CADTH Health Technology Review
Retesting Intervals for Tryptase
Rapid Review
Key Messages
What Is the Issue?
Tryptase is a serine protease primarily produced and released by mast cells. Tryptase measures are most used to diagnose and manage anaphylaxis and mastocytosis, and the timing of tryptase measurement is crucial for its utility.
The clinical utility of tryptase remains unclear, and available evidence showed that more than 30% of patients with acute anaphylaxis did not exhibit an elevated tryptase level, which suggests that repeated tryptase testing may be overused in this population.
Appropriate retesting intervals or frequency for tryptase retesting in patients with anaphylaxis or mastocytosis remain unclear.
What Did We Do?
To inform decisions about the use and timing of repeat tryptase testing for patients with confirmed or suspected anaphylaxis and patients with cutaneous or systemic mastocytosis, we identified and summarized related recommendations and publications on the potential biological or physiological factors that may impact retesting intervals in these populations.
We searched key resources, including journal citation databases, and conducted a focused internet search for relevant evidence published since 2014. One reviewer screened articles for inclusion based on predefined criteria, critically appraised the included evidence-based guidelines, and narratively summarized the findings.
What Did We Find?
For patients with suspected anaphylaxis, identified guidelines suggest measuring tryptase levels 1 to 2 times during the event onset (e.g., immediately or within 4 hours) and 1 to 2 times after resolution of symptoms (e.g., after 24 hours) to establish baseline tryptase levels. These recommendations were based on very low certainty of evidence.
For patients with systemic mastocytosis, 1 evidence-based guideline in Brazil recommends testing tryptase once a year, which is based on very low certainty of evidence.
Baseline tryptase level varies very little over time within the same individual and is determined by their genetic background.
For patients with anaphylaxis, the timing of the peak tryptase level is from 1 minute to 6 hours (median 30 minutes), and the half-life of serum tryptase is about 1.5 hours to 2.5 hours and needs up to 24 hours to return to baseline level.
We did not find any recommendations that met our inclusion criteria regarding the minimum retesting interval for tryptase testing or the use of repeat or serial tryptase testing in patients with confirmed or suspected anaphylaxis or with cutaneous or systemic mastocytosis.
What Does It Mean?
The available recommendations suggest testing blood tryptase at the acute (1 or 2 times) and baseline phases (1 or 2 times) for patients with suspected anaphylaxis. There is little rationale for the ongoing monitoring of tryptase levels beyond the recommended 4 time points for patients with anaphylaxis.
For patients with mastocytosis, the guidelines recommend retesting tryptase only once a year and do not support frequent repeat tryptase testing within a year.
Decision-makers and clinicians should consider the cost of tryptase testing, potential burden on health care resources, local lab capacity, or accessibility of testing facilities when making decisions regarding tryptase retesting.
Given the very low-quality evidence regarding measuring tryptase and the unclear utility of tryptase testing for patients with anaphylaxis, future research that focuses on the clinical utility of tryptase relative to clinical assessment for anaphylaxis is needed.
Abbreviations
AGREE
Appraisal of Guidelines for Research and Evaluation
GRADE
Grading of Recommendations Assessment, Development and Evaluation
NICE
National Institute for Health and Care Excellence
Context and Policy Issues
What Is a Tryptase Test and What Is It Used For?
Tryptase, also known as mast cell tryptase, is a serine protease primarily produced by mast cells and stored in their secretory granules.1,2 Mast cells are widely distributed throughout the body, particularly in connective tissues, and are important components of the immune system.3 In addition to participating in immune responses, they also have implications for various diseases.3 Tryptase is released into the bloodstream during mast cell activation and can be measured in serum or plasma as an indicator of mast cell degranulation and allergic reaction.4 There are several isoforms of tryptase in humans, but the beta isoforms are the most clinically relevant, which is the primary active form released during mast cell degranulation.2,4
The measurement of serum tryptase levels plays a role in various medical conditions, including anaphylaxis and mastocytosis2,4-6 Anaphylaxis is a severe and potentially life-threatening allergic reaction that can occur within 1 to 2 hours of exposure to an allergen and affects multiple systems.7 Elevated tryptase levels compared to baseline levels are associated with anaphylaxis.7-9 However, the absence of elevated tryptase does not rule out anaphylaxis.7-9 The diagnostic criteria for anaphylaxis mostly rely on clinical characteristics such as time of symptom onset after exposure to a likely allergen, involvement of multiple body systems, and rapid reduction in blood pressure.7-9
Mastocytosis is a heterogeneous disorder characterized by the abnormal accumulation of mast cells in various tissues.10 Patients with mastocytosis could present with a wide array of symptoms, including skin lesions, recurrent anaphylactic episodes, syncope, hypotension, fatigue, diarrhea, and weight loss.10-12 These symptoms can significantly impact patients’ daily quality of life. The burden of mast cells in mastocytosis plays an important role in disease severity and prognosis, which is the major criterion for diagnosis of mastocytosis.10,13 To diagnose mastocytosis, clinicians need to examine the infiltration of mast cells in the bone marrow or other extracutaneous organs. Persistently elevated basal serum tryptase levels (> 20 ng/mL) are 1 of the minor criteria for diagnosing systemic mastocytosis based on WHO criteria.10-12 In contrast, for individuals experiencing anaphylaxis, the increase in tryptase levels is transient and returns to baseline within a specific time frame.7-9 However, normal tryptase levels also cannot rule out mastocytosis.11,12 Additional minor criteria for diagnosing mastocytosis include detecting an activating point mutation (i.e., at codon 816 of KIT) or accessing other biomarkers for mast cells (e.g., CD25).11,12
What Are Retesting Intervals for Laboratory Tests?
A minimum retesting interval is the minimum time before a test should be repeated, considering the test's characteristics and the specific clinical circumstances in which it is used.14 It does not specify how often the test should be repeated in patients, but it indicates that if a test is to be repeated, it should not be done more frequently than the specified retesting interval.14 This differs from optimal retesting intervals or recommendations about how often to conduct a test, which provide guidance for repeat testing for clinical monitoring purposes. Retesting intervals can inform the appropriate use of laboratory tests.
Why Is It Important to Do This Review?
The timing of tryptase measurement is crucial for its utility, particularly for patients with anaphylaxis.7,8 Tryptase levels typically peak 1 to 2 hours after the onset of anaphylaxis and return to baseline within 12 to 24 hours.4,7,8 Therefore, tryptase measurements are most diagnostically useful when measured within 1 to 2 hours of symptom onset and compared to baseline levels.4,7,8 Proper sampling protocols and interpretation of tryptase levels can assist in the diagnosis of anaphylaxis. In addition, testing tryptase also helps the classification and monitoring of mastocytosis.10-13 Measuring serum tryptase is a noninvasive way to estimate the burden of mast cells in patients with mastocytosis. Additionally, testing tryptase can help distinguish between cutaneous mastocytosis (no increase or mild increase) and systemic mastocytosis (significant increase). It is also useful for assessing disease severity, monitoring disease progression, and evaluating the response to treatment.11,12
While tryptase testing is useful for some patients, there are challenges related to its cost and accessibility. The cost of tryptase is not well reported in the literature. The costs may relate to the assay kits and the resources required for testing and retesting, which may vary depending on different health care settings. A cohort study showed that more than 1 in 3 patients with acute anaphylaxis did not exhibit an elevated tryptase level in sequential serum tryptase measurements.9 This study indicates that repeated tryptase testing may be overused in the diagnosis of anaphylaxis. Additionally, the optimal or minimum retesting intervals for tryptase testing among these populations remain unclear. It is crucial to explore recommendations and biological or physiological factors that may impact tryptase testing for patients with confirmed or suspected anaphylaxis and for those with cutaneous or systemic mastocytosis. This exploration could enhance the diagnosis and management of these conditions and support the appropriate use of repeat tryptase testing.
Objective
To aid decision-making about the use and timing of repeated tryptase testing, this Rapid Review summarizes related recommendations and biological or physiological factors that may impact retesting intervals in patients with confirmed or suspected anaphylaxis and in those with cutaneous or systemic mastocytosis.
Research Questions
What are the recommendations regarding repeat tryptase testing in patients with confirmed or suspected anaphylaxis?
What are the biological or physiological factors that may impact how often tryptase testing should be repeated for patients with confirmed or suspected anaphylaxis?
What are the recommendations regarding repeat tryptase testing in patients with cutaneous or systemic mastocytosis?
What are the biological or physiological factors that may impact how often tryptase testing should be repeated for patients with cutaneous or systemic mastocytosis?
Methods
An information specialist conducted a customized literature search, balancing comprehensiveness with relevancy, of multiple sources and grey literature on June 18, 2024. One reviewer screened citations and selected studies based on the inclusion criteria presented in Table 1.
In this review, evidence-based guidelines are defined as publications with a clear methods section that includes details of the evidence collection and the formulation of the recommendations, presents formal relevant recommendations based on evidence, and indicates the strength of each recommendation. When relevant recommendations are solely based on consensus, we define them as consensus-based guidelines. The reviewer critically appraised the included evidence-based guidelines using the Appraisal of Guidelines for Research and Evaluation (AGREE) II instrument.15 The reviewer did not critically appraise consensus-based guidelines and other publications. Appendix 1 presents a detailed description of methods.
Criteria | Description |
|---|---|
Population | Q1 and Q2: Patients with confirmed or suspected anaphylaxis Q3 and Q4: Patients with an established diagnosis of cutaneous or systemic mastocytosis |
Intervention | Tryptase testing |
Comparator | Not applicable |
Outcomes | Q1 and Q3: Recommendations regarding whether testing should be repeated and at what interval(s); recommendations regarding the minimum time before a test should be repeated Q2 and Q4: Biological or physiological factors that impact the amount of time between repeat tryptase tests (e.g., half-life, typical time course of tryptase levels) |
Study designs | No restriction on type of publication |
Publication date | Since January 1, 2014 |
Summary of Evidence
Quantity of Research Available
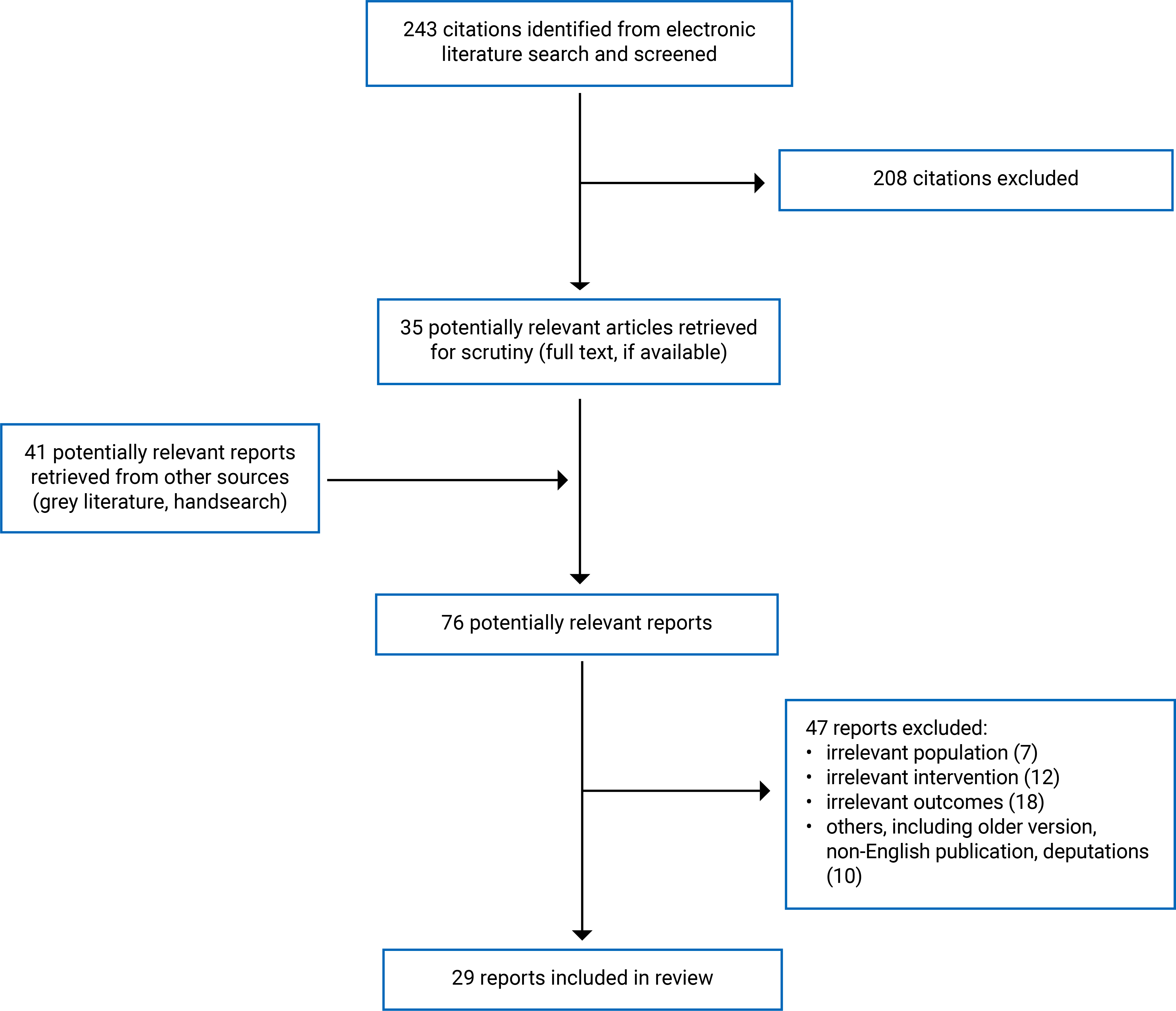
This review includes 29 publications,4,16-43 including 4 evidence-based guidelines (3 guidelines21,27,40 for patients with suspected anaphylaxis and 1 guideline34 for patients with systemic mastocytosis),21,27,34,40 6 consensus-based guidelines,19,20,28,30-32 12 other publications that provide recommendations for repeated tryptase testing,4,22,23,29,33,35,37-39,41-43 8 publications16-18,24-26,32,36 that solely report the factors influencing the time between repeat tryptase tests, and 7 publications4,38-43 that report both recommendations and factors for patients with suspected anaphylaxis. We did not identify any publications that report biological or physiological factors that may impact how often tryptase testing should be repeated for patients with cutaneous or systemic mastocytosis (research question 4). Figure 1 (Appendix 1) presents the PRISMA44 flow chart of the study selection.
Summary of Study Characteristics
Included Publications for Research Question 1: Recommendations Regarding Repeat Tryptase Testing in Patients With Confirmed or Suspected Anaphylaxis
We identified 3 evidence-based guidelines21,27,40 in which recommendations related to repeat tryptase testing in patients with suspected anaphylaxis were developed based on relevant evidence. The 3 evidence-based guidelines were supported by 3 different organizations, including the American Academy of Allergy, Asthma & Immunology (AAAAI) or the American College of Allergy, Asthma and Immunology (ACAAI);21 the European Academy of Allergy and Clinical Immunology (EAACI);27 and the National Institute for Health and Care Excellence (NICE).40 The developers of the 3 guidelines searched for and identified relevant evidence and adopted the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach to assess the certainty of evidence and formulate the recommendations. Appendix 2 presents additional characteristics of the included evidence-based guidelines.
We also found 6 publications19,20,28,30-32 with consensus-based recommendations and 12 other publications4,22,23,29,33,35,37-39,41-43 that provide recommendations for repeated tryptase testing for patients with confirmed or suspected anaphylaxis. These publications consist of narrative reviews, laboratory guidance documents, or clinical practice guidelines with unclear methods.
Included Publications for Research Question 2: Biological or Physiological Factors That May Impact How Often Tryptase Testing Should Be Repeated for Patients With Confirmed or Suspected Anaphylaxis
We found 16 publications4,16-18,24-26,32,36,38-43 that report biological or physiological factors influencing the time between repeat tryptase tests. These publications consist of narrative reviews, guidance documents, or clinical practice guidelines.
Included Publications for Research Question 3: Recommendations Regarding Repeat Tryptase Testing in Patients With Cutaneous or Systemic Mastocytosis
We found 1 evidence-based guideline34 from Brazil with recommendations developed based on relevant evidence. Eighteen panel members from Brazil conducted a literature search, but the guideline does not provide the details of their search. They used the Oxford Centre for Evidence-Based Medicine 2011 Levels of Evidence document to assess the certainty of evidence.34 The panel voted on 30 multiple-choice questions to establish recommendations or suggestions.34 Appendix 2 presents additional characteristics of the included evidence-based guideline for systemic mastocytosis. We also identified a laboratory document33 from the Division of Laboratory Medicine at Manchester University that provides recommendations for people with mastocytosis.
Summary of Critical Appraisal
All the included evidence-based guidelines21,27,34,40 have clear objectives, guideline questions, and target populations (e.g., patients with suspected anaphylaxis or systemic mastocytosis). All the guidelines21,27,34,40 are based on a search for relevant evidence and developed through consensus to formulate recommendations. For 1 guideline,34 the details of the search are not provided, and another primarily searched PubMed,21 potentially missing relevant evidence due to unclear or incomplete searches.
Three of the guidelines were developed by a team of clinical experts and methodologists.21,27,40 However, it is uncertain whether at least 1 methodology expert was involved in the development of 1 included guideline.34 The developers of 3 of the guidelines sought the views or preferences of the target population or public review.21,27,40 It is unclear whether the perspectives or preferences of the target populations were sought or had an influence on the recommendations in the remaining 1 guideline34 for patients with mastocytosis. Therefore, the recommendations regarding tryptase testing may not adequately reflect the values and preferences of patients or other partners.
For 3 of the guidelines,21,27,40 the GRADE framework was used to assess the certainty of the evidence, and for 1 guideline,34 the Oxford Centre for Evidence-Based Medicine 2011 Levels of Evidence document was used. The links between the recommendations and the supporting evidence are unclear in 2 guidelines.21,34 In all the guidelines, the competing interests of the development group are disclosed.21,27,34,40 However, several authors of 1 guideline34 for patients with mastocytosis had received research grants from industries, and it is unclear how they addressed these competing interests and if the competing interests could have impacted the development of recommendations. These limitations could impact the internal validity of the guidelines.
The 3 included guidelines include a discussion of the potential facilitators and barriers to implementing the recommendations,21,27,40 whereas the remaining 1 does not.34 All relevant recommendations are specific and clear.21,27,34,40 The NICE guideline40 considers the economic impact (cost) when making recommendations, whereas the other 3 guidelines21,27,34 do not consider the potential resources required for repeated tryptase testing. These limitations could be a barrier to implementing recommendations.
Appendix 3 provides additional details regarding the strengths and limitations of included evidence-based guidelines.
All the included consensus-based guidelines19,20,28,30-32 provide consensus-based statements or recommendations on retesting tryptase for patients with suspected anaphylaxis, for which the evidence base and strength of the recommendations is uncertain. We did not conduct a formal critical appraisal for the included consensus-based guidelines but note there is uncertainty in the findings given the unclear methods.
Summary of Findings
Recommendations for Patients With Confirmed or Suspected Anaphylaxis
We did not find any recommendations regarding the minimum retesting interval for tryptase testing in the diagnosis or management of anaphylaxis. However, we identified 3 evidence-based guidelines,21,27,40 6 consensus-based guidelines,19,20,28,30-32 and 12 other documents4,22,23,29,33,35,37-39,41-43 with recommendations regarding the testing frequency for tryptase for persons with confirmed or suspected anaphylaxis.
The recommended procedure for tryptase testing involves taking 2 to 4 blood samples. One or 2 blood samples should be taken during the acute phase of anaphylaxis onset, as soon as possible and a few hours (most guidelines recommend or suggest 1 to 2 hours but no later than 4 hours) after symptom onset. Another blood sample should be taken to measure the basal tryptase level, preferably 24 hours after onset or after the resolution of symptoms. Only 1 narrative review42 suggests taking the fourth blood sample 1 week after symptom resolution. The guidelines emphasize the importance of comparing tryptase levels between the acute phase and baseline levels for diagnosis of anaphylaxis. An increase in tryptase during early hours of onset of anaphylaxis confirms a diagnosis of anaphylaxis retrospectively. Measuring baseline tryptase levels may be also helpful for differentiating between temporary elevations due to acute anaphylaxis and persistently elevated levels caused by other conditions like mastocytosis.
Evidence-Based Guidelines
Two evidence-based guidelines21,27 suggest taking 2 blood samples at the following time points (weak recommendations):
The first sample: as early as possible21 or half an hour to 2 hours after onset of symptoms of anaphylaxis27
The second sample: at a later time, after the acute phase, as a baseline for comparison (no specific time reported)21 or least 24 hours after complete resolution of symptoms27).
The NICE guideline40 suggests taking 3 blood samples from people with suspected anaphylaxis at the following time points:
The first sample: as soon as possible after onset of symptoms40
The second sample: ideally within 1 to 2 hours after onset of symptoms but no later than 4 hours40
The third sample: may be required at follow-up with the specialist allergy service to measure baseline mast cell tryptase.40
The NICE guideline40 provides the same guidance based on very low-quality evidence for adults or young people aged 16 years or older and for children younger than 16 years. The recommendation is strong for the first 2 sample timings for adults or young people aged 16 or older; the recommendations for children younger than 16 are weak.40 The recommendations for the third sample are weak for all age groups.40
Consensus-Based Guidelines
Two consensus-based guidelines suggest obtaining 2 blood samples (immediately after onset of the anaphylactic event and 24 hours after onset or after full recovery) from individuals suspected of anaphylaxis.28,30 One consensus-based guideline32 recommends a minimum of 1 blood sample but ideally suggests taking 3 blood samples. The 4 consensus-based guidelines19,20,31,32 suggest taking 3 blood samples at the following time points after the onset of the anaphylactic event:
The first sample: as soon as feasible (3 guidelines)19,20,32 or at 1 hour after onset of symptoms (1 guideline)31
The second sample: 1 to 2 hours (2 guideline),19,32 2 to 4 hours (1 guideline),20 or 4 hours (1 guideline) after onset of symptoms 31
The third sample: at least 24 hours after onset of symptoms or in convalescence (4 guidelines).19,20,31,32
Recommendations From Other Documents
We identified 12 other publications4,22,23,29,33,35,37-39,41-43 that recommend repeated tryptase testing for patients experiencing an anaphylactic event. All these recommendations support sequenced tryptase testing and suggest taking 2 to 4 blood samples (with most guidelines4,22,23,29,33,39,41,42 recommending taking 3 blood samples) for patients with confirmed or suspected anaphylaxis. These publications recommend taking blood samples at the following time points after the onset of anaphylaxis symptoms:
The first sample: immediately or from 15 minutes to 3 hours after onset of symptoms
The second sample: within 1 to 6 hours after onset of symptoms
The third sample: obtaining baseline serum tryptase sampling at least 24 hours after onset of symptoms or later in convalescence.
One narrative review4 recommends always measuring tryptase levels in people who have experienced an anaphylactic reaction following a hymenoptera (e.g., bee, wasp) sting, even if the event occurred 24 hours before, based on consensus by the Italian allergy societies on the management of hymenoptera venom allergy. To establish the baseline serum tryptase, 1 guideline42 suggests taking an additional sample a week after the reaction; another guideline42 recommends repeating the tryptase measurement if the baseline serum tryptase levels are 8 ug/L or higher.
Factors That Impact Tryptase Levels in Patients With Anaphylaxis
We found 15 publications4,16-18,24-26,32,36,38-43 that report the factors influencing the time between repeat tryptase tests, which may inform the development or understanding of appropriate tryptase retesting intervals. There are several factors that impact tryptase levels:
Timing of the sample relative to the start of an anaphylaxis event correlates with the tryptase levels, which follow a predictable pattern over time.4,16-18,24-26,32,36,38-43 Table 6 presents the timing of tryptase that relates to the onset of anaphylaxis.
Time to serum tryptase rise begins: 5 minutes to 30 minutes
Timing of peak level: 1 minute to 6 hours (median 30 minutes)
Return to baseline level: up to 24 hours
Half-life: about 1.5 to 2.5 hours. This indicates that the levels of tryptase decrease rapidly after the peak level, so taking the blood sample early to capture peak levels after the anaphylaxis event is important.
Low intraindividual biological variability: The basal tryptase level varies very little over time within the same individual, which is determined by their genetic background and not by environmental factors.4 The low intraindividual variability suggests that repeat testing is not necessary to obtain the baseline tryptase.
Reproducibility of the test: The currently commercially available assay has low intra-assay and interassay coefficient of variation values.4 The low coefficient of variation values suggest that the tryptase test is reliable using 1 assay or across different assays and is precise, with a low likelihood of random errors and variability in the results. Therefore, it is not necessary to retest the tryptase using the same blood sample.
Recommendations for Patients With Cutaneous or Systemic Mastocytosis
We did not find any recommendations regarding the minimum retesting interval for tryptase in the management of cutaneous or systemic mastocytosis. However, we found 1 evidence-based guideline that recommends testing for tryptase at least once a year for people with systemic mastocytosis (strong recommendation). The guideline also states that measuring tryptase levels is necessary for diagnosing and monitoring systemic mastocytosis. The laboratory document from the Division of Laboratory Medicine at Manchester University suggests repeating the tryptase test “after 1 year or following significant clinical change” for patients with mastocytosis.33
Appendix 4 presents the main findings from included studies, including the detailed recommendation statements along with supporting evidence, the certainty of evidence, and the strength of recommendations, if available.
Limitations
We did not find any recommendations regarding the minimum retesting interval for tryptase testing in the diagnosis or management of anaphylaxis or for the management of patients with cutaneous or systemic mastocytosis. Although we identified 4 evidence-based guidelines21,27,34,40 that make recommendations for tryptase testing frequency, most of the recommendations are based on very low certainty of evidence and refer to the timing or kinetics of tryptase after the onset of an anaphylactic reaction.27,34,40 One guideline21 provides a recommendation based on moderate certainty of evidence. However, the guideline did not clearly report the evidence base.
We did not formally critically appraise consensus-based guidelines19,20,28,30-32 and other publications.4,22,23,29,33,35,37-39,41-43 Although these recommendations appear consistent with evidence-based guidelines regarding retesting tryptase, it is important to note that these recommendations or statements lack clear evidence, strength of recommendation, or clear methods for development.4,19,20,22,23,28-33,35,37-39,41-43 Therefore, we need to interpret these recommendations with caution. In addition, we did not conduct a systematic review to identify all the potential factors that may impact tryptase repeat testing, particularly for factors other than the kinetics of tryptase, so we potentially overlooked some studies that reported the factors of interest.
Only the NICE guideline40 considers the economic considerations for testing tryptase and states that the tryptase test being conducted early in emergency settings would not significantly increase the overall health care cost for National Health Service in the UK and would provide some benefits for patients. Other evidence-based guidelines21,27,34 did not assess the potential burden or accessibility of repeated tryptase testing. Although some Canadian panel members were involved in the development of 1 evidence-based guideline,21 we did not identify any evidence-based guidelines led by Canadian organizations or that considered the costs and other implementation issues (e.g., accessibility or lab capacity) in the Canadian context. Thus, the generalizability of the findings to settings in Canada is unclear.
Conclusions and Implications for Decision- or Policy-Making
We conducted this review to summarize recommendations regarding the use and timing of repeat tryptase testing in patients with confirmed or suspected anaphylaxis and for those with cutaneous or systemic mastocytosis. We also explored potential biological or physiological factors that may impact the tryptase repeat testing intervals in these populations. We did not find any recommendations regarding the minimum retesting interval for tryptase testing (i.e., the minimum time before the test should be repeated) in the management of cutaneous or systemic mastocytosis. In patients with suspected anaphylaxis, the recommendations suggest testing tryptase levels during the event onset (e.g., immediately or within 4 hours) and to establish baseline tryptase levels (e.g., after 24 hours or in convalescence).4,19-23,27-33,35,37-43 Most of the recommendations are weak and based on very low certainty of evidence regarding the kinetics of tryptase.
Based on the kinetics of serum tryptase, these guidelines recommend collecting blood samples at 2 to 3 time points: immediately (within 1 hour) to capture the initial rise, 1 to 2 hours after the reaction to capture the peak level, and 24 hours after the acute-phase resolution to establish the baseline tryptase level. Given the low intraindividual biological stability of baseline tryptase levels, the half-life of tryptase, and the reliability of the tryptase test, retesting tryptase beyond the third baseline sample is generally unnecessary unless new clinical conditions arise. However, there is 1 narrative review42 that suggests taking the fourth blood sample 1 week after symptom resolution.
We found 1 evidence-based guideline34 from Brazil that recommends testing for tryptase at least once a year for people with systemic mastocytosis. This recommendation is strong but based on very low certainty of evidence. The guideline34 states that a persistently elevated serum tryptase level (> 20 ng/mL) is a minor diagnostic criterion for mastocytosis in the WHO diagnostic framework. Additionally, basal tryptase levels are associated with disease progression and response to treatment. Therefore, it is recommended to periodically test tryptase levels, especially in advanced cases. A laboratory document suggests repeating the tryptase test after 1 year or following significant clinical changes in patients with mastocytosis.33 We did not find any publications that reported the biological or physiological factors that may impact tryptase repeat testing in patients with cutaneous or systemic mastocytosis.
Considerations for Future Research
Given the very low-quality evidence regarding measuring tryptase and the unclear utility of tryptase for patients with anaphylaxis, future research that focuses on the clinical utility of tryptase is needed. For example, The NICE guideline40 notes that no evidence of the clinical utility of tryptase testing or its timing in the diagnosis of anaphylaxis in children was identified. In the NICE guideline,40 only very low-quality evidence from observational studies was identified showing that tryptase testing had a high specificity (87% to 100%) and a lower sensitivity (35% to 93%) for diagnosing anaphylaxis compared with clinical assessment. Given that measuring tryptase is not an immediate procedure (it needs 4 hours to 2 working days for results to become available depending on lab protocol and capacity), the results will not be available during the acute phase of an anaphylaxis event.4 Several recommendations state that testing tryptase should not delay treatment.19,22,32 Future studies examining sensitivity and specificity for diagnosing anaphylaxis and mastocytosis compared with clinical assessment alone, or studies exploring how tryptase testing impact the treatment plan, would be helpful to inform decision-making related to retesting. Future clinical practice guidelines should assess the cost, burden, and other practical issues related to tryptase retesting. A guideline that considers the Canadian context will aid decision-making in Canada.
Implications for Clinical Practice
For patients with suspected anaphylaxis, recommendations suggest measuring tryptase levels during the event onset (e.g., immediately or within 4 hours) and to establish baseline levels (e.g., after 24 hours or in convalescence). For patients with systemic mastocytosis, recommendations suggest testing tryptase once a year or following significant clinical changes. Most of the included recommendations regarding tryptase frequency are weak. Decision-makers or clinicians should consider the cost of tryptase testing, potential burden on health care resources, local lab capacity, or accessibility of testing facilities in making decisions regarding repeated tryptase testing.
It is important to note that testing tryptase should not delay intervention for suspected anaphylaxis. The available recommendations suggest testing blood tryptase at the acute (1 or 2 times) and baseline phases (1 or 2 times; only 1 narrative review42 suggests taking the fourth blood sample 1 week after symptom resolution) for patients with suspected anaphylaxis. Clinical assessment is typically sufficient in acute settings, and tryptase testing may not significantly alter initial management strategies for patients with anaphylaxis. Additionally, considering the half-life and low variability in baseline tryptase levels, there is little rationale for ongoing monitoring of tryptase levels. Therefore, repeated testing beyond the recommended 4 time points may not provide additional clinical benefit for patients with suspected anaphylaxis. For patients with mastocytosis, testing tryptase is 1 of the minor criteria; however, the guidelines recommend retesting tryptase only once a year and do not support frequent repeat tryptase testing within a year.
References
1.Sprinzl B, Greiner G, Uyanik G, et al. Genetic Regulation of Tryptase Production and Clinical Impact: Hereditary Alpha Tryptasemia, Mastocytosis and Beyond. Int J Mol Sci. 2021;22(5). PubMed
2.Beyens M, Toscano A, Ebo D, Gülen T, Sabato V. Diagnostic Significance of Tryptase for Suspected Mast Cell Disorders. Diagnostics (Basel). 2023;13(24). PubMed
3.Krystel-Whittemore M, Dileepan KN, Wood JG. Mast Cell: A Multi-Functional Master Cell. Front Immunol. 2015;6:620. PubMed
4.Platzgummer S, Bizzaro N, Bilo MB, et al. Recommendations for the Use of Tryptase in the Diagnosis of Anaphylaxis and Clonal Mastcell Disorders. Eur Ann Allergy Clin Immunol. 2020;52(2):51-61. PubMed
5.Schwartz LB, Metcalfe DD, Miller JS, Earl H, Sullivan T. Tryptase levels as an indicator of mast-cell activation in systemic anaphylaxis and mastocytosis. N Engl J Med. 1987;316(26):1622-1626. PubMed
6.Payne V, Kam P. Mast cell tryptase: a review of its physiology and clinical significance. Anaesthesia. 2004;59(7):695-703. PubMed
7.Pflipsen MC, Vega Colon KM. Anaphylaxis: Recognition and Management. Am Fam Physician. 2020;102(6):355-362. PubMed
8.LoVerde D, Iweala OI, Eginli A, Krishnaswamy G. Anaphylaxis. Chest. 2018;153(2):528-543. PubMed
9.Sala-Cunill A, Cardona V, Labrador-Horrillo M, et al. Usefulness and limitations of sequential serum tryptase for the diagnosis of anaphylaxis in 102 patients. Int Arch Allergy Immunol. 2013;160(2):192-199. PubMed
10.Valent P, Akin C, Sperr WR, et al. New Insights into the Pathogenesis of Mastocytosis: Emerging Concepts in Diagnosis and Therapy. Annu Rev Pathol. 2023;18:361-386. PubMed
11.Castells M. Mastocytosis (cutaneous and systemic) in adults: Epidemiology, pathogenesis, clinical manifestations, and diagnosis. In: Post TW, ed. UpToDate. Waltham (MA): UpToDate; 2024: https://www.uptodate.com. Accessed 2024 Jun 19.
12.Castells M. Mastocytosis (cutaneous and systemic) in children: Epidemiology, clinical manifestations, evaluation, and diagnosis. In: Post TW, ed. UpToDate. Waltham (MA): UpToDate; 2024: https://www.uptodate.com. Accessed 2024 Jun 10.
13.Sperr WR, Jordan JH, Fiegl M, et al. Serum tryptase levels in patients with mastocytosis: correlation with mast cell burden and implication for defining the category of disease. Int Arch Allergy Immunol. 2002;128(2):136-141. PubMed
14.Canada's Drug Agency. Minimum Retesting Intervals for Lab Tests. 2024; https://www.cadth.ca/minimum-retesting-intervals-lab-tests. Accessed 2024 Jul 07.
15.Agree Next Steps Consortium. The AGREE II Instrument. Hamilton (ON): AGREE Enterprise; 2017: https://www.agreetrust.org/wp-content/uploads/2017/12/AGREE-II-Users-Manual-and-23-item-Instrument-2009-Update-2017.pdf. Accessed 2024 Jun 18.
16.Beck SC, Wilding T, Buka RJ, Baretto RL, Huissoon AP, Krishna MT. Biomarkers in Human Anaphylaxis: A Critical Appraisal of Current Evidence and Perspectives. Front Immunol. 2019;10:494. PubMed
17.Buka RJ, Knibb RC, Crossman RJ, et al. Anaphylaxis and Clinical Utility of Real-World Measurement of Acute Serum Tryptase in UK Emergency Departments. J Allergy Clin Immunol Pract. 2017;5(5):1280-1287 e1282. PubMed
18.Philbin D, IAEM Guideline Development Committee. IAEM Clinical Guideline Emergency Management of Anaphylaxis in Adult Patients Version 1. Dublin (IRE): Irish Association for Emergency Medicine; 2022: https://iaem.ie/wp-content/uploads/2022/11/IAEM-Management-of-Anaphylaxis-in-adult-patient-V1-Final-1.pdf. Accessed 2024 Jul 03.
19.Lott C, Truhlář A, Alfonzo A, et al. European Resuscitation Council Guidelines 2021: Cardiac arrest in special circumstances. Resuscitation. 2021;161:154-219. https://www.cprguidelines.eu/assets/guidelines/European-Resuscitation-Council-Guidelines-2021-Ca.pdf. Accessed 2024 Jul 4. PubMed
20.Garvey LH, Dewachter P, Hepner DL, et al. Management of suspected immediate perioperative allergic reactions: an international overview and consensus recommendations. Br J Anaesth. 2019;123(1):e50-e64. PubMed
21.Golden DBK, Wang J, Waserman S, et al. Anaphylaxis: A 2023 practice parameter update. Ann Allergy Asthma Immunol. 2024;132(2):124-176. PubMed
22.NSW Health. Investigations to support the clinical diagnosis of anaphylaxis following COVID-19 vaccination. 2022; https://www.health.nsw.gov.au/immunisation/Pages/investigations-for-anaphylaxis.aspx. Accessed 2024 Jul 04.
23.NHS South Tees Hospitals. Tryptase (Mast Cell). 2022; https://www.southtees.nhs.uk/services/pathology/tests/tryptase-mast-cell/. Accessed 2024 Jul 04.
24.Laguna JJ, Archilla J, Dona I, et al. Practical Guidelines for Perioperative Hypersensitivity Reactions. J Investig Allergol Clin Immunol. 2018;28(4):216-232. PubMed
25.Littlejohns A, Savic L. Management and treatment of perioperative hypersensitivity. Curr Opin Allergy Clin Immunol. 2024;31:31. PubMed
26.Mayorga C, Celik G, Rouzaire P, et al. In vitro tests for drug hypersensitivity reactions: an ENDA/EAACI Drug Allergy Interest Group position paper. Allergy. 2016;71(8):1103-1134. PubMed
27.Muraro A, Worm M, Alviani C, et al. EAACI guidelines: Anaphylaxis (2021 update). Allergy. 2022;77(2):357-377. PubMed
28.Systemic Mastocytosis V3.2024. NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®). Plymouth Meeting (PA): National Comprehensive Cancer Network; 2024: www.nccn.org. Accessed 2024 Jul 04.
29.Lutman D, Chigaru L. CATS clinical guideline: Anaphylaxis/ Latex allergy. London (GB): NHS Children’s Acute Transport Service; 2022: https://cats.nhs.uk/wp-content/uploads/cats_anaphylaxis_2022.pdf. Accessed 2024 Jun 28.
30.Takazawa T, Yamaura K, Hara T, Yorozu T, Mitsuhata H, Morimatsu H. Practical guidelines for the response to perioperative anaphylaxis. J Anesth. 2021;35(6):778-793. PubMed
31.Tran R, Pedersen K, Kolawole H, Roessler P, Scolaro R. Australian and New Zealand Anaesthetic Allergy Group/Australian and New Zealand College of Anaesthetists perioperative anaphylaxis management guideline 2022. Anaesth Intensive Care. 2024;52(3):147-158. PubMed
32.Working Group of Resuscitation Council UK. Emergency treatment of anaphylaxis Guidelines for healthcare providers. London (GB): Resuscitation Council UK; 2021: https://www.resus.org.uk/sites/default/files/2021-05/Emergency%20Treatment%20of%20Anaphylaxis%20May%202021_0.pdf. Accessed 2024 Jul 03.
33.Division of Laboratory Medicine, Immunology. Mast Cell Tryptase. Manchester (GB): NHS Manchester University; 2023: https://mft.nhs.uk/app/uploads/2023/10/Mast-Cell-Tryptase.pdf. Accessed 2024 Jul 04.
34.Velloso E, Padulla GA, de Cerqueira AMM, et al. Diagnosis and treatment of systemic mastocytosis in Brazil: Recommendations of a multidisciplinary expert panel. Hematol. 2022;44(4):582-594. PubMed
35.Vitte J, Gonzalez C, Klingebiel C, Michel M. Tryptase and anaphylaxis: The case for systematic paired samples in all settings, from the playground to the COVID-19 vaccination center. Rev Fr Allergol (2009). 2022;62(3):287-288.
36.Vitte J, Sabato V, Tacquard C, et al. Use and Interpretation of Acute and Baseline Tryptase in Perioperative Hypersensitivity and Anaphylaxis. J Allergy Clin Immunol Pract. 2021;9(8):2994-3005. PubMed
37.PathWest Laboratory Medicine WA. Sampling time recommendations for mast cell tryptase in association with suspected event causing mast cell activation. 2024; https://www.pathwest.health.wa.gov.au/News/2023/12/22/Sampling-time-recommendations-for-mast-cell-tryptase. Accessed 2024 Jul 04.
38.Broyles AD, Banerji A, Barmettler S, et al. Practical Guidance for the Evaluation and Management of Drug Hypersensitivity: Specific Drugs. J Allergy Clin Immunol Pract. 2020;8(9S):S16-S116. PubMed
39.Tryptase (serum, plasma). London (GB): The Association for Laboratory Medicine; 2017: https://labmed.org.uk/asset/0FB2B081-1E23-494A-817726574313F632/. Accessed 2024 Jul 04.
40.Centre for Clinical Practice. Anaphylaxis: assessment and referral after emergency treatment. (NICE clinical guideline 134). Manchester (GB): National Institute for Health and Care Excellence; 2021: https://www.nice.org.uk/guidance/cg134/evidence/anaphylaxis-full-guideline-pdf-184946941. Accessed 2024 Jul 03.
41.Safer Care Victoria. Anaphylaxis clinical care standard: Improving how we manage adults with anaphylaxis in Victoria. Melbourne (AUS): State of Victoria; 2022: https://www.safercare.vic.gov.au/sites/default/files/2019-04/Anaphylaxis%20Clinical%20Care%20Standard_WEB_0.pdf. Accessed 2024 Jul 03.
42.Waterfield T, Dyer E, Wilson K, Boyle RJ. How to interpret mast cell tests. Arch Dis Child Educ Pract Ed. 2016;101(5):246-251. PubMed
43.Health New Zealand. Laboratory Test Reference Guide: Tryptase. 2024; https://lab.waikatodhb.health.nz/test-guide/view/867/tryptase. Accessed 2024 Jul 04.
44.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
Appendix 1: Detailed Methods and Selection of Included Studies
Literature Search Methods
An information specialist conducted 2 literature searches on key resources including MEDLINE, the Cochrane Database of Systematic Reviews, the International HTA Database, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search approach was customized to retrieve a limited set of results, balancing comprehensiveness with relevancy. The search strategies were comprised of both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. Search concepts were developed based on the elements of the research questions and selection criteria. The main search concepts of the first search were tryptase and repeat or serial testing. The main search concepts of the second search were tryptase, anaphylaxis, and mastocytosis. Search filters were applied to this search to limit retrieval to health technology assessments or guidelines. Retrieval for both searches was limited to the human population. The searches were completed on June 18, 2024 and limited to English-language documents published since January 1, 2014.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1. Figure 1 presents the PRISMA44 flow chart of the study selection.
Eligible Recommendations
Recommendations were considered minimum retesting intervals if the document did 1 or more of the following:
Specified the minimum time before a test should be repeated,
Specified that a test would not be performed by a laboratory or should not be ordered within a set number of days of a previous result (i.e., restrictions on repeat testing),
Specifically called the recommendation a “minimum retesting interval.”
Recommendations were considered to be monitoring requirements/testing frequency if the document:
Suggested a time frame for patient monitoring or retesting,
Did not specify the minimum time before a test should be repeated.
Exclusion Criteria
We excluded publications that did not meet the selection criteria outlined in Table 1 and were duplicate publications. We have excluded older versions of guidelines from the same author or organization by examining the context of the relevant recommendations. For example, if they provided recommendations for the same condition (i.e., anaphylaxis or mastocytosis). During the title and abstract screening, the reviewer also excluded citations that did not mention tryptase in the title or abstract.
Critical Appraisal of Evidence-Based Guidelines
The included evidence-based guidelines were critically appraised by 1 reviewer using the Appraisal of Guidelines for Research and Evaluation (AGREE) II instrument.15 Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively. Consensus-based guidelines and other publications were not formally critically appraised, but a high-level summary of their overall limitations was provided.
Appendix 2: Characteristics of Included Evidence-Based Guidelines
Note this appendix has not been copy-edited.
Table 2: Characteristics of Included Evidence-Based Guidelines
Study citation, intended users, target population | Evidence collection, selection, and synthesis | Evidence quality assessment | Recommendations development and evaluation | Guideline validation |
|---|---|---|---|---|
Patients with suspected anaphylaxis | ||||
AAAAI/ACAAI Joint Task Force on Practice Parameters (2024)21 Intended users: Clinicians Target population: patients with suspected anaphylaxis | Literature searches were conducted on PubMed and, in some cases, also on MEDLINE, Medscape, Google Scholar, and the Cochrane Database of Systematic Reviews. Most searches covered the period from 2015 to 2022, with some topics requiring searches from 1960 to the present. | The group assessed the certainty of the evidence using a modified GRADE approach. The level of evidence could be from high (large and robust RCTs or systematic reviews; further research is very unlikely to change the confidence in the estimate of effect) to very low (very low-quality studies and/or on expert opinion; any estimate of effect is very uncertain). | Most recommendations are consensus-based statements; however, the guideline did report the formal recommendation regarding retesting tryptase, and provide the recommendation based on evidence. They were determined based on an assessment of anticipated benefits and harms, as well as the quality of evidence, contextual factors, and expert opinion. The strength of the recommendation is classified as either strong or conditional based on these factors. | The guideline was supported by AAAAI/ACAAI and published in a peer-reviewed medical journal. |
EAACI (2022)27 Intended users: clinical allergists, primary care, pediatricians, emergency physicians, anesthetists and intensivists, nurses, dieticians, and other health care professionals Target population: patients with suspected anaphylaxis | Based on a systematic review aimed to assess the effectiveness of any approach for the immediate diagnosis, emergency management, and prevention or long-term management of anaphylaxis in children and adults. | Independent methodologists assessed the evidence using GRADE, and its certainty was judged as “high,” “moderate,” “low,” and “very low.” | The recommendations are formulated by GRADE approach as “strong recommendation” or “conditional recommendation.” | The guideline is a publication on behalf of the EAACI and was peer-reviewed by external experts and reviewed in a public consultation. |
NICE, et al. (2020)40 Intended users: health care, social care professionals, commissioners and providers, people with suspected anaphylaxis, and their families and carers Target population: people with suspected anaphylaxis and their families and carers | Systematic reviews and health economic evidence synthesis. | GRADE framework | Actions that should (or should not) be offered and the directive language such as “offer,” “advise” or “ask about” were used to indicate a strong recommendation. Actions with a closer balance between benefits and harms: use “consider” indicating a “weak” recommendation. | The guideline is a NICE-approved guideline that underwent the necessary peer-review process. |
Patients with systemic mastocytosis | ||||
Velloso, et al. (2022)34 Intended users: Clinicians in Brazil Target population: patients with systemic mastocytosis | NR | The level of evidence was assessed using the Oxford Centre for Evidence-Based Medicine 2011 Levels of Evidence document, which covers levels 1 (systematic review of RCTs) to 5 (Mechanism-based reasoning). | Eighteen Brazilian experts, including hematologists, immunologists, and dermatologists, held an online meeting to discuss diagnostic and treatment-related issues for patients with systemic mastocytosis. They voted on 30 multiple-choice questions and established recommendations if at least 75% of the panel agreed with an answer. If the agreement was less than 75% but greater than 49%, a suggestion was presented. No recommendations or suggestions were made if there was less than 50% agreement. | The guideline was published in a peer-reviewed medical journal. |
AAAAI = American Academy of Allergy, Asthma & Immunology; ACAAI = American College of Allergy, Asthma and Immunology; EAACI = European Academy of Allergy and Clinical Immunology; GRADE = Grading of Recommendations Assessment, Development and Evaluation; NICE = National Institute for Health and Care Excellence.
Appendix 3: Critical Appraisal of Included Publications
Note this appendix has not been copy-edited.
Table 3: Strengths and Limitations of Evidence-Based Guidelines Using AGREE II15
Item | AAAAI/ACAAI Joint Task Force on Practice Parameters, (2024)21 | Velloso, et al. (2022)34 | EAACI guidelines (2022)27 | NICE guideline (2018)40 |
|---|---|---|---|---|
Domain 1: scope and purpose | ||||
1. The overall objective(s) of the guideline is (are) specifically described. | Yes | Yes | Yes | Yes |
2. The health question(s) covered by the guideline is (are) specifically described. | Yes | Yes | Yes | Yes |
3. The population (patients, public, etc.) to whom the guideline is meant to apply is specifically described. | Yes | Not explicit but implied | Yes | Yes |
Domain 2: stakeholder involvement | ||||
4. The guideline development group includes individuals from all relevant professional groups. | Yes | Unclear if at least 1 methodology expert was included. | Yes | Yes |
5. The views and preferences of the target population (patients, public, etc.) have been sought. | Unclear | Unclear | Yes | Yes |
6. The target users of the guideline are clearly defined. | Yes | Not explicit but implied | Yes | Yes |
Domain 3: rigour of development | ||||
7. Systematic methods were used to search for evidence. | No | Unclear | Yes | Yes |
8. The criteria for selecting the evidence are clearly described. | No | No | Yes | Yes |
9. The strengths and limitations of the body of evidence are clearly described. | No | No | Yes | Yes |
10. The methods for formulating the recommendations are clearly described. | Yes | Yes | Yes | Yes |
11. The health benefits, side effects, and risks have been considered in formulating the recommendations. | Unclear | Unclear | Yes | Yes |
12. There is an explicit link between the recommendations and the supporting evidence. | No | No | Yes | Yes |
13. The guideline has been externally reviewed by experts before its publication. | Yes | Unclear | Yes | Yes |
14. A procedure for updating the guideline is provided. | Yes | No | Yes | Yes |
Domain 4: clarity of presentation | ||||
15. The recommendations are specific and unambiguous. | Yes | Yes | Yes | Yes |
16. The different options for management of the condition or health issue are clearly presented. | NA | NA | NA | NA |
17. Key recommendations are easily identifiable. | Yes | Yes | Yes | Yes |
Domain 5: applicability | ||||
18. The guideline describes facilitators and barriers to its application. | Yes | No | Yes | Yes |
19. The guideline provides advice and/or tools on how the recommendations can be put into practice. | Yes | Yes | Yes | Yes |
20. The potential resource implications of applying the recommendations have been considered. | No | No | No | No |
21. The guideline presents monitoring and/or auditing criteria. | No | No | Yes | Yes |
Domain 6: editorial independence | ||||
22. The views of the funding body have not influenced the content of the guideline. | Yes | Unclear | Yes | Yes |
23. Competing interests of guideline development group members have been recorded and addressed. | Yes | Conflicts of interest were declared, but it was unclear how they were addressed. Novartis provided funding support for the guideline, and some authors had received grants from industries or participated in industry advisory boards. | Yes | Yes |
AAAAI = American Academy of Allergy, Asthma & Immunology; ACAAI = American College of Allergy, Asthma and Immunology; AGREE II = Appraisal of Guidelines for Research and Evaluation II; EAACI = European Academy of Allergy and Clinical Immunology; NA = not applicable; NICE = National Institute for Health and Care Excellence.
Appendix 4: Main Study Findings
Note this appendix has not been copy-edited.
Table 4: Summary of Recommendations for Patients With Confirmed or Suspected Anaphylaxis
Guideline developer, year, title | Populations or conditions | Recommendation or statement | Strength of the recommendation and quality of evidence | Supporting evidence and/or rationale |
|---|---|---|---|---|
Evidence-based guidelines | ||||
AAAAI/ACAAI Joint Task Force on Practice Parameters (2024)21 Anaphylaxis: A 2023 practice parameter update | Patients with suspected anaphylaxis | “We suggest drawing an acute-phase tryptase level as early as possible during a suspected anaphylactic event (ideally within 2 hours after onset of symptoms). We suggest drawing a second tryptase measurement at a later time as a baseline for comparison to determine whether there was a significant acute elevation.” (p. 130 and p. 138) | Conditional recommendation based on moderate certainty of evidence (i.e., somewhat limited evidence, for example, randomized trials with study limitations). | There was moderate certainty of evidence, but the supporting evidence or rationale for the recommendation was unclear. |
EAACI (2022)27 EAACI guidelines: Anaphylaxis (2021 update) | Patients with suspected anaphylaxis | “The EAACI task force suggests measuring serum tryptase half to two hours after the start of the reaction, and baseline tryptase at least 24 hours after complete resolution of symptoms, to support diagnosing anaphylaxis respectively.” (p. 361) | Conditional (weak) recommendation based on very low certainty of evidence (consecutive case series or case-control studies). | “Although measuring serum tryptase will not help to make a diagnosis of anaphylaxis in a clinical emergency, an elevated level within two hours of the reaction compared to a baseline value (measured before or after the reaction) can be helpful in confirming the diagnosis of anaphylaxis during subsequent allergy consultation. (p. 361)” |
NICE (2021)40 Anaphylaxis: assessment and referral after emergency treatment | Adults or young people aged 16 years or older with suspected Anaphylaxis | “After a suspected anaphylactic reaction in adults or young people aged 16 years or older, take timed blood samples for mast cell tryptase testing as follows:
| The directive language (i.e., “take”) indicates a strong recommendation. The recommendation is based on very low certainty of evidence. | “No information on the optimal timing of baseline measurement of mast cell tryptase was identified.” (p 23) “Very low-quality evidence from seven observational studies including 178 patients showed that the timing of peak levels ranged from 1 minute to 6 hours (median 30 minutes).” (p 23) “Very low-quality evidence from six observational studies including 147 patients showed that the half-life of tryptase ranged from 30 minutes to 300 minutes (median 90 minutes).” |
Children younger than 16 years with suspected anaphylaxis | “After a suspected anaphylactic reaction in children younger than 16 years, consider taking blood samples for mast cell tryptase testing as follows if the cause is thought to be venom-related, drug-related or idiopathic:
| The wording “consider” indicates a weak recommendation. The recommendation is based on very low certainty of evidence. | “No evidence on the timing of mast cell tryptase testing in the diagnosis of anaphylaxis in children was identified.” (p. 23) | |
Anaphylaxis | “Inform the person (or, as appropriate, their parent and/or carer) that a blood sample may be required at follow-up with the specialist allergy service to measure baseline mast cell tryptase.” (p. 10) | The wording “may be” indicates a weak recommendation. The recommendation is based on very low certainty of evidence. | “Levels returned to normal by 24 hours after the onset of symptoms.” (p. 23) “The pattern of mast cell tryptase levels after anaphylaxis is consistent with the GDG’s clinical experience so the GDG also considered the use of the repeated mast cell tryptase measurements to be justified.” (p. 25) | |
Consensus-based guidelines | ||||
ANZAAG and ANZCA (2024)31 Perioperative anaphylaxis management guideline 2022 | Patients with suspected perioperative anaphylaxis | For anaphylaxis during anesthesia postcrisis management “A serum tryptase sample should be taken as soon as possible after the onset of symptoms and then repeated at 1 h, 4 h and after 24.” (p. 156) | Unclear | Unclear |
Japanese Society of Anesthesiologists (2021)30 Practical guidelines for the response to perioperative anaphylaxis | Patients with suspected perioperative anaphylaxis | “Blood for tryptase/histamine testing should be collected at two points, including at the time of onset and at the post-onset reference value” (p. 781) “In either case, if affordable, blood samples should be collected for tryptase and histamine tests at two-time points: immediately after onset and 24 hour after onset, as a reference value.” (p. 783) | Unclear | Unclear |
Working Group of Resuscitation Council UK (2021)32 Emergency treatment of anaphylaxis: Guidelines for healthcare providers | Patients with suspected anaphylaxis | “a) Minimum: one sample, ideally within 2 h (when peak tryptase levels generally occur) and no later than 4 h after onset of symptoms. b) Ideally: take three timed samples: 1. An initial sample as soon as feasible — but do not delay treatment to take sample. 2. A second sample 1 – 2 h (but no later than 4 h) after onset of symptoms. 3. A third sample at least 24 hour after complete resolution, or in convalescence (for example, at a follow-up allergy clinic).” (p. 41) | Unclear | Unclear |
Garvey, et al. (2019)20 Management of suspected immediate perioperative allergic reactions: an international overview and consensus recommendations | Patients with suspected perioperative allergic reactions | “In our Delphi process, the strongest consensus supported the first sample being obtained at 1 h after reaction onset and we recommend samples at 1 h and 2-4 h with a baseline sample for comparison obtained at least 24 h post reaction.” (p. e56) | Unclear | Unclear |
European Resuscitation Council Guidelines (2021)19 Cardiac arrest in special circumstances | Patients with suspected anaphylaxis | “Mast cell tryptase measurement can help diagnose anaphylaxis. The consensus on optimal timing for measurement is that ideally three timed samples should be taken:
| Unclear | Unclear |
NCCN (2024)28 Systemic Mastocytosis Guidelines (Version 3) | Patients with systemic Mastocytosis who had suspected anaphylaxis or other mast cell activation event | “In the event of anaphylaxis or other mast cell activation event, a full allergic workup should be initiated. The workup should include skin tests or detection of specific IgE antibodies for the identification of IgE-mediated hypersensitivity to drugs and measurement of serum tryptase level within 30 to 120 minutes of symptom onset and also after full recovery.” (p. MS-22) | Unclear | Unclear |
Recommendations from other documents | ||||
Platzgummer, et al. (2020)4 Recommendations for the Use of Tryptase in the Diagnosis of Anaphylaxis and Clonal Mastcell Disorders (narrative review) | Patient with suspected anaphylaxis | 1. “ Make the first blood withdrawal preferably 30 minutes – 3 hours after the event. 2. If possible, take a second sample 1 – 6 hours after the event to evaluate the kinetics. 3. Make another blood withdrawal at least 24 hours after the event (better after 42 −78 hours) 4. Always perform tryptase measurement in subjects who have experienced an anaphylactic reaction following a hymenoptera sting even if the event occurred 24 hours before.” (p. 57) | — | — |
Waterfield, et al. (2016)42 How to interpret mast cell tests (narrative review) | Patient with suspected anaphylaxis | “It is recommended that when used to aid the diagnosis of anaphylaxis, at least three samples are taken. The first is taken at the onset of the reaction, another at 1-2 hours and the third at 24 hours. An additional sample may need to be taken at 1 week after the reaction to establish a true baseline tryptase level.” (p. 247) | — | — |
CATS (2022)29 CATS clinical guideline: Anaphylaxis/Latex Allergy (guideline with unclear methods) | Anaphylaxis | “Ideally send three timed samples for mast cell tryptase:
| — | — |
Safer Care Victoria (2022)41 Anaphylaxis clinical care standard: Improving how we manage adults with anaphylaxis in Victoria (standard/guideline with unclear methods) | Anaphylaxis | “Timing of samples
| — | — |
Broyles, et al. (2020)38 Practical Guidance for the Evaluation and Management of Drug Hypersensitivity (narrative review) | Anaphylaxis (drug hypersensitivity) | “Sampling is recommended within 30 minutes and 2 hours in cases of grade III and IV reactions.” (p. s75) “Baseline tryptase level should be obtained more than 24 hours after the clinical event or when the patient is referred for investigation and compared with acute tryptase levels” (p. s75) | — | — |
Health New Zealand (NA)43 Laboratory Test Reference Guide (laboratory guidance) | Anaphylaxis | “Two samples should be collected; one sampled between 15 mins and 3 hours post anaphylactic reaction, and one 24 hours post anaphylactic reaction. Specimens taken outside this time frame may give misleadingly low results.” (p. 1) | — | — |
NHS South Tees Hospitals (2022)23 Tryptase (Mast Cell) (laboratory guidance) | Anaphylaxis | “As Tryptase values usually return to normal at 24 hours post reaction, three samples (EDTA plasma or serum) are required to be taken up to 1 hour, 3 hours and more than 24 hours of a suspected anaphylactic reaction.” | — | — |
NHS Manchester University (2023)33 Mast Cell Tryptase (laboratory guidance) | Anaphylaxis | “For suspected anaphylaxis samples should be taken
| — | — |
NSW Health (2022)22 Investigations to support the clinical diagnosis of anaphylaxis following COVID-19 vaccination (guideline with unclear methods) | Anaphylaxis (following COVID-19 vaccination) | 1. Collect an initial serum sample as soon as feasible, but do not delay initiating treatment. 2. Collect a second sample at 1 to 2 hours (but no later than 4 hours) from onset of symptoms. 3. If possible, take an extra 5 to 10 mL for storage to facilitate further investigations.” (web page) | — | — |
PathWest Laboratory Medicine WA (2023)37 Sampling time recommendations for mast cell tryptase in association with a suspected event causing mass cell activation (e.g., anaphylaxis) (guideline with unclear methods) | Suspected event causing mass cell activation, including anaphylaxis | “Sample collections for mast cell tryptase are now recommended to be taken: Close to 1 to 2 hours after the event (no later than 4 hours), and At least 24 hours after the event to obtain a baseline level.” (web page) | — | — |
Association for Laboratory Medicine (2017)39 Tryptase (serum, plasma) (laboratory guidance) | Patient with suspected anaphylaxis | “After a suspected reaction, timed blood samples should be taken for mast cell tryptase as follows: 1. as soon as possible after emergency treatment has started 2. within 1 to 2 hour (maximum 4 hour) from the onset of symptoms 3. at follow-up, at least 24 hour post-event to determine the baseline value. Serial measurements are essential for interpretation.” (p. 3) | — | — |
Vitte, et al. (2022)35 Tryptase and anaphylaxis: The case for systematic paired samples in all settings, from the playground to the COVID-19 vaccination center (narrative review) | Patient with suspected anaphylaxis | For suspected anaphylaxis: “Acute tryptase sampling
Baseline serum tryptase sampling
| — | — |
AAAAI = American Academy of Allergy, Asthma & Immunology; ACAAI = American College of Allergy, Asthma and Immunology; AGREE II = Appraisal of Guidelines for Research and Evaluation II; ANZAAG = Australian and New Zealand Anesthetic Allergy Group; ANZCA = Australian and New Zealand College of Anaesthetists; CATS = Children’s Acute Transport Service; EAACI = European Academy of Allergy and Clinical Immunology; h = hour(s); NA = not applicable; NCCN = National Comprehensive Cancer Network; NHS = National Health Service; NICE = National Institute for Health and Care Excellence; NSW = New South Wales.
Table 5: Summary of Recommendations for Patients With Confirmed Systemic Mastocytosis
Guideline developer, year, title | Populations or conditions | Recommendation or statement | Strength of the recommendation and quality of evidence | Supporting evidence and/or rationale |
|---|---|---|---|---|
Evidence-based recommendations | ||||
Brazil expert panel recommendations (2022)34 Diagnosis and treatment of systemic mastocytosis in Brazil: Recommendations of a multidisciplinary expert panel | Patients with SM | “Tryptase level measurements are necessary for the Systemic Mastocytosis diagnosis and follow-up (Grade 2) at least once a year (Grade 5).” (p. 585) | The recommendation was agreed upon by at least 75% of the panel. Grade 2 indicates intermediate evidence and Grade 5 indicates lowest grade evidence. | In SM, a persistently elevated serum tryptase level (> 20 ng/mL) is a minor diagnostic criterion in the WHO diagnostic framework and is elevated in most SM patients. It is a sensitive marker for the SM diagnosis and correlates with disease progression and treatment response, especially in advanced cases. |
Recommendations from laboratory guidance | ||||
NHS Manchester University (2023)33 Mast Cell Tryptase | Mastocytosis | “For mastocytosis repeat after 1 year or following significant clinical change.”(p. 1) | — | — |
SM = systemic mastocytosis.
Table 6: Summary of Timing of Tryptase Levels in Blood Sample After the Onset of Anaphylaxis Event
Author, year, study design | Conditions | Time to rise significantly | Half-life of tryptase | Timing of the peak levels | Returning to prereaction or baseline |
|---|---|---|---|---|---|
Centre for Clinical Practice at NICE (2021),40 evidence- based guideline | Anaphylaxis | NR | 30 minutes to 300 minutes (median 90 minutes) | 1 minute to 6 hours (median 30minutes) | By 24 hours |
Littlejohns, et al. (2024),25 narrative review | Anaphylaxis (perioperative hypersensitivity) | NR | About 2 hours | 1 to 2 hours | Within 6 to 8 hours |
Platzgummer, et al. (2020),4 narrative review | Anaphylaxis | 5 to 30 minutes (begin to rise) | 1.5 to 2.5 hours | 1 to 3 hours | Within 16 to 24 hours |
Beck, et al. (2019),16 narrative review | Anaphylaxis | NR | About 2 hours | The first 90 minute | Up to or beyond 24h |
Laguna, et al. (2018),24 guideline (the relevant information from their narrative review) | Anaphylaxis (perioperative hypersensitivity) | NR | NR | 1 to 2 hours | 4 to 6 hours |
Buka, et al. (2017),17 retrospective cohort study | Anaphylaxis | NR | About 2 hours | 1 to 2 hours | 6 to 8 hours |
Waterfield, et al. (2016),42 narrative review | Anaphylaxis | NR | About 2 hours | 1 to 6 hours | About 24 hours |
Safer Care Victoria (2022),41 standard/guideline with unclear methods | Anaphylaxis | 30 minute or more | 2h | 1 to 2 hours | 6 to 8 hours |
Irish Association for Emergency Medicine (2022),18 guideline (the relevant information from their narrative review) | Anaphylaxis | 30 minute or more | 2 hours | 1 to 2 hours | 6 to 8 hours |
Working Group of Resuscitation Council UK (2021),32 guideline (the relevant information from their narrative review) | Anaphylaxis | 30 minute or more | About 2 hours | 1 to 2 hours | 6 to 8 hours |
Broyles, et al. (2020),38 narrative review | Anaphylaxis (drug hypersensitivity) | NR | About 90 minutes | 1 hour | NR |
Mayorga, et al. (2016),26 position paper from ENDA/EAACI | Anaphylaxis (drug hypersensitivity) | NR | 90 −120 minutes | NR | NR |
Health New Zealand laboratory test reference guide (publication year not available),43 laboratory guidance | Anaphylaxis | NR | 2 hours | NR | Up to 24 hours |
Association for Laboratory Medicine (2017),39 laboratory guidance | Anaphylaxis | NR | 2h | NR | NR |
Vitte (2021),36 narrative review | Anaphylaxis (perioperative hypersensitivity) | NR | About 2 hours | NR | NR |
EAACI = European Academy of Allergy and Clinical Immunology; ENDA = European Network of Drug Allergy; NICE = National Institute for Health and Care Excellence; NR = not reported.
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up to date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for noncommercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca