CADTH Health Technology Review
Nabilone for Chronic Non-Cancer Pain
Rapid Review
Key Messages
What Is the Issue?
Chronic pain is pain that lasts beyond 3 months. Chronic non-cancer pain conditions include osteoarthritis, low back pain, musculoskeletal pain, fibromyalgia, and neuropathic pain. Approximately 1 in 5 people in Canada live with chronic pain.
Nabilone (a cannabinoid) is indicated for the management of severe nausea and vomiting associated with cancer chemotherapy. Nabilone is also used in the management of chronic non-cancer pain. It is important to understand the potential benefits and harms of nabilone in people living with chronic non-cancer pain to support decision-making.
What Did We Do?
We sought to identify, summarize, and critically appraise literature comparing the clinical effectiveness of nabilone and placebo or alternative pharmacological options. We also searched for evidence-based guidelines that provide recommendations about the use of nabilone for the treatment of chronic non-cancer pain.
We searched key resources, including journal citation databases, and conducted a focused internet search for relevant evidence published since 2015. One reviewer screened articles for inclusion based on predefined criteria, critically appraised the included studies, and narratively summarized the findings.
What Did We Find?
We found 1 overview of reviews and 2 systematic reviews that assessed the clinical efficacy and safety of nabilone for the treatment of chronic non-cancer pain.
The evidence on the clinical efficacy of nabilone was mixed with some studies reporting an improvement in pain in those treated with nabilone versus placebo or active comparators and other studies reporting no difference between groups. Adverse events were more common in people living with chronic non-cancer pain who received nabilone than those who received placebo, ibuprofen, or amitriptyline. Adverse events were more common in those who received dihydrocodeine or gabapentin than nabilone.
It is uncertain if nabilone is an effective treatment for people living with chronic non-cancer pain due to the varied results and methodological limitations of the included studies.
We found 1 guideline that included a recommendation specific to nabilone and 2 guidelines that included recommendations on the use of cannabinoids in general. One guideline recommends against the use of nabilone for chronic pain, 1 guideline recommends offering a trial of non-inhaled cannabinoids (such as nabilone) for people living with chronic pain, and 1 guideline suggests cannabinoids be avoided in people with osteoarthritis and low back pain and discussed with people with neuropathic pain.
What Does This Mean?
Due to the uncertainty of the clinical evidence, decision-makers may wish to consider other factors such as costs, equity, and patient values and preferences when making decisions on the use of nabilone for people living with chronic non-cancer pain.
Future high-quality, longer-term (e.g., RCT with follow-up studies) studies are needed to understand the efficacy and safety of nabilone for the treatment of people living with chronic non-cancer pain.
Abbreviations
BMJ
British Medical Journal
CB1
cannabinoid receptor type 1
CB2
cannabinoid receptor type 2
NICE
National Institute for Health and Care Excellence
PEER
Patients Experience Evidence Research
RCT
randomized controlled trial
Context and Policy Issues
What Is Chronic Non-Cancer Pain?
Approximately 1 in 5 people in Canada, or an estimated 7.6 million people, live with chronic pain.1Chronic non-cancer pain is typically defined as pain that lasts for more than 3 months or beyond the time of normal tissue healing.2 Chronic pain conditions can include (but are not limited to) osteoarthritis, low back pain, musculoskeletal pain, fibromyalgia, and neuropathic pain.2 Pain can be described in terms of 3 main biological mechanisms (nociceptive, neuropathic, and nociplastic).3 Nociceptive pain arises from actual or threatened tissue damage resulting from disease, injury, or inflammation.3,4 Neuropathic pain results from damaged or dysfunctional nerves.4 Nociplastic pain is altered pain perception without clear evidence of direct damage to tissue.4 Chronic pain can interfere with a person’s ability to perform daily activities and develop meaningful relationships with family and friends.5 Living with chronic pain can negatively impact sleep, physical functioning, and mental health.1 Chronic pain is largely invisible which can lead those affected to feel disbelieved and stigmatized.1
What Is the Current Practice?
Chronic pain is difficult to cure and treatment is geared toward optimizing pain management to improve functioning and reduce suffering.3 There are a wide range of possible interventions for the treatment and management of chronic pain. These include pharmacological interventions (e.g., nonsteroidal anti-inflammatory drugs, acetaminophen, opioids), psychological interventions (e.g., individual or group psychotherapy, cognitive behavioural therapy, acceptance and commitment therapy), physical interventions (e.g., physical activity, activity modification, graded motor imagery), medical device or procedural interventions (e.g., deep brain stimulation, steroid injection, transcutaneous electrical nerve stimulation), practitioner administered/ manual therapy (e.g., acupuncture, massage therapy, osteopathic treatments), and self-management interventions (e.g., life skills and self-efficacy programs, support groups, dietary practices).3 The management of chronic non-cancer pain involves a combination of different treatment options through an individualized and multidisciplinary approach.4
What Is Nabilone?
Cannabinoids are the pharmacologically active components of cannabis.6 Naturally occurring cannabinoids found in the cannabis plant include delta9-tetrahydrocannabinol (THC) and cannabidiol (CBD).6 Synthetic cannabinoids (those made in a laboratory) include dronabinol and nabilone.6 There are 2 primary types of receptors for cannabinoids in the human body: cannabinoid receptors type 1 (CB1) and cannabinoid receptors type 2 (CB2).7 CB1 receptors are located in the centers of the brain involved in pain modulation, the spinal cord pathways that perceive pain, and peripheral nerves (nerves located outside the brain and spinal cord).7 CB2 receptors are located in the immune and hematological (blood-forming) systems and are involved in decreasing inflammation.7 Nabilone is a synthetic derivative of THC which binds to and partially activates both CB1 and CB2 receptors.6,7 In Canada, nabilone is indicated for the management of severe nausea and vomiting associated with cancer chemotherapy.8 The usual dosage for nabilone is 1 mg or 2 mg twice a day, and it is available as a capsule intended for oral administration.8
Why Is It Important to Do This Review?
Opioid medications are sometimes prescribed to people living with chronic non-cancer pain; however, there are potential harms associated with their use.9 Lack of access to non-opioid options to treat pain is 1 of several factors that has led to a significant increase in opioid-related harms and deaths over the past 20 years.1 The 2017 Canadian Guideline for Opioids for Chronic Non-Cancer Pain recommends optimizing non-opioid pharmacotherapy and non-pharmacological therapy rather than a trial of opioids for people living with chronic non-cancer pain.10 There are some people living with chronic non-cancer pain who may benefit from treatment with opioids.3 However, due to the harms associated with opioid use, there is a need for additional effective pharmacological options.
A previous report on the use of nabilone for the treatment of chronic pain was published in 2017 and updated in 2018.11,12 Several limitations to the studies included in the reports suggested that larger and longer prospective trials are needed to confirm the clinical effectiveness and safety of nabilone in people living with chronic pain.11,12
Objective
To support decision-making regarding the use of nabilone, we prepared this rapid review to summarize and critically appraise clinical studies and evidence-based guidelines on its use for people living with chronic non-cancer pain.
Research Questions
What is the clinical efficacy and safety of nabilone for the treatment of chronic non-cancer pain?
What are the evidence-based guidelines regarding the use of nabilone for the treatment of chronic non-cancer pain?
Methods
Literature Search Methods
An information specialist conducted a literature search on key resources including MEDLINE, the Cochrane Database of Systematic Reviews, the International HTA Database, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search approach was customized to retrieve a limited set of results, balancing comprehensiveness with relevancy. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. Search concepts were developed based on the elements of the research questions and selection criteria. The main search concepts were nabilone and chronic, non-cancer pain. No filters were applied to limit the retrieval by study type. The search was completed on April 2, 2024, and limited to English-language documents published since January 1, 2015.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed, and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
|---|---|
Population | Adults with chronic non-cancer pain |
Intervention | Nabilone |
Comparator | Q1: Active pharmacological treatments, placebo Q2: NA |
Outcomes | Q1: Clinical effectiveness and benefits (e.g., reduction in pain, pain relief, patient satisfaction) and safety (e.g., harms, adverse events, misuse) Q2: Guidelines regarding the use of nabilone for the treatment of chronic non-cancer pain |
Study designs | Health technology assessments, systematic reviews, randomized controlled trials, nonrandomized studies, and evidence-based guidelines |
NA = not applicable.
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, or they were duplicate publications. Articles published before 2018 were excluded due to the large number of recent systematic reviews. Systematic reviews in which all relevant studies were captured in other more recent or more comprehensive systematic reviews were excluded. Primary studies retrieved by the search were excluded if they were captured in 1 or more included systematic reviews. Guidelines with unclear methodology were also excluded.
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the following tools as a guide: A MeaSurement Tool to Assess systematic Reviews 2 (AMSTAR 2)13 for systematic reviews, and the Appraisal of Guidelines for Research and Evaluation (AGREE) II instrument14 for guidelines. Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Summary of Evidence
Quantity of Research Available
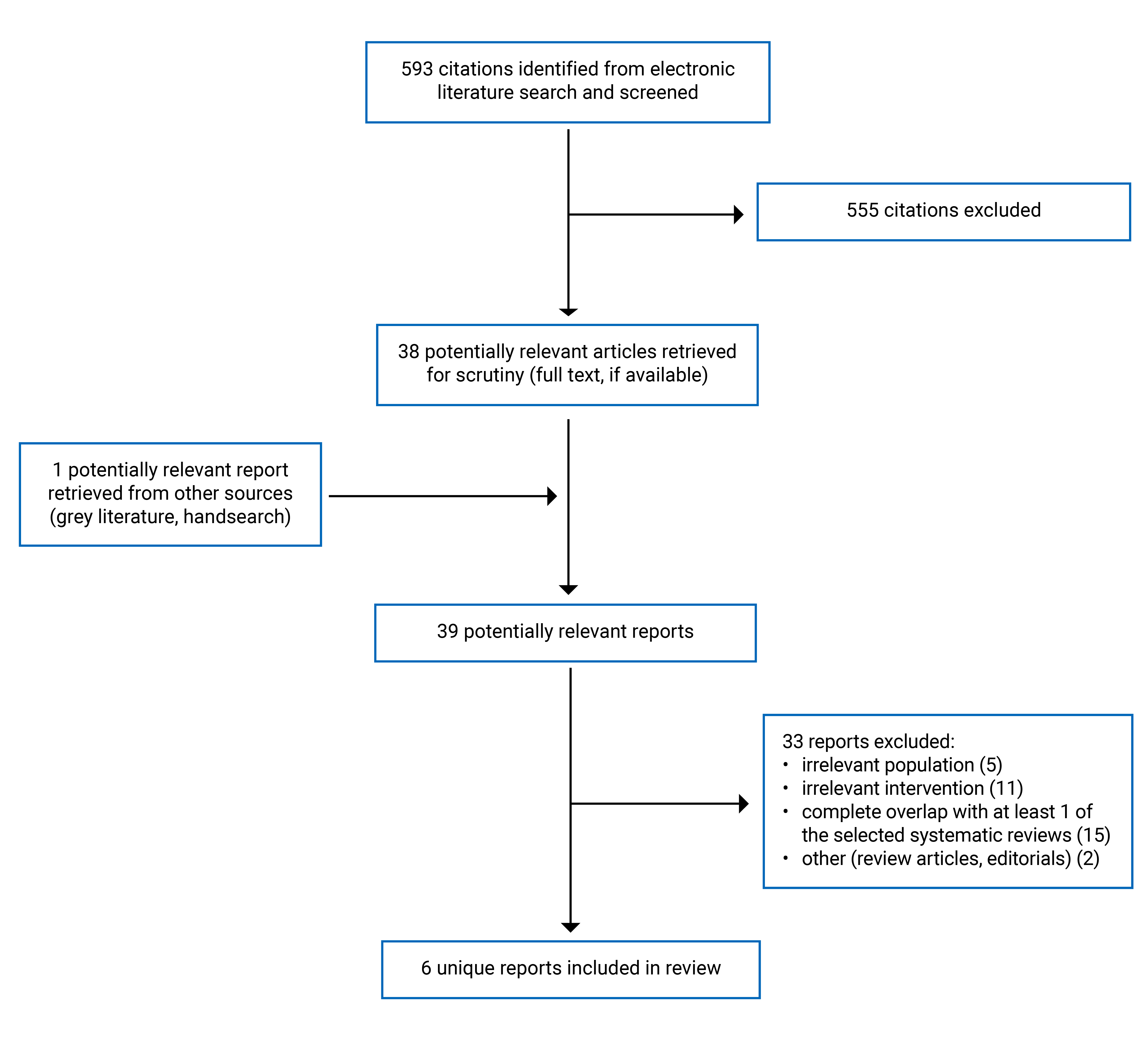
A total of 593 citations were identified in the literature search. Following screening of titles and abstracts, 555 citations were excluded and 38 potentially relevant reports from the electronic search were retrieved for full-text review. One potentially relevant publication was retrieved from the grey literature search for full-text review. Of these potentially relevant articles, 33 publications were excluded for various reasons, and 6 publications met the inclusion criteria and were included in this report. These comprised 1 overview of reviews, 2 systematic reviews, and 3 evidence-based guidelines. Appendix 1 presents the PRISMA15 flow chart of the study selection. Additional references of potential interest are provided in Appendix 6.
Summary of Study Characteristics
In total, 1 overview of reviews,16 2 systematic reviews,17,18 and 3 evidence-based guidelines19-21 were included in this report. Both systematic reviews17,18 included meta-analyses; however, the research protocol differed from the present report. Therefore, the results of the meta-analyses are not described in this report. The results from the relevant individual studies included in the systematic reviews are reported instead.
The overview of reviews and 2 systematic reviews had broader inclusion criteria than the present report. Specifically, all the reviews included studies of cannabis or cannabinoids other than nabilone. Additionally, the overview by Riera et al. (2022)16 and the systematic review by Bilbao and Spanagel (2022)17 included patients with any health condition, and the systematic review by Zeraatkar et al. (2022)18 included people with cancer pain. Only the characteristics and results of the subset of relevant studies are described in this report.
Two of the guidelines19,20 included recommendations on the use of cannabinoids for chronic non-cancer pain; however, the recommendations were not specific to nabilone.
Additional details regarding the characteristics of included publications are provided in Appendix 2.
Study Design
The overview of reviews by Riera et al. (2022)16 included 68 systematic reviews of randomized controlled trials (RCTs), 4 of which are relevant to the present report. The search was conducted on December 14, 2020 and no restrictions were imposed based on date of publication.16 The systematic review by Bilbao and Spanagel (2022)17 included 152 RCTs, 10 of which are relevant to the present report. The search included all studies published until October 2021.17 The systematic review by Zeraatkar et al. (2022)18 included 39 nonrandomized studies in total, 1 longitudinal study is relevant to the present report. The search included all studies published up to April 1, 2020.18
The overview of reviews16 and 2 systematic reviews17,18 had overlap in their included primary studies. Eight primary studies were included in more than 1 review. A citation matrix depicting the overlap between the included reviews is provided in Appendix 5.
The Patients Experience Evidence Research (PEER) guideline was published in 2022.19To inform the guideline, 3 systematic reviews were conducted to identify relevant RCTs, and supplemental questions were addressed through a rapid review process.19 The guideline committee developed the recommendations through consensus.19 The British Medical Journal (BMJ) guideline was published in 2021.20 Four systematic reviews were conducted for the BMJ guideline to identify the evidence on benefits and harms as well as patient values and preferences.20 The guideline panel met to discuss the evidence and develop the recommendation.20 The National Institute for Health and Care Excellence (NICE) guideline was published in 2019 and updated in 2021.21 A systematic review was conducted for the NICE guideline to identify relevant RCTs and systematic reviews of RCTs.21 The guideline committee discussed the evidence and reached decisions through an informal consensus process.21 All 3 guidelines19-21 used the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) methodology to assess the quality of evidence as being high, moderate, low, or very low. All the guidelines rated recommendations as being either strong or weak.19-21
Country of Origin
The overview of reviews was conducted by authors from Brazil.16 The systematic reviews were conducted by authors from Germany17 and Canada.18
The PEER guideline is intended for use in Canada.19 The NICE guideline is intended for use in the UK.21 The BMJ was developed by an international guideline panel that included individuals from Canada, Belgium, China, Norway, Switzerland, Australia, and the US.20
Patient Population
The relevant populations included in the overview of reviews were adults with chronic headache related to analgesic overuse, chronic spinal pain, or fibromyalgia.16 The relevant population in the systematic review by Bilbao and Spanagel (2022)17 was adults with chronic non-cancer pain (included people with Parkinson disease, Alzheimer disease, multiple sclerosis, neuropathic pain, fibromyalgia, upper motor neuron syndrome, and medication overuse headache). The relevant population in the systematic review by Zeraatkar et al. (2022)18 was adults with peripheral neuropathic pain.
The intended users of the PEER guideline19 are primary care clinicians and patients, and the target population is people living with chronic low back, osteoarthritic, and neuropathic pain. The intended users of the BMJ guideline20 are clinicians and patients, and the target population is adults and children living with moderate to severe chronic pain mechanisms as well as cancer-related chronic pain. The intended users of the NICE guideline21 are health care professionals and people taking cannabis-based medicinal products, their families and carers. The target population is people with intractable nausea and vomiting, chronic pain, spasticity, and severe treatment-resistant epilepsy.21 The target populations of the BMJ and NICE guidelines are broader than the current report. Only recommendations regarding adults with chronic non-cancer pain are summarized in this report.
Interventions and Comparators
The relevant intervention in all the included reviews was nabilone with dosages that ranged from 0.25 mg to 4 mg per day.16-18 The comparators included placebo, amitriptyline, ibuprofen, dihydrocodeine, and gabapentin.16-18
The PEER guideline19 considered physical activity, psychological interventions, and pharmacological interventions (including cannabinoids). The BMJ guideline20 considered medical non-inhaled cannabis or cannabinoids. The NICE guideline21 considered cannabis-based medicinal products.
Outcomes
The overview of reviews by Riera et al. (2022)16 assessed pain and quality of life. Most of the systematic reviews included in the overview assessed pain using the visual analogue scale however, 1 of the systematic reviews assessed pain intensity, but did not report the scale or measurement tool used.16 One of the systematic reviews included in the overview assessed quality of life using the short form 36 questionnaire; however, 2 other systematic reviews did not report the measurement tool used.16 The systematic review by Bilbao and Spanagel (2022)17 assessed chronic pain using a variety of measurement tools including visual analogue scale, numerical rating scale, Neuropathic Pain Symptom Inventory, Pain Treatment Satisfaction Scale, headache index, Pain Assessment in Alzheimer Disease, King’s Parkinson Disease Pain Scale, McGill Pain Questionnaire, and 11-point box scale. The overview of reviews and both systematic reviews also assessed adverse events.16-18
The outcomes considered in the PEER guideline19 were responder analysis for chronic pain and safety. The BMJ guideline20 considered pain relief, physical, emotional, role, and social functioning, sleep quality, opioid substitution, and adverse events. The NICE guideline21 considered pain relief, reduction in analgesics, pain intensity, functional impairment, global impression of change, quality of life, adverse events, substance abuse (language retained from the original source), and misuse or diversion.
Summary of Critical Appraisal
Additional details regarding the strengths and limitations of included publications are provided in Appendix 3.
Systematic Reviews
The overview of reviews and systematic reviews all had clear objectives. The overview of reviews by Riera et al. (2022)16 and the systematic review by Zeraatkar et al. (2022)18 had clear study eligibility criteria. The inclusion criteria for the systematic review by Bilbao and Spanagel (2022)17 included components of population, intervention, and outcomes; however, eligible comparators were not specified. The review methods for the overview of reviews by Riera et al. (2022)16 and the systematic review by Bilbao and Spanagel (2022)17 were established before conducting the reviews and the protocols were registered. However, the systematic review by Bilbao and Spanagel (2022)17 had several deviations from the published protocol (changes to eligible interventions and comparators, change to date restriction for literature search, protocol did not include a plan for meta-analysis) and the authors did not provide a discussion or justification for these deviations. The systematic review by Zeraatkar et al. (2022)18 did not include a statement on whether the review methods were established before conducting the review, which has the potential to introduce bias if the review methods were adjusted after the review had begun. All the reviews used comprehensive literature search methods including searching in multiple databases and handsearching the reference lists of included articles.16-18 Additionally, the full search strategy was provided in all the reviews, which increases its reproducibility.16-18
Study selection was performed independently by 2 reviewers in all the reviews, reducing the risk of bias in this domain. The list of excluded studies and reasons for exclusion was provided in all 3 reviews.16-18 Data extraction was performed independently by 2 reviewers in 2 of the reviews.16,18 In the systematic review by Bilbao and Spanagel (2022)17 the authors do not state whether data extraction was performed in duplicate. Performing data extraction in duplicate reduces the likelihood of inconsistencies. The included studies were described in adequate detail in the reviews by Riera et al. (2022)16 and Zeraatkar et al. (2022).18 In the systematic review by Bilbao and Spanagel (2022)17 the populations, interventions, outcomes, and designs of the included studies were well described, however, the dosages for comparators were not reported. The risk of bias of included studies was assessed in duplicate using appropriate methods in all the reviews.16-18 The authors declared that they had no conflicts of interest and reported whether funding was received and the funding source in all 3 reviews.16-18
Guidelines
The objectives, health questions covered by the guidelines, and target populations were clearly described in all 3 guidelines.19-21 The target users of the NICE guideline21 were clearly defined however, in the PEER and BMJ guidelines19,20 the target users were not explicitly defined. The guideline development groups for all 3 guidelines included individuals from all relevant professional groups.19-21 The views and preferences of the target populations were sought in all 3 guidelines.19-21 All the guidelines used systematic methods to search for evidence. The selection criteria were clearly described and the evidence quality was assessed in all the guidelines.19-21 All 3 guidelines described the methods for formulating the recommendations.19-21 All the guidelines included a discussion of the rationale behind the recommendations, and there was an explicit link between the supporting evidence and recommendations.19-21 All the guidelines were externally reviewed by experts before publication.19-21 All the recommendations are specific and unambiguous and easily identifiable in all 3 guidelines.19-21 The PEER and BMJ guidelines19,20 included statements about their sources of funding; however, they did not include statements as to whether the funders had influence on the content of the guidelines. The NICE guideline21 did not include a statement about funding. The competing interests of the guideline group members were recorded and addressed in all 3 guidelines.19-21
Summary of Findings
Appendix 4 presents the main study findings.
Clinical Effectiveness of Nabilone
There was some overlap in the primary studies that were included in the overview of reviews and systematic reviews; therefore, to avoid duplication of results, outcome data from an individual primary study are only reported once.
Pain
One overview of reviews16 and 1 systematic review17 reported mixed evidence on the effectiveness of nabilone for the treatment of chronic non-cancer pain. For comparisons of nabilone versus placebo, there was no significant difference in pain between groups for people with chronic spinal pain (1 RCT), Parkinson disease (1 RCT), or Alzheimer disease (1 RCT).16,17 There were statistically significant decreases in pain in favour of nabilone versus placebo in people with multiple sclerosis (1 RCT), diabetic peripheral neuropathic pain (1RCT), fibromyalgia (1 RCT), neuropathic pain (1 RCT), and upper motor neuron syndrome (1 RCT).17 There was a statistically significant decrease in pain favouring nabilone versus ibuprofen in people with medication overuse headaches (1 RCT).17 There was no significant difference in pain between nabilone and amitriptyline in people with fibromyalgia (1 RCT).17 There was a statistically significant decrease in pain in favour of dihydrocodeine versus nabilone in people with neuropathic pain (1 RCT).17 The confidence intervals for many of the comparisons were wide, indicating imprecision in the effect estimates. This is likely due to the sample sizes of many of the RCTs included in the reviews.
Quality of Life
One overview of reviews reported mixed evidence on the effectiveness of nabilone on quality of life in people with chronic non-cancer pain.16 There was a statistically significant benefit of nabilone versus ibuprofen on quality of life in people with chronic headache related to analgesic overuse (1 RCT).16 There was no difference in quality of life between people with fibromyalgia who received nabilone versus amitriptyline (1 RCT).16 There was no difference in quality of life in people with chronic spinal pain who received nabilone versus placebo (1 RCT).16
Safety
One overview of reviews16 and 2 systematic reviews17,18 reported evidence on the safety of nabilone for the treatment of people with chronic non-cancer pain. Adverse events were more frequent in people with chronic non-cancer pain who received nabilone than those who received placebo (6 RCTs), ibuprofen (1 RCT), or amitriptyline (1 RCT).17 Adverse events were more frequent in people with chronic non-cancer pain treated with dihydrocodeine (1 RCT) and gabapentin (1 longitudinal study) than nabilone.17,18 Adverse events causing discontinuation were more frequent in people with peripheral neuropathic pain who received gabapentin than nabilone (1 longitudinal study).18 There was 1 serious adverse event (fall and fracture due to dizziness) in a participant with chronic spinal pain who received nabilone (1 RCT).16 There were no serious adverse events in people with neuropathic pain who received either nabilone or gabapentin (1 longitudinal study).18
Guidelines Regarding the Use of Nabilone
Three guidelines were identified that included recommendations on the use of cannabinoids for the treatment of chronic non-cancer pain.19-21
The PEER guideline19 suggests that the harms likely exceed the benefits for cannabinoids and they should be avoided in most patients with osteoarthritis and low back pain (weak recommendation based on very low-quality evidence). The PEER guideline19 suggests that cannabinoids have unclear benefit in people with neuropathic pain and that they could be discussed with patients when interventions with clear evidence of benefit have already been considered (weak recommendation based on very low-quality evidence). The BMJ guideline20 recommends that a trial of non-inhaled cannabinoids, in addition to standard care, be offered for people living with chronic pain (weak recommendation based on moderate to high-quality evidence). The NICE guideline21 does not recommend nabilone for the management of chronic pain in adults (strong recommendation based on low-quality evidence).
Limitations
The relevant primary studies summarized in the included overview of reviews and systematic reviews were of variable methodological quality. In the overview of reviews by Riera et al. (2022)16 the authors rated 1 of the relevant systematic reviews as low quality and the other 3 as moderate quality. The authors of the systematic review by Bilbao and Spanagel (2022)17 rated the relevant RCTs as being from low to high risk of bias. The overall certainty of the evidence for chronic pain was judged by the systematic review authors to be low for nabilone versus placebo and very low for nabilone versus active comparators.17 Additionally, the confidence intervals for many of the estimates for pain outcomes were wide, indicating imprecision in the estimates. The authors of the Zeraatkar et al. (2022)18 systematic review judged the outcomes from the relevant longitudinal study to be very low certainty due to the risk of bias and imprecision. An additional limitation is the relatively short follow-up periods in many of the relevant studies included in the reviews. Aside from the longitudinal study which had a follow-up of 24 weeks, the other relevant primary studies included in the reviews had shorter follow-up periods ranging from 2 to 9 weeks.16-18
Two of the identified guidelines included recommendations for cannabinoids in general that were not specific to nabilone.19,20 There may be differences in the efficacy and safety profiles of nabilone versus other cannabinoids in people living with chronic non-cancer pain. Therefore, some decision-makers may find guidelines that consider the evidence and make recommendations separately for different cannabinoids more useful.
Conclusions and Implications for Decision- or Policy-Making
This report comprised 1 overview of reviews,16 2 systematic reviews,17,18 and 3 evidence-based guidelines19-21 on nabilone for the treatment of chronic non-cancer pain.
Overall, evidence from the overview of reviews and systematic review that reported on pain outcomes was mixed. When nabilone was compared to placebo for pain outcomes, some of the primary studies included in the reviews found no difference between groups (3 RCTs) and other studies found a statistically significant difference in favour of nabilone (5 RCTs).16,17 When nabilone was compared to active comparators for pain outcomes, there was no difference versus amitriptyline (1 RCT), a statistically significant difference in favour of nabilone versus ibuprofen (1 RCT), and a statistically significant difference in favour of dihydrocodeine versus nabilone (1 RCT).17 Evidence on the effect of nabilone on quality of life in people with chronic non-cancer pain was limited and mixed. There was a statistically significant benefit of nabilone versus ibuprofen for quality of life (1 RCT); however, there were no differences in quality of life for comparisons of nabilone versus amitriptyline (1 RCT) or placebo (1 RCT).16
The safety of nabilone in people living with chronic non-cancer pain was assessed in the overview of reviews and both systematic reviews. Adverse events were more frequent in people with chronic non-cancer pain who received nabilone than those who received placebo (6 RCTs), ibuprofen (1 RCT), or amitriptyline (1 RCT).17 Adverse events were more frequent in people with chronic non-cancer pain treated with dihydrocodeine (1 RCT) and gabapentin (1 longitudinal study) than nabilone.17,18 Serious adverse events were assessed in the overview of reviews and 1 systematic review. There was 1 serious adverse event (fall and fracture due to dizziness) in a participant with chronic spinal pain who received nabilone (1 RCT), and there were no serious adverse events in people with neuropathic pain who received nabilone (1 longitudinal study).16,18
The PEER guideline19 suggests that for people with osteoarthritis and low back pain, the harms of cannabinoids likely exceed the benefits, and they should be avoided in most patients. For people with neuropathic pain, the PEER guideline19 suggests that cannabinoids have unclear benefits and could be discussed with patients once interventions with clear evidence of benefit have already been considered. The BMJ guideline20 recommends offering a trial of non-inhaled cannabinoids, in addition to standard care, for people living with chronic pain. The NICE guideline21 does not recommend nabilone for the management of chronic pain in adults.
A previous report we conducted on the use of nabilone for the treatment of chronic pain was published in 2017 and updated in 2018.11,12 These reports both included people living with chronic cancer or non-cancer pain. The 2017 report identified 1 systematic review, 1 RCT, and 1 retrospective study.11 The 2018 update identified 2 overviews of reviews and 2 evidence-based guidelines.12 Overall, the results of the included studies were mixed, but suggested there were some positive benefits and limited harms of nabilone in people with chronic pain.11,12 The studies had important limitations outlined in the previous reports. These included small sample sizes, low-quality relevant studies, and lack of detailed reporting in systematic reviews.11,12 The guidelines included in the 2018 update did not recommend cannabinoids for the treatment of chronic pain.12 Both reports concluded that larger and longer prospective trials are needed to confirm the clinical effectiveness and safety of nabilone in people living with chronic pain.11,12 Additionally, we published a report in 2019 on the use of medical cannabis (including nabilone) for people with chronic pain and also concluded that higher-quality studies of longer duration are needed to confirm the clinical effectiveness and safety of medical cannabis.22
Due to the mixed results of the included studies and limited long-term data, it is difficult to draw conclusions on the clinical efficacy and safety of nabilone for the treatment of chronic non-cancer pain. The recommendations in the included guidelines varied: 1 guideline recommends against the use of nabilone for chronic pain,21 1 guideline recommends offering a trial of non-inhaled cannabinoids for people living with chronic pain,20 and 1 guideline suggests cannabinoids be avoided in people with osteoarthritis and low back pain and discussed with people with neuropathic pain.19 Future high-quality longer-term studies on the comparative efficacy and safety of nabilone versus placebo or alternative pharmacological treatments for people living with chronic non-cancer pain would aid in decision-making around the use of nabilone.
References
1.Canadian Pain Task Force report: March 2021. An action plan for pain in Canada. Ottawa: Health Canada; 2021: https://www.canada.ca/en/health-canada/corporate/about-health-canada/public-engagement/external-advisory-bodies/canadian-pain-task-force/report-2021.html Accessed April 24, 2024.
2.Management of chronic non-cancer pain. Toronto (ON): Centre for Effective Practice; 2018: https://cep.health/media/uploaded/CEP_CNCP_Updated2018.pdf Accessed April 24, 2024.
3.Canadian Pain Task Force report: June 2019. Chronic pain in Canada: laying a foundation for action. Ottawa: Health Canada; 2019: https://www.canada.ca/en/health-canada/corporate/about-health-canada/public-engagement/external-advisory-bodies/canadian-pain-task-force/report-2019.html. Accessed April 24, 2024.
4.Managing patients with pain in primary care – part 1 [Last updated September 17, 2023] Victoria (BC): Government of British Columbia; 2022: https://www2.gov.bc.ca/gov/content/health/practitioner-professional-resources/bc-guidelines/managing-patients-with-pain-in-primary-care-part-1. Accessed April 24, 2024.
5.Genova A, Dix O, Thakur M, Sangha PS. Chronic Non-cancer Pain Management and Addiction: A Review. Cureus. 2020;12(2):e6963. PubMed
6.Clearing the smoke on cannabis. Medical use of cannabis and cannabinoids – an update. Ottawa: Canadian Centre on Substance Abuse and Addiction; 2016: https://www.ccsa.ca/sites/default/files/2019-04/CCSA-Medical-Use-of-Cannabis-Report-2016-en.pdf. Accessed April 24, 2024.
7.Bains S, Mukhdomi T. Medicinal cannabis for treatment of chronic pain. StatPearls. Treasure Island (FL) StatPearls Publishing; 2022: https://www.ncbi.nlm.nih.gov/books/NBK574562/. Accessed April 24, 2024.
8.NCESAMET® nabilone capsules; 1 mg, 0.5 mg, 0.25 mg [product monograph]. Laval (QC): Bausch Health, Canada Inc.; 2019: https://pdf.hres.ca/dpd_pm/00051389.PDF. Accessed April 24, 2024.
9.Health Canada’s statement on opioids and pain management. Ottawa: Health Canada; 2022: https://www.canada.ca/en/health-canada/news/2022/11/health-canadas-statement-on-opioids-and-pain-management.html. Accessed April 24, 2024.
10.The 2017 Canadian guideline for opioids for chronic non-cancer pain. 2018; https://app.magicapp.org/#/guideline/8nyb0E. Accessed April 25, 2024.
11.Nabilone for chronic pain management: a review of clinical effectiveness and guidelines (CADTH rapid response report: summary with critical appraisal). Ottawa: CADTH; 2017: https://www.cadth.ca/nabilone-chronic-pain-management-review-clinical-effectiveness-and-guidelines Accessed April 24, 2024.
12.Nabilone for chronic pain management: a review of clinical effectiveness and guidelines – an update (CADTH rapid response report: summary with critical appraisal). Ottawa: CADTH; 2018: https://www.ncbi.nlm.nih.gov/books/NBK538943/. Accessed April 24, 2024.
13.Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. PubMed
14.Agree Next Steps Consortium. The AGREE II Instrument. Hamilton (ON): AGREE Enterprise; 2017: https://www.agreetrust.org/wp-content/uploads/2017/12/AGREE-II-Users-Manual-and-23-item-Instrument-2009-Update-2017.pdf. Accessed April 24, 2024.
15.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
16.Riera R, Pacheco RL, Bagattini AM, Martimbianco ALC. Efficacy and safety of therapeutic use of cannabis derivatives and their synthetic analogs: Overview of systematic reviews. Phytother Res. 2022;36(1):5-21. PubMed
17.Bilbao A, Spanagel R. Medical cannabinoids: a pharmacology-based systematic review and meta-analysis for all relevant medical indications. BMC Med. 2022;20(1):259. PubMed
18.Zeraatkar D, Cooper MA, Agarwal A, et al. Long-term and serious harms of medical cannabis and cannabinoids for chronic pain: a systematic review of non-randomised studies. BMJ Open. 2022;12(8):e054282. PubMed
19.PEER simplified chronic pain guideline. Can Fam Physician. 2022;68:179-190. PubMed
20.Busse JW, Vankrunkelsven P, Zeng L, et al. Medical cannabis or cannabinoids for chronic pain: a clinical practice guideline. BMJ. 2021;374:n2040. PubMed
21.Cannabis-based medicinal products [NICE guideline NG144]. London National Institute for Health and Care Excellence; 2021: https://www.nice.org.uk/guidance/ng144. Accessed April 24, 2024.
22.Medical cannabis for the treatment of chronic pain: a review of clinical effectiveness and guidelines (CADTH Rapid Response report: summary with critical appraisal). Ottawa: CADTH; 2020: https://www.cadth.ca/sites/default/files/pdf/htis/2019/RC1153%20Cannabis%20Chronic%20Pain%20Final.pdf. Accessed April 25, 2024.
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Table 2: Characteristics of Included Overview of Reviews and Systematic Reviews
Study citation, country, funding source | Study design, outcomes | Intervention and comparators | Included studies | Population characteristics |
|---|---|---|---|---|
Overview of Reviews | ||||
Riera et al. (2022)16 Brazil Funding source: Sociedade Beneficente de Senhoras Hospital Sírio-Libanês. | Overview of systematic reviews of RCTs Relevant outcomes: pain, quality of life, adverse events | Eligible interventions: any intervention derived from cannabis and its synthetic analogues Relevant intervention: nabilone Eligible comparators: any pharmacological or non-pharmacological intervention Relevant comparators: placebo, amitriptyline, ibuprofen | 68 systematic reviews in total; 4 systematic reviews relevant to the present report. | Relevant population: Adults with chronic headache related to analgesic overuse, chronic spinal pain, or fibromyalgia. |
Systematic Reviews | ||||
Bilbao and Spanagel (2022)17 Germany Funding source: Bundesministerium für Bildung und Forschung funded SysMedSUDs consortium and the Deutsche Forschungsgemeinschaft (German Research Foundation). | Systematic review and meta-analysis of RCTs Relevant outcomes: pain, adverse events | Eligible interventions: dronabinol, nabilone, cannabidiol, and nabiximols Relevant intervention: nabilone Eligible comparators: NR Relevant comparators: placebo, amitriptyline, ibuprofen, dihydrocodeine | 152 RCTs in total; 10 RCTs relevant to the present report | Relevant population: adults with chronic non-cancer pain. |
Zeraatkar et al. (2022)18 Canada Funding source: None | Systematic review and meta-analysis of nonrandomized studies Relevant outcomes: adverse events, serious adverse events, discontinuation due to adverse events | Eligible interventions: medical cannabis or cannabinoids Relevant intervention: nabilone Eligible comparators: no comparator or any pharmacological or non-pharmacological intervention Relevant comparator: gabapentin | 39 nonrandomized studies in total; 1 longitudinal study relevant to the present report | Relevant population: adults with peripheral neuropathic pain. |
RCT = randomized controlled trial.
Note this table has not been copy-edited.
Table 3: Characteristics of Included Guidelines
Intended users, target population | Intervention and practice considered | Major outcomes considered | Evidence collection, synthesis, and quality assessment | Recommendations development and evaluation | Guideline validation |
|---|---|---|---|---|---|
PEER (2022)19 | |||||
Intended users: primary care clinicians and patients. Target population: people living with chronic low back, osteoarthritic, and neuropathic pain. | Physical activity, psychological interventions, and pharmacological interventions (including cannabinoids) | Responder analysis for chronic pain, safety (adverse events). | Three systematic reviews focused on therapies for chronic pain were conducted between March 2020 and May 2021. The reviews included 285 RCTs. Supplemental questions were addressed through a rapid review process. Evidence was assessed using GRADE methodology. | An iterative process was used for identifying key questions, reviewing evidence, and developing recommendations. The guideline committee made recommendations using the GRADE framework. Key recommendations were derived through consensus. Considerations included efficacy and safety, data quality, cost, patient preferences and values, equity, feasibility, and acceptability. Strong recommendations were prefaced by “we recommend” and weak recommendations by “we suggest.” | The guideline underwent review by clinicians and patients before publication. |
BMJ (2021)20 | |||||
Intended users: clinicians and patients. Target population: adults and children living with moderate to severe chronic pain regardless of pain mechanism as well as cancer-related chronic pain. | Medical non-inhaled cannabis or cannabinoids | Patient-important outcomes: pain relief, physical functioning, emotional functioning, role functioning, social functioning, sleep quality, opioid substitution, and adverse events. | Systematic reviews were conducted on the benefits and harms of medical cannabis or cannabinoids, long-term harms of medical cannabis or cannabinoids, the impact of providing medical cannabis or cannabinoids on opioid substitution, and patients’ values and preferences. Evidence was critically appraised using the GRADE approach. | The guideline panel met virtually to discuss the evidence and formulate the recommendation. The panel followed the BMJ rapid recommendations procedures including using the GRADE approach to create the recommendation. The panel considered the balance of benefits, harms, and burdens of medical cannabis, the certainty of the evidence for each outcome, patient values and preferences, and acceptability. The recommendation was assigned a strength of either strong (all or almost all fully informed patients would choose the recommended course of action) or weak (reflects the uncertainty in typical patients’ preferences, as well as the variability in preferences between patients). | NR |
NICE (2021)21 | |||||
Intended users: health care professionals, and people taking cannabis-based medicinal products, their families and carers. Target population: people with intractable nausea and vomiting, chronic pain, spasticity, and severe treatment-resistant epilepsy. | Cannabis-based medicinal products | Pain relief, reduction in analgesics, pain intensity, functional impairment, global impression of change, quality of life, adverse events, substance abusea, and misuse/ diversion. | A systematic review was conducted that included RCTs and systematic reviews of RCTs. Meta-analyses were conducted where possible. Individual studies were assessed using the Cochrane risk of bias tool. The quality of evidence for the selected outcomes was assessed using GRADE methodology. | The guideline committee had a discussion of the evidence that followed a structured format. Decisions were reached through an informal consensus process. The committee considered the clinical evidence as well as an economic model. The strength of recommendations is reflected in the wording as either strong (directive language such as offer, advise, or ask about) or weak (consider). | A draft version of the guideline was sent to stakeholders and the guideline was revised based on comments. |
BMJ = British Medical Journal; GRADE = Grading of Recommendations Assessment, Development, and Evaluation; NICE = National Institute for Health and Care Excellence; NR = not reported; PEER = Patients Experience Evidence Research; RCT = randomized controlled trial.
aLanguage retained from original source.
Note this table has not been copy-edited.
Appendix 3: Critical Appraisal of Included Publications
Note that this appendix has not been copy-edited.
Table 4: Strengths and Limitations of Systematic Reviews Using AMSTAR 213
Strengths | Limitations |
|---|---|
Riera et al. (2022)16 | |
Clear objective and inclusion criteria that included components of population, intervention, comparator, and outcomes The review methods were established before conducting the review and the protocol was registered The choice of study designs included in the review (i.e., SRs of RCTs) was explained The literature search was conducted in multiple databases, reference lists of included articles were handsearched for additional relevant literature, grey literature search was conducted, the search strategy was provided, and no language or date restrictions were imposed Study selection and data extraction were performed independently by 2 reviewers List of excluded studies and reasons for exclusion provided Included studies were described in adequate detail Risk of bias of included SRs was assessed independently by 2 reviewers using a satisfactory technique Authors declared they had no conflicts of interest and reported their funding source | The sources of funding of the SRs included in the review were not reported There was no discussion of overlap of the included SRs and a citation matrix was not provided |
Bilbao and Spanagel (2022)17 | |
Clear objective The choice of study designs included in the review (i.e., RCTs) was explained The literature search was conducted in multiple databases and a trial registry, reference lists and systematic reviews were handsearched for additional relevant literature, and the search strategy was provided Study selection was performed independently by 2 reviewers List of excluded studies and reasons for exclusion provided Risk of bias of included studies was assessed independently by 2 reviewers using a satisfactory technique Authors declared they had no conflicts of interest and reported their funding sources | Inclusion criteria included components of population, intervention, and outcomes however, eligible comparators were not specified The review methods were established before conducting the review and the protocol was registered however there were several deviations from the published protocol (inclusion criteria, analysis plan) that were not discussed or justified Only articles published in English and German were eligible The authors did not state whether data extraction was performed in duplicate Populations, interventions, outcomes, and design of included studies were described in adequate detail however, dosages for comparators were not reported |
Zeraatkar et al. (2022)18 | |
Clear objective and inclusion criteria that included components of population, intervention, comparator, outcomes, and time frame for follow-up The choice of study designs included in the review (i.e., nonrandomized studies) was explained The literature search was conducted in multiple databases and a trial registry, reference lists of included articles were handsearched for additional relevant literature, the search strategy was provided, and content experts were contacted for unpublished studies Study selection and data extraction were performed independently by 2 reviewers List of excluded studies and reasons for exclusion provided Risk of bias was assessed independently by 2 reviewers using a satisfactory technique Authors declared that they had no conflicts of interest and no funding was received | The authors did not state whether the review methods were established before conducting the review |
AMSTAR 2 = A MeaSurement Tool to Assess systematic Reviews 2; RCT = randomized controlled trial; SR = systematic review.
Table 5: Strengths and Limitations of Guidelines Using AGREE II14
Item | PEER (2022)19 | BMJ (2021)20 | NICE (2021)21 |
|---|---|---|---|
Domain 1: Scope and purpose | |||
1. The overall objective(s) of the guideline is (are) specifically described. | Yes | Yes | Yes |
2. The health question(s) covered by the guideline is (are) specifically described. | Yes | Yes | Yes |
3. The population (patients, public, etc.) to whom the guideline is meant to apply is specifically described. | Yes | Yes | Yes |
Domain 2: Stakeholder involvement | |||
4. The guideline development group includes individuals from all relevant professional groups. | Yes | Yes | Yes |
5. The views and preferences of the target population (patients, public, etc.) have been sought. | Yes | Yes | Yes |
6. The target users of the guideline are clearly defined. | Partially | Partially | Yes |
Domain 3: Rigour of development | |||
7. Systematic methods were used to search for evidence. | Yes | Yes | Yes |
8. The criteria for selecting the evidence are clearly described. | Yes | Yes | Yes |
9. The strengths and limitations of the body of evidence are clearly described. | Yes | Yes | Yes |
10. The methods for formulating the recommendations are clearly described. | Yes | Yes | Yes |
11. The health benefits, side effects, and risks have been considered in formulating the recommendations. | Yes | Yes | Yes |
12. There is an explicit link between the recommendations and the supporting evidence. | Yes | Yes | Yes |
13. The guideline has been externally reviewed by experts before its publication. | Yes | Yes | Yes |
14. A procedure for updating the guideline is provided. | No | Yes | Yes |
Domain 4: Clarity of presentation | |||
15. The recommendations are specific and unambiguous. | Yes | Yes | Yes |
16. The different options for management of the condition or health issue are clearly presented. | NA | NA | NA |
17. Key recommendations are easily identifiable. | Yes | Yes | Yes |
Domain 5: Applicability | |||
18. The guideline describes facilitators and barriers to its application. | No | No | No |
19. The guideline provides advice and/or tools on how the recommendations can be put into practice. | Yes | Yes | Yes |
20. The potential resource implications of applying the recommendations have been considered. | No | Partially | Yes |
21. The guideline presents monitoring and/or auditing criteria. | No | No | No |
Domain 6: Editorial independence | |||
22. The views of the funding body have not influenced the content of the guideline. | Partially | Partially | Unclear |
23. Competing interests of guideline development group members have been recorded and addressed. | Yes | Yes | Yes |
AGREE II = Appraisal of Guidelines for Research and Evaluation II; NA = not applicable.
Appendix 4: Main Study Findings
Table 6: Summary of Findings by Outcome — Pain
Citation Study design | Primary study | Population | Comparison | Outcome, time point | Results |
|---|---|---|---|---|---|
Riera et al. (2022)16 Overview of reviews | Fitzcharles 2016 (SR, results from 1 RCT) | Chronic spinal pain (N = 30) | Nabilone (0.25 mg to 1 mg/day) vs placebo | Change in pain intensity (VAS), 4 weeks |
|
Bilbao and Spanagel (2022)17 SR | Peball 2020 (RCT) | Parkinson disease (N = 38) | Nabilone (max 2 mg/day) vs placebo | Chronic pain, 4 weeks | SMD = −0.19 (95% CI, −0.82 to 0.45) |
Herrmann 2019 (RCT) | Alzheimer disease (N = 39) | Nabilone (max 2 mg/day) vs placebo | Chronic pain, 6 weeks | SMD = 0.03 (95% CI, −0.29 to 0.35) | |
Turcotte 2015 (RCT) | Multiple sclerosis (N = 15) | Nabilone (max 2 mg/day) vs placebo | Chronic pain, 9 weeks | SMD = −1.88 (95% CI, −3.09 to −0.66) | |
Toth 2012 (RCT) | Diabetic peripheral neuropathic pain (N = 26) | Nabilone (1 to 4 mg/day) vs placebo | Chronic pain, 5 weeks | SMD = −1.30 (95% CI, −2.14 to −0.45) | |
Skrabek 2008 (RCT) | Fibromyalgia (N = 40) | Nabilone (max 2 mg/day) vs placebo | Chronic pain, 4 weeks | SMD = −0.75 (95% CI, −1.46 to −0.04) | |
Pinsger 2006 (RCT) | Neuropathic pain (N = 30) | Nabilone (0.25 to 1 mg/day) vs placebo | Chronic pain, 4 weeks | SMD = −0.54 (95% CI, −0.92 to −0.16) | |
Wissel 2006 (RCT) | Upper motor neuron syndrome (N = 13) | Nabilone (1 mg/day) vs placebo | Chronic pain, 4 weeks | SMD = −0.64 (95% CI, −1.24 to −0.04) | |
Pini 2012 (RCT) | Medication overuse headache (N = 30) | Nabilone (0.5 mg/day) vs ibuprofen | Chronic pain, 8 weeks | SMD = −0.44 (95% CI, −0.84 to −0.03) | |
Ware 2010 (RCT) | Fibromyalgia (N = 32) | Nabilone (0.5 to 1 mg/day) vs amitriptyline | Chronic pain, 2 weeks | SMD = −0.18 (95% CI, −0.53 to 0.17) | |
Frank 2008 (RCT) | Neuropathic pain (N = 96) | Nabilone (max 2 mg/day) vs dihydrocodeine | Chronic pain, 6 weeks | SMD = 0.31 (95% CI, 0.07 to 0.54) |
NR = not reported; SMD = standardized mean difference.
Note: SMD < 0 favours nabilone.
Note this table has not been copy-edited.
Table 7: Summary of Findings by Outcome — Quality of Life
Citation Study design | Primary study | Population | Comparison | Follow-up | Results |
|---|---|---|---|---|---|
Riera et al. (2022)16 Overview of reviews | Johal 2020 and Wong 2020 (SRs, results from 1 RCT) | Fibromyalgia (N = 36) | Nabilone (0.5 to 1 mg/day) vs amitriptyline (10 to 20 mg) | 2 weeks | No difference between groups (numeric data NR) |
Hassan 2018 (SR, results from 1 RCT) | Chronic headache related to analgesic overuse (N = 30) | Nabilone (0.5 mg/day) vs ibuprofen (400 mg/day) | 2 weeks | SF-36 physical and mental domain:
| |
Fitzcharles 2016 (SR, results from 1 RCT) | Chronic spinal pain (N = 30) | Nabilone (0.25 mg to 1 mg/day) vs placebo | 4 weeks |
|
NR = not reported; RCT = randomized controlled trial; SF-36 = short form 36 questionnaire; SR = systematic review.
Note this table has not been copy-edited.
Table 8: Summary of Findings by Outcome — Adverse Events
Citation Study design | Primary study | Population | Comparison | Follow-up | Results |
|---|---|---|---|---|---|
All adverse events | |||||
Bilbao and Spanagel (2022)17 SR | Peball 2020 (RCT) | Parkinson disease (N = 38) | Nabilone (max 2 mg/day) vs placebo | 4 weeks | OR = 5.16 (95% CI, 1.23 to 21.55) |
Herrmann 2019 (RCT) | Alzheimer disease (N = 39) | Nabilone (max 2 mg/day) vs placebo | 6 weeks | OR = 7.59 (95% CI, 3.58 to 16.11) | |
Toth 2012 (RCT) | Diabetic peripheral neuropathic pain (N = 26) | Nabilone (1 to 4 mg/day) vs placebo | 5 weeks | OR = 1.36 (95% CI, 0.29 to 6.36) | |
Skrabek 2008 (RCT) | Fibromyalgia (N = 40) | Nabilone (max 2 mg/day) vs placebo | 4 weeks | OR = 4.37 (95% CI, 0.88 to 21.71) | |
Pinsger 2006 (RCT) | Neuropathic pain (N = 30) | Nabilone (0.25 to 1 mg/day) vs placebo | 4 weeks | OR = 4.50 (95% CI, 1.58 to 12.80) | |
Wissel 2006 (RCT) | Upper motor neuron syndrome (N = 13) | Nabilone (1 mg/day) vs placebo | 4 weeks | OR = 3.44 (95% CI, 0.89 to 13.32) | |
Pini 2012 (RCT) | Medication overuse headache (N = 30) | Nabilone (0.5 mg/day) vs ibuprofen | 8 weeks | OR = 1.59 (95% CI, 0.73 to 3.47) | |
Ware 2010 (RCT) | Fibromyalgia (N = 32) | Nabilone (0.5 to 1 mg/day) vs amitriptyline | 2 weeks | OR = 3.18 (95% CI, 1.25 to 8.10) | |
Frank 2008 (RCT) | Neuropathic pain (N = 96) | Nabilone (max 2 mg/day) vs dihydrocodeine | 6 weeks | OR = 0.30 (95% CI, 0.13 to 0.73) | |
Zeraatkar et al. (2022)18 SR | Bestard and Toth 2011 (longitudinal) | Peripheral neuropathic pain (N = 220) | Nabilone (mean = 3 mg/day) vs gabapentin (mean = 2.3 g/day) | 24 weeks | Risk difference = −13.1% (95% CI, −26.2 to 0) |
Mild adverse events | |||||
Riera et al. (2022)16 Overview of reviews | Fitzcharles 2016 (SR, results from 1 RCT) | Chronic spinal pain (N = 30) | Nabilone (0.25 mg to 1 mg/day) vs placebo | 4 weeks | Nabilone vs placebo
|
Adverse events causing discontinuation | |||||
Zeraatkar et al. (2022)18 SR | Bestard and Toth 2011 (longitudinal) | Peripheral neuropathic pain (N = 220) | Nabilone (mean = 3 mg/day) vs gabapentin (mean = 2.3 g/day) | 24 weeks | Risk difference = −9.4% (95% CI, −18.5 to −0.2) |
Serious adverse events | |||||
Riera et al. (2022)16 Overview of reviews | Fitzcharles 2016 (SR, results from 1 RCT) | Chronic spinal pain (N = 30) | Nabilone (0.25 mg to 1 mg/day) vs placebo | 4 weeks | One event in nabilone group (fall and fracture due to dizziness)
|
Zeraatkar et al. (2022)18 SR | Bestard and Toth 2011 (longitudinal) | Peripheral neuropathic pain (N = 220) | Nabilone (mean = 3 mg/day) vs gabapentin (mean = 2.3 g/day) | 24 weeks | Risk difference = 0% (95% CI, 0 to 0) |
NR = not reported; OR = odds ratio; RCT = randomized controlled trial; SR = systematic review.
Note: OR < 1 and risk difference < 0 favour nabilone.
Note this table has not been copy-edited.
Table 9: Summary of Recommendations in Included Guidelines
Recommendations and supporting evidence | Quality of evidence and strength of recommendations |
|---|---|
PEER (2022)19 | |
Osteoarthritis “We suggest that treatments where the harms likely exceed the benefits be avoided in most patients: opioids, cannabinoids.” (p. 185)19 Supporting evidence: 1 RCT of cannabinoids in osteoarthritic pain that did not demonstrate any benefit over placebo on pain outcomes. An evidence review that demonstrated a high rate of adverse events associated with cannabinoids. | Quality of evidence: very low Strength of recommendations: weak |
Low back pain “We suggest that treatments where the harms likely exceed the benefits be avoided in most patients: opioids, cannabinoids.” (p. 186)19 Supporting evidence: 1 RCT of cannabinoids in low back pain that reported no evidence of benefit vs. placebo for most outcomes. | Quality of evidence: very low Strength of recommendations: weak |
Neuropathic pain “We suggest that the following treatments with no or unclear benefit could be discussed with patients when interventions with clear evidence of benefit have already been considered.
Supporting evidence: A review of cannabinoids for neuropathic pain that demonstrated a greater number of participants who experienced pain reduction vs. placebo. | Quality of evidence: very low Strength of recommendations: weak |
BMJ (2021)20 | |
“The panel made a weak recommendation to offer a trial of non-inhaled medical cannabis or cannabinoids, in addition to standard care and management (if not sufficient to manage pain symptoms), for people living with chronic cancer or non-cancer pain.” (p. 4)20 Supporting evidence: SR of 32 RCTs that reported the use of cannabinoids results in small to very small improvements in self-reported pain intensity, physical functioning, and sleep quality as well as small to modest risk of mostly self-limited and transient harms. | Quality of evidence: moderate to high Strength of recommendation: weak |
NICE (2021)21 | |
“Do not offer the following to manage chronic pain in adults:
Supporting evidence: 1 RCT that reported a reduction in functional impairment caused by pain in people treated with nabilone vs. placebo and 2 RCTs that reported more adverse events in people treated with nabilone vs. placebo. An economic analysis that found that the potential benefits were small compared with the high and ongoing costs. | Quality of evidence: low Strength of recommendation: strong |
BMJ = British Medical Journal; CBD = cannabidiol; NICE = National Institute for Health and Care Excellence; PEER = Patients Experience Evidence Research; RCT = randomized controlled trial; SR = systematic review; THC = delta-9-tetrahydrocannabinol.
Note this table has not been copy-edited.
Appendix 5: Overlap Between Included Systematic Reviews
Table 10: Overlap in Relevant Primary Studies Between Included SRs
Primary study citation | Riera et al. (2022)16 Overview of reviews | Bilbao and Spanagel (2022)17 SR | Zeraatkar et al. (2022)18 SR | |||
|---|---|---|---|---|---|---|
Johal H et al. Clin Med Insights, Arthritis Musculoskelet Disord. 2020;13, 1179544120906461. | Wong SSC et al. J Neuroimmune Pharmacol. 2020;15(4): 801 to 29. | Hassan S. J Pain Manag and Med. 2018;4(1). | Fitzcharles MA et al. Schmerz. 2016;30(1): 47 to 61. | |||
Toth C et al. Pain. 2012;153(10): 2073 to 82. | Yes | Yes | Yes | — | Yes | Yes |
Turcotte D et al. Pain Med. 2015;16(1): 149 to 59. | Yes | Yes | — | — | Yes | — |
Skrabek RQ et al. J Pain. 2008;9(2): 164 to 73. | Yes | Yes | Yes | Yes | Yes | — |
Wissel J et al. J Neurol. 2006;253(10): 1337 to 41. | Yes | Yes | Yes | — | Yes | — |
Ware MA et al. Anesth Analg. 2010;110(2): 604 to 10. | — | Yes | Yes | Yes | Yes | — |
Pini LA et al. J Headache Pain. 2012;13(8): 677 to 84. | — | Yes | Yes | — | Yes | — |
Frank B et al. BMJ. 2008; 336(7637): 199 to 201. | — | Yes | — | — | Yes | — |
Pinsger M et al. Wien Klin Wochenschr. 2006;118(11 to 12):327 to 35. | — | — | Yes | Yes | Yes | — |
Herrmann N et al. Am J Geriatr Psychiatry. 2019; 27(11):1161 to 73 | — | — | — | — | Yes | — |
Peball M et al. Ann Neurol. 2020; 88(4):712 to 22 | — | — | — | — | Yes | — |
Bestard AA and Toth CC. Pain Pract. 2011;11:353 to 68 | — | — | — | — | — | Yes |
SR = systematic review.
Note this table has not been copy-edited.
Appendix 6: References of Potential Interest
Previous CADTH Reports
Nabilone for the Treatment of Post-Traumatic Stress Disorder: A 2021 Update. 2021. https://www.cadth.ca/nabilone-treatment-post-traumatic-stress-disorder-2021-update
Non-Opioid Options for Managing Adult Chronic Pain; 2020 https://www.cadth.ca/non-opioid-options-managing-pain
Nabilone for the Treatment of Nausea and Vomiting or Anorexia: A Review of Clinical Effectiveness and Guidelines; 2019. https://www.cadth.ca/nabilone-treatment-nausea-and-vomiting-or-anorexia-review-clinical-effectiveness-and-guidelines
Medical Cannabis Use in Palliative Care: Review of Clinical Effectiveness and Guidelines – An Update; 2019. https://www.cadth.ca/medical-cannabis-use-palliative-care-review-clinical-effectiveness-and-guidelines-update
Medicinal and Synthetic Cannabinoids for Pediatric Patients: A Review of Clinical Effectiveness and Guidelines; 2019. https://www.cadth.ca/medicinal-and-synthetic-cannabinoids-pediatric-patients-review-clinical-effectiveness-and
Review Articles
Sirbu CA, Georgescu R, Plesa FC, et al. Cannabis and Cannabinoids in Multiple Sclerosis: From Experimental Models to Clinical Practice-A Review. Am J Ther. 2023;30(3):e220-e231. PubMed
Carreira DS, Garden S, Huffman A, Ueland T. Cannabinoids in the Orthopedic Setting: A Literature Review. Orthopedics. 2022;45(4):e183-e189. PubMed
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for noncommercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca.