CADTH Health Technology Review
Leucovorin Dosing for Gastrointestinal Cancer
Rapid Review
Authors: Khai Tran, Melissa Walter
Key Messages
What Is the Issue?
Since 2008, the shortage of leucovorin has had a significant impact on fluorouracil-based chemotherapy. Many institutions worldwide provided possible options to relieve the leucovorin shortage, including using treatment without leucovorin, lowering the standard leucovorin dose, or using alternative drugs.
If lowering the body surface area-adjusted standard dose of leucovorin does not affect efficacy and safety, then implementation of a low flat-dose protocol may prevent mistakes that result during dose calculation and save pharmacy compounding time and costs.
Decision-makers want to know if any clinical evidence supports a low flat-dose protocol for leucovorin.
What Did We Do?
To inform decisions about using flat-dose leucovorin in conjunction with fluorouracil-based chemotherapy, CADTH sought to identify and summarize literature comparing the clinical effectiveness of flat dosing versus weight-based leucovorin dosing. We also attempted to identify evidence-based recommendations for leucovorin dosing for colorectal or upper gastrointestinal cancer.
A research information specialist conducted a literature search of the peer-reviewed and grey literature with a search strategy focused on leucovorin, dosing, and colorectal or gastrointestinal cancers. The search was limited to English-language documents published since 2013. One reviewer screened articles for inclusion based on predefined criteria, critically appraised the included studies, and narratively summarized the findings.
What Did We Find?
We found 1 small retrospective cohort study (58 patients) comparing low flat-dose 50 mg leucovorin with body surface area-adjusted to high-dose 200 mg/m2 to 500 mg/m2 leucovorin in patients with colorectal cancer. The study found no statistically significant differences between the 2 doses in survival or complication rates.
We found no evidence-based guidelines regarding leucovorin dosing for colorectal or upper gastrointestinal cancer. However, we found several guidelines with unclear methodology reporting leucovorin doses used in different fluorouracil-based regimens.
What Does it Mean?
Limited evidence from this review suggests that the standard weight-based dosing of leucovorin may be reduced to a low flat-dose. However, we require a larger and well conducted trial to confirm the findings of that study.
Decision-makers may wish to consider that reducing the dose of leucovorin may conserve the supply, reduce pharmacy compounding time and control acquisition costs.
Abbreviations
AE
adverse event
BSA
body surface area
FOLFOX
fluorouracil, leucovorin, oxaliplatin
IV
intravenous
OS
overall survival
PFS
progression-free survival
Context and Policy Issues
Colorectal and Gastrointestinal Cancers in Canada
Colorectal cancer represents 11.3% of all 25-year prevalent cancers in Canada.1 It is the third most common cancer type after breast and prostate cancers.1 It is estimated that 1 in 16 men and 1 in 19 women will develop colorectal cancer during their lifetime. One in 34 men and 1 in 40 women will die from it.2 Upper gastrointestinal cancers, including those of the esophagus and stomach, are relatively rare in Canada, but they can be deadly.3 There were 13,555 and 5,100 Canadians diagnosed with stomach and esophagus cancers over the past 25 years, respectively.1 Stomach and esophagus cancers represent the 14th and 19th most common cancer types in Canada, respectively.1
What Is the Current Practice?
There are different treatment options for colorectal and upper gastrointestinal cancer, including surgery, radiation therapy, chemotherapy, targeted therapy, and immunotherapy.4,5 Depending on the stage of colorectal cancer, different treatments may be recommended.4 Surgery is often the first treatment for stage I and II colorectal cancer.4 Radiation therapy and adjuvant chemotherapy may be recommended for some people of stage II and III.4 For stage IV and metastatic colorectal cancers, for which surgery is not an option, various fluorouracil-based chemotherapy regimens are recommended.4 Similarly, the management of gastrointestinal cancers often involves multiple therapies, such as surgery plus chemotherapy, surgery plus radiation therapy, or a combination of all 3, depending on the severity of the disease.5
Fluorouracil was discovered over 6 decades ago as a new class of tumour-inhibitory compounds.6 It is a prodrug that is converted inside the cells to various metabolites that inhibit the enzyme thymidylate synthase responsible for the synthesis of thymidine, a building block of DNA.7 Some metabolites are incorporated into ribonucleic acid (RNA) and interfere with RNA function, or they are incorporated into DNA and break the DNA into fragments.6 It has a broad spectrum of anticancer activity against common solid tumours of the gastrointestinal system, but it does not have a robust anticancer activity when administered alone.6
Leucovorin (or folinic acid) is a folate analogue used to increase the anticancer activity of fluorouracil.6 It forms a stable ternary complex that increases and prolongs the inhibition of thymidylate synthase by fluorouracil.6 In vitro studies suggested that extracellular levels of leucovorin should be at least 10 micromolar for optimal enhancement of fluorouracil cytotoxicity.6 Therefore, clinical studies of leucovorin and fluorouracil for the treatment of cancer patients have generally used large, body surface area (BSA)-adjusted doses of leucovorin (200 to 500 mg/m2) to attain plasma levels of 10 micromolar or higher.6
Why Is it Important to Do This Review?
A shortage of leucovorin first occurred in 2008 and worsened between 2009 and 2012 due to manufacturing delays, thus limiting the supply around the world.8-10 This shortage had a significant impact on fluorouracil-based chemotherapy.11 As a result, many health care organizations were required to use alternative measures, such as reducing the leucovorin dose, using treatment without leucovorin, or switching to levoleucovorin, an active isomer.12,13 Levoleucovorin has demonstrated a similar efficacy and toxicity profile as leucovorin, but concerning cost, leucovorin remains the drug of choice.13,14 Findings from several randomized and nonrandomized studies suggest no difference in efficacy and safety outcomes between body surface area (BSA)-adjusted low-dose (20 mg/m2 to 25 mg/m2) and BSA-adjusted high-dose (200 mg/m2 to 500 mg/m2) leucovorin in fluorouracil-based therapy of colorectal cancer.15-21 However, it is unclear whether offering a flat dose of leucovorin is as safe and effective as BSA-adjusted dosing. From the health system resource management perspective, standardization with flat dosing instead of weight-based dosing may reduce mistakes during dose calculation, simplify treatment protocols, and save pharmacy compounding time and costs.
Objective
The current report aims to summarize evidence regarding the clinical effectiveness of flat dosing versus weight-based dosing of leucovorin for colorectal or upper gastrointestinal cancer. The report also aims to summarize the recommendations from evidence-based guidelines regarding dosing of leucovorin for colorectal or upper gastrointestinal cancer.
Research Questions
What is the clinical effectiveness of flat dosing versus weight-based dosing of leucovorin for colorectal or upper gastrointestinal cancer?
What are the evidence-based guidelines regarding dosing of leucovorin for colorectal or upper gastrointestinal cancer?
Methods
Literature Search Methods
An information specialist conducted a literature search on key resources including MEDLINE, Embase, the Cochrane Database of Systematic Reviews, the International Health Technology Assessment Database, the websites of Canadian and major international health technology agencies, and a focused internet search. The search approach was customized to retrieve a limited set of results, balancing comprehensiveness with relevancy. The search strategy comprised controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. Search concepts were developed based on the elements of the research questions and selection criteria. The main search concepts were leucovorin, dosing, and gastrointestinal cancers. The search was completed on October 16, 2023 and limited to English-language documents published since January 1, 2013.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first screening level, the reviewer reviewed the titles and abstracts and retrieved potentially relevant articles for inclusion. Table 1 presents the inclusion criteria for final selection of full-text articles.
Criteria | Description |
|---|---|
Population | Adults with colorectal or upper gastrointestinal cancer |
Intervention | Q1: Flat dose of leucovorin administered with fluorouracil Q2: Leucovorin administered with fluorouracil |
Comparator | Weight-based dosing of leucovorin administered with fluorouracil |
Outcomes | Q1: Clinical benefits and harms (e.g., safety, mortality, treatment response,) Q2: Recommendations regarding dosing of leucovorin with fluorouracil (e.g., weight-based vs flat dosing, optimal dose) |
Study designs | Health technology assessments, systematic reviews, randomized controlled trials, nonrandomized studies, evidence-based guidelines |
Exclusion Criteria
We excluded articles that did not meet the selection criteria outlined in Table 1, articles published in language other than English, articles published before 2013, or guidelines with unclear methodology.
Critical Appraisal of Individual Studies
One reviewer critically appraised the included publication using the Downs and Black checklist22 for the nonrandomized study. Summary scores were not calculated for the included study; rather, the strengths and limitations of the included publication were described narratively.
Summary of Evidence
Quantity of Research Available
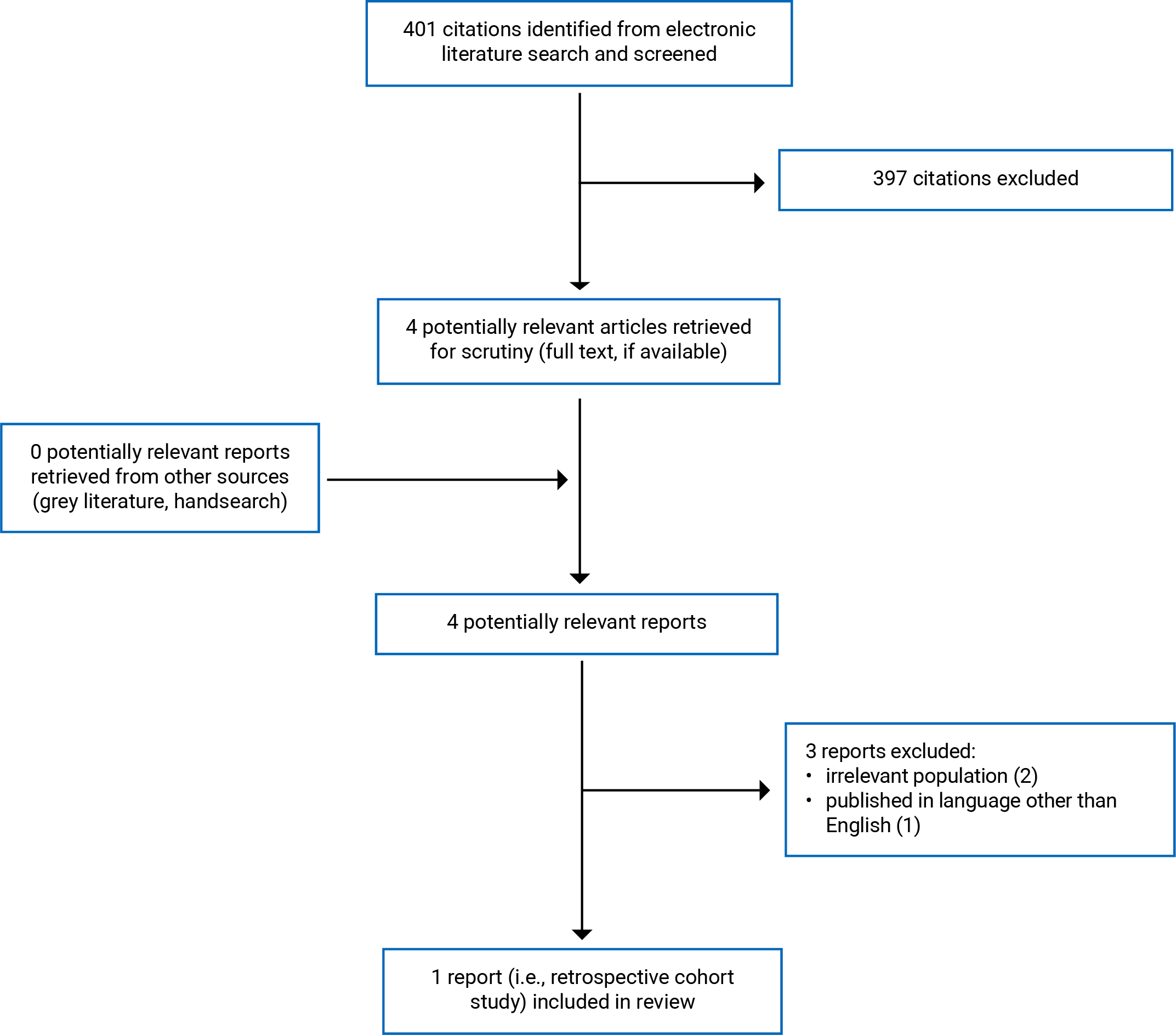
We identified a total of 401 citations from the literature search. Following screening of titles and abstracts, we excluded 397 citations and retrieved 4 potentially relevant reports from the electronic search for full-text review. We did not find any potentially relevant publications from the grey literature search. Of the 4 potentially relevant articles, we excluded 3 publications (2 for irrelevant intervention, and 1 published in language other than English), and included 1 publication, which is a retrospective matched cohort study that met the inclusion criteria. Appendix 1 presents the PRISMA23 flow chart of the study selection. We did not identify any relevant evidence-based guidelines that could be included in this report. However, we identified 13 guidelines with unclear methodology, in which the doses of leucovorin used in different fluorouracil-based regimens for the management of colorectal and gastrointestinal cancers were presented in Table 8 of Appendix 5.
Summary of Study Characteristics
Appendix 2 provides details regarding the characteristics of the included primary study24 (Table 2).
Study Design
The included primary study by Shank et al. (2017)24 was a single-centre, retrospective matched cohort study. Patients were identified from the electronic pharmacy order system if they were prescribed IV (IV) leucovorin. Patient demographic characteristics were collected from each patient’s electronic medical record. The low-dose cohort patients received a flat-dose leucovorin treatment between 1 January 2012 to 31 December 2012. The matched cohort patients received at least 1 BSA-adjusted leucovorin dose from 1 January 2009 to 31 December 2011. The study was published in 2017.
Country of Origin
The included study24 was conducted by authors from US.
Patient Population
The study24 involved adult patients with stage III or stage IV colon cancer or first-line metastatic colorectal cancer receiving fluorouracil-containing therapy. A total of 58 patients were included in the study. Patients’ baseline characteristics were balanced between groups. The median age was around 57 years with a range between 32 to 80 years. Approximately 76% of patients had metastatic disease. Most patients (72.4%) in both groups received surgical resection of primary tumour. The most common regimen was FOLFOX alone (52%) or in combination with bevacizumab (38%). The FOLFOX regimen consists of oxaliplatin, fluorouracil, and leucovorin. Few patients received FOLFIRI regimen alone (3%) or in combination with bevacizumab (7%). The FOLFIRI regimen consists of irinotecan, fluorouracil, and leucovorin.
Interventions and Comparators
Patients in the BSA-adjusted leucovorin group received a treatment regimen of FOLFOX or FOLFIRI, in which the dose of leucovorin range between 200 mg/m2 and 500 mg/m2 per dose IV.24 Patients in the flat-dose group also received a treatment regimen of FOLFOX or FOLFIRI, but the BSA-adjusted dose was replaced by a flat dose of 50 mg IV leucovorin.24
Outcomes
The efficacy outcomes considered in the study24 were progression-free survival (PFS), determined by radiographic evidence of progression, and overall survival (OS). The date of death was collected from medical records. Safety outcomes were adverse events (AEs), whose rates were calculated for each group per cycle. The authors also reported the rates of dose reduction or delay in therapy in patients with severe AEs.
Summary of Critical Appraisal
Table 3 in Appendix 3 presents the strengths and limitations of the included primary study.24
For reporting, the authors of the included study24 clearly described the objective of the study, the main outcomes to be measured, the characteristics of the participants included in the study, the interventions of interest, and the main findings. The authors reported actual P values for the primary outcomes and reported AEs of the intervention.
For external validity, the treatment settings (i.e., hospitals) in the included study24 were representative of the treatment received by most of the patients. However, the patients may not represent the entire population from which they were selected, as the authors of the study24 conducted a chart review of a small sample size from a single hospital.
For internal validity related to bias, the authors24 used statistical tests appropriately to compare variables and assessed the main outcome measures using an accurate and reliable method.
For internal validity related to confounding, most baseline characteristics of the treatment groups appeared balanced, thus reducing the risk of confounding bias. The study's authors did not report whether sample size calculation was performed, and it is unclear whether the non-significant differences in specific outcomes were because the studies were underpowered for those outcomes.
Summary of Findings
Appendix 4 presents the study findings, which were summarized by outcome: PFS (Table 4); OS (Table 5); supportive care for patients with different AEs (Table 6); and other AEs (Table 7).
Clinical Effectiveness of Flat Dosing Versus Weight-Based Dosing of Leucovorin for Colorectal or Upper Gastrointestinal Cancer
Progression-Free Survival
Median PFS was 9.5 months (95% confidence interval [CI] 4.8 to 14.2) in the flat-dose group compared with 8.8 months (95% CI 6.2 to 11.4) in the BSA-adjusted dose group. Between group comparison showed no statistically significant difference (P = 0.254).24
Overall Survival
Median OS was 28 months in the flat-dose group compared with 36.2 months in the BSA-adjusted dose group. There was no statistically significant difference in median OS between groups (P = 0.923).24
Supportive Care in Patients With Different Adverse Events
The authors of the study24 assessed 4 AEs including thrombocytopenia, neutropenia, diarrhea, and mucositis that were severe enough to require dose reduction or delay therapy of the combination of leucovorin and fluorouracil. There were no statistically significant differences between the flat-dose and the BSA-adjusted dose cohorts in the percentage of patients requiring dose reduction or delay in treatment greater than 5 days. There were also no statistically significant differences between groups in hospitalizations due to various conditions such as infection, obstruction, neutropenic fever, and dehydration.
Other Adverse Events
The authors of the study24 documented the percentage of patients with AEs that did not result in dose reduction or delay in treatment without providing any statistical comparisons between groups. The events in the flat-dose group versus BSA-adjusted dose group included neuropathy (21.3% versus 13.2%), nausea (3.5% versus 8.3%), constipation (2.1% versus 0), confusion (0.7% versus 0), fever (0.7% versus 2.1%), and pulmonary embolism (0 versus 0.7%).
Guidelines Regarding Dosing of Leucovorin for Colorectal or Upper Gastrointestinal Cancer
We did not identify any evidence-based guidelines regarding dosing of leucovorin for colorectal or gastrointestinal cancer; therefore, no summary can be provided.
However, we identified 13 guidelines with unclear methodology, in which the doses of leucovorin used in different fluorouracil-based regimens for treatment of colorectal or gastrointestinal cancer were presented in Table 8 of Appendix 5.
Limitations
There is limited evidence regarding comparing a low flat dose with a high BSA-adjusted dose of leucovorin, as 1 relevant study with a sample size of 58 patients was identified from the past 10 years. No evidence was identified regarding such comparison for treating upper gastrointestinal cancer. The included study also had several limitations, including a small sample size (underpowered), retrospective design (risk of selection bias), and inability to measure patient-reported outcomes such as quality of life. It was unclear whether the non-statistically significant differences between groups in survival and safety outcomes were true or whether the study was not powered to detect differences. Selection bias would have occurred if the cohort selected was not representative of all possible patients with the condition of interest in the larger population. The AEs were not graded; thus, the interpretation of AE severity may have varied among providers. Supportive care interventions may also have varied over the study period and from provider preference. Evidence for a flat-dose leucovorin is limited, and evidence-based guidelines informed by a systematic review of evidence and an assessment of the benefits and harms of dose modifications were unavailable.
Conclusions and Implications for Decision- or Policy-Making
We reviewed the clinical evidence of 1 pilot study with small sample size (n = 58), comparing a flat-dose (50 mg) with a BSA-adjusted dose (200 to 500 mg/m2) of leucovorin in patients with colon or metastatic colorectal cancer receiving fluorouracil-containing therapy. We did not identify any evidence-based guideline regarding the dosing of leucovorin for the treatment of colorectal or upper gastrointestinal cancer. We provide a summary table (Table 8 in Appendix 5) presenting the doses of leucovorin used in the fluorouracil-based regimens for treating colorectal or upper gastrointestinal cancers in guidelines with unclear methodology.
For clinical evidence, the included study24 did not detect differences in efficacy (i.e., PFS, OS) or adverse event rates between flat-dose and BSA-adjusted dose groups in patients with colorectal cancer. However, this was a pilot study, which may not be sufficiently powered to detect differences. A larger and well conducted trial would be needed to confirm the findings of this study.
Notably, a systematic review and meta-analysis exists25 comparing low-dose (20 mg/m2 to 50 mg/m2) versus high-dose (200 mg/m2 to 500 mg/m2) BSA-adjusted leucovorin in patients with metastatic colorectal cancer. The results of the meta-analyses revealed a nonsignificant difference between groups in median survival time, tumour response rate, and hematological and nonhematological toxicities.25 In addition, the large QUASAR RCT26 (N = 4,927) comparing a low flat-dose (25 mg) with a high flat-dose (175 mg) of leucovorin in patients with stage I to stage III colorectal cancer reported no significant difference in recurrence and survival rates after 3 years of follow-up. Since those studies did not compare flat dosing with BSA-adjusted dosing of leucovorin, they did not meet our inclusion criteria, and we excluded them from the analysis in this report; however, they may provide some insight on the potential effectiveness of low, flat-dose leucovorin. For example, if the average BSAs of adult men and women are 1.9 m2 and 1.6 m2, respectively,27 then a low dose of 20 mg to 50 mg/m2 would translate to a flat dose of 38 mg to 95 mg for men and 32 mg to 80 mg for women with metastatic colorectal cancer. Thus, the findings in those studies may provide additional support to the decision to reduce the dose of leucovorin for treatment of colorectal or gastrointestinal cancers in patients receiving fluorouracil-containing therapy.
Most of the non-evidence-based guidelines (Table 8 in Appendix 5) present different fluorouracil-based regimens with BSA-adjusted dose of leucovorin ranging from 200 to 500 mg/m2. With the few regimens containing only fluorouracil and leucovorin, the leucovorin dose was used at 20 mg/m2 to 25 mg/m2. The Australian eviQ guidelines present a treatment protocol using a modified FOLFOX6 regimen, in which the dose of oxaliplatin and leucovorin have been modified from the original clinical trial doses (i.e., 100 mg/m2 to 85 mg/m2 for oxaliplatin and 200 mg/m2 to 50 mg flat-dose for leucovorin). Evidence supporting the recommendations to reduce leucovorin dosing in those guidelines was unclear. Despite limited evidence on the clinical effectiveness of low flat-dose leucovorin identified in this report, collective evidence from the systematic review and meta-analysis25 and some non-evidence-based guidelines suggest that flat low-dose leucovorin regimens appear to be feasible approaches for colorectal cancer treatment with the purpose to relieve the leucovorin shortage and to reduce pharmacy compounding time and acquisition costs.
References
1.Canadian Cancer Statistics - A 2022 special report on cancer prevalence. Toronto (ON): Canadian Cancer Society; 2022: https://cdn.cancer.ca/-/media/files/research/cancer-statistics/2022-statistics/2022-special-report/2022_prevalence_report_final_en.pdf. Accessed 2023 Oct 25.
2.Canadian Cancer Society. Colorectal cancer statistics. 2022; https://cancer.ca/en/cancer-information/cancer-types/colorectal/statistics. Accessed 2023 Oct 25.
3.Kim A. Stomach, pancreatic and other upper GI cancers: new findings are providing much-needed treatment guidance. Sunnybrook Research Institute 2016; https://sunnybrook.ca/research/content/?page=sri-magazine-2016-gi-gancers-new-findings. Accessed 2023 Oct 25.
4.Cancer.Net. Colorectal Cancer: Types of Treatment. 2022; https://www.cancer.net/cancer-types/colorectal-cancer/types-treatment. Accessed 2023 Nov 9.
5.Rupawala A. Gastrointestinal Cancers. American College of Gastroenterology 2021; https://gi.org/topics/gastrointestinal-cancers/. Accessed 2023 Nov 9.
6.DeLap RJ. The effect of leucovorin on the therapeutic index of fluorouracil in cancer patients. Yale J Biol Med. 1988;61(1):23-34. PubMed
7.Midgley RS, Kerr DJ. ABC of colorectal cancer: adjuvant therapy. BMJ. 2000;321(7270):1208-1211. PubMed
8.McBride A, Holle LM, Westendorf C, et al. National survey on the effect of oncology drug shortages on cancer care. Am J Health Syst Pharm. 2013;70(7):609-617. PubMed
9.Gatesman ML, Smith TJ. The shortage of essential chemotherapy drugs in the United States. N Engl J Med. 2011;365(18):1653-1655. PubMed
10.Devi S. US drug shortages could continue for years. Lancet. 2012;379(9820):990-991. PubMed
11.Thirion P, Michiels S, Pignon JP, et al. Modulation of fluorouracil by leucovorin in patients with advanced colorectal cancer: an updated meta-analysis. J Clin Oncol. 2004;22(18):3766-3775. PubMed
12.Traynor K. FDA approves levoleucovorin. Am J Health Syst Pharm. 2008;65(8):686. PubMed
13.Hayes MS, Ward MA, Slabaugh SL, Xu Y. Lessons from the leucovorin shortages between 2009 and 2012 in a medicare advantage population: where do we go from here? Am Health Drug Benefits. 2014;7(5):264-270. PubMed
14.Chuang VT, Suno M. Levoleucovorin as replacement for leucovorin in cancer treatment. Ann Pharmacother. 2012;46(10):1349-1357. PubMed
15.Jäger E, Heike M, Bernhard H, et al. Weekly high-dose leucovorin versus low-dose leucovorin combined with fluorouracil in advanced colorectal cancer: results of a randomized multicenter trial. Study Group for Palliative Treatment of Metastatic Colorectal Cancer Study Protocol 1. J Clin Oncol. 1996;14(8):2274-2279. PubMed
16.O'Connell MJ. A phase III trial of 5-fluorouracil and leucovorin in the treatment of advanced colorectal cancer. A Mayo Clinic/North Central Cancer Treatment Group study. Cancer. 1989;63(6 Suppl):1026-1030. PubMed
17.Petrelli N, Douglass HO, Jr., Herrera L, et al. The modulation of fluorouracil with leucovorin in metastatic colorectal carcinoma: a prospective randomized phase III trial. Gastrointestinal Tumor Study Group. J Clin Oncol. 1989;7(10):1419-1426. PubMed
18.Poon MA, O'Connell MJ, Wieand HS, et al. Biochemical modulation of fluorouracil with leucovorin: confirmatory evidence of improved therapeutic efficacy in advanced colorectal cancer. J Clin Oncol. 1991;9(11):1967-1972. PubMed
19.Ychou M, Fabbro-Peray P, Perney P, et al. A prospective randomized study comparing high- and low-dose leucovorin combined with same-dose 5-fluorouracil in advanced colorectal cancer. Am J Clin Oncol. 1998;21(3):233-236. PubMed
20.Reynolds J, Chamberland-Tremblay A, Herrington JD, Munoz Maldonado Y, Wong L. High- versus low-dose leucovorin in the modified FOLFOX6 regimen for first-line treatment of metastatic colorectal cancer. J Oncol Pharm Pract. 2017;23(3):173-178. PubMed
21.Buroker TR, O'Connell MJ, Wieand HS, et al. Randomized comparison of two schedules of fluorouracil and leucovorin in the treatment of advanced colorectal cancer. J Clin Oncol. 1994;12(1):14-20. PubMed
22.Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377-384. PubMed
23.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
24.Shank BR, Seung AH, Kinsman K, Newman MJ, Donehower RC, Burton B. Effects of the leucovorin shortage: Pilot study investigating cost, efficacy, and toxicity comparison of low fixed-dose versus body surface area-adjusted leucovorin dosing in patients with resectable colon or metastatic colorectal cancer. J Oncol Pharm Pract. 2017;23(3):163-172. PubMed
25.Hsu CY, Chen CY, Lin YM, Tam KW. Efficacy and safety of high-dose vs low-dose leucovorin in patients with colorectal cancer: systematic review and meta-analysis. Colorectal Dis. 2020;22(1):6-17. PubMed
26.Comparison of fluorouracil with additional levamisole, higher-dose folinic acid, or both, as adjuvant chemotherapy for colorectal cancer: a randomised trial. QUASAR Collaborative Group. Lancet. 2000;355(9215):1588-1596. PubMed
27.Mosteller RD. Simplified calculation of body-surface area. N Engl J Med. 1987;317(17):1098. PubMed
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Note that this appendix has not been copy-edited.
Table 2: Characteristics of Included Primary Study
Study citation, country, funding source | Study design | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Shank et al. (2017)24 US Funding source: The authors indicated that they received no financial support for the research, authorship, and/or publication of this article | A single-centre, retrospective matched cohort study | Adult patients with stage III or stage IV colon cancer or first-line mCRC receiving fluorouracil-containing therapy. Median age (IQR), years:
% Male/female:
Stage at diagnosis:
Received surgical resection of primary tumour:
Patients with metastatic disease:
Initial regimen:
| Intervention: Flat-dose leucovorin 50 mg IV (n = 29) Comparator: BSA-adjusted leucovorin 200 mg/m2 to 500 mg/m2 per dose (n = 29) | Outcomes:
Follow-up: NR |
AE = adverse event; BSA = body surface area; IQR = interquartile range; IV = IV; mCRC = metastatic colorectal cancer; NR = not reported; OS = overall survival; PFS = progression-free survival.
aFOLFOX: Oxaliplatin 85 mg/m2 IV on day 1, fluorouracil 400 mg/m2 IV bolus over 1 hour on day 1, followed by 2,400 mg/m2 IV over 46 to 48 hour as a continuous infusion, and leucovorin 200 to 500 mg/m2 IV on day 1 repeated every 2 weeks.
bFOLFIRI: Irinotecan 180 mg/m2 IV on day 1, fluorouracil 400 mg/m2 IV bolus over 1 hour on day 1, followed by 2,400 mg/m2 IV over 46 to 48 hour as a continuous infusion, and leucovorin 200 mg/m2 to 500 mg/m2 IV on day 1 repeated every 2 weeks.
Appendix 3: Critical Appraisal of Included Publications
Note that this appendix has not been copy-edited.
Table 3: Strengths and Limitations of Clinical Study Using the Downs and Black Checklist22
Strengths | Limitations |
|---|---|
Shank et al. (2017)24 | |
Reporting:
External validity:
Internal validity – bias:
Internal validity – confounding:
| External validity:
Internal validity – bias:
Internal validity – confounding:
|
Appendix 4: Main Study Findings
Note that this appendix has not been copy-edited.
Table 4: Summary of Findings by Outcome — Progressive Free Survival
Dose of leucovorin | Median PFS | 95% CI | P value |
|---|---|---|---|
Flat-dose | 9.5 months | 4.8 to 14.2 months | 0.254 |
BSA-adjusted dose | 8.8 months | 6.2 to 14.1 months |
BSA = body surface area; CI = confidence interval; PFS = progressive free survival.
Table 5: Summary of Findings by Outcome — Overall Survival
Dose of leucovorin | Median OS | 95% CI | P value |
|---|---|---|---|
Flat-dose | 28 months | NR | 0.923 |
BSA-adjusted dose | 36.2 months | NR |
BSA = body surface area; CI = confidence interval; NR = not reported; OS = overall survival.
Table 6: Summary of Findings by Outcome — Supportive Care for Patients with Different Adverse Events
Adverse events and Supportive care | Flat-dose | BSA-adjusted dose | OR (95% CI) | P value |
|---|---|---|---|---|
Thrombocytopenia | ||||
Dose reduction | 15.6% | 9.7% | 1.72 (0.84 to 3.51) | 0.13 |
Delay in treatment > 5 days | 9.2% | 5.6% | 1.73 (0.69 to 4.30) | 0.24 |
Neutropenia | ||||
Dose reduction | 10.6% | 18.1% | 0.54 (0.27 to 1.07) | 0.07 |
Delay in treatment > 5 days | 11.3% | 8.3% | 1.41 (0.64 to 3.09) | 0.39 |
Diarrhea | ||||
Dose reduction | 3.5% | 1.4% | 2.61 (0.50 to 13.68) | 0.23 |
Delay in treatment > 5 days | 0.7% | 0.7% | 1.02 (0.06 to 16.49) | 0.99 |
Mucositis | ||||
Dose reduction | 0 | 1.4% | NR | NR |
Delay in treatment > 5 days | 0 | 0.7% | NR | NR |
Hospitalized | ||||
Infection | 0.7% | 2.8% | 0.25 (0.03 to 2.26) | 0.18 |
Obstruction | 2.1% | 0.7% | 3.11 (0.32 to 30.25) | 0.30 |
Neutropenic fever | 0 | 2.8% | NR | 0.12 |
Dehydration | 0 | 1.4% | NR | 0.50 |
CI = confidence interval; H = high-dose leucovorin regimen; L = low-dose leucovorin regimen; NR = not reported; NS = not statistically significant; OR = odds ratio; RCT = randomized controlled trial.
Table 7: Summary of Findings by Outcome — Other Adverse Events
Adverse events | Flat-dose | BSA-adjusted dose |
|---|---|---|
Neuropathy | 21.3% | 13.2% |
Nausea | 3.5% | 8.3% |
Constipation | 2.1% | 0 |
Confusion | 0.7% | 0 |
Fever | 0.7% | 2.1% |
Pulmonary embolism | 0 | 0.7% |
Appendix 5: References of Potential Interest
Note that this appendix has not been copy-edited.
Guidelines With Unclear Methodology
Table 8 summarizes the doses of leucovorin used in the fluorouracil-based regimens for treatment of gastrointestinal cancer in guidelines with unclear methodology.
Table 8: Summary of Leucovorin Doses in Different Fluorouracil-Based Regimens
Guidelines | Condition | Fluorouracil-based regimens | Leucovorin dose | Route of administration |
|---|---|---|---|---|
Advanced or metastatic disease | FOLFOX6 (modified) | 400 mg/m2 | IV on day 1 | |
FOLFOX7 (modified) | 400 mg/m2 | IV on day 1 | ||
FOLFIRI | 400 mg/m2 | IV on day 1 | ||
FOLFIRINOX | 400 mg/m2 | IV on day 1 | ||
Roswell Park regimen (Bolus or infusional 5-fluorouracil/leucovorin) | 500 mg/m2 | IV over 2 hours, days 1, 8, 15, 22, 29, and 36 | ||
NCCN – Esophageal and Esophagogastric Junction Cancers, 2023 | Unresectable locally advanced, recurrent, or metastatic disease | FOLFOX (for perioperative chemotherapy; for definitive chemoradiation; for postoperative systemic therapy; for first-line therapy of HER2 overexpression positive adenocarcinoma; for MSI-H/dMMR tumours) | 400 mg/m2 | IV on day 1 |
FOLFIRI | 400 mg/m2 | IV on day 1 | ||
FLOT (for perioperative chemoradiation) | 200 mg/m2 | IV on day 1 | ||
Unresectable locally advanced, recurrent, or metastatic disease | FLOT (for perioperative chemotherapy) | 200 mg/m2 | IV on day 1 | |
FOLFOX (for perioperative chemotherapy; for perioperative chemoradiation; for postoperative chemoradiation; for postoperative chemotherapy; for chemoradiation for unresectable disease; for first-line therapy of HER2 overexpression positive adenocarcinoma; for MSI-H/dMMR tumours) | 200 mg/m2, 400 mg/m2 | IV on day 1 | ||
FOLFIRI (for second-line and subsequent therapy) | 400 mg/m2 | IV on day 1 | ||
Metastatic cancer | FOLFCIS | 400 mg/m2 | IV on day 1 | |
FOLFOX6 (modified) | 400 mg/m2 | IV on day 1 | ||
Unresectable locally advanced, recurrent, or metastatic disease | FOLFOX6 (modified) (for perioperative chemotherapy; | 400 mg/m2 | IV on day 1 | |
FOLFOX7 (modified) | 400 mg/m2 | IV on day 1 | ||
FOLFIRI | 400 mg/m2 | IV on day 1 | ||
FOLFIRINOX | 400 mg/m2 | IV on day 1 | ||
Roswell Park regimen (Bolus or infusional 5-fluorouracil/leucovorin) | 500 mg/m2 | IV over 2 hours, days 1, 8, 15, 22, 29, and 36 | ||
Unresectable locally advanced, recurrent, or metastatic disease | FOLFOX6 (modified) | 400 mg/m2 | IV on day 1 | |
5-FU/LV | 400 mg/m2 | IV on day 1 | ||
FOLFOX7 (modified) | 400 mg/m2 | IV on day 1 | ||
FOLFIRI | 400 mg/m2 | IV on day 1 | ||
FOLFIRINOX (modified) | 400 mg/m2 | IV on day 1 | ||
Roswell Park regimen 5-FU/LV | 500 mg/m2 | IV over 2 hours, days 1, 8, 15, 22, 29, and 36 | ||
Simplified biweekly infusional 5-FU/LV | 500 mg/m2 | IV over 2 hours on day 1 | ||
Weekly infusional 5-FU/LV | 20 mg/m2 | IV over 2 hours on day 1 | ||
Colon cancer | FOLFOX6 (modified) | 50 mg flat dose | IV bolus | |
QUASAR (modified) – Weekly infusional 5-FU/LV | 50 mg flat dose | IV bolus | ||
Saskatchewan guidelines – Esophageal Cancer and Gastro-esophageal Junction Cancer, 2018 | Gastro-esophageal junction adenocarcinoma | 5-FU/LV | 20 mg/m2 | IV day 1 to 5 |
Localized cancer, unresectable advanced, or metastatic disease | Biweekly infusional 5-FU/LV | 400 mg/m2 | IV on day 1 | |
Roswell Park regimen 5-FU/LV | 500 mg/m2 | IV over 2 hours | ||
Mayo clinic regimen 5-FU/LV | 20 mg/m2 to 25 mg/m2 per day | IV bolus day 1 to 5 | ||
FOLFOX6 (modified) | 400 mg/m2 | IV on day 1 | ||
Metastatic colon cancer | FOLFIRI | 400 mg/m2 | IV on day 1 | |
FOLFOX6 (modified) | 400 mg/m2 | IV on day 1 | ||
FOLFIRINOX | 400 mg/m2 | IV on day 1 | ||
Simplified biweekly infusional 5-FU/LV | 500 mg/m2 | IV over 2 hours on day 1 | ||
Gastric cancer | FLOT (for perioperative chemotherapy) | 200 mg/m2 | IV over 2 hours on day 1 | |
5-FU/LV + radiotherapy | 20 mg/m2 | IV | ||
5-FU/LV (de Gramont) | 100 mg/m2 | IV over 2 hours | ||
FOLFOX | 400 mg/m2 | IV | ||
FOLFIRI | 400 mg/m2 | IV | ||
Esophageal cancer | FLOT (for perioperative chemotherapy) | 200 mg/m2 | IV over 2 hours on day 1 | |
Unresectable esophageal cancer | FOLFOX | 200 mg/m2 | IV |
dMMR = MSI-H or mismatch repair deficient; 5-FU = 5-fluorouracil; FLOT = fluorouracil, leucovorin, oxaliplatin, docetaxel; FOLFIRI = fluorouracil, leucovorin, irinotecan; FOLFIRINOX = fluorouracil, leucovorin, irinotecan, oxaliplatin; FOLFCIS = fluorouracil, leucovorin, cisplatin; FOLFOX = fluorouracil, leucovorin, oxaliplatin; IV = IV; LV = leucovorin; MSI-H = microsatellite instability-high; NCCN = National Comprehensive Cancer Network.
Note: eviQ is an Australian Government, freely available online resource of cancer treatment protocols developed by multidisciplinary teams of cancer specialists.
Systematic Review
Hsu CY, Chen CY, Lin YM, Tam KW. Efficacy and safety of high-dose vs low-dose leucovorin in patients with colorectal cancer: systematic review and meta-analysis. Colorectal Dis. 2020;22(1):6-17. PubMed
Randomized Controlled Trial
Comparison of fluorouracil with additional levamisole, higher-dose folinic acid, or both, as adjuvant chemotherapy for colorectal cancer: a randomised trial. QUASAR Collaborative Group. Lancet. 2000;355(9215):1588-1596. PubMed
Contributors: Elizabeth Carson, Camille Santos
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-ma//king process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for noncommercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca