CADTH Health Technology Review
Oral Ketorolac for Renal Colic in Outpatient Settings
Rapid Review
Authors: Chantelle C. Lachance, Quenby Mahood
Key Messages
What Is the Issue?
Renal colic is a common problem that is primarily caused by kidney stones. Renal colic, specifically kidney stones, can be a recurrent condition that can negatively impact a person’s quality of life and health system utilization.
Ketorolac through IV or intramuscular routes is a common nonsteroidal anti-inflammatory drug (NSAID) used in hospital to treat renal colic. Oral ketorolac for the management of renal colic may reduce patients’ need for opioids after discharge but it is unclear if it is clinically effective when compared to alternative analgesics or whether it is recommended for use in the management of people with renal colic.
What Did We Do?
To inform decisions about oral ketorolac for the management of outpatients with renal colic, we sought to identify and summarize literature comparing the clinical effectiveness of oral ketorolac and alternative analgesics. We also searched for evidence-based guidelines that provide recommendations about the use of oral ketorolac for the management of people with renal colic.
A research information specialist conducted literature searches of peer-reviewed and grey literature sources published between January 1, 2013, and December 4, 2023. The search was limited to English-language documents. One reviewer screened articles for inclusion based on predefined criteria.
What Did We Find?
The tailored search for this rapid review did not find any studies evaluating the clinical effectiveness of oral ketorolac versus alternative analgesics for the management of people with renal colic in outpatient settings that met our criteria for this review. There is therefore no specific evidence available on the efficacy oral ketorolac in the management of renal colic in the community setting in this review.
We did not find any eligible evidence-based guidelines concerning the use of oral ketorolac for the management of people with renal colic in outpatient settings. NSAIDs have been generally mentioned as an option for renal colic in the available guidance.
Research regarding ketorolac for renal colic published since 2013 has focused on IV or intramuscular administration. Research regarding oral ketorolac focused on indications other than renal colic (e.g., postoperative pain) may be of interest; these are listed in the appendix. These studies suggest the effectiveness of ketorolac for pain management for other indications, such as pain management following endoscopy.
What Does It Mean?
Without comparative evidence, decision-makers may want to consider how oral ketorolac is used for related indications (e.g., procedures for removing kidney stones, ureteroscopies) to examine how it performed compared with alternative analgesics.
Research focused on the management of renal colic is needed to evaluate the clinical effectiveness of oral ketorolac and inform guidance concerning oral ketorolac in outpatient settings.
Research Questions
What is the clinical effectiveness of oral ketorolac for the management of people with renal colic in outpatient settings?
What are the evidence-based guidelines regarding the use of oral ketorolac for the management of people with renal colic in outpatient settings?
Context and Policy Issues
What Is Renal Colic?
Renal colic is described as a severe form of flank pain that is often caused by an acute obstruction from a stone in the urinary system.1 Renal colic is mainly caused by nephrolithiasis (kidney stones).1 In North America and Europe, kidney stones affect 5% to 15% of the population at some point (i.e., lifetime prevalence) with a yearly incidence of 0.5%.1 Kidney stones are more common for some individuals; for example, the prevalence of kidney stones among males is nearly double that of females.2 Kidney stones can be a recurrent condition that has a significant impact on health system utilization as well as the individual’s quality of life.2-4 Aside from kidney stones, renal colic may also be caused by other issues such as ureteral spasms after stent removal or after ureteroscopy.1
What Is the Current Practice?
To ascertain the cause of renal colic, diagnosis is usually determined through a patient’s history, physical exam, laboratory testing (e.g., blood and urine test), and imaging studies (e.g., ultrasound, X-ray, CT).1 Given the acuity of this condition, the immediate intervention is analgesia (for pain) and antiemetics (for when nausea and vomiting is experienced with the pain).1 For renal colic, NSAIDs are the first-line therapy for analgesia.1
Among NSAIDs, ketorolac is commonly used when people present with renal colic in the emergency department.5-7 Ketorolac is in the NSAID class of medications used for the short-term management and treatment of moderate to severe acute onset pain that also includes pain after an operation or painful procedure.5,6,8 Ketorolac can be administered in multiple dose forms, including oral, intranasal, IV, and intramuscular, as well as an ophthalmic solution.5-7,9 If the patient is being treated in the hospital for renal colic, ketorolac would be administered via IV or intramuscular routes. For different indications, health care providers may choose to continue the patient’s treatment with oral ketorolac.6,10
Oral Ketorolac and Its Potential Benefits
The oral administration of ketorolac is only indicated as a continuation to IV or intramuscular therapy (e.g., prescription for oral ketorolac following discharge from the hospital).5,6,10 Ketorolac is intended for short-term use (< 5 days) regardless of the dosage form(s) used.5,6,11,12 However, ketorolac is viewed as a way to reduce the use of opioids when appropriate; opioids have unfavourable side effect profiles and have the potential for tolerance and misuse.12 Transitioning people to oral ketorolac versus other medications as they are discharged may reduce complications because health care providers are aware of the patient’s response to other forms of ketorolac in hospital (e.g., pain control, side effects); however, it is unclear whether oral ketorolac is clinically beneficial or recommended for people with renal colic.
By conducting this review, we can explore the available evidence to determine whether oral ketorolac is a clinically effective option for the management of renal colic.
Objective
The purpose of this report is to summarize and critically appraise the evidence regarding the clinical effectiveness of oral ketorolac for the management of outpatients with renal colic. We also aimed to identify evidence-based guidelines about the use of oral ketorolac for the management of outpatients with renal colic.
Methods
Literature Search Methods
An information specialist conducted a literature search on December 4, 2023, of key resources including MEDLINE, the Cochrane Database of Systematic Reviews, the International HTA Database, the websites of Canadian and international health technology agencies, and Google. The search strategies were developed from elements of the research questions and selection criteria. They included both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. We limited the searches to English-language documents published since January 1, 2013.
The first search strategy contained concepts for ketorolac, renal colic, oral administration, and outpatients. We applied no study design search filters to the first search.
The second search strategy contained concepts for renal colic, NSAIDs, and pain management. We also applied CADTH-developed study design search filters for guidelines, health technology assessments, systematic reviews, meta-analyses, indirect treatment comparisons, and any types of clinical trials or observational studies.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, 1 reviewer screened titles and abstracts and then retrieved potentially relevant articles to assess for inclusion. Table 1 presents the final selection of full-text articles based on the inclusion criteria.
Criteria | Description |
|---|---|
Population | People (all ages) with renal colic in outpatient settings |
Intervention | Oral ketorolac (any dose) |
Comparators | Q1: Alternative analgesics (e.g., alternative nonsteroidal anti-inflammatory drugs, acetaminophen, opioids) Q2: Not applicable |
Outcomes | Q1: Clinical benefits (e.g., pain, need for rescue analgesia, health-related quality of life) and harms (e.g., adverse events) Q2: Recommendations regarding the appropriate use of oral ketorolac for renal colic (e.g., appropriate patient populations, treatment protocols [e.g., duration, dosage], contraindications) |
Study designs | Q1: Health technology assessments, systematic reviews, randomized controlled trials, nonrandomized studies Q2: Evidence-based guidelines |
Exclusion Criteria
We excluded articles if they did not meet the selection criteria outlined in Table 1, were duplicate publications, or were published before 2013.
Summary of Evidence
Quantity of Research Available
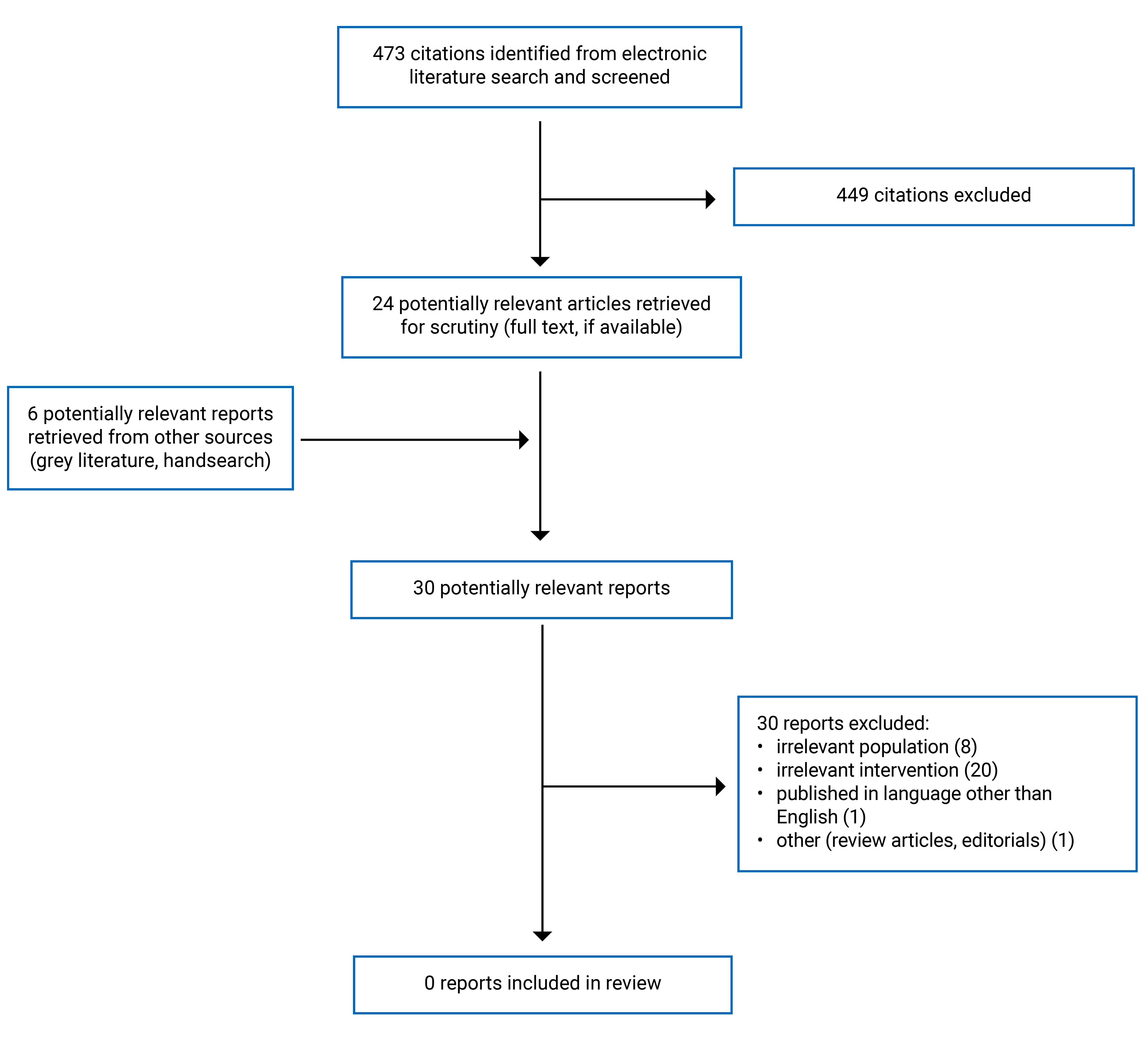
Appendix 1 presents the study selection details. We did not identify any eligible studies or evidence-based guidelines that met the inclusion criteria for this report. The literature mainly focused on other settings (e.g., hospital) or other routes of administration (IV, intramuscular). Appendix 2 provides additional references of potential interest that did not meet the inclusion criteria.
Summary of Findings
Clinical Effectiveness of Oral Ketorolac for Renal Colic
We did not identify any relevant evidence regarding the clinical effectiveness of oral ketorolac for the management of outpatients with renal colic; therefore, no summary can be provided.
Evidence-Based Guidelines
We did not identify any evidence-based guidelines regarding the use of oral ketorolac for the management of outpatients with renal colic; therefore, no summary can be provided.
Limitations
There is a paucity of literature on the clinical effectiveness as well as evidence-based guidelines that provided recommendations on the use of oral ketorolac for the management of people with renal colic. This report is limited by the time frame used for literature searches (January 1, 2013, to December 4, 2023).
Conclusions and Implications for Decision- or Policy-Making
We did not identify any relevant literature about the clinical effectiveness of and recommendations for oral ketorolac for the management of people with renal colic in outpatient settings. We did identify research around ketorolac for renal colic focused on IV or intramuscular administration in hospital. We also found studies investigating oral ketorolac for different indications (listed in Appendix 2), including percutaneous nephrolithotomy (kidney stone removal) and ureteroscopy. For example, study authors of a double-blinded randomized controlled trial reported noninferiority of oral ketorolac versus opioids for postoperative pain control after endoscopy, with similar efficacy, safety profile, physician contact, and earlier convalescence (i.e., recuperation) between groups.13 While this can provide some insights into the potential clinical benefits and harms of oral ketorolac for some people, we are not able to provide conclusions on the clinical effectiveness of oral ketorolac versus alternative analgesics for the management of renal colic in outpatient settings. Likewise, we did not identify any recommendations about the use oral ketorolac for the management of outpatients with renal colic.
We require comprehensive research with rigorous methodological approaches for decision-making in this context. For example, we need high-quality clinical studies to inform conclusions about the potential benefits of oral ketorolac compared with alternative analgesics (e.g., alternative NSAIDs, acetaminophen, opioids), such as need for rescue analgesia and health-related quality of life. We also need evidence-based guidelines to provide recommendations on the use of oral ketorolac for the management of people with renal colic in outpatient settings.
References
1.Patti L, Leslie SW. Acute renal colic. StatPearls. Treasure Island (FL): StatPearls Publishing; 2023 Jan: https://www.ncbi.nlm.nih.gov/books/NBK431091/. Accessed 2023 Dec 19.
2.Saigal CS, Joyce G, Timilsina AR, Urologic Diseases in America Project. Direct and indirect costs of nephrolithiasis in an employed population: opportunity for disease management? Kidney Int. 2005;68(4):1808-1814. PubMed
3.Bryant M, Angell J, Tu H, Goodman M, Pattaras J, Ogan K. Health related quality of life for stone formers. J Urol. 2012;188(2):436-440. PubMed
4.Innes G, McRae A, Grafstein E, et al. Variability of renal colic management and outcomes in two Canadian cities. CJEM. 2018;20(5):702-712. PubMed
5.Mahmoodi AN, Kim PY. Ketorolac. StatPearls. Treasure Island (FL): StatPearls Publishing; 2023 Jan: https://www.ncbi.nlm.nih.gov/books/NBK545172/. Accessed 2023 Dec 19.
6.Toradol. Prescribers' Digital Reference by ConnectiveRX. 2023; https://www.pdr.net/drug-summary/?drugLabelId=1793. Accessed 2023 Dec 21.
7.Rule AD, Lieske JC, Pais VM. Management of kidney stones in 2020. JAMA. 2020;323(19):1961-1962. PubMed
8.Ketorolac (oral route, injection route). Mayo Clinic. 2023 Dec 1; https://www.mayoclinic.org/drugs-supplements/ketorolac-oral-route-injection-route/side-effects/drg-20066882?p=1. Accessed 2023 Dec 21.
9.Chou R, Wagner J, Ahmed AY, et al. Treatments for acute pain: a systematic review. (Comparative effectiveness review no. 240). Rockville (MD): Agency for Healthcare Research and Quality; 2020: https://www.ncbi.nlm.nih.gov/books/NBK566506/. Accessed 2023 Dec 21.
10.MedlinePlus. Ketorolac. 2021; https://medlineplus.gov/druginfo/meds/a693001.html. Accessed 2023 Dec 21.
11.Strom BL, Berlin JA, Kinman JL, et al. Parenteral ketorolac and risk of gastrointestinal and operative site bleeding. A postmarketing surveillance study. JAMA. 1996;275(5):376-382. PubMed
12.Vadivelu N, Gowda AM, Urman RD, et al. Ketorolac tromethamine: routes and clinical implications. Pain Pract. 2015;15(2):175-193. PubMed
13.Fedrigon D, Faris A, Kachroo N, et al. SKOPE-study of ketorolac vs opioid for pain after endoscopy: a double-blinded randomized control trial in patients undergoing ureteroscopy. J Urol. 2021;206(2):373-381. PubMed
Appendix 1: Selection of Included Studies
Appendix 2: References of Potential Interest
Note that this appendix has not been copy-edited.
Previous CADTH Reports
Marchand DK, Loshak H. Nonsteroidal anti-inflammatory drugs and acute kidney injury: safety. (CADTH rapid response report: summary of abstracts). Ottawa (ON): CADTH; 2019 Jan. Ottawa (ON): CADTH; 2019; https://www.cadth.ca/sites/default/files/pdf/htis/2019/RB1299%20NSAIDs%20and%20AKI%20Final.pdf. Accessed Dec 21, 2023.
Ketorolac versus other non-steroidal anti-inflammatory drugs for the management of acute pain: comparative clinical effectiveness. (CADTH rapid response report: summary of abstracts). Ottawa (ON): CADTH; 2017; https://www.cadth.ca/sites/default/files/pdf/htis/2017/RB1055%20Toradol%20vs%20NSAIDS%20Final.pdf. Accessed Dec 21, 2023.
Ketorolac for pain management: a review of the clinical evidence. (CADTH rapid response report: summary with critical appraisal). Ottawa (ON): CADTH; 2014 Jun 30; https://www.ncbi.nlm.nih.gov/books/NBK254117/. Accessed Dec 21, 2023.
Different Indications
Khargi R, Yaghoubian AJ, Blake RM, et al. Opioid-free percutaneous nephrolithotomy: an initial experience. World J Urol. 2023;41(11):3113-9. PubMed
Mengers SR, Strony JT, Sivasundaram L, et al. Oral ketorolac as an adjuvant agent for postoperative pain control after arthroscopic anterior cruciate ligament reconstruction: a prospective, randomized controlled study. J Am Acad Orthop Surg. 2022;30(24):e1580-e1590. PubMed
Fedrigon D, Faris A, Kachroo N, et al. SKOPE-study of ketorolac vs opioid for pain after endoscopy: a double-blinded randomized control trial in patients undergoing ureteroscopy. J Urol. 2021;206(2):373-81. PubMed
Derwich M, Mitus-Kenig M, Pawlowska E. Orally administered NSAIDs: general characteristics and usage in the treatment of temporomandibular joint osteoarthritis: a narrative review. Pharmaceuticals (Basel). 2021;14(3):219. PubMed
Sivasundaram L, Mengers S, Trivedi NN, et al. Oral ketorolac as an adjuvant agent for postoperative pain control after arthroscopic rotator cuff repair: a prospective, randomized, controlled study. J Am Acad Orthop Surg. 2021;29(24):e1407-e1416. PubMed
DeAndrade JF, Maslanka M, Maneatis T, Bynum L, Burchmore M. The use of ketorolac in the management of postoperative pain. Orthopedics. 2013;17(2):157-166. PubMed
Contributors: Chris Kamel, Calvin Young
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for noncommercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca.