CADTH Health Technology Review
Review of Guidelines on Clonidine for Various Indications
Rapid Review
Key Messages
What Is the Issue?
Clonidine is an antihypertensive medication that has been used for a range of health conditions including hypertension, substance use disorders, menopause, restless leg syndrome, migraines, attention-deficit/hyperactivity disorder (ADHD), and Tourette syndrome. The role of clonidine in the treatment of these health conditions is unclear.
What Did We Do?
To inform decisions around the use of clonidine in various health conditions, we sought to identify and summarize recommendations from evidence-based guidelines.
We searched key resources, including journal citation databases, and conducted a focused internet search for relevant evidence published since 2014. One reviewer screened articles for inclusion based on predefined criteria, critically appraised the included guidelines, and narratively summarized the findings.
What Did We Find?
We identified 12 evidence-based guidelines that included recommendations on the use of clonidine. We identified 1 guideline on hypertension, 4 guidelines on substance use disorders, 4 guidelines on menopause, 2 guidelines on restless leg syndrome, and 1 guideline on Tourette syndrome. We did not identify any evidence-based guidelines that included recommendations on the use of clonidine for the treatment of ADHD or migraine prophylaxis.
The included guidelines recommend clonidine for hypertension in pregnant women, management of opioid withdrawal and alcohol withdrawal, and Tourette syndrome.
The recommendations in the guidelines for menopause were mixed. Two guidelines do not recommend clonidine and 2 guidelines recommend clonidine for the treatment of vasomotor symptoms (i.e., hot flashes) of menopause.
One guideline does not recommend the use of clonidine for restless leg syndrome in people who are pregnant or lactating and 1 guideline states that there is insufficient evidence to support or refute the use of clonidine in restless leg syndrome.
What Does It Mean?
The use of clonidine is recommended for some health conditions and is not recommended for others. Due to the inconsistency in recommendations on the use of clonidine for the control of hot flashes in menopause, decision-makers may wish to consider other factors such as patient preferences and availability of other treatment options.
Future evidence-based guidelines that include recommendations on the use of clonidine for the prevention of migraines, treatment of ADHD and the treatment of hypertension in a broader population would help fill the gaps identified in this report.
Abbreviations
AAN
American Academy of Neurology
ADHD
attention-deficit/hyperactivity disorder
ASAM
American Society of Addiction Medicine
CRISM
Canadian Research Initiative in Substance Misuse
DoD
Department of Defense
IRLSSG
International Restless Legs Syndrome Study Group
NAMS
North American Menopause Society
NICE
National Institute of Health and Care Excellence
SOGC
Society of Obstetricians and Gynaecologists of Canada
VA
Veterans Affairs
Context and Policy Issues
What Are the Health Conditions Included in This Review?
Guidelines on hypertension, substance use disorders, menopause, restless leg syndrome, migraine prevention, ADHD, and Tourette syndrome were eligible for inclusion in this review. Hypertension (high blood pressure) is when the pressure in your arteries is consistently too high.1 Treatment can include lifestyle changes and medications (e.g., diuretics, angiotensin-converting enzyme inhibitors, angiotensin II receptor blockers, and calcium channel blockers).2 Substance use disorder is a condition in which there is a problematic pattern of substance use that causes distress or impairs day-to-day functioning.3 Treatment for substance use disorder can include detoxification, cognitive and behavioural therapies, and medications.3 Menopause is a time that marks the end of menstrual cycles and is diagnosed after a person has gone 12 months without a menstrual period.4 A potential symptom of menopause is hot flashes (also known as vasomotor symptoms) which are a sudden feeling of warmth that spreads over the body.5 Treatment for menopause can include hormonal (i.e., estrogen or estrogen and progesterone) and nonhormonal treatments (e.g., diet, exercise, medications).5
Restless leg syndrome is a condition which causes a strong urge to move the legs and usually occurs in the evening or at night when sitting or lying down.6 Treatment for restless leg syndrome can include at-home therapies (e.g., exercise, warm baths, stress reduction) or medications (e.g., iron supplements, antiseizure medications, dopamine agonists, benzodiazepines, opioids).7 A migraine is a headache that can cause severe throbbing pain or a pulsing sensation and is often accompanied by nausea, vomiting, and extreme sensitivity to light and sound.8 Medications aimed at preventing migraines can include blood-pressure lowering medications, antidepressants, antiseizure drugs, and calcitonin gene-related peptides monoclonal antibodies.9 ADHD is a mental health disorder that include symptoms such as difficulty paying attention, hyperactivity, and impulsive behaviour.10 Treatment for ADHD includes medication (stimulants and other medications), education, skills training, and psychological counselling.11 Tourette syndrome is a neurologic disorder that may cause sudden unwanted and uncontrolled repetitive movements or vocal sounds called tics.12 Treatment for Tourette syndrome can include behavioural treatments, psychotherapy, and medications (e.g., dopamine blocking agents, alpha-adrenergic agonists, stimulants, antidepressants).12
What Is Clonidine?
Clonidine is an alpha-2 adrenergic agonist that has antihypertensive (blood pressure lowering) effects.13 Clonidine lowers blood pressure by relaxing the arteries and increasing the blood supply to the heart.13 Common side effects of clonidine may include abdominal pain, headache, hypotension, fatigue, nausea, constipation, dry mouth, sexual dysfunction, dizziness, and sedation.13 There is also potential for rebound hypertension and withdrawal symptoms if clonidine is discontinued abruptly.13 Clonidine is indicated for the treatment of hypertension and should normally be used in patients in whom treatment with a diuretic or beta-blocker was ineffective or associated with unacceptable adverse effects.14 Clonidine is available as tablets for oral administration and the initial dose is 0.1 mg twice daily.14 After 2 to 4 weeks, further increments of 0.1 mg per day may be added until the desired response is achieved.14 The common therapeutic dose ranges from 0.2 mg to 0.6 mg per day.14 When discontinuing clonidine, the dosage should be reduced gradually.14
Why Is It Important to Do This Review?
In addition to its use in hypertension, clonidine has also been used for a range of other health conditions including ADHD, Tourette syndrome, managing withdrawal from opioids, benzodiazepines, and alcohol, restless leg syndrome, migraine prophylaxis, and control of hot flashes in menopause.13 A review of guidelines of clonidine can help decision-making around which indications clonidine should be used for as well as provide guidance on potential dosing and safety considerations.
Objective
The purpose of this report is to summarize and critically appraise evidence-based guidelines regarding the use of clonidine for hypertension, substance use disorders, control of hot flashes in menopause, restless leg syndrome, migraine prophylaxis, ADHD, and Tourette syndrome.
Research Questions
What are the evidence-based guidelines regarding the use of clonidine in adults with hypertension?
What are the evidence-based guidelines regarding the use of clonidine in adults with substance use disorders (i.e., opioids, benzodiazepines, alcohol)?
What are the evidence-based guidelines regarding the use of clonidine for the control of hot flashes in adults with menopause?
What are the evidence-based guidelines regarding the use of clonidine in adults with restless leg syndrome?
What are the evidence-based guidelines regarding the use of clonidine for prevention of migraines in adults?
What are the evidence-based guidelines regarding the use of clonidine in adults with ADHD?
What are the evidence-based guidelines regarding the use of clonidine in adults with Tourette syndrome?
Methods
Literature Search Methods
An information specialist conducted a literature search on key resources including MEDLINE, Embase, PsycInfo, the Cochrane Database of Systematic Reviews, the International HTA Database, the websites of major international health technology agencies, and those in Canada, as well as a focused internet search. The search approach was customized to retrieve a limited set of results, balancing comprehensiveness with relevancy. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. Search concepts were developed based on the elements of the research questions and selection criteria. The main search concept was clonidine. Search filters were applied to limit retrieval to guidelines. Conference reviews and conference abstracts were excluded. The search was completed on June 12, 2024 and limited to English-language documents published since January 1, 2014.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
|---|---|
Population | Adults with hypertension, opioid use disorder, alcohol withdrawal, benzodiazepine withdrawal, menopause, restless leg syndrome, migraines, ADHD, or Tourette syndrome. |
Intervention | Clonidine |
Comparator | Not applicable |
Outcomes | Guidelines regarding the use of clonidine for the treatment of adults with hypertension, opioid use disorder, alcohol withdrawal, benzodiazepine withdrawal, menopause, restless leg syndrome, migraines, ADHD, or Tourette's syndrome (e.g., recommendations regarding appropriate use, dose, and duration of use). |
Study designs | Evidence-based guidelines. |
ADHD = attention-deficit/hyperactivity disorder.
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, they were duplicate publications, or were published before 2014. Guidelines with unclear methodology were also excluded.
Critical Appraisal of Individual Studies
The included guidelines were critically appraised by 1 reviewer using the Appraisal of Guidelines for Research and Evaluation (AGREE) II instrument15 as a guide.
Summary of Evidence
Quantity of Research Available
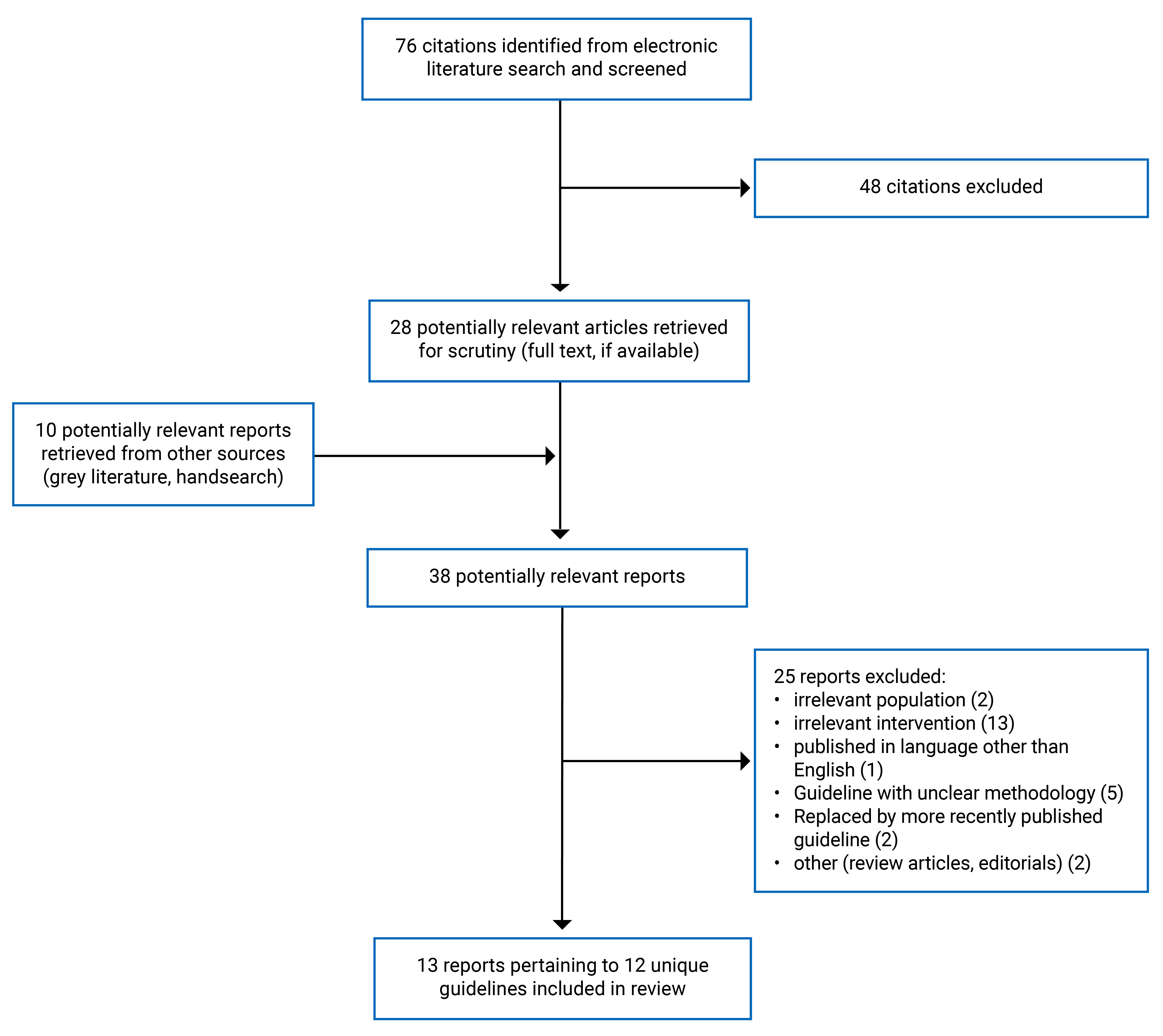
A total of 76 citations were identified in the literature search. Following screening of titles and abstracts, 48 citations were excluded and 28 potentially relevant reports from the electronic search were retrieved for full-text review. Ten potentially relevant publications were retrieved from the grey literature search for full-text review. Of these potentially relevant articles, 25 publications were excluded for various reasons, and 13 publications met the inclusion criteria and were included in this report. These comprised 13 reports pertaining to 12 unique evidence-based guidelines. Appendix 1 presents the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA)16 flow chart of the study selection.
Additional references of potential interest are provided in Appendix 2.
Summary of Guideline Characteristics
This report included 12 evidence-based guidelines17-28 that included recommendations regarding the use of clonidine for various indications.
The Hypertension Canada (2020)17 guideline included recommendations on hypertension. The Canadian Research Initiative in Substance Misuse (CRISM) (2023),18 Veterans Affairs (VA)/Department of Defense (DoD) (2021),19 American Society of Addiction Medicine (ASAM) (2020),20 and Commonwealth of Australia (2014)21 guidelines included recommendations on substance use disorder. The North American Menopause Society (NAMS) (2023),22 Society of Obstetricians and Gynaecologists of Canada (SOGC) (2021),23 National Institute for Health and Care Excellence (NICE) (2019),24 and Endocrine Society (2015)25 guidelines included recommendations on menopause. The American Academy of Neurology (AAN) (2016)26 and International Restless Legs Syndrome Study Group (IRLSSG) (2015)27 guidelines included recommendations on restless leg syndrome. The AAN (2019)28 guideline included recommendations on Tourette syndrome. Two of the guidelines on substance use disorder included recommendations on the management of opioid withdrawal (VA/DoD [2021]19 and Commonwealth of Australia [2014]21) and 2 of the guidelines included recommendations on alcohol withdrawal (CRISM [2023]18 and ASAM [2020]20). We did not identify any evidence-based guidelines that included recommendations on the use of clonidine for the prevention of migraines or treatment of ADHD that met our inclusion criteria.
The guideline development groups were from Canada,17,18,23 the US,19,20 Australia,21 the UK,24 North America,22 or were international.25-28
Additional details regarding the characteristics of included guidelines are provided in Appendix 3.
Summary of Critical Appraisal
All the included guidelines had clear objectives, guideline questions, and target populations. Only 3 of the guidelines18,19,24 specifically sought the views and preferences of the target populations and 1 of the guidelines20 posted the recommendations for public feedback. Therefore, the recommendations in some of the guidelines may not adequately reflect the values and preferences of patients. Systematic methods were used to search for evidence in 7 of the included guidelines.18-20,24-26,28 In 4 of the guidelines,17,21-23 they state that literature searches were conducted, however, limited details on the search (e.g., databases searched, time frame, screening methods, and so forth.) were provided. The IRLSSG (2015)27 guideline only performed a search in a single database and therefore relevant evidence may have been missed due to lack of a comprehensive search strategy.
There was an explicit link between the recommendations and supporting evidence in 9 of the guidelines.17-19,22,24-28 The SOGC (2021)23 and ASAM (2020)20 guidelines did not include discussion of the evidence that supports the recommendations. The Commonwealth of Australia (2014)21 guideline stated that the approach of using clonidine and other medications to control symptoms of opioid withdrawal is well supported by evidence, however, do not include a description of this evidence. Providing clear descriptions of the evidence used to inform the recommendations increases transparency in the recommendation development process.
The competing interests of the guideline development group were disclosed in all the guidelines. The SOGC (2021)23 and ASAM (2020)20 guidelines did not include statements about any funding received for the development of the guideline.
Additional details regarding the strengths and limitations of included guidelines are provided in Appendix 4.
Summary of Findings
An overview of the recommendations and supporting evidence regarding the use of clonidine for the health conditions covered in the included guidelines is provided in Table 2.
Appendix 5 presents the recommendation in the included guidelines.
Table 2: Overview of Included Guidelines
Guideline (Year) | Target Population | Recommendation(s) Strength of Recommendation(s) | Supporting Evidence Quality of Evidence | Possible Side Effects | Dosing |
|---|---|---|---|---|---|
Hypertension | |||||
Hypertension Canada (2020)17 | Adults and children at risk of or with hypertension | Clonidine can be considered as a second-line drug for antihypertensive therapy for pregnant women with chronic hypertension, gestational hypertension, or preeclampsia (SBP measurements of 140 mm Hg or DBP measurements of 90 mm Hg). Grade D | Based on expert opinion alone. | NR | NR |
Substance Use Disorders | |||||
CRISM (2023)18 | High-risk drinking and alcohol use disorder in youth (aged 11 to 25 years) and adults | Clinicians should consider offering clonidine for withdrawal management in an outpatient setting (e.g., primary care, virtual) for patients at low risk of severe complications of alcohol withdrawal (e.g., PAWSS < 4). Strong | 2 RCTs that reported clonidine is as effective as chlordiazepoxide in the management of mild to moderate withdrawal symptoms with better control of sympathetic symptoms and reductions in patient anxiety. Low | Hypotension, dry mouth, dizziness, fatigue, headache, nausea, vomiting, constipation, malaise, sleep disorder, sedation, and erectile dysfunction. | Starting dose: 0.1 to 0.2 mg BID Titration: Add 0.2 mg OD PRN Final dose: 0.1 mg to 0.6 mg BID |
VA/DoD (2021)19 | Adults with a diagnosis of substance use disorder | Clonidine is suggested as a second-line drug for opioid withdrawal management for patients with opioid use disorder when methadone and buprenorphine are contraindicated, unacceptable, or unavailable. Weak | 1 SR that included comparisons of alpha2-adrenergic agonists vs. placebo, methadone, or another alpha2-adrenergic agonist. 1 SR that included comparisons of buprenorphine vs clonidine, lofexidine, or methadone. The work group considered that the benefits of improved withdrawal symptoms outweighed potential harms, and that patient values and preferences varied somewhat. Low | Hypotension | NR |
ASAM (2020)20 | Adults with a diagnosis of alcohol withdrawal | Clonidine can be used to control autonomic hyperactivity and anxiety when symptoms are not controlled by benzodiazepines alone. Clonidine should not be used alone to prevent or treat withdrawal-related seizures or delirium. Recommendation strength NR | NR | NR | NR |
Commonwealth of Australia (2014)21 | People who are opioid dependent | 2 approaches are recommended for management of opioid withdrawal: 1. Abrupt cessation of opioid use and relief of symptoms using non-opioid drugs (e.g., benzodiazepines, nonsteroidal anti-inflammatory drugs, antiemetics, clonidine, antispasmodic drugs). 2.Short course of reducing doses of buprenorphine. Recommendation strength NR | The guideline authors state that both approaches are well supported by evidence, however, the use of buprenorphine to manage withdrawal is associated with significantly better relief of withdrawal than clonidine and supplementary medications (1 SR). 4 stars (body of evidence can be trusted to guide practice) | Hypotension | Test dose: 150 mcg to check for hypotensive effects. Treatment dose: 12 to 15 mcg/ kg/day in 4 divided doses. Doses are tapered and then ceased 7 to 10 days after cessation of opioids. |
Menopause | |||||
NAMS (2023)22 | People experiencing menopause | Clonidine is not recommended for the treatment of vasomotor symptoms of menopause. Recommendation strength NR | 1 SR that reported that clonidine is modestly more beneficial than placebo at reducing vasomotor symptoms. 2 SRs that reported that clonidine is less beneficial than SSRIs, SNRIs, and gabapentin at reducing vasomotor symptoms. Levels 1 to 3 (good and consistent scientific evidence, limited or inconsistent scientific evidence, and consensus and expert opinion). | Hypotension, lightheadedness, headache, dry mouth, dizziness, sedation, and constipation. Sudden cessation can lead to significant increases in blood pressure. | NR |
SOGC (2021)23 | Perimenopausal and postmenopausal women | Clonidine is a nonhormonal option for refractory vasomotor symptoms. Conditional | Supporting evidence NR. Moderate | NR | NR |
NICE (2019)24 | Menopausal women and women with premature ovarian insufficiency | 1. Give information to menopausal women and their family about nonhormonal treatments (e.g., clonidine) for menopausal symptoms Recommendation Strength NR 2. Do not routinely offer clonidine as first-line treatment for vasomotor symptoms alone. Strong | Clonidine was not included in the NMA conducted for the guideline due to the way outcomes were reported in studies of clonidine. Therefore, the relative effectiveness of clonidine in relieving short-term symptoms for women in menopause could not be estimated. Evidence quality NR | NR | NR |
Endocrine Society (2015)25 | Menopausal and postmenopausal women | A trial of clonidine is suggested for women seeking relief of moderate to severe vasomotor symptoms who do not respond to or are intolerant of SSRIs/SNRIs, gabapentin, or pregabalin. Weak | Several RCTs that demonstrated that clonidine reduces hot flashes but is less effective than SSRI/SNRIs, gabapentin, and pregabalin, and is associated with more side effects. Low | Lightheadedness, hypotension, headache, and constipation. Sudden cessation can be associated with significant increases in blood pressure. | NR |
Restless Leg Syndrome | |||||
AAN (2016)26 | Adults with restless leg syndrome | There is insufficient evidence to support or refute the use of clonidine for the treatment of restless leg syndrome. Level U (insufficient evidence) | 1 crossover trial of clonidine vs placebo in which patients reported less paresthesia, motor restlessness, and daytime fatigue during the clonidine treatment arm. There was no difference in periodic limb movement index between groups. Class III (low quality) | Hypotension, decreased cognition, dry mouth, and sleepiness. | NR |
IRLSSG (2015)27 | People with restless leg syndrome who are pregnant or lactating | Clonidine should probably not be considered for people with restless leg syndrome who are pregnant or lactating. Level 4 (evidence for risk/ ineffectiveness) | A small RCT found limited efficacy of clonidine for restless leg syndrome. Clonidine passes on to breast milk. Evidence quality NR | NR | NR |
Tourette Syndrome | |||||
AAN (2019)28 | Children and adults with Tourette syndrome or a chronic tic disorder | 1. Physicians should counsel individuals with tics and ADHD that alpha2 adrenergic agonists (e.g., clonidine) may provide benefit for both conditions Level B (moderate) 2. Alpha2 adrenergic agonists should be prescribed for the treatment of tics when the benefits outweigh the risks Level B (moderate) 3. Physicians must counsel patients on the common side effects of alpha2 adrenergic agonists, including sedation. Level A (strong) 4. Heart rate and blood pressure must be monitored in patients with tics treated with alpha2 adrenergic agonists. Level A (strong) 5. Alpha2 adrenergic agonists must be gradually tapered to avoid rebound hypertension. Level A (strong) | 1. One study reported reduced tic severity in children with tics and a comorbid diagnosis of ADHD who received clonidine plus methylphenidate vs placebo. Class I (highest quality) 2. Three studies reported reduced tic severity in people with tics receiving clonidine vs placebo. Class I and II 3. Two studies reported that sedation was more common in people with tics receiving clonidine vs placebo. 1 SR of alpha2 adrenergic agonists for ADHD in children and adolescents demonstrated hypotension, bradycardia, and sedation with these agents. Class I and II 4. One SR of alpha2 adrenergic agonists for ADHD in children and adolescents demonstrated hypotension, and bradycardia with these agents Evidence quality NR 5. NR | Hypotension, bradycardia, and sedation. Abrupt cessation of alpha2 adrenergic agonists may cause rebound hypertension. | NR |
AAN = American Academy of Neurology; ADHD = attention-deficit/hyperactivity disorder; ASAM = American Society of Addiction Medicine; BID = twice a day; CRISM = Canadian Research Initiative in Substance Misuse; DoD = Department of Defense; DBP = diastolic blood pressure; IRLSSG = International Restless Legs Syndrome Study Group; NAMS = North American Menopause Society; NICE = National Institute for Health and Care Excellence; NMA = network meta-analysis; NR = not reported; OD = once daily; PAWSS = Prediction of Alcohol Withdrawal Severity Scale; PRN = as needed; RCT = randomized controlled trial; SBP = systolic blood pressure; SNRI = serotonin-norepinephrine reuptake inhibitor; SOGC = Society of Obstetricians and Gynaecologists of Canada; SR = systematic review; SSRI = selective serotonin reuptake inhibitor; VA = Veterans Affairs.
Limitations
Some of the included guidelines are limited by the evidence identified to inform the recommendations. The supporting evidence for some of the recommendations was rated as low quality by the guideline authors or the recommendations were based on expert opinion. Additionally, we cannot determine whether the literature searches conducted to inform 4 of the guidelines17,21-23 were comprehensive as very limited details were provided. The IRLSSG (2015)27 guideline only searched a single database and may have missed relevant evidence.
We did not identify any evidence-based guidelines on the use of clonidine for the prevention of migraines or treatment of ADHD that met our inclusion criteria. However, the AAN (2019)28 guideline included a recommendation on the use of clonidine for patients with comorbid ADHD and tics. Most of the included guidelines did not include recommendations or guidance on clonidine dosing. The Hypertension Canada (2020)17 guideline included a recommendation for the use of clonidine in pregnant women however, it did not include recommendations on the use of clonidine for the treatment of hypertension in other populations.
There were inconsistencies in some of the recommendations in the included guidelines on menopause. The NAMS (2023)22 and NICE (2019)24 guidelines do not recommend clonidine for the treatment of vasomotor symptoms of menopause, whereas the SOGC (2021)23 and Endocrine Society (2015)25 guidelines included positive recommendations for clonidine for the treatment of vasomotor symptoms.
Conclusions and Implications for Decision- or Policy-Making
We included 12 evidence-based guidelines on the use of clonidine for various health conditions in this report. These comprised 1 guideline on hypertension,17 4 guidelines on substance use disorders (2 on opioid withdrawal19,21 and 2 on alcohol withdrawal18,20), 4 guidelines on the treatment of vasomotor symptoms of menopause,22-25 2 guidelines on restless leg syndrome,26,27 and 1 guideline on Tourette syndrome.28
The Hypertension Canada (2020)17 guideline recommends considering clonidine as a second-line option for pregnant women with chronic hypertension, gestational hypertension, or preeclampsia.
The 4 guidelines on substance use disorders all included positive recommendations for the use of clonidine. The CRISM (2023)18 guideline recommends offering clonidine for withdrawal management in an outpatient setting for patients at low risk of severe complications of alcohol withdrawal. The ASAM (2020)20 guideline recommends clonidine for the control of autonomic hyperactivity and anxiety when symptoms are not controlled by benzodiazepines alone. The ASAM (2020)20 guideline does not recommend clonidine be used alone to prevent or treat withdrawal-related seizures or delirium. The VA/DoD (2021)19 guideline suggests clonidine as a second-line drug for opioid withdrawal management when methadone and buprenorphine are contraindicated, unacceptable, or unavailable. The Commonwealth of Australia (2014)21 guideline recommends abrupt cessation of opioid use and control of symptoms using non-opioid drugs such as clonidine as an option for the management of opioid withdrawal.
The recommendations on the use of clonidine for the treatment of vasomotor symptoms of menopause were mixed. The NAMS (2023)22 guideline does not recommend clonidine for the treatment of vasomotor symptoms of menopause. The NICE (2019)24 guideline does not recommend routinely offering clonidine as first-line treatment for vasomotor symptoms alone. The SOGC (2021)23 guideline recommends clonidine as a nonhormonal option for refractory vasomotor symptoms. The Endocrine Society (2015)25 guideline suggests a trial of clonidine for women with moderate to severe vasomotor symptoms who do not respond to or are intolerant of SSRIs/SNRIs, gabapentin, or pregabalin.
Neither of the guidelines for restless leg syndrome recommend the use of clonidine. The AAN (2016)26 guideline states that there is insufficient evidence to support or refute the use of clonidine for the treatment of restless leg syndrome. The IRLSSG (2015)27 guideline states that clonidine should probably not be considered for people with restless leg syndrome who are pregnant or lactating.
The AAN (2019)28 guideline includes several recommendations on the use of clonidine for Tourette syndrome. The guideline recommends the use of alpha2 adrenergic agonists (e.g., clonidine) for the treatment of tics when the benefits outweigh the risks.28 The guideline also recommends counselling patients on common side effects and monitoring heart rate and blood pressure of patients treated with alpha2 adrenergic agonists.28
Future evidence-based guidelines that include recommendations on the use of clonidine for the prevention of migraines, treatment of ADHD and the treatment of hypertension in a broader population would help fill the gaps identified in this report. Due to the inconsistency in recommendations on the use of clonidine for the treatment of vasomotor symptoms of menopause, decision-makers may wish to consider other factors such as patient preferences and availability of other treatment options when making decisions around the use of clonidine for this indication.
References
1.Mayo Clinic. High blood pressure (hypertension). 2024; https://www.mayoclinic.org/diseases-conditions/high-blood-pressure/symptoms-causes/syc-20373410. Accessed 2024 Jul 8.
2.Mayo Clinic. High blood pressure (hypertension): Diagnosis & treatment. 2024; https://www.mayoclinic.org/diseases-conditions/high-blood-pressure/diagnosis-treatment/drc-20373417. Accessed 2024 Jul 8.
3.Cleveland Clinic. Substance Use Disorder (SUD). 2022; https://my.clevelandclinic.org/health/diseases/16652-drug-addiction-substance-use-disorder-sud. Accessed 2024 Jul 8.
4.Mayo Clinic. Menopause. 2023; https://www.mayoclinic.org/diseases-conditions/menopause/symptoms-causes/syc-20353397. Accessed 2024 Jul 8.
5.Cleveland Clinic. Menopause. 2024; https://my.clevelandclinic.org/health/diseases/21841-menopause. Accessed 2024 Jul 8.
6.Mayo Clinic. Restless legs syndrome. 2024; https://www.mayoclinic.org/diseases-conditions/restless-legs-syndrome/symptoms-causes/syc-20377168. Accessed 2024 Jul 8.
7.Cleveland Clinic. Restless legs syndrome. 2023; https://my.clevelandclinic.org/health/diseases/9497-restless-legs-syndrome. Accessed 2024 Jul 8.
8.Mayo Clinic. Migraine. 2023; https://www.mayoclinic.org/diseases-conditions/migraine-headache/symptoms-causes/syc-20360201. Accessed 2024 Jul 8.
9.Mayo Clinic. Migraine: Diagnosis & treatment 2023; https://www.mayoclinic.org/diseases-conditions/migraine-headache/diagnosis-treatment/drc-20360207. Accessed 2024 Jul 8.
10.Mayo Clinic. Adult attention-deficit/hyperactivity disorder (ADHD). 2023; https://www.mayoclinic.org/diseases-conditions/adult-adhd/symptoms-causes/syc-20350878. Accessed 2024 Jul 8.
11.Mayo Clinic. Adult attention-deficit/hyperactivity disorder (ADHD): Diagnosis & treatment. 2023; https://www.mayoclinic.org/diseases-conditions/adult-adhd/diagnosis-treatment/drc-20350883. Accessed 2024 Jul 8.
12.National Institute of Neurological Disorders and Stroke. Tourette syndrome. https://www.ninds.nih.gov/health-information/disorders/tourette-syndrome. Accessed 2024 Jul 8.
13.Yasaei R, Saadabadi A. Clonidine. Treasure Island (FL): StatPearls Publishing; 2023: https://www.ncbi.nlm.nih.gov/books/NBK459124/. Accessed 2024 Jul 8.
14.Clonidine (clonidine hydrochloride): 0.1 mg and 0.2 mg tablets [product monograph]. Saint-Laurent (QC): Sivem Pharmaceuticals ULC; 2023 Jun 1.
15.Agree Next Steps Consortium. The AGREE II Instrument. Hamilton (ON): AGREE Enterprise; 2017: https://www.agreetrust.org/wp-content/uploads/2017/12/AGREE-II-Users-Manual-and-23-item-Instrument-2009-Update-2017.pdf. Accessed 2024 Jul 3.
16.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
17.Rabi DM, McBrien KA, Sapir-Pichhadze R, et al. Hypertension Canada's 2020 comprehensive guidelines for the prevention, diagnosis, risk assessment, and treatment of hypertension in adults and children. Can J Cardiol. 2020;36(5):596-624. PubMed
18.Wood E, Bright J, Hsu K, et al. Canadian guideline for the clinical management of high-risk drinking and alcohol use disorder. CMAJ. 2023;195(40):E1364-E1379. PubMed
19.U.S. Department of Veterans Affairs. VA/DoD Clinical Practice Guidelines: Management of substance use disorder (SUD). 2021; https://www.healthquality.va.gov/guidelines/MH/sud/. Accessed 2024 Jul 3.
20.American Society of Addiction Medicine. The ASAM clinical practice guideline on alcohol withdrawal management. 2020; https://www.asam.org/quality-care/clinical-guidelines/alcohol-withdrawal-management-guideline. Accessed 2024 Jul 3.
21.Australian Government Department of Health and Aged Care. National guidelines for medication-assisted treatment of opioid dependence. 2014; https://www.health.gov.au/resources/publications/national-guidelines-for-medication-assisted-treatment-of-opioid-dependence. Accessed 2024 Jul 3.
22.“The Nonhormone Therapy Position Statement of The North American Menopause Society” Advisory Panel. The 2023 nonhormone therapy position statement of The North American Menopause Society. Menopause. 2023;30(6):573-590. PubMed
23.Jacobson M, Mills K, Graves G, Wolfman W, Fortier M. Guideline no. 422f: Menopause and breast cancer. J Obstet Gynaecol Can. 2021;43(12):1450-1456 e1451. PubMed
24.National Institute for Health and Care Excellence. Menopause: Diagnosis and management. (NICE guideline NG23). 2019: https://www.nice.org.uk/guidance/ng23/. Accessed 2024 Jul 3.
25.Stuenkel CA, Davis SR, Gompel A, et al. Treatment of symptoms of the menopause: An Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab. 2015;100(11):3975-4011. PubMed
26.Winkelman JW, Armstrong MJ, Allen RP, et al. Practice guideline summary: Treatment of restless legs syndrome in adults: Report of the Guideline Development, Dissemination, and Implementation Subcommittee of the American Academy of Neurology. Neurology. 2016;87(24):2585-2593. PubMed
27.Picchietti DL, Hensley JG, Bainbridge JL, et al. Consensus clinical practice guidelines for the diagnosis and treatment of restless legs syndrome/Willis-Ekbom disease during pregnancy and lactation. Sleep Med Rev. 2015;22:64-77. PubMed
28.Pringsheim T, Okun MS, Muller-Vahl K, et al. Practice guideline recommendations summary: Treatment of tics in people with Tourette syndrome and chronic tic disorders. Neurology. 2019;92(19):896-906. PubMed
29.Pringsheim T, Holler-Managan Y, Okun MS, et al. Comprehensive systematic review summary: Treatment of tics in people with Tourette syndrome and chronic tic disorders. Neurology. 2019;92(19):907-915. PubMed
Appendix 1: Selection of Included Studies
Figure 1: Preferred Reporting Items for Systematic reviews and Meta-Analyses PRISMA16 Flow Chart of Study Selection
Appendix 2: References of Potential Interest
Note this appendix has not been copy-edited.
Guidelines (Unclear Methodology)
BC Guidelines. High-Risk Drinking and Alcohol Use Disorder. 2024; https://www2.gov.bc.ca/gov/content/health/practitioner-professional-resources/bc-guidelines/high-risk-drinking-and-alcohol-use-disorder
Canadian ADHD Resource Alliance. Canadian ADHD Practice Guidelines, 4.1 Edition, Toronto (ON); CADDRA, 2020. Available from https://adhdlearn.caddra.ca/wp-content/uploads/2022/08/Canadian-ADHD-Practice-Guidelines-4.1-January-6-2021.pdf
BC Guidelines. Opioid Use Disorder - Diagnosis and Management in Primary Care. 2018; https://www2.gov.bc.ca/gov/content/health/practitioner-professional-resources/bc-guidelines/opioid-use-disorder
Review Articles
Mattes JA. Treating ADHD in Prison: Focus on Alpha-2 Agonists (Clonidine and Guanfacine). J Am Acad Psychiatry Law. 2016;44(2):151-157. PubMed
Appendix 3: Characteristics of Included Publications
Table 3: Characteristics of Included Guideline – Hypertension
Intended users, target population | Intervention(s) and major outcomes considered | Evidence collection, synthesis, and quality assessment | Recommendations for development and evaluation | Guideline validation |
|---|---|---|---|---|
Hypertension Canada (2020)17 | ||||
Intended Users: clinicians Target Population: adults and children at risk of or with hypertension | Interventions: pharmacotherapy, health behaviours Outcomes: NR | A medical librarian conducted comprehensive literature searches for 16 subgroups that represent distinct areas of hypertension. The literature was reviewed independently by subgroup members in a standardized manner. | The guideline panel consisted of content and methodological experts divided into 16 subgroups. The subgroups developed new or revised existing recommendations based on the identified evidence. Recommendations were reviewed and assigned a grade by a methodological expert from a central review committee. Recommendations were assigned a grade from D (lowest) to A (highest) based on the strength and quality of the clinical evidence. Members of the Hypertension Canada Guidelines Committee voted on the draft recommendations with > 70% support required for approval. | Feedback is received from end users to improve guideline processes and content and address identified needs. |
NR = not reported.
Note this table has not been copy-edited.
Table 4: Characteristics of Included Guidelines – Substance Use Disorders
Intended users, target population | Intervention(s) and major outcomes considered | Evidence collection, synthesis, and quality assessment | Recommendations for development and evaluation | Guideline validation |
|---|---|---|---|---|
CRISM (2023)18 | ||||
Intended Users: health care professionals in primary care and community-based settings, policy-makers developing health system interventions and people with alcohol use problems, their families and other affected populations seeking direction on evidence-based care Target Population: high-risk drinking and alcohol use disorder in youth (aged 11 to 25 years) and adults | Interventions: screening tools, risk assessment tools, pharmacotherapies, psychosocial treatment interventions Outcomes: NR | A systematic literature search was performed to update a previous guideline on alcohol use disorder. A contracted information specialist performed the literature search in multiple databases. Two authors independently screened and identified eligible studies. Study quality was assessed using validated tools by one author. | Evidence summaries from the previous guideline were updated and provided to working groups. The working groups decided through consensus whether recommendations would be accepted without modification, adapted, or removed. The full committee then reviewed the recommendations, incorporated feedback, and approved revisions by consensus. | 13 relevant experts and interested parties from Canada and international jurisdictions reviewed the draft guideline. Feedback from external reviewers was incorporated, and the committee accepted the final version through consensus. |
VA/DoD (2021)19 | ||||
Intended users: providers (e.g., physicians, physician assistants, nurse practitioners, nurses, psychologists, social workers, pharmacists, addiction counsellors, chaplains, nutritionists, dieticians, emergency care providers, behavioural health providers) Target population: veterans, active-duty Service Members, or non–active-duty Service Members > 18 years old, as well as other adults > 18 years old who are eligible for care in the VA and/or DoD health care delivery systems, who have symptoms and/or a diagnosis of substance use disorder, including AUD, OUD, sedative-hypnotic use disorder, stimulant use disorder, or cannabis use disorder | Interventions: pharmacotherapies, psychosocial interventions Outcomes: consumption/ abstinence/ frequency of use, retention/ duration in treatment, withdrawal symptoms, QoL, mortality, overdoses, suicide ideation or attempt. | A systematic review was conducted in multiple databases, including RCTs or other systematic reviews. Evidence was assessed using the GRADE methodology. | A development meeting was held to develop the recommendations. A work group interpreted the systematic review findings and developed the recommendations. When appropriate, recommendations from the previous guideline version were carried forward and modified as necessary. Recommendations were rated based on a modified GRADE and USPSTF methodology. Ratings were based on the quality of the evidence base, associated benefits and harms, patient values and preferences, and other implications. | A draft of the guideline was sent to experts from VA and DoD health care systems and outside organizations for external review. The work group considered all feedback and modified the guideline where appropriate, in line with the evidence. |
ASAM (2020)20 | ||||
Intended Users: clinicians, nurse practitioners, physician assistants, and pharmacists who provide alcohol withdrawal management in specialty and nonspeciality addiction treatment settings (including primary care and intensive care and surgery units in hospitals). Target Population: Adults (≥ 18 years) with a diagnosis of alcohol withdrawal | Interventions: pharmacological (excluding those that are not widely available in the US) and nonpharmacological interventions Outcomes: severity of withdrawal syndrome, treatment completion, transfer to a more intensive level of care, incidence of seizure, delirium, death and adverse events, and linkage to long-term AUD treatment. | A systematic literature review was conducted in multiple databases that included all levels of published literature, including nonrandomized studies and case studies. Additionally, a search for grey literature was conducted. Two independent reviewers screened abstracts and full texts of articles for inclusion. The quality of the included studies was evaluated using validated tools. Systematic reviews of RCTs and guidelines based on systematic reviews were included. Where these study designs were not available, lower-quality evidence sources were included. | The guideline committee and project team developed the draft recommendations using RAM, which involves multiple rounds of rating and a face-to-face meeting. Committee members rated the appropriateness of each guideline statement on a scale from 1 to 9. A statement was deemed appropriate if the median rating was in the 7 to 9 range, and no more than one-third of the experts rated it outside that range. | The guideline was sent to interested parties and posted publicly for external review. Feedback was incorporated as appropriate and in line with the evidence. |
Commonwealth of Australia (2014)21 | ||||
Intended users: generalist service providers Target population: people who are opioid dependent | Interventions: pharmacotherapies Outcomes: NR | Literature searches were conducted to identify systematic reviews and clinical trials. | A list of issues to be addressed in the guidelines was developed based on previous guidelines and the authors' experience. Evidence statements were designed for the list of issues. The recommendations were graded using a 4-star rating system.
| NR |
ASAM = American Society of Addiction Medicine; AUD = alcohol use disorder; CRISM = Canadian Research Initiative in Substance Misuse; DoD = Department of Defense; GRADE = Grading of Recommendations Assessment, Development and Evaluation; NR = not reported; OUD = opioid use disorder; QoL = quality of life; RAM = RAND/UCLA Appropriateness Method; RCT = randomized controlled trial; USPSTF = US Preventive Services Task Force; VA = Veterans Affairs.
Note this table has not been copy-edited.
Table 5: Characteristics of Included Guideline – Menopause
Intended users, target population | Intervention(s) and major outcomes considered | Evidence collection, synthesis, and quality assessment | Recommendations for development and evaluation | Guideline validation |
|---|---|---|---|---|
NAMS (2023)22 | ||||
Intended Users: NR Target Population: people experiencing menopause | Interventions: lifestyle interventions, mind-body techniques, prescription therapies, dietary supplements, and acupuncture, other treatments, and technologies Outcomes: NR | An extensive review of the literature was conducted. | The guideline was written based on the literature review and was submitted to and approved by the NAMS board of trustees. The guideline panel assessed the available literature to develop the recommendations. The level of evidence was assigned a rating from 1 to 3.
| NR |
SOGC (2021)23 | ||||
Intended Users: physicians, including gynecologists, obstetricians, family physicians, internists, and emergency medicine specialists; nurses, including registered nurses and nurse practitioners; pharmacists; medical trainees, including medical students, residents, fellows; and other providers of health care for the target population Target Population: perimenopausal and postmenopausal women | Interventions: hormone therapy and nonhormonal options Outcomes: NR | A literature search was conducted in multiple databases. The quality of evidence was rated using the GRADE methodology (ratings range from very low to high). | Details on the development of the recommendations were not provided. The strength of recommendations was rated using the GRADE methodology (strong or conditional). | NR |
NICE (2019)24 | ||||
Intended users: health care professionals who care for women in menopause, women in menopause, and their families and carers Target population: menopausal women, women with premature ovarian insufficiency | Interventions: hormonal pharmaceutical treatments, nonhormonal pharmaceutical treatments, nonpharmaceutical treatments, psychological therapy Outcomes: frequency of hot flushes (including night sweats), frequency of sexual activity, psychological symptoms, anxiety, low mood (not clinical depression), musculoskeletal symptoms, safety outcomes, discontinuation, vaginal bleeding | Systematic literature searches were conducted in multiple databases to identify all published clinical evidence (RCTs, nonrandomized trials, and observational studies) relevant to the review questions. Titles and abstracts were screened, and full texts of relevant studies were obtained and screened based on prespecified inclusion and exclusion criteria. Relevant studies were critically appraised using the checklists specified in the NICE guidelines manual. Evidence summaries were generated, and data were combined in meta-analysis where appropriate. Evidence was assessed using the GRADE methodology (ratings range from very low to high). | The guideline development group drafted recommendations based on their interpretation of the relevant evidence. Considerations included balancing the benefits, harms, and costs of different options. | The guideline was subject to a 6-week public consultation and feedback period. |
Endocrine Society (2015)25 | ||||
Intended users: health care professionals Target population: menopausal and postmenopausal women | Interventions: hormonal and nonhormonal therapies Outcomes: NR | The guideline task force commissioned 3 systematic reviews on hormone therapies. Other existing meta-analyses and trials were also considered. The quality of evidence was assessed using the GRADE methodology (ratings range from very low to high). | The task force followed the GRADE methodology to develop the recommendations. Consensus on recommendations was determined through email communications, conference calls, and 1 face-to-face meeting. The phrases “we recommend” and “we recommend against” and the number 1 were used for strong recommendations. The phrases “we suggest” and “we suggest against” and the number 2 were used for weak recommendations. | The Australasian Menopause Society, the British Menopause Society, the European Menopause and Andropause Society, the European Society of Endocrinology, and the International Menopause Society (co-sponsors of the guideline) reviewed and commented on the draft. |
GRADE = Grading of Recommendations, Development and Evaluation; NAMS = North American Menopause Society; NICE = National Institute for Health and Care Excellence; NR = not reported; SOGC = Society of Obstetricians and Gynaecologists of Canada.
Note this table has not been copy-edited.
Table 6: Characteristics of Included Guidelines – Restless Leg Syndrome
Intended users, target population | Intervention(s) and major outcomes considered | Evidence collection, synthesis, and quality assessment | Recommendations for development and evaluation | Guideline validation |
|---|---|---|---|---|
AAN (2016)26 | ||||
Intended users: clinicians Target population: adults with restless leg syndrome | Interventions: pharmacologic and nonpharmacologic therapies Outcomes: symptoms and clinical consequences of restless leg syndrome (disturbed sleep, periodic limb movements of sleep, depression/anxiety, QoL) | The guideline panel developed the clinical question and search terms. An independent medical librarian performed a systematic literature search in multiple databases. The guideline panel chair reviewed abstracts for inclusion. Two panel members individually reviewed the full articles for inclusion and assessed the quality of evidence and risk of bias. Identified studies were rated on a scale from class IV (lowest quality) to class I (highest quality). Meta-analyses were performed when needed.
| The guideline panel based recommendations strictly on the identified evidence and did not use expert opinion. The panel considered statistical significance, clinical significance, and precision when drawing conclusions from the evidence. Recommendations were assigned a level based on the quality of evidence.
| NR |
IRLSSG (2015)27 | ||||
Intended users: health practitioners Target population: people with restless leg syndrome/ Willis-Ekbom disease who are pregnant or lactating. | Interventions: pharmacologic and nonpharmacologic therapies Outcomes: NR | A literature review was conducted in 1 database. | The guideline committee held monthly teleconferences and a single face-to-face meeting. Consensus questions were agreed upon and discussed. The committee used an integrative approach to develop the recommendations considering the existing literature and their clinical experience. Recommendations were rated from 1 to 5: 1. Recommended (high level of evidence for safety/effectiveness) 2. May be considered (evidence for safety effectiveness) 3. Insufficient evidence to reach consensus 4. Probably should not be considered (evidence for risk/ineffectiveness) 5. Not recommended (high level of evidence for risk/ ineffectiveness) | NR |
AAN = American Academy of Neurology; IRLSSG = International Restless Legs Syndrome Study Group; NR = not reported; QoL = quality of life.
Note this table has not been copy-edited.
Table 7: Characteristics of Included Guidelines – Tourette Syndrome
Intended users, target population | Intervention(s) and major outcomes considered | Evidence collection, synthesis, and quality assessment | Recommendations development and evaluation | Guideline validation |
|---|---|---|---|---|
AAN (2019)28 | ||||
Intended users: clinicians Target population: children and adults with Tourette syndrome or a chronic tic disorder | Interventions: medical, behavioural, and neurostimulation interventions Outcomes: tic severity and tic-related impairment | A systematic review that included systematic reviews and RCTs was conducted in multiple databases.29 Two reviewers independently screened articles for inclusion. Two panel members rated the class of evidence for each article according to the AAN classification scheme on a scale from class IV (lowest quality) to class I (highest quality). Meta-analysis was performed when appropriate.
| A modified form of the GRADE process was used to develop conclusions. Four types of premises were used to support recommendations: evidence-based conclusion from the systematic review, generally accepted principals of care, strong evidence from related conditions, and deductive inferences from other premises. The guideline panel assigned each recommendation a level of A, B, or C.
| NR |
AAN = American Academy of Neurology; GRADE = Grading of Recommendations Assessment, Development and Evaluation; NR = not reported; RCT = randomized controlled trial.
Note this table has not been copy-edited.
Appendix 4: Critical Appraisal of Included Publications
Note this appendix has not been copy-edited.
Table 8: Strengths and Limitations of Guidelines Using AGREE II15 – Part 1
Item | CRISM (2023)18 | NAMS (2023)22 | SOGC (2021)23 | VA/ DoD (2021)19 | ASAM (2020)20 | Hypertension Canada (2020)17 |
|---|---|---|---|---|---|---|
Domain 1: scope and purpose | ||||||
1. The overall objective(s) of the guideline is (are) specifically described. | Yes | Yes | Yes | Yes | Yes | Yes |
2. The health question(s) covered by the guideline is (are) specifically described. | Yes | Yes | Yes | Yes | Yes | Yes |
3. The population (patients, public, etc.) to whom the guideline is meant to apply is specifically described. | Yes | Yes | Yes | Yes | Yes | Yes |
Domain 2: stakeholder involvement | ||||||
4. The guideline development group includes individuals from all relevant professional groups | Yes | Yes | Unclear | Yes | Yes | Yes |
5. The views and preferences of the target population (patients, public, etc.) have been sought. | Yes | No | No | Yes | Partially | No |
6. The target users of the guideline are clearly defined. | Yes | No | Yes | Yes | Yes | Yes |
Domain 3: rigour of development | ||||||
7. Systematic methods were used to search for evidence. | Yes | Unclear | Unclear | Yes | Yes | Unclear |
8. The criteria for selecting the evidence are clearly described. | Yes | No | No | Yes | Yes | No |
9. The strengths and limitations of the body of evidence are clearly described. | Yes | Partially | Yes | Yes | No | Yes |
10. The methods for formulating the recommendations are clearly described. | Yes | Partially | No | Yes | Yes | Yes |
11. The health benefits, side effects, and risks have been considered in formulating the recommendations. | Yes | Yes | Yes | Yes | Yes | Yes |
12. There is an explicit link between the recommendations and the supporting evidence. | Yes | Yes | No | Yes | No | Yes |
13. The guideline has been externally reviewed by experts before its publication. | Yes | No | No | Yes | Yes | No |
14. A procedure for updating the guideline is provided. | Partially | No | Yes | Yes | No | Yes |
Domain 4: clarity of presentation | ||||||
15. The recommendations are specific and unambiguous. | Yes | Yes | Yes | Yes | Yes | Yes |
16. The different options for management of the condition or health issue are clearly presented. | Yes | Yes | Yes | Yes | Yes | Yes |
17. Key recommendations are easily identifiable. | Yes | Yes | Yes | Yes | Yes | Yes |
Domain 5: applicability | ||||||
18. The guideline describes facilitators and barriers to its application. | Yes | No | No | No | No | No |
19. The guideline provides advice and/or tools on how the recommendations can be put into practice. | Yes | No | No | Yes | Yes | Yes |
20. The potential resource implications of applying the recommendations have been considered. | No | No | No | Yes | No | No |
21. The guideline presents monitoring and/or auditing criteria. | No | No | No | No | No | No |
Domain 6: editorial independence | ||||||
22. The views of the funding body have not influenced the content of the guideline. | Yes | Yes | Unclear | Yes | Unclear | Yes |
23. Competing interests of guideline development group members have been recorded and addressed. | Yes | Yes | Partially | Yes | Yes | Yes |
AGREE II = Appraisal of Guidelines for Research and Evaluation II; ASAM = American Society of Addiction Medicine; CRISM = Canadian Research Initiative in Substance Misuse; DoD = Department of Defense; NAMS = North American Menopause Society; SOGC = Society of Obstetricians and Gynaecologists of Canada; VA = Veterans Affairs.
Table 9: Strengths and Limitations of Guidelines Using AGREE II15 – Part 2
Item | AAN (2019)28 | NICE (2019)24 | AAN (2016)26 | Endocrine Society (2015)25 | IRLSSG (2015)27 | Commonwealth of Australia (2014)21 |
|---|---|---|---|---|---|---|
Domain 1: scope and purpose | ||||||
1. The overall objective(s) of the guideline is (are) specifically described. | Yes | Yes | Yes | Yes | Yes | Yes |
2. The health question(s) covered by the guideline is (are) specifically described. | Yes | Yes | Yes | Yes | Yes | Yes |
3. The population (patients, public, etc.) to whom the guideline is meant to apply is specifically described. | Yes | Yes | Yes | Yes | Yes | Yes |
Domain 2: stakeholder involvement | ||||||
4. The guideline development group includes individuals from all relevant professional groups. | Yes | Yes | Yes | Yes | Yes | Yes |
5. The views and preferences of the target population (patients, public, etc.) have been sought. | No | Yes | No | No | No | No |
6. The target users of the guideline are clearly defined. | Yes | Yes | Yes | Yes | Yes | Yes |
Domain 3: rigour of development | ||||||
7. Systematic methods were used to search for evidence. | Yes | Yes | Yes | Yes | Partially | Unclear |
8. The criteria for selecting the evidence are clearly described. | Yes | Yes | Yes | Yes | Partially | No |
9. The strengths and limitations of the body of evidence are clearly described. | Yes | Yes | Yes | Yes | Yes | Yes |
10. The methods for formulating the recommendations are clearly described. | Yes | Yes | Yes | Yes | Yes | Partially |
11. The health benefits, side effects, and risks have been considered in formulating the recommendations. | Yes | Yes | Yes | Yes | Yes | Yes |
12. There is an explicit link between the recommendations and the supporting evidence. | Yes | Yes | Yes | Yes | Yes | Partially |
13. The guideline has been externally reviewed by experts before its publication. | No | No | No | Yes | No | Yes |
14. A procedure for updating the guideline is provided. | No | Yes | No | No | No | No |
Domain 4: clarity of presentation | ||||||
15. The recommendations are specific and unambiguous. | Yes | Yes | Yes | Yes | Yes | Yes |
16. The different options for management of the condition or health issue are clearly presented. | Yes | Yes | Yes | Yes | Yes | Yes |
17. Key recommendations are easily identifiable. | Yes | Yes | Yes | Yes | Yes | No |
Domain 5: applicability | ||||||
18. The guideline describes facilitators and barriers to its application. | No | Yes | No | No | No | No |
19. The guideline provides advice and/or tools on how the recommendations can be put into practice. | No | Yes | No | Yes | Partially | Yes |
20. The potential resource implications of applying the recommendations have been considered. | No | Yes | No | No | No | Yes |
21. The guideline presents monitoring and/or auditing criteria. | No | No | No | No | No | No |
Domain 6: editorial independence | ||||||
22. The views of the funding body have not influenced the content of the guideline. | Yes | Yes | Yes | Yes | Yes | Yes |
23. Competing interests of guideline development group members have been recorded and addressed. | Yes | Yes | Yes | Yes | Yes | Partially |
AAN = American Academy of Neurology; AGREE II = Appraisal of Guidelines for Research and Evaluation II; IRLSSG = International Restless Legs Syndrome Study Group; NICE = National Institute for Health and Care Excellence.
Appendix 5: Recommendations in Included Guidelines
Note this appendix has not been copy-edited.
Table 10: Summary of Recommendations – Hypertension
Recommendation | Quality of evidence and strength of recommendation |
|---|---|
Hypertension Canada (2020)17 | |
“Antihypertensive therapy is recommended for average SBP measurements of 140 mm Hg or DBP measurements of 90 mm Hg in pregnant women with chronic hypertension, gestational hypertension, or preeclampsia.
Supporting evidence: NA | Grade D (based on expert opinion alone) |
DBP = diastolic blood pressure; NA = not applicable; SBP = systolic blood pressure.
Table 11: Summary of Recommendations – Substance Use Disorders
Recommendations and supporting evidence | Quality of evidence and strength of recommendations |
|---|---|
CRISM (2023)18 | |
“For patients at low risk of severe complications of alcohol withdrawal (e.g., PAWSS < 4), clinicians should consider offering nonbenzodiazepine medications, such as gabapentin, carbamazepine or clonidine for withdrawal management in an outpatient setting (e.g., primary care, virtual). (p. E1368).”18 Supporting evidence: 2 RCTs reported clonidine is as effective as chlordiazepoxide in the management of mild to moderate withdrawal symptoms with better control of sympathetic symptoms and reductions in patient anxiety. | Certainty of evidence: Low Strength of recommendation: Strong |
VA/DoD (2021)19 | |
“For patients with opioid use disorder for whom withdrawal management is indicated and for whom methadone and buprenorphine are contraindicated, unacceptable, or unavailable, we suggest offering clonidine or lofexidine as a second-line agent for opioid withdrawal management (p. 31)”19 Supporting evidence: 1 SR included comparisons of alpha2-adrenergic agonists vs. placebo, methadone, or another alpha2-adrenergic agonist. 1 SR that included comparisons of buprenorphine vs clonidine, lofexidine, or methadone. The work group considered that the benefits of improved withdrawal symptoms outweighed potential harms (minimal side effects and adverse events [hypotension for lofexidine and clonidine]) and that patient values and preferences varied somewhat. | Quality of evidence: Low Strength of recommendation: Weak |
ASAM (2020)20 | |
Ambulatory and inpatient management of alcohol withdrawal: “Alpha2-adrenergic agonists such as clonidine can be used as an adjunct to benzodiazepine therapy to control autonomic hyperactivity and anxiety when symptoms are not controlled by benzodiazepines alone. They should not be used alone to prevent or treat withdrawal-related seizures or delirium. (p. 9)”20 Supporting evidence: NR | Quality of evidence: NR Strength of recommendation: NR |
Commonwealth of Australia (2014)21 | |
“Two distinct medication approaches are recommended for the management of opioid withdrawal:
Supporting evidence: The guideline authors stated that both approaches are well supported by evidence. They also stated that the use of buprenorphine to manage withdrawal is associated with significantly better relief of withdrawal than clonidine and supplementary medications (1 SR). The SR also reported that completion of withdrawal is significantly more likely when managed with buprenorphine vs clonidine. Buprenorphine is associated with fewer adverse effects and fewer withdrawals from treatment due to adverse effects than clonidine. | Quality of evidence: 4 stars (body of evidence can be trusted to guide practice) Strength of recommendation: NR |
ASAM = American Society of Addiction Medicine; CRISM = Canadian Research Initiative in Substance Misuse; DoD = Department of Defense; NR = not reported; PAWSS = Prediction of Alcohol Withdrawal Severity Scale; RCT = randomized controlled trial; SR = systematic review; VA = Veterans Affairs.
Table 12: Summary of Recommendations – Menopause
Recommendations and supporting evidence | Quality of evidence and strength of recommendations |
|---|---|
NAMS (2023)22 | |
“Because there are other more effective therapies with fewer AEs, clonidine is not recommended. (p. 578)”22 Supporting evidence: 1 SR reported that clonidine is modestly more beneficial than placebo at reducing vasomotor symptoms. 2 SRs reported that clonidine is less beneficial than SSRIs, SNRIs, and gabapentin at reducing vasomotor symptoms. The guideline authors stated that clonidine is used infrequently due to AEs, including hypotension, lightheadedness, headache, dry mouth, dizziness, sedation, and constipation. They also stated that sudden cessation of clonidine can lead to significant elevation of blood pressure. | Quality of evidence: Levels 1 to 3 (good and consistent scientific evidence, limited or inconsistent scientific evidence, and consensus and expert opinion) Strength of recommendation: NR |
SOGC (2021)23 | |
“Paroxetine, gabapentin, oxybutynin, and clonidine are nonhormonal options for refractory vasomotor symptoms. Paroxetine should be used with caution in patients receiving tamoxifen (p. 1451)”23 Supporting evidence: NR | Quality of evidence: Moderate Strength of recommendation: Conditional |
NICE (2019)24 | |
“Give information to menopausal women and their family members or carers (as appropriate) about the following types of treatment for menopausal symptoms:
Supporting evidence: Clonidine was not included in the network meta-analysis conducted for the guideline due to how outcomes were reported in studies of clonidine. Therefore, the relative effectiveness of clonidine in relieving short-term symptoms for women in menopause could not be estimated. In the absence of this data, the guideline development group recognized the importance of clonidine for the treatment of some women in menopause. | Quality of evidence: NR Strength of recommendation: NR |
“Do not routinely offer SSRIs, SNRIs or clonidine as first-line treatment for vasomotor symptoms alone. (p. 8)”24 Supporting evidence: Clonidine was not included in the network meta-analysis conducted for the guideline due to how outcomes were reported in studies of clonidine. Therefore, the relative effectiveness of clonidine in relieving short-term symptoms for women in menopause could not be estimated. | Quality of evidence: NR Strength of recommendation: Strong |
Endocrine Society (2015)25 | |
“For those women seeking relief of moderate to severe vasomotor symptoms who are not responding to or tolerating the nonhormonal prescription therapies SSRIs/SNRIs or gabapentin or pregabalin, we suggest a trial of clonidine (if there are no contraindications). (p. 3995)”25 Supporting evidence: Several RCTs demonstrated that clonidine reduces hot flashes. However, it is less effective than SSRI/SNRIs, gabapentin, and pregabalin and is associated with more side effects. | Quality of evidence: Low Strength of recommendation: Weak |
AE = adverse event; NAMS = North American Menopause Society; NICE = National Institute for Health and Care Excellence; NR = not reported; RCT = randomized controlled trial; SNRI = serotonin-norepinephrine reuptake inhibitor; SOGC = Society of Obstetricians and Gynaecologists of Canada; SSRI = selective serotonin reuptake inhibitor.
Table 13: Summary of Recommendations – Restless Leg Syndrome
Recommendations and supporting evidence | Quality of evidence and strength of recommendations |
|---|---|
AAN (2016)26 | |
“There is insufficient evidence to support or refute the use of gabapentin, iron sucrose, oxycodone, clonazepam, bupropion, clonidine, selenium, rifaximin, botulinum neurotoxin, valproic acid, carbamazepine, or valerian in the treatment of restless leg syndrome (p. 2590)”26 Supporting evidence: 1 crossover trial of clonidine vs placebo in which patients reported less paresthesia, motor restlessness, and daytime fatigue during the clonidine treatment arm. There was no difference in periodic limb movement index between groups. The most common adverse events were hypotension, decreased cognition, dry mouth, and sleepiness. | Quality of evidence: Class III Strength of recommendation: Level U (insufficient evidence) |
IRLSSG (2015)27 | |
Clonidine should probably not be considered for people with restless leg syndrome who are pregnant or lactating. Supporting evidence: A small RCT found limited efficacy of clonidine for restless leg syndrome. Clonidine passes on to breast milk. | Level 4 (evidence for risk/ ineffectiveness) |
AAN = American Academy of Neurology; IRLSSG = International Restless Legs Syndrome Study Group; RCT = randomized controlled trial.
Table 14: Summary of Recommendations – Tourette Syndrome
Recommendations and supporting evidence | Quality of evidence and strength of recommendations |
|---|---|
AAN (2019)28 | |
“Physicians should counsel individuals with tics and comorbid ADHD that alpha2 adrenergic agonists may provide benefit for both conditions (p. 900)”28 Supporting evidence: 1 study that reported reduced tic severity in children with tics and a comorbid diagnosis of ADHD who received clonidine plus methylphenidate vs placebo.29 | Quality of evidence: Class I Strength of recommendation: Level B |
“Physicians should prescribe alpha2 adrenergic agonists for the treatment of tics when the benefits of treatment outweigh the risks (p. 900)”28 Supporting evidence: 3 studies that reported reduced tic severity in people with tics receiving clonidine vs placebo.29 | Quality of evidence: Class I and II Strength of recommendation: Level B |
“Physicians must counsel patients regarding common side effects of alpha2 adrenergic agonists, including sedation (p. 900)”28 Supporting evidence: 2 studies reported that sedation was more common in people with tics receiving clonidine vs placebo.29 1 SR of alpha2 adrenergic agonists for ADHD in children and adolescents demonstrated hypotension, bradycardia, and sedation with these agents.28 | Quality of evidence: Class I and II Strength of recommendation: Level A |
“Physicians must monitor heart rate and blood pressure in patients with tics treated with alpha2 adrenergic agonists (p. 900)”28 Supporting evidence: 1 SR of alpha2 adrenergic agonists for ADHD in children and adolescents demonstrated hypotension and bradycardia with these agents.28 | Quality of evidence: NR Strength of recommendation: Level A |
“Physicians discontinuing alpha2 adrenergic agonists must gradually taper them to avoid rebound hypertension (p. 900)”28 Supporting evidence: NR. | Quality of evidence: NR Strength of recommendation: Level A |
AAN = American Academy of Neurology; ADHD = attention-deficit/hyperactivity disorder; NR = not reported; SR = systematic review.
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for noncommercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca