CADTH Health Technology Review
Choline Supplementation for Infants, Children, and Pregnant People
Rapid Review
Key Messages
What Is the Issue?
Choline is an essential nutrient produced by humans and animals and is important during pregnancy, fetal growth, and the development of the brain and nervous system. Most people do not get enough choline from their diet.
Fetal alcohol spectrum disorders (FASD) are a set of conditions where fetuses have been exposed to alcohol and this affects memory, learning, and development from early childhood to later life.
Choline supplements are products used to complement choline-deficient diets. Given the role of choline in fetal development, choline supplements are a potential intervention to support pregnancy or to mitigate the developmental harms in children from prenatal exposure to alcohol if supported by evidence of their effectiveness for these purposes.
What Did We Do?
To inform decisions about the use and timing of choline supplementation to support health outcomes in infants and children, CADTH sought to identify and summarize the literature about the effectiveness and safety of choline supplementation given to any pregnant people or given to children with either prenatal alcohol exposure or FASD. We also attempted to identify evidence-based recommendations for using choline supplementation in these populations.
We searched key resources and conducted a focused internet search for relevant evidence published since 2014. One reviewer screened articles for inclusion based on predefined criteria, critically appraised the included studies, and narratively summarized the findings.
What Did We Find?
We found few publications investigating this topic, and several studies had low statistical power and imprecise results. The clinical evidence was mixed depending on whether choline was given to the pregnant person or child, which interventional groups were compared, what the clinical exposures or diagnoses were in the study population, the time point and duration of choline supplementation, which outcomes were measured, and how old children were during follow-up.
For choline supplementation in healthy pregnant people, evidence was mixed for infant and child neurocognitive and neurodevelopmental outcomes or behavioural symptoms; there were little-to-no differences in safety outcomes.
For choline supplementation in pregnant people exposed to alcohol, evidence was mixed for infant and child neurocognitive and neurodevelopmental outcomes, body size, and brain region sizes; some minor side effects were reported overall.
For choline supplementation in children with FASD, most evidence showed little-to-no benefits for neurocognitive and neurodevelopmental outcomes, and brain structure; limited evidence showed higher fishy body odour and some other unspecified adverse symptoms for children given choline.
Guidelines based mostly on low-quality evidence or expert opinion recommend that all pregnant people, including those with gestational diabetes mellitus or on vegan or vegetarian diets, increase their choline intake through diet or supplements.
We did not find clinical effectiveness evidence for choline supplementation in infants with FASD, or guidelines regarding choline supplementation in either infants or children with FASD, that met inclusion criteria for our report.
What Does it Mean?
Health care professionals and decision-makers can use this evidence to inform decisions around applicability of choline supplementation for pregnant people, or for infants and children with FASD, in their practice.
There may be a need to balance the knowledge that choline intake is low at the population level and important for fetal development with the identified clinical effectiveness evidence for choline supplementation, which was limited and mixed for all evaluated patient populations.
Careful consideration of the following may also be important to inform decisions about the appropriateness of choline supplementation: the care plan and other intensive and concurrent interventions for children with FASD; stigma and challenges faced by pregnant people and children in the context of prenatal alcohol exposure; cultural dietary practices; and accessibility, cost, and availability of supplements.
Abbreviations
FASD
fetal alcohol spectrum disorders
PAE
prenatal alcohol exposure
RCT
randomized controlled trial
SR
systematic review
Key Terminology
Gender: “Gender can refer to the individual and/or social experience of being a man, a woman, or neither. Social norms, expectations and roles related to gender vary across time, space, culture, and individuals.”1
Nonbinary: “An umbrella term for gender identities that fall outside of the man-woman binary.”1
Pregnant person: In this Rapid Review, this term refers to anyone who is pregnant and is inclusive of all sexes and genders. Where included study authors conducted research for a specific sex or gender group (e.g., women), or where the authors report the sex or gender of the population, they are reported in this Rapid Review as the study authors describe them.
Trans: “An umbrella term referring to people whose gender identities differ from the sex they were assigned at birth. “Trans” can mean transcending beyond, existing between, or crossing over the gender spectrum. It includes but is not limited to people who identify as transgender, transsexual, nonbinary or gender nonconforming (gender variant or genderqueer).”1
Research Questions
What is the clinical effectiveness of choline supplementation during pregnancy for health outcomes in infants and children?
What is the clinical effectiveness of choline supplementation in infants and children with prenatal alcohol exposure or fetal alcohol spectrum disorders?
What are the evidence-based guidelines regarding choline supplementation for infants, children, or pregnant people?
Context and Policy Issues
What Is Choline and Choline Supplementation?
Choline is an essential nutrient that is needed for animal and plant cell membrane integrity, metabolism, and functioning of the brain and nervous system; it is specifically important for mood, memory, muscle control, cell membrane signalling, and early brain development.2,3 During pregnancy, choline demand is higher because it plays a role in the safety of the pregnant person and in the growth and development of the fetus, the brain, and the placenta.2,4 A lack of choline can result in adverse outcomes such as neural tube defects, cognitive deficits, and fatty liver disease in fetuses, or preeclampsia or hypertension in the pregnant person.2,4 Studies in animals and humans have shown that lower maternal choline intake is associated with more neural tube defects in children, and that higher choline intake in pregnant people is associated with better neurocognitive function in children.5
Dietary choline can come from animal sources such as eggs, fish, poultry, and dairy products, and from plant sources with lower levels of choline, such as seeds, whole grains, cruciferous vegetables, beans, and nuts.3,5 Choline is also available as a dietary supplement that can be provided alone, as a multivitamin product, or combined with B-complex vitamins; they can be in different forms, including phosphatidylcholine, citicoline-CDP—choline, choline bitartrate, choline chloride, alpha glycerophosphocholine, or lecithin.2,4-6
Although humans can produce choline in their bodies, the amount is not high enough to meet requirements; they may need additional choline through the diet or through supplements.5 Certain groups may be more likely to have inadequate choline levels such as pregnant people, those with genetic variations involved in choline pathways, and infants and adults who need parenteral nutrition where food consumption bypasses the gastrointestinal tract.5 Canadian data show that across multiple ages, genders, pregnancy stages, and jurisdictions, choline intake from food and supplements is less than the recommended intake.7,8
What Are FASDs?
FASD are a group of diagnoses that can lead to long-lasting disability and result from prenatal alcohol exposure (PAE); alcohol is harmful to human development and can lead to issues with memory, learning, social skills, motor skills, attention, social skills, and over 400 comorbidities.9,10 FASD is not necessarily caused by people knowingly drinking alcohol while pregnant, something that is completely preventable or specific to a certain group of people, although it is frequently stereotyped as such.11 The social determinants of health also play a large role in the incidence of FASD.11 A 2017 meta-analysis showed the worldwide prevalence in children up to 16 years old was 7.7 per 1000.12 In Canada, data on this condition is scarce; some research suggests that its prevalence is 7.9 per 1,00013 and other data shows that between 0.1% and 3% of children and youth have a FASD diagnosis.10 FASD may be higher in populations with limited access to care or in equity-deserving groups.14 There may also be inequities in how children with FASD access services and are supported by the health care system.11 Accurate diagnosis and early and long-term support are important in helping people manage the disorder and prevent lifelong difficulties.10 Interventions for FASD include behavioural and education therapy, medication, medical specialists (e.g., speech-language pathologist, mental health professional, physical therapist), parent training, creative art therapy, and auditory training.15 The inequities in the distribution of FASD across equity-deserving groups, and the way the social determinants of health can affect its manifestation, development, and management are important considerations for appropriate patient care; however, these elements are not directly assessed within the scope of this review.
Why Is it Important to Do This Review?
Given that pregnant people have low dietary intakes of choline and that choline is important for fetal development, it is necessary to understand whether choline supplementation during pregnancy improves outcomes in infants and children and to identify guidelines around supplementation during pregnancy.
Research in animal models has suggested that choline supplementation in offspring with PAE can decrease harmful structural, behavioural, and cognitive effects, even after alcohol exposure has stopped; however, it is unclear whether choline supplementation is effective or recommended for children with PAE or FASD.6,16-18
Therefore, the current report aims to review the evidence on choline supplementation broadly in pregnant people and, more specifically, in children with PAE or FASD who require multiple supports to determine its effects on health outcomes in children. This report also aims to summarize any recommendations on choline supplementation for pregnant people and for children with PAE or FASD.
Objectives
To support decision-makers by identifying, summarizing, and critically appraising evidence on the clinical effectiveness of or recommendations on choline supplementation in pregnant people, and in children with PAE or FASD.
Methods
Literature Search Methods
An information specialist conducted a literature search on key resources including MEDLINE, the Cochrane Database of Systematic Reviews, the International HTA Database, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search approach was customized to retrieve a limited set of results, balancing comprehensiveness with relevancy. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. Search concepts were developed based on the elements of the research questions and selection criteria. The main search concepts were choline, pregnancy, and FASD or PAE. Additional searches were also conducted using the search concepts choline or FASD/PAE; CADTH-developed search filters were applied to limit retrieval to guidelines. Retrieval was limited to the human population. The searches were completed on January 4 and 5, 2024 and limited to English-language documents published since January 1, 2014. To capture a fuller range of literature on FASD/PAE, additional searching was also conducted in Embase and Scopus for research question 2.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening titles and abstracts were reviewed, and then potentially relevant full-text articles were retrieved and assessed for inclusion in the second level of screening. The final set of full-text articles is based on the inclusion criteria in Table 1.
Criteria | Description |
|---|---|
Population | Q1 and Q3: Pregnant people Q2 and Q3: Infants and children with PAE or FASD |
Intervention | Choline supplementation |
Comparator | Q1 and Q2: Placebo, no choline (e.g., multivitamins), alternative doses of choline supplementation, usual care Q3: No comparator necessary |
Outcomes | Q1 and Q2: Clinical benefits (e.g., infant or child outcomes related to cognition, memory, growth, motor skills, behaviour) and harms (e.g., adverse events) Q3: Recommendations regarding best practices for choline supplementation (e.g., indications for use, optimal timing for supplementation, type of choline supplementation intervention) |
Study designs | Health technology assessments, systematic reviews, randomized controlled trials, nonrandomized studies, evidence-based guidelines |
FASD = fetal alcohol spectrum disorder; PAE = prenatal alcohol exposure.
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1 or were duplicate publications.
Articles were also excluded if:
choline supplementation was considered an exposure in an association study but clinical benefits or harms of choline supplementation were not reported
they were broadly about supplementation but did not describe supplements or mention choline
they measured outcomes in plasma, umbilical cords, or human milk
the intervention was a combination of supplements where the effect of choline could not be determined.
Systematic reviews (SRs) in which all relevant studies were captured in other more recent or more comprehensive SRs were excluded. Primary studies retrieved by the search were excluded if they were captured in 1 or more included SRs. Guidelines with unclear methodology or that did not specify pregnant people, or infants and children with PAE or FASD were also excluded.
Critical Appraisal of Individual Studies
One reviewer critically appraised the included SR using A MeaSurement Tool to Assess systematic Reviews 2 (AMSTAR 2),19 randomized controlled trials (RCTs) using the Downs and Black checklist,20 and guidelines using the Appraisal of Guidelines for Research and Evaluation (AGREE) II instrument.21 Summary scores for the included studies were not calculated; rather, the strengths and limitations of each included publication were described narratively in this report.
Equity Considerations
CADTH recognizes the need for and importance of equity considerations in health technology reviews. In this Rapid Review, PROGRESS-Plus22 was used to guide data extraction and report writing. Each included publication was checked to determine if PROGRESS-Plus22 criteria were reported by study authors to describe the participants; detailed characteristics, if available, were then extracted and reported in tables in Appendix 2. The main PROGRESS-Plus22 criteria include place of residence, race/ethnicity/culture/language, occupation, gender/sex, religion, education, socioeconomic status, and social capital. As part of report writing, we provide a discussion of these characteristics across the evidence, where available, when presenting results within the text.
We did not conduct an explicit search for information related to inequity or equity-deserving groups in relation to choline supplementation in pregnancy, or for children with PAE or FASD. We are aware that pregnant people who have consumed alcohol during pregnancy or have children with FASD experience stigma by the public, media, health care providers (e.g., clinician stereotyping), and institutions and that this can be harmful to their health; they may be worried about sharing their alcohol use history, feel uncomfortable seeking health care, experience judgment, shame, or social isolation, and this may prevent pregnant people from getting the health and social resources they need.23-25 This Rapid Review does not include an equity analysis of these issues, which may be better suited to a dedicated review around equity considerations for choline supplementation so that these topics can be understood properly.
When reporting on sex or gender in this Rapid Review, we retained the language used by the original study authors if research was conducted specifically for women or investigators recorded participant-identified gender. In all other cases, we use the term pregnant people when referring to this population. In addition, when reporting on race or ethnicity, whenever possible, we referred to these groups based on guidance from the CADTH Style Guide at the time this Rapid Review was conducted, with an understanding that language is constantly evolving. Otherwise, we reported race and ethnicity terminology as described by the original study authors.
Summary of Evidence
Quantity of Research Available
This report includes clinical effectiveness evidence from 1 SR26 and 3 RCTs27-30 (1 RCT was based on 2 publications28,29), and recommendations from 4 guidelines31-34 (2 guidelines32,33 had companion articles35,36 describing further details on methodology or the recommendations).
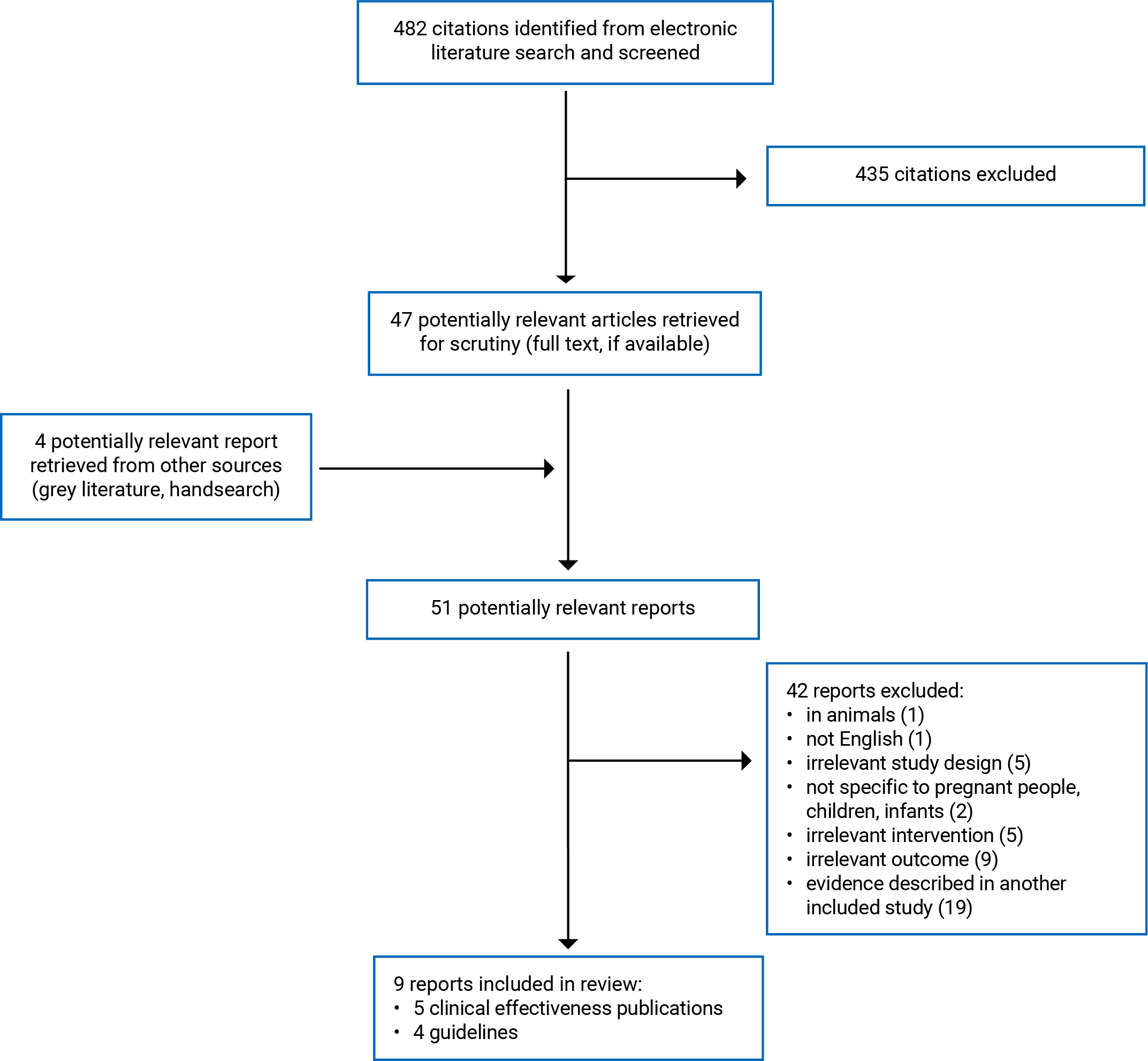
Appendix 1 presents the PRISMA37 flow chart of the study selection. Appendix 5 includes additional references of potential interest such as publications with evidence already in included studies, ongoing trials, a SR protocol, nonsystematic reviews, recommendations with unclear methods, and a non-English article.
Summary of Study Characteristics
Appendix 2 contains detailed characteristics of included publications.
Included Studies for Clinical Effectiveness
The SR26 included 10 publications based on 7 RCTs conducted in South Africa, Ukraine, US. The 3 RCTs were conducted in South Africa and the US; 2 of the RCTs28-30 included in this review were conducted in a population that was also included in the SR but reported results for a different sample, different outcome, or different follow-up time.26
Intervention-comparisons included:
Choline supplementation versus placebo.26,28-30
Type of choline supplementation included phosphatidylcholine, choline bitartrate, or glycerophosphocholine liquid.
Doses of choline supplementation varied by type of supplement and population (i.e., healthy pregnant person, alcohol-exposed pregnant person, or child with FASD)
High-dose choline chloride supplementation (930 mg/day) versus low dose (480 mg/day) choline chloride supplementation for healthy pregnant person26,27
Choline supplementation (750 mg/day) plus multivitamin versus multivitamin only for alcohol-exposed pregnant person26 (choline type not reported).
Across all studies, populations included pregnant people in their second or third trimester who were described as healthy,26 had no alcohol or tobacco use,27 or were exposed to alcohol;26,30 or children with PAE or FASD.26,28,29 Dietary assessments for choline adequacy at baseline were not well reported across studies; average choline intake was assessed in 1 primary study within the SR26 and most pregnant people included in 1 identified RCT were reported to have choline deficiency.30 Pregnant people were aged 26.6 to 28.4 years old and were all described as women; sex and gender were not explicitly reported. Children were assessed from birth to 11.44 years old across studies. Two publications27,29 reported child sex and 1 reported child gender.28 For the 2 publications28,29 of the same trial, 1 publication reported child gender28 and 1 reported child sex.29 The included SR26 did not report the sex and gender of the included children. Articles did not report how sex and gender were defined or measured or on sex or genders outside male and female.
Two studies reported education levels of participants,27,30 2 reported family income27 or socioeconomic status,30 2 reported child race (based on 3 publications),27-29 2 reported child ethnicity (based on 3 publications),27-29 and 1 reported whether English was a primary language for children.27 One article29 indicated that race was self-identified; no other articles indicated how race or ethnicity was recorded. No other PROGRESS-Plus criteria,22 such as place of residence, occupation, religion, social capital, or disability status were reported.
Effectiveness outcomes in children included:
neurocognitive outcomes measuring cognitive functioning, memory, attention, and reasoning, including physiological responses to tasks (e.g., saccade reaction time, brain electrical activity)
parent-reported behaviour measuring early signs of schizophrenia (e.g., attention symptoms, withdrawn symptoms, behavioural issues)
brain or body size or structure (e.g., weight, head circumference, brain region sizes).
Safety outcomes in children were only reported in the included SR26 and not any of the included RCTs.
Included Guidelines
All guidelines provided broad nutrition recommendations for both diets and supplements that had specific sections on choline, among other micronutrients; there were no guidelines that only focused on choline. Three32-36 were conducted by groups in the US (not-for profit health care professional group, government department, and academic group), and 1 from a medical professional society in Canada.31 Three were for pregnant people in the general population31,33,34,36 and 1 was for pregnant people with gestational diabetes mellitus (GDM).32,35
No guidelines were found regarding choline supplementation for children with PAE or FASD.
Summary of Critical Appraisal
Appendix 3 contains detailed about strengths and limitations of included publications.
Clinical Effectiveness Studies
Systematic Review
The SR’s26 strengths included clear reporting of the research question of interest, establishing review methods and registration beforehand, performing study screening and data extraction in duplicate, and discussing bias and heterogeneity of included studies when summarizing the evidence.
A limitation of the SR26 is that the search strategy may not have been comprehensive since 1 database was searched; there may have been other relevant studies in other databases or in the grey literature that could have contributed to the findings. In addition, the sources of funding for each included article were not reported; it is unclear whether there may have been any conflicts or bias in these studies. Some SR authors26 also received funds from the pharmaceutical company that sponsored the review and that manufactures supplements including those for pregnant people; it is unclear whether this affected the review. The SR authors26 also mentioned limitations of the included studies such as low adherence, high dropout rates, short study duration, missing data, low generalizability, and unplanned testing or analyses.
Randomized Controlled Trials
Across included RCT publications,27-30 there were clearly reported objectives, population criteria, interventions, main outcomes, and study findings. Authors declared no conflicts of interest, or funder participant in study conduct. Participants and the research team were blinded to study assignment; all RCTs27-30 included a placebo that was consumed in the same way as the intervention (fruit-flavoured drink). This may have reduced performance bias (e.g., where participants may be treated differently if researchers knew what treatment they received, or participants self-reported outcomes differently if they knew what study group they were in) or detection bias (e.g., outcome assessors measuring outcomes differently by knowing study assignment).
All trials were randomized to aim to make study groups comparable and attribute study findings to the effect of the intervention. One RCT27 indicated groups were well matched and that participants lost to follow-up were no different from those who remained in the study. Another trial28,29 reported that groups differed by race and had issues with missing data and loss to follow-up; authors indicated that because of a small sample size, confounding effects could not be explored.
The authors of all RCTs indicated issues with small sample sizes. One RCT27 conducted a power calculation and found statistically significant results for some outcomes, the authors of the other RCTs indicated that there was not enough power to detect effects.28-30 The generalizability of populations in each trial is also unclear since each was different from another and may be different from the general population; 1 trial27 reported including highly educated white mothers who had not consumed alcohol and whose children were mostly male, another trial30 reporting including pregnant people who reported drinking during pregnancy, had inadequate choline intake, and were economically disadvantaged with low education levels, and the third trial28,29 was reported on a racially diverse group of children with FASD.
Guidelines
All guidelines31-36 clearly outlined their scope and purpose, who the target users and intended population of the guideline were, and had a grading system for assessing the quality of evidence used to make recommendations. Two guidelines32,33,35,36 conducted SRs, 1 conducted literature searches,34 and one31 indicated consulting literature but did not provide details (e.g., databases searched). Three guidelines31,32,34,35 presented each recommendation in an easily identifiable way (e.g., recommendation statements separated from explanatory text, tables within body of guideline to organize statements).
It is unclear whether any of the guidelines specifically included views and preferences of the target population; 1 guideline33,36 mentioned seeking feedback from the public. For 3 guidelines,31,33,34,36 the specific processes for creating recommendations (e.g., voting, consensus) were not reported. For 2 guidelines,31,33,36 the explicit links to the evidence did not follow clearly from recommendation statements. Two guidelines31,34 did not report supporting documents or tools to aid readers in understanding or implementing recommendations. For 3 guidelines,31,33,34,36 it is unclear whether there were any conflicts of interest in guideline development; 1 of these guidelines34 included authors who developed prenatal supplements or had pending patents on prenatal supplements.
Summary of Findings
Appendix 4 presents the main study findings.
We found clinical effectiveness evidence for choline supplementation in:
healthy pregnant people
pregnant people exposed to alcohol
children with FASD.
We found guidelines for choline supplementation for:
pregnant people
lactating people
pregnant people with GDM
pregnant people consuming vegetarian or vegan diets.
Clinical Effectiveness and Safety of Choline Supplementation in Healthy Pregnant People
Choline Versus Placebo
Infants and children birthed by individuals who received choline supplementation during their healthy pregnancy showed better early results for neurocognitive outcomes and later had little-to-no differences in these outcomes compared with infants and children of those who were given placebo, specifically:
infants showed better cerebral inhibition, a sign of fetal development, at 1 month26
infants showed little-to no differences in cerebral inhibition, global cognitive development, language, visuospatial perception, discrimination, or memory, or long-term episodic memory between groups from 3 to 12 months.26
Children who were 40-months old had lower parent-reported attention issues and withdrawn symptoms on a questionnaire to detect schizophrenia, and little-to-no difference in behavioural issues on the same questionnaire.26
Safety results from the included SR26 had limited information:
One trial reported little-to-no difference in adverse events between groups and no serious adverse events were reported overall
Another trial reported 7 preterm births in the placebo group and 4 in the choline group (no statistical significance given) and little-to-no difference in infant weight, length, head circumference, perinatal complications, and general health using Apgar scores.
High-Dose Choline Versus Low-Dose Choline
Infants and children birthed by individuals who received a higher choline supplement dose during their healthy pregnancy showed mixed evidence for neurocognitive outcomes compared to infants and children of those who were given a lower dose:
infants up to 13 months old had faster reaction times and little-to-no difference in predictive cascades26
children who were 7 years old had better attention during a signal detection task (i.e., they had better signal detection and were better at detecting difficult stimuli) and little-to-no difference in false alarms, omissions, and off-task behaviours.27
One trial in the included SR26 indicated that no adverse events were reported by any participants.
Clinical Effectiveness and Safety of Choline Supplementation in Pregnant People Exposed to Alcohol
Choline Versus Placebo
Infants birthed by individuals who were exposed to alcohol during pregnancy and received choline supplementation showed mixed results for neurocognitive outcomes compared to infants who were given placebo:
infants who were 6.5 months old had little-to-no difference in learning and memory measured by eyeblink conditioning, but the choline group had higher increases in conditioned responses26
infants who were 12 months old showed better visual recognition memory as measured by FTII, a test of infant intelligence, which was based on 1 RCT from the included SR (no numerical results reported)26 and little-to-no difference in FTII score measured in a smaller sample of the same trial which focused on investigating brain measurements.30
Infants from birth to 12 months had higher increases in weight and head circumference,26 and greater sizes in 6 out of 12 brain regions when birthed by individuals who were exposed to alcohol during pregnancy and received choline supplementation compared with infants of those who received placebo during pregnancy.30
There were unclear results for safety. Dyspepsia and nausea were reported in 1 trial in the included SR;26 it is unclear which study participants these data were for (e.g., pregnant person, child, intervention, or comparator group).
Choline and Multivitamin Versus Multivitamin Only
Infants birthed by individuals exposed to alcohol during pregnancy and given choline supplementation with multivitamin showed mixed results for neurocognitive outcomes compared to infants of those who were given multivitamin only:
infants who were 4 to 11 months old had better information processing and learning based on heart rate responses to visual stimuli26 and little-to-no difference in score for mental development, psychomotor development, and behaviour at 6 months26
Safety outcomes were not reported for this comparison.
Clinical Effectiveness and Safety of Choline Given to Children With FASD
We found evidence for children with FASD given choline supplementation; no evidence was found for infants with FASD given choline supplementation. Overall, evidence differed depending on child age at intervention, trial duration, and which outcome was measured. Some benefits were seen when older children were given choline supplementation.
Children with FASD between ages 2.5 and 5 years given choline supplementation for 9 months were little-to-no different for neurocognitive outcomes from children with FASD given placebo:
little-to-no difference in global cognitive development or elicited imitation memory but those aged 2.5 to 4 years had the greatest improvement in elicited imitation delayed performance suggesting that age may moderate this effect
little-to-no differences in brain functioning and memory measured by brain electrical activity.28
Children with FASD aged 5 to 10 years given choline supplementation for 6 weeks were little-to-no different for neurocognitive outcomes from children with FASD given placebo:
little-to-no differences in paired-associate learning, design fluency, spatial working memory, spatial working memory strategy, quotient attention-deficit/hyperactivity disorder, and fine motor speed.26
Children with FASD aged 8.6 years on average who were given choline supplementation for 4 years had better intelligence scores compared to children with FASD given placebo:
children in the supplementation group had better nonverbal IQ and working memory; there were statistically significant subscores for nonverbal visual-spatial reasoning and nonverbal working memory.26
Children with FASD and an average age of 10.56 years given choline supplementation for 9 months showed mixed results for neurocognitive outcomes and brain structures compared to children with FASD and an average age of 11.44 years given placebo:
little-to-no differences in digit span, picture span, visual scanning, number sequencing, letter sequencing, number/letter sequencing, word reading, inhibition, and inhibition/switching; the choline group showed better motor speed and colour naming29
little-to-no differences in 7 of 8 brain white matter microstructures; 1 microstructure (the splenium) was better in the choline group.29
Safety results from the included SR26 had limited information in the choline group:
in 1 trial, choline was reported to be well-tolerated in children (no further details provided) and children in the choline group reported higher levels of fishy body odour (no statistical significance given) at 4 years of follow-up
in another trial, there were little-to-no differences in adverse events; however, children in the choline group reported more adverse events in specific symptom categories (no further details provided).
Guidelines for Pregnant People
Based on limited, low-quality, or unclear evidence, the identified guidelines31-36 made weak to fair recommendations for increased choline intake during pregnancy through diet or supplementation, given that intake is known to be lower in pregnant people and is important for maternal health and fetal development. Three guidelines32-36 had recommendations for pregnant people who may have insufficient dietary intake (e.g., low egg consumption, vegetarian or vegan diet). Choline supplementation recommendations were 350 mg to 450 mg during the first 2 trimesters, 450 mg to 600 mg in the last trimester, and 550 mg during lactation.
Diet
Pregnant people are encouraged to consume choline-containing foods during pregnancy and lactation stages; meeting needs through food is preferred, and they should speak with health care provider about the appropriateness of choline supplementation if they have individual concerns about not meeting recommendations.33
Pregnant people should be supported to understand how to meet recommendations for choline, and which foods are rich in choline as pregnancy advances.31-33,35,36
Daily nutritional goals for pregnant people:
Daily nutritional goals for lactating people:
For pregnant people with vegetarian or vegan diets:
For those with GDM:
Supplementation
For all pregnant people:
For those with GDM:
Where there is inadequate dietary intake or documented deficiency, nutritionists should consider recommending prenatal supplements (including for choline). Indications may include high risk for inadequate micronutrient intake, food insecurity, substance use or dependency (alcohol, tobacco), anemia, vegetarian or vegan diets, and poor eating habits.32,35
Considerations for recommending prenatal supplementation include malabsorption disorder, gastrointestinal discomfort, religious diets, tolerance for supplements, increased costs.32,35
Pregnant people taking over-the-counter or herbal supplements should consult a pharmacist or physician.32,35
Limitations
Study Quality
The included SR26 reported limitations of the included clinical studies such as high dropout rates, unplanned outcome measurements and statistical analyses, missing data, and low generalizability (e.g., low compliance, high drop outs). The primary clinical studies26-30 also noted small sample sizes and missing data; the magnitude of the treatment effects reported may not be as precise as they would be if the studies had higher sample sizes. Most guidelines were based on low-quality evidence or expert opinion.
Generalizability
The clinical studies26-30 included in the current review were conducted in South Africa, Ukraine, and the US; the generalizability of the findings to settings in Canada is unknown. For clinical studies where pregnant people were given choline supplementation, 2 RCTs27,30 reported ages ranging from 26.6 to 28.4 years; ages were not reported in the included SR.26 Therefore it is unclear whether results are applicable to younger or older pregnant people or if results apply to all ages as seen in the included guidelines where recommendations were the same for different age groups. Across evidence where children with FASD were given choline, ages ranged from 2 to 11.44 years, and trial duration lasted from 6 weeks to 4 years.26,28,29 Since no studies were found where infants were given choline, it is unclear whether the results apply to this younger age group. The different values for age at which choline supplementation was initiated, and duration of supplementation present a challenge for interpreting when and how long supplementation is needed to realize an effect; for example, there appeared to be some or little-to-no benefits when older children were given choline.
Average choline dietary intake, type of diet, or descriptions of choline adequacy were only reported in 1 RCT in the included SR,26 and 1 included RCT;30 this information could have helped to contextualize the choline intake of pregnant people and children, helping to provide information to ascertain the baseline levels of choline within groups and how comparable study populations were.
Three included guidelines31,33,34,36 were for the general population of pregnant people and 1 guideline was for pregnant people with GDM.32,35 Two guidelines were specifically for health professionals and people from the US33,34,36 and 1 was for health professionals in Canada;31 it is unclear whether these guidelines may apply to pregnant people with other comorbidities and from other countries.
Heterogeneity of Clinical Studies
There were several differences between the included primary studies which may make it difficult to interpret results as a whole. Where information was available, included primary studies26-30 varied based on population race, education-levels, economic-levels, and whether and how much the pregnant participants consumed alcohol. When the same variable was not reported across multiple studies, it was difficult to assess whether participants were similar or different across the evidence base. The included SR26 did not report on race, education-levels, economic-levels, so it is unclear whether the studies included in the SR26 were similar or different to the primary studies identified for this Rapid Review.
Another limitation of the included clinical studies was the variety of ways that effectiveness was measured. The evidence included over 20 tests, scales, or measurements to assess cognition, behaviour, or neurophysiological responses in infants and children. Given the variability in measurement tools and their results, it is unclear whether included studies measure the same or similar outcomes. Clinical studies also had poor reporting of safety outcomes; in some cases, no numerical information was reported making it difficult to judge potential differences between groups.
Gaps in Equity Reporting
This Rapid Review did not include an explicit search for information related to inequity or equity-deserving groups, or a thorough investigation of the ways that stigma can affect appropriate health care for pregnant people exposed to alcohol, or infants and children with PAE or FASD, and how this relates to choline supplementation strategies for this population. A fulsome equity review and analysis would have provided a better understanding on these issues. PROGRESS-Plus22 was used to guide data extraction and report writing to identify gaps in the evidence where these criteria were not reported or were reported insufficiently. Although PROGRESS-Plus22 includes several criteria, there may be other criteria it does not include that were not extracted that may be important for this population (e.g., timeliness of FASD diagnosis based on demographics or social determinants of health).
No included study described how gender or sex were defined and did not include gender identities outside of male and female. When reporting on pregnant people, the studies referred to the population as “women” or “mothers.” It is unclear whether any of the studies included trans or nonbinary pregnant people, or people with other gender identities. Two clinical trials reported on race and ethnicity; 1 trial29 indicated this was self-identified and it is unclear how it was defined in the other trial.27 Two trials reported education and income, and 1 trial reported English language, but not other languages spoken. No other PROGRESS-plus22 criteria were reported. Identifying these factors for each included study could have given insights into how similar or dissimilar the populations were. Because these criteria were not reported clearly or consistently across the evidence, the generalizability of the evidence is unclear, and the effect of choline supplementation in the context of potential health inequities is unknown. It is unclear whether the study populations included people from equity-deserving groups or whether these groups have access to the intervention.
Conclusions and Implications for Decision- or Policy-Making
We conducted a Rapid Review of the evidence on the clinical effectiveness of choline supplementation in pregnant people or children with PAE or FASD; we also included guidelines with recommendations for these populations. We found 5 articles26-30 published since 2021 based on 1 SR and 3 RCTs, and 4 guidelines31-36 published since 2016 with recommendations. Populations in the clinical evidence included healthy pregnant people, pregnant people exposed to alcohol, and children with FASD. Interventions included choline supplementation compared to placebo, choline supplementation with multivitamin compared to multivitamin only, and higher-dose choline compared to low dose choline. Guidelines were found for choline supplementation in pregnant people including those with GDM or vegan or vegetarian diets; no guidelines were found for choline supplementation in children with PAE or FASD.
Choline Supplementation Evidence
This Rapid Review found heterogenous evidence for child outcomes for studies with sample sizes ranging from 18 to 313 and with most reporting limited statistical power making findings uncertain.
More specifically, for healthy pregnant people given choline compared to those given placebo, there was favourable evidence for cerebral inhibition for 1-month old children and for parent-reported attention and withdrawn symptoms on a schizophrenia questionnaire for 40-month olds.26 There were little-to-no differences between groups in cerebral inhibition, cognitive development, language, visuospatial perception, discrimination, memory, and parent-reported behavioural symptoms measured from 3 to 40 months.26
For healthy pregnant people given high-dose choline compared to those given low-dose choline, there was favourable evidence for reaction times in 13-month olds26 and attention during a signal detection task in 7-year-olds.27 There were little-to-no differences between groups in predictive cascades in 13-month olds,26 or in false alarms, omissions, and off-task behaviours in 7-year-olds.27
For pregnant people exposed to alcohol and given choline compared to those given placebo, there was favourable evidence for conditioned responses in 6.5-month olds,26 visual recognition memory in 12-month olds,26 and weight,26 head circumference,26 and 6 of 12 brain regions in infants from birth to 12 months of age.26 There were little-to-no differences between groups in learning and memory measured by eyeblink conditioning in 6.5-month-olds.26
For pregnant people exposed to alcohol and given choline and multivitamin compared to those given multivitamin only, there was favourable evidence for information processing and learning based on heart rate responses to visual stimuli in 4 to 11-month-olds and little-to-no differences between groups in the score for mental development, psychomotor development, and behaviour at 6 months.26
For children with FASD given choline compared to those given placebo, there was favourable evidence for intelligence (nonverbal IQ and working memory) in 8.6-year-olds with 4-year supplementation,26 and splenium brain structure, motor speed, and colour naming for 10 to 11 year-olds given supplementation for 9 months.28,29 There were little-to-no differences in various neurocognitive outcomes in 2.5 to 5-year-olds given supplementation for 9 months,26,28,29 5 to 10-year-olds given supplementation for 6 weeks,26 and 10 to 11 year-olds given supplementation for 9 months.28,29
Based on limited safety information from 1 SR,26 some results showed little-to-no differences in adverse events in children after choline supplementation during healthy pregnancies, and some adverse events when children with FASD were given supplementation such as fishy body odour and adverse events in specific symptom categories which were reported unclearly.
All 4 guidelines31-36 based on limited and low-quality evidence, and with recommendations informed mostly by expert opinion, recommended that pregnant people, including those with GDM, increase their consumption of choline through diet or supplements. Recommended choline amounts ranged from 350 mg to 600 mg depending on diet versus supplement intake and on pregnancy or postpartum stage. Guidelines also brought attention to the need for health care professional support when deciding whether to supplement diet with choline, the low general intakes of choline in the population, vegetarian and vegan diets, and consideration of the total consumption of micronutrients through diet and supplements. No recommendations were found regarding choline supplementation in children with PAE or FASD.
Across the 5 included publications for effectiveness, none had participants in Canada; generalizability of the evidence as a whole to the Canadian context is unclear. Both clinical studies and guidelines were for different populations of pregnant people of different backgrounds; it may be difficult to interpret evidence and recommendations from the findings as a whole or generalize to all populations. Similarly, since there was limited information on equity-deserving groups, it is unclear what the effect of choline supplementation is in the context of potential health inequities.
Considerations for Future Research
Further clinical research may be needed in the following areas: clinical trials with larger populations and better statistical power, better investigation and reporting of safety outcomes, clear selection and reporting of clinically relevant outcomes given the variability in measures across the evidence, studies where the amounts of choline given to study populations match recommendations for the intervention groups or average intake for comparator groups, meaningful and respectful inclusion and reporting for more pregnant people including nonbinary or trans persons. The following factors may need to be considered in future guideline development: recommendations based on higher-quality evidence (if available), inclusion of the target population when making recommendations, and clearer reporting of methods with links to evidence.
Implications for Clinical Practice
Decision-makers can use clinical effectiveness and guideline evidence from this Rapid Review to inform decisions for use of choline supplementation in pregnant people and children with PAE or FASD, keeping in mind that the evidence is limited and of low quality. Evidence for most effectiveness outcomes was mixed, showing that either choline supplementation was favourable or it had little-to-no benefit; limited safety information showed some adverse events for children with FASD. However, all guidelines recommended higher choline intake through diet or supplementation for all pregnant people. In this Rapid Review, no recommendations were found for choline supplementation in children with PAE or FASD; however, given the range and intensity of interventions that children with FASD need including behaviour therapy, education therapy, medical specialists, and parent training, researchers and health care providers may need to make careful consideration of what is best for children including an appropriate balance of benefits and harms when multiple interventions are applied together. Health care providers who choose to recommend increased choline intake may wish to consider accessibility and cost concerns for pregnant people trying to obtain additional sources of choline through the diet or through supplements, the availability of choline supplements in certain regions and contexts, training on how to read and interpret nutrition information on supplement packaging, and cultural practices and needs of certain populations that affect how they incorporate choline into an existing diet. Further, given the existence of stigma around alcohol exposure during pregnancy and for children with FASD, health care providers should consider providing patient-centred care informed by the stigma and challenges faced by this population to ensure that they feel safe and have the appropriate social and health care resources they need.
References
1.The 519. The 519 Glossary of Terms. 2020; https://www.the519.org/education-training/glossary/. Accessed 2024 Feb 5.
2.Kansakar U, Trimarco V, Mone P, Varzideh F, Lombardi A, Santulli G. Choline supplements: An update. Front Endocrinol (Lausanne). 2023;14:1148166. PubMed
3.National Institutes of Health, Office of Dietary Supplements. Choline. Fact Sheet for Health Professionals 2022; https://ods.od.nih.gov/factsheets/Choline-HealthProfessional/. Accessed 2024 Jan 27.
4.Jaiswal A, Dewani D, Reddy LS, Patel A. Choline Supplementation in Pregnancy: Current Evidence and Implications. Cureus. 2023;15(11):e48538. PubMed
5.Garner CD. Nutrition in pregnancy: Dietary requirements and supplements. In: Post TW, ed. UpToDate. Waltham (MA): UpToDate; 2024: https://www.uptodate.com. Accessed 2024 Jan 2.
6.Ernst AM, Gimbel BA, de Water E, et al. Prenatal and Postnatal Choline Supplementation in Fetal Alcohol Spectrum Disorder. Nutrients. 2022;14(3):06.
7.Health Canada. Summary of Health Canada’s safety assessment of L-alpha-glycerylphosphorylcholine for use as a supplemental ingredient. 2023; https://www.canada.ca/en/health-canada/services/food-nutrition/reports-publications/summary-safety-assessment-l-alpha-glycerylphosphorylcholine-use-supplemental-ingredient.html. Accessed 2024 Jan 27.
8.Lewis ED, Subhan FB, Bell RC, et al. Estimation of choline intake from 24 h dietary intake recalls and contribution of egg and milk consumption to intake among pregnant and lactating women in Alberta. Br J Nutr. 2014;112(1):112-121. PubMed
9.U.S. Department of Health & Human Services, Centers for Disease Control and Prevention. Fetal Alcohol Spectrum Disorders: Basics about FASDs. 2023: https://www.cdc.gov/ncbddd/fasd/facts.html. Accessed 2024 Jan 27.
10.Public Health Agency of Canada. Fetal alcohol spectrum disorder: About, causes and co-occurring conditions. 2023; https://www.canada.ca/en/public-health/services/diseases/fetal-alcohol-spectrum-disorder.html. Accessed 2024 Jan 27.
11.Charlesworth J. Excluded: Increasing Understanding, Support and Inclusion for Children with FASD and Their Families. Victoria (BC): Representative for Children and Youth (British Columbia); 2021: https://rcybc.ca/reports-and-publications/excluded/. Accessed 2024 Feb 8.
12.Lange S, Probst C, Gmel G, Rehm J, Burd L, Popova S. Global Prevalence of Fetal Alcohol Spectrum Disorder Among Children and Youth: A Systematic Review and Meta-analysis. JAMA Pediatr. 2017;171(10):948-956. PubMed
13.Popova S, Lange S, Chudley AE, et al. World Health organization International study on the prevalence of fetal alcohol spectrum disorder (FASD). Canadian Component. Toronto (ON): Centre for Addiction and Mental Health, Institute for Mental Health Policy Research; 2018: https://canfasd.ca/wp-content/uploads/2018/05/2018-Popova-WHO-FASD-Prevalance-Report.pdf. Accessed 2024 Jan 27.
14.Flannigan K, Unsworth K, Harding K. FASD prevalence in special populations. Vancouver (BC): Canada FASD Research Network; 2018: https://canfasd.ca/wp-content/uploads/publications/Prevalence-2-Issue-Paper-FINAL.pdf. Accessed 2024 Feb 8.
15.Centre for Addiction and Mental Health (CAMH). Fetal Alcohol Spectrum Disorders. [2024]; https://www.camh.ca/en/health-info/mental-illness-and-addiction-index/fetal-alcohol-spectrum-disorder. Accessed 2024 Jan 27.
16.Baker JA, Breit KR, Bodnar TS, Weinberg J, Thomas JD. Choline Supplementation Modifies the Effects of Developmental Alcohol Exposure on Immune Responses in Adult Rats. Nutrients. 2022;14(14):2868. PubMed
17.Popova S, Charness ME, Burd L, et al. Fetal alcohol spectrum disorders. Nat Rev Dis Primers. 2023;9(1):11. PubMed
18.Murawski NJ, Moore EM, Thomas JD, Riley EP. Advances in Diagnosis and Treatment of Fetal Alcohol Spectrum Disorders: From Animal Models to Human Studies. Alcohol Res. 2015;37(1):97-108. PubMed
19.Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. PubMed
20.Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377-384. PubMed
21.Agree Next Steps Consortium. The AGREE II Instrument. [Hamilton (ON)]: AGREE Enterprise; 2017: https://www.agreetrust.org/wp-content/uploads/2017/12/AGREE-II-Users-Manual-and-23-item-Instrument-2009-Update-2017.pdf. Accessed 2024 Jan 22.
22.O'Neill J, Tabish H, Welch V, et al. Applying an equity lens to interventions: using PROGRESS ensures consideration of socially stratifying factors to illuminate inequities in health. J Clin Epidemiol. 2014;67(1):56-64. PubMed
23.Morrison K, Wolfson L, Harding K, Poole N. Mothers' Experiences of Stigma: Multi-Level Ideas for Action. Vancouver (BC): Canada FASD Research Network; 2020: https://canfasd.ca/wp-content/uploads/publications/Mothers-Experiences-of-Stigma-final.pdf. Accessed 2024 Feb 5.
24.Roozen S, Stutterheim SE, Bos AER, Kok G, Curfs LMG. Understanding the Social Stigma of Fetal Alcohol Spectrum Disorders: From Theory to Interventions. Foundations of Science. 2022;27(2):753-771.
25.Weber A, Miskle B, Lynch A, Arndt S, Acion L. Substance Use in Pregnancy: Identifying Stigma and Improving Care. Subst Abuse Rehabil. 2021;12:105-121. PubMed
26.Obeid R, Derbyshire E, Schon C. Association between Maternal Choline, Fetal Brain Development, and Child Neurocognition: Systematic Review and Meta-Analysis of Human Studies. Adv Nutr. 2022;13(6):2445-2457. PubMed
27.Bahnfleth CL, Strupp BJ, Caudill MA, Canfield RL. Prenatal choline supplementation improves child sustained attention: A 7-year follow-up of a randomized controlled feeding trial. FASEB J. 2022;36(1):e22054. PubMed
28.Fuglestad AJ, Miller NC, Fink BA, et al. Neurophysiological correlates of memory change in children with fetal alcohol spectrum disorders treated with choline. Front Psychol. 2022;13:936019. PubMed
29.Gimbel BA, Anthony ME, Ernst AM, et al. Long-term follow-up of a randomized controlled trial of choline for neurodevelopment in fetal alcohol spectrum disorder: corpus callosum white matter microstructure and neurocognitive outcomes. J Neurodev Disord. 2022;14(1):59. PubMed
30.Warton FL, Molteno CD, Warton CMR, et al. Maternal choline supplementation mitigates alcohol exposure effects on neonatal brain volumes. Alcohol Clin Exp Res. 2021;45(9):1762-1774. PubMed
31.Nutrition Working Group, O'Connor DL, Blake J, et al. Canadian Consensus on Female Nutrition: Adolescence, Reproduction, Menopause, and Beyond. J Obstet Gynaecol Can. 2016;38(6):508-554.e518. PubMed
32.Duarte-Gardea MO, Gonzales-Pacheco DM, Reader DM, et al. Academy of Nutrition and Dietetics Gestational Diabetes Evidence-Based Nutrition Practice Guideline. J Acad Nutr Diet. 2018;118(9):1719-1742. PubMed
33.Dietary Guidelines for Americans, 2020-2025. 9th ed. Washington (DC): U.S. Department of Agriculture and U.S. Department of Health and Human Services; 2020: https://www.dietaryguidelines.gov/sites/default/files/2021-03/Dietary_Guidelines_for_Americans-2020-2025.pdf. Accessed 2024 Jan 22.
34.Adams JB, Kirby JK, Sorensen JC, Pollard EL, Audhya T. Evidence based recommendations for an optimal prenatal supplement for women in the US: vitamins and related nutrients. Matern Health Neonatol Perinatol. 2022;8(1):4. PubMed
35.Gestational Diabetes. GDM: Full Recommendations and Supporting Evidence (2016). Evidence Analysis Library. Chicago (IL): Academy of Nutrition and Dietetics; 2017: https://www.andeal.org/vault/pq152.pdf. Accessed 2024 Jan 24.
36.Dietary Guidelines Advisory Committee. Scientific report of the 2020 Dietary Guidelines Advisory Committee: advisory report to the Secretary of Agriculture and the Secretary of Health and Human Services. Washington (DC): U.S. Department of Agriculture, Agricultural Research Service; 2020: https://www.dietaryguidelines.gov/sites/default/files/2020-07/ScientificReport_of_the_2020DietaryGuidelinesAdvisoryCommittee_first-print.pdf. Accessed 2024 Jan 22.
37.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Table 2: Characteristics of Included Systematic Review
Study citation, country, funding source | Study designs, number of primary studies included | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Obeid et al. (2022)26 South Africa, Ukraine, US Funding source: Procter and Gamble Health Germany | Literature published between 1997 and 2021 30 studies 10 publications relevant to the present review based on 7 different RCTsa | Reported as healthy pregnant women or women exposed to alcohol during pregnancy in second and third trimestersb (Studies in healthy pregnant people: n = 29 to 140 across studies; studies in pregnant people exposed to alcohol: n = 62 to 313 across study groups) Age: NR Sex or gender: Referred to as women Race or ethnicity: NR SES: NR Children with FASD (n = 31 to 60 across studies) Age: 2.5 to 10 years across studies Sex or gender: NR Race or ethnicity: NR SES: NR | Choline supplementation vs. placebo (5 different formats) 900 mg/day phosphatidylcholine for healthy pregnant person from week 16 to delivery and 100 mg/day for infant from birth to 3 months 750 mg/day phosphatidylcholine for health pregnant person from week 18 to 90 days after birth on top of 360 mg/day average dietary choline (from a “Western” diet) 1.25 g choline bitartrate twice daily for alcohol-exposed pregnant person from week 20 until birth 1.25 g choline bitartrate (513mg/day) for child with FASD for 9 months Glycerophosphocholine liquid providing 625 mg/day for child with FASD for 6 weeks High-dose choline chloride supplementation (930 mg/day) vs. low dose (480 mg/day) choline chloride for health pregnant people, for 12 weeks Choline (750 mg/day) plus multivitamin vs. multivitamin onlyc for alcohol-exposed pregnant people from week 19 until birth | Outcomes in children: Neurocognition and neurodevelopmental outcomesd (e.g., reaction time, behaviour, cerebral inhibition, memory, global cognitive development, conditioned responses, cardiac responses, intelligence, language, motor ability, perception, executive functioning) Weight Head circumference Safety (e.g., adverse events, live births, side effects, fish body odour) Follow-up in children: Up to 10 years |
FASD = fetal alcohol spectrum disorder; NR = not reported; SES = socioeconomic status.
aSome publications reported on the same study population for different outcomes or analyses.
bOut of the 7 included RCTs, the SR reported a average of 360mg per day dietary choline intake and a “Western diet” for 1 RCT; details for diet or choline adequacy status for other RCTs was not reported.
cCholine type not reported.
dSpecific measures included the Child Behaviour Checklist, Mullen Scales of Early Learning, Mac-Arthur-Bates Short form Vocabulary Checklist, Bayley Scales of Infant Development (II), Stanford–Binet Intelligence Scales, Fifth Edition (SB-5), Cambridge Neuropsychological Test Automated Battery (CANTAB), NEPSY-2 Design Fluency test, Quotient ADHD system, and Grooved Pegboard.
Note that this table has not been copy-edited.
Table 3: Characteristics of Included Randomized Controlled Trials
Study citation, country, funding sources | Study design details | Population characteristicsa | Intervention and comparator | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Bahnfleth et al. (2022)27 US Funding sources: NIFA-USDA | Long-term follow-up of double-blind trial | Reported as women in their third trimester with no alcohol or tobacco useb Age: 27.6 years vs. 28.4 years Sex or gender: Referred to as women Masters or Doctoral degree: 28% vs. 67% Family income ≥ $100,000: 45% vs. 56% Family income < $50,000: 18% vs. 0% Race: NR Ethnicity: NR Children (n = 20) Age: 7.3 years vs. 7.2 years Sex: 73% vs. 67% male, other sexes or genders NR English not primary language: 27% vs. 11% First grade complete: 82% vs. 67% Race: Asian (18% vs. 11%), Black (9% vs. 0%), Indigenous (9% vs. 0%), white (64% vs. 89%) Ethnicity: “Hispanic” (18% vs. 22%) | Intervention: 930 mg/day choline supplementation in pregnant people (380 mg/day from diet plus 550 mg/day supplement from choline chloridec) Comparator: 480 mg/day choline supplementation in pregnant people (380 mg/day from diet plus 100 mg/day supplement from choline chloridec) Duration: 12 weeks | Outcomes in children: Neurocognition and neurodevelopmental outcomes (SAT score, signal identification, vigilance decrement, false alarms, omissions, off-task behaviours) Follow-up: 7 years |
Fuglestad et al. (2022)28 Gimbel et al. (2022)29 US | After original double-blind trial,d 1 publication has results for a secondary outcome (ERP)28 and another publication is a long-term follow-up for brain microstructures and neurocognitive outcomes | Children with FASD,b n = 18 to 24d Age: 2.5 to 5 years at enrolment Sex or gender:e female (55.6% to 71%), male (29%), other sexes or genders NR Race:e white (11.1% to 56.6%), Black/African-American (0% to 25%), Indigenous (0% to 29%), Asian (4% to 11.1%), multiracial (22.2% to 25%), unknown (0% to 11.1%) Ethnicity:e “Hispanic or Latino” (0% to 11.1%), not “Hispanic or Latino” (92%), unknown (0% to 11.1%) SES: NR | Intervention: Choline supplementation in children (513 mg choline from once daily 1.25 g choline bitartrate)c Comparator: Placebo in childrenc Duration: 9 months | Outcomes in children: Neuro-cognitive and neurodevelopmental outcomes (ERP familiarity response, WISC-V, D-KEFS Trail Making Test D-KEFS Colour-Word Interference Test) Corpus callosum NODDI ODI Follow-up: Up to 10 years |
Warton et al. (2021)30 South Africa Funding sources: NIAAA–NIH, Lycaki-Young Fund from the State of Michigan, National Research Foundation of South Africa | Exploratory analysis of a sample following a double-blind triald | Reported as women in second trimester of pregnancy who reported an average of 2 drinks/day or 4+ drinks/occasion, more than 70% choline deficient Age: 26.6 years vs. 27.9 years Sex or gender: Referred to as women Race or ethnicity: NR Education (highest grade): 8.9 vs. 9.5 (referred to as having low education levels) SES: Economically disadvantaged Infants with prenatal alcohol exposure (n = 52) Age: mean 22.1 days vs. 20.1 days Sex or gender: 30% vs. 70% male, other sexes or genders NR Race or ethnicity: NR | Intervention (n = 28): Choline supplementation in pregnant people (twice daily 1.25 g choline bitartrate with 1g of bioavailable choline cation)c Comparator (n = 24): Placebo in pregnant peoplec Duration: second trimester to delivery | Outcomes in infants: FTII score, brain region sizes Follow-up: Up to 12 months |
D-KEFS = Delis-Kaplan Executive Function System; ERP = event-related potential; FASD = fetal alcohol spectrum disorder; FTII = Fagan Test of Infant Intelligence; NIAAA = National Institute on Alcohol Abuse and Alcoholism; NIFA = National Institute of Food and Agriculture; NIH = National Institutes of Health; NODDI ODI neurite orientation dispersion and density imaging orientation dispersion index; NR = not reported; SAT = sustained attention task; SES = socioeconomic status; UNC = University of North Carolina; USDA = US Department of Agriculture; WISC-V = Wechsler Intelligence Scale for Children, Fifth Edition.
aIntervention group vs. comparator group, respectively, unless otherwise indicated.
bInformation about diet or choline adequacy status not reported.
cConsumed as a fruit-flavoured powder mixed with water or in cran-grape juice.
dThe participants in this trial are also included in the systematic review by Obeid et al. (2022) under a different publication.
eAcross groups in the 2 articles.
Note that this table has not been copy-edited.
Table 4: Characteristics of Included Guidelines
Intended users, target population | Intervention and practice considered | Major outcomes considered | Evidence collection, selection, and synthesis | Evidence quality assess-ment | Recommend-ations development and evaluation | Guideline validation |
|---|---|---|---|---|---|---|
Adams et al. (2022)34 | ||||||
Intended users: General population, physicians, nutritionists Target population: Reported as women in the US from the general population | Daily dietary intake, RDA, recommendations on prenatal supplements for 13 vitamins and 3 related nutrients; choline is relevant to the present review | Pregnancy and infant health outcomes | Literature review of studies, proposal of evidence-based recommend-ations using NHANES data of daily intake by what was reported as women in the US | GRADE | Consideration of quality of evidence, benefit vs. adverse effects, uncertainty, and costs | NR |
Intended users: Health leaders; medical and nutritional professionals; federal, medical, voluntary, and patient care organizations Target population: US population (any age) including healthy people, those at-risk of diet-related conditions, and those with a diet-related chronic illness | Dietary guidelines for health promotion and public health; choline is relevant to the present review | Pregnancy, infant, child health and nutrition outcomes | SR by NESR of peer-reviewed English studies, food pattern modelling, data analysis of national datasets Two reviewers screened SR results, conducted handsearching, extracted data, assessed risk of bias | NESR’s rubric based on risk of bias, consist-ency, direct-ness, precision, and general-izability (rubric informed by GRADE, AHRQ, and OHAT) | Committee meetings open to the public to discuss evidence review and report creation, collaborative review of evidence to create advice and conclusion statements | Peer-review of NESR SRs; oral and written comments from the public; internal review; external peer-review |
Intended users: RDNs or health professionals caring for what was reported as adult women with GDM; policy-makers, consumers (education purposes) Target population: Reported as pregnant women with GDM | Nutrition and lifestyle management of what was reported as women with GDM; choline recommendations are relevant to the present review | Glycemic control; maternal weight gain; fetal growth/ birth weight; and adverse fetal, maternal, and neonatal outcomes | SR with article inclusion based on work group consensus; evidence analysts extracted data, appraised articles and drafted summaries; final revisions made by consensus | Academy Rating Scheme of Recommendations | Work group reviewed and graded evidence into conclusion statements and recommend-ations; conference calls, shared online work space | Internal review, external review with 14 interdisciplinary exerts in GDM |
Nutrition Working Group SOGC (2016)31 | ||||||
Intended users: Health care professionals in Canada Target population: Reported as women at all stages of life cycle | Nutrition guidance for woman; choline recommendations are relevant to the present review | Optimal nutrition through the female life cycle including adolescence, preconception, pregnancy, postpartum, menopause | Literature searches of published literature, governmental and health agency reports, clinical practice guidelines, grey literature, and textbooks | Criteria from Canadian Task Force on Preventive Health Care | NR | NR |
AHRQ = Agency for Health care Research and Quality; ALT = alanine aminotransferase; AST = aspartate aminotransferase; CBC = complete blood count; DRI = Dietary Reference Intakes; ESPEN = The European Society for Clinical Nutrition and Metabolism; GDM = gestational diabetes mellitus; GGT = glutamyl transferase; GRADE = Grading of Recommendations Assessment, Development and Evaluation; HHS = US Department of Health and Human Services; MN = micronutrient; NASEM = National Academies of Sciences, Engineering, and Medicine; NESR = Nutrition Evidence Systematic Review; NHANES = National Health and Nutrition Examination Survey; NR = not reported; OHAT = Office of Health Assessment and Translation; RDA = Recommended Dietary Allowance; RDN = registered dietitian nutritionist; SIGN = Scottish Intercollegiate Guidelines Network; SOGC = Society of Obstetricians and Gynaecologists of Canada; SR = systematic review; USDA = US Department of Agriculture.
Note that this table has not been copy-edited.
Appendix 3: Critical Appraisal of Included Publications
Note that this appendix has not been copy-edited.
Table 5: Strengths and Limitations of the Systematic Review Using AMSTAR219
Strengths | Limitations |
|---|---|
Obeid et al. (2022)29 | |
Authors clearly stated the population, intervention, comparators, and outcomes of interest. A protocol outlining detailed methods was established beforehand and the review was registered. Authors provided explanations for the types of studies to include and exclude. Authors provided keywords for the search strategy, justified publication restrictions, and screened reference lists of previous systematic reviews. Authors performed study selection and data extraction in duplicate. Authors provided a list of excluded studies with justifications. Authors described the populations, interventions, comparators, outcomes, and study designs of included studies in sufficient detail. Authors used a satisfactory technique for assessing the risk of bias of included studies. Authors discussed the impact of bias within the individual studies they included. Authors discussed the heterogeneity of the included studies. | It is unclear whether the literature search strategy was comprehensive since 1 database was searched during the study and a different database was searched separately at the time of manuscript preparation. The ages of pregnant people in the studies were not reported. Sex, gender, race, ethnicity, and SES for children were not provided. SR authors mentioned limitations of the included studies such as low adherence, high dropout rates, short study duration, missing data, low generalizability, and unplanned testing or analyses. Sources of funding for each included study were not reported. All authors received consulting fees from the company that sponsored the review. Authors indicated that they had no further conflicts of interest. Authors indicated that the sponsor had no role in concept, design, review conduct, data collection, interpretation, or manuscript writing. |
AMSTAR 2 = A MeaSurement Tool to Assess systematic Reviews 2; SES = socioeconomic status.
Table 6: Strengths and Limitations of Clinical Studies Using the Downs and Black Checklist20
Strengths | Limitations |
|---|---|
Bahnfleth et al. (2022)27 | |
Authors described the objectives, main outcomes, participant criteria, interventions, demographic characteristics, and main findings. Authors provided the random variability of the outcome data and reported actual P values. Characteristics of the participants lost to follow-up (n = 5) or who did not follow study protocol and whose data were removed (n = 1) were described; authors indicated that these children were not different from those included in the final analyses. Participants and outcome assessors were blinded to study assignment. Authors conducted appropriate statistical analyses and sensitivity analyses. Participants were randomized to intervention and comparator groups and authors indicated that the study groups were matched on demographic and birth characteristics, with a nonsignificant trend for higher education in pregnant people in the comparator group. Although the study sample was small, authors indicated that they had adequate power to detect an effect of the intervention and developed their statistical plan before conducting analyses. Authors reported no conflicts of interest; funders had no role in study conduct. | It is unclear whether the study population is representative; the authors described children as predominantly white males who completed first grade, and that most pregnant people were highly educated. Pregnant people including in this study did not consume alcohol or tobacco during pregnancy; it is unclear if the results can be generalized to other pregnant people who may consume these substances during pregnancy. Authors indicated that a larger sample size would have increased their confidence in the representativeness of the study sample and that larger trials are needed. |
Authors described the objectives, main outcomes, participant criteria, interventions, demographic characteristics, and main findings. Authors provided the random variability of the outcome data and reported actual P values. In one of the publications,29 authors noted there were no differences between those who remained in the study and those who were lost to follow-up. Participants, investigators, and the research team were blinded to study assignment. Participants were randomized to intervention and comparator groups. Authors reported no conflicts of interest. | In one of the publications28 that reported secondary outcome analyses, only the subset of RCT participants with ERP data at baseline and study completion were included in this analysis; reasons for missing data were not undergoing procedures, not having enough data, or discontinuing the trial. Of the participants who completed the trial at 9 months, 29% had non-usable ERP data and were excluded from this analysis. Children with usable ERP data and included in the analysis were slightly older, had higher scores on cognitive functioning tests, and had milder forms of FASD than those with unusable data. Authors indicated that treatment effects may have been diluted because of this. In another publication for a long-term follow-up of the same trial on executive function and neuroimaging,29 authors indicated that participants were excluded from analyses if they had significant missing data and that 2 participants were eliminated for not completing neuroimaging; it is unclear whether this affected the results. Authors indicated that participants differed racially between groups. One publication29 noted that because of limited power and small samples sizes, exploring confounding effects due to differences in race between groups was not possible. Authors indicated that there were small sample sizes which limit generalizability of the neurodevelopmental findings29 or clear conclusions about ERP in children.28 Authors of the long-term follow-up29 indicated that few participants returned for follow-up assessments and that the analyses were exploratory given the small sample size. Authors indicated limited power to detect differences in outcomes between groups. Authors that reported on the secondary ERP outcome29 noted that the duration of time between trial completion and outcome measurement (4 to 10 year follow-up) is a potential limitation because brain development and cognitive performance change quickly as children age; it is unclear whether the correction for this in the analyses was sufficient. |
Warton et al. (2021)30 | |
Authors described the objectives, main outcomes, participant criteria, interventions, demographic characteristics, and main findings. Authors provided the random variability of the outcome data and reported actual P values. Participants, investigators, and the research team were blinded to study assignment. Participants were randomized to intervention and comparator groups. Authors evaluated potential confounding and made appropriate adjustments where present. Authors reported no conflicts of interest; funders had no role in study conduct. | Data from 2 participants were removed because of technical error and poor image quality; it is unclear whether this affected the results. It is unclear whether the study population is representative. Pregnant people reported an average of 2 drinks/day or 4+ drinks/occasion during pregnancy and were > 70% choline deficient; it is unclear if the results can be generalized to other pregnant people who may consume different amounts of alcohol or choline during pregnancy. The population was also described as having low education levels and being economically disadvantaged; these characteristics also point to unclear generalizability to other populations. |
ERP = event-related potentials (from brain responses).
Table 7: Strengths and Limitations of Guidelines Using AGREE II21
Item | Adams et al. (2022)34 | Nutrition Working Group SOGC (2016)31 | ||
|---|---|---|---|---|
Domain 1: Scope and purpose | ||||
1. The overall objective(s) of the guideline is (are) specifically described. | Yes | Yes | Yes | Yes |
2. The health question(s) covered by the guideline is (are) specifically described. | Yes | Yes | Yes | Yes |
3. The population (patients, public, etc.) to whom the guideline is meant to apply is specifically described. | Yes | Yes | Yes | Yes |
Domain 2: Stakeholder involvement | ||||
4. The guideline development group includes individuals from all relevant professional groups. | Unclear | Yes | Yes | Unclear |
5. The views and preferences of the target population (patients, public, etc.) have been sought. | Unclear | Unclear | Unclear | Unclear |
6. The target users of the guideline are clearly defined. | Yes | Yes | Yes | Yes |
Domain 3: Rigour of development | ||||
7. Systematic methods were used to search for evidence. | Yes | Yes | Yes | Unclear |
8. The criteria for selecting the evidence are clearly described. | Yes | Yes | Yes | Unclear |
9. The strengths and limitations of the body of evidence are clearly described. | Yes | Yes | Yes | Yes |
10. The methods for formulating the recommendations are clearly described. | No | No | Yes | No |
11. The health benefits, side effects, and risks have been considered in formulating the recommendations. | Yes | Yes | Yes | Yes |
12. There is an explicit link between the recommendations and the supporting evidence. | Yes | No | Yes | No |
13. The guideline has been externally reviewed by experts before its publication. | Unclear | Yes | Yes | Unclear |
14. A procedure for updating the guideline is provided. | No | No | No | No |
Domain 4: Clarity of presentation | ||||
15. The recommendations are specific and unambiguous. | Yes | Yes | No | No |
16. The different options for management of the condition or health issue are clearly presented. | Yes | Yes | Yes | No |
17. Key recommendations are easily identifiable. | Yes | No | Yes | Yes |
Domain 5: Applicability | ||||
18. The guideline describes facilitators and barriers to its application. | Yes | Yes | Yes | No |
19. The guideline provides advice and/or tools on how the recommendations can be put into practice. | No | Yes | Yes | No |
20. The potential resource implications of applying the recommendations have been considered. | Yes | Yes | Yes | No |
21. The guideline presents monitoring and/or auditing criteria. | Yes | Yes | Yes | No |
Domain 6: Editorial independence | ||||
22. The views of the funding body have not influenced the content of the guideline. | Unclear | Unclear | NAa | Yes |
23. Competing interests of guideline development group members have been recorded and addressed. | Unclear | Yes | Yes | Unclear |
AGREE II = Appraisal of Guidelines for Research and Evaluation II; NA = not applicable; SOGC = Society of Obstetricians and Gynaecologists of Canada.
aAuthors reported that there were no potential conflicts of interest.
Appendix 4: Main Study Findings
Note that this appendix has not been copy-edited.
Table 8: Summary of Findings by Outcomes in Infants and Children — Effectiveness and Safety of Choline Supplementation Versus Placebo in Healthy Pregnant People
Study citation and design | Outcome | Child agea | Treatment effects |
|---|---|---|---|
Neurocognitive and neurodevelopmental outcomes | |||
Obeid et al. (2022)26 SR:
| Intact cerebral inhibition | 1 | Higher intact cerebral inhibition for choline group 76% vs. 43%, P = 0.009 |
Intact cerebral inhibition | 3 | Little-to-no difference in intact cerebral inhibition between groups 76% vs. 72%, P value NR | |
Mullen Scales of Early Learningc - visual perception and discrimination and receptive or expressive language | 6 | Little-to-no difference between groups | |
Obeid et al. (2022)26 SR:
| Neurocognition outcomes | 10 | Little-to-no difference between groups |
Global cognitive developmentc | 10 or 12 | Little-to-no difference in between groups | |
Number of words spoken | 10 or 12 | Little-to-no difference in between groups | |
Short-term visuospatial memory | 10 or 12 | Little-to-no difference in between groups | |
Long-term episodic memory | 10 or 12 | Little-to-no difference in between groups | |
Long-term memory task | 12 | Trend toward lower long-term episodic memory not statistically significant (P = 0.056) Mean = 0.45; SD = 0.22 vs. mean 0.53; SD = 0.20 | |
Behavioural symptoms | |||
Obeid et al. (2022)26 SR:
| Attention issuese | 40 | Lower for choline group (P = 0.038) |
Withdrawn issuese | 40 | Lower for choline group (P = 0.003) | |
Behaviour issuese | 40 | Little-to-no difference between groups | |
Safety | |||
Obeid et al. (2022)26 SR:
| Preterm birth (< 37 gestational weeks) | NR | 4 people in the choline group vs. 7 in the placebo group |
Apgar scores,f weight, length, head circumference, and perinatal complications | NR | Little-to-no difference between groups | |
Obeid et al. (2022)26 SR:
| Adverse events | NR | Little-to-no difference between groups Adverse events were not more frequent or severe than a typical obstetric population. |
Severe adverse events | NR | No severe adverse events reported | |
CI = confidence interval; mg/d = milligrams per day; ms = milliseconds; NR = not reported; RCT = randomized controlled trial; SAT = sustained attention task; SD = standard deviation; SR = systematic review; vs. = versus.
aFollow-up in months unless otherwise indicated.
bCholine was given to pregnant person from second trimester until birth, and to infants after birth until 3 months.26
cMeasures global cognitive development and includes motor ability, language, and visual reception.26
dCognition outcomes included Short-term Visuospatial Memory Delayed Response Task to measure visuospatial memory, long-term episodic memory, The Mac-Arthur-Bates Short Form Vocabulary Checklist – level I to measure language development, and Mullen Scales of Early Learning to measure motor ability, language, and visual reception.26
eOutcomes were based on parent-reports on the Child Behaviour Checklist to detect early signs of schizophrenia, withdrawn symptoms, and attention disturbances.26
fA measure of a baby’s general condition.26
Table 9: Summary of Findings by Outcomes in Infants and Children — Effectiveness and Safety of High-Dose Versus Low-Dose Choline Supplementation in Healthy Pregnant People
Study citation and design | Outcome | Child agea | Treatment effects |
|---|---|---|---|
Neurocognitive and neurodevelopmental outcomes | |||
Obeid et al. (2022)26 SR
| Saccade reaction timeb | 4, 7, 10 and 13 | Faster saccade reaction time in higher-dose choline group at 4, 7, 10 and 13 months Adjusted mean = 33.8ms; 95% CI, 2.7 to 54.8 |
Number of predictive cascadesb | 4, 7, 10 and 13 | Little-to-no difference (P = 0.6) | |
Bahnfleth et al. (2022)27 RCT Long-term follow-up of Caudill et al. (2018) | SAT scorec | 7 years | Higher SAT score for higher-dose group Mean = 0.71; SE = 0.04 vs. mean 0.56; SD = 0.04; P = 0.02 |
Signal identificationd | 7 years | More children in the higher-dose choline group could accurately identify signals and reject nonsignals 95% CI, 0.03 to 0.27; P = 0.02 | |
Vigilance decrementd | 7 years | Groups differed in based on length of signal 1.5% increase in hits in higher-dose choline vs. 22.9% decline in hits in lower-dose choline at 17ms (P = 0.04) Little-to-no difference in hits between groups at 20ms or 50ms signals between groups | |
False alarms, omissions, off-task behaviours | 7 years | Little-to-no difference between groups | |
Safety | |||
Obeid et al. (2022)26 SR
| Adverse events | NR | No adverse effects reported by participants. |
CI = confidence interval; mg/d = milligrams per day; ms = milliseconds; NR = not reported; RCT = randomized controlled trial; SAT = sustained attention task; SD = standard deviation; SE = standard error; SR = systematic review; vs. = versus.
aFollow-up in months unless otherwise indicated.
bMeasures information processing and intelligent quotient (IQ) scores.26
cBased on the child’s performance on a signal detection task that measures attentional processes.26
dMeasures sustained attention.27
Table 10: Summary of Findings by Outcomes in Infants and Children — Effectiveness and Safety of Choline Supplementation Versus Placebo in Pregnant People Exposed to Alcohol
Study citation and design | Outcome | Child agea | Treatment effects |
|---|---|---|---|
Neurocognitive and neurodevelopmental outcomes | |||
Obeid et al. (2022)26 SR
| Eyeblink conditioningb | 6.5 | Trend toward favourable effect of choline was not statistically significant (P = 0.090). After removing 4 participants with low adherence, effect favoured choline (P = 0.036) Higher increases in percent of conditioned responses across 3 sessions for choline group (P < 0.01) |
Visual recognition memory based on FTIIc | 12 | Better visual recognition memory for choline group (numerical values not reported) | |
Warton et al. (2021)30 RCT Smaller sample of population in Jacobson et al. (2018) | FTII scorec | 12 | Little-to-no difference on FTII (P = 0.11) Choline: mean = 63.2; 95% CI, 60.8 to 65.7 Placebo: mean = 60.2; 95% CI, 57.4 to 62.9 Statistical significance achieved when including infants with low maternal adherence and controlling for birth weight (P = 0.03) |
Brain, body size | |||
Obeid et al. (2022)26 SR
| Weight | Birth, 6.5, 12 | Higher increases for choline group (P = 0.009) |
Head circumference | Birth, 6.5, 12 | Higher increases choline group (P = 0.006) | |
Warton et al. (2021)30 RCT Smaller sample of population in Jacobson et al. (2018) | Brain region sizes | 1 to 7 weeks | Sizes were greater for choline vs. placebo for 6 of 12 brain regionsd Left thalamus (P = 0.01) Right thalamus (P = 0.05) Left caudate (P = 0.05) Right caudate (P = 0.05) Right putamen (P = 0.04) Corpus callosum (P = 0.01) |
Safety | |||
Obeid et al. (2022)26 SR
| Side effects | NR | Minor side effects such as dyspepsia and nausea were reported (unclear for which groups). |
CI = confidence interval; FTII = Fagan Test of Infant Intelligence; NR = not reported; RCT = randomized controlled trial; SR = systematic review; vs. = versus.
aFollow-up in months unless otherwise indicated.
bTest indicates learning and memory and is sensitive to fetal alcohol syndrome.26
cA measure of information processing speed and visual recognition memory based on a child’s ability to distinguish familiar from novel pictures.26
dPAE is thought to reduce brain volumes and choline may mitigate these effects.30
Table 11: Summary of Findings by Outcomes in Infants and Children — Effectiveness and Safety of Multivitamin Choline Supplementation Versus Multivitamin Only in Pregnant People Exposed to Alcohol
Study citation and design | Outcome | Child agea | Treatment effects |
|---|---|---|---|
Neurocognitive and neurodevelopmental outcomes | |||
Obeid et al. (2022)26 SR
| Heart rate after visual stimulib | 4 to 11 months | Change in heart rate after visual stimulie for choline group (P < 0.001) Change in latency in the visual habituation trials for choline group (adjusted P < 0.003) |
Bayley Scales of Infant Developmentc | 6 months | Little-to-no difference between groups | |
Safety | |||
Obeid et al. (2022)26 SR
| Safety outcomes | NA | Publication did not report safety outcomes. |
NA = not applicable; RCT = randomized controlled trial; SR = systematic review; vs. = versus.
aFollow-up in months unless otherwise indicated.
bIndicates information processing and learning.26
cA measure of mental development, psychomotor development, and behaviour including problem solving, prelinguistic development, fine and gross motor skills, orientation and engagement, emotional regulation, motor quality, and total behaviour quality.26
Table 12: Summary of Findings by Outcomes in Infants and Children — Effectiveness and Safety of Choline Supplementation Versus Placebo for Children With PAE or FASD
Study | Outcome | Enrolment age and trial duration | Age at follow-upa | Treatment effects |
|---|---|---|---|---|
Neurocognitive and neurodevelopmental outcomes | ||||
Obeid et al. (2022)26 SR
| Global cognitive development measured by the Mullen Scales of Early Learningb | 2.5 to 5 years old at enrolment 9 month trial | 2.5 to 5 | Little-to-no differences between groups |
Elicited imitation memory paradigmc | 2.5 to 5 years old at enrolment 9 month trial | 2.5 to 5 | Little-to-no differences between groups Children aged 2.5 to 4 years from the choline group had the greatest improvement in elicited imitation delayed performance, suggesting that age may moderate the effect. | |
Fuglestad et al. (2022)28 RCT Gimbel et al. (2022)29 RCT Same study as Wozniak et al. (2020), Wozniak et al. (2015) | ERP familiarity responsed | 2.5 to 5 years old at enrolment (average 3.97 years old) 9 month trial | NR | Little-to-no difference in change of the ERP familiarity response |
Obeid et al. (2022)26 SR
| Paired-associate learning | 6 week trial | 5 to 10 | Little-to-no difference between groups (P > 0.05) |
Design fluency | 6 week trial | 5 to 10 | Little-to-no difference between groups (P > 0.05) | |
Spatial working memory | 6 week trial | 5 to 10 | Little-to-no difference between groups (P > 0.05) | |
Spatial working memory strategy | 6 week trial | 5 to 10 | Little-to-no difference between groups (P > 0.05) | |
Quotient attention-deficit/ hyperactivity disorder | 6 week trial | 5 to 10 | Little-to-no difference between groups (P > 0.05) | |
Fine motor speed | 6 week trial | 5 to 10 | Little-to-no difference between groups (P > 0.05) | |
Obeid et al. (2022)26 SR
| Stanford–Binet Intelligence Scale, Fifth Edition (SB-5) | 2.5 to 5 years old at enrolment 4 year trial | Average 8.6 | Non-verbal IQ higher for choline group (P = 0.03) Working memory 11.7% higher for choline group (P = 0.01) Statistically significant subscores for nonverbal visual-spatial reasoning component (P = 0.004) and nonverbal working memory component (P = 0.018) |
Fuglestad et al. (2022)28 RCT Gimbel et al. (2022)29 RCT Same study as Wozniak et al. (2020), Wozniak et al. (2015) | Executive function performance | Choline group at enrolment: average 3.54 years old Placebo group at enrolment: average 4.18 years old Average 7 year follow-up (range 4 to 10 years) 9 month trial | Choline: average 10.56 Placebo: average 11.44 | Although choline group had numerically better values than placebo group, there was little-to-no difference between groups based on statistical significance in WISC-V working memory subtests (digit span, picture span), most of the D-KEFS Colour-Word Interference Test subtests (word reading, inhibition, inhibition/switching) and most of the subtests of the D-KEFS Trail Making Testf (visual scanning, number sequencing, letter sequencing, number/letter sequencing) Motor speed higher for choline vs. placebo (effect size = 1.14; P = 0.04). Colour naming better for choline vs. placebo (effect size = 1.27; P = 0.05) |
Brain structure | ||||
Fuglestad et al. (2022)28 RCT Gimbel et al. (2022)29 RCT Same study as Wozniak et al. (2020), Wozniak et al. (2015) | Corpus callosum measures | Choline group at enrollment: average 3.54 years old Placebo group at enrolment: average 4.18 years old Average 7 year follow-up (range 4 to 10 years) 9 month trial | Choline: average 10.56 Placebo: average 11.44 | Little-to-no difference in 7 out of 8 measures of corpus callosum NODDI ODIg Rostrum (P = 0.34) Genu (P = 0.55) Body prefrontal (P = 0.67) Body premotor (P = 0.61) Body central (P = 0.09) Body parietal (P = 0.05) Body temporal (P = 0.39) Lower ODI in the spleniumh effect size = −1.26 (P = 0.02) |
Safety | ||||
Obeid et al. (2022)26 SR
| Choline tolerance | NR | NR | Choline was tolerated well. |
Fishy body odour | 4 years | NR | Fishy body odour reported in 56% choline vs. 0% placebo | |
Obeid et al. (2022)26 SR
| Adverse events | NR | NR | Little-to-no difference in adverse events between groups (P > 0.15). Number of children reporting ≥ 1 adverse event in any symptom category was higher for choline vs. placebo (P = 0.03) |
D-KEFS = Delis-Kaplan Executive Function System; ERP = event-related potential; FASD = fetal alcohol spectrum disorder; IQ = intelligence quotient; NODDI = neurite orientation dispersion and density imaging; ODI = orientation dispersion index; PAE = prenatal alcohol exposure; SB-5 = Stanford–Binet Intelligence Scale Fifth Edition; vs. = versus; WISC-V = Wechsler Intelligence Scale for Children.
aFollow-up age in years unless otherwise indicated.
bMeasures global cognitive development and includes motor ability, language, and visual reception.26
cA measure of hippocampus-dependent sequential memory.26
dA measure of brain functioning and memory using brain electrical activity.28
eOutcomes were measured using the Cambridge Neuropsychological Test Automated Battery (CANTAB), NEPSY-2 Design Fluency test, Quotient ADHD system and grooved pegboard.26
fOutcomes measure executive function performance.29
gMRI (MRI) data were used to measure brain white matter microstructure which can indicate cognitive functioning.29
hMore coherent fibres and less fanning or bending.
Table 13: Summary of Recommendations in Included Guidelines – For Pregnant People
Recommendations and supporting evidence | Quality of evidence and strength of recommendations |
|---|---|
Adams et al. (2022)34 | |
“Therefore, for US women, we recommend that prenatal supplements contain at least 350 mg of choline during the first 2 trimesters, and roughly 600 mg in the third trimester, especially for women who do not consume several eggs/week (eggs have the highest dietary content of choline per serving, with one large egg containing 300 mg of choline). This recommendation appears likely to improve brain development in infants, and possibly help with other conditions as well. Choline is included in 40% of prenatal supplements; when included, the median level is 25 mg (Q1:10/Q3: 55) of 0.6 ± 550 mg. Only 2% of prenatal supplements meet or exceed our recommendation for choline” (p.24).34 Based on limited evidence; the authors cite 1 observational study, 3 reviews, and 4 treatment studies. | Quality of evidence: Low Strength of recommendation: Weak |
“Vegetarian or Vegan Dietary Patterns During Pregnancy and Lactation. Women following a vegetarian or vegan dietary pattern during these life stages may need to take special care to ensure nutrient adequacy. […] Women following a vegetarian or vegan dietary pattern should consult with a healthcare provider to determine whether supplementation of iron, vitamin B12, and/or other nutrients such as choline, zinc, iodine, or EPA/DHA is necessary and if so, the appropriate levels to meet their unique needs” (p. 116).33 Supporting evidence NR | NR |
“Most women do not meet recommended intakes of choline during pregnancy and lactation. Women are encouraged to consume a variety of choline-containing foods during these life stages. Choline can be found throughout many food groups and subgroups. Meeting recommended intakes for the dairy and protein food groups—with eggs, meats, and some seafood being notable sources—as well as the beans, peas, and lentils subgroup can help meet choline needs. Meeting nutrient needs through foods and beverages is preferred, but women who are concerned about meeting recommendations should speak with their healthcare provider to determine whether choline supplementation is appropriate. Many prenatal supplements do not contain choline or only contain small amounts inadequate to meet recommendations” (p. 117).33 Supporting evidence NR | NR |
Daily Nutritional Goals for Choline in Pregnant “Women” by Age and Trimester
Based on DRI reports from the Institute of Medicine and National Academies of Sciences, Engineering, and Medicine | NR |
Daily Nutritional Goals for Choline in Lactating “Women” by Age and Months Postpartum
Based on DRI reports from the Institute of Medicine and National Academies of Sciences, Engineering, and Medicine | NR |
“GDM: Dietary vitamin and mineral intake. RDNs should encourage women with GDM to make healthy food choices and consume a variety of foods to meet the micronutrient needs of pregnancy. The micronutrient needs of women with GDM are the same as for pregnant women without diabetes (i.e., emphasis on dietary intake of iron, folate, calcium, vitamin D, choline, and iodine). The consumption of more food to meet caloric needs and the increased absorption and efficiency of nutrient utilization that occurs in pregnancy, are generally adequate to meet the needs for most nutrients, when good food choices are consistently made” (p. 1736).32 Based on best practice clinical care guidelines; recommendation is supported by credible sources. | Rating: Consensusa Condition: Imperativeb |
“GDM: Vitamin and mineral supplementation. An RDN should consider recommending dietary supplementation within the DRI for pregnancy with a prenatal multivitamin/mineral or specific vitamin or mineral supplement(s) to address inadequate dietary vitamin and mineral intake (e.g., iron, folate, calcium, vitamin D, choline, and iodine) or documented micronutrient deficiency. Dietary supplements may be indicated in pregnant women at high risk for inadequate micronutrient intake, such as food insecurity; alcohol, tobacco, or other substance dependency; anemia; strict vegetarian (vegan) diet; or poor eating habits” (p. 1736).32 “Assessing for conditions and sociocultural factors, including vegan diet, multiple gestations, food insecurity, anemia, malabsorption disorder, gastrointestinal discomfort, substance [use], religious dietary restrictions, and poor quality diets that may influence adequate micronutrient intake can help identify pregnant women who require additional vitamin and mineral supplementation. Clinical judgment should be used when assessing nutritional status and recommending vitamin and mineral supplementation for high-risk patients. Some pregnant women might not tolerate vitamin and mineral supplementation and may require more intense nutrition therapy. Pregnant women who are taking or planning to take a nonprescribed OTC micronutrient supplement that exceeds the Tolerable Upper Limits for a specific vitamin or mineral or is taking herbal or dietary supplements should seek consultation from a pharmacist or physician” (p. 1737).32 “Risks/Harms of implementing this recommendation. Some individuals may not tolerate vitamin or mineral supplementation In general, pregnant women should seek medical consultation before or while taking a non-prescribed OTC micronutrient supplement that exceeds the Tolerable Upper Limits for a particular vitamin or mineral […] or if taking herbal supplements” (p.13).35 “Conditions of application. Consideration should be given to the total intake of micronutrients from all sources in the diet, such as fortified foods and beverages (e.g., calcium-fortified juice; grains enriched with iron, folic acid and other B-vitamins) and prescribed or non-prescribed vitamin and mineral supplements The RDN should use professional judgment when assessing nutrition status and determining the need for vitamin and mineral supplementation for those at high risk of nutrient deficiencies, including history of malabsorptive disorders (bariatric surgery), multifetal pregnancy, omission of food groups and eating disorders “(p.13).35 “Potential costs associated with application. There is an increased cost for vitamin and mineral supplements” (p.13).35 “The micronutrient needs of pregnant women with GDM are the same as for those without diabetes. Consuming sufficient calories to support recommended weight gain and eating a variety of foods to meet nutrient needs are beneficial for pregnant women […]. As long as good food choices are made, the higher intake of calories, coupled with the increased absorption and efficiency of nutrient utilization that occurs in pregnancy are generally adequate to meet the needs for most nutrients […]. However, vitamin and mineral supplementation may be warranted in pregnant women with multiple gestations, smoking and other substance dependency, poor quality diets, food insecurity, anemia or who are strict vegetarians (vegans) […]. For example, a vegan may need to supplement her diet with Vitamin D and Vitamin B12 […]” (p.13).35 “Choline. Because of its high rate of transport from mother to fetus, choline is considered an essential nutrient during pregnancy. A deficiency can interfere with normal fetal brain development […]. The AI for choline is 450 mg […]. Most pregnant women do not consume the AI for choline, despite its presence in many foods” (p.13).35 Based on credible resources with applicability to all pregnant women; DRIs, the California Diabetes and Pregnancy Program Sweet Success Guidelines for Care, the Academy’s position statement on nutrient supplementation, and the US Preventative Services Task Force. | Rating: Consensusa Condition: Imperativeb |
Nutrition Working Group SOGC (2016)31 | |
“Support women in understanding how to meet recommendations for specific nutrients of concern during pregnancy, which include folate, iron, choline, omega-3 fatty acids, and iodine” (p. 511).31 Supporting evidence for specific recommendation NR | Quality of evidence: Level IIIc Strength of recommendation: Good |
“Emerging evidence suggests that choline […] may be limited in the diets that pregnant women consume. Discuss foods rich in these nutrients (e.g., eggs for choline […]) with women as the pregnancy progresses (p. 511).31 Supporting evidence for specific recommendation NR | Quality of evidence: Level II-2d Strength of recommendation: Fair |
AI = adequate intake; DRI = Dietary Reference Intake; GDM = gestational diabetes mellitus; mg = milligram; NR = not reported; OTC = over the counter; RDN = registered dietitian nutritionist; SOGC = Society of Obstetricians and Gynaecologists of Canada
aExpert opinion supports the recommendation even though controlled trials were lacking or the evidence was inconsistent.
bBroadly applies to the target population.
cBased on opinions of authorities, clinical experience, descriptive studies, or expert committee reports.
dBased on well-design cohort or case-control studies.
Appendix 5: References of Potential Interest
Additional Publications With Findings also Reported in an Included Study
Curioni CC, Mocellin MC, Tavares MDS, et al. Effectiveness of nutritional interventions to prevent nonprogressive congenital and perinatal brain injuries: a systematic review and meta-analysis of randomized trials. Nutr Rev. 2022;80(11):2136-2153. PubMed
Freedman R, Hunter SK, Law AJ, Clark AM, Roberts A, Hoffman MC. Choline, folic acid, Vitamin D, and fetal brain development in the psychosis spectrum. Schizophr Res. 2022;247:16-25. PubMed
Ordenewitz LK, Weinmann T, Schluter JA, et al. Evidence-based interventions for children and adolescents with fetal alcohol spectrum disorders - A systematic review. Eur J Paediatr Neurol. 2021;33:50-60. PubMed
Derbyshire E, Obeid R. Choline, Neurological Development and Brain Function: A Systematic Review Focusing on the First 1000 Days. Nutrients. 2020;12(6):10. PubMed
Wozniak JR, Fink BA, Fuglestad AJ, et al. Four-year follow-up of a randomized controlled trial of choline for neurodevelopment in fetal alcohol spectrum disorder. J Neurodev Disord. 2020;12(1):9. PubMed
Sarkar DK, Gangisetty O, Wozniak JR, et al. Persistent Changes in Stress-Regulatory Genes in Pregnant Women or Children Exposed Prenatally to Alcohol. Alcohol Clin Exp Res. 2019;43(9):1887-1897. PubMed
Akison LK, Kuo J, Reid N, Boyd RN, Moritz KM. Effect of Choline Supplementation on Neurological, Cognitive, and Behavioral Outcomes in Offspring Arising from Alcohol Exposure During Development: A Quantitative Systematic Review of Clinical and Preclinical Studies. Alcohol Clin Exp Res. 2018;42(9):1591-1611. PubMed
Caudill MA, Strupp BJ, Muscalu L, Nevins JEH, Canfield RL. Maternal choline supplementation during the third trimester of pregnancy improves infant information processing speed: a randomized, double-blind, controlled feeding study. FASEB J. 2018;32(4):2172-2180. PubMed
Jacobson SW, Carter RC, Molteno CD, et al. Feasibility and Acceptability of Maternal Choline Supplementation in Heavy Drinking Pregnant Women: A Randomized, Double-Blind, Placebo-Controlled Clinical Trial. Alcohol Clin Exp Res. 2018;42(7):1315-1326. PubMed
Nguyen TT, Risbud RD, Mattson SN, Chambers CD, Thomas JD. Randomized, double-blind, placebo-controlled clinical trial of choline supplementation in school-aged children with fetal alcohol spectrum disorders. Am J Clin Nutr. 2016;104(6):1683-1692. PubMed
Ross RG, Hunter SK, Hoffman MC, et al. Perinatal Phosphatidylcholine Supplementation and Early Childhood Behavior Problems: Evidence for CHRNA7 Moderation. Am J Psychiatry. 2016;173(5):509-516. PubMed
Coles CD, Kable JA, Keen CL, et al. Dose and Timing of Prenatal Alcohol Exposure and Maternal Nutritional Supplements: Developmental Effects on 6-Month-Old Infants. Matern Child Health J. 2015;19(12):2605-2614. PubMed
Freedman R, Ross RG. Prenatal choline and the development of schizophrenia. Shanghai Arch Psychiatry. 2015;27(2):90-102. PubMed
Kable JA, Coles CD, Keen CL, et al. The impact of micronutrient supplementation in alcohol-exposed pregnancies on information processing skills in Ukrainian infants. Alcohol. 2015;49(7):647-656. PubMed
Leermakers ET, Moreira EM, Kiefte-de Jong JC, et al. Effects of choline on health across the life course: a systematic review. Nutr Rev. 2015;73(8):500-522. PubMed
Wozniak JR, Fuglestad AJ, Eckerle JK, et al. Choline supplementation in children with fetal alcohol spectrum disorders: a randomized, double-blind, placebo-controlled trial. Am J Clin Nutr. 2015;102(5):1113-1125. PubMed
Ongoing Trials
NCT05108974: Choline Supplementation as a Neurodevelopmental Intervention in Fetal Alcohol Spectrum Disorders Study (CHOLINE4). ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine; https://clinicaltrials.gov/study/NCT05108974. Accessed 2024 Jan 26.
NCT04395196: RCT of Prenatal Choline Supplementation During Pregnancy to Mitigate Adverse Effects of Prenatal Alcohol Exposure. ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine; https://clinicaltrials.gov/study/NCT04395196. Accessed 2024 Jan 26.
Systematic Review Protocol
Saha S, Saha S. The effects of prenatal dietary supplements on blood glucose and lipid metabolism in gestational diabetes mellitus patients: A systematic review and network meta-analysis protocol of randomized controlled trials. PLoS One. 2022;17(5):e0267854. PubMed
Nonsystematic Reviews
Jaiswal A, Dewani D, Reddy LS, Patel A. Choline Supplementation in Pregnancy: Current Evidence and Implications. Cureus. 2023;15(11):e48538. PubMed
Ernst AM, Gimbel BA, de Water E, et al. Prenatal and Postnatal Choline Supplementation in Fetal Alcohol Spectrum Disorder. Nutrients. 2022;14(3):06.
Recommendations or Position Papers with Unclear Methods
Health Canada. Reference values for Folate, Vitamin B12, Pantothenic acid, Biotin, and Choline. 2023: https://www.canada.ca/en/health-canada/services/food-nutrition/healthy-eating/dietary-reference-intakes/tables/reference-values-vitamins.html. Accessed 2024 Jan 26.
Marshall NE, Abrams B, Barbour LA, et al. The importance of nutrition in pregnancy and lactation: lifelong consequences. Am J Obstet Gynecol. 2022;226(5):607-632. PubMed
EFSA Panel on Dietetic Products, Nutrition and Allergies (NDA). Dietary Reference Values for choline. EFSA Journal. 2016;14(8):e04484.
Hanson MA, Bardsley A, De-Regil LM, et al. The International Federation of Gynecology and Obstetrics (FIGO) recommendations on adolescent, preconception, and maternal nutrition: “Think Nutrition First”. Int J Gynaecol Obstet. 2015;131 Suppl 4:S213-253. PubMed
Procter SB, Campbell CG. Position of the Academy of Nutrition and Dietetics: Nutrition and Lifestyle for a Healthy Pregnancy Outcome. J Acad Nutr Diet. 2014;114(7):1099-1103. PubMed
Not in English
Heras-Sola J, Gallo-Vallejo JL. Importance of choline during pregnancy and lactation: A systematic review. Semergen. 2024 Jan-Feb;50(1):102089. PubMed
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for noncommercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca