CADTH Health Technology Review
Re-Treatment With Immune Checkpoint Inhibitors
Rapid Review
Abbreviations
cHL
classical Hodgkin lymphoma
CSCC
cutaneous squamous cell carcinoma
ICI
immune checkpoint inhibitor
NSCLC
non–small cell lung cancer
Key Messages
We did not find any evidence regarding the clinical effectiveness and safety of second re-treatment with pembrolizumab for non–small cell lung cancer, classical Hodgkin lymphoma, and advanced melanoma.
We did not find any evidence regarding the clinical effectiveness and safety of second re-treatment with cemiplimab for cutaneous squamous cell carcinoma.
We did not find any evidence-based guidelines regarding the second re-treatment with immune checkpoint inhibitors for non–small cell lung cancer, classical Hodgkin lymphoma, advanced melanoma, and cutaneous squamous cell carcinoma.
Context and Policy Issues
What Are Immune Checkpoint Inhibitors?
Immune checkpoint inhibitors (ICIs) are a type of immunotherapy using monoclonal antibodies to treat cancer.1 The immune system cells, such as T-cells, have protein receptors on cell surface called immune checkpoints that help keep the immune responses in check, preventing autoimmune diseases.1 Some cancer cells evade destruction from the immune system by triggering the expression of immune checkpoints, thus stopping the immune system from attacking cancer cells.1 By blocking these checkpoints, ICIs reactivate and boost the T-cell mediated immune response against cancer cells and destroy them.1
Seven ICIs have been approved by Health Canada for immune therapy of various cancer types.1 They are grouped into 3 main types of ICIs and named after the checkpoint proteins such as anti–PD-1 (pembrolizumab, nivolumab, cemiplimab), anti–PD-L1 (atezolizumab, avelumab, durvalumab), and anti–CTLA-4 (ipilimumab).1 This report focuses on 2 anti–PD-1 antibodies, pembrolizumab and cemiplimab.
Pembrolizumab, marketed as Keytruda, has been approved without conditions by Health Canada for the treatment of various types of cancer including advanced melanoma, non–small cell lung cancer (NSCLC), lung cancer, renal cell carcinoma, advanced colorectal cancer, endometrial carcinoma, head and neck squamous cell carcinoma, stomach cancer, breast cancer, cervical cancer, and gallbladder cancer.2 Pembrolizumab has also been approved with conditions to treat classical Hodgkin lymphoma (cHL), mediastinal B-cell lymphoma, and urothelial carcinoma.2
Cemiplimab, marketed as Libtayo, has been initially approved by Health Canada to treat advanced cutaneous squamous cell carcinoma (CSCC), and now is extended to treat other cancers including NSCLC, basal cell carcinoma, and cervical cancer.3
What Is the Current Practice?
The recommended dose of pembrolizumab is 200 mg or 400 mg in adults, or 2 mg/kg (up to a maximum of 200 mg) in children (12 years and older), given intravenously for about 30 minutes every 3 weeks or every 6 weeks.2 The recommended dose of cemiplimab is 350 mg every 3 weeks administered as an IV infusion over 30 minutes.3 These ICIs can be given to patients for a fixed duration or until progression. For instance, several pivotal trials on immunotherapy of NSCLC have shown that a maximum 35 cycles or 2 years of treatment with pembrolizumab demonstrated significant survival benefits.4 Similarly, Phase I and II clinical trials and real-world observational studies have demonstrated that cemiplimab is effective, safe, and well-tolerated in most patients with CSCC, when given up to 96 weeks.5,6
Despite the improvements in early-stage treatments, a large proportion of patients may show relapse while off therapy or disease progression over time even with continued treatment.7 The incidence of disease progression after ICI treatment varies from 10% to 70%, depending on the disease.8 Subsequent treatment options, so called re-treatment or rechallenge with the same or another ICI, seems to be a suitable treatment option for patients who have disease progression after the first course of therapy with ICIs. Recent evidence from pivotal trials has shown that re-treatment with ICIs in solid tumours exhibits encouraging efficacy and acceptable safety.7,9 For instance, the KEYNOTE trials on NSCLC allowed an additional 1 year or 17 cycles of re-treatment with pembrolizumab after completing 35 cycles and experiencing disease progression.10 Based on the findings from those trials, reimbursement policies have been made for an additional 1 year (17 cycles) of re-treatment with pembrolizumab in all indications.11 Similar policies have been adopted for cemiplimab, with re-treatment funded for an additional 1 year (17 cycles) in patients who completed 2 years of cemiplimab treatment and subsequently progressed and patients who discontinued cemiplimab after less than 2 years due to complete response.12
Why Is It Important to Do This Review?
Patients who undergo their first re-treatment may relapse again after the authorized 1-year re-treatment. Decision-makers are wondering if those patients may benefit from a second re-treatment (i.e., a third round of therapy) with the same ICIs. Particularly, pembrolizumab has been used in patients with NSCLC, cHL, or melanoma, and cemiplimab has been used in patients with CSCC.
Objective
To support decision-making about the possibility of a second re-treatment with the same ICIs, we prepared this Rapid Review to summarize and critically appraise the available studies on the efficacy and safety of a second re-treatment with pembrolizumab for NSCLC, cHL, and advanced melanoma, and the efficacy and safety of a second re-treatment with cemiplimab for CSCC. This report also aims to review the evidence-based guideline recommendations on the second re-treatment with ICIs for NSCLC, cHL, advanced melanoma, and CSCC.
Research Questions
What is the clinical effectiveness and safety of a second re-treatment with pembrolizumab for NSCLC, cHL, and advanced melanoma?
What is the clinical effectiveness and safety of a second re-treatment with cemiplimab for CSCC?
What are the evidence-based guideline recommendations on the second re-treatment with ICIs for NSCLC, cHL, advanced melanoma, and CSCC?
Methods
Literature Search Methods
An information specialist conducted a literature search on key resources including MEDLINE, the Cochrane Database of Systematic Reviews, the International HTA Database, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search approach was customized to retrieve a limited set of results, balancing comprehensiveness with relevancy. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. Search concepts were developed based on the elements of the research questions and selection criteria. The main search concepts were pembrolizumab, cemiplimab, or ICIs; non–small cell lung cancer, classic Hodgkin lymphoma, melanoma, or CSCC; and re-treatment. No filters were applied to limit the retrieval by study type. An additional search for guidelines was conducted with the main search concepts non–small cell lung cancer, classic Hodgkin lymphoma, melanoma, or CSCC, and ICIs or re-treatment. Search filters were applied to limit retrieval to guidelines. The searches were completed on June 12, 2024, and limited to English-language documents.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
|---|---|
Population | Patients previously treated with pembrolizumab (RQ1) or cemiplimab (RQ2) in the advanced or metastatic setting, who then relapsed while off therapy, were treated with a second course of the same drug, and relapsed again RQ1: Patients with NSCLC, cHL, or melanoma RQ2: Patients with CSCC RQ3: Patients with NSCLC, cHL, melanoma, CSCC |
Subgroup | PD-L1 expression Prior response to ICI (complete, partial, stable disease) Prior targeted therapy for advanced disease Oncogenic driver mutation (e.g., BRAF, ALK, EGFR) |
Intervention | RQ1: Pembrolizumab RQ2: Cemiplimab RQ3: Pembrolizumab or cemiplimab |
Comparator | Any comparator or no comparator |
Outcomes | RQ1 to 2: Clinical effectiveness: ORR, PFS, OS, HRQoL; safety RQ3: Evidence-based guidelines on use of ICI after 2 successive relapses on the same drug |
Study designs | RQ1 to 2: SR, HTA, RCTs (phase II, III, IV), nonrandomized studies including single-arm trials RQ3: Evidence-based guidelines |
ALK = anaplastic lymphoma kinase; BRAF = v-raf murine sarcoma viral oncogene homologue B1; cHL = classical Hodgkin lymphoma; CSCC = cutaneous squamous cell carcinoma; EGFR = epidermal growth factor receptor; HRQoL = health-related quality of life; HTA = health technology assessment; ICI = immune checkpoint inhibitor; NSCLC = non–small cell lung cancer; ORR = objective response rate; OS = overall survival; PFS = progression-free survival; RCT = randomized controlled trial; RQ = research question; SR = systematic review.
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1.
Summary of Evidence
Quantity of Research Available
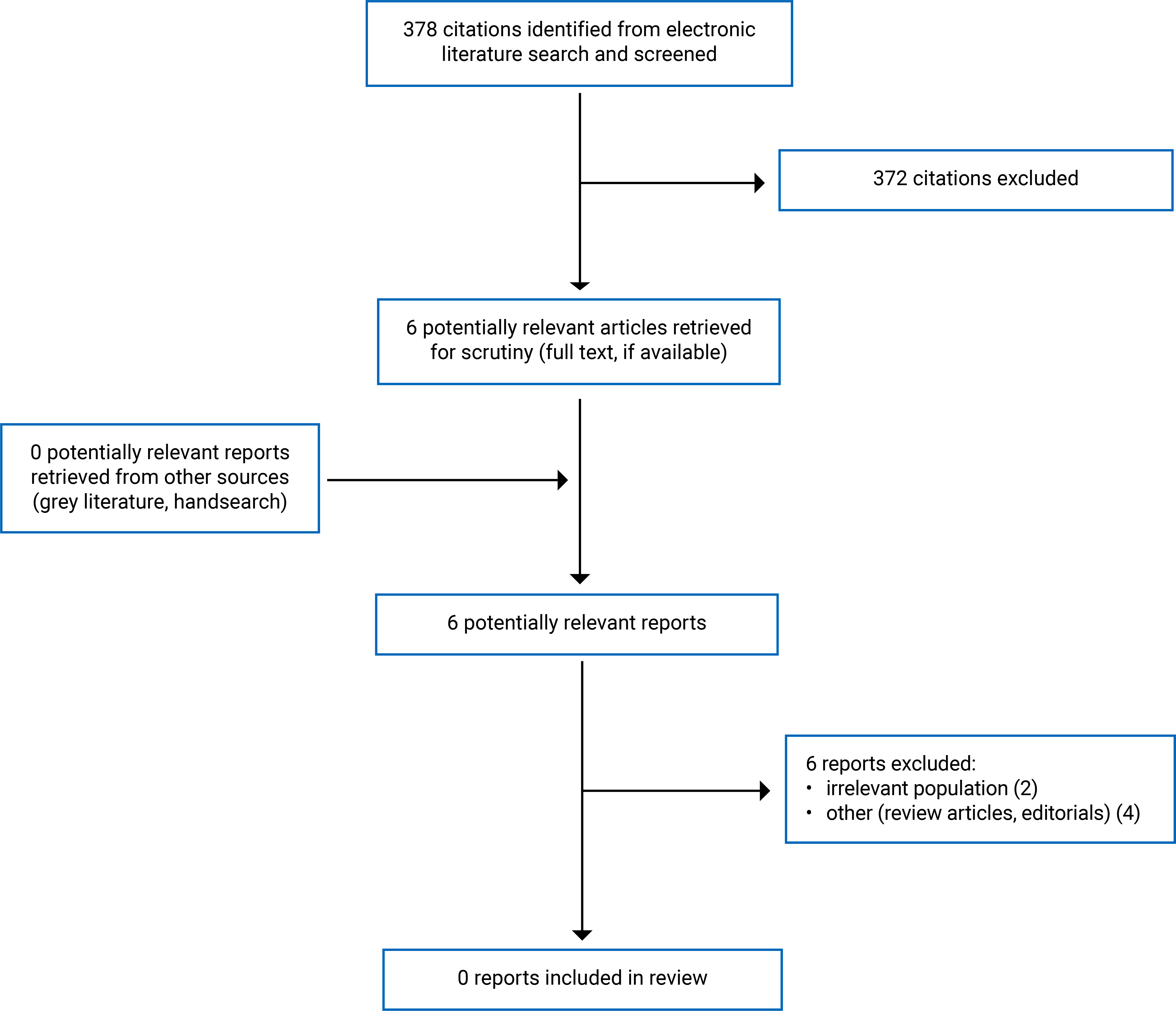
A total of 378 citations were identified in the literature search. Following screening of titles and abstracts, 372 citations were excluded and 6 potentially relevant reports from the electronic search were retrieved for full-text review. No potentially relevant publications were retrieved from the grey literature search for full-text review. None of these 6 potentially relevant articles met the inclusion criteria and they were excluded from this report for various reasons. Appendix 1 presents the PRISMA13 flow chart of the study selection.
Summary of Findings
We did not find any evidence regarding the clinical effectiveness and safety of second re-treatment with pembrolizumab for NSCLC, cHL, and advanced melanoma, or the clinical effectiveness and safety of second re-treatment with cemiplimab for CSCC. We also did not find any evidence-based guideline recommendations on the second re-treatment with ICIs for NSCLC, cHL, advanced melanoma, and CSCC.
Limitations
No evidence was identified for a relevant population that consists of patients previously treated with pembrolizumab or cemiplimab in the advanced or metastatic setting who then relapsed while off therapy, were treated with a second course of the same drug, then relapsed again.
Conclusions and Implications for Decision- or Policy-Making
No relevant literature was identified to answer the research questions; therefore, conclusions could not be provided regarding the clinical effectiveness and safety, or recommendations on, the second re-treatment with ICIs for NSCLC, cHL, advanced melanoma, and CSCC.
Recent prospective and retrospective clinical studies mostly evaluated the efficacy and safety of ICI re-treatment with the same or another ICIs for patients with solid tumours who had disease progression or relapse after the initial treatment with ICIs.7,9,10,14-16 We did not find any evidence about the second re-treatment with ICIs, particularly pembrolizumab or cemiplimab, if those patients relapse again. Future investigation on immunotherapy rechallenge is needed to evaluate whether a second re-treatment (i.e., a third round of therapy) with ICIs should be given for those patients.
References
1.Himmel ME, Saibil SD, Saltman AP. Immune checkpoint inhibitors in cancer immunotherapy. CMAJ. 2020;192(24):E651. PubMed
2.Keytruda (pembrolizumab): solution for infusion 100 mg/4 mL vial [product monograph]. Kirkland (QC): Merck Canada Inc.; 2024 Jun 20: https://www.merck.ca/en/wp-content/uploads/sites/20/2021/04/KEYTRUDA-CI_E.pdf. Accessed 2024 Jun 14.
3.Libtayo (cemiplimab for injection): 50 mg/mL solution for infusion [product monograph]. Mississauga (ON): Sanofi Genzyme, a division of sanofi-aventis Canada Inc.; 2023 Aug 15: https://pdf.hres.ca/dpd_pm/00072119.PDF. Accessed 2024 Jun 14.
4.Putzu C, Canova S, Paliogiannis P, et al. Duration of immunotherapy in non-small cell lung cancer survivors: a lifelong commitment? Cancers (Basel). 2023;15(3):689. PubMed
5.Mager L, Gardeen S, Carr DR, Shahwan KT. Cemiplimab for the treatment of advanced cutaneous squamous cell carcinoma: appropriate patient selection and perspectives. Clin Cosmet Investig Dermatol. 2023;16:2135-2142. PubMed
6.Potestio L, Scalvenzi M, Lallas A, et al. Efficacy and safety of cemiplimab for the management of non-melanoma skin cancer: a drug safety evaluation. Cancers (Basel). 2024;16(9):1732. PubMed
7.Yang K, Li J, Sun Z, Zhao L, Bai C. Retreatment with immune checkpoint inhibitors in solid tumors: a systematic review. Ther Adv Med Oncol. 2020;12:1758835920975353. PubMed
8.Schoenfeld AJ, Hellmann MD. Acquired resistance to immune checkpoint inhibitors. Cancer Cell. 2020;37(4):443-455. PubMed
9.Perdyan A, Sobocki BK, Balihodzic A, Dabrowska A, Kacperczyk J, Rutkowski J. The effectiveness of cancer immune checkpoint inhibitor retreatment and rechallenge-a systematic review. Cancers (Basel). 2023;15(13):3490. PubMed
10.Rossi S, Masini S, Finocchiaro G, Lorenzi E, Toschi L, Santoro A. Retreatment with immune checkpoint inhibitors in the new scenario of immunotherapy in non-small cell lung cancer. Cancers (Basel). 2024;16(9):1683. PubMed
11.Provincial Funding Summary - pembrolizumab (Keytruda) for non-small cell lung cancer (second line or beyond). Ottawa (ON): CADTH; 2020 Oct 29: https://www.cadth.ca/sites/default/files/pcodr/pcodr_provfund_pembrolizumab_keytruda_nsclc_2lnbeyond.pdf. Accessed 2024 Jun 14.
12.Drug Reimbursement Expert Review Committee final recommendation: Cemiplimab (Libtayo - Sanofi Genzyme, a division of Sanofi-Aventis Canada Inc.). Can J Health Technol. 2022;2(6). https://www.canjhealthtechnol.ca/index.php/cjht/article/view/pc0262/pc0262. Accessed 2024 Jul 03.
13.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
14.Feng Y, Tao Y, Chen H, et al. Efficacy and safety of immune checkpoint inhibitor rechallenge in non-small cell lung cancer: a systematic review and meta-analysis. Thorac Cancer. 2023;14(25):2536-2547. PubMed
15.Feng J, Chen X, Wei J, et al. Safety and efficacy of immune checkpoint inhibitor rechallenge in advanced non-small cell lung cancer: a retrospective study. Sci Rep. 2024;14(1):2315. PubMed
16.Livanou ME, Nikolaidou V, Skouras V, Fiste O, Kotteas E. Efficacy of NSCLC rechallenge with immune checkpoint inhibitors following disease progression or relapse. Cancers (Basel). 2024;16(6):1196. PubMed
Appendix 1: Selection of Included Studies
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up to date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for noncommercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca