CADTH Health Technology Review
Newborn Screening for Congenital Cytomegalovirus
Rapid Review
Key Messages
What Is the Issue?
Congenital cytomegalovirus (cCMV) is estimated to affect between 0.2% and 2.4% of newborns worldwide, and may cause long-term effects, including hearing loss and neurodevelopmental disability.
Newborn screening for cCMV can identify affected neonates and provide an opportunity for early treatment, which may reduce any long-term effects from infection.
We wanted to know if universal newborn screening is a clinically effective and cost-effective intervention for identifying and managing cCMV.
What Did We Do?
We identified and summarized published literature comparing the clinical effectiveness and cost-effectiveness of universal newborn screening with either targeted newborn screening or no screening for congenital cytomegalovirus in neonates. We also identified and summarized published, evidence-based guidelines that make recommendations concerning the use of newborn screening for congenital cytomegalovirus to help inform decisions considering the use of this intervention.
An information specialist searched for peer-reviewed and grey literature sources published between January 1, 2014, and March 19, 2024. The search was limited to English-language documents. One reviewer screened articles for eligibility based on predefined criteria, critically appraised the included studies, and narratively summarized the findings.
What Did We Find?
Evidence from 1 prospective cohort study in the US found that, compared to universal newborn screening for cCMV, targeted newborn screening failed to identify a significant proportion of neonates who developed hearing loss associated with infection.
Three cost-effectiveness evaluations concluded that universal newborn screening for cCMV was cost-effective when compared to targeted newborn screening or no screening. None of these analyses were specific to the Canadian context.
While 1 of 3 evidence-based guidelines identified by this review makes a recommendation favouring universal newborn screening for cCMV, 2 evidence-based guidelines recommend against the implementation of universal newborn screening for cCMV (including 1 from the Canadian context), generally citing a lack of sufficient clinical evidence.
What Does This Mean?
The included cost-effectiveness studies and evidence-based guidelines in this report emphasize that limited clinical evidence is currently available to inform decision-making concerning newborn screening for cCMV.
Jurisdictions where universal newborn screening for cCMV has been implemented provide an opportunity for clinical research to support and inform future decision-making.
The current limitation of available clinical data describing newborn screening for cCMV will require decision-makers to draw from a broader set of inputs and sources than those available from empirical studies.
Abbreviations
CI
confidence interval
cCMV
congenital cytomegalovirus
CMV
cytomegalovirus
DBS
dried blood spot
GDP
gross domestic product
HL
hearing loss
ICER
incremental cost-effectiveness ratio
NBS
newborn screening
NHS
newborn hearing screening
SNHL
sensorineural hearing loss
Context and Policy Issues
What Is cCMV?
Cytomegalovirus (CMV) is a common herpesvirus that infects most adults, but often goes unnoticed and/or is asymptomatic.1 During pregnancy, maternal antibodies do not fully protect the fetus from CMV infection, which can result in transmission to the fetus and congenital cytomegalovirus (cCMV) infection at birth.1 CMV is reported to be the largest contributor to congenital infection in the world, with a range of 0.2% to 2.4% of newborns affected.2-5 Neonates with symptomatic cCMV may present with rash, jaundice, small for gestational age, and/or neurologic findings (e.g., encephalitis), and are at risk of long-term and permanent sequelae, including sensorineural hearing loss (SNHL), developmental delay, and intellectual and learning disabilities.1-4,6 Mortality is estimated to occur in one-third of neonates with a severe presentation of the disease.1,2 While most neonates with cCMV will not have symptoms, it is estimated that 10% to 20% of neonates who are asymptomatic may develop long-term sequelae, including SNHL.2-5
How Is cCMV Managed?
There is no vaccine or preventive medical intervention to protect from cCMV infection.2,4,7 However, there is some evidence to demonstrate a beneficial long-term effect of antiviral medication for preventing SNHL and other neurodevelopmental sequelae.2 Treatment with an antiviral medication should begin in the first month after birth for neonates with cCMV to ensure optimal benefit.2 Nonetheless, antiviral medication is generally limited to neonates with moderate to severe symptoms of cCMV, and may not be available to other neonates with cCMV, who are at risk for long-term sequelae, as well.2 Consequently, detection of cCMV must occur within the first 3 weeks after birth — not only to allow an opportunity for the potentially effective treatment of cCMV, but also to distinguish the infection as congenital versus acquired after birth, as the latter is expected to pose less of a risk to the infant.1,2,4,5,8,9
What Is Newborn Screening for cCMV?
There are generally 2 approaches to newborn screening (NBS) for cCMV: universal screening for all neonates and targeted screening for neonates believed to be at risk of having cCMV.2 Targeted screening may rely on clinical suspicion of cCMV infection in neonates who are symptomatic or on a newborn hearing screen, with neonates who demonstrate a risk of impaired hearing referred for cCMV testing. Prenatal screening may also be performed,2 but was not the focus of this report.
While universal NBS infrastructure is in place for multiple metabolic, inherited, and other conditions in many jurisdictions, most existing NBS programs use dried blood spots (DBSs), making this method of screening desirable for the addition of cCMV.3 However, previous studies have demonstrated that DBSs are unlikely to be ideal samples for the detection of cCMV, as the viral load in DBSs may not be detectable at birth.2,3,10 Urine is generally considered to be the optimal sample for detection of cCMV.2,5,11 Saliva samples may also be used, and are more easily obtainable than urine samples, but generally have lower specificity, introducing a higher risk of false-positive results.2 However, either urine or saliva sample collection for NBS will demand significant changes and impacts to existing NBS programs that are likely to be challenging and costly.3,8,10 While research is under way and ongoing to investigate methods for improved test performance of DBS, a feasible and effective DBS method currently requires further investigation.3,10,11 Nonetheless, several jurisdictions in Canada and the US — including Saskatchewan, Ontario, and Minnesota — have begun universal NBS programs that use DBSs.4,12
Why Is It Important to Do This Review?
Given the public health burden of cCMV for neonates, approaches to NBS for cCMV have been considered for years; however, the optimal approach to NBS for cCMV remains uncertain and continues to be debated.4-6 To support and inform Canadian health care policy and decision-making for the detection and management of cCMV, this report aims to identify and summarize clinical effectiveness and cost-effectiveness evidence comparing universal NBS for cCMV with either targeted screening or no screening, and to identify and summarize the evidence-based guidelines that make recommendations concerning NBS for cCMV.
Research Questions
What is the clinical utility of universal NBS versus targeted or no newborn screening for cCMV?
What is the cost-effectiveness of universal NBS versus targeted or no newborn screening for cCMV?
What are the evidence-based guidelines regarding NBS for cCMV?
Methods
Literature Search Methods
An information specialist conducted a focused literature search on key resources, including MEDLINE, the Cochrane Database of Systematic Reviews, the International HTA Database, and the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search approach was customized to retrieve a limited set of results, balancing comprehensiveness with relevance. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. Search concepts were developed based on the elements of the research questions and selection criteria. The focused search concepts (limiting to focused MeSH headings and concepts appearing in the title and keywords only) were cytomegalovirus, screening, and newborns. No study design filters were applied to limit retrieval. The search was completed on March 19, 2024, and limited to English-language documents published since January 1, 2014.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the eligibility criteria presented in Table 1.
Criteria | Description |
|---|---|
Population | Q1 to Q3: Neonates |
Intervention | Q1 and Q2: Universal screening for congenital cytomegalovirus (i.e., blood spot, urine, or saliva) Q3: Screening for congenital cytomegalovirus (i.e., universal, targeted, or other) |
Comparator | Q1 and Q2: No screening, targeted screening (e.g., hearing loss) Q3: NA |
Outcomes | Q1: Clinical utility (e.g., number needed to screen, time to diagnosis, time to treatment, morbidity, mortality, quality of life) Q2: Cost-effectiveness (e.g., cost per unit of health benefit gained, cost per QALY gained, ICER) Q3: Recommendations regarding newborn screening for congenital cytomegalovirus |
Study designs | Health technology assessments, systematic reviews, randomized controlled trials, nonrandomized studies, economic evaluations, evidence-based guidelines |
ICER = incremental cost-effectiveness ratio; NA = not applicable; QALY = quality-adjusted life-year.
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, were duplicate publications, or were published before 2014. Guidelines with unclear methodologies were also excluded.
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the following tools as a guide: the Downs and Black checklist13 for nonrandomized studies, the Drummond checklist14 for economic evaluations, and the Appraisal of Guidelines for Research and Evaluation (AGREE) II instrument15 for guidelines. Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Summary of Evidence
Quantity of Research Available
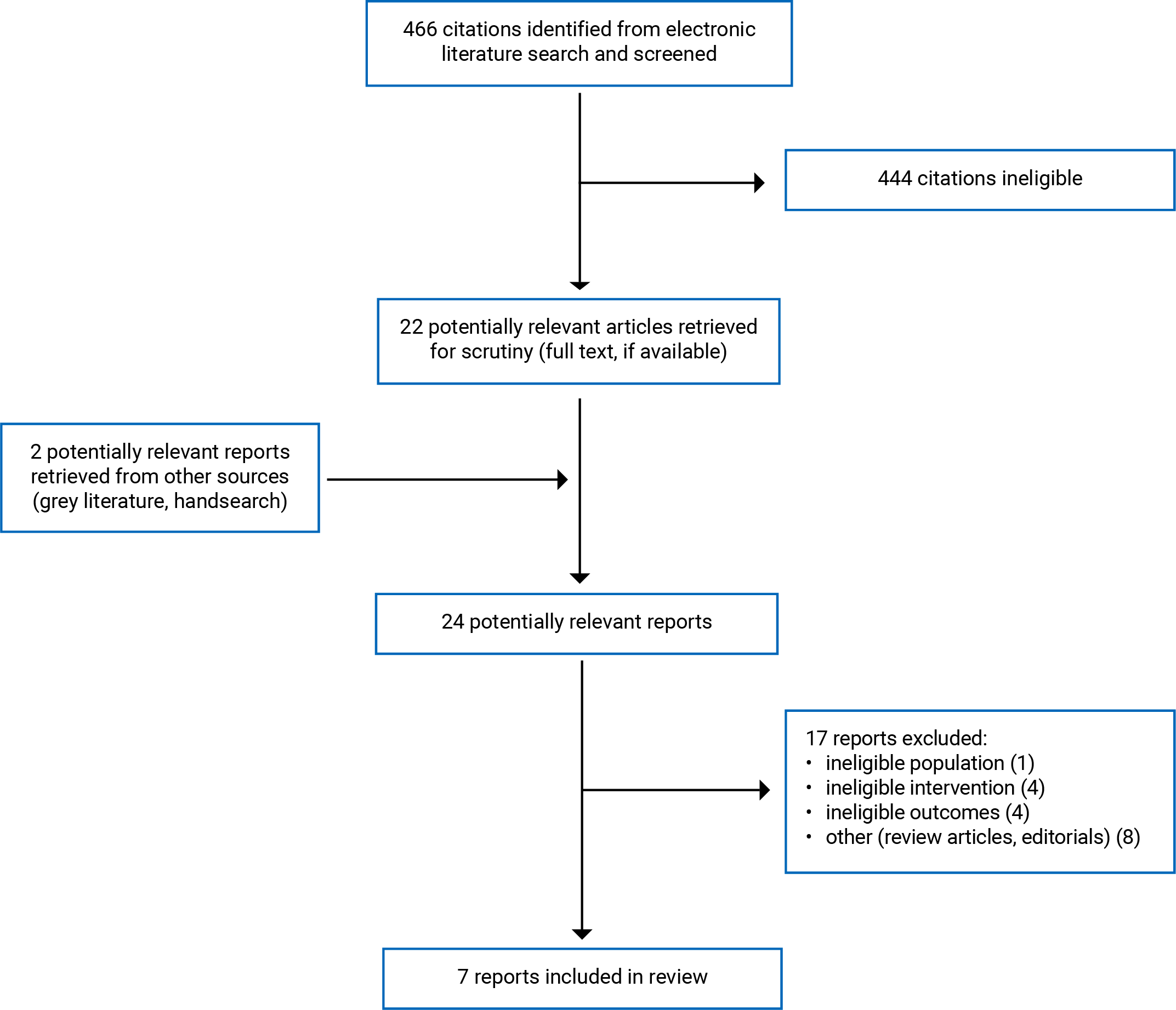
This report included and summarized 7 publications that met the eligibility criteria.16-22 These comprised 1 nonrandomized study,19 3 economic evaluations,17,18,22 and 3 evidence-based guidelines.16,20,21 Appendix 1 presents the PRISMA23 flow chart of the study selection.
To support and inform consideration of cCMV NBS programs for decision-makers, in addition to the eligible studies identified in this report, studies that described noncomparative assessments of NBS programs (i.e., ineligible comparator), or did not describe the features of clinical utility (i.e., ineligible outcomes), but were otherwise relevant to the research questions (i.e., universal NBS and/or targeted cCMV NBS programs) were summarized by abstract only. Description of these ineligible studies was limited to the past 5 years of publication. A tabulated summary of the abstracts from these studies is presented in Appendix 5.
Summary of Study Characteristics
This report summarizes the characteristics and findings from 1 prospective cohort study,19 3 cost-effectiveness evaluations,17,18,22 and 3 evidence-based guidelines.16,20,21
Additional details regarding the characteristics of the included publications are provided in Appendix 2.
Study Design
The prospective cohort study was published in 2017 and was conducted across 7 sites, with data collected between 2007 and 2012.19
The 3 cost-effectiveness studies used lifetime horizons in their models.17,18,22 While 2 of the cost-effectiveness studies described a public health payer perspective,18,22 1 did not describe the perspective used in the study.17 All 3 cost-effectiveness studies used decision-tree and/or Markov modelling, using clinical and cost inputs from referenced, published, and governmental data sources.17,18,22 Key model assumptions included appropriate diagnosis and treatment for all study participants.17,18,22
One of the evidence-based guidelines was developed by the Institut national d'excellence en santé et en services sociaux (INESSS),16 another by the International Congenital Cytomegalovirus Recommendations Group,20 and another by the UK National Screening Committee.21 The 3 evidence-based guidelines reported reviews of available evidence, synthesis, and critical appraisal of eligible studies, with an explicit link from the evidence to the relevant recommendations that were developed.16,20,21 One of the guidelines was reported as an updated review of the evidence for a previous version of the guideline that was published in 2012.21 One guideline provided a description of the quality of evidence informing the recommendations (i.e., ranging from levels 1 to 3),20 whereas 2 did not.16,21 None of the evidence-based guidelines explicitly described a strength for the recommendations of relevance to this report.16,20,21
Country of Origin
The prospective cohort study was conducted in the US.19 The economic evaluations were conducted in Japan,17 China,18 and the US.22 Of the evidence-based guidelines, 1 was developed in the Canadian province of Quebec,16 another in the UK,21 and the third was developed by an international group, with no country of origin reported (though experts were invited from Europe, the US, and Australia to develop the guidance, and the group was convened in Australia).20
Patient Population
All of the included studies and evidence-based guidelines described neonates as the population of interest.16-22
Interventions and Comparators
The prospective cohort study described NBS for cCMV and compared universal versus targeted approaches.19 The 3 cost-effectiveness studies reported data comparing universal NBS for cCMV to targeted screening or no screening.17,18,22 Three of the studies described NBS programs using saliva samples,18,19,22 2 described NBS programs using urine samples,17,18 and 1 described a NBS program using DBS.19 The timing of screening was described variably, with the prospective cohort indicating NBS occurred while neonates were in the newborn nursery (though no quantitative time frame was reported).19 Two of the cost-effectiveness studies reported that NBS occurred within the first 3 weeks after birth,17,22 while 1 cost-effectiveness study reported that NBS occurred after birth (with no quantitative time frame reported).18
The prospective cohort study exposed all neonates in the cohort to both a universal cCMV NBS program using saliva and DBS samples, as well as a targeted screening program using newborn hearing screening (NHS) with Auditory Brainstem Response to detect risk for SNHL at birth.19 Neonates with a diagnosis of cCMV, and those who failed the NHS, were referred for audiologic assessment.19
The evidence-based guidelines describe NBS for cCMV, with 1 evidence-based guideline focusing on the use of DBS16 and 2 describing NBS without a focus on sample type.20,21 The timing of NBS is not addressed in the evidence-based guidelines.16,20,21
Outcomes
The prospective cohort and cost-effectiveness studies focused on the role of NBS for cCMV in the reduction of hearing loss (HL).16,19-21 Additional features of clinical utility (i.e., number needed to screen, time to diagnosis, time to treatment, morbidity other than HL, mortality, and quality of life) were not addressed by the clinical effectiveness or cost-effectiveness studies.16,19-21
The prospective cohort study reported on cases of cCMV detected by the universal NBS program (diagnoses only, with no data describing screening results), symptoms associated with cCMV, the findings of NHS (i.e., pass or fail), and the findings of audiologic assessment between 3 and 8 weeks of life for all neonates who were either diagnosed with cCMV and/or who failed the NHS.19
The cost-effectiveness studies reported on incremental costs of universal NBS as compared to targeted or no screening.17,18,22 Two of the studies reported costs in US dollars18,22 and 1 study reported costs in Japanese yen (¥) (valued at approximately 0.006 US dollars as of April 17, 202424).17 Two of the cost-effectiveness studies reported on incremental quality-adjusted life-years and calculated incremental cost-effectiveness ratios (ICERs),17,18 while 1 did not.22 Though neither of the cost-effectiveness studies that reported ICERs characterized cost-effectiveness in terms of a willingness-to-pay threshold, both described the ICERs expressed as gross domestic product (GDP) per capita for the respective countries in which the studies were conducted.17,18 The cost-effectiveness of the ICERs was interpreted in accordance with thresholds established by the WHO (i.e., an ICER of less than 3 times the GDP per capita indicates cost-effectiveness, whereas an ICER that is greater than 3 is considered not to be cost-effective).17,18 Clinical inputs to the cost-effectiveness models included cases of cCMV identified, costs of screening and treatment for cCMV and/or HL, and costs saved with reduced morbidity caused by cCMV-associated HL.17,18,22 All 3 cost-effectiveness studies reported the findings from one-way sensitivity analyses.17,18,22
The 3 evidence-based guidelines considered features of clinical utility of NBS for cCMV (primarily as it concerned cCMV-associated HL, with some consideration of developmental delay) and cost (for screening and diagnosis, treatment, and reduced HL) outcomes in the development of their recommendations.16,20,21 Additional considerations included populational, organizational, sociocultural,16 and health system.21
Summary of Critical Appraisal
Overall, a key limitation of the included studies and guidelines summarized in this report was a focus on cCMV-associated HL as an outcome of NBS screening strategies, with limited information describing a broader set of relevant clinical utility outcomes (e.g., morbidity from neurodevelopmental and other possible sequelae, as well as impacts to quality of life).16-22
Prospective Cohort Study
The prospective cohort study was well reported, with a description of the characteristics of the population, intervention, comparator, and outcomes.19 The main findings were clearly reported, including estimates of random variability.19 The study’s external validity appeared robust, with a large cohort from multiple study sites, including study participants and health care that were likely to be representative of the population.19 Follow-up of the cohort was consistent across the universal and targeted screening approaches, and compliance with screening, diagnostic testing, and treatment was also consistent.19 Losses to follow-up were minimal.19 These study features, which demonstrated internal and external validity of the study methods, provide confidence in the findings of the study.
The limitations of the prospective cohort study included a lack of randomization and/or blinding;19 however, these limitations are a consistent feature of studies describing and comparing NBS programs, given the characteristics of the intervention. Furthermore, in this study, all neonates were exposed to both universal and targeted screening approaches,19 which rendered the value of randomization and/or blinding less important to establishing internal validity.
Cost-Effectiveness Evaluations
The 3 cost-effectiveness studies were generally well reported, and included sources and references to data used for the model inputs.17,18,22 The key features of the cost-effectiveness analyses were described, including currency and price data, the time horizons over which the outcomes were considered (which were lifetime horizons, thus appropriate to the research questions), primary outcomes, model structures, and discount rates applied.17,18,22 These study features are essential for informing an assessment of the utility of the findings generated.
While 2 of the cost-effectiveness studies included some description of the viewpoint from which the analyses were conducted,18,22 1 did not,17 which limited the extent to which the costs and benefits included in the model could be ascertained as relevant. Similarly, while 2 of the studies described productivity costs,17,22 1 did not,18 which limited the interpretation of the cost-effectiveness findings reported, as any sequelae from cCMV may have downstream consequences that could impact the productivity of affected neonates and their families. None of the cost-effectiveness studies reported detailed data describing the characteristics of patients or studies from which data were drawn to inform the model estimates; however, estimated rates of cCMV diagnosis in the study populations were reported.17,18,22 Notably, the estimated rates of cCMV in 2 of the cost-effectiveness studies (i.e., the studies conducted in the Japanese and Chinese contexts)17,18 appeared to be lower than in the third (i.e., the study conducted in a US context),22 and also appeared to be lower than that found in the prospective cohort study that was included in this report (also conducted in the US).19 This variability in the estimated prevalence of cCMV across the cost-effectiveness study populations may have impacted the inputs used to estimate cost-effectiveness (e.g., costs of diagnosis and treatment, and cost savings of long-term sequelae avoided). Nonetheless, it is known that the presence of cCMV does vary widely across various populations,2,25 and must therefore be accounted for in modelled data.
While all of the cost-effectiveness studies reported on sensitivity analyses, no explicit justification for the selection of variables used in these analyses was reported,17,18,22 and 1 study did not clearly describe the methods used to inform the sensitivity analyses.22 A clear and detailed description of sensitivity analyses is essential to consider uncertainty in the model estimates and inform interpretation around the robustness and meaningfulness of the findings.14
Whereas 2 of the studies were clear about the limitations of their studies, and the associated caveats around interpretation of their findings,17,18 1 did not provide an explicit acknowledgement of these caveats,22 which limited the interpretation concerning how the findings may be used in a decision-making context. Nonetheless, all 3 author groups conceded that the available clinical evidence was limited, which consequently limited the interpretation of their findings.17,18,22 Generally, all 3 cost-effectiveness studies made assumptions of health care that characterized ideal scenarios (e.g., that diagnosis and treatment was always appropriate and effective), which may not reflect real-world experience and could potentially inflate cost-effectiveness estimates.17,18,22
Evidence-Based Guidelines
The scope and purpose are generally well reported by the 3 included evidence-based guidelines.16,20,21 Stakeholder involvement and appropriate input into the development of the recommendations are clear in 1 of the guidelines.21,26,27 While expert involvement from relevant professional groups was apparent for all of the included evidence-based guidelines,16,20,21,26,27 it was not clear whether members of the public (including those affected) were consulted, nor who the target users of the recommendations were for 2 of the guidelines.16,20 These details are important when considering the utility of the recommendations (i.e., considerations of input from the public and those affected are essential elements of a robust recommendation for screening, and identification of target users is important for understanding the scope and purpose of the guideline).
Rigour of development is generally apparent for all of the 3 evidence-based guidelines, with all describing a consultation of the evidence by literature review (either systematic or with unclear methods).16,20,21 However, the strengths and limitations of the body of evidence are not clearly reported for 2 of the evidence-based guidelines (i.e., whereas critical appraisal for individual studies is reported, an assessment of the totality of the evidence considered is not).16,21 Similarly, external review is not clear for 2 of the guidelines,16,21 and a procedure for updating the recommendations is not clear for 2 of the guidelines.16,20
Presentation of the recommendations is generally clear for the 3 evidence-based guidelines.16,20,21 However, 1 guideline does not provide a clear and unambiguous recommendation in its wording; rather, indicating that universal NBS for cCMV should be considered (as opposed to providing a recommendation concerning whether it should or should not be adopted).20 This limits the utility of the recommendation, as it does not provide clear guidance concerning implementation. The applicability of the recommendations is generally not clearly reported in the 3 included evidence-based guidelines, with little to no guidance provided concerning how to implement the recommendations.16,20,21 Nonetheless, 1 of the guidelines described consideration of resource implications in the development of its relevant recommendation.16
A demonstration of editorial independence is clear for 1 of the evidence-based guidelines;20 nonetheless, 2 of the guidelines do not clearly describe whether the recommendations may have been influenced by the views of any funders,16,21 and 1 of the guidelines did not report potential conflicts of interest for guideline development group members.21
Additional details regarding the strengths and limitations of included publications are provided in Appendix 3.
Summary of Findings
Of the studies included in this review, 1 addressed clinical utility, 3 described cost-effectiveness, and 3 evidence-based guidelines stated recommendations relevant to universal NBS for cCMV.
Appendix 4 presents the main study findings.
Comparative Clinical Utility of Universal Newborn Screening for cCMV
Universal Versus Targeted NBS for cCMV
The prospective cohort study identified 443 cases of cCMV from 99,945 neonates (0.4%) who underwent universal NBS (i.e., only diagnosed cases were reported; numbers of cCMV screen positive results were not reported). Of the 443 neonates diagnosed with cCMV, 40 (9%) exhibited symptoms at birth and 35 (7.9%; 95% confidence interval [CI], 5.6 to 10.8) were later diagnosed with SNHL.19
Of the 443 neonates diagnosed with cCMV, 31 (7.0%; 95% CI, 4.8 to 9.8) did not pass the NHS. Of these 31 neonates, 20 were diagnosed with SNHL between 3 and 8 weeks of life and 11 were not. In addition to these neonates, 15 neonates with cCMV who passed the NHS were identified as having SNHL by the audiologic assessment between 3 and 8 weeks of life.19
Consequently, among the 35 neonates diagnosed with both cCMV and SNHL, 20 (57%) were identified by both universal NBS and targeted NBS programs, whereas 15 (43%) were not identified by targeted NHSs alone. Neonates with cCMV who exhibited symptoms at birth had a statistically significantly higher rate of SNHL (38%; 95% CI, 23.6 to 54.4) as compared to those who were asymptomatic (4.7%; 95% CI, 2.9 to 7.3).
Study authors concluded that, while a targeted NBS approach to cCMV identifies most of the neonates who are later found to be affected by SNHL as a consequence of cCMV, a substantial proportion of cCMV-associated SNHL cases were missed by the targeted NBS approach.19 The study authors urge that approaches to cCMV be improved to more effectively identify neonates who are at risk of cCMV-associated SNHL.19
Universal Versus No NBS for cCMV
No studies comparing the clinical utility of universal NBS versus no NBS for cCMV were identified; therefore, no summary of the evidence could be provided.
Comparative Cost-Effectiveness of Universal Newborn Screening for cCMV
Universal Versus Targeted NBS for cCMV
Of the 2 cost-effectiveness studies that reported ICERs, both reported that universal NBS for cCMV was cost-effective as compared to targeted NBS for cCMV (i.e., ICERs were less than 3, as expressed by GDP per capita).17,18 The Japanese study reported an ICER of ¥2,966,296,17 and the Chinese analysis generated an ICER of US$2,963.18 The third cost-effectiveness study also concluded that universal NBS for cCMV was more cost-effective than targeted NBS for cCMV (assuming all neonates identified with cCMV receive treatment with valganciclovir regardless of symptoms, and including projected loss-of-productivity costs), reporting an estimated saving of US$10.66 per newborn screened using a universal NBS strategy.22
The findings from the sensitivity analyses demonstrated that the prevalence or incidence of cCMV, the cost of the CMV screening test, the rate of development of SNHL, and the cost of antiviral treatment were the most influential variables with regard to cost-effectiveness.17,18,22 In the Japanese study, the most influential variable was the cost of the screening test, with ICERs ranging from ¥520,872 to ¥9,940,633 at various estimated costs for the screening test.17 In the Chinese study, the prevalence of cCMV was reported as the most influential variable, with ICERs ranging from US$1,390 to 9,011, depending on the prevalence estimates used.18 In the US cost-effectiveness analyses, only the cost of antiviral therapy was subjected to sensitivity analysis; though, the findings of these analyses were not reported for the comparison between universal NBS versus targeted NBS for cCMV.22
Universal Versus No NBS for cCMV
Of the 2 cost-effectiveness studies that reported ICERs, both reported that universal NBS for cCMV was cost-effective as compared to no NBS for cCMV (i.e., ICERs were less than 3, as expressed by GDP per capita).17,18 The Japanese study reported an ICER of ¥2,175,121,17 and the Chinese analysis reported and ICER of US$2,087.18 The third cost-effectiveness study also concluded that universal NBS for cCMV was more cost-effective than no NBS for cCMV (again, assuming all neonates identified with cCMV receive treatment with valganciclovir regardless of symptoms, and including projected loss-of-productivity costs), generating an estimated cost saving of US$37.97 per newborn screened.22
The findings from the sensitivity analyses in the Japanese cost-effectiveness study were not reported for the comparison between universal NBS for cCMV screening and no NBS.17 In the Chinese cost-effectiveness comparison between universal NBS for cCMV and no screening, sensitivity analyses again demonstrated that it was the estimated prevalence of cCMV in the population that was the most influential variable to cost-effectiveness, with ICERs ranging from US$932 to US$6,532.18 In the US cost-effectiveness analyses, the variable estimated costs of antiviral therapy produced an estimated range of cost savings between US$14.60 and US$61.34 per newborn screened using a universal NBS strategy for cCMV as compared to no NBS.22
Evidence-Based Recommendations Regarding the Use of Newborn Screening for cCMV
Of the 3 evidence-based guidelines included in this report,16,20,21 2 make recommendations against the use of universal NBS for cCMV16,21 and 1 makes a recommendation in favour of universal NBS for cCMV.20
The most recent evidence-based guideline included in this report (published in 2024 in Canada’s province of Quebec) recommends that universal NBS for cCMV not be added to the provincial newborn DBS program.16 The limited availability of appropriate evidence is indicated as 1 reason for the recommendation against universal NBS for cCMV.16 The quality of the studies reviewed was critically appraised; however, the quality of the evidence base is not graded or systematically characterized, and there is no strength of the recommendation provided.16
The other guideline recommending against universal NBS for cCMV was published in 2017 in the UK and reports an updated review of the evidence from a previous guideline that recommended against universal NBS for cCMV (published in 2012); similarly, the updated review concludes that the evidence remains insufficient to support universal NBS for cCMV.21 Again, the authors report critical appraisal of studies reviewed but do not describe the quality of the evidence base overall.21 Similarly, no strength of the recommendation is reported.21
The International Congenital Cytomegalovirus Recommendations Group published its guidance in 2017 and recommends that universal NBS for cCMV be considered.20 While no strength of the recommendation is indicated, the quality of the evidence supporting the recommendation was characterized as moderate (i.e., from nonrandomized studies).20 Notably, the recommendation does not clearly favour implementation of NBS for cCMV; rather “consideration” of NBS for cCMV,20 which may be interpreted as less clear than a recommendation supporting implementation. Unlike the other 2 evidence-based guidelines, the authors of this guideline do not describe concerns around the implementation of NBS for cCMV, such as costs, impacts to health systems, uncertainty around which neonates will most benefit from treatment, and potential harms of screening (e.g., false-positive screen results). In supporting statements, the group indicates that additional, high-quality (i.e., prospective) studies may further inform recommendations concerning universal or targeted NBS for cCMV.20
Limitations
This review identified 1 prospective cohort study,19 3 cost-effectiveness evaluations,17,18,22 and 3 evidence-based guidelines16,20,21 describing NBS for cCMV. Overall, the studies identified were limited in their coverage of relevant clinical outcomes, with HL being the focus of the findings (other outcomes of relevance to clinical utility were not described, including the number needed to screen, time to diagnosis, time to treatment, morbidity, mortality, and quality of life). This limits the findings of this report from describing a broader set of sequelae that are known to affect neonates with cCMV through infancy, childhood, and beyond, including developmental delays, learning difficulties, cerebral palsy, and visual impairments.4
Comparative evidence describing the clinical utility of universal NBS for cCMV was limited, with findings from 1 study published in the US in 2017 identified and summarized in this report.19 Some of the limitations of the study included no description of the precise timing of NBS and limited data describing long-term outcomes (i.e., findings from audiological assessments between 3 and 8 weeks were described).19 The effects of cCMV on other outcomes across a longer time frame were not described and remain unclear, limiting the interpretation of clinical utility in this report.
The 3 cost-effectiveness studies modelled data from Japan,17 China,18 and the US,22 which may have limited relevance to the Canadian context. The assumptions and variables used in the models may not be relevant in Canada, such as costs of screening and treatment. Furthermore, the cost-effectiveness models made assumptions concerning the effectiveness of screening and treatment that may not be characteristic of the care and outcomes experienced in real-world settings (e.g., the long-term effectiveness of antiviral treatments for the reduction of cCMV-associated HL remains unclear).5 This limits the generalizability of the findings from these studies.
Finally, the 3 evidence-based guidelines identified in this review make conflicting recommendations concerning the implementation of universal NBS for cCMV. While 1 guideline recommends in favour of universal NBS for cCMV,20 2 guidelines recommend against the implementation of universal NBS for cCMV.16,21 In addition, the recommendation in favour of universal NBS for cCMV is not clear, with guidance that favours consideration of universal NBS as opposed to clear guidance in favour of implementing NBS for cCMV.20 All of the guidelines make reference to the paucity of available clinical evidence to inform recommendations concerning the use of universal NBS for cCMV.16,20,21 Limited available clinical evidence was also identified in this report, which constrains the interpretation of its findings.
Conclusions and Implications for Decision- or Policy-Making
This report summarized and described 7 sources describing the comparative clinical utility and cost-effectiveness of universal NBS for cCMV, as well as evidence-based guidelines regarding NBS for cCMV.16-22 Of these, 1 prospective cohort study reported on the comparative clinical utility of universal NBS versus targeted NBS for cCMV,19 3 economic evaluations reported on the comparative cost-effectiveness of universal versus targeted or no NBS for cCMV,17,18,22 and 3 evidence-based guidelines make recommendations concerning universal NBS for cCMV.16,20,21
Overall, the limited clinical utility evidence and cost-effectiveness findings appear to be supportive of a universal approach to NBS for cCMV, as is also acknowledged by the authors of these studies.17-19,22 Specifically, a considerable proportion of neonates with cCMV and associated SNHL who were missed by targeted NHS were identified by a universal approach to NBS.19 Similarly, the 3 cost-effectiveness studies all reported a benefit of universal as compared to targeted NBS or no NBS for cCMV under a range of assumptions (though, all 3 papers also acknowledge a lack of available clinical evidence as a limitation of their work).17,18,22 The potential benefits of universal NBS for cCMV, including clinical and cost benefits (i.e., the opportunity for early treatment and potential reduction of long-term sequalae), as well as the opportunity for families to have a diagnosis for their affected infant(s), are widely acknowledged in the broader literature, as well.4,6,7,10,11 Nonetheless, 2 of the 3 evidence-based guidelines identified in this review are not supportive of the implementation of universal NBS for cCMV, generally citing the limited availability of meaningful and high-quality clinical evidence.16,20,21
This current lack of clinical evidence describing key considerations for NBS for cCMV is likewise acknowledged in the broader literature,1,2 and was also observed in this review, which consequently limits the findings of this report. Some of the key areas for clinical research that are yet needed to inform decision-making concerning universal NBS for cCMV include the effectiveness of screening and therapy for cCMV.1,2,8 While NBS programs that currently use DBS present an opportune infrastructure that may allow for the addition of cCMV screening, the limitations of DBS test performance for cCMV remain a barrier, with additional research needed to understand and develop this technology.1,4 In addition, the effectiveness of antiviral treatments for reducing cCMV-associated sequelae remains unclear, which similarly constitutes a barrier to establishing the utility and value of a universal NBS program for cCMV.2,5,8 The potential for overtreatment with antiviral medications has also been raised as a concern around universal NBS for cCMV.4 Importantly, research that includes long-term evaluation of the clinical utility of NBS for cCMV — and considers a range of outcomes broader than HL alone — is still needed.1,5 Another key consideration is health system readiness to manage the increased numbers of affected neonates that will be identified by a universal NBS program for cCMV — particularly given the unanswered questions concerning treatment and its effectiveness (particularly among neonates with cCMV who are asymptomatic).7
Jurisdictions where universal NBS for cCMV have been implemented12 offer the opportunity to support research that may elucidate these key considerations and inform evidence-based decision-making.4 The evidence-based guideline included in this review from INESSS highlights the importance of evidence generated by these recently established universal NBS programs to inform guidance and decision-making for other jurisdictions.16 As these universal NBS programs are able to generate and accrue data, there is opportunity to increase an understanding of the clinical utility of NBS for cCMV through evaluation and reporting,4 which can support and inform other jurisdictions in considering best approaches to NBS for cCMV — though, an imperative is needed to generate and report the necessary data to inform a more robust clinical evidence base for the universal NBS of cCMV.
Given the currently available clinical effectiveness and cost-effectiveness evidence, as well as available guidelines describing NBS for cCMV, deliberation and decision-making around the implementation of universal NBS for cCMV may also benefit from extra evidentiary sources; for example, clinical and public health expertise, as well as public (including families and those who may have been affected by cCMV), health payer, and other stakeholder input.
References
1.Lawrence SM, Goshia T, Sinha M, Fraley SI, Williams M. Decoding human cytomegalovirus for the development of innovative diagnostics to detect congenital infection. Pediatr Res. 2024;95(2):532-542. PubMed
2.Leber AL. Maternal and congenital human cytomegalovirus infection: laboratory testing for detection and diagnosis. J Clin Microbiol. 2024:e0031323. PubMed
3.Kim JH, Robles V, Weimer KED, Gehtland LM, Kucera KS. Improved Dried Blood Spot PCR Assay for Universal Congenital Cytomegalovirus Screening in Newborns. Microbiol. 2023:e0404122. PubMed
4.Gantt S. Newborn cytomegalovirus screening: is this the new standard? Curr Opin Otolaryngol Head Neck Surg. 2023;31(6):382-387. PubMed
5.Pinninti S, Boppana S. Congenital cytomegalovirus infection diagnostics and management. Curr Opin Infect Dis. 2022;35(5):436-441. PubMed
6.Pesch MH, Danziger P, Ross LF, Antommaria AHM. An Ethical Analysis of Newborn Congenital Cytomegalovirus Screening. Pediatrics. 2022;149(6):01.
7.Gantt S, Brophy J, Dunn J, et al. AMMI Canada: Response to FAQs about the management of children with congenital cytomegalovirus infection in Canada. J Assoc Med Microbiol Infect Dis Can. 2019;4(4):208-214. PubMed
8.Lazzarotto T, Blazquez-Gamero D, Delforge ML, et al. Congenital Cytomegalovirus Infection: A Narrative Review of the Issues in Screening and Management From a Panel of European Experts. Front Pediatr. 2020;8:13. PubMed
9.Samedi VM, Skappak C, Jantzie L, et al. Comparison of Presentation, Course, and Outcome of Congenital and Acquired Cytomegalovirus Infection in Twins. AJP Rep. 2016;6(1):e1-5. PubMed
10.Demmler-Harrison GJ. Newborn Dried Blood Spot Testing for Congenital Cytomegalovirus Screening: The Little Engine That Could. JAMA Pediatr. 2021;175(3):e205445. PubMed
11.Demmler Harrison GJ. Newborn Screening for Congenital Cytomegalovirus Infection...It Is Time. Clin Infect Dis. 2020;70(7):1385-1387. PubMed
12.CADTH health technology review: Newborn screening for cyongenital cytomegalovirus. Can J Health Technol. 2024;4.
13.Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377-384. PubMed
14.Drummond MF, Jefferson TO. Guidelines for authors and peer reviewers of economic submissions to the BMJ. The BMJ Economic Evaluation Working Party. BMJ. 1996;313(7052):275-283. PubMed
15.Brouwers MC, Kerkvliet K, Spithoff K, AGREE Next Steps Consortium. The AGREE Reporting Checklist: a tool to improve reporting of clinical practice guidelines. BMJ. 2016;352:i1152. PubMed
16.Institut national d'excellence en santé et services sociaux. Relevance of adding universal screening for congenital cytomegalovirus (CMV) infection to Québec newborn screening program: English summary. Quebec (QC): INESSS; 2024: https://www.inesss.qc.ca/fileadmin/doc/INESSS/Rapports/Depistage/INESSS_Depistage_icCMV_Summary.pdf. Accessed 2024 Mar 27.
17.Aoki H, Bitnun A, Kitano T. The cost-effectiveness of maternal and neonatal screening for congenital cytomegalovirus infection in Japan. J Med Virol. 2023;95(1):e28391. PubMed
18.Chen K, Zhong Y, Gu Y, et al. Estimated Cost-effectiveness of Newborn Screening for Congenital Cytomegalovirus Infection in China Using a Markov Model. JAMA Netw Open. 2020;3(12):e2023949. PubMed
19.Fowler KB, McCollister FP, Sabo DL, et al. A Targeted Approach for Congenital Cytomegalovirus Screening Within Newborn Hearing Screening. Pediatrics. 2017;139(2). PubMed
20.Rawlinson WD, Boppana SB, Fowler KB, et al. Congenital cytomegalovirus infection in pregnancy and the neonate: consensus recommendations for prevention, diagnosis, and therapy. Lancet Infect Dis. 2017;17(6):e177-e188. PubMed
21.Bazian Ltd. Newborn screening for cytomegalovirus: External review against programme appraisal criteria for the UK National Screening Committee (UK NSC). London (GB): UK National Screening Committee; 2017: https://view-health-screening-recommendations.service.gov.uk/document/334/download Accessed 2024 Mar 27.
22.Gantt S, Dionne F, Kozak FK, et al. Cost-effectiveness of Universal and Targeted Newborn Screening for Congenital Cytomegalovirus Infection. JAMA Pediatr. 2016;170(12):1173-1180. PubMed
23.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. PLoS Med. 2009;6(7):e1000100. PubMed
24.Forbes. Convert Japanese Yen To United States Dollar. 2024; https://www.forbes.com/advisor/money-transfer/currency-converter/jpy-usd/. Accessed 2024 Apr 17.
25.Ssentongo P, Hehnly C, Birungi P, et al. Congenital Cytomegalovirus Infection Burden and Epidemiologic Risk Factors in Countries With Universal Screening: A Systematic Review and Meta-analysis. JAMA Netw Open. 2021;4(8):e2120736. PubMed
26.UK National Screening Committee. UK NSC stakeholder engagement strategy 2022 to 2024. 2023; https://www.gov.uk/government/publications/uk-nsc-stakeholder-engagement/uk-nsc-stakeholder-engagement-strategy-2022-to-2024. Accessed 2024 Apr 7.
27.UK National Screening Committee. UK NSC Research and Methodology Group terms of reference. 2023; https://www.gov.uk/government/publications/uk-nsc-rmg-terms-of-reference/uk-nsc-research-and-methodology-group-terms-of-reference. Accessed 2024 Apr 7.
28.Orb QT, Pesch M, Allen CM, et al. Congenital Cytomegalovirus Testing Outcomes From the ValEAR Trial. Otolaryngol Head Neck Surg. 2024;28:28. PubMed
29.Phillips VL, Xu J, Park A, Gantt S, Dedhia K. The cost-effectiveness of targeted screening for congenital cytomegalovirus in newborns compared to clinical diagnosis in the US. Int J Pediatr Otorhinolaryngol. 2023;166:111450. PubMed
30.Schleiss MR, Panther L, Basnet S, Workneh M, Diaz-Decaro J. Comparison of Overall Sensitivity and Specificity across Different Newborn Screening Algorithms for Congenital Cytomegalovirus. Int J Neonatal Screen. 2023;9(2):14. PubMed
31.Manzar S, Pichilingue-Reto P, Bhat R. Successful Implementation of Single Urine Polymerase Chain Reaction Test for Evaluating Suspected Cytomegalovirus Infection in Neonates. Pediatr Qual Saf. 2022;7(4):e586. PubMed
32.Melamed R, Shemer-Avni Y, Shany E, Kurtzman L, Gorali R, Landau D. Targeted and universal screen in term and preterm infants for congenital CMV infection. Infect Dis. 2020;52(10):730-735. PubMed
33.Falkenius Schmidt K, Nystrom A, Karltorp E, Magnusson M, Lofkvist U. Long-term linguistic outcome in adults with congenital cytomegalovirus infection. Infect Dis. 2024;56(1):32-41. PubMed
34.Akiva MH, Hyde De Souza H, Lamarre V, et al. Identifying Clinical Criteria for an Expanded Targeted Approach to Screening for Congenital Cytomegalovirus Infection-A Retrospective Study. Int J Neonatal Screen. 2023;9(3):24. PubMed
35.Chasqueira MJ, Fernandez C, Marques A, et al. Pooling Saliva Sample as an Effective Strategy for the Systematic CMV Screening of Newborns-A Multicentric Prospective Study. Pediatr Infect Dis J. 2023;42(12):1117-1120. PubMed
36.Del Valle Penella A, Miller J, Rochat R, Demmler-Harrison G. Utility of Dried Blood Spots for the Diagnosis of Congenital Cytomegaloviruses within the First 21 Days of Life in a Single Center. Int J Neonatal Screen. 2023;9(3):04.
37.Gunlemez A, Kolayli F, Yazici Ozcelik E, et al. Congenital Cytomegalovirus Infection Screening in Newborns From Saliva Samples by Real-Time Polymerase Chain Reaction Analysis. Turk Arch Pediatr. 2023;58(4):371-375. PubMed
38.Izquierdo G, Farfan MJ, Villavicencio L, et al. Optimizing congenital cytomegalovirus detection by pool testing in saliva by a rapid molecular test. Eur J Pediatr. 2023;182(11):5131-5136. PubMed
39.Merino-Hernandez A, Sanchez-Barriopedro L, Villar-Castro S, Aguado-Del Hoyo A, Marsinyach-Ros I, Sanchez-Luna M. Cost-effectiveness of a cytomegalovirus screening strategy in neonates born after 34 weeks small for gestational age. An Pediatr (Engl Ed). 2023;98(1):41-47.
40.Chiereghin A, Pavia C, Turello G, et al. Universal Newborn Screening for Congenital Cytomegalovirus Infection - From Infant to Maternal Infection: A Prospective Multicenter Study. Front Pediatr. 2022;10:909646. PubMed
41.Letamendia-Richard E, Perillaud-Dubois C, de La Guillonniere L, et al. Universal newborn screening for congenital cytomegalovirus infection: feasibility and relevance in a French type-III maternity cohort. BJOG. 2022;129(2):291-299. PubMed
42.Dollard SC, Dreon M, Hernandez-Alvarado N, et al. Sensitivity of Dried Blood Spot Testing for Detection of Congenital Cytomegalovirus Infection. JAMA Pediatr. 2021;175(3):e205441. PubMed
43.Huang Y, Wang H, Li T, et al. Comparison of detection strategies for screening and confirming congenital cytomegalovirus infection in newborns in a highly seroprevalent population: a mother-child cohort study. Lancet Reg Health West Pac. 2021;12:100182. PubMed
44.Shlonsky Y, Smair NS, Mubariki R, et al. Pooled saliva CMV DNA detection: A viable laboratory technique for universal CMV screening of healthy newborns. J Clin Virol. 2021;138:104798. PubMed
45.Blazquez-Gamero D, Soriano-Ramos M, Vicente M, et al. Prevalence and Clinical Manifestations of Congenital Cytomegalovirus Infection in a Screening Program in Madrid (PICCSA Study). Pediatr Infect Dis J. 2020;39(11):1050-1056. PubMed
46.Nagel A, Dimitrakopoulou E, Teig N, et al. Characterization of a universal screening approach for congenital CMV infection based on a highly-sensitive, quantitative, multiplex real-time PCR assay. PLoS One. 2020;15(1):e0227143. PubMed
47.Pasternak Y, Oikawa MT, Mendelson E, Osovsky M, Klinger G, Bilavsky E. Diagnosing congenital cytomegalovirus by saliva on Guthrie paper. J Clin Virol. 2020;126:104337. PubMed
48.Vercauteren KOA, Keymeulen A, Mahieu L, et al. Prospective multicenter comparison of urine culture with PCR on dried blood spots using 2 different extraction and PCR methods in neonates suspected for congenital cytomegalovirus infection. Diagn Microbiol Infect Dis. 2020;97(3):115051. PubMed
49.Beswick R, David M, Higashi H, et al. Integration of congenital cytomegalovirus screening within a newborn hearing screening programme. J Paediatr Child Health. 2019;55(11):1381-1388. PubMed
50.Puhakka L, Lappalainen M, Lonnqvist T, et al. The Burden of Congenital Cytomegalovirus Infection: A Prospective Cohort Study of 20 000 Infants in Finland. J Pediatric Infect Dis Soc. 2019;8(3):205-212. PubMed
51.Viswanathan R, Bafna S, Mergu R, et al. Direct Saliva Real-time Polymerase Chain Reaction Assay Shows Low Birth Prevalence of Congenital Cytomegalovirus Infection in Urban Western India. Pediatr Infect Dis J. 2019;38(4):e65-e68. PubMed
52.Vives-Onos I, Codina-Grau MG, Noguera-Julian A, et al. Is Polymerase Chain Reaction in Neonatal Dried Blood Spots Reliable for the Diagnosis of Congenital Cytomegalovirus Infection? Pediatr Infect Dis J. 2019;38(5):520-524. PubMed
53.Fernandes C, Marques A, de Jesus Chasqueira M, et al. Saliva pools for screening of human cytomegalovirus using real-time PCR. Eur J Pediatr. 2021;180(4):1067-1072. PubMed
54.Yamada H, Tanimura K, Fukushima S, et al. A cohort study of the universal neonatal urine screening for congenital cytomegalovirus infection. J Infect Chemother. 2020;26(8):790-794. PubMed
55.Lu CY, Tsao PN, Ke YY, et al. Concurrent Hearing, Genetic, and Cytomegalovirus Screening in Newborns, Taiwan. J Pediatr. 2018;199:144-150.e141. PubMed
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Note that this appendix has not been copy-edited.
Table 2: Characteristics of Included Primary Clinical Study
Study citation, country, funding source | Study design | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Fowler et al. (2018)19 US Funding source: NIDCD grants N01-DC-5 to 0008 and HHSN-263 to 2012 to 00010-C; NIH (grant #s NR) | Prospective cohort | Neonates born at 7 US medical sites between 2007 and 2012 | Intervention: Universal NBS Sampling method: DBS and saliva, performed concurrently with targeted NBS Timing of screen: Described as ‘while in the newborn nursery’ (no quantitative time frame reported) Comparator: Targeted NHS Screening method: 2-stage hearing screening using ABR, performed concurrently with universal NBS Timing of screen: Described as ‘while in the newborn nursery’ (no quantitative time frame reported) | Outcomes of relevance: cCMV cases identified, cCMV symptomatology, NHS result, audiologic assessment result Follow-up: While in the newborn nursery; 3 to 8 weeks |
ABR = auditory brainstem response; cCMV = congenital cytomegalovirus; DBS = dried blood spot; NBS = newborn screening; NHS = newborn hearing screening; NIDCD = National Institute on Deafness and Other Communication Disorders; NIH = National Institutes of Health; NR = not reported
Table 3: Characteristics of Included Economic Evaluations
Study citation country, funding source | Type of analysis, time horizon, perspective | Population characteristics | Intervention and comparator(s) | Approach | Source of clinical, cost, and utility data used in analysis | Main assumptions |
|---|---|---|---|---|---|---|
Aoki et al. (2023)17 Country: Japan Funding source: Reported as none | Analysis type: CEA Time horizon: Lifetime Perspective: NR | Neonates from a 2021 birth cohort in Japan (N = 811,604) | Intervention: Universal NBS (i.e., urine PCR in the first 3 weeks of life) Comparators: Targeted NBS (i.e., NHS, with referrals followed by cCMV diagnostic testing No screening | Decision tree model | Clinical parameters: Published data from the Japanese context Cost data: Published studies and governmental data sources Discount rate: Japanese guideline i.e., 2% | Appropriate baseline investigation, treatment and follow-up were assumed for all cCMV and/or SNHL cases For all screening interventions, treatment with valganciclovir was assumed for cCMV positive infants |
Chen et al. (2020)18 Country: China Funding source: This study was funded in part by grants from the Jiangsu Science and Technology Department (BE2015655) and from Nantong Science and Technology Bureau (HS2016002). | Analysis: CEA Time horizon: Lifetime (i.e., 76 years) Perspective: Chinese health care system | Neonates from a simulated birth cohort in China (N = 15,000,000) | Intervention: Universal NBS (i.e., saliva and/or urine) after birth (quantitative time frame NR) Comparator: Targeted NBS (i.e., NHS, with referrals followed by cCMV diagnostic testing) No screening | Decision-analytic Markov model | Clinical and cost data: Published and referenced data sources Discount rate: 3.5% (source NR) | It was assumed that 25% of symptomatic cCMV cases would be diagnosed with no screening. It was assumed that the CMV diagnostic evaluation was 100% accurate |
Gantt et al. (2016)22 Country: US Funding sources: Child & Family Research Institute; NIH Institute on Deafness and Other Communication Disorders grants HHS-N-263 to 2012 to 00010-C, P01 HD10699, R01 DC02139; NIH Institute of Allergy and Infectious Disease grant P01 AI43681 | Analysis: CEA Time horizon: Lifetime (i.e., 79 years) Perspective: Public payer | Neonates (characteristics and N = NR) | Intervention: Universal NBS (i.e., saliva) within 3 weeks after birth Comparator: Targeted NBS (i.e., NHS, with referrals followed by cCMV diagnostic testing) No screening | Decision tree model | Clinical parameters: Published data from the US context Cost data: US Medicaid reimbursement costs and published, referenced sources Discount rate: 1% (in accordance with interest rates on US bods) | It was assumed that 25% of symptomatic cCMV cases would be diagnosed with no screening. Appropriate baseline investigation, treatment and follow-up were assumed for all cCMV and/or SNHL cases It was assumed that antiviral therapy had a long-term benefit to HL for cCMV cases. Loss-of-productivity costs were assumed for those with severe-to-profound HL. |
cCMV = congenital cytomegalovirus; CMV = cytomegalovirus; CEA = cost effectiveness analysis; DBS = dried blood spot; NBS = newborn screening; NHS = newborn hearing screening; NIH = National Institutes of Health; NR = not reported; PCR = polymerase chain reaction; SNHL = sensorineural hearing loss
Table 4: Characteristics of Included Evidence-Based Guidelines
Intended users, target population | Intervention and practice considered | Major outcomes considered | Evidence collection, selection, and synthesis | Evidence quality assessment | Recommendations development and evaluation | Guideline validation |
|---|---|---|---|---|---|---|
INESSS (2024)16 | ||||||
Intended users: NR Target population: Neonates | Universal NBS for cCMV using DBS | Clinical (i.e., test performance, effectiveness, screening safety) and economic. Additional considerations included populational, organizational, and sociocultural | A rapid review and a narrative literature review | Critical appraisal of included studies and guidelines | Consultation and deliberation among experts from an advisory committee and the CDP concerning the evidence and information reviewed | NR |
International Congenital Cytomegalovirus Recommendations Group (2017)20 | ||||||
Intended Users: NR Target Population: Neonates | Diagnosis (including NBS), prevention and therapy | Clinical i.e., test performance and utility | Systematic review | Studies were critically appraised and the evidence was graded | Consultation and deliberation among experts of the International Congenital Cytomegalovirus Recommendations Group concerning the evidence reviewed | Internal and external review of the final recommendations report |
UK National Screening Committee (2017)21 | ||||||
Intended Users: Health policy and decision-makers Target Population: Neonates | Universal NBS for cCMV | Clinical i.e., test performance and utility and guideline recommendations | Literature review (systematic search; 1 reviewer with unclear involvement of a 2nd reviewer); synthesis methods are NR but reporting uses narrative description | Critical appraisal of included studies and guidelines | Evidence was assembled to answer key questions posed against UK NSC criteria for appraising the value and appropriateness of screening programs Methods for applying the evidence to the key questions and criteria were NR While the report does not self-indicate as a guideline, evidence-based recommendations are included | NR |
cCMV = congenital cytomegalovirus; CDP = Comité délibératif permanent-Approches diagnostiques et dépistage; DBS = dried blood spot; INESSS = Institut national d'excellence en santé et services sociaux; NBS = newborn screening; NR = not reported
Appendix 3: Critical Appraisal of Included Publications
Note that this appendix has not been copy-edited.
Table 5: Strengths and Limitations of Clinical Study Using the Downs and Black Checklist13
Strengths | Limitations |
|---|---|
Fowler (2017)19 | |
Reporting
External validity
Internal validity
| Internal validity
Power
Other
|
HL = hearing loss; NBS = newborn screening
Table 6: Strengths and Limitations of Economic Evaluations Using the Drummond Checklist14
Strengths | Limitations |
|---|---|
Aoki (2023)17 | |
|
|
Chen (2020)18 | |
|
|
Gantt (2016)22 | |
|
|
HL = hearing loss
Table 7: Strengths and Limitations of Evidence-Based Guidelines Using AGREE II15
Item | INESSS (2024)16 | International Congenital Cytomegalovirus Recommendations Group (2017)20 | UK NSC21 |
|---|---|---|---|
Domain 1: scope and purpose | |||
1. The overall objective(s) of the guideline is (are) specifically described. | Yes | Yes | Yes |
2. The health question(s) covered by the guideline is (are) specifically described. | Yes | Yes | Yes |
3. The population (patients, public, etc.) to whom the guideline is meant to apply is specifically described. | Yes | Yes | Yes |
Domain 2: stakeholder involvement | |||
4. The guideline development group includes individuals from all relevant professional groups. | Yes | Yes | Yes |
5. The views and preferences of the target population (patients, public, etc.) have been sought. | Unclear | Unclear | Yes |
6. The target users of the guideline are clearly defined. | No | Unclear | Yes |
Domain 3: rigour of development | |||
7. Systematic methods were used to search for evidence. | Yes | Yes | Yes |
8. The criteria for selecting the evidence are clearly described. | Yes | Yes | Yes |
9. The strengths and limitations of the body of evidence are clearly described. | Unclear | Yes | Unclear |
10. The methods for formulating the recommendations are clearly described. | Yes | Yes | No |
11. The health benefits, side effects, and risks have been considered in formulating the recommendations. | Yes | Yes | Yes |
12. There is an explicit link between the recommendations and the supporting evidence. | Yes | Yes | Yes |
13. The guideline has been externally reviewed by experts before its publication. | Unclear | Yes | Unclear |
14. A procedure for updating the guideline is provided. | Unclear | Unclear | Yes |
Domain 4: clarity of presentation | |||
15. The recommendations are specific and unambiguous. | Yes | No | Yes |
16. The different options for management of the condition or health issue are clearly presented. | Yes | Yes | Yes |
17. Key recommendations are easily identifiable. | Yes | Yes | Yes |
Domain 5: applicability | |||
18. The guideline describes facilitators and barriers to its application. | No | No | No |
19. The guideline provides advice and/or tools on how the recommendations can be put into practice. | No | No | No |
20. The potential resource implications of applying the recommendations have been considered. | Yes | No | No |
21. The guideline presents monitoring and/or auditing criteria. | No | No | No |
Domain 6: editorial independence | |||
22. The views of the funding body have not influenced the content of the guideline. | Unclear | Yes | Unclear |
23. Competing interests of guideline development group members have been recorded and addressed. | Yes | Yes | No |
AGREE II = Appraisal of Guidelines for Research and Evaluation II; INESS = Institut national d'excellence en santé et services sociaux; NSC = National Screening Committee.
Appendix 4: Main Study Findings
Note that this appendix has not been copy-edited.
Table 8: Summary of Findings by Outcome — Comparative Clinical Utility of Concurrent Universal Versus Targeted NBS for cCMV
Study citation and study design | Outcome, Measure | Result | Main Conclusion(s) |
|---|---|---|---|
Fowler et al., 201719 Prospective cohort | cCMV diagnosis and symptoms, n/N (%) | “A targeted CMV screening approach does identify the majority of infants with CMV-related SNHL in the newborn period. However, this method fails to identify a significant number of infants with CMV-related SNHL during infancy highlighting the need to develop approaches to improve detection of CMV-related hearing loss at birth. Strategies to identify all infants with cCMV who remain at risk for late onset and progressive hearing losses are needed.” (p. 6) | |
cCMV diagnosis (neonates with a NHS) | 443/99,945 (0.4) | ||
Symptoms among cCMV cases | 40/443 (9.0) | ||
NHS referrals to audiological assessment (i.e., screen positive), n/N (%, 95% CI) | |||
cCMV positive | 31/443 (7.0, 4.8 to 9.8) | ||
Symptomatic | 11/40 (28.0, 15.0 to 44.0) | ||
Asymptomatic | 20/403 (5.0, 3.1 to 7.6) | ||
cCMV negative | 930/99,502 (0.9, 0.8 to 1.0) | ||
Group difference by cCMV status | P < 0.0001 | ||
SNHL diagnosed by audiological assessment (3 to 8 weeks of life), n/N (%, 95% CI) | |||
cCMV positive | 35/443 (7.9, 5.6 to 10.8) | ||
NHS Status | |||
Referred from NHS | 20/31 (65, NR) | ||
Passed NHS | 15/412 (3.6, NR) | ||
Symptom Status | |||
Symptomatic | NR (38.1, 23.6 to 54.4) | ||
Asymptomatic | NR (4.7, 2.9 to 7.3) | ||
cCMV negative, n/N | NR | ||
Group difference by cCMV status | NR | ||
cCMV = congenital cytomegalovirus; CMV = cytomegalovirus; NHS = newborn hearing screening; NR = not reported; SNHL = sensorineural hearing loss
Table 9: Summary of Findings by Outcome — Comparative Cost-Effectiveness of Universal Versus Targeted or No NBS for cCMV
Analyses and relevant parameters | Comparison | Main Conclusion(s) | |
|---|---|---|---|
No Screening | Targeted Screening | ||
Aoki (2023)17 | |||
Model estimates for relevant clinical parameters | “This study suggested that... universal newborn screening with valganciclovir treatment for those fulfilling treatment criteria... may be cost-effective [sic] than a targeted newborn screening program. The cost effectiveness of the universal newborn screening with valganciclovir treatment strategy is a robust finding and its implementation should be strongly considered.” (p. 6/9) | ||
Additional cCMV cases identified | 2,516 | 2,511 | |
Additional cCMV cases treated (valganciclovir) | 398 | 193 | |
Additional cCMV cases with reduced SNHL due to treatment | 60 | 8 | |
Costs and cost-effectiveness estimates (JPY) | |||
Total incremental cost | 1,296,258,974 | 1,418,787,054 | |
Incremental medical costs | 3,856,015,251 | 3,773,721,707 | |
Parental productivity costs saved | 258,373,777 | 240,675,757 | |
Incremental education costs saved | 2,301,382,500 | 2,115,167,493 | |
Incremental QALYs gained | 596 | 478 | |
ICER (JPY/QALY gained) | 2,175,121 | 2,966,296 | |
Expressed as Japanese GDP/capita | NR | 0.74 | |
One-way sensitivity estimates of ICERs for influential variables, low to high | |||
Incidence of cCMV | — | 156,050 to 6,195,089 | |
Rate of developing SNHL | — | 1,913,140 to 5,098,663 | |
Cost of urine PCR test | — | 520,872 to 9,940,633 | |
Chen (2020)18 | |||
Model estimates for relevant clinical parameters | “This evaluation demonstrated that universal screening could be cost-saving and more effective compared with targeted screening or no screening. Many children with cCMVi in China could benefit each year from newborn CMV screening, early detection, and interventions. The results presented in this study could be used by Chinese policy makers to make an informed decision about the scale-up of universal screening programs. While the results are specific to China, the model may be easily adapted to health settings in other middle-income countries. Further research is warranted to include long-term indirect costs, estimate health state utilities in the Chinese population, and conduct PSAs to reflect uncertainty in the economic estimates.” (p. 10/13) | ||
Additional cCMV cases identified | 101,325 | 97,501 | |
Additional cCMV cases treated (antiviral therapy) | 12,108 | 9,276 | |
Mild-to-moderate cases of cCMV-associated HL avoided | 1,331 | 1,008 | |
Severe-to-profound cases of cCMV-associated HL avoided | 985 | 488 | |
Cost and cost-effectiveness estimates (USD) | |||
Total incremental cost | 264,114,151 | 261,079,770 | |
Incremental QALYs gained | 126,540 | 88,125 | |
ICER (USD/QALY gained) | 2,087 | 2,963 | |
Expressed as Chinese GDP/capita | < 1 to 3 | < 1 to 3 | |
One-way sensitivity estimates of ICERs for influential variables, low to high | |||
Prevalence of cCMV | 932 to 6,532 | 1,390 to 9,011 | |
Cost of CMV PCR test | 1,199 to 4,754 | 1,705 to 6,734 | |
Cost of antiviral treatment | 2,027 to 2,628 | 2,879 to 3,717 | |
Gantt (2016)22 | |||
Model estimates for relevant clinical parameters | “Newborn screening for cCMV infection appears to be cost-effective under a wide range of assumptions. Universal screening offers larger net savings and the greatest opportunity to provide directed care. Targeted screening also appears to be cost-effective and requires testing for fewer newborns. These findings suggest that implementation of newborn cCMV screening programs is warranted.” (p. 1173) | ||
Incremental mean reduction in severe to profound HL, (assuming treatment for all cCMV cases with HL at birth), % (95% CI) | 13 (5.3 to 21) | 3.3 (NR) | |
Cost estimates (USD) | |||
Incremental mean cost to identify 1 case of cCMV infection, $ | |||
Assuming $10/test | 2,000 | 1,434 | |
Assuming $50/test | 10,000 | 7,168 | |
Incremental mean cost to identify 1 case of cCMV-associated HL, $ | |||
Assuming $10/test | 27,460 | 26,485 | |
Assuming $50/test | 90,038 | 86,122 | |
Incremental mean cost to prevent 1 cochlear implant, $ | |||
Assuming $10/test | 4,064,157 | 4,024,756 | |
Assuming $50/test | 12,620,277 | 12,348,330 | |
Incremental mean cost (-) or saving (+) per newborn undergoing screening (assuming valganciclovir treatment for all cCMV cases with HL identified at birth), $ | |||
Direct (excluding loss-of-productivity) | −6.83 | −11.78 | |
Sensitivity estimates for valganciclovir benefit, low to high | −12.98 to −0.68 | NR | |
Net (including loss-of-productivity) | 37.97 | 10.66 | |
Sensitivity estimates for valganciclovir benefit, low to high | 14.60 to 61.34 | NR | |
cCMV = congenital cytomegalovirus; cCMVi = congenital cytomegalovirus infection; GDP = gross domestic product; HL = hearing loss; JPY = Japanese Yen; NR = not reported; PCR = polymerase chain reaction; SNHL = sensorineural hearing loss; USD = US dollar(s)
Table 10: Summary of Recommendations in Included Evidence-Based Guidelines
Recommendations and supporting evidence | Quality of evidence and strength of recommendations |
|---|---|
INESSS (2024)16 | |
Relevant recommendation: “INESSS does not recommend adding universal screening for congenital cytomegalovirus infection to the blood testing platform of the Québec newborn screening program.” (p. 5) | Quality of the evidence: While individual studies were critically appraised, there was no systematic grading of the quality of the body of evidence supporting the recommendation described in the report. Strength of the recommendation: NR |
Relevant supporting statements: “The CDP members raised several arguments against screening, the main ones being the lack of evidence of its effectiveness, the absence of reliable markers to discern the severity of cases and the risk of overdiagnosis (absence of health gains) for most of the asymptomatic children detected. In addition, the blood test that would be favoured by the Québec newborn screening program currently shows sub-optimal performance, and no program that has implemented universal CMV screening has yet published results. Finally, the addition of such screening would have significant organizational impact.” (p. 5) “INESSS remains open to a re-evaluation when there is evidence in the literature on the performance of programs that use dried blood samples, on the effectiveness of universal screening or on the effectiveness of treatment in a wider range of patients.” (p. 5) | |
International Congenital Cytomegalovirus Recommendations Group (2017)20 | |
Relevant recommendations: “The group recommended that consideration should be given to universal neonatal cytomegalovirus screening to enable early detection of congenital cytomegalovirus-infected infants, facilitating early detection and intervention for sensorineural hearing loss and developmental delay where appropriate (level 2b evidence).” (pp. e182 to 3) “The diagnosis of congenital cytomegalovirus-infected neonates should include real-time PCR of saliva, urine, or both within the first 3 weeks of life, with saliva as the preferred sample.” (p. e178) | Quality of the evidence: Level 2b evidence i.e., cohort or case-control studies Strength of the recommendation: NR |
Relevant supporting statement: “Additional prospective studies and cost-effectiveness studies would further inform any recommendation regarding universal or targeted cytomegalovirus testing of neonates.” (p. e182) | |
UK National Screening Committee (2017)21 | |
Relevant recommendation: “Screening recommendations based on the current review: The findings of this review indicate that the current recommendation not to perform universal newborn screening for CCMV should be maintained.” (p. 6) | Quality of the evidence: While individual studies were critically appraised, there was no systematic grading of the quality of the body of evidence supporting the recommendation described in the report. Strength of the recommendation: NR |
Relevant supporting statements: “Newborn screening is not recommended because: 1. An option for newborn screening would be to test a saliva sample but research is needed to understand more about it. 2. No reliable way of knowing which babies are going to develop long-term health problems from cytomegalovirus infection. The review found some research looking in to this. It included looking at newborn blood test results or scanning the baby’s brain. But this would also need more research to ensure that these approaches were reliable and safe. 3. Screening is likely to identify a greater number of infants with cCMV than is currently the case. These are likely to have minimal symptoms or no symptoms. The management and treatment approach for these children is unclear, and it is unknown whether screening improves their outcomes.” (p. 3) | |
cCMV = congenital cytomegalovirus; CDP = Comité délibératif permanent-Approches diagnostiques et dépistage; cCMV = congenital cytomegalovirus; INESS = Institut national d'excellence en santé et services sociaux; NR = not reported; PCR = polymerase chain reaction
Appendix 5: Ineligible Studies With Relevance to the Research Questions
Table 11: Summary of Abstracts — Studies Comparing NBS Programs for cCMV
Study citation, country, Study design | Reason(s) for exclusion | Study characteristics | Relevant findings and conclusions | ||||
|---|---|---|---|---|---|---|---|
Population and Setting | Intervention (n patients) | Comparator(s) or reference test (n patients) | Relevant outcome(s) | Results | Conclusions | ||
Orb et al., 202428 Country: NR Study design: Prospective survey | Wrong outcome | Neonates Setting: Multicentre (N = 82) | Universal NBS (7,677) Sample type: NR Timing of NBS: Described as ‘early’ | Targeted NBS Screen method: NHS referral (9,017) Delayed DBS (535) Timing of NHS: Described as ‘early’ | cCMV positivity rates | cCMV positivity, % Universal: 0.5 Targeted:
| “Rates of cCMV positivity differed among the 3 approaches. The rates are comparable to cohort studies reported in the literature.” |
Phillips et al., 202329 Country: US Study design: Cost-effectiveness analysis | Wrong intervention | Neonates Setting: NR | Targeted NBS (NR) Screening method: NHS referral Timing of NBS: NR cCMV diagnostic method NR | No screening (NR) | Cost-effectiveness: Additional HL cases identified Cost per neonate screened Cost per case of HL identified Overall cost | Additional cases of HL identified by targeted NBS, n: 38 per 10,000 (± 22) Incremental cost per neonate screened, $b:: 2.96 (± 2.26) Incremental cost per case of HL identified, $: 8,197 (± 4,217) Estimated overall cost of targeted NBS for all neonatesc, $: 193,229 | “Although cases numbers are small, our model shows that targeted newborn screening and cCMV testing reduced cases of HL progression. Adoption of newborn targeted screening as standard of care should be considered given it may prevent disability at very low cost.” |
Schleiss et al., 202330 Country: NR Study design: Modelling study | Wrong outcome | Neonates Setting: NR | Universal NBS algorithms (NR) Sample types: urine, saliva, DBS Timing of NBS: NR | Targeted NBS algorithms (NR) Screen method: Hearing targeted one-fail; Hearing targeted two-fail Timing of NBS: NR Both methods followed with urine/saliva or DBS confirmatory diagnostic testing | Screen algorithm performance | Overall sensitivity, % Universal algorithms:
Targeted algorithms:
| “Universal screening using DBS testing and universal screening using saliva and urine testing can potentially detect 312 and 373 more cCMV cases per 100,000 live births, respectively, than two-fail serial testing. Overall, implementing universal cCMV newborn screening would improve cCMV detection, ultimately leading to better health outcomes.” |
Manzar et al., 202231 Country: NR Study design: Retrospective study | Wrong comparison; wrong outcome | Neonates Setting: Single centre | Universal NBS from 2020 to 2021 (97) Sample type: 3 urine samples Timing of NBS: NR | Universal NBS, from 2021 to 2022 (149) Sample type: 1 urine sample Timing of NBS: NR | cCMV sample evaluation rate Screening cost | cCMV evaluation rate, % 3 samples: 53.6 1 sample: 98.6 Monthly average cost per neonate screened, $ 3 samples: 39.5 1 sample: 70.1 | “The intervention resulted in reducing waste and improving resource utilization.” |
Melamed et al., 202032 Country: NR Study design: Retrospective study | Wrong comparison; wrong outcome | Neonates Setting: NR | Targeted NBSa i.e., premature neonates born before 33 weeks gestation (549) Sample type: Urine Timing of NBS: Described as “soon after birth” | Targeted NBS i.e., NHS referral or growth restricted (2,078) Screen method: NR Timing of NBS: Described as “soon after birth” | cCMV positivity rates | cCMV positivity, n/N(%) Targeted NBS (premature neonates): 0/549 (0) Targeted NBS (NHS referral or growth restricted): 19/2,078 (0.9) | “A joint strategy of targeted CMV screening in infants who fail hearing screen test with universal screen of premature infants can select infants at risk of hearing impairment due to congenital CMV soon after birth, allows for timely initiation of treatment and prevents dilemmas regarding congenital CMV diagnosis in infants who fail hearing screen in a later age until universal screen will be widely adopted.” |
bVL = birth viral load; cCMV = congenital cytomegalovirus; CI = confidence interval; CMV = cytomegalovirus; DBS = dried blood spot; HL = hearing loss; NBS = newborn screening; NHS = newborn hearing screening; NPA = negative percent agreement; NPV = negative predictive value; NR = not reported; PCR = polymerase chain reaction; PPA = positive percent agreement; PPV = positive predictive value; RT = real time; SGA = small for gestational age; SNHL = sensorineural hearing loss.
Note: This table has not been copy-edited.
aWhile the study describes the intervention targeted to premature neonates as ‘universal’, it has been characterized in this report as a targeted strategy (i.e., targeted to premature neonates only; not universal to all neonates).
bCurrently NR
cThe time frame over which the cost estimate applies was not reported.
Table 12: Summary of Abstracts — Studies Not Comparing NBS Programs
Study citation, country, Study design | Reason(s) for exclusion | Study characteristics | Relevant findings and conclusions | |||
|---|---|---|---|---|---|---|
Population and Setting | Intervention (n patients) | Relevant outcome(s) | Results | Conclusions | ||
Falkenius et al., 202433 Country: Sweden Study design: Retrospective case-control | Wrong comparison | Neonates who tested positive for cCMV and were asymptomatic at birth; controls who tested negative for cCMV Setting: Observational study | Universal NBS for cCMV administered between 197 and 1985 (56) Sample types: NR Timing of NBS: NR cCMV diagnostic method NR | Long-term linguistic measures: two-word fluency (measured as adequate/not compared to Swedish norms); word retrieval Long-term follow-up with participants as adults, aged 34 to 43 years | Adequate two-word fluency, %:
Total retrieved words, n:
| “This study suggests that adults with cCMV infection may have deficits in the word retrieval process, even in the absence of known neurodevelopmental disorders. Long-term effects of cCMV infection may exist even in those with asymptomatic infection at birth.” |
Akiva et al., (2023)34 Country: NR Study design: Retrospective cohort | Wrong intervention; wrong comparison; wrong outcome | Neonates Setting: Single centre between 2014 and 2018 | Targeted NBS administered from 2014 to 2018 (465) Relevant screen method: NHS Timing of NBS: NR cCMV diagnostic method NR | cCMV cases | cCMV cases, n/N (%): 22/465 (4.7) | “In addition to CMV screening of newborns who fail the NHS, these data suggest that certain clinical signs of cCMV-in particular: thrombocytopenia, growth impairment, and HIV exposure in pregnancy-should be additional criteria for expanded targeted newborn CMV screening, where universal screening is not yet the standard of care.” |
Chasqueira et al., (2023)35 Country: Portugal Study design: Prospective cohort | Wrong comparison; wrong outcome | Neonates Setting: Multicentre (N = 7) | Mass NBS administered between 2020 and 2022 (7,033) Sample types: saliva (i.e., pools, N = 704) Timing of NBS: NR cCMV diagnosis of individual screen positives confirmed by urine | cCMV screen positivity (pools and individuals) cCMV cases Study prevalence of cCMV | cCMV screen positivity, n:
cCMV cases, n: 15 cCMV study prevalence, % (95% CI) :0.21 (0.12 to 0.35) | “In this study, the pooling strategy proved to be effective for the systematic screening of newborns, although this low prevalence raises questions regarding the cost-effectiveness of implementing universal screening.” |
Del Valle Penella et al., 202336 Country: NR Study design: Retrospective cohort | Wrong comparison; wrong outcome | Neonates diagnosed with cCMV Setting: NR | Approach to NBS NR (NBS was not conducted for cCMV; NBS samples collected for other conditions were retrospectively assessed) (89) Sample type: DBS Timing of NBS: First 21 days of life cCMV diagnostic method NR | Screen test performance (compared to the reference standard i.e., diagnostic testing for cCMV cases only) cCMV cases with HL identified by DBS | Screen test performance, %:
cCMV cases with HL identified by DBS, %: 100 | “These results suggest that DBS-based testing is useful in the diagnosis of cCMV, and its performance may be related to levels of CMV viremia. DBS testing accurately identified those patients with congenital/early onset hearing loss and those at risk of developing late-onset hearing loss.” |
Gunlemez et al., (2023)37 Country: NR Study design: Prospective cohort | Wrong comparison; wrong outcome | Neonates Setting: Single centre between 2020 and 2021 | Universal NBS (545) Sample type: Saliva (328) Timing of NBS: First day of life (before first feeding) cCMV diagnosis confirmed by testing urine and/or blood samples in screen positive neonates | cCMV screen positives False-positive screens cCMV cases | cCMV screen positives, n: 6 False positive screens, n: 5 cCMV case, n: 1 | “It has been concluded that the frequency of congenital cytomegalovirus infection is low in our study group and studying saliva samples showed high false-positive rates. It is seen that saliva is not a suitable sample for detecting cytomegalovirus deoxyribonucleic acid by real-time polymerase chain reaction method.” |
Izquierdo et al., (2023)38 Country: NR Study design: Prospective cohort | Wrong comparison; wrong outcome | Neonates Setting: NR | Universal NBS, using a point-of-care rapid molecular test (1,642) Sample type: Saliva (pool-testing N = 328 pools) Timing of NBS: < 21 days of life cCMV diagnosis confirmed by saliva and urine; viral load tested in blood for cCMV cases | cCMV cases Point-of-care screen pool-test performance | cCMV infection cases, n/N (%) Universal: 8/1,642 (0.49) Pool-testing performance, %:
False-positive results in individuals, %: 0.12 | “CMV pool-testing using a rapid molecular test in saliva proved feasible when compared to PCR gold standards.” |
Merino-Hernandez et al., 202339 Country: Spain Study design: Retrospective cohort | Wrong comparison | Neonates born ≥ 34 weeks gestation with SGA Setting: Single centre | Targeted NBS administered in 2019 (259) Screen method: Clinical suspicion Sample type: Urine (plus head ultrasound) | cCMV positivity Cost-effectiveness (cumulative cost) | cCMV positivity rate, %: 0.54 Cumulative cost per asymptomatic cCMV case identified, €: 17,000 | “In our population, screening for congenital CMV infection in asymptomatic late preterm and term newborns whose only risk factor is SGA does not seem to be cost effective.” |
Chiereghin et al., 202240 Country: Italy Study design: Prospective cohort | Wrong comparison | Neonates Setting: Multicentre (N = 3) | Universal NBS (3,151) Sample type: Saliva Timing of NBS: Within the first 21 days of life cCMV diagnosis confirmed by saliva and urine | cCMV cases Screen test performance (i.e., false positive screen results) Symptoms among cCMV cases SNHL in infancy (measured at 5 months of age) | cCMV cases, n/N (%): 21/3,151 (0.66) False positive rate, %: 7.5 Symptoms among cCMV cases, n/N (%): 3/21 (14.3) Cases with moderate unilateral SNHL at 5 months after birth: 1/21 (4.7) | “Without universal neonatal CMV screening, some infected infants who develop late neurological sequelae may not be recognized and, consequently, they are not able to benefit early from instrumental and therapeutic interventions to limit and/or treat CMV disease.” |
Letamendia-Richard et al., 202241 Country: France Study design: Retrospective cohort | Wrong comparison; wrong outcome | Neonates Setting: Single centre between 2016 and 2020 | Universal NBS (15,341) Sample types: Saliva Timing of NBS: Described as ‘at birth’ cCMV diagnosis confirmed by urine | cCMV cases cCMV cases with/without clinical suspicion Acceptability of screening test among health care staff | cCMV cases, n/N (%): 63/15,341 (0.4) cCMV cases with clinical suspicion, n/N (%): 24/63 (38) cCMV cases without clinical suspicion, n/N (%): 39/63 (62) Health care staff reporting acceptability of screening, %: > 90% | “Universal screening for cCMVI with CMV PCR on saliva samples is feasible and highly acceptable to parents and healthcare providers. Over half (62%) of the cases had no prenatal/neonatal signs of cCMVI or a maternal history of CMV infection during pregnancy and would probably not have been diagnosed without universal screening.” |
Dollard et al., 202142 Country: US Study design: Prospective cohort | Wrong comparison; wrong outcome | Neonates Setting: Multicentre (N = 8) | Universal NBS administered between 2016 and 2019 (12,554) Sample types: DBS and saliva Timing of NBS: 1 to 2 days after birth cCMV diagnosis confirmed with urine | cCMV cases Screen test performance of DBS NBS Screen test performance of saliva NBS | cCMV cases, n: 56 Overall test performance, % (95% CI): DBS:
Saliva:
| “This study demonstrates relatively high analytical sensitivity for DBS compared with previous studies that performed population-based screening.” |
Huang et al., 202143 Country: US Study design: Cohort | Wrong comparison; wrong outcome | Neonates Setting: NR | Universal NBS (6,350) Sample types: Saliva, urine, or saliva and urine Timing of NBS: NR cCMV diagnosis confirmed with saliva and urine | cCMV cases Screen test performance | cCMV cases, n: 49 Screen test performance, %:
| “In populations with high seroprevalence, saliva screening with saliva and urine confirmation might be an alternative strategy for screening cCMV infections. The suggested timeframes for screening and confirmation are within 13 (ideally 5) and 21 (ideally 13) days of birth, respectively.” |
Shlonsky et al., 202144 Country: NR Study design: Prospective cohort | Wrong comparison; wrong outcome | Neonates Setting: Single centre | Universal NBS conducted in 2019 (1,000) Sample types: single saliva samples, saliva pools Timing of NBS: Within 24 hours of birth cCMV diagnosis confirmed by urine | cCMV cases Screen test performance | cCMV cases, n (%): 6 (0.6) Screen test performance, %: Single saliva samples:
Saliva pools:
| “Pooling saliva of healthy newborns appears to be a reliable method to identify asymptomatic cCMV infection when positive results are confirmed by urine CMV DNA. Pooling in sizes appropriate to the cCMV prevalence rate may improve the laboratory workflow and decrease costs. Further studies should evaluate the clinical implications of this widespread cCMV pooled screening technique.” |
Blazquez-Gamero et al., 202045 Country: Spain Study design: Prospective cohort | Wrong comparison; wrong outcome | Neonates Setting: Single centre | Universal NBS (3,190) Sample types: Saliva Timing of NBS: Within the first 72 hours of life cCMV diagnosis confirmed by urine | cCMV screen positives cCMV cases Screen test performance cCMV cases with symptoms | cCMV screen positives, n/N (%): 24/3190 (0.75) cCMV cases, n/N (%, 95% CI): 15/3190 (0.47, 0.29 to 0.77) Screen test performance, % (95% CI):
Symptomatic cCMV cases, n: 2 | “One in 200 neonates born in our hospital presented a cCMV infection. CMV viral load in saliva has been shown to be a simple and highly accepted screening method but should be confirmed by CMV detection in urine. … diagnosis during the neonatal period would have been impossible without a screening program in most cases.” |
Nagel et al., (2020)46 Country: NR Study design: Cross-sectional | Wrong comparison; wrong outcome | Neonates Setting: NR | Universal NBS (NR) Sample types: Saliva Timing of NBS: NR cCMV diagnosis confirmed by testing blood and/or urine samples | cCMV screen positives cCMV cases | cCMV screen positives, n/N: 34/NR cCMV cases, n/N: 18/34 | “Clinical follow-up of these newborns with confirmed cCMV infection should reveal whether the risk of late-onset cCMV disease correlates with CMV DNA load in early life saliva samples and whether a cut-off can be defined identifying cCMV infected infants with or without risk for late-onset cCMV disease.” |
Pasternak et al., 202047 Country: NR Study design: Case-control | Wrong intervention i.e., not universal NBS; wrong comparison; wrong outcome | Neonates with and without cCMV Setting: Single centre | cCMV screen test conducted from 2018 to 2019 (cCMV cases = 42; cCMV negative = 41) Sample type: Saliva applied to Guthrie paper Timing of NBS: NR Diagnostic confirmation reported as ‘standard methods’ | Screen test performance | Screen test performance, % (95% CI):
| “CMV testing with saliva real-time PCR on Guthrie paper displayed a high sensitivity and specificity, rendering it a powerful screening test. The accuracy, simplicity of sampling, storage and transportation and the potential reliance on existing logistic resources, establishes this method as a candidate for cCMV universal screening programs.” |
Vercauteren et al., 202048 Country: Belgium Study design: Prospective cohort | Wrong comparison; wrong outcome | Neonates Setting: Multicentre (N = 6) | Targeted NBS (276) Screen method: Clinical suspicion Sample types: DBS vs. urine Timing of NBS: NR | cCMV cases by sample type | cCMV cases, n/N(%): DBS: NR Urine: 48/276 (17.4) | “Not all [DBS] methods successfully detected urine-culture-positive neonates born after first-trimester seroconversions... all urine-culture-positive neonates having clinical signs of cCMV did consistently score positive.” |
Beswick et al., 201949 Country: Australia Study design: Prospective cohort | Wrong comparison | Neonates Setting: Multicentre (N = 3) | Targeted NBS administered between 2014 and 2016 (234) Screen method: NHS referral Timing of NBS: NR Sample type: Saliva cCMV diagnostic method NR | cCMV screen positives cCMV cases cCMV cases with HL | cCMV screen positive, n/N (%): 8/234 (3.4) cCMV cases, n: 3 cCMV cases with HL, n/N (%, 95% CI): 2/55 (3.64, 0.44 to 12.53) | “Incorporating cCMV testing into Universal Newborn Hearing Screening within Queensland is realistic and achievable, both practically and financially.” |
Puhakka et al., 201950 Country: Finland Study design: Case-control | Wrong comparison | Neonates Setting: Multicentre (N = NR) | Universal NBS (19,868) Sample type: Saliva Timing of NBS: NR cCMV diagnostic method NR | cCMV cases Symptomatic cCMV cases Neurodevelopment at 18 months of age (Griffith’s scale) Otoacoustic emission testing at 18 months of age (cases vs. controls) Ophthalmologic testing | cCMV cases, n, n/1000 (95% CI): 40, 2/1000 (1.4 to 2.6) Symptomatic cCMV cases, n/N (%): 4/40 (10) Neurodevelopment score, mean:
Otoacoustic emission test failures, n/N:
Ophthalmologic testing:
| “The prevalence of cCMV was low, and outcomes at 18 months of age did not differ between the infected infants and healthy control infants. With such a low burden in Finland, universal newborn screening for cCMV seems unwarranted.” |
Viswanathan et al., 201951 Country: India Study design: Prospective cohort | Wrong comparison | Neonates Setting: Single centre | Universal NBS (750) Sample type: Saliva Timing of NBS: NR cCMV diagnosis confirmed by testing saliva, blood and urine samples | cCMV cases Survival to 1 year of age Sequelae at 1 year of age | cCMV cases, n/N (%, 95% CI): 3/750 (0.4, 0.13 to 1.2) Survival to 1 year of age, n/N (%) : 3/3 (100) Sequelae at 1 year of age, n/N (%): 0/3 (0) | “The use of direct real-time polymerase chain reaction of saliva samples can be considered as a feasible option for newborn screening of congenital CMV infection in developing countries. Relatively low birth prevalence of cCMV infection was observed in our study, which needs to be corroborated through further studies.” |
Vives-Onos et al., 201952 Country: Spain Study design: Retrospective case-control | Wrong intervention i.e., not universal NBS; wrong comparison; wrong outcome | Neonates Setting: Multicentre (N = 10) | cCMV screen test (cCMV positive = 103; cCMV negative = 81) Sample type: DBS Timing of NBS: NR cCMV diagnosis confirmed by ‘any body fluid’ | Screen test performance | Screen test performance, % (95% CI):
| “The sensitivity of CMV… DBS in our series was low and correlated with the bVL. Thus, a negative DBS result would not rule out cCMV infection, especially in patients with a low viremia level at birth.” |
Fernandes et al., 202153 Country: Portugal Study design: Prospective cohort | Wrong comparison | Neonates Setting: Multicentre (N = 2) | Universal NBS (1,492) Sample type: Saliva pools (150) Timing of NBS: NR cCMV diagnosis confirmed by urine | cCMV screen positives cCMV cases | cCMV screen positives, n: 14 cCMV cases, n (%, 95% CI): 10 (0.67, 0.36 to 1.23) | “The use of saliva pools proved to be effective for the screening of this congenital infection, allowing timely screening and confirmation in a large population, with associated cost reduction.” |
Yamada et al., 202054 Country: NR Study design: Prospective cohort | Wrong comparison | Neonates Setting: Multicentre (N = 3) | Universal NBS (11,736) Sample types: Urine Timing of NBS: NR cCMV diagnostic method NR Symptomatic cCMV cases were treated with valganciclovir for 6 weeks or 6 months | cCMV cases cCMV cases with/without symptoms Symptomatic cases treated with valganciclovir, Treated cases with normal development/mild sequelae | cCMV cases, n/N (%): 56/11,736 (0.48) cCMV cases with symptoms, n/N: 23/56 cCMV cases without symptoms, n/N: 33/56 Symptomatic cCMV cases treated with valganciclovir, n/N: 20/23 Treated cases with normal development/mild sequelae, %: 58 | “…a series of universal neonatal urine screening, diagnosis, workup, and VGCV therapy for neonates with symptomatic cCMV may decrease neurological impairments… The universal urine screening likely identifies subclinical symptomatic cCMV.” |
Lu et al., 201855 Country: NR Study design: Prospective cohort | Wrong comparison | Neonates Setting: Single centre in 2016 | Universal NBS assessed in a 2016 cohort study (1,716) Sample type: NR Timing of NBS: NR cCMV diagnostic method NR | cCMV cases Audiologic assessment of cCMV cases at birth and 3 months | cCMV cases, n(%): 3 (0.2) Failure of audiologic assessment among cCMV cases, n: Birth: 0 3 months: NR | “This study confirms the feasibility of performing hearing… and CMV screenings concurrently in newborns and provides evidence that the incorporation of these screening tests could potentially identify an additional subgroup of infants with impaired hearing that might not be detected by the NHS programs.” |
cCMV = congenital cytomegalovirus; CCMVI = congenital cytomegalovirus infection; CI = confidence interval; CMV = cytomegalovirus; DBS = dried blood spot; DTA = diagnostic test accuracy; HL = hearing loss; NBS = newborn screening; NHS = newborn hearing screening; NPA = negative percent agreement; NR = not reported; NS = not statistically significant; PCR = polymerase chain reaction; PPA = positive percent agreement; SGA = small for gestational age; VGVC = valganciclovir.
Note: This table has not been copy-edited.
Appendix 6: References of Potential Interest
Systematic Reviews
Ineligible Systematic Review (No Study Selection Criteria Reported)
Hilditch C, Liersch B, Spurrier N, Callander EJ, Cooper C, Keir AK. Does screening for congenital cytomegalovirus at birth improve longer term hearing outcomes? Arch Dis Child. 2018 Oct;103(10):988-992. PubMed
Guidelines and Recommendations
Guidance With No Apparent Link to Evidence
2022.Congenital Cytomegalovirus Screening Guidelines. Tallahassee (FL): Florida Department of Health, Florida Newborn Hearing Screening (NBHS) Program; 2022: https://floridanewbornscreening.com/wp-content/uploads/CMV-Screening-Guidelines-FINAL.pdf. Accessed 2024 Mar 27.
Relevant Position and Other Statements With No Explicit Recommendation(s) Regarding NBS
Position Statement on Universal Congenital Cytomegalovirus Screening in Canadian Newborns. Toronto (ON): Canadian Infant Hearing Task Force; 2022: https://canadianaudiology.ca/wp-content/uploads/2022/04/SAC_cCMV-Position-statement_EN.pdf. Accessed 2024 Mar 27.
Barton M, Forrester AM, McDonald J, Canadian Paediatric Society Infectious Diseases and Immunization Committee. Update on congenital cytomegalovirus infection: Prenatal prevention, newborn diagnosis, and management. Ottawa (ON): Canadian Paediatric Society; 2020: https://cps.ca/en/documents/position/update-on-congenital-cytomegalovirus-infection-prenatal-prevention-newborn-diagnosis-and-management. Accessed 2024 Mar 27.
Review Articles
Commentary on 1 of The Cost-Effectiveness Assessments Included in This Report
Hilditch C, Keir AK. Cost-effectiveness of universal and targeted newborn screening for congenital cytomegalovirus infection. Acta Paediatr. 2018 May;107(5):906. PubMed
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up to date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca