CADTH Health Technology Review
Aerosol Therapy With Inhalers During Mechanical Ventilation
Rapid Review
Authors: Robyn Haas, Jennie Horton
Key Messages
What Is the Issue?
Mechanical ventilation helps individuals breathe when they cannot do so on their own. During mechanical ventilation, aerosol therapy is used to deliver medication to the lungs of the person who is using the ventilator.
High doses of aerosol therapy administered via metered dose inhaler for adults and older adults who are mechanically ventilated is common clinical practice. However, the reasoning behind this practice, and whether it has clinical benefits compared to no doses and standard doses, is unclear.
What Did We Do?
To inform decisions about high doses of aerosol therapy delivered with metered dose inhalers in adults and older adults receiving mechanical ventilation, we sought to identify and summarize literature comparing the clinical effectiveness of inhaled high doses of aerosol therapy versus no aerosol therapy. We also sought to identify and summarize literature comparing the clinical effectiveness of inhaled high doses of aerosol therapy versus standard doses.
A research information specialist conducted a literature search of peer-reviewed and grey literature sources published between January 1, 2004, and January 25, 2024. The search was limited to English-language documents. One reviewer screened articles for inclusion based on predefined criteria, critically appraised the included study, and narratively summarized the findings.
What Did We Find?
We found 1 retrospective chart review that compared the clinical effectiveness of 2 different doses of inhaled high doses of aerosol therapy. The findings from this study suggest that, compared to lower doses, higher doses of salbutamol are associated with more days alive and free of acute lung injury and more days alive and free of indicators of acute respiratory distress and respiratory failure.
We did not find any studies that compared the clinical effectiveness of inhaled high doses of aerosol therapy to no aerosol therapy for adults and older adults receiving mechanical ventilation that met inclusion criteria for our review.
What Does It Mean?
The available evidence with methodological limitations suggests that high doses of aerosol therapy with salbutamol may be associated with better clinical respiratory outcomes when compared to low doses in patients with acute lung injury who are mechanically ventilated. To inform future clinical practice, decision-makers may want to consider the potential risks and benefits and environmental implications of aerosol therapy, as well as implementation factors (e.g., resource needs, risk of contamination).
Additional clinical studies would help provide a better understanding of the optimal dosage and clinical effectiveness of aerosol therapy for patients who are mechanically ventilated.
Abbreviations
ALI
acute lung injury
COPD
chronic obstructive pulmonary disease
FiO2
fraction of inspired oxygen
ICU
intensive care unit
MDI
metered dose inhaler
PaO2
partial pressure of oxygen
Context and Policy Issues
What Is Mechanical Ventilation?
Mechanical ventilation is a method that helps a person breathe when they cannot do so on their own.1,2 It works by applying a positive pressure breath, which pushes air into the lungs to provide oxygen and remove carbon dioxide.1,2 The ventilator, which is the primary device used for mechanical ventilation, ensures that the airways stay open and the lungs do not collapse.1,2 Mechanical ventilation can be invasive or noninvasive.1 Noninvasive ventilation uses a face mask secured over a person’s nose and mouth and is typically used in those with mild to moderate difficulty breathing.1 Invasive ventilation is for people with severe breathing difficulties and uses an endotracheal tube that is placed into the upper airway.1 There are many reasons why a person might need a ventilator, but some common reasons include compromised airways, low oxygen levels, and severe shortness of breath related to infection.2,3 One specific condition that may require the use of a ventilator is acute lung injury (ALI), which is a life-threatening disease that manifests as inflammation in the lungs and is defined by impaired oxygenation and abnormalities on both sides of a chest radiograph.4
Aerosol Therapy During Mechanical Ventilation
Aerosol therapy is the administration of medication to the lungs through inhalation.5,6 It can help treat numerous respiratory conditions, including asthma, chronic obstructive pulmonary disease (COPD), and cystic fibrosis.5,6 One type of medication that can be aerosolized and inhaled is bronchodilators,5,6 which are medications that relax the muscles surrounding the airway to help improve breathing.7,8 When used during mechanical ventilation, bronchodilators work to decrease airway resistance and treat bronchospasms or bronchoconstriction, which in turn improves the synchrony between the person and the ventilator.7,8 Inhaled bronchodilators in those who are mechanically ventilated may be administered by either a nebulizer or a metered dose inhaler (MDI).7
What Is the Current Practice?
In people who are mechanically ventilated, bronchodilators can be administered systemically (i.e., intravenously) or directed at the target site via inhalation.7 Providing a high dose of aerosol therapy with MDIs in this population has been the standard practice for more than 20 years.7 This is also the case for individuals who have coexisting respiratory conditions such as asthma, COPD, or other underlying lung conditions.7 The most used bronchodilators in these populations include salbutamol and ipratropium bromide.9,10 An example of a high dose of salbutamol is 8 puffs administered via an MDI every 2 hours.7 Each puff contains 100 mcg of salbutamol and is given to help relieve bronchospasm or wheezing.7 An example of a high dose of ipratropium bromide is 8 puffs administered via an MDI every 6 hours.7 Each puff contains 20 mcg of ipratropium bromide and is given to help relieve bronchospasm or wheezing.7 Ipratropium bromide is only administered to individuals with asthma or COPD.7 In addition to bronchodilators, corticosteroids can also be administered to people receiving mechanical ventilation.11,12 One of these medications is fluticasone, which can reduce inflammation and improve patient synchrony with the ventilator. An example of a high dosage of fluticasone is 1,000 mcg administered twice per day.11,12
Why Is It Important to Do This Review?
While providing high doses of aerosol therapy via MDIs is common practice, the reason behind this practice is unclear. In situations where there is a surplus of inhalers, this practice can result in wasted products, which has environmental and cost implications. This review can help inform clinical practice by investigating whether high doses of aerosol therapy have clinical benefits compared to no doses of aerosol therapy and, if so, whether these benefits also exist when compared to standard doses. These findings can, in turn, potentially help reduce waste and decrease spending.
Objective
The purpose of this report is to summarize and critically appraise the evidence identified from medical databases and grey literature about the clinical effectiveness of inhaled high doses of aerosol therapy versus standard doses or no aerosol therapy in adults and older adults receiving mechanical ventilation.
Research Questions
What is the clinical effectiveness of inhaled high doses of aerosol therapy versus no aerosol therapy in adults and older adults receiving mechanical ventilation?
What is the clinical effectiveness of inhaled high doses of aerosol therapy versus standard doses in adults and older adults receiving mechanical ventilation?
Methods
Literature Search Methods
An information specialist conducted a literature search on key resources including MEDLINE, the Cochrane Database of Systematic Reviews, the International HTA Database, and the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search approach was customized to retrieve a limited set of results, balancing comprehensiveness with relevancy. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. Search concepts were developed based on the elements of the research questions and selection criteria. The main search concepts were metered dose inhalers and mechanical ventilation. The search was completed on January 24, 2024, and limited to English-language documents published since January 1, 2004.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
|---|---|
Population | Adults and older adults receiving mechanical ventilation (≥ 18 years of age) |
Intervention | High doses of aerosol therapy delivered with metered dose inhalers, specifically:
|
Comparator | Q1: No aerosol therapy, placebo Q2: Standard dose of aerosol therapy delivered with a metered dose inhaler, specifically:
|
Outcomes | Q1 to Q2: Clinical benefits (e.g., improved respiratory function) and harms (e.g., adverse effects) |
Study designs | Health technology assessments, systematic reviews, randomized controlled trials, nonrandomized studies |
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, were duplicate publications, or were published before 2004.
Critical Appraisal of Individual Studies
The included publication was critically appraised by 1 reviewer using the Downs and Black checklist13 for randomized and nonrandomized studies as a guide. Summary scores were not calculated for the included studies; rather, the strengths and limitations of the included publication was described narratively.
Summary of Evidence
Quantity of Research Available
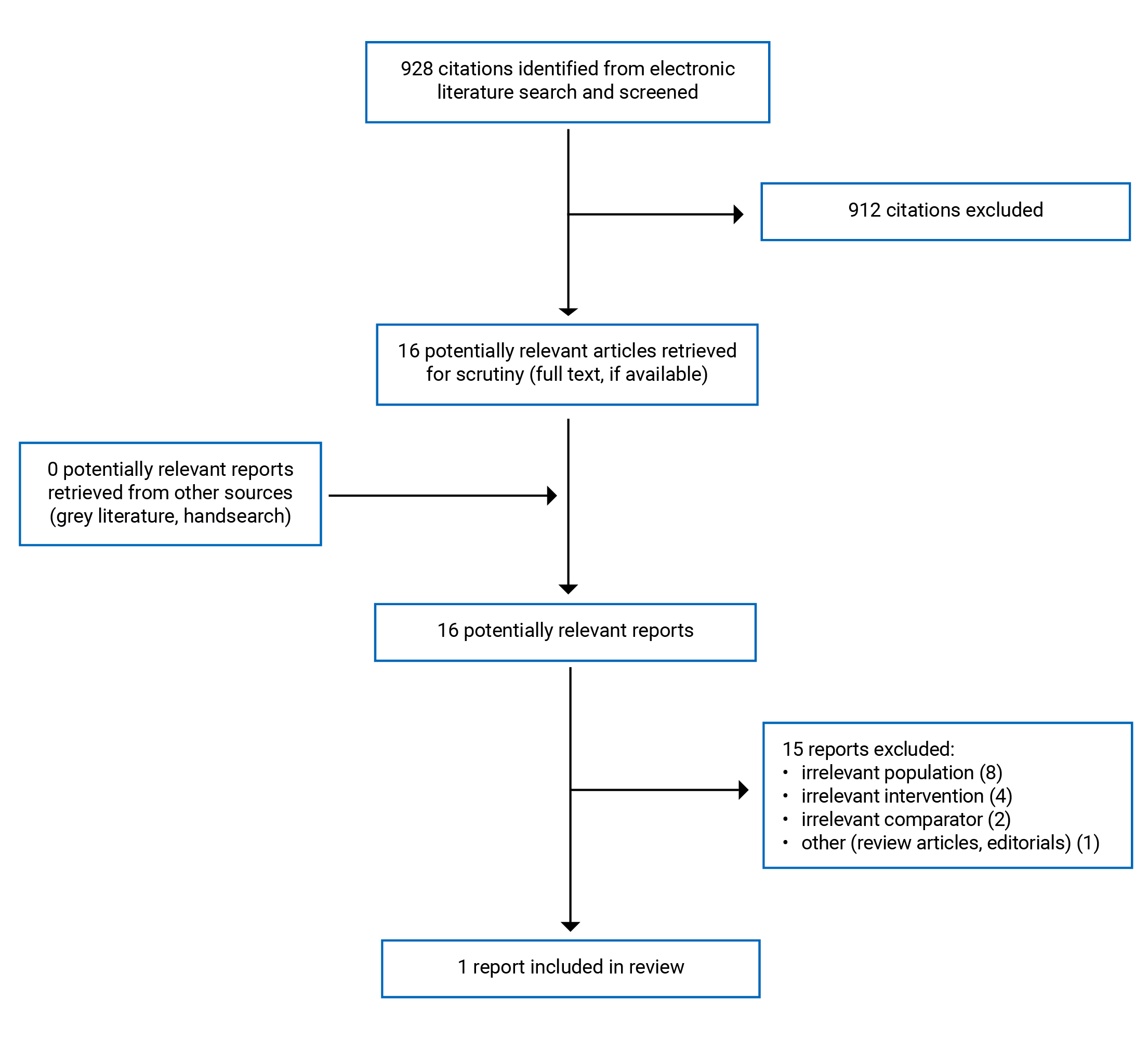
We identified a total of 928 citations in the literature search. Following screening of titles and abstracts, we excluded 912 citations and retrieved 16 potentially relevant reports from the electronic search for full-text review. Of these potentially relevant articles, we excluded 15 publications for various reasons; 1 retrospective chart review cohort study14 met the inclusion criteria and was included in this report. Appendix 1 presents the PRISMA15 flow chart of the study selection.
Appendix 5 presents additional reference of potential interest. These additional studies include a related CADTH report, a single-arm study about the effect of albuterol on expiratory resistance, and a mixed intervention study about personalized bronchodilator dosing.
Summary of Study Characteristics
This report includes 1 retrospective chart review14 conducted at a hospital in Canada. The study compared the clinical effectiveness of 2 different doses (referred to as “low dose” and “high dose”) of salbutamol on duration and severity of ALI in patients who were mechanically ventilated.14 This study was a chart review of 86 adults who were consecutively admitted to a tertiary care medical-surgical intensive care unit (ICU).14 All patients met the definition of ALI and were receiving mechanical ventilation.14 There were 64 patients in the low dose salbutamol group; their average age was 54.7 years, 41% were female, and 15.6% had a history of COPD, asthma, or smoking.14 There were 22 patients in the high dose salbutamol group; their average age was 65.7 years, 45% were female, and 45.5% had a history of COPD, asthma, or smoking.14
In this study, the authors included patients who were administered salbutamol by either an MDI (8 to10 puffs at 100 mcg per puff) or a nebulizer (2.5 mg to 5 mg).14 The authors calculated the average daily dose of salbutamol (mg per day) while in the ICU as the sum of total MDI and nebulization dose divided by the number of days in the ICU.14 They classified the low dose group as patients who received less than 2.2 mg per day of salbutamol and the high dose group as patients who received 2.2 mg per day or more of salbutamol.14
The primary outcome investigated in this study was the number of days alive and free of ALI over the span of 28 days.14 Days alive and free of ALI is a measure of the disease’s duration and severity. Secondary outcomes included 28-day mortality; days alive and free of cardiovascular, renal, hepatic, neurologic, and hematological dysfunction; and days alive and free of PaO2/ FiO2 < 300 (PaO2 is the partial pressure of oxygen and FiO2 is the fraction of inspired oxygen).14 The PaO2/FiO2 ratio helps identify acute respiratory distress and respiratory failure.14 The authors did not separately report outcomes for patients who received salbutamol via an MDI from those who received salbutamol via nebulization.14
Appendix 2 presents the additional details regarding the characteristics of the included publication.
Summary of Critical Appraisal
The included study had several strengths related to reporting. The aim, intervention, comparator, and main findings of the study were all clearly described.14 Additionally, it provided the standard error and reported actual P values for most of the main outcomes.14 The exception to this was the outcome of days alive and free of PaO2/FiO2 < 300.14 The study reported a significant difference in days alive and free of PaO2/FiO2 < 300 between the high dose and low dose salbutamol groups but it did not provide the mean and standard errors associated with these results; rather, the authors only presented a bar graph and P value.14
This study took some steps to help improve its internal validity; for instance, all included patients were consecutively enrolled and were recruited from 1 ICU in the same hospital.14 The authors performed appropriate statistical tests for the main outcomes; for example, they performed a t test for continuous variables and a chi-square test for categorical variables, which are appropriate to compare means between the low and high dose salbutamol groups for the outcomes of interest.14 The study also reported potential confounding variables such as age and history of COPD, asthma, or smoking.14 These baseline characteristics differed between the high and low dose salbutamol groups, as the high dose group had older participants and a greater proportion of patients with a history of COPD, asthma, or smoking.14 The authors addressed this by performing a multivariate analysis to adjust for the differences in these baseline characteristics.14 Finally, hospital ICUs are often where patients who are receiving mechanical ventilation are treated; therefore, this study was representative of the treatment the majority of patients receive. This, in turn, contributes to the external validity of the study.
This study also had limitations. It used a retrospective chart review design, which has inherent limitations, including a lack of randomization or blinding.14 Participants were grouped into cohorts based on the dose of salbutamol they received; however, the methods or parameters used to determine these dosages were not clear.14 These factors, in addition to the differences in baseline characteristics, created challenges in interpreting between-group differences.14 The authors did not report adverse events that may have been a consequence of low or high dose salbutamol.14 As well, the included patients were administered salbutamol by both an MDI and nebulization.14 Administration of a medication via an MDI is measured in the number of puffs and the amount of mcg in each puff (e.g., 4 puffs of salbutamol at 100 mcg per puff), whereas administration of a medication via nebulization is measured in mg (e.g., 2.5 mg of salbutamol). In this study, the authors reported the calculated average dose of salbutamol that patients received over the 28-day period in mg only.14 However, they did not provide information on how they converted the MDI dosing to match the nebulizer dosing, or what considerations where in place when they did so.14 As a result, the information that users can gather from these results is less detailed.
Finally, the authors did not report if, or from where, they received funding, though they did declare that they had no related conflicts of interest.14
Appendix 3 presents additional details about the strengths and limitations of the included publication.
Summary of Findings
We identified 1 retrospective chart review that compared the clinical effectiveness of low dose and high dose salbutamol on duration and severity of ALI in patients receiving mechanical ventilation.14 The study reported days alive and free of ALI; days alive and free of PaO2/ FiO2 < 300; days alive and free of cardiovascular, renal, neurologic, and hematological dysfunction; and 28-day mortality.14
Appendix 4 presents the main study findings.
Clinical Effectiveness of High Doses of Aerosol Therapy
Days Alive and Free of ALI
Patients in the high dose salbutamol group had significantly more days alive and free of ALI than the low dose salbutamol group.14 The high dose group had a mean of 12.2 days (standard error = 4.4) alive and free of ALI, whereas the low dose group had a mean of 7.6 days (standard error = 1.9).14
Days Alive and Free of PaO2/FiO2 < 300
Patients in the high dose salbutamol group had significantly more days alive and free of PaO2/FiO2 < 300 than those in the low dose salbutamol group.14 The authors presented these results graphically and did not provide exact numerical values.
Days Alive and Free of Cardiovascular, Renal, Hepatic, Hematological, and Neurologic Dysfunction
The results of the study indicate that there was no significant difference in cardiovascular, renal, hepatic, hematological, or neurologic dysfunction between the high dose salbutamol group and low dose salbutamol group.14
28-Day Mortality
The results of the study indicate that there was no significant difference in 28-day mortality between the high and low dose salbutamol group.14
Limitations
While the study included in this report had several strengths in terms of validity and reporting, the overall paucity of literature in this area limits our ability to draw strong conclusions. As there was only 1 study14 that met the criteria for this review, we cannot investigate if there are consistent findings or discrepancies in the clinical outcomes of different doses of aerosol therapy. Additionally, the included study only examined the effects of salbutamol.14 While salbutamol is a commonly used bronchodilator in Canada, other medications, such as ipratropium bromide or corticosteroids such as fluticasone, may also be used. However, because the identified study did not investigate these 2 medications, our findings about high doses of aerosol therapy may not apply in scenarios where they are used. The included study reported outcomes for patients who received salbutamol by both an MDI and a nebulizer.14 It reported outcomes for the entire cohort but did not provide any subgroup analyses for patients who received salbutamol only by an MDI or only by a nebulizer.14 Consequently, based on the included study, we are unable to determine if the outcomes are similar between the 2 methods of administration or if they differed in clinical benefits and harms; we also cannot draw conclusions specific to the clinical effectiveness of MDIs only.14 Finally, because we did not identify any relevant literature that compared high dose aerosol therapy to no aerosol therapy, we are unable to comment on how clinical outcomes such as respiratory function and adverse events may compare in such situations.
Conclusions and Implications for Decision- or Policy-Making
Summary of Evidence
This report aimed to summarize evidence about the clinical effectiveness of inhaled high doses of aerosol therapy versus standard doses or no aerosol therapy in adults and older adults receiving mechanical ventilation. We included 1 retrospective chart review14 that compared the clinical effectiveness of low doses and high doses of salbutamol administered via either an MDI or a nebulizer. We did not identify any health technology assessments, systematic reviews, or randomized controlled trials. We also did not identify any evidence about the clinical effectiveness of inhaled high doses of aerosol therapy versus no aerosol therapy. The findings of this report suggest that, compared to lower doses, higher doses of salbutamol administered via an MDI or a nebulizer may be associated with more days alive and free of ALI and more days alive and free of PaO2/FiO2 < 300 (PaO2/FiO2 < 300 is an indicator of respiratory distress and failure).14 The findings also suggest that the dose of salbutamol is not associated with differences in days alive and free of cardiovascular, renal, hepatic, hematological, and neurologic dysfunction.14
Considerations for Future Research
This is an area of research that would benefit from additional high-quality clinical studies. For instance, placebo-controlled studies could provide findings about respiratory function, duration of mechanical ventilation or hospitalization, and mortality related to high doses of aerosol therapy. Additionally, randomized controlled trials that examine the comparative clinical effectiveness of high doses and standard doses of aerosol therapy could provide insight into whether dosing plays a meaningful role in such outcomes. Studies that examine other types of medications used in aerosol therapy, such as other bronchodilators or corticosteroids, could help inform whether the clinical benefits and harms of high doses of aerosol therapy are dependent on the type of medication used. Based on the included study, there also seems to be a lack of consistency around the dosages of these medications. While the authors in the study defined the threshold between the high dose and low dose salbutamol groups based on past research, they noted that other studies indicate that even higher doses may be required to achieve clinical benefits.16 Future studies that investigate the benefits and harms of varying doses of aerosol therapy could help identify which dosage would be optimal for use in people who are receiving mechanical ventilation. Finally, further research in this area may also have environmental impacts. MDIs produce notable carbon emissions, so it is important to ensure they are being used appropriately and only when necessary to help reduce waste.17
Implications for Clinical Practice
Administering high doses of aerosol therapy via metered dose inhaler for people who are mechanically ventilated has been the standard practice for over 20 years.7 Generally, bronchodilators are relatively safe to use, easy to administer, do not require a great deal of personnel time, have a low risk of contamination, and provide reliable dosages.7 While a common risk of MDIs is improper use, this concern is not as relevant in settings where health care providers administer the medication.7 Given the limited amount of evidence about the comparative clinical effectiveness of different doses, or no doses, of aerosol therapy, it is important to consider the potential risks to patients if aerosol therapy were not used. Considering the known benefits and relatively low risk of bronchodilators, and the critical role ventilators have in survival, it may be reasonable to provide patients who are mechanically ventilated with a treatment that aims to optimize synchrony between the person and ventilator.
From a broader environmental standpoint, it is important to be cognizant of the impact of MDIs on greenhouse gas emissions. Ensuring that MDIs are used appropriately can help decrease the carbon footprint.17,18 When deciding whether to administer high doses of aerosol therapy to people who are mechanically ventilated, it may be beneficial to consider whether there are other methods of administration that are similarly effective but produce lower greenhouse gas emissions.
References
1.Walter K. Mechanical Ventilation. JAMA. 2021;326(14):1452-1452. PubMed
2.Hickey SM, Giwa AO. Mechanical Ventilation. StatPearls. Treasure Island (FL): StatPearls Publishing; 2023: https://www.ncbi.nlm.nih.gov/books/NBK539742/. Accessed 2024 Feb 07.
3.Mechanical Ventilation. ATS Patient Education Series. New York (NY): American Thoracic Society; 2017: https://www.thoracic.org/patients/patient-resources/resources/mechanical-ventilation.pdf. Accessed 2024 Feb 07.
4.Johnson ER, Matthay MA. Acute lung injury: epidemiology, pathogenesis, and treatment. J Aerosol Med Pulm Drug Deliv. 2010;23(4):243-252. PubMed
5.Dhanani J, Fraser JF, Chan HK, Rello J, Cohen J, Roberts JA. Fundamentals of aerosol therapy in critical care. Crit Care. 2016;20(1):269. PubMed
6.Hess D, Dhand R. Delivery of inhaled medication in adults. In: Post TW, ed. UpToDate. Waltham (MA): UpToDate; 2023: http://www.uptodate.com/. Accessed 2024 Jan 17.
7.Georgopoulos D, Mouloudi E, Kondili E, Klimathianaki M. Bronchodilator delivery with metered-dose inhaler during mechanical ventilation. Crit Care. 2000;4(4):227-234. PubMed
8.Maccari JG, Teixeira C, Gazzana MB, Savi A, Dexheimer-Neto FL, Knorst MM. Inhalation therapy in mechanical ventilation. J Bras Pneumol. 2015;41(5):467-472. PubMed
9.Dhand R. How Should Aerosols Be Delivered During Invasive Mechanical Ventilation? Respir Care. 2017;62(10):1343-1367. PubMed
10.Dhand R, Tobin MJ. Inhaled bronchodilator therapy in mechanically ventilated patients. Am J Respir Crit Care Med. 1997;156(1):3-10. PubMed
11.Nava S, Compagnoni ML. Controlled short-term trial of fluticasone propionate in ventilator-dependent patients with COPD. Chest. 2000;118(4):990-999. PubMed
12.Remien K, Bowman A. Fluticasone. StatPearls. Treasure Island (FL): StatPearls Publishing; 2022: https://www.ncbi.nlm.nih.gov/books/NBK542161/. Accessed 2024 Jan 26.
13.Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377-384. PubMed
14.Manocha S, Gordon AC, Salehifar E, Groshaus H, Walley KR, Russell JA. Inhaled beta-2 agonist salbutamol and acute lung injury: an association with improvement in acute lung injury. Crit Care. 2006;10(1):R12. PubMed
15.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
16.Dhand R, Duarte AG, Jubran A, et al. Dose-response to bronchodilator delivered by metered-dose inhaler in ventilator-supported patients. Am J Respir Crit Care Med. 1996;154(2 Pt 1):388-393. PubMed
17.Sustainable Inhalers in Primary Care. Toronto (ON): CASCADES Canada; 2022: https://cascadescanada.ca/wp-content/uploads/2022/07/CASCADES-INHALER-PLAYBOOK-FINAL_EN.pdf. Accessed 2024 Feb 07.
18.Smith A, Severn M. Reducing the Environmental Impact of Clinical Care. Can J Health Technol. 2023;3(4). https://canjhealthtechnol.ca/index.php/cjht/article/view/EH0112. Accessed 2024 Feb 8. PubMed
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Note that this appendix has not been copy-edited.
Table 2: Characteristics of Included Primary Clinical Study
Study citation, country, funding source | Study design | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Manocha et al.(2006)14 Canada Funding source: NR. Authors declared they had no competing interests. | Nonrandomized, retrospective chart review | 86 patients admitted to a tertiary care medical-surgical ICU. All patients met the definition of ALI and were receiving mechanical ventilation. Low Dose Group
High Dose Group:
| Intervention: High dose salbutamol (≥ 2.2 mg/day) Comparator: Low dose salbutamol (< 2.2mg/day) Salbutamol was administered via MDI and nebulizer both groups. | Outcomes:
Follow-up: 28 days or until discharge from the ICU (if less than 28 days) |
ALI = acute lung injury; COPD = chronic obstructive pulmonary disease; ICU = intensive care unit; MDI = metered dose inhaler; NR = not reported.
Note: Only the percentage of female patients was reported in the study. Values for age are reported as the mean ± standard error, in years.
Appendix 3: Critical Appraisal of Included Publications
Note that this appendix has not been copy-edited.
Table 3: Strengths and Limitations of Clinical Study Using the Downs and Black Checklist13
Strengths | Limitations |
|---|---|
Manocha et al.(2006)14 | |
The aim of the study was clearly described. The intervention and comparators were clearly described. The main findings of the study were clearly described. The places and facilities that patients were treated was representative of the treatment that the majority of patients receive. The patients were consecutively enrolled and were recruited from the same hospital unit. The study used appropriate statistical tests to assess the main outcomes. The study provided estimates of the variability (standard error) in most of the outcome data. The actual p values were reported. The study stated potential confounding variables (differences in baseline characteristics) and included them in their regression model to adjust for these differences. The study authors declared no related conflicts of interest. | The study design was a retrospective chart review. As a result, there was no randomization or blinding in the study. The baseline characteristics differed between the low dose and high dose groups. The high dose group was older and had a higher proportion of patients with a history of COPD, asthma, or smoking. It was unclear how the daily amounts of salbutamol that patients received were determined. Adverse events that may have been a consequence of the intervention were not reported. The study included individuals who were administered the intervention by 2 different methods (MDI and nebulization) but it was unclear how they converted the MDI dosing (in mcg per puff) to match nebulization dosing (in mg) or how conversion may have influenced results. The study reported a significant result for one of the outcomes of interest and presented the result graphically but did not provide the associated numerical value or estimate of variability. Authors did not report if, or from where, they received funding. |
COPD = chronic obstructive pulmonary disease; MDI = metered dose inhaler.
Appendix 4: Main Study Findings
Note that this appendix has not been copy-edited.
Table 4: Summary of Findings by Outcome — Days Alive and Free of ALI, PaO2/FiO2 < 300, Cardiovascular Dysfunction, Renal Dysfunction, Hepatic Dysfunction, Hematological Dysfunction, and Neurologic Dysfunction
Study | Days Alive and Free of | Low Dose Salbutamola (n = 22) | High Dose Salbutamola (n = 64) | p value |
|---|---|---|---|---|
Manocha et al.(2006)14 | ALI | 7.6 ± 1.9 | 12.2 ± 4.4 | 0.02 |
PaO2/FiO2 ratio < 300 | NR | NR | 0.05 | |
Cardiovascular dysfunction | 11.5 ± 2.6 | 13.2 ± 4.2 | 0.50 | |
Renal dysfunction | 14.3 ± 2.9 | 16.0 ± 4.5 | 0.55 | |
Hepatic dysfunction | 17.4 ± 2.8 | 19.6 ± 4.4 | 0.42 | |
Hematological dysfunction | 15.9 ± 2.9 | 19.6 ± 4.5 | 0.10 | |
Neurologic dysfunction | 16.6 ± 2.6 | 19.0 ± 3.9 | 0.35 |
ALI = acute lung injury; FiO2 = fraction of inspired oxygen; NR = not reported; PaO2 = partial pressure of oxygen.
aValues are reported as the mean ± standard error, in days.
Table 5: Summary of Findings by Outcome — 28-Day Mortality
Study | Low Dose Salbutamol (n = 22) | High Dose Salbutamol (n = 64) | p value |
|---|---|---|---|
Manocha et al.(2006)14 | 46.9% | 50.0% | 0.080 |
Appendix 5: References of Potential Interest
Previous CADTH Reports
Discussion of Environmental Impacts of Metered Dose Inhalers
Smith A, Severn M. Reducing the Environmental Impact of Clinical Care. Can J Health Technol. 2023;3(4). https://canjhealthtechnol.ca/index.php/cjht/article/view/EH0112 PubMed
Nonrandomized Studies
Combined Fluticasone and Salmeterol; Personalized Dosing
Wu SH, Shyu LJ, Li CH, et al. Better airway resistance reduction profile in intubated COPD patients by personalized bronchodilator dosing: A pilot randomized control trial. Pulm Pharmacol Ther. 2018;49:134-139. PubMed
Before-and-After Study
Kondili E, Alexopoulou C, Prinianakis G, Xirouchaki N, Vaporidi K, Georgopoulos D. Effect of albuterol on expiratory resistance in mechanically ventilated patients. Respir Care. 2011;56(5):626-632. PubMed
Contributors: Anusree Subramonian, Elizabeth Carson
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for noncommercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca.