CADTH Health Technology Review
Point-of-Care Ultrasound for Guided Central Venous Catheter Insertion
Rapid Review
Authors: Khai Tran, Jennifer Horton
Abbreviations
CVC
central venous catheter
ESA
European Society of Anesthesiology
ESPNIC
European Society of Pediatric and Neonatal Intensive Care
ICU
intensive care unit
IJV
internal jugular vein
PICC
peripheral inserted central catheter
POCUS
point-of-care ultrasound
SHM
Society of Hospital Medicine
US
ultrasound
Key Messages
Limited evidence suggested that the use of point-of-care ultrasound (POCUS) to guide the insertion of central venous lines in adults was effective and safe compared with traditional or fluoroscopic guidance method.
All 3 included guidelines recommend the use of POCUS to guide cannulation through different locations of insertion in both adults and children.
We did not identify any economic studies on the cost-effectiveness of POCUS-guided central venous line insertion.
Context and Policy Issues
A central line, also known as central venous line, central venous catheter (CVC), or central venous access device, is a long soft tube (catheter) inserted through a vein that leads to a position near the heart or inside the heart.1 The central line allows doctors and nurses easy access to patients’ veins for extended periods of time and is essential for delivery of large amounts of medicine (e.g., chemotherapy), fluids or nutrition that may not go through a regular IV line (a line inserted into a vein in the hand, arm, foot, leg or scalp).2 The central lines are classified depending on the duration of catheter use (i.e., short-term, midterm, long-term), type of insertion (i.e., central, peripheral), and insertion location.2 Four common types of central lines include peripheral inserted central catheter (PICC); subclavian line; internal jugular line; and femoral line.1,2 PICC is more popular as it is easy to insert into a large vein in the upper arm (e.g., brachial vein, basilic vein) and has lower procedural risk, such as pneumothorax, than other central lines.2 The other 3 lines, which bear the name of the corresponding veins (i.e., subclavian vein, internal jugular vein, femoral vein), are more common for temporary venous access.2
Traditional central line insertion using the landmark techniques is associated with a high risk of mechanical complications.3 Potential complications include catheter malposition, pneumothorax or hemothorax (a collection of air or blood, respectively, between the lung and chest wall), air embolism, thrombosis (blood clot), bleeding, and infection.4 On the other hand, central line insertion under the guidance of ultrasonography has become a routine method in emergency medicine, with the goal of reducing these complications.3 The term POCUS has become more common in clinical practice.5 It represents bedside ultrasound (US)-based procedures using portable US devices for diagnostic or therapeutic purposes.5 For vascular access, POCUS helps identify the vein's location and provides real-time guidance for the insertion of central catheter lines.6The operator inserts the catheter into the vein of choice until the tip of the catheter is close to the heart under the guidance of POCUS. However, the placement of the central line, even under US guidance, is not free of the mechanical complications mentioned above. The operator then performs a chest X-ray immediately to verify the catheter position and check for complications.4 Chest X-ray represents the gold standard for verification of tip position after the catheter has been inserted.4 Recent studies7-9 have shown that POCUS can be equally effective as the radiography method in the determination of the catheter position and complications; thus, reducing the potential risk of radioactive exposure.
Although some health care providers prefer the use of POCUS to guide vascular access in emergency and internal medicine as it is easy to use and provides real-time guidance for central line insertion,6,10 its clinical effectiveness, safety and cost-effectiveness compared with other non-POCUS guidance techniques such as fluorography or the traditional landmark methods remain to be elucidated. The current report aims to summarize the clinical effectiveness and cost-effectiveness of POCUS for guided central venous line insertion. The report also aims to summarize the recommendations from evidence-based guidelines regarding the use of POCUS for guided central venous line insertion.
Research Questions
What is the clinical effectiveness of point-of-care ultrasound for guided central venous catheter insertion?
What is the cost-effectiveness of point-of-care ultrasound for guided central venous catheter insertion?
What is the evidence-based guidelines regarding the use of point-of-care ultrasound for guided central venous catheter insertion?
Methods
Literature Search Methods
An information specialist conducted a literature search on key resources including MEDLINE, the Cochrane Database of Systematic Reviews, the International HTA Database, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search approach was customized to retrieve a limited set of results, balancing comprehensiveness with relevancy. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. Search concepts were developed based on the elements of the research questions and selection criteria. The main search concepts were point-of-care ultrasound and catheters. The search was completed on August 23, 2023, and limited to English-language documents published since January 1, 2018.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first screening level, the reviewer reviewed the titles and abstracts and retrieved potentially relevant articles for inclusion. Table 1 presents the inclusion criteria for the final selection of full-text articles.
Criteria | Description |
|---|---|
Population | Patients (of any age) who require central venous catheter access procedures |
Intervention | Point-of-care ultrasound for guided central venous catheter insertion |
Comparator | Q1 and Q2: Guided central venous catheter insertion without the use of point-of-care ultrasound imaging Q3: Not applicable |
Outcomes | Q1: Clinical benefits (e.g., precision rate or insertion accuracy, time to treatment, patient or provider preference, patient quality of life) or harms (e.g., safety, rate of adverse events, type of adverse events, length of hospital stay) Q2:Cost-effectiveness (e.g., cost per QALY gained, ICER) Q3: Recommendations regarding use of point-of-care ultrasound for guided central venous catheter insertion (e.g., appropriate use of point-of-care ultrasound [when not to use point-of-care ultrasound], patient population, type of guided central venous catheter insertion) |
Study designs | Health technology assessments, systematic reviews, randomized controlled trials, nonrandomized studies, economic evaluations, evidence-based guidelines |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Exclusion Criteria
We excluded articles that did not meet the selection criteria outlined in Table 1, or articles published before 2018.
Critical Appraisal of Individual Studies
One reviewer critically appraised the included publications using the following tools as a guide: The Downs and Black checklist11 for nonrandomized studies, and the Appraisal of Guidelines for Research and Evaluation (AGREE) II instrument12 for guidelines. Summary scores were not calculated for the included studies; rather, each publication's strengths and limitations were described narratively.
Summary of Evidence
Quantity of Research Available
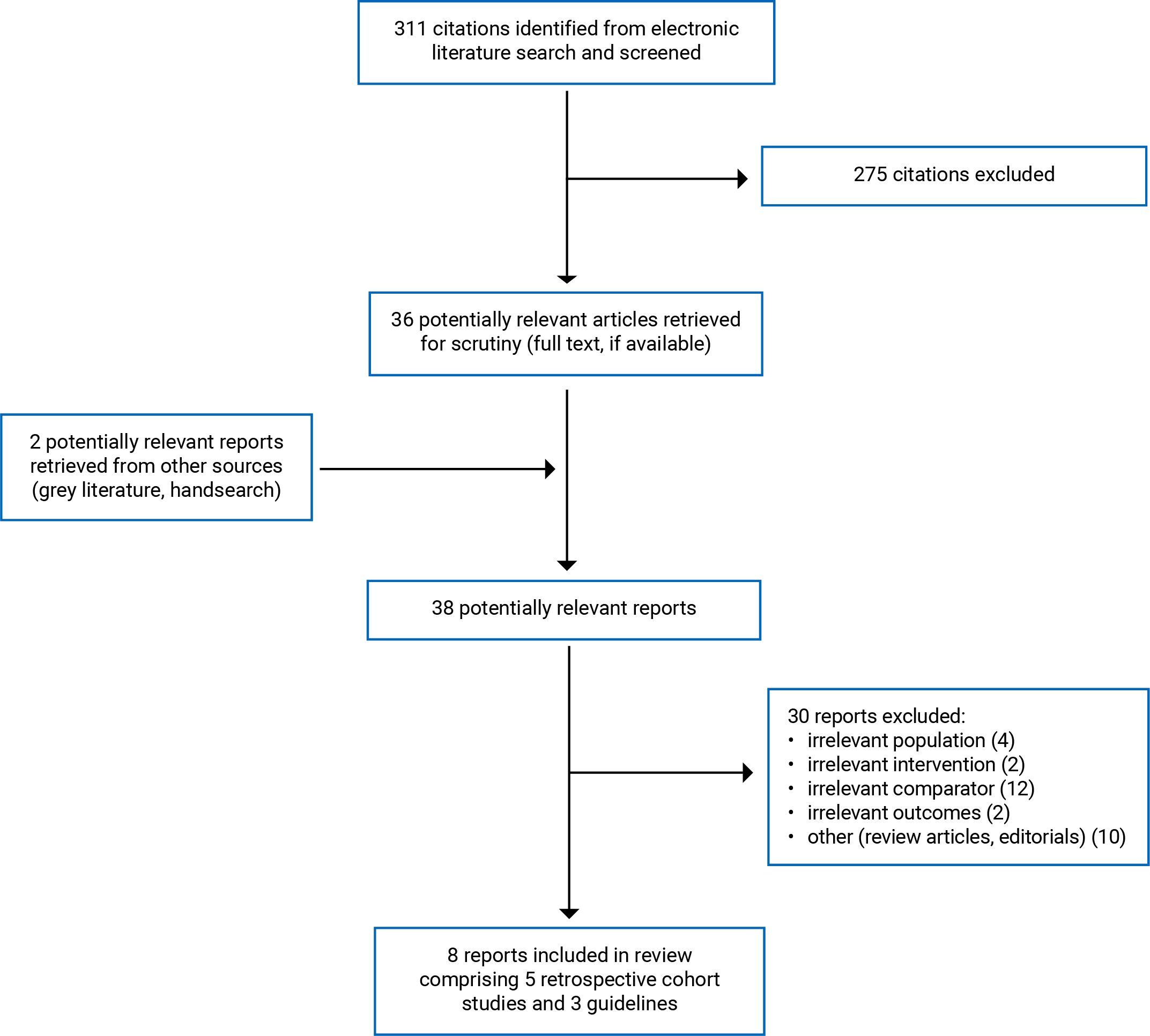
We identified a total of 311 citations from the literature search. Following the screening of titles and abstracts, we excluded 275 citations and retrieved 36 potentially relevant reports from the electronic search for full-text review. We also retrieved 2 potentially relevant publications from the grey literature search. Of these potentially relevant articles, we excluded 30 publications for various reasons, and included 8 publications that met the inclusion criteria. These comprised 5 nonrandomized studies and 3 evidence-based guidelines. Appendix 1 presents the PRISMA13 flow chart of the study selection.
Summary of Study Characteristics
Appendix 2 provides details regarding the characteristics of 5 included primary studies14-18 (Table 2) and 3 evidence-based guidelines19-21 (Table 3).
Study Design
The 5 included primary studies were all retrospective cohort studies.14-18 The studies were published from 2022 to 2019.
The 3 evidence-based guidelines include: The European Society of Anesthesiology (ESA) guidelines by Lamperti et al. (2020),19 the European Society of Pediatric and Neonatal Intensive Care (ESPNIC) guidelines by Singh et al. (2020),20 and the Society of Hospital Medicine (SHM) guidelines by Franco-Sadud et al. (2019).21
The authors of the ESA and SHM guidelines19,21 conducted a systematic literature review from multiple databases, while the authors of the ESPNIC guideline performed a literature search for relevant studies from PubMed. The authors of the ESA and ESPNIC guidelines19,20 used the Grading of Recommendations, Assessment, Development, and Evaluations (GRADE) tool to assess the level of evidence and strength of recommendations. In contrast, the authors of the SHM guideline21 established the quality of evidence and strength of recommendations by consensus using the Research and Development (RAND) Appropriateness method. The authors in all 3 included guidelines19-21 clearly described the development and evaluation methods of the recommendations.
Country of Origin
The included primary studies were conducted by authors from Israel14 and the Republic of Korea.15-18 All studies were conducted at a single institution (i.e., hospital).
The authors of the ESA and ESPNIC guidelines19,20 were from Europe, while those of the SHM guideline21 were in the US.
Patient Population
Patients from all included primary studies14-18 were adults who were admitted to the medical or surgical intensive care unit (ICU) for central line insertion for various reasons. In 3 studies,14,15,17 the mean age ranged from 54 to 75 years, and in 2 studies,16,18 the median age was 59 and 65. Underlying comorbidities (e.g., sepsis, shock, respiratory failure, acute kidney injury, ventilator use, or cerebrovascular accident) were more frequent in the US-guided groups compared to the corresponding comparators.14-16,18
For the included guidelines:
The target population in the ESA guideline19 was adults and children who underwent vascular cannulation. The intended users were clinicians involved in perioperative procedures.
The target population in the ESPNIC guideline20 was critically ill neonates and children in pediatric ICU. The intended users were critical care providers and clinicians working in pediatric ICU.
The target population in the SHM guideline21 was acutely ill adult patients who required central venous access. The intended users were health care providers and clinicians who routinely place central and peripheral access catheters in acutely ill patients.
Interventions and Comparators
For terminology, we used the term “central venous line” wherever possible to describe all central lines, irrespective to location of insertion (e.g., PICC, subclavian line, internal jugular line, and femoral line). The authors in some studies referred to “peripheral venous access” for PICC, and “central venous access” for the 3 central venous lines using the subclavian vein, internal jugular vein, or femoral vein. In studies where the authors referred to CVC for specific central lines, we reported the name of the veins where the catheters passed through. Some studies synonymously used the term “US guidance at bedside” with “POCUS guidance” in vascular access. Also, some studies used the term “cannulation” or “catheterization” to indicate central venous line insertion.
The authors of the included primary studies compared CVC inserted under POCUS guidance at a medical ICU versus CVC inserted using landmark method at a surgical ICU,14 PICC inserted under US guidance at bedside versus PICC inserted under fluoroscopic guidance in an angiography room or interventional radiology suite,15,16,18 and PICC inserted under US guidance at bedside versus PICC inserted using the blind method (synonymous with the landmark method) at bedside.17 Access veins for CVC were mainly internal jugular and subclavian veins,14 while those for PICC were mostly basilic and brachial veins.15,16,18
The authors of the included guidelines considered the use of US guidance for central venous line insertion in adult19,21 and pediatric patients.19,20
Outcomes
We present the outcomes reported in the included studies into groups of related outcomes, such as:
procedural characteristics (i.e., correct catheter tip placement,14-18 catheter tip malposition,14-16,18 technical failure,15,16 and procedure time16,18)
complications (i.e., pneumothorax,14,18 insertion site bleeding,15,18 thrombosis,15 insertion site infection,15 and systemic infection15)
other clinical outcomes (i.e., ICU mortality,15,16,18 length of ICU stay,16,18 and catheter insertion duration15,16,18)
The included guidelines19-21 considered all safety and effectiveness outcomes on the use of US for guidance for vascular access.
Summary of Critical Appraisal
Appendix 3 provides details regarding the strengths and limitations of included primary studies14-18 (Table 4) and guidelines19-21 (Table 5).
Primary Studies
The included studies14-18 were explicit in term of reporting, but had several limitations related to the external and internal validity that may reduce the certainty and generalizability of the findings.
For reporting, the authors of all included studies14-18 clearly described the study's objective, the main outcomes to be measured, the characteristics of the participants included in the study, the interventions of interest, and the main findings. The authors reported actual P values for the main outcomes in all studies.14-18 The authors of 4 studies14-16,18 reported adverse events of the intervention.
For external validity, the treatment settings (i.e., hospitals) in all studies14-18 were representative of the treatment most of the patients received. However, the patients may not be representative of the entire population from which they were selected, as the authors of each of the included studies14-18 conducted chart reviews from a single hospital.
For internal validity related to bias, all studies14-18 were of retrospective design, which had several limitations, including risks of selection bias, and missing data. However, the authors used statistical tests appropriately for comparison of variables and assessed the main outcome measures using accurate and reliable method using chest X-ray to verify the catheter tip positioning and the presence of potential complications immediately after catheter insertion.
For internal validity related to confounding, there were some differences between groups in demographic and clinical features of patients, and in experience of operators who performed the procedures. The authors of all included studies did not identify and adjust for potential confounding factors in the analyses. For instance, patients in the POCUS group were more ill with frequent underlying comorbidities compared with those in the control groups. The authors in all studies14-18 did not report whether sample size calculations were performed, and it is unclear whether the nonsignificant differences in certain outcomes were because the studies were underpowered for those outcomes.
Guidelines
The included guidelines19-21 had several strengths related to reporting. They were explicit in terms of scope and purpose (i.e., objectives, health questions and populations), and had clear presentation of recommendations (i.e., specific, unambiguous, and easy to find key recommendations, with options for managing the different conditions or health issues). In terms of stakeholder involvement, the authors of all included guidelines19-21 clearly defined target users and the development groups but did not report whether the views and preferences of the patients were sought. The methodology for the development of all included guidelines19-21 was robust. The authors of the guidelines,19-21 clearly reported methods for evidence collection, criteria for selection, and methods for evidence synthesis. There were explicit links between recommendations and the supporting evidence, and methods of formulating the recommendations in all guidelines.19-21 Also, the authors of all guidelines19-21 considered health benefits and risks of side effects in formulating the recommendations.
However, there were also some limitations related to guideline implementation and review. Specifically, the authors did not report the procedures for updating the guidelines.19-21 Facilitators and barriers to application, advice and/or tools on how the recommendations can be put into practice, and monitoring or auditing criteria were also unclear in the included guidelines.19-21 For editorial independence, the authors of all guidelines19-21 reported that all guideline development group members had no competing interest. However, the authors of 2 guidelines19,21 did not report if the views of the funding body had any influence on the content of the guidelines.
Overall, all 3 included guidelines19-21 were robust in terms of scope and development, rigour of development, and clarity of presentation.
Summary of Findings
Appendix 4 presents the main study findings, which were summarized by groups of major outcomes such as procedural characteristics (i.e., correct placement, malposition, technical failure, and median procedure time) (Table 6), complications (i.e., pneumothorax, insertion site bleeding, thrombosis, insertion site infection, and systemic infection) (Table 7), and other outcomes (i.e., ICU mortality, length of ICU stay, and insertion duration) (Table 8). The recommendations of the included guidelines19-21 were presented in Table 9 of Appendix 4.
Clinical Effectiveness of POCUS for Guided CVC Insertion
Procedural Characteristics
Correct Placement:
Five retrospective cohort studies14-18 reported mixed findings for this outcome.
In 1 study,14 CVC insertion using POCUS for guidewire visualization at a medical ICU resulted a statistically significantly higher correct placement rate compared to that of CVC insertion by traditional method in a surgical ICU (97.6% versus 88.0%; P = 0.001).
Three studies15,16,18 compared POCUS-guided PICC versus fluoroscopic-guided PICC. In 2 studies, the difference in correct placement rates did not reach statistical significance between US-guided PICC insertion at bedside and fluoroscopic-guided PICC insertion in an angiography room,15 or between US-guided PICC insertion at bedside and US-guided PICC insertion at bedside in an interventional radiology suite.16 In contrast, the results of 1 study18 on patients admitted to the neurosurgical ICU showed that US-guided PICC insertion at bedside by a neurointensivist had statistically significantly lower correct placement rate compared to fluoroscopic-guided PICC insertion at the interventional radiology suite by interventional radiologists (81.2% versus 100%; P = 0.004).
In another study,17 the difference in correct placement rates also did not reach statistical significance between PICC insertion under US guidance and PICC insertion using a blind method.
Malposition:
Four studies reported this outcome. The results of this outcome were mixed, following a similar pattern as results for the correct placement outcome.
In the study with CVC insertion,14 CVC tip was located too low among 2.4% of patients in the POCUS group compared with 12% of patients in the non-POCUS group (P = 0.001).
Three studies15,16,18 provided mixed findings for the comparison between POCUS-guided PICC and fluoroscopic-guided PICC. Two studies15,16 found no statistically significant difference in malposition rate between groups, while 1 study18 found that malposition rate was statistically significantly higher in the placement of US-guided PICC than the fluoroscopy-guided placement (P = 0.005).
Technical Failure:
There were no significant differences in the rates of technical failures, including puncture failure and guidewire passage disturbance, between US-guided PICC insertion group and fluoroscopic-guided PICC insertion group (2 studies).15,16
Procedure Time:
Two studies comparing POCUS-guided PICC versus fluoroscopic-guided PICC reported this outcome with different findings.
The results in 1 study16 showed that time required for a vascular surgeon to complete the US-guided PICC insertion procedure was statistically significantly shorter than the time required to insert a fluoroscopy-guided PICC by interventional radiologists (P = < 0.001). However, the results in another study18 showed no statistically significant difference in procedure times between US-guided PICC placement and fluoroscopy-guided PICC placement.
Complications
Three studies14,15,18 reported complications and did not find any statistically significant differences between groups.
Pneumothorax:
There were no statistically significant differences in pneumothorax rates between US-guided CVC and traditional CVC placements (1 study)14 or between US-guided PICC and fluoroscopy-guided PICC placements (1 study).18
Insertion Site Bleeding:
There were no statistically significant differences in rates of insertion site bleeding between US-guided PICC placement and fluoroscopy-guided PICC placement (2 studies).15,18
Thrombosis:
There was no statistically significant difference in the rate of thrombosis between US-guided PICC group and fluoroscopy-guided PICC group (1 study).15
Infection:
There was no statistically significant difference in the rates of insertion site infection and systemic infection between US-guided PICC placement group and fluoroscopy-guided PICC group (1 study).15
Other Outcomes
ICU Mortality:
Three studies comparing POCUS-guided PICC versus fluoroscopic-guided PICC reported this outcome with different results.
The results of 2 studies15,18 showed that the ICU mortality rates were statistically significantly higher in the US-guided PICC group than those in the fluoroscopy-guided PICC group (P < 0.001), while the results in another study16 showed no statistically significant difference in ICU mortality rate between the 2 groups.
Length of ICU Stay:
Two studies comparing POCUS-guided PICC versus fluoroscopic-guided PICC reported this outcome with different results.
The results in 1 study16 showed no statistically significant difference in the median length of ICU stay between US-guided PICC placement group and fluoroscopy-guided PICC group, while the results in other study18 showed that the ICU stay length was statistically significantly longer in patients who underwent US-guided PICC placement than those who underwent fluoroscopy-guided PICC placement.
Insertion Duration:
Three studies comparing POCUS-guided PICC versus fluoroscopic-guided PICC reported this outcome with different results.
The results in 1 study15 showed no statistically significant difference in median duration of PICC insertion between US-guided PICC placement group and fluoroscopy-guided PICC group, while the results in the other study16 showed that the US-guided PICC was used for a statistically significantly shorter duration than the fluoroscopy-guided PICC (P = 0.002). Another study18 reported that the median duration of using central line in the US-guided PICC was 20 days and that in the fluoroscopy-guided PICC was 28 days, without reporting statistical comparison between groups.
Guidelines Regarding the Use of POCUS for Guided CVC Insertion
The ESA guideline19 on perioperative use of US-guided for vascular access
US-Guided Vascular Cannulation in Adults
The ESA guideline provides recommendations for US-guided (including POCUS-guided) cannulation in adults via the internal jugular vein, the subclavian vein, the axillary vein, the femoral vein, the peripheral vein, and any central vein for long-term vascular access device placement.
The ESA guideline makes strong recommendations on the use of US guidance for internal jugular vein cannulation, for subclavian vein cannulation, for femoral vein cannulation, and for peripheral vein cannulation. Low to moderate quality evidence supported these recommendations.
The ESA guideline makes a weak recommendation on the use of US guidance for axillary vein cannulation, based on low-quality evidence.
The ESA guideline makes strong recommendations to use US guidance for placement of long-term vascular access devices via the axillary vein at the thorax, for catheter tip location and tip navigation, for preprocedural sonographic evaluation of all possible venous option, and for timely diagnosis of all potentially life-threatening complications (pneumothorax, hemothorax, cardiac tamponade and so on) after central venipuncture. Low to moderate quality evidence supported these recommendations.
US-Guided Vascular Cannulation in Children
The ESA guideline provides recommendations for US-guided cannulation in children via the internal jugular vein, the brachiocephalic vein, the femoral vein, and the peripheral vein.
The ESA guideline makes strong recommendations on the use of US guidance for internal jugular vein cannulation, for brachiocephalic vein cannulation, and for femoral cannulation. Low to moderate quality evidence supported these recommendations.
The ESA guideline makes a weak recommendation for routine use of US guidance for peripheral vein cannulation, based on moderate quality evidence.
The ESPNIC Guideline20 on the Use of POCUS in Critically Ill Neonates and Children
The ESPNIC guideline provides recommendations for use of vascular POCUS in central line placement.
For neonates and children, the ESPNIC guideline makes strong recommendations on the use of POCUS-guided technique to place ventral lines in the internal jugular vein, the subclavian vein, and the femoral vein. Supporting evidence for these recommendations was graded as level A or B, reflecting high or moderate confidence in the estimate of effect, respectively.
For children, the ESPNIC guideline makes a moderate recommendation for the use of POCUS-guided technique for PICC insertion, based on evidence with a quality level of B.
The SHM Guideline21 on the Use of US Guidance for Central and Peripheral Vascular Access in Adults
The SHM guideline provides recommendations on central venous access techniques and peripheral venous access techniques, including “real-time ultrasound guidance” (i.e., POCUS guidance).
Central venous access techniques
The SHM guideline makes strong recommendations, with very good consensus, on the use of real-time ultrasound guidance for internal jugular vein catheterization, for subclavian vein catheterization, and for femoral venous access.
Peripheral venous access techniques
The SHM guideline also makes a strong recommendation, with very good consensus, on the use of real-time ultrasound guidance for the insertion of PICCs.
Limitations
The existing evidence from the included clinical studies had some limitations. First, the nonrandomized, retrospective nature of the included studies cannot not rule out selection bias. Second, none of the studies reported data regarding the exact level of experience and expertise of the various operators from different ICUs, which may significantly impact the findings. In the study by Choi et al. (2021),16 a difference in procedure quality may occur between the vascular surgeons in the trauma ICU who conducted bedside PICC insertion under US guidance and the interventional radiologists who inserted PICC under fluoroscopic guidance due to difference in level of experience. Similar limitations may occur in the study by Kim et al. (2019),18 where PICC placement was performed by a neurointensivist under US guidance or by interventional radiologist under fluoroscopic guidance. In the study by Kwon et al. (2020),17 a skilled expert conducted the blind method, while US-guided PICC placements were performed by several operators with different skill sets, which could have affected the success rate of the procedure. Third, patients having US-guided central catheter insertion at beside were usually more critically ill and had more underlying comorbidities compared to those of corresponding comparators who were relatively healthier. Both patient groups had different causes of ICUs admission. US-guided bedside insertion would be difficult to apply in patients who had been hospitalized with prolonged chronic disease, who tend to have poor venous access. It is therefore conceivable that lower skill operators and patients with more comorbidities in the POCUS group would negatively impact the success rate of the procedure. Fourth, all included studies only reported short-term in-hospital clinical outcomes during admission such as correct placement of central line, and some procedural complications that occurred right after catheter insertion. However, the included studies did not investigate late complications during a longer duration of use such as catheter-related blood stream infections, central vein stenosis, catheter-related deep vein thrombosis, and complication-related mortality. In general, due to differences in patients’ characteristics and operators’ competence between groups, it is hard to conclude whether POCUS-guided central line insertion is more or less effective compared to the corresponding comparators. The evidence found in this report appeared to be institution-specific, and therefore it may not be generalizable to other institutions.
A limitation in both guidelines was that some recommendations were developed primarily based on generally weak evidence, with studies having high degree of heterogeneity due to different patient populations, settings and operators performing the procedures. As US guidance is not a therapeutic intervention, but rather a diagnostic and monitoring technique, evidence supporting the recommendation was mostly derived from short-term outcomes. We did not identify any Canadian guidelines regarding the use of POCUS for guidance of central catheter insertion.
Conclusions and Implications for Decision- or Policy-Making
We reviewed the clinical evidence from 5 studies,14-18 which were all retrospective nature in design comparing US-guided insertion of central lines at bedside with traditional landmark techniques or fluoroscopic guidance method. We did not identify any economic studies on cost-effectiveness of POCUS-guided central line insertion. We identified 3 evidence-based guidelines,19-21 which provided detailed recommendations on the use of US-guided for vascular access in children and adults.
For clinical evidence, bedside insertion of central line under US guidance in adults had high success rates, which were comparable with those under fluoroscopic guidance or traditional method. The between-group differences in patients’ characteristics and operators’ performance, as well as the procedure itself, may contribute to the mixed findings in success rates and certain outcomes (e.g., ICU mortality, length of ICU stay, insertion duration) between groups. Thus, US guidance for central line insertion at bedside appeared to be safe with few complications (e.g., pneumothorax, bleeding, infection) that were comparable with corresponding comparators.
All guidelines identified in this report support the use of US guidance cannulation using different vein location in both adults and children. The strengths of the recommendations were generally strong despite mixed levels of evidence due to heterogeneity from previous randomized controlled trials and observational studies. As POCUS devices are more portable and reportedly less expensive and easier to use, they are rapidly adopted and are widespread used in diverse clinical settings.6 By allowing direct visualization of the needle tip and target vessel, central line insertion at bedside using POCUS can be effective and safe during short-term of use, provided that it is performed by well-trained and experienced operators. A systematic training program with well-defined procedure competence is needed to ensure the overall success rates. Future well-controlled studies are needed to evaluate both short-term and long-term outcomes (including patient survival) of US guidance for central line insertion at bedside. Economic evaluation studies are also needed to determine whether the US guidance for central venous line insertion is cost-effective compared with non-US guidance approach. Publication of new literature may require future revision of the guidelines. As the included guidelines were developed by authors in Europe and US, the recommendations of the guidelines can be applied to the Canadian clinical practice.
References
1.Saint Luke's. Central Line (Central Venous Access Device). https://www.saintlukeskc.org/health-library/central-line-central-venous-access-device. Accessed 2023 Sep 19.
2.Chopra V. Central venous access: Device and site selection in adults. UpToDate 2023; https://www.uptodate.com. Accessed 2023 Sep 19.
3.Saugel B, Scheeren TWL, Teboul JL. Ultrasound-guided central venous catheter placement: a structured review and recommendations for clinical practice. Crit Care. 2017;21(1):225. PubMed
4.Tse A, Schick MA. Central Line Placement. StatPearls. Treasure Island (FL): StatPearls Publishing LLC.; 2023.
5.Moore CL, Copel JA. Point-of-care ultrasonography. N Engl J Med. 2011;364(8):749-757. PubMed
6.Required and Preferred Ultrasound Scanner Features for Conventional and Point-of-Care Applications. Plymouth Meeting (PA): ECRI; 2022.
7.Smit JM, Raadsen R, Blans MJ, Petjak M, Van de Ven PM, Tuinman PR. Bedside ultrasound to detect central venous catheter misplacement and associated iatrogenic complications: a systematic review and meta-analysis. Crit Care. 2018;22(1):65. PubMed
8.Kim YI, Ryu JH, Min MK, et al. Usefulness of ultrasonography for the evaluation of catheter misplacement and complications after central venous catheterization. Clin Exp Emerg Med. 2018;5(2):71-75. PubMed
9.Raman D, Sharma M, Moghekar A, Wang X, Hatipoglu U. Utilization of Thoracic Ultrasound for Confirmation of Central Venous Catheter Placement and Exclusion of Pneumothorax: A Novel Technique in Real-Time Application. J Intensive Care Med. 2019;34(7):594-598. PubMed
10.Huggins JTM, P.H. Indications for bedside ultrasonography in the critically ill adult patient. In: Post TW, ed. UpToDate. Vol 2023. Waltham (MA): UpToDate; 2023: https://www.uptodate.com. Accessed 2023 Sep 19.
11.Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377-384. PubMed
12.Agree Next Steps C. The AGREE II Instrument. Hamilton, ON: AGREE Enterprise; 2017: https://www.agreetrust.org/wp-content/uploads/2017/12/AGREE-II-Users-Manual-and-23-item-Instrument-2009-Update-2017.pdf. Accessed 2023 Sep 19.
13.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
14.Galante O, Sadeh R, Smoliakov A, et al. Real time wire localization by ultrasound during central line insertion improves accurate positioning in all upper torso sites. J Crit Care. 2022;67:79-84. PubMed
15.Cho S. Peripherally inserted central catheter procedure at the bedside by a nephrologist is safe and successful. Kidney Res Clin Pract. 2021;40(1):153-161. PubMed
16.Choi K, Keum MA, Kim MS, et al. Feasibility of the Ultrasound-Guided Insertion of the Peripherally Inserted Central Catheter (PICC) by the Vascular Surgeon at the Bedside in the Trauma Intensive Care Unit. Ann Vasc Surg. 2022;80:143-151. PubMed
17.Kwon S, Son SM, Lee SH, et al. Outcomes of bedside peripherally inserted central catheter placement: a retrospective study at a single institution. Acute Crit. 2020;35(1):31-37. PubMed
18.Kim YO, Chung CR, Gil E, Park CM, Suh GY, Ryu JA. Safety and feasibility of ultrasound-guided placement of peripherally inserted central catheter performed by neurointensivist in neurosurgery intensive care unit. pLoS ONE. 2019;14(5):e0217641. PubMed
19.Lamperti M, Biasucci DG, Disma N, et al. European Society of Anaesthesiology guidelines on peri-operative use of ultrasound-guided for vascular access (PERSEUS vascular access). Eur J Anaesthesiol. 2020;37(5):344-376. PubMed
20.Singh Y, Tissot C, Fraga MV, et al. International evidence-based guidelines on Point of Care Ultrasound (POCUS) for critically ill neonates and children issued by the POCUS Working Group of the European Society of Paediatric and Neonatal Intensive Care (ESPNIC). Crit Care. 2020;24(1):65. PubMed
21.Franco-Sadud R, Schnobrich D, Mathews BK, et al. Recommendations on the Use of Ultrasound Guidance for Central and Peripheral Vascular Access in Adults: A Position Statement of the Society of Hospital Medicine. J Hosp Med. 2019;14(9):E1-E22. PubMed
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Note that this appendix has not been copy-edited.
Table 2: Characteristics of Included Primary Clinical Studies
Study citation, country, funding source | Study design | Population characteristics | Intervention and comparator(s) | Clinical outcomes |
|---|---|---|---|---|
Galante et al. (2022)14 Country: Israel Funding source: NR | Retrospective cohort study conducted at a medical centre in Israel | Patients admitted to medical or surgical ICU and underwent CVC cannulation in the subclavian or internal jugular veins. Mean age (SD), years:
No statistically significant differences between groups in:
Comorbidities such as sepsis, shock, respiratory failure were more common in POCUS group (P = 0.001). Access vein:
| Intervention: CVC inserted under POCUS guidance at a medical ICU (N = 205) Comparator: CVC inserted traditionally at a surgical ICU (N = 191) Subsequent chest X-ray was used to determine tip position and to detect complications. | Outcomes:
|
Cho (2021)15 Country: Korea Funding source: NR | Retrospective cohort study conducted at a teaching hospital in Korea | Patients who had a PICC inserted by a nephrologist at a hospital in Korea. Mean age (SD), years:
No statistically significant differences between groups in:
Comorbidities such as sepsis, shock, acute kidney injury, ventilator use were more common in US-guided group (P < 0.001). | Intervention: PICC inserted under US guidance at bedside (N = 98) Comparator: PICC inserted under fluoroscopic guidance in an angiography room (N = 126) After the insertion procedure, the location of the catheter was verified by chest X-ray. | Outcomes:
|
Choi et al. (2021)16 Country: Korea Funding source: NR | Retrospective cohort study conducted at a regional trauma centre. | Patients who were severely injured and hospitalized in a trauma ICU underwent PICC insertion. Median age (range), years:
No statistically significant differences between groups in:
Comorbidity such as cerebrovascular accident was more common in US-guided group (P = 0.018) | Intervention: PICC inserted under US guidance at bedside (N = 55). Location of the catheter tip was confirmed with portable chest radiographs. Comparator: PICC inserted under fluoroscopic guidance in an interventional radiology suite (N = 42). Location of the catheter tip was determined via fluoroscopy in the suite. | Outcomes:
|
Kwon et al. (2020)17 Country: Korea Funding source: NR | Retrospective cohort study conducted at a hospital in Korea | Patients underwent PICC insertion at bedside.
Differences in patient characteristics between groups were not reported. | Intervention: PICC inserted under US guidance (N = 880) Comparator: PICC inserted using blind method, without US or fluoroscopy guidance (N = 447) Tip position was determined by a chest X-ray. | Outcomes:
|
Kim et al. (2019)18 Country: Korea Funding source: NR | Retrospective cohort study conducted at a hospital ICU in Korea | Patients underwent PICC or conventional CVC insertion. Median age (range), years:
No statistically significant differences between groups in:
Comorbidity such as previous stroke was more common in US-guided group (P = 0.049) Assess vein:
| Intervention: PICC inserted under US guidance at bedside (N = 32) Comparator:
Tip position was determined by a chest X-ray. | Outcomes:
|
APACHE II = Acute Physiology and Chronic Health Evaluation II; BMI = body mass index; CVC = central venous catheter; GFR = glomerular filtration rate; ICU = intensive care unit; ISS = injury severity score; NR = not reported; PICC = peripherally inserted central catheter; POCUS = point-of-care ultrasound; SD = standard deviation; US = ultrasound.
aMalposition was defined if the tip extended beyond the arc of the right atrium (too deep) or was located more than 2.5 cm above the entrance of the superior vena cava to the right atrium (too high), or when the tip migrated to the contralateral subclavian vein or the ipsilateral internal jugular vein.
bGood catheter function with catheter tip located between the superior vena cava and midportion of the right atrium.
cSubstandard inflow/outflow or catheter tip malposition.
dOptimal: location being within 3-cm margin (superiorly or inferiorly) from the cavoatrial junction; suboptimal: tip located within the superior vena cava or the right atrium, and if the coiled tip could be repositioned simply by pulling back on the catheter; malposition: tip was in other veins.
eMalposition was defined if the catheter tip is not located at the cavoatrial junction in chest radiographs.
Table 3: Characteristics of Included Guidelines
Intended users, target population | Intervention and practice considered | Major outcomes considered | Evidence collection, selection, and synthesis | Evidence quality assessment | Recommendations development and evaluation | Guideline validation |
|---|---|---|---|---|---|---|
ESA, Lamperti et al. (2020)19 | ||||||
Intended users: Clinicians involved in perioperative procedures Target population: Adults and children underwent vascular cannulation | Perioperative use of US guidance for vascular access in adults and children. | All safety and effectiveness outcomes of US-guided vascular access. |
| Quality of evidence was classified according to the GRADE system.a |
| Internally and externally reviewed, and published in a peer-reviewed journal. |
ESPNIC, Singh et al. (2020)20 | ||||||
Intended users: Critical care providers, clinicians working in pediatric ICU Target population: Critically ill neonates and children | The use of vascular, lung, vascular, cerebral, and abdominal POCUS in pediatric intensive care units. | Clinical outcomes on the use of POCUS. |
| Quality of evidence was rated from A (strong evidence) to C (very low evidence).b |
| Internally and externally reviewed, and published in a peer-reviewed journal. |
SHM, Franco-Sadud et al. (2019)21 | ||||||
Intended Users: Hospitalists and health care providers routinely place central and peripheral access catheters in acutely ill patients Target Population: Acutely ill adult patients | Use of US guidance for central and peripheral catheters access in adult patients. | Clinical outcomes, techniques, and training for the use of US guidance for vascular access. |
| Quality of evidence was established by consensus. |
| Internally and externally reviewed, and published in a peer-reviewed journal. |
ESPNIC =.European Society of Pediatric and Neonatal Intensive Care; POCUS = point-of-care ultrasound; RAND = Research and Development; SHM = Society of Hospital Medicine; US = ultrasound.
aStrength of recommendation:
1A (strong recommendation; high-quality evidence): Supporting by consistent evidence from well performed randomized, controlled trials or overwhelming evidence of some other form. Further research is unlikely to change our confidence in the estimate of benefit and risk.
1B (strong recommendation, moderate quality evidence): Supporting by evidence from randomized, controlled trials with important limitations (inconsistent results, methodologic flaws, indirect or imprecise), or very strong evidence of some other research design. Further research (if performed) is likely to have an impact on our confidence in the estimate of benefit and risk and may change the estimate.
2A (weak recommendation; high-quality evidence): Supporting by consistent evidence from well performed randomized, controlled trials or overwhelming evidence of some other form. Further research is unlikely to change our confidence in the estimate of benefit and risk.
2B (weak recommendation; moderate quality evidence): Supporting by evidence from randomized, controlled trials with important limitations (inconsistent results, methodologic flaws, indirect or imprecise), or very strong evidence of some other research design. Further research (if performed) is likely to have an impact on our confidence in the estimate of benefit and risk and may change the estimate.
2C (weak recommendation; low-quality evidence): Supporting by evidence from observational studies, unsystematic clinical experience, or from randomized, controlled trials with serious flaws. Any estimate of effect is uncertain.
bLevel of evidence:
A: Further research is very unlikely to change our confidence in the estimate of effect or accuracy.
B: Further research is likely to have an important impact on our confidence in the estimate of effect or accuracy and may change the estimate.
C: Further research is very likely to have an important impact on our confidence in the estimate of effect or accuracy and is likely to change the estimate. Any estimate of effect or accuracy is very uncertain (very low).
cStrength of recommendation: Range from 1 (for complete disagreement) to 9 (complete agreement). Labelled as “Strong agreement” if median score was between 7 and 9, and no score < 7; “Agreement” if median score was between 7 and 9, and no score < 4; “Disagreement” if score was between 1 and 3.
dVoting on draft recommendations considering 5 transforming factors: 1) Problem priority and importance; 2) Level of quality of evidence; 3) Benefit/harm balance; 4) Benefit/burden balance; 5) Certainty/concern about PEAF (Preferences/Equity/ Acceptability/Feasibility)
Voting on appropriateness using 9-point Likert scale: Inappropriate (1 to 3 points); Uncertain (4 to 6 points); Appropriate (7 to 9 points).
For a recommendation to be “appropriate,” it requires at least 70% agreement.
eLevels of consensus:
Perfect consensus: All respondents agree on one number (excluding the uncertain zone of 4 to 6).
Very good consensus: Median and middle 50% (interquartile range) of respondents are found at one integer (e.g., median and interquartile range are both at 8) or 80% of respondents are within one integer of the median (e.g., median is 8, 80% respondents are from 7 to 9).
Good consensus: 50% of respondents are within one integer of the median (e.g., median is 8, 50% of respondents are from 7 to 9) or 80% of the respondents are within 2 integers of the median (e.g., median is 7, 80% of respondents are from 5 to 9).
Some consensus: 50% or respondents are within 2 integers of the median (e.g., median is 7, 50% of respondents are from 5 to 9) or 80% of respondents are within 3 integers of the median (e.g., median is 6, 80% of respondents are from 3 to 9).
No consensus: All other responses. Any median with disagreement.
fStrength of recommendation:
Strong: based on perfect consensus. Wording: Recommend – must/to be/will.
Strong: based on very good consensus. Wording: Recommend – should be/can.
Weak/Conditional: based on good consensus. Wording: Suggest – to do.
Weak/Conditional: based on some consensus. Wording: Suggest – may do.
No: based on no consensus/disagreement. Wording: No recommendation was made regarding.
Appendix 3: Critical Appraisal of Included Publications
Note that this appendix has not been copy-edited.
Table 4: Strengths and Limitations of Clinical Studies Using the Downs and Black Checklist11
Strengths | Limitations |
|---|---|
Galante et al. (2022)14 | |
Reporting:
External validity:
Internal validity – bias:
| External validity:
Internal validity – bias:
Internal validity – confounding:
|
Cho (2021)15 | |
Reporting:
External validity:
Internal validity – bias:
| External validity:
Internal validity – bias:
Internal validity – confounding:
|
Choi et al. (2021)16 | |
Reporting:
External validity:
Internal validity – bias:
| External validity:
Internal validity – bias:
Internal validity – confounding:
|
Kwon et al. (2020)17 | |
Reporting:
External validity:
Internal validity – bias:
| Reporting:
External validity:
Internal validity – bias:
Internal validity – confounding:
|
Kim et al. (2019)18 | |
Reporting:
External validity:
Internal validity – bias:
| External validity:
Internal validity – bias:
Internal validity – confounding:
|
CVC = central venous catheter; ICU = intensive care unit; PICC = peripherally inserted central venous catheter; US = ultrasound.
Table 5: Strengths and Limitations of Guidelines Using AGREE II12
Item | ESA, Lamperti et al. (2020)19 | ESPNIC, Singh et al. (2020)20 | SHM, Franco-Sadud et al. (2019)21 |
|---|---|---|---|
Domain 1: Scope and purpose | |||
1. The overall objective(s) of the guideline is (are) specifically described. | Yes | Yes | Yes |
2. The health question(s) covered by the guideline is (are) specifically described. | Yes | Yes | Yes |
3. The population (patients, public, etc.) to whom the guideline is meant to apply is specifically described. | Yes | Yes | Yes |
Domain 2: Stakeholder involvement | |||
4. The guideline development group includes individuals from all relevant professional groups. | Yes | Yes | Yes |
5. The views and preferences of the target population (patients, public, etc.) have been sought. | Unclear | Unclear | Unclear |
6. The target users of the guideline are clearly defined. | Yes | Yes | Yes |
Domain 3: Rigour of development | |||
7. Systematic methods were used to search for evidence. | Yes | Yes | Yes |
8. The criteria for selecting the evidence are clearly described. | Yes | Yes | Yes |
9. The strengths and limitations of the body of evidence are clearly described. | Yes | Yes | Yes |
10. The methods for formulating the recommendations are clearly described. | Yes | Yes | Yes |
11. The health benefits, side effects, and risks have been considered in formulating the recommendations. | Yes | Yes | Yes |
12. There is an explicit link between the recommendations and the supporting evidence. | Yes | Yes | Yes |
13. The guideline has been externally reviewed by experts before its publication. | Yes | Yes | Yes |
14. A procedure for updating the guideline is provided. | Unclear | Unclear | Unclear |
Domain 4: Clarity of presentation | |||
15. The recommendations are specific and unambiguous. | Yes | Yes | Yes |
16. The different options for management of the condition or health issue are clearly presented. | Yes | Yes | Yes |
17. Key recommendations are easily identifiable. | Yes | Yes | Yes |
Domain 5: Applicability | |||
18. The guideline describes facilitators and barriers to its application. | Unclear | Unclear | Unclear |
19. The guideline provides advice and/or tools on how the recommendations can be put into practice. | Unclear | Unclear | Unclear |
20. The potential resource implications of applying the recommendations have been considered. | Unclear | Unclear | Unclear |
21. The guideline presents monitoring and/or auditing criteria. | Unclear | Unclear | Unclear |
Domain 6: editorial independence | |||
22. The views of the funding body have not influenced the content of the guideline. | Unclear | The project received no funding | Unclear |
23. Competing interests of guideline development group members have been recorded and addressed. | Yes | Yes | Yes |
AGREE II = Appraisal of Guidelines for Research and Evaluation II.
Appendix 4: Main Study Findings
Table 6: Summary of Findings by Outcome — Procedural Characteristics
Outcomes | Galante et al. (2022)14 | Cho (2021)15 | Choi et al. (2021)16 | Kwon et al. (2020)17 | Kim et al. (2019)18 | |||||
|---|---|---|---|---|---|---|---|---|---|---|
US-guided CVC | Traditional CVC | US-guided PICC | Fluoroscopic-guided PICC | US-guided PICC | Fluoroscopic-guided PICC | US-guided PICC | Blind-inserted PICC | US-guided PICC | Fluoroscopic-guided PICC | |
Correct placement, % (n/N) | 97.6 (200/205) | 88.0 (168/191); P = 0.001 | 93.9 (92/98) | 97.6 (123/126); P = 0.171 | 89.1 (49/55) | 100 (42/42); P = NS | 98.6 (868/880) | 97.1 (434/447); P = 0.05 | 81.2 (26/32) | 100 (52/52); P = 0.004 |
Malposition, % (n/N) | 2.4 (5/205) | 12.0 (23/191); P = 0.001 | 4.1 (4/98) | 1.6 (2/126); P = 0.505 | 7.3 (4/55) | 0.0; P = 0.127 | — | — | 18.8 (6/32) | 0.0 (0/52); P = 0.005 |
Technical failure, % (n/N) | — | — | 2.0 (2/98) | 0.8 (1/126); P > 0.999 | 3.6 (2/55) | 0.0; P = 0.504 | — | — | — | — |
Median procedure time (range), min | — | — | — | — | 10 (3 to 43) | 30 (15 to 55); P < 0.001 | — | — | 20 (15 to 40) | 15 (14 to 24); P = 0.236 |
CVC = central venous catheter; NS = not statistically significant; PICC = peripherally inserted venous catheter; US = ultrasound.
Note that this appendix has not been copy-edited.
Table 7: Summary of Findings by Outcome — Complications
Outcomes | Galante et al. (2022)14 | Cho (2021)15 | Choi et al. (2021)16 | Kwon et al. (2020)17 | Kim et al. (2019)18 | |||||
|---|---|---|---|---|---|---|---|---|---|---|
US-guided CVC | Traditional CVC | US-guided PICC | Fluoroscopic-guided PICC | US-guided PICC | Fluoroscopic-guided PICC | US-guided PICC | Blind-inserted PICC | US-guided PICC | Fluoroscopic-guided PICC | |
Pneumothorax, % (n/N) | 1.5 (3/205) | 2.1 (4/191); P > 0.05 | — | — | — | — | — | — | 0.0 (0/32) | 0.0 (0/52) |
Insertion site bleeding, % (n/N) | — | — | 5.1 (5/98) | 6.3 (8/126); P = 0.779 | — | — | — | — | 0.0 (0/32) | 0.0 (0/52) |
Thrombosis | — | — | 1.0 (1/98) | 1.6 (2/126); P = 0.714 | — | — | — | — | — | — |
Insertion site infection, % (n/N) | — | — | 2.0 (2/98) | 0.8 (1/126); P = 0.582 | — | — | — | — | — | — |
Systemic infection, % (n/N) | — | — | 2.0 (2/98) | 3.2 (4/126); P = 0.698 | — | — | — | — | — | — |
CVC = central venous catheter; PICC = peripherally inserted venous catheter; US = ultrasound.
Note that this appendix has not been copy-edited.
Table 8: Summary of Findings by Outcome — Other Outcomes
Outcomes | Galante et al. (2022)14 | Cho (2021)15 | Choi et al. (2021)16 | Kwon et al. (2020)17 | Kim et al. (2019)18 | |||||
|---|---|---|---|---|---|---|---|---|---|---|
US-guided CVC | Traditional CVC | US-guided PICC | Fluoroscopic-guided PICC | US-guided PICC | Fluoroscopic-guided PICC | US-guided PICC | Blind-inserted PICC | US-guided PICC | Fluoroscopic-guided PICC | |
ICU mortality, % (n/N) | — | — | 44.9% (44/98) | 20.6% (26/126); P < 0.001 | 0.0 (0/55) | 4.8% (2/42); P = 0.185 | — | — | 12.5 (4/32) | 0.0 (0/52); P < 0.001 |
Median length of ICU stay (range), days | — | — | — | — | 32 (3 to 102) | 36 (7 to 289); P = 0.284 | — | — | 24 (16 to 41) | 15 (6 to 29); P = 0.003 |
Median insertion duration (range), days | — | — | 26 (10 to 35) | 20 (15 to 30); P = 0.597 | 18 (3 to 93) | 27 (8 to 74); P = 0.002 | — | — | 20 (10 to 35) | 28 (16 to 34); P = NR |
CVC = central venous catheter; PICC = peripherally inserted venous catheter; US = ultrasound.
Note that this appendix has not been copy-edited.
Table 9: Summary of Recommendations in the Included Guidelines
Recommendations and supporting evidence | Quality of evidence and strength of recommendations |
|---|---|
ESA, Lamperti et al. (2020)19 | |
Should ultrasound guidance be used during cannulation of the internal jugular vein for central venous line placement in adults? | |
“We recommend the use of ultrasound guidance for IJV cannulation in adults, as it is safer in terms of a reduction in overall complications, it improves both overall and first-time success, and it reduces the time to successful puncture and cannulation of the vein (1B).” (p. 345) | Quality of evidence: Moderate Strength of recommendation: Strong |
“In terms of safety and efficacy, the use of an out-of-plane approach is similar to the in-plane approach when ultrasound guidance is used for IJV cannulation (2A).” (p. 345) | Quality of evidence: High Strength of recommendation: Weak |
Supporting evidence: Evidence was generally weak, with RCTs having high degree of heterogeneity due to different patient populations, settings and operators performing the procedures. | — |
Should ultrasound guidance be used during cannulation of the subclavian vein for central venous line placement in adults? | |
“We recommend the use of ultrasound guidance for subclavian vein cannulation in adult patients, as it is safer, and it reduces the incidence of both failures and of overall complications when compared with the landmark technique (1C).” (p. 345) Supporting evidence: Evidence was generally weak data from clinically heterogeneous RCTs with some methodological problems. | Quality of evidence: Low Strength of recommendation: Strong |
Should ultrasound guidance be used for cannulation of the axillary vein for central venous line placement in adults? | |
“We recommend the use of ultrasound guidance during axillary vein cannulation, as it reduces the risk of major complications and increases the rate of first time success when compared with the landmark technique (2C).” (p. 345) Supporting evidence: Evidence was generally weak, with data from only a few, small, clinically heterogeneous RCTs. | Quality of evidence: Low Strength of recommendation: Weak |
Should ultrasound guidance be used during cannulation of the femoral vein, or other veins in the groin, for venous line placement in adults? | |
“We recommend the use of ultrasound guidance for cannulation of the femoral vein (or other veins in the groin) in adults, as it is safer, it reduces the incidence of major complications, it improves the success rate and it reduces the time to successful cannulation (1C).” (p. 345) | Quality of evidence: Low Strength of recommendation: Strong |
“We also recommend the use of ultrasound guidance for cannulation of the femoral vein (or other veins in the groin) in adults, as it may indirectly decrease infectious and thrombotic complications by reducing the likelihood of some risk factors (e.g., haematoma) related to the puncture (1C).” (p. 345) | Quality of evidence: Low Strength of recommendation: Strong |
“We suggest considering ultrasound-guided puncture of the superficial femoral vein at the mid-thigh to enable an exit site in a safe area, reducing the risk of infection and thrombosis (2C).” (p. 346) | Quality of evidence: Low Strength of recommendation: Weak |
“We recommend an out-of-plane puncture of the femoral vein using a short axis view. A short axis view allows a panoramic view of arteries and nerves and so helps to avoid inadvertent damage to these structures (1C).” (p. 346) | Quality of evidence: Low Strength of recommendation: Strong |
Supporting evidence: Evidence was weak, with data from only small RCTs and cohort studies with high heterogeneity and some methodological problems. | — |
Should ultrasound guidance be used for cannulation of any peripheral vein in adults during elective or emergency procedures? | |
“We recommend adopting and applying a tool for the assessment of difficult peripheral venous access in order to best identify those patients who may benefit from ultrasound-guided peripheral vein cannulation (1C).” (p. 346) | Quality of evidence: Low Strength of recommendation: Strong |
“We recommend the use of ultrasound guidance for peripheral vein cannulation in adults with moderate to difficult venous access, both in emergency and elective situations, as it is safer and more effective in terms of reduction of complications and improved overall success rate and reduced time to achieve vascular access (1C).” (p. 346) | Quality of evidence: Low Strength of recommendation: Strong |
“We recommend the use of ultrasound before peripheral vein cannulation in order to evaluate the location of the vein as well as its diameter and depth. This will enable the choice of the most appropriate length and diameter of peripheral vascular access device and the safest puncture site, so as to reduce risks of accidental dislodgment and extravasation, phlebitis and thrombus formation (1C).” (p. 346) | Quality of evidence: Low Strength of recommendation: Strong |
“We recommend routine use of ultrasound for peripherally inserted central catheter placement, taking care that the exit site is located at mid-arm level (1C).” (p. 346) | Quality of evidence: Low Strength of recommendation: Strong |
Supporting evidence: Evidence was weak, with data from only small RCTs and prospective cohort studies with high heterogeneity. | — |
Should ultrasound guidance be used for cannulation of any central vein for long-term vascular access device placement in adults? | |
“We recommend ultrasound guidance for placement of long-term vascular access devices, as it has been shown to significantly reduce early mechanical complications (arterial puncture, hematoma, pneumothorax, haemothorax) (1C).” (p. 346) | Quality of evidence: Low Strength of recommendation: Strong |
“We recommend ultrasound guidance for placement of long-term vascular access devices, as it has been shown to be cost-effective by indirectly reducing complications such as catheter-related thrombosis and catheter-related infections (1C).” (p. 346) | Quality of evidence: Low Strength of recommendation: Strong |
“We recommend ultrasound-guided puncture of the axillary vein at the thorax for long-term vascular access device placement, as it has been shown to reduce the risk of pinch-off syndrome (1C).” (p. 346) | Quality of evidence: Low Strength of recommendation: Strong |
“We recommend ultrasound for catheter tip location and tip navigation to avoid primary malposition (1C).” (p. 346) | Quality of evidence: Low Strength of recommendation: Strong |
“We recommend preprocedural sonographic evaluation of all possible venous option for long-term vascular access device placement to plan and choose the safest approach (1C).” (p. 346) | Quality of evidence: Low Strength of recommendation: Strong |
“We recommend ultrasound for timely diagnosis of all potentially life-threatening complications (pneumothorax, haemothorax, cardiac tamponade and so on) after central venepuncture, as it has been shown to be more accurate and faster than a chest radiograph (1B).” (p. 346) | Quality of evidence: Moderate Strength of recommendation: Strong |
Supporting evidence: Evidence was weak, with data from only small RCTs with high heterogeneity. | — |
Should ultrasound guidance be used during cannulation of the IJV for central venous line placement in children? | |
“We recommend the use of ultrasound-guided cannulation for IJV cannulation in children, as it increases the success rate, reduces the time to successful cannulation and incidence of complications (1B).” (p. 347) Supporting evidence: Evidence was weak, with data from relatively few small RCTs and prospective cohort studies with high heterogeneity. | Quality of evidence: Moderate Strength of recommendation: Strong |
Should ultrasound guidance be used during cannulation of the brachiocephalic vein for central venous line placement in children? | |
“We recommend ultrasound guidance for brachiocephalic vein cannulation only when used by experts (1C).” (p. 347) Supporting evidence: Evidence was weak, with data relatively few small prospective cohort studies that have a high degree of heterogeneity and some methodological problems. | Quality of evidence: Low Strength of recommendation: Strong |
Should ultrasound guidance be used during cannulation of the femoral vein for central venous line placement in children? | |
“We recommend the use of ultrasound guidance for femoral vein cannulation in children, as it increases the success rate, with a tendency to reduce the risk of complications, without reducing the time of successful cannulation (1C).” (p. 347) Supporting evidence: Evidence was weak, with data relatively few RCTs that have a high degree of heterogeneity. | Quality of evidence: Low Strength of recommendation: Strong |
Should ultrasound guidance be used during cannulation of peripheral veins for venous line placement in children? | |
“Due to the paucity of well conducted studies, we cannot recommend the routine use of ultrasound guidance for peripheral vein cannulation in paediatric patients. Some evidence suggests that the use of ultrasound by an experienced operator improves the success rate of difficult peripheral vein cannulation in children; in these circumstances, it may be of some benefit (2B).” (p. 347) Supporting evidence: Paucity of evidence (1 RCT). | Quality of evidence: Moderate Strength of recommendation: Weak |
ESPNIC, Singh et al. (2020)20 | |
“POCUS-guided technique should be used for internal jugular vein (IJV) line placement in neonates and children.” (p. 8) Supporting evidence: Five studies including nonrandomized studies, RCTs, and meta-analysis provided evidence in favour of US guidance for IJV cannulation compared to landmark technique. Five studies observational studies, systematic review and meta-analysis have shown high success rates on first attempt, and decreased incidence of complications of US-guided technique. | Quality of evidence: A Strength of recommendation: Strong agreement |
“POCUS-guided technique is helpful for subclavian venous line placement in neonates and children.” (p. 8) Supporting evidence: Seven studies including a systematic review, meta-analysis, RCT and observational studies showed that ultrasound-guided subclavian cannulation in neonates and children is safe, doable and is advised over a blind cannulation technique. | Quality of evidence: B Strength of recommendation: Strong agreement |
“POCUS-guided technique is helpful for femoral line placement in neonates and children.” (p. 8) Supporting evidence: Two RCTs and 2 systematic reviews showed higher overall success rate and on the first attempt of US-guided femoral line placement compared with landmark technique in pediatric patients. | Quality of evidence: B Strength of recommendation: Strong agreement |
“POCUS-guided technique is helpful for peripherally inserted central catheters (PICC) in children.” (p. 8) Supporting evidence: An RCT comparing US-guided vs. landmark PICC placement showed higher first attempt cannulation rate, successful PICC positioning rate and shorter time to success. | Quality of evidence: B Strength of recommendation: Agreement |
SHM, Franco-Sadud et al. (2019)21 | |
“We recommend that providers should use real-time ultrasound guidance for internal jugular vein catheterization, which reduces the risk of mechanical and infectious complications, the number of needle passes, and time to cannulation and increases overall procedure success rates.” (p. E10) Supporting evidence: Evidence from a meta-analysis, a systematic review, and observational studies have shown that real-time US guidance for IJV CVC insertion had better outcomes compared to a landmark-based approach in adults. US-guided insertion reduced the risk of procedure-related mechanical and infectious complications, and improves first-pass and overall success rates in diverse care settings. | Degree of consensus: Very good Strength of recommendation: Strong |
“We recommend that providers who routinely insert subclavian vein CVCs should use real-time ultrasound guidance, which has been shown to reduce the risk of mechanical complications and number of needle passes and increase overall procedure success rates compared with landmark-based techniques.” (p. E10 to 11) Supporting evidence: Evidence from systematic review, RCTs, and observational studies showed that subclavian vein CVC insertion is feasible and safe. | Degree of consensus: Very good Strength of recommendation: Strong |
“We recommend that providers should use real-time ultrasound guidance for femoral venous access, which has been shown to reduce the risk of arterial punctures and total procedure time and increase overall procedure success rates.” (p. E11) Supporting evidence: Evidence from systematic review of RCTs and other observational studies showed that US guidance for femoral vein CVC insertion reduced arterial punctures, reduced total procedural time, and increased procedure success rates compared to a landmark-based approach. | Degree of consensus: Very good Strength of recommendation: Strong |
“We recommend that providers should use real-time ultrasound guidance for the insertion of peripherally inserted central catheters (PICCs), which is associated with higher procedure success rates and may be more cost effective compared with landmark-based techniques.” (p. E11) Supporting evidence: Evidence from several studies including RCTs and observational studies demonstrated that providers who use ultrasound guidance vs landmarks for PICC insertion have higher procedural success rates, lower complication rates, and lower total placement costs. | Degree of consensus: Very good Strength of recommendation: Strong |
CVC = central venous catheter; IJV = internal jugular vein; PICC = peripherally inserted central catheter; POCUS = point-of-care ultrasound; RCT = randomized controlled trial; US = ultrasound.
Note that this appendix has not been copy-edited.
Contributors: Elizabeth Carson, Shannon Hill
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for noncommercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca