CADTH Health Technology Review
Buprenorphine-Naloxone Film Versus Tablets for Opioid Use Disorder
Rapid Review
Authors: Kylie Tingley, Monika Mierzwinski-Urban
Key Messages
What Is the Issue?
Medication for opioid use disorder is essential for reducing cravings, withdrawal symptoms, and facilitating recovery, with buprenorphine being preferred over methadone by health care providers and people with opioid use disorder due to its lower overdose risk and perceived lower side effect profile.
In Canada, buprenorphine is available in various formulations, including buprenorphine-naloxone (BUP-NAL), commonly chosen for its safety benefits and convenience.
Sublingual buprenorphine-naloxone films offer faster dissolution and potentially other benefits compared to sublingual tablets, evaluating their comparative clinical and cost-effectiveness is important as they become more widely available.
What Did We Do?
To inform decisions about the appropriate selection of BUP-NAL formulations for treating individuals with opioid use disorder, CADTH sought to identify and summarize literature comparing the clinical effectiveness and cost-effectiveness of sublingual BUP-NAL films versus tablets. We also attempted to identify evidence-based recommendations for the use of BUP-NAL film.
A research information specialist conducted a literature search of the peer-reviewed and grey literature with a search strategy focused on sublingual BUP-NAL. The search was limited to English-language documents published since January 1, 2018. One reviewer screened articles for inclusion based on predefined criteria, critically appraised the included study, and narratively summarized the findings.
What Did We Find?
Sublingual BUP-NAL films may have lower abuse rates compared to sublingual BUP-NAL tablets among people who seek treatment at substance abuse treatment centres or who present needing medical advice or treatment for intentional misuse or abuse of potentially toxic substances, including opioids (1 study).
We did not find any clinical effectiveness studies that assessed aspects related to drug ingestion, drug abuse cessation, treatment programs, health-related quality of life, mental health or safety of BUP-NAL films or tablets that met our criteria for this review.
We did not find any studies on cost-effectiveness or evidence-based guidelines of sublingual BUP-NAL films or tablets that met our criteria for this review.
What Does It Mean?
Limited evidence from this review suggests that sublingual BUP-NAL films may lead to lower substance abuse rates compared to sublingual BUP-NAL tablets among people with OUD; however, we require more comprehensive research with rigorous methodological approaches to understand this topic better.
Considering the low abuse potential for BUP-NAL film, decision-makers may wish to use this formulation in settings where the potential for substance abuse is high.
Abbreviations
ASI-MV
Addiction Severity Index-Multimedia Version
BUP-NAL
combination product of buprenorphine with naloxone, as a single preparation
CI
confidence interval
HTA
health technology assessment
MOUD
medication for opioid use disorder
OUD
opioid use disorder
Context and Policy Issues
What Is Opioid Use Disorder?
Opioid use disorder (OUD) is a serious medical condition characterized by the compulsive and problematic use of opioid drugs, such as prescription painkillers (e.g., oxycodone, hydrocodone) or illicit opioids (e.g., heroin).1,2 Individuals with OUD experience a range of symptoms, including a strong desire to use opioids, loss of control over opioid use, and continued use despite adverse consequences, such as health problems, social difficulties, and legal issues.2
OUD can manifest in various degrees of severity, from mild to severe, depending on factors like the frequency and quantity of opioids used, the duration of use, and the individual's physiological and psychological responses to opioids.1 It is a chronic and relapsing condition that can have devastating effects on a person's physical and mental health, relationships, and overall quality of life.
According to data from the 2018 Canadian Community Health Survey, 3.7 million (12.7%) of those who answered, aged 15 years and older, reported the use of opioid pain relievers, and nearly 10% of those (351,000) reported problematic use of opioids.3 After adjusting for socioeconomic circumstances and other health conditions, those who reported unmet needs for emotional or mental health or problems with substances were more than 2.5 times as likely to use opioid pain relief medication compared to those without such needs.3 The Public Health Agency of Canada recently reported that between January 2016 and March 2023, there was a total of 38,514 apparent opioid toxicity deaths across Canada.4 Opioid toxicity deaths disproportionately affect males and individuals who were to 20 to 59 years old.4 Similarly, there was a total of 37,697 opioid-related poisoning hospitalizations reported between January 2016 and March 2023, with the highest proportion among males between ages 30 to 39.4 Other populations that have reported disproportionately higher opioid harms include those with lower income or who have experienced periods of employment instability, those who are employed in the construction industry, as well as those from Indigenous backgrounds.5
What Is the Current Practice?
OUD typically requires a combination of medication for opioid use disorder (MOUD) and psychosocial support, including counselling and behavioural therapies like Cognitive Behavioural Therapy.6 While counselling can be effective, it is even more so when combined with MOUD, as some individuals may struggle to maintain abstinence without the support of medication. MOUD includes drugs like methadone, buprenorphine, and extended-release naltrexone, which have been proven to aid in recovery by reducing withdrawal symptoms, cravings, and the body's response to opioids.6 These medications help individuals reduce their use of injected drugs, lowering the risk of diseases and even death.
Why Is It Important to Do This Review?
MOUD is a crucial component of treatment for OUD. They are used to reduce cravings, alleviate withdrawal symptoms, and help individuals achieve and maintain recovery.7 Several medications are approved for OUD treatment, each with unique mechanisms and formulations.8 Buprenorphine is generally preferred over methadone for the treatment of individuals with moderate to severe OUD because of the lower risk of death with overdose, accessibility, and fewer drug interactions.7
In Canada, buprenorphine is available in several formulations for the treatment of people with OUD, including the single-ingredient buccal film, buprenorphine extended-release injection, subcutaneous implant, as well as the combination product of buprenorphine-naloxone (BUP-NAL) in a sublingual film and tablet.8 BUP-NAL, commonly known as Suboxone, is often preferred over methadone or single-ingredient buprenorphine for the treatment of OUD due to its lower risk of overdose, reduced potential for diversion and misuse, and the option for office-based treatment. BUP-NAL's partial agonist nature offers a safer treatment option compared to full opioid agonists like methadone while providing a more flexible and convenient approach to recovery. According to a CADTH report from 2019, individuals with OUD demonstrated a more favourable perception of buprenorphine compared to methadone.9 This preference was driven by the perception of fewer side effects and the belief that buprenorphine had the potential to restore a sense of normalcy in their lives and alleviate withdrawal symptoms.9
BUP-NAL is available in 2 formulations: sublingual films and tablets. Sublingual BUP-NAL films may offer an advantage over tablets because the time required for the medication to dissolve is quicker due to their thin, flexible structure. Sublingual BUP-NAL film may also be more effective at lower doses due to improved absorption, which may be beneficial in certain health care contexts (e.g., correctional facilities). Before sublingual BUP-NAL film becomes widely available across Canada, it is important to understand its potential advantages and disadvantages compared to sublingual BUP-NAL tablets both from a clinical- and cost-effectiveness perspective.
Objective
To support decision-making about sublingual BUP-NAL films for the treatment of individuals with OUD, we prepared this Rapid Review to summarize and critically appraise the studies available on the clinical effectiveness, cost-effectiveness, and evidence-based guidance for sublingual BUP-NAL films versus tablets for individuals with OUD.
Research Questions
What is the comparative clinical effectiveness of sublingual buprenorphine/naloxone film versus tablets for people with opioid use disorder?
What is the comparative cost-effectiveness of sublingual buprenorphine/naloxone film versus tablets for people with opioid use disorder?
What are the evidence-based recommendations for sublingual buprenorphine/naloxone film for people with opioid use disorder?
Methods
Literature Search Methods
An information specialist conducted a literature search on key resources, including MEDLINE, Embase, the Cochrane Database of Systematic Reviews, the International HTA Database, and the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search approach was customized to retrieve a limited set of results, balancing comprehensiveness with relevancy. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. Search concepts were developed based on the elements of the research questions and selection criteria. The main search concept was sublingual buprenorphine/naloxone. CADTH-developed search filters were applied to limit retrieval to health technology assessments, systematic reviews, meta-analyses, indirect treatment comparisons, clinical trials or observational studies, economic studies, and guidelines. The search was completed on September 21, 2023, and limited to English-language documents published since January 1, 2018.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first screening level, titles and abstracts were reviewed, and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
|---|---|
Population | Q1 to Q3: People (≥ 16 years of age) requiring treatment for opioid use disorder |
Intervention | Q1 to Q3: Sublingual buprenorphine/naloxone film |
Comparator | Q1 and Q2: Sublingual buprenorphine/naloxone tablets |
Outcomes | Q1: Clinical effectiveness (e.g., complete ingestion of the drug, comparative time to ingestion of the drug, impact on drug diversion, cessation of opioid use, cessation of use of other drugs of abuse, transition to long-term recovery programs, retention in treatment, health-related quality of life, withdrawal symptoms, mental health scores) and safety (e.g., toxicity, adverse events [including deleterious impacts on dental health], mortality) Q2: Cost-effectiveness (e.g., cost per health benefit gained, cost per quality-adjusted life-year, incremental cost-effectiveness ratio) Q3: Evidence-based recommendations (e.g., the role of witness ingestion, appropriateness as a substitute for standard of care, dosing and/or administration [including those specific to dental health], settings of use) |
Study designs | Q1: Health technology assessments, systematic reviews, randomized controlled trials, nonrandomized studies Q2: Economic evaluations Q3: Evidence-based guidelines |
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, were duplicate publications, or were published before 2018. Guidelines with unclear methodology were also excluded.
Critical Appraisal of Individual Studies
One reviewer critically appraised the included publication using the following tool as a guide: the Downs and Black checklist10 for randomized and nonrandomized studies. Summary scores were not calculated for the included studies; rather, each publication's strengths and limitations were described narratively.
Summary of Evidence
Quantity of Research Available
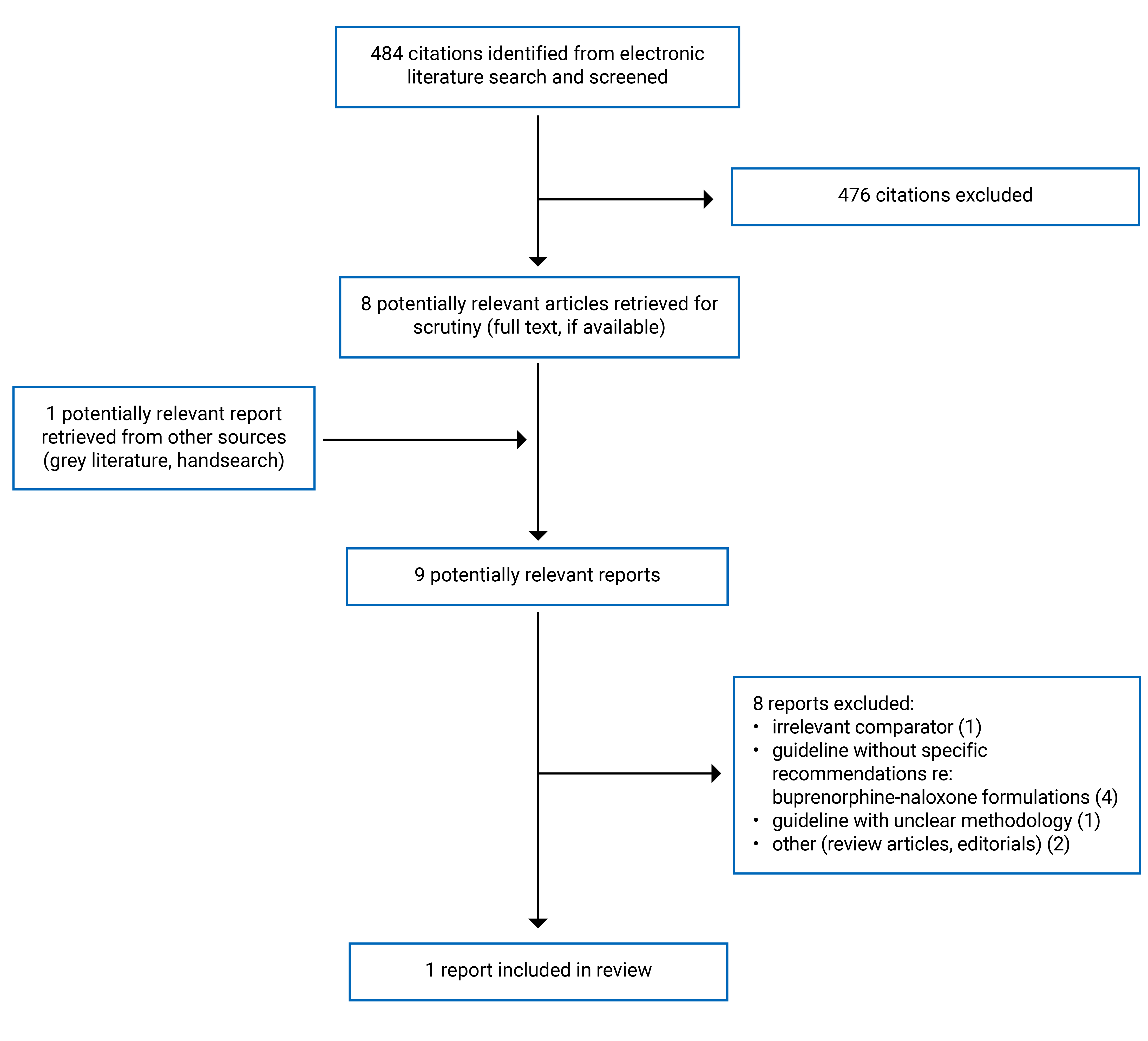
A total of 484 citations were identified in the literature search. Following the screening of titles and abstracts, 476 citations were excluded, and 8 potentially relevant reports from the electronic search were retrieved for full-text review. 1 potentially relevant publication was retrieved from the grey literature search for full-text reviews. Of these potentially relevant articles, 8 publications were excluded for various reasons, and 1 publication met the inclusion criteria and was included in this report. The included publication is an observational study that compared abuse rates of film versus tablet formulations of sublingual BUP-NAL. Appendix 1 presents the PRISMA11 flow chart of the study selection.
Additional references of potential interest are provided in Appendix 5.
Summary of Study Characteristics
Additional details regarding the characteristics of included publications are provided in Appendix 2.
Study Design
A single observational study12 using a cross-sectional design was identified comparing abuse rates between sublingual BUP-NAL films and tablets.
Country of Origin
The study by Butler et al. (2018)12 was conducted in the US.
Patient Population
Butler and colleagues (2018)12 included 2 distinct study populations. The first was adults, aged 18 years and older, assessed for substance use problems and treatment-planning using the Addiction Severity Index-Multimedia Version (ASI-MV) between Q1 2015 and Q3 2015. These data derived from the National Addictions Vigilance Intervention and Prevention Program surveillance system. The second population included individuals within the general population (unclear reporting regarding age) and health care providers seeking medical management advice regarding potentially toxic exposures to prescription opioids, other prescription medications, and illicit drugs between Q1 2015 to Q3 2015. These data were derived from the RADARS System Poison Center Program, which uses a nationally standardized electronic health record to collect data.
Interventions and Comparators
In both study populations in the Butler et al. (2018)12 study the intervention of interest was sublingual BUP-NAL film (Suboxone film), and the comparator was sublingual BUP-NAL tablets (generic or Zubsolv tablets).
Outcomes
In both study populations in the Butler et al. (2018)12 study, the outcomes included prescription volume-adjusted and prescription volume-unadjusted abuse rates as well as the probability of abusing sublingual BUP-NAL film and tablets through alternate routes of administration (e.g., insufflation and injection).
Summary of Critical Appraisal
The included study12 exhibits certain strengths and notable limitations that bear consideration when evaluating its findings. On the positive side, the study demonstrates clear and transparent reporting, covering various essential aspects such as objectives, outcomes, patient characteristics, interventions, potential confounders, and statistical analyses, including P values. This transparency enhances the comprehension of the research process. The study also maintains internal validity by avoiding data dredging and employing appropriate statistical tests while clearly describing the outcome measures. Moreover, it minimizes the risk of confounding by drawing patients from the same population over the same time period.
However, several limitations in the study's design and execution have the potential to introduce bias. Notably, the study's external validity is hindered by the study populations’ and settings' lack of representativeness. These populations are exclusively drawn from individuals seeking treatment at specific centres, raising concerns about selection bias and limiting the generalizability of the findings. For example, specific subpopulations of people with OUD are more likely to seek treatment based on age, gender, and severity of addiction. They may not be representative of the broader population of people with OUD. Additionally, the representativeness of the study settings is unclear, with a lack of information regarding the inclusion of various substance use treatment centres and their geographic locations. This may introduce bias related to the diversity of settings within the population. Finally, the lack of reported power calculations raises questions about the study's statistical power to detect significant effects, potentially leading to type II errors where meaningful associations or differences may go undetected. Considering these strengths and limitations, a careful and critical approach to the study's findings is essential for researchers and readers alike.
Additional details regarding the strengths and limitations of included publications are provided in Appendix 3.
Summary of Findings
Appendix 4 presents the main study findings.
Clinical Effectiveness of Sublingual BUP-NAL Films Versus Tablets
We found limited evidence regarding the clinical effectiveness of sublingual BUP-NAL film compared to tablets for people diagnosed with OUD. A single study12 comparing abuse rates between sublingual BUP-NAL film and tablets is summarized below. No summary can be provided with respect to any further clinical effectiveness measures (e.g., cessation of opioid use, withdrawal symptoms) given that no other clinical studies were identified that met the inclusion criteria for this review.
Abuse Rates
Butler and colleagues (2018)12 compared abuse rates between sublingual BUP-NAL film to tablets in 2 distinct populations. In study population 1 (N = 45,695 adults assessed for substance use problems), sublingual BUP-NAL tablets had a higher prevalence of abuse by any route of administration compared to sublingual BUP-NAL film after adjusting for prescription volume (relative risk = 1.08, 95% confidence interval 1.07 to 1.09, P < 0.001). Similarly, in study population 2 (individuals within the general population seeking medical management advice regarding potentially toxic exposures to opioids), sublingual BUP-NAL tablets had a higher prevalence of abuse by any route of administration after adjusting for prescription volume (relative risk = 1.23, 95% confidence interval 1.02 to 1.50, P = 0.034). These trends held true in both populations when looking at abuse rates by specific routes of administration, including insufflation and injection.
When looking at the effects of gender, race, age, and US region, few significant differences in abuse prevalence were noticed. Among those in study population 1 in the 18 to 34 age group, the prescription-adjusted rate of abuse for sublingual BUP-NAL tablets was significantly higher than for sublingual BUP-NAL film, with a rate of 0.48 cases per 100 ASI-MV respondents per 100,000 dosage units for tablets compared to 0.40 cases for film (relative risk = 1.20, 95% confidence interval 1.05 to 1.38, P = 0.009). Prescription-adjusted rates of abuse within the older groups (35 to 54, 55 plus) were not significantly different for BUP-NAL formulations. The study did not identify any significant effects of gender, race, or US region.
Cost-Effectiveness of Sublingual BUP-NAL Films Versus Tablets
We identified no relevant evidence regarding the cost-effectiveness of sublingual BUP-NAL film versus tablets for treating people with OUD that met our inclusion criteria for this review. Thus, no summary can be provided.
Evidence-Based Guidance for Sublingual BUP-NAL Films
We did not identify any evidence-based guidelines that directly focused on recommendations regarding sublingual BUP-NAL film for treating individuals diagnosed with OUD; therefore, no summary can be provided.
Limitations
Overall Completeness of the Evidence
The findings in this review are constrained by the limited volume of pertinent evidence we could identify. We did not identify any HTA, systematic reviews, or randomized controlled trials that met the inclusion criteria for this review and addressed our research questions. Consequently, we were unable to draw conclusions regarding several aspects of our research questions, including:
the clinical effectiveness of sublingual BUP-NAL films versus tablets beyond potential abuse rates among people with OUD
the cost-effectiveness of sublingual BUP-NAL films versus tablets among individuals with OUD
the availability of evidence-based guidance specifically related to sublingual BUP-NAL films.
Nevertheless, we did manage to locate 1 publication that compared abuse rates for sublingual BUP-NAL films versus tablets among individuals with OUD. It remains unclear whether the scarcity of evidence is due to a true lack of available data regarding sublingual BUP-NAL films or if it reflects an inherent limitation of the methodology employed in this review, particularly the restricted literature search spanning the past 5 years. It is worth noting that during our literature screening, we observed that many of the cited publications concerning BUP-NAL films within the potentially relevant literature were published before 2018, including some that were summarized in a CADTH Rapid Review published in 2019.13 This suggests that research on this topic may have been conducted earlier than the time frame considered for this review, highlighting the evolving nature of the field. In addition, information included within several of the guidelines that were reviewed as potentially relevant to this review did not include specific recommendations about BUP-NAL film, rather, the authors made general recommendations about buprenorphine medication for the treatment of OUD.
Generalizability of the Findings
The included study12 was conducted in the US, using data collected by substance abuse treatment centres and poison centres across the US. Given the paucity of evidence identified in this review, it is unclear whether the results summarized in this review are generalizable to the health care context in Canada. Additionally, the review highlights the absence of evidence regarding specific subpopulations that might be at a higher risk of experiencing elevated opioid-related harms, such as Indigenous groups, disparities between genders, and individuals with lower income levels. This lack of data further underscores the uncertainty regarding the applicability of the review's findings to the Canadian health care context.
Caution should be taken when interpreting the findings of this review.
Conclusions and Implications for Decision- or Policy-Making
This review identified and summarized the clinical effectiveness evidence available on sublingual BUP-NAL films compared to sublingual BUP-NAL tablets (1 cross-sectional study).12
Limited evidence was found on the clinical effectiveness of sublingual BUP-NAL films versus tablets for individuals with OUD. A single study comparing abuse rates between BUP-NAL formulations indicated that in 2 distinct populations, sublingual BUP-NAL tablets had a higher prevalence of abuse than sublingual BUP-NAL films, after adjusting for prescription volume.12 However, no other clinical studies met the inclusion criteria, and there was no available evidence regarding cost-effectiveness or evidence-based guidelines for sublingual BUP-NAL films in managing OUD.
As mentioned above, much of the literature comparing sublingual BUP-NAL films to tablets was published before 2018; thus, it is out of scope for this current review. However, a previous CADTH report published in 2019 assessed clinical and cost-effectiveness evidence and evidence-based guidelines related to buprenorphine formulations for treating OUD and included literature published from 2014 to 2019.13 The literature revealed mixed conclusions on the clinical effectiveness, safety, and cost-effectiveness of various buprenorphine formulations for OUD. While some studies observed differences in outcomes, it was unclear if these differences were clinically meaningful or if 1 formulation was superior. The safety profiles of buprenorphine formulations did not significantly differ, suggesting that they are generally safe and well-tolerated. Economic evaluations indicated that implantable buprenorphine with psychosocial therapy may be more cost-effective than sublingual buprenorphine with psychosocial therapy. Two evidence-based guidelines recommend the use of BUP-NAL for treatment initiation or maintenance in OUD. However, the findings in this report are subject to uncertainty, emphasizing the need for further research, particularly large, well-designed studies, to reduce this uncertainty.
In conclusion, while limited evidence from this review suggests that sublingual BUP-NAL films may lead to lower abuse rates compared to sublingual BUP-NAL tablets among people with OUD, we require more comprehensive research with rigorous methodological approaches to understand this topic better.
References
1.The diagnostic and statistical manual of mental disorders (DSM-5). 5th ed. Washington (DC): American Psychiatric Association; 2013.
2.Strain E. Opioid use disorder: epidemiology, clinical features, health consquences, screening, and assessment. In: TW P, ed. UpToDate. Waltham (MA): UpToDate; 2023: http://www.uptodate.com. Accessed 2023 Oct 15.
3.Carrière G, Garner R, Sanmartin C. Significant factors associated with problematic use of opioid pain relief medications among the household population, Canada, 2018. Ottawa (ON): Statistics Canada; 2021: https://www150.statcan.gc.ca/n1/en/pub/82-003-x/2021012/article/00002-eng.pdf?st=r5oKQpze. Accessed 2023 Oct 6.
4.Federal, provincial, and territorial Special Advisory Committee on the Epidemic of Opioid Overdoses. Opioid- and stimulant-related harms in Canada. Ottawa (ON): Public Health Agency of Canada; 2023: https://health-infobase.canada.ca/substance-related-harms/opioids-stimulants/. Accessed 2023 Oct 15.
5.Carrière G, Garner R, Sanmartin C. Social and economic characteristics of those experiencing hospitalizations due to opioid poisonings. Health Rep. 2018;29(10):23-28. PubMed
6.Hoffman KA, Ponce Terashima J, McCarty D. Opioid use disorder and treatment: challenges and opportunities. BMC Health Serv Res. 2019;19(1):884. PubMed
7.Strain E, Peavy M. Opioid use disorder: treatment overview. In: TW P, ed. UpToDate. Waltham (MA): UpToDate; 2023: http://www.uptodate.com. Accessed 2023 Oct 15.
8.Kampman K, Jarvis M. American Society of Addiction Medicine (ASAM) National Practice Guideline for the use of medications in the treatment of addiction involving opioid use. J Addict Med. 2015;9(5):358-367. PubMed
9.Opioid agonist treatments for opioid use disorders: a rapid qualitative review (CADTH Rapid response report: summary with critical appraisal). Ottawa (ON): CADTH; 2019: https://www.cadth.ca/sites/default/files/pdf/htis/2019/RC1100%20Buprenorphine%20for%20OUD%20Final.pdf. Accessed 2023 Oct 23.
10.Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and nonrandomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377-384. PubMed
11.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
12.Butler SF, Black RA, Severtson SG, Dart RC, Green JL. Understanding abuse of buprenorphine/naloxone film versus tablet products using data from ASI-MV substance use disorder treatment centres and RADARS System Poison Centers. J Subst Abuse Treat. 2018;84:42-49. PubMed
13.Buprenorphine for opioid use disorder: a review of comparative clinical effectiveness, safety, cost-effectiveness, and guidelines (CADTH Rapid response report: summary with critical appraisal). Ottawa (ON): CADTH; 2019: https://www.cadth.ca/sites/default/files/pdf/htis/2019/RC1092%20Buprenorphine%20for%20OUD%20Final.pdf. Accessed 2023 Oct 15.
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Note that this appendix has not been copy-edited.
Table 2: Characteristics of Included Primary Clinical Study
Study citation, country, funding source | Study design | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Butler et al. (2018)12 US Funding source: Indivior Inc., Richmond, VA | Observational study using a cross-sectional study design that makes use of administrative data collected from 2 different study populations | Population 1:
Population 2:
| Intervention: BUP-NAL film (Suboxone® film) Comparator: BUP-NAL tablets including generic and Zubsolv® tablets | Outcomes Population 1: Prescription-adjusted and prescription-unadjusted abuse rates, probability of abusing BUP-NAL film and tablets via alternate routes of administration Population 2: Prescription-adjusted and prescription-unadjusted abuse rates, proportion of cases reporting insufflation or injection use Follow-up: Both populations analyzed data collected from Q1 2015 to Q3 2015 |
BUP-NAL = buprenorphine-naloxone combination product; NR = not reported.
Appendix 3: Critical Appraisal of Included Publications
Note that this appendix has not been copy-edited.
Table 3: Strengths and Limitations of Clinical Study Using the Downs and Black Checklist10
Strengths | Limitations |
|---|---|
Butler et al. (2018)12 | |
Reporting
Internal validity (bias)
Internal validity (confounding)
Power
| External validity
Power
|
Appendix 4: Main Study Findings
Table 4: Summary of Findings by Outcome — Abuse Rates
Butler et al., 201812 cross-sectional study | ||||
|---|---|---|---|---|
BUL-NAL formulation | NAVIPPRO ASI-MV substance abuse treatment centre data (N = 45,695) | RADARS System Poison Center Program data (N = NR) | ||
Abuse prevalence (95% CI) | Tablet vs. Film Relative risk (95% CI) | Abuse prevalence (95% CI) | Tablet vs. Film Relative risk (95% CI) | |
Unadjusted abuse rate per 100 ASI-MV respondents | ||||
Film | 7.01 (6.77 to 7.25) | 0.390 (0.370 to 0.413), P < 0.001 | NA | NA |
Tablet | 2.64 (2.49 to 2.79) | NA | ||
Abuse rate by any route per 100,000 US Census population unadjusted for prescription volume | ||||
Film | 1.126 (1.12 to 1.13) | 0.376 (0.374 to 0.378), P < 0.001 | 0.0364 (0.0326 to 0.0405) | 0.442a (0.364 to 0.538), P < 0.001 |
Tablet | 0.424 (0.42 to 0.43) | 0.0161 (0.0136 to 0.0189) | ||
Abuse rate by any route per 100,000 US Census population adjusted for prescription volume | ||||
Film | 0.00164 (0.001636 to 0.001647) | 1.08 (1.07 to 1.09), P < 0.001 | 0.1703 (0.1525 to 0.1896) | 1.23a (1.02 to 1.50), P = 0.034 |
Tablet | 0.00177 (0.00176 to 0.00178) | 0.2114 (0.1787 to 0.2483) | ||
Abuse rate by insufflation per 100 cases involving intentional abuse of the product | ||||
Film | 8.9 (7.9 to 9.9) | 3.89 (3.30 to 4.58), P < 0.001 | 3.4 (1.5 to 7.4) | 1.73 (0.54 to 5.53), P = NR |
Tablet | 34.4 (31.0 to 38.2) | 5.8 (2.5 to 13.6) | ||
Abuse rate by injection per 100 cases involving intentional abuse of the product | ||||
Film | 18.0 (16.1 to 19.1) | 1.47 (1.25 to 1.72) | 15.6 (11.1 to 22.0) | 1.71 (1.05 to 2.79) |
Tablet | 25.7 (22.5 to 29.3) | 26.7 (18.9 to 37.9) | ||
ASI-MV = Addiction Severity Index-Multimedia Version; CI = confidence interval; NA = not applicable; NAVIPPRO = National Addictions Vigilance Intervention and Prevention Program; NR: Not reported; RADARS = Researched Abuse, Diversion and Addiction-Related Surveillance.
aAdjusted for region.
Note that this appendix has not been copy-edited.
Appendix 5: References of Potential Interest
Previous CADTH Reports
Opioid agonist therapies for adults with opioid dependence in correctional settings (CADTH reference list). Ottawa (ON): CADTH; 2022: https://www.cadth.ca/sites/default/files/pdf/htis/2022/RA1213%20OAT%20Correctional%20Settings%20Final.pdf. Accessed 2023 Oct 15.
Buprenorphine-naloxone tablet versus methadone for the treatment of patients with opioid use disorder: a review of clinical effectiveness, cost-effectiveness, and guidelines (CADTH Rapid response report: summary with critical appraisal). Ottawa (ON): CADTH; 2019: https://www.cadth.ca/sites/default/files/pdf/htis/2019/RC1150%20Suboxone%20vs.pdf. Accessed 2023 Oct 15.
Guidelines and Recommendations
Not Specific to BUP-NAL Films
Opioid therapy: a synthesis of Canadian guidelines for treating opioid use disorder. Toronto (ON): Centre for Addiction and Mental Health; 2021: https://www.camh.ca/-/media/files/professionals/canadian-opioid-use-disorder-guideline2021-pdf.pdf. Accessed 2023 Oct 15.
Unclear Methodology
NSW clinical guidelines: treatment of opioid dependence - 2018. North Sydney (AU): NSW Ministry of Health; 2018: nsw-clinical-guidelines-opioid.pdf. Accessed 2023 Oct 15.
Contributors: Sara Khangura, Chris Kamel
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for noncommercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca