CADTH Health Technology Review
Hernia Support Garments for Parastomal Hernia Following Ostomy Procedure
Rapid Review
Authors: Robyn Haas, Jennie Horton, Angie Hamson
Key Messages
What Is the Issue?
Parastomal hernia is a common complication that can occur following ostomy surgery. They can have a negative impact on a person’s quality of life, affecting them both physically and psychologically. One intervention that may be used to help prevent or manage parastomal hernias are hernia support garments.
To help inform decisions about the most appropriate use for hernia support garments, it is important to understand the current best practices as well as potential benefits and harms of using these garments.
What Did We Do?
We searched for clinical and cost-effectiveness literature comparing hernia support garments to alternative hernia prevention or management strategies or no intervention. We also searched for evidence-based guidelines that provide recommendations about the use of hernia support garments for the prevention or management of parastomal hernias.
An information specialist searched for peer-reviewed and grey literature sources published between January 1, 2013, and November 1, 2023.
We engaged with an individual who has lived experience of an ostomy and parastomal hernia and who wears a hernia belt regularly. They shared thoughts on the physical and psychological benefits, impact on quality of life, and challenges of using a hernia belt. This gave CADTH a more nuanced understanding of the literature.
What Did We Find?
We did not find any studies directly evaluating the clinical or cost-effectiveness of hernia support garments versus alternative hernia prevention or management interventions or no treatment that met the inclusion criteria for this review.
Three evidence-based guidelines made recommendations related to using hernia support garments to prevent and manage parastomal hernia. One guideline recommends that individuals with an ostomy should be assessed to determine the type and level of support required to prevent or manage hernia. Another guideline recommends that health providers provide postoperative education on using support garments. The third guideline recommends that stoma care nurses provide lifestyle advice about support garments to individuals with a stoma. This guideline also recommends that these nurses should be available to advise on non-operative management options for parastomal hernias more generally.
What Does This Mean?
Decision-makers might wish to consider ways to ensure that individuals who have had or are scheduled to have an ostomy surgery have timely access to parastomal hernia risk assessment, education, and advice on the use of hernia support garments from nurses specialized in wound, ostomy, and continence care. They may also want to consider out-of-pocket costs that may be a barrier to this care.
Abbreviations
ACPGBI
Association of Coloproctology of Great Britain and Ireland
NSWOCC
Nurses Specialized in Wound, Ostomy, and Continence Canada
RNAO
Registered Nurses’ Association of Ontario
Research Questions
What is the clinical effectiveness of hernia support garments for the prevention and management of parastomal hernia in patients living with an ostomy?
What is the cost-effectiveness of hernia support garments for preventing and managing parastomal hernia in patients living with an ostomy?
What are the evidence-based guidelines for the use of hernia support garments for the prevention and management of parastomal hernia in patients living with an ostomy?
Context and Policy Issues
What Is a Parastomal Hernia?
Parastomal hernia is a common complication that occurs after a person undergoes surgery to create an ostomy, which is a surgically created opening in the abdominal wall that allows bodily waste to pass into an external pouch or bag.1 This type of hernia occurs when part of the intestine protrudes through the abdominal muscles, causing a bulge around the ostomy site.2 The reported incidence of parastomal hernia following ostomy surgery varies. Some literature suggests that incidence may range from 0% to 50%, while others indicate that it may be as high as 78%.1,2 Most people who develop a parastomal hernia will do so within the first 2 years following surgery, though they can occur at any time. People with a parastomal hernia may experience pouch leakages, leading to skin damage and difficulties maintaining a seal for the ostomy pouching system.2 Additionally, they might experience bowel obstructions and chronic pain in the abdomen, back, or hips. In rare instances, people can experience bowel strangulation and ischemia.2 In addition to these complications, living with a parastomal hernia can negatively impact a person’s quality of life due to stress related to body image, fatigue, and the physical burden of the hernia.3
What Is a Hernia Support Garment?
A hernia support garment, sometimes called a hernia belt, is specifically designed to compress and stabilize the stoma site lightly, which is the visible part of the ostomy.2 Patients commonly wear these garments following ostomy surgery to help prevent the occurrence of a parastomal hernia, or they may wear them after developing a hernia to manage symptoms and reduce complications.2 Hernia support garments are available in a range of sizes and widths and provide various levels of support.4 Some garments have a hole cut-out that goes around the ostomy pouching system, while others do not.4 These garments can also vary in cost. The type of garment a person might wear can depend on their type of stoma, function, type of pouch, size and shape of stoma, and personal characteristics and comorbidities.4 Ideally, these garments should be comfortable, provide the necessary level of support, fit appropriately, and suit the individual’s needs.4
Why Is It Important to Do This Review?
Approximately 750,000 people are living with an ostomy in North America.1 In Canada alone, surgeons perform about 13,000 new ostomies per year, and each of these individuals are at risk for developing a parastomal hernia.5 Those living with an ostomy may avoid participating in certain types of physical activity due to fear of developing a parastomal hernia, which can, in turn, affect their overall well-being.6 People who develop a parastomal hernia may have the option to undergo surgical repair, but this option is expensive, and the recurrence rate of hernia is around 50%.2,7 Surgical repair can also be associated with an increased risk of morbidity and mortality.8 As such, strategies for prevention and management of parastomal hernia, such as hernia support garments, may be a better option. By conducting this review, we can explore the available evidence to determine whether hernia support garment are effective options for parastomal hernias.
Objective
The purpose of this report is to summarize and critically appraise the evidence identified from medical databases and grey literature searching about the clinical and cost-effectiveness of hernia support garments for parastomal hernia following ostomy procedure. We also aimed to identify evidence-based guidelines about the use of hernia support garments.
Methods
Literature Search Methods
An information specialist conducted a literature search on key resources including MEDLINE, the Cochrane Database of Systematic Reviews, the International Health Technology Assessment Database, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search approach was customized to retrieve a limited set of results, balancing comprehensiveness with relevancy. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. Search concepts were developed based on the elements of the research questions and selection criteria. The main search concepts were parastomal hernia and support garments. No filters were applied to limit the search by study type. An additional search was run for parastomal hernia with CADTH-developed search filters applied to limit retrieval to guidelines. The search was completed on November 1, 2023 and limited to English-language documents published since January 1, 2013.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
|---|---|
Population | Any patient at risk of parastomal hernia development postostomy (regardless of age and time postsurgery) |
Intervention | Hernia support garment |
Comparator | Q1 and Q2: Alternative hernia prevention or management interventions (e.g., rehabilitative exercise, lifestyle changes); No intervention (which may include before and after studies) Q3: Not applicable |
Outcomes | Q1: Clinical benefits (e.g., parastomal hernia prevention or management, reduced pouching system changes, reduction in surgical repair, patient preference, health-related quality of life outcomes) and harms (e.g., rate of adverse events, impact on hospital stays, frequency of subsequent patient follow-up) Q2: Cost-effectiveness (e.g., cost per QALY gained, ICER, cost per adverse event avoided) Q3: Recommendations regarding the use of hernia support garments for parastomal hernia prevention (e.g., optimal postop duration for intervention, hernia support garment structure or mechanism, appropriate patient populations for hernia support garments) |
Study designs | Health technology assessments, systematic reviews, randomized controlled trials, nonrandomized studies, economic evaluations, evidence-based guidelines |
ICER = Incremental cost-effectiveness ratio; QALY = quality-adjusted life-years.
Exclusion Criteria
We excluded articles if they did not meet the selection criteria in Table 1, they were duplicate publications, or were published before 2013. We also excluded guidelines with unclear methodology.
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the Appraisal of Guidelines for Research and Evaluation (AGREE) II instrument.9 Summary scores were not calculated for the included studies; instead, each publication's strengths and limitations were described narratively.
Patient Engagement
Patient engagement is an important component of CADTH’s work. CADTH has a Patient Engagement Framework to guide our engagement processes. Patients contribute their thoughts and perspectives to highlight their priorities and contextualize what is found in the literature. For this report, CADTH engaged a patient contributor with the lived experience of wearing a hernia support garment.
Invitation to Participate and Consent
A request to engage was disseminated through a wound, ostomy, and continence nurse. A patient with an ostomy and parastomal hernia who wears a hernia belt daily was identified to participate. The patient contributor was invited to participate in a Zoom video call with a Patient Engagement Officer and Research Officer. They signed a consent form and participated in a 1-hour dialogue about his experiences, perspectives, and priorities. A summary of the key points was drafted, approved by the patient, and shared with the Research Officer authoring the report. An honorarium was offered to the patient as a gesture of thanks for his time and expertise, and they elected to remain anonymous in the report’s acknowledgements.
Engagement Activities
An individual with lived experience of an ostomy and a parastomal hernia, who regularly wears a hernia belt shared his experiences with CADTH staff. We used the perspectives gained through this process to provide insight and context to this report.
Patient involvement was guided by the Guidance for Reporting Involvement of Patients and the Public (version 2) Short Form reporting checklist,10 which is outlined in Appendix 5.
Summary of Evidence
Quantity of Research Available
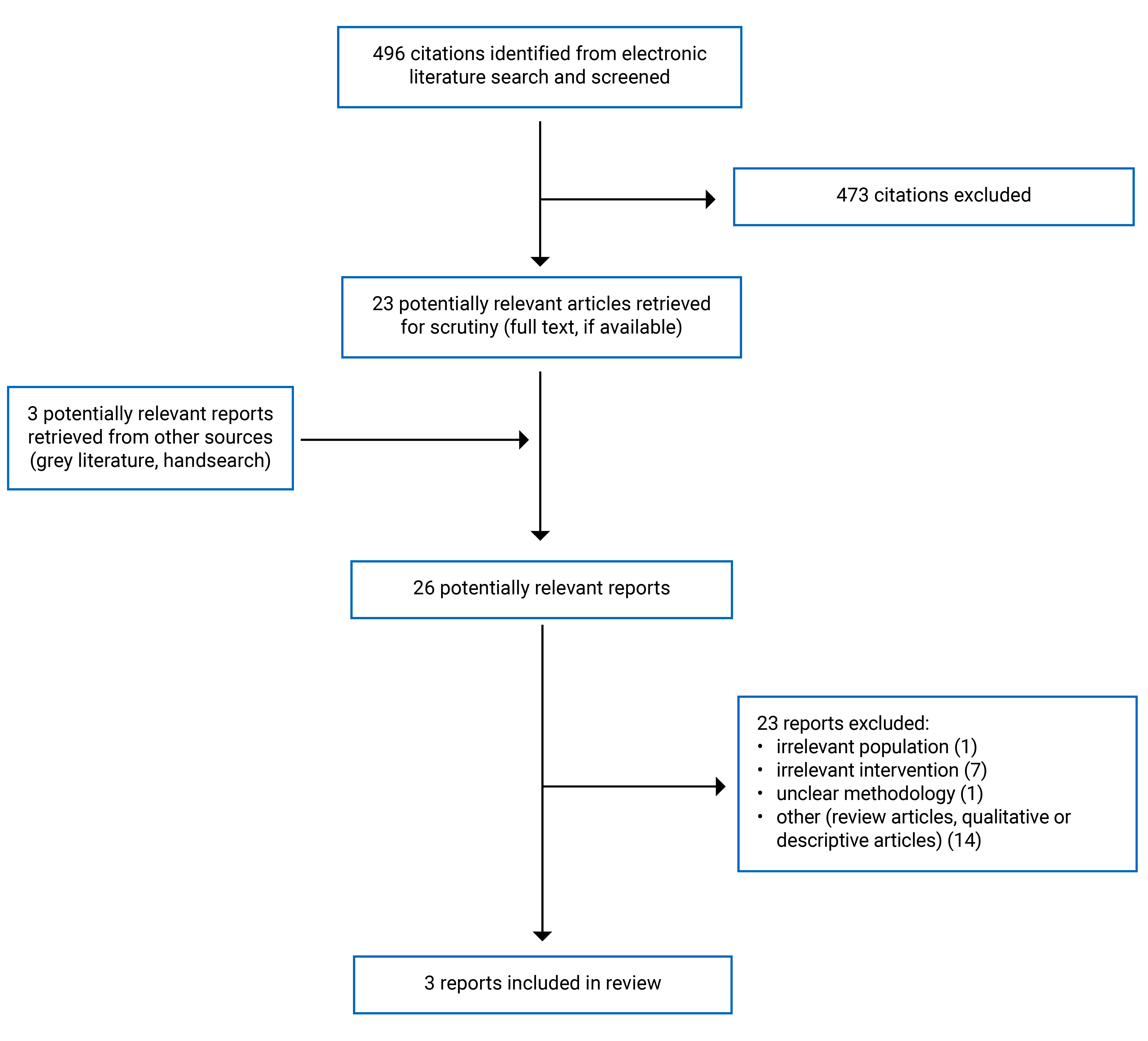
A total of 496 citations were identified in the literature search. Following screening of titles and abstracts, 473 citations were excluded and 23 potentially relevant reports from the electronic search were retrieved for full-text review. Three potentially relevant publications were retrieved from the grey literature search for full-text review. Of these potentially relevant articles, 23 publications were excluded for various reasons and 3 publications met the inclusion criteria and were included in this report. All 3 of these publications were evidence-based guidelines. Appendix 1 presents the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA)8 flow chart of the study selection. Additional references of potential interest are provided in Appendix 6.
Summary of Guideline Characteristics
This report includes 3 evidence-based guidelines with recommendations that were developed from systematic searches for relevant evidence.1,4,11 The recommendations provide guidance related to parastomal hernia risk assessment and postoperative education regarding using hernia support garments in individuals who have had or anticipate having ostomy surgery.
Appendix 2 presents additional details regarding the characteristics of the included guidelines.
Study Design
The evidence-based guidelines in this report were developed by the Nurses Specialized in Wound, Ostomy, and Continence Canada (NSWOCC),4 the Registered Nurses’ Association of Ontario (RNAO),1 and the Association of Coloproctology of Great Britain and Ireland (ACPGBI) Parastomal Hernia Group.11 The guidelines were published in 2023, 2019, and 2018.1,4,11
All of the guidelines systematically searched the literature using multiple databases.1,4,11 The NSWOCC and ACPGBI guidelines also included a handsearch of the literature.4,11 The RNAO and ACPGBI guidelines used the Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) approach to rate the certainty of evidence used to inform recommendations as high, moderate, low, or very low.1,11 The RNAO guideline also used the Confidence in the Evidence from Reviews of Qualitative (CERQual) research to help assess qualitative studies.1 The RNAO guideline classified the strength of recommendations as either solid or conditional. The ACPGBI guideline classified the strength of recommendations as either strong or weak.1 The authors of the NSWOCC guideline assigned a level of evidence to their recommendations based on a 7-level scale.4 The levels were: Ia (highest), Ib, IIa, IIb, II, IV, V (lowest). Each level corresponds to the study design of the source of the evidence.4 Refer to Appendix 2 for a full description of these levels of evidence.
Country of Origin
The authors of both the RNAO and NSWOCC guidelines were from Canada and the guidance was developed for use in Canada.1,4 The authors of the ACPGBI guideline were from the UK and were intended for use by practitioners in Great Britain and Ireland.11
Patient Population
The target population for all the guidelines were people living with an ostomy or those who anticipate living with an ostomy (i.e., people awaiting ostomy surgery).1,4,11 The RNAO guideline was specifically targeted toward adults 18 years and older.1 The NSWOCC and ACPGBI guidelines did not report whether their recommendations applied to specific age groups. The intended users for the RNAO and NSWOCC guidelines included nurses specialized in wound, ostomy, and continence care as well as others on the interprofessional team (e.g., physicians, allied health professionals) who support people who currently live or who will live with an ostomy.1,4 The ACPGBI guideline reported that their intended users were ACPBGI members.11
Interventions
All the guidelines examined various interventions for assessing, preventing, and managing parastomal hernias, including hernia support garments.1,4,11 These guidelines specifically considered the role of nurses specialized in wound, ostomy, and continence care, sometimes referred to as stoma care nurses, in providing perioperative or postoperative assessment, counselling, and educating individuals about garments that would best fit their needs and lifestyle.1,4,11 The ACPGBI guideline also includes a recommendation about the role of nurses specialized in wound, ostomy, and continence care for non-operative care options for parastomal hernias more generally.11
Outcomes
All 3 guidelines considered the risk of developing a parastomal hernia and the severity of symptoms associated with the hernia when formulating recommendations relevant to this report.1,4,11 The guidelines also considered outcomes not related to the use of hernia support garments. However, these were not relevant to this report.
Summary of Critical Appraisal
This section presents a narrative summary of the strengths and limitations of the included guidelines. Additional details are provided in Appendix 3.
All guidelines stated their scope and objectives, described the range of health questions covered and their target users, and indicated the populations to whom the guidelines were meant to apply.1,4,11 They also included individuals from relevant professional groups during the guideline development process.1,4,11 These professional groups included nurses specialized in the field, colorectal surgeons, and allied health professionals (e.g., physiotherapists).1,4,11 While the NSWOCC guideline noted that it underwent review by individuals with subject matter expertise, it was not clear whether any of these individuals were patients or members of the public.4 The RNAO guideline indicated that they sought out and incorporated the views and preferences of individuals with lived experience as part of the guideline development process.1 The guideline developers engaged these individuals in virtual focus groups intended to understand their needs.1 The ACPGBI guideline did not report whether they sought out views and preferences of the target population.11
All guidelines used systematic methods to search for evidence for consideration when developing recommendations.1,4,11 The RNAO guideline clearly presented their criteria for selecting evidence and described the strengths and limitations of this evidence.1 The NSWOCC and ACPGBI guidelines only partially included this information.4,11 They provided the overall parameters for selecting evidence (e.g., time frame, language restrictions) and mentioned that they used inclusion and exclusion criteria, but they did not report specific details of these criteria.1,4,11 These 2 guidelines also noted some limitations around the quality of evidence they included but provided minimal details.1,4,11 This lack of detail in the NSWOCC and ACPGBI guidelines may, in turn, decrease the reproducibility in the selection of studies that informed the recommendations.1,4,11 All 3 guidelines considered the health benefits, side effects, and risks of their recommendations and clearly presented the link between the recommendations and supporting evidence.1,4,11 The NSWOCC and RNAO guidelines were both externally reviewed by experts before publication.1,4 A total of 28 peer reviewers with expertise on parastomal hernias reviewed the NSWOCC guideline.4 Nurses and individuals with lived experience reviewed the RNAO guideline.1 The ACPGBI guideline did not report whether it had been externally reviewed by experts before its publication.11 Only the RNAO guideline provided a procedure for updating their guideline.1
The key recommendations in all guidelines were easily identifiable and included different options for assessment, prevention, and management for parastomal hernias.1,4,11 While most recommendations across all guidelines were specific and unambiguous, the ACPGBI guideline included some recommendations that were broad in scope as they lacked details around the population(s) for whom they were intended and to whom they applied.11 This may be a result of the lack of high-quality evidence that the authors noted.11
The RNAO guideline considered the potential resource implications of their recommendations by implementing a previously created toolkit12 designed to facilitate the implementation of their guidelines into clinical practice based on the local context (e.g., the availability of resources).1 The NSWOCC guideline gave some consideration to the resource implications of their recommendations by acknowledging costs to the health care system and potential costs and accessibility for interventions such as hernia support garments.4 The ACPBGI guideline did not report on the potential resource implications of their recommendations.11 The RNAO guideline was the only 1 that presented monitoring criteria, described facilitators and barriers to its application, and provided tools to implement the recommendations.1
All guidelines declared potential conflicts of interest of guideline development group members. The RNAO and NSWOCC guidelines reported on their sources of funding. The RNAO guideline explicitly stated that the authors had editorial independence from the funding organizations. One author from the NSWOCC guideline declared a relevant conflict of interest. It is unclear if the funding body influenced the recommendations made in the guideline. The ACPBGI guideline declared that the authors had no conflicts of interest but did not report a source of funding.
All the guidelines used rigorous methodology and were comprehensively and clearly reported.1,4,11
Summary of Findings
Appendix 4 presents the detailed recommendations and supporting evidence that are relevant to this report.
Clinical Effectiveness of Hernia Support Garments
No relevant evidence was identified regarding the clinical effectiveness of hernia support garments for patients at risk of parastomal hernia development postostomy; therefore, no summary can be provided.
Cost-Effectiveness of Hernia Support Garments
No relevant evidence was identified regarding the cost-effectiveness of hernia support garments for patients at risk of parastomal hernia development postostomy; therefore, no summary can be provided.
Guidelines Regarding the Use of Hernia Support Garments
The NSWOCC guideline recommends that a nurse specialized in wound, ostomy, and continence care or other health care provider should assess individuals who live with an ostomy to determine the type and level of support garment needed for the prevention or management of a parastomal hernia.4 The assessment should consider the person’s lifestyle, activities of daily living, and personal preferences.4 This recommendation was based on the 3 lowest levels of evidence on the 7-level scale, including qualitative studies, non-experimental observational studies, and expert opinion, committee report, or clinical experiences.4
The RNAO guideline recommends that health professionals provide postoperative education about lightweight support garments to individuals who have or will have an ostomy (conditional recommendation), based on a very low certainty evidence.1 Similarly, the ACPGBI recommends that stoma care nurses provide counselling and advice about support garments for people with a stoma (weak recommendation) based on low-quality evidence.11 They also recommend that individuals with a stoma have access to stoma care nurses to advise them on non-operative management for parastomal hernias more generally (strong recommendation), based on low-quality evidence.11
Limitations
There were few guidelines that met the inclusion criteria for this report, and those that did meet the criteria contained a small number of applicable recommendations. The scope of these recommendations was limited to the role of nurses specialized in wound, ostomy, and continence care or stoma care nurses in assessing and educating patients about hernia support garments. One recommendation indicated that the patient’s lifestyle, activities of daily living, and personal preference are important considerations when determining the type and level of support garment to recommend. However, the recommendations did not include more granular details such as the number of hours a day 1 should wear a support garment, how often 1 might need to replace a garment, or when to provide a more supportive versus a less supportive garment. Additional gaps in the identified literature include information about the types of patient populations who should use a support garment and the duration for which patients should use a support garment after surgery. Finally, all the recommendations were based on low- or very low-quality evidence. This, in turn, can limit their applicability.
Through the search of medical databases and grey literature, we did not identify any eligible studies evaluating the clinical or cost-effectiveness of hernia support garments for people who have or who are at risk of developing parastomal hernia. As a result, we can neither comment on the comparative benefits or harms of hernia support garments, nor can we comment on the quality of evidence in this area. It is possible that relevant literature about hernia support garments for preventing and managing parastomal hernia exists but was published more than 10 years ago. However, it does not appear that there is a large body of literature about hernia support garments for these outcomes.
Conclusions and Implications for Decision- or Policy-Making
Based on the literature search conducted for this review, we did not identify any evidence about the clinical or cost-effectiveness of hernia support garments for patients at risk of or who have a parastomal hernia. We included 3 evidence-based guidelines in this report, all rigorous, comprehensive, and clear in their methodology and reporting.1,4,11 The relevant recommendations were based on very low to low-quality evidence.1,4,11 Based on the guidelines’ recommendations, nurses specialized in wound, ostomy, and continence care play a critical role in providing care for individuals at risk for developing a parastomal hernia and should help assess, advise, and educate patients on hernia support garments.1,4,11 The patient we engaged with echoed the importance of nurses specializing in wound, ostomy, and continence care in our conversation. Overall, the target population for each of the evidence-based guidelines was broad, which makes the recommendations generalizable to most individuals who have or are at risk of a parastomal hernia postostomy.1,4,11 Additionally, because 2 of the guidelines were developed for use in Canada, they directly apply to this setting.1,4
To date, most of the research around hernia support garments is qualitative or descriptive. While this can provide important insights into the perspectives and experiences of individuals who use these garments, we cannot provide conclusions on the clinical or cost-effectiveness of hernia support garments versus alternative hernia prevention or management interventions. High-quality clinical studies are needed to inform conclusions about the potential benefits of these garments, such as parastomal hernia prevention or impact on quality of life. Based on the dialogue from our patient engagement activities, it would be valuable for future clinical research to examine health-related quality-of-life outcomes specifically. Both physical outcomes, such as the ability to engage in physical activity, and mental health outcomes, such as well-being, are important to consider. Adverse events such as pain and discomfort related to garment wear are also important to explore. Additionally, studies that compare the benefits and harms of different types of belts, or no belt at all, could also provide valuable insight into patient preference around hernia support garments and the types of garments may be most appropriate for patient use.
It is also important to better understand the cost's role in using these garments. The price of hernia support garments can vary, and the garment will likely need to be replaced 1 or more times per year depending on how frequently it is worn.4 We heard in our patient engagement dialogue that the individual replaces 1 of his belts every 2 to 3 months and his other belt 1 to 2 times per year. Every time the patient replaces their belt they must pay out of pocket. An important implication of this is that people of lower socioeconomic status may have difficulty accessing hernia support garments.
Finally, higher quality clinical studies could also result in more robust and detailed recommendations, such as guidance on the best material or width of garment to use depending on the patient, their unique circumstances, and the context in which they would wear the garment.
References
1.Supporting Adults Who Anticipate or Live with an Ostomy. Toronto (ON): Registered Nurses' Association of Ontario. 2019; https://rnao.ca/sites/rnao-ca/files/bpg/OSTOMY_FINAL_WEB_Updated_July_5.pdf. Accessed 2023 Nov 6.
2.Cima R. Parastomal hernia. UpToDate 2021; www.uptodate.com. Accessed 2023 Nov 8.
3.Bland C. Nurse activity to prevent and support patients with a parastomal hernia. Gastrointestinal Nursing. 2015;13(10):16-24.
4.Parastomal Hernia Prevention, Assessment, and Management: Canadian Best Practice Recommendations. Ottawa (ON): Nurses Specialized in Wound, Ostomy and Continence Canada. 2023; https://www.nswoc.ca/_files/ugd/9d080f_35f5f525ff6944da831af9fdd1793bf5.pdf?index=true. Accessed 2023 Nov 6.
5.A handbook for new ostomy patients. Vancouver (BC): Vancouver United Ostomy Association Chapter, Inc. 2019; http://www.uoavancouver.com/uploads/2/6/8/9/26894454/handbook_for_new_patients_web_8th_printing_2019.pdf. Accessed 2023 Nov 20.
6.North J. Early intervention, parastomal hernia and quality of life: a research study. Br J Nurs. 2014;23(5 Supp):S14-S18. PubMed
7.Borglit T, Krogsgaard M, Theisen SZ, Juel Rothmann M. Assessment of a support garment in parastomal bulging from a patient perspective: a qualitative study. Int J Qual Stud Health Well-being. 2022;17(1):2039428. PubMed
8.Helgstrand F, Rosenberg J, Kehlet H, Jorgensen LN, Wara P, Bisgaard T. Risk of Morbidity, Mortality, and Recurrence After Parastomal Hernia Repair: A Nationwide Study. Dis Colon Rectum. 2013;56(11):1265-1272. PubMed
9.Agree Next Steps C. The AGREE II Instrument. Hamilton, ON: AGREE Enterprise; 2017: https://www.agreetrust.org/wp-content/uploads/2017/12/AGREE-II-Users-Manual-and-23-item-Instrument-2009-Update-2017.pdf. Accessed 2023 Nov 6.
10.Staniszewska S, Brett J, Simera I, et al. GRIPP2 reporting checklists: tools to improve reporting of patient and public involvement in research. BMJ. 2017;358:j3453. PubMed
11.Anonymous. Prevention and treatment of parastomal hernia: a position statement on behalf of the Association of Coloproctology of Great Britain and Ireland. Colorectal Dis. 2018;20 Suppl 2:5-19. PubMed
12.Leading Change Toolkit. Toronto (ON): Registered Nurses' Association of Ontario. 2012; https://rnao.ca/leading-change-toolkit. Accessed 2023 Nov 20.
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Table 2: Characteristics of Included Guidelines
Intended users, target population | Intervention and practice considered | Major outcomes considered | Evidence collection, selection, and synthesis | Evidence quality assessment | Recommendations development and evaluation | Guideline validation |
|---|---|---|---|---|---|---|
NSWOCC (2023)4 | ||||||
Intended users: Nurses Specialized in Wound, Ostomy, and Continence, registered nurses, physicians, and other allied health care professionals who support individuals who will have or already have an ostomy. Target population: People living with an abdominal ostomy. | A range of interventions for the assessment, prevention, and management for parastomal hernias. Relevant intervention: hernia support garments | Relevant outcomes: prevention and symptom severity of parastomal hernias | The expert panel collected evidence through a systematic search of the literature to identify articles of any study design. They also conducted additional handsearching. | The expert panel assigned a level of evidence to each recommendation using the RNAO system. The levels ranged from Ia to V. They were defined as follows: Ia: Evidence from meta-analysis or systematic review of RCTs and/or synthesis of multiple studies primarily of quantitative research. Ib: Evidence from at least one RCT. IIa: Evidence from at least one well-designed controlled study without randomization. IIb: Evidence from at least one other type of well-designed quasi-experimental study without randomization. III: Synthesis of multiple studies primarily by qualitative research. IV: Evidence from well-designed non-experimental observational studies, such as analytical, descriptive, and/or qualitative studies. V: Evidence from expert opinion or committee reports, and/or clinical experiences of respected authorities. | A panel made up of experts in relevant fields proposed, discussed, and voted on consensus statements. They used a Delphi methodology to achieve consensus. The panel accepted statements that achieved agreement of at least 80%. If a statement did not achieve 80% agreement, a moderator led discussions to revise the statement. If the panel could not reach agreement after 3 rounds of revisions and voting, the statement was excluded from the final list. The panel reached consensus for 15 statements and assigned a RNAO level of evidence to each recommendation. | The expert panel nominated peers with subject matter expertise to be external reviewers. Twenty-eight peer reviewers provided feedback on the consensus statements and voted to accept or reject the statements. Authors made refinements to the guideline document and overall takeaways were discussed with the expert panel. The NSWOCC Board approved the final guideline document. |
RNAO (2019)1 | ||||||
Intended users: Nurses and the interprofessional team who support adults who anticipate or live with an ostomy. Target population: Adults (18 years and older) who anticipate or live with an ostomy | Access to NSWOCs, ostomy care programs, prevention strategies for parastomal hernia, and quality of life assessment. Relevant intervention: postoperative education related to lightweight support garments for parastomal hernia | Peristomal dermatitis, peristomal irritation, ostomy leakage, quality of life, hospital health of stay, readmission rates to hospital, patient satisfaction, staff satisfaction, parastomal hernia rates, psychological health status and self-identity Outcome associated with relevant recommendation: parastomal hernia rates | The BPG was based on a systematic review of the literature to identify articles of any study design. Authors also conducted an additional search of guidelines. | The guideline development group used GRADE and CERQual methods to assess the certainty of evidence. Both methods categorize the confidence in evidence as high, moderate, low, or very low. The group categorized the strength of recommendations as either strong or conditional by considering the certainty of evidence and key criteria of:
| The guideline development group used an Evidence-to-Decision framework to formulate recommendations. Expert panel members participated in an online vote for each recommendation based on guiding questions. Guideline development and expert panel members discussed the results of the vote and made decisions on the direction and strength of each recommendation. Methodologists drafted the BPG for which an expert panel then reviewed and provided feedback. Changes were discussed and incorporated. | The BPG underwent stakeholder review by subject matter experts and individuals who may be affected by the implementation of the BPG. The RNAO recruited stakeholder reviewers through a public call on their website and using referral from the research team and expert panel. Reviewers read the BPG before publication and responded to a survey of questions about the guideline and its recommendations. The guideline development group reviewed and discussed the feedback and modified the guideline accordingly. |
ACPGBI (2018)11 | ||||||
Intended users: ACPGBI members. Target population: People with stomas | A range of interventions related to prevention, diagnosis, classification, management, and operative repair for parastomal hernias. Relevant intervention: hernia support garments, non-operative management of parastomal hernias | Relevant outcome: incidence and symptom severity of parastomal hernias | The guideline development group members collected evidence using a systematic search of the literature to identify articles of any study design. They also conducted additional handsearching of references lists and conference abstracts. | The guideline development group members classified the quality of evidence and strength of recommendations using GRADE methods. Quality of evidence was classified as either high, moderate, low, or very low. Strength of the recommendations were classified as either strong or weak. | The guideline development group members followed a standardized 4 step approach used in previously developed ACPGBI position statements. The approach consisted of:
| NR. |
ACPGBI = Association of Coloproctology of Great Britain and Ireland; BPG = best practice guideline; CERQual = Confidence in the Evidence from Reviews of Qualitative research; GRADE = Grading of Recommendations, Assessment, Development, and Evaluation, Confidence in the Evidence from Reviews of Qualitative research; NR = not reported; NSWOCC = Nurses Specialized In Wound, Ostomy, and Continence Canada; RCT = randomized controlled trial; RNAO = Registered Nurses’ Association of Ontario.
Note that this table has not been copy-edited.
Appendix 3: Critical Appraisal of Included Publications
Note that this table has not been copy-edited.
Table 3: Strengths and Limitations of Guidelines Using AGREE II9
Item | NSWOCC (2023)4 | RNAO (2019)1 | ACPGBI (2018)11 |
|---|---|---|---|
Domain 1: Scope and purpose | |||
1. The overall objective(s) of the guideline is (are) specifically described. | Yes | Yes | Yes |
2. The health question(s) covered by the guideline is (are) specifically described. | Yes | Yes | Yes |
3. The population (patients, public, etc.) to whom the guideline is meant to apply is specifically described. | Yes | Yes | Yes |
Domain 2: Stakeholder involvement | |||
4. The guideline development group includes individuals from all relevant professional groups. | Yes | Yes | Yes |
5. The views and preferences of the target population (patients, public, etc.) have been sought. | Unclear | Yes | NR |
6. The target users of the guideline are clearly defined. | Yes | Yes | Yes |
Domain 3: Rigour of development | |||
7. Systematic methods were used to search for evidence. | Yes | Yes | Yes |
8. The criteria for selecting the evidence are clearly described. | Partially (lack of detail around inclusion and exclusion criteria) | Yes | Partially (lack of detail around inclusion and exclusion criteria) |
9. The strengths and limitations of the body of evidence are clearly described. | Partially (some mention around the quality of evidence) | Yes | Partially (some mention around the quality of evidence) |
10. The methods for formulating the recommendations are clearly described. | Yes | Yes | Yes |
11. The health benefits, side effects, and risks have been considered in formulating the recommendations. | Yes | Yes | Yes |
12. There is an explicit link between the recommendations and the supporting evidence. | Yes | Yes | Yes |
13. The guideline has been externally reviewed by experts before its publication. | Yes | Yes | NR |
14. A procedure for updating the guideline is provided. | No | Yes | No |
Domain 4: Clarity of presentation | |||
15. The recommendations are specific and unambiguous. | Yes | Yes | Partially (some recommendations are broad in scope) |
16. The different options for management of the condition or health issue are clearly presented. | Yes | Yes | Yes |
17. Key recommendations are easily identifiable. | Yes | Yes | Yes |
Domain 5: Applicability | |||
18. The guideline describes facilitators and barriers to its application. | No | Yes | No |
19. The guideline provides advice and/or tools on how the recommendations can be put into practice. | Yes | Yes | No |
20. The potential resource implications of applying the recommendations have been considered. | Partially (some cost considerations briefly mentioned) | Yes | No |
21. The guideline presents monitoring and/or auditing criteria. | No | Yes | No |
Domain 6: Editorial independence | |||
22. The views of the funding body have not influenced the content of the guideline. | Unclear | Yes | NR |
23. Competing interests of guideline development group members have been recorded and addressed. | Yes | Yes | Yes |
ACPBGI = Association of Coloproctology of Great Britain and Ireland; AGREE II = Appraisal of Guidelines for Research and Evaluation II; NR = not reported; NSWOCC = Nurses Specialized in Wound, Ostomy, and Continence Canada; RNAO = Registered Nurses’ Association of Ontario.
Appendix 3: Main Study Findings
Note that this table has not been copy-edited.
Table 4: Summary of Recommendations in Included Guidelines
Recommendations and supporting evidence | Quality of evidence and strength of recommendations |
|---|---|
NSWOCC (2023)4 | |
“An individual with an ostomy should be assessed to determine the type and level of support garment/belt required for prevention or management of parastomal hernia, considering the person’s lifestyle, activities of daily living, and personal preference. (p.10)” Supporting evidence:1 clinical practice guideline, 1 narrative review, 2 qualitative reviews, and 1 descriptive study. Note: a table that outlines the criteria for support garment selection is also available on p.23. | Levels of Evidence III, IV, V: III: Synthesis of multiple studies primarily by qualitative research IV: Evidence obtained from well-designed non-experimental observational studies, such as analytical studies, or descriptive studies, and/or qualitative studies V: Evidence obtained from expert opinion or committee reports, and /or clinical experiences of respected authorities |
RNAO (2019)1 | |
“The expert panel suggests that health providers implement the following interventions to prevent parastomal hernias for persons who anticipate or live with an ostomy:
Supporting evidence: 1 narrative review, 1 descriptive study with 100 participants Note: elaborative comments about preferences and equity related to hernia support garments are also available on p.44. | Certainty of evidence: very low Strength of recommendation: conditional |
ACPGBI (2018)11 | |
“SCNs should be involved in the perioperative counselling of patients with a stoma and offer lifestyle advice regarding support garments and exercise. (p. 6)” Supporting evidence: 1 clinical practice guideline and 1 RCT. | Quality of evidence: low Strength of recommendation: weak |
“Patients need access to SCNs to advise on the best non-operative management options for PSHs. (p. 12)” Supporting evidence: 1 clinical practice guideline. | Quality of evidence: low Strength of recommendation: strong |
ACPBGI = Association of Coloproctology of Great Britain and Ireland; NSWOCC = Nurses Specialized in Wound, Ostomy, and Continence Canada; PSH = parastomal hernia; RCT = randomized controlled trial; RNAO = Registered Nurses’ Association of Ontario; SCN = stoma care nurse.
Appendix 5: Patient Involvement
Note that this table has not been copy-edited.
Table 5: Summary of Patient Involvement Using the Guidance for Reporting Involvement of Patients and the Public (version 2) Short Form Reporting Checklist10
Section and topic | Item | Report section(s) |
|---|---|---|
Aim | A patient with lived experience of an ostomy, parastomal hernia, and regular use of an ostomy hernia belt was engaged to share their perspective, allowing for a more nuanced understanding of the literature. | Key Messages |
Methods | A request to engage was disseminated through a Wound, Ostomy, and Continence nurse. A patient with an ostomy and parastomal hernia, who wears a hernia belt daily, was identified to participate. The patient contributor was invited to participate in a Zoom video call with a Patient Engagement Officer and Research Officer. They signed a consent form and participated in a 1-hour dialogue about his experiences, perspectives, and priorities. A short summary of the key points was drafted, approved by the patient, and shared with the Research Officer authoring the report. An honorarium was offered to the patient as a gesture of thanks for his time and expertise, and the patient elected to remain anonymous in the report’s acknowledgements. | Methods |
Results of engagement | The patient contributor highlighted several key benefits to regular use of hernia belts. They has been wearing a belt since developing a parastomal hernia 6 years ago and described feeling physically secure and contained when wearing a hernia belt. They related that sometimes inadvertently they leave the house without his wallet, keys, or cell phone, but never without his hernia belt. It is integral to the patient They described feeling more confident and secure, both physically and psychologically, when wearing the hernia belt. They stated that it makes the difference between wanting to stay at home and going out and enjoying life. One challenge with wearing the belts is learning how tightly to wear them. The patient noted that they wear a 2-inch belt daily and finds it comfortable, but if they tighten it too much, they develop a sore back. The patient reported having 2 belts, one for everyday use and a larger one that they use while exercising. The larger belt is not comfortable for all-day use but makes a difference while exercising. The larger belt necessitated a fitting from the nurse at a private ostomy clinic, but they can reorder replacements without requiring subsequent refittings. The patient described the financial implications of the need to frequently replace his belts. They need to purchase his hernia belts privately with his ostomy supplies. While the patient has health benefits through his employer that cover the cost, not everyone does and that can be a barrier for people. They replace their regular belt every 2 to 3 months, and his larger exercise belt 1 to 2 times a year. | Conclusions and Implications for Decision- or Policy-Making |
Discussion and conclusions | The patient highlighted several key themes, primarily the physical and psychological benefits, improved quality of life, and ease of use of hernia belts. The patient described significant benefits and limited drawbacks. The main barrier was the financial implication for someone without extended health benefits. Though the belts are not a significant expense, there is the need to replace regularly so that can present an issue for someone who is already struggling to afford their ostomy care supplies. | Conclusions and Implications for Decision- or Policy-Making |
Reflections and critical perspective | The patient contributor was highly engaged and enthusiastic in his participation with CADTH. They were supported in his engagement by a Patient Engagement Officer, and the dialogue was attended by a Research Officer. The introductory and engagement calls were scheduled at the patient’s convenience, accommodating a difference in time zones. The patient was offered the opportunity to be thanked by name in the acknowledgements section of the report but preferred to remain anonymous. An honorarium was offered as a gesture of thanks for his time. One limitation in our approach is that the request was disseminated through a Wound, Ostomy, and Continence nurse. This limited our respondents to individuals receiving those specialized services. While our virtual approach enabled participation from individuals across Canada, the need for patients to have reliable technology and internet access to participate in a Zoom or telephone call potentially excluded some voices. |
Appendix 6: References of Potential Interest
Nonrandomized Studies
Qualitative Studies
Borglit T, Krogsgaard M, Theisen SZ, Juel Rothmann M. Assessment of a support garment in parastomal bulging from a patient perspective: a qualitative study. Int J Qual Stud Health Well-being. 2022;17(1):2039428. PubMed
Winter A, Cusack L, Bolton F, Vickers K, Rushworth L, Salter A. Perceptions and attitudes of ostomates towards support garments for prevention and treatment of parastomal hernia: a qualitative study. Journal of Stomal Therapy Australia. 2022;42(3):19-24.
Hubbard G, Taylor C, Munro J, et al. Experiences of support garments following bowel stoma formation: analysis of free-text responses in a cross-sectional survey. BMJ Open Gastroenterol. 2019;6(1):e000291. PubMed
Guidelines and Recommendations
Unclear Methodology
ASCN Stoma Care: National Clinical Guidelines. Association of Stoma Care Nurses UK. 2016; https://ascnuk.com/_userfiles/pages/files/national_guidelines.pdf. Accessed 2023 Nov 8.
Review Articles
Readding LA. Assessing support garments in the management of parastomal hernia. Gastrointestinal Nursing. 2014;12(4):32-42.
Contributors: Calvin Young, Shannon Hill
ISSN: 2563-6596
The authors would like to sincerely thank the individual who kindly shared his lived experiences and expertise with us, and who preferred to remain anonymous.
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for noncommercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca