CADTH Health Technology Review
Reprocessed Single-Use Semicritical and Critical Medical Devices
Rapid Review
Authors: Kellee Kaulback, Jennifer Horton
Key Messages
What Is the Issue?
Reprocessing a medical device includes cleaning, reconditioning, testing, and disinfection to ensure the device can safely be reused. In contrast to reusable medical devices, manufacturers are not required to provide instructions for properly cleaning and sterilizing single-use medical devices (SUMDs).
Health Canada regulates third-party device reprocessors and requires they meet the same requirements as new device manufacturers. Health Canada does not provide oversight for hospital onsite reprocessing, deferring to the oversight provided at the provincial and territorial levels. Given the potential economic and environmental benefits of using reprocessed SUMDs, there is a growing interest in determining the clinical safety of reprocessed SUMDs.
Current standards for reprocessing medical devices use definitions for sterilization and disinfection based on measurement of bioburden, but not necessarily clinical outcomes such as infection.
What Did We Do?
To inform decisions about the appropriate use of reprocessed critical and semicritical SUMDs, CADTH sought to identify and summarize literature evaluating the clinical safety of reprocessed SUMDs, defined as infections, mortality, or other adverse events, compared with nonreprocessed (new) SUMDs. Microbiological outcomes, such as bacterial colony counts, were not included. An information specialist searched for peer-reviewed and grey literature sources.
This report does not provide a comprehensive list of device reprocessors in Canada or recommend any specific methods of reprocessing medical devices.
What Did We Find?
We identified 8 studies, including one study based in Canada, which evaluated the use of reprocessed SUMDs compared with new SUMDs; most did not report statistically significant differences in patient outcomes between groups.
Most of the included studies were of very low to moderate quality, which limits confidence in the observed outcomes resulting from the reuse of these devices. Half of the included studies were published before the year 2005, which may limit applicability given potential improvements and changes over time in reprocessing standards, surgical approaches, device specifications, and patient care protocols.
Most of the studies evaluated a different type of reprocessed single-use medical device for different surgical populations, so there is very limited evidence for the use of a specific device in a specific population or intervention of interest. All included studies evaluated SUMDs classified as critical, and all were conducted in surgical settings; however, it is unclear whether patient risk levels would be different for semicritical devices or in nonsurgical settings.
What Does it Mean?
Given various devices, clinical applications, and reprocessing methods, it is difficult to draw broad conclusions about the appropriateness of reprocessing SUMDs.
While the evidence base in this review was insufficient to conclude whether reprocessed critical SUMDs in surgical settings affect patient outcomes, Canadian standards and other resources exist to help inform decisions around medical device reprocessing based on infection risk.
To ensure patient safety, any reprocessing of SUMDs should meet standards for safety, effectiveness, and labelling that follow Health Canada regulations.
Abbreviations
MI
myocardial infarction
PSI
port-site infection
SUMDs
single-use medical devices
Context and Policy Issues
What Is Medical Device Reprocessing?
Reprocessing a medical device encompasses cleaning, reconditioning, function testing, and disinfection or sterilization to ensure the device can safely be reused.1 The terms reuse, reprocessing, and remanufacturing are used somewhat interchangeably in the literature. However, the terms reuse and reprocessing can often refer to more rudimentary checking, cleaning and re-sterilization, often within the health care institution.2 On the other hand, remanufacturing usually describes a process conducted by a third-party, and modern remanufacturing is performed on an industrial scale with rigorous adherence to defined protocols, producing a remanufactured device which has been performance-tested, shown to meet the original equipment manufacturer requirements, and demonstrates verifiable elimination of infective drugs.2
It is up to each manufacturer to decide how to design and label each medical device, and SUMDs that Health Canada licences are intended by their manufacturers to be used once during a single procedure and not to be disassembled, cleaned, reassembled, and reused, where doing so can jeopardize their performance, safety, and effectiveness.3 Manufacturers of SUMDs are not obliged to provide instructions for proper cleaning and sterilization, as they are for reusable devices.
Provincial and territorial policies regarding the reprocessing of medical devices are typically based on the device category, and the internationally accepted classification scheme described by Spaulding, which groups devices according to the risk of infection associated with the device, categorizes medical devices, as follows:4,5
critical – Devices that come in contact with blood or normally sterile tissue, such as surgical forceps
semicritical – Devices that come in contact with mucous membranes, such as endoscopes
noncritical – Devices that come in contact with unbroken skin, such as stethoscopes.
Why Is it Important to Do This Review?
In 2016, Health Canada updated its policy on the purchase and use of reprocessed SUMDs, concluding that it has authority to require that commercially reprocessed devices meet appropriate standards for safety, effectiveness, and labelling, with third-party reprocessing companies held to the same requirements as manufacturers of new devices.6 However, Health Canada does not provide oversight for hospital onsite reprocessing or in community health care settings, deferring to the oversight provided at the provincial and territorial level. Provincial policies generally refer to using third-party commercial processors in accordance with Health Canada requirements.7,8 Given the potential economic and environmental benefits of using reprocessed SUMDs,9-12 yet limited guidance for hospitals to pursue onsite SUMD reprocessing, there is a growing interest in determining the clinical safety of reprocessed SUMDs.
In June 2023, CADTH published a brief summary of studies evaluating critical device category SUMDs that were published over the previous 5 years.5 The report provided limited abstract-level information from 3 studies that met the inclusion criteria. Therefore, this Rapid Review is being undertaken to expand upon the previous report by providing a full-text review and critical appraisal of relevant studies, without limiting to literature published within the past 5 years and including any literature in semicritical device categories. The 3 studies identified in the original report will also be critically appraised and summarized in this update.
Objective
To support decision-making about the appropriate use of reprocessed critical and semicritical SUMDs, this report aims to identify literature evaluating the clinical safety of reprocessed SUMDs compared with nonreprocessed (new) SUMDs.
Research Question
What is the clinical evidence regarding the safety of reprocessed single-use semicritical or critical medical devices compared with new single-use semicritical or critical medical devices?
Methods
Literature Search Methods
An information specialist conducted a literature search on key resources including MEDLINE, the Cochrane Database of Systematic Reviews, the International HTA Database, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search approach was customized to retrieve a limited set of results, balancing comprehensiveness with relevancy. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. Search concepts were developed based on the elements of the research questions and selection criteria. The main search concepts were single-use medical devices and reprocessing. CADTH-developed search filters were applied to limit retrieval to health technology assessments, systematic reviews, meta-analyses, indirect treatment comparisons, and any types of clinical trials or observational studies. The search was completed on September 7, 2023.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1. This report is meant to provide a summary of the safety of reprocessing and does not provide a comprehensive list of device reprocessors in Canada or recommend any specific methods of reprocessing medical devices.
Criteria | Description |
|---|---|
Population | Patients of any age in contact with semicritical or critical medical device |
Intervention | Reprocessed single-use semicritical or critical medical device |
Comparator | New single-use semicritical or critical medical device |
Outcomes | Patient safety (e.g., adverse events, infections, mortality, hospitalizations) |
Study designs | Health technology assessments, systematic reviews, randomized controlled trials, nonrandomized studies |
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1. Articles were also excluded if they evaluated a single-use device that was reused and not reprocessed between uses according to a described reprocessing protocol, whether in-hospital or by a third-party. Articles were excluded if they did not report patient-related outcomes. Systematic reviews were excluded if they did not provide an analysis of patient-related outcomes.
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the Downs and Black checklist13 for randomized and nonrandomized studies as a guide. Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Summary of Evidence
Quantity of Research Available
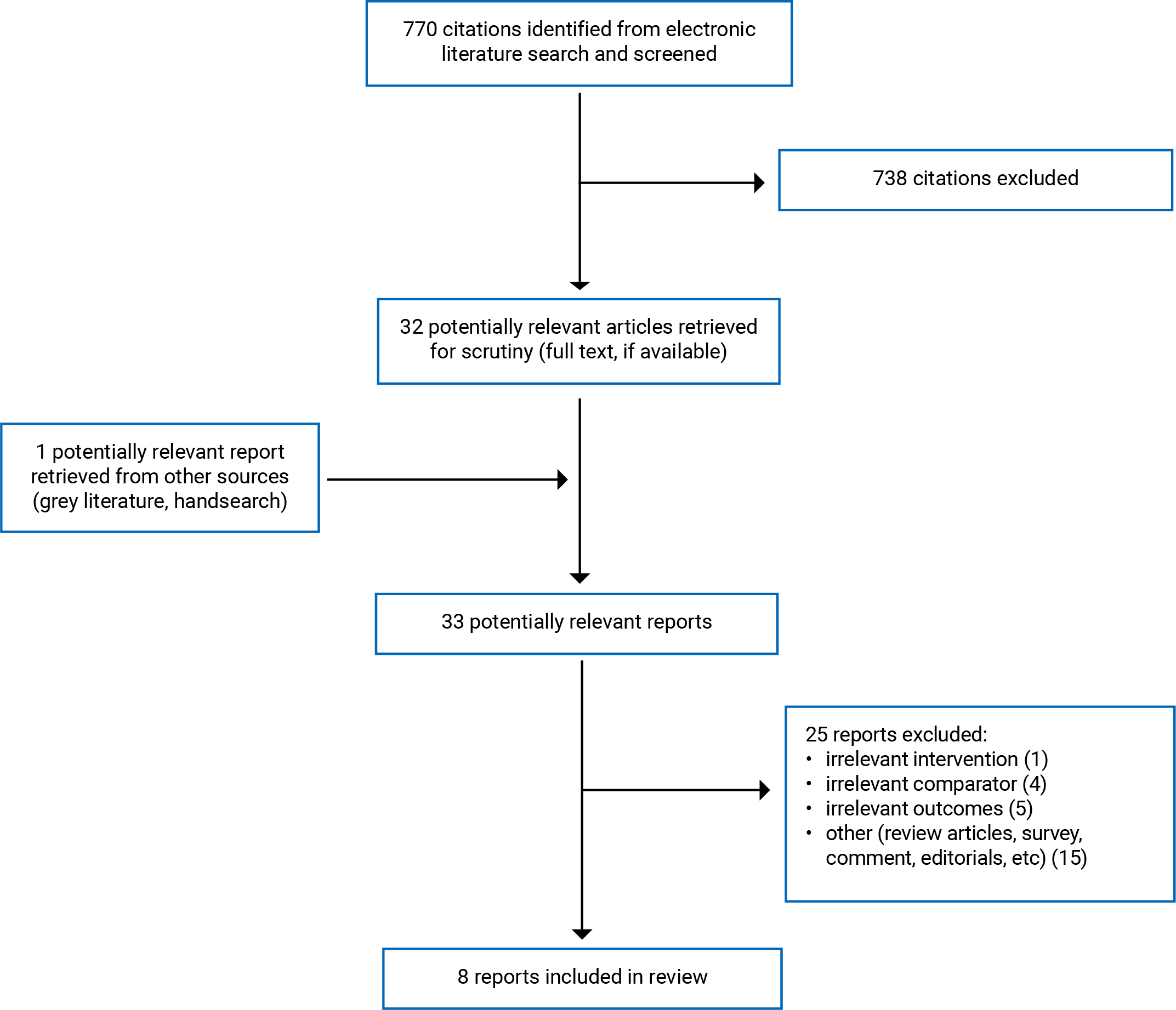
A total of 770 citations were identified in the literature search. Following screening of titles and abstracts, 738 citations were excluded, and 32 potentially relevant reports from the electronic search were retrieved for full-text review. One potentially relevant publication was retrieved from the grey literature search for full-text review. Of these potentially relevant articles, 25 publications were excluded for various reasons, and 8 publications met the inclusion criteria and were included in this report. These comprised 1 randomized controlled trial (RCT), and 7 nonrandomized studies. Appendix 1 presents the PRISMA14 flow chart of the study selection. Additional references of potential interest are provided in Appendix 5.
Summary of Study Characteristics
The literature search identified 8 publications meeting the inclusion criteria.2,15-21 Two publications describing a systematic literature review process conducted in Canada in 1994 were excluded because they focused on economic outcomes and did not provide any synthesis or analysis of patient-related outcomes.1,12
Additional details regarding the characteristics of included publications are provided in Appendix 2.
Study Design
Two prospective cohorts with historical controls were published in 199715 and in 2019,2 and 1 RCT was published in 2004.16 The rest of the included studies were prospective cohort studies published in 1994,17 1998,18 2018,22 2021,20 and 2022.21
Country of Origin
The included studies were conducted in the US,15 Canada,17Brazil,20 Iran,21 Turkey,16,18Portugal,22 and the UK.2
Patient Population
Browne et al.15 enrolled 107 patients scheduled for percutaneous transluminal coronary angioplasty (PTCA) at a single US institution. The mean age of the patients was 64 years, and 56% were male. The indication for coronary angioplasty was stable coronary insufficiency in 69 patients, unstable angina in 22 patients and acute myocardial infarction (MI) in 16 patients.
Plante et al.17 evaluated 693 patients with 853 lesions who underwent coronary angioplasty at 1 of 2 study centres. One study centre used new single-use catheters (n = 373 patients with 452 lesions), while the other used reprocessed single-use catheters (n = 320 patients with 401 lesions). The baseline patient and angiographic characteristics of the 2 groups were comparable except for a higher incidence of unstable angina (70% versus 57%. P < 0035) and nitroglycerin infusions (25% versus I5%) in patients at the reuse centre. The mean age in the single-use group was 60 years, and 73% were male. The mean age in the reprocessed group was 61 years, and 72% were male.
Zacharias et al.20 included 590 endolaser probes used during vitrectomy surgeries performed in a single institution, of which 375 (63.56%) were original and 215 (36.44%) were reprocessed. No details about the patients were provided.
The study population in Jokar et al21 included all candidates for elective laparoscopic cholecystectomy from August 2018 to August 2020. Detailed inclusion and exclusion criteria were provided. The reason for surgery was acute or chronic cholecystitis, biliary colic, or a group described as polyps, stones, or wall thickening. They evaluated 473 patients receiving a new port (n = 215) or a reprocessed disposable port (n = 258) in laparoscopic surgery. The mean age of patients in the new port group was 45.89 versus 46.29 years in the reprocessed port group. In the new port group, 68.8% of the patients were female, compared to 72.1% of the patients in reprocessed port group.
Marins et al.22 included all patients undergoing a wide variety of surgical interventions in a single year (2014) at their institution using specific surgical scissors and a suture machine. The mean age in the reprocessed device group (n = 316) was 56.7 years and 56.6 years in the nonreprocessed group (n = 417). There were 184 (58.2% females in the reprocessing group and 251 [60.2%]) in the nonreprocessed group.
Gundogdu et al.18 evaluated 45 patients (30 female, 15 male) who underwent laparoscopic cholecystectomy due to cholecystitis. The mean age of the patients was 48 years (range 21 to 71 years). Thirty patients were assigned to the reprocessed plastic trocar group, and 15 were assigned to the new plastic trocar group.
In the RCT by Colak et al.,16 of 125 consecutive patients with symptomatic cholelithiasis were randomly assigned to undergo laparoscopic cholecystectomy with either new (group 1) or reprocessed (group 2) disposable laparoscopic instruments. Group 1 consisted of 15 men and 47 women whose mean age was 51 years, and group 2 comprised 12 men and 51 women with a mean age of 52.
Leung et al.2 evaluated 100 consecutive patients undergoing elective atrial fibrillation (AF) ablation with a remanufactured circular mapping catheter. All cases were propensity matched to cases performed using a previously unused circular mapping catheter of the same model selected from a database of 806 patients receiving AF ablations over the previous 4 years. There were an equal number of males in each group (n = 68), and the average age in the remanufactured group was 67.1 years versus 65.8 years in the new catheter group.
Interventions and Comparators
For coronary angioplasty procedures, the Browne et al.15 study reused single-use PTCA balloon catheters shipped to a central facility and decontaminated, cleaned and tested for endotoxin using the Limulus amebocyte lysate gel clot method. Physical testing and quality assurance were performed. Standard angioplasty was then performed using these reprocessed devices. The comparison group was a case-matched control group of 108 patients evaluated retrospectively from an institutional database of patients undergoing PTCA with new catheters. In the Plante et al.17 study, 1 study site used new balloon catheters, and 1 study site employed previously used single-use balloon catheters subject to a strict reprocessing protocol described in detail. Standard angioplasty was performed using these devices.
Zacharias et al.20 included 590 endolaser probes used during vitrectomy surgeries of which 375 (63.56%) were new and 215 (36.44%) were reprocessed following a formal in-hospital reprocessing procedure that was detailed in the publication.
Jokar et al.21 evaluated new single-use surgical ports versus disposable ones previously used for other patients, cleaned and resterilized based on the hospital protocol. A detailed description of the reprocessing protocol was not provided.
Marins et al.22 evaluated a specific brand of single-use surgical scissors and suture machine, either new, or reprocessed, with the reprocessing carried out by a certified reprocessor. The devices can be reprocessed up to 2 times.
Colak et al.16 evaluated new disposable laparoscopic instruments versus reprocessed disposable laparoscopic instruments reused after high-level disinfection by alkalinized 2% glutaraldehyde solution following a detailed in-hospital reprocessing protocol. Gundogdu et al.18 evaluated new single-use plastic trocars versus reprocessed single-use plastic trocars for laparoscopic cholecystectomy, reprocessed according to a detailed in-hospital reprocessing protocol.
Leung et al.2 evaluated using third-party remanufactured single-use circular mapping catheters compared to new catheters for AF ablation. The remanufacturing process addressed both structural and functional integrity and a disinfection protocol.
Outcomes
Browne et al.15 evaluated patient temperature and white blood cell count (WBC) before and 24 hours after the PTCA procedure to screen for pyrogenic reactions. All patients were followed until hospital discharge for evidence of subsequent MI or requirement for emergent percutaneous or surgical revascularization of the target vessel. Long-term follow-up was not performed. The authors also reported mean procedure time, mean fluoroscopy time, mean dye volume, and the average number of balloons used per lesion, though it is unclear what impact these might have on patient outcomes. The need for additional procedures, as well the incidence of MI and mortality, along with the angiographic failure rate was also reported in the reprocessing group. Still, it was not reported for the comparison group.
Plante et al.17 reported procedure duration, fluoroscopy time and volume of contrast medium but did not report how these might impact patient outcomes. Temperatures were recorded 1 hour before angioplasty and every 8 hours during the first 24 hours after the procedure (starting 1 hour after angioplasty) and at least once daily until hospital discharge. Blood was drawn to measure creatine kinase levels before and at 8 and 24 hours after the procedure. Angiographic success was defined as lesional residual stenosis of less than 50%, as determined by visual assessment. Clinical success was defined as an angiographically successful angioplasty of all attempted lesions without any procedure-related in-hospital adverse clinical event, defined as death, MI, stroke, emergency angioplasty or bypass surgery. Clinical failure was designated when all attempted lesions could not be dilated successfully.
Zacharias et al.20 evaluated the functionality of endolaser probes in vitrectomy surgeries, with malfunction defined as the nonvisualization of the burns during intraoperative use that required the use of another probe. The authors did not describe malfunction as being related to patient outcomes. They also reported the frequency of infectious endophthalmitis. The authors describe infectious endophthalmitis as a rare but serious complication related to unfavourable visual outcomes.
Jokar et al.21 reported the incidence of port-site infection (PSI), both superficial and deep infection, through patient self-assessment obtained by telephone call using a researcher-made checklist of infection assessment standards at intervals of 3 to 5 days, and 5 to 14 days, and through physical examination in the hospital on day 14. Superficial infection was described as serous wound drainage, pain and tenderness, redness and warmth, edema and fever, while deep infection was described as suppuration, spontaneous dehiscence, and abscess.
Marins et al.22 reported on the duration of surgical intervention, postoperative infection incidence, antibiotic consumption, reoperations, length of hospital stay, in-hospital mortality, and rehospitalization rate (complications 30 days after surgical intervention).
Gundogdu et al.18 reported the incidence of infection at the wound site and intra-abdominally.
Colak et al.16 evaluated operating time, postoperative pain, duration of intramuscular analgesic administration, hospital stay, complications, and patient satisfaction. Operating time was defined as the time from the first incision to the placement of the last suture, while postoperative pain was assessed 6-hours after the operation according to a linear analogue scale (LAS) that ranged from 0 (no pain) to 10 (worst pain imaginable). The patients were also asked to indicate their overall level of satisfaction (1 = poor, 4 = excellent) at 1 week after cholecystectomy.
Leung et al.2 primarily evaluated device-related outcomes which could potentially affect patient outcomes, including catheter-related complications during or after the procedure, ease of handling the catheter, failure of electrodes to record electrograms or to stimulate appropriately, failure of communication with the electro-anatomic mapping system, and physical defect or deformation of the catheter on inspection after use. Indirect markers of catheter function were also measured, including procedure duration and fluoroscopy duration, as well as complications, including any major adverse cardiovascular/cerebrovascular events (MACCE), vascular injury, or cardiac tamponade.
Summary of Critical Appraisal
Prospective Cohort Studies with Historical Controls
The Browne et al.15 prospective cohort study with historical controls demonstrated serious reporting issues, external and internal validity issues. Very limited outcomes were reported for the historical comparison group. The included participants were selected from the same hospital, but it is not described whether they are consecutive, or whether any potential participants might have been excluded, limiting the generalizability and validity of the study results. The retroactive comparison group was not well-described, and a list of potential confounders was not provided. Most outcomes were not reported with statistical significance or statistical ranges, including patient safety outcomes. Follow-up for fever, chills and elevated WBC was reported only up to 24 hours postprocedure, and therein patients were followed only until hospital discharge. There was no long-term follow-up. The study was powered to detect a 5% difference in the angiographic failure rates of new and reused balloons, yet the failure rate for the comparison group did not appear to be provided.
Leung et al.2 conducted a well-reported prospective cohort study with historical controls. Loss to follow-up was not reported, a power calculation was not described, and most importantly, there are bias and confounding concerns due to the lack of randomization and blinding, which is typical of observational studies. Also, as the study used historical controls, the treatment groups were not recruited over the same period, which means there could be differences between patients, providers, or other factors that may have impacted the observed outcomes.
Prospective Cohort Studies
The Plante et al.17 study was a prospective cohort study evaluating balloon catheters for coronary angioplasty at 2 sites in the same province in Canada, with 1 site using reprocessed single-use catheters and 1 site using new catheters. While the 2 sites were described as performing a comparative number of angioplasty procedures, having similar case selection, and comparable operator experience and skills, the use of a control group at a second centre has the potential for differences in patient groups, practice patterns and other factors that could confound the observed results. At baseline, there were statistically significant differences in the incidence of unstable angina (and related IV heparin and nitroglycerin use before the procedure) between the 2 centres, which may suggest that more high-risk lesions were treated in the reprocessed device group. Therefore, the observed outcomes (such as longer procedure duration, adverse events, etc.) may have been at least partly due to differences in the groups at baseline. Overall, the Plante et al.17 study was well-reported, but demonstrates issues with external validity and internal validity, particularly confounding.
Zacharias et al.20 reported on a prospective cohort study comparing reprocessed single-use endolaser probes with new probes in vitrectomy surgeries. The study demonstrated issues with reporting, external validity, and internal validity. There was no description of the patient groups or any indication of how the patients were selected or assigned to treatment. Because of the flaws in the study design there is considerable likelihood of bias, confounding, and lack of generalizability, limiting confidence in the reported results.
Jokar et al.21 conducted a well-reported prospective cohort study evaluating the incidence of PSIs in patients undergoing laparoscopic cholecystectomy. There was no description of blinding of patients or outcome assessors or allocation concealment. They did report quasi-randomized allocation to treatment groups (if the last digit of the ID patient was odd, the patient was selected for the disposable port group, and if it was even, the patient was selected for the reprocessed port group), which may have limited bias to some extent. There appears to be a small loss to follow-up of 3 patients that was not reported or addressed by the authors, though this small number is unlikely to have impacted the observed outcomes. Though adverse events were reported, they were largely determined through patient self-report (which may not be as objective as if assessed by a health care professional using a validated outcome measure). Follow-up may not have been sufficiently long-term to assess all adverse events.
Marins et al.22 conducted a well-reported prospective cohort study evaluating surgical scissors and suture machines. Although the study scored well in terms of external validity and therefore generalizability, and also in many aspects related to confounding and bias, it had a few flaws typical of observational studies, including lack of randomization of patients to each intervention arm with assignment concealment, and there was no blinding of patients and outcome assessors described. Length of follow-up and loss to follow-up were not reported, and a power calculation was not performed. Without a power calculation, it is unclear whether nonsignificant differences between groups were real or related to the underpowering of the study to detect a difference between groups.
Gundogdu et al.18 conducted a prospective cohort comparing new versus reprocessed single-use plastic trocars. The study demonstrated serious issues with reporting and external validity, and internal validity, with regards to bias and confounding. There was very little focus on patient outcomes. The primary outcome of interest seemed to be on culturing bacteria on surgical equipment and at the patient's surgical site rather than on actual patient outcomes such as infection.
Randomized Controlled Trials
Colak et al. (2004)16 conducted an RCT evaluating the reuse of disposable laparoscopic instruments compared with new use. The RCT was well-reported, and scored very well with regard to external validity, and internal validity, both bias and confounding, meaning that the study results are generalizable to similar populations, and that 1 can have confidence in the results of the study. The only issues noted were that the proportion of patients that agreed to participate in the study was not stated, and it is not known if blinding of outcome assessors occurred, though patients and surgeons were blinded. No power calculation was described, which may have affected the lack of observed differences between groups.
Additional details regarding the strengths and limitations of included publications are provided in Appendix 3.
Summary of Findings
Balloon Catheters
Infection
Browne et al.15 concluded that there was “no significant difference” in frequency of fever or WBC count (a measure of infection) between the reprocessing group and the new catheters group. No patient in the control group had chills, while 1 person in the reprocessing group had chills. Other causes explained the elevated WBC in the reprocessing group in 9 patients (MI in 4, hematoma in 3, steroids in 1, and urinary tract infection in 1).
Plante et al.17 reported that fever was noted in 3 patients in the reprocessing group (in association with urinary tract infection, pneumonia and the postoperative period after urgent bypass surgery) and in 1 patient in the single-use centre (flulike illness), and in all cases, fever did not appear to be related to the catheterization procedure.
Other Outcomes
Browne et al.15 reported that the mean procedure time was 67 minutes in the reprocessing group compared with 83 minutes in the comparison group. The mean fluoroscopy time for the procedures was 13 minutes in the reprocessing group compared with 18 minutes in the comparison group. The mean dye volume was 275 mL compared with 307 mL in the comparison group. The incidence of device failure was 7%, which the authors claim compares with a 10% rate reported in the literature for new balloon catheters. Device failure was not reported for the comparison group in the retrospective review. P values were not reported for any outcomes.
Plante et al.17 reported that the angiographic success rate in both the reprocessed and single-use groups was identical at 88%. The reprocessing site utilized more balloon catheters per lesion (mean 2.4 catheters in the reprocessing group versus 1.2 in the single-use group, P < 0.00001), and had a higher incidence of initial balloon failure (10.2% versus 3.3%, P < 0.0001). The reprocessing group exhibited longer procedure times (81 minutes versus 68 minutes, P < 0.0001) and utilized an increased volume of contrast medium. (201 mL versus 165 mL, P < 0.0001), and increased adverse events, particularly in patients with unstable angina (7.8% versus 3.8%, P < 0.25). Hospital stay was significantly greater in the reprocessing group (5.1 days versus 3.4 days, P < 0.0001). No statistically significant differences in clinical success and failure were reported between the 2 groups. Overall clinical success rate and the rate of clinical failure without adverse clinical events were comparable in the 2 groups. Still, the rate of clinical failure with adverse clinical events was significantly higher in the reuse group (7.8% versus 3.8%. P < 0.025).
Endolaser Probes
Zacharias et al.20 conducted a two-phase study, with the first phase reporting in vitro results for the feasibility, sterility and physical integrity of single-use Endolaser probe reprocessing in vitreoretinal surgery. The results of the first phase are not in scope for this report based on the inclusion criteria in Table 1 and therefore are not reported here. The second phase included 590 endolaser probes, of which 375 were original and 215 were reprocessed, and reported statistically significant functionality rates between groups. Among the original probes, 373 (99.47%) were functioning and 2 (0.53%) were nonfunctioning. Among the reprocessed ones, 201 (93.5%) were functioning and 14 (6.5%) were nonfunctioning (P < 0.001) for an odds ratio OR = 12.99 (P < 0.001). It is not clear if the functionality rates would impact patient outcomes. The frequency of infectious endophthalmitis was zero in both groups.
Surgical Ports
Jokar et al.21 reported that the incidence of PSI was significantly higher in the reprocessed port group than in the new port group at all evaluated time points up to 2 weeks after surgery. All PSIs were considered superficial, and no symptoms of deep infection were reported. Individuals in the disposable port group had a maximum of 2 symptoms of superficial infection, but there were usually more than 2 symptoms in the reprocessed port group.
Surgical Scissors and Suture Machines
Marins et al.22 reported that the differences in postoperative infection rate between the reprocessed and nonreprocessed group were not statistically significant. There was a wide range of differences in postoperative infection rate depending on the severity of the condition and the type of surgery. There were also no statistically significant differences in antibiotic consumption.
The duration of the surgical intervention was on average 2 hour and 23 minute (P = 0.161), and length of hospital stay was approximately 10 days in both groups (P = 0.881). Rehospitalization was required for 28 patients in the reprocessing group and for 33 patients in the nonreprocessed group (P = 0.678). There was no statistically significant difference in mortality (P = 0.396). Hospital mortality in the reprocessing group was 1.90%, resulting in 6 deaths, and it was 2.88% (12 deaths) in the nonreprocessing group. There were no reoperations in either group.
Laparoscopic Plastic Trocars
Gundogdu et al.18 focused mainly on nonpatient outcomes in a prospective cohort study. Nonpatient related outcomes are not reported here because they are out of scope. The only patient outcome reported was infection which was evaluated using Cruise’s criteria. None of the patients had infection at the wound site or intra-abdominally.
Laparoscopic Surgical Instruments
Colak et al.16 reported that there was no statistically significant difference between the new and the reprocessed disposable laparoscopic instrument groups in mean operating time, LAS, duration and amount of analgesic administration, or hospital stay. The total incidence of complications (3.2% vs 4.8%, P = 0.50) and infection rates (1.6% vs 3.2%, P = 0.57) were also similar. The median satisfaction rate of the patients was excellent in both groups (P = 0.87)
Circular Mapping Catheters
Leung et al.2 reported that the procedure duration was similar in the remanufactured group (178.9 minutes) and the matched new catheter control group (189.5), P = 0.16). There was a statistically significant higher overall fluoroscopy duration in the new catheter group (21.5 minutes) versus the remanufactured group (11.8 minutes), P < 0.0001). There were no minor or major complications in either group. There was 1 mapping catheter failure in the manufactured group versus no failures in the new use group.
Appendix 4 presents the main study findings.
Limitations
There is just 1 study conducted in Canada,17, and the results of the studies conducted in the other countries may not be generalizable to Canadian populations and settings. In addition, the study conducted in Canada was published in 1994, and it is unknown if the same surgical methods, device specifications, patient care protocols, and reprocessing standards would be relevant today. In fact, of the 8 included studies,415-18 were published before the year 2005, which potentially limits the applicability of at least half of the studies reported. As an example, in 1 study using historical controls, the authors suggested that the decreased fluoroscopy time observed in the reprocessed device group during angiography was likely due to progressive decline in reliance on fluoroscopy seen in their institution over time, rather than to the intervention.2
The body of evidence was appraised to be of very low to moderate quality, and there is just 1 high-quality RCT16 that evaluated the use of reprocessed SUMDs. However, the RCT was published in 2004, was conducted in Turkey, and evaluates SUMDs that were reprocessed using an in-hospital protocol, which could limit its generalizability to the Canadian population and Canadian health care settings, as well as setting where third-party reprocessing is utilized.
While 8 studies met the inclusion criteria in this Rapid Review, they mostly looked at different devices for different interventions, which limits the amount of evidence available to evaluate the patient outcomes for a specific device/intervention. Two studies evaluated balloon catheters for coronary angioplasty,15,17 1 evaluated a mapping catheter for AF,2 1 evaluated plastic trocars for laparoscopic cholecystectomy,18 1 evaluated disposable laparoscopic instruments for laparoscopic cholecystectomy,16 1 evaluated surgical ports in laparoscopic cholecystectomy,21 1 evaluated surgical scissors and suture machine across a wide variety of surgical interventions,22 1 study evaluated endolaser probe reprocessing in vitreoretinal surgery.20 Due to the heterogeneity across studies, including reported outcomes, it is difficult to make comparisons or draw conclusions about the safety of reusing SUMDs. The majority of studies did not report statistically significant impacts on patient outcomes.
None of the included studies evaluated semicritical use devices, and all of the included studies took place in surgical settings.
Finally, the majority of the studies employed an in-house reprocessing protocol, and not the presumably more rigorous third-party reprocessing protocol, which has the potential to impact study results. Protocols varied by institution, by device, and it is assumed, also by third-party processor.
Conclusions and Implications for Decision- or Policy-Making
Conclusions Based on the Available Evidence
This Rapid Review identified 8 studies evaluating the use of reprocessed SUMDs compared with new SUMDs, most of which employed a different reprocessing protocol, and evaluated different reprocessed SUMDs in patients undergoing different surgical interventions. Three studies2,15,19 used third-party reprocessing or remanufacturing of SUMDs, while the rest described in-hospital reprocessing protocols that varied by institution. Of the 8 included studies, only 2 studies evaluated the same device in the same population (balloon catheters for coronary angiography15,17) while the rest of the included studies evaluated a variety of devices across different populations. It is difficult to compare outcomes or draw conclusions on the safety of reprocessed SUMDs based on the existing body of evidence since the population under study, the intervention, the outcomes reported, and the method of reprocessing varies. In addition, most of the published evidence was of very low to moderate quality, and published in countries outside of Canada, with at least half of the evidence published before 2005, which raises concerns regarding generalizability and applicability. It is likely that device specifications, reprocessing protocols, and surgical approaches and patient care protocols have changed since some of these studies were published.
The 2 studies that reported on the same intervention (balloon catheters) in the same population (coronary angiography) came to different conclusions, with Plante et al17 reporting higher rates of adverse events and other procedure-related issues in the reprocessed SUMD group, while Browne et al15 described much more favourable results. However, Plante et al17 used an in-house reprocessing protocol, whereas Browne et al15 used a third-party reprocessor, and there may have been differences between the patients groups at baseline in each study. Three studies evaluated the same study population, patients undergoing laparoscopic cholecystectomy, but in each case evaluated a different intervention: disposable laparoscopic instruments,16 plastic trocars,18 and surgical ports.21 For laparoscopic cholecystectomy patients, the use of reprocessed surgical ports led to a significant increase in PSI,21 while the use of reprocessed plastic trocars and other disposable laparoscopic instruments reportedly did not increase infection rates.16,18 The majority of studies did not report statistically significant differences in patient outcomes with the use of reprocessed SUMDs. However, it is unclear whether the observed outcomes are due to the reuse of single-use devices, or to differences between the devices themselves, or reprocessing protocols.
Studies evaluating semicritical devices were not identified, and all included studies evaluated critical category devices in surgical settings. However, it may be reasonable to assume that there would not be greater risks to patient safety when considering use of reprocessed semicritical SUMDs than reprocessed critical SUMDs. Most of the included studies had limited follow-up, so long-term outcomes for many patients were not available. In addition, outcomes were reported in which the impact on patient outcomes was not made clear. For example, reported outcomes such as procedure duration, fluoroscopy duration, and device failure would likely have some impact on patient outcomes, but it was not always clear what these impacts might be.
In the included studies, it was not always clear how often a SUMD was reprocessed, which is an important consideration in any reprocessing policy. For balloon catheters specifically, Browne et al.15 reported that it is unknown how many cycles of restoration a single balloon angioplasty catheter can tolerate, and that data are required to evaluate the degradation of these products with each subsequent cycle. Browne et al.15 also reported that using simple methods of cleaning and decontamination followed by radiation sterilization does not offer enough of a guarantee of safety to permit reuse. Plante et al.17 have emphasized that before a policy of balloon catheter reuse is initiated, it is imperative to establish clear and rigorous guidelines for cleaning and sterilization, and with adequate monitoring and quality control in place at all stages. Browne et al.15 emphasized the important differences between in vitro evaluation and in vivo evaluation and stated that methods of restoration must be highly controlled and reproducible. Marins et al22 emphasize that a certified reprocessing process requires rigorous inspection, with demanding criteria and guidelines specific to each device. They point out that these stringent criteria allow the detection of any type of anomaly, which is not the case in original medical devices whose quality control is done by sampling.
The reuse of SUMDs also has important potential economic and environmental benefits, which have been evaluated elsewhere.9-12
Standards and Resources to Inform Medical Device Reprocessing
In community health care settings (defined as any location outside of an acute care hospital where health care is provided), reprocessing of critical and semicritical medical equipment/devices, when not performed according to current standards, has been linked with health care-associated infections and outbreaks.23 Therefore, a 2019 position statement for community health care settings published by Infection Prevention and Control Canada, states that critical and semicritical medical equipment/devices labelled as single-use must not be reprocessed and reused unless a licensed reprocessor does the reprocessing.23
The Canadian Standards Association has published a 2023 standard regarding Canadian medical device reprocessing for all health care settings (CSA Z314:23), superseding an earlier version published in 2018, but excludes reprocessing of SUMDs.24
In 2018, the FDA (FDA) reviewed and officially reported on the remanufacturing industry over the previous 2 decades and found no evidence that using remanufactured devices increased risk to health.2 The Medicines and Health care Products Regulatory Agency also permits remanufacturing single-use devices within strict guidelines.25
Suggestions for Future Research
There is a need for high-quality studies evaluating patient outcomes using the following reprocessed SUMDs in Canadian health care settings and populations, using standardized reprocessing protocols, to inform the existing body of evidence. Standardized measures should be employed to evaluate the desired patient outcomes, and the length of follow-up is an important consideration. Defining the number of reprocessing cycles that a particular SUMD can tolerate is also important.
References
1.Hailey D, Jacobs PD, Ries NM, Polisena J. Reuse of single use medical devices in Canada: clinical and economic outcomes, legal and ethical issues, and current hospital practice. Int J Technol Assess Health Care. 2008;24(4):430-436. PubMed
2.Leung LW, Evranos B, Grimster A, et al. Remanufactured circular mapping catheters: safety, effectiveness and cost. J Interv Card Electrophysiol. 2019;56(2):205-211. PubMed
3.Reprocessing of Single-Use Medical Devices: A 2015 Update. Ottawa (ON): CADTH; 2015: https://www.cadth.ca/reprocessing-single-use-medical-devices-2015-update. Accessed 2023 Oct 12.
4.Spaulding's Classification of Medical Equipment/Devices and Required Level of Processing/Reprocessing. Toronto (ON): Public Health Ontario; 2017: https://www.publichealthontario.ca/-/media/documents/c/2017/cds-spaulding-table.pdf?la=en. Accessed 2023 Sep 25.
5.Reprocessed Single-Use Medical Devices. Ottawa (ON): CADTH; 2023: https://www.cadth.ca/sites/default/files/pdf/htis/2023/RB1671%20Single-Use%20Devices%20Final.pdf. Accessed 2023 Sep 25.
6.Update: Notice to Stakeholders - Health Canada's Regulatory Approach to Commercial Reprocessing of Medical Devices Originally Labelled for Single Use. Ottawa (ON): Health Canada; 2016: https://www.canada.ca/en/health-canada/services/drugs-health-products/medical-devices/activities/announcements/update-notice-stakeholders-regulatory-approach-commercial-reprocessing-medical-devices-originally-labelled-single-use.html. Accessed 2023 Sep 25.
7.Reusable & Single-Use Medical Devices Standards: Standards for the reprocessing of reusable medical devices and for the use of single-use medical devices in all health care facilities and settings. Edmonton (AB): Alberta Health; 2019: https://open.alberta.ca/dataset/fd371ac2-b2be-49ac-93ef-43865a0bc0fb/resource/56c1cd3c-b617-4d91-947d-3e0e4a68cd09/download/health-reusable-single-use-medical-devices-standards.pdf. Accessed 2023 Sep 25.
8.Best Practices for Cleaning, Disinfection and Sterilization of Medical Equipment/Devices In All Health Care Settings, 3rd edition Toronto (ON): Public Health Ontario; 2013: https://www.publichealthontario.ca/-/media/Documents/B/2013/bp-cleaning-disinfection-sterilization-hcs.pdf?rev=7a36d8e526644eb794a9ef066d97a120&sc_lang=en. Accessed 2023 Sep 25.
9.Keil M, Viere T, Helms K, Rogowski W. The impact of switching from single-use to reusable healthcare products: a transparency checklist and systematic review of life-cycle assessments. Eur J Public Health. 2023;33(1):56-63. PubMed
10.Lam K, Gadi N, Acharya A, Winter Beatty J, Darzi A, Purkayastha S. Interventions for sustainable surgery: a systematic review. Int J Surg. 2023;109(5):1447-1458. PubMed
11.Bolten A, Kringos DS, Spijkerman IJB, Sperna Weiland NH. The carbon footprint of the operating room related to infection prevention measures: a scoping review. J Hosp Infect. 2022;128:64-73. PubMed
12.Jacobs P, Polisena J, Hailey D, Lafferty S. Economic analysis of reprocessing single-use medical devices: a systematic literature review. Infect Control Hosp Epidemiol. 2008;29(4):297-301. PubMed
13.Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377-384. PubMed
14.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
15.Browne KF, Maldonado R, Telatnik M, Vlietstra RE, Brenner AS. Initial experience with reuse of coronary angioplasty catheters in the United States. J Am Coll Cardiol. 1997;30(7):1735-1740. PubMed
16.Colak T, Ersoz G, Akca T, Kanik A, Aydin S. Efficacy and safety of reuse of disposable laparoscopic instruments in laparoscopic cholecystectomy: a prospective randomized study. Surg Endosc. 2004;18(5):727-731. PubMed
17.Plante S, Strauss BH, Goulet G, Watson RK, Chisholm RJ. Reuse of balloon catheters for coronary angioplasty: a potential cost-saving strategy? J Am Coll Cardiol. 1994;24(6):1475-1481. PubMed
18.Gundogdu H, Ocal K, Caglikulekci M, Karabiber N, Bayramoglu E, Karahan M. High-level disinfection with 2% alkalinized glutaraldehyde solution for reuse of laparoscopic disposable plastic trocars. J Laparoendosc Adv Surg Tech A. 1998;8(1):47-52. PubMed
19.de Sousa Marins B, Queiroz e Melo J, Logarinho Monteiro JL, Rente G, Teixeira Bastos P. Reprocessing of single-use medical devices: Clinical and financial results. Port J Public Health. 2019;36(3):150-156. https:// karger.com/ pjp/ article/ 36/ 3/ 150/289169/ Reprocessing -of -Single -Use -Medical -Devices. Accessed 2023 Sep 19.
20.Zacharias LC, da Silva Conci L, Megnis BP, et al. Safety and cost-effectiveness of single-use endolaser probe reprocessing in vitreoretinal surgery. Int J Retina Vitreous. 2021;7(1):22. PubMed
21.Jokar M, Larti N, Zarei M, et al. Comparative Study of the Incidence of Port Site Infection in Disposable Ports and Reprocessed Disposable Ports in Laparoscopic Cholecystectomy. Surg Laparosc Endosc Percutan Tech. 2022;32(6):650-654. PubMed
22.de Sousa Marins B, Queiroz e Melo J, Logarinho Monteiro JL, Rente G, Teixeira Bastos P. Reprocessing of single-use medical devices: Clinical and financial results. Port J Public Health. 2019;36(3):150-156.
23.POSITION STATEMENT: Reprocessing of Critical and Semi Critical Devices in Community Healthcare Settings. Winnipeg (MB): Infection Prevention and Control Canada. 2019. https://ipac-canada.org/photos/custom/Members/pdf/Reprocessing%20of%20Critical%20and%20%20%20Semi-Critical%20Devices%20in%20the%20Community_Pos.._6Nov2019%20(1)%20-%20FINAL.pdf Accessed 2023 Sep 25. 2019.
24.CSA Z314:23: Canadian medical device reprocessing in all health care settings. Toronto (ON): Canadian Standards Association; 2023: https://www.csagroup.org/store/product/2704392/. Accessed 2023 Sep 26.
25.Single-use medical devices: UK guidance on re-manufacturing. London (UK): Medicines and Healthcare Products Regulatory Agency; 2016: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/534784/Remanufacture_SUD_guidance.pdf. Accessed 2023 Sep 26.
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Note that this appendix has not been copy-edited.
Table 2: Characteristics of Included Primary Clinical Studies
Study citation, country, funding source | Study design | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Browne et al. (1997)15 US Funding source: Supported by Watson Clinic Center for Research, Inc., Lakeland, Florida. | Prospective cohort with historical controls | All patients scheduled for coronary angioplasty at a single institution PTCA (Reprocessed): N = 107 Mean age, years (SD): 64 (12) (range: 29 to 87 years) Male: 56% Stable coronary insufficiency: 69 Unstable angina: 22 Acute MI: 16. Comparator (new): N = 108 Case-matched control group from retrospective database | Intervention: Reprocessed PTCA balloon catheters using strict reprocessing protocol Comparator: New single-use PTCA balloon catheters | Outcomes: Temperature, WBC, chills within 24 hour Follow-up: Within 24 hours and until hospital discharge No long-term follow-up performed |
Plante et al.(1994)17 Canada Funding source: Supported in part by a grant from the Centre Hospitalier Universitaire de Sherbrooke (the reprocessed device centre) | Prospective cohort (2-site) | N = 693 patients with 853 lesions undergoing coronary angioplasty Balloon catheter (reprocessed) group: n = 320 patients with 401 lesions Mean age: 61 +/− 11 years 72% male Balloon catheter (new): n = 373 patients with 452 lesions Mean age: 60 +/− 11 years 73% male Significant between-group differences: Unstable angina Reprocessed: n = 224 (70%) Single use: n = 213 (57%) P < 0.005 Nitroglycerin infusions Reprocessed: n = 81 (25%) Single use: n = 54 (15%) P < 0.0005 | Intervention: Reprocessed balloon catheters using strict reprocessing protocol Comparator: New single-use balloon catheter | Outcomes:
Follow-up: Temperatures were recorded 1 hour before angioplasty and every 8 hours during the first 24 hours after the procedure, and at least once daily until hospital discharge. |
Zacharias et al. (2021)20 Brazil Funding source: Self-funded | Prospective cohort (single site) | Patients undergoing vitreoretinal surgery Population characteristics not described | N = 590 endolaser probes n = 375 new endolaser probes; n = 215 reprocessed using a formal reprocessing protocol | Outcomes: Probe malfunction Incidence of infectious endophthalmitis Follow-up: 1 year |
Jokar et al. (2022)21 Iran Funding: NR | Prospective cohort | N = 473 candidates for elective LC meeting the inclusion criteria Reason for surgery:
New port: n = 215 Reprocessed disposable port: n = 258 Mean age: New port: 45.89 years Reprocessed disposable port: 46.29 years Gender New port: 68.8% female Reprocessed disposable port: 72.1% | Intervention: Reprocessed single-use surgical port, limited description of reprocessing according to hospital protocol Comparator: New single-use surgical port | Outcomes and follow-up: PSI 3 to 5 days after surgery, 5 to 14 days after surgery, and overall, 3 to 14 days after surgery |
Marins et al. (2018)22 Portugal Funding: NR | Prospective cohort | All patients undergoing a wide variety of surgical interventions in a single year at a single institution N = 733 Mean age: Reprocessed device group (n = 316): 56.7 (± 17.3) years Nonreprocessed device group (n = 417): 56.6 (± 16.7) years | Intervention: Reprocessed single-use linear suture machine GIA CovidienTM and the Harmonic ACE® scissors reprocessed by a certified reprocessor Comparator: New single-use linear suture machine GIA CovidienTM and the Harmonic ACE® scissors | Outcomes:
Follow-up: NR but 30-day rehospitalization rate reported so assumed follow-up of 30 days |
Gundogdu et al. (1998)18 Turkey Funding: NR | Prospective cohort | N = 45 patients undergoing LC for cholecystitis 30 female, 15 male Mean age: 48 years (range approximately21 to 71 years) Reprocessed trocars: n = 30 New single-use trocars: n = 15 | Intervention: Plastic trocars reprocessed according to a detailed protocol, including after high-level disinfection by alkalinized 2% glutaraldehyde Comparator: New single-use plastic trocars | Outcomes: Infection at the wound site or intra-abdominally Follow-up: Until surgical discharge on the 1st or 2nd postoperative day |
Colak et al. (2004)16 Turkey Funding: NR | RCT | N = 125 consecutive patients with symptomatic cholelithiasis New DLIs: n = 62 Gender: 15 men and 47 women Mean age: 51 ± 12.57 years Reprocessed DLIs (n = 63): Gender: 12 men and 51 women (P = 0.48) Mean age: 52 ± 12.29 years (P = 0.39) | LC using new DLIs LC using reprocessed DLIs Reprocessed using high-level disinfection by alkalinized 2% glutaraldehyde solution according to a detailed reprocessing protocol | Outcomes:
Follow-up: 6 months |
Leung et al. (2019)2 Funding: One author reported funding from Biosense Webster and from Medtronic (not clear if funding was for this study) | Prospective cohort with historical controls | N = 100 consecutive patients undergoing elective AF ablation using a remanufactured catheter Propensity matched case-controls from a database of 806 receiving AF ablation over the previous 4 years Males: n = 68 in both groups Average age: Remanufactured: 67.1 ± 8.5 years New 65.8 ± 9.1 SD | Remanufactured circular mapping catheter (third-party remanufacturer) at the first reuse cycle New use circular mapping catheter | Outcomes:
Follow-up: 3 months |
AF = atrial fibrillation; DLIs = disposable laparoscopic instruments; LC = laparoscopic cholecystectomy; NR = not reported; PTCA = percutaneous transluminal coronary angioplasty; RCT: randomized controlled trial.
Note: For all studies, outcomes clearly not related to patient outcomes, such as economic or in vitro outcomes, were not included here as they are out of scope.
Appendix 3: Critical Appraisal of Included Publications
Note that this appendix has not been copy-edited.
Table 3: Strengths and Limitations of Clinical Studies Using the Downs and Black Checklist13
Strengths | Limitations |
|---|---|
Browne et al. (1997)15 | |
Reporting
External validity
Internal validity (bias)
Internal validity (confounding)
Power
| Reporting
External Validity
Internal Validity (Bias)
Internal Validity (Confounding)
|
Plante et al. (1994)17 | |
Reporting
External validity
Internal Validity (Bias)
Internal validity (confounding)
| Reporting
External Validity
Internal Validity (Bias)
Internal Validity (Confounding)
Power
Other: Very limited length of follow-up may not be adequate to assess outcomes |
Zacharias et al. (2021)20 | |
Reporting
External validity
Internal validity (bias)
Internal Validity (Confounding)
| Reporting
External Validity
Internal Validity (Bias)
Internal Validity (confounding)
Power
|
Jokar et al. (2022)21 | |
Reporting
External Validity
Internal Validity (Bias)
Internal validity – confounding
Power
| Reporting
External Validity
Internal Validity (Bias)
Internal Validity (Confounding)
|
Marins et al. (2018)22 | |
Reporting
External Validity
Internal Validity – Bias
Internal validity – Confounding
| Reporting
Internal Validity – Bias
Internal validity – Confounding
Power
|
Gundogdu et al. (1998)18 | |
Reporting
External Validity
Interval Validity - Bias
Internal Validity – Confounding
| Reporting
External Validity
Interval Validity - Bias
Internal Validity – Confounding
Power
|
Colak et al. (2004)16 | |
Reporting
External Validity
Internal Validity – Bias
Internal Validity – Confounding
| External Validity
Internal Validity – Bias
Power
|
Leung et al. (2019)2 | |
Reporting
External Validity
Internal Validity – Bias
Internal validity – Confounding
| Reporting
External Validity
Interval Validity - Bias
Internal Validity – Confounding
Power
|
Appendix 4: Main Study Findings
Note that this appendix has not been copy-edited.
Study citation and study design | Type of reprocessed device | Reprocessed outcomes | New device outcomes | Notes |
|---|---|---|---|---|
Browne et al. (1997)15 Retrospective case-control | PTCA Balloon Catheter | Fever: n = 11 Elevated WBC: n = 12 Chills: n = 1 Mean procedure time: 67 +/− 30 minutes Mean fluoroscopy time: 13 +/− 10 minutes Mean dye volume: 275 +/− 125 mL Average balloons per lesion: 1.5 +/− 0.7 Angiographic failure rate: 7% (10 /108, 95% CI, 2% - 12%) | Fever: n = 12 Elevated WBC: n = 14 Chills: n = 0 Mean procedure time: 83 +/− 49 minutes Mean fluoroscopy time: 18 +/− 15 minutes Mean dye volume: 307 +/− 157 mL Average balloons per lesion: 1.6 +/− 0.6 Angiographic failure rate: NR | P values were not reported Angiographic failure rate reportedly comparable to the 10% rate seen with new balloons in other studies but not reported for comparison group. |
Plante et al. 199417 | Balloon catheter | Angiographic success rate: 88% Clinical failure with adverse clinical events: n = 25 (7.8%) Balloon catheter use per lesion: Mean 2.4 +/− 1.5 catheters Initial balloon failure: 10.2% Procedure times: 81 +/− 41 minutes Volume of contrast medium: 201 mL +/− 86 Adverse clinical events: 7.8% Length of hospital stay: 5.1 +/− 5.7 days Fever: n = 3 | Angiographic success rate: 88% Clinical failure with adverse clinical events: N = 14 (3.8%) P < 0.025 Balloon catheter use per lesion: Mean 1.2 +/− 0.5 catheters P < 0.00001) Initial balloon failure: 3.3%; P < 0.0001 Procedure times: 68 +/− 32 minutes, P < 0.0001 Volume of contrast medium: 165 +/− 61 mL P < 0.0001) Adverse clinical events: 3.8%, P < 0.025 Length of hospital stay: 3.4 +/− 2 to 8 days; (P < 0.0001) Fever: n = 1 | Fever in 3 patients in the reprocessing group was in association with urinary tract infection, pneumonia and in the postoperative period after urgent bypass surgery, not considered to be procedure related. Fever in in 1 patient in the single-use centre (flulike illness) also not thought to be procedure related. No statistically significant differences in clinical success and clinical failure without adverse events were reported between the 2 groups. |
Zacharias et al. (2021)20 | Endolaser Probe | Functionality of device n = 201 (93.5%) functioning n = 14 (6.5%) were nonfunctioning Infectious endophthalmitis n = 0 | Functionality of Device n = 373 (99.47%) functioning n = 2 (0.53%) nonfunctioning (P < 0.001) OR = 12.99 (P < 0.001) Infectious Endophthalmitis n = 0 | It is not clear whether functionality of the device is related to patient outcomes. |
Jokar et al. 202221 | Surgical port | PSI incidence at days 3 to 5: 6.6% PSI incidence at days 5 to 14: 2.7 Overall PSI: 8.5% | PSI incidence at days 3 to 5: 1.9% P = 0.013 PSI incidence at days 5 to 15: 0 P = 0.018 Overall PSI: 1.9% P = 0.002 | All PSIs in both groups were considered superficial, and no symptoms of deep infection were reported. Individuals in the disposable port group had a maximum of 2 symptoms of superficial infection, but in the reprocessed port group, there were usually more than 2 symptoms. |
Marins et al. (2018)22 | Surgical scissors and suture machine | Postoperative infection rate 12.3% Consumption of antibiotics (defined daily dose) 4.10 ± 7.63 Length of Hospital Stay 9.55 ± 8.92 days Duration of Surgery 2.33 ± 1.53 hours Rehospitalization n = 33 (7.91%) Mortality n = 6 (1.90%) Reoperations n = 0 | Postoperative Infection Rate 13.4% P = 0.664 Consumption of antibiotics (defined daily dose) 5.61 ± 15.21 P = 0.319 Length of Hospital Stay 10.36 ± 12.00 days P = 0.881 Duration of Surgery 2.45 ± 1.52 hours P = 0.161 Rehospitalization n = 28 (8.86%) P = 0.678 Mortality n = 12 (2.88%) P = 0.396 Reoperations n = 0 | There was a wide range differences in postoperative infection rate depending on the severity of the condition and the type of surgery. Mortality differed between patients in 2 surgery types, described as major procedures in the small and/or large intestine with complications (P = 0.044) and in major procedures in the stomach, esophagus, duodenum, small intestine, and/or large intestine, with complications (P = 0.141). |
Gundogdu et al. (1998)18 | Plastic trocar | Wound and intra-abdominal infection N = 0 | Wound and intra-abdominal infection N = 0 | Bacterial cultures on surgical equipment, disinfection solution, and various patient wound/bile locations are not reported here. |
Colak et al. (2004)16 | DLIs | Mean operating time (minutes): 43.88 ± 16.29 Mean LAS score 4.80 ± 1.07 Duration of Postop Analgesia (days) 0.90 ± 0.81 Amount of analgesic required (mg) 67.85 ± 61.30 Hospital stay (days) 1.30 ± 0.75 Conversion rate (%) 2 (3.2) Infection 2 (3.2) Other Complications 1 (1.6) | Mean operating Time (minutes) 42.66 ± 13.92, P = 0.65 Mean LAS score 4.95 ± 1.07, P = 0.54 Duration of Postop Analgesia (days) 0.88 ± 0.68, P = 0.89 Amount of analgesic required (mg) 65.32 ± 49.86, 0.49 Hospital stay (days) 1.53 ± 2.61, P = 0.50 Conversion rate (%) 1 (1.6) Infection 1 (1.6%) Other Complications 1 (1.6), P = 0.31 | The satisfaction of the surgeon with the instruments was excellent in 46 patients (74.2%) and good in 16 patients (25.8%) of the new DLI group vs excellent in 41 patients. (65.1%) and good in 22 patients (34.9%) of the reprocessed DLI group (P = 0.27). The median satisfaction rate of the patients was excellent in both groups (P = 0.87). |
Leung et al. (2019)2 | Circular mapping catheter | Procedure duration: 178.9 ± 51.3 minutes Fluoroscopy duration 11.8 ± 9.6 minutes, respectively, Mapping catheter failure: n = 1 Major or minor complications: n = 0 | Procedure duration: 189.5 ± 55.3 minutes, P = 0.16 Fluoroscopy duration: 21.5 ± 13.5 minutes, P < 0.0001 Mapping catheter failure: n = 0 Major or minor complications: n = 1 (cardiac tamponade) | Cardiac tamponade considered to be not procedure-related. Decreased fluoroscopy time observed in the reprocessed device group during angiography was likely due to progressive decline in reliance on fluoroscopy seen in their institution. |
DLIs = disposable laparoscopic instruments; LAS: linear analogue pain scale; NR = not reported; PSI = port-site infection; PTCA = percutaneous transluminal coronary angioplasty.
Note: For all studies, outcomes definitely not related to patient outcomes, such as economic and in vitro outcomes, were not included here as they are out of scope.
Appendix 5: References of Potential Interest
Reuse Without Processing
Saadat SH, Shepherd S, Van Asseldonk B, Elterman DS. Clean intermittent catheterization: Single use vs. reuse. Can Urol Assoc J. 2019;13(2):64-69. PubMed
Zabaleta-Del-Olmo E, Vlacho B, Jodar-Fernandez L, et al. Safety of the reuse of needles for subcutaneous insulin injection: A systematic review and meta-analysis. Int J Nurs Stud. 2016;60:121-132. PubMed
Environmental Impact of Single-Use Devices
Anonymous. Reducing the environmental impact of surgery on a global scale: systematic review and co-prioritization with healthcare workers in 132 countries. Br J Surg. 2023;110(7):804-817. PubMed
Contributors: Shannon Hill, Elizabeth Carson
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for noncommercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca