CADTH Health Technology Review
Auditory Verbal Therapy for Children With Hearing Loss
Rapid Review
Key Messages
What Is the Issue?
Children with hearing loss may experience delays in language, speech, and cognitive development, which can have long-lasting implications if unaddressed.
Early hearing detection and intervention programs aim to identify and avoid long-term impacts of hearing loss for infants and children. Interventions include the use of hearing devices (e.g., cochlear implants, hearing aids) and habilitation with the intent to minimize delays in development.
Auditory verbal therapy (AVT) is a specialized habilitation intervention that focuses on improving listening skills while avoiding visual cues to communicate. The overall goal is to minimize the difference in speech and language capabilities between children with hearing loss and their peers without hearing loss. It requires certified professionals to deliver.
The effectiveness of AVT for children with hearing loss compared to other habilitation approaches remains unclear.
What Did We Do?
To inform decisions regarding the use of AVT, we summarized evidence that compared the effectiveness of AVT to alternative habilitation approaches for children with hearing loss using cochlear implants, bone-conduction hearing devices, or conventional hearing aids. We also sought to identify evidence-based guidelines regarding appropriate habilitation approaches for this population.
We searched key resources, including journal citation databases, and conducted a focused internet search for relevant evidence published since 2019. One reviewer screened articles for inclusion based on predefined criteria.
What Did We Find?
For children with cochlear implants, AVT may result in better speech and language outcomes than standard habilitation, oral communication, total communication, or the bilingual-bicultural approach. However, AVT did not result in a significant difference in speech and language skills compared to sign and spoken language (1 systematic review).
AVT may result in better executive function compared to standard auditory training for children with cochlear implants (1 randomized controlled trial).
We did not find any evidence-based guidelines regarding appropriate habilitation approaches that met the predefined criteria for this rapid review. We also did not identify relevant evidence for children using bone conduction hearing devices and conventional hearing aids.
What Does It Mean?
Limited and low-quality evidence suggests that AVT is more effective than some alternative habilitation approaches for children using cochlear implants. High-quality studies are needed with rigorous methodology, detailed reporting of results, and analysis controlling for confounding factors to make definitive conclusions about the performance of AVT against alternative habilitation for this population.
Although the literature comparing AVT to alternative approaches is limited, findings from before-and-after studies suggest that AVT improves speech, language, and executive function for children with cochlear implants. Decisions around the use of AVT may also depend on the individual needs and goals of the child and their parents or guardians and the resources needed to ensure capacity to deliver AVT, such as time and costs to certify professionals.
Abbreviations
AG
Alexander Graham
AVT
auditory verbal therapy
EHDI
early hearing detection and intervention
Context and Policy Issues
Hearing Loss in Children in Canada
Children with hearing loss can experience delays in speech, language, and cognitive development.1-3 A cross sectional study estimated that 7.7% of youth aged 6 to 19 years in Canada have some type of hearing loss in 1 ear (unilateral) or both ears (bilateral).4
Hearing loss can be due to genetics or ear damage caused by infection (e.g., otitis externa), trauma, congenital malformations, or disease (e.g., tumours).1 Hearing loss can be categorized as sensorineural, conductive, or a combination of both.1 Sensorineural is the most common type of hearing loss and is due to damage in the inner ear or auditory nerve,1,4 whereas conductive hearing loss is due to damage in the outer ear.1 Early intervention can avoid the long-term consequences of hearing loss by offering programs that support social and emotional development, improve academic performance, and minimize potential psychological distress.5
Early Hearing Detection and Intervention Programs
An early hearing detection and intervention (EHDI) program will typically offer screening and interventions to detect hearing loss and minimize delays in development.3,5 Most jurisdictions in Canada offer newborn hearing screening as part of their EHDI program.5 During screening, the provider will conduct at least 1 test to assess hearing (e.g., auditory brainstem response, visual reinforcement audiometry, or pure tone audiometry).6 Based on the results of the test, the provider may refer the child for an intervention appropriate to their needs, such as the use of hearing devices (e.g., cochlear implants, bone conduction hearing devices, conventional hearing aids) or habilitation.3,5
Habilitation interventions during speech-language therapy aim to help children with hearing loss build their communication skills. Speech-language pathologists or audiologists can deliver these interventions to individuals with hearing loss.7 Their approach may be auditory-oral driven or visual driven.2,3 The former promotes the use of residual hearing, whereas a visual-driven approach focuses on gestures and cues (e.g., sign language).2 Other therapies use a combined approach that includes auditory and visual cues. For example, total communication therapy teaches children to use a variety of methods to communicate, including sign language, speech, listening, lip reading, finger spelling, facial expression, and gesture.2,3
Auditory Verbal Therapy
Providers may offer auditory verbal therapy (AVT) as a specialized habilitation intervention for children with hearing loss.8 It is an auditory-oral approach that places emphasis on listening skills and teaches children with hearing loss to avoid visual cues to communicate.9 The sessions must be delivered by health professionals, such as speech-language therapists or audiologists, who are also certified by the Alexander Graham (AG) Bell Academy for Listening and Spoken Language.9 They must uphold 10 principles for AVT practice,9,10 which are listed in Appendix 5.
The goal of AVT is for children with hearing loss to have the same language and speech capabilities as their peers without hearing loss.9 It requires parents to be involved in sessions and for all adults in the child’s everyday life to encourage the use of auditory and verbal strategies.8,9 Given the importance of auditory stimulation in AVT, it encourages the use of hearing devices, such as cochlear implants and hearing aids.9 AVT shows potential to improve communication and avoid delays in development for children with hearing loss.11 However, it remains unclear if it is the best approach to habilitation.
Objective
The purpose of this report is to summarize and critically appraise the evidence regarding the clinical effectiveness of AVT compared to other forms of therapy for children with hearing loss using cochlear implants, bone conduction hearing devices, or conventional hearing aids. We also aimed to summarize and critically appraise evidence-based guidelines for therapies that facilitate auditory and verbal skill development for this population.
Research Questions
What is the clinical effectiveness of AVT for children with hearing loss using cochlear implants, bone conduction hearing devices, or conventional hearing aids?
What are the evidence-based guidelines regarding therapies for children with hearing loss using cochlear implants, bone conduction hearing devices, or conventional hearing aids?
Methods
An information specialist conducted a customized literature search, balancing comprehensiveness with relevancy, of multiple sources and grey literature on June 27, 2024.
One reviewer screened citations and selected studies based on the inclusion criteria presented in Table 1, and critically appraised included publications using established critical appraisal tools.
Appendix 1 presents a detailed description of methods.
Criteria | Description |
|---|---|
Population | Children (≤ 18 years old) with hearing loss using 1 of the following devices:
|
Intervention | Q1: Auditory verbal therapy Q2: Habilitation therapies to facilitate auditory and verbal skill development |
Comparators | Q1: Other forms of habilitation therapies for hearing loss (e.g., total communication therapy, auditory-oral therapy, speech-language pathology) Q2: Not applicable |
Outcomes | Q1: Clinical benefits and harms (e.g., cognitive development, executive function, language development) Q2: Recommendations regarding appropriate therapies |
Study designs | Health technology assessments, systematic reviews, randomized controlled trials, nonrandomized studies, evidence-based guidelines |
Publication date | Since January 1, 2019 |
Summary of Evidence
Quantity of Research Available
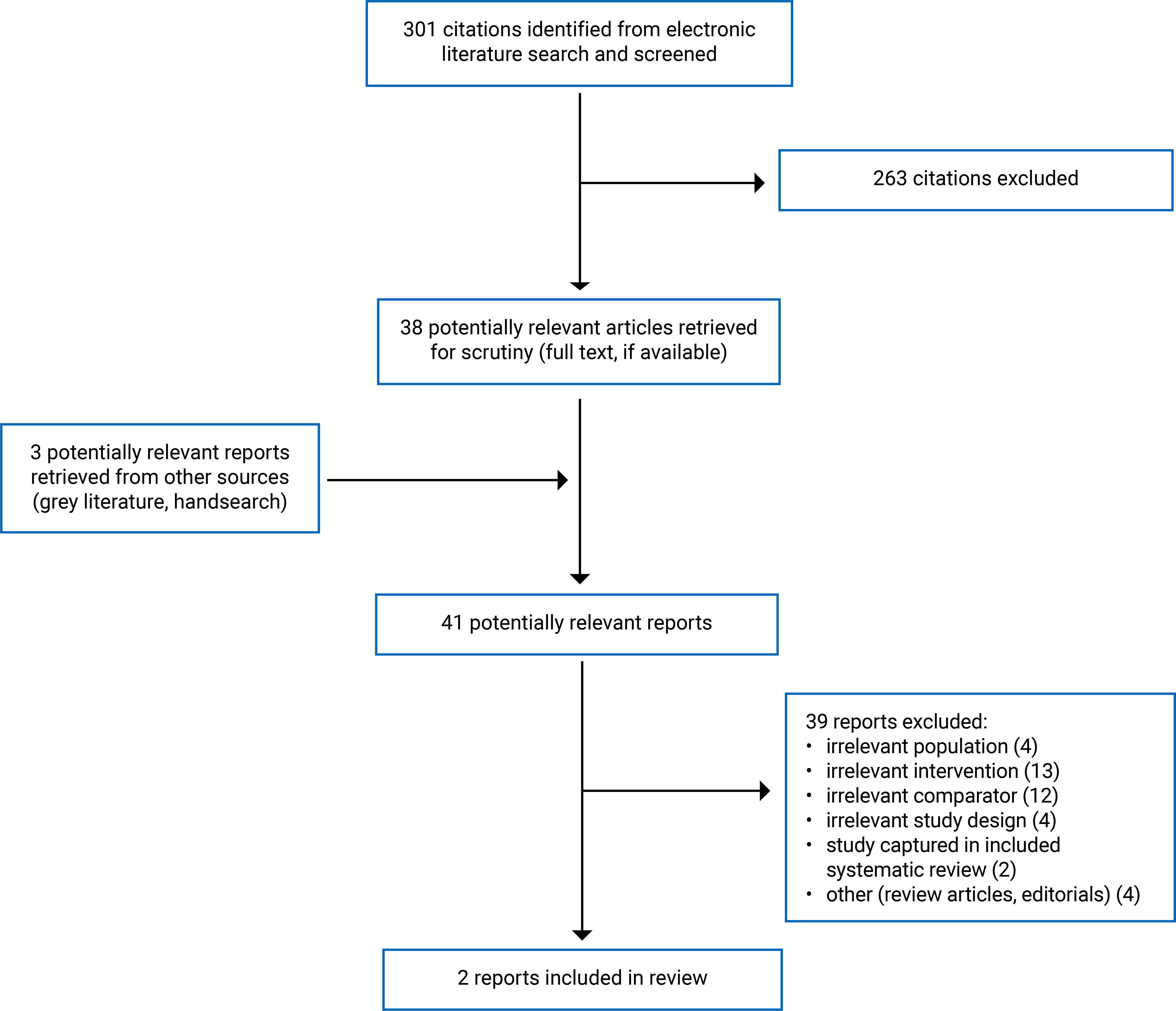
This report includes 2 publications that met our inclusion criteria, of which 1 is a systematic review2 and 1 is a randomized controlled trial.8 The PRISMA12 flow chart of the study selection is presented in Appendix 1.
Appendix 6 lists additional references of potential interest that provide information about AVT but did not meet our inclusion criteria, such as noncomparative evidence and guidelines with unclear methods.
Summary of Study Characteristics
The systematic review had broader inclusion criteria than this report, specifically their comparators and outcomes of interest.2 Of note, we reported on the characteristics and results of the subset of relevant primary studies included in the systematic review throughout this report.
Appendix 2 presents details regarding the characteristics of included publications.
Included for Question 1
We included 1 systematic review2 and 1 randomized controlled trial13 with evidence regarding the clinical effectiveness of AVT compared to alternative habilitation therapies. The systematic review was published in 2021 and conducted in Cyprus.2 The systematic review searched for relevant peer-reviewed articles published between 1951 and 2020.2 It included 4 primary retrospective studies relevant to this report.2 The review authors did not report where included primary studies were conducted, but they reported that these studies were conducted in English or Danish.2 The randomized controlled trial was published in 2022 and conducted in Iran.13
Both studies compared AVT with alternative habilitation therapies for children with cochlear implants.2,13 The randomized controlled trial randomized participants to receive 20 AVT sessions over 10 weeks or continue standard auditory training offered in Iran during the same period.13 The systematic review compared AVT to auditory-oral therapy, total communication, sign and spoken language, the bilingual-bicultural approach, and standard habilitation.2
The primary studies included in the systematic reviews varied in the duration of AVT for participants.2 Of the 4 relevant studies in the systematic review, 1 primary study in the review required participants to have a minimum of 6 months of AVT therapy (1 to 2 hours per week), and another required at least 10 months of AVT therapy.2 Another study in the review reported an average of 19.74 months of AVT for participants in the AVT group.2 The remaining included study did not report the duration of therapy for participants.2
The systematic review focused on language and speech development outcomes. A variety of tools were used in to measure the impact of AVT on speech and language development, including:2
Peabody Picture Vocabulary Test
Expressive Vocabulary Test
Passage Comprehension subtest of the Woodcock-Johnson Test of Achievement
Goldman-Fristoe Test of Articulation, Arizona Articulation Proficiency Scale
Preschool Language Scale, Fourth Edition
Reynell
Viborg Materialet
Consonant-Nucleus-Consonant
Bamford-Kowal-Bench.
Authors of the randomized controlled trial evaluated the effectiveness of AVT on executive function using the BRIEF-P (parent version), which includes 63 questions related to 5 subscales (i.e., inhibition, shifting, working memory, emotional control, and planning).13
Summary of Critical Appraisal
The strengths of the systematic review include the clear statement on research objectives and questions, risk of bias assessment using adequate tools, discussion of confounding factors, explicit reporting of funding for reviews, and lack of competing interests reported by review authors.2 However, it lacked a published protocol. Hence, we were unable to distinguish whether selective reporting or deviations from the protocol had occurred.2 In terms of risk for selection bias, the systematic review lacked justification of language restrictions for the study selection and the authors did not justify their decision to include randomized controlled trials and nonrandomized studies.2 They also limited the literature search to 1 database and it is unclear whether screening and data extraction was done in duplicate.2
The systematic review lacked important details about the quantitative findings of the included primary studies.2 The review authors narratively synthesized their findings.2 They noted significance (i.e., P values < 0.05), but they did not report specific P values across all studies.2 Hence, their reporting does not provide a comprehensive picture of the magnitude of the impact of AVT on children with cochlear implants compared to auditory-oral therapy, total communication, sign and spoken language, bilingual-bicultural, and standard habilitation.2
The strengths of the randomized controlled trial include the clear description of its research question and interventions, consideration of potential confounders in analysis, a randomized sample, use of proper statistical tests, and use of valid and reliable tools to measure outcomes.13 Given the nature of the interventions, blinding of participants was not possible. However, researchers were also not blinded to the intervention allocation of participants. They also recruited a sample size of 36 children from rehabilitation centres and preschools for children with hearing loss.13 The external validity of the study is a concern. It is unclear whether the participants or individuals ready to participate were representative of the source population. Additionally, the authors did not describe the “standard auditory training” that the source population and the control group received.13 It is unclear how generalizable these findings are to standard auditory training provided in other settings outside of Iran. The authors also did not report the proportion of the participants who completed and attended all AVT and standard auditory training during the 10-week period.13 It is unclear how attrition bias may have influenced the results of this study.
Additional details regarding the strengths and limitations of included publications are provided in Appendix 3.
Summary of Findings
Appendix 4 presents the main study findings.
Clinical Effectiveness of AVT
Language and Speech Development
The systematic review2 narratively reported that AVT resulted in better language and speech outcomes compared to standard habilitation, oral communication, total communication, and the bilingual-bicultural approach. However, the review authors provided limited quantitative data to support these conclusions.2 The same review did not find any significant differences in speech and language outcomes between AVT and sign and spoken language.2
When comparing AVT to auditory-oral therapy, the systematic review found mixed results.2 One relevant primary study included in the review found no significant difference between AVT and auditory-oral therapy.2 However, it is unclear if the study had the statistical power to detect significance with a sample size of 42.2 Another study in the systematic review found that AVT resulted in better outcomes compared to auditory-oral therapy in 2 of 3 measures, specifically Peabody Picture Vocabulary Test and Consonant-Nucleus-Consonant.2 However, the children in the AVT group were significantly older and had their cochlear implants longer compared to children in the auditory-oral group.2 Hence, it is unclear whether the children in the AVT group performed better than the children in the auditory-oral group because of AVT or because of the significant differences in chronological age and age at hearing aid implantation between the 2 groups.
Executive Function
The authors of the randomized controlled trial found that 10 weeks of AVT significantly improved overall executive function in children living in Iran.13 Children in the AVT group significantly exceeded improvements in executive function and measured subscales (i.e., inhibition, shifting, emotional control, working memory, and planning or organization) when compared to children in the standard auditory training group.13
Guidelines Regarding Therapy for Children With Hearing Loss
We did not identify relevant evidence-based guidelines regarding therapy for children with hearing loss that met our inclusion criteria. Therefore, no summary can be provided.
Limitations
External Validity
It is unclear how generalizable these findings are to children living in Canada. None of the studies was conducted in Canada and the systematic review provided a limited description of the interventions and settings of the interventions, especially for the comparators (i.e., standard habilitation, oral communication, total communication, auditory-oral, and bilingual-bicultural).2 The randomized controlled trial did not provide details regarding the comparator, specifically standard auditory training provided in Iran.13 It is unclear how these auditory driven therapies differ from auditory-driven therapies available in Canada.
Lack of Studies on Bone Conduction Hearing Devices and Conventional Hearing Aids
We only identified studies specific to children with cochlear implants.2,13 We did not identify relevant studies specific to children with bone conduction hearing devices and conventional hearing aids. Hence, we can not make any conclusions on the impact of AVT for these populations.
The Nature of AVT
A certified professional delivers sessions guided by the 10 principles of AVT.10 The principles have flexibility that allow those delivering the sessions to uphold these principles differently in their practice. Additionally, AVT requires considerable involvement from parents, guardians, or any adults that may interact with the child.8,9 Such confounding factors may be difficult to control or monitor in clinical studies.
Conclusions and Implications for Decision- or Policy-Making
This rapid review evaluated the literature regarding the clinical effectiveness of AVT compared to other forms of therapy for children with hearing loss. We identified a total of 2 relevant publications, specifically 1 systematic review2 and 1 randomized controlled trial.13 We also conducted a search for evidence-based guidelines but did not identify any relevant to our selection criteria. We also did not identify any literature that includes children using bone conduction hearing devices or regular hearing aids. We would need evidence on these populations to better inform the effectiveness of AVT.
Children undergoing AVT performed better than children receiving standard habilitation, oral communication, total communication, and the bilingual-bicultural approach for speech and language outcomes.2 The same systematic review included 2 studies with conflicting results regarding AVT versus auditory-oral therapy, with 1 study favouring AVT and 1 study reporting no significant difference between therapies.2 However, it is unclear to what extent the significant difference in chronological age and experience with cochlear implants impacted the results in the study that reported better outcomes in the AVT group than the auditory-oral group.2 For executive function, children undergoing AVT performed better than children in standard auditory training in Iran.13
We found the systematic review to have limitations in methodological quality related to a lack of a published protocol, high risk of selection bias, and inadequate reporting of quantitative findings, study characteristics, and results.2 The review authors reported concerns around the sample size of their included primary studies.2 Similarly, the randomized controlled recruited a total of 36 participants.13 It is also unclear whether findings are applicable in habilitation settings in Canada. None of the studies clearly described the alternative approaches evaluated against AVT, and it is unclear how they differ from or align with its delivery in Canada.2,13
AVT professionals uphold the 10 principles of AG Bell Academy for Listening and Spoken Language.10 However, how they uphold these principles in practice may vary. Researchers may find it difficult to control for these differences in clinical studies, and blinding of participants may not be possible given the nature of AVT. Other components of an EHDI program may also impact the development for children with hearing loss, such as age at diagnosis of hearing loss, age at implantation of cochlear implant(s), severity of hearing loss, number of implants, other diagnosed disability, duration of therapy, and parental involvement.2,3
However, no studies reported worsening outcomes because of AVT. The authors of the systematic review concluded that AVT can improve language and speech based on studies that evaluated the difference in performance pre and post intervention.2 Additionally, the randomized controlled trial found significant improvement from baseline in executive function for children after 10 weeks of AVT.13 Although it remains unclear if AVT is the most effective habilitation therapy, evidence suggests that AVT may minimize potential delays in language, speech, and executive function development for children using cochlear implants. This aligns with the findings of a systematic review by Noel et al. (2023),11 which concluded that AVT leads to progression in auditory skills for this population. Although this rapid review focused on studies that investigated AVT’s effectiveness relative to other habilitation therapies, the evidence regarding the progression from baseline in children undergoing AVT, especially for children with cochlear implants, may support considerations for its use.
Beyond clinical effectiveness, clinicians and decision-makers may consider other factors that impact the success of habilitation in practice. For instance, AVT requires parents or guardians to attend sessions and apply what they learn in the child’s daily life. Hence, clinicians may wish to consider the parent’s or guardian’s preferences and goals, in addition to the child’s, when deciding the best fit for habilitation therapy. Professionals also need to be certified by AG Bell Academy for Listening and Spoken Language to deliver AVT. From a systems perspective, decision-makers may wish to evaluate the potential barriers and facilitators for health professionals to obtain the appropriate certification, such as costs and time allocated for training.
References
1.Smith RJH, Gooi A. Hearing loss in children: Etiology. In: Post TW, ed. UpToDate. Waltham (MA): UpToDate; 2024: http://www.uptodate.com. Accessed 2024 Jun 18.
2.Binos P, Nirgianaki E, Psillas G. How effective is auditory-verbal therapy (AVT) for building language development of children with cochlear implants? A systematic review. Life (Basel). 2021;11(3):13. PubMed
3.Casoojee A, Kanji A, Khoza-Shangase K. Therapeutic approaches to early intervention in audiology: A systematic review. Int J Pediatr Otorhinolaryngol. 2021;150:110918. PubMed
4.Feder KP, Michaud D, McNamee J, Fitzpatrick E, Ramage-Morin P, Beauregard Y. Prevalence of hearing loss among a representative sample of canadian children and adolescents, 3 to 19 years of age. Ear Hear. 2017;38(1):7-20. PubMed
5.Khurana P, Cushing SL, Chakraborty PK, et al. Early hearing detection and intervention in Canada. Paediatr Child Health. 2021;26(3):141-144. PubMed
6.HealthLink BC. Hearing tests for infants and children. 2022: https://www.healthlinkbc.ca/healthlinkbc-files/hearing-tests-infants-and-children. Accessed 2024 Jun 18.
7.American Speech-Language Hearing Association. Who are speech-language pathlogists and what do they do? 2024: https://www.asha.org/public/who-are-speech-language-pathologists/. Accessed 2024 July 2.
8.Van Bogaert L, Machart L, Gerber S, Loevenbruck H, Vilain A, Consortium EULALIES. Speech rehabilitation in children with cochlear implants using a multisensory (French Cued Speech) or a hearing-focused (Auditory Verbal Therapy) approach. Front Hum Neurosci. 2023;17:1152516. PubMed
9.Brennan-Jones CG, White J, Rush RW, Law J. Auditory-verbal therapy for promoting spoken language development in children with permanent hearing impairments. Cochrane Database Syst Rev. 2014;2014(3):CD010100. PubMed
10.AG Bell Academy for Listening and Spoken Language. Principles of certified LSL specialists. https://agbellacademy.org/certification/principles-of-lsl-specialists/. Accessed 2024 Jun 19.
11.Noel A, Manikandan M, Kumar P. Efficacy of auditory verbal therapy in children with cochlear implantation based on auditory performance: A systematic review. Cochlear implants int. 2023;24(1):43-53. PubMed
12.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
13.Ashori M. Impact of auditory-verbal therapy on executive functions in children with cochlear implants. J Otol. 2022;17(3):130-135. PubMed
14.Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: A critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. PubMed
15.Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377-384. PubMed
16.Yanbay E, Hickson L, Scarinci N, Constantinescu G, Dettman SJ. Language outcomes for children with cochlear implants enrolled in different communication programs. Cochlear Implants Int. 2014;15(3):121-135. PubMed
Appendix 1: Detailed Methods and Selection of Included Studies
Note that this appendix has not been copy-edited.
Literature Search Methods
An information specialist conducted a literature search on key resources including MEDLINE, Embase, PsycINFO, the Cochrane Database of Systematic Reviews, the International HTA Database, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search approach was customized to retrieve a limited set of results, balancing comprehensiveness with relevancy. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. Search concepts were developed based on the elements of the research questions and selection criteria. The main search concepts were auditory verbal therapy (AVT) and assistive hearing devices. Search filters were applied to the assistive hearing devices search to limit retrieval to guidelines. Conference reviews and conference abstracts were excluded. The search was completed on June 27, 2024, and limited to English-language documents published since January 1, 2019.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1. Figure 1 presents the PRISMA12 flow chart of the study selection.
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, they were duplicate publications, or were published before 2019. Systematic reviews in which all relevant studies were captured in other more recent or more comprehensive systematic reviews were excluded. Primary studies retrieved by the search were excluded if they were captured in 1 or more included systematic reviews. Guidelines with unclear methodology were also excluded.
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the following tools as a guide: A MeaSurement Tool to Assess systematic Reviews 2 (AMSTAR 2)14 for systematic reviews, and the Downs and Black checklist15 for randomized and nonrandomized studies. Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Appendix 2: Characteristics of Included Publications
Note that this appendix has not been copy-edited.
Table 2: Characteristics of the Included Systematic Review by Binos et al. (2021)2
Study design, country, funding source | Number of primary studies included | Population characteristics | Intervention and comparators | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
SR evaluated the effectiveness of AVT in the speech and language development of children with cochlear implants. Country: Cyprus Funding source: No external funding | 8 peer-reviewed studies included in this SR. There are 4 studies relevant to this rapid review. | Children under 18 with cochlear implants. N = 756 (n = 414 for the 4 nonrandomized studies) | Intervention: AVT Comparator (for relevant studies only): Other habilitative approaches (auditory-oral, total communication, sign and spoken language, bilingual-bicultural, standard habilitation) | Outcomes: Speech and language development (Auditory perception and expressive, and receptive language) Follow-up: NR |
AVT = Auditory Verbal Therapy; NR = not reported; SR = systematic review.
Table 3: Characteristics of the Included Randomized Controlled Trial by Ashori (2022)13
Country, funding source | Recruitment, randomization, and study sample | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Country: Iran Funding source: Exceptional Education Organization (ID 97000 to 20223) | Participants were selected from what study authors reported as “deaf schools” and rehabilitation centres in Iran. The authors used simple random sampling method to randomize participants. N = 36 children (with bilateral profound hearing loss between 2 and 4 years of age) and their mothers | Sex: 50% male Race or ethnicity: 100% Iranian or Persian AVT, n = 18 Age, mean years (SD) = 3.11 (0.31) Control, n = 18 Age, mean years (SD) = 3.20 (0.29) No significant difference in mean hearing thresholds, cochlear implant-aided thresholds, and age of implementation of cochlear implants between study arms. Inclusion Criteria:
| Intervention: AVT consisting of 20 sessions over 10 weeks with standard auditory training Comparator: Standard auditory training intervention at a rehabilitation centre or deaf preschool in Iran | Outcomes: Executive function using BRIEF-P scores, inclusive of 5 subscales
Follow-up: pre intervention and post intervention (after 10 weeks) |
AVT = auditory verbal therapy; BRIEF-P = Behaviour Rating Inventory of Executive Function Preschool Version; RCT = randomized controlled trials.
Appendix 3: Critical Appraisal of Included Publications
Note that this appendix has not been copy-edited.
Table 4: Strengths and Limitations of Systematic Reviews Using AMSTAR 214
Strengths | Limitations |
|---|---|
Binos et al. (2021)2 | |
The review authors reported:
The authors evaluated the studies using the Critical Appraisal of Treatment Evidence (CATE) checklist. The review authors accounted for the risk of bias and heterogeneity when discussing the results of studies and the review. | The report lacked an explicit statement regarding established methods before the conduct of the review. The review authors did not justify selection criteria for study designs and language restrictions. The search strategy involved 1 database (i.e., PubMed). It is unclear whether study selection and data extraction were performed in duplicate. The review authors did not report quantitative results of included primary studies. The review authors did not report on the sources of funding for individual studies. |
AMSTAR 2 = A MeaSurement Tool to Assess systematic Reviews 2; ISPOR = International Society for Pharmacoeconomics and Outcomes Research; PICO = population, intervention, comparator, outcome.
Table 5: Strengths and Limitations of Clinical Studies Using the Downs and Black Checklist15
Strengths | Limitations |
|---|---|
Ashori (2022)13 | |
The authors clearly described the objective, intervention, main outcomes, inclusion criteria, and exclusion criteria of the study. They also compared a list of potential confounders between intervention and control groups. Further, the authors used a statistical test used (i.e., ANCOVA) that accounted for the preintervention (baseline) scores from the tool to measure outcomes. The authors used a simple random sampling methods to recruit participants from rehabilitation centres or deaf schools. The authors reported simple descriptive statistics and the variability of data pre and post intervention for both study arms. The authors used an appropriate statistical test (i.e., ANCOVA) to assess the main outcomes. P values were reported in the publication. The authors did not conduct any unplanned analysis. The authors recruited participants in both study arms from the same population. The intervention and control groups had the same follow-up period. The authors used valid and reliable tool to measure outcomes. The authors declared no conflicts of interest. | The study recruited 36 participants for the study. It is unclear if participants were representative of the population they were recruited from. Additionally, it is unclear if the staff, facilities, and treatments are representative of the source population. It is unclear if individuals who were prepared to participate representative of the entire population from which they were recruited. It is unclear if any participants were lost to follow up. The authors did not report on the proportion of participants that completed 10 weeks of AVT or standard auditory training The authors did not describe the auditory training the control group received. The authors did not report on potential adverse events. |
ANCOVA = analysis of covariance; AVT = auditory verbal therapy; NA = not applicable; NR = not reported.
Appendix 4: Main Study Findings
Note that this appendix has not been copy-edited.
Table 6: Summary of Findings by Outcome — Speech and Language Outcomes from Studies Included in the Systematic Review by Binos and Colleagues2
Author (Year) and study design of the included study, as cited by the systematic review2 | Method of measurement | Time point | Result | P value |
|---|---|---|---|---|
AVT vs. standard habilitation | ||||
Retrospective study by Percy-Smith et al. (2022). | PPVT-4, Reynell, and Viborg materials | NR | Children enrolled in AVT significantly outperformed in every test. | NR |
AVT vs. oral communication | ||||
Retrospective study by Thomas and Zwolan (2019). | PPVT, Expressive vocabulary test, WJPV, GFT-AAPS | Over a 7-year period in 6 different phases (i.e., yearly from 2 to 7 years after implantation) | The children enrolled in AVT would significantly outperform children using oral communication in every measure and at every test interval. | < 0.05 |
AVT vs. total communication | ||||
Retrospective study by Thomas and Zwolan (2019). | PPVT, Expressive vocabulary test, WJPV, GFT-AAPS | Over a 7-year period in 6 different phases (i.e., yearly from 2 to 7 years after implantation) | The children enrolled in AVT significantly outperformed at each measure and at every test interval. | < 0.05 |
AVT vs. auditory-oral | ||||
Retrospective study by Yanbay et al. (2014). | PPVT, PLS-4, IRSAD, FPRS | NR | No significant differences in language outcomes between groups.16 | NR |
Retrospective study by Dettman et al. (2013). | PPVT | NR | The AVT group performed better than children in the AO. | NR |
CNC | NR | The AVT group performed better than the AO group. | NR | |
BKB | NR | The AVT and auditory-oral groups did not differ in performance. | NR | |
AVT vs. sign and spoken language | ||||
Retrospective study by Yanbay et al. (2014) | PPVT, PLS-4, IRSAD, FPRS | NR | No significant differences in language outcomes between groups.16 | NR |
AVT vs. bilingual-bicultural | ||||
Retrospective study by Dettman et al. (2013). | PPVT, CNC, BKB | NR | The AVT group outperformed the bilingual-bicultural group in all measures of speech perception. | NR |
AVT = auditory verbal therapy; NA = not applicable; NR = not reported; PLS-4 = Preschool language scale-4; PPVT = Peabody Picture Vocabulary Test.
Note: We collated the results as reported by the systematic review by Binos et al. (2021).2 We did not review or appraise the primary studies from which Binos and colleagues2 collected these results.
Table 7: Summary of Findings by Outcome — Executive Function from the Randomized Controlled Trial by Ashori (2022)13
BRIEF-P and Subscalesa | AVT vs. Standard Auditory Training | |
|---|---|---|
F value | P value | |
Executive Function | 56.65 | 0.001 |
Executive Function Subscalesb | 15.08 | 0.001 |
BRIEF-P = Behaviour Rating Inventory of Executive Function Preschool version; NA = not applicable; NR = not reported.
Note: The authors compared postintervention scores of the interventions using ANCOVA for executive function and MANCOVA for the subscales. They used the preintervention scores as covariates for the analysis. Hence, the F value indicates the difference in postintervention scores while accounting for the difference in preintervention scores.
aBRIEF-P is an assessment used to evaluate everyday behaviour of children ages 2 to 6 at home or in preschool settings.13 The authors of this study used the parent version.13
bBRIEF-P subscales of executive function include inhibition, shifting, emotional control, working memory, and planning/organization.
Appendix 5: The 10 Principles by Alexander Graham Bell Academy for Listening and Spoken Language
Note that this appendix has not been copy-edited.
We retrieved and listed these principles as reported on Alexander Graham Bell Academy for Listening and Spoken Language website.10
“The Principles of Certified LSLS Auditory-Verbal Therapists (LSLS Cert. AVT)
Promote early diagnosis of hearing loss in newborns, infants, toddlers, and young children, followed by immediate audiologic management and auditory-verbal therapy.
Recommend immediate assessment and use of appropriate, state-of-the-art hearing technology to obtain maximum benefits of auditory stimulation.
Guide and coach parents to help their child use hearing as the primary sensory modality in developing listening and spoken language.
Guide and coach parents to become the primary facilitators of their child’s listening and spoken language development through active consistent participation in individualized auditory-verbal therapy.
Guide and coach parents to create environments that support listening for the acquisition of spoken language throughout the child’s daily activities.
Guide and coach parents to help their child integrate listening and spoken language into all aspects of the child’s life.
Guide and coach parents to use natural developmental patterns of audition, speech, language, cognition, and communication.
Guide and coach parents to help their child self-monitor spoken language through listening.
Administer ongoing formal and informal diagnostic assessments to develop individualized auditory-verbal treatment plans, to monitor progress and to evaluate the effectiveness of the plans for the child and family.
Promote education in regular schools with peers who have typical hearing and with appropriate services from early childhood onwards.
*An Auditory-Verbal Practice requires all 10 principles.
The term “parents” also includes grandparents, relatives, guardians, and any caregivers who interact with the child.”
Appendix 6: References of Potential Interest
Note that this appendix has not been copy-edited.
Nonrandomized Studies
Irrelevant Comparator
Sarker MZ, Rahim MZ, Patawary KU, et al. Functional and speech outcome of unilaterally cochlear implanted children after 1 year of implantation in NIENT: A retrospective study. Mymensingh Med J. 2023;32(1):213-220. PubMed
Percy-Smith L, Wischmann S, Josvassen JL, Schioth C, Caye-Thomasen P. Language development for the new generation of children with hearing impairment. J Clin Med. 2021;10(11):27. PubMed
Estrella-Castillo DF, Rubio-Zapata H, Gómez-de-Regil L. Auditory perception of Mexican children with profound bilateral hearing loss receiving auditory verbal therapy. Child Lang Teach Ther. 2020;37(1):5-17.
Haddadi Aval M, Abdollahi F, Jafarzadeh S. Auditory rehabilitation based on auditory verbal therapy approach on children with bilateral sensory-neural hearing loss. Aud Vestib Res. 2020;29(3):172-177.
Alternative Comparator
Tejeda-Franco CD, Valadez-Jimenez VM, Hernandez-Lopez X, et al. Hearing aid use and auditory verbal therapy improve voice quality of deaf children. J Voice. 2020;34(2):301.e307-301.e311. PubMed
Threshold Estimation
Jafarzadeh S. The relationship between hearing thresholds estimation and results of auditory-verbal therapy in children with bilateral congenital severe to profound sensorineural hearing loss. Journal of Rehabilitation Sciences & Research. 2021;8(2):86-89.
Guidelines and Recommendations
Unclear Methodology
Auditory Verbal UK. Auditory verbal therapy position paper. 2023; https://www.avuk.org/auditory-verbal-therapy-position-paper. Accessed 2024 May 18.
Park LR, Griffin AM, Sladen DP, Neumann S, Young NM. American Cochlear Implant Alliance Task Force guidelines for clinical assessment and management of cochlear implantation in children with single-sided deafness. Ear Hear. 2022;43(2):255-267. PubMed
Alzahrani MA, Aldajani NF, Alghamdi SA. Guidelines for cochlear implantation in Saudi Arabia. Saudi Med J. 2021;42(12):1265-1271. PubMed
Gustafson SJ, Corbin NE. Pediatric hearing loss guidelines and consensus statements: Where do we stand? Otolaryngol Clin North Am. 2021;54(6):1129-1142. PubMed
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up to date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for noncommercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca