CADTH Health Technology Review
Methoxyflurane Inhalation as an Analgesic for Minor Gynecological, Ambulatory, or Emergency Procedures
Rapid Review
Key Messages
What Is the Issue?
Patients presenting to outpatient clinics or emergency departments often undergo procedures that cause pain.
Procedural sedation and analgesia for pain management requires a trained person to administer sedative agents and manage any drug-related complications during and after the procedures.
Inhaled methoxyflurane (Penthrox) was approved in Canada in 2022 for short-term relief of moderate to severe acute pain associated with trauma or interventional medical procedures in conscious adult patients.
Unlike conventional sedation, patients can self-administer and titrate the amount of methoxyflurane by inhaling through a 3 mL device of 99.9% methoxyflurane, which provides continuous analgesia for 25 to 30 minutes.
Decision-makers are interested in understanding the use of inhaled methoxyflurane for analgesia in minor gynecological procedures or for use in ambulatory or emergency care settings.
What Did We Do?
We identified and summarized literature on the clinical effectiveness and safety of methoxyflurane compared to placebo or other analgesics in minor medical and surgical procedures. We also searched for economic evaluations of the cost-effectiveness of methoxyflurane to manage pain during minor procedures.
We searched peer-reviewed and grey literature sources published between January 1, 2012, and July 3, 2024. One reviewer screened citations for inclusion based on predefined criteria, critically appraised the included studies, and narratively summarized the findings.
What Did We Find?
We identified 1 systematic review, 1 randomized controlled trial, 1 prospective cohort study, and 2 retrospective chart review studies that provided evidence on the efficacy and safety of methoxyflurane during various minor medical procedures, including cancer-related procedures (i.e., colonoscopy, transrectal ultrasonography-guided prostate biopsy, bone marrow biopsy, and solid organ biopsy) and other minor procedures (i.e., portacath insertion, portacath removal, and reduction of acute shoulder dislocation and acute elbow dislocation).
Collective evidence from the few studies available for each type of procedure shows that methoxyflurane is an effective analgesic that, compared with sedation, shortens the duration of both the procedure and recovery without impacting procedural success.
Methoxyflurane at the analgesic dose appears to be safe — that is, not associated with kidney or liver toxicity and resulting in fewer cardiorespiratory complications or severe adverse events — despite being more likely to cause drowsiness and dizziness compared with placebo or conventional sedation.
We did not find any studies on the clinical efficacy and safety or cost-effectiveness of methoxyflurane inhalation for the treatment of pain for minor gynecological procedures.
We did not find any studies on cost-effectiveness of methoxyflurane inhalation for the treatment of pain for minor ambulatory or emergency procedures.
What Does This Mean?
The limited studies available suggested that patient-controlled analgesia with methoxyflurane is feasible and safe for use during various ambulatory and emergency procedures.
The benefits of methoxyflurane in terms of reducing procedural and recovery time may facilitate workflow and shorten waiting lists in ambulatory and emergency care settings.
More studies are needed to provide stronger evidence on the efficacy and safety of methoxyflurane during medical and surgical procedures.
Abbreviations
AE
adverse event
AED
acute elbow dislocation
ASD
acute shoulder dislocation
ED
emergency department
PETB
patient’s experience of transrectal ultrasonography-guided prostate biopsy
RCT
randomized controlled trial
SR
systematic review
TRUSB
transrectal ultrasonography-guided prostate biopsy
Context and Policy Issues
What Is Methoxyflurane?
Methoxyflurane belongs to a fluorinated hydrocarbon group, and it was first used as a general anesthetic drug in the 1960s.1,2 It became more popular than other volatile anesthetics because it does not impair cardiovascular stability and it provides analgesia that extends into the postoperative period.2,3 However, the use of methoxyflurane as an anesthetic drug disappeared from clinical practice in the late 1970s when it was found to cause serious dose-related nephrotoxicity when used at high doses over prolonged periods.3
Despite the stop in its use as an anesthetic drug, methoxyflurane has been reintroduced for use at subanesthetic doses as an analgesic for short-term relief of moderate to severe acute pain in patients with trauma or procedure-related pain.4 The risk of nephrotoxicity of methoxyflurane is low at low doses.4 Methoxyflurane is manufactured under the brand name Penthrox and is currently distributed in Canada through Paladin Labs (Montreal, QC, Canada).5 Penthrox has been approved by Health Canada for short-term relief of moderate to severe acute pain associated with trauma or interventional medical procedures in conscious adult patients.6
Penthrox is a portable, lightweight, noninvasive inhaler for self-administration.4,6 The Penthrox kit has 3 main components: the Penthrox inhaler (mouthpiece or “the green whistle”), the activated carbon chamber, and 99.9% methoxyflurane in 3 mL bottle.4,6 The unique characteristics of methoxyflurane — such as noninvasive administration, rapid onset of action, short half-life, and portability — make it a favourable option for acute pain management in different medical settings, including paramedic services, outpatient care, and the emergency department (ED).2,4
Why Is It Important to Do This Review?
Painful outpatient procedures normally require conventional sedation, which requires a trained health care worker to administer the sedative agents and monitor for complications, including excessively deep sedation, loss of airway control, and impairment of cardiovascular function.3 It is, therefore, important to find out if there is any evidence that methoxyflurane can be an alternative to traditional sedation methods for procedural analgesia.
Objective
To support decision-making about the role of methoxyflurane for procedural analgesia, we prepared this Rapid Review to summarize and critically appraise the available studies on the clinical efficacy and safety of methoxyflurane for pain management during minor medical and surgical procedures.
Research Questions
What is the clinical effectiveness and safety of methoxyflurane inhalation for the treatment of pain during minor gynecological procedures?
What is the clinical effectiveness and safety of methoxyflurane inhalation for the treatment of pain during minor ambulatory or emergency procedures?
What is the cost-effectiveness of methoxyflurane inhalation for the treatment of pain during minor gynecological procedures?
What is the cost-effectiveness of methoxyflurane inhalation for the treatment of pain during minor ambulatory or emergency procedures?
Methods
Literature Search Methods
An information specialist conducted a literature search on key resources including MEDLINE, Embase, the Cochrane Database of Systematic Reviews, the International HTA Database, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search approach was customized to retrieve a limited set of results, balancing comprehensiveness with relevancy. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. Search concepts were developed based on the elements of the research questions and selection criteria. The main search concept was methoxyflurane. The search was completed on July 3, 2024 and limited to English-language documents published since January 1, 2012.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
|---|---|
Population | Adult patients undergoing minor gynecological, ambulatory, or emergency procedures |
Intervention | Methoxyflurane inhalation (Penthrox) |
Comparator | Placebo, analgesics (e.g., NSAIDs, acetaminophen, opioids, ketamine) |
Outcomes | Clinical effectiveness (e.g., pain relief, need for other analgesics) or harm (e.g., nausea, dizziness, abdominal pain, malignant hypothermia) Cost-effectiveness (e.g., cost per QALY gained, ICER) |
Study designs | HTAs, RCTs, SRs with or without MA or NMA, nonrandomized studies |
HTA = health technology assessment; ICER = incremental cost-effectiveness ratio; MA = meta-analysis; NMA = network meta-analysis; NSAID = nonsteroidal anti-inflammatory drug; QALY = quality-adjusted life-year; RCT = randomized controlled trial; SR = systematic review.
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1 or were published before 2012. Primary studies retrieved by the search were excluded if they were captured in the selected systematic review (SR). Studies without a comparator were excluded, but they are listed in Appendix 5 as references of potential interest.
Critical Appraisal of Individual Studies
One reviewer critically appraised the included publications using the following tools as a guide: A MeaSurement Tool to Assess systematic Reviews 2 (AMSTAR 2)7 for the SR and the Downs and Black8 checklist for randomized controlled trials (RCTs) and nonrandomized studies. Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Summary of Evidence
Quantity of Research Available
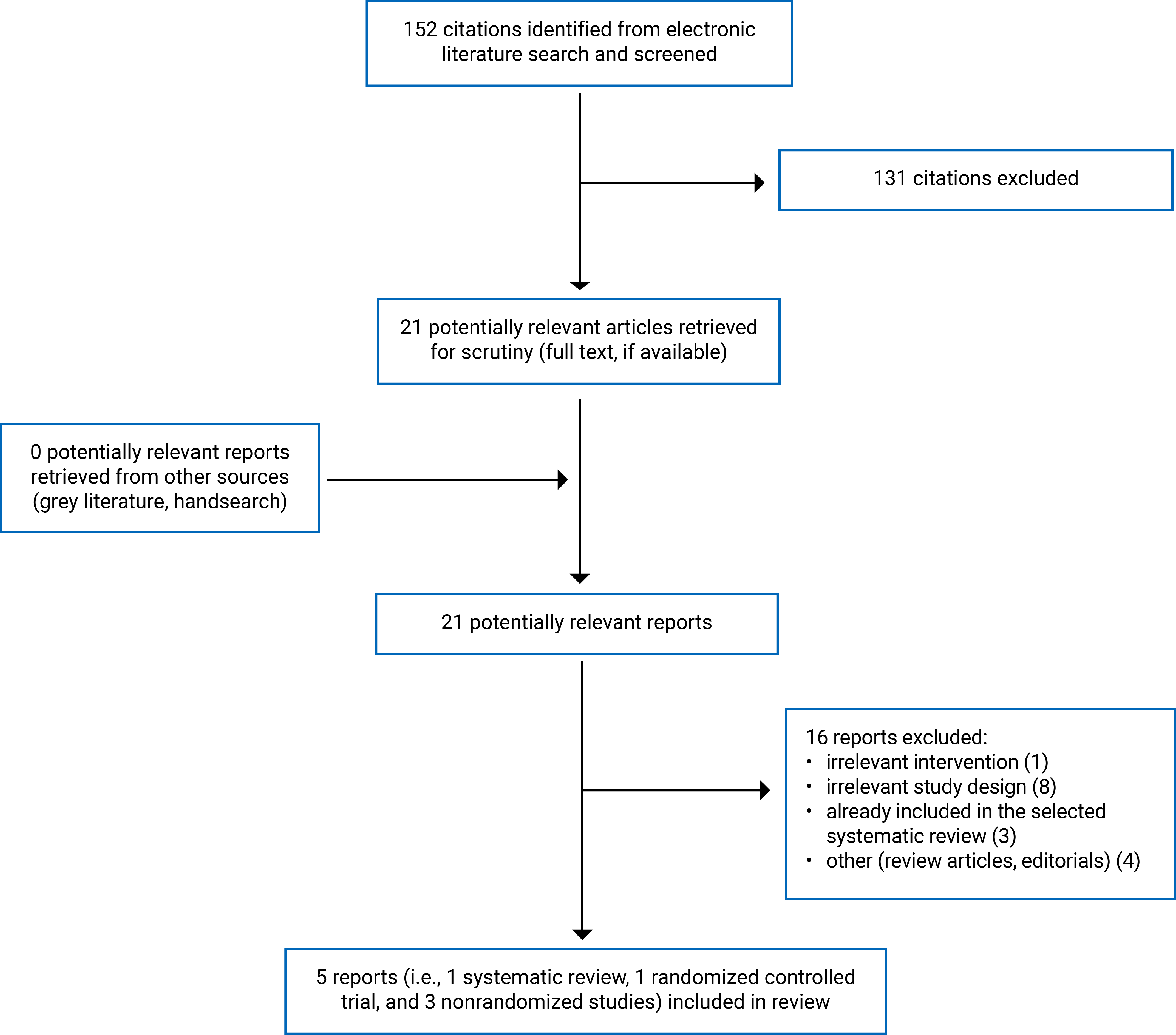
We identified a total of 152 citations from the literature search. Following screening of titles and abstracts, we excluded 131 citations and retrieved 21 potentially relevant reports from the electronic search for full-text review. We found no potentially relevant publications from the grey literature search. Of the 21 potentially relevant articles, we excluded 16 publications for various reasons and included 5 publications that met the inclusion criteria. These comprised 1 SR, 1 RCT, and 3 nonrandomized studies. Appendix 1 presents the PRISMA9 flow chart of the study selection.
Summary of Study Characteristics
Appendix 2 provides details regarding the characteristics of the 1 SR10 (Table 2) and the 4 primary studies (Table 3).11-14
Included Studies for Question 1: What Is the Clinical Effectiveness and Safety of Methoxyflurane Inhalation for the Treatment of Pain During Minor Gynecological Procedures?
We did not identify any studies on the comparative clinical effectiveness and safety of methoxyflurane inhalation for the treatment of pain during minor gynecological procedures.
Included Studies for Question 2: What Is the Clinical Effectiveness and Safety of Methoxyflurane Inhalation for the Treatment of Pain During Minor Ambulatory or Emergency Procedures?
Study Design
We identified 1 SR,10 1 RCT,11 1 prospective cohort study,12 and 2 retrospective chart reviews studies.13,14
The SR10 included 7 studies, of which 3 RCTs were relevant and are discussed in this report. Of the 4 irrelevant studies, 3 did not have a control treatment arm and 1 had an irrelevant comparator.
Three included primary studies10-12 involved procedures in the ambulatory setting, and 2 studies13,14 involved procedures in the ED setting.
Country of Origin
The SR10 was conducted by authors in Canada. The 3 relevant RCTs included in the SR10 were all conducted by authors in Australia.
The 4 included primary studies were conducted by authors in Australia,11,12 Ireland,14 and Singapore.13
Patient Population
The population in the 3 RCTs included in the SR10 had had undergone colonoscopy, transrectal ultrasonography-guided prostate biopsy (TRUSB), or bone marrow biopsy.
The RCT by Copping et al. (2024)11 included patients presenting for various minor procedures such as portacath insertion, portacath removal, or solid organ biopsy.
The prospective cohort study by Nguyen et al. (2015)12 included patients with morbid obesity and/or obstructive sleep apnea who underwent colonoscopy procedures.
The 2 retrospective chart review studies by Ho et al. (2022)13 and Umana et al. (2019)14 included patients presenting to the ED for manipulation and reduction of acute shoulder dislocation (ASD)13,14 and acute elbow dislocation (AED).13
Interventions and Comparators
The intervention in all the included studies was methoxyflurane formulated in the Penthrox inhaler, a small, disposable, hand-held device that allows patients to self-administer and control the amount of methoxyflurane through frequency and depth of inhalation.
The comparators were either placebo or conventional IV sedation (e.g., fentanyl, midazolam, ketamine, propofol, or ketofol). For placebo, patients were given an identical-looking inhaler in a plastic bag, like the intervention. One drop of methoxyflurane was placed in the plastic bag for both groups to give all patients the characteristic fruity odour of methoxyflurane and, thereby, maintaining the blinding process.
For the colonoscopy procedure, methoxyflurane was compared with conventional sedation in the nonblinded RCT included in the SR10 and in a prospective cohort study.12 For other procedures — such as TRUSB, bone marrow biopsy, portacath insertion, portacath removal, or solid organ biopsy — methoxyflurane was compared with placebo in double-blind RCTs.10,11 The 2 retrospective chart review studies13,14 compared methoxyflurane with sedation for pain management for the manipulation and reduction of ASD or AED in the ED.
Outcomes
Pain was an outcome measured during various procedures, including colonoscopy, TRUSB, bone biopsy, portacath insertion, portacath removal, and solid organ biopsy.10-12 The visual analogue scale and the numerical rating scale (NRS) were used to assess pain. Pain was not measured in studies13,14 involving the manipulation and reduction of ASD and AED in the ED.
Other outcomes included anxiety,10-12 procedural performance,10,12-14 adverse events (AEs),10-13 discomfort,10 drowsiness,10 dizziness,10 proceduralist perception,10,11 patient perception,10 and length of stay in the ED.13,14
Included Studies for Question 3: What Is the Cost-Effectiveness of Methoxyflurane Inhalation for the Treatment of Pain During Minor Gynecological Procedures?
We did not identify any studies on the cost-effectiveness of methoxyflurane inhalation for the treatment of pain during minor gynecological procedures.
Included Studies for Question 4: What Is the Cost-Effectiveness of Methoxyflurane Inhalation for the Treatment of Pain During Minor Ambulatory or Emergency Procedures?
We did not identify any studies on the cost-effectiveness of methoxyflurane inhalation for the treatment of pain during minor ambulatory or emergency procedures.
Summary of Critical Appraisal
Appendix 3 provides details regarding the strengths and limitations of the included SR (Table 4) and primary studies (Table 5).
Systematic Review
The included SR10 was explicit in its objective, inclusion criteria for the review, and selection of the study designs for inclusion. The literature search strategy was partially comprehensive as the authors did not indicate that they searched the reference lists of the included studies, trial registries, or grey literature. Not providing details of the literature search strategy reduces the reproducibility of the review. The SR did not report whether a protocol had been published before the review was conducted; the publishing of a protocol before conducting the review would increase the confidence that methods were not modified after the SR had been conducted. Although study selection was performed independently by 2 reviewers, it is unclear if data extraction was also similarly performed. Although the characteristics of the included studies were described in adequate detail — including study design, intervention, control, and outcomes — the methodological quality of the included studies was not assessed, and patient characteristics were not adequately described. Moreover, a list of excluded studies and the reasons for exclusion were not provided. Therefore, it was not possible to assess whether any relevant articles were excluded and, if so, for what reasons. The review authors did not report the sources of funding for the included studies nor the sources of funding for the SR itself. Knowing the funding sources could determine the degree of confidence in the findings. Overall, the SR that narratively summarized the findings from the included studies had several methodological limitations regarding literature search strategy, reporting, data collection process, and analysis that may increase the uncertainty of the findings. Therefore, we referred to the original primary studies included in the SR for description of the findings to accurately capture all the details of relevant outcomes.
Primary Studies
The included RCT11 and the prospective cohort study12 were explicit in terms of reporting (i.e., objectives, intervention of interest, main outcomes, main findings, and characteristics of the participants). AEs of the intervention and actual P values for the main outcomes were reported. The 2 retrospective chart review studies13,14 were also explicit in terms of reporting, except that safety outcomes of the intervention were not reported. For external validity, the staff, places, and facilities (i.e., hospitals) where the patients were treated were representative of the treatment the majority of the patients receive in all included studies.11-14 The patients in the included RCT11 and prospective cohort study12 may be representative of the entire population from which they were recruited; however, the recruitment of patients from a single centre in those studies might limit the generalizability of the findings. Those in the 2 retrospective chart review studies13,14 may not be representative of the entire population from which they were recruited, due to small sample size and high risk of selection bias. For internal validity related to bias, the RCT by Copping et al. (2024)11 had low risk of selection, performance, and detection biases because the procedural team, patients, and data analysts were blinded to randomization order. Statistical tests were used appropriately, and the main outcome measures were accurate and reliable.11 The prospective cohort study by Nguyen et al. (2015)12 had a similar strength of internal validity related to bias, except the study allowed participants to choose either methoxyflurane or anesthesia-assisted deep sedation, which may introduce some risk of selection bias. Both retrospective chart review studies13,14 had a high risk of selection bias due to the nature of study design. The RCT by Copping et al. (2024)11 had a low risk of internal validity related to confounding for all items. The prospective cohort study by Nguyen et al. (2015)12 also had a low risk of internal validity related to confounding, as the patient characteristics between groups were well balanced. In both retrospective chart review studies,13,14 limitations in terms of internal validity related to confounding included lack of sample size calculation and lack of identification and adjustment for potential confounders in the analyses. Overall, unlike the RCT11 and the prospective cohort study,12 both retrospective chart review studies13,14 had several limitations related to reporting, external validity, internal validity related to bias, and internal validity related to confounding that may reduce the certainty of the findings.
Summary of Findings
Appendix 4 presents the main study findings, which were summarized by procedure (i.e., colonoscopy in Table 6, TRUSB in Table 7, bone marrow biopsy in Table 8, reduction of ASD and AED in Table 9, and other minor procedures in Table 10).
Clinical Effectiveness and Safety of Methoxyflurane Inhalation for the Treatment of Pain During Minor Gynecological Procedures
We did not identify any studies on the clinical effectiveness and safety of methoxyflurane; therefore, no summary can be provided.
Clinical Effectiveness and Safety of Methoxyflurane Inhalation for the Treatment of Pain During Minor Ambulatory or Emergency Procedures
Colonoscopy
One RCT included in the SR10 and 1 prospective study12 evaluated the efficacy and safety of methoxyflurane in colonoscopy (Table 6).
The RCT included in the SR10 was a multicentre, nonblinded RCT comparing methoxyflurane to conventional sedation (i.e., fentanyl and midazolam) in a population without major comorbidities. The study found no statistically significant differences between groups in visual analogue scale (VAS) pain scores before, during, or immediately after colonoscopy. Although the anxiety scores were statistically significantly higher in the methoxyflurane group, the “nervousness” subscores were not statistically significantly different between groups. The procedural preparation time, cecal arrival time, total colonoscopy time, success rate of complete colonoscopy, and rate of polyp detection and polypectomy were also not statistically significant different between groups. Colonoscopist perceptions in terms of patient’s discomfort, procedural difficulty, and patient’s cooperation were similar between groups. Patients receiving methoxyflurane had no desaturation (oxygen saturation [SaO2] < 90%, events: 0/115 versus 5/116; P = 0.03), awoke quicker (3 ± 0 minutes versus 19 ± 1 minute; P < 0.001), and were ready for discharge earlier (37 ± 1 minute versus 66 ± 2 minutes; P < 0.001) than those receiving IV sedation. The rates of AEs (i.e., respiratory depression, hypotension, and cardiac arrythmia) were similar between groups. For patient perception of the use of methoxyflurane for colonoscopy, 97% of patients who had successful colonoscopy with methoxyflurane were willing to use methoxyflurane again for future colonoscopy.
The same group of authors published a single-centre, prospective cohort study12 evaluating the efficacy and safety of methoxyflurane compared with conventional sedation in patients with morbid obesity and/or obstructive sleep apnea. Although patients receiving methoxyflurane had statistically significantly higher pain scores during colonoscopy (3.6 ± 2 versus 0.9 ± 1; P < 0.001) compared with those receiving sedation, the pain was perceived as tolerable and short-lasting as there were no differences in pain scores between groups right after colonoscopy. There were also no differences between groups in total anxiety scores and “nervousness” subscores. The in-room preparation time (4.8 ± 0.2 minutes versus 16.5 ± 1.8 minutes; P < 0.01), cecal arrival time (8.8 ± 0.5 minutes versus 11.6 ± 1.0 minutes; P < 0.01), total colonoscopy time (18.4 ± 0.9 minutes versus 25.9 ± 1.7 minutes; P < 0.01), and total in-room time (23.9 minutes ± 0.9 versus 51.6 ± 1.3 minutes; P < 0.001) were statistically significantly shorter in the methoxyflurane group than in the sedation group. However, the rates of polyp detection and polypectomy were not statistically significantly different between groups. Patients receiving methoxyflurane had statistically significantly lower intraprocedural events of respiratory depression (0% versus 26%; P < 0.001), hypotension (1% versus 42%; P < 0.001) and tachycardia (1% versus 15%; P < 0.001) compared to those receiving sedation. No patient in either group was readmitted to the hospital due to nephrotoxicity or hepatotoxicity. For recovery and discharge time, patients who received methoxyflurane had a statistically significantly (P < 0.001) shorter time to awake, to oral intake, to be ready for discharge, and to actual discharge than those who received sedation. Patients receiving methoxyflurane had comparable satisfaction scores with sedation (98 ± 5 versus 94 ± 6; P = 0.76), with more than 90% of patients willing to undergo colonoscopy with inhaled methoxyflurane in the future.
Transrectal Ultrasonography-Guided Prostate Biopsy
The RCT included in the SR10 was a multicentre, placebo-controlled, double-blind, randomized phase III trial that evaluated the efficacy of adding inhaled methoxyflurane to periprostatic infiltration of local anesthesia during TRUSB (Table 7). Using the patient’s experience of TRUSB (PETB) questionnaires, the trial did not find any statistically significant differences in patient-related pain scores between the methoxyflurane and placebo groups 15 minutes after biopsy. Other domains of the PETB questionnaires showed that the methoxyflurane group had lower scores for discomfort (2.86 ± 0.22 versus 3.34 ± 0.22; P = 0.035; adjusted P = 0.076) and the whole experience (2.51 ± 0.21 versus 2.65 ± 0.21; P = 0.021; adjusted P = 0.053) after 15 minutes biopsy, but higher scores in drowsiness (2.36 ± 0.21 versus 0.72 ± 0.21; P < 0.001; adjusted P < 0.001) and dizziness (2.45 ± 0.23 versus 0.67 ± 0.23; P < 0.001; adjusted P < 0.001) compared to placebo. Fifteen minutes after biopsy, 60% of patients in the methoxyflurane group responded that they would like to undergo repeat prostate biopsy in the future compared to 47% in the placebo group. In terms of AEs, methoxyflurane was associated with statistically significantly higher incidence rates of dizziness (51% versus 30%; P < 0.001) and somnolence (44% versus 26%; P < 0.001) compared to placebo. There was no statistically significant difference between groups in the incidence of AEs of grade 3 and up. Of note, urologists’ assessments using the modified PETB questionnaire scores suggested statistically significantly less pain, less discomfort, but more drowsiness and dizziness in patients assigned to methoxyflurane than placebo. However, urologists’ assessment for pain and other outcomes may have some risk of bias, due to potential jeopardizing of the blinding process, given that patients receiving methoxyflurane had high incidence of drowsiness and dizziness.
Bone Marrow Biopsy
The SR10 included a single-centre, double-blind, placebo RCT assessing the efficacy and safety of methoxyflurane for the management of pain during bone marrow biopsy (Table 8). Methoxyflurane was associated with a statistically significant reduction in overall worst pain scores during the procedure compared to placebo (mean difference = 1.08; 95% CI, 0.21 to 1.95; P = 0.011). However, the authors of the study noted that the difference of 1.08 was not clinically relevant, as the placebo effect in a trauma trial was equivalent to 1.5 on an 11-point VAS scale.15 Significantly more patients in the methoxyflurane group rated the medication as “very good” or “excellent” compared to those in placebo group (49% versus 16.5%; P < 0.001). Ten patients (20.4%) in the methoxyflurane group experienced grade 1 AEs compared to 2 patients (4.2%) in placebo group. The AEs in the methoxyflurane group included dizziness, euphoria, flushing, hypertension, anxiety, depression, sensory neuropathy, and somnolence.
Reduction of Acute Shoulder and Elbow Dislocation in the ED
Two retrospective chart review studies13,14 compared the use of inhaled methoxyflurane with traditional procedural sedation and analgesia for manipulation and reduction of ASD and AED (Table 9). Both studies assessed length of stay in the ED and procedural performance as outcomes. Pain was not reported as an outcome in both studies.
In the study by Ho et al. (2022),13 methoxyflurane was associated with a statistically significantly shorter mean patient length of stay in the ED (99.0 [136.8] minutes versus 246.5 [163.0] minutes; P < 0.001) and shorter duration of procedure (16.0 [17.0] minutes versus 32.0 [40.3] minutes; P < 0.001) compared to procedural sedation and analgesia. The authors of the study stated that there were no AEs reported for either group of patients. They also noted that patients’ pain score data were incomplete and hence no conclusions could be drawn on this aspect.
The study by Umana et al. (2019)14 also found a statistically significantly shorter median duration of patient length of stay in the ED (70.5 [49.3 to 105] minutes versus 135 [77 to 21] minutes; P < 0.001) and median recovery time (30 [19.3 to 44] minutes versus 47 [32 to 68] minutes; P < 0.004) in the methoxyflurane group compared with the procedural sedation (propofol) group. The authors reported that no AEs were documented.
Other Minor Procedures
A single-centre, double-blind placebo-controlled RCT by Copping et al. (2024) evaluated the efficacy and safety of methoxyflurane for minor procedures such as portacath insertion, portacath removal or solid organ biopsy in the interventional radiology unit. The methoxyflurane group had lower pain scores (0.72 versus 1.80; P < 0.001) and anxiety scores (1.53 versus 2.50; P < 0.001) overall throughout the procedure. The proceduralist’s perspective suggested that more patients in the methoxyflurane group felt comfortable (91.0% versus 79.4%; P = 0.013) and perceived that the medication was effective (88.0% versus 75.0%; P = 0.032) during the procedure compared to placebo. There were no drug-related AEs or major procedural-related AEs (grades 3 to 6). Minor symptoms associated with methoxyflurane compared with placebo were nausea (6 versus 3), dizziness (5 versus 2), and headache (3 versus 0). Blood test results revealed no significant difference in the change of renal function or liver function between groups.
Cost-Effectiveness of Methoxyflurane Inhalation for the Treatment of Pain During Minor Gynecological Procedures
We did not identify any studies on cost-effectiveness of methoxyflurane inhalation for the treatment of pain for minor gynecological procedures; therefore, no summary can be provided.
Cost-Effectiveness of Methoxyflurane Inhalation for the Treatment of Pain During Minor Ambulatory or Emergency Procedures
We did not identify any studies on cost-effectiveness of methoxyflurane inhalation for the treatment of pain for minor ambulatory or emergency procedures; therefore, no summary can be provided.
Limitations
Evidence Gaps
No evidence was found for the 3 research questions related to:
The clinical effectiveness and safety of methoxyflurane inhalation for the treatment of pain during minor gynecological procedures.
The cost-effectiveness of methoxyflurane inhalation for the treatment of pain during minor gynecological procedures.
The cost-effectiveness of methoxyflurane inhalation for the treatment of pain during minor ambulatory or emergency procedures.
Generalizability
The small number of existing studies on the use of methoxyflurane for each type of minor procedure, and the strict inclusion criteria of those studies, limit the generalizability of their findings to the general patient population. Additional research is needed to further explore the benefits methoxyflurane can offer in minor medical and surgical procedures in a real-world population in Canada.
Heterogeneity
Our review included studies on several procedures, such as colonoscopy, TRUSB, bone marrow biopsy, and the manipulation and reduction of ASD and AED. Patient populations were completely different among the studies. Therefore, the observed efficacy of methoxyflurane, particularly on pain reduction, of 1 procedure may not be applicable to the other and is likely to be procedure-specific.
Certainty of Evidence
The included SR10 identified only a few studies on the use of methoxyflurane on pain reduction in cancer-related procedures (i.e., colonoscopy, TRUSB, and bone marrow biopsy), which yields unclear significance without additional research. The small available number of studies suggested that there was a risk of publication bias, as articles with nonsignificant results might not be published.
For colonoscopy, an RCT included in the SR10 might have potential selection bias toward patients who were healthy and did not have serious medical conditions, as defined in its selection criteria. In addition, patients who refused to participate in the assessment of pain and anxiety were not included in the trial. Thus, the patients included in the trial might be less anxious than the general patient population referred for colonoscopy. The trial found no difference between methoxyflurane and sedation groups in terms of pain score, procedural performance, AEs, and colonoscopist perception. In contrast, the prospective cohort study12 conducted later by same group of authors involved patients with morbid obesity and/or obstructive sleep apnea found slightly different results, in terms of pain, anxiety, procedural performance, and AEs. This study might be limited by selection bias because participants were given the choice of either methoxyflurane or conventional sedation. The results need to be verified with a randomized study.
For TRUSB, although the trial included in the SR10 was a multicentre study, 65% of participants were recruited from a single institution, which limits the generalizability of the findings. Fifteen percent of patients used another analgesic 24 hours before the procedure, which might have reduced their reported pain scores. The use of questionnaires completed by urologists and patients as outcomes measures was susceptible to bias if the assigned treatment was recognized by those who completed the form.
For bone marrow biopsy, all patients in the trial included in the SR10 received local anesthetic as well as the study drug. The addition of local anesthesia might reduce the difference in pain scores between the methoxyflurane and placebo groups. This might be the reason the difference in pain scores was not clinically relevant.
For the manipulation and reduction of ASD and AED, the limitations of the studies13,14 were their retrospective design and their dependence on documentation by doctors and nurses. The use of methoxyflurane or procedural sedation was at the discretion of the treating physician and, therefore, may have led to selection bias. Different reduction techniques used for ASD or AED were not accounted for as covariates in the analyses, which may impact the findings.
Conclusions and Implications for Decision- or Policy-Making
This review included 1 SR,10 1 RCT,11 1 prospective cohort study,12 and 2 retrospective chart review studies13,14 that evaluated the efficacy and safety of various medical procedures including colonoscopy, TRUSB, bone marrow biopsy, the manipulation and reduction of ASD and AED, and other minor procedures (i.e., portacath insertion, portacath removal or solid organ biopsy). We did not identify any studies assessing the efficacy and safety of methoxyflurane compared to placebo or other analgesics for minor gynecological procedures. We also did not identify any economic studies evaluating the cost-effectiveness of methoxyflurane for the treatment of pain for minor ambulatory or emergency procedures, including gynecological procedures.
Colonoscopy
One RCT included in the identified SR10 and 1 prospective cohort study12 evaluated the efficacy and safety of methoxyflurane for colonoscopy in patients without comorbidities, and in patients with morbid obesity and/or obstructive sleep apnea, respectively. In the noncomorbid patient population, there were no statistically significant differences in VAS pain scores before, during, and after colonoscopy between patients who received methoxyflurane and conventional sedation. In contrast, patients with morbid obesity and/or obstructive sleep apnea had higher pain scores with methoxyflurane than conventional sedation during colonoscopy. Mixed results were also found between the 2 studies for other outcomes such as anxiety, procedural performance, and AEs. Despite these mixed findings, patients receiving methoxyflurane in both studies had no oxygen desaturation, awoke more quickly, and were ready for discharge earlier than those receiving conventional sedation. Patients receiving methoxyflurane had good satisfaction overall, which was comparable with sedation, with more than 90% of patients willing to undergo colonoscopy with methoxyflurane if required. Thus, pain and anxiety may not be the relevant outcomes in colonoscopy, and the use of methoxyflurane may be feasible and safe with shorter recovery and discharge time, similar or better in terms of procedural performance, and result in similar or fewer intraprocedural AEs compared to sedation.
Transrectal Ultrasonography-Guided Prostate Biopsy
A double-blind, placebo-controlled RCT included in the identified SR10 provided no evidence that addition of methoxyflurane to periprostatic infiltration of local anesthesia during TRUSB improved pain scores; however, improvements were observed in patient discomfort, overall experience, and willingness to undergo repeat biopsy if needed. Although methoxyflurane was associated with higher incidence of dizziness and drowsiness, its use appeared to be safe, with no differences in the number of grade 3 or higher AEs or 30-day hospitalization rate compared to placebo.
Bone Marrow Biopsy
For bone marrow biopsy, a double-blind, placebo-controlled RCT included in the identified SR10 provided evidence that methoxyflurane reduced pain during the procedure compared to placebo, but the difference in pain scores may not be clinically relevant. Almost 50% of patients who received methoxyflurane reported “very good” or “excellent experience” despite a higher incidence of grade 1 AEs, including dizziness and euphoria.
Reduction of Acute Shoulder and Elbow Dislocation in the ED
Two retrospective chart review studies13,14 provided evidence that the use of methoxyflurane in the manipulation and reduction of ASD and AED in the ED was associated with shorter patient length of stay and shorter duration of procedure, without compromising the successful rate compared to sedation. Patients’ pain score and AE data were not reported in both studies; therefore, no conclusions can be drawn on those aspects.
Other Minor Procedures
The findings of a double-blind, placebo-controlled RCT11 suggested that methoxyflurane provided effective analgesia and anxiolysis (i.e., pain and anxiety score reduction) in minor procedures such as portacath insertion, portacath removal or solid organ biopsy. Methoxyflurane appeared to be safe, as there were no major procedural-related AEs (grades 3 to 6), no drug-related AEs, and no significant difference in the change of renal function or liver function compared to placebo.
Considerations for Future Research
More studies are needed to provide stronger evidence on the efficacy and safety of methoxyflurane in the procedures reviewed in this report. Since evidence on the efficacy and safety of methoxyflurane in minor gynecological procedures is currently lacking, evaluation in future studies is warranted. Based on the clinical evidence reviewed in this report so far, the benefits of methoxyflurane regarding reduction procedural time and recovery time need to be further evaluated in an economic model to determine if methoxyflurane is cost-effective compared to placebo or other analgesics. Evidence of economic evaluations on this aspect is urgently required to inform funding decisions of methoxyflurane for procedural use in ambulatory or emergency settings.
Implications for Clinical Practice
The findings of this report suggest that methoxyflurane is suitable for use in procedural analgesia in the ambulatory or emergency environment. Although pain may not be the only relevant outcome, methoxyflurane has a demonstrated ability to reduce pain with shorter procedural and recovery time and without influence on the procedural success. Despite existing incidence of drowsiness and dizziness, risk of high-grade AEs, kidney injury, and liver injury is low. Thus, the use of methoxyflurane in medical procedures may facilitate workflow and shorten waiting lists.
Decision-makers should be cognizant that the evidence collected in this report is sparce, as the available studies were few and have several limitations. Therefore, interpretation of the findings should be taken with caution.
References
1.Ikeda S. The reincarnation of methoxyflurane. J Anesth Hist. 2020;6(2):79-83. PubMed
2.Porter KM, Dayan AD, Dickerson S, Middleton PM. The role of inhaled methoxyflurane in acute pain management. Open Access Emerg Med. 2018;10:149-164. PubMed
3.Williams OD, Pluck G. The use of methoxyflurane (Penthrox) for procedural analgesia in the emergency department and pre-hospital environment. Trauma (United Kingdom). 2020;22(2):85-93.
4.Ferreira R, Zorn KC, Bhojani N, Chughtai B, Elterman DS. How I do it: Penthrox in urology. Can J Urol. 2023;30(1):11448-11452. PubMed
5.Paladin Pharma. 2024; https://www.paladin-pharma.com/. Accessed 2024 Jul 17.
6.Penthrox (methoxyflurane): 99.9% volatile liquid for inhalation. St-Laurent (QC): Paladin Labs Inc.; 2022 Apr 21: https://pdf.hres.ca/dpd_pm/00065552.PDF. Accessed 2024 Jul 17.
7.Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. PubMed
8.Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377-384. PubMed
9.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
10.Finkelstein S, Oliogu E, Yee A, et al. Literature review on the use of methoxyflurane in the management of pain in cancer-related procedures. Support Care Cancer. 2023;31(4):232. PubMed
11.Copping R, Balamon P, Lau M, Catt J, Schlaphoff G. MethOxyfluraNe in InTerventiOnal Radiology (MONITOR): a randomised controlled trial. J Med Imaging Radiat Oncol. 2024. PubMed
12.Nguyen NQ, Toscano L, Lawrence M, et al. Portable inhaled methoxyflurane is feasible and safe for colonoscopy in subjects with morbid obesity and/or obstructive sleep apnea. Endosc Int Open. 2015;3(5):E487-493. PubMed
13.Ho SF, Ganti S, Omar E, et al. Comparison of inhaled methoxyflurane versus procedural sedation for manipulation and reduction of acute shoulder and elbow dislocation in the emergency department. Proc Singap Healthc. 2022;31.
14.Umana E, Kelliher JH, Blom CJ, McNicholl B. Inhaled methoxyflurane for the reduction of acute anterior shoulder dislocation in the emergency department. CJEM. 2019;21(4):468-472. PubMed
15.Coffey F, Wright J, Hartshorn S, et al. STOP!: a randomised, double-blind, placebo-controlled study of the efficacy and safety of methoxyflurane for the treatment of acute pain. Emerg Med J. 2014;31(8):613-618. PubMed
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Note this appendix has not been copy-edited.
Table 2: Characteristics of Included Systematic Reviews
Study citation, country, funding source | Study design, outcomes | Intervention and comparators | Included studies | Population characteristics |
|---|---|---|---|---|
Finkelstein et al. (2023)10 Canada Funding source: NR | SR Outcomes:
| Intervention: Methoxyflurane Comparator:
| 7 studies, but only 3 fulfilled the criteria in Table 1 3 RCTs of patients who underwent cancer-related procedures:
| Colonoscopy Mean age (SD), years:
TRUSB Median age (IQR), years:
Bone marrow biopsy Mean age (SD), years:
|
AE = adverse event; IQR = interquartile range; NR = not reported; NRS = numerical rating scale; SD = standard deviation; SR = systematic review; TRUSB = transrectal ultrasonography-guided prostate biopsy; VAS = visual analogue scale; VRS = verbal rating scale.
Table 3: Characteristics of Included Primary Clinical Studies
Study citation, country, funding source | Study design | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Randomized controlled trials | ||||
Copping et al. (2024)11 Australia Funding source: The authors reported that no financial support was received for the study. | RCT, double-blind | Patients (N = 314) presenting for portacath insertion (55.4%), portacath removal (15.6%) or solid organ biopsy (29.0%) Mean age (SD), years:
| Intervention: Methoxyflurane (N = 169) Comparator: Placebo (N = 145) | Primary outcomes:
Secondary outcomes:
Follow-up: NA |
Observational studies | ||||
Ho et al. (2021)13 Singapore Funding source: The authors reported that no financial support was received for the study. | Retrospective health record review study | Patients (N = 192) presenting with either ASD (n = 153) or AED (n = 39) in the ED who underwent reduction with either methoxyflurane or PSA Mean age (SD), years:
| Intervention: Methoxyflurane (N = 74) Comparator: PSA (N = 118) PSA: midazolam (n = 39) or short-acting sedative agents (i.e., ketamine, propofol, ketofol) (n = 79) | Primary outcome:
Secondary outcomes:
|
Umana et al. (2019)14 Ireland Funding source: The authors reported that no grants have been awarded for this study. | Retrospective health record review study | Patients presenting with ASD in the ED who underwent reduction with either methoxyflurane or propofol Median age (IQR), years:
% male:
% female:
| Intervention: Methoxyflurane (N = 30) Comparator: Propofol (N = 52) | Primary outcome:
Secondary outcomes:
Follow-up: NA |
Nguyen et al. (2015)12 Australia Funding source: NR | Prospective cohort study | Patients with morbid obesity/OSA who were referred to colonoscopy unit. Mean age (SD), years:
Sedation (fentanyl and midazolam): 54.9 (1.1) | Intervention: Methoxyflurane (N = 85) Comparator: Sedation (N = 55) | Primary outcomes:
Secondary outcomes:
Follow-up: NA |
AE = adverse event; AED = acute elbow dislocation; ASD = acute shoulder dislocation; ED = emergency department; IQR = interquartile range; NA = not applicable; NR = not reported; OSA = obstructive sleep apnea; PSA = procedural sedation and analgesia; SD = standard deviation; VAS = visual analogue scale.
aDefined as time from procedure onset to the postreduction X-ray.
bDefined as the time until the caring nurses and physician deemed it to be “medically safe” for the patient to leave the endoscopy unit.
Appendix 3: Critical Appraisal of Included Publications
Note this appendix has not been copy-edited.
Table 4: Strengths and Limitations of Systematic Review Using AMSTAR 27
Strengths | Limitations |
|---|---|
Finkelstein et al. (2023)10 | |
The research question or objective and the inclusion criteria for the review clearly include the components of PICO. The review authors explained their selection of eligible study designs (i.e., any study design that included cancer-related procedures, and reported on efficacy of methoxyflurane for pain relief using empirical data). The literature search strategy was partially comprehensive (i.e., search at least 2 databases, provide keywords, and justified publication restrictions). The review authors performed study selection in duplicate. The characteristics of the included studies were described in adequate details, including study design, intervention, control, and outcomes. The review authors declared that they had no conflicts of interest related to this work. | There was no explicit statement that the review methods were established before the conduct of the review. The review authors did not report whether data extraction was performed in duplicate. The methodological quality of the included studies was not assessed. Patient characteristics were not adequately described. A list of excluded studies and the reasons for exclusion were not provided. Therefore, it was not possible to assess whether any relevant articles were excluded and if so, for what reasons. The review authors did not report the sources of funding for the included studies. Knowing the funding sources could determine the degree of confidence in the findings. |
AMSTAR 2 = A MeaSurement Tool to Assess systematic Reviews 2; PICO = population, intervention, comparator, and outcome.
Table 5: Strengths and Limitations of Clinical Studies Using the Downs and Black Checklist8
Strengths | Limitations |
|---|---|
Copping et al. (2024)11 | |
Reporting:
External validity:
Internal validity – bias:
Internal validity – confounding:
| External validity:
|
Ho et al. (2021)13 | |
Reporting:
External validity:
Internal validity – bias:
Internal validity – confounding:
| Reporting:
External validity:
Internal validity – bias:
Internal validity – confounding:
|
Umana et al. (2019)14 | |
Reporting:
External validity:
Internal validity – bias:
Internal validity – confounding:
| External validity:
Internal validity – bias:
Internal validity – confounding:
|
Nguyen et al. (2015)12 | |
Reporting:
External validity:
Internal validity – bias:
Internal validity – confounding:
| External validity:
Internal validity – bias:
|
RCT = randomized controlled trial.
Appendix 4: Main Study Findings
Note this appendix has not been copy-edited.
Table 6: Summary of Findings by Procedures — Colonoscopy
Study citation and study design | Outcomes and method of measurement | Results | Notes |
|---|---|---|---|
Finkelstein et al. (2023)10 SR Included study: RCT, nonblinded Methoxyflurane (N = 125) vs. sedation (N = 126) | Pain VAS (0 to 100) | There were no statistically significant differences in VAS pain scores before, during, and after colonoscopy between patients who received methoxyflurane and IV sedation. | The results were presented in a graphical format. |
Anxiety STAI-Y anxiety scorea | Total score:
Nervousness subscore:
| Although the total STAI-Y anxiety scores were higher in the methoxyflurane group, the nervousness subscores were similar between groups. | |
Procedural performance |
| There were no differences between groups in procedural preparation time, cecal arrival time, total colonoscopy time, success rate of complete colonoscopy, and rate of polyp detection and polypectomy. | |
AEs |
| The rates of AEs were similar between groups. | |
Colonoscopist perception |
| There were no differences in various outcomes between groups from colonoscopist perception. | |
Patient perception on the use of methoxyflurane for colonoscopy VAS (0 to 100; 0 = don’t like it at all; 100 = like it very much) |
| Of patients who had successful colonoscopy with methoxyflurane, 97% were willing to use methoxyflurane again for future colonoscopy. | |
Recovery and discharge time |
| Patients receiving methoxyflurane had no desaturation, awoke quicker, and ready for discharge earlier than those receiving IV sedation. | |
Nguyen et al. (2015)12 RCT, nonblinded Methoxyflurane (N = 85) vs. sedation (N = 55) Patients with obesity and/or obstructive sleep apnea | Pain VAS (0 to 10) |
| The pain was perceived as tolerable and short-lasting. |
Anxiety STAI-Y anxiety scorea |
| There were no differences in total anxiety score, nervousness subscore between groups. | |
Procedural performance |
| The in-room preparation time, cecal arrival time, total colonoscopy time, and the total in-room time were statistically significantly shorter in the methoxyflurane group than in the sedation group. | |
AEs |
| There are more intraprocedural events of respiratory depression, hypotension, and tachycardia in the sedation group compared to the methoxyflurane group. | |
Patient perception on the use of methoxyflurane for colonoscopy |
| Although satisfaction scores were not different between groups, more patients in the methoxyflurane group prefer the drug. | |
Recovery and discharge time | Patients who received methoxyflurane had statistically significantly shorter (P < 0.001):
than those who received sedation.
| The results were presented graphically. Patients who had methoxyflurane were ready to be discharged at least 60 minute earlier than those who had sedation. |
AE = adverse event; min = minute; NS = not statistically significant; RCT = randomized controlled trial; SR = systematic review; STAI-Y = Speiberger State-Trait Anxiety Inventory Form Y; VAS = visual analogue scale.
aThe STAI-Y varies from a minimum score of 20 to a maximum score of 80. The STAI-Y scores are classified as follows: 20 to 37 for “no or low anxiety,” 38 to 44 for “moderate anxiety,” and 45 to 80 for “high anxiety.”
Table 7: Summary of Findings by Procedures — Transrectal Ultrasonography-Guided Prostate Biopsy (TRUSB)
Study citation and study design | Outcomes and method of measurement | Results | Notes |
|---|---|---|---|
Finkelstein et al. (2023)10 SR Included study: RCT, double-blind Methoxyflurane (N = 209) vs. placebo (N = 211) All patients received periprostatic infiltration of local anesthesia | Pain NRS (0 to 10) | PETB questionnaire scores (0 to 10; 0 = no trouble at all; 10 = worst I can imagine)
PETB questionnaire scores assessed by urologist
| Pain is not the only relevant outcome. |
Discomfort NRS (0 to 10) | PETB questionnaire scores (0 to 10; 0 = no trouble at all; 10 = worst I can imagine)
PETB questionnaire scores assessed by urologist
| Methoxyflurane was associated with better scores for discomfort. | |
Drowsiness NRS (0 to 10) | PETB questionnaire scores (0 to 10; 0 = no trouble at all; 10 = worst I can imagine)
PETB questionnaire scores assessed by urologist
| Methoxyflurane resulted with higher scores for drowsiness. | |
Dizziness NRS (0 to 10) | PETB questionnaire scores (0 to 10; 0 = no trouble at all; 10 = worst I can imagine)
PETB questionnaire scores assessed by urologist
| Methoxyflurane resulted with higher scores for dizziness. | |
Patient perception on the use of methoxyflurane for biopsy | Willingness to undergo repeat biopsy:
Overall experience (PETB scores):
| Recall bias might occur after 7 to 35 days. | |
Biopsy completion rate | 99% vs. 99%; P = 1 | There was no difference between groups. | |
AEs | Dizziness: 51% vs. 30%; P < 0.001 Somnolence: 44% vs. 26%; P < 0.001 Grade 3 or higher: 2.6% vs. 4.1%; P = 0.4 Hospitalizations within 30 days: 2.1% vs. 4.1%; NS Intensive care unit admissions or death: 0 | There were no statistically significant differences in the number of grade 3 or higher AEs, or 30-day hospitalization rate between groups. |
AE = adverse event; NRS = numeric rating scale; NS = not statistically significant difference; PETB = patient’s experience of transrectal ultrasonography-guided prostate biopsy; RCT = randomized controlled trial; SR = systematic review.
Table 8: Summary of Findings by Procedures — Bone Marrow Biopsy
Study citation and study design | Outcomes and method of measurement | Results | Notes |
|---|---|---|---|
Finkelstein et al. (2023)10 SR Included study: RCT, double-blind Methoxyflurane (N = 49) vs. placebo (N = 48) | Pain NRS (0 to 10; 0 = no pain; 10 = worst possible pain) | Reduction in pain
| Methoxyflurane was associated with a reduction in pain during the procedure compared to placebo. The difference of 1.08 was not clinically relevant. |
Patient perception on the use of methoxyflurane for biopsy | Rated medication as very good or excellent: 49% vs. 16.5%; P = 0.005 | Significantly higher number of patients in the methoxyflurane group rated medication as very good or excellent compared to placebo. | |
AEs | AEs (grade 1) 30 to 45 minute after procedure: 20.4% vs. 4.2%; P = 0.028
| Methoxyflurane was associated with dizziness and euphoria. |
AE = adverse event; CI = confidence interval; min = minute; NRS = numerical rating scale; RCT = randomized controlled trial; SR = systematic review.
Table 9: Summary of Findings by Procedures — Reduction of Acute Shoulder and Elbow Dislocation in the Emergency Department
Study citation and Study design | Outcomes and method of measurement | Results | Notes |
|---|---|---|---|
Ho et al. (2022)13 Retrospective chart review study Methoxyflurane (N = 74) vs. sedation (N = 118) Patients with ASD and AED | Length of stay |
| Methoxyflurane was associated with shorter patient length of stay, and shorter duration of procedure compared to procedural sedation and analgesia. |
Procedural performance |
| ||
Umana et al. (2019)14 Retrospective chart review study Methoxyflurane (N = 30) vs. propofol (N = 52) Patients with ASD | Length of stay |
| Methoxyflurane was associated with shorter length of stay in the ED and recovery time compared to procedural sedation, without affecting the success rate. |
Procedural performance |
|
AED = acute elbow dislocation; AED = acute elbow dislocation; ASD = acute shoulder dislocation; ED = emergency department; IQR = interquartile range; min = minute; SD = standard deviation.
Table 10: Summary of Findings by Procedures — Other Minor Procedures
Study citation and Study design | Outcomes and method of measurement | Results | Notes |
|---|---|---|---|
Copping et al. (2024)11 RCT, double-blind Methoxyflurane (N = 169) vs. placebo (N = 145) Patients presenting for portacath insertion (55.4%), portacath removal (15.6%) or solid organ biopsy (29.0%) | Pain VAS (0 to 10) |
| Methoxyflurane group had lower pain and anxiety scores throughout the procedure. |
Anxiety VAS (0 to 10) |
| ||
Proceduralist perspectives Questionnaires |
| Proceduralist perspectives on various outcomes were in favour of methoxyflurane over placebo. | |
AEs |
| There were no drug-related or procedure-related AEs. |
AE = adverse event; CI = confidence interval; RCT = randomized controlled trial; VAS = visual analogue scale.
Appendix 5: References of Potential Interest
Note this appendix has not been copy-edited.
Single-arm Studies
Locke JA, Neu S, Lawrence J, Herschorn S. Pilot study to assess the feasibility of self-administered, low-dose methoxyflurane for cystoscopic procedures. Can Urol Assoc J. 2024 Apr 2. doi: 10.5489/cuaj.8676. Online ahead of print..PubMed
Ekansh Debuka, Patrick Birkenhead, Sohan Shah et al. Penthrox® (Methoxyflurane) as an Analgesic for Removal of Circular External Fixators and Minor Procedures during the COVID-19 Pandemic. Strategies Trauma Limb Reconstr. 2023 May-Aug;18(2):82-86. PubMed
Alexandra J Stewart, Ciarna Brooker, Gemma Vose et al. Pain and symptom relief using inhaled methoxyflurane for gynecologic brachytherapy applicator removal. J Contemp Brachytherapy. 2023 Feb;15(1):37-42. PubMed
Ceb Gray Stephens, A Dias, E Skinner et al. Penthrox enables quicker management of fractures, dislocations and more: learning lessons from expedited care of trauma patients during the COVID-19 pandemic. Ann R Coll Surg Engl. 2023 Aug;105(S2):S22-S27. PubMed
A L Gaskell, C G Jephcott, J R Smithells, J W Sleigh. Self-administered methoxyflurane for procedural analgesia: experience in a tertiary Australasian centre. Anesthesia. 2016 Apr;71(4):417-23. PubMed
Jamil S Anwari, Laith Khalil, Abdullah S Terkawi. Efficacy of the methoxyflurane as bridging analgesia during epidural placement in laboring parturient. Saudi J Anaesth. 2015 Oct-Dec;9(4):370-5. PubMed
Chanyang Lee, Henry H Woo. Penthrox inhaler analgesia in transrectal ultrasound-guided prostate biopsy. ANZ J Surg. 2015 Jun;85(6):433-7. PubMed
Wasiak J, Mahar PD, Paul E, et al. Inhaled methoxyflurane for pain and anxiety relief during burn wound care procedures: an Australian case series. Int Wound J. 2014 Feb;11(1):74-8. PubMed
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up to date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for noncommercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca