO therapy for wounds in 2020. This review aimed to determine if new evidence has since been published on this topic.
What Did We Do?
To inform decisions about CDO therapy for wound healing, we sought to identify and summarize literature comparing the clinical effectiveness and cost-effectiveness of CDO therapy versus conventional wound care. We also attempted to identify evidence-based recommendations for the use of CDO therapy.
We searched key resources, including journal citation databases, and conducted a focused internet search for relevant evidence published since 2019. One reviewer screened articles for inclusion based on predefined criteria, critically appraised the included studies, and narratively summarized the findings.
What Did We Find?
CDO therapy appears to be clinically effective for treating patients with diabetic foot ulcers, particularly chronic or hard-to-heal ulcers that have not responded to standard care. Rates of adverse events were comparable between patients receiving CDO and patients receiving standard care. Two cost-effectiveness studies reported that CDO is likely to be cost-effective compared to standard care for patients with chronic, hard-to-heal diabetic foot ulcers.
We identified fewer studies for other types of wounds. Preliminary evidence suggests that CDO therapy may be helpful for patients with other types of wounds that are chronic or have not responded to standard care. Reporting on adverse events was limited.
Limited evidence suggests that patients receiving CDO therapy had better outcomes if their wound was debrided more frequently as well as if they received CDO therapy for a longer time.
The evidence-based guidelines recommend the use of topical oxygen therapy (of which CDO is a subtype) for treating diabetic foot ulcers that have failed to heal with standard care. One guideline suggested that topical oxygen therapy may be considered for other types of non-neoplastic, hard-to-heal wounds.
We did not find cost-effectiveness evidence for wounds other than diabetic foot ulcers that met the inclusion criteria for our report. We also did not identify any clinical effectiveness or cost-effectiveness evidence, or any guidelines regarding the use of CDO to treat First Nations, Inuit, and Métis patients, that met the inclusion criteria for our report.
What Does This Mean?
CDO therapy may be beneficial and more cost-effective than standard care for patients with hard-to-heal, chronic diabetic foot ulcers that have not responded to standard care. Evidence-based guidelines also recommend the use of CDO therapy for this patient population.
The clinical effectiveness and cost-effectiveness of CDO therapy for other types of wounds is still unclear. It is also unclear if there is an optimal way to provide CDO (e.g., oxygen flow rate, debridement, length of treatment).
We identified limited evidence that reported on patient ethnicity. Considering that some groups, including First Nations, Inuit, and Métis Peoples, have higher rates of diabetes than the overall population in Canada — which may lead to higher rates of diabetic foot ulcers — decision-makers involved in implementing CDO therapy should consider ways to ensure equitable access for all patients who may need this treatment.
Abbreviations
CDO
continuously diffused oxygen
HTA
health technology assessment
NPWT
negative pressure wound therapy
NRS
nonrandomized study
QALY
quality-adjusted life-year
RCT
randomized controlled trial
SR
systematic review
TPOT
topical pressurized oxygen therapy
Context and Policy Issues
The Impact and Cost of Wounds
Wounds are prevalent across health care settings, impacting patients, health care providers, and the health care system. A study based on Canadian Institute for Health Information data from 2011 to 2012 reported an estimated 28.2% of patients with continuing complex care had potentially preventable wounds, particularly chronic wounds (15.8%).1 The prevalence across other settings included 9.6% in long-term care, 7.3% in home care, and 3.7% in acute care. However, the authors also noted this is an underestimate as the data did not capture all wounds.1 In Ontario, 30% to 50% of service delivery includes acute and chronic wound care.2 Recent reports estimate that the cost of wound care in Canada is approximately $12 billion per year.3 However, this estimate is from the perspective of the health system and focuses on the direct costs of care and not the indirect costs (e.g., to patients and their carers and/or families). The report also notes the difficulty of accurately estimating the costs of chronic wounds.3
Chronic wounds are wounds that do not go through the typical sequence of repair or do not heal in the typical amount of time.4,5 This may be because the wounds are closing very slowly, are reopening, or are not healing due to impaired physiological processes; this may be caused by conditions like poor blood flow or diabetes. A wound may be considered chronic if it does not heal within 4 to 12 weeks despite treatment4,5 or if surface area of the wound does not reduce by approximately 15% weekly or 50% over a 1-month period.6 Chronic wounds can impact a patient’s quality of life (e.g., pain, poor sleep due to pain, depression), lead to infection, or require amputation.4,5
Caring for Wounds
Currently, standard wound care involves ensuring the wound is dressed, cleaned regularly, and debrided (removing materials like scabs, necrotic materials, infected tissues, pus, and other impurities that may delay wound healing) as needed.7,8 Adjunct treatments may be also used to aid wound healing, such as delivering oxygen. Healing tissue has a high need for oxygen and nutrients for processes like forming new blood vessels (neovascularization), collagen deposition, and resisting infection.9
Oxygen can be delivered in several ways. Hyperbaric oxygen therapy involves having patients breathe in 100% oxygen, and it has been shown to be beneficial for some conditions; however, it also can cause adverse events such as oxygen toxicity and damage to surrounding tissue (i.e., around the wound).9-11
What Is CDO Therapy?
An alternative to hyperbaric oxygen is topical oxygen therapy, which provides localized oxygen directly to the wound.6 There are several categories of topical oxygen therapy, including topical pressurized oxygen therapy (TPOT) and topical continuous oxygen therapy, which is also known as continuously diffused oxygen (CDO) therapy.11 TPOT uses a chamber or bag that encloses the wound while enriched oxygen (87% to 93%) is administered into the chamber or bag using a respiratory oxygen concentrator. TPOT requires the patient to be immobile during treatment (typically 90 minutes). In CDO therapy, a device takes oxygen from room air and electrochemically converts it to pure, humidified oxygen, which is then continuously delivered to the wound using an oxygen diffusion dressing to ensure even delivery of oxygen across the wound.11 CDO devices are wearable, silent, and compact, allowing patients to engage in daily activities while being treated.12,13
Why Is It Important to Do This Review?
We previously published a Rapid Review on the use of CDO for wound healing in 2020, which identified 1 systematic review (SR), 3 randomized controlled trials (RCTs), and 1 guideline.14 The identified evidence indicated that CDO is safe and most effective for patients with diabetic foot ulcers and limited comorbidities, with limited evidence (2 case series identified by the SR) indicating it is effective for patients with other chronic wounds. The guideline recommended against topical oxygen therapy as a primary or adjunctive intervention for diabetic foot ulcers; the strength of the recommendation was weak, and the evidence was graded as low-quality. The previous report also did not identify evidence related to the cost-effectiveness of CDO for wound healing. Overall, it concluded that further studies were needed, including on patients with chronic wounds other than diabetic foot ulcers.14
We prepared this report to identify new evidence that has been published since the previous report. Best practice-based wound care may help to improve patient outcomes as well as save health care costs.15
Objective
To support decision-making regarding the use of CDO therapy, we prepared this Rapid Review to summarize and critically appraise clinical studies, economic evaluations, and evidence-based guidelines on its use for wound healing.
Additional details of the methods used for this report are presented in Appendix 1.
Research Questions
What is the clinical effectiveness of CDO therapy compared with conventional wound care?
What is the cost-effectiveness of CDO therapy?
What are the evidence-based guidelines regarding the use of CDO therapy?
Methods
Literature Search Methods
An information specialist conducted a customized literature search, balancing comprehensiveness with relevancy, of multiple sources and grey literature on June 20, 2024. One reviewer screened citations, selected studies based on the inclusion criteria presented in Table 1, and critically appraised included publications using established critical appraisal tools.
Appendix 1 presents a detailed description of the methods.
Criteria | Description |
|---|---|
Population | Individuals with wounds. Subpopulations of interest:
|
Intervention | CDO therapy |
Comparator | Conventional wound care |
Outcomes |
|
Study designs | HTAs, SRs, RCTs, NRSs, economic evaluations, evidence-based guidelines |
Publication date | Since January 1, 2019 |
CDO = continuously diffused oxygen; HTA = health technology assessment; NRS = nonrandomized study; QALY = quality-adjusted life-year; RCT = randomized controlled trial; SR = systematic review.
Summary of Evidence
Quantity of Research Available
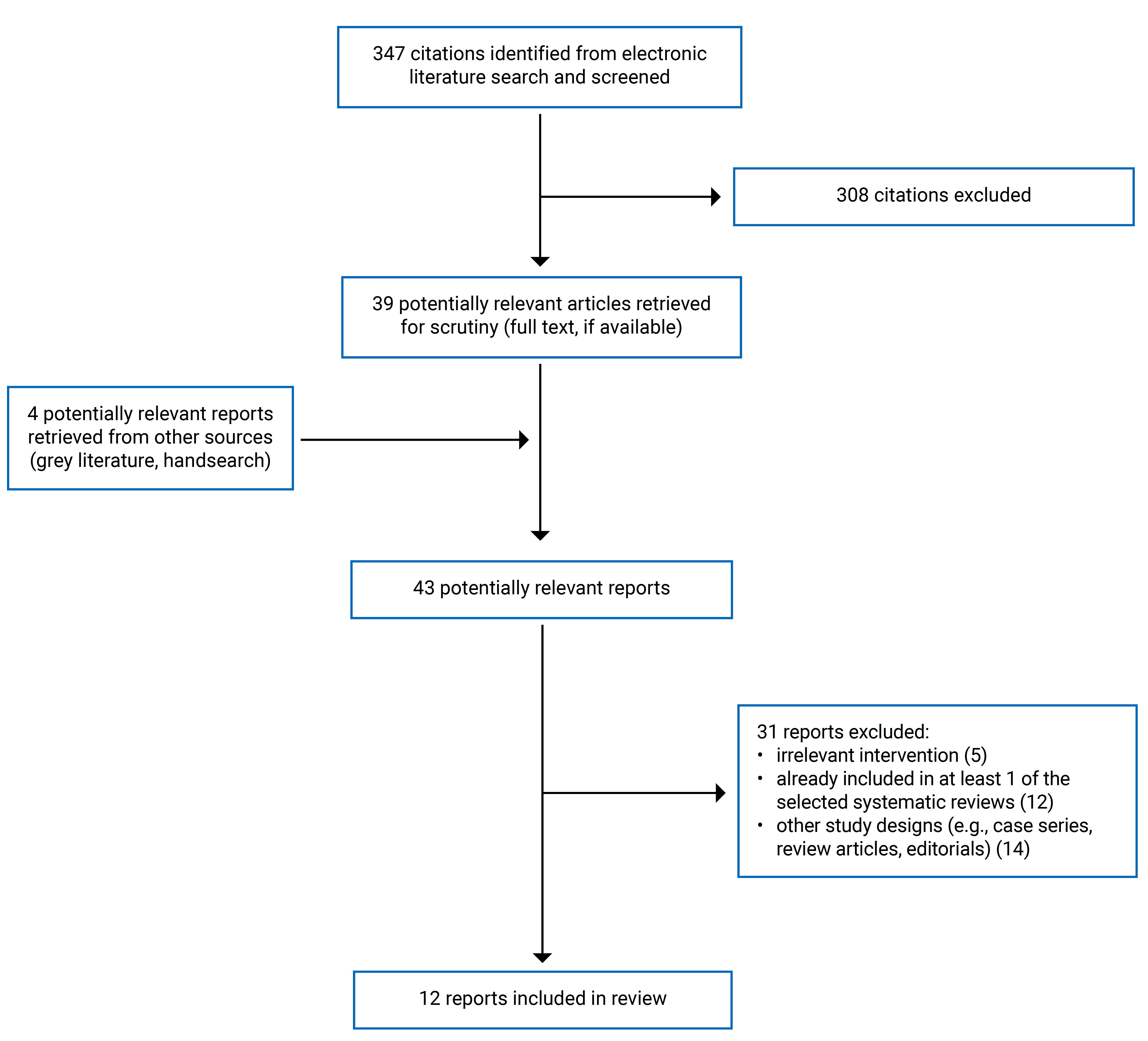
A total of 347 citations were identified in the literature search. Following screening of titles and abstracts, 308 citations were excluded and 39 potentially relevant reports from the electronic search were retrieved for full-text review. Four potentially relevant publications were retrieved from the grey literature search for full-text review. Of these potentially relevant articles, 31 publications were excluded for various reasons, and 12 publications met the inclusion criteria and were included in this report. These comprised 1 health technology assessment (HTA) which included 1 SR and 1 economic evaluation,16 1 scoping review,17 2 SRs,7,18 1 RCT,19 3 nonrandomized studies (NRSs),20-22 and 4 evidence-based guidelines.23-26
Appendix 1 presents the PRISMA27 flow chart of the study selection. Additional references of potential interest are provided in Appendix 7.
Summary of Study Characteristics
We identified 1 HTA (which included 1 SR and 1 economic evaluation),16 1 scoping review,17 2 SRs,7,18 1 RCT,19 3 NRSs,20-22 and 4 evidence-based guidelines.23-26 The scoping review17 and 1 SR18 had broader inclusion criteria than the current report: the scoping review17 included topical oxygen therapy in general, while the SR18 covered interventions to assist with healing of chronic diabetic foot ulcers. Only the characteristics and results of the subset of relevant studies will be described in this report.
Additional details regarding the characteristics of included publications are provided in Appendix 3.
Included Studies for Clinical Effectiveness
The HTA16 and scoping review17 were conducted in the UK, while the SRs were conducted in Australia18 and the US.7 The SR from the HTA16 included studies from Canada, China, France, Germany, Israel, the UK, and the US as well as multinational studies; it included 2 SRs, 4 RCTs, and 2 NRSs. The scoping review17 and 2 SRs7,18 did not report where their included primary studies were conducted. The scoping review17 identified 6 SRs and 12 primary clinical studies. One SR7 was also focused on CDO and included 10 RCTs and 12 NRSs, while another SR18 identified 7 RCTs relevant to this report. There was some overlap in the primary studies included in the reviews; the overlap table is available in Appendix 6. We also identified 1 RCT19 and 3 NRSs20-22 that were not covered by the reviews: the RCT19 and 2 NRSs21,22 were conducted in the US, while 1 NRS20 was conducted in Singapore.
The intervention of interest was CDO, which was also referred to as continuous topical oxygen therapy; where reported, the duration of treatment ranged from 3 weeks to more than 25 weeks, using a flow rate from 3 mL/h to 15 mL/h. One study19 had 2 CDO groups: 1 group had their wounds covered by a film, while the other group had their wounds covered by a silicone sheet. Comparators included standard care,7,16-19 pre-post comparisons,7,17,20,21 or placebo.7,22 Some reviews did not clearly describe the control groups of the included studies.7,17
Across studies, populations included people with any type of wounds;7,17 people with diabetic foot ulcers;18,20,21 people with chronic, nonhealing, and complex wounds;16 and people undergoing bilateral reduction mammoplasty (i.e., a surgical wound).19 The scoping review17 included patients with any wounds, but all articles relevant to this report were focused on patients with diabetic foot ulcers. Recognizing that gender is a spectrum, when the terms “men” or “women” were used in the included studies, we retained these terms in reporting on these studies. Reported mean ages ranged from 33 years to 76 years, with 0% to 82% of patients reported as male; articles did not report how sex or gender were defined or measured or report on sex or genders outside male and female. Three primary studies reported on ethnicity.19-21
Reported clinical effectiveness outcomes by the SRs and primary studies included:
complete wound healing (e.g., proportion of wounds healed or proportion of patients whose wound healed)7,16,20-22
change in wound size or partial healing (e.g., wounds less than 90% healed, change in wound size in cm2)7,16,20,21
score on the Pressure Ulcer Scale for Healing (PUSH) scale, a validated tool for monitoring foot ulcer healing that measures wound size, exudates, and tissue type7,28
scar length17
amputations16
ulcer recurrence rates (e.g., wounds emerging in the same area as the previously treated wound) or proportion of wounds that stay closed7,16,20
pain, measured by validated scales like the visual analogue scale (VAS)28 or the Diabetic Foot Ulcer Scale-Short Form,29 or general scales (e.g., on a scale of 1 to 10)7,16,20
Included Studies for Cost-Effectiveness
The SR from the HTA16 included economic evaluations and identified 1 relevant study; the authors of the review also conducted their own economic evaluation. The identified study by Chan and Campbell was a microsimulation model with a time horizon of 5 years and the perspective of a public payer (Ontario Ministry of Health). The economic evaluation conducted by Health Technology Wales was a Markov model with a time horizon of 50 years from the perspective of the UK National Health Service and personal social services.16
Both models looked at patients with hard-to-heal or nonhealing diabetic foot ulcers; in the model by Health Technology Wales, the simulated patients had an average age of 58.20 years and 24% were female.16 Both models used 6 health states (healed ulcer, diabetic foot ulcer, infected ulcer, minor lower leg amputation, major lower leg amputation, and death), though Chan and Campbell used a 1-year cycle and Health Technology Wales used a 1-month cycle.16 Both models assessed 12 weeks of CDO compared to standard care; the model by Chan and Campbell also compared CDO to negative pressure wound therapy (NPWT), moist wound therapy, and offloading. Reported outcomes included quality-adjusted life-years (QALYs), life-years, and costs per person.16
Key assumptions in the model by Health Technology Wales included that patients had received treatment 12 weeks before model initiation and patients who had previously had an amputation also were at risk of reamputation.16 Key assumptions in the model by Chan and Campbell included that clinical data from 2 primary studies had similar populations, that results from a US clinical trial were similar to what would occur in Canada, and that there are no additional benefits to CDO treatment after 12 weeks of treatment.16
Included Evidence-Based Guidelines
We identified 4 evidence-based guidelines that provided recommendations regarding the use of topical oxygen therapy for wounds; there were no guidelines or recommendations specific to CDO. All were developed by a working group or expert panel.
Two guidelines23,25 were classified as international: the guideline from the International Working Group on the Diabetic Foot23 had a working group with members from the US, the Caribbean, Europe, Asia, and Australia, while the other guideline25 included an expert panel with members from the US and Europe. These guidelines thus may be intended to be used internationally. One guideline was from the Wound Healing Society24 and another was from the American Diabetes Association;26 as both associations are based in the US, they may be intended to apply to the US.
Three guidelines23,24,26 were focused on people with diabetes and provided guidance for treating diabetic foot ulcers. One guideline25 included patients with wounds in general, including diabetic foot ulcers and other types of hard-to-heal wounds.
Summary of Critical Appraisal
Additional details are provided in Appendix 4.
Scoping Reviews and SRs
All the reviews, including the SR from the HTA as well as the scoping review, stated their objective, the population, and the interventions of interest; all also provided their search strategy, searched multiple databases, and reported the funding source for the review.7,16-18 All except the scoping review reported risk of bias of the included studies,7,16,18 though 116 did not state what tool they used. Two SRs7,18 stated that articles were assessed for inclusion by 2 reviewers and 1 reviewer conducted data extraction. In the scoping review,17 1 person reviewed the articles, but it was unclear how many reviewers were involved in data extraction. In the SR from the HTA, it was not reported how many reviewers were involved in screening or data extraction.16 One SR7 conducted meta-analyses and provided pooled estimates separately for double-arm and single-arm studies; however, they did not explain their choice of model and did not provide pooled results of RCTs only. One SR18 reported registering the protocol in advance; it was unclear if this was done for the other 3 reviews.
None of the included reviews reported on sources of funding for included studies. It is unclear how many of these studies may have been funded by the device manufacturer and if that may have influenced the reporting. It is also unclear if any of the reviews searched grey literature, which may have resulted in some relevant literature being excluded.
Primary Clinical Studies
All primary clinical studies described their objective, main outcomes, patient characteristics, and intervention.19-22 The staff and facilities may also have been representative of typical care for patients.19-22
The RCT19 reported withdrawal rates with rationales. One NRS20 reported that 5 patients discontinued the intervention and provided rationales; analyses appear to include all patients. It is unclear from the remaining 2 NRSs21,22 if any patients were lost to follow-up or discontinued treatment. The RCT19 did not blind patients or staff, but this may have had limited influence on the outcome of interest for this report (wound dehiscence or reopening of the surgical wound). None of the NRSs described confounders; thus, it is unclear if their findings may have been influenced by other noncontrolled factors. Although the RCT and 2 NRSs provided details about patient characteristics, no analyses were presented regarding associations between characteristics and outcomes, perhaps due to the relatively small sample sizes. Thus, it is unclear if certain patient characteristics may influence healing with CDO.
Adverse events are presented in 1 NRS20. The authors of the RCT19 did not present adverse events in their analyses, but they noted that some patients discontinued the intervention due to allergies or noncompliance. Limited reporting of adverse events makes it unclear if the intervention may result in any unintended side effects, particularly for patients who are older and thus may be more susceptible to adverse events.
All primary clinical studies disclosed their funding source: the RCT19 and 2 NRSs21,22 were funded by a manufacturer of CDO devices, while 1 NRS20 was funded by a local distributer of a CDO device and stated that the CDO devices were provided at a heavily subsidized price. The RCT19 stated their report does not necessarily represent the official views of the funder, and 1 NRS20 also confirmed the funding source did not impact the study design or execution. Two NRSs21,22 did not state if the funding source had any influence on study design or execution.
Economic Evaluations
For the economic evaluation conducted by Health Technology Wales as well as the cost-effectiveness study identified by that SR (Chan and Campbell), both reported their objective, the model’s viewpoint, the time horizon, and the sources of data.16 Both also conducted sensitivity analyses. The economic evaluation by Health Technology Wales did not provide a justification for the discount rate used and did not report quantities of events; only annual and per-event costs were reported. The authors based their clinical inputs on studies identified from a meta-analysis as well as a more recent primary study, but they did not describe how they chose the weights for each study. The study by Chan and Campbell used 2 trials for clinical inputs, with 1 comparing CDO to standard care and the other comparing NPWT to standard care; both studies assessed patients with diabetic foot ulcers, and it was assumed their cohorts were similar. The model inputs also used US clinical data when Canadian data were unavailable, but the US data may not be applicable to a Canadian context.
Evidence-Based Guidelines
All identified guidelines23-26 were clear regarding their scope, purpose, and target users; in all, the guideline authors clearly presented their recommendations, described their methods of formulating recommendations, and appeared to be editorially independent. Three guidelines23,24,26 were developed by a group of individuals from various professions, used systematic search methods to search for evidence, and clearly described the strengths and limitations of the evidence; it was unclear if 1 guideline25 met these criteria. In 3 guidelines,23,25,26 the authors indicated that they sought views of the target population. Two guidelines were externally reviewed before publication, and a procedure for updating them was provided.23,26
All guidelines23-26 provided recommendations regarding the use of topical oxygen therapy. CDO is a subtype of topical oxygen therapy, and thus it is assumed these recommendations also apply to CDO. However, guidance was limited regarding details of how to provide treatment, such as the use of debridement or recommended oxygen flow rates.
Summary of Findings
There was some overlap in the primary studies that were included in the SRs; therefore, to avoid duplication of results, outcome data from an individual primary study are only reported once. Some SRs only presented meta-analyses results, which in some cases had overlapping primary studies. Appendix 5 presents the main study findings, with details regarding overlapping studies.
Clinical Effectiveness of CDO Therapy Versus Conventional Wound Care
Patients With Diabetic Foot Ulcers
Patients with diabetic foot ulcers who received CDO tended to show better results compared to standard care, including:
greater reduction in wound size16 — though the authors of the 1 identified RCT reported that their intention-to-treat analysis was not statistically significant, which may have been due to high levels of patient withdrawal.
Two noncomparative studies reported partial wound closure: in 1, 53% of wounds had healed by at least 50% after 3 weeks,21 and in another, 70% of wounds had healed by at least 75% after 12 weeks.20
Patients with more severe diabetic foot ulcers may also be more likely to benefit from CDO — in 2 studies,16,20 more patients with grade 2 and 3 ulcers (based on the University of Texas Classification scale) in the CDO group healed compared to patients in the standard care group.
Patients whose wounds are debrided more often may have better clinical outcomes. We identified 1 multicentre NRS22 assessing the impact of CDO on patients with diabetic foot ulcers, and whereas most sites debrided at almost all visits, 1 site debrided at less than half of patient visits. The relative efficacy of CDO versus placebo was 240% when only sites with high debridement were included (i.e., when the 1 site with low debridement was excluded), which is higher than the overall rate with all sites included (204%).
Overall, adverse event rates were low for both the CDO and control groups. Reported adverse events included:
Mortality: 2 RCTs from 1 SR16 reported few deaths, with all stated as unrelated to the intervention; 1 NRS20 reported no deaths.
Amputation rates: 2 of 3 studies identified in 1 SR16 had few amputations; 1 RCT (N = 120) reported that 12.5% (CDO plus standard care) and 15% (moist wound dressing therapy plus standard care) of patients had an amputation. However, none of the patients receiving CDO plus moist wound care plus standard care had an amputation. This effect was reported as statistically significant, though further research may be required to determine if other factors contributed to this high amputation rate.
Wound recurrence (or reopening): No wound recurrence was reported in 2 trials,16,20 while in 1 trial,19 a few patients were reported to have experienced wound recurrence. The proportion of patients whose wound stayed closed was high for both the CDO and standard care groups in 2 studies identified by 1 SR16 and the difference was not statistically significant.
Self-reported pain: the CDO and control groups tended to both report reduced pain.7,16 In a single-arm study, the change in pain for patients receiving CDO was reported to be statistically significant.20 However, in studies that compared CDO to a control group, there was no statistically significant difference between groups on change in reported pain.7,16
General and other adverse events (e.g., infection): Rates were low and tended to be similar between the CDO and control groups, with reported differences not being statistically significantly different across studies.16,20 Rates of serious adverse events were low and reported as not related to the study.16
Patients With Other Types of Wounds — Clinical Benefits
One SR16 identified 1 RCT and 1 NRS (Kaufman et al.) that included patients with venous leg ulcers:
The RCT reported that, compared to the control group, the number of patients in the CDO group who had complete wound healing was statistically significantly higher, and their wound size was also statistically significantly smaller at follow-up.
The NRS reported that 34% of venous ulcers had healed by at least 90%, and another 25% had healed by between 50% and 90%.
The NRS by Kaufman et al.16 also reported on patients with arterial wounds, pressure ulcers, and other wounds (including burns, post-trauma, and postoperative wounds). The authors did not compare CDO with standard care, but they reported overall healing rates:
For arterial wounds, 16% of arterial wounds had healed by at least 90%, and another 16% had healed by between 50% and 90%.
For pressure ulcers, 31% of wounds had healed by at least 90%, and 23% had healed by between 50% and 90%.
For other types of wounds, 20% of wounds had healed by at least 90%, and 36% of wounds had healed by between 50% and 90%.
The SR with meta-analysis7 included patients with a mix of etiologies, including some studies also included in the SR16 conducted by Health Technology Wales; details regarding which studies overlapped are available in Appendix 5. Overall, the meta-analyses of double-arm studies reported that CDO was:7
statistically significantly more effective than control groups in terms of complete wound healing and wound reduction
not statistically different from control groups in terms of ulcer healing as assessed by the PUSH scale.
They also conducted meta-analyses of single-arm studies, which reported that 48.0% of patients’ ulcers completely healed after CDO treatment but wound reduction was not statistically significant.
Reporting on adverse events was limited for this patient population and was limited to wound recurrence or wounds staying closed:
A meta-analysis of 2 studies7 reported that the proportion of patients whose wound stayed closed was statistically significantly higher in the CDO group compared to the control group. This may be due to the inclusion of 1 NRS of patients with venous leg ulcers, where 14 of 30 patients had wound recurrence. It is unclear if this is due to patients with venous leg ulcers tending to have higher rates of wound recurrence compared to patients with diabetic foot ulcers or if it is due to other factors.
An RCT19 of patients who underwent a bilateral reduction mammoplasty found that the number of patients whose wounds reopened was low and not statistically significant between the CDO and standard care groups.
Cost-Effectiveness of CDO Therapy Versus Conventional Would Care
Health Technology Wales conducted an SR that included economic evaluations and identified 1 relevant study (Chan and Campbell, 2020); they also conducted their own cost-effectiveness study.16 Overall, both studies reported that for patients with nonhealing or hard-to-heal diabetic foot ulcers, when compared to standard care, CDO was associated with higher total QALYs and lower costs, making the incremental cost-effectiveness ratio dominant (i.e., a greater benefit at a lower cost). Scenario analyses indicated that CDO remained dominant except under the following scenarios:
Reported by Health Technology Wales:
Grade 1 ulcers (CDO and standard care were equally effective, but CDO costs more)
Reported by Chan and Campbell; these scenarios reported lower costs for CDO, but worse outcomes:
Proportion of patients in the NPWT group whose ulcers healed was higher (57 out of 169 healed, or 33.7%; base case assumed 27.8%)30
Patients in the subgroup with a baseline ulcer size of 1.5 cm2 to 2.15 cm2 (the smallest size; the base case included ulcer sizes from 1.5 cm2 to > 4.9 cm2)
The economic evaluation by Health Technology Wales16 also reported that CDO is likely to be cost-effective compared to standard care, with a probability of 95.36% at a willingness-to-pay threshold of £20,000 per QALY. They also reported that CDO was cost-effective if it could heal 32% of wounds, and was dominant if it could heal 40% of wounds.
Recommendations Regarding the Use of CDO Therapy
Three guidelines recommended the use of topical oxygen therapy for diabetic foot ulcers.23,24,26 The recommendation from the International Working Group on the Diabetic Foot (IWGDF) group23 was a conditional recommendation due to low-certainty evidence, such as lack of reporting on adverse events and concerns around equity due to the costs of the device. The other 2 guidelines24,26 noted that the evidence was of high quality but did not provide a strength of recommendation.
Two guidelines23,26 recommended using topical oxygen therapy as an adjunct therapy for diabetic foot ulcers that have failed to heal following standard care.
The Wound Healing Society’s guideline for diabetic foot ulcers states that topical oxygen increases healing and reduces time to heal, which may be an indirect recommendation for the use of topical oxygen therapy.24
The last guideline by Frykberg et al. (2023)25 provided recommendations for topical oxygen therapy for hard-to-heal wounds in general, but noted the evidence for CDO was of high quality. They also did not provide strength of recommendations.
They recommended using topical oxygen therapy for hard-to-heal wounds in general, including venous leg ulcers and pressure ulcers.
They stated that there is currently insufficient evidence for patients with critical limb ischemia.
They recommended against using topical oxygen therapy on wounds that are infected, undebrided or necrotic, or have a malignancy.
Recommendations regarding treatment duration were limited; this may be because treatment duration will depend on the patient’s healing. Frykberg et al.25 provided a treatment algorithm, stating that if topical oxygen therapy is provided, to reassess the patient at 1 to 2 weeks; if the wound is healing (defined as having reduced in size by at least 50%), the treatment could continue and be reassessed at 1 to 2 weeks.
First Nations, Inuit, and Métis Patients
We did not conduct any searches specific to First Nations, Inuit, and Métis patients. However, based on our general search of CDO and wound healing, we did not identify any studies on the clinical effectiveness or cost-effectiveness on CDO in these populations. We also did not identify any evidence-based guidelines regarding the use of CDO to treat First Nations, Inuit, and Métis patients. Three studies were identified that reported demographic information related to ethnicity, and these did not report analyses of First Nations, Inuit, and Métis patients.
Limitations
Study Quality
The included clinical effectiveness studies noted various limitations, including high withdrawal rates,16 lack of blinding,16,19 small sample sizes,19-21 and short follow-up periods.19,21 The meta-analysis7 also tended to pool studies with different patient populations (i.e., different types of wounds). This may have resulted in biased or imprecise treatment effects.
Generalizability
Much of the clinical literature, as well as both economic evaluations and most guidelines identified by this report, were specific to patients with diabetic foot ulcers. We did not identify any cost-effectiveness studies for patients with nondiabetic foot ulcer wounds. Thus, the clinical- and cost-effectiveness of CDO compared to standard care for other types of wounds is unclear. It is also unclear if there are differences between different CDO devices.
There was limited information regarding patient ethnicity in most of the identified studies: we did not identify any relevant studies or recommendations related to the use of CDO for First Nations, Inuit, and Métis patients. In Canada, certain groups have higher prevalence rates for diabetes, including people who are South Asian, Black, First Nations, Inuit, or Métis; thus, they may also be disproportionately affected by diabetic foot ulcers.31,32 Thus, it is unclear if the findings from the identified studies are generalizable to certain patient groups that may have high need for treatment for diabetic foot ulcers.
The identified publications included studies from various countries including Canada: 3 studies identified within 1 SR16 were from Canada, including 1 RCT, 1 NRS, and 1 economic evaluation. All 3 of these studies focused on patients with diabetic foot ulcers. It is unclear if the findings for patients with other types of wounds would be applicable to Canada, as clinical outcomes may vary due to differences between countries (e.g., how health care is delivered, population characteristics). We also did not identify any Canada-specific guidelines, though the international guidelines may be applicable for health care providers and patients within Canada.
Conclusions and Implications for Decision- or Policy-Making
In 2020, we published a review on CDO for wounds:14 this report found limited clinical evidence related to CDO for wounds other than diabetic foot ulcers, no economic evaluations, and 1 weak recommendation for the use of topical oxygen therapy for diabetic foot ulcers based on low-quality evidence.
In this update, we identified 1 HTA that included 1 SR and 1 economic evaluation,16 1 scoping review,17 2 SRs,7,18 1 RCT,19 3 NRSs,20-22 and 4 evidence-based guidelines23-26 related to the use of CDO for patients with wounds. The reviews included 6 of the 7 primary studies previously identified in the 2020 report; the studies that were previously included are indicated in Appendix 6. However, we have also identified several new clinical studies in this report, adding evidence that suggests CDO is effective for diabetic foot ulcers (particularly those that are chronic and nonhealing), as well as a few studies related to other types of wounds. We also identified 2 economic evaluations16 indicating that CDO has the potential to be cost-effective for hard-to-heal, chronic diabetic foot ulcers, including 1 from the perspective of the Ontario Ministry of Health. Several new evidence-based guidelines have been published that recommend topical oxygen therapy as an adjunctive therapy for nonhealing diabetic foot ulcers that have not healed with standard care alone,26,33 with 1 also recommending the use of topical oxygen therapy for other types of hard-to-heal or chronic wounds.25
Thus, CDO appears to be clinically effective and cost-effective for hard-to-heal diabetic foot ulcers and has been recommended as an adjunct treatment for patients with diabetic foot ulcers that have not responded to standard care. Some studies suggest CDO may also be effective for treating other types of hard-to-heal wounds like venous leg ulcers and pressure ulcers, though we identified only a few studies related to patients with these types of wounds. Regarding implementation, it may be helpful to consider methods of ensuring equitable access to CDO so that all patients who need the treatment can receive it.
Considerations for Future Research
Overall, most of the identified evidence was focused on patients with diabetic foot ulcers, though a few studies also found positive outcomes for patients with other types of wounds. There was limited reporting on adverse events for other types of wounds (i.e., not diabetic foot ulcers), and we did not identify any cost-effectiveness studies on CDO for other types of wounds. In addition, most of the included studies did not report on patient ethnicity. Future research should consider investigating CDO for different types of wounds, including clinical effectiveness as well as adverse events, its cost-effectiveness compared to standard care, as well as its impact for different groups of patients. This would allow for a better understanding of whether CDO is effective for other types of wounds and across patient groups.
Additional research comparing CDO to other types of treatment may also be of interest. The guidelines by ElSayed et al.26 and Chen et al. (IWGDF)23 both suggest considering various treatments for nonhealing diabetic foot ulcers, including topical oxygen therapy, placental-derived products, and autologous fibrin and leukocyte platelet patches, but it is unclear if certain treatments are more effective and if they should be used for different situations (e.g., types of wounds). Additional studies comparing CDO to other active comparators may help to determine if certain treatments are more clinically effective overall or for specific types of wounds.
We identified limited evidence regarding the need for debridement with CDO as well as what oxygen flow rate is most effective. One NRS22 indicates that patients who had follow-up visits at sites with higher rates of surgical debridement had greater benefits. One guideline25 also recommends against using topical oxygen therapy on wounds that are undebrided. The authors of 1 SR7 stated that studies of devices that deliver oxygen at a flow rate of 3 mL/h suggest they are as clinically effective as devices that deliver oxygen at 15 mL/h, but they did not report any formal analyses comparing devices with different flow rates. It is thus unclear if debridement is necessary and what types are best (e.g., autolytic, enzymatic, mechanical) as well as if certain flow rates are more clinically effective. Additional studies are required to better understand these factors, as they may help improve outcomes for patients receiving CDO therapy.
Advances in remote monitoring technology may also be applicable to CDO therapy. A case series reported on a pilot study in which patients with diabetic foot ulcers were treated with CDO alongside a remote assessment and monitoring tool that was able to capture wound measurement data remotely from patients and communicate it to a clinician via a noninvasive app.34 The preliminary study reported positive outcomes, suggesting that this may be a useful tool for some patients (e.g., those who have difficulty travelling to a clinic regularly for appointments); however, in-clinic visits may still be required for patients who need wound debridement. Larger studies are required to better determine if CDO with remote monitoring technology should be adopted more widely and to assess the associated clinical outcomes, costs, and resource requirements.34
References
1.Denny K, Lawand C, Perry S. Compromised wounds in Canada. Healthc Q. 2014;17(1):7-10. PubMed
2.Four pillars: recommendations for achieving a high performing health system. Toronto (ON): Ontario Hospital Association (OHA), Ontario Association of Community Care Access Centres (OACCAC); 2011: https://nhh.ca/document/four-pillars-recommendations-for-achieving-a-high-performing-health-system-pdf. Accessed 2024 Jul 2.
3.Queen D, Botros M. The true cost of wounds for Canadians. Wound Care Canada. 2024;22(1):16-20. PubMed
4.Bowers S, Franco E. Chronic wounds: evaluation and management. Am Fam Physician. 2020;101(3):159-166. PubMed
5.Overview: chronic wounds. Köln (DE): Institute for Quality and Efficiency in Health Care (IQWiG); 2022: https://www.ncbi.nlm.nih.gov/books/NBK326431/. Accessed 2024 Jul 2.
6.Evans K, Kim PJ. Overview of treatment of chronic wounds. In: Post TW, ed. UpToDate. Waltham (MA): UpToDate; 2022: http://www.uptodate.com. Accessed 2024 Jul 2.
7.Nagarsheth K, Kankaria A, Marsella J, et al. Systematic review of the effects of topical oxygen therapy on wound healing. JVS Vasc Insights. 2024;2:100051.
8.Nowak M, Mehrholz D, Barańska-Rybak W, Nowicki RJ. Wound debridement products and techniques: clinical examples and literature review. Postepy Dermatol Alergol. 2022;39(3):479-490. PubMed
9.Castilla DM, Liu ZJ, Velazquez OC. Oxygen: implications for wound healing. Adv Wound Care (New Rochelle). 2012;1(6):225-230. PubMed
10.Health Canada. Hyperbaric oxygen therapy. 2019; https://www.canada.ca/en/health-canada/services/healthy-living/your-health/medical-information/hyperbaric-oxygen-therapy.html. Accessed 2024 Jul 2.
11.Sayadi LR, Banyard DA, Ziegler ME, et al. Topical oxygen therapy & micro/nanobubbles: a new modality for tissue oxygen delivery. Int Wound J. 2018;15(3):363-374. PubMed
12.He S, Liang C, Yi C, Wu M. Therapeutic effect of continuous diffusion of oxygen therapy combined with traditional moist wound dressing therapy in the treatment of diabetic foot ulcers. Diabetes Res Clin Pract. 2021;174:108743. PubMed
13.Kaufman H, Gurevich M, Tamir E, et al. Topical oxygen therapy used to improve wound healing in a large retrospective study of wounds of mixed aetiology. Wounds Int. 2021;12:63-68.
14.Continuously diffused oxygen therapy for wound healing: a review of the clinical effectiveness, cost-effectiveness, and guidelines. (CADTH Rapid response report: summary with critical appraisal). Ottawa (ON): CADTH; 2020: https://www.ncbi.nlm.nih.gov/books/NBK564989/. Accessed 2024 June 25.
15.Wounds Canada. About Wounds Canada. https://www.woundscanada.ca/about-wounds-canada. Accessed 2024 Jul 2.
16.Health Technology Wales. Continuous topical oxygen therapy to treat people with chronic non-healing and complex diabetic foot ulcers. 2022; https://healthtechnology.wales/reports-guidance/topical-oxygen-therapy-natrox/. Accessed 2024 June 28.
17.Sykorova M, Moffatt CJ, Stentiford N, Burian EA, Katsuhiro S, Wei Y. Topical oxygen therapy and singlet oxygen in wound healing: a scoping review. Int Wound J. 2024;21(4):e14846. PubMed
18.Chen P, Vilorio NC, Dhatariya K, et al. Effectiveness of interventions to enhance healing of chronic foot ulcers in diabetes: a systematic review. Diabetes Metab Res Rev. 2024;40(3):e3786. PubMed
19.Zulbaran-Rojas A, Bara RO, Lee M, et al. Optimizing tissue oxygenation in reduction mammoplasty: the role of continuous diffusion of oxygen: a feasibility pilot randomized controlled trial. J Surg Res. 2023;292:113-122. PubMed
20.Tang TY, Mak MYQ, Yap CJQ, et al. An observational clinical trial examining the effect of topical oxygen therapy (Natrox™) on the rates of healing of chronic diabetic foot ulcers (OTONAL Trial). Int J Low Extrem Wounds. 2024;23(2):326-337. PubMed
21.Lavery LA, Killeen AL, Farrar D, et al. The effect of continuous diffusion of oxygen treatment on cytokines, perfusion, bacterial load, and healing in patients with diabetic foot ulcers. Int Wound J. 2020;17(6):1986-1995. PubMed
22.Lavery LA, Niederauer MQ, Papas KK, Armstrong DG. Does debridement improve clinical outcomes in people with diabetic foot ulcers treated with continuous diffusion of oxygen? Wounds. 2019;31(10):246-251. PubMed
23.Chen P, Vilorio NC, Dhatariya K, et al. Guidelines on interventions to enhance healing of foot ulcers in people with diabetes (IWGDF 2023 update). Diabetes Metab Res Rev. 2024;40(3):e3644. PubMed
24.Lavery LA, Suludere MA, Attinger CE, et al. WHS (Wound Healing Society) guidelines update: diabetic foot ulcer treatment guidelines. Wound Repair Regen. 2024;32(1):34-46. PubMed
25.Frykberg R, Andersen C, Chadwick P, et al. Use of topical oxygen therapy in wound healing. J Wound Care. 2023;32(Sup8b):S1-S32.
26.ElSayed NA, Aleppo G, Aroda VR, et al. 12. Retinopathy, neuropathy, and foot care: standards of care in diabetes—2023. Diabetes Care. 2022;46(Supplement_1):S203-S215. PubMed
27.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
28.Assessment and management of foot ulcers for people with diabetes. Toronto (ON): Registered Nurses' Association of Ontario; 2013: https://rnao.ca/bpg/guidelines/assessment-and-management-foot-ulcers-people-diabetes-second-edition. Accessed 2024 Jul 11.
29.Bann CM, Fehnel SE, Gagnon DD. Development and validation of the Diabetic Foot Ulcer Scale-short form (DFS-SF). Pharmacoeconomics. 2003;21(17):1277-1290. PubMed
30.Chan BC, Campbell KE. An economic evaluation examining the cost-effectiveness of continuous diffusion of oxygen therapy for individuals with diabetic foot ulcers. Int Wound J. 2020;17(6):1791-1808. PubMed
31.Public Health Agency of Canada. Infographic: inequalities in diabetes in Canada. 2019; https://www.canada.ca/en/public-health/services/publications/science-research-data/inequalities-diabetes-infographic.html. Accessed 2024 Jul 9.
32.Diabetes in Canada: backgrounder. Ottawa (ON): Diabetes Canada; 2020: https://www.diabetes.ca/DiabetesCanadaWebsite/media/Advocacy-and-Policy/Backgrounder/2020_Backgrounder_Canada_English_FINAL.pdf. Accessed 2024 Jul 9.
33.Schaper N, van Netten J, Apelqvist J, et al. IWGDF guidelines on the prevention and management of diabetes-related foot disease. International Working Group on the Diabetic Foot (IWGDF); 2023: https://iwgdfguidelines.org/wp-content/uploads/2023/07/IWGDF-Guidelines-2023.pdf. Accessed 2024 Jun 25.
34.Lee A, Woodmansey E, Klopfenstein B, O'Leary JL, Cole W. Remote assessment and monitoring with advanced wound therapy to optimise clinical outcomes, access and resources. J Wound Care. 2024;33(2):90-101. PubMed
35.Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. PubMed
36.Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377-384. PubMed
37.Higgins JPT, Green S, editors. Figure 15.5.a: Drummond checklist (Drummond 1996). Cochrane handbook for systematic reviews of interventions. London (GB): The Cochrane Collaboration; 2011: http://handbook-5-1.cochrane.org/chapter_15/figure_15_5_a_drummond_checklist_drummond_1996.htm. Accessed 2024 Jul 10.
38.Agree Next Steps C. The AGREE II Instrument. Hamilton (ON): AGREE Enterprise; 2017: https://www.agreetrust.org/wp-content/uploads/2017/12/AGREE-II-Users-Manual-and-23-item-Instrument-2009-Update-2017.pdf. Accessed 2024 Jul 7.
39.Schünemann H, Brożek J, Guyatt G, Oxman A. GRADE Handbook. 2013; https://gdt.gradepro.org/app/handbook/handbook.html. Accessed 2024 Jul 8.
Appendix 1: Methods
Note this appendix has not been copy-edited.
Methods
Literature Search Methods
An information specialist conducted a literature search on key resources including MEDLINE, the Cochrane Database of Systematic Reviews, the International HTA Database, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search approach was customized to retrieve a limited set of results, balancing comprehensiveness with relevancy. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. Search concepts were developed based on the elements of the research questions and selection criteria. The main search concepts were CDO therapy and wound healing. The search was completed on June 20, 2024 and limited to English-language documents published since January 1, 2019.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. As an update to a previous CADTH report, articles were included if they were made available since the previous search date and were not included in the 2020 CADTH report.14 The final selection of full-text articles was based on the inclusion criteria presented in Table 1. Figure 1 presents the PRISMA27 flow chart of the study selection.
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1 or were duplicate publications. SRs in which all relevant studies were captured in other more recent or more comprehensive SRs were excluded. Primary studies retrieved by the search were excluded if they were captured in 1 or more included SRs. Guidelines with unclear methodology were also excluded.
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the following tools as a guide: A MeaSurement Tool to Assess systematic Reviews 2 (AMSTAR 2)35 for SRs, the Downs and Black checklist36 for RCTs and NRSs, the Drummond checklist37 for economic evaluations, and the Appraisal of Guidelines for Research and Evaluation (AGREE) II instrument38 for guidelines. Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Appendix 2: Selection of Included Studies
Appendix 3: Characteristics of Included Publications
Note this appendix has not been copy-edited.
Table 2: Characteristics of Included HTA, Scoping Review, and SRs
Study citation, country, funding source | Study designs and numbers of primary studies included | Population characteristics | Intervention and comparator(s) | Outcomes, length of follow-up |
|---|---|---|---|---|
HTA | ||||
Health Technology Wales (2022)16 Wales Funding source: Health Technology Wales is funded by the Welsh Government | A rapid SR that prioritized SRs of RCTs, followed by RCTs, comparative NRSs, and then single-arm NRSs. Search was conducted on August 4, 2022, with no date limits. Included 9 studies:
| Population of interest was people with chronic, nonhealing and complex wounds (e.g., DFUs, venous leg ulcers, arterial ulcers). People with acute wounds were excluded. | Intervention: Continuous topical oxygen wound therapy (3 mL/h to 15 mL/h) in addition to standard care Comparator: Cleaning and dressing the wound, as well as standard care for the wound type:
| Outcomes:
Follow-up: preferred longer follow-up, but would include short-term if longer was not available |
Scoping review | ||||
Sýkorová et al. (2024)17,a UK Funding source: University of Nottingham; University of Nottingham; SOE Health Ltd. | A review of topical oxygen therapies, including CDO. Databases were searched for papers published until December 14, 2022. Included 49 studies in total, including 8 SRs (3 with MAs). Of the studies relevant to this report, there were
| Patients with any wounds. All relevant SRs and most primary studies were all related to patients with DFUs; other populations covered by the primary studies included surgical wounds and venous leg ulcers. | Eligible interventions: Topical oxygen therapies Relevant intervention: CDO (3 mL/h to 15 mL/h) Comparator: Any | Outcomes of interest:
Follow-up: relevant included studies follow-up ranged from 4 weeks to 1 year where reported |
SRs | ||||
Chen et al. (2024)18 Australia Funding source: developed for the IWGDF guidelines,33 which were sponsored by Mölnlycke, Urgo Medical, Reapplix, Advanced Oxygen Therapy Inc., and Essity | An SR of all RCTs up until October 2022. Included 262 RCTs in total. There were 10 studies for topical oxygen therapy, 7 of which were on CDO and thus relevant to this report. | Patients with DFUs | Eligible interventions: Interventions relevant to wound healing Relevant intervention: Topical oxygen therapy (flow rate NR) Comparator: Standard care unless otherwise stated | Outcomes:
Length of follow-up: NR |
Nagarsheth et al. (2024)7 US Funding source: NIH Awards and Veteran Affairs Awards | An SR with MA of literature on human patients published after 2012, as authors stated articles published before this were not relevant. Date of search not reported, but manuscript was submitted in 2023. Included 22 studies (10 RCTs and 12 NRSs; NRSs included prospective double-arm and single-arm studies, as well as case reports). | Patients with cutaneous wounds of any etiology. Identified papers included patients with:
| Intervention: CDO (3 mL/h to 15 mL/h) Comparator: Standard of care, pre-post comparison, or undescribed control group | Outcomes:
Follow-up: Ranged from 10 days to 9 years |
CDO = continuous diffused oxygen; DFU = diabetic foot ulcer; HTA = health technology assessment; IWGDF = International Working Group on the Diabetic Foot; MA = meta-analysis; NR = not reported; NRS = nonrandomized study; RCT = randomized controlled trial; SR = systematic review; VAS = visual analogue scale.
Note: All outcomes reported by the reviews that were relevant to this report are listed. Due to overlap between reviews on included primary studies, some outcomes reported by a review may not be presented in the findings, as they have already been reported by a different review, to avoid double-reporting.
aSýkorová et al. (2024)17 labelled their study as a scoping review and used typical scoping review methodology. However, as they summarized clinical outcomes relevant to this report, it was included.
Table 3: Characteristics of Included Primary Clinical Studies
Study citation, country, funding source | Study design | Population characteristics | Intervention and comparator(s) | Relevant clinical outcomes, length of follow-up |
|---|---|---|---|---|
RCT | ||||
Zulbaran-Rojas et al. (2023)19 US Funding source: EO2 Concepts, Inc. | RCT (within person randomized trial, or split body trial: all patients received the intervention on 1 breast and the comparator on the other breast) | Adults (N = 16; does not include 3 participants who withdrew) undergoing a bilateral reduction mammoplasty:
| Intervention: CDO (15 mL/h) for 4 weeks; included
Comparator: standard of care using an identical topical skin adhesive system | Outcomes of interest:
Follow-up: 4 weeks |
NRSs | ||||
Tang et al. (2024)20 Singapore Funding source:
| NRS – before-after | Adults (aged 21 to 90 years) with diabetes and a DFU for more than 12 weeks but fewer than 18 weeks (between 0.5 cm2 to 50 cm2), minor amputation sites with < 50% healed in 4 weeks, 4 weeks of standard care at the hospital-based diabetic foot clinic (N = 20)
Wound types and characteristics:
| Intervention: CDO (15 mL/h) at home for 12 weeks Comparator: Baseline measures | Outcomes:
Follow-up:
|
Lavery et al. (2020)21 US Funding source: EO2 Concepts, Inc. | NRS – Prospective cohort study with before-after comparison | Adults (aged 18 to 89) with a diagnosis of diabetes mellitus (based on American Diabetes Association criteria) with a full thickness ulcer below the ankle. Patient characteristics provided by patients who healed (healers; N = 12) and for those who did not heal (nonhealers, N = 11). Means of continuous variables are presented per group; dichotomous variables are presented as overall for both groups. Groups were not statistically significantly different on any characteristics.
| Intervention: CDO (flow rate NR) for 3 weeks Comparator: baseline (pre-post comparison) | Outcome of interest:
Follow-up: 3 weeks |
Lavery et al. (2019)22 US Funding source: EO2 Concepts, Inc. | Post hoc analysis of RCT (double-blind, placebo-controlled) | Adults with DFUs (N = 146)
| Intervention: CDO (3 mL/h) with debridement (frequency at discretion of physician) for 12 weeks Comparator: placebo | Outcomes: • Percentage of healed ulcers Follow-up: 12 weeks or wound closure |
CDO = continuously diffused oxygen; DFU = diabetic foot ulcer; NR = not reported; NRS = nonrandomized study; RCT = randomized controlled trial; SD = standard deviation; VAS = visual analogue scale.
Table 4: Characteristics of Included Economic Evaluations
Study citation country, funding source | Type of analysis, time horizon, perspective | Population characteristics | Intervention and comparator(s) | Approach | Source of clinical, cost, and utility data used in analysis | Main assumptions |
|---|---|---|---|---|---|---|
Health Technology Wales (2022)16 Wales Funding source: Health Technology Wales is funded by the Welsh Government | Analysis: Cost-utility analysis Time horizon: 50 years Perspective: UK NHS and personal social services | Patients with chronic, nonhealing DFUs; initiated with average age of 58.20 years, 24% female | Intervention: 12 weeks of CDO with standard care Comparator: 12 weeks of standard care | Markov structure with a 1-month cycle length, tracking patients over 6 health states over a lifetime:
|
|
|
Chan and Campbell (2020) as reported by Health Technology Wales16 Canada Funding source: EO2 Concepts Inc. | Analysis: Cost-utility analysis Time horizon: 5 years Perspective: Public health care payer (Ontario Ministry of Health) | Individuals with hard-to-heal DFUs (Grade IA according to the University of Texas staging system for DFU); ulcer may be present for more than 1 month but less than 1 year | Intervention: 12 weeks of CDO Comparator: 12 weeks of NPWT, standard care, moist wound therapy, and offloading | Microsimulation model with 1-year cycle length; simulated individuals could move between 6 mutually exclusive states:
|
|
|
CDO = continuous diffusion oxygen; DFU = diabetic foot ulcer; NPWT = negative pressure wound therapy; OECD = Organisation for Economic Co-operation and Development.
Table 5: Characteristics of Included Guidelines
Intended users, target population | Intervention and practice considered | Major outcomes considered | Evidence collection, selection, and synthesis | Evidence quality assessment | Recommendations development and evaluation | Guideline validation |
|---|---|---|---|---|---|---|
Guidelines on interventions to enhance healing of foot ulcers in people with diabetes (IWGDF 2023 update)23 | ||||||
Intended users: Health care professionals involved in care of people with diabetes Target population: People with diabetes | Intervention of interest: Topical oxygen therapya Practice considered: NR |
| GRADE and Cochrane methodology used to develop clinical questions and outcomes, conduct an SR (and a MA where appropriate). |
| Multidisciplinary working group summarized findings, then drew conclusions for each intervention as evidence statements. Based on these and expert opinion, summary of judgment tables for each clinical question and the recommendation was drafted. The working group included members from podiatric surgery, podiatry, and endocrinology disciplines, with members from the US, Caribbean, Europe, Asia, and Australia. A voting procedure was used for each recommendation for the direction (for or against) and strength of the recommendation (strong or condition), with a majority vote needed for final recommendations. | Guidelines were sent to a panel of independent international experts and people with lived experience for their critical review; the guidelines were revised based on their comments. |
WHS (Wound Healing Society) guidelines update: Diabetic foot ulcer treatment guidelines24 | ||||||
Intended users: Clinicians Target population: People with diabetic foot ulcers | Intervention of interest: Topical oxygen therapya Practice considered: NR | Unclear | Keyword search of multiple databases, focused on human and disease-specific data, limited to SRs, MAs, RCTs, retrospective series reviews, clinical case series, and expert recommendations published since January 2006. | Strength of evidence:
| Delphi consensus by panel members, which included academics, clinicians, and researchers. | NR |
Use of topical oxygen therapy in wound healing25 | ||||||
Intended users: Health care professionals Target population: People with wounds | Intervention of interest: CDO devices, disposable CDO devices Practice considered: NR | Outcomes from relevant studies included:
| NR | Quality of evidence and strength of recommendations were based on the American Diabetes Association GRADE system:
| Expert panel of 9 key opinion leaders from US and Europe met to discuss clinical evidence in support of TOT in care of hard-to-heal wounds; meeting resulted in a consensus document. | NR |
12. Retinopathy, neuropathy, and foot care: Standards of care in diabetes—202326 | ||||||
Intended users: Health care professionals Target population: People with diabetes | Intervention of interest: Topical oxygen therapy Practice considered: NR | Unclear | Systematic literature review conducted. Evidence summaries are made by the Professional Practice Committee. | Quality of evidence and strength of recommendations were based on the American Diabetes Association GRADE system:
| Expert panel met for 2-day meeting to present evidence summaries and develop recommendations. A year-long public comment period requesting feedback was held. | Feedback obtained from external peer reviewers. |
EWMA = European Wound Management Association; GRADE = Grading of Recommendations Assessment Development and Evaluation; IWGDF = International Working Group on the Diabetic Foot; MA = meta-analysis; NR = not reported; RCT = randomized controlled trial; SIGN = Scottish Intercollegiate Grouping Network; SR = systematic review.
aRecommendation is for topical oxygen therapy; it does not specify if this includes continuous diffused oxygen therapy.
Appendix 4: Critical Appraisal of Included Publications
Note this appendix has not been copy-edited.
Table 6: Strengths and Limitations of SRs Using AMSTAR 235
Strengths | Limitations |
|---|---|
HTA | |
Health Technology Wales (2022)16 | |
|
|
Scoping review | |
Sýkorová et al. (2024)17 | |
|
|
SRs | |
Chen et al. (2024)18 | |
|
|
Nagarsheth et al. (2024)7 | |
|
|
AMSTAR 2 = A MeaSurement Tool to Assess systematic Reviews 2; HTA = health technology assessment; MeSH = Medical Subject Headings; NRS = nonrandomized study; RCT = randomized controlled trial; SR = systematic review.
Table 7: Strengths and Limitations of Clinical Studies Using the Downs and Black Checklist36
Strengths | Limitations |
|---|---|
RCT | |
Zulbaran-Rojas et al. (2023)19 | |
|
|
NRSs | |
Tang et al. (2024)20 | |
|
|
Lavery et al. (2020)21 | |
|
|
Lavery et al. (2019)22 | |
|
|
NRS = nonrandomized studies; RCT = randomized controlled trial.
Table 8: Strengths and Limitations of Economic Evaluations Using the Drummond Checklist37
Strengths | Limitations |
|---|---|
Health Technology Wales (2022)16 | |
|
|
Chan and Campbell (2020) based on reporting by Health Technology Wales (2022)16 | |
|
|
CDO = continuous diffused oxygen; DFU = diabetic foot ulcer; NPWT = negative pressure wound therapy.
Table 9: Strengths and Limitations of Guidelines Using AGREE II38
Item | Guidelines on interventions to enhance healing of foot ulcers in people with diabetes (IWGDF 2023 update) (2024)23 | WHS (Wound Healing Society) guidelines update: Diabetic foot ulcer treatment guidelines (2024)24 | Use of topical oxygen therapy in wound healing (2023)25 | 12. Retinopathy, neuropathy, and foot care: Standards of care in diabetes—2023 (2023)26 |
|---|---|---|---|---|
Domain 1: Scope and purpose | ||||
1. The overall objective(s) of the guideline is (are) specifically described. | Yes | Yes | Yes | Yes |
2. The health question(s) covered by the guideline is (are) specifically described. | Yes | Yes | Yes | Yes |
3. The population (patients, public, etc.) to whom the guideline is meant to apply is specifically described. | Yes | Yes | Yes | Yes |
Domain 2: Stakeholder involvement | ||||
4. The guideline development group includes individuals from all relevant professional groups. | Yes | Yes | NR | Yes |
5. The views and preferences of the target population (patients, public, etc.) have been sought. | Yes | NR | Yes | Yes |
6. The target users of the guideline are clearly defined. | Yes | Yes | Yes | Yes |
Domain 3: Rigour of development | ||||
7. Systematic methods were used to search for evidence. | Yes | Yesa | NR | Yes |
8. The criteria for selecting the evidence are clearly described. | Yes | No | No | No |
9. The strengths and limitations of the body of evidence are clearly described. | Yes | Yes | No | Yes |
10. The methods for formulating the recommendations are clearly described. | Yes | Yes | Yes | Yes |
11. The health benefits, side effects, and risks have been considered in formulating the recommendations. | Yes | Unclear | Unclear | Yes |
12. There is an explicit link between the recommendations and the supporting evidence. | Yes | Yes | No | Yes |
13. The guideline has been externally reviewed by experts before its publication. | Yes | NR | NR | Yes |
14. A procedure for updating the guideline is provided. | Yes | No | No | Yes |
Domain 4: Clarity of presentation | ||||
15. The recommendations are specific and unambiguous. | Yes | Yes | Yes | Yes |
16. The different options for management of the condition or health issue are clearly presented. | Yes | Yes | Yes | Yes |
17. Key recommendations are easily identifiable. | Yes | Yes | Yes | Yes |
Domain 5: Applicability | ||||
18. The guideline describes facilitators and barriers to its application. | Yes | No | Yes | Yes |
19. The guideline provides advice and/or tools on how the recommendations can be put into practice. | Yes | No | Yes | No |
20. The potential resource implications of applying the recommendations have been considered. | Yes | No | Yes | No |
21. The guideline presents monitoring and/or auditing criteria. | NR | NR | NR | Yes |
Domain 6: Editorial independence | ||||
22. The views of the funding body have not influenced the content of the guideline. | Yes | Yes | Yes | Yes |
23. Competing interests of guideline development group members have been recorded and addressed. | Yes | Yes | Yes | Yes |
AGREE II = Appraisal of Guidelines for Research and Evaluation II; IWGDF = International Working Group on the Diabetic Foot; NR = not reported.
aKeyword search of databases.
Appendix 5: Main Study Findings
Note this appendix has not been copy-edited.
Table 10: Summary of Main Findings – Complete and Partial Wound Healing for Patients With Diabetic Foot Ulcers
Study citation and study design | For SRs: included study, first author, and study design | Method of measurement | Result | Notes |
|---|---|---|---|---|
Health Technology Wales (2022)16 HTA (SR) | Thanigaimani (2021) SR-MA including 6 RCTs: 530 participants from: Driver et al. (2017), Driver et al. (2013), Frykberg et al. (2020), Niederauer et al. (2017), Niederauer et al. (2018), Yu et al. (2016) | Main meta-analysis for complete wound healing, RR (95% CI) | 1.94 (1.19 to 3.17) | Assumes patients lost to follow-up had full healing. |
Sensitivity meta-analysis for complete wound healing, RR (95% CI) | 1.54 (1.07 to 2.30) | Assumes patients lost to follow-up did not achieve full healing. | ||
Meta-analysis for complete wound healing, including only 3 low risk of bias studies, RR (95% CI) | 2.37 (1.52 to 3.68) | NA | ||
Leave-one-out analysis for complete wound healing, effect size (95% CI) | 1.83 (1.03 to 3.25)
| Omits 1 study (Frykberg et al., 2020). | ||
Serena (2021)a RCT N = 145; for PP analysis, N = 128 Follow-up: 12 weeks | Number of wounds healed in ITT analysis: |
| Results from PP analysis are included in the MA by Nagarsheth et al. (2024). | |
Number of wounds healed in PP analysis: |
| NA | ||
Difference in wound area between continuous TOT and control groups, mean (95% CI) |
| PP analysis appears to have been included in the MA by Nagarsheth, 2024. This result has been included here to present both the ITT and PP analyses. Study had high withdrawal. | ||
Reduction in wound area (%), mean (SD) |
| NA | ||
Yu (2016) RCT | Healing rate of ulcers by UTC grade | Grade 1:
Grade 2:
Grade 3:
| Pooled results are included in the MA by Thanigaimani (2021); this result is presented here to show the differences by ulcer grade (i.e., severity). | |
Connaghan, 2021 to 1 RCT N = 124 Follow-up: 4 weeks | Wound size reduction at week 4 (%), mean (range) |
| RCT: Driver, 2017 | |
Kaufman, 2021 NRS Follow-up: NR | Percentage of wounds by healed state |
| Refer to note in footnotes. | |
Tang et al. (2024)20 NRS Follow-up: 12 weeks | NA | Complete healing by UTC grade ulcer, n of N (%) |
| Pooled results are included in Nagarsheth et al. (2024); this result is presented here to show the difference between healing by ulcer grade. |
Wounds with > 75% closure, n (%) | 14 (70.0%) | |||
Lavery et al. (2020)21 NRS Follow-up: 3 weeks | NA | Proportion of patients with healed ulcers | 13% | NA |
Percentage of patients with at least 50% wound closure after 3 weeks | 53% | NA | ||
Lavery et al. (2019)22 NRS Follow-up: 12 weeks | NA | Proportion of ulcers healed | At sites that debrided the wound at nearly every visit:
| At sites with high debridement rates, the frequency was high for both CDO and placebo groups. Surgical debridement was used. |
Relative efficacy of active vs. placebo by frequency of ulcer debridement |
| Mean debridement across all sites was 90.0% (of visits). Most sites had debridement at 92% to 100% of visits, except 1 site that conducted debridement at 41.3% of visits. When this 1 site was excluded, the average debridement rate 98.4%. | ||
Analysis of patients who were Hispanic: relative efficacy of active vs. placebo by frequency of ulcer debridement |
| High debridement: average of 97.9% of visits had debridement. Included most sites except 1 (41.3% debridement). |
CI = confidence interval; HTA = health technology assessment; ITT = intention-to-treat; NA = not applicable; NRS = nonrandomized study; OR = odds ratio; PP = per-protocol; RCT = randomized controlled trial; RR = risk ratio; SMD = standardized mean difference; SR = systematic review; TOT = topical oxygen therapy; UTC = University of Texas Classification.
Note: The UTC ulcer grading system ranges from 0 to 4 (least to most severe respectively).28 All patients in the study by Kaufman et al. (2021) had been previously treated with SoC but their wounds had failed to heal, with wounds being open for an average of 10.7 (SD = 15.7) months before study initiation.
aPatients in the study by Serena et al. (2021) included patients with diabetic foot ulcers and minor amputation wounds. Health Technology Wales included these findings alongside other studies focused on patients with diabetic foot ulcers only, so we have done the same here to match their reporting.
Table 11: Summary of Main Findings – Complete and Partial Wound Healing for Patients With Arterial Wounds, Leg Venous Ulcers, Pressure Ulcers, and Other Types of Wounds
Study citation and study design | For SRs: included study | Method of measurement | Result | Notes |
|---|---|---|---|---|
Arterial wounds | ||||
Health Technology Wales (2022)16 HTA (SR) | Kaufman, 2021 NRS Follow-up: unclear | Percentage of wounds by healing state |
| Refer to note in footnotes. |
Leg venous ulcers | ||||
Health Technology Wales (2022)16 HTA (SR) | Altinbas and Şahsivar, 2022 RCT Follow-up: 45 days | Number of people with complete wound healing |
| NA |
Wound size (cm2), mean (SD) | Baseline:
Day 15:
Day 30:
Day 45:
Mean:
| Unclear if “mean” indicates total mean across the follow-up period or at a specific follow-up time. | ||
Statistical significance of wound size change from baseline to day 45 |
| NA | ||
Kaufman, 2021 NRS Follow-up: varied; some followed for more than 25 days | Percentage of wounds by healing state |
| Refer to note in footnotes. | |
Reduction in wound area for patients treated with continuous TOT plus standard care by length of treatment (%), mean (SD) |
| NA | ||
Pressure ulcers | ||||
Health Technology Wales (2022)16 HTA (SR) | Kaufman, 2021 NRS N = 13 Follow-up: NR | Percentage of wounds by healing state |
| Refer to note in footnotes. |
Mixed or unclear etiologies | ||||
Nagarsheth et al. (2024)7 SR with MA | MA of double-arm studies: includes 7 studies. N = 725 (treatment: n = 369; control: n = 356) | Complete healing, OR (95% CI) | 4.48 (2.05 to 9.77) P < 0.001 I2 = 76.34% | Includes results from Serena (2021) reported above (from Health Technology Wales, 2022), as well as 3 studies presented by Thanigaimani’s SR (also from Health Technology Wales, 2022): Driver (2017), Frykberg (2020), Niederauer (2017). The remaining 3 studies included in this meta-analysis (Azimian (2015), Tawfick (2013; NRS), Altinbas (2022)) have not been reported elsewhere in this report. |
Single-arm studies; includes 9 studies N = 4,273 | Participants who completely healed after continuous TOT, n/N | 1195/4273 | Studies included: Includes results from Tang (2021) which are also reported above (by UTC grade). Other studies included: Hunter (2020), Kaufman (2018), Segey (2019), Copeland (2017), Hayes (2017), Igwegbe (2015), Cole (2020), Massenburg (2016). Removal of case series did not change results regarding proportion of wound healed. | |
Pooled prevalence, % (95% CI) | 48.0% (0.34 to 0.62)
| NA | ||
MA of 6 double-arm studies N:
| Difference in wound reduction between treatment and control, SMD (95% CI) | –0.85 (–1.88 to 0.18)
| Includes Serena (2021) described above in the report by Health Technology Wales. This MA appears to based on their PP analysis. | |
MA of 2 single-arm studies N = 29 | Wound reduction after continuous TOT, treatment mean (95% CI) | 1.54 (0.71 to 2.38)
| Heterogeneity was < 25% (I2 = 0). | |
MA of 2 RCTs N:
| Difference in change on PUSH score between intervention and control, SMD (95% CI) | 0.65 (–0.56 to 1.86)
| Includes children with pressure ulcers and patients infected chronic surgical wounds. | |
Health Technology Wales (2022)16 HTA (SR) | Kaufman, 2021 NRS Follow-up: unclear | Percentage of wounds by healing state |
|
|
CI = confidence interval; HTA = health technology assessment; ITT = intention-to-treat; MA = meta-analysis; NA = not applicable; NRS = nonrandomized study; PP = per-protocol; PUSH = pressure ulcer scale for healing; RCT = randomized controlled trial; SMD = standardized mean difference; SR = systematic review; TOT = topical oxygen therapy.
Note: All patients in the study by Kaufman et al. (2021) had been previously treated with SoC but their wounds had failed to heal, with wounds being open for an average of 10.7 (SD = 15.7) months before study initiation.
Table 12: Summary of Main Findings — Mortality in Patients With Diabetic Foot Ulcers
Variable | Health Technology Wales (2022)16 – HTA (SR) | Tang (2024)20 – NRS | |
|---|---|---|---|
Thanigaimani, 2022 – SR (1 RCT) | Serena et al., 2021 – RCT | ||
Total number of patients | NR | 145 | 20 |
Follow-up | 12 weeks | 12 weeks | 12 weeks |
Number of deaths | |||
Continuous TOT plus standard care | 0 | 1a | 0 |
Standard care | 2a | 0 | 0 |
HTA = health technology assessment; ITT = intention-to-treat; NR = not reported; PP = per-protocol; NRS = nonrandomized study; SR = systematic review; TOT = topical oxygen therapy.
aDeaths reported as not related to the intervention.
Table 13: Summary of Main Findings — Amputations in Patients With Diabetic Foot Ulcers
Variable | Health Technology Wales (2022)16 – HTA (SR) | ||
|---|---|---|---|
Thanigaimani, 2022 – SR (1 RCT) | Al-Jalodi, 2022 – Post hoc analysis of RCT | He, 2021 – RCT | |
Total number of patients | 124 | 22 | 120 |
Follow-up | 12 weeks | 1 year | 1 year |
Number of amputations (n) | |||
Continuous TOT plus standard care | 0 | 0 | NR |
Standard care | 1 | 1 | NR |
Proportion of patients who had amputations (%) | |||
Continuous TOT plus standard care | NR | NR | 12.5% |
Moist wound dressing therapy plus standard care | NR | NR | 15% |
Continuous TOT plus moist wound care dressing plus standard care | NR | NR | 0% |
P value | NR | NR | 0.045 |
HTA = health technology assessment; NR = not reported; RCT = randomized controlled trial; SR = systematic review; TOT = topical oxygen therapy.
Table 14: Summary of Main Findings — Wound Recurrence or Wounds Staying Closed in Patients
Variable | Health Technology Wales (2022)16 – HTA (SR) | Nagarsheth et al. (2024)7 – SR | Tang et al. (2024)20 – NRS | Zulbaran-Rojas et al. (2023)19 – RCT | ||
|---|---|---|---|---|---|---|
Connaghan, 2021 (SR – 1 RCT) | Connaghan, 2021 (SR – 1 NRS) | Al-Jalodi, 2022 (Post hoc analysis of RCT) | MA of 2 double-arm studies (1 RCT, 1 NRS) | NA | NA | |
Total number of patients | 100 | 10 | 22a | 101 | 20 | 32 |
Follow-up | 12 weeks | 8 weeks | 1 year | 12 or 50 weeks | 12 weeks | 4 weeks |
Type of wound(s) included | DFUs | DFUs | DFUs | DFUs, venous ulcers | DFUs | Postsurgery |
Number of patients who had recurrence or reopening of wound | ||||||
CDO plus standard care | NR | 0 | NR | 4/66 | 0 | 1 |
Silicon CDO | NR | NR | NR | NR | NR | 0 |
Standard care | NR | 0 | NR | 16/35b | 0 | 2 |
Pooled odds ratio (95% CI) | NR | NR | NR | 0.08 (0.02 to 0.26) | NR | NR |
P value | NR | NR | NR | 0.001 | NR | NR |
I2 | NR | NR | NR | 45.99% | NR | NR |
Proportion of patients whose wound stays closed | ||||||
Continuous TOT plus standard care | 90% | NR | 85% | NR | NR | NR |
Standard care | 87.5% | NR | 60% | NR | NR | NR |
Statistical significance | Not significantly different | NR | Too small to reach statistical significance | NR | NR | NR |
DFU = diabetic foot ulcer; HTA = health technology assessment; ITT = intention-to-treat; NA = not applicable; NR = not reported; NRS = nonrandomized study; PP = per-protocol; RCT = randomized controlled trial; SR = systematic review; TOT = topical oxygen therapy.
Note: Recurrence typically defined as a wound emerging in the same area as the previously treated wound.
a29 participants consented to participants; 7 were lost to follow-up.
bMost of these events (14/30) occurred in the study of patients with venous ulcers.
Table 15: Summary of Findings by Outcome — Pain for Patients With Diabetic Foot Ulcers
Study citation and study design | For SRs: included studies (study design), follow-up | Method of measurement | Result | Notes |
|---|---|---|---|---|
Nagarsheth et al. (2024)7 SR-MA | 3 RCTs Follow-up: NR N =
| SMD of VAS between treatment and control arms (95% CI) | −0.17 (−0.92 to 0.59):
| NR |
Health Technology Wales (2022)16 SR | Connaghan, 2021 – includes 1 NRS Follow-up: 8 weeks N = 10 | Number of patients who rated their pain as 5 or higher on a scale of 1 to 10 (analogue scale) |
| NR |
Serena (2021) RCT Follow-up: 12 weeks N = 145; for PP analysis, N = 128 | VAS score, mean (SD) | ITT analysis
PP analysis
| Nagarsheth et al. (2024)’s MA includes the results from this study; however, it is unclear if they used the ITT or PP analysis results. | |
Tang et al. (2024)20 N = 33 Follow-up (days), mean (SD): 70.9 (33.0) after finishing 3 months of treatment | NA | Mean pain score based on the Diabetic Foot Ulcer Scale-Short Form (DFU-SF) |
| NR |
ITT = intention-to-treat; MA = meta-analysis; NA = not applicable; NR = not reported; PP = per-protocol; RCT = randomized controlled trial; SD = standard deviation; SMD = standardized mean difference; SR = systematic review; TOT = topical oxygen therapy; VAS = visual analogue scale.
Table 16: Summary of Findings by Outcome — General and Miscellaneous Adverse Events
Study citation and study design | For SRs: included studies (study design), follow-up | Method of measurement | Result | Notes |
|---|---|---|---|---|
Diabetic Foot Ulcers | ||||
Health Technology Wales (2022)16 HTA (SR) | Thanigaimani, 2021 (SR – includes 2 RCTs) Follow-up: 12 weeks N = 163 | Number of adverse events |
| None of the adverse events reported as related to the intervention. |
Number of serious adverse events |
| None of the adverse events reported as related to the intervention. | ||
Connaghan, 2021 (SR – includes 1 RCT) Follow-up: 12 weeks N = 124 | Proportion of patients who had infections |
| Not statistically significantly different. | |
Proportion of patients who had cellulitis incidents |
| Not statistically significantly different. | ||
Serena, 2021 – RCT Follow-up: 12 weeks N = 145 | Number of adverse events, n/N | Continuous TOT group:
Standard care group:
| Life-threatening adverse event reported as not related to the study. Unclear if any severe adverse events were due to the device; 2 events (1 intervention, 1 control) were deemed as possibly related to the intervention used. | |
Tang et al. (2024)20 NRS N = 33 Follow-up (days), mean (SD): 70.9 (33.0) after finishing 3 months of treatment | NA | Number of adverse events | 4 (all due to secondary infection) | NR |
CDO = continuous diffused oxygen; HTA = health technology assessment; NA = not applicable; NR = not reported; NRS = nonrandomized study; RCT = randomized controlled trial; SR = systematic review; TOT = topical oxygen therapy.
Table 17: Summary of Main Findings of Included Economic Evaluations
Outcome | Result |
|---|---|
Health Technology Wales (2022)16 | |
Total QALYs | |
Continuous TOT + standard of care | 7.89 |
Standard of care | 7.72 |
Incremental | 0.17 |
Total life-years | |
Continuous TOT + standard of care | 10.75 |
Standard of care | 10.59 |
Incremental | 0.17 |
Total costs per patient | |
Continuous TOT + standard of care | £35,786 |
Standard of care | £35,997 |
Incremental | -£211 |
ICER | Dominant (greater benefit at lower cost) |
Sensitivity analyses |
|
Author conclusions | “There appeared to be improvements across outcomes for DFUs, usually over a period of up to 12- weeks of continuous TOT-use, but up to one-year for some outcomes. However, the evidence we identified varied according to DFU aetiology, DFU grade, duration of continuous TOT treatment and follow-up times, duration of SoC prior to study, and type of SoC.”16 |
Chan and Campbell (2020) as reported in Health Technology Wales (2022)16 | |
Base-case, 5-year cost per person | |
CDO (US$), mean (95% CI) | $78,500 ($77,700 to $79,300) |
NPWT (US$), mean (95% CI) | $83,300 ($82,500 to $84,100) |
Mean difference (CDO – NPWT) | -$4,800 |
5-year QALYs per person | |
CDO, mean (95% CI) | 3.650 (3.639, 3.661) |
NPWT, mean (95% CI) | 3.625 (3.6137, 3.637) |
Mean difference (CDO – NPWT) | 0.025 |
ICER | Dominant (greater benefit at lower cost) |
For other scenario analyses (e.g., different time frames, comparators, costs, outcome variables, discount rates) |
|
Probabilistic sensitivity analysis results for 5,000 repetitions of the model simulation |
|
CDO = continuous diffusion oxygen; CI = confidence interval; DFU = diabetic foot ulcer; ICER = incremental cost-effectiveness ratio; NA = not applicable; NPWT = negative pressure wound therapy; NR = not reported; QALY = quality-adjusted life-year; TOT = topical oxygen therapy.
Table 18: Summary of Recommendations in Included Guidelines
Recommendations | Strength of recommendations, supporting evidence, and quality of evidence |
|---|---|
Guidelines on interventions to enhance healing of foot ulcers in people with diabetes (IWGDF 2023 update) (2023)23 | |
Recommendation: For DFUs where standard of care alone has failed and resources exist: consider using TOT as an adjunct therapy. | Strength of recommendation: Conditional; low. Supporting evidence: 3 double-blinded RCTs and 7 nonblinded studies, overall found moderate benefits on wound healing and reduced ulcer area but no evidence for reduced amputation up to 12 weeks; few reported adverse events. Quality of evidence: Evidence was of low certainty across different devices, and concerns were raised regarding the costs of single-use devices potentially reducing equity. Thus, although there was evidence favouring the intervention, a conditional recommendation was made. |
WHS (Wound Healing Society) guidelines update: Diabetic foot ulcer treatment guidelines24 | |
Guideline: “Topical oxygen has been shown to increase the incidence of healing and decrease the time to heal.”24 (p. 44) | Strength of recommendation: NR Supporting evidence: Cites 1 SR-MA, 1 SR, 3 double-blinded RCTs. Quality of evidence: Level I (high) |
Use of topical oxygen therapy in wound healing (2023)25 | |
Recommendation: TOT as an adjunctive therapy is endorsed for hard-to-heal wounds or wounds that have failed to reduce in size by at least 50% after 4 weeks of optimal standard of care. | Strength of recommendation: NR Supporting evidence: Several RCTs and NRSs indicated improved outcomes with CDO, including higher proportion of healed wounds, faster healing rates, greater reduction in wound area, and pain relief. Studies were primarily for patients with DFU, though review panels have suggested that venous leg ulcers and ischemic ulcers may be responsive to TOT as well. Quality of evidence for CDO: Grade A (high) |
Recommendation: TOT is generalizable to most nonneoplastic, hard-to-heal wounds (not just DFUs). Considering the use of TOT earlier for these wounds is appropriate. | Strength of recommendation: NR Supporting evidence: Cited 4 studies supporting use of TOT in venous leg ulcers and pressure ulcers. Quality of evidence: NR |
Recommendation: For patients with critical limb ischemia, there is insufficient evidence to support use of TOT. | Strength of recommendation: NR Supporting evidence: Limited evidence, insufficient to support use of TOT; anecdotal reports indicate it has been used in patients with no option for revascularization and only partial revascularization was achieved Quality of evidence: NR |
Recommendation: TOT can be considered for early treatment of ischemic DFUs. | Strength of recommendation: NR Supporting evidence: Unclear; may be based on RCTs and NRSs, but did not report if any of these studies were focused on ischemic DFUs. Quality of evidence: NR |
Recommendation: TOT should not be used:
| Strength of recommendation: NR Supporting evidence: NR Quality of evidence: NR |
Treatment algorithm: 1. If healing of the hard-to-heal wound has stalled (less than 50% size reduction after 4 weeks of standard care), consider topical oxygen therapy and reassess at 1 to 2 weeks. 2. If the wound is healing (more than 50% size reduction), continue topical oxygen therapy and reassess at 1 to 2 weeks. If healing is stalled, stop therapy and re-evaluate the wounds. 3. Continue to reassess every 1 to 2 weeks of topical oxygen therapy; continue to use if wound is healing and stop if healing has stalled. | Strength of recommendation: NR Supporting evidence: NR Quality of evidence: NR |
12. Retinopathy, neuropathy, and foot care: Standards of care in diabetes—202326 | |
Recommendation: For chronic DFUs that have failed to heal with optimal standard care alone, adjunctive treatment with RCT-proven agents should be considered, such as TOT. | Strength of recommendation: NR Supporting evidence: Several high-quality RCTs, at least 5 SR and meta-analyses. Quality of evidence: A (high) |
DFU = diabetic foot ulcer; CDO = continuous diffusion oxygen; IWGDF = International Working Group on the Diabetic Foot; MA = meta-analysis; NR = not reported; NRS = nonrandomized study; RCT = randomized controlled trial; SR = systematic review; TOT = topical oxygen therapy.
Appendix 6: Overlap Between Included SRs
Note this appendix has not been copy-edited.
Table 19: Overlap in Relevant Primary Studies Between Included SRs
Primary study citation | Chen et al. (2024)18 | Nagarsheth et al. (2024)7 | Sýkorová et al. (2024)17 | Health Technology Wales (2022)16 |
|---|---|---|---|---|
Ahmadinejad M et al. Int J Pharm Phytopharm Res. 2020;10(1):61 to 9. | — | Yes | — | — |
Al‐Jalodi O et al. Int Wound J. 2022;19(7):1838 to 1842 | — | — | Yes | Yes |
Altinbas O and Şahsıvar MO. Ann Clin Anal Med. 2022;13(1):50 to 3. | — | Yes | Yes | Yes |
Azimian J et al. Iran Red Crescent Med J. 2015;17:e20211. | — | Yes | — | — |
Cole W et al. Wounds. 2020;32:294e298. | — | Yes | — | — |
Copeland K and Purvis AR. Adv Wound Care. 2017;6:143e152. | — | Yes | — | — |
Driver VR et al. Ostomy/Wound Manag. 2013;59:19e26.d | — | Yes | Yes | Yesa |
Driver VR et al. Ostomy/Wound Manag. 2017;63:12e28.d | Yes | Yes | Yesa | Yesa |
Frykberg RG et al. Diabetes Care. 2020;43:616e624. | Yes | Yes | Yesa | Yesa |
Hayes PD et al. J Wound Care. 2017;26:652e660. | — | Yes | — | Yesa |
He S et al. Diabetes Res Clin Pract. 2021;174:108743. | Yes | — | Yes | Yes |
Hunter P et al. Wounds. 2020;32:81e85. | — | Yes | — | — |
Igwegbe I et al. Adv Skin Wound Care. 2015;28: 206e210. | — | Yes | — | — |
Kaufman H et al. J Wound Care. 2018;27: 426e433. | — | Yes | — | Yes |
Kaufman H et al. Wounds Int. 2021;12:63 to 8. | — | — | — | Yes |
Massenburg BB and Himel HN. J Wound Care. 2016;25:S23eS27. | — | Yes | — | — |
Niederauer MQ et al. Wound Med. 2015 Apr 1;8:19 to 23.c,d | — | — | Yesc | — |
Niederauer MQ et al. J Diabetes Sci Technol. 2017;11(5):883 to 891.d | — | Yes | Yes | Yes a |
Niederauer MQ et al. J Wound Care. 2018;27: S30eS45. | Yes | — | Yesa | Yesa |
Otaviano MH et al. Braz J Infect Dis. 2021;25:1e9. | — | Yes | — | — |
Segev R. Nephrol Nurs J. 2019;46:330e336. | — | Yes | — | — |
Serena TE et al. J Wound Care. 2021;30:S7eS14 | Yes | Yes | Yesa | Yes |
Song Z et al. Am J Transl Res. 2021;13:7294e7299. | — | Yes | — | — |
Tang TY et al. Int J Low Extrem Wounds. 2021:15347346211053694. | — | Yes | Yes | — |
Tawfick WA and Sultan S. Vasc Endovascular Surg. 2013;47:30e37. | — | Yes | — | — |
Varetto G et al. Ann Vasc Surg. 2020;64: 246e252. | — | Yes | — | — |
Wang S et al. Ann Palliat Med. 2021;10(2):973‐983. | Yes | — | — | — |
Woo KY et al. Adv Skin Wound Care. 2012;25:543e547.d | — | Yes | — | — |
Yu J et al. Wound Repair Regen. 2016;24(6):1066‐1072.d | Yes | — | Yes | Yesb |
Zulbaran-Rojas A et al. J Surg Res. 2021;268:585 to 594. | — | — | Yes | — |
— = not included in the systematic review; SR = systematic review.
Notes: Sýkorová et al. (2024) and Health Technology Wales (2022) included and reported findings from previous systematic reviews (SRs). These have been indicated with letters as described below. For example, Health Technology Wales (2022) included an SR by Connaghan et al. (2021), which included 2 randomized controlled trials and 2 nonrandomized studies; these 4 primary studies are indicated in the table as “Yes” with a footnote “a”; Sýkorová et al. (2024) included several relevant SRs. The primary studies included in these SRs have all been included in other SRs that are included in this report.
aIndicates a primary study that was included as part of an SR; the author of the report presented findings from the SR.
bIndicates a primary study that was included as part of an SR; the author of the report presented findings from the SR as well as results from the original primary study that were not presented in the SR.
cWhile the results from Niederauer (2015) were reported, the review authors noted that these are interim findings, with the final results published in Niederauer (2017). To avoid double-counting, the findings from Niederauer (2015) have not been included in this report.
dIndicates studies that were identified by and described in our previous report published in 202014 reviewing continuously diffused oxygen for wound healing.
Appendix 7: References of Potential Interest
Note this appendix has not been copy-edited.
Previous CADTH Reports
Continuously diffused oxygen therapy for wound healing: a review of the clinical effectiveness, cost-effectiveness, and guidelines. (CADTH Rapid response report: summary with critical appraisal). Ottawa (ON): CADTH; 2020. PubMed: PM33289990
Nonrandomized Studies
Unclear Methods
Su S, Ding X, Zou H, et al. Wound management of multi-site pressure ulcer at different stages in elderly patients. Clin Cosmet Investig Dermatol. 2021;14:747-751. PubMed: PM34234500
Alternative Outcome
Hunter P, Greco E, Cross K, Perry J. Topical oxygen therapy shifts microbiome dynamics in chronic diabetic foot ulcers. Wounds. 2020 Mar;32(3):81-85. PubMed: PM32163040
Case Series
Cole W, Woodmansey E. Monitoring the effect of continuous topical oxygen therapy with near-infrared spectroscopy: a pilot case series in wound healing. Wounds. 2024 05;36(5):154-159. PubMed: PM38861210
Lee A, Woodmansey E, Klopfenstein B, O'Leary JL, Cole W. Remote assessment and monitoring with advanced wound therapy to optimise clinical outcomes, access and resources. J Wound Care. 2024 Feb 02;33(2):90-101. PubMed: PM38329827
Cole W, Woodmansey E, LoDico III LR. Management of late radiation tissue injury ulcers with continuous topical oxygen therapy supports wound healing in patients of advanced age following Mohs surgery: a case series. Wounds. 2023 12;35(12):E420-E424. PubMed: PM38277630
Jebril W, Nowak M, Palin L, Nordgren M, Bachar-Wikstrom E, Wikstrom JD. Topical oxygen treatment relieves pain from hard-to-heal leg ulcers and improves healing: a case series. J Wound Care. 2022 Jan 02;31(1):4-11. PubMed: PM35077209
Tabanjeh SF, Al-Malki T, Alhazzani AR, Robert AA. Management of Diabetic Foot Ulcers Using Topical oxygen Therapy: a case series. Curr Diabetes Rev. 2022;18(6):e051021196984. PubMed: PM34636303
Guidelines and Recommendations
Consensus-Based Methodology
Bem R, Chadwick P, Cvjetko I, Koliba M, Kokeny Z, Lipinski P, Mrozikiewicz-Rakowska B, Rozsos I, Wegrzynowski A. A new algorithm for the management of diabetic foot ulcer: recommendations from Central and Eastern Europe. J Wound Care. 2023 May 2;32(5):264-72. https://www.magonlinelibrary.com/doi/full/10.12968/jowc.2023.32.5.264 Accessed 2024 Jul 2. PubMed
Wounds International: International consensus document on diabetic foot ulcer care in the Asia-Pacific region (2022) https://woundsinternational.com/wp-content/uploads/sites/8/2023/02/065579205d506991f8070505779d5ba3.pdf Accessed 2024 Jun 26.
Serena T, Andersen C, Cole W, Garoufalis M, Frykberg R. Guidelines for the use of topical oxygen therapy in the treatment of hard-to-heal wounds based on a Delphi consensus. J Wound Care. 2021 Sep 1;30(Sup9):S30-4. https://www.magonlinelibrary.com/doi/abs/10.12968/jowc.2021.30.Sup9.S30 Accessed 2024 Jul 3.
Review Articles
Oyebode OA, Jere SW, Houreld NN. Current therapeutic modalities for the management of chronic diabetic wounds of the foot. J Diabetes Res. 2023;2023:1359537. PubMed: PM36818748
Ngeow WC, Tan CC, Goh YC, Deliberador TM, Cheah CW. A narrative review on means to promote oxygenation and angiogenesis in oral wound healing. Bioengineering (Basel). 2022 Nov 02;9(11):02. PubMed: PM36354548
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up to date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for noncommercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca