CADTH Health Technology Review
Intraocular Lenses for Cataract Surgery
Rapid Review
Authors: Candyce Hamel, Sharon Bailey
Key Messages
What Is the Issue?
A cataract is an opacity of the lens and is the leading cause of reversible visual impairment worldwide. There are no medical treatments for cataracts but surgical procedures that replace the lens with a synthetic lens (called an intraocular lens [IOL]) have shown to be effective for restoring vision.
Premium lenses, including lenses to correct astigmatism (called toric lenses), are available but may not be covered by public or private health plans.
Given that there is an increased cost associated with toric lenses, there is a need to evaluate their effectiveness compared to other available corrective options, including glasses.
What Did We Do?
To inform decisions about the appropriate use of astigmatism-correcting IOLs, CADTH sought to identify and summarize literature that evaluates the clinical effectiveness of toric lenses against other corrective options.
An information specialist conducted a search of peer-reviewed and grey literature sources. One reviewer screened citations, and selected and critically appraised the included studies.
What Did We Find?
One systematic review (SR), 3 randomized controlled trials (RCTs), 1 prospective nonrandomized study, and 6 retrospective nonrandomized studies were identified that evaluated the clinical effectiveness of toric versus nontoric IOLs implanted during cataract surgery, including 1 with a pediatric focus.
Toric IOLs may be better than nontoric IOLs for postoperative astigmatism, but this may be dependent on the measurement of astigmatism evaluated (e.g., corneal astigmatism, residual refractive astigmatism, subjective refraction astigmatism, autorefraction astigmatism, spherical equivalent astigmatism, cylinder astigmatism, surgically induced astigmatism).
Toric IOLs may be better than nontoric IOLs for postoperative uncorrected visual acuity (VA), but it is unclear if this results in a clinically meaningful difference to the patient. None of the studies reported on spectacle independence.
Patient-centred outcomes were seldomly reported across the studies, and rarely used validated tools, making it difficult to conclude if there were patient-centred outcome differences between toric and nontoric IOLs.
Harms were reported across the studies through intraoperative complications, postoperative complications, and adverse events. Postoperative complications were statistically higher in the toric group in the SR, but there were not statistically significant differences in harms reported in the primary studies.
What Does it Mean?
It is difficult to draw conclusions across the studies and outcomes due to the variation in how outcomes were reported or because few studies report on these outcomes.
A proposed minimum set of core outcomes for cataract surgery was published in 2015. The studies included in this report did not align with this minimum set of outcomes. For example, as VA is not synonymous with improved visual functioning for patients, evaluating patient-reported visual functioning with a patient-reported outcome measure (PROM) tool is part of the minimum set of core outcomes. Future research should incorporate core outcomes, including PROMs.
Although toric IOLs statistically improved uncorrected VA, when compared to nontoric lenses, statistical significance does not imply a difference that is clinically meaningful to a patient.
Abbreviations
CI
confidence interval
D
diopters
IOL
intraocular lens
LogMAR
Logarithm of the Minimum Angle of Resolution
MD
mean difference
RCT
randomized controlled trial
SD
standard deviation
SR
systematic review
VA
visual acuity
Context and Policy Issues
What Are Cataracts?
A cataract is an opacity of the lens and is the leading cause of reversible visual impairment worldwide.1 The lens of the eye has a unique structure and unlike other epithelia, it cannot shed nonviable cells. These cells compress in the eye over time and lose their transparency.2 Cataracts occur frequently with increasing age. In 2019 to 2020, Statistics Canada reported that 17.9% (n = 1,143,000) of people over the age of 65 were diagnosed with cataracts by a health professional.3 However, in children and adults, cataracts may also be caused by poor nutrition, disease, medication, trauma, and excessive exposure to sunlight.2,4,5 Bilateral congenital cataracts have been reported in infants with low birth weight (< 2,000 g).5 The development of cataracts is painless, but cataracts may cause blurred or distorted vision, glare problems, and blindness.2 Approximately 90% of blindness in developed countries can be attributed to cataracts.4
How Are Cataracts Treated?
There are no proven medical therapies to treat cataracts,2 but cataract surgery (i.e., removal of the lens and replacement with a synthetic lens, called an IOL)4 is an effective procedure and can restore normal vision in most patients.2,4 In adults, surgery may be indicated if the symptoms interfere with daily activities and is not usually based on a specific level of VA.2,4 In children, the management of cataracts depends on factors such as the child’s age and the potential for interference with visual development.5 The most common technique used for cataract surgery is phacoemulsification (e.g., 99% of cataract surgeries in the US use phacoemulsification),4 where a small incision is made to remove the natural lens, which is then replaced with the IOL.2 In adults, surgery is most often performed in an outpatient setting using a topical anesthetic with monitored sedation, while the pediatric population typically requires general anesthetic sedation.2,6
There are 3 main IOL types: monofocal, multifocal or accommodating, and toric. Monofocal and multifocal lenses refer to the focus of the lens. More specifically, a monofocal lens usually targets distance vision and patients often still require spectacles for near activities. A multifocal lens is designed to minimize dependence of spectacles after surgery at multiple focal lengths. Toric lenses aim to eliminate or reduce preoperative astigmatism and can reduce or eliminate the need for astigmatism-correcting spectacles or contact lenses.2 Multifocal and toric lens are considered premium lenses and may not be covered by public and/or private insurance plans, with the extra expense paid by the patient. Because cataract surgery is performed only once, the type of IOL implanted is important and should be discussed between the patient and the surgeon. Factors that may influence this decision are the amount of preexisting astigmatism, the desired level of spectacle independence, and budget.2
Why Is it Important to Do This Review?
In 2020, CADTH produced a Rapid Response report that evaluated premium versus standard IOLs.7 Five SRs and 2 RCTs were included. Although some of the included studies within the 2020 report would be relevant to this rapid review, all were published before 2018, with others comparing multifocal or accommodating lenses to monofocal lenses.
As there is a potential reduction in the requirement for astigmatism-correcting spectacles with toric IOLs, albeit with an increased cost to the patient or private insurance (if it was covered), evidence regarding the clinical effectiveness is required. The objective of this review is to summarize the evidence regarding the clinical effectiveness of the monofocal toric IOL compared to the monofocal nontoric IOL implanted during cataract surgery.
Research Question
What is the clinical effectiveness of cataract surgery using monofocal toric IOLs versus conventional monofocal IOLs with or without astigmatism-correcting spectacles for people with cataracts?
Methods
Literature Search Methods
An information specialist conducted a literature search on key resources including MEDLINE, Embase, the Cochrane Database of Systematic Reviews, the International HTA Database, and the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search approach was customized to retrieve a limited set of results, balancing comprehensiveness with relevancy. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. Search concepts were developed based on the elements of the research questions and selection criteria. The main search concepts were IOLs, cataract surgery, and toric lenses. CADTH-developed search filters were applied to limit retrieval to health technology assessments, systematic reviews, meta-analyses, or indirect treatment comparisons, any types of clinical trials or observational studies, and guidelines. The search was completed on September 18, 2023, and limited to English-language documents published since January 1, 2018.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
|---|---|
Population | People with cataracts |
Intervention | Cataract surgery using monofocal toric intraocular lenses |
Comparator | Cataract surgery using conventional monofocal intraocular lenses with or without astigmatism-correcting spectacles |
Outcomes | Clinical benefits (e.g., severity of astigmatism, visual acuity, quality of life, patient satisfaction) and harms (e.g., adverse events) |
Study designs | Health technology assessments, systematic reviews, randomized controlled trials, nonrandomized studies |
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, they were duplicate publications, or were published before 2018. Systematic reviews in which all relevant studies were captured in other more recent or more comprehensive systematic reviews were excluded. Primary studies retrieved by the search were excluded if they were captured in 1 or more included systematic reviews. Guidelines with an unclear methodology were also excluded.
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the following tools as a guide: A MeaSurement Tool to Assess systematic Reviews 2 (AMSTAR 2)8 for systematic reviews and the Downs and Black checklist9 for randomized and nonrandomized studies. Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Summary of Evidence
Quantity of Research Available
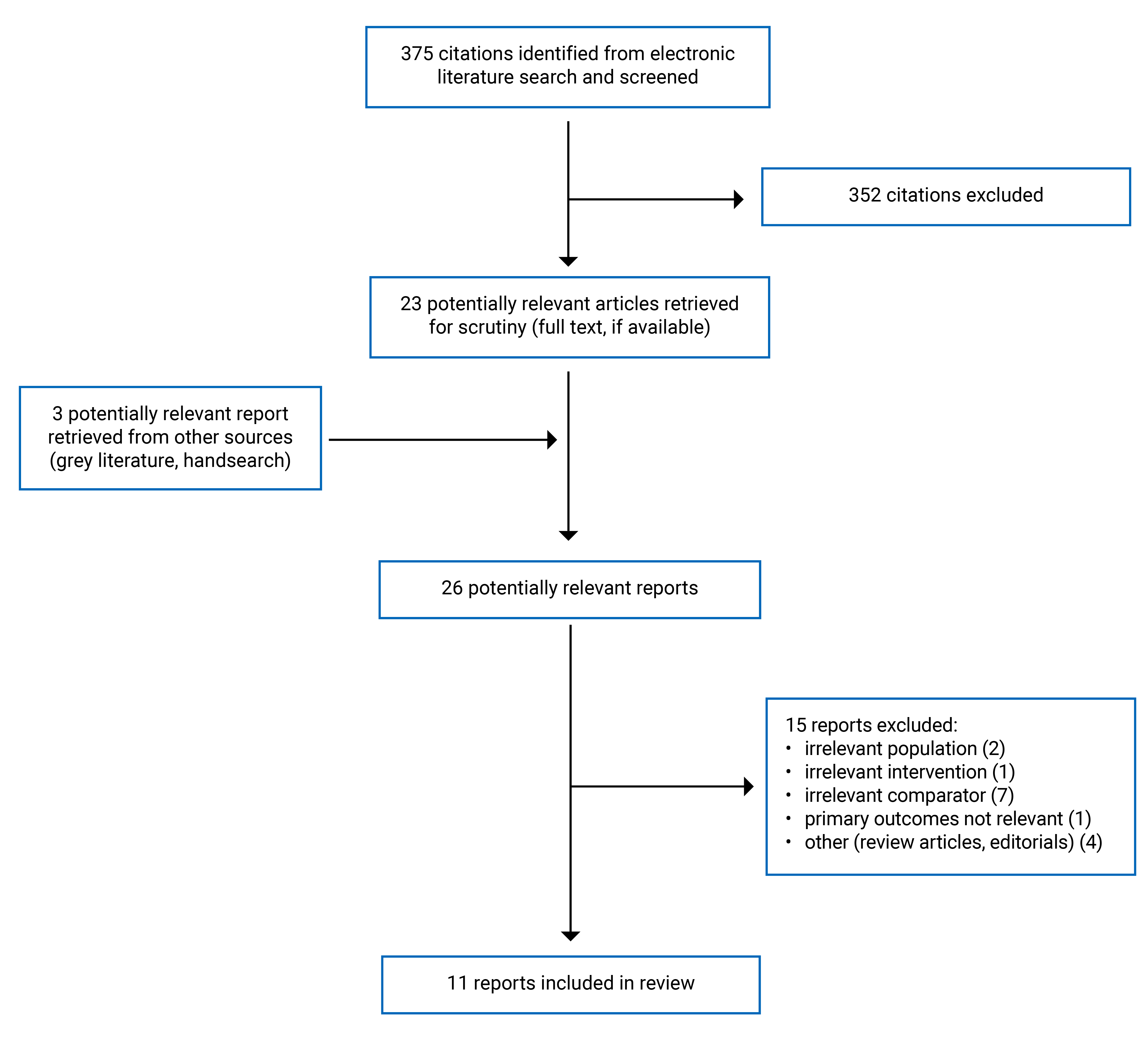
A total of 375 citations were identified in the literature search. Following screening of titles and abstracts, 352 citations were excluded and 23 potentially relevant reports from the electronic search were retrieved for full-text review. Three potentially relevant publications were retrieved from the grey literature search for full-text review. Of these potentially relevant articles, 15 publications were excluded for various reasons and 11 publications met the inclusion criteria and were included in this report. These comprised 1 SR, 3 RCTs, and 7 nonrandomized studies. Appendix 1 presents the PRISMA10 flow chart of the study selection.
Additional references of potential interest are provided in Appendix 5.
Summary of Study Characteristics
This report includes 1 SR,11 3 RCTs,12-14 and 7 nonrandomized studies (1 prospective and 6 retrospective).15-21
Additional details regarding the characteristics of the included publications are provided in Appendix 2.
Study Design
One SR published in 2022 was identified.11 The search date was up to July 25, 2021. The review included 12 RCTs, published between 2009 and 2015. All 12 RCTs were relevant to this current review.
The 3 RCTs were published in 2023,12 2021,13 and 2020.14 One prospective study published in 202316 and 6 retrospective studies were published between 2021 and 2023.15,17-21
Country of Origin
The SR was published by a first author from China and does not report where the primary studies were conducted.11 The RCTs were conducted in Austria,12 China,13 and the UK.14 The prospective nonrandomized study was conducted in China,16 2 retrospective studies were conducted in China,17,18 with 1 retrospective study each conducted in Italy,15 Egypt,19 Japan,20 and Korea.21
Patient Population
The SR11 included RCTs if the study population were patients with cataracts and corneal astigmatism. Most primary studies included patients with a mean age of 60 years or older. One subgroup in 1 study had patients 49 years and older. Other study and patient characteristics, like setting and comorbidities, were not presented. Eleven of the 12 studies included patients with a mean corneal divergence of more than 1.00 diopters (D), with 3 studies with corneal divergence of more than 2.00 D.
Patients in the 3 RCTs were 161 eyes of 126 male and females (as described in the original source) with mean ages of 69.5 years or older. Two RCTs were conducted in a hospital,12,13 with the other study not specifying where the surgery occurred, but patients were recruited from clinics.14 To be eligible for the study, baseline astigmatism ranged from 0.75 D to 1.5 D,12 1.0 D to 2.0 D,13 and at least 2.0 D.14
Patients in the 1 prospective and 6 retrospective studies were 543 eyes of 483 males and females (as described in the original source). Six of 7 studies were in adults, with a mean age of 53 years or older 15,16,18,19,21 and 1 study including patients 80 years or older.17 One study was performed in a pediatric population, with a mean age of 7.8 years.20 One study did not report the setting for surgery,15 1 study was performed in an ophthalmic centre at a university,16 and all other surgeries were performed in hospitals.17-21 One study included patients with preoperative astigmatism of 1.0 D or less.15 Three studies included patients with minimum levels of astigmatism, 0.75 D or more,17 more than 1.0 D,16 and more than 1.5 D.21 Two studies included patients with a range of astigmatism, 0.75 D to 1.5 D18 and 1.0 D to 4.0 D.19 The study in the pediatric population did not specify the level of astigmatism for inclusion.20
Interventions and Comparators
The SR11 the RCT by Liu et al. (2021),13 and 5 of the retrospective studies (Bellucci [2023],15 Wang [2023],17 Ding [2022],18 El-Shehawy [2022],19 Young Shin [2021]21) compared phacoemulsification or ultrasonic emulsification cataract surgery with 1 group receiving toric lenses and the other group receiving nontoric lenses. The RCT by Hienert et al. (2023)12 reported using “standard cataract surgery” with either toric or nontoric IOLs, and the RCT by Stanojcic et al. (2020)14 did not report the type of cataract surgery performed. One retrospective study, in the pediatrics population, reported using the optic capture technique.20 The prospective nonrandomized study by Fan et al. (2023)16 compared femtosecond laser-assisted cataract surgery and phacoemulsification cataract surgery combined with either toric IOLs or nontoric IOLs.
Outcomes
Astigmatism
Astigmatism, reported in Ds, was reported several different ways. A list of all astigmatism-related outcomes are presented in Appendix 2, with a subset of these outcomes reported here. In the SR by Chi et al. (2022),11 astigmatism was reported as corneal astigmatism. In the RCTs, astigmatism was reported as subjective refraction astigmatism (at a 6-month follow-up),12 autorefraction astigmatism (at a 6-month follow-up),12 cylinder (at a 4-week follow-up),14 spherical equivalent (at 4-week and 3-month follow-ups),13,14 corneal astigmatism (at a 3-month follow-up),13 and surgically induced astigmatism (at 4-week, 3-month, and 6-month follow-ups).12-14 In the prospective and retrospective nonrandomized studies, astigmatism was reported as cylinder (at 2-month, 2- to 4-month, and 3-month follow-ups),15,17,18,21 spherical equivalent (at 2-month, 2- to 4-month, and 3-month follow-ups),15-19,21 corneal astigmatism (at 2-month and 2- to 4-month follow-ups),15,21 residual refractive astigmatism (at a 3-month follow-up),16,19 postoperative refractive astigmatism (defined as surgically induced plus corneal) (at a 2- to 4-month follow-up),15 surgically induced astigmatism (at 2- to 4-month and 3-month follow-ups),15,18,19 and internal astigmatism in the pseudophakia (at a 2- to 4-month follow-up).15
Uncorrected VA
Uncorrected VA was reported in 10 of the 11 included studies, but were reported at distance (at 4-week, 2- to 4-month, 3-month, and 6-month follow-ups), intermediate (at a 3-month follow-up), and near (at 2- to 4-month and 3-month follow-ups) VA.
Uncorrected distance VA: The SR,11 the 3 RCTs,12-14 and 5 of the nonrandomized studies15,17-19,21 reported uncorrected distance VA. The SR did not report the distance at which this was measured.11 Two RCTs measured distance VA at 4 m,12,14 while the third did not report the distance.13 One retrospective study reported VA at a distance of 6 m,21 while the other 4 retrospective studies did not report the distance at which this was measured.15,17-19
Uncorrected intermediate VA: The prospective nonrandomized study16 reported uncorrected intermediate VA at 80 cm.
Uncorrected near VA: Two retrospective studies15,21 and the prospective nonrandomized study16 reported on uncorrected near VA. The prospective nonrandomized studies reported near VA at a distance of 40 cm.16 One retrospective study reported near VA at a distance of 33 cm,21 and 1 retrospective study did not report the distance at which this was measured.15
Corrected Visual Acuity
All 11 included studies reported best-corrected or corrected distance VA (at 4-week, 2- to 4-month, 3-month, 6-month, and 1-year follow-ups). The SR did not report the distance this was measured.11 Two RCTs reported that the distance measured was at 4 m,12,14 while the third did not report the distance.13 The prospective nonrandomized study reported best-corrected distance VA at 5 m.16 The retrospective study reported this at 4 m,15 5 m,20 and 6 m.21 The other 3 retrospective studies did not report the distance at which this was measured.17-19
Patient-Centred Outcomes
The RCT by Hienert et al. (2023)12 reported on a patient questionnaire (at a 6-month follow-up) that asked the patients to evaluate which eye (1 eye received a toric lens and the other received a nontoric lens) was superior for car driving, recognizing faces, reading text in TV, seeing irregularity on the street, reading mobile phone, playing cards, cooking, crafting, and reading a book. The RCT by Stanojcic et al. (2020)14 reported on Cat-PROM5 Rasch-calibrated score, 3-Level EQ-5D index score, and EQ-5D visual analogue scale at 4-weeks follow-up. The range of the scale for each of these tools was not provided.
Harms Outcomes
The RCT by Stanojcic et al. (2020)14 and 2 retrospective studies20,21 reported on intraoperative complications. The SR,11 2 RCTs,13,14 and 4 retrospective studies18-21 reported on postoperative complications. The RCT by Hienert et al. (2023)12 reported on adverse events. Follow-up times for postoperative complications and adverse events were not reported, with the exception of Hienert et al. (2023), which reported these times at a 6-month follow-up.12
Summary of Critical Appraisal
Systematic Review
The SR was assessed using the A MeaSurement Tool to Assess systematic Reviews 2 (AMSTAR 2) tool.8 The SR11 had several strengths, including searching 8 electronic databases, supplemental searching of professional journals, and contacting experts, which decreases the risk of missing relevant studies. The quality of reporting was sufficient in some areas; for example, the elements of PICO were well described, a PRISMA flow diagram was provided, the source of funding for the review was provided, and the authors declared their conflicts of interest. The quality of conduct was well performed and reported for some areas; for example, the methods for extraction and risk of bias were performed by 2 independent reviewers. Publication bias was assessed for all meta-analysis, regardless of the number of studies included in the analysis, which may not provide an accurate indication of publication bias (i.e., if there were fewer than 10 studies). Three of 4 meta-analyses had fewer than 10 studies. There were also limitations, including no statement that the methods were established before the review conduct (and no protocol mentioned), and it was unclear what languages of the primary studies were included and how study selection was performed. A list of the excluded studies was not provided, but high-level reasons were provided in the PRISMA flow diagram. Finally, the source of funding of the primary studies was not provided.
Randomized Controlled Trials
The RCTs12-14 were assessed using the Downs and Black checklist.9 The strengths in the RCTs were well-defined objectives, detailed descriptions of the inclusion and exclusion criteria, a description on how randomization was performed, detailed descriptions of the surgical procedure and both lenses, and all reported specific P values. There were also differences in the quality of conduct and reporting in the RCTs. In 2 RCTs, patients and examiners were masked to the intervention group,12,14 with the other RCT described as an open-label study,13 but it was unclear who was aware of the intervention assignments. Sample size calculations (with a sufficient number of patients recruited),12,13 estimates of variability (e.g., standard deviations),13,14 and baseline patient characteristics13,14 were each provided in 2 RCTs. Across all 3 RCTs,12-14 the surgery occurred in a single facility and the patients had baseline astigmatism in specific ranges, which may limit the generalizability of the surgical procedure and study population. Outcome reporting was poor in all 3 RCTs. For example, the number of outcomes reported in the results section were more than what was described in the methods section12-14 or the trial registry.12 Most12,14 or all13 outcome results did not include the number of patients who contributed to the outcome.
Prospective and Retrospective Nonrandomized Studies
The prospective nonrandomized study and retrospective studies15-21 were assessed using the Downs and Black checklist.9 There were several strengths in these studies; for example, the objectives, inclusion and exclusion criteria, surgical procedures, and IOL types were well described in all studies. Additionally, estimates of variability (e.g., standard deviations) and specific P values were reported in all studies. However, there was variability in conduct and reporting across the studies; for example, 7 studies reported detailed baseline patient characteristics,15-21 4 studies reported a sample size calculation,15-17,19 and 1 study reported the number of patients contributing to the outcomes.17 In all 7 studies, it is unclear if the facility(ies) where the surgeries occurred were representative of all cataract surgeries. Similarly, in most studies, patients had specific ranges of astigmatism (e.g., ≤ 1 D15) or it was not reported,16 which may not be representative all of patients with astigmatism. One study included patients 80 years and older17 and 1 study included pediatric patients,20 which may limit the generalizability of these studies. As the patients in these 7 studies were not randomized to an intervention group, it is possible there were unmeasured baseline differences between the groups, and no studies reported an adjusted analysis. Six of 7 studies were retrospective;15,17-21 therefore, it is likely that patients and assessors would have been aware of lens type during surgery and follow-up. In the prospective study,16 patients selected which lens was implanted. Although this would not impact objective outcomes, it may influence subjective outcomes. Most15,18,20,21 or all16,19 outcomes did not describe the number of patients that contributed to the outcome. Finally, surgical complication and adverse events were not reported in 3 studies.15-17
Additional details regarding the strengths and limitations of the included publications are provided in Appendix 3.
Summary of Findings
Appendix 4 presents the main study findings.
Clinical Effectiveness of Toric Versus Nontoric IOLs
Astigmatism
Astigmatism was reported several different ways. They are presented in the following as reported in these studies.
Corneal astigmatism: The SR11 meta-analysis included 4 results from 3 RCTs (1 RCT included 2 groups) and reported a non-statistically significant difference favouring toric over nontoric IOLs (mean difference [MD] = −0.34; 95% confidence interval [CI], −0.83 to 0.15; P = 0.18; I2 = 96%). One RCT13 and 2 retrospective studies15,21 reported no significant difference in the mean level of astigmatism between the 2 groups.
Subjective refraction astigmatism: One RCT12 reported a statistically significant difference in the median and average level of astigmatism favouring the toric IOL group over the nontoric IOL group at a 6-month follow-up, 0.25/0.23 D compared to 0.50/0.53 D, respectively (P = 0.04).
Autorefraction astigmatism: One RCT12 reported a statistically significant difference in the median and average level of astigmatism favouring the toric IOL group over the nontoric IOL group at a 6-month follow-up, 0.50/0.52 D compared to 1.00/1.17 D, respectively (P < 0.001).
Cylinder: One RCT14 and 2 retrospective studies17,21 reported a statistically significant lower mean (standard deviation [SD]) astigmatism in the cylinder, favouring the toric IOL group over the the nontoric IOL group. However, 2 retrospective studies reported no difference between groups.15,18
Spherical equivalent: Two RCTs13,14 and 5 of the 6 nonrandomized studies15-18,21 reported no difference in the spherical equivalent between those who received toric and those who received nontoric IOLs. El-Shehawy (2022)19 reported a statistically significant difference favouring the toric IOL group over the nontoric IOL group.
Surgically induced astigmatism: Results differed between the RCTs and the nonrandomized studies. The 3 RCTs12-14 reported no difference between the toric and nontoric groups. One retrospective study18 reported a statistically significant difference, with higher levels of surgically induced astigmatism in the toric IOL group. Two retrospective studies15,19 reported the mean for each group but did not provide a statistical value (e.g., P value) to measure if there was difference between groups; however, in 1 study, the mean was higher in the toric IOL group than in the nontoric IOL group, 3.47 (SD = 1.14) and 1.66 (SD = 1.46), respectively.
Postoperative refractive astigmatism: One retrospective study15 defined postoperative refractive astigmatism as surgically induced plus corneal components and reported a lower mean astigmatism favouring the toric IOL group over the nontoric IOL group; however, the difference was not statistically significant.
Residual refractive astigmatism: One prospective nonrandomized study16 and 1 retrospective study19 reported statistically significant differences between the toric and nontoric groups, with the toric group having lower levels of residual refractive astigmatism.
Internal astigmatism in the pseudophakia: One retrospective study15 reported no difference between the toric and nontoric groups.
Uncorrected Visual Acuity
Visual acuity was measured using the Logarithm of the Minimum Angle of Resolution (LogMAR) scoring system, with visual acuity decreasing as the LogMAR value increases. It was measured using distance, intermediate distances, and near distances in the included studies.
Uncorrected distance visual acuity: The SR11 meta-analysis included 12 RCTs and reported a statistically significant difference between toric and nontoric IOLs (MD = −0.05; 95% CI, −0.09 to −0.00; P = 0.03; I2 = 85%). All 3 RCTs also reported statistically significant differences, with the toric group having lower LogMAR values than the nontoric group. Four15,17,19,21 of the 5 retrospective studies reported statistically lower LogMAR scores in the toric IOL group than in the nontoric IOL group. One retrospective study18 reported higher LogMAR scores in the toric group, but the difference was not statistically significant.
Uncorrected intermediate visual acuity: The prospective nonrandomized study16 reported a statistically significant lower LogMAR score in the toric group than in the nontoric group.
Uncorrected near visual acuity: One prospective nonrandomized study16 and 1 retrospective study21 reported statistically significant lower LogMAR scores in the toric group than in the nontoric group. The retrospective study15 with patients with preoperative astigmatism of 1.0 D or lower did not report a statistically significant difference.
Corrected Distance Visual Acuity
Corrected distance visual acuity was reported across all 11 included studies with LogMAR scores.
The SR11 meta-analysis included 7 results from 6 RCTs (1 RCT included 2 groups) and reported no difference between toric and nontoric IOLs (MD = −0.00; 95% CI, −0.02 to 0.01; P = 0.77; I2 = 0%). Results across the RCTs differed; 1 RCT14 reported a statistically significant lower LogMAR score in the toric group compared to the nontoric group, and 2 RCTs12,13 reported no difference. Five of 7 nonrandomized studies reported no difference,16-18,20,21 1 study15 did not provide a statistical value (e.g., P value) to measure if there was difference between groups, and 1 study reported a statistically significant difference, with the toric group reporting a lower LogMAR score than the nontoric group.19 Specific to the retrospective study that included the pediatric population, there was no difference between groups.
Patient-Centred Outcomes
Two RCTs reported on patient-centred outcomes. The RCT by Hienert et al. (2023),12 which randomized eyes to toric or nontoric IOLs, asked patients a series of questions comparing the 2 eyes. Patients could have answered no difference between eyes, or if 1 eye was better than the other for car driving, recognize faces, reading text in TV, seeing irregularity on the street, reading mobile phone, playing cards, cooking, crafting, and reading a book. Generally, the toric eye was superior to the nontoric eye, but there were high levels of “no difference” reported across these questions. In the RCT by Stanojcic et al (2020),14 23 of the 77 patients were included in the patient-centred outcomes. There was a statistically significant difference in the Cat-PROM5 Rasch-calibrated score, although the study did not report which group reported better scores (e.g., no score values were provided for this tool and no text around which group had better scores). There was no difference in the 3-Level EQ-5D index score and the EQ-5D visual analogue scale between the toric and nontoric groups.
Harms Outcomes
Intraoperative complications: One RCT14 reported 2 patients who had intraoperative complications in the toric IOL group and 0 in the nontoric group, this was not statistically significant (P = 0.49). Two retrospective studies reported on intraoperative complications; 1 study reported no herniation of the vitreous in the anterior chamber20 and 1 study reported no complications during surgery, such as rupture of the capsule.21
Postoperative complications: The SR11 reported on postoperative complications, which mainly included persistent edema, pupillary block, retinal detachment, and endophthalmitis. There were fewer postoperative complications in the toric group, which reached statistical significance (MD = 0.47; 95% CI, 0.23 to 0.96; P = 0.04; I2 = 0%). Few postoperative complications were reported in the RCTs. In Stanojcic et al. (2020),14 3 patients in the toric group had cystoid macular edema and 1 patient in the toric group had mild posterior capsule opacification. Liu et al. (2021)13 reported that there were no surgical complications. In the 2 retrospective studies that reported this outcome, there were no complications reported.18,21 Tachibana et al. (2021) reported no increase in postoperative intraocular pressure.20 El-Shehawy et al. (2022)19 reported corneal edema, uveitis, posterior capsular opacification, and immediate postoperative anterior chamber reactions in some patients, although there did not appear to be differences between the toric and nontoric groups.
Adverse events: Hienert et al (2023)12 reported that no serious adverse events occurred during the study.
Limitations
One SR, 3 RCTs, 1 prospective nonrandomized study, and 6 retrospective studies that compared toric to nontoric IOLs combined with cataract surgery were identified. There were some important limitations with the evidence identified in this review.
Although a formal test for heterogeneity (e.g., I2 value) was not performed for the narrative summaries, it is important to note that there were differences between the studies that may affect the overall results across the studies. For example, in the RCT studies, Hienert et al. (2023)12 and Liu et al. (2021)13 included patients with preoperative astigmatism values of 2.0 D or less (0.75 D to 1.5 D and 1.0 D to 2.0 D, respectively), whereas Stanojcic et al. (2020)14 included patients with preoperative astigmatism of 2.0 D or greater. Follow-up duration also differed, ranging from 4 weeks in Stanojcic (2020),14 3 months in Liu (2021),13 and 6 months in Hienert (2023).12 In the nonrandomized studies, Bellucci (2023)15 included patients with a preoperative astigmatism value of less than 1.0 D, Fan et al. (2023) performed femtosecond laser-assisted cataract surgery before phacoemulsification cataract surgery, Wang et al. (2023)17 included patients aged 80 years and older, and Tachibana et al. (2021)20 reported on a pediatric population. Follow-up durations also differed in these studies.
Most nonrandomized studies (i.e., the prospective and retrospective nonrandomized studies) reported no differences between baseline characteristics. However, as patients were not randomized to toric or nontoric IOL, there is opportunity for unmeasured and residual confounding, and none of these studies performed adjusted analyses. El-Shehawy et al. (2022)19 reported no statistical baseline difference between the 3 groups in the study; however, there appears to be baseline differences between the 2 groups relevant to this review. For example, the toric group mean baseline spherical equivalent was −5.3 D (SD = 5 D) compared to the nontoric group baseline spherical equivalent of −1.3 D (SD = 3.7 D). This study reported statistically significant differences in all outcomes (among those where P values were reported).
Outcomes were reported in several different ways using different measures across the studies. Astigmatism is used here as an example; however, this was seen in uncorrected visual acuity, corrected visual acuity, and harms outcomes, although to a lesser degree. A comprehensive list of outcomes for astigmatism can be found in Appendix 2, but several here are provided as an example: residual corneal astigmatism, subjective refraction astigmatism, autorefraction astigmatism, surgically induced astigmatism, astigmatism cylinder range in 0.25 D steps (e.g., 0.25 D, 0.50 D, 0.75 D, 1.0 D), spherical equivalent refraction (attempted, absolute achieved, spherical equivalent error, absolute spherical equivalent error), refractive astigmatism (by Snellen visual acuity), target-induced astigmatism versus surgically induced astigmatism (Snellen lines), correction index, refractive astigmatism angle of error (change in Snellen lines), target induced astigmatism vector, difference vector. For feasibility, astigmatism was extracted from the included studies reported 9 different ways. A more consistent terminology would reduce the number of outcomes and increase the number of studies in each outcome, thereby increasing the precision in the results.
Few studies reported on patient-centred outcomes (e.g., quality of life). Among the 2 RCTs that reported these, 1 did not use a validated tool12 and the other used 3 validated tools,14 but did not provide any details on how to interpret the results (e.g., no scale or indication if a lower score is worse or better), requiring the reader to look externally to interpret the findings. Additionally, in this study, not all patients contributed to this outcome (23 of 77 patients).14
The SR did not list where the primary studies were conducted. The primary studies identified in this review were conducted in Austria, China, Egypt, Italy, Japan, Korea, and the UK. As there may be differences in surgical procedures and insurance coverages, studies conducted in other counties may limit the generalizability to the Canadian context.
Conclusions and Implications for Decision- or Policy-Making
One SR,11 3 RCTs,12-14 and 7 nonrandomized studies (1 prospective and 6 retrospective)15-21 evaluated the clinical effectiveness of toric compared to nontoric IOLs combined with cataract surgery.
It is difficult to make conclusions across studies and outcomes due to the variation in how outcomes are reported or due to a lack of studies reporting outcomes. For example, all studies reported on at least 1 measure of astigmatism, with mixed results across the studies depending on how the outcome was reported. Both subjective and autorefraction astigmatism reported statistically significant results, favouring those who received toric IOLs in 1 RCT.12 There were mixed results across the studies that reported cylinder, with 3 studies reporting a statistically significant lower mean level of astigmatism in the toric group,14,17,21 and 2 studies reporting no difference between groups.15,18 Seven of 8 studies reported no difference in the spherical equivalent,13-18,21 except for 1 study19 that had a baseline difference in this measure. There was no difference in corneal astigmatism in the SR,11 the 1 RCT,13 and 2 retrospective studies.15,21 Therefore, depending on the measurement of astigmatism that is most relevant to the patient, it is unclear if toric IOLs significantly reduce the level of astigmatism in patients who have undergone cataract surgery compared to nontoric IOLs. Furthermore, 2 RCTs reported on patient-centred outcomes,12,14 limiting conclusions relating to quality of life and visual function outcomes. A working group of international experts in cataract outcomes and registries published the results of a modified Delphi process in 2015, which included a list of postoperative outcomes for cataract surgery. This study can be found on the Core Outcomes Measures in Effectiveness Trials (COMET) initiative database using the search term cataract. Refractive outcomes is listed and the working group suggested to include the target refraction and the actual postoperative refractive error.22 Additionally, patient-reported visual function should be reported using Rasch-calibrated score from Catquest-9SF or other Rasch-calibrated PROM. This was reported in 1 RCT.14 As all primary studies in this review were published after 2015, more studies should have included this outcome.
Toric IOLs were favoured over nontoric IOLs in most studies when evaluating uncorrected visual acuity (i.e., without glasses or contact lenses). This was measured in distance, intermediate distances, and near distances. However, not all statistically significant differences are clinically meaningful to a patient. The American Academy of Ophthalmology reports that most people have between 0.5 D and 0.75 D of astigmatism and that people with a measurement of ≥ 1.5 D typically required corrective lenses to have a clear vision.23 Therefore, even a statistically significant difference between toric and nontoric IOLs may not result in a clinically meaningful difference (i.e., patients may still require corrective lenses in both groups). In a 2018 CADTH Rapid Response report,7 the 1 primary study that reported on uncorrected distance visual acuity reported statistically significant differences, favouring toric IOLs, between those who received medium-to-high and low-toric lenses compared to nontoric lenses. In this 2018 CADTH report, although not a direct link between outcomes, in general, spectacle independence was found to be better in patients with premium IOLs compared to monofocal IOLs. Spectacle independence was favoured in the toric group among the 2 SRs that included studies that compared toric to nontoric IOLs.
The additional costs or availability of toric IOLs may have impacted the results in the nonrandomized studies. It was not always reported why patients received toric or nontoric lenses, but among the studies where this was reported, it was selected by the patient,16,21 or as a result of the timing of the surgery (pre or post 2012).20
Study sizes ranged from as few as 26 eyes in 20 patients up to 159 eyes in 159 patients, 3 primary study RCTs were published between 2018 and 2023,12-14 and among the studies that reported the setting, almost all were performed in a single centre, with 1 studies being performed in more than 1 clinic or hospital.19 Based on the primary studies identified in this review, larger multicentre RCTs should be performed that compare toric to nontoric lenses. These studies should, at a minimum, report on the core outcomes as suggested in the publication by Mahmud et al. (2015).22 This may increase the generalizability of the results and provide a better indication of objective, subjective, and patient-important outcomes in studies that compared the clinical effectiveness of toric and nontoric IOLs implanted during cataract surgery.
References
1.Jin S, Chan SWS, Gupta N. Distribution gaps in cataract surgery care and impact on seniors across Ontario. Can J Ophthalmol. 2019;54(4):451-457. PubMed
2.Jacobs D. Cataract in adults. In: Gardiner M, Givens J, eds. UpToDate. Waltham (MA): UpToDate; 2023: http://www.uptodate.com/. Accessed 2023 Sep 13.
3.Statistics Canada. Chronic conditions among seniors aged 65 and older, Canadian Health Survey on Seniors, two-year period estimates. 2022; https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1310084901. Accessed 2023 Oct 4.
4.Thompson J, Lakhani N. Cataracts. Prim Care. 2015;42(3):409-423. PubMed
5.McCreery K. Cataract in children. In: Paysse E, Armsby C, eds. UpToDate. Waltham (MA): UpToDate; 2023: http://www.uptodate.com/. Accessed 2023 Sep 13.
6.American Association for Pediatric Ophthalmology and Strabismus. Anesthesia for children having eye surgery. 2021; https://aapos.org/glossary/anesthesia-for-children-having-eye-surgery. Accessed 2023 Oct 10.
7.Khangura S, Adcock L, Campbell K. Premium versus standard intraocular lenses for cataracts: a review of clinical effectiveness and cost-effectiveness. (CADTH rapid response report: summary with critical appraisal). Ottawa (ON): CADTH; 2018: https://www.ncbi.nlm.nih.gov/books/NBK581858/pdf/Bookshelf_NBK581858.pdf. Accessed 2023 Sep 13.
8.Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. PubMed
9.Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377-384. PubMed
10.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
11.Chi Q, Yang T, Chen Y. A systematic review and meta-analysis on intraocular lens implantation with different performances for the treatment of cataract. Ann Palliat Med. 2022;11(1):260-271. PubMed
12.Hienert J, Ruiss M, Hirnschall N, Findl O. Assessing the astigmatism-reducing effect of toric intraocular lenses in eyes with low astigmatism: Randomized masked bilateral comparison. J Cataract Refract Surg. 2023;49(8):826-831. PubMed
13.Liu Z, Zhou R, Xu K, et al. Efficacy comparison between toric intraocular lens and aspheric intraocular lens plus steep-axis incision in cataract patients with low corneal astigmatism. Ann Palliat Med. 2021;10(3):2610-2619. PubMed
14.Stanojcic N, Roberts H, Wagh V, Zuberbuhler B, O'Brart D. A randomised, prospective study of 'off-the-shelf' use of toric intraocular lenses for cataract patients with pre-existing corneal astigmatism in the NHS. Eye (Lond). 2020;34(10):1809-1819. PubMed
15.Bellucci C, Panico A, Tedesco SA, et al. One-dioptre toric IOL versus spherical IOL in eyes with low preoperative corneal astigmatism. Int Ophthalmol. 2023;43(5):1711-1719. PubMed
16.Fan W, Zhang G. Stereopsis after bilateral implantation of toric intraocular lenses in high myopic cataract patients with astigmatism. Adv Ophthalmol Pract Res. 2023;3(3):147-152. PubMed
17.Wang Y, Yang F, Lou X, et al. Efficacy of toric intraocular lens implantation in patients older than 80 years with cataracts and corneal astigmatism. Ophthalmol Ther. 2023;12(3):1583-1594. PubMed
18.Ding N, Song X, Wang X, Wei W. Comparison of visual outcomes between toric intraocular lenses and clear corneal incisions to correct astigmatism in image-guided cataract surgery. Front Med (Lausanne). 2022;9:837800. PubMed
19.El-Shehawy A, El-Massry A, El-Shorbagy MS, Atef M, Sabry M. Correction of pre-existing astigmatism with phacoemulsification using toric intraocular lens versus spherical intraocular lens and wave front guided surface ablation. BMC Ophthalmol. 2022;22(1):114. PubMed
20.Tachibana K, Maeda N, Abe K, Kusaka S. Efficacy of toric intraocular lens and prevention of axis misalignment by optic capture in pediatric cataract surgery. J Cataract Refract Surg. 2021;47(11):1417-1422. PubMed
21.Young Shin D, Sik Hwang H, Seung Kim H, Sew Kim M, Chul Kim E. Clinical differences between toric intraocular lens (IOL) and monofocal intraocular lens (IOL) implantation when myopia is determined as target refraction. BMC Ophthalmol. 2021;21. PubMed
22.Mahmud I, Kelley T, Stowell C, et al. A proposed minimum standard set of outcome measures for cataract surgery. JAMA Ophthalmol. 2015;133(11):1247-1252. PubMed
23.American Academy of Ophthalmology. What do astigmatism measurements mean? 2021; https://www.aao.org/eye-health/diseases/what-do-astigmatism-measurements-mean. Accessed 2023 Sep 13.
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Note that this appendix has not been copy-edited.
Table 2: Characteristics of Included Systematic Review
Study citation, country, funding source | Study designs and numbers of primary studies included | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Chi et al. (2022)11 China Funding source: None | RCTs Studies published up to July 25, 2021 Number of RCTs included: 12 Number of relevant RCTs: 12 | Inclusion criteria: Cataract patients with corneal astigmatism Setting: not reported | Intervention: phacoemulsification combined with Toric IOL Comparator: phacoemulsification combined with traditional IOL (with or without LRI, OCCI, PCRI, AK) a | Outcomes: uncorrected distance VA; Best-corrected distance VA; Residual corneal astigmatism; Postoperative complications Follow-up: 1 week to 9 months after surgery |
AK = astigmatic keratotomy; IOL = intraocular lens; LRI = limbal relaxing incisions; OCCI = opposite clear corneal incisions; PCRI = peripheral corneal relaxing incisions; RCT = randomized controlled trials; VA = visual acuity.
a1 study used LRI, 4 studies used PCRI, 2 studies used OCCI, and 1 study used AK in addition to non-toric lens; 4 studies were reported as using only non-toric lens with phacoemulsification.
Table 3: Characteristics of Included Primary Clinical Studies
Study citation, country, funding source | Study design | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Randomized Controlled Trials | ||||
Hienert 202312 Austria Funding source: Not reported | RCT (NCT03538964) | N = 58 eyes in 29 patients Patients scheduled for bilateral cataract surgery and a corneal astigmatism in both eyes between 0.75 D and 1.5 D Sex: NR Age: Mean (SD): 72.9 ± 7.9 years (range 52 to 84 years). Setting: hospital | Intervention: standard cataract surgery combined with Toric IOL (AT TORBI 709M/MP) [n = 29 eyes in 29 patients] Comparator: standard cataract surgery combined with non-Toric IOL (CT ASPHINA 409M IOL) [n = 29 eyes in 29 patients)] First eye was randomized and contralateral eye received other type of IOL | Outcomes: Uncorrected distance VA (at 4 m); Corrected distance VA (at 4 m); Subjective refraction astigmatism; Autorefraction astigmatism; Surgically induced astigmatism; Serious adverse events; Patient questionnaire; Astigmatism cylinder range of 0.25 D steps; Preoperative Keratometry and Total Keratometry with 6-month postoperative autorefraction and subjective refraction (average absolute error, average distance, limits of agreement) Follow-up: 6 months after the second cataract surgery |
Liu 202113 China Funding source: None | RCT | N = 26 eyes of 20 patients Age-related cataract patients with regular corneal astigmatism of 1.0 to 2.0 diopters; normal ocular length of 22.0 to 24.5 mm; pupil could be dilated to 6 mm; goal of emmetropia; patients had to be physically healthy and able to complete follow-up visits for 3 months Sex (as described from original source): 10 male eyes, 16 female eyes Mean (SD) Age: Toric: 74 (5.7) years; Non-Toric: 71 (9.2) years Setting: hospital | Intervention: ultrasonic emulsification with Toric IOL (AcrySof® IQ Toric IOL) [n = 13 eyes] Comparator: ultrasonic emulsification with single-focus aspheric IOL with steep axis corneal incision (AcrySof® IQ Aspheric IOL) [n = 13 eyes] | Outcomes: Uncorrected distance VA (distance not reported); Corrected distance VA (distance not reported); Spherical equivalent refraction (achieved); Anterior corneal surface astigmatism; Surgically induced astigmatism; Surgical complications; Spherical equivalent refraction (attempted, absolute achieved, spherical equivalent error, absolute spherical equivalent error); Intraocular pressure; Uncorrected distance VA (by D); Uncorrected distance VA vs Corrected distance VA (by D); Change in corrected distance VA; Refractive astigmatism (by Snellen VA); Target induced astigmatism vs Surgically induced astigmatism (Snellen lines); Correction index; Refractive astigmatism angle of error (change in Snellen lines); Target induced astigmatism vector (D); Surgically induced astigmatism vector (D); Difference vector (D) Follow-up: 1-day, 1-month, and 3-month post-surgery |
Stanojcic 202014 UK Funding source: Rayner Ltd, UK. | RCT | N = 77 eyes in 77 patients Patients with bilateral cataracts and at least 2.00 D corneal astigmatism; over 18 years of age, with visually significant cataract, could understand the rationale and processes of the study Sex (as described from original source): 33 males, 44 females Mean (SD) age: Toric: 69.5 (15.1) years; Non-Toric: 70.3 (14.7) Setting: not reported (patients recruited from clinics at Guy’s and St. Thomas’ NHS Foundation Trust, London) | Intervention: cataract surgery with Ashperic Toric IOL (T-Flex 623T) [n = 39 eyes in 39 patients] Comparator: cataract surgery with Aspheric monofocal + limbal relaxing incisions (C-Flex 970C) [n = 38 eyes in 38 patients] | Outcomes: Uncorrected distance VA (at 4 m); Corrected distance VA (at 4 m); Refractive cylinder; Spherical equivalent; Cat-PROM5; EQ-5D-3L index score; EQ-5D visual analogue scale; Surgically induced astigmatism; Intraoperative complications; Postoperative complications; Cumulative uncorrected distance VA (Snellen VA); Uncorrected distance VA vs Corrected distance VA (Snellen lines); Spherical equivalent refractive accuracy (by D); Refractive cylinder (by D); Target-induced astigmatism; Target induced vs Surgically induced astigmatism; Keratometric cylinder; Difference vector magnitude; Magnitude of error; Angle of error; Index of success; Coefficient of adjustment; Torque; Flattening; Flattening index; Correction coefficient Follow-up: 4 weeks |
Nonrandomized Studies | ||||
Bellucci 202315 Italy Funding source: Università degli Studi di Parma | Retrospective comparative series | N = 60 eyes in 60 patients Patients undergoing cataract surgery with preoperative topographic astigmatism ≤ 1.0 D; regular corneal topography; targeted IOL power between 18.0 D and 25.0 D as calculated with the Kane formula; uneventful in-the bag IOL implantation; no combined ocular surgery; final best-corrected visual acuity ≤ 0.1 LogMAR Sex (as described from original source): 26 male, 34 females Mean (SD) age: Toric: 77.1 (6.2), Non-Toric: 78.4 (6.3) years Setting: not reported | Intervention: phacoemulsification with 1.0 D Toric single-piece monofocal IOL (PerfecTor) following temporal clear cornea 2.2 mm incision [n = 30 eyes in 30 patients] Comparator: phacoemulsification with spherical single-piece monofocal IOL (Incise) following 2.2mm incision on the steepest axis when the corneal astigmatism was > 0.5, and horizontally for corneal astigmatism ≤ 0.5 D [n = 30 eyes in 30 patients] | Outcomes: Uncorrected distance VA (distance not reported); Uncorrected near VA (distance not reported); Best-corrected distance VA (at 4 m); Mean corneal astigmatism; Surgically induced astigmatism; Internal astigmatism in the pseudophakia; Postoperative refraction (sphere and cylinder); Postoperative refractive astigmatism (surgical induced + corneal); Postoperative refractive astigmatism (by D) Follow-up: last postoperative visit (2 to 4 months after surgery) |
Fan 202316 China Funding source: Fujian Youth Health Science and Technology Program | Prospective, nonrandomized study Patients selected implantation of Toric or non-Toric lens | N = 80 eyes in 40 patients Patients undergoing cataract surgery with pre-existing bilateral corneal regular astigmatism > 1.00 D, long axial length > 26mm, visually significant cataracts interfering with activities of daily living, long-term habit of wearing glasses, and pupil dilation of at least 6.0 mm before surgery Sex (as described from original source): 19 men; 21 women Mean (SD) age: Toric: 58.2 (8.0) years (range: 48 to 74); Non-Toric: 59.1 (7.4) years (range: 44 to 75). Setting: Ophthalmic Center at a university | Intervention: FLACS combined with Toric IOL implantation (Tecnis Toric ZCT) [n = 40 eyes in 40 patients] Comparator: FLACS combined with non-Toric IOL implantation (Tecnis PCB00) [n = 40 eyes in 40 patients] All patients received conventional phacoemulsification cataract surgery. | Outcomes: Best-corrected distance VA (at 5 m); Uncorrected intermediate VA (at 80 cm); Uncorrected near VA (at 40 cm); Residual refractive astigmatism; Spherical equivalent; Near, intermediate, and distance stereoacuity Follow-up: 7 days, 1 month, and 3 months postoperatively |
Wang 202317 China Funding source: No funding | Retrospective study | N = 159 eyes in 159 patients Patients older than 80 years with corneal astigmatism (≥ 0.75 D) Sex (as described from original source): 78 males, 81 females Mean (SD) age: Toric: 83.98 (2.98); Non-Toric groups: 84.08 (3.11) and 83.62 (2.99) Setting: hospital | Intervention: phacoemulsification with Toric IOL (Acrysof IQ® toric IOLs, SN6AT2 to 5) [n = 53 eyes in 53 patients] Comparator: phacoemulsification with non-Toric IOL (2 types of lenses: Acrysof IQ®,SN60WF and A1-UV) [n = 51 eyes in 51 patients and n = 55 eyes in 55 patients] | Outcomes: Uncorrected distance VA (distance not reported); Corrected distance VA (distance not reported); Refraction (spherical equivalent, refractive cylinder); Cumulative Snellen VA; Difference between UDVA and CDVA; Astigmatic power vector; Spherical equivalent refraction (by D); Refractive cylinder (by D) Follow-up: 3 months postoperatively |
Ding 202218 China Funding source: Capital Health Research and Development of Special, Science and Technology Project of Beijing Municipal Science, and Technology Commission. | Retrospective study | N = 68 eyes in 68 patients Patients with cataracts and preoperative anterior corneal astigmatism with optical biometry of 0.75 to 1.5 D; regular and symmetric astigmatism shape on the corneal topographic map, pupil dilation > 6.00mm, and no obvious ocular and systemic diseases Sex (as described from original source): 23 males, 45 females Mean (SD) Age: Toric: 65.00 years (8.03) (range: 46 to 71); Non-Toric: 59.22 years (13.80) (range: 32 to 82) Setting: hospital | Intervention: phacoemulsification with Toric IOL (AcrySof Toric IOL) [n = 36 eyes in 36 patients] Comparator: phacoemulsification with aspheric monofocal IOL with corneal astigmatism incisions (MI60) [n = 32 eyes in 32 patients] | Outcomes: Uncorrected distance VA (distance not reported); Best-corrected spectacle VA (distance not reported); Residual refractive cylinder astigmatism; Spherical equivalent refraction; Surgically induced astigmatism; Complications; Cumulative VA; Difference between UDVA and BSCVA; Spherical equivalent refraction (by D); Refractive cylinder (by D); Refractive Astigmatism Angle of Error (by degrees); Target induced astigmatism; Difference vector; Angle of error; Magnitude of error; Correction index; Index of success Follow-up: 1 day, 1 week, 1 months, and 3 months postoperatively (most outcomes reported only at 3 months) |
El-Shehawy 202219 Egypt Funding source: None | Retrospective study | N = 40 eyes of 33 patients Patients diagnosed with visually significant cataracts and regular astigmatism between 1 to 4 D and completed follow-up Sex (as described from original source): 14 males, 19 females Mean (SD) age: Toric: 53.20 (5.60) (range: 47 to 70); Non-Toric: 55.20 (6.10) years (range: 45 to 66) Setting: ophthalmology clinics in University hospitals | Intervention: phacoemulsification with Toric IOL (lens model not reported) [n = 20 eyes of 14 patients] Comparator: phacoemulsification with spherical IOL (lens model not reported) [n = 20 eyes of 19 patients] Note: Group C received phacoemulsification with spherical intraocular lens and wavefront guided PRK three months later (not extracted) | Outcomes: Uncorrected distance VA (distance not reported); Best-corrected distance VA (distance not reported); Mean refraction spherical equivalent; Refractive astigmatism; Surgically induced astigmatism; Complications; Target induced astigmatism; Difference vector; Magnitude of error; Correction index; Angle of error; Absolute angle of error; Torque effect; Flattening effect; Index of success; Percentage of success Follow-up: 3 months postoperatively |
Tachibana 202120 Japan Funding source: Alcon Japan Ltd. | Retrospective study (chart review) | N = 36 eyes of 23 patients Pediatric patients with cataracts who underwent surgery Sex (as described from original source): 21 eyes of 14 boys, 15 eyes of 9 girls Mean (SD) age: All: 7.8 (3.8) years; Toric: 8.1 (4.1) years (range: 3 to 16); non-Toric: 7.7 ± 3.7 years (range: 3 to 13) Setting: hospital | Intervention: optic capture technique with Toric IOL (AcrySof IQ toric IOL and Tecnis toric IOL) [n = 14 eyes of 11 patients] Comparator: optic capture technique with non-Toric (lens model not reported) [n = 22 eyes of 15 patients] | Outcomes: Corrected distance VA (at 5 m); Intraoperative complications; Postoperative complications Follow-up: 1 year postoperatively |
Young Shin 202121 Korea Funding source: National Research Foundation of Korea funded by the Ministry of Education | Retrospective study (chart review) | N = 100 eyes of 100 patients Patients with age-related cataract with corneal astigmatism > 1.5 diopters Sex (as described from original source): 35 males, 65 females Mean (SD) age: Toric: 62.7 (11.3) years; non-Toric: 64.4 (4.64) years Setting: hospital | Intervention: phacoemulsification with Toric IOL (Tecnis® ZCT toric IOL) [n = 40 eyes of 40 patients] Comparator: phacoemulsification with non-Toric monofocal IOL (Tecnis® ZCB IOL) [n = 60 eyes of 60 patients] | Outcomes: Uncorrected near VA (at 33 cm): Uncorrected distance VA (at 6 m); Corrected distance VA (at 6 m); Spherical equivalent; Refractive cylinder astigmatism; Corneal astigmatism; Intraoperative complications; Postoperative complications; Distance UCVA (by LogMAR values) postoperative day; Residual keratometric cylinder (D) Follow-up: 1-day, 1-week, 1-months, 2-months postoperatively |
BDVA = best-corrected distance visual acuity; D = diopters; IOL = intraocular lens; LogMAR = logarithm of the minimum angle of resolution; NR = not reported; RCT = randomized controlled trial; UDVA = uncorrected distance visual acuity.
Note: Italicized outcomes were not extracted.
Appendix 3: Critical Appraisal of Included Publications
Note that this appendix has not been copy-edited.
Table 4: Strengths and Limitations of Systematic Reviews Using AMSTAR 28
Strengths | Limitations |
|---|---|
Chi 202211 | |
|
|
AMSTAR 2 = A MeaSurement Tool to Assess systematic Reviews 2.
Table 5: Strengths and Limitations of Clinical Studies Using the Downs and Black Checklist9
Strengths | Limitations |
|---|---|
Randomized Controlled Trials | |
Heinert 202312 | |
|
|
Liu 202113 | |
|
|
Stanojcic 202014 | |
• Objectives well described
|
|
Nonrandomized Studies | |
Bellucci 202315 | |
|
|
Fan 202316 | |
• Objectives well described
|
|
Wang 202317 | |
• Objectives well described
|
|
Ding 202218 | |
• Objectives well described
|
|
El-Shehawy 202219 | |
• Objectives well described
|
|
Tachibana 202120 | |
|
|
Young Shin 202121 | |
• Objectives well described
|
|
IOL = intraocular lens.
Appendix 4: Main Study Findings
Note that this appendix has not been copy-edited.
Table 6: Summary of Findings by Outcome — Astigmatism
Study | Time point | Intervention | Differences | |
|---|---|---|---|---|
Toric lens (diopters) | Non-Toric lens (diopters) | |||
Systematic Review | ||||
Corneal astigmatism | ||||
Chi 202211 | NA | Residual astigmatism: MD (95% CI): −0.34 (−0.83 to 0.15); P = 0.18 Degrees of freedom = 3; I2 = 96% | ||
Randomized Controlled Trials | ||||
Subjective refraction astigmatism | ||||
Hienert 202312 | 6 months | Median/Average: 0.25/0.23 | Median/Average: 0.50/0.53 | P = 0.04 |
Autorefraction astigmatism | ||||
Hienert 202312 | 6 months | Median/Average: 0.50/0.52 | Median/Average: 1.00/1.17 | P < 0.001 |
Cylinder | ||||
Stanojcic 202014 | 4 weeks | 1.35 (0.84) (range: 0.25 to 3.75) | 1.91 (1.07) (range: 0.25 to 5) | P = 0.01 (95%CI −1 to −0.12) |
Spherical equivalent | ||||
Liu 202113 | 3 months | Achieved: 0.14 (0.49) | Achieved: 0.12 (0.45) | P = 0.92 |
Stanojcic 202014 | 4 weeks | −0.48 (0.49) | −0.53 (0.71) | P = 0.72 (95%CI −0.23 to 0.33) |
Corneal astigmatism | ||||
Liu 202113 | 3 monthsb | 1.42 (0.41) | 1.19 (0.41) | P = 0.154 |
Surgically induced astigmatism | ||||
Hienert 202312 | 6 months | The analysis of surgically induced astigmatism for each group with double-angle plot toll from Koch et al. showed no difference between the groups. | ||
Liu 202113 | 3 months | 1.22 (0.64) | 0.84 (0.45) | P = 0.093 |
Stanojcic 202014 | 4 weeks | 2.67 (1.28) (range: 0.74 to 6.12) | 2.35 (1.79) (range: 0.19 to 7.07) | P = 0.37 (95%CI −1.03 to 0.39) |
Nonrandomized Stuies | ||||
Cylinder | ||||
Bellucci 202315 | 2 to 4 months | 0.58 (0.32) | 0.73 (0.37) | NS |
Wang 202317 | 3 months | 0.58 (0.36) Median (IQR): 0.50 (0.50; 0.75) | 1.10 (0.53) Median (IQR): 1.00 (0.75; 1.50) 1.35 (0.90) Median (IQR): 1.25 (0.75; 1.75) | P < 0.001 |
Ding 202218 | 3 months | 0.34 (0.40) (range: 0 to 1.00) | 0.64 (0.57) (range: 0 to 1.25) | P = 0.24 |
Young Shin 202121 | 2 months | 0.80 (0.46) | 1.65 (0.77) | P = 0.001 |
Spherical equivalent | ||||
Bellucci 202315 | 2 to 4 months | −0.58 (0.43) | −0.58 (0.82) | NS |
Fan 202316 | 3 monthsa | −2.99 (0.70) | −2.93 (0.56) | P = 0.662 |
Wang 202317 | 3 months | −0.42 (0.68) Median (IQR): −0.25 (−0.50; 0.00) | −0.70 (0.93) Median (IQR): −0.50 (−0.88; −0.07) −0.49 (0.71) Median (IQR): −0.38 (−0.75; −0.13) | P = 0.17 |
Ding 202218 | 3 months | 0.17 (0.28) (range: −0.21 to 0.59) | 0.13 (0.45) (range: −0.43 to 0.90) | P = 0.83 |
El-Shehawy 202219 | 3 months | −0.36 (0.4) (−1:0.25) | −0.76 (0.64) (−1.75:1.25) | P = 0.004 |
Young Shin 202121 | 2 months | −3.23 (0.85) | −3.05 (0.63) | P = 0.465 |
Corneal astigmatism | ||||
Bellucci 202315 | 2 to 4 months | 0.56 (0.38) | 0.55 (0.39) | NS |
Young Shin 202121 | 2 months | 1.50 (0.62) | 1.45 (0.64) | P = 0.465 |
Postoperative refractive astigmatism [defined as: surgically induced + corneal] | ||||
Bellucci 202315 | 2 to 4 months | 0.58 (0.31) | 0.73 (0.37) | NS |
Residual refractive astigmatism | ||||
Fan 202316 | 3 monthsa | 0.44 (0.24) | 1.49 (0.55) | P < 0.001 |
El-Shehawy 202219 | 3 months | 0.53 (0.32) (0:1.25) | 2.15 (0.6) (1:3.5) | P < 0.00001 |
Surgically induced astigmatism | ||||
Bellucci 202315 | 2 to 4 months | 0.32 (0.16) | 0.35 (0.21) | NR |
Ding 202218 | 3 months | 1.04 (0.38) (range: 0.40 to 1.59) | 0.61 (0.29) (range: 0.31 to 0.96) | P = 0.02 |
El-Shehawy 202219 | 3 months | 3.47 (1.14) (1.5:5.47) | 1.66 (1.46) (0.3:5.5) | NR |
Internal astigmatism in the pseudophakia | ||||
Bellucci 202315 | 2 to 4 months | 0.73 (0.43) | 0.70 (0.33) | NS |
CI = confidence interval; D = diopters; MD = mean difference; NA = not applicable; NR = not reported; NS = not significant; RRA = residual refractive astigmatism; SE = spherical equivalent.
Note: Reported as mean (SD) unless otherwise specified.
aResults also reported at 7 days and 1 month after surgery.
Table 7: Summary of Findings by Outcome — Uncorrected Visual Acuity
Study | Time point | Intervention | Difference | |
|---|---|---|---|---|
Toric lens (LogMAR) | Non-Toric lens (LogMAR) | |||
Systematic Review | ||||
Uncorrected distance visual acuity | ||||
Chi 202211 | NA | MD (95% CI): −0.05 (−0.09 to −0.00); P = 0.03 Degrees of freedom = 11; I2 = 85% | ||
Randomized Controlled Trials | ||||
Uncorrected distance visual acuity | ||||
Hienert 202312 | 6 months | Median: 0.00 Average: 0.00 Min to Max: 0.40 to −0.20 | Median: 0.10 Average: 0.10 Min to Max: 0.50 to 0.00 | P = 0.03 |
Liu 202113 | 3 monthsa | 0.03 (0.08) | 0.13 (0.14) | P = 0.033 |
Stanojcic 202014 | 4 weeks | 0.18 (0.19) | 0.27 (0.15) | P = 0.02 (95%CI −0.17 to −0.01) |
Nonrandomized Studies | ||||
Uncorrected distance visual acuity | ||||
Bellucci 202315 | 2 to 4 months | 0.08 (0.07) | 0.13 (0.07) | P = 0.007 |
Wang 202317 | 3 months | 0.15 (0.10) Median (IQR): 0.10 (0.10; 0.22) | 0.29 (0.16) Median (IQR): 0.30 (0.16; 0.40) 0.29 (0.17) Median (IQR): 0.30 (0.22; 0.40) | P < 0.001 |
Ding 202218 | 3 months | 0.17 (0.22) (range: 0 to 0.52) | 0.12 (0.11) (range: −0.08 to 0.30) | P = 0.57 |
El-Shehawy 202219 | 3 months | 0.14 (0.1) (0:0.4) | 0.36 (0.13) (0.097:0.52) | P < 0.001 |
Young Shin 202121 | NR | 0.38 (0.14) | 0.55 (0.22) | P = 0.026 |
Uncorrected intermediate visual acuity | ||||
Fan 202316 | 3 monthsb | 0.30 (0.11) | 0.46 (0.09) | P < 0.001 |
Uncorrected near visual acuity | ||||
Bellucci 202315 | 2 to 4 months | The uncorrected near visual acuity was also tested to check if the 1.0 toric implant could play a role in near vision for these eyes founding no difference between the two groups. | ||
Fan 202316 | 3 monthsb | 0.23 (0.14) | 0.35 (0.09) | P < 0.001 |
Young Shin 202121 | NR | 0.26 (0.33) | 0.48 (0.32) | P = 0.030 |
CI = confidence interval; IQR = interquartile range; LogMAR = logarithm of the minimum angle of resolution; MD = mean difference.
Note: Reported as mean (SD) unless otherwise specified.
aResults also reported before, at 1-day, 1 week, and 1-month post-surgery.
bResults also reported at 7 days and 1 month after surgery.
Table 8: Summary of Findings by Outcome — Corrected Distance Visual Acuity
Study | Time point | Intervention | Difference | |
|---|---|---|---|---|
Toric lens (LogMAR) | Non-Toric lens (LogMAR) | |||
Systematic Review | ||||
Chi 202211 | NA | MD (95% CI): −0.00 (−0.02 to 0.01); P = 0.77 Degrees of freedom = 6; I2 = 0% | ||
Randomized Controlled Trials | ||||
Hienert 202312 | 6 months | Median: 0.00 Average: 0.0 Min to Max: 0.20 to −0.20 | Median: 0.00 Average: 0.00 Min to Max: 0.20 to −0.10 | P = 0.60 |
Liu 202113 | 3 monthsa | −0.02 (0.04) | 0.03 (0.13) | P = 0.458 |
Stanojcic 202014 | 4 weeks | 0.01 (0.12) | 0.06 (0.12) | P = 0.07 (95%CI −0.11 to 0.01) |
Nonrandomized Studies | ||||
Bellucci 202315 | 2 to 4 months | 0.01 (0.04) | 0.02 (0.04) | NR |
Fan 202316 | 3 monthsb | 0.08 (0.07) | 0.09 (0.09) | P = 0.914 |
Wang 202317 | 3 months | 0.10 (0.09) Median (IQR): 0.10 (0.00; 0.15) | 0.15 (0.11) Median (IQR): 0.10 (0.10;0.22) 0.15 (0.12) Median (IQR): 0.10 (0.10;0.22) | P = 0.059 |
Ding 202218 | 3 months | 0.04 (0.09) (range: −0.08 to 0.22) | 0.03 (0.07) (range: −0.08 to 0.10) | P = 0.92 |
El-Shehawy 202219 | 3 months | 0.09 (0.1) (0:0.4) | 0.185 (0.1) (0.0:0.3) | P = 0.003 |
Tachibana 202120 | 1 year | 0.003 (0.8) (range: −0.08 to 0.15) | 0.09 (NR) (range: −0.30 to 1.30) | P = 0.464 |
Young Shin 202121 | NR | 0.08 (0.08) | 0.11 (0.14) | P = 0.710 |
CI = confidence interval; LogMAR = logarithm of the minimum angle of resolution; MD = mean difference; NA = not applicable; NR = not reported.
aResults also reported before, at 1-day, 1 week, and 1-month post-surgery.
bResults also reported at 7 days and 1 month after surgery.
Note: Reported as mean (SD) unless otherwise specified.
Table 9: Summary of Findings by Outcome — Patient-Centred Outcomes
Study | Time point | Intervention | Difference | |
|---|---|---|---|---|
Toric lens | Non-Toric lens | |||
Randomized Controlled Trials | ||||
Patient questionnaire | ||||
Hienert 202312 | 6 months | Patients were asked to compare the 2 eyes and indicate which was superior for car driving; recognize faces; text in TV; see irregularity on the street; reading mobile phone; playing card, cooking, crafting; reading a book. Toric eyes tended to be superior to non-Toric eyes for most, but mostly there was no difference between eyes. | ||
Change in Cat-PROM5 Rasch-calibrated score | ||||
Stanojcic 202014 | 4 weeks | −2.72 (5.39) (n = 12) | −7.06 (3.75) (n = 11) | P = 0.04 (95%CI 0.28 to 8.4) |
Change in EQ-5D-3L index score | ||||
Stanojcic 202014 | 4 weeks | 0.03 (0.09) (n = 12) | 0.005 (0.07) (n = 11) | P = 0.47 (95%CI −0.05 to 0.1) |
Change in EQ-5D visual analogue scale | ||||
Stanojcic 202014 | 4 weeks | 4 (9.70) (n = 12) | 1.09 (13.55) (n = 11) | P = 0.56 (95%CI −7.24 to 13.06) |
CI = confidence interval; EQ-5D-3L = European Quality of Life 5 Dimensions 3 Level Version; PROM = patient-reported outcome measures
Table 10: Summary of Findings by Outcome — Harms Outcomes
Study | Time point | Intervention | |
|---|---|---|---|
Toric lens | Non-Toric lens | ||
Systematic Review | |||
Postoperative complications | |||
Chi 202211 | NA | MD (95% CI): 0.47 (0.23 to 0.96); P = 0.04 Degrees of freedom = 2; I2 = 0% Postoperative complications mainly include persistent edema, pupillary block, retinal detachment and endophthalmitis. | |
Randomized Controlled Trials | |||
Intraoperative complications | |||
Stanojcic 202014 | During surgery | Complications were only encountered in the TIOL group. Two patients (2/39; 5.1%) required TIOL exchange at the time of surgery due to broken haptics, which was believed to have happened during injection of the IOL. Intraoperative complications were not statistically significance between the groups (P = 0.49). | |
Postoperative complications | |||
Liu 202113 | NR | There were no surgical complications. | |
Stanojcic 202014 | NR | Cystoid macular edema: Toric: 3 (8%) patients; Non-toric: 0 patients (P = 0.24). Mild posterior capsule opacification: Toric: 1 (3%) patient. The patient did not experience any symptoms and did not require Nd:YAG capsulotomy. | |
Adverse events | |||
Hienert 202312 | 6 months | No serious adverse events during the study. | |
Nonrandomized Studies | |||
Intraoperative complications | |||
Tachibana 202120 | During surgery | No herniation of the vitreous into the anterior chamber was observed in any of the eyes. | |
Young Shin 202121 | During surgery | There were no complications during surgery, such as rupture of the capsule. | |
Postoperative complications | |||
Ding 202218 | NR | No complications occurred. | |
El-Shehawy 202219 | NR | Corneal edema: Toric: 6 eyes (30%); Non-toric: 5 eyes (25%). All were reversible with medical treatment. Uveitis: Toric: 0 eyes; Non-toric: 2 eyes (10%). All were reversible with medical treatment. Posterior capsular opacification: Toric: 2 eyes (10%); Non-toric: 3 eyes (15%) Immediate postoperative anterior chamber reactions: Toric: 1 eye (5%); Non-toric; 0 eyes. Reversible with medical treatments. | |
Tachibana 202120 | NR | There was no increase in postoperative intraocular pressure (> 21 mm Hg) in any of the included eyes. | |
Young Shin 202121 | NR | There were no postoperative complications. | |
CI = confidence interval; MD = mean difference; NA = not applicable; NR = not reported.
Appendix 5: References of Potential Interest
Note that this appendix has not been copy-edited.
Previous CADTH Reports
Khangura S, Adcock L, Campbell K. Premium versus standard intraocular lenses for cataracts: a review of clinical effectiveness and cost-effectiveness. (CADTH rapid response report: summary with critical appraisal). Ottawa (ON): CADTH; 2018: https://www.ncbi.nlm.nih.gov/books/NBK581858/pdf/Bookshelf_NBK581858.pdf. Accessed 2023 Sep 13.
Randomized Controlled Trials
Primary Outcomes Not Relevant
Vukich JA, Ang RE, Straker BJK, et al. Evaluation of intraocular lens rotational stability in a multicenter clinical trial. Clin Ophthalmol. 2021;15:3001-3016. PubMed
Nonrandomized Studies
Population After Uncomplicated Cataract or Refractive Lens Exchange Surgery
Gundersen KG, Potvin R. Comparing visual acuity, low contrast acuity and refractive error after implantation of a low cylinder power toric intraocular lens or a non-toric intraocular lens. Clin Ophthalmol. 2020;14:3661-3666. PubMed
Additional References
Analysis of 4 Randomized Controlled Trials
Holladay JT, Pettit G. Improving toric intraocular lens calculations using total surgically induced astigmatism for a 2.5 mm temporal incision. J Cataract Refract Surg. 2019;45(3):272-283. PubMed
Contributor: Calvin Young
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up to date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca.