CADTH Health Technology Review
Routine Dental Polishing for Oral Health
Rapid Review
Authors: Kendra Brett, Jennifer Horton
Key Messages
What Is the Issue?
Professional dental care is important to help maintain oral health. Routine dental cleaning usually includes both scaling and polishing. Scaling is the removal of plaque and tartar from the crown and root surfaces of teeth. Polishing is the removal of residual plaque and external stains from the teeth.
To support decisions about the optimal components for professional dental cleaning, it is important to understand the potential benefits and harms of routine dental polishing when compared to no routine dental polishing.
What Did We Do?
We searched for clinical and cost-effectiveness literature comparing routine dental polishing with no routine dental polishing. We also looked for evidence-based guidelines that provide recommendations about the use of routine dental polishing for the maintenance of oral health in adults and children.
An information specialist conducted a search of peer-reviewed and grey literature sources published between January 1, 2018, and September 28, 2023.
Documents were excluded if we could not isolate the effects of dental polishing from other dental procedures or if polishing techniques were used for a purpose other than the routine polishing of teeth.
What Did We Find?
We did not find any studies directly evaluating the clinical or cost-effectiveness of routine dental polishing versus no routine dental polishing, or guidelines about the use of routine dental polishing, that met the inclusion criteria for this review.
We identified limited literature that examines the combined effects of routine scaling and polishing. Research is needed that distinguishes the effects of routine dental polishing from the effects of other dental procedures.
What Does This Mean?
Without comparative clinical or cost-effectiveness evidence about routine dental polishing versus no routine dental polishing, decision-makers may also wish to consider that patients value routine scaling and polishing, and that the cost of dental care may be a barrier to visiting the dentist for some people.
New polishing methods, such as air powder polishing, may also be useful to consider when making decisions about routine polishing to support dental health. These methods include some of the benefits of scaling and may present opportunities to reduce periodontal inflammation or the length of a dental appointment.
Research Questions
What is the clinical effectiveness of routine dental polishing for the maintenance of oral health in adults and children?
What is the cost-effectiveness of routine dental polishing for the maintenance of oral health in adults and children?
What are the evidence-based guidelines regarding the use of routine dental polishing for the maintenance of oral health in adults and children?
Context and Policy Issues
What Is Oral Health?
The health of the mouth (i.e., oral health) includes the ability to chew, taste, swallow, speak, and convey facial expressions, without pain or disease of the mouth.1 Risk factors for poor oral health include age, diabetes, some medications, and lifestyle factors, such as alcohol, a diet that is high in sugar, tobacco, and poor oral hygiene.2
Oral health is part of overall health and well-being, and periodontal (gum) disease can be a risk factor for other conditions, such as cardiovascular disease, cancer, dementia, and poor pregnancy outcomes.3
Two common periodontal diseases are gingivitis and periodontitis. Gingivitis is the inflammation of the gums and is the most common form of periodontal disease.3 Periodontitis includes inflammation of the gums, the loss of tissue and bone that surround and support the teeth, and eventual tooth loss.3
Dental plaque (also known as bacterial biofilm) is a common cause of periodontal diseases. Plaque is a dense, nonmineralized mass of bacterial colonies in a gel-like matrix that forms at, above, and below the gum line. If plaque is not removed it will harden (or mineralize) and form tartar (i.e., hardened plaque deposits; also known as calculus).3 Effective ways to remove plaque are regular toothbrushing and flossing and routing dental cleanings.3
The Canadian Dental Association developed 5 steps to maintain oral health and help prevent oral diseases.2,4 Briefly, these steps include:
practice good oral hygiene (e.g., brushing your teeth twice a day; flossing at least once a day)
eat a balanced and nutritious diet (e.g., limit sugar consumption)
check your mouth regularly (e.g., check for signs of gum disease)
limit alcohol and avoid smoking, smokeless tobacco, and vaping
visit your dentist regularly for routine preventive dental care (i.e., clinical exam and dental cleanings).
What Does Professional Dental Cleaning Involve?
Routine professional dental cleaning typically includes scaling and polishing by a dentist or dental hygienist to remove plaque and tartar.5
Scaling is the mechanical removal of plaque, tartar, and debris from the crown and root surfaces of the teeth. It is typically done with hand or ultrasonic instruments.5
Polishing is the mechanical removal of residual extrinsic stains and plaque deposits on teeth above the gum line. Polishing also smooths the surface of the teeth and makes them look clean.6 There are 2 routine polishing methods:6
Rubber cup polishing: A slow drill with a rubber cup or bristle brush is loaded with an abrasive polishing paste and applied to the teeth to scrub away stains and plaque.
Air powder polishing: A slurry of water and baking soda is applied to the teeth using air and water pressure to polish the teeth. Air polishing can also be conducted with other powders (e.g., glycine).
Why Is It Important to Do This Review?
Routine dental visits can help detect and prevent oral health problems, but not all people in Canada have equal access to professional preventive dental care. Coverage for dental care services varies across Canada, and visits to dental health professionals are usually covered through insurance plans (private or job-based), through government-funded programs, or may need to be paid out of pocket.7 For many people, cost can be a barrier to visiting the dentist. In 2018 in Canada, 22.4% of people avoided visiting the dentist due to cost.7 Members of certain groups may also have inequitable access to professional dental care, including those in lower income households, members of the Black community, Indigenous people, rural or remote residence, and those without dental insurance.7-10
To improve access to dental care services, the federal government is working on the Canadian Dental Care Plan, which will provide dental care coverage for uninsured people in Canada with a household income of less than $90,000 a year.11 The Canada Dental Benefit was developed as an interim step to help lower dental costs for eligible families while the details of the Canadian Dental Care Plan are established.12 The details on the Canadian Dental Care Plan are expected to be available starting at the end of 2023 or in 2024,11 and it is unknown whether there may still be barriers for dental care coverage with the plan or before the plan is fully implemented.
Dental care that improves the look and feel of the teeth and reduces bleeding at the gums is important to patients.13 The general population values scaling and polishing,13 and routine dental care generally includes scaling in conjunction with polishing. However, the potential clinical benefits and harms of these procedures should be examined separately given the different functions of scaling and polishing. To support decisions about the optimal components for professional dental cleaning, it is important to understand the potential benefits and harms of routine dental polishing when compared to no routine dental polishing. Comparative clinical and cost-effectiveness evidence and guidelines about the use of routine dental polishing may provide useful context to inform decisions around routine dental care for the maintenance of oral health.
Objective
The purpose of this report is to summarize and critically appraise the evidence identified from medical databases and grey literature searching about the clinical and cost-effectiveness of routine dental polishing versus no routine dental polishing for the maintenance of oral health. We also aimed to identify evidence-based guidelines about routine dental polishing in adults and children.
Methods
Literature Search Methods
An information specialist conducted a literature search on key resources including MEDLINE, the Cochrane Database of Systematic Reviews, the International HTA Database, and the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search approach was customized to retrieve a limited set of results, balancing comprehensiveness with relevancy. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. Search concepts were developed based on the elements of the research questions and selection criteria. The main search concepts were dental cleaning, dental deposits, and oral disease. CADTH-developed search filters were applied to limit retrieval to health technology assessments, systematic reviews, meta-analyses, or indirect treatment comparisons; any types of clinical trials or observational studies; economic studies; and guidelines. The search was completed on September 28, 2023, and limited to English-language documents published since January 1, 2018.
Selection Criteria and Methods
One reviewer screened citations and selected studies. First, we screened titles and abstracts and retrieved potentially relevant articles, then we assessed full-text articles for inclusion based on the criteria in Table 1.
Criteria | Description |
|---|---|
Population | Pediatric and adult populations |
Intervention | Routine dental polishing at planned, regular intervals (e.g., every 6 months) |
Comparator | Q1 and Q2: No dental polishing Q3: Not applicable |
Outcomes | Q1: Clinical benefits (e.g., incidence of dental caries or periodontal disease, calculus and plaque, tooth lose, oral health-related quality of life) and harms (e.g., adverse events) Q2: Cost-effectiveness (e.g., cost per QALY gained) Q3: Recommendations regarding best practices (e.g., appropriate patient populations, treatment protocols and intervals, contraindications) |
Study designs | Health technology assessments, systematic reviews, randomized controlled trials, nonrandomized studies, economic evaluations, evidence-based guidelines |
QALY = quality-adjusted life-year.
Exclusion Criteria
We excluded articles if they did not meet the criteria in Table 1, they were duplicate publications, or were published before 2018.
Studies were excluded if:
the effect of dental polishing could not be isolated from the other interventions (e.g., studies that examined the combined effects of routine scaling and polishing were excluded)
the intervention was used for a purpose other than the routine polishing of teeth (e.g., treating periodontal pockets, procedures performed during dental surgery, polishing root surfaces, removing subgingival (below the gum) biofilm)
the study design did not reflect routine dental practices (e.g., extracted teeth).
Guidelines with unclear methodology were also excluded.
Summary of Evidence
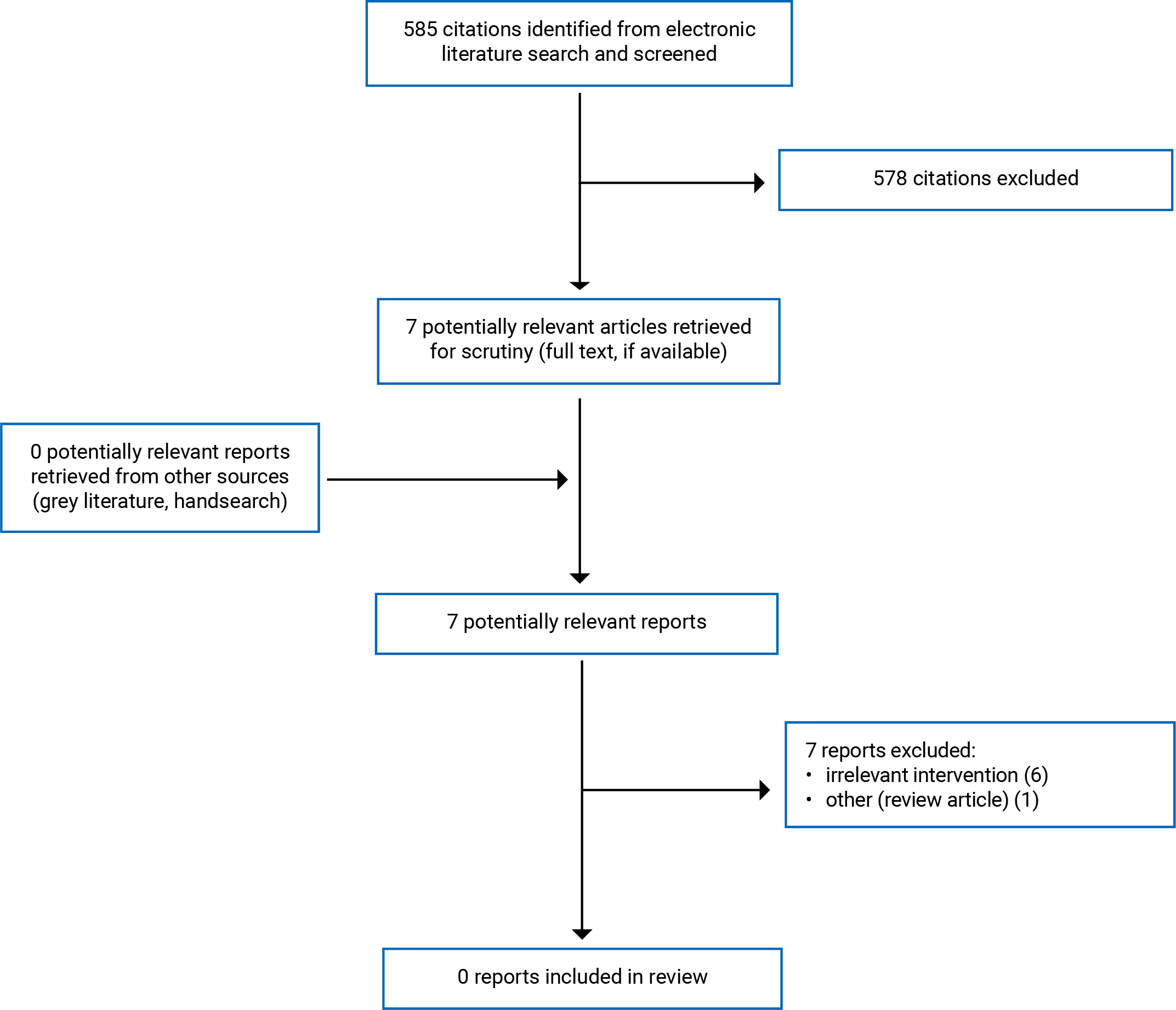
Quantity of Research Available
No relevant studies were identified that meet the criteria for this review. Appendix 1 presents the study selection details. Appendix 2 lists additional references of potential interest.
Summary of Findings
We searched for documents published between January 1, 2018, and September 28, 2023, and screened literature search results based on the research questions and inclusion criteria in Table 1. In this search, there were no studies or evidence-based guidelines meeting those criteria. Therefore, we could not provide a summary on the clinical effectiveness or cost-effectiveness of routine dental polishing compared to no dental polishing, nor could we provide recommendations regarding the use of routine dental polishing for the maintenance of oral health in adults and children.
Limitations
No eligible studies evaluating the clinical or cost-effectiveness of routine dental polishing versus no dental polishing, and no evidence-based guidelines about routine dental polishing were identified through a search of medical databases and grey literature. We are unable to comment on the quality of evidence in this area as no studies or guidelines met the inclusion criteria for this review. This report was focused on the potential benefits and harms of routine dental polishing; however, the majority of the existing literature (as summarized in a Cochrane Systematic Review published in 201814) examines the combined effects of routine scaling and polishing, which were excluded from this report. In line with Rapid Review methodology, which balances rigour with timeliness, the literature search conducted to inform this report was limited to 5 years (January 1, 2018, to September 28, 2023). It is possible that relevant literature regarding routine dental polishing alone for the maintenance of oral health exists, but was published more than 5 years ago, and therefore excluded by the date-limited search. However, there are no clear indications from scoping that there is abundant literature about routine polishing, either alone or combined with routine scaling.
Conclusions
Based on the literature search conducted for this review, we did not identify any evidence about the clinical or cost-effectiveness or evidence-based guidelines regarding the use of routine dental polishing for the maintenance of oral health in adults or children that met the inclusion criteria for this report. Without comparative evidence and recommendations from evidence-based guidelines, we are not able to conclude whether routine dental polishing is more beneficial than not receiving routine dental polishing for the maintenance of oral health.
Routine dental cleaning usually includes both scaling and polishing, and research in this field often examines the combined effects of both procedures. Still, there are indications that the body of clinical effectiveness evidence for routine polishing is limited, even when evaluating combined polishing and scaling. The 2018 Cochrane systematic review only identified 2 relevant randomized controlled trials of routine scaling and polishing for periodontal health.14 When scaling and polishing provided every 6 or 12 months over 2 to 3 years was compared to no scheduled treatments, the systematic review reported a small reduction in tartar, little-to-no difference in gingivitis or quality of life, and potentially little or no difference in plaque levels.14 To better inform decisions around routine dental polishing for the maintenance of oral health and to clarify the contributions of polishing to oral health care, researchers should consider conducting studies that would allow the effects of routine dental polishing to be isolated from the effects of other dental procedures.
In addition to routine polishing, air powder polishing with glycine, trehalose, or erythritol powder has also been explored as an alternative to hand and ultrasonic scaling to reduce periodontal inflammation.15 Air powder polishing with these particles may be more comfortable for patients and could reduce the length of the appointment time.15 However, as polishing only removes plaque (biofilm) but not tartar (calculus), it has been suggested that air powder polishing be provided in combination with hand scaling during initial therapy, or alone to treat residual periodontal pockets (after initial therapy), or as part of supportive periodontal therapy (i.e., dental care provided after periodontitis has been treated satisfactorily).15 Furthermore, there are numerous studies comparing the effectiveness of different types of polishing techniques (e.g., rubber cup method, erythritol powder air polishing) for biofilm removal (refer to Appendix 2), which may further support decisions for oral health care.
Routine dental care typically involves both scaling and polishing, and decisions-makers should consider that patients value dental care that improves the look and feel of their teeth (i.e., polishing to remove stains and scaling to remove plaque and tartar),13 and that cost might be a barrier to visiting the dentist for some people,7 including those in lower income households or people who are uninsured.
References
1.FDI World Dental Federation. FDI’s definition of oral health. https://www.fdiworlddental.org/fdis-definition-oral-health. Accessed 2023 Oct 06.
2.Canadian Dental Association. Your Oral Health. 2023; https://www.cda-adc.ca/en/oral_health/index.asp. Accessed 2023 Oct 06.
3.Wilder RS, Moretti AJ. Overview of gingivitis and periodontitis in adults. In: Post TW, ed. UpToDate. Waltham (MA): UpToDate; 2023: https://www.uptodate.com/. Accessed 2023 Oct 10.
4.Canadian Dental Association. 5 Steps to a Healthy Mouth. 2023; https://www.cda-adc.ca/en/oral_health/cfyt/good_for_life/default.asp. Accessed 2023 Oct 06.
5.Ontario Dental Association. Common Dental Procedures. 2023; https://www.oda.ca/oral-health-basics/dental-procedures/common-dental-procedures/. Accessed 2023 Oct 06.
6.Brennan D. What to Know About Dental Polishing. 2021; https://www.webmd.com/oral-health/what-to-know-about-dental-polishing. Accessed 2023 Oct 06.
7.Statistics Canada. Dental Care, 2018. 2019; https://www150.statcan.gc.ca/n1/pub/82-625-x/2019001/article/00010-eng.htm. Accessed 2023 Oct 06.
8.Gordon NP, Mosen DM, Banegas MP. Oral Health Care: A Missing Pillar of Total Health Care? Perm. 2021;25(12):03.
9.De Rubeis V, Jiang Y, de Groh M, et al. Barriers to oral care: a cross-sectional analysis of the Canadian longitudinal study on aging (CLSA). BMC Oral Health. 2023;23(1):294. PubMed
10.Hussain A, Jaimes SB, Crizzle AM. Predictors of self-rated oral health in Canadian Indigenous adults. BMC Oral Health. 2021;21(1):430. PubMed
11.Government of Canada. The Government of Canada announces progress on the Canadian Dental Care Plan. 2023; https://www.canada.ca/en/public-services-procurement/news/2023/09/the-government-of-canada-announces-progress-on-the-canadian-dental-care-plan.html. Accessed 2023 Oct 30.
12.Government of Canada. Canada Dental Benefit. 2023; https://www.canada.ca/en/revenue-agency/services/child-family-benefits/dental-benefit.html. Accessed 2023 Oct 30.
13.Boyers D, van der Pol M, Watson V, et al. The Value of Preventative Dental Care: A Discrete-Choice Experiment. J Dent Res. 2021;100(7):723-730. PubMed
14.Lamont T, Worthington HV, Clarkson JE, Beirne PV. Routine scale and polish for periodontal health in adults. Cochrane Database Syst Rev. 2018;12:CD004625. PubMed
15.Nascimento GG, Leite FRM, Pennisi PRC, Lopez R, Paranhos LR. Use of air polishing for supra- and subgingival biofilm removal for treatment of residual periodontal pockets and supportive periodontal care: a systematic review. Clin Oral Investig. 2021;25(3):779-795. PubMed
Appendix 1: Selection of Included Studies
Appendix 2: References of Potential Interest
Note that this appendix has not been copy-edited.
Systematic Reviews
Mixed Intervention
Lamont T, Worthington HV, Clarkson JE, Beirne PV. Routine scale and polish for periodontal health in adults. Cochrane Database Syst Rev. 2018;12:CD004625. PubMed
Alternative Purpose (i.e., Not Routine Polishing)
Nascimento GG, Leite FRM, Pennisi PRC, Lopez R, Paranhos LR. Use of air polishing for supra- and subgingival biofilm removal for treatment of residual periodontal pockets and supportive periodontal care: a systematic review. Clin Oral Investig. 2021;25(3):779-795. PubMed
Randomized Controlled Trials
Mixed Intervention
Ramsay CR, Clarkson JE, Duncan A, et al. Improving the Quality of Dentistry (IQuaD): a cluster factorial randomised controlled trial comparing the effectiveness and cost-benefit of oral hygiene advice and/or periodontal instrumentation with routine care for the prevention and management of periodontal disease in dentate adults attending dental primary care. Health Technol Assess. 2018;22(38):1-144. PubMed
Clarkson J, Ramsay C, Lamont T, et al. Examining the impact of oral hygiene advice and/or scale and polish on periodontal disease: the IQuaD cluster factorial randomised controlled trial. Br Dent J. 2021;230(4):229-235. PubMed
Studies Comparing Different Methods of Polishing
Fu JH, Wong LB, Tong HJ, Sim YF. Conventional versus comprehensive dental prophylaxis: comparing the clinical outcomes between rubber cup and air polishing and the importance of plaque disclosure. Quintessence Int. 2021;52(3):264-274. PubMed
Kaur A, Bhardwaj A, Kansil S, Kaur R, Kaur S, Gambhir RS. Efficacy evaluation of rubber cup and air polishing techniques using glycine in plaque and stain removal - A clinical trial. J Family Med Prim Care. 2021;10(2):636-641. PubMed
Wolgin M, Frankenhauser A, Shakavets N, Bastendorf KD, Lussi A, Kielbassa AM. A randomized controlled trial on the plaque-removing efficacy of a low -abrasive air-polishing system to improve oral health care. Quintessence Int. 2021 Sep 09;52(9):752-762. PubMed
Chowdhary Z, Mohan R. Efficiency of three different polishing methods on enamel and cementum: A scanning electron microscope study. J Indian Soc Periodontol. 2018;22(1):18-24. PubMed
Poormoradi B, Tamasoki S, Shahbazi A, et al. The comparison of two professional prophylaxis systems in plaque removal and debonding of orthodontic brackets. J Indian Soc Periodontol. 2018;22(5):414-418. PubMed
Nonrandomized Studies
Studies Comparing Different Methods of Polishing
Petersilka G, Koch R, Vomhof A, et al. Retrospective analysis of the long-term effect of subgingival air polishing in supportive periodontal therapy. J Clin Periodontol. 2021;48(2):263-271. PubMed
Contributors: Elizabeth Carson, Calvin Young
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for noncommercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca.