CADTH Health Technology Review
Intra-Articular Hyaluronic Acid for Osteoarthritis of the Hip, Shoulder, and Ankle
Rapid Review
Authors: Angela M. Barbara, Lindsay Ritchie, Melissa Severn
Key Messages
What Is the Issue?
Osteoarthritis (OA) is a chronic disease of the joints, such as the hip, shoulder, and ankle. OA causes the joints to be painful, unstable, and less functional. In adults 55 years and younger, joint trauma is a common cause of OA.
Hyaluronic acid (HA) is a naturally occurring molecule found in human cells that provides lubrication when injected into the joint. HA injections are a less invasive option than surgery, with potentially fewer complications.
To support decision-making about treating hip, shoulder, or ankle OA in adults 55 years and younger, it is important to understand the potential benefits and harms of using HA in this population.
What Did We Do?
We reviewed the clinical effectiveness of high molecular weight (MW) injection of HA in adults between the ages of 18 and 55 years with OA of the hip, shoulder, or ankle joints to guide decisions on the use of high MW HA injection.
An information specialist searched for peer-reviewed and grey literature sources published on January 1, 2013 to December 12, 2023. One reviewer screened citations and selected and critically appraised the included studies.
What Did We Find?
The evidence for this report was based on observational before-and-after studies. We found no relevant comparative studies examining the effect of high MW HA versus placebo or no treatment.
While most studies reported post-treatment outcome improvements, it is uncertain whether high MW injection of HA improves pain, function, and disability in adults 55 years and under with hip, shoulder, or ankle OA. This is due to the low-quality evidence, small sample sizes, and methodological problems. Serious side effects of high MW HA were not reported.
What Does This Mean?
Due to the uncertainty of the clinical effectiveness evidence, health care providers and decision-makers may consider other factors when considering high MW IA-HA for patients with hip, shoulder, or ankle OA; these factors could include acceptability, feasibility, costs, health equity, and patient values and preferences.
Future research from randomized studies in large populations is needed to understand the effectiveness and safety of high MW HA injections for hip, shoulder, and ankle OA.
Abbreviations
HA
hyaluronic acid
IA
intra-articular
MW
molecular weight
NICE
National Institute for Health and Care Excellence
OA
osteoarthritis
SR
systematic review
Context and Policy Issues
What Is OA?
Osteoarthritis (OA) is a progressive disorder of the joint.1,2 It is the most common type of arthritis that causes damage to the articular cartilage and underlying bone.1 The most frequently affected joints include the knee and hip, and the less commonly affected joints include the shoulder (glenohumeral) and ankle.1 In response to OA, the body produces additional synovial fluid to offset the affected joint.3 The increased fluid causes inflammation and pain.3 OA can also cause other symptoms, such as limitation of movement, stiffness, and disability.4 Risk factors for OA include older age (due to progressive degeneration), female sex, family history, excess body weight, joint trauma, and repeated stress on a particular joint (e.g., through sport or work-related activities).1,5 Approximately 219,000 Canadians aged 20 years and older (8.7 per 1,000 persons per year) were newly diagnosed with OA from 2016 to 2017.2 The prevalence of OA during these years was 13.6% and is projected to increase to 18.6% among adults in Canada and the direct cost of OA (including hospitalization, physician and outpatient services, alternative care, out-of-pocket costs, drugs, rehabilitation, home care, formal caregiver, and side effects of drugs) to increase from CAD $2.9 billion to CAD $7.6 billion (2010 values).2,6
What Is the Current Practice?
OA is a chronic disease, and there is no cure.7 Therefore, treatment focuses on reducing pain and improving functional outcomes.4 Front-line treatment includes exercise, physical therapy, local analgesics, and nonsteroidal anti-inflammatory drugs to relieve pain and inflammation.1,8,9 Conservative treatment before surgery includes injections of glucocorticoids, corticosteroids, and platelet-rich plasma.1,8,9 Operative treatments include arthroscopy, joint preserving surgery, joint fusion, and joint replacement.10 Surgery is often considered a last resort option for end-stage OA due to the risks of surgical complications (e.g., infectious disease, nerve injuries, dislocation).4,11 Surgery is especially problematic in patients 35 years of age and younger because of the requirement for longer implant survival and the need for revision surgery.12 None of these interventions have been shown to stop disease progression or reverse cartilage deterioration.4
What Is IA-HA?
HA is a natural component of synovial fluid.4,11 Intra-articular (IA-) HA injections (also called viscosupplementation) are gel-like fluid injections that help lubricate the joint and protect the cartilage and surrounding soft tissues.4,11 HA has been approved in Canada for treating mild to moderate knee OA since 1992.13 IA-HA injections have been accepted as an alternative treatment for OA in people who do not respond to front-line interventions, such as physical therapy or pain medication.14-16 However, most evidence on the clinical effectiveness of IA-HA comes from research on knee OA,17,18, while the effects reported for the hip, shoulder, and ankle joints are limited.17 The evidence suggests that IA-HA products with high MW; defined as greater than 3,000 kDa) have better effectiveness and safety for OA of the knee than lower MW products.13,18,19
Why Is it Important to Do This Review?
In 2019, CADTH produced 2 Rapid Reviews on IA-HA to manage OA of the hip and ankle,14 and the shoulder.15 In 1 report,14 the evidence suggested no effect of IA-HA compared to placebo on pain and adverse events for hip OA, and a potential benefit of IA-HA compared to saline on pain and disability for ankle OA. In the other report,15 there were no significant differences between IA-HA and placebo on pain reduction and functional outcomes for shoulder OA. Adverse events were considered unrelated to the study products.
These 2 CADTH reports14,15 focused on older populations with degenerative OA. For this report, we focus on adults between the ages of 18 and 55 years. While the average age of diagnosis in Canadian adults is 50 years, many experience symptoms of OA years earlier and nearly 1/3 of people with OA have been diagnosed before the age of 45 years.20 OA is prevalent within specific occupations such as the military, sports, construction, mining, and other types of physical labour due to extreme activities and demands,1,5,21 and joint trauma is increasingly being recognized as a common cause of OA.22 The burden of OA on younger adults is similar to and potentially worse than that on older adults.20 Surgery for OA in patients 55 years and younger is problematic, especially total joint replacement, due to the need for long-term durability and the possibility of multiple revisions.12,22 Therefore, effective conservative treatment options for younger patients are required, but the effectiveness of high MW IA-HA for this patient population has not yet been established.
Objective
To support decision-making about the use of HA for OA in younger adults, we prepared this Rapid Review to summarize and critically appraise the most recent clinical effectiveness studies on high MW IA-HA in adults between the ages of 18 and 55 years with OA of the hip, shoulder, or ankle joints.
Research Question
What is the clinical effectiveness of intra-articular hyaluronic acid for people with osteoarthritis of the hip, glenohumeral, or ankle (i.e., tibiotalar or subtalar) joints?
Methods
Literature Search Methods
An information specialist conducted a literature search on key resources including MEDLINE, Embase, the Cochrane Database of Systematic Reviews, the International HTA Database, the websites of Canadian and major international health technology agencies, and a focused internet search. The search approach was customized to retrieve a limited set of results, balancing comprehensiveness with relevancy. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. Search concepts were developed based on the elements of the research questions and selection criteria. The main search concepts were hyaluronic acid and hip, shoulder, and ankle osteoarthritis. The search was completed on December 12, 2023, and limited to English-language documents published since January 1, 2013.
Selection Criteria and Methods
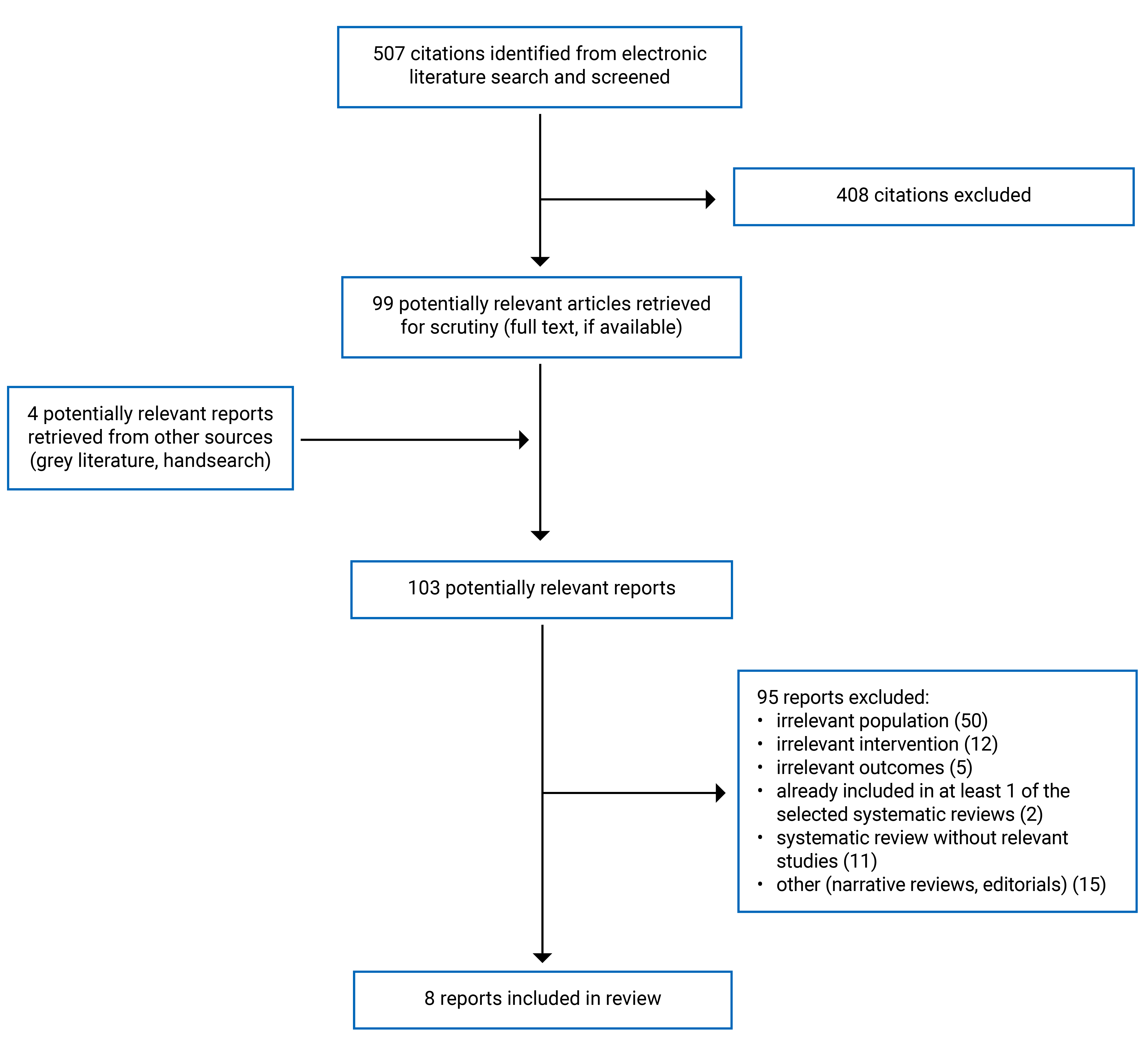
One reviewer screened citations and selected studies. In the first screening level, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. No comparative randomized or nonrandomized studies meeting the selection criteria were identified from the literature search results. Therefore, 1 reviewer re-screened for single-arm studies (i.e., without a relevant comparator group) with before-and-after data published since 2018. Based on the volume of relevant evidence from before-and-after studies published since 2018, literature screening was not extended further.
Several systematic reviews (SRs) with similar eligibility criteria met our inclusion criteria. Still, they did not include any comparative studies that met our inclusion criteria (i.e., SRs with no relevant primary studies). Therefore, 1 recent and comprehensive SR was selected to include in this Rapid Review. The other SRs with no relevant primary studies are listed in Appendix 5.
The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
|---|---|
Population | Adults (between 18 and 55 years of age) with osteoarthritis of the hip, glenohumeral, or ankle (i.e., tibiotalar or subtalar) joints, including posttraumatic arthritis (e.g., due to osteochondral lesions or labral tears) |
Intervention | Intra-articular injection of high molecular weight hyaluronic acid (defined as greater than 3,000 kDa) |
Comparator | No treatment (e.g., placebo, sham interventions, waitlist) |
Outcomes | Clinical benefits (e.g., disease severity, pain, function, disability, quality of life) and harms (e.g., adverse events) |
Study designs | Health technology assessments, systematic reviews, randomized controlled trials, nonrandomized studies |
Exclusion Criteria
The following were excluded:
articles that did not meet the selection criteria outlined in Table 1
duplicate publications
mean or median age of the study population was not within the range of 18 to 55 years; or age of participants was not reported
primary studies that were captured in an included SR. However, if the SR did not describe the primary study in sufficient detail, then the primary study was included rather than the SR
SRs in which all relevant studies were captured in other more recent or more comprehensive SRs.
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the following tools as a guide: A MeaSurement Tool to Assess systematic Reviews 2 (AMSTAR 2)23 for systematic reviews, and the Downs and Black checklist24 for randomized and nonrandomized studies. We assessed only the relevant items in the critical appraisal tools. Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Summary of Evidence
Quantity of Research Available
This report includes 3 SRs with relevant primary studies,26-28 1 SR without relevant studies,25 and 4 nonrandomized open-label before-and-after studies.12,29-31 Study selection details are presented in Appendix 1.
We selected the SR by the National Institute for Health and Care Excellence (NICE)25 to include in our Rapid Review as the most recent, comprehensive, and high-quality SR of comparative studies that met our inclusion criteria but did not include any relevant primary studies. The other SRs that met our selection criteria but with no relevant primary studies are listed in Appendix 5.
Summary of Study Characteristics
Six publications12,25-30 had broader inclusion criteria than the present review:
The NICE SR25 included adult patients (i.e., 16 years and older) with OA affecting any joint and 3 IA interventions (HA, corticosteroids, and stem cell therapy). The review included any MW HA intervention and included placebo-controlled trials.25 However, none of the included studies evaluated the comparison of interest for this report, namely the clinical effectiveness of high MW IA-HA compared to placebo for hip, shoulder, or ankle OA in adults between 18 and 55 years.
The SR by Boffa et al.27 assessed the clinical effectiveness of IA injection treatments (i.e., platelet-rich plasma, methylprednisolone, botulinum toxin type A, mesenchymal stem cells, prolotherapy, and any MW HA) for people with ankle lesions (e.g., osteochondral of the talus and ankle OA) of all ages. Of the 24 studies included in the SR,27 2 studies on high MW HA for ankle OA in the relevant age group met the criteria for this report.
Two SRs26,28 included any MW HA injections for hip OA and did not restrict the population by age group. One study in each SR26,28 was relevant to this report.
The primary study by Kany et al.29 included 273 patients aged 50 years or younger at onset of OA of the shoulder who were treated with high MW HA, platelet-rich plasma, or arthroscopy. Only the 88 patients treated with HA are included and summarized separately in this report.
the primary study by Koyano et al.30 evaluated high MW HA in 29 patients with hip OA. Data were stratified by severity of OA. The 20 patients with severe OA did not meet our criteria for population age (mean 61 years). The 9 patients with mild hip OA did meet our criteria for population age (mean 53 years);30; thus, only data on this group is included in this report.
Additional details regarding the characteristics of included publications are provided in Appendix 2.
Study Design
The NICE SR25 searched multiple databases for comparative studies from inception to November 2021.
The SR by Boffa et al.27 on ankle diseases queried the electronic databases from inception to March 2020. The 2 SRs26,28 on hip OA searched the electronic databases from January 2000 to January 202028 and from inception to April 2020.26 These 3 SRs26-28 included 4 relevant primary studies (single-arm before-and-after studies) published between 2002 and 2008.
The 4 primary studies12,29-31 were observational open-label studies with uncontrolled before-and-after data. Two studies were prospective30,31 and 2 were retrospective designs.12,29
Population
One study reported in 1 SR26 and another study reported in another SR28 included patients with hip OA. The mean age was 55 years in 1 study in 1 SR,26 but not reported in the other SR (though young adults were eligible for this primary study).28 The sample sizes were 2226 and 78.28 Three primary studies12,30,31 identified for this Rapid Review also included patients with hip OA. The severity of OA in these studies ranged from mild30,31 to severe.12 The studies were conducted at a single site each in Australia,31 Italy,12 and Japan.30 Samples sizes ranged from 930 to 87.31 Mean ages ranged from 3312 to 54 years.31
One primary study29 included 88 patients with OA of the shoulder (glenohumeral joint) from multiple centres in France. Patients with posttraumatic OA (fracture sequalae) or OA following rotator cuff tear were excluded. The mean age was 40 years (range 20 to 65).29
Two studies reported in the SR by Boffa et al.27 included patients with ankle OA and mean ages were 41 and 45 years. The sample sizes were 21 and 55.27 The SR27 did not specify whether tibiotalar or subtalar joints were affected.
The 3 SRs26-28 did not report the countries where the relevant primary studies were conducted.
Intervention
Most studies assessed single or multiple high MW (6,000 kDa) injections of 2 mL IA-HA (Hylan G-F 2012,26,28,30 or Synvisc brand27,29). One study assessed a single ultra-high MW (> 100,000 kDa) injection of 3 mL HA (Durolane brand).31
The HA injections were guided by fluoroscopy,26 ultrasound,12,29,31 radioscopy,29 or air arthrogram.30 No imaging guidance was used in the 2 studies included in the SR by Boffa et al.27 The SR by Acuna et al.28 did not report whether imaging was used to guide the HA injection.
Outcomes
Clinical benefits included:
pain, using the visual analogue scale.12,26-28,30 One study also reported the use of nonsteroidal anti-inflammatory drugs or analgesics for pain relief19
physical function, using the Constant score,29 the Japanese Orthopedic Association score,30 and the Subject Shoulder Value.29 One SR27 did not report which tool was used to measure functional impairment
health-related quality of life, using EuroQol 5-Dimension Questionnaire30
composite measures of pain, function, and/or other outcomes including the modified Harris Hip Score,31 the Lequesne index,26,28 and the Western Ontario and McMaster Universities Arthritis Index;12 and other outcomes29
Harms were assessed by adverse events.12,26,27,29-31 Follow-up ranged from 6 weeks to 15 years.29
Brief descriptions of the tools used to measure clinical effectiveness outcomes are presented as footnotes in the Summary of Findings tables in Appendix 4.
Summary of Critical Appraisal
Systematic Reviews
The 4 SRs25-28 provided some description of the inclusion criteria; however, 3 reviews26-28 did not report establishing an a priori method or developing a review protocol. A preestablished review method is important for informing the conduct of reviews and allows readers to assess any protocol deviations that could introduce potential risk of bias to the findings of the review. The authors of the 4 SRs25-28 performed literature searches in 2 or more electronic databases. The NICE SR25 described the search strategies in detail, while the other 3 SRs26-28 provided the search string27 or key search terms.26,28 This increases the transparency and reproducibility of the literature searches and article selection process. All SRs25-28 presented a flow chart illustrating the study selection process. Study selection was performed in duplicate in 3 SRs;25-27 thus, reducing the likelihood that relevant studies were missed.
There were several limitations that were common to the included SRs.25-28 None incorporated searches of the grey literature25-28 and only the NICE review25 searched trial registries. Of the 3 SRs that included relevant studies,26-28 2 SRs,26,28 did not report that data extraction was performed in duplicate, thus, increasing the possibility of errors in data extraction in those 2 SRs.26,28 Two SRs26,28 did not provide a list of excluded studies. One SR28 did not assess risk of bias of included studies or quality of evidence, and another SR26 did not indicate if risk of bias was accounted for in their findings. The clarity of reporting is fundamental to understand the results and assess the validity of the results. However, 1 SR reported only narrative findings per study,27 and another SR28 did not report effect estimates. The statement of conflicts of interest helps readers understand the potential bias of study funders. However, 2 SRs26,27 did not report the funding sources for the relevant studies included in their review. The authors of 2 SRs25,26 received government funding to conduct the reviews, another SR27 did not report whether financial support was received, and 3 authors of another SR28 disclosed ties with pharmaceutical companies.
Primary Studies
The 4 primary studies12,29-31 reported the study objective, inclusion and exclusion criteria, interventions used, and demographics of included participants. Because HA was administered by study personnel, it was assumed that each study's adherence to the intervention was reliable. Outcomes of interest were assessed using validated scales.12,29-31 All 4 studies12,29-31 reported adverse events associated with the intervention.
There were many limitations across the included studies.12,29-31 The 4 studies12,29-31 were open-label with either 1-arm cohort27-29 or without a relevant comparator group.19 Therefore, the risk of confounding is high, and, in the absence of a frame of reference for comparison, we cannot determine how much the intervention, a placebo effect, or the natural history of the disease have contributed to study outcomes. The lack of blinding could result in bias in outcomes favouring the intervention, particularly since most outcomes were based on self-reported measures. All studies12,29-31 had sample sizes less than 89 patients that might not represent the entire population from which they were recruited. In all studies,12,29-31 the outcome data were not adequately described or lacked clarity, which makes interpretation of the results challenging. While 2 studies12,30 declared no conflicts of interest, the authors of another study29 disclosed ties with pharmaceutical companies (consultant or royalties), but not with the manufacturer of the HA (Sanofi) used in their study. One of the authors of the other study31 had previously been on the medical advisory board for Bioventus Global, the manufacturer of the HA assessed in the study.
Additional details regarding the strengths and limitations of the included publications are provided in Appendix 3.
Summary of Findings
The main study findings are presented in Appendix 4.
OA of the Hip
Pain
Two SRs26,28 and 2 primary studies12,30 assessed the effect of HA on pain in adults with hip OA.
The following effects were reported with single injections of high MW IA-HA guided by imaging (fluoroscopy,26 ultrasound,12 or air arthrogram30):
statistically significant decrease from baseline in pain at 1 month (1 study in 1 SR26 and 2 primary studies12,30)
statistically significant decrease from baseline in overall pain at 3 months (1 study26)
no statistically significant difference from baseline in pain at 12 weeks (1 study30)
statistically significant decrease from baseline in pain at 6 months (1 study in 1 SR26).
The following effect was also reported with single injections of high MW IA-HA (imaging guidance NR):
statistically significant decrease from baseline in pain at 1 year (1 study in 1 SR).28
The cohort study by De Lucia et al.12 reported that pain was reduced from baseline at 6 months with multiple ultrasound-guided injections of high MW IA-HA (data presented graphically only, statistical significance not reported). At the 2-year follow-up, pain response differed according to the type of hip OA:
in patients with primary OA, there was a statistically significant decrease from baseline in pain and use of pain medication (nonsteroidal anti-inflammatory drugs or analgesics) at 2 years12
in patients with OA secondary to juvenile idiopathic arthritis, there was no difference from baseline in pain at 2 years (data depicted graphically only, statistical significance not reported).12
Function
One study30 reported no statistically significant difference from baseline in hip joint function with single injection of high MW HA (guided by air arthrogram) at 4 or 12 weeks in patients with mild hip OA.
Health-Related Quality of Life
One study30 reported the following effects on health-related quality of life with a single injection of high MW HA guided by air arthrogram in patients with mild hip OA:
statistically significant increase from baseline at 4 weeks30
no statistically significant difference from baseline at 12 weeks.30
Composite Outcomes
Two SRs26,28 and 2 primary studies12,31 assessed the effect of HA on composite measures of pain, function, and/or other outcomes in adults with hip OA.
The following effects were reported with a single injection of high MW weight IA-HA:
statistically significant and clinically important improvement from baseline in hip pain and joint function at 6 weeks (1 study)31
statistically significant decrease from baseline in pain and disability at 3 and 6 months with fluoroscopy-guided IA-HA (1 study in 1 SR)26
statistically significant decrease from baseline in pain and disability at 1 year (imaging guidance not reported, 1 study in 1 SR)28
The cohort study by De Lucia et al.12 reported that pain, stiffness, and function was improved from baseline at 6 months with multiple ultrasound-guided injections of high MW IA-HA (data presented graphically only, statistical significance not reported). At 2 years, treatment response differed according to type of hip OA:
in patients with primary OA, there was a statistically significant decrease from baseline in pain, stiffness, and function at 2 years12
in patients with OA secondary to juvenile idiopathic arthritis, there was no difference from baseline in pain, stiffness, and functional limitations at 2 years (data depicted graphically only, statistical significance not reported).12
Adverse Events
No severe adverse events were reported in patients with hip OA.30,31 However, there were reports of mild or temporary hip pain in a small proportion of patients (e.g., 5 or fewer patients per study).12,26,31
OA of the Shoulder
One study29 assessed ultrasound or radioscopy-guided injections of high MW IA-HA in adults with shoulder OA.
Function
There was an improvement from baseline of 12 points on functional quality and 14% on shoulder self-assessment at 12 to 182 months follow-up (statistical significance and clinical importance not reported).29
Other Outcomes
Eighty-six percent of patients had no arthroscopy at a minimum 4 years’ follow-up (range 12 to 321 months), indicating treatment success according to study authors.29
Adverse Events
No complications were reported in 88 patients.29
OA of the Ankle
Two studies reported in the SR by Boffa et al.27 studied the effectiveness and safety of unguided high MW HA in adults with OA of the ankle.
Pain
The SR authors27 narratively reported that a single injection of IA-HA was effective at reducing pain from baseline at 6 months (within-group difference and statistical significance not reported, 1 study in 1 SR).27
The SR authors27 narratively reported that 3 weekly injections (1 per week over 3 weeks) of IA-HA provided pain relief from baseline at 18 months (within-group difference and statistical significance not reported, 1 study in 1 SR).27
Function
The SR authors27 narratively reported that 3 injections of IA-HA were effective at providing functional improvement from baseline at 18 months (within-group difference and statistical significance not reported, 1 study in 1 SR).27
Adverse Events
No treatment-related adverse events were reported in 76 patients with OA of the ankle.27
Limitations
Evidence Gaps
We did not identify any clinical effectiveness studies with a relevant comparator group (placebo, wait list, or sham treatment); instead, all identified studies reported a within-group change from baseline (before-and-after treatment). The placebo effect has been demonstrated with therapies for OA.33-35 Without a comparator group, it is not possible to attribute the reported effects to the intervention alone due to potential confounding. With the exception of 1 primary study,31 the minimally important differences on the patient-reported scales were not reported in the evidence; therefore, it is unknown whether the results of pain, function, and composite outcomes were clinically meaningful to patients.
Certainty of the Evidence
Risk of Bias of Included Studies in SRs
Of the 4 included studies in the 3 SRs, 2 studies from 2 of the SRs26,27 were good quality as assessed by the SR authors and 1 study in 1 SR26 was fair quality. One study included in another SR28 was not assessed for risk of bias by the review authors.
Generalizability
None of the primary studies12,29-31 were conducted in Canada, which may limit the generalizability of the findings of this Rapid Review to the Canadian health care context. The 3 SRs with relevant studies26-28 did not identify the countries in which the studies were conducted; therefore, the generalizability (or directness) of their findings is unknown.
Heterogeneity
There was variability in patient populations (e.g., OA diagnosis, disease severity), interventions (e.g., number of injections, method of guidance), and outcomes (e.g., instruments used to assess function and compositive outcomes, end points) across included studies. There was also substantial heterogeneity regarding how adverse events were categorized, reported, and presented.
Imprecision
For each outcome, there were very few events or patients included in the results. All included studies had very small sample sizes, ranging from 930 to 88 patients.29 The evidence also had inadequate or unclear reporting of findings. The effect estimates and/or confidence intervals were not reported for several outcomes.27-31 Thus, the results presented in this Rapid Review are generally imprecise.
Other Biases
While none of the included studies reported direct funding from industry, 1 SR28 and 2 primary studies29,31 disclosed potential conflicts of interest with HA manufacturers. This could potentially lead to publication, performance, or other bias in favour of the intervention.
Conclusions and Implications for Decision- or Policy-Making
This report comprises 4 SRs25-28 and 4 observational before-and-after studies12,29-31 on the clinical effectiveness of high MW IA-HA for adults between 18 and 55 years of age with OA of the hip, shoulder, or ankle joints.
OA of the Hip
In adults with hip OA, compared to baseline, high MW IA-HA may have a favourable effect on pain at 1 month12,26,30 and on pain and disability at 6 months12,26,31 and 1 year28 following treatment. However, these findings are uncertain due to high risk of bias and imprecision. Also, our confidence in the results of the 2 SRs26,28 is very low (based on our assessment using AMSTAR 2).
High MW IA-HA had a neutral effect (e.g., not statistically significant within-group difference) on pain, hip function, and health-related quality of life at 3 months following treatment, but this finding is uncertain due to high risk of bias, imprecision, and indirectness.26,30
High MW IA-HA may have a favourable effect from baseline on pain, stiffness and function at 2 years in patients with primary hip OA, but a neutral effect on these outcomes in patients with OA secondary to juvenile idiopathic arthritis.12 However, these results are uncertain due to high risk of bias, imprecision, and indirectness.12
There were no severe adverse events reported for high MW IA-HA in patients with hip OA.30,31
OA of the Shoulder
While 1 study29 reported improvement in function scores after treatment with high MW IA-HA in patients with shoulder OA, the certainty in the evidence is reduced due to high risk of bias, imprecision, and potential indirectness.29 There were no complications reported with high MW IA-HA in patients with shoulder OA.29
OA of the Ankle
In adults with ankle OA, high MW IA-HA may have a favourable effect from baseline on pain at 6 months and 18 months after treatment and on pain and function at 18 months following treatment, but these findings are uncertain due to imprecision and low confidence in the results of the SR.27 There were no treatment-related adverse events with high MW IA-HA in patients with ankle OA.27
Considerations for Future Research
The evidence in this report was from limited certainty evidence in nonrandomized before-and-after studies. High-quality data from randomized placebo-controlled trials in large populations are needed to conclusively determine the effectiveness and safety of high MW IA-HA in adults between the ages of 18 and 55 years with OA of the hip, shoulder, and ankle. Many SRs were excluded from this report because the authors did not describe the included studies in adequate details. Specifically, the age of the population and/or the HA MW were not described. Future SRs must provide sufficient information about the populations and interventions (e.g., product name, MW, guidance used) of their included studies. While this was a reporting issue, we also suspect that younger adults are a less studied population, as we did find 12 SRs without relevant primary studies.
To help address health equity concerns in future studies, researchers should consider collecting equity-relevant population characteristics (e.g., gender, education, socioeconomic status, place of residence) to assess potential health inequities related to IA-HA treatment for OA. Compared to older adults, adults younger than 45 years with OA report a great proportion of poor mental health.20 Therefore, future research could assess the impact of high MW IA-HA on psychological outcomes.
Implications for Clinical Practice
While there may be improvements in pain and function up to 2 years following high MW IA-HA in younger adults with hip, shoulder, or ankle OA, the evidence is limited in quantity and quality, and we are uncertain whether high MW IA-HA is clinically effective compared to no treatment. Given this uncertainty, health care providers and decision-makers may wish to consider other factors when considering high MW IA-HA as part of an overall treatment approach for their patients with hip, shoulder, or ankle OA. These factors include acceptability by younger adults and clinicians administering the intervention, feasibility of implementing high MW IA-HA in clinical practice, cost of treatment and other resources required, health equity, and patient values and preferences.
References
1.Canada AS. Osteoarthritis. 2023. https://arthritis.ca/about-arthritis/arthritis-types-(a-z)/types/osteoarthritis. Accessed 2024 January 14.
2.Canada PHAo. Osteoarthritis in Canada. 2020. https://www.canada.ca/content/dam/phac-aspc/documents/services/publications/diseases-conditions/osteoarthritis/osteoarthritis-factsheet.pdf. Accessed 2024 January 15.
3.Konstantakos E. What Is a Synovial Joint? 2016: https://www.arthritis-health.com/types/joint-anatomy/what-synovial-joint. Accessed 2024 Jan 30.
4.Wu B, Li YM, Liu YC. Efficacy of intra-articular hyaluronic acid injections in hip osteoarthritis: a meta-analysis of randomized controlled trials. Oncotarget. 2017;8(49):86865-86876. PubMed
5.website To. Osteoarthritis and work. 2024: https://www.arthrolink.com/en/osteoarthritis-folders/all-folders/osteoarthritis-and-work#:~:text=People%20at%20risk%20are%20those%3A%201%20who%20have,spine%20%28such%20as%20with%20construction%20machinery%20and%20lorries%29. Accessed 2024 Jan 30.
6.Sharif B, Kopec J, Bansback N, et al. Projecting the direct cost burden of osteoarthritis in Canada using a microsimulation model. Osteoarthritis and Cartilage. 2015;23(10):1654-1663. PubMed
7.Smedslund G, Kjeken I, Musial F, Sexton J, Osteras N. Interventions for osteoarthritis pain: A systematic review with network meta-analysis of existing Cochrane reviews. Osteoarthritis and Cartilage Open. 2022;4(2) (no pagination).
8.Chandrasekaran S, Lodhia P, Suarez-Ahedo C, Vemula SP, Martin TJ, Domb BG. Symposium: evidence for the use of intra-articular cortisone or hyaluronic acid injection in the hip. Journal of Hip Preservation Surgery. 2016;3(1):5-15. PubMed
9.Familiari F, Ammendolia A, Rupp MC, et al. Efficacy of intra-articular injections of hyaluronic acid in patients with glenohumeral joint osteoarthritis: A systematic review and meta-analysis. Journal of Orthopaedic Research. 2023;41(11):2345-2358. PubMed
10.Brumat P, Kunšič O, Novak S, et al. The surgical treatment of osteoarthritis. Life (Basel). 2022;12(7):982. PubMed
11.Witteveen AG, Hofstad CJ, Kerkhoffs GM. Hyaluronic acid and other conservative treatment options for osteoarthritis of the ankle. Cochrane Database of Systematic Reviews. 2015(10):CD010643. PubMed
12.De Lucia O, Luppino AF, Pregnolato F, et al. Hyaluronic Acid Therapy in Hip OA Does Not Perform Equally in Osteoarthritis Secondary to Juvenile Idiopathic Arthritis When Compared to Primary Osteoarthritis: A 2-Year Preliminary Evaluation. Advances in Therapy. 2022;39(3):1267-1278. PubMed
13.Canada AAo. Arthroscopy Association of Canada (AAC) Position Statement on Intra-Articular Injections for Knee Osteoarthritis. 2022. https://coa-aco.org/wp-content/uploads/2023/03/AAC-Intra-articular-Injections-for-Knee-OA-Updated-August-2020.pdf. Accessed 2024 January 14.
14.Chao Y-S. Intra-Articular Hyaluronic Acid for Osteoarthritis of the Hip or Ankle: A Review of Clinical Effectiveness. 2019. https://www.cadth.ca/sites/default/files/pdf/htis/2019/RC1154%20HA%20for%20Hip%20and%20Ankle%20Final.pdf. Accessed 2023 December 22.
15.Tran K. Intra-Articular Hyaluronic Acid for Viscosupplementation in Osteoarthritis of the Hand, Shoulder, and Temporomandibular Joint: A Review of Clinical Effectiveness and Safety. 2019. https://www.cadth.ca/sites/default/files/pdf/htis/2019/RC1155%20HA%20for%20Viscosupp%20for%20hand%2C%20shoulder%20and%20TMJ%20OA%20Final.pdf. Accessed 2023 December 22.
16.Authority WSHC. Hyaluronic Acid/Viscosupplementation and Platelet Rich Plasma for Knee or Hip Osteoarthritis: Final Evidence Report. 2023. https://www.hca.wa.gov/assets/program/HA-PRP-final-evidence-report.pdf. Accessed 2024 January 15.
17.Zaffagnini M, Boffa A, Andriolo L, Raggi F, Zaffagnini S, Filardo G. Orthobiologic Injections for the Treatment of Hip Osteoarthritis: A Systematic Review. Journal of Clinical Medicine. 2022;11(22) (no pagination).
18.Tran K. Intra-Articular Hyaluronic Acid for Viscosupplementation in Osteoarthritis of the Knee: A Review of Clinical Effectiveness and Safety. 2019. https://www.cadth.ca/sites/default/files/pdf/htis/2019/RC1136%20HA%20for%20Viscosupp%20for%20Knee%20OA%20Final.pdf. Accessed 2023 December 22.
19.Altman RD, Bedi A, Karlsson J, Sancheti P, Schemitsch E. Product differences in intra-articular hyaluronic acids for osteoarthritis of the knee. The American journal of sports medicine. 2016;44(8):2158-2165. PubMed
20.Badley EM WJ, Zahid S, and Perruccio AV. Burden Of Osteoarthritis In Canada. 2021: https://arthritis.ca/getmedia/36cbffb1-f1d3-4689-8cad-39ef47954840/OAReportSummary_EN.pdf. Accessed 2024 January 12.
21.Langworthy MJ, Nelson F, Owens BD. Viscosupplementation for treating osteoarthritis in the military population. Military Medicine. 2014;179(8):815-820. PubMed
22.Migliore A, Bizzi E, Massafra U, et al. Viscosupplementation: a suitable option for hip osteoarthritis in young adults. Eur Rev Med Pharmacol Sci. 2009;13(6):465-472. PubMed
23.Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. PubMed
24.Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377-384. PubMed
25.Excellence NIfHaC. Osteoarthritis: assessment and management (update) Evidence reviews for the clinical and cost effectiveness of intra-articular injections for the management of osteoarthritis [draft for consultation]. 2022: https://www.nice.org.uk/guidance/ng226/documents/evidence-review-12. Accessed 2024 January 2.
26.Wu YZ, Huang HT, Ho CJ, et al. Molecular Weight of Hyaluronic Acid Has Major Influence on Its Efficacy and Safety for Viscosupplementation in Hip Osteoarthritis: A Systematic Review and Meta-Analysis. Cartilage. 2021;13(1_suppl):169S-184S. PubMed
27.Boffa A, Previtali D, Di Laura Frattura G, Vannini F, Candrian C, Filardo G. Evidence on ankle injections for osteochondral lesions and osteoarthritis: a systematic review and meta-analysis. International Orthopaedics. 2021;45(2):509-523. PubMed
28.Acuna AJ, Samuel LT, Jeong SH, Emara AK, Kamath AF. Viscosupplementation for hip osteoarthritis: Does systematic review of patient-reported outcome measures support use? Journal of Orthopaedics. 2020;21:137-149. PubMed
29.Kany J, Benkalfate T, Favard L, et al. Osteoarthritis of the shoulder in under-50 year-olds: A multicenter retrospective study of 273 shoulders by the French Society for Shoulder and Elbow (SOFEC). Orthop Traumatol Surg Res. 2021;107(1):102756. PubMed
30.Koyano G, Jinno T, Koga D, Hoshino C, Okawa A. Intra-articular Injections of Cross-linked Hyaluronic Acid in Japanese Patients with Symptomatic Osteoarthritis of the Hip. Prog. 2021;6:20210038. PubMed
31.Long DM, Fitzpatrick J. Safety and efficacy of a single intra-articular injection of hyaluronic acid in osteoarthritis of the hip: a case series of 87 patients. BMC Musculoskeletal Disorders. 2021;22(1):797. PubMed
32.Zhu JB, Lim AJC, McCaskie AW, Khanduja V. Viscosupplementation is Effective for the Treatment of Osteoarthritis in the Hip. A Systematic Review. Arthroscopy. 2023;22:22. PubMed
33.Yu SP, van Middelkoop M, Deveza LA, et al. Predictors of Placebo Response to Local (Intra-Articular) Therapy In Osteoarthritis: An Individual Participant Data Meta-Analysis. Arthritis Care Res (Hoboken). 2023;31:31. PubMed
34.Doherty M, Dieppe P. The “placebo” response in osteoarthritis and its implications for clinical practice. Osteoarthritis and cartilage. 2009;17(10):1255-1262. PubMed
35.Zhang W, Robertson J, Jones AC, Dieppe PA, Doherty M. The placebo effect and its determinants in osteoarthritis–meta-analysis of randomised controlled trials. Annals of the rheumatic diseases. 2008.
36.Kellgren JH, Lawrence J. Radiological assessment of osteo-arthrosis. Annals of the rheumatic diseases. 1957;16(4):494. PubMed
37.Constant C. An evaluation of the Constant-Murley shoulder assessment. The Journal of Bone and Joint Surgery British Volume. 1997;79(4):695-696. PubMed
38.Gilbart MK, Gerber C. Comparison of the subjective shoulder value and the Constant score. Journal of shoulder and elbow surgery. 2007;16(6):717-721. PubMed
39.Wakabayashi H, Hasegawa M, Yoshida K, Nishioka K, Sudo A. Hip score and disease activity correlation in patients with rheumatoid arthritis after total hip arthroplasty. International orthopaedics. 2013;37:1245-1250. PubMed
40.EUROQOL G. EuroQol-A new facility for the measurement of health-related quality of life. Health Policy. 1990;16:199-208. PubMed
41.Dawson J, Linsell L, Doll H, et al. Assessment of the Lequesne index of severity for osteoarthritis of the hip in an elderly population. Osteoarthritis and cartilage. 2005;13(10):854-860. PubMed
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Table 2: Characteristics of Included Systematic Reviews
Study citation, country, funding source | Review objective, search dates, numbers of primary studies included | Population characteristics | Relevant intervention(s) and comparator(s) | Relevant clinical outcomes, length of follow-up |
|---|---|---|---|---|
NICE (2022)25 England Funding source: NICE | Review objective: To evaluate the clinical and cost-effectiveness of IA injections of corticosteroids, HA, and stem cell therapy for the management of OA. Search dates: Electronic database inception to November 2021. Number of included studies:
| Adults (age ≥ 16 years) with OA affecting any joint N = 0 | Intervention: IA-HA (of any formulation) Comparator: Placebo | NA |
Boffa et al. (2021)27 Italy Funding source: NR | Review objective: To evaluate the safety and quantify the evidence supporting the effectiveness of the different injective options for the treatment of ankle lesions ranging from OLT to OA. Search dates: Electronic database inception to March 2020. Number of included studies:
| Patients with ankle OA N = 21 to 55 Sex: female 38% to 40%, male 60% to 62% Age: mean 41.0 to 45.0 years Symptom duration: mean 2.7 to 25.0 years | Intervention: 1 or 3 injections of 2 mL Synvisc (6,000 kDa), no guidance Comparator: Before treatment | Outcomes Pain: VAS Function Adverse events Follow-up: 6 to 18 months |
Wu et al. (2021)26 Taiwan Source of funding: Kaohsiung Medical University Hospital | Review objective: To make clear the role of MW in clinical therapeutic effects on hip OA. Search dates: Electronic database inception to April 2020. Number of included studies:
| Patients with hip OA (K-L gradesa 1 to 3) N = 22 Sex: female 59%, male 41% Age: mean 54.7 years | Intervention: 2mL HMW HA (Hylan G-F 20) once at baseline, and second injection at 30, 60, or 90 days if clinically necessary; fluoroscopy-guided Comparator: Before treatment | Outcomes Pain: VAS Composite outcome: Lequesne index (pain, discomfort, function) Adverse events Follow-up: 6 months |
Acuna et al. (2020)28 US Source of funding: No funding | Review objective: To determine how hyaluronic acid administration impacts patient-reported outcome measures and rates of conversion to total hip arthroplasty. Search dates: January 2000 to January 2020 Number of included studies:
| Young adultsb with hip OA (K-L gradesa 1 to 4) N = 78 Sex: NR Age: NRb | Intervention: Single injection of HMW HA (Hylan G-F 20), guidance NR Comparator: Before treatment | Outcomes Pain: VAS Composite outcome: Lequesne index (pain, discomfort, function) Follow-up: 1 year |
HA = hyaluronic acid; HMW = high molecular weight; IA = intra-articular; K-L = Kellgren-Lawrence; NA = not applicable; NR = not reported; OA = osteoarthritis; NRS = nonrandomized studies; OLT = osteochondral lesions of the talus; RCT = randomized controlled trial; SR = systematic review; VAS = visual analogue scale.
aThe K-L classification grades radiographic abnormalities at the tibiofemoral joint as: grade 0 = no radiographic abnormalities; grade 1 = doubtful joint space narrowing with possible osteophyte formation; grade 2 = possible joint space narrowing with definite osteophyte formation; grade 3 = definite joint space narrowing, moderate osteophyte formation, some sclerosis, and possible deformity of bone ends; grade 4 = severe joint space narrowing, large osteophyte formation, marked sclerosis, and definite deformity of bone ends.36
bWe checked the primary study publication22 to confirm that the study met our selection criteria. Young adults were defined as younger than 40 years of age (mean 36.82, range 26 to 40).22
Note that this table has not been copy-edited.
Table 3: Characteristics of Included Primary Clinical Studies
Study citation, country, funding source | Study design, setting | Population characteristics | Relevant intervention | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
De Lucia et al. (2022)12 Italy Source of funding: No funding | Retrospective open-label cohort study 1 rheumatology unit | Patients aged 18 to 50 years, with symptomatic hip OA according to ACR criteria, radiological OA (K-L gradesa 2 to 4) assessed by standard hip X-rays, and hip pain duration ≥ 1 year. N = 40 patients Primary OA: n = 26 OA secondary to JIA: n = 14 Sex, % female: Primary OA: 26.9 OA secondary to JIA: 64.3 Age, mean years (SD): Primary OA: 41.7 (6.8) OA secondary to JIA: 32.5 (10.1) Hip pain duration, mean years (SD): Primary OA: 3.4 (4.2) OA secondary to JIA: 11.9 (9.4) | Ultrasound-guided IA injections 2ml Hylan GF-20 (1 every month for 3 months, and every 6 months for 2 years). | Outcomes Pain:
Composite: WOMAC (pain, stiffness, function) Adverse events Follow-up: 2 years |
Kany et al. (2021)29 France Funding source: Ramsay Generale De Sante | Retrospective open-label cohort study 13 specialized shoulder centres | Patients aged ≤ 50 years at diagnosis; treated for primary OA of the shoulder, post-instability OA, operated on or not, or other cause of OA (except not posttraumatic OA). N = 88 patients Sex: male 72% Primary OA: 56% Post-instability OA: 44% Age at treatment: mean 40 years, range 20 to 65 years | Ultrasound or radioscopy-guided viscosupplementation with 3 2 mL injections or 6 mL reticulated HA (Synvisc). | Outcomes Function:
Adverse events Follow-up: 12 to 182 monthsb |
Koyano et al. (2021)30 Japan Funding source: NR | Prospective open-label single-arm trial (case seriesc) 1 hospital | Relevant population: Outpatients diagnosed with mild OA (pre and initial OA, K-L gradesa 0 to 2) of the hip joint by plain radiographs, who can walk, and aged > 20 years of age. N = 9 patients Sex: female 89%, male 11% Age: mean 52.7 years, SD 12.0 years | Single IA preparation of 2 mL of Hylan G-F 20 (6,000 kDa) after confirmation of needle position using air arthrogram. | Outcomes Pain:
Function: JOA HRQoL: EQ-5D Adverse events Follow-up: 12 weeks |
Long and Fitzpatrick (2021)31 Australia Funding source: No funding | Prospective open-label single-arm trial (case seriesc) 1 private clinic | Patients aged > 18 years old, presenting with symptomatic mild to moderate hip joint OA (K-L gradesa 2 to 3 as determined by radiologist). N = 87 patients Sex: female 56.3%, male 43.7% Age: mean 54.0 years, SD 10.8 (range 26 to 82) years | Single injection of HA (Durolane; 3 mL preparation) with patient supine-using aseptic technique under ultrasound guidance. | Outcomes Composite: mHHS (pain, function) Adverse events Follow-up: 6 weeks |
ACR = American College of Rheumatology; HA = hyaluronic acid; HRQoL = health-related quality of life; IA = intra-articular; JOA = Japanese Orthopedic Association; JIA = juvenile idiopathic arthritis; K-L = Kellegren-Lawrence; mHHS = modified Harris Hip Score; NR = not reported; OA = osteoarthritis; RCT = randomized controlled trial; SD = standard deviation; SSV = subjective shoulder value; VAS-G = visual analogue scale – gait; VAS-R = visual analogue scale – rest; WOMAC = Western Ontario and McMaster Universities Arthritis Index.
aThe K-L classification grades radiographic abnormalities at the tibiofemoral joint as: grade 0 = no radiographic abnormalities; grade 1 = doubtful joint space narrowing with possible osteophyte formation; grade 2 = possible joint space narrowing with definite osteophyte formation; grade 3 = definite joint space narrowing, moderate osteophyte formation, some sclerosis, and possible deformity of bone ends; grade 4 = severe joint space narrowing, large osteophyte formation, marked sclerosis, and definite deformity of bone ends.36
bThe mean follow-up was unclear; the mean was reported as 96 months in the text but 61.2 months in Table 2.29
cThe authors described the design of their study as case series.30,31
Note that this table has not been copy-edited.
Appendix 3: Critical Appraisal of Included Publications
Note that this appendix has not been copy-edited.
Table 4: Strengths and Limitations of Systematic Reviews Using AMSTAR 223
Strengths | Limitations |
|---|---|
NICE (2022)25 | |
|
|
Boffa et al. (2021)27 | |
|
|
Wu et al. (2021)26 | |
|
|
Acuna et al. (2020)28 | |
|
|
AMSTAR 2 = A MeaSurement Tool to Assess systematic Reviews 2; NICE = National Institute for Health and Care Excellence; RCT = randomized controlled trial; SR = systematic review.
Table 5: Strengths and Limitations of Clinical Studies Using the Downs and Black Checklist24
Strengths | Limitations |
|---|---|
De Lucia et al. (2022)12 | |
Reporting
Internal validity
| Reporting
External validity
Internal validity:
Power:
|
Kany et al. (2021)29 | |
Reporting
Internal validity
| Reporting
External validity
Internal validity
Power
|
Koyano et al. (2021)30 | |
Reporting
Internal validity:
| Reporting
External validity
Internal validity
Power
|
Long and Fitzpatrick (2021)31 | |
Reporting
Internal validity
| Reporting
External validity
Internal validity
Power
|
SES = socioeconomic background.
Appendix 4: Main Study Findings
Table 6: Summary of Findings by Outcome — Pain
Citation, population | Study design | Outcome | Primary study or subgroup | Outcome result | P value | ||
|---|---|---|---|---|---|---|---|
Baseline (pre-injection) | Follow-up (post-injection) | Effect estimate (95% CI) | |||||
Boffa et al. (2021)27 Ankle OA | SR (2 cohort studies) | VASa scores at 6 months compared to baseline (n = 55) | Witteveen 2008 | HA was effective | |||
VASa scores at 12 months, mean (95% CI) (n = 21) | Luciani 2008 | NR | 2.0 (0.58 to 3.42) | HA provided pain relief and effect lasted until 18-month follow-up | |||
Wu et al. (2021)26 Mild to moderate hip OA | SR (1 cohort study) | VASa scores at baseline and 1 month, mean (SD) | Brocq 2002 | 5.54 (1.49) n = 22 | 3.07 (2.22) n = 22 | MD 2.47 (1.35 to 3.59) | NR |
VASa scores at baseline and 3 months, mean (SD) | 3.04 (2.22) n = 17 | MD 2.50 (1.27 to 3.73) | NR | ||||
VASa scores at baseline and 6 months, mean (SD) | 2.47 (1.71) n = 11 | MD 3.07 (1.88 to 4.26) | NR | ||||
Acuna et al. (2020)28 Mild to severe hip OA | SR (1 cohort study) | VASa scores at baseline and 12 months (n = 78), mean | Migliore 2009 | 6.0 | 3.63 | NR | < 0.0005 |
De Lucia et al. (2022)12 Hip OA | Cohort study | VASa scores at 1 month compared to baseline (n = 40) | All OA | NR | NR | Adjustedb difference −18.9 (−27.8 to −10.0) | < 0.0001 |
VASa scores at 12 months compared to 6 months (n = 26) | Primary OA | NR | NR | Adjustedb difference −18.4 (−27.6 to −9.2) | 0.0001 | ||
VASa scores at 12 months compared to 6 months (n = 14) | Secondary OA | NR | NR | Adjustedb difference 1.3 (−11.5 to 14.1) | NR | ||
VASa scores at 24 months compared to baseline (n = 26) | Primary OA | NR | NR | Adjustedb difference −38.1 (−47.6 to −28.7) | < 0.0001 | ||
NSAIDs or analgesics at 24 months compared to baseline (n = 26), days per month | Primary OA | NR | NR | MD −2.7 (0.3 to 5.1) | 0.031 | ||
Koyano et al. (2021)30 Mild hip OA | Single-arm trial | VAS-Ga scores at 4 weeks compared to baseline (n = 9) | NA | VAS-G significantly improved | < 0.050 | ||
VAS-Ga scores at 12 weeks compared to baseline (n = 9) | NR | NSS | |||||
VAS-Ra scores at 4 weeks compared to baseline (n = 9) | VAS-R significantly improved | < 0.050 | |||||
VAS-Ra scores at 12 weeks compared to baseline (n = 9) | NR | NSS | |||||
BMI = body mass index; MD = mean difference; NA = not applicable; NR = not reported; NSS = not statistically significant; OA = osteoarthritis; SD = standard deviation; VAS-G = visual analogue scale – gait; VAS-R = visual analogue scale – rest.
aThe VAS is a continuous scale with a line of fixed length of 10 cm26 or 100 mm12,30 for measuring severity of pain. The left end of the line (0 cm or 0 mm) is anchored with “no pain” and the right end (100 cm or 100 mm) is anchored with “the worst pain imaginable.”26 The VAS-G is used to assess pain during gait and the VAS-R is used to assess pain at rest.30
bAdjusted for BMI and radiological grade.12
Note that this table has not been copy-edited.
Table 7: Summary of Findings by Outcome — Function
Citation, population | Study design | Outcome | Primary study | Outcome result | Effect estimate (95% CI) | P value | |
|---|---|---|---|---|---|---|---|
Baseline (pre-injection) | Follow-up (post-injection) | ||||||
Boffa et al. (2021)27 Ankle OA | SR (2 cohort studies) | Function (measure NR) at 18 months (n = 21) | Luciani 2008 | HA provided functional improvements | |||
Kany et al. (2021)29 Shoulder OA | Cohort study | Constant scorea at baseline and follow-upb (n = 88), mean (range) | NA | 50 (20 to 76) | 62 (25 to 95) | Difference 12 points | NR |
SSVc at baseline and follow-upb (n = 88), mean (range) | 51% (20 to 80) | 65% (20 to 100) | Difference 14% | NR | |||
Koyano et al. (2021)30 Mild hip OA | Single-arm trial | JOAd scores at baseline and 4 weeks (n = 9), mean (SD) | NA | 75.1 (17.7) | 81.2 (10.9) | NR | 1.0 |
JOAd scores at baseline and 12 weeks (n = 9), mean (SD) | 78.2 (12.8) | NR | 0.837 | ||||
JOA = Japanese Orthopedic Association; HA =; MD = mean difference; NA = not applicable; NR = not reported; OA = osteoarthritis; SD = standard deviation; SSV = subjective shoulder value.
aThe Constant score measures functionality after the treatment of a shoulder injury. The test is divided into 4 subscales: pain (15 points), activities of daily living (20 points), strength (25 points) and mobility (forward elevation, external rotation, abduction, and internal rotation of the shoulder, 40 points). A higher score indicates higher quality of function.37
bThe mean follow-up was unclear; the mean was reported as 96 months in the text but 61.2 months in Table 2, The range of follow-up was reported as 12 to 182 months in Table 2.29
cThe SSV is a patient's subjective shoulder assessment expressed as a percentage of an entirely normal shoulder, which would score 100%.38
dThe JOA was used to assess hip joint function in 4 subcategories: pain, range of motion, ability to walk, and activities of daily living.30 A higher score indicates better hip function.39
Note that this table has not been copy-edited.
Table 8: Summary of Findings by Outcome: Health-Related Quality of Life
Citation, population | Study design | Outcome | Outcome result | Effect estimate | P value | |
|---|---|---|---|---|---|---|
Baseline (pre-injection) | Follow-up (post-injection) | |||||
Koyano et al. (2021)30 Mild hip OA | Single-arm trial | EQ-5Da scores at baseline and 4 weeks (n = 9), mean (SD) | 0.60 (0.12) | 0.72 (0.14) | NR | 0.010 |
EQ-5Da scores at baseline and 12 weeks (n = 9), mean (SD) | 0.60 (0.12) | 0.68 (0.15) | NR | 0.234 | ||
EQ-5D = EuroQol 5-Dimension Questionnaire; NR = not reported; OA = osteoarthritis; SD = standard deviation.
aThe EQ-5D assesses health-related quality of life in 5 dimensions (mobility, pain, self-care, usual activities, and anxiety depression). A higher score indicates greater problems.40
Note that this table has not been copy-edited.
Table 9: Summary of Findings by Outcome: Composite and Other Outcomes
Citation, population | Study design | Outcome | Primary study or subgroup | Outcome result | P value | ||
|---|---|---|---|---|---|---|---|
Baseline (pre-injection) | Follow-up (post-injection) | Effect estimate (95% CI) | |||||
Wu et al. (2021)26 Mild to moderate hip OA | SR (1 cohort study) | Lequesne indexa scores at baseline and 3 months, mean (SD) | Brocq 2002 | 11.6 (4.1) n = 22 | 5.7 (4.2) n = 17 | MD 5.90 (95% CI 3.27 to 8.53) | NR |
Lequesne indexa scores at baseline and 6 months, mean (SD) | 5.6 (3.9) n = 11 | MD 6.00 (95% CI 3.13 to 8.87) | NR | ||||
Acuna et al. (2020)28 Mild to severe hip OA | SR (1 cohort study) | Lequesne indexa scores at baseline and 12 months (n = 78), mean | Migliore 2009 | 7.84 | 4.12 | NR | < 0.0005 |
De Lucia et al. (2022)12 Hip OA | Cohort study | WOMACb scores at 1 month compared to baseline (n = 40) | All OA | NR | NR | Adjustedc difference −16.6 (−25.0 to −8.2) | 0.0001 |
WOMACb scores at 12 months compared to 6 months (n = 26) | Primary OA | NR | NR | Adjustedc difference −7.5 (−16.2 to 1.2) | 0.091 | ||
WOMACb scores at 12 months compared to 6 months (n = 14) | Secondary OA | NR | NR | Adjustedc difference 6.2 (−5.93 to 18.3) | NR | ||
WOMACb scores at 24 months compared to baseline (n = 26) | Primary OA | NR | NR | Adjustedc difference - 31.6 (- 40.5 to - 22.7) | < 0.0001 | ||
Kany et al. (2021)29 Shoulder OA | Cohort study | No arthroscopy at minimum 4 years (treatment success), n/N (%) | NA | NA | 76/88 (86.3) | NA | NA |
No arthroscopy at last follow-upd, n/N (%) | NA | 53/88 (60) | NA | NA | |||
Long and Fitzpatrick (2021)31 Mild to moderate hip OA | Single-arm trial | mHHSe scores at baseline and 6 weeks, mean (SD) | NA | 58.47 (14.82) n = 87 | 71.30 (16.46) n = 82 | Difference 12.83f | < 0.01 |
BMI = body mass index; MD = mean difference; mHHS = modified Harris Hip Score; MRAW = raw means; NA = not applicable; NR = not reported; NSS = not statistically significant; OA = osteoarthritis; SD = standard deviation; VAS-G = visual analogue scale – gait; VAS-R = visual analogue scale – rest; WOMAC = Western Ontario and McMaster Universities Arthritis Index.
aThe Lequesne index consists of 11 items assessing pain and discomfort and functional status (including maximal walking distance, and ability for daily activity). Scoring of each item ranges from 0 (no discomfort, no disability) to 8 (maximum pain, maximum disability), and the maximum total score is 24.26,41
bThe WOMAC is a Likert-type instrument that assess the 3 domains of pain, stiffness, and joint function. A higher score indicates greater pain, stiffness, and functional limitations.12
cAdjusted for BMI and radiological grade.12
dThe mean follow-up was unclear; the mean was reported as 96 months in the text but 61.2 months in Table 2, The range of follow-up was reported as 12 to 182 months in Table 2.29
eThe mHHS is a self-report instrument to measure hip pain and function. A higher score indicates less disability.31
fThe effect was greater than the minimally clinically important difference of 10 for clinical improvement at 6 weeks.31
Note that this table has not been copy-edited.
Table 10: Summary of Findings by Outcome: Adverse Events
Citation, population | Study design | Outcome | Primary study or subgroup | Outcome result |
|---|---|---|---|---|
Boffa et al. (2021)27 Ankle OA | SR (2 cohort studies) | Severe AEs related to treatment, n of N | Luciani 2008 | 0 of 21 |
Witteveen 2008 | 0 of 55a | |||
Wu et al. (2021)26 Mild to moderate hip OA | SR (1 cohort study) | Systemic AEs, n of N (%) | Brocq 2002 | 1 of 22 (4.5) Aseptic arthritis with fever up to 38.5°C |
Local AEs, n of N (%) | 2 of 22 (9.1) Local transient pain | |||
De Lucia et al. (2022)12 Hip OA | Cohort study | Withdrawal due to temporary hip pain, n of N | Primary OA | 1 of 26 |
Secondary OA | 0 of 14 | |||
Kany et al. (2021)29 Shoulder OA | Cohort study | Complications, n of N | NA | 0 of 88 |
Koyano et al. (2021)30 Mild hip OA | Single-arm trial | Systemic AEs or serious local complications (e.g., hematoma, femoral nerve injury, infection, air embolism), n of N | NA | 0 of 9 |
Long and Fitzpatrick (2021)31 Mild to moderate hip OA | Single-arm trial | Treatment-related significant AEs, n of N | NA | 0 of 87 |
Infection, n of N | 0 of 87 | |||
Moderate pain (lasting > 24 hours or requiring stronger analgesia), n of N | 0 of 87 | |||
Mild pain (lasting < 24 hours or requiring no treatment or minimal analgesia), n of N | 5 of 87 |
AE = adverse events; NA = not applicable; OA = osteoarthritis.
aOne occurrence of osteochondritis dissecans was reported 4 months after HA injection, but this event was not considered to be treatment-related.27
Note that this table has not been copy-edited.
Appendix 5: References of Potential Interest
Note that this appendix has not been copy-edited.
Previous CADTH Reports
Intra-Articular Hyaluronic Acid for Osteoarthritis of the Hip or Ankle: A Review of Clinical Effectiveness. 2019. https://www.cadth.ca/sites/default/files/pdf/htis/2019/RC1154%20HA%20for%20Hip%20and%20Ankle%20Final.pdf Accessed 22 December 2023.
Intra-Articular Hyaluronic Acid for Viscosupplementation in Osteoarthritis of the Hand, Shoulder, and Temporomandibular Joint: A Review of Clinical Effectiveness and Safety. 2019. https://www.cadth.ca/sites/default/files/pdf/htis/2019/RC1155%20HA%20for%20Viscosupp%20for%20hand%2C%20shoulder%20and%20TMJ%20OA%20Final.pdf Accessed 22 December 2023.
Intra-Articular Hyaluronic Acid for Viscosupplementation in Osteoarthritis of the Knee: A Review of Clinical Effectiveness and Safety. 2019. https://www.cadth.ca/sites/default/files/pdf/htis/2019/RC1136%20HA%20for%20Viscosupp%20for%20Knee%20OA%20Final.pdf Accessed 22 December 2023.
Systematic Reviews
No Relevant Primary Studies
Familiari F, Ammendolia A, Rupp MC, et al. Efficacy of intra-articular injections of hyaluronic acid in patients with glenohumeral joint osteoarthritis: A systematic review and meta-analysis. Journal of Orthopaedic Research. 2023. 41:2345-2358. PubMed
Paget LDA, Mokkenstorm MJ, Tol JL, Kerkhoffs G, Reurink G. What Is the Efficacy of Intra-articular Injections in the Treatment of Ankle Osteoarthritis? A Systematic Review. Clin Orthop. 2023. 481:1813-1824. PubMed
Sambe HG, Yasir M, Man RK, et al. Comparing Intra-articular Platelet-Rich Plasma With Hyaluronic Acid for the Treatment of Hip Osteoarthritis: A Systematic Review and Meta-Analysis. Cureus. 2023. 15:e47919. PubMed
Washington State Health Care Authority. Hyaluronic Acid/Viscosupplementation and Platelet Rich Plasma for Knee or Hip Osteoarthritis; 2023. https://www.hca.wa.gov/assets/program/HA-PRP-final-evidence-report.pdf Accessed 22 December 2023.
Ebad Ali SM, Farooqui SF, Sahito B, Ali M, Khan AA, Naeem O. Clinical Outcomes Of Intra-Articular High Molecular Weight Hyaluronic Acid Injection For Hip Osteoarthritis- A Systematic Review And Meta-Analysis. J Ayub Med Coll Abbottabad. 2021. 33:315-321. PubMed
Ministry of Health Malaysia. Intra-articular Injection of Hyaluronic Acid combined with Sorbitol / Mannitol for Osteoarthritis; 2021. https://www.moh.gov.my/index.php/database_stores/attach_download/347/383 Accessed 22 December 2023.
Liao YY, Lin T, Zhu HX, Shi MM, Yan SG. Intra-Articular Viscosupplementation for Patients with Hip Osteoarthritis: A Meta-Analysis and Systematic Review. Medical Science Monitor. 2019. 25:6436-6445. PubMed
Leite VF, Daud Amadera JE, Buehler AM. Viscosupplementation for Hip Osteoarthritis: A Systematic Review and Meta-Analysis of the Efficacy on Pain and Disability, and the Occurrence of Adverse Events. Arch Phys Med Rehabil. 2018. 99:574-583.e1. PubMed
Vannabouathong C, Del Fabbro G, Sales B, et al. Intra-articular Injections in the Treatment of Symptoms from Ankle Arthritis: A Systematic Review. Foot Ankle Int. 2018. 39:1141-1150. PubMed
Wu B, Li YM, Liu YC. Efficacy of intra-articular hyaluronic acid injections in hip osteoarthritis: a meta-analysis of randomized controlled trials. Oncotarget. 2017. 8:86865-86876. PubMed
Witteveen AG, Hofstad CJ, Kerkhoffs GM. Hyaluronic acid and other conservative treatment options for osteoarthritis of the ankle. Cochrane Database of Systematic Reviews. 2015. CD010643. PubMed
Relevant Studies Included in at Least 1 Selected Systematic Review
Zhu JB, Lim AJC, McCaskie AW, Khanduja V. Viscosupplementation is Effective for the Treatment of Osteoarthritis in the Hip. A Systematic Review. Arthroscopy. 2023. 22:22. PubMed
Papalia R, Albo E, Russo F, et al. The use of hyaluronic acid in the treatment of ankle osteoarthritis: a review of the evidence. J Biol Regul Homeost Agents. 2017. 31:91-102. PubMed
Contributors: Elizabeth Carson, Calvin Young
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for noncommercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca