CADTH Health Technology Review
Semaglutide for Type 2 Diabetes (2 mg)
Rapid Review
Authors: Deepa Jahagirdar, Quenby Mahood
Abbreviations
BMI
body mass index
hemoglobin A1C
glycated hemoglobin
RCT
randomized controlled trial
SEM
semaglutide
T2DM
type 2 diabetes mellitus
Key Messages
For patients with type 2 diabetes mellitus, a single randomized controlled trial (SUSTAIN FORTE) suggested that once-weekly subcutaneous semaglutide 2.0 mg may achieve better glycemic control than once-weekly subcutaneous semaglutide 1.0 mg. However, it is unclear whether between-group differences are clinically meaningful.
Gastrointestinal disorders were the most common adverse event resulting in premature discontinuation in both groups. One participant in each study arm experienced a cardiovascular disorder serious enough for premature discontinuation.
As most trial patients were white, it is unclear if the results are generalizable to groups with higher prevalence of T2DM in Canada, such as Indigenous peoples or those of South Asian descent.
We did not find any studies on the cost-effectiveness of subcutaneous semaglutide 2.0 mg, compared to placebo or other doses of semaglutide.
Context and Policy Issues
Diabetes mellitus is a metabolic disease characterized by persistent hyperglycemia. Over 10 million Canadians are living with the condition. There are 2 main subtypes: type 1 diabetes mellitus, where insulin production is inadequate, and type 2 diabetes mellitus (T2DM), where the body does not use insulin properly. In Canada, T2DM accounts for approximately 90% of cases of diabetes mellitus.1
Genetic risk factors can contribute to the development of T2DM, along with modifiable risk factors such as obesity and smoking.2 T2DM treatment aims to keep blood sugars within a target range. Sometimes this can be achieved with lifestyle changes including a healthy overall diet and exercise.3 When lifestyle changes are not enough to maintain appropriate blood glucose levels, pharmacologic therapy may be required to prevent complications, including high blood pressure, cardiovascular disease, diabetic retinopathy, and kidney damage.3 The first-line treatment is usually a medication called metformin, which helps improve the body’s response to insulin.3 When metformin therapy is not enough for diabetic control, other oral antidiabetic drugs can be used (e.g., sulfonylureas or sodium-glucose cotransporter-2 inhibitors). If these drugs fail, the patient may progress to injectable medication.4
Semaglutide (SEM), marketed as Ozempic, is an injectable medication indicated for use in adult patients with T2DM where metformin therapy alone was insufficient for glycemic control or contraindicated.5 The drug is a selective long-acting glucagon-like peptide 1 (GLP-1) receptor agonist that stimulates insulin production, thus reducing blood glucose levels. It can also have a role in appetite suppression, increasing the feeling of fullness.6 The SUSTAIN trials established efficacy and safety for once-weekly subcutaneous SEM treatment at doses 0.5 mg and 1.0 mg.7 Based on this and other evidence,8 the CADTH Canadian Drug Expert Committee recommended in 2019 that SEM should be reimbursed for adult patients with T2DM with inadequate glycemic control.5 As of 2022 SEM is still being used in doses up to 1.0 mg per week in Canada in 96.4% of claimants nationally,4 despite approval as of January 2022 to use once-weekly doses as high as 2.0 mg in Canada.9
While SEM at higher doses than 1.0 mg are being used in Canada, there is also the potential for increased cost and risks associated with the higher, 2.0 mg once-weekly dose without a comprehensive evidence review for its benefits. Understanding this trade off could help to support decision-making on more widespread use of SEM injectable 2.0 mg instead of lower doses. While off-label use of Ozempic for weight loss is suspected,4 this review excludes weight-related outcomes due to a previous CADTH Reimbursement Review that did not recommend reimbursement of a similar SEM medication (Wegovy) for chronic weight management, including in those with T2DM.10 The purpose of this review is to summarize the evidence regarding the clinical and cost-effectiveness of SEM 2.0 mg subcutaneous once-weekly injection compared to lower 0.5 mg and 1.0 mg doses or placebo for managing T2DM in adults.
Research Questions
What is the clinical effectiveness of semaglutide subcutaneous injection 2 mg once weekly for the management of type 2 diabetes in adults?
What is the cost-effectiveness of semaglutide subcutaneous injection 2 mg once weekly for the management of type 2 diabetes in adults?
Methods
Literature Search Methods
An information specialist conducted a literature search on key resources including MEDLINE, the Cochrane Database of Systematic Reviews, the International HTA Database, the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search approach was customized to retrieve a limited set of results, balancing comprehensiveness with relevancy. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. Search concepts were developed based on the elements of the research questions and selection criteria. The main search concepts were semaglutide, dosage, and type 2 diabetes. CADTH-developed search filters were applied to limit retrieval to health technology assessments, systematic reviews, meta-analyses, indirect treatment comparisons, any types of clinical trials or observational studies, or economic studies to a secondary search of the concepts semaglutide and type 2 diabetes. The search was completed on August 15, 2023, and limited to English-language documents published since January 1, 2018.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
|---|---|
Population | Adults (ages 18+) with type 2 diabetes who have inadequate glycemic control with prior therapy |
Intervention | Semaglutide subcutaneous injection 2 mg once weekly, as monotherapy or add-on therapy with one or more antidiabetic drugs |
Comparator | Alternative doses of semaglutide (e.g., 0.5 mg once weekly, 1 mg once weekly) or placebo |
Outcomes | Q1: Clinical benefits (i.e., glycemic control, mortality, diabetes-related cardiovascular outcomes [i.e., MACE, cardiovascular death, nonfatal stroke, nonfatal MI], hospitalizations, health-related quality of life, blood pressure, fasting plasma glucose, lipid profile) and harms (e.g., adverse events) Q2: Cost-effectiveness (e.g., cost per quality-adjusted life-year gained) |
Study designs | Health technology assessments, systematic reviews, randomized controlled trials, nonrandomized studies, economic evaluations |
MACE = major adverse cardiovascular events; MI = myocardial infarction.
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, they were duplicate publications, or were published before 2018.
Critical Appraisal of Individual Studies
The included publication was critically appraised by 1 reviewer using the Downs and Black checklist11 for randomized and nonrandomized studies. A summary score was not calculated for the included study; rather, the strengths and limitations of the included publication were described narratively.
Summary of Evidence
Quantity of Research Available
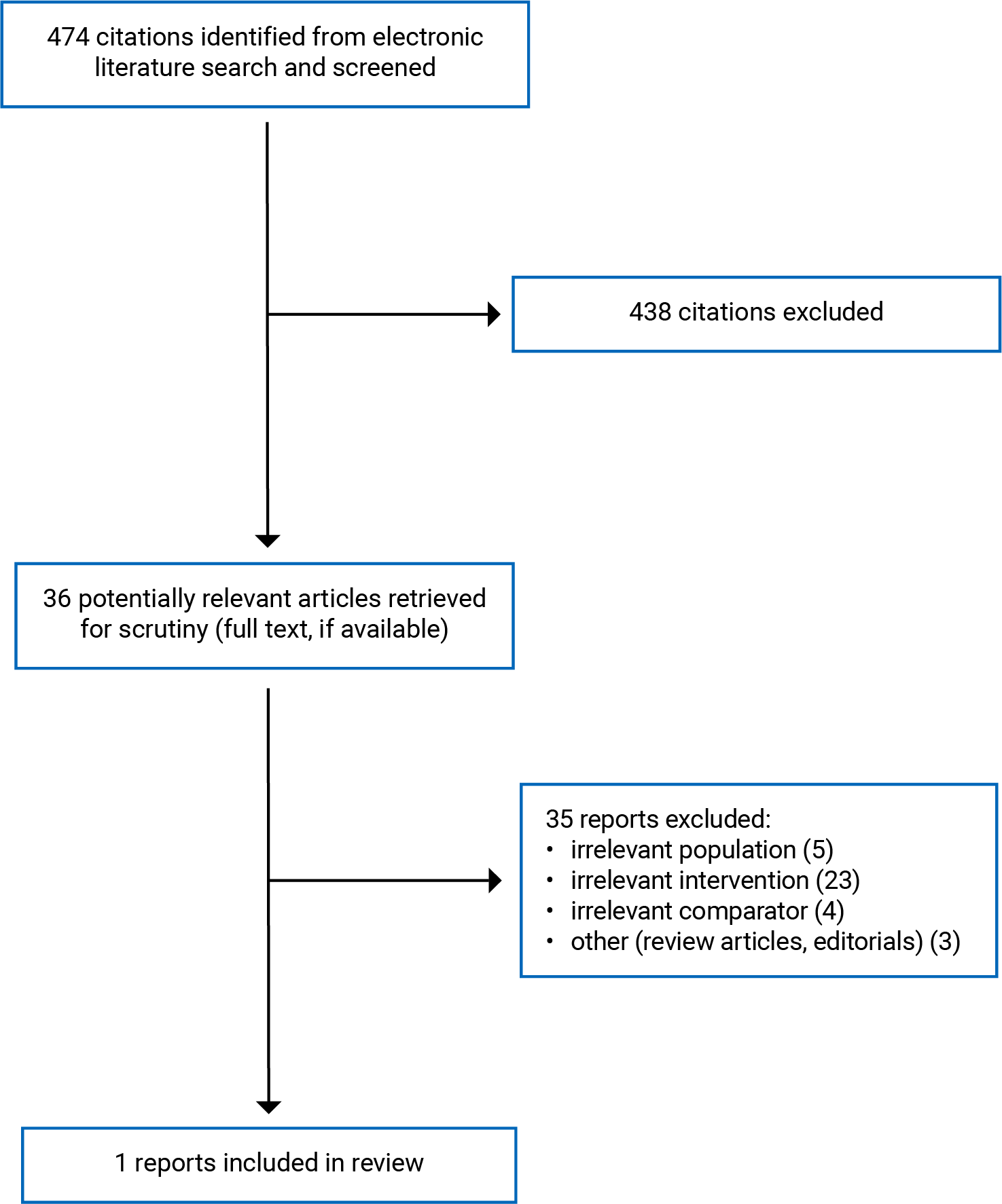
A total of 474 citations were identified in the literature search. Following screening of titles and abstracts, 438 citations were excluded and 36 potentially relevant reports from the electronic search were retrieved for full-text review. Of these potentially relevant articles, 35 publications were excluded for various reasons. One randomized controlled trial (RCT) met the inclusion criteria and was included in this report. Appendix 1 presents the PRISMA12 flow chart of the study selection.
Additional references of potential interest are provided in Appendix 5.
Summary of Study Characteristics
Appendix 2 presents detailed study characteristics of the included publication.
Study Design
We identified 1 double-blinded RCT (SUSTAIN FORTE) published in 2021.13
Country of Origin
The study had 129 trial sites from 10 countries, including Bulgaria, Canada, Czech Republic, Greece, Hungary, Japan, Poland, Slovakia, Ukraine, US.13
Patient Population
The study was limited to adults aged 18 and older who had inadequately controlled type 2 diabetes for at least 180 days. ‘Inadequate control’ was defined as glycated hemoglobin (hemoglobin A1C) 64 to 86 mmol/mol or 8% to 10%. In addition, patients had to be on a stable metformin dose for at least 90 days. The final randomized sample (N = 961) had a mean overall age of 58; 88% of patients were white with a mean duration of diabetes of 9.5 years. 41% were female, while all patients took metformin at randomization, and 53% took sulfonylurea. The average baseline hemoglobin A1C was 73.3 mmol/mol or 8.9%, and the body mass index was 34.6 kg/m2.13
Interventions and Comparators
The intervention and comparator group had SEM once-weekly subcutaneous injection dose escalation from 0.25 mg to 1.0 mg over 8 weeks. The 1.0 mg dose was then maintained for an additional 4 weeks. Starting at week 13, the intervention group received an additional 1.0 mg pen, for a total of 2.0 mg, once-weekly, while the control group was maintained at 1.0 mg using a placebo pen. Follow-up was at week 40.13
Outcomes
The primary outcome was the percentage point change from baseline in hemoglobin A1C.13
Secondary outcomes that were relevant to this report included change in fasting plasma glucose. Additional group-level outcomes included the number of patients who reached hemoglobin A1C less than 7%, and the number of patients who reached hemoglobin A1C less than 6.5%.13
While not a protocol-defined outcome, the authors also measured changes to blood pressure for completeness.
Summary of Critical Appraisal
The included study13 achieved randomization using an interactive web response system, limiting the possibility that randomization was inadequate. Further demonstrating successful randomization, the patients in both groups had balanced characteristics. Bias favouring either the intervention or control group was also limited through masking among patients, site personnel, the investigators, and those conducting the study (the clinical study group). Patients in the SEM 1.0 mg and SEM 2.0 mg dose group received an identical injection pen; 1 was a placebo, while the other provided an additional SEM 1.0 mg dose. Discontinuation was similar in both groups. In the SEM 2.0 mg arm, 447 of 481 completed treatment while 34 prematurely discontinued, while in the 1.0 mg arm, 442 of 480 completed treatment and 38 patients discontinued prematurely.
Regarding the statistical analysis, the study13 had adequate power (87%) to detect a 0.22 percentage point reduction from baseline in hemoglobin A1C. The authors conducted both a traditional intention-to-treat analysis (termed ‘treatment policy estimand’), where outcomes are analyzed regardless of discontinuation or change in treatment dose, which limits bias associated with dropout, as well as an analysis where observations were regardless of change in treatment dose only (‘trial product estimand’).
Missing data were handled through multiple imputations, assuming they were ‘missing at random,’ or the missingness was unrelated to the patient’s outcome once other observed characteristics were accounted for. This assumption was not explained, and the extent of missing data were unclear, making it difficult to assess whether outstanding bias could be significant. However, sensitivity analysis was conducted to assess the impact of handling missing data on the results; the findings supported the main results.
Two concerns about study quality included the exclusive funding by the drug manufacturer, Novo Nordisk, and the lack of clear outcomes reporting by analysis method. The manufacturer funding may not have influenced the study results; however, objective funders are usually preferred. Lastly, the authors also state 2 analysis methods (trial product and treatment policy estimand), but, for example, only the trial product estimand results were shown for the reduction in fasting plasma glucose and the proportion of patients achieving hemoglobin A1C lower than 6.5%.13 Showing both results would have enabled a clearer interpretation of the findings.
Additional details regarding the strengths and limitations of included publications are provided in Appendix 3.
Summary of Findings
Appendix 4 presents the main study findings.
Clinical Effectiveness of Semaglutide 2.0 mg
Glycemic Control
The 1 eligible RCT (SUSTAIN FORTE)13 found that SEM 2.0 mg.
was superior to SEM 1.0 mg to achieve glycemic control. The intervention group experienced a 2.1 percentage point reduction in hemoglobin A1C, while the control group had an average 1.9 percentage point reduction in hemoglobin A1C. The estimated absolute difference in percentage point reduction between the groups was 0.18 (95% confidence interval = 0.04 to 0.31, P < 0.001), which was statistically significant at the 5% level.
In terms of secondary outcomes, SEM 2.0 mg, patients also achieved statistically significantly greater reductions in fasting plasma glucose than SEM 1.0 mg patients. Finally, the SEM 2.0 mg group had statistically significantly greater proportions of patients who achieved hemoglobin A1C less than 6.5%, or less than 7%, than the SEM 1.0 mg group.13
Blood Pressure
The changes to blood pressure were not assessed for statistical significance; however, in the intervention group systolic and diastolic blood pressure were 5.3 mm Hg and 0.8 mm Hg lower than baseline respectively, while in the comparator group systolic and diastolic blood pressure were 4.5 mm Hg and 0.4 mm Hg lower, respectively.
Adverse Events
A total of 272 (57%) patients in the intervention group and 251 (52%) in the comparator group had at least 1 adverse event. Overall, 4% (n = 21) of patients had serious events in the intervention group, while 5% (n = 25) were serious in the comparator group. Two patients in the 2.0 mg group died, and both deaths were judged as unlikely to be related to treatment, while a single death in the 1.0 mg group was from neuromyelitis optica spectrum disorder. The latter was judged by the investigator as possibly related to treatment, but the sponsor thought this was unlikely as SEM is not previously linked to autoimmune mediated disorders. Two patients had level 3 hypoglycemia (severe hypoglycemia requiring assistance for recovery) in the intervention group while 1 patient had level 3 hypoglycemia in the comparator group. The most common reported side effects were gastrointestinal symptoms including nausea, diarrhea and vomiting, which occurred among 163 (34%) and 148 (31%) of patients in the intervention and control groups, respectively. One patient in the 1.0 mg group and 1 patient in the 2.0 mg group experienced a cardiac disorder resulting in premature discontinuation.
Cost-Effectiveness of Semaglutide 2.0 mg
No eligible studies were identified; therefore, no summary can be provided.
Limitations
There was 1 RCT identified that answered the research question. The study was conducted across several countries, suggesting generalizability to Canada may be appropriate. However, the patient population was overwhelmingly white (88%), thus failing to represent ethnic minorities who have greater prevalence of diabetes in Canada.14 For example, a single participant categorized by study authors as “American Indian or Alaska native” was included, and a breakdown of the 69 “Asian”’ patients was unavailable. At the same time, people of South Asian descent have a prevalence 8 times higher than white adults. For First Nations individuals living off-reserve, the prevalence is 1.72 times higher than in adults who do not identify as Indigenous.14
Not all the relevant outcomes, as stated in the PICO for this review, were explored in this trial. Diabetes-related cardiovascular outcomes were not explored in detail, other than captured as a general organ system (cardiovascular disorders) in terms of safety outcomes. Further, lipid profiles and health-related quality of life were not outcomes in this study.
This is also only 1 clinical trial. A larger evidence base could corroborate the findings in this study. Given that no cost-effectiveness studies were available, future studies assessing the cost of SEM 2.0 mg compared to other doses of semaglutide would also help with policy decision-making.
Conclusions and Implications for Decision- or Policy-Making
This review summarizes the most recent evidence regarding a 2.0 mg once-weekly dose of subcutaneous semaglutide for the glycemic management of T2DM, compared with alternative doses of semaglutide. A previous CADTH Reimbursement Review8 summarized evidence for doses up to 1.0 mg once weekly in Canada for this indication. Based on this review, the CADTH Canadian Expert Drug Committee issued a reimbursement recommendation with conditions.5
In this Rapid Review, a single RCT, the SUSTAIN FORTE trial13 was identified that suggests that once-weekly subcutaneous semaglutide 2.0 mg may achieve better glycemic control, with apparently similar rates of adverse events, compared to once-weekly subcutaneous semaglutide 1.0 mg. While the 0.18% difference in hemoglobin A1C between the doses was statistically significant, elsewhere a decline in hemoglobin A1C of at least 0.5% has been considered clinically meaningful.15 Thus, both arms did achieve clinically meaningful within-group reductions in hemoglobin A1C, with the difference between groups failing to achieve that threshold; whether such a difference between the 2 doses is therefore important in terms of long-term outcomes and diabetic control was not clear from this study.
Finally, while this trial was conducted across several countries, there was limited representation of minority groups with higher prevalence of T2DM in Canada such as Indigenous peoples or those of South Asian descent. Further, a single trial may not be enough to alter clinical practice in Canada, and a larger evidence base could further support the findings. Cost-effectiveness studies comparing various doses of semaglutide were also unavailable, comprising a research gap that, if filled, could assist in policy-making.
References
1.Diabetes Canada. What is diabetes? 2023; https://www.diabetes.ca/about-diabetes/what-is-diabetes. Accessed 2023 Sep 06.
2.Lyssenko V, Jonsson A, Almgren P, et al. Clinical risk factors, DNA variants, and the development of type 2 diabetes. N Engl J Med. 2008;359(21):2220-2232. PubMed
3.Wexler DJ. Patient education: type 2 diabetes: treatment (beyond the basics). In: Post TW, ed. UpToDate. Waltham (MA): UpToDate; 2022: http://www.uptodate.com. Accessed 2023 Sep 19.
4.Vannabouathong C, Crotty C, Le K, Eurich D, Dydra P. Current utilization patterns of glucagon-like peptide-1 receptor agonists (CADTH health technology review). Can J Health Technol. 2022;2(9). https://www.cadth.ca/sites/default/files/hta-he/HC0042-Utilization-of-Glucagon-Like-Peptide1-(GLP-1)-Agonists-aug26_KT-meta.pdf. Accessed 2023 Sep 19.
5.CADTH Common Drug Review. CADTH Canadian Drug Expert Committee recommendation (final): semaglutide (Ozempic - Novo Nordisk Canada Inc.). Ottawa (ON): CADTH; 2019 May: https://www.cadth.ca/sites/default/files/cdr/complete/SR0594%20Ozempic%20-%20CDEC%20Final%20Recommendation%20May%2017%2C%202019%20%28redacted%29_For%20posting.pdf. Accessed 2023 Sep 6.
6.Dungan K, DeSantis A. Glucagon-like peptide 1-based therapies for the treatment of type 2 diabetes mellitus. In: Post TW, ed. UpToDate. Waltham (MA): UpToDate; 2023: http://www.uptodate.com. Accessed 2023 Sep 19.
7.Aroda VR, Erhan U, Jelnes P, et al. Safety and tolerability of semaglutide across the SUSTAIN and PIONEER phase IIIa clinical trial programmes. Diabetes Obes Metab. 2023;25(5):1385-1397. PubMed
8.CADTH Common Drug Review. Clinical review report: semaglutide (Ozempic - Novo Nordisk Canada Inc.). Ottawa (ON): CADTH; 2019 Jun: https://www.cadth.ca/sites/default/files/cdr/clinical/sr0594-ozempic-clinical-review-report.pdf. Accessed 2023 Sep 19.
9.PROzempic® (semaglutide injection): 2mg/pen (0.68 mg/mL or 1.34 mg/mL), 4mg/pen (1.34 mg/mL), 8mg/pen (2.68 mg/mL) [product monograph] Mississauga (ON): Novo Nordisk Canada; 2023.
10.CADTH Reimbursement Review: semaglutide (Wegovy - Novo Nordisk Canada Inc.). Can J Health Technol. 2022;2(10). https://www.cadth.ca/sites/default/files/DRR/2022/SR0725%20Wegovy%20-%20CADTH%20Final%20Recommendation-meta.pdf.
11.Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377-384. PubMed
12.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
13.Frias JP, Auerbach P, Bajaj HS, et al. Efficacy and safety of once-weekly semaglutide 2.0 mg versus 1.0 mg in patients with type 2 diabetes (SUSTAIN FORTE): a double-blind, randomised, phase 3B trial. Lancet Diabetes Endocrinol. 2021;9(9):563-574. PubMed
14.Diabetes Canada. Diabetes in Canada: estimated prevalence and cost of diabetes. 2023; https://www.diabetes.ca/advocacy---policies/advocacy-reports/national-and-provincial-backgrounders/diabetes-in-canada. Accessed 2023 Sep 19.
15.Dankers M, Nelissen-Vrancken M, Hart BH, Lambooij AC, van Dijk L, Mantel-Teeuwisse AK. Alignment between outcomes and minimal clinically important differences in the Dutch type 2 diabetes mellitus guideline and healthcare professionals' preferences. Pharmacol Res Perspect. 2021;9(3):e00750. PubMed
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Note that this appendix has not been copy-edited.
Table 2: Characteristics of Included Primary Clinical Study
Study citation, country, funding source | Study design | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Frias et al. (2012)13 Multicountry Funding source: Novo Nordisk | Randomized Controlled Trial | Inclusion: Adults ≥ 18 with type 2 diabetes for at least 180 days, inadequately controlled (hemoglobin A1C 8.0% to 10.0%; 64 to 86 mmol/mol), using a stable dose of metformin or sulfonylurea for at least 90 days Exclusion: Glomerular filtration rate < 30 mL/min per 1.73 m2, receiving medications other than metformin or sulfonylurea for obesity or diabetes, diabetic retinopathy/ maculopathy, pancreatitis, heart failure | Intervention: 2.0 mg subcutaneous once weekly semaglutide Comparator: 1.0 mg subcutaneous once weekly semaglutide | Outcomes: Percentage point change from baseline in hemoglobin A1C, fasting plasma glucose (mmol/L), hemoglobin A1C less than 7.0% or 6.5% or lower, blood pressure, safety outcomes Follow-up: 40 weeks |
BMI = body mass index; hemoglobin A1C = glycated hemoglobin.
Appendix 3: Critical Appraisal of Included Publications
Note that this appendix has not been copy-edited.
Table 3: Strengths and Limitations of Clinical Study Using the Downs and Black Checklist11
Strengths | Limitations |
|---|---|
Frias (2021)13 | |
Randomization was done centrally using an interactive web response system. Masking maintained using an identical injection pen that was either placebo or an extra 1 mg dose (for intervention group) - masking included patients, site personnel, the clinical study group, and investigators. Power calculation suggests 87% power to detect a 0.22 percentage point change in hemoglobin A1C with standard deviation 1.1 at the 5% significance level. Intention-to-treat analysis as well as as-treated analysis helps to prevent bias related to differential treatment discontinuation. Balanced patient characteristics, low dropout rate in both groups: > 90% completed the trial at required dose. Sensitivity analyses supporting main findings. | Funded by the drug manufacturer (Novo Nordisk). Did not clearly report all outcomes by analysis method (selective reporting of trial product vs trial policy estimand) which can have different results; where available, trial policy estimand was included in this report. Did not specify the extent of missing data or justify assumption of ‘missing at random.’ Limited representation of groups with higher prevalence of T2DM in Canada, e.g., South Asian and First Nations. |
hemoglobin A1C = glycated hemoglobin; T2DM = type 2 diabetes mellitus.
Appendix 4: Main Study Findings
Note that this appendix has not been copy-edited.
Outcome | Frias (2021)13 | ||
|---|---|---|---|
SEM 2.0 mg n = 480 | SEM 1.0 mg n = 481 | Estimated difference between groups (95% CI) | |
Primary outcomes (absolute percentage point change)a | |||
Percentage point change from baseline in hemoglobin A1C | −2.1 | −1.9 | –0·18 (–0·31 to –0·04); P = 0.0098 |
Secondary outcomes (absolute unit change)a | |||
Fasting plasma glucose (mmol/L) | −3.4 | –3.1 | –0.33 (–0.61 to –0.04); P = 0·026 |
Blood pressure (mm Hg): Systolic | –5·3 (SD 14.99) | −4.5 (SD 14) | NA |
Blood pressure (mm Hg): Diastolic | –0·8 (SD 8.99) | −0.4 (SD 9) | NA |
Group-level outcomes (proportion yes)b | |||
Hemoglobin A1C < 7·0% | 67.66 | 57.5 | 1.60 (1·21 to 2.13); P = 0·0010 |
Hemoglobin A1C < 6.5% | 51.7 | 38.5 | 1.80 (1.36 to 2.36); P < 0·0001 |
Safety outcomes (n [%]) | |||
All adverse events | 251 (52) | 272 (57) | NA |
Adverse events leading to premature treatment discontinuation | 22 (4·6) | 21 (4·4) | NA |
95% CI = 95% confidence interval; hemoglobin A1C = glycated hemoglobin; OR = odds ratio; SEM = semaglutide; SD = standard deviation.
aEstimated effect is an absolute unit change; bEstimated effect is an odds ratio except for blood pressure outcomes where no estimated difference was calculated.
Appendix 5: References of Potential Interest
Note that this appendix has not been copy-edited.
Randomized Controlled Trials
Davies M, Faerch L, Jeppesen OK, et al. Semaglutide 2.4 mg once a week in adults with overweight or obesity, and type 2 diabetes (STEP 2): a randomised, double-blind, double-dummy, placebo-controlled, phase 3 trial. Lancet 2021;397(10278):971-984. PubMed
Bjorner JB, Larsen S, Lubker C, Holst-Hansen T. The improved health utility of once-weekly subcutaneous semaglutide 2.4 mg compared with placebo in the STEP 1-4 obesity trials. Diabetes Obes Metab. 2023;25(8):2142-2150. PubMed
Frias JP, Deenadayalan S, Erichsen L, et al. Efficacy and safety of co-administered once-weekly cagrilintide 2.4 mg with once-weekly semaglutide 2.4 mg in type 2 diabetes: a multicentre, randomised, double-blind, active-controlled, phase 2 trial. Lancet. 2023;23:23. PubMed
Ongoing Trial
Buse JB, Nordahl Christensen H, Harty BJ, et al. Study design and baseline profile for adults with type 2 diabetes in the once-weekly subcutaneous SEmaglutide randomized PRAgmatic (SEPRA) trial. BMJ Open Diabetes Res. 2023;11(3):05. PubMed
Economic Evaluations
Azuri J, Hammerman A, Aboalhasan E, Sluckis B, Arbel R. Tirzepatide versus semaglutide for weight loss in patients with type 2 diabetes mellitus: a value for money analysis. Diabetes Obes Metab. 2023;25(4):961-964. PubMed
Contributors: Calvin Young, Elizabeth Carson, Farhana Shivji
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for noncommercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca