CADTH Health Technology Review
Anti–Vascular Endothelial Growth Factor Drugs for Age-Related Macular Degeneration
Rapid Review
Authors: Qiukui Hao, Sharon Bailey
Key Messages
What Is the Issue?
Wet age-related macular degeneration (AMD) is a serious health concern that causes reduced vision-related function, poor overall quality of life, and increased health care resource usage.
Anti–vascular endothelial growth factor (VEGF) drugs are the first-line treatment for wet AMD, and they are injected into the eye. These drugs can slow disease progression but are expensive and require trained medical professionals to administer and monitor treatment response.
The criteria for initial injection, maintenance, and discontinuation of anti-VEGF drugs in patients with wet AMD remain unclear.
What Did We Do?
To inform decisions about the appropriate use of anti-VEGF drugs to treat adults with wet AMD, CADTH sought to identify and summarize recommendations about criteria for the diagnosis of wet AMD and best practices for subsequent treatment with anti-VEGF drugs.
An information specialist searched the peer-reviewed and grey literature for clinical practice guidelines published since 2018.
What Did We Find?
Three evidence-based guidelines recommend optical coherence tomography (OCT) to assess patients with suspected wet AMD. The National Institute for Health and Care Excellence (NICE) guidelines then strongly recommend fundus fluorescein angiography only when OCT does not exclude neovascular disease.
The evidence-based guidelines recommend anti-VEGF drugs for wet or neovascular AMD in adults, particularly for patients with recent disease progression. One guideline suggests starting anti-VEGF treatment as soon as possible once the diagnosis of wet AMD is made.
The NICE guideline suggests that there may not be any clinically significant distinctions in the effectiveness and safety of various anti-VEGF treatments, including aflibercept, bevacizumab, and ranibizumab, indicating a need for an individualized approach when selecting specific anti-VEGF drugs. However, 1 guideline is inconsistent with NICE, as it suggests choosing bevacizumab first.
During the maintenance phase of using anti-VEGF drugs, it is important to closely monitor the patient's response and the disease activity and adjust the injection intervals accordingly.
Guidelines recommend taking an individualized approach and emphasizing active patient involvement in switching and discontinuing anti-VEGF drugs for adults with wet AMD.
Guidelines or guidance documents without a literature search or unclear methods provided generally consistent recommendations with the included evidence-based guidelines.
We did not identify any evidence-based guidelines regarding the use of faricimab or brolucizumab. However, NICE published technology appraisals supporting the use of recently approved anti-VEGF drugs (faricimab and brolucizumab) as alternative options for patients who meet similar criteria for treatment with bevacizumab or aflibercept, and under agreed pricing conditions.
What Does It Mean?
All identified guidelines consistently recommend anti-VEGF drugs for adults with wet active AMD, with some providing guidance on the use of OCT and other ophthalmological assessments to identify criteria for starting and adjusting treatment.
These guidelines recommend personalized and patient-centred approaches for selecting, switching, and discontinuing anti-VEGF medications. Cost is also a crucial factor in decision-making, especially for aflibercept, ranibizumab, and recently approved anti-VEGF drugs such as faricimab and brolucizumab.
Further research and evidence-based guidelines are necessary to confirm whether newer drugs can be used in similar situations as older drugs.
Abbreviations
AMD
age-related macular degeneration
BCVA
best-corrected visual acuity
FFA
fundus fluorescein angiography
MNV
macular neovascularization
nAMD
neovascular age-related macular degeneration
NICE
National Institute for Health and Care Excellence
OCT
optical coherence tomography
OCT-A
optical coherence tomography angiography
PED
pigment epithelial detachment
RPE
retinal pigment epithelium
VEGF
vascular endothelial growth factor
Context and Policy Issues
What Is Age-Related Macular Degeneration?
Age-related macular degeneration (AMD) is a prevalent eye disease that can lead to permanent central vision loss in older adults.1 The disease occurs when the retina's central portion (the macula), which is responsible for sharp and straight-ahead vision, is damaged due to aging and other risk factors. AMD may affect 1 eye (unilateral AMD), with a high risk of progressing to both eyes (bilateral AMD) in 5 years.2 While advanced age is the primary risk factor for developing AMD, modifiable risk factors like cigarette smoking, increased body mass index, hyperlipidemia, and hypertension are also important.3 Family history and genetic issues also contribute to the development of AMD.3
There are 2 main types of AMD: dry (atrophic) and wet (neovascular or exudative) AMD.3 Dry AMD accounts for approximately 80% to 85% of all cases and may progress to wet AMD, which accounts for the remaining 15% to 20% of AMD and results in the most severe vision loss.3 The progression of AMD varies from person to person and can be slow or fast.4 Wet AMD is characterized by the abnormal growth of new blood vessels underneath the macula, which can cause hemorrhaging, fluid leakage, or fibrosis in the inner retinal layers or subretinal space.3
Ophthalmological exams are necessary for diagnosing AMD. These may include measuring best-corrected visual acuity (BCVA), Amsler grids, funduscopic evaluation with dilated pupils, macular layer imaging with optical coherence tomography (OCT), or fluorescein angiography.1,3 Patients in the early or intermediate stages of dry and wet AMD may not experience noticeable symptoms or suffer from substantial changes in their vision.1,3 When these vision changes develop, they may include distorted images, increased blurring (especially while reading), loss of visual acuity, central scotoma (blind spot), and decreased contrast sensitivity (ability to detect differences in shades and patterns).1,3 Wet AMD, also known as neovascular AMD (nAMD) or exudative AMD, typically results in more rapid and severe visual symptoms that may suddenly or gradually worsen, which is the most common form of advanced AMD.1,3
How Is AMD Managed?
There are no curative interventions for AMD. Clinicians usually advise all patients with AMD to pursue lifestyle modifications such as quitting smoking, getting regular physical activity, and changing diet patterns with foods rich in antioxidants or unsaturated fatty acids.1,3 Available therapies that can help slow down the progression of wet AMD include nutritional supplementation with antioxidants (e.g., vitamin C, vitamin E, copper, lutein, zeaxanthin, and zinc), laser therapy, intravitreal injections with anti–vascular endothelial growth factor (VEGF) drugs, and others.3
Based on the results of major clinical trials in AMD, anti-VEGF drugs have become first-line interventions for wet AMD.1,3,5,6 VEGF plays a crucial role in the formation and growth of abnormal blood vessels and the leakage of blood plasma components from vessels into the retina.3 Anti-VEGF drugs reduce vessel permeability by blocking VEGF. Available anti-VEGF agents administered by intravitreal injection include ranibizumab, aflibercept, brolucizumab, bevacizumab, and faricimab. Bevacizumab is not approved for treating wet AMD, but clinicians may prescribe it as an off-label treatment.3 Faricimab is a new bispecific antibody (angiopoietin-2 and VEGF) inhibitor, which shows promising results for treating wet AMD in phase II trials and real-world settings.3,7 It was approved by the FDA and Health Canada for wet AMD in 2022.8,9
The cost of the approved anti-VEGF treatments (ranibizumab, aflibercept, brolucizumab, and faricimab) is more expensive than bevacizumab.1,10 A trained health professional is required to administer intravitreal injections of anti-VEGF drugs. Typically, patients with wet AMD need a total of 7 or 8 injections in the first year of treatment.1 Most patients may need long-term anti-VEGF injections, and the injection interval can be adjusted based on comprehensive assessment.1 The ophthalmologist and patient usually discuss and select anti-VEGF protocols based on multiple factors, such as patient or clinician preferences, costs, response, and other practical issues.1,3,6,11
Why Is It Important to Do This Review?
AMD is a leading cause of blindness, responsible for about 9% of global blindness cases.1 AMD affected approximately 200 million people worldwide in 2020.3 In Canada, almost 1 million people have early AMD, with approximately 25% having advanced forms of AMD.12 The number is increasing due to the aging population.3 Although AMD does not lead to complete blindness, with the functioning of peripheral vision preserved, it can cause loss of central vision, making it difficult to perform activities of daily living, such as cooking, eating, reading, driving, watching television, and recognizing objects and faces.3,13 Visual impairment or disability caused by AMD is associated with poor quality of life, depression, falls, and hip fractures in older adults.13
In Canada, wet AMD is a serious health concern, causing a significant burden on individuals with the disease.14 It leads to limitations in vision-related functional abilities, poor overall quality of life, and increased health care resource usage.14 People with wet AMD also experience higher medical costs, are at a greater risk of falls, and often need more assistance with daily activities, compared to healthy individuals.14 Therefore, it is crucial to explore evidence-based treatments for wet AMD to prevent vision loss or blindness, which can improve the quality of life and reduce the economic burden associated with this disease. However, there is still ambiguity on how to use anti-VEGF regimens for treating adults with wet AMD in clinical practice, such as criteria for initial injection, maintenance, and discontinuation of the treatment.
Objective
This Rapid Review summarizes evidence-based clinical practice guidelines to support decision-making about using anti-VEGF drugs for wet AMD in adults, including ranibizumab, aflibercept, brolucizumab, faricimab, and bevacizumab.
Research Question
What are the evidence-based guidelines regarding the use of anti-VEGF drugs for adult patients with suspected or confirmed wet AMD?
Methods
Literature Search Methods
An information specialist conducted a literature search on key resources, including MEDLINE, Embase, the Cochrane Database of Systematic Reviews, the International HTA Database, and the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search approach was customized to retrieve a limited set of results, balancing comprehensiveness with relevancy. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine's MeSH (Medical Subject Headings), and keywords. Search concepts were developed based on the elements of the research questions and selection criteria. The main search concepts were wet age-related macular degeneration and anti–vascular endothelial growth factor drugs. CADTH-developed search filters were applied to limit retrieval to health technology assessments, systematic reviews, meta-analyses, indirect treatment comparisons, and guidelines. The search was completed on August 24, 2023. A supplemental search for guidelines related to wet age-related macular degeneration more broadly was completed on October 20, 2023. Searches were limited to English-language documents published since January 1, 2018.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
|---|---|
Population | Adult patients with suspected or confirmed wet age-related macular degeneration |
Intervention | Anti–vascular endothelial growth factor drugs:
|
Comparator | Not applicable |
Outcomes | Recommendations regarding best practices for initiation, monitoring, and discontinuation of treatment (e.g., diagnostic criteria, appropriate patient populations, contraindications) |
Study designs | Evidence-based guidelines |
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, they were duplicate publications, or they were published before 2018. Guidelines, position statements, action papers, and guidance documents with unclear methodology or without a systematic literature search were excluded as well. We also excluded guidelines that only focused on patients with polypoidal choroidal vasculopathy.
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the Appraisal of Guidelines for Research and Evaluation (AGREE) II instrument.15 Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Summary of Evidence
Quantity of Research Available
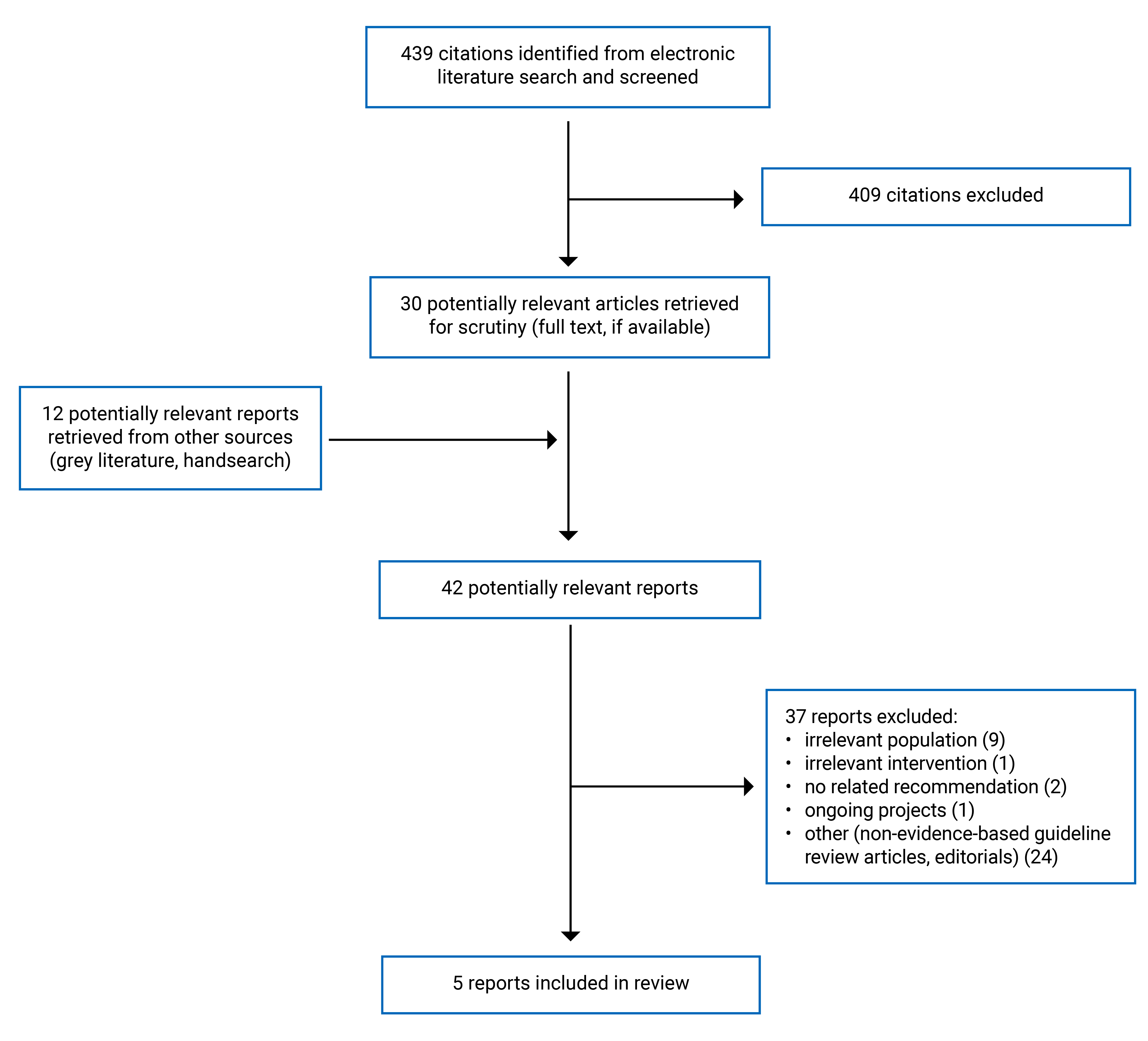
A total of 439 citations were identified in the literature search. Following screening of titles and abstracts, 409 citations were excluded, and 30 potentially relevant reports from the electronic search were retrieved for full-text review. 12 potentially relevant publications were retrieved from the grey literature search for full-text review. Of these potentially relevant articles, 37 publications were excluded for various reasons, and 5 publications (evidence-based guidelines) met the inclusion criteria and were included in this report. Appendix 1 presents the PRISMA16 flow chart of the study selection.
We also identified several publications with recommendations, which did not meet our criteria for evidence-based guidelines but provided content relevant to the research question. Appendix 5 presents the characteristics and relevant recommendations from these publications. Appendix 6 presents additional references of potential interest.
Summary of Guideline Characteristics
This report included 5 evidence-based guidelines in which recommendations were developed from a systematic search for relevant evidence.17-21 The recommendations cover various aspects such as diagnosis, risk factors, referring suggestions, and management. For this report, we have summarized the recommendations that relate to the use of anti-VEGF drugs in treating wet AMD in the sections below.
Appendix 2 presents additional characteristics of the included guidelines.
The guideline development groups were from European17 and Asia-Pacific countries,18 the US (American Academy of Ophthalmology),19 Iran,20 and the UK (National Institute for Health and Care Excellence [NICE]).21 We assume that these guidelines are intended to apply to these specific countries. Of these guidelines, 2 provide recommendations for patients with wet or neovascular AMD,17,18 2 provide recommendations for patients with AMD,19,21 and the remaining 1 provides guidelines for patients with ocular vascular disease.20 The authors of 2 guidelines18,21 clearly stated that their recommendations are for adults, while it is assumed that the remaining guidelines17,19,20 are also for adults, although they do not have a clear description.
The authors of 2 guidelines17,18 performed a literature search to find relevant systematic reviews, guidelines, and primary studies. They then presented the obtained evidence to a consensus panel for further discussion and development of recommendations.17,18 For 2 of the guidelines,19,21 the guideline panel also reviewed health economic evidence. In the remaining guideline,20 the technical committee created scientifically possible answers or scenarios based on the evidence from a systematic search of the literature for each clinical question. The panel members then voted to finalize the recommendations.
One guideline included evidence regarding aflibercept, bevacizumab, brolucizumab, and ranibizumab.19 The remaining 4 guidelines included evidence regarding aflibercept, bevacizumab, and ranibizumab.17,18,20,21 No guideline included evidence for faricimab. All guidelines17-21 based recommendations on visual outcomes such as best-corrected visual acuity (BCVA). However, 2 guidelines19,21 also considered quality-of-life measures as the main outcomes in developing recommendations.
Summary of Critical Appraisal
All of the included guidelines had clear objectives, guideline questions, and target populations (e.g., patients with wet AMD) and were aimed at health care providers who manage wet AMD in adults.17-21 All of the guidelines attempted to apply systematic methods to search for evidence and then achieve consensus to finalize recommendations.17-21 One guideline20 lacked clarity on search methods and another only searched PubMed,17 potentially missing relevant evidence due to uncomprehensive searches.
Two of the guidelines19,21 were developed by a team of clinical experts and research professionals. However, it is uncertain whether at least 1 methodology expert was involved in the development of 317,18,20 of the 5 included guidelines. Only 1 of the guidelines, from NICE, sought the views or preferences of the target population.21 We are also unsure whether the perspectives or preferences of the target populations were sought or had an influence on the recommendations in the remaining 4 guidelines.17-20 Therefore, the recommendations may not adequately reflect the values and preferences of patients.
Two guidelines19,21 adopted the Grading of Recommendations Assessment, Development and Evaluation (GRADE) framework to assess the certainty of evidence, but the certainty of evidence was unclear in the remaining 3 guidelines.17,18,20 The link between the recommendations and the supporting evidence was unclear in these same 3 guidelines.17,18,20 In the other 2 guidelines,19,21 such links were clear for main recommendations. The strength of some or all recommendations in all included guidelines was not clear.17-21 Two guidelines lacked clarity in explaining the process of transitioning from evidence to recommendation.17,18 While 3 of the guidelines were published in peer-reviewed journals, none of them described an explicit external review process.17,18,20 These limitations could limit the internal validity of the guidelines.
The NICE guideline21 had good applicability by describing the facilitators and barriers, offering practical tools for implementing the recommendations and considering the potential resources needed to follow the guideline recommendations. Although 2 other guidelines provided algorithms for managing wet AMD,17,18 the 2 remaining guidelines do not offer advice or tools on how to put the recommendations into practice.19,20 The relevant recommendations in 3 guidelines were specific and unambiguous,17,18,21 whereas 2 guidelines provided ambiguous recommendations,19,20 such as lack of specific information on choosing specific anti-VEGF drugs. These limitations could be a barrier to implementing their recommendations.
All guidelines disclosed the competing interests of their development group.17-21 It is unlikely that the funding body influenced the contents of the guideline in 3 guidelines.19-21 However, several authors in the 2 guidelines had received grants or consultation fees from industries, but it is unclear how they addressed these competing interests. The commercial company Novartis, related to 2 anti-VEGF drugs (brolucizumab and ranibizumab), performed the preliminary literature review in 1 guideline.17 The authors state that the company was not involved in interpreting the search results or developing recommendations. However, the potential impact on the guideline recommendations cannot be ruled out. We are unclear if the competing interests could impact the development of recommendations.
Appendix 3 provides additional details regarding the strengths and limitations of included publications.
Summary of Recommendations
We have summarized the relevant recommendations regarding diagnosis of wet AMD and subsequent treatment with anti-VEGF drugs from the included clinical practice guidelines. This also includes recommendations related to specific drug selection and dosing, initiation of therapy, treatment intervals, and disease monitoring during the maintenance phase, switching and stopping anti-VEGF drugs, and other recommendations. Appendix 4 presents the detailed recommendation statements, along with supporting evidence, certainty of evidence, and strength of the recommendations, if available.
Recommendations for Diagnosis of Wet AMD
Three guidelines17,19,21 recommend OCT for patients with suspected wet AMD.
One guideline17 noted that the most important criteria are the morphological parameters observed on OCT, which should be evaluated using the entire stack of images when diagnosing wet AMD. The morphological parameters include subretinal fluid, intraretinal fluid, intraretinal neovascularization (type 3 macular neovascularization [MNV]), subretinal hyperreflective material (type 2 MNV or mixed type 1 and type 2 MNV).17 Another guideline states that OCT, fluorescein angiography, and optical coherence tomography angiography (OCT-A) are useful diagnostic tests for detecting new or recurrent disease activity and guiding therapy.19 However, the strength of the recommendations and quality of the supporting evidence were unclear in the 2 guidelines.17,19
The NICE guideline recommends making an urgent referral to a macula service for people suspected to have late AMD (wet active), even if they do not report any visual impairment.21 The referral should be made within 1 working day, but it does not require an emergency referral.21 For individuals presenting with visual changes (including micropsia and metamorphopsia) or disturbances, the NICE guideline strongly recommends fundus examination.21 The NICE guideline strongly recommends the use of OCT for people who are suspected to have wet active AMD. If OCT does not exclude neovascular disease, then the NICE guideline strongly recommends fundus fluorescein angiography (FFA) to confirm the diagnosis of wet active AMD. However, if clinical examination and OCT exclude neovascularization, then the NICE guideline strongly recommends against offering FFA to people with suspected wet active AMD. These strong recommendations were based on very low- to moderate-quality evidence.
General Recommendations for Use of Anti-VEGF Drugs
All included guidelines17-21 recommended anti-VEGF drugs for adults with wet AMD. One guideline19 provided a strong recommendation based on a Cochrane systematic review, and noted that anti-VEGF therapies have become first-line therapy for treating and stabilizing most cases of wet AMD. One guideline20 recommended using bevacizumab and other anti-VEGF drugs to treat wet AMD due to their effectiveness and safety (level I evidence, unclear strength of recommendation).
The NICE guideline21 provided a strong recommendation based on high-quality evidence regarding using anti-VEGF drugs for wet active AMD for eyes with the following conditions: BCVA is between 6/12 and 6/96; there is no permanent structural damage to the central fovea; the lesion size is less than or equal to 12 disc areas in greatest linear dimension; and there is evidence of recent disease progression (blood vessel growth, as indicated by fluorescein angiography, or recent visual acuity changes).
For adults who have wet active AMD and a visual acuity of 6/96 or worse, or better than 6/12, the NICE guideline panel has made weak recommendations based on observational studies.21 For those who have a visual acuity of 6/96 or worse, the guideline panel suggests considering anti-VEGF treatment if the treatment is expected to improve the person’s overall visual function (e.g., the affected eye is the person’s better-seeing eye). For those who have a visual acuity better than 6/12, anti-VEGF treatment is effective and may be cost-effective, depending on the regimen used. However, the guideline did not mention a specific anti-VEGF regimen in the recommendation.21
Recommendations for Choosing Specific Anti-VEGF Drugs
The NICE guideline21 committee agreed that there were no clinically significant differences in the effectiveness and safety of different anti-VEGF treatments (aflibercept, bevacizumab, and ranibizumab). This is a weak recommendation based on moderate-quality evidence.
This guideline makes specific recommendations for ranibizumab and aflibercept but not for bevacizumab, as bevacizumab did not have a UK marketing authorization for treating wet AMD at the time of guideline publication (2018). The NICE guideline recommends ranibizumab and aflibercept as a treatment option for wet AMD, according to their marketing authorizations, and if the manufacturer provides ranibizumab or aflibercept with the discount agreed upon in the patient access scheme. For patients with active wet AMD coexisting with retinal pigment epithelium (RPE), 1 guideline20 recommended intravitreal bevacizumab to improve their visual acuity (supporting evidence level III, unclear strength of recommendation).
Recommendations for Initial Treatment, Dosing, and Intervals
Initial Treatment
The NICE guideline strongly recommends antiangiogenic treatment (anti-VEGF drugs) within 14 days of referral for adults with confirmed wet AMD.21
Two guidelines17,18 made recommendations for initial anti-VEGF treatment with unclear supporting evidence and strength of recommendations. One guideline17 noted that treatment with anti-VEGF drugs should be initiated as soon as possible once the diagnosis of wet AMD is made; the initiation phase involves at least 2 injections at monthly intervals. The other guideline18 stated that after a diagnosis of wet AMD, at least 3 consecutive monthly intravitreal anti-VEGF injections should be administered until no disease activity, such as new hemorrhage or fluid on OCT, is observed.
Dosing
One guideline20 provided recommendations for the dosage of using anti-VEGF: bevacizumab (1.25 mg/0.05 mL), aflibercept (2 mg/0.05 mL), and ranibizumab (0.5 mg/0.05 mL).
Intervals
Two guidelines17,18 recommend using the treat-and-extend (T and E) regimen approach to adjust anti-VEGF injection intervals using algorithms. The 2 guidelines summarized related evidence and recommended 2 algorithms for the management of wet AMD. However, we are unclear on the evidence supporting the recommendations and the strength of recommendations.
One guideline17 noted the key aspect of the T and E approach is that anti-VEGF treatment should be given proactively at each visit. It emphasizes the OCT measure, and noted that the decisions to modify treatment intervals for subsequent visits should be based on OCT measures of disease activity.17
We summarized the main points or steps in the 2 algorithms.
If disease activity is observed:
confirm the initial diagnosis of wet AMD and continue at least 2 to 3 additional injections at the minimum interval permitted by the product label, then consider switching to an alternative anti-VEGF drug17
shorten the treatment interval by 2 to 4 weeks (to a minimum of 4 weeks),17 until intraretinal fluid and/or subretinal fluid are not observed, then the treatment interval can be gradually extended.18
If no disease activity is observed, extend the injection interval by 2 to 4 weeks between visits, up to a maximum interval of 16 weeks,17,18 or potentially more with longer-acting anti-VEGF drugs.17
Recommendation for Disease Monitoring
One guideline17 noted that the signs of disease activity in OCT include the following: new subretinal or intraretinal hemorrhage, persistent or increased diffuse retinal thickening, new subretinal fluid or an increase in subretinal fluid, new or increased pigment epithelial detachment or subpigment epithelial detachment fluid, or subretinal hyperreflective material representing a neovascular membrane. The guideline recommends that if disease activity is observed over 3 consecutive anti-VEGF injections with no signs of anatomic or functional improvement, the clinician should reassess the initial diagnosis of wet AMD.17
One guideline18 suggests self-monitoring for declining vision; however, the details of self-monitoring, supporting evidence, and the strength of recommendation were unclear.
The NICE guideline strongly recommends close monitoring of individuals with wet active AMD in both eyes using OCT.21 If the OCT results appear stable but there is a decline in visual acuity or function, the guideline strongly recommends a fundus examination or colour photography.21 For identifying unrecognized neovascularization, a weak recommendation is provided for FFA.21 If the OCT results suggest macular abnormalities that are not responding to treatment, the NICE guideline advises using alternative imaging or alternative diagnoses.21
Recommendation for Switching or Stopping Anti-VEGF Drugs
Active involvement of patients and personalized approaches are crucial in the decision-making process regarding switching and stopping anti-VEGF. The strength of recommendations regarding switching and stopping anti-VEGF drugs is unclear or weak. The supporting evidence for these recommendations was mostly unclear or limited.
Switching Anti-VEGF Drugs
One guideline17 noted that if a patient is switched to an alternative anti-VEGF therapy due to lack of efficacy (the definition of efficacy was unclear), a new initiation phase is required. The supporting evidence and the strength of the recommendation are not clearly defined. Another guideline more specifically recommends that patients who are unresponsive to bevacizumab may be switched to ranibizumab or aflibercept, based on level I evidence (systematic reviews or randomized controlled trials [RCTs]).20 However, the NICE guideline recommends considering switching anti-VEGF drugs for practical reasons or patient preference, although there may be limited clinical benefits given the committee’s agreement that there are no significant differences in effectiveness and safety between aflibercept, bevacizumab, and ranibizumab (weak recommendations based on very low evidence).21
Stopping Anti-VEGF Drugs
The NICE guideline21 made weak recommendations for stopping anti-VEGF drugs in the following 2 conditions: the eye develops severe, progressive loss of visual acuity despite treatment as recommended; or the eye develops wet inactive AMD with no prospect of functional improvement. The NICE guideline emphasized the importance of involving patients in treatment decisions regarding switching or discontinuation.21 The NICE guideline21 also weakly recommends observation without giving anti-VEGF drugs for patients with stable wet AMD (the definition of stable was unclear) based on very low evidence.
One guideline18 recommends discontinuing anti-VEGF therapy on a case-by-case basis after careful discussion with patients. The guideline suggests that it may be a reasonable choice to discontinue anti-VEGF injections for patients with stable, inactive disease who have been treated at 16-week intervals for consecutive visits, or patients with advanced nAMD who have significant scarring or atrophy. The supporting evidence and strength of these recommendations were not clearly defined. One guideline17 states that long-term anti-VEGF therapy may not be beneficial for patients with low vision who have certain retinal conditions such as fibrosis, extensive subretinal hemorrhage, subfoveal disruption of the external limiting membrane, or central atrophy of the RPE.
Other Recommendations for Intravitreal Injection of Anti-VEGF
Three guidelines17,20,21 offer other recommendations for the intravitreal injection anti-VEGF procedure.
One guideline20 advises administering anti-VEGF injections with caution in patients with recent systemic vascular events, such as stroke or myocardial infarction, after appropriate consultation with a health care provider. Although the guideline does not recommend bilateral injection, surgeons can perform it at their discretion. The guideline emphasizes the use of separate equipment for each eye, such as gloves and surgical preps.20 The guideline recommends using a 29-gauge or 30-gauge needle for injections and avoiding postinjection antibiotics.20 Clinicians should perform the injections between the horizontal and vertical rectus muscles at the pars plana (3 mm to 4 mm posterior to the limbus).20 Additionally, the guideline suggests that clinicians monitor for rare retinal detachment risk after each injection, particularly in patients with myopia.20 The guideline authors did not clearly present the strengths of recommendation and the supporting evidence.20
According to the NICE guideline,21 administering intraocular injections requires trained health care professionals like ophthalmologists, nurse practitioners, optometrists, and experienced technicians. If a person without medical qualifications is administering the injection, it is important to have plans and resources in place to manage any potential complications.21 However, the strength of recommendations and the supporting evidence were unclear.
Limitations
We have identified 5 evidence-based guidelines for the use of anti-VEGF drugs in treating wet AMD in adults.17-21 However, most of these guidelines have serious limitations, as detailed in the critical appraisal summary section. In these guidelines, unclear reporting in evidence synthesis and recommendation development is a significant issue for 317,18,20 of the 5 included guidelines. Specifically, although all included guidelines claimed they conducted the literature search and consensus process, the literature review process and the links between supporting evidence and recommendations were often unclear. The supporting evidence for certain recommendations was either unclear or based solely on expert consensus.17-21 Therefore, we need to interpret these recommendations with caution.
There were inconsistencies in some of the recommendations. For instance, 1 guideline suggests a minimum of 2 injections at monthly intervals during the initial phase,17 while another guideline recommends 3 consecutive injections at same injection intervals.18 Given that the links between the recommendations and the supporting evidence were unclear, it is challenging to determine which recommendation is more reasonable.
We identified some gaps between the available evidence and guideline recommendations. None of the existing guidelines provided recommendations for the newly approved anti-VEGF drug faricimab (approved in 2022 by Health Canada), and only 1 guideline19 included evidence for brolucizumab (approved in 2020 by Health Canada). We did not find any specific recommendations for these 2 anti-VEGF drugs. To ensure that the latest available evidence is considered, an updated evidence-based guideline on all anti-VEGF drugs for wet AMD is needed.
Additionally, we did not find evidence-based guidelines from Canada. In the included 5 guidelines, the guideline panel members were from European17 and Asia-Pacific countries,18 the US,19 Iran,20 and the UK,21 while no panel members were from a Canadian institution. Thus, the generalizability of the findings to settings in Canada was unclear.
Conclusions and Implications for Decision- or Policy-Making
We included 5 evidence-based guidelines,17-21 including guidelines from NICE and the American Academy of Ophthalmology, in this report.
Three guidelines17,19,21 provided recommendations regarding measures to diagnose wet AMD, as a preliminary step to pursuing treatment with anti-VEGF drugs. For individuals presenting with visual changes (including micropsia and metamorphopsia) or disturbances, the NICE guidelines strongly recommend fundus examination.21 Three guidelines17,19,21 recommend OCT for patients with suspected wet AMD. The NICE guideline21 strongly recommends the use of OCT: if OCT does not exclude neovascular disease, then FFA is strongly recommended, while if clinical examination and OCT exclude neovascularization, then the guideline strongly recommends against offering FFA to people with suspected wet active AMD.
All included guidelines recommended antivascular drugs for wet AMD in adults, particularly for the affected eyes with the following conditions: the BCVA is between 6/12 and 6/96; there is no permanent structural damage to the central fovea; the lesion size is less than or equal to 12 disc areas in greatest linear dimension; or there is evidence of recent disease progression (blood vessel growth, as indicated by fluorescein angiography, or recent visual acuity changes). For eyes with wet active AMD and visual acuity of 6/96 or worse, NICE provides a weak recommendation for anti-VEGF only if a benefit in the person's overall visual function is expected; for eyes with wet active AMD and visual acuity better than 6/12, anti-VEGF is effective.21 One guideline17 suggests that anti-VEGF drugs should be initiated as soon as possible once the diagnosis of wet AMD is made. For the initial phase of using anti-VEGF drugs, 1 guideline17 suggests a minimum of 2 injections, while the other guideline recommends18 at least 3 consecutive injections at monthly intervals at same injection intervals.
The NICE guideline21 noted that there are no clinically significant distinctions in the effectiveness and safety of various anti-VEGF treatments, including aflibercept, bevacizumab, and ranibizumab. This recommendation is considered weak due to moderate-quality evidence and did not involve the evidence assessment for faricimab and brolucizumab. They recommend considering either ranibizumab or aflibercept as a treatment option for wet AMD, in accordance with their marketing authorizations, and highlight that the recommendation requires that the manufacturer offer these medications with the agreed-upon discount.21 Similarly, 1 guideline19 does not recommend a specific treatment option, and emphasizes that physicians and patients should discuss and choose an individualized anti-VEGF drug. In contrast, 1 guideline20 suggests using bevacizumab to improve visual acuity in patients with active wet AMD and coexisting RPE, although the recommendation's strength is unclear (evidence level III).
During the maintenance phase of using anti-VEGF drugs, it is important to closely monitor the patient's response and the disease activity. The injection intervals could be adjusted by following a T and E regimen plan, according to 2 guidelines.17,18 The intervals for anti-VEGF injections should be adjusted based on disease activity: shortened intervals when activity is present, and extended intervals when no disease activity is observed. The NICE guideline strongly recommends close monitoring of individuals with wet active AMD in both eyes using OCT.21 For patients with normal OCT but a decline in visual acuity or function, the guideline strongly recommends a fundus examination or colour photography.21
The included guidelines17-21 recommend taking an individualized approach and emphasizing active patient involvement in switching and discontinuing anti-VEGF drugs for adults with wet AMD. The NICE guideline suggests that switching anti-VEGF drugs may have limited clinical benefits and should only be considered for practical reasons, such as patient preference. If a decision is made to switch, it may be necessary to go through a new initiation phase.17 The evidence for discontinuing anti-VEGF drugs is limited, and the strength of recommendations is unclear or weak. Careful patient discussion can lead to the consideration of discontinuation, especially for those treated at 16-week intervals and having stable, inactive disease.18,21
Two guidelines provided recommendations related to the intravitreal injection procedure for anti-VEGF drugs. According to the NICE guideline,21 intraocular injections should be administered by trained health care professionals, such as ophthalmologists or nurse practitioners. One guideline20 suggests cautious administration in cases of recent systemic vascular issues, employing 29-gauge or 30-gauge needles, and avoiding postinjection antibiotics. They recommend injecting between rectus muscles, and monitoring for rare retinal detachment risk, particularly in patients with myopia.20
Guidelines or guidance documents that were considered as non–evidence-based22-27 for the purposes of this Rapid Review still provided recommendations that were generally consistent with the evidence-based guidelines that were included. The Ministry of Health Singapore suggests using ranibizumab as an alternative to bevacizumab for treating visual impairment due to wet AMD in adults.24 This non–evidence-based guideline did not conduct a literature search as part of its methods. Two NICE technology appraisal guidance papers,22,26 based on manufacturer-submitted evidence, recommended the newly approved anti-VEGF drugs faricimab or brolucizumab as options for treating wet AMD in adults with similar situations as bevacizumab and aflibercept, including specific discount agreement. Two expert consensus papers from Taiwan23,25 and 1 recommendation paper27 for a UK expert panel provided recommendations for a T and E approach for using anti-VEGF drugs. The consensus papers23,25,27 suggested adjusting injection intervals based on monitoring disease activity or visual function after the loading phase, and recommended initiating a loading phase of 3 consecutive monthly anti-VEGF injections. The suggested frequency is consistent with 1 of the included guidelines.18
Appendix 5 presents additional details regarding the relevant guidelines with alternative or unclear methodology.
The included guidelines17-21 used various guideline development frameworks or processes to develop recommendations, resulting in challenges in summarizing and interpreting the recommendations. Although it can be easy to find key recommendations, distinguishing between additional recommendation and nonrecommendation statements can be challenging in 3 guidelines.17-19 Future guideline development research should prioritize transparency by clearly linking evidence to recommendations and indicating the strength of recommendations. A consistent framework or strict adherence to reporting guidelines may be helpful for guideline users and decision-makers. Evidence-based guidelines with comprehensive literature searches are required to guide use or policy-making regarding the most recently approved anti-VEGF drugs, including faricimab and brolucizumab.
References
1.Stahl A. The diagnosis and treatment of age-related macular degeneration. Dtsch Arztebl Int. 2020;117(29-30):513-520. PubMed
2.Joachim N, Colijn JM, Kifley A, et al. Five-year progression of unilateral age-related macular degeneration to bilateral involvement: The Three Continent AMD Consortium report. Br J Ophthalmol. 2017;101(9):1185-1192. PubMed
3.Thomas CJ, Mirza RG, Gill MK. Age-related macular degeneration. Med Clin North Am. 2021;105(3):473-491. PubMed
4.Heesterbeek TJ, Lores-Motta L, Hoyng CB, Lechanteur YTE, den Hollander AI. Risk factors for progression of age-related macular degeneration. Ophthalmic Physiol Opt. 2020;40(2):140-170. PubMed
5.Al-Zamil WM, Yassin SA. Recent developments in age-related macular degeneration: A review. Clin Interv Aging. 2017;12:1313-1330. PubMed
6.Flores R, Carneiro A, Vieira M, Tenreiro S, Seabra MC. Age-related macular degeneration: Pathophysiology, management, and future perspectives. Ophthalmologica. 2021;244(6):495-511. PubMed
7.Nicolo M, Ferro Desideri L, Vagge A, Traverso CE. Faricimab: An investigational agent targeting the Tie-2/angiopoietin pathway and VEGF-A for the treatment of retinal diseases. Expert Opin Investig Drugs. 2021;30(3):193-200. PubMed
8.Stanga PE, Valentin-Bravo FJ, Stanga SEF, Reinstein UI, Pastor-Idoate S, Downes SM. Faricimab in neovascular AMD: First report of real-world outcomes in an independent retina clinic. Eye (Lond). 2023;37(15):3282-3289. PubMed
9.CADTH reimbursement recommendation: Faricimab (Vabysmo). Can J Health Technol. 2022;2(8). https://www.cadth.ca/sites/default/files/DRR/2022/SR0719REC-Vabysmo.pdf. Accessed 2023 Sep 28.
10.Meer EA, Oh DH, Brodie FL. Time and distance cost of longer acting anti-VEGF therapies for macular degeneration: Contributions to drug cost comparisons. Clin Ophthalmol. 2022;16:4273-4279. PubMed
11.Khanani AM, Thomas MJ, Aziz AA, et al. Review of gene therapies for age-related macular degeneration. Eye (Lond). 2022;36(2):303-311. PubMed
12.Cruess AF, Berger A, Colleaux K, et al. Canadian expert consensus: Optimal treatment of neovascular age-related macular degeneration. Can J Ophthalmol. 2012;47(3):227-235. PubMed
13.Wysong A, Lee PP, Sloan FA. Longitudinal incidence of adverse outcomes of age-related macular degeneration. Arch Ophthalmol. 2009;127(3):320-327. PubMed
14.Cruess A, Zlateva G, Xu X, Rochon S. Burden of illness of neovascular age-related macular degeneration in Canada. Can J Ophthalmol. 2007;42(6):836-843. PubMed
15.Agree Next Steps C. The AGREE II Instrument. [Hamilton, ON]: AGREE Enterprise; 2017: https://www.agreetrust.org/wp-content/uploads/2017/12/AGREE-II-Users-Manual-and-23-item-Instrument-2009-Update-2017.pdf.
16.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
17.Kodjikian L, Parravano M, Clemens A, et al. Fluid as a critical biomarker in neovascular age-related macular degeneration management: Literature review and consensus recommendations. Eye (Lond). 2021;35(8):2119-2135. PubMed
18.Chaikitmongkol V, Sagong M, Lai TYY, et al. Treat-and-extend regimens for the management of neovascular age-related macular degeneration and polypoidal choroidal vasculopathy: Consensus and recommendations from the Asia-Pacific Vitreo-Retina Society. Asia Pac J Ophthalmol (Phila). 2021;10(6):507-518. PubMed
19.Flaxel CJ, Adelman RA, Bailey ST, et al. Age-Related Macular Degeneration Preferred Practice Pattern®. Ophthalmology. 2020;127(1):P1-P65. PubMed
20.Nikkhah H, Karimi S, Ahmadieh H, et al. Intravitreal injection of anti-vascular endothelial growth factor agents for ocular vascular diseases: Clinical practice guideline. J Ophthalmic Vis Res. 2018;13(2):158-169. PubMed
21.National Institute for Health and Care Excellence. Age-related macular degeneration (NICE guideline NG82). 2018; https://www.nice.org.uk/guidance/ng82. Accessed 2023 Sep 9.
22.National Institute for Health and Care Excellence. Faricimab for treating wet age-related macular degeneration (Technology appraisal guidance TA800). 2022; https://www.nice.org.uk/guidance/ta800. Accessed 2023 Sep 10.
23.Cheng CK, Chen SJ, Chen JT, et al. Optimal approaches and criteria to treat-and-extend regimen implementation for neovascular age-related macular degeneration: Experts consensus in Taiwan. BMC Ophthalmol. 2022;22(1):25. PubMed
24.Agency for Care Effectiveness (ACE). Ranibizumab for treating age-related macular degeneration, diabetic macular oedema and retinal vein occlusion. 2022; https://www.ace-hta.gov.sg/healthcare-professionals/ace-technology-guidances/details/ranibizumab-for-treating-age-related-macular-degeneration-diabetic-macular-oedema-and-retinal-vein-occlusion. Accessed 2023 Sep 9.
25.Yeung L, Hsieh YT, Yang CH, et al. Management of neovascular age-related macular degeneration: Taiwan expert consensus. J Formos Med Assoc. 2021;120(12):2061-2071. PubMed
26.National Institute for Health and Care Excellence. Brolucizumab for treating wet age-related macular degeneration (Technology appraisal guidance TA672). 2021; https://www.nice.org.uk/guidance/ta672. Accessed 2023 Sep 10.
27.Ross AH, Downey L, Devonport H, et al. Recommendations by a UK expert panel on an aflibercept treat-and-extend pathway for the treatment of neovascular age-related macular degeneration. Eye (Lond). 2020;34(10):1825-1834. PubMed
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Table 2: Characteristics of Included Guidelines
Intended users, target population | Intervention and practice considered | Major outcomes considered | Evidence collection, selection, and synthesis | Evidence quality assessment | Recommendations development and evaluation | Guideline validation |
|---|---|---|---|---|---|---|
Kodjikian et al. (2021)17 | ||||||
Intended users: Clinicians Target population: Patients with nAMD | Management of nAMD: diagnosis and treatment Anti-VEGF drugs: ranibizumab, aflibercept, and bevacizumab | Visual outcomes | A literature search of PubMed was performed, and 66 publications (guidelines, consensus statements, systematic reviews, and primary studies) were included. | The grading of evidence was based on recent European guidance but the methods used were unclear. | The consensus panel discussed the evidence and relied on their expert opinion and experience to develop a management algorithm for patients with nAMD. The recommended algorithm for treatment was primarily based on OCT monitoring of intraretinal fluid. | The guideline was published in a peer-reviewed medical journal, which is the official journal of the Royal College of Ophthalmologists. |
Chaikitmongkol et al. (2021)18 | ||||||
Intended users: Clinicians in the Asia-Pacific region Target population: Adult patients with nAMD | T and E regimens (ranibizumab, aflibercept, and bevacizumab) for nAMD and polypoidal choroidal vasculopathy | Key outcomes: Changes in best-corrected visual acuity from baseline to end of the study. | A systematic search of the MEDLINE, EMBASE, and Cochrane databases, in addition to abstracts from the Asia-Pacific Vitreo-retina Society, European Society of Retina Specialists, American Academy of Ophthalmology, and Controversies in Ophthalmology: Asia-Australia congresses. The guidelines included 17 RCTs, observational studies or systematic reviews. | The methods for grading evidence were unclear. | A group of 18 medical retina specialists from the Asia-Pacific Vitreo-retina Society discussed factors such as drug efficacy and safety, molecular properties, and different types of fluid in the retina. The expert panel developed a set of consensus recommendations for the implementation of T and E regimens, which were agreed upon by all members of the panel. | The guideline is a publication on behalf of the Asia-Pacific Vitreo-retina Society. |
Flaxel et al. (2020)19 | ||||||
Intended users: Ophthalmologists Target population: Patients with AMD | AMD interventions such as antioxidant vitamins and minerals, intravitreal injection of anti-VEGF agents (ranibizumab, aflibercept, brolucizumab and bevacizumab), photodynamic therapy, and laser photocoagulation | Patient outcomes: visual, anatomic outcomes or QoL. | Cochrane systematic reviews | To rate individual studies, a scale based on SIGN is used. The individual studies were divided into 7 levels from I++ (high) to III (low). The body of evidence quality ratings are defined by GRADE as “good,” “moderate,” and “insufficient.” | Key recommendations for care are defined by GRADE as “strong recommendation” or “discretionary recommendation.” | The guideline is a publication on behalf of the American Academy of Ophthalmology. |
Nikkhah et al. (2018)20 | ||||||
Intended users: Ophthalmologists in Iran Target population: Patients with ocular vascular disease | Intravitreal injection of anti-VEGF agents (ranibizumab, aflibercept, and bevacizumab) | Effectiveness and safety outcomes, such as visual and anatomic outcomes. | Several websites and databased were searched to find relevant clinical practice guidelines and additional evidence. | The level of evidence was determined from level I (systematic reviews or meta-analysis) to level IV (expert opinion or consensus). | The technical committee created various scientifically possible answers (scenarios) for each question, based on the available evidence. The retina specialists then reviewed the draft answers and rated the best one on a scale of 1 (being the worst choice) to 9 (being the best choice). | This guideline was created with the supervision of the Office for Health care Standards, Deputy of Curative Affairs, Iran Ministry of Health and Medical Education. |
NICE guideline (2018)21 | ||||||
Intended users: Health care and social care professionals, commissioners, and providers, and people with AMD Target Population: adults with AMD | Diagnosis, pharmacological and non-pharmacological management, including anti-VEGF (ranibizumab, aflibercept, and bevacizumab) | Patient-relevant outcomes such as visual acuity, and QoL, and health economic outcomes. | Systematic reviews and health economic evidence synthesis: where possible, meta-analyses were conducted to combine the results of studies for each outcome. | GRADE framework | Interventions that must (or must not) be used. Interventions that should (or should not) be used – a “strong” recommendation. Interventions that could be used - a “weak” recommendation. | The guideline is a NICE-approved guideline that underwent the necessary peer-review process. |
AMD = age-related macular degeneration; GRADE = Grading of Recommendations Assessment, Development and Evaluation; nAMD = neovascular age-related macular degeneration; NICE = National Institute for Health and Care Excellence; OCT = optical coherence tomography; QoL = quality of life; RCT = randomized controlled trial; SIGN = Scottish Intercollegiate Guideline Network; T and E = treat-and-extend; VEGF = vascular endothelial growth factor.
Note that this table has not been copy-edited.
Appendix 3: Critical Appraisal of Included Publications
Table 3: Strengths and Limitations of Guidelines Using AGREE II15
Item | Kodjikian et al. (2021)17 | Chaikitmongkol et al. (2021)18 | Flaxel et al. (2020)19 | Nikkhah et al. (2018)20 | NICE guideline (2018)21 |
|---|---|---|---|---|---|
Domain 1: Scope and purpose | |||||
1. The overall objective(s) of the guideline is (are) specifically described. | Yes | Yes | Yes | Yes | Yes |
2. The health question(s) covered by the guideline is (are) specifically described. | Yes | Yes | Yes | Yes | Yes |
3. The population (patients, public, etc.) to whom the guideline is meant to apply is specifically described. | Not explicit but implied | Yes | Not explicit but implied | Not explicit but implied | Yes |
Domain 2: Stakeholder involvement | |||||
4. The guideline development group includes individuals from all relevant professional groups. | Unclear if at least 1 methodology expert was included. | Unclear if at least 1 methodology expert was included. | Yes | Unclear if at least 1 methodology expert was included. | Yes |
5. The views and preferences of the target population (patients, public, etc.) have been sought. | Unclear | Unclear | Unclear | Unclear | Yes |
6. The target users of the guideline are clearly defined. | Not explicit but implied | Not explicit but implied | Yes | Yes | Yes |
Domain 3: Rigour of development | |||||
7. Systematic methods were used to search for evidence. | Partially (only PubMed was searched) | Yes | Yes | Unclear | Yes |
8. The criteria for selecting the evidence are clearly described. | No | Yes | Yes | No | Yes |
9. The strengths and limitations of the body of evidence are clearly described. | No | No | Yes | No | Yes |
10. The methods for formulating the recommendations are clearly described. | Yes | Yes | Yes | Yes | Yes |
11. The health benefits, side effects, and risks have been considered in formulating the recommendations. | Unclear | Unclear | Unclear | Unclear | Yes |
12. There is an explicit link between the recommendations and the supporting evidence. | No | No | Partially yes | No | Partially yes |
13. The guideline has been externally reviewed by experts before its publication. | Unclear | Unclear | Yes | Unclear | Yes |
14. A procedure for updating the guideline is provided. | No | No | Yes | No | Yes |
Domain 4: Clarity of presentation | |||||
15. The recommendations are specific and unambiguous. | Yes | Yes | No | No | Yes |
16. The different options for management of the condition or health issue are clearly presented. | No | No | Yes | No | Yes |
17. Key recommendations are easily identifiable. | Yes | Yes | Yes | Yes | Yes |
Domain 5: Applicability | |||||
18. The guideline describes facilitators and barriers to its application. | No | Yes | No | No | Yes |
19. The guideline provides advice and/or tools on how the recommendations can be put into practice. | Yes | Yes | No | No | Yes |
20. The potential resource implications of applying the recommendations have been considered. | No | No | Yes | Yes | Yes |
21. The guideline presents monitoring and/or auditing criteria. | Yes | Yes | No | No | Yes |
Domain 6: Editorial independence | |||||
22. The views of the funding body have not influenced the content of the guideline. | Unclear | Unclear | Yes | No financial support | Yes |
23. Competing interests of guideline development group members have been recorded and addressed. | Conflicts of interest were declared but it was unclear how they were addressed. Several authors had received grants or consultation fees from industries. | Conflicts of interest were declared but it was unclear how they were addressed. Several authors had received grants or consultation fees from industries. | Yes | No conflicts of interest | Yes |
NICE = National Institute for Health and Care Excellence.
Note that this table has not been copy-edited.
Appendix 4: Main Study Findings
Note that this appendix has not been copy-edited.
Table 4: Summary of Recommendations in Included Guidelines
Recommendations and supporting evidence | Quality of evidence and strength of recommendations |
|---|---|
Kodjikian et al. (2021)17 | |
The consensus panel recommended an algorithm for managing patients with nAMD based on fluid observed using OCT and other imaging technologies. | Unclear |
“The consensus panel agreed that morphological parameters observed on OCT are the most important criteria in routine clinical practice for the diagnosis of nAMD. The whole stack of images should be used, to give as full a picture as possible.” (p. 2130) | Unclear |
For patients with suspected nAMD, the consensus panel recommends OCT to look for morphological parameters indicative of nAMD:
If these parameters are not present, the panel suggests considering differential diagnoses. (“Figure 2a in the publication”) If one or more parameters are present, the panel recommends further tests: “If available, OCT-angiography (OCT-A) is considered to be valuable in order to visualise the neovascular complex.” “If OCT-A is not available, FA can be used to visualise leakage from the lesion, but is otherwise no longer judged to be a mandatory technique for nAMD diagnosis in all AMD cases.” “However, clinical signs visualised using biomicroscopy or fundus photography/examination are still considered useful to support the diagnosis.” (p. 2130) The recommended algorithm listed hemorrhage, hard exudates, macular edema, subretinal fibrosis, and pigment epithelial elevation as examples of supporting clinical signs of nAMD detectable through biomicroscopy or fundus examination. | Unclear |
“In cases where PCV or type 3 MNV is suspected, ICGA and OCT-A are recommended to confirm this diagnosis. In addition to the morphological and clinical signs of nAMD, patient age over 50 years is an important criterion for a diagnosis of nAMD.” (p. 2130) | Unclear |
“…regardless of the anti-VEGF agent used, T&E is the recommended regimen for the management of nMAD because it provides comparable clinical outcomes, reduction in the number of clinic visits, to fixed monthly or bimonthly injections with a reduction in injection burden compared with fixed dosing.” (p. 2130) Supporting evidence was unclear; the guideline authors cited 2 references. | Unclear |
“Treatment with anti-VEGF therapy should be initiated as soon as possible once the diagnosis of nAMD is made.” (p. 2131) | Unclear |
Initiate anti-VEGF treatment “Initiation phase of at least 2 injections at monthly intervals. Duration of initiation phase should be individualized based on initial patient response” (p. 2129) | Unclear |
“Treatment should be given proactively at each visit—a key aspect of T&E treatment design. The decision on whether the treatment interval should be extended, retained, or reduced is also made at each visit, and is based on disease activity as assessed using OCT.” (p. 2131) | Unclear |
“If disease activity is observed at three consecutive visits, with no sign of anatomical and/or functional improvement, the clinician should consider whether the initial diagnosis of nAMD was correct, using additional imaging modalities to provide more information if necessary.” (p. 2131) | Unclear |
“If further investigation confirms the original diagnosis, then the consensus panel recommends treatment should be continued for at least 2 to 3 additional injections at the minimum interval permitted by the product label before a switch to an alternative anti-VEGF therapy is considered. If a patient is switched to a different anti-VEGF therapy due to lack of efficacy, this should be done with a new initiation phase.” (p. 2131) | Unclear |
“If there is no evidence of disease activity at the treatment visit, the clinician may consider extending the treatment interval by 2–4 weeks, to a maximum of 16 weeks (or potentially more with longer-acting anti-VEGF agents), however, there will be a higher risk of recurrence.” (p. 2131) | Unclear |
“If a patient reaches stability at a particular treatment interval, this should be maintained over the long term if feasible. If the treatment interval is alternately being extended and reduced at each visit, the clinician can consider that the shorter of the two intervals is the more appropriate one for the patient and maintain this interval for a period of time before re-evaluating the patient’s treatment needs in due course.” (p. 2131) | Unclear |
“There is currently no evidence to support stopping anti-VEGF treatment in patients with stable disease, as disease activity will very likely recur, but the clinician may consider that continued long-term anti-VEGF therapy may not be appropriate or beneficial in patients with low vision who have fibrosis, extensive subretinal haemorrhage, subfoveal disruption of the external limiting membrane or the ellipsoid zone or central atrophy of the RPE.” (p. 2131) | Unclear |
Chaikitmongkol et al. (2021)18 | |
Initiation phase (p, 514) “Following nAMD or PCV diagnosis, at least 3 consecutive monthly intravitreal anti-VEGF injections should be given until no disease activity (ie, new hemorrhage or fluid on OCT) is observed.” | Unclear |
Maintenance phase and interval adjustments (p. 514) “If no disease activity is observed at indicates follow-up visits: when using ranibizumab or bevacizumab, inject and extend treatment interval by 2 weeks between visits up to 12 weeks; when using aflibercept, inject and extend treatment interval by 2–4 weeks between visits up to a maximum interval of 16 weeks.” If disease activity is observed, inject and shorten the treatment interval by 2 to 4 weeks, until IRF and/or SRF are not observed, then the treatment interval can be gradually extended.” | Unclear |
Fluid compartment considerations (p. 514) “IRF should always be treated until resolved.” “For persistent residual SRF despite continuous anti-VEGF injections, subfoveal fluid of ≤ 200mm may be tolerated, and the treatment interval could be maintained or gradually extended by 2–4 weeks, depending on the anti-VEGF agent, if vision is stable and there are no signs of disease worsening.” | Unclear |
Stopping anti-VEGF treatment (p. 514) “Clinical experience from the panel suggests anti-VEGF therapy may be discontinued in some patients on a case-by-case basis after careful discussion with patients. Specifically, patients should be counselled regarding the increased risk of disease reactivation that may lead to irreversible vision loss.” “The panel suggests it may be reasonable to attempt discontinuing injections in patients with stable inactive disease who have received treatments at 16-week intervals for a few consecutive visits (eg, two 16-week intervals) to avoid lifelong injections. After discontinuation, patients should be advised to regularly self-monitor for symptoms of declining vision. Scheduled monitoring visits are crucial for detecting early recurrences and for monitoring the fellow eye status. Additionally, treatment discontinuation can be considered in patients with advanced nAMD/PCV with substantial scarring and/or atrophy (ie, medical futility).” “There is currently no level 1 evidence in the literature regarding stopping anti-VEGF treatment for nAMD.” | Unclear |
Flaxel et al. (2020)19 | |
“Fluorescein angiography, optical coherence tomography (OCT), and optical coherence tomography angiography (OCTA) are useful diagnostic tests in clinical practice to detect new or recurrent neovascular disease activity and guide therapy.” | Unclear |
“In patients with neovascular AMD, early detection and prompt treatment improves the visual outcome. Intravitreal injection therapy using anti-vascular endothelial growth factor (VEGF) agents (e.g., aflibercept, bevacizumab, and ranibizumab) is the most effective way to manage neovascular AMD and represents the first line of treatment. Symptoms suggestive of postinjection endophthalmitis or retinal detachment require prompt evaluation.” (p. 9) | Unclear |
“Anti-VEGF therapies have become first-line therapy for treating and stabilizing most cases of neovascular AMD.” (p. 22) Supporting evidence: A Cochrane systematic review demonstrates the effectiveness of these agents to maintain visual acuity. | I+, Good quality, Strong recommendation |
Nikkhah et al. (2018)20 | |
General recommendations for intravitreal anti-VEGF injection procedure | |
“Anti-VEGFs should be used cautiously in patients with a history of systemic vascular diseases such as stroke or myocardial infarction (MI) during the past three months. Appropriate consultations should be made before administration of anti-VEGF injections.” (p. 161) | Evidence levels: Consensus |
“Bilateral intravitreal injection is not recommended. However, it is not contraindicated and can be performed at the surgeon’s discretion. Separate gloves, surgical preps, and vials with different batches should be used for each eye.” (p. 161) | Evidence levels: Consensus |
“The procedure can be conducted in the outpatient sterile operating room.” (p. 161) | Evidence levels: Consensus |
“Individual sterile gloves should be used for each patient.” (p. 161) | Evidence levels: Consensus |
“Physicians should wear surgical masks when performing the injection. Physicians and patients should minimize speaking during the procedure.” (p. 161) | NR |
“The patient’s name, anti-VEGF agent type, and laterality should be checked immediately before intravitreal injection.” (p. 161) | NR |
“It is recommended that topical anesthetics be used before prep and drapes to minimize patient discomfort.” (p. 161) | NR |
“Eyelids and the lid margins should be sterilized with povidone-iodine (10%).” (p. 161) | NR |
“The eyelids should be retracted from the intended injection site by a sterile speculum and the needle should not have any touch with the lid margins.” (p. 161) | Evidence levels: Consensus |
“Diluted povidone-iodine (5%) should be applied to the conjunctival injection site for at least 30 seconds before injection.” (p. 161) | NR |
“It is recommended that a 29 or 30 -gauge needle be used to perform anti-VEGF intravitreal injections.” (p. 161) | Evidence levels: Consensus |
“It is recommended that intravitreal injection be performed between the horizontal and vertical rectus muscles at the pars plana 3 and 4mm posterior to the limbus in pseudophakic and aphakic eyes, prospectively. However, the quadrant selection can be chosen using patient-specific considerations and preference of the physician. In the majority of settings, a simple perpendicular injection approach is preferred” (p. 161 to 162) | Evidence levels: Consensus |
“It is not necessary to prescribe topical antibiotics immediately and/or for a few days after intravitreal injection. A growing body of evidence discourages the post-injection antibiotics.” (p. 162) | Evidence levels: Consensus |
“It is recommended that intravitreal bevacizumab, aflibercept and ranibizumab be injected at a dosage of 1.25 mg/0.05 ml, 2 mg/0.05 ml and 0.5 mg/0.05 ml, respectively in patients with ocular vascular diseases.” (p. 162) | NR |
“An information brochure about the signs and symptoms of post-injection complications and emergency contact details should be presented to patients after injection. Patients should be aware of the necessity of urgent visit in case of ocular pain and visual impairment. Therefore, a routine first day post-injection visit is not necessary.” (p. 162) | Evidence levels: Consensus |
“In patients at risk for optic nerve damage due to the rise in intraocular pressure (IOP) after intravitreal injection, topical anti-glaucoma drugs or anterior chamber paracentesis should be administered.” (p. 161) | Evidence levels: Consensus |
“One of the following strategies can be used for injecting intravitreal anti-VEGF agents based on the clinician’s priority:
| NR |
“Although the rhegmatogenous retinal detachment (RRD) following intravitreal anti-VEGF injections is rare (incidence = 0.013%), the risk of RRD should be considered, especially among myopic patients, who should be monitored after each injection.” (p. 162) | Evidence levels: II |
Recommendations for nAMD | |
“Considering the effectiveness, safety, and rare and transient complications of IVB and other anti-VEGF drugs injections, it is recommended these drugs be used to treat patients with neovascular AMD.” (p. 163) | Evidence levels: I |
“It is recommended that patients be given sufficient information regarding the need for repeated, frequent intravitreal anti-VEGF injections for the treatment of neovascular AMD.” (p. 163) | Evidence levels: III |
“Multiple intravitreal anti-VEGF injections do not reduce retinal nerve fiber layer thickness. Therefore, it is recommended that intravitreal anti-VEGF injections be repeated as needed.” (p. 163) | Evidence levels: III |
“In unilateral anti-VEGF injections, it is recommended that physicians consider the condition of the fellow eye.” (p. 163) | Evidence levels: I |
“It is also recommended that IVB injection be used to treat patients with active neovascular AMD coexisting with retinal pigment epithelium (RPE) tear to improve their visual acuity.” (p. 163) | Evidence levels: III |
“In patients with neovascular AMD who are undergoing anti-VEGF treatment, there is a risk of scar formation, especially in the cases of classic CNV, increased central retinal thickness, and the presence of excessive subfoveal fluids or deposits.” (p. 163) | Evidence levels: II |
“To stabilize the visual and anatomic (CMT) outcomes in patients with persistent neovascular AMD (unresponsive to IVB), it is recommended that IVR or aflibercept injections be used. The presence of intraretinal fluid has an adverse effect on visual acuity improvement. However, residual subretinal fluid does not impede visual improvement and may even improve the visual acuity prognosis.” (p. 163) | Evidence levels: I |
NICE guideline (2018)21 | |
Recommendations: 5 “Offer fundus examination as part of the ocular examination to people presenting with changes in vision (including micropsia and metamorphopsia) or visual disturbances.” (p. 79) Quality of evidence: Very low | Strong |
Recommendations: 8 for late AMD (wet active)
Quality of evidence: Very low to moderate | Strong |
Recommendations: 9 “Make an urgent referral for people with suspected late AMD (wet active) to a macula service, whether or not they report any visual impairment. The referral should normally be made within 1 working day but does not need emergency referral.” No supporting evidence | Unclear |
Recommendations: 12 “For eyes with confirmed late AMD (wet active) for which antiangiogenic treatment is recommended (see recommendations 21–30), offer treatment as soon as possible (within 14 days of referral to the macula service).” No supporting evidence | Strong |
Recommendations: 13 “Ensure intraocular injections are given by suitably trained healthcare professionals, for example:
If the injection is delivered by someone who is not medically qualified, ensure that cover is in place to manage any ophthalmological or medical complications.” (p. 109) No supporting evidence | Unclear |
Recommendations: 21 “Offer intravitreal anti-vascular endothelial growth factor (VEGF) treatment for late AMD (wet active) for eyes with visual acuity within the range specified in recommendation 26.” (p. 172) Main supporting evidence “High-quality evidence from a network meta-analysis showed that people receiving anti-VEGF treatments have better visual acuity than those receiving placebo (the probability that all anti-VEGF regimens are at least 5 ETDRS letters better than placebo was 0.999 at 1 year and 0.995 at 2 years) (up to 26 RCTs of 10,925 people).” (p. 150) | Strong recommendation |
Recommendations: 22 “Be aware that no clinically significant differences in effectiveness and safety between the different anti-VEGF treatments have been seen in the trials considered by the guideline committee.” (p. 172) Main supporting evidence: “Moderate- to high-quality evidence from a network meta-analysis showed that there is no difference in visual acuity between people receiving different anti-VEGF treatments at up to 2 years’ follow-up (the probability that any anti-VEGF agent is at least 5 ETDRS letters better than any other was 0.045 at 1 year and 0.060 at 2 years) (up to 26 RCTs of 10,925 people).” (p. 151) “High-quality evidence could not differentiate vision-related quality of life (NEI VFQ-25) between aflibercept and ranibizumab at 1 year’s follow-up (MD −0.39 [95%CI −1.71 to 0.93]; 2 RCTs of 2,412 people).” (p. 151) | Could be used (weak recommendation) |
Recommendations: 23 “In eyes with visual acuity of 6/96 or worse, consider anti-VEGF treatment for late AMD (wet active) only if a benefit in the person’s overall visual function is expected (for example, if the affected eye is the person’s better-seeing eye).” (p. 172) | Could be used (weak recommendation) |
Recommendations: 24 “Be aware that anti-VEGF treatment for eyes with late AMD (wet active) and visual acuity better than 6/12 is clinically effective and may be cost effective depending on the regimen used.” | Unclear |
Recommendations: 26 “Ranibizumab, within its marketing authorisation, is recommended as an option for the treatment of wet age-related macular degeneration if:
Main supporting evidence “Moderate- to high-quality evidence showed that people receiving ranibizumab were much more likely to have a large improvement in visual acuity and less likely to have a large deterioration in visual acuity compared with those receiving control treatment at 1 year’s follow-up (gain of 15+ ETDRS letters RR 3.25 [95%CI 1.44 to 7.33]; loss of fewer than 15 ETDRS letters RR 1.51 [95%CI 1.41 to 1.63]; 4 RCTs of 1,415 people).” High-quality evidence reported that people receiving ranibizumab had substantially better visual acuity than those receiving control treatment at 1 year’s follow-up (MD 17.80 ETDRS letters [95%CI 15.95 to 19.65]; 3 RCTs of 1,322 people).” (p. 149) “High-quality evidence showed greater vision-related quality of life (NEI-VFQ-25) in people receiving ranibizumab compared with people receiving control treatment at 1 year’s follow-up (MD 6.69 [95%CI 3.38 to 9.99]; 2 RCTs of 1,134 people).” (p. 150) | Unclear |
Recommendations: 29 “Aflibercept solution for injection is recommended as an option for treating wet age-related macular degeneration only if:
Main supporting evidence from NICE technology appraisals and health economic evidence. | Unclear |
Recommendations: 30 “People currently receiving aflibercept solution for injection whose disease does not meet the criteria in recommendation 29 should be able to continue treatment until they and their clinician consider it appropriate to stop.” (p. 173) Main supporting evidence from NICE technology appraisals. | Unclear |
Recommendations: 34 “Consider switching anti-VEGF treatment for people with late AMD (wet active) if there are practical reasons for doing so (for example, if a different medicine can be given in a regimen the person prefers) but be aware that clinical benefits are likely to be limited.” (p. 198) Quality of evidence: Very low | Could be used (weak recommendation) |
Recommendations: 35 “Consider observation without giving anti-VEGF treatment if the disease appears stable.” (p. 198) Quality of evidence: Very low | Could be used (weak recommendation) |
Recommendations: 36 “Consider stopping anti-VEGF treatment if the eye develops severe, progressive loss of visual acuity despite treatment as recommended in the section on antiangiogenic therapies.” (p. 198) Quality of evidence: Very low | Could be used (weak recommendation) |
Recommendations: 37 “Stop anti-VEGF treatment if the eye develops late AMD (wet inactive) with no prospect of functional improvement.” (p. 198) Quality of evidence: Very low | Unclear |
Recommendations: 38 “Ensure that patients are actively involved in all decisions about the stopping or switching of treatment.” (p. 198) Supporting evidence: patients experiences or comments from stakeholders | Unclear |
Recommendations: 46 “Offer people with late AMD (wet active) ongoing monitoring with OCT for both eyes.” (p. 219) Quality of evidence: Very low to moderate | Strong |
Recommendations: 47 “Offer fundus examination or colour photography if OCT appearances are stable, but:
Quality of evidence: Very low to moderate | Strong |
Recommendations: 48 “Consider FFA to identify unrecognised neovascularisation if OCT appearances are stable, but:
Quality of evidence: Very low to moderate | Weak |
Recommendations: 49 “If OCT results suggest macular abnormalities but the abnormalities are not responding to treatment, think about:
Quality of evidence: Very low to moderate | Unclear |
AMD = age-related macular degeneration; CI = confidence interval; CMT = central macular thickness; CNV = choroidal neovascularization; FDA = US FDA; IRF = intraretinal fluid; IVB = intravitreal bevacizumab; IVR = intravitreal ranibizumab; MD = mean difference; MNV= macular neovascularization; nAMD = neovascular age-related macular degeneration; NEI-VFQ-25 = National Eye Institute 25-Item Visual Function Questionnaire; NICE = National Institute for Health and Care Excellence; NR = not reported; OCT = optical coherence tomography; PCV = polypoidal choroidal vasculopathy; RCT = randomized controlled trial; RPE = subretinal pigment epithelium; RR = risk ratio; RRD = rhegmatogenous retinal detachment; PRN = pro re nata; SRF = subretinal fluid; T&E = treat-and-extend; VEGF = vascular endothelial growth factor.
Appendix 5: Other Relevant Guidelines with Alternative or Unclear Methodology
Note that this appendix has not been copy-edited.
Description
We have compiled recommendations from guidelines or guidance documents that are considered non–evidence-based, as identified in our literature search. The development methods of these guidelines were either unclear or used nonsystematic methods (alternative methodology). These publications were not critically appraised using AGREE II.15 Refer to Table 5 for more information on the Characteristics of Guidelines with Alternative or Unclear Methodology.
The Ministry of Health Singapore suggests using ranibizumab as an alternative to bevacizumab for treating visual impairment due to wet AMD in adults.24 The certainty of supporting evidence and the strength of the recommendation are unclear. Two NICE technology appraisal guidance papers22,26 recommended the newly approved anti-VEGF drugs, faricimab or brolucizumab, as potions for treating wet AMD in adults with similar situations as bevacizumab and aflibercept only if, the best-corrected visual acuity is between 6/12 and 6/96; there is no permanent structural damage to the central fovea; the lesion size is 12 disc areas or less in greatest linear dimension, there is recent presumed disease progression (for example, blood vessel growth, as shown by fluorescein angiography, or recent visual acuity changes), and the manufacturer provides these drugs according to the commercial arrangement with confidential discount. Two expert consensus papers from Taiwan23,25 and 1 recommendation paper27 for a UK expert panel provided recommendations for a treat-and-extend (T and E) approach using anti-VEGF drugs. The consensus papers23,25,27 recommend initiating a loading phase of 3 consecutive monthly anti-VEGF injections, followed by adjusting the injection intervals based on monitoring disease activity or visual functions. Table 6 presents the Summary of Recommendations from Guidelines with Alternative or Unclear Methodology.
Table 5: Characteristics of Guidelines with Alternative or Unclear Methodology
Intended users, target population | Intervention and major outcomes considered | Evidence collection, synthesis, and assessment | Recommendation development | Guideline validation |
|---|---|---|---|---|
Agency for Care Effectiveness (2022)24 | ||||
Intended users: NR Target population: Adults with visual impairment | Relevant intervention: Ranibizumab Outcomes considered: NR | NR | NR | Established by the Ministry of Health (Singapore). |
NICE (2022)22 | ||||
Intended users: Health care providers and patients Target population: Adults with wet AMD | Relevant intervention: Faricimab Outcomes considered: Best-corrected visual acuity | “The appraisal committee considered evidence submitted by Roche, a review of this submission by the evidence review group (ERG), and responses from stakeholders.” (p. 7) | Committee discussion | NR |
Cheng et al. (2022)23 | ||||
Intended users: Health care providers Target population: patients with nAMD | Relevant Intervention: Anti-VEGF treat-and-extend regimens (aflibercept, bevacizumab, and ranibizumab) Outcomes considered: Visual outcomes and treatment burden | Evidence from RCTs and real-world studies and recommendations from guidelines, but the search methods and evidence synthesis were unclear. | Face-to-face meeting discuss by 14 local retina specialists in Taiwan. | NR |
NICE (2021)26 | ||||
Intended users: Health care providers and patients Target population: Adults with wet AMD | Relevant intervention: Brolucizumab Outcomes considered: Best-corrected visual acuity | “The appraisal committee considered evidence submitted by Novartis, a review of this submission by the evidence review group (ERG), and submissions from other stakeholders.” (p. 7) | Committee discussion | NR |
Yeung et al. (2021)25 | ||||
Intended users: Health care professionals Target population: patients with nAMD | Relevant intervention: Anti-VEGF therapy (aflibercept, bevacizumab, ranibizumab, and brolucizumab) Outcomes considered: visual outcomes | A nonsystematic review of published studies. | Eleven retina specialists, each with at least 10 years of experience, discussed a recommendation statement. All procedures or statements receiving endorsement from at least half of the experts. | Taiwan Retina Society initiated the development. |
Ross et al. (2020)27 | ||||
Intended users: Health care professionals and patients Target population: Patients with nAMD | Relevant intervention: Aflibercept T and E pathway Outcomes considered: Visual outcomes | A nonsystematic review of published studies. | Bayer hosted and financed 2 roundtable meetings with retinal specialists to inform recommendations in London in 2018 and 2019. | NR |
AMD = age-related macular degeneration; nAMD = neovascular age-related macular degeneration; NICE = National Institute for Health and Care Excellence; NR = not reported; RCT = randomized controlled trial; T and E = treat-and-extend; VEGF = vascular endothelial growth factor.
Table 6: Summary of Recommendations From Guidelines With Alternative or Unclear Methodology
Recommendations and rationale |
|---|
Agency for Care Effectiveness (2022)22 |
“Ranibizumab 1.65 mg/0.165 ml pre-filled syringe and 2.3 mg/0.23 ml solution for injection as an alternative to intravitreal bevacizumab for treating adults with visual impairment due to:
|
NICE (2022)24 |
“Faricimab is recommended as an option for treating wet age-related macular degeneration in adults, only if:
|
“If patients and their clinicians consider faricimab to be 1 of a range of suitable treatments (including aflibercept and ranibizumab), choose the least expensive treatment. Take account of administration costs, dosage, price per dose and commercial arrangements.” (p. 4) |
“Only continue faricimab if an adequate response to treatment is maintained. Criteria for stopping should include persistent deterioration in visual acuity and anatomical changes in the retina.” (p. 4) |
“These recommendations are not intended to affect treatment with faricimab that was started in the NHS before this guidance was published. People having treatment outside these recommendations may continue without change to the funding arrangements in place for them before this guidance was published, until they and their NHS clinician consider it appropriate to stop.” (p. 4) |
Rationale: Faricimab is a treatment option for wet AMD, working similarly to aflibercept and ranibizumab. Clinical trials show that faricimab is equally effective as aflibercept, and an indirect comparison with ranibizumab suggests similar clinical effectiveness. Cost comparison reveals similar costs and overall health benefits to aflibercept or ranibizumab. |
Cheng et al. (2022)23 |
Treatment goal “The treatment goal of nAMD is to maximize and maintain BCVA benefits for patients while minimizing treatment burden.” (p. 3, table 2 in the original publication) |
Initiation of an anti-VEGF therapy “Treatment could start with 3 consecutive monthly (or 4-weekly) injections.” (p. 3, table 2 in the original publication) |
Length of treatment interval extension or shortening
|
Treatment adjustment criteria
Notes for the recommendation were available in the paper. |
Treatment exit criteria
Notes for the recommendation were available in the paper. |
NICE (2021)26 |
“Brolucizumab is recommended as an option for treating wet age-related macular degeneration in adults, only if, in the eye to be treated:
It is recommended only if the company provides brolucizumab according to the commercial arrangement.” (p. 4) |
“If patients and their clinicians consider brolucizumab to be one of a range of suitable treatments, including aflibercept and ranibizumab, choose the least expensive (taking into account administration costs and commercial arrangements).” (p. 4) |
“Only continue brolucizumab in people who maintain an adequate response to therapy. Criteria for stopping should include persistent deterioration in visual acuity and identification of anatomical changes in the retina that indicate inadequate response to therapy.” (p. 4) |
“These recommendations are not intended to affect treatment with brolucizumab that was started in the NHS before this guidance was published. People having treatment outside these recommendations may continue without change to the funding arrangements in place for them.” (p. 4) |
Rationale: Brolucizumab is a treatment option for wet AMD. Clinical trials and a network meta-analysis show that brolucizumab has similar overall health benefits, safety and cost to aflibercept and ranibizumab. |
Yeung et al. (2021)25 |
Diagnosis (p. 2063) “…initial nAMD diagnosis should include a comprehensive ophthalmologic examination consisting of best-corrected visual acuity (BCVA) measurement, OCT, color fundoscopy (CF), and fluorescein angiography (FA). FA should be performed with caution or avoided in patients with fluorescein allergy or high risks of adverse reactions to intravenous administration of the dye. OCT angiography (OCTA) may be an alternative choice for patients who cannot receive FA. Regular follow-up is suggested for patients with nAMD in order to provide prompt intervention for accelerated or irreversible disease progression indicated by vision loss and/or changes found by ophthalmological examinations.” |
Evaluation (p. 2063 to p. 2064) Functional parameter (VA) “Assessment of BCVA during the initial consultation and each follow-up visit is highly recommended. In contrast to the Early Treatment Diabetic Retinopathy Study (ETDRS) chart predominantly adopted by clinical trials of anti-VEGF agents, the Snellen and the Landolt C charts are more accessible and commonly used in clinical practice in Taiwan. The Snellen and ETDRS measurements can be converted to a logarithm of the Minimum Angle of Resolution (logMAR) for cross-referencing.” Parameters in multimodal imaging-OCT findings “Subretinal fluid (SRF) and subretinal pigment epithelium (sub-RPE) fluid are both regarded as early signs of active disease. Intraretinal fluid (IRF) abnormally accumulating in intraretinal cysts may cause neurosensory deficiencies and lead to vision loss. Subretinal hyper-reflective material (SHRM) is a morphological characteristic reported to affect VA, and hyper-reflective foci (HF) are thought to indicate severe disease progression or advancement. Central retinal thickness (CRT) is a measurement of the macula from the internal limiting membrane to the RPE and can be quantified by OCT scans.” Parameters in multimodal imaging CF/FA/OCT-A “CF, FA, ICGA, and OCTA provide ancillary and alternative imaging evidence to support the diagnosis and treatment efficacy of nAMD. CF can reveal hemorrhages or exudations from neovascular lesions. Assisted by fluorescein, FA further provides details for the classification and characteristics of the neovascular lesions. OCTA is noninvasive examination that produces three-dimensional images for the evaluation and monitoring of neovascular activities.” “OCTA results can be presented in place of FA when intravenous administration of fluorescein is contraindicated.” |
Loading phase (p. 2064 to p. 2065) “Patients with nAMD are recommended to receive anti-VEGF treatment.” “An initial 3-month loading phase is recommended as the primary strategy for anti-VEGF treatment on the basis of favourable clinical trial outcomes.” “…the expert panel suggests a 3-month loading phase, which consists of regular follow-ups that include OCT and optional BCVA examination and a flexible number of injections at the ophthalmologist’s discretion.” |
Evaluation after the 3 loading doses (p. 2066, table 2 in the original publication) “The panel recommends the evaluation of treatment efficacy within the first month after the end of the loading phase.” Evaluation targets
Decreased or unchanged sub-RPE fluid/PED/SHRM/HF/CRT.” |
Maintenance phase and recommendation for treat-and-extend strategy (p. 2067 to p. 2068, table 3 in the original publication) Shorten (−2 to −4 weeks, minimum 4-week)
OR
Maintain
AND
Extend ( + 2 to + 4 weeks, maximum 16-week)
AND
|
Recommendations for the PRN strategy in maintenance phase (table 4 in the original publication) Treat
OR
OR
Follow-up only
AND
|
When to stop and reinitiate therapy (p. 2068 to p. 2069) “…the consensus recommends that, with sufficient treatment duration and followup assessment, treatment discontinuation or follow-up interval extension could be considered according to the following patient status: (i) patients who are nonresponsive to treatment showing end-stage disease or fibrosis, and (ii) patients who show stable disease and demonstrate financial concerns.” “The expert panel recommends that intervals between follow-up visits can be extended if the disease is stable and the patient is well-educated about the disease. Patients with extended follow-up periods are highly recommended to monitor changes in their vision and to self-examine with the Amsler grid once a day.” |
Ross et al. (2020)27 |
The panel recommended an aflibercept T and E pathway for treating nAMD. (p. 1826 to p. 1827, figure 1 in the original publication) “The loading phase consists of three consecutive aflibercept doses at 4-weekly intervals. Visual acuity (VA) should be assessed at each visit during the loading phase. The panel suggests using optical coherence tomography (OCT) imaging at Visit 1 to provide baseline data and at Visit 3 to provide early treatment response data; however, the use of OCT during the loading phase is optional and at the treating clinician’s discretion.” |
“Patients receive a fourth aflibercept dose 8 weeks after the third loading dose. Both VA and OCT should be checked at this visit, and at every subsequent visit, to assess the length of the next treatment interval.” (p. 1826) |
“According to the licensed posology of aflibercept, three 4-weekly loading injections should be given, followed by a fourth injection 8 weeks later, before treatment interval extension can begin. However, in clinical practice, the treating physician may, at their discretion, choose to maintain or extend treatment intervals immediately after the third injection according to the individual needs of the patient” (p. 1826) |
“After the fourth injection, the treatment interval is either maintained with active disease or extended by 2- or 4-week adjustments with inactive disease. After the fifth aflibercept dose, the treatment interval is reduced, maintained or extended based on specific criteria.” (p. 1826) |
“The expert panel recommends using 2-week increments for most patients to minimise the risk of disease reactivation. However, 4-week adjustments may be considered in patients who respond particularly well and have a dry macula after the loading phase. Occasionally, finer adjustments of the treatment interval may be required, e.g., by 1 week or 3 weeks, at the discretion of the treating clinician.” (p. 1828) |
“The expert panel recommends treatment interval reduction with intraretinal fluid (IRF) on OCT, as it is considered a sign of active disease.” (p. 1828) “The expert panel recommends treating SRF to stability.” (p. 1828) |
AMD = age-related macular degeneration; BCVA = best-corrected visual acuity; CRT = central retinal thickness; ETDRS = Early Treatment Diabetic Retinopathy Study; HF = hyperreflective foci; IRF = intraretinal fluid; nAMD = neovascular age-related macular degeneration; NICE = National Institute for Health and Care Excellence; NV = neovascular; OCT = optical coherence tomography; PED = pigment epithelial detachment; PRN = pro re nata; SHRM = subretinal hyperreflective material; SRF = subretinal fluid; sub-RPE = subretinal pigment epithelium; T and E = treat-and-extend; VEGF = vascular endothelial growth factor.
Appendix 6: References of Potential Interest
Note that this appendix has not been copy-edited.
Systematic Reviews of Clinical Practice Guidelines
Han X, Chen Y, Gordon I, et al. A systematic review of clinical practice guidelines for age-related macular degeneration. Ophthalmic Epidemiol. 2023;30(3):213-220. PubMed
Additional References
Editorial
Sivaprasad S, Barnes B, Barrett T, et al. The Royal College of Ophthalmologists Commissioning guidelines on age macular degeneration: Executive summary. Eye (Basingstoke). 2022;36(11):2078-2083. PubMed
Tuuminen R, Sipilä R, Komulainen J, Saarela V, Kaarniranta K, Tuulonen A. The first ophthalmic Choosing Wisely recommendations in Finland for glaucoma and wet age-related macular degeneration. Acta Ophthalmol. 2019;97(5):e808-e810. PubMed
Guidance Paper for Administrating Brolucizumab in Unclear Population
Fonollosa A, Gallego-Pinazo R, Sararols L, Adán A, López-Gálvez M, Figueroa MS. Guidance on brolucizumab management recommendations. Arch Soc Esp Oftalmol (Engl Ed). 2022:S2173-5794(22)00084-6.
Action Paper Based on Included NICE Guidelines
Gale RP, Mahmood S, Devonport H, et al. Action on neovascular age-related macular degeneration (nAMD): Recommendations for management and service provision in the UK hospital eye service. Eye (Lond). 2019;33(Suppl 1):1-21. PubMed
Publication Excluded for Unclear Recommendation
Amoaku W, Balaskas K, Cudrnak T, et al. Initiation and maintenance of a Treat-and-Extend regimen for ranibizumab therapy in wet age-related macular degeneration: Recommendations from the UK Retinal Outcomes Group. Clin Ophthalmol. 2018;12:1731-1740. PubMed
Liang L-N, Xie L-K, Wu X-W. International clinical practice guideline of Chinese medicine-age-related macular degeneration. World J Tradit Chin Med. 2022;8(4):556-564.
Sadda SR, Guymer R, Holz FG, et al. Consensus definition for atrophy associated with age-related macular degeneration on OCT: Classification of atrophy report 3. Ophthalmology. 2018;125(4):537-548. PubMed
Recommendation for Monitoring the Fellow Eyes in Patients With Wet AMD
Wong TY, Lanzetta P, Bandello F, et al. Current concepts and modalities for monitoring the fellow eye in neovascular age-related macular degeneration: An expert panel consensus. Retina. 2020;40(4):599-611. PubMed
Contributors: Elizabeth Carson, Kim Le, Thyna Vu
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up to date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners' own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada's federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user's own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for noncommercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada's health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada's federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca