CADTH Health Technology Review
IV Acetaminophen for Acute Pain in Emergency Departments
Rapid Review
Authors: Kendra Brett, Melissa Severn
Abbreviations
ED
emergency department
GRADE
grading of recommendations, assessment, development, and evaluation
NSAID
nonsteroidal anti-inflammatory drug
RCT
randomized controlled trial
SR
systematic review
VAS
visual analogue scale
Key Messages
For adults with moderate to severe pain in the emergency department (ED), IV acetaminophen may offer similar levels of pain relief and a similar risk of adverse events as oral acetaminophen or IV nonsteroidal anti-inflammatory drugs (NSAIDs).
For adults with moderate to severe pain in the ED, IV acetaminophen may offer a similar or modestly lower level of pain relief, and a lower risk of adverse events, when compared to IV opioids.
We did not find any studies on the cost-effectiveness of IV acetaminophen compared to oral acetaminophen, IV NSAIDs, or IV opioids for treating patients with moderate to severe pain in the ED that met our inclusion criteria.
One guideline recommends IV NSAIDs for the initial management of moderate to severe pain for patients in the ED. IV acetaminophen is recommended instead of IV opioids alone.
Context and Policy Issues
Acute Pain in the Emergency Department
Pain is 1 of the most common reasons patients use the emergency department (ED). In Canada, pain occurring in the abdomen, pelvis, throat, chest, or back were some of the most frequent reasons for patients to use the ED in 2022 to 2023.1 Unfortunately, not all patients report receiving adequate pain relief in the ED. In a 2007 study from Canada and the US, 40% of patients presenting to the ED with severe acute pain did not receive analgesics, and over 70% of patients were discharged while still experiencing moderate to severe pain.2
For patients experiencing pain due to trauma, adequate pain management can improve patient comfort, reduce the stress response, and potentially reduce the risk of acute pain developing into chronic pain.3 Failure to provide adequate treatment for patients experiencing acute pain in the ED has the potential to decrease patient comfort, impact length of stay in the hospital, impair quality of life, increase the risk of complications, or delay returning work.4
What Is the Current Practice?
Pain management aims to achieve a level of pain that the patient finds tolerable and allows them to function.4 For the management of moderate to severe acute pain in the ED, drugs should be effective, easy to administer, and have limited side effects.4 These drugs include acetaminophen, nonsteroidal anti-inflammatory drugs (NSAIDs) (e.g., ibuprofen), and opioids, which may be administered using different routes (e.g., oral, IV, intramuscular).4 As of 2019, oxycodone and hydromorphone were the most commonly prescribed opioids for moderate to severe pain in Canada.5 Opioids can be associated with adverse effects, including high blood pressure, changes in mental status (e.g., delirium), itchiness, nausea, and vomiting,6 and the misuse of opioids can lead to opioid use disorder.7 NSAIDs can also be associated with adverse effects, such as gastrointestinal effects (e.g., peptic ulcer), high blood pressure, or a risk of bleeding.8
What Is IV Acetaminophen and How Might It Benefit Patients?
Acetaminophen is a drug that provides pain relief and reduces fever; it can be administered orally, rectally, or intravenously.9 Acetaminophen injection is a sterile solution administered through IV infusion (herein called IV acetaminophen). It is indicated for the short-term management and treatment of mild to moderate pain, moderate to severe pain with adjunctive opioid analgesics, and fever.10 It is approved by Health Canada for use in patients 2 years of age or older.10 According to the product monograph, the most common adverse events from IV acetaminophen include nausea, vomiting, headache, and constipation, which are predominantly mild to moderate in severity.10 Assuming IV acetaminophen provides comparable pain relief and safety profile compared to IV opioids or IV NSAIDs, it has the potential to be an alternative analgesic drug in the ED for patients with moderate to severe pain.
The IV route for acetaminophen has been proposed as an alternative to oral acetaminophen due to the potential that it may provide more rapid and more predictable acetaminophen analgesia.11 IV acetaminophen could also be an alternative for patients who cannot take oral medications. However, the cost of IV acetaminophen is often substantially higher for pediatric and adult patients when compared to oral (tablet or liquid) or rectal formulations of acetaminophen.12,13 Thus it is important to evaluate both the clinical effectiveness and the cost-effectiveness of IV acetaminophen.
Objective
To support decision-making about the use of IV acetaminophen in the ED, this Rapid Review summarizes and critically appraises the available clinical and cost-effectiveness studies and evidence-based guidelines on the use of IV acetaminophen use for patients experiencing moderate to severe pain in the ED.
Research Questions
What is the clinical effectiveness of IV acetaminophen use for patients experiencing moderate to severe pain in the ED setting?
What is the cost-effectiveness of IV acetaminophen use for patients experiencing moderate to severe pain in the ED setting?
What are the evidence-based guidelines regarding IV acetaminophen use for patients experiencing moderate to severe pain in the ED setting?
Methods
Literature Search Methods
An information specialist conducted a literature search on key resources including MEDLINE, Embase, the Cochrane Database of Systematic Reviews, the International HTA Database, and the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search approach was customized to retrieve a limited set of results, balancing comprehensiveness with relevancy. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. Search concepts were developed based on the elements of the research questions and selection criteria. The main search concepts were IV acetaminophen and ED settings. The search was completed on August 24, 2023, and limited to English-language documents.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
|---|---|
Population | Patients (all ages) presenting to ED with moderate to severe acute pain |
Intervention | IV APAP (any dose) |
Comparator | Q1 and Q2: IV opioids, IV NSAIDs, oral APAP, no treatment or placebo Q3: Not applicable |
Outcomes | Q1: Clinical benefits (e.g., pain relief, length of stay in ED, rate of rescue analgesia, first-line use versus second-line use) and harms (e.g., rate of adverse events) Q2: Cost-effectiveness (e.g., cost per QALY gained, ICER) Q3: Recommendations regarding the appropriate use of IV APAP in ED settings (e.g., pain severity, appropriate patient populations, dosage recommendations, pre-ED APAP use) |
Study designs | Health technology assessments, systematic reviews, randomized controlled trials, nonrandomized studies, economic evaluations, evidence-based guidelines |
APAP = acetaminophen; ED = emergency department; ICER = incremental cost-effectiveness ratio; NSAID = nonsteroidal anti-inflammatory drug; QALY = quality-adjusted life-year.
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1 or they were duplicate publications. Studies were excluded if they evaluated concurrent IV acetaminophen and opioid. We excluded systematic reviews (SRs) in which all relevant studies were captured in other more recent or more comprehensive SRs and primary studies retrieved by the search if they were captured in 1 or more included SRs. If an SR did not provide sufficient detail about the findings in the relevant primary studies, we excluded the SR and included the relevant primary studies. Guidelines with an unclear methodology were also excluded.
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the following tools as a guide: A MeaSurement Tool to Assess systematic Reviews 2 (AMSTAR 2)14 for SRs, the Downs and Black checklist15 for randomized studies, and the Appraisal of Guidelines for Research and Evaluation (AGREE) II instrument16 for guidelines. Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Summary of Evidence
Quantity of Research Available
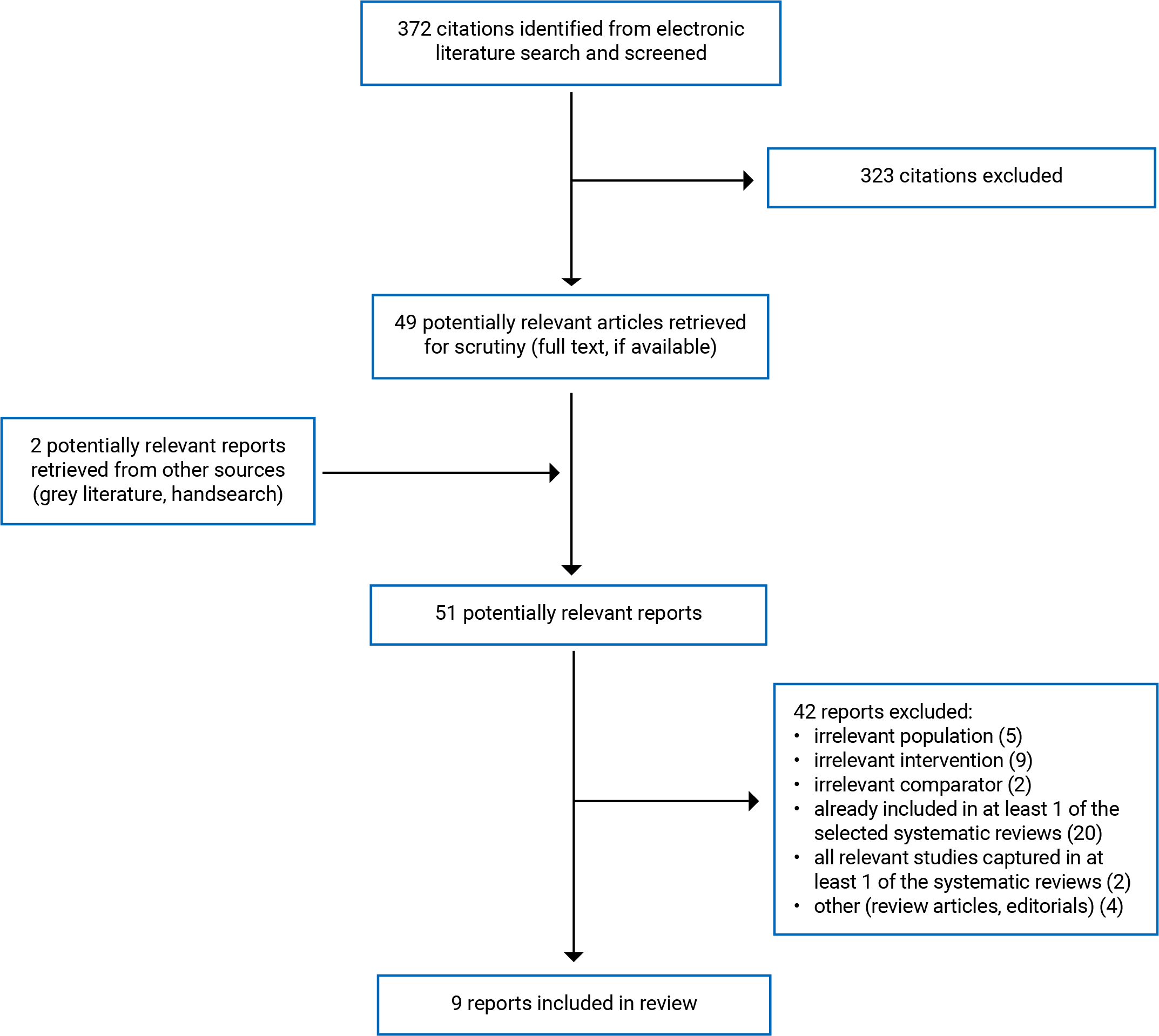
This report includes 3 SRs,11,17-19 5 randomized controlled trials (RCTs),20-24 and 1 evidence-based guideline.25 Study selection details are presented in Appendix 1. Additional references of potential interest are provided in Appendix 6.
One additional SR (Sin et al.19) was identified. This SR searched the literature until July 2015 and included studies that compared IV acetaminophen to IV opioids, IV NSAIDS, or placebo in patients of any age in the ED with moderate to severe acute pain.19 It included 9 relevant RCTs, of which 8 RCTs overlapped with the SR by Quereshi et al.17 The remaining relevant RCT was not reported with sufficient detail in the SR by Sin et al.;19 thus, the primary study (Oguzturk et al.)24 was included instead of the SR.
Summary of Study Characteristics
Detailed characteristics of the included publications are provided in Appendix 2. Two of the SRs17,18 included overlapping primary studies, with 10 out of the 11 studies in the 2019 SR18 included in the more comprehensive 2023 SR17 (refer to Appendix 5 for details regarding overlap). To avoid duplication of results, information from individual primary studies is only reported once.
Included Studies for Question 1: Clinical Effectiveness
We identified 3 SRs11,17-19 and 5 RCTs20-24 to address this research question, comparing IV acetaminophen with oral acetaminophen,11,16,20 IV NSAIDS,17,22 IV opioids,17,18,21,23,24 and placebo.24
IV Acetaminophen Compared to Oral Acetaminophen
One SR11 had broader inclusion criteria than the present review. Specifically, this SR searched for studies in children younger than 18 years with pain or fever in any setting, and assessed clinical effectiveness, pharmacokinetics, and cost of IV acetaminophen. It included studies published up to October 2019; however, none of the included studies were relevant to this report (i.e., none of the studies evaluated the clinical effectiveness of IV acetaminophen compared with oral acetaminophen for moderate to severe pain in the ED setting).
One RCT20 included 180 adults in the ED with moderate to severe pain due to a femur fracture and compared 1,000 mg of IV acetaminophen to 1,000 mg of oral acetaminophen. Patients were followed for 4 hours, and the outcomes included pain, the requirement for rescue analgesia, and adverse events.
IV Acetaminophen Compared to IV NSAIDs
One SR with meta-analysis17 searched for studies in adults attending the ED with acute pain published up until May 2022, and identified 12 RCTs with relevant comparisons between IV acetaminophen and IV NSAIDs. The scope of this SR was broader than that of this report in terms of the level of pain (i.e., they did not limit the patients to those with moderate to severe pain) and comparators (i.e., they also included intramuscular NSAIDs). While all the patients in the IV NSAIDs RCTs had moderate to severe pain at baseline, some of the relevant meta-analyses combined studies that used intramuscular NSAIDs with studies that used IV NSAIDs as the comparator.
One RCT22 included 210 adults with acute low back pain in the ED with pain severity that was moderate or higher. Patients were treated with 1,000 mg IV acetaminophen, 50 mg IV dexketoprofen, or 400 mg IV ibuprofen and followed for 60 minutes.
Relevant outcomes for the SR and the RCT were pain, the need for rescue analgesia, and adverse events.17,22
Another SR18 searched for studies in adults and pediatric patients with acute moderate to severe pain published through May 2019. It did not identify any unique primary studies comparing IV acetaminophen with IV NSAIDs; thus, this SR did not contribute any findings to this comparison.
IV Acetaminophen Compared to IV Opioids
Two SRs17,18 included RCTs that compared IV acetaminophen to IV opioids. The SR with meta-analysis by Qureshi et al.17 included 18 RCTs in adults with acute pain in the ED with relevant comparisons between IV acetaminophen and IV opioids. As the population of interest to this SR was broader than the current review in terms of pain severity, in the meta-analysis there is 1 RCT for which the baseline pain is unclear and another RCT in which the mean pain for patients who received IV acetaminophen was mild whereas the mean pain for the patients who received the opioids was moderate. The SR by Sobieraj et al.18 identified 10 RCTs relevant to this report, 9 of which were also included in the Qureshi et al. SR.17 The remaining RCT in the Sobieraj et al. SR included 55 people aged 15 to 60 (mean age of 35 years) and patients received either 1,000 mg IV acetaminophen or 0.1 mg/kg IV morphine.
Three RCTs21,23,24 compared IV acetaminophen to IV opioids with moderate to severe pain in the ED. The RCTs included 162 adults 65 years or older,21 220 adults between 21 and 64 years,23 and 140 patients 17 years or older.24 Two of the RCTs used 1,000 mg IV acetaminophen compared to IV hydromorphone (0.5 mg21 or 1 mg23) and the other RCT compared 15 mg/kg IV acetaminophen against 1 mg/kg IV tramadol.24
Relevant outcomes for the SRs and the RCTs were pain,17,18,21,23,24 the need for rescue analgesia,17,21,23 and adverse events.17,18,21,23,24
IV Acetaminophen Compared to Placebo
One of the included RCTs24 also included a comparison between 15 mg/kg IV acetaminophen and placebo in patients 17 years or older with severe abdominal pain in the ED. This study included 70 patients per group (mean age 32), followed patients for 40 minutes, and assessed pain and adverse events.
Included Studies for Question 2: Cost-Effectiveness
No relevant studies were identified for question 2; therefore, no summary can be provided.
Included Studies for Question 3: Evidence-Based Guidelines
One evidence-based guideline25 provided recommendations regarding the use of IV acetaminophen in the ED setting. This 2023 guideline was developed by a technical expert panel of emergency medicine clinicians in the US to provide guidance for the use of analgesics for treating patients with moderate to severe pain in the ED. The guideline followed the Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) framework to develop the recommendations26 using evidence identified in a 2019 SR,18 which is also included in this report. The GRADE framework was also used to rate the strength of the evidence (from very low to high quality) and to classify the strength of the recommendations (strong or conditional).
Summary of Critical Appraisal
Critical appraisal summaries are organized by research question, comparison (where appropriate), and study design. For the SR that did not contain any relevant primary studies, only the relevant items from the AMSTAR 2 tool were assessed.
Additional details regarding the strengths and limitations of the included publications are provided in Appendix 3.
Clinical Effectiveness Studies
Studies Comparing IV Acetaminophen to Oral Acetaminophen
The SR on IV acetaminophen in pediatric patients11 clearly stated the population, intervention, comparator, and outcomes of interest and registered its protocol a priori, thus reducing the risk of reporting bias. Although no primary studies relevant to the current Rapid Review were identified, the authors of this SR used a comprehensive search strategy (i.e., searched 5 databases, provided the full search strategy, and searched references lists of relevant publications) and study selection was performed in duplicate, reducing the likelihood that relevant literature was missed. However, the authors did not justify why they restricted the studies to those published in English, thus it is unknown whether relevant studies in other languages were missed.
Strengths of the RCT by Francheschi et al.20 included a good description of the aim, the outcomes, and the interventions; reporting simple outcomes data and actual P values; and appropriate statistical tests were used to compare the main outcomes. The patients were described with limited detail, with baseline pain only reported in a figure, thus making the variation in baseline pain between groups difficult to determine. In addition, confidence intervals were not reported for the main outcomes, thus limiting the certainty in these findings. Insufficient details were reported regarding the methods of randomization and allocation concealment, and it is unclear whether the study is at risk of selection bias. In addition, it was unclear why the authors randomized the patients in a 5 to 1 ratio of IV versus oral acetaminophen, or whether the authors accounted for this ratio when they conducted the sample size calculation. Due to the nature of the interventions (i.e., IV versus oral acetaminophen), it was not possible to blind the patients to the intervention (which suggests a risk of performance bias), and it was not reported whether there was an attempt to blind the researchers assessing the main outcomes to the interventions (which could mean a potential risk of detection bias). The authors used a validated visual analogue scale (VAS) for pain but it was not reported whether the primary outcome (i.e., at least a 1 point reduction in VAS at 1 hour, on a 10-point scale) represents a minimally important difference (i.e., the smallest improvement considered worthwhile by a patient) in this specific population.
Studies Comparing IV Acetaminophen to IV NSAIDs
Two SRs17,18 were included that searched for studies comparing IV acetaminophen to IV NSAIDs. The SR by Sobieraj et al.18 did not contribute unique primary studies for this comparison to this review, thus the summary of the critical appraisal is in the Studies Comparing IV Acetaminophen to IV Opioids section.
The SR by Qureshi et al.17 clearly stated the population, intervention, comparator, and outcomes of interest and registered its protocol a priori, thus reducing the risk of reporting bias. A comprehensive search strategy was used and study selection and data extraction were performed in duplicate, thus reducing the likelihood that relevant studies were missed or that there were errors in data extraction. For the individual primary studies in the SR, baseline pain scores were not reported, but the populations were adequately described, and the interventions, comparators, and outcomes were well described. The authors used appropriate tools to assess the risk of bias of the included studies and to assess the quality of the evidence by outcome; however, they did not account for risk of bias in the meta-analysis, nor did they discuss the potential impact of the risk of bias or the quality of the evidence on the findings, and the potential impact is unclear. There is also considerable statistical heterogeneity in the meta-analyses, which the authors explored using subgroup analyses by type of pain and by specific NSAID (not reported in this Rapid Review). The reporting of the findings was unclear, with some discrepancies between the findings reported in the main publication and the appendices, which limits the certainty in the findings.
Strengths of the RCT by Dogan et al.22 include a good description of the aim of the study, the inclusion criteria, the outcomes, and the interventions, as well as reporting the patients’ baseline levels of pain, and simple outcomes data. The methods of randomization and allocation concealment were appropriate, which reduced the risk of selection bias. The patients, those administering the medications and those assessing the outcomes, were blinded to the interventions, reducing the risk of performance and detection bias. Limited information is reported about the patients (e.g., age is not reported and sex is not reported by group), and the statistical analysis did not adjust for any potential confounders (e.g., the difference in baseline pain between the groups) thus reducing our understanding of the potential impact of confounding factors. It was unclear whether any patients were lost to follow-up as the reporting of the number of people randomized to each intervention group was unclear, with the text and the patient flow diagram reporting different numbers. The authors used a validated VAS for pain to assess pain, but they did not specify what was considered a minimally important improvement in pain for this population, thus limiting the understanding of the clinical implications of the findings.
Studies Comparing IV Acetaminophen to IV Opioids
Two SRs17,18 were included that searched for studies comparing IV acetaminophen to IV opioids. The summary of the critical appraisal of the SR by Qureshi et al.17 is in the Studies Comparing IV Acetaminophen to IV NSAIDs section.
The SR by Sobieraj et al.18 clearly stated the population, intervention, comparator, and outcomes of interest and registered its protocol a priori, thus reducing the risk of reporting bias. A comprehensive search strategy was used and study selection was performed in duplicate, thus reducing the likelihood that relevant studies were missed. Data extraction was performed by 1 reviewer and verified by a second reviewer, thus limiting the possibility of errors in data extraction. The included studies were well described in terms of population, interventions, comparators, and outcomes; an appropriate tool was used to assess the risk of bias of the included studies; and the authors considered the certainty of the evidence when interpreting the findings.
Three RCTs21,23,24 were included that compared IV acetaminophen to IV opioids. The aim of study, the interventions, and the eligibility criteria for patients were well described in all 3 RCTs. Across the RCTs, there were minimal or no losses to follow-up and the methods of randomization and allocation concealment were sufficient to reduce the risk of selection bias. The patients and those administering the medications were blinded in all 3 RCTs (reducing the risk of performance bias) and in 1 RCT23 those assessing the outcomes were also blinded to the intervention (reducing the risk of detection bias). In 2 RCTs21,23 the main outcomes are well described and well reported, including simple outcome data, mean differences between groups, and 95% confidence intervals. In the RCT by Oguzturk et al.,24 the authors reported P values and the median plus the range of the VAS scores at various time points, but did not report confidence intervals, nor the mean difference between time points by intervention groups, nor did they compare the change in pain score between groups, thus limiting the interpretation of the findings. Furthermore, this RCT24 did not specify what was considered a minimally important improvement in pain for this population, and it is unclear whether appropriate statistical tests were used to assess the main outcomes (e.g., t tests used to assess differences between 3 groups for some outcomes), which further limits the interpretation of this study’s findings. In the other 2 RCTs21,23 the authors specified the minimally important improvement in pain and the results focused on whether the interventions achieved this improvement in pain.
Studies Comparing IV Acetaminophen to Placebo
One RCT by Oguzturk et al.24 included a comparison between IV acetaminophen and placebo. This study also included a comparison between IV acetaminophen and opioids, and the summary of the critical appraisal is in the Studies Comparing IV Acetaminophen to IV Opioids section.
Guidelines
The guideline25 had a clear objective, described the population and target users of the guideline, and reported the health questions covered by the guideline. The recommendations were specific and easily identifiable. The names, affiliations, and areas of expertise were provided for the guideline development group members, who were from relevant professional groups. Systematic methods were used to identify the evidence informing the recommendations (published in a separate SR18). The methods used to synthesize the evidence and to develop the recommendations were clearly described in the companion methods paper,26 and the guideline development group considered the health benefits and side effects, as well as certainty of evidence, values, resources required, cost-effectiveness, equity, acceptability, and feasibility when formulating the recommendations. The authors provide a summary of the evidence that supports each recommendation, and there is a clear link between the recommendations and supporting evidence. However, while the main guideline publication indicates that the companion paper includes the summary of findings tables and the evidence-to-decision tables, no supplementary files or appendices were found for the companion paper, thus we were unable to review these evidence tables. It was not reported whether the recommendations were externally validated by experts; however, it is likely that the guideline underwent peer review before its publication. Fourteen authors declared no conflicts of interest and 1 author declared receiving an honorarium for their work on the project. The source of funding was declared, and an explicit statement was made that the authors had editorial independence from the funding organizations.
Summary of Findings
Appendix 4 presents the main study findings.
There was some overlap in the primary studies included in the SRs17,18 (refer to Appendix 5); therefore, to avoid duplication of results, outcomes data from individual primary studies are only reported once.
Clinical Effectiveness of IV Acetaminophen Versus Oral Acetaminophen
One RCT20 was identified that examined the clinical effectiveness of IV acetaminophen compared to oral acetaminophen.
Pain
In adults in the ED with moderate to severe pain due to a femur fracture, IV acetaminophen reduced pain in a significantly greater proportion of patients at 1 hour compared to oral acetaminophen, but there was no difference in pain relief between the groups at 4 hours.20
Rescue Analgesia
A greater proportion of adults who received IV acetaminophen required rescue therapy at 4 hours compared to those who received oral acetaminophen (17.5% and 3.7%, respectively), but the difference was not statistically significant.20
Adverse Events
No adverse events were reported within 4 hours of adults receiving IV acetaminophen or oral acetaminophen.20
Clinical Effectiveness of IV Acetaminophen Versus IV NSAIDs
One SR17 and 1 RCT22 were identified that examined the clinical effectiveness of IV acetaminophen compared to IV NSAIDs. Within the SR,17 the authors assessed the evidence to be low quality for pain, the need for rescue analgesia, and adverse events.
Pain
One SR with meta-analysis17 compared the analgesic effects of IV acetaminophen to NSAIDs (either IV or intramuscular administration) in adults with moderate to severe pain. This study reported:
no difference in mean pain reduction at 30 minutes (meta-analysis of 14 RCTs, NSAIDs via IV in 12 RCTs, and intramuscular in 2 RCTs)
a greater reduction in pain at 60 minutes favouring NSAIDs (statistically significant but not a difference that is considered clinically important to patients; meta-analysis of 6 RCTs, NSAIDs via IV in 5 RCTs, and intramuscular in 1 RCT).
One RCT22 compared IV acetaminophen with 2 different IV NSAIDs (dexketoprofen and ibuprofen) in patients with acute low back pain and reported no differences in mean pain reduction between the 3 groups at 30 minutes or 60 minutes.
Rescue Analgesia
One SR with meta-analysis17 that compared IV acetaminophen to NSAIDs (either IV or intramuscular administration) in adults with moderate to severe pain reported the following:
more frequent need for rescue analgesia in those treated with IV acetaminophen at 30 minutes (statistically significant difference; meta-analysis of 8 RCTs, NSAIDs via IV in 7 RCTs, and intramuscular in 1 RCTs)
more frequent need for rescue analgesia in those treated with IV acetaminophen at 60 minutes (statistically significant difference; meta-analysis of 2 RCTs).
In patients with acute low back pain, 1 RCT reported that no patients required rescue analgesia after 60 minutes in either the IV acetaminophen group or the IV NSAID group (dexketoprofen or ibuprofen).22
Adverse Events
The SR17 found no statistically significant difference in adverse events from IV acetaminophen compared to IV NSAIDs (meta-analysis of 8 RCTs, NSAIDs via IV in 6 RCTs, and intramuscular in 2 RCTs). The RCT22 reported no adverse events in either group (IV acetaminophen or IV NSAIDs).
Clinical Effectiveness of IV Acetaminophen Versus IV Opioids
Two SRs17,18 and 3 RCTs21,23,24 were identified that examined the clinical effectiveness of IV acetaminophen compared to IV opioids. The authors of 1 SR17 assessed the evidence to be low quality for pain and the need for rescue analgesia, and moderate quality for adverse events.
Pain
In adults with moderate to severe pain in the ED, most of the identified evidence did not report significant differences in pain between IV acetaminophen and IV opioids. Specifically, 1 SR with meta-analysis found no evidence of a difference in pain reduction at 30 minutes, 60 minutes, or 120 minutes when IV acetaminophen was compared with IV opioids.17 One additional RCT also reported no difference in pain at 20 minutes or 40 minutes (results of statistical test not reported).24
Of the remaining identified evidence that addressed pain, 3 RCTs reported that IV opioids reduced pain statistically significantly more than IV acetaminophen at 30 minutes (1 RCT from 1 SR)18 or 60 minutes.21,23 However, the difference in pain reduction between the treatments was only clinically meaningful to patients in 1 RCT23 (the difference was not clinically meaningful in the RCT21 and not reported in the other RCT18).
Rescue Analgesia
When adults with moderate to severe pain in the ED were treated with IV acetaminophen compared with IV opioids, 3 studies found no difference in the requirement for rescue analgesia within 30 minutes (SR with meta-analysis)17 or within 60 minutes (2 RCTs).21,23 When patients were asked whether they would like additional analgesia at 60 minutes, a significantly higher proportion of patients in the IV opioid group declined additional analgesia (1 RCT).23
Adverse Events
In adults with moderate to severe pain in the ED, most of the identified evidence reported a safety benefit for IV acetaminophen compared with IV opioids. Specifically, 1 SR with meta-analysis found that those treated with IV acetaminophen had significantly fewer adverse events than those treated with IV opioids17 and 1 RCT reported significantly fewer cases of nausea and a nonsignificant trend toward fewer cases of vomiting in those treated with IV acetaminophen.23
Of the remaining evidence that addressed safety outcomes, 4 RCTs reported no statistically significant difference in adverse events,21 dizziness (1 RCT from 1 SR),18 nausea or vomiting,24 or pruritus.23
Clinical Effectiveness of IV Acetaminophen Versus With Placebo
One RCT24 was identified that examined the clinical effectiveness of IV acetaminophen compared to placebo.
Pain
Compared to those who received a placebo, patients with severe abdominal pain who received IV acetaminophen experienced a greater decrease in pain at 20 minutes and 40 minutes (statistically significant differences; 1 RCT).24
Adverse Events
In patients with severe abdominal pain, 18.6% of patients who received IV acetaminophen experienced nausea or vomiting after 40 minutes, and no patients who received the placebo experienced nausea or vomiting (1 RCT).24
Cost-Effectiveness of IV Acetaminophen
No relevant evidence was identified regarding the cost-effectiveness of IV acetaminophen use for patients experiencing moderate to severe pain in the ED setting; therefore, no summary can be provided.
Guidelines Regarding the Use of IV Acetaminophen
In the ED, for the initial management of moderate to severe pain, the following is recommended in 1 guideline:25
IV acetaminophen is suggested over IV opioids alone, if IV acetaminophen is available, affordable, and easy to administer (conditional recommendation, based on evidence with low certainty).
IV NSAIDs are suggested over IV acetaminophen (conditional recommendation, based on evidence with low certainty).
Limitations
Evidence Gaps
No evidence was found for the following; therefore, no conclusions can be formed on these research questions:
the clinical effectiveness of IV acetaminophen in pediatric patients
the cost-effectiveness of IV acetaminophen.
While we identified 1 SR11 that searched for studies specifically comparing IV acetaminophen to oral acetaminophen in pediatric patients, and another SR18 that searched for studies of IV acetaminophen compared to IV opioids or IV NSAIDS in people of any age, neither SR identified any relevant primary studies exclusively focused on pediatric patients. One relevant primary study in the Sobieraj et al. SR18 included patients between 15 and 60 years of age, but the mean age of the population was 35; thus, no conclusions can be drawn regarding pediatric patients from this study.
There was limited evidence for some comparisons, with 1 RCT20 comparing IV acetaminophen to oral acetaminophen and 1 RCT24 comparing IV acetaminophen to placebo, potentially limiting the reliability of these findings.
None of the studies reported length of stay in the ED as an outcome, thus no conclusions can be formed on the impact of IV acetaminophen on this outcome.
Generalizability
None of the included studies were conducted in Canada and the guideline25 was developed for the US, which may limit the generalizability of the findings of this Rapid Review to the Canadian health care context. One SR11 was conducted by authors from Canada, but this SR did not include any primary studies relevant to this report.
The specific opioids and NSAIDs used in the studies may also limit the generalizability of the findings to the Canadian health care context if the specific drugs or formulations are not available in Canada. For the IV opioid comparison, IV tramadol was the opioid used in 1 RCT24 and 2 of the studies in the SR by Qureshi et al.17 Health Canada only lists oral formulations of tramadol and does not list any IV formulations for tramadol on the Drug Product Database.27 For the IV NSAID comparison, IV dexketoprofen and IV ketorolac were used in 1 RCT22 and 8 of the studies in the SR by Qureshi et al.17 (6 RCTs used IV dexketoprofen and 2 RCTs used IV ketorolac). IV formulations of these specific NSAIDS are not listed on Health Canada’s Drug Product Database.27
Heterogeneity of the Evidence
There was considerable clinical heterogeneity in the evidence evaluating IV acetaminophen, as well significant statistical heterogeneity in the SR with meta-analysis.17 There was substantial heterogeneity in the indication causing the pain (e.g., fractures, low back pain, abdominal pain, migraine, dysmenorrhea, renal colic, pancreatis, nonspecific pain).17,18,20-24 In addition, while the majority of the studies included patients with moderate to severe pain, there were 2 primary studies within the SR with meta-analysis17 that included patients with low or unclear levels of pain.
In the SR with meta-analysis,17 the authors explored the statistical heterogeneity using subgroup analyses by type of and by specific NSAIDs, and results were generally consistent with the primary analyses showing no differences between groups. There was moderate to substantial statistical heterogeneity in the subgroup analyses by type of pain, and for back pain the reduction in pain was greater for IV opioids than for IV acetaminophen. However, there was no evidence of a difference for the other types of pain (i.e., renal colic, musculoskeletal injuries, abdominal pain, and headaches) when IV acetaminophen was compared to IV opioids or IV NSAIDS.17 In the subgroup analyses by type of NSAID, the reduction in pain was greater for IV ibuprofen than for IV acetaminophen, but there was no evidence of a difference for dexketoprofen or ketorolac.17
There was also heterogeneity in the dose of IV acetaminophen as well as the specific drugs and doses used as comparators. Six studies used a 1,000 mg dose of IV acetaminophen17,18,20-23 while 1 study used a dose of 15 mg/kg IV acetaminophen.24 The IV opioids included morphine, tramadol, fentanyl, and hydromorphone,17,18,21,23,24 and the IV NSAIDs included ibuprofen, dexketoprofen, and ketorolac.17,22 In addition, some of the meta-analyses in the SR combined studies that used intramuscular NSAIDs with studies that used IV NSAIDs as the comparator;17 thus, conclusions cannot be made about IV NSAIDs alone.
Conclusions and Implications for Decision- or Policy-Making
This report comprises 3 SRs11,17-19 and 5 RCTs20-24 regarding the clinical effectiveness of IV acetaminophen and 1 evidence-based guideline25 regarding the use of IV acetaminophen for patients experiencing moderate to severe pain in the ED. No relevant evidence was identified regarding the cost-effectiveness of IV acetaminophen in this population.
Different Formulations of Acetaminophen
In adults with moderate to severe pain in the ED, limited evidence suggests that IV acetaminophen may offer an improvement in pain relief within the first hour of administration, but similar reductions in pain after 4 hours, when compared to oral acetaminophen (1 RCT).20 After 4 hours, a smaller, but not statistically significant, proportion of patients treated with oral acetaminophen required rescue analgesia (compared to IV acetaminophen),20 which may be due to the initially slower onset of pain relief provided by the oral formulation. As the need for rescue analgesia was not reported at different time points in this study, it is unknown whether similar findings for rescue analgesia would have been observed earlier than at 4 hours. No adverse events were reported following treatment with IV or oral acetaminophen. There were some limitations identified with this study (e.g., no confidence intervals reported, insufficient details about randomization, lack of blinding) which may limit the certainty of this evidence.
IV Acetaminophen Compared to Alternative Analgesics
Compared to NSAIDs
IV acetaminophen and IV NSAIDs provide clinically similar reductions in pain after 30 minutes in adults in the ED with moderate to severe pain.17,22 After 60 minutes, NSAIDs may offer a modestly greater improvement in pain relief than IV acetaminophen, but the difference is not clinically meaningful (1 SR),17 or they may provide similar pain relief (1 RCT).22 IV NSAIDs may offer more sustained pain relief, as patients treated with IV acetaminophen may experience a more frequent need for rescue analgesia (1 SR).17 However, in those with acute low back pain, no patients required additional analgesia with IV acetaminophen or IV NSAIDs (1RCT).22 The risk of adverse events was comparable between IV acetaminophen and IV NSAIDs (1 SR),17 with 1 study reporting no side effects from either drug.22 The authors of the SR17 assessed the evidence comparing IV acetaminophen to IV NSAIDs to be of low quality with significant heterogeneity, and there are some limitations in the RCT22 (e.g., minimal reporting of patient characteristics, uncertainty with the main outcome). These limitations should be considered when interpreting these findings.
Compared to Opioids
The findings for pain relief were mixed, but most of the identified evidence comparing IV acetaminophen with IV opioids did not observe a clinically important difference or a statistically significant difference in pain between groups (1 SR with meta-analysis, 1 RCT).17,24 The remaining identified studies reported a statistically significant improvement in pain favouring IV opioids (but not a clinically meaningful difference; 1 RCT from 1 SR and 1 RCT),18,21 and 1 study reported a larger decrease in pain favouring opioids that is both clinically and statistically different (1 RCT).23 No difference was observed in the proportion of patients requiring rescue analgesia between IV acetaminophen and IV opioids within the first hour after treatment (1 SR, 2 RCTs).17,21,23 However, when patients were asked whether they would like additional analgesia at 60 minutes, a higher proportion of patients in the IV opioid group declined (1 RCT).23 Patients treated with IV acetaminophen experienced either fewer adverse events (2 SRs, 1 RCT)17,18,23 or a similar number of adverse events (3 RCTs)21,23,24 than those treated with IV opioids. The limitations of the evidence should be considered when interpreting these findings. Specifically, the authors of the SR17 assessed the evidence comparing IV acetaminophen to IV opioids to be of low quality for pain and the need for rescue analgesia, and of moderate quality for adverse events, as well as the specific limitations of the 3 RCTS21,23,24 (e.g., uncertainty in the statistical analysis, reporting of the main outcome).
IV Acetaminophen Compared to Placebo
Limited evidence suggests that IV acetaminophen provides greater pain relief in adults with severe abdominal pain, but may cause more patients to experience nausea and vomiting, compared to those who received a placebo (1 RCT).24
Recommendations Regarding IV Acetaminophen in the ED
For the initial management of moderate to severe pain for patients in the ED, IV NSAIDs are recommended instead of IV acetaminophen (1 guideline).25 If IV acetaminophen is available, affordable, and easy to administer, then IV acetaminophen is recommended instead of IV opioids alone (1 guideline).25 These are both conditional recommendations, based on evidence with low certainty.
Considerations for Future Research
The authors of the SR with meta-analysis17 and the authors of the guideline25 both used GRADE to evaluate the strength of the evidence comparing IV acetaminophen to IV NSAIDs and IV opioids, and reported that the quality of the evidence was low17,25 or moderate (only for adverse events when compared to NSAIDs).17 Researchers should consider that the current findings related to the use of IV acetaminophen in the ED should be confirmed with additional well-conducted RCTs (e.g., with appropriate randomization procedures and blinding to reduce the risk of selection and performance bias) and SRs with meta-analysis. From the Canadian health care context, additional studies that compare IV acetaminophen to IV NSAIDs and IV opioids that are available for use in Canada are needed.
In addition, given the potentially higher cost of IV acetaminophen,12,13 research is needed to determine whether IV acetaminophen is cost-effective compared to the other available options for treating patients with moderate to severe pain in the ED. Studies specifically evaluating the effectiveness of IV acetaminophen compared to oral acetaminophen, IV opioids, or IV NSAIDs in pediatric patients with moderate to severe pain in the ED are also needed.
This report is focused of the use of IV acetaminophen for acute pain in the ED. Future research may consider the potential impacts of IV acetaminophen after the initial acute phase of treatment, such as the duration of analgesia required in the ED and the need for analgesia at discharge.
Implications for Clinical Practice and Policy-Making
The findings for this report suggest that IV acetaminophen may initially offer an improvement in pain relief when compared to oral acetaminophen, but that both drugs offer similar reductions in pain over time.20 However, decision-makers should consider that patients treated with oral acetaminophen may be less likely to need rescue analgesia at 4 hours (possibly due to the initial slower onset of pain relief provided by oral acetaminophen), but the evidence is uncertain.20
In general, IV acetaminophen and IV NSAIDs provide similar reductions in pain and a comparable risk of adverse events in adults in the ED with moderate to severe pain.17,22 However, decision-makers should consider that there is the potential that IV NSAIDs offer a modest improvement in pain relief (statistically but not clinically significant difference) with fewer patients requiring rescue analgesia compared to IV acetaminophen.17 This aligns with the recommendation to use IV NSAIDs for initial pain management for patients with moderate to severe pain in the ED (1 guideline).25 When selecting a pain reliever, decision-makers must also consider the contraindications for use for the specific drug and ensure that it is appropriate for the patient.
There is the potential that IV opioids may offer an improvement in pain relief compared with IV acetaminophen;18,21,23 however, some studies reported no evidence of a difference between the treatments17,24 or a difference that is statistically different (favouring opioids) but not clinically meaningful.18,21 Decision-makers should also consider that IV opioids may be associated with an increased risk of adverse events, such as nausea and vomiting,17,18,23 with a comparable incidence of rescue analgesia, when compared to IV acetaminophen.17,21,23 In the included guideline, IV acetaminophen is recommended instead of IV opioids alone for treating patients with moderate to severe pain in the ED, if IV acetaminophen is available, affordable, and easy to administer in the ED (1 guideline).25
References
1.Canadian Institute for Health Information. NACRS emergency department visits and lengths of stay. 2023; https://www.cihi.ca/en/nacrs-emergency-department-visits-and-lengths-of-stay#:~:text=In%202022%E2%80%932023%2C%20abdominal%20and,problem%20diagnoses%20in%202022%E2%80%932023. Accessed 2023 Sep 18.
2.Todd KH, Ducharme J, Choiniere M, et al. Pain in the emergency department: results of the pain and emergency medicine initiative (PEMI) multicenter study. J Pain. 2007;8(6):460-466. PubMed
3.Zanza C, Romenskaya T, Zuliani M, et al. Acute Traumatic Pain in the Emergency Department. Diseases. 2023;11(1). PubMed
4.Fabbri A, Voza A, Riccardi A, Serra S, Iaco F. The Pain Management of Trauma Patients in the Emergency Department. J Clin Med. 2023;12(9). PubMed
5.Opioid Prescribing in Canada. How Are Practices Changing? Ottawa: Canadian Institute for Health Information 2019: https://www.cihi.ca/sites/default/files/document/opioid-prescribing-canada-trends-en-web.pdf. Accessed 2023 Sep 18.
6.Pandharipande P, Hayhurst CJ. Pain control in the critically ill adult patient. Waltham (MA): UpToDate; 2023 Aug: https://www.uptodate.com/contents/pain-control-in-the-critically-ill-adult-patient?search=intravenous%20opioids&source=search_result&selectedTitle=2~150&usage_type=default&display_rank=2#. Accessed 2023 Sep 18.
7.Strain E. Opioid use disorder: Epidemiology, clinical features, health consequences, screening, and assessment. Waltham (MA): UpToDate; 2023 Aug: https://www.uptodate.com/contents/opioid-use-disorder-epidemiology-clinical-features-health-consequences-screening-and-assessment/print?search=opioid%20use%20disorder&source=search_result&selectedTitle=2~150&usage_type=default&display_rank=2. Accessed 2023 Sep 26.
8.Solomon DH. Nonselective NSAIDs: Overview of adverse effects. Ottawa: UpToDate; 2023: https://www.uptodate.com/contents/nonselective-nsaids-overview-of-adverse-effects/print?search=NSAIDs%20adverse%20effects&source=search_result&selectedTitle=1~150&usage_type=default&display_rank=1. Accessed 2023 Sep 18.
9.Acetaminophen: (paracetamol): drug information. Waltham (MA): UpToDate; 2023.
10.Acetaminophen injection sterile solution for infusion, 10 mg/mL, intravenous [product monograph]. 2023: https://pdf.hres.ca/dpd_pm/00069718.PDF. Accessed 2023 SEP 18.
11.Ulrich M, Chamberland M, Bertoldi C, Garcia-Bournissen F, Kleiber N. Newly approved IV acetaminophen in Canada: Switching from oral to IV acetaminophen. Is IV worth the price difference? A systematic review. Paediatr child health. 2021;26(6):337-343. PubMed
12.Bourgeois FT, Graham DA, Kesselheim AS, Randolph AG. Cost Implications of Escalating Intravenous Acetaminophen Use in Children. JAMA Pediatr. 2019;173(5):489-491. PubMed
13.Utilization and Cost Savings of an Emergency Department Acetaminophen Route Pathway. Western Journal of Emergency Medicine: Integrating Emergency Care with Population Health. 2022;23(5.1). https://escholarship.org/uc/item/7xf654vs#main. Accessed 2023 Sep 18.
14.Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. PubMed
15.Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377-384. PubMed
16.Agree Next Steps C. The AGREE II Instrument. [Hamilton, ON]: AGREE Enterprise; 2017: https://www.agreetrust.org/wp-content/uploads/2017/12/AGREE-II-Users-Manual-and-23-item-Instrument-2009-Update-2017.pdf. Accessed 2023 Sep 18.
17.Qureshi I, Abdulrashid K, Thomas SH, Abdel-Rahman ME, Pathan SA, Harris T. Comparison of intravenous paracetamol (acetaminophen) to intravenously or intramuscularly administered non-steroidal anti-inflammatory drugs (NSAIDs) or opioids for patients presenting with moderate to severe acute pain conditions to the ED: systematic review and meta-analysis. Emerg Med J. 2023;40(7):499-508. PubMed
18.Sobieraj DM, Baker WL, Martinez BK, et al. Comparative Effectiveness of Analgesics To Reduce Acute Pain in the Prehospital Setting. Rockville (MD): Agency for Healthcare Research and Quality; 2019: . Accessed 2023 Sep 18.
19.Sin B, Wai M, Tatunchak T, Motov SM. The Use of Intravenous Acetaminophen for Acute Pain in the Emergency Department. Acad Emerg Med. 2016;23(5):543-553. PubMed
20.Franceschi F, Saviano A, Covino M, et al. Oral vs. IV paracetamol for pain control in patients with femur fracture in the emergency department: a practical randomized controlled trial. Signa Vitae. 2023;19(4):72-78.
21.Kolli S, Friedman BW, Latev A, et al. A Randomized Study of Intravenous Hydromorphone Versus Intravenous Acetaminophen for Older Adult Patients with Acute Severe Pain. Ann Emerg Med. 2022;80(5):432-439. PubMed
22.Dogan C, Yilmaz A, Ozen M, et al. Comparative evaluation of the effectiveness of intravenous paracetamol, dexketoprofen and ibuprofen in acute low back pain. Am J Emerg Med. 2022;56:223-227. PubMed
23.Barnaby DP, Chertoff AE, Restivo AJ, et al. Randomized Controlled Trial of Intravenous Acetaminophen Versus Intravenous Hydromorphone for the Treatment of Acute Pain in the Emergency Department. Ann Emerg Med. 2019;73(2):133-140. PubMed
24.Oguzturk H, Ozgur D, Turtay MG, et al. Tramadol or paracetamol do not effect the diagnostic accuracy of acute abdominal pain with significant pain relief - a prospective, randomized, placebo controlled double blind study. Eur Rev Med Pharmacol Sci. 2012;16(14):1983-1988. PubMed
25.Lindbeck G, Shah MI, Braithwaite S, et al. Evidence-Based Guidelines for Prehospital Pain Management: Recommendations. Prehosp Emerg Care. 2023;27(2):144-153. PubMed
26.Powell JR, Browne LR, Guild K, et al. Evidence-Based Guidelines for Prehospital Pain Management: Literature and Methods. Prehosp Emerg Care. 2023;27(2):154-161. PubMed
27.Government of Canada. Health Canada Drug Product Database Online Query. 2023; https://health-products.canada.ca/dpd-bdpp/?lang=eng. Accessed 2023 Sep 14.
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Table 2: Characteristics of Included Systematic Reviews
Study citation, country, funding | Study design, outcomes | Intervention and comparators | Included studies | Population characteristics |
|---|---|---|---|---|
Qureshi et al. (2023)17 Qatar Funding: No funding received. | SR and meta-analysis of RCTs reporting the NRS or VAS for pain at baseline and 30 minutes. Literature searched until May 20, 2022. Primary outcome was pain reduction at 30 minutes. Secondary outcomes were pain reduction at 60, 90, and 120 minutes; the need for rescue analgesia, and adverse events. MID defined as median reduction of 17 mm on VAS. | Intervention: IV APAP alone Dose 1000 mg (24 RCTs) or 15 mg/kg (1 RCT) Comparators: NSAIDs (IV or intramuscular) or opioids (IV) alone (or in combination). [intramuscular NSAIDs were not relevant to this report] Dose and drugs used varied by RCT. | 27 RCTs included in the SR, with 24 RCTs included in the meta-analysis. 25 RCTs relevant to this report (with 12 RCTs including a comparison to IV NSAIDs, and 18 RCTs including a comparison to IV opioids) Studies published between 2009 and 2020. | Adults attending the ED with acute pain. N = 5,427 Range by study: 50 to 1645 patients Pain score (out of 10), mean (range) = 7.6 (2.7 to 9.2) Pain at baseline was:
|
Ulrich et al. (2021)11 Canada Funding: No funding received. | SR of prospective studies Literature searched until October 2019. Relevant outcome: pain | Intervention: IV APAP Comparator: Oral APAP | 3 studies included in SR; none of the studies are relevant to this report. | Children up to 18 years of age, with any indication (e.g., pain, temperature control) and all settings. |
Sobieraj et al. (2019)18 US Funding: National Highway Traffic Safety Administration | SR of RCTs, case-control, and cohort studies. Literature searched through May 9, 2019. Pain, adverse events. | Relevant intervention: IV APAP Relevant comparatorsa: IV opioids, IV NSAIDs | Overall = 11 RCTs published between 2012 and 2018. APAP vs. opioids = 10 RCTs APAP vs. NSAIDs = 1 RCT Of the 11 RCTs relevant to this report, only 1 RCT (APAP vs. opioids) did not overlap with the Qureshi SR (Refer to Appendix 5).b | People of any age, with acute onset moderate to severe pain in the pre-hospital setting including the ED. APAP vs. opioids: N = 2,001 Baseline pain (scale of 0 to 10), mean or median: ranged from 7.4 to 9.1 APAP vs. NSAIDs: N = 200 Baseline pain (100mm VAS), mean (SD): APAP = 71.6 (15.1) NSAID = 69.7 (13.9) |
APAP = acetaminophen; ED = emergency department; MID = minimally important difference; NRS = numerical rating scale; NSAID = non-steroidal anti-inflammatory drug; RCT = randomized controlled trial; SR = systematic review; VAS = visual analogue scale.
Note: This appendix has not been copy-edited.
aThe scope of this SR was broader than that of this report, and included additional drugs or routes of administration. Only the comparisons relevant to this report are included.
bThe RCT by Mollaei et al. (2016) included people aged 15 to 60 years with moderate to severe pain. Morphine (0.1 mg/kg) group: n = 28; mean age = 35 years; 60.7% male. APAP (1000 mg) group: n = 27; mean age = 36 years; 63% male.
Table 3: Characteristics of Included Primary Clinical Studies
Study citation, country, funding | Study design | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Franceschi et al. (2023)20 Italy Funding: None | RCT Single-centre Randomized in a 1:5 ratio (orally vs. IV APAP) | Adults 18 years or older at the ED with a femur fracture Pain at enrollment (VAS), median = 9 N, randomized = 180 N, completed the study = 171 APAP Oral, n = 27 APAP IV, n = 144 Age (years), median (IQR) APAP Oral = 81.5 (72 to 87) APAP IV = 81 (76 to 88) Sex (male), n (%) APAP Oral = 42 (29.2) APAP IV = 4 (14.8) (no additional information about sex was reported) | Intervention: 1000 mg APAP IV Comparator: 1000 mg APAP orally | Outcomes:
Follow-up: 4 hours after administration |
Kolli et al. (2022)21 US Funding: Harold and Muriel Block Institute for Clinical and Translational Research at Einstein and Montefiore | Double-blind, parallel group RCT Conducted in 2 EDs | Adults 65 years or older with severe acute pain in the ED. Severe pain defined as the attending physician’s plan to use IV opioids. N = 162 APAP, n = 81 Hydromorphone, n = 81 Age (years), mean (SD) APAP = 75 (8) Hydromorphone = 74 (6) Sex APAP = 31% male, 69% female Hydromorphone = 37% male, 63% female Baseline pain (0 to 10), median (IQR) APAP = 10 (8 to 10) Hydromorphone = 10 (8 to 10) | Intervention: 1000 mg IV APAP Comparator: 0.5 mg IV hydromorphone (opioid) | Outcomes:
Follow-up: 180 minutes |
Dogan et al. (2022)22 Turkey Funding: not reported | Double-blind, 3-arm RCT Conducted in a single ED | Adults between 18 and 65 years, with acute low back pain at the ED, with pain > 50mm on the VAS N = 210 APAP, n = 71 Dexketoprofen, n = 70 Ibuprofen, n = 69 Sex: 46.7% male, 53.3% female Baseline pain (0 to 100), mean (SD): APAP = 84.64 (9.68) Dexketoprofen = 78.84 (12.91) Ibuprofen = 85.39 (10.61) P = 0.002 | Intervention: 1000 mg IV APAP Comparator 1: 50 mg IV dexketoprofen (NSAID) Comparator 2: 400 mg IV ibuprofen (NSAID) | Outcomes:
Follow-up: 60 minutes |
Barnaby et al. (2019)23 US Funding: none | Double-blind, 2-arm, RCT Conducted in 2 inner-city EDs | Adults aged 21 to 64 years in the ED with acute pain. Pain judged by attending physician as sufficient severity to warrant use of IV opioids. Baseline pain ranged from 4 to 10 (on a scale of 0 to 10) in both groups. N = 220 (206 available to data analysis) APAP, n = 110 Hydromorphone, n = 110 Age (years), mean (SD) APAP = 43 (13) Hydromorphone = 42 (12) Sex APAP = 62% female Hydromorphone = 58% female (no additional information about sex was reported) | Intervention: 1000 mg IV APAP Comparator: 1 mg IV hydromorphone (opioid) | Outcomes:
Follow-up: 120 minutes |
Oguzturk et al. (2012)24 Turkey Funding: not reported | Double-blind, RCT Conducted in a single ED | Patients 17 years or older with abdominal pain less than 72 hours duration in the ED. N = 210 Age (years), mean (SD) = 32.8 (12.1) Sex: 44% male, 55.7% female n = 70 per group Baseline characteristics across groups were similar. Baseline pain (0 to 100), median (range): APAP: 83 (73 to 97) Tramadol: 85 (71 to 97) Placebo: 83.5 (73 to 97) | Intervention: 15 mg/kg IV APAP Comparators: 1 mg/kg IV tramadol (opioid), placebo | Outcomes:
Follow-up: 40 minutes |
APAP = acetaminophen; ED = emergency department; IQR = interquartile range; MID = minimally important difference; NSAID = non-steroidal anti-inflammatory drug; RCT = randomized controlled trial; SD = standard deviation; VAS = visual analogue scale.
Note: This appendix has not been copy-edited.
Table 4: Characteristics of Included Guideline
Intended users, target population | Intervention(s) and major outcomes considered | Evidence collection, synthesis, and quality assessment | Recommendations development and evaluation | Guideline validation |
|---|---|---|---|---|
Intended users: clinicians in the ED Target population: patients with moderate to severe pain in the ED | Pain severity, pain resolution, time to analgesic effect, adverse events | The evidence informing this guideline is based on a SR (Sobeiraj et al. 2019)18 that is included in this report. 9 PICO questions were generated and addressed using the evidence in the SR. Summary of findings tables were generated, including strength of the evidence. GRADE framework applied to classify the strength of the evidence (from very low to high quality). | A guideline development group, including individuals with expertise in emergency medicine (adult and pediatric), trauma, acute care, substance misuse disorder, and GRADE methodology, formulated the recommendations. To inform the recommendations, evidence-to-decision table were generated for each PICO question by reviewing the summary of findings tables, asynchronous judging of the evidence by the members of the guideline group, and a facilitated panel to generate final consensus-based recommendations. The evidence to decisions tables followed GRADE methodology, and considered the following: problem, desirable effects, undesirable effects, certainty of evidence, values, balance of effects, resources required, certainty of evidence of required resources, cost effectiveness, equity, acceptability, and feasibility. GRADE framework was used to classify the strength of the recommendations (strong or conditional). | Not reported. |
ED = emergency department. GRADE = Grading of Recommendations, Assessment, Development, and Evaluation; PICO = population, intervention, comparator, outcomes.
Note: This appendix has not been copy-edited.
Appendix 3: Critical Appraisal of Included Publications
Note that this appendix has not been copy-edited.
Table 5: Strengths and Limitations of Systematic Reviews Using AMSTAR 214
Strengths | Limitations |
|---|---|
Qureshi et al. (2023)17 | |
The population, intervention, comparators, and outcomes of interest were clearly stated. A protocol was registered in PROSPERO. The authors only included RCTs. The search was conducted in 4 databases, plus hand searching, searching for grey literature, and clinical trial registries. Key search terms were provided. No language restrictions were applied. The search was conducted within 24 months of publication. Study selection, data extraction, and quality assessments were performed in duplicate by 2 independent reviewers. For the included studies, the interventions, comparators, and outcomes were described in detail, and the populations were adequately described. Appropriate tools were used to assess the risk of bias of the included studies and the quality of the evidence by outcome. Appropriate statistical methods were used for the meta-analysis. The authors reported the various sources of heterogeneity in the results, including the variations in pain etiology, patients, medications, doses, and methods of reporting pain scores. The authors declared that they have no potential conflicts of interest, and no funding was received for this work. | The authors reported the number and reasons for exclusions, but did not provide a list of excluded studies with the justification for their exclusion. The baseline pain scores for the populations were not reported. The authors did not report the sources of funding for the included studies. The meta-analysis included all studies, regardless of risk of bias of the individual studies. Considerable statistical heterogeneity in the meta-analyses. The authors report the quality of the evidence for the outcomes, but do not discuss the potential impact of risk of bias or the quality of the evidence on the results. The authors investigating publication bias using funnel plots and reported that there may be minor publication bias, but did not describe the potential impact of this bias. The reporting of the findings is unclear. There are some discrepancies between the findings reported in the main paper and those in the appendices, and it is not always clear which studies are included in which meta-analyses nor how many studies are included in the analysis. |
Ulrich et al. (2021)11 | |
The population, intervention, comparator, and outcomes of interest were clearly stated. A protocol was registered in PROSPERO. The authors included prospective studies but did not further restrict by study design. The search was conducted in 5 databases, the full search strategy was provided, and the authors searched reference lists of included studies and relevant reviews, and the search was conducted within 24 months of publication. Two independent reviewers conducted study selection, and disagreements were resolved with a third reviewer. Data extraction was performed in duplicate. The authors declared no conflicts of interest, and no funding was received for this work. | Authors did not provide justification for restricting to studies published in English. A list of excluded studies with justifications for exclusion was not provided. |
Sobieraj et al. (2019)18 | |
The population, intervention, comparators, and outcomes of interest were clearly stated. A protocol was registered in PROSPERO. The authors included both RCTs and nonrandomized studies. The search was conducted in 3 databases, plus hand searching the references of relevant studies and trial registries. The full search strategy was provided. No language restrictions were applied. The search was conducted within 24 months of publication. Study selection and quality assessments were performed in duplicate by 2 independent reviewers. Data was extracted by 1 investigator and verified by a second investigator. For the included studies, the populations, interventions, comparators, and outcomes were well described. An appropriate tool was used to assess the risk of bias of the included studies. The authors considered the strength of the evidence when discussing the findings of the review. The source of funding for the review was reported, and the authors declared that they had no conflicts of interest, and that the work is independent of the sponsor of the work. | A list of excluded studies with justifications for exclusion was not provided. The authors did not report the sources of funding for the included studies. |
AMSTAR 2 = A MeaSurement Tool to Assess systematic Reviews 2; RCT = randomized controlled trials.
Table 6: Strengths and Limitations of Clinical Studies Using the Downs and Black Checklist15
Strengths | Limitations |
|---|---|
Franceschi et al. (2023)20 | |
The aim of the study, the main outcomes, and the interventions are well described. Simple outcome data were provided for the main findings (i.e., number and percentages). Actual P values were reported. Appropriate statistical tests were used to assess the main outcomes. The authors recruited the required number of patients based on their reported sample size calculation Consecutive patients were recruited and the participants are representative of the population of interest. Compliance with the intervention was reliable. All patients were followed for the same length of time. The study attempted to capture all adverse events related to the interventions. Minimal losses to follow up within each group. The authors declared that they had no conflicts of interest. No funding was received, thus no risk that the source of funding would impact the study. | Patients are described with limited detail. Baseline pain is only reported in a figure, thus the variation in the pain scores within the groups are unclear. Other potential confounders, such as body weight or whether they are taking other medications is not reported. Estimates of random variability (e.g., confidence intervals) were not provided for the main outcomes. Patients could not be blinded to the intervention (i.e., oral vs. IV APAP). It was not reported whether there was an attempt to blind those measuring the main outcome. The findings included additional unplanned analyses, including different time points and by subgroups. Method of randomization was unclear. Authors reported that randomization was conducted according to their department’s protocol, but no further details provided. The authors did not report why they randomized the patients in a 5 to 1 ratio of IV to oral APAP, and it is unclear whether they accounted for this ratio in the sample size calculation Unclear whether intervention assignment was adequately concealed (risk of selection bias). VAS pain scale was used to assess pain, but it is unclear whether the primary outcome of a reduction of at least 1 point of the VAS at 1 hour, represents a minimum clinically important improvement in pain in this specific population. |
Kolli et al. (2022)21 | |
The aim of the study, the patients, and the interventions are well described. The main outcome is well described and accurately reported. For all outcomes, the authors report simple outcome data, the mean difference between the groups, and 95% confidence intervals. The number and types of adverse events are reported. No patients were lost to follow-up. All patients were followed for the same length of time. The authors focused on whether the interventions achieved a minimum clinically important improvement in pain rather than whether the results were statistically significant. The patients and those administering the medications were blinded to the intervention. Compliance with the interventions was reliable. The method of randomization ensured that patients were randomly allocated to the interventions. Allocation assignment was concealed from the patients and health care staff using appropriate methods. The authors conducted a sample size calculation and recruited an appropriate number of patients. The authors declared that they had no conflicts of interest. The source of funding was reported and the authors declared that the funders had no influence on the conduct of the study. | Potential confounders, such as body weight or whether they are taking other medications is not reported. The reporting of the secondary outcomes is unclear. For 2 outcomes (i.e., the percentage of patients who failed to achieve a minimum clinically important improvement in pain, and the percentage who failed to achieve a 50% improvement in pain), the methods did not report the time frame, and these were only reported at 1 hour, rather than the full length of follow-up (i.e., 3 hours). The authors do not report which statistical tests were used and it is unclear whether these were appropriate. The authors do not report P values alongside the confidence intervals. The verbal NRS (from 0 to 10) was used to assess pain, but it is unclear whether a reduction in pain score of 1.3 at 1 hour represents a minimum clinically important improvement in pain in this specific population. |
Dogan et al. (2022)22 | |
The aim of the study, the outcomes, the inclusion and exclusion criteria, and the interventions were well described. The patients’ baseline level of pain is reported. The authors report simple outcome data (mean plus standard deviation). The study attempted to capture all adverse events related to the interventions. The patients, those administering the medications, and those assessing the outcome scores were blinded to the intervention. Compliance with the interventions was reliable. The method of randomization ensured that patients were randomly allocated to the interventions. Allocation assignment was concealed from the patients and health care staff using appropriate methods. The authors conducted a sample size calculation and recruited an appropriate number of patients. The authors declared that they had no conflicts of interest. | The age of the patients is not reported, and the sex of the patients in each group is not described. Other potential confounders, such as body weight or whether they are taking other medications is not reported. It is unclear whether any patients were lost to follow-up. The patient flow diagram suggests that more people were randomized to each group than received the intervention (e.g., around 140 people per group refused IV treatment or the 1 hour follow-up), but the text suggests that only those who consented to participate were randomized and received treatment (i.e., groups of 70, 71, and 69). VAS pain scale from 0 to 100 was used to assess pain, but the authors did not specify what was considered a minimum clinically important improvement in pain for this population. The statistical analysis did not adjust for potential confounders, including the significant difference in baseline pain between the groups. The source of funding was not reported, but all authors are listed as being involved with the acquisition of funding, which suggests that funding may have been received but not disclosed. |
Barnaby et al. (2019)23 | |
The aim of the study, the inclusion and exclusion criteria, and the interventions were well described. The patient groups are well described by age, sex, baseline pain, and race. The outcomes are well described and accurately reported. The authors report simple outcome data, the difference between the groups, and 95% confidence intervals. Important adverse events are reported. Minimal losses to follow up within each group. The patients, those administering the medications, and those assessing the outcome scores were blinded to the intervention. Compliance with the interventions was reliable. The main pain outcome was measured using a validated numerical rating scale, and a validated cut point was used for the minimum clinically important difference in pain. The method of randomization ensured that patients were randomly allocated to the interventions. Allocation assignment was concealed from the patients and health care staff using appropriate methods. The authors conducted a sample size calculation and recruited an appropriate number of patients. The authors declared that they had no conflicts of interest, and no funding was received for this work. | Other potential confounders, such as body weight or whether they are taking other medications is not reported. The authors do not report P values alongside the confidence intervals. |
Oguzturk et al. (2012)24 | |
The aim of the study, the inclusion and exclusion criteria, and the interventions were well described. The patient groups are well described by age, sex, and baseline pain. Adverse events reported included nausea, vomiting and dizziness. No patients were lost to follow-up. Actual P values were reported. The patients and those administering the medications were blinded to the intervention. Compliance with the interventions was reliable. The method of randomization was sufficient to ensure that patients were randomly allocated to the interventions. Allocation assignment was concealed from the patients and health care staff using appropriate methods. The authors conducted a sample size calculation and recruited an appropriate number of patients. | Other potential confounders, such as body weight, duration of pain, or whether they are taking other medications is not reported for the patients. The authors reported the median plus the range for the VAS scores at various time points, but did not report the mean difference between the times points by group. The authors did not specify what was considered a minimum clinically important improvement in pain for this population. Estimates of random variability (e.g., standard deviation, confidence intervals) were not provided for the main outcomes. It was not reported whether any patients required rescue analgesia. It is unclear whether appropriate statistical tests were used to assess the main outcomes. The authors report that they used independent t tests (a test designed for 2 groups), but there were 3 groups compared in the study. The findings were reported in such a way that it was unclear whether all 3 groups were compared in one statistical test, or whether the active interventions were compared to the placebo separately. It is unclear whether a statistical test was used to compare the 2 active interventions. The authors did not declare whether they had any conflicts of interest, nor did they report whether they received any funding for this report, and it is unclear whether there are any potential risks due to non-financial or financial conflicts that may have influenced the conduct or reporting of the study. |
APAP = acetaminophen; VAS = visual analogue scale
Table 7: Strengths and Limitations of Guideline Using AGREE II16
Item | |
|---|---|
Domain 1: scope and purpose | |
1. The overall objective(s) of the guideline is (are) specifically described. | Yes |
2. The health question(s) covered by the guideline is (are) specifically described. | Yes |
3. The population (patients, public, etc.) to whom the guideline is meant to apply is specifically described. | Yes |
Domain 2: stakeholder involvement | |
4. The guideline development group includes individuals from all relevant professional groups. | Yes |
5. The views and preferences of the target population (patients, public, etc.) have been sought. | Yes |
6. The target users of the guideline are clearly defined. | Yes |
Domain 3: rigour of development | |
7. Systematic methods were used to search for evidence. | Yes |
8. The criteria for selecting the evidence are clearly described. | Yes |
9. The strengths and limitations of the body of evidence are clearly described. | Unclear |
10. The methods for formulating the recommendations are clearly described. | Yes |
11. The health benefits, side effects, and risks have been considered in formulating the recommendations. | Yes |
12. There is an explicit link between the recommendations and the supporting evidence. | Yes |
13. The guideline has been externally reviewed by experts before its publication. | No |
14. A procedure for updating the guideline is provided. | No |
Domain 4: clarity of presentation | |
15. The recommendations are specific and unambiguous. | Yes |
16. The different options for management of the condition or health issue are clearly presented. | Yes |
17. Key recommendations are easily identifiable. | Yes |
Domain 5: applicability | |
18. The guideline describes facilitators and barriers to its application. | No |
19. The guideline provides advice and/or tools on how the recommendations can be put into practice. | No |
20. The potential resource implications of applying the recommendations have been considered. | Yes |
21. The guideline presents monitoring and/or auditing criteria. | No |
Domain 6: editorial independence | |
22. The views of the funding body have not influenced the content of the guideline. | Yes |
23. Competing interests of guideline development group members have been recorded and addressed. | Yes |
AGREE II = Appraisal of Guidelines for Research and Evaluation II.
Appendix 4: Main Study Findings
Note that this appendix has not been copy-edited.
Table 8: Summary of Findings by Comparison — IV APAP versus Oral APAP
Citation | Study design | Outcome | Outcome result | P value | |
|---|---|---|---|---|---|
IV APAP | Oral APAP | ||||
Pain | |||||
Franceschi et al. (2023)20 | RCT | Patients with a reduction of ≥ 1 point at 1 hour (10 point VAS), n (%) | 108 (75.0%) | 12 (44.0%) | 0.001 |
Patients with a reduction of ≥ 2 points at 4 hours (10 point VAS), n (%) | 129 (89.6%) | 24 (88.9) | 0.914 | ||
Rescue Therapy | |||||
Franceschi et al. (2023)20 | RCT | Requirement of rescue therapya at 4 hours, n (%) | 25 (17.5%) | 1 (3.7%) | 0.082 |
Adverse Events | |||||
Franceschi et al. (2023)20 | RCT | Adverse events reported within 4 hours, n | 0 | 0 | — |
APAP = acetaminophen; VAS = visual analogue scale.
aIf the primary therapy failed, rescue therapy was provided as a second dose of APAP (orally or IV), or treatment with opioids
Table 9: Summary of Findings by Comparison — IV APAP Versus IV NSAIDs
Citation | Study design | Outcome | Outcome results | Effect Estimate (95% CI) | P value | Heterogeneity (I2), % (P value) | ||
|---|---|---|---|---|---|---|---|---|
IV APAP | IV NSAID | |||||||
Pain | ||||||||
Qureshi et al. (2023)17 | SR with MA (14 RCTs) (2 RCTs used IM NDSAIDs) | Pain reduction at 30 minutes | — | — | SMD = 0.12 (–0.45 to 0.69) | NR | 94.2 (< 0.001) | |
SR with MA (6 RCTs) (1 RCT used IM NSAIDs) | Pain reduction at 60 minutes | — | — | SMD = 0.22 (0.05 to 0.38) | 0.01 | 49.9 (0.09) | ||
Dogan et al. (2022)22 | RCT | Pain reduction at 30 minutes (VAS 0 to 100), mean (SD) | 27.88 (16.09) | DK 27.95 (14.04) | IB 27.78 (16.22) | — | 0.998 | — |
Pain reduction at 60 minutes (VAS 0 to 100), mean (SD) | 39.94 (18.63) | DK 42.48 (19.69) | IB 42.92 (24.22) | — | 0.662 | — | ||
Rescue Therapy | ||||||||
Qureshi et al. (2023)17 | SR with MA (8 RCTs) (1 RCT used IM NSAIDs) | Required rescue analgesia within 30 minutes | — | — | RR = 1.50 (1.23 to 1.83) | < 0.001 | 2.37 (0.37) | |
SR with MA (2 RCTs) | Required rescue analgesia within 60 minutes | — | — | RR = 2.42 (1.51 to 3.86) | NR | 0 (0.65) | ||
Dogan et al. (2022)22 | RCT | Required rescue analgesia within 60 minutes | 0 | 0 | — | — | — | |
Adverse Events | ||||||||
Qureshi et al. (2023)17 | SR with MA (8 RCTs) (2 RCTs used IM NSAIDs) | Adverse events | — | — | RR = 1.30 (0.78 to 2.15) | — | 0 (0.83) | |
Dogan et al. (2022)22 | RCT | Adverse events, n | 0 | 0 | — | — | — | |
APAP = APAP; CI = confidence interval; DK = dexketoprofen; IB = ibuprofen; MA = meta-analysis; MD = mean difference; MCID = minimum clinically important difference; NR = not reported; RCT = randomized controlled trial; RR = risk ratio; SD = standard deviation; SMD = standardized mean difference; SR = systematic review; VAS = visual analogue scale.
aMCID defined at a reduction in pain score of > 1.3 (on a scale from 1 to 10)
Table 10: Summary of Findings by Comparison — IV APAP Versus IV Opioids
Citation | Study design | Outcome | Outcome results | Effect Estimate (95% CI) | P value | Heterogeneity (I2), % (P value) | |
|---|---|---|---|---|---|---|---|
IV APAP | IV Opioid | ||||||
Pain | |||||||
Qureshi et al. (2023)17 | SR with MA (17 RCTs) | Pain reduction at 30 minutes | — | — | SMD = –0.06 (–0.67 to 0.55) | — | 93.7 (< 0.001) |
SR with MA (6 RCTs) | Pain reduction at 60 minutes | — | — | SMD = –0.04 (–1.21 to 1.13) | — | 97.1 (< 0.001) | |
SR with MA (2 RCTs) | Pain reduction at 120 minutes | — | — | SMD = 0.56 (–3.29 to 4.41) | — | 98.9 (< 0.001) | |
Kolli et al. (2022)21 | RCT | Improvement in pain at 60 minutes (scale of 0 to 10), mean (SD) | 3.6 (2.9) | 4.6 (3.3) | Difference = 1.0 (0.1 to 2.0) | — | — |
Achieved MCIDa by 1 hour, n (%) | 62 (77) | 63 (78) | Difference = 1 (–12 to 14) | — | — | ||
Improved pain score by > 50% by 1 hour, n (%) | 30 (37) | 43 (53) | Difference = 16 (1 to 31) | — | — | ||
Sobieraj et al. (2019)18 | SR (1 RCT)b | Change in pain score at 30 minutes | — | — | MD = –0.70 (–1.30 to –0.10) | — | — |
Barnaby et al. (2019)23 | RCT | Decrease in pain at 60 minutes (NRS 0 to 10), mean (SD) | 3.3 (2.8) | 5.3 (2.8) | Difference = –2.0 (–2.7 to –1.2)c | — | — |
Oguzturk et al. (2012)24 | RCT | Decrease in pain (VAS 0 to 100) at 20 minutes, %d | 45 | 55 | — | Not reported | — |
Decrease in pain (VAS 0 to 100) at 40 minutes, %d | 60 | 67 | — | Not reported | — | ||
Rescue Therapy | |||||||
Qureshi et al. (2023)17 | SR with MA (10 RCTs) | Required rescue analgesia within 30 minutes | — | — | RR = 1.07 (0.67 to 1.70) | — | 66 (0.59) |
Kolli et al. (2022)21 | RCT | Required additional analgesia within 60 minutes, n (%) | 37 (46) | 37 (46) | MD = 7 (–8 to 23) | — | — |
Barnaby et al. (2019)23 | RCT | Received rescue analgesia within 60 minutes, n (%) | 3 (3) | 2 (2) | Difference = 1 (–3 to 5)c | — | — |
Declined additional analgesia at 60 minutes, n (%) | 45 (44) | 67 (65) | Difference = –21 (–35 to –8)c | — | — | ||
Adverse Events | |||||||
Qureshi et al. (2023)17 | SR with MA (13 RCTs) | Adverse events | — | — | RR = 0.50 (0.40 to 0.62) | < 0.001 | 0 (0.59) |
Kolli et al. (2022)21 | RCT | Adverse event related to medication, n (%) | 6 (7) | 10 (12) | Difference = 5 (–4 to 14) | — | — |
Sobieraj et al. (2019)18 | SR (1 RCT)b | Dizziness, n (%) | 0 (0) | 3 (10.7) | RD = –11% (–24% to 2%)e | — | — |
Barnaby et al. (2019)23 | RCT | Nausea, n/N (%)f | 1/40 (3) | 8/43 (19) | Difference = –16 (–28 to –4)c | — | — |
Vomiting, n/N (%)f | 1/40 (3) | 6/43 (14) | Difference = –11 (–23 to 0)c | — | — | ||
Pruritus, n/N (%) | 2/103 (2) | 3/103 (3) | Difference = –1 (–5 to 3)c | — | — | ||
Oguzturk et al. (2012)24 | RCT | Nausea or vomiting, n (%) | 13 (18.6) | 14 (20) | — | — | — |
APAP = acetaminophen; CI = confidence interval; MA = meta-analysis; MD = mean difference; MCID = minimum clinically important difference; NRS = numerical rating scale; RCT = randomized controlled trial; RD = risk difference; RR = risk ratio; SMD = standardized mean difference; SR = systematic review; VAS = visual analogue scale.
aMCID defined at a reduction in pain score of > 1.3 (on a scale from 1 to 10)
bOnly 1 RCT from this SR was not included in the more recent SR by Qureshi, thus the findings of this RCT are reported separately to avoid overlap and duplication of results, rather than reporting the results from the meta-analysis conducted in this SR.
cThe findings from Barnaby et al.23 were calculated with as IV opioid as the intervention compared to IV APAP. To align with the direction of this review (i.e., IV APAP compared to IV opioid) the difference and the confidence intervals were reversed by multiplying the values by –1, and swapping the upper and lower confidence intervals. The findings as reported in the RCT were: decrease in pain = 2.0 (1.2 to 2.7); declined additional analgesia = 21 (8 to 35); received rescue analgesia = –1 (–5 to 3); nausea = 16 (4 to 28); vomiting = 11 (0 to 23); pruritus = 1 (–3 to 5).
dCalculated by the RCT authors, using the following equation: (Median baseline VAS score — median VAS score at time point)/ median baseline VAS score * 100
eThis finding from Sobeiraj et al.18 were calculated with as IV opioid as the intervention compared to IV APAP. To align with the direction of this review (i.e., IV APAP compared to IV opioid) the risk difference and the confidence intervals were reversed by multiplying the values by –1, and swapping the upper and lower confidence intervals. The findings as reported in the SR was Dizziness, RD = 0.11 (–0.02 to 0.24).
fNausea and vomiting were only reported in those patients who did not have nausea or vomiting before administering study medication and then developed nausea and vomiting.
Table 11: Summary of Findings by Comparison — IV APAP Versus Placebo
Citation | Study design | Outcome | Outcome result | P value | |
|---|---|---|---|---|---|
IV APAP | Placebo | ||||
Pain | |||||
Oguzturk et al. (2012)24 | RCT | Decrease in pain (VAS 0 to 100) at 20 minutes, %a | 45 | 1 | < 0.001 |
Decrease in pain (VAS 0 to 100) at 40 minutes, %a | 60 | 0 | < 0.001 | ||
Adverse Events | |||||
Oguzturk et al. (2012)24 | RCT | Nausea or vomiting, n (%) | 13 (18.6) | 0 | — |
APAP = acetaminophen; RCT = randomized controlled trial.
aCalculated by the RCT authors, using the following equation: (Median baseline VAS score — median VAS score at time point)/ median baseline VAS score *
Table 12: Summary of Recommendations in the Included Guideline
Recommendations and supporting evidence | Quality of evidence and strength of recommendations |
|---|---|
Lindbeck et at. (2023)25 | |
“We suggest in favor of IV APAP over IV opioids alone for the initial management of moderate to severe pain in the prehospital setting if IV APAP is available, affordable, and easy to administer.” (p. 147) Supporting evidence: Conditional recommendation based on evidence of equivalent pain control and improved tolerability. The evidence did not suggest a clinically important difference in pain reduction at 15, 30, or 60 minutes. Adverse events, such as nausea and vomiting were generally higher with IV opioids than IV APAP. Cost differences between IV APAP and other analgesics was considered. | Low certainty of evidence Conditional recommendation |
“We suggest in favor of IV NSAIDs over IV APAP for the initial management of moderate to severe pain in the prehospital setting.” (p. 148) Supporting evidence: Evidence from 1 study found higher pain scores at 15 minutes with IV APAP compared to IV NDSAIDs, but the remaining evidence did not show a difference at 30 or 60 minutes. There were fewer adverse events with APAP. The cost difference between IV APAP and IV NSAIDs was considered. | Low certainty of evidence Conditional recommendation |
APAP = acetaminophen; NSAID = non-steroidal anti-inflammatory drug; PO = per os (i.e., by mouth).
Appendix 5: Overlap Between Included Systematic Reviews
Note that this appendix has not been copy-edited.
Table 13: Overlap in Relevant Primary Studies Between Included Systematic Reviews
Primary study citation | Qureshi et al. (2023)17 | Sobieraj et al. (2019)18 |
|---|---|---|
Al B, et al. Am J Emerg Med 2018;36:571 to 6. | Yes | Yes |
Al-Terki A, et al. Urology 2021;149:76 to 80. | Yes | — |
Azizkhani R, et al. J Res Med Sci 2013;18:772 to 6. | Yes | — |
Bektas F, et al. Ann Emerg Med 2009;54:568 to 74. | Yes | — |
Cenker E, et al. Urolithiasis 2018;46:369 to 73. | Yes | Yes |
Craig M, et al. Emerg Med J 2012;29:37 to 9. | Yes | Yes |
Demirozogul E, et al. Am J Emerg Med 2019;37:2136 to 42. | Yes | — |
Eken C, et al. Emerg Med J 2014;31:177 to 81. | Yes | Yes |
Esmailian M, et al. Emerg (Tehran) 2015;3:99 to 102. | Yes | — |
Far AAA, et a. Hong Kong J Emerg Med 2020 | Yes | — |
Ghamry NK, et al. Gynecol Obstet Invest 2020;85:388 to 95. | Yes | — |
Gülen B,, et al. Turk J Gastroenterol 2016;27:192 to 6. | Yes | — |
Jalili M, et al. Trauma Mon 2016;21:e19649. | Yes | Yes |
Masoumi K, et al. Emerg Med Int 2014;2014:571326. | Yes | Yes |
Montazer et al. J Emerg Pract Trauma 2018;4:39 to 43. | Yes | — |
Pathan SA, et al. The Lancet 2016;387:1999 to 2007. | Yes | Yes |
Serinken M, et al. Acad Emerg Med 2016;23:674 to 8. | Yes | Yes |
Serinken M, et al. Balkan Med J 2018;35:301 to 5. | Yes | — |
Serinken M, et al. Emerg Med J 2012;29:902 to 5. | Yes | Yes |
Shams Vahdati S, et al. Anesth Pain Med 2014;4.(3):e14903 | Yes | Yes |
Talebi Deloee M, et al. Trauma Mon 2017;22. | Yes | — |
Turkcuer I, et al. Emerg Med J 2014;31:182 to 5. | Yes | — |
Yalçınlı S, et al. Am J Emerg Med 2020;38:2014 to 8. | Yes | — |
Yazdani et al. Journal of Research in Medical and Dental Science 2018;6:169 to 73. | Yes | — |
Yilmaz A, et al. Am J Emerg Med 2019;37:2136 to 42. | Yes | — |
Mollaei M, et al. J Isfahan Med Sch. 2016;34(376):293 to 298. | — | Yes |
Appendix 6: References of Potential Interest
Note that this appendix has not been copy-edited.
Previous CADTH Reports
Pain Management in the Emergency Department and Upon Discharge. Ottawa: CADTH: 2021. https://www.cadth.ca/sites/default/files/pdf/htis/2021/RB1542%20ER%20Pain%20Final.pdf
Post Discharge Outcomes Following Intravenous Acetaminophen Treatment in Acute Care Settings. Ottawa: CADTH: 2021. https://www.cadth.ca/post-discharge-outcomes-following-intravenous-acetaminophen-treatment-acute-care-settings
Intravenous Acetaminophen for the Management of Short-Term Post-Operative Pain: A Review of Clinical Effectiveness and Cost Effectiveness. Ottawa: CADTH; 2019. https://www.cadth.ca/sites/default/files/pdf/htis/2019/RC1023%20IV%20Acetaminophen%20v2%20Revised%20Final.pdf
Randomized Controlled Trials
Alternative Intervention: APAP Plus Opioids
Minotti B, Mansella G, Sieber R, Ott A, Nickel CH, Bingisser R. Intravenous acetaminophen does not reduce morphine use for pain relief in emergency department patients: A multicenter, randomized, double-blind, placebo-controlled trial. Acad Emerg Med. 2022;29(8):954-962. PubMed
Dhebaria T, Sivitz A, Tejani C. Does Intravenous Acetaminophen Reduce Opioid Requirement in Pediatric Emergency Department Patients With Acute Sickle Cell Crises? Acad Emerg Med. 2021;28(6):639-646. PubMed
Bijur PE, Friedman BW, White D, et al. Randomized Clinical Trial of Intravenous (IV) Acetaminophen as an Adjunct to IV Hydromorphone for Acute Severe Pain in Emergency Department Patients. Acad Emerg Med. 2020;27(8):717-724. PubMed
Chang AK, Bijur PE, Ata A, et al. Randomized Clinical Trial of Intravenous Acetaminophen as an Analgesic Adjunct for Older Adults With Acute Severe Pain. Acad Emerg Med. 2019;26(4):402-409. PubMed
Furyk J, Levas D, Close B, et al. Intravenous versus oral paracetamol for acute pain in adults in the emergency department setting: a prospective, double-blind, double-dummy, randomised controlled trial. Emerg Med J. 2018;35(3):179-184. PubMed
Farnia MR, Babaei R, Shirani F, et al. Analgesic effect of paracetamol combined with low-dose morphine versus morphine alone on patients with biliary colic: a double blind, randomized controlled trial. World J Emerg Med. 2016;7(1):25-29. PubMed
Alternative Comparator: Opioid plus NSAID
Shams-Vahdati S, Robaei N, Habibollah P, Jafari-Rouhi A, Mohammadi S, Piri R. Paracetamol vs. Intravenous morphine plus diclofenac in renal colic pain: A randomized clinical trial. Nephro-Urology Monthly. 2018;10(4).
Nonrandomized Studies
Alternative Setting
Charlton K, Limmer M, Moore H. Intravenous versus oral paracetamol in a UK ambulance service: a case control study. Br. 2020;5(1):1-6.
Alternative Intervention: APAP Plus Opioids
Blok Z, Ridderikhof ML, Goddijn H, Berendsen M, Hollmann MW. Intravenous acetaminophen does not have an opioid sparing effect in Emergency Department patients with painful conditions. Am J Emerg Med. 2021;39:1-5. PubMed
Guidelines and Recommendations
Guidance With Unclear Methodology
Emergency Care BC. Pain Management in the ED (Diagnosis and Treatment); 2022. https://emergencycarebc.ca/clinical_resource/pain-management-in-the-ed-diagnosis-and-treatment/
Hachimi-Idrissi S, Dobias V, Hautz WE, Leach R, Sauter TC, Sforzi I, Coffey F. Approaching acute pain in emergency settings; European Society for Emergency Medicine (EUSEM) guidelines-part 2: management and recommendations. Intern Emerg Med. 2020 Oct;15(7):1141-1155. https://link.springer.com/article/10.1007/s11739-020-02411-2 PubMed
Contributors: Elizabeth Carson, Shannon Hill, Farhana Shivji.
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up to date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca.