CADTH Health Technology Review
Short-Cycle Autoclave Sterilization of Instruments in Same-Day Ophthalmic Surgeries
Rapid Review
Key Messages
What Is the Issue?
The volume of ophthalmic surgeries is increasingly high, with cataract surgery being 1 of the most performed surgeries in Canada.
Infections following ophthalmic surgeries, while rare, can cause severe complications that may lead to irreversible vision loss. Reducing postsurgery infections is a high priority in clinical practice.
Running a full wrapped, terminal steam sterilization cycle for ophthalmic instruments in autoclaves may be inefficient for ophthalmic surgeries and may cause unnecessary heavy economic and environmental burdens due to high surgical volumes.
Using instruments sterilized on a short cycle between sequential same-day ophthalmic surgeries may help improve efficiency and reduce resources used. These instruments are generally processed using autoclaves (i.e., steam sterilizers); the effectiveness of a shorter-cycle method of sterilization is unclear.
What Did We Do?
To inform decisions regarding the use of autoclaves for short-cycle sterilization for sequential same-day instrument use in ophthalmic surgery, we sought to identify and summarize evidence comparing this method to full-cycle sterilization of wrapped instruments and identify any relevant recommendations.
We searched key resources, including journal citation databases, and conducted a focused internet search for relevant evidence published since 2012. One reviewer screened articles for inclusion based on predefined criteria.
What Did We Find?
In a laboratory setting to simulate sequential same-day procedures, short-cycle sterilization with interrupted dry time for unwrapped ophthalmic instruments is feasibly as effective as full-cycle sterilization for wrapped instruments using the STATIM autoclave. Similarly, short-cycle sterilization with interrupted dry time for contained ophthalmic instruments is feasibly as effective as full-cycle sterilization for contained instruments using the AMSCO autoclave.
For sequential same-day ophthalmic procedures, wet instruments sterilized by a short-cycle process with an interrupted dry time can remain sterile for at least 3 minutes if kept in a covered sterilizer containment device.
One guideline recommends that wrapped or unwrapped ophthalmic instruments sterilized by a short-cycle process without full drying should be stored in a covered containment device until retrieved by staff wearing sterile gloves and gowns in the operating room for the subsequent surgery after a short delay. Phaco handpieces should be immediately primed with a balanced salt solution and remain wet as they sit on the sterile instrument table.
We did not identify any clinical setting evidence from studies or autoclave manufacturers. It is unclear if clinical outcomes differ between patients undergoing sequential same-day ophthalmic surgeries using short-cycle sterilized instruments and those undergoing surgery using full-cycle sterilized instruments.
What Does This Mean?
Preliminary laboratory evidence and guideline recommendations supporting the use of autoclaves for short-cycle sterilization of instruments for sequential same-day ophthalmic surgeries are available. However, there is no clinical effectiveness evidence available on this process in patient settings.
Future research is necessary to understand the clinical safety of using instruments sterilized by short cycles for sequential same-day use for patients undergoing ophthalmic surgeries.
In addition to the evidence and recommendations identified, other factors, such as environmental influence, may be useful considerations when making decisions about short-cycle sterilization for sequential same-day instrument use for ophthalmic surgery.
Abbreviations
IFU
instructions for use
Context and Policy Issues
What Is an Autoclave?
Autoclaves, also known as steam sterilizers, are widely used to sterilize critical instruments such as surgical instruments, which make direct contact with blood or sterile tissue and increase the risk of infections if contaminated.1 In the autoclave, instruments are exposed to saturated steam contact at the required temperature and pressure for a specified time to destroy all microorganisms. The required sterilization time varies based on the instrument type, packaging (i.e., wrapped or unwrapped), and the type of autoclave used.2 Depending on the manufacturers’ instructions for use (IFU), short sterilization cycles may range from 3 minutes to 3.5 minutes, while long cycles may last from 15 minutes to 45 minutes.3-5 In this report, full-cycle sterilization is defined as using a long sterilization time with a full drying phase.
Ophthalmic Surgeries in Canada
The volume of ophthalmic interventions increased by 30% from 2014 to 2018 in Canada, reaching more than 1 million in 2018.6 This trend continued, with 1 million ophthalmic procedures reported again in 2021.7 Cataract surgery, an ambulatory surgery to replace a cloudy lens with a clear artificial lens, is 1 of the most performed surgeries in Canada and globally, with 415,923 completed in 2018 in Canada.6,8 It is estimated that 527,491 and 643,009 cataract surgeries will be performed in Canada in 2030 and 2040, respectively.6
The infection rate following ophthalmic surgeries in Canada is unclear. In Canada, the annual incidence of endophthalmitis after cataract surgery was estimated to be 1.4 to 1.5 per 1,000 surgical procedures.9 Endophthalmitis is a serious complication caused by fungal and bacterial infections in the eye and can result in irreversible vision loss.10
What Is Sequential Same-Day Instrument Use and Short-Cycle Sterilization?
Sequential same-day instrument use for ophthalmic surgery means using sterilized instruments for subsequent ophthalmic surgeries on the same day after they are resterilized.11 Short-cycle steam sterilization is commonly used for consecutive procedures, whereas complete terminal, wrapped sterilization cycles are used for instruments stored overnight.12 The US Centers for Medicare & Medicaid Services defines short-cycle steam sterilization as a terminal sterilization acceptable for routine use for a wrapped or contained load where instruments are precleaned based on the IFU, the load meets the IFU, includes drying time, and the load is packaged in a wrap or rigid sterilization container validated for later use.13 This process is different from immediate-use steam sterilization, which allows for minimal or no drying after the sterilization cycle and is not intended for storage for later use.14,15 By contrast, short-cycle steam sterilization includes drying time and packing for storage.13
What Is the Current Practice and Why Is It Important to Do This Review?
A US survey of 182 ophthalmic ambulatory surgical settings found that 52.3% routinely used short-cycle sterilization between sequential same-day surgeries. The survey reported a 12-month infection rate of 0.02% for all ophthalmic surgeries.11,12 Canadian guidelines regarding the sterilization of general surgical instruments do not recommend routine use of immediate-use steam sterilization. 12 These guideline recommendations were focused on all critical medical devices and did not specifically consider ophthalmic surgical instruments, which are small and generally not heavily soiled.12 The use of short-cycle sterilization for ophthalmic surgeries in Canada and any relevant recommendations are not known.
The full wrapped, terminal sterilization cycle may result in unnecessary inefficiency of cataract surgeries, 1 of the highest volume procedures in Canada, and may cause heavy economic and environmental burdens.6,8 One study found that the large volume of cataract surgeries in Canada led to substantial waste and a high carbon footprint. The study suggested that more efficient autoclave settings could mitigate some of this environmental impact. It also found that short-cycle sterilization for ophthalmic surgery was safe, efficient, and sustainable for cataract surgery.8
STATIM and AMSCO autoclaves are the most common autoclaves used for sequential same-day ophthalmic procedures in the US;11,12 the prevalence of use in Canada is unclear. These autoclaves, which have different modes with varying sterilization and drying times,3,4 have been approved by the US FDA for sterilization based on nonclinical performance data and have also been approved by Health Canada for steam sterilization (not specifically for ophthalmic use).16,17 The drying phase in the sterilization cycle helps prevent potential recontamination of wet sterilized instruments.18 The STATIM and AMSCO autoclaves allow interruption during the drying phase.11 However, the clinical effectiveness and safety of short-cycle sterilization with interrupted drying for instruments used between sequential same-day ophthalmic surgeries has not yet been established. It is unknown whether this method is equivalent to full-cycle sterilization in the clinical setting.
Objective
This review summarizes and critically appraises evidence identified from medical databases and grey literature regarding the use of autoclaves for sequential same-day instrument use for ophthalmic surgery.
Research Questions
What is the clinical effectiveness of short-cycle autoclave sterilization of instruments used in sequential same-day ophthalmic surgeries compared with those that have undergone full-cycle sterilization?
If any, what are the recommended conditions to follow after instruments are sterilized using short-cycle autoclave sterilization for sequential same-day use in ophthalmic surgeries?
Methods
An information specialist conducted a customized literature search, balancing comprehensiveness with relevancy, of multiple sources and grey literature on June 24, 2024.
One reviewer screened citations and selected studies based on the inclusion criteria presented in Table 1 and critically appraised included publications using established critical appraisal tools.
Appendix 1 presents a detailed description of methods.
Criteria | Description |
|---|---|
Population | Patients undergoing ophthalmic procedures |
Intervention | Use of short-cycle autoclave sterilization for sequential same-day instrument use for ophthalmic surgeries |
Comparator | Q1: Full-cycle sterilization of wrapped instrumentation Q2: NA |
Outcomes | Q1: Sterility, infection rates, sterilization time Q2: Recommendations regarding best practices (e.g., appropriate handling of instruments sterilized by short-cycle autoclave sterilization for sequential same-day use in ophthalmic surgeries) |
Study designs | Health technology assessments, guidelines, systematic reviews, randomized controlled trials, nonrandomized studies |
Publication date | Since January 1, 2012 |
NA = not applicable.
Summary of Evidence
Quantity of Research Available
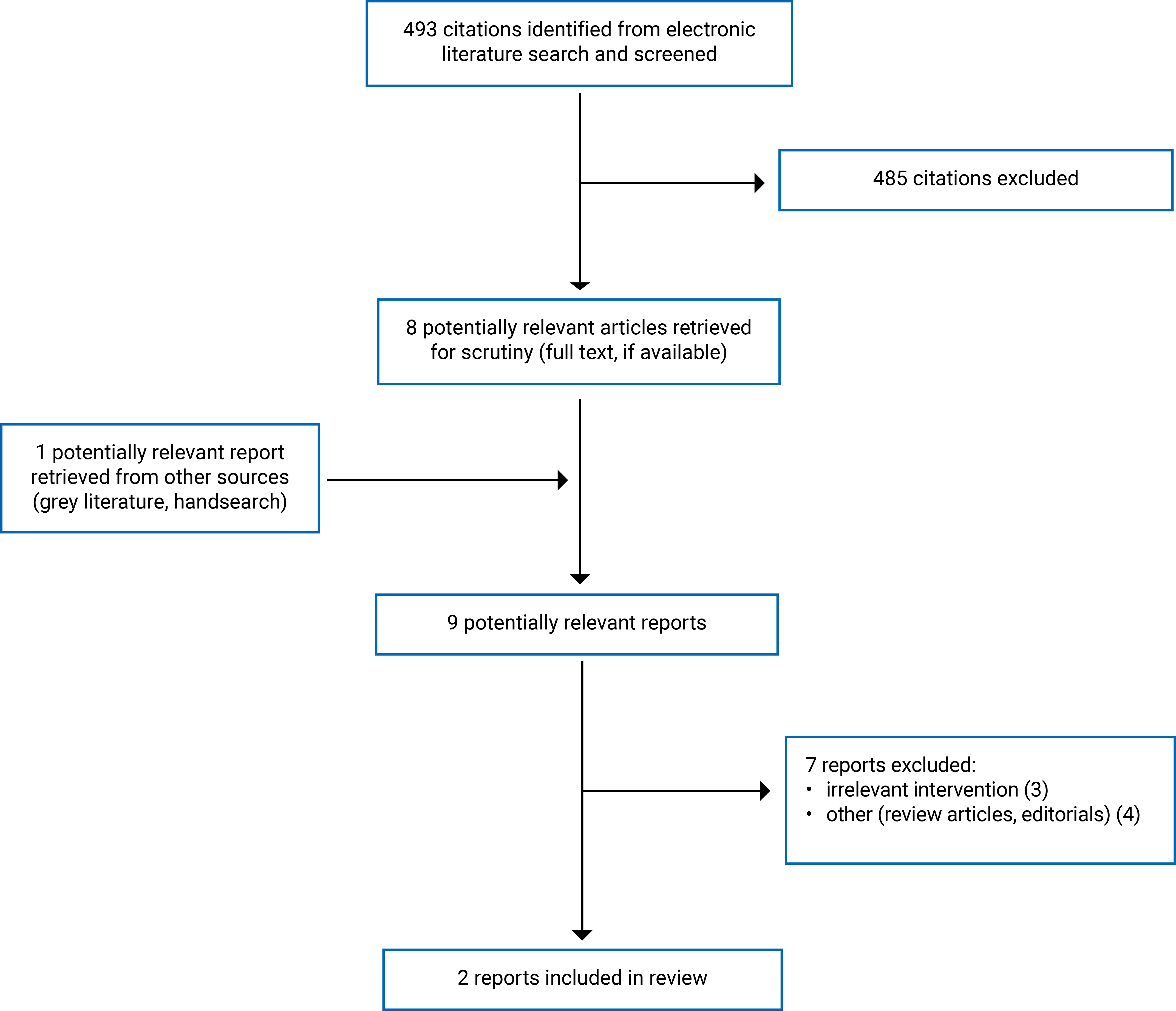
This report includes 1 laboratory sterility validation study11 and 1 guideline.12 We did not identify any health technology assessments, systematic reviews, randomized controlled trials, or nonrandomized studies that met the inclusion criteria. Figure 1 (Appendix 2) presents the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA)19 flow chart of the study selection. Appendix 6 presents additional references of potential interest.
Summary of Study Characteristics
Summaries of study characteristics are organized by research questions. Additional details regarding the characteristics of the included publications are provided in Appendix 3.
Included Studies for Research Question 1
We found 1 laboratory sterilization validation study comparing the effectiveness of short-cycle sterilization with interrupted air-dry phase, simulating the use for consecutive same-day cataract procedures, to full-cycle wrapped or contained sterilization. The instruments involved were phaco tips and handpieces inoculated with Geobacillus stearothermophilus, a highly heat-resistant bacterium, to assess sterility based on microbial growth. The presence of the bacterium after sterilization indicated inadequate sterility.11 The study used 2 brands of autoclaves, STATIM and AMSCO Century, both approved by the FDA and Health Canada.11,16,17 The study also tested the moisture sterility, meaning the sterility of the wet unwrapped and contained instruments that were kept in a covered container after short-cycle sterilization with interrupted drying time.11
Included Studies for Research Question 2
We found 1 consensus-based guideline published in 2018 by the US Ophthalmic Instrument Cleaning and Sterilization Task Force.12 Recommendations regarding short-cycle sterilization of ophthalmic instruments for sequential same-day use were based on data from the sterilizer manufacturers and the study included in this report.11,12 Details about the manufacturer data were not reported.
Summary of Critical Appraisal
Primary Study
The sterility validation study clearly stated the objective, the sterilization process being tested, the comparator (for the comparative validation), instruments used, and outcomes.11 The researchers noted that the phaco handpieces used in validation (for both short- and full-cycle sterilization) represented the worst-case scenario for ophthalmic instrument sterilization due to their large size and small lumens, which makes them the most difficult items to sterilize on a cataract tray.11,12 The testing followed US and international validation standards, with 3 repetitive test cycles for each sterility verification test to ensure reproducibility. The study also used environmental, negative, and positive control biological indicators, although details were not provided. Additionally, a visual indicator was used to document the required steam sterilization parameter. Sources of funding were disclosed.11
An additional limitation was that no patients were involved in the study, making it impossible to infer how this process may influence patient outcomes, such as postsurgery infection rates. Therefore, the study may have a high risk of bias due to limited external validity to the clinical setting. The single-arm validation of moisture sterility was difficult to interpret without a comparator. This study provides some insight into moisture sterility.11
Guideline
The included guideline was of low methodological quality. It clearly outlined its scope and purpose, including objectives, health questions, and the sterilization procedure to which the recommendations were meant to apply. The guideline development group included individuals from relevant professional groups. The benefits and risks were considered in formulating the recommendation.12
The rigour of guideline development was reduced because a systematic search for research evidence was not performed.12 Recommendations relevant to short-cycle sterilization for sequential same-day use were mainly supported by a study performed by the guideline development group members. This study included validation of the sterilization process in a laboratory setting.11,12 The guideline did not evaluate the quality of the evidence nor the strength of the recommendations. In addition, it did not include an external expert review, details of the expert consensus process, or the procedure for guideline update.12 The guideline provided advice on how the recommendations can be put into practice and considered potential resource implication but did not present monitoring or auditing criteria. For editorial independence, the guideline reported no competing interests of development group members, but it did not clarify whether the funding body influenced the guideline content.12 Additional details regarding the strengths and limitations of the guidelines included are provided in Appendix 4.
Summary of Findings
The main findings from the included publications are summarized in the following sections and Appendix 5.
Effectiveness of Short-Cycle Sterilization
Short-Cycle Sterilization Versus Full-Cycle Sterilization
Sterility
Chang and colleagues assessed the sterility of ophthalmic instruments processed by short-cycle sterilization compared with full-cycle sterilization.11 They found the following:
Using the STATIM 2000 autoclave, all inoculated test samples were negative for growth of the target organism (G. stearothermophilus) in both unwrapped short and wrapped full sterilization cycles.
Using the AMSCO Century V116 prevacuum autoclave, all inoculated test samples were negative for growth of the target organism in both contained short and full sterilization cycles.
These findings indicated that even when the drying time was interrupted, short cycles following the IFU can effectively sterilize inoculated unwrapped and contained instruments using the STATIM and AMSCO autoclaves, respectively.11
Sterilization Time
Chang and colleagues reported the sterilization times of short and full cycles for the 2 autoclaves used in the study:11
STATIM 2000 autoclave
unwrapped, short-cycle sterilization included a 3.5-minute exposure time with a 1-minute drying time
wrapped, full-cycle sterilization included a 10-minute exposure time with a 1-hour drying time
AMSCO Century V116 prevacuum autoclave
contained, short-cycle sterilization included a 3-minute exposure time with a 1-minute drying time
contained, full-cycle sterilization included a 3-minute exposure time with a 20-minute drying time
Moisture Sterility After Short-Cycle Sterilization
Chang and colleagues tested the moisture sterility of phaco handpieces kept within a covered containment device for 3 minutes after short-cycle unwrapped and contained sterilization with a 1-minute drying time using the STATIM and AMSCO autoclaves.11 The 3-minute storage and transit time represented the maximum time required to transport the containment device to the operating room for subsequent prompt use. They found no growth of the target organism in all inoculated test samples, indicating the wet unwrapped or contained instruments were not contaminated by moisture within the containment device for at least 3 minutes.
The study concluded that a full drying phase was unnecessary when the wet sterilized instruments were kept within the covered containment device for prompt use in a sequential surgery.
Published Recommendations Regarding Short-Cycle Sterilization
The 2018 US Ophthalmic Instrument Cleaning and Sterilization Task Force guideline recommends unwrapped, short-cycle sterilization adhering to the IFU of US FDA-approved sterilizers for routine use between sequential same-day ophthalmic surgeries.12 Table 7 (Appendix 5) presents details of the recommendations.
The guideline also suggests adhering to the following conditions after the short-cycle sterilization phase without full drying, specifically noting:
“Complete drying is not necessary to maintain the sterility of wrapped or unwrapped ophthalmic instruments that are kept in the covered containment device until retrieved by sterile gloved and gowned staff within the OR [operating room] for the subsequent case after some short delay.”
“Phaco handpieces are immediately primed with a balanced salt solution and remain wet as they sit on the sterile instrument table.”
Limitations
Evidence Gap
We did not identify any evidence about the potential impact of using instruments sterilized by shorter autoclave cycles for sequential same-day ophthalmic surgeries on patient health outcomes, such as infection rates after ophthalmic procedures.
Generalizability
Chang and colleagues validated the laboratory sterility of the STATIM and AMSCO autoclaves only, and the generalizability to other brands of autoclaves is unknown.11 Recommendations included in this report by the US Ophthalmic Instrument Cleaning and Sterilization Task Force were developed mainly based on this study because the STATIM and AMSCO autoclaves were commonly used for short-term sterilization in the US.11,12 Although the STATIM and AMSCO sterilizers are approved by Health Canada,16,17 their prevalence in Canada is uncertain. Therefore, the generalizability of recommendations to health care settings in Canada is unknown.
Conclusions and Implications for Decision- or Policy-Making
This report included 1 laboratory validation study11 and 1 guideline regarding the use of short-cycle autoclave sterilization for sequential same-day instrument use in ophthalmic surgeries.12 The study findings had limited generalizability to the clinical setting, and the guideline was of low methodological quality. No literature investigating patient health outcomes was identified. More evidence on patient infection rates is needed to inform the clinical effectiveness of autoclaves for short-cycle sterilization for sequential same-day instrument use for ophthalmic surgery.
When adhering to the IFU, short-cycle sterilization of 3-minute exposure and 1-minute drying time, simulating sequential same-day procedures, for unwrapped ophthalmic instrument loads is feasibly as effective as full-cycle sterilization for wrapped instruments using the STATIM autoclave in the laboratory setting.
Similarly, 3.5-minute sterilization and 1-minute drying time for contained ophthalmic instrument loads using the AMSCO autoclave is feasibly as effective as full-cycle sterilization for contained instruments in the laboratory setting. Additionally, the sterility of wet instruments sterilized by the 3-minute to 3.5-minute short-cycle process and dried for 1 minute can be maintained for at least 3 minutes if kept in a covered sterilizer containment device.11 However, it is unclear if clinical outcomes differ between patients undergoing ophthalmic surgeries with short-cycle sterilized instruments and those undergoing surgery with full-cycle sterilized instruments. Based on the included study and manufacturer data, the US Ophthalmic Instrument Cleaning and Sterilization Task Force supports unwrapped, short-cycle sterilization adhering to the IFU of US FDA-approved sterilizers for routine use between sequential same-day ophthalmic surgeries.12
Considerations for Future Research
The evidence included in this report was from a laboratory study without patient participation.11 We found no evidence regarding patient outcomes after using instruments sterilized by a shorter-cycle process for sequential same-day ophthalmic surgeries compared with the full-cycle process. Researchers should consider assessing the clinical effectiveness of short-cycle sterilization using autoclaves for ophthalmic instruments used between sequential same-day surgeries to understand its influence on patient health status.
Implications for Clinical Practice
Evidence identified in this report may provide some preliminary insights into the effectiveness of short-cycle autoclave sterilization in the laboratory setting, simulating sequential same-day instrument use in ophthalmic surgeries in the clinical setting.11 No evidence is available to provide conclusions on the equivalency of short-cycle sterilization or the potential harm or benefits for patients undergoing sequential same-day ophthalmic procedures. Recommendations included in this report require caution in interpretation.11,12 In addition to the laboratory evidence, decision-makers may wish to consider whether short-cycle sterilization of instruments for sequential same-day ophthalmic surgeries would help reduce the environmental impact of high-volume cataract surgeries.
References
1.US Centers for Disease Control and Prevention. Sterilization. 2023; https://www.cdc.gov/infection-control/hcp/disinfection-sterilization/sterilization.html. Accessed 2024 Jul 18.
2.US Centers for Disease Control and Prevention. Steam sterilization. 2023; https://www.cdc.gov/infection-control/hcp/disinfection-sterilization/steam-sterilization.html. Accessed 2024 Jul 18.
3.U.S. Food and Drug Administration. Center for Devices and Radiological Health. 510(k) Summary for the STATIM 5000 Cassette Autoclave. Silver Spring (MD): U.S. Food and Drug Administration (FDA); 1996: https://www.accessdata.fda.gov/cdrh_docs/pdf/K962179.pdf. Accessed 2024 Jul 25.
4.U.S. Food and Drug Administration. Department of Health and Human Services. Correspondence. AMSCO 400 Small Steam Sterilizers, AMSCO 400 Medium Steam Sterilizers. Company: STERIS Corporation. 501(K) Number: K212424. Approval date: 2021 Oct 28. (FDA approval package). Silver Spring (MD): U.S. Food and Drug Administration (FDA); 2021: https://www.accessdata.fda.gov/cdrh_docs/pdf21/K212424.pdf. Accessed 2024 Jul 25.
5.SciCan. STATIM G4 Sterilization Cycle Specifications. 2024: https://www.scican.com/eu/products/autoclaves/statim/. Accessed 2024 Jul 30.
6.Gagnon-Arpin I, Moroz N, Slovinec D’Angelo M, Ye Z. Ophthalmology in Canada: Why vision loss should not be overlooked Ottawa (ON): The Conference Board of Canada; 2020: https://www.cos-sco.ca/wp-content/uploads/2022/04/10874_IP_Ophthalmology-in-Canada.pdf. Accessed 2024 Jul 18.
7.Canadian Ophthalmological Society Submission to the Standing Committee on Health Canada’s Health Workforce. Ottawa (ON): Canadian Ophthalmological Society; 2022: https://www.ourcommons.ca/Content/Committee/441/HESA/Brief/BR11634687/br-external/CanadianOphthalmologicalSociety-e.pdf. Accessed 2024 Jul 29.
8.Taboun OS, Orr SMA, Pereira A, Choudhry N. Factors contributing to the carbon footprint of cataract surgery. J Cataract Refract Surg. 2023;49(7):759-763. PubMed
9.Freeman EE, Roy-Gagnon MH, Fortin E, Gauthier D, Popescu M, Boisjoly H. Rate of endophthalmitis after cataract surgery in Quebec, Canada, 1996-2005. Arch Ophthalmol. 2010;128(2):230-234. PubMed
10.Wadbudhe AM, Tidke SC, Tidake PK. Endophthalmitis after cataract surgery: A postoperative complication. Cureus. 2022;14(10):e30110. PubMed
11.Chang DF, Hurley N, Mamalis N, Whitman J. Evaluation of ophthalmic surgical instrument sterility using short-cycle sterilization for sequential same-day use. Ophthalmology. 2018;125(9):1320-1324. PubMed
12.Chang DF, Mamalis N, Ophthalmic Instrument Cleaning and Sterilization Task Force. Guidelines for the cleaning and sterilization of intraocular surgical instruments. J Cataract Refract Surg. 2018;44(6):765-773. PubMed
13.Change in terminology and update of Survey and Certification (S&C) memorandum 09-55 regarding immediate use steam sterilization (IUSS) in surgical settings (Ref: S&C: 14-44-Hospital/CAH/ASC). Baltimore (MD): US Centers for Medicare & Medicaid Services; 2014: https://www.cms.gov/medicare/provider-enrollment-and-certification/surveycertificationgeninfo/downloads/survey-and-cert-letter-14-44.pdf. Accessed 2024 Jul 18.
14.Best practice guidelines for cleaning, disinfection and sterilization of critical and semi-critical medical devices Victoria (BC): BC Ministry of Health; 2011: https://divisionsbc.ca/sites/default/files/Divisions/Burnaby/Best-practice-guidelines-cleaning.pdf. Accessed 2024 Jul 18.
15.Best practices for cleaning, disinfection and sterilization of medical equipment/devices. Toronto (ON): Ontario Agency for Health Protection and Promotion (Public Health Ontario); 2013: https://www.publichealthontario.ca/-/media/documents/B/2013/bp-cleaning-disinfection-sterilization-hcs.pdf. Accessed 2024 Jul 18.
16.Steris Mexico; company ID 129044. Medical devices active listing (MDALL): Active licence listing by company. 2024; https://health-products.canada.ca/mdall-limh/information?companyId=129044&lang=eng. Accessed 2024 Jul 18.
17.STATIM cassette autoclaves; licence no. 108053. Medical devices active listing (MDALL). 2024; https://health-products.canada.ca/mdall-limh/index-eng.jsp. Accessed 2024 Jul 18.
18.Chobin N. Drying is a critical phase of the sterilization process. 2017; https://www.infectioncontroltoday.com/view/drying-critical-phase-sterilization-process.
19.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
20.Agree Next Steps Consortium. The AGREE II Instrument. Hamilton (ON): AGREE Enterprise; 2017: https://www.agreetrust.org/wp-content/uploads/2017/12/AGREE-II-Users-Manual-and-23-item-Instrument-2009-Update-2017.pdf. Accessed 2024 Jul 18.
Appendix 1: Detailed Methods and Selection of Included Studies
Note that this appendix has not been copy-edited.
Literature Search Methods
An information specialist conducted a literature search on key resources including MEDLINE, Embase, the Cochrane Database of Systematic Reviews, the International HTA Database, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search approach was customized to retrieve a limited set of results, balancing comprehensiveness with relevancy. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. Search concepts were developed based on the elements of the research questions and selection criteria. The main search concepts were steam autoclaves and ophthalmology. Search filters were applied to limit retrieval to health technology assessments, systematic reviews, meta-analyses, or indirect treatment comparisons, randomized controlled trials, controlled clinical trials, or any other type of clinical trial, and guidelines. Conference abstracts and conference reviews were excluded. The search was completed on June 18, 2024, and limited to English-language documents published since January 1, 2019.
Based on further discussions, an expanded search was completed on June 24, 2024. The main search concepts were sterilization methods, eye surgery, and ophthalmological instruments. The search incorporated English-language documents published since January 1, 2012. No search filters were applied, and conference abstracts and conference reviews were excluded.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1. Figure 1 presents the PRISMA19 flow chart of the study selection.
Exclusion Criteria
We excluded publications if they did not meet the selection criteria outlined in Table 1, they were duplicate publications, or were published before 2012.
Critical Appraisal of Individual Studies
The included guideline was critically appraised by 1 reviewer using the Appraisal of Guidelines for Research and Evaluation (AGREE) II instrument.20 Summary scores were not calculated for the included guideline; rather, the strengths and limitations were described narratively. The reviewer also summarized the strengths and limitations of the included laboratory study narratively.
Appendix 2: Selection of Included Studies
Appendix 3: Characteristics of Included Publications
Note that this appendix has not been copy-edited.
Table 2: Characteristics of the Included Study
Study citation, country, funding source, study design | Study setting, instruments | Interventions, comparators | Relevant outcomes |
|---|---|---|---|
Chang et al. (2018)11 US Funding source: the Ophthalmic Outpatient Surgery Society, the American Society of Cataract and Refractive Surgery, and the American Academy of Ophthalmology Sterilization method validation study | Setting: An independent medical device validation testing laboratory Instruments used for validation: Phaco tips and handpiecesa from 3 manufacturers: the Infiniti (Alcon, Fort Worth, TX), the Signature (Abbott Medical Optics/Johnson & Johnson Vision, Santa Ana, CA), and the Stellaris (Bausch & Lomb, Rochester, NY) phaco platforms. Instruments were inoculated with Geobacillus stearothermophilus as the biological indicator. All 3 different brands of phaco handpieces and tips were placed together as a mixed batch within a single containment device for all sterility testing. | Interventions: Short-cycle sterilization for unwrapped loads using a STATIM 2000 sterilizer (SciCan, Canonsburg, PA) with the metal cassette provided with the STATIM 2000, at 135°C (275°F). Sterility tested after:
Short-cycle sterilization for contained loads using a AMSCO Century V116 pre-vacuum sterilizer (STERIS, Mentor, OH) with a Case Medical SteriTite container (Case Medical, South Hackensack, NJ), at 132°C (270°F). Sterility tested after:
Comparators: Full-cycle sterilization for wrapped loads using a STATIM 2000 sterilizer with the metal cassette provided with the STATIM 2000, at 135°C (275°F). Sterility tested after:
Full-cycle sterilization for contained loads using a AMSCO Century V116 pre-vacuum sterilizer with a Case Medical SteriTite container, at 132°C (270°F). Sterility tested after:
Each of the handpieces was aseptically swabbed twice and those swabs were incubated for 14 days. Each sterility verification test was performed in triplicate. The sterilization process adhered to the manufacturers’ IFU. | Outcomes: Short-cycle and moisture sterility based on presence or absence of microbial growth from cultured test samples. Sterility demonstrated by a minimum of 1.0 × 106 Geobacillus stearothermophilus spores were killed by a full steam sterilization cycle. |
CA = California; IFU = instructions for use; NY = New York; OH = Ohio; PA = Pennsylvania; TX = Texas.
aPhaco handpieces represented the worst-case scenario for ophthalmic instrument sterilization due to their bulkier size and small lumens.
bThe 1-minute dry time simulated prompt use of sterilized, still-wet instruments for sequential same-day procedures. Instruments were immediately removed for testing after the dry time.
cThe 3-minute storage/transit time represented the upper limit of time needed to transfer the sterilized instruments within a covered containment device (cassette or rigid container) to a nonadjacent operating room for subsequent prompt use on the sterile field.
dThis cycle corresponded to sterile processing for a wrapped or contained instrument set that would be stored and not used until 7 days later.
Table 3: Characteristics of the Included Guideline
Intended users, target procedures | Practice considered | Major outcomes considered | Evidence collection, synthesis, and quality assessment | Recommendations development and evaluation | Guideline validation |
|---|---|---|---|---|---|
OICS Task Force (2018)12 | |||||
Intended users: Ophthalmologists and the clinical staff of ophthalmic outpatient surgery centers, including surgeons, nurses, and technicians Target procedures: Cataract surgery and other intraocular surgical procedures | Short-cycle steam sterilization for sequential same-day ophthalmic procedures | Sterilization of intraocular surgical instruments | Systematic search of the literature NR. Most of the recommended practices were derived from existing evidence-based recommendations for cleaning and sterilizing all surgical instruments in general, from published analyses of TASS outbreaks, from manufacturers’ IFU for surgical instruments and equipment, and from the new research performed by task force members Quality assessment: NR | Recommendations were based on a consensus of experts representing the 3 sponsoring societies, including the US ASCRS, AAO, and OOSS. Details of consensus development and recommendation evaluation NR. | NR |
AAO = Academy of Ophthalmology; ASCRS = American Society of Cataract and Refractive Surgery; IFU = instructions for use; NR = not reported; OICS = Ophthalmic Instrument Cleaning and Sterilization; OOSS = Outpatient Ophthalmic Surgery Society; TASS = toxic anterior segment syndrome.
Appendix 4: Critical Appraisal of Included Publications
Note that this appendix has not been copy-edited.
Table 4: Strengths and Limitations of the Included Guideline Using AGREE II20
Item | OICS Task Force (2018)12 |
|---|---|
Domain 1: scope and purpose | |
1. The overall objective(s) of the guideline is (are) specifically described. | Yes |
2. The health question(s) covered by the guideline is (are) specifically described. | Yes |
3. The population (patients, public, etc.) to whom the guideline is meant to apply is specifically described. | Yes |
Domain 2: stakeholder involvement | |
4. The guideline development group includes individuals from all relevant professional groups. | Yes |
5. The views and preferences of the target population (patients, public, etc.) have been sought. | NA |
6. The target users of the guideline are clearly defined. | Yes |
Domain 3: rigour of development | |
7. Systematic methods were used to search for evidence. | No |
8. The criteria for selecting the evidence are clearly described. | No |
9. The strengths and limitations of the body of evidence are clearly described. | No |
10. The methods for formulating the recommendations are clearly described. | No |
11. The health benefits, side effects, and risks have been considered in formulating the recommendations. | Yes |
12. There is an explicit link between the recommendations and the supporting evidence. | Yes |
13. The guideline has been externally reviewed by experts before its publication. | No |
14. A procedure for updating the guideline is provided. | No |
Domain 4: clarity of presentation | |
15. The recommendations are specific and unambiguous. | Yes |
16. The different options for management of the condition or health issue are clearly presented. | NA |
17. Key recommendations are easily identifiable. | Yes |
Domain 5: applicability | |
18. The guideline describes facilitators and barriers to its application. | No |
19. The guideline provides advice and/or tools on how the recommendations can be put into practice. | Yes |
20. The potential resource implications of applying the recommendations have been considered. | Yes |
21. The guideline presents monitoring and/or auditing criteria. | No |
Domain 6: editorial independence | |
22. The views of the funding body have not influenced the content of the guideline. | NR |
23. Competing interests of guideline development group members have been recorded and addressed. | Yes |
AGREE II = Appraisal of Guidelines for Research and Evaluation II; NA = not applicable; NR = not reported; OICS = Ophthalmic Instrument Cleaning and Sterilization.
Appendix 5: Main Study Findings
Table 5: Summary of Findings by Outcome — Sterility After Short-Cycle Sterilization
Study | Interventions, Comparators | Sterilization time | Storage time | Microbial growth from positive, negative, and environmental controls | Microbial growth from cultured test samples | Authors’ conclusion | |||
|---|---|---|---|---|---|---|---|---|---|
Exposure time | Dry time | Positive controls | Negative controls | Environmental controls | |||||
Chang et al. (2018)11 | STATIM 2000 sterilizer | “Unwrapped, short-cycle sterilization that adheres to the IFU of these 2 popular, FDA-cleared sterilizers is appropriate for routine use in between sequential same-day cataract surgeries.” | |||||||
Intervention: Unwrapped short-cycle sterilization | 3.5 minutes | 1 minute | – | Positive for growth | Negative for growth | Negative for growth | Negative for growth | ||
Comparator: Wrapped full-cycle sterilization | 10 minutes | 1 hour | 7 days | Positive for growth | Negative for growth | Negative for growth | Negative for growth | ||
AMSCO Century V116 pre-vacuum sterilizer | |||||||||
Intervention: Contained short-cycle sterilization | 3 minutes | 1 minute | – | Positive for growth | Negative for growth | Negative for growth | Negative for growth | ||
Comparator: Contained full-cycle sterilization | 3 minutes | 20 minutes | 7 days | Positive for growth | Negative for growth | Negative for growth | Negative for growth | ||
IFU = instructions for use.
Note: This table has not been copy-edited.
Table 6: Summary of Findings by Outcome — Moisture Sterility After Short-Cycle Sterilization
Study | Interventions | Sterilization time | Transit /storage time | Microbial growth from positive, negative, and environmental controls | Microbial growth from cultured test samples | Authors’ conclusion | |||
|---|---|---|---|---|---|---|---|---|---|
Exposure time | Dry time | Positive controls | Negative controls | Environmental controls | |||||
Chang et al. (2018)11 | Unwrapped short-cycle sterilization using STATIM 2000 sterilizer | 3.5 minutes | 1 minute | 3 minutes | Positive for growth | Negative for growth | Negative for growth | Negative for growth | “With the STATIM 2000, any moisture evaluated was found sterile if the unwrapped instruments are not completely dried, but are kept within the covered sterilizer cassette until needed and handled in the operating room for the subsequent case after some short delay.” |
Contained short-cycle sterilization using AMSCO Century V116 pre-vacuum sterilizer | 3 minutes | 1 minute | 3 minutes | Positive for growth | Negative for growth | Negative for growth | Negative for growth | ||
Note: This table has not been copy-edited.
Table 7: Summary of Recommendations in the Included Guideline
Recommendations and supporting evidence | Quality of evidence and strength of recommendations |
|---|---|
OICS Task Force (2018)12 | |
“It is our position that unwrapped settings and short-cycle sterilization used in accordance with the IFU of FDA-approved sterilizers are appropriate for routine use in between sequential same-day ophthalmic cases.” (p. 770) Supporting evidence: 1 sterilization validation study and data from the sterilizer manufacturers. | Quality of evidence: NR Strength of recommendation: NR |
“It is our position that complete drying is not necessary to maintain the sterility of wrapped or unwrapped ophthalmic instruments that are kept in the covered containment device until retrieved by sterile gloved and gowned staff within the OR for the subsequent case after some short delay.” (p. 770) Supporting evidence: 1 sterilization validation study and data from the sterilizer manufacturers. | Quality of evidence: NR Strength of recommendation: NR |
“ Phaco handpieces are immediately primed with a balanced salt solution and remain wet as they sit on the sterile instrument table.” (p. 770) Supporting evidence: 1 sterilization validation study | Quality of evidence: NR Strength of recommendation: NR |
IFU = instructions for use; NR = not reported; OICS = Ophthalmic Instrument Cleaning and Sterilization; OR = operating room.
Note: This table has not been copy-edited.
Appendix 6: References of Potential Interest
Note this appendix has not been copy-edited.
Narrative Reviews
Land V, Dickerson S, Goldman A, Shirley ED. The surgical instrument sterilization process: What every surgeon should know. JBJS Reviews. 2023;11(11) (no pagination).
Editorials
Mamalis N, Chang DF. Guidelines for the cleaning and sterilization of intraocular surgical instruments. J Cataract Refract Surg. 2018;44(6):675-676. PubMed
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up to date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca