CADTH Health Technology Review
Budesonide Extended Release for Ulcerative Colitis
Rapid Review
Authors: Sara D. Khangura, Carolyn Spry
Abbreviations
5-ASA
5-aminosalicylic acid
AE
adverse event
MA
meta-analysis
MMX
multi-matrix system
NMA
network meta-analysis
QALY
quality-adjusted life-year
RCT
randomized controlled trial
SR
systematic review
UC
ulcerative colitis
Key Messages
In 2017, the CADTH Canadian Drug Expert Committee recommended that budesonide extended release (with multi-matrix system) not be reimbursed for the induction of remission in patients with active mild to moderate ulcerative colitis based on limitations in the evidence at that time.
The limited primary clinical evidence (i.e., 1 randomized controlled trial) published since the literature searches conducted for the previous CADTH Reimbursement Review corroborates the clinical findings of that report. The evidence demonstrates that budesonide extended release is more effective for inducing remission in patients with mild to moderate ulcerative colitis compared to placebo.
No new clinical evidence was identified describing head-to-head comparisons of budesonide extended release with active therapies. Indirect comparative evidence between budesonide extended release and other active therapies suggests minimal or no difference in remission, clinical response, or adverse events.
Cost-effectiveness evidence from 1 study conducted in the Netherlands indicates that budesonide extended release is a more effective and less costly second-line therapy versus aggregated comparators for patients with mild to moderate ulcerative colitis.
Evidence-based recommendations support the use of budesonide extended release for patients with mild to moderate ulcerative colitis who have not responded to 5-ASAs.
No clinical or cost-effectiveness evidence or evidence-based recommendations were found describing the use of budesonide extended release in patients with moderate to severe ulcerative colitis.
Context and Policy Issues
Ulcerative colitis (UC) is a form of irritable bowel syndrome.1,2 UC is an immune-mediated, chronic illness that affects the rectum and can extend into the colon causing diarrhea, abdominal pain, and bowel frequency.3-5 Active UC is categorized as mild, moderate, or severe depending on the extent to which the colon is involved and the severity of the symptoms of the disease.3,6 The severity of the disease often worsens; it has been estimated that more than half of patients develop disease progression over time.5 UC can also increase the risk of developing colorectal cancer.2,4,5
The prevalence of UC has been estimated at 249 cases per 100,000 people in North America and 505 cases per 100,000 people in Europe.7 Canada has reported some of the highest estimates; in 2018, it was estimated that 120,000 people in Canada were affected.8 UC is usually characterized by flares of illness and periods of remission, with active periods causing deleterious effects on quality of life and productivity,3,9 or more severe outcomes, including hospitalization or death.10 The burden to patients on quality of life is exacerbated by the costs incurred by the disease. One estimate from the US was that the direct costs of treating UC each year were in the billions of dollars in addition to indirect costs, such as loss of productivity.7
The primary goal of treatment for UC is to control disease flares and induce remission, with an aim of maintaining remission over the long-term.2,11 Remission and response to therapy can be measured clinically or endoscopically. A recent focus has been on the importance of endoscopic measurement of mucosal healing due to its association with improved patient outcomes.12 The most common and/or recommended first-line therapy for UC are 5-aminosalicylic acids (5-ASAs), such as mesalamine .3,4,6,7,13,14 Some patients remain refractory to first-line therapy with 5-ASAs and require additional therapeutic options.2 For disease that is refractory to 5-ASAs, systemic corticosteroids, such as prednisolone, are often used.3,9,11 However, systemic corticosteroids can cause side effects, including headache, pain, nausea and/or vomiting, skin rash, and others15 that can be disruptive to daily life, so systemic corticosteroids are tapered in the maintenance phase of the disease.3,6,9,16 Adherence to treatment has also been highlighted as a potential barrier to the effectiveness of treatment, with multiple doses per day and burdensome treatment regimens (including administration both orally and rectally) affecting adherence to therapy.3,5,15
Budesonide delayed and extended release is an oral corticosteroid. It uses a multi-matrix system (MMX) technology, which ensures the tablet remains intact through the stomach and small intestine, releasing the drug throughout the colon.5,7,14,17 The delayed-release property of budesonide MMX distinguishes it from other formulations of budesonide, which are available in either rectal or systemic formulations. Some systemic formulations release the drug starting in the small intestines.18 Budesonide MMX has been described as 1 of several second-line therapies that can be used in patients who are refractory to 5-ASA therapy.11 In comparison to other systemic corticosteroids, budesonide MMX acts locally and has low systemic absorption, which may minimize side effects.3,4,6,9,11,13 The efficacy and safety of budesonide MMX has been assessed in 2 double-blind, placebo-controlled randomized controlled trials (RCTs) (the CORE I and CORE II studies) in patients with mild to moderate UC, demonstrating both efficacy and safety for induction of remission.7,14 However, longer-term use of corticosteroids — including budesonide MMX — for maintenance therapy following remission in UC has been discouraged due to the risk of glucocorticoid-related side effects.2
Based on a CADTH Reimbursement Review clinical report published in 2017,1 the CADTH Canadian Drug Expert Committee (CDEC) recommended that budesonide MMX not be reimbursed for the induction of remission in patients with active mild to moderate UC.19 Specifically, the lack of head-to-head and sufficiently powered evidence describing the efficacy and safety of budesonide MMX versus active comparators was highlighted as an important limitation of the evidence.19 This Rapid Review aims to identify and summarize recent clinical and cost-effectiveness evidence and guidelines regarding the use of budesonide MMX for patients with UC.
Research Questions
What is the clinical effectiveness of budesonide delayed and extended release for the induction of remission in patients with active mild to moderate UC?
What is the clinical effectiveness of budesonide delayed and extended release for the induction of remission in patients with active moderate to severe UC?
What is the cost-effectiveness of budesonide delayed and extended release for the induction of remission in patients with active mild to moderate UC?
What is the cost-effectiveness of budesonide delayed and extended release for the induction of remission in patients with active moderate to severe UC?
What are the evidence-based guidelines regarding the use of budesonide delayed and extended release for the induction of remission in patients with active mild, moderate, or severe UC?
Methods
Literature Search Methods
An information specialist conducted a literature search on key resources including MEDLINE, Embase, the Cochrane Database of Systematic Reviews, the International HTA Database, the websites of Canadian and major international health technology agencies, and a focused internet search. The search approach was customized to retrieve a limited set of results, balancing comprehensiveness with relevancy. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. Search concepts were developed based on the elements of the research questions and selection criteria. The main search concepts were Cortiment, budesonide, and ulcerative colitis. The search was completed on August 4, 2023, and limited to English-language documents published since January 1, 2016.
Selection Criteria and Methods
One reviewer screened citations and selected sources. In the first level of screening, titles and abstracts were reviewed and potentially relevant sources were retrieved and assessed for eligibility. The final selection of full-text sources was based on the inclusion criteria presented in Table 1.
Criteria | Description |
|---|---|
Population | Q1, Q3, Q5: Patients with active mild to moderate ulcerative colitis Q2, Q4, Q5: Patients with active moderate to severe ulcerative colitis |
Intervention | Budesonide delayed and extended releasea |
Comparator | Q1 to Q4: 5-aminosalicylates (e.g., mesalamine, olsalazine, sulfasalazine); corticosteroids (e.g., prednisone, hydrocortisone, betamethasone, other budesonide formulations), immunomodulators (e.g., thiopurines, methotrexate, JAK inhibitors), biologics (e.g., adalimumab, golimumab, infliximab, vedolizumab); placebo Q5: Not applicable |
Outcomes | Q1 and Q2: Clinical benefits (e.g., clinical and endoscopic remission, clinical and endoscopic response, health-related quality of life, function, disability, mucosal healing) and harms (e.g., adverse events, mortality) Q3 and Q4: Cost-effectiveness (e.g., cost per quality-adjusted life-year gained) Q5: Recommendations regarding best practices (e.g., appropriate patient populations, treatment protocols, contraindications) |
Study designs | Health technology assessments, systematic reviews, randomized controlled trials, nonrandomized studies, economic evaluations, evidence-based guidelines |
JAK = Janus kinase.
aBudesonide delayed and extended release is commonly known as budesonide multi-matrix system (MMX).
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, were duplicate publications, were summarized in the previous CADTH Reimbursement Review,1,19 or were published before January 2016. Systematic reviews (SRs) in which all relevant studies were captured in other more recent or more comprehensive SRs or meta-analyses (MAs) were excluded. Primary studies retrieved by the search were excluded if they were captured in 1 or more included SRs or MAs. In addition, SRs, MAs, network meta-analyses (NMAs), and primary studies that contained only clinical data already summarized in the previous CADTH report presenting evidence on budesonide extended release for UC1 were excluded. Guidelines with unclear methodology were also excluded.
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the following tools as a guide: the Questionnaire to assess the relevance and credibility of a network meta-analysis20 for NMAs, the Downs and Black checklist21 for randomized and nonrandomized studies, the Drummond checklist22 for economic evaluations, and the Appraisal of Guidelines for Research and Evaluation (AGREE) II instrument23 for guidelines. Summary scores were not calculated for the included studies; rather, the strengths and limitations of each included publication were described narratively.
Summary of Evidence
Quantity of Research Available
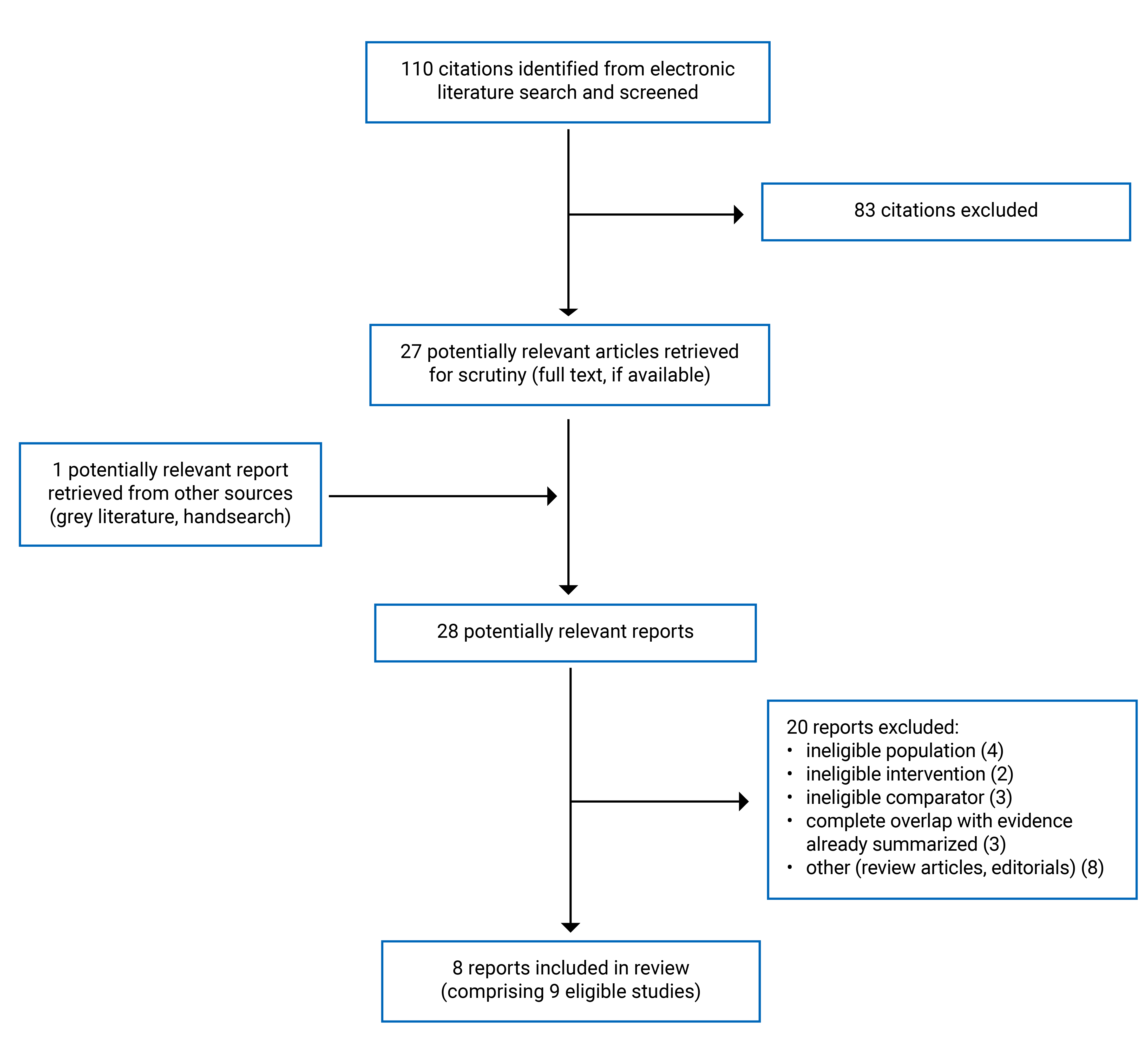
A total of 110 citations were identified in the electronic literature database search. Following screening of titles and abstracts, 83 citations were excluded, and 27 potentially relevant reports were retrieved for full-text review. One potentially relevant publication was retrieved from the grey literature search for full-text review. Of these potentially relevant articles, 20 publications were excluded for various reasons, and 8 publications met the inclusion criteria (comprising 9 eligible studies; 1 report described both an NMA and a cost-effectiveness study) and were included in this report. These comprised 3 NMAs,24-26 1 RCT,27 1 cost-effectiveness study,25 and 4 evidence-based guidelines.28-31 Figure 1 presents the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses)32 flow diagram of the study selection.
Additional references of potential interest are provided in Appendix 5.
Summary of Study Characteristics
This review identified 3 NMAs24-26 and 1 RCT27 that presented data of relevance to research question 1, 1 cost-effectiveness study25 with data of relevance to research question 3, and 4 evidence-based guidelines28-31 with information of relevance to research question 5. One of the NMAs was conducted and reported as part of an economic evaluation;25 the clinical and cost-effectiveness findings were described within the same report and are summarized separately in this report.
The 3 NMAs included data about budesonide MMX from the CORE I and CORE II studies, which compared budesonide MMX with placebo and were previously summarized in a CADTH Reimbursement Review.1 Although the 3 NMAs included comparators that were eligible for this report, they also included additional network comparisons beyond those of interest to this review.24-26 Specifically, 1 NMA included comparisons between different doses of mesalamine and placebo24 and another NMA included comparisons between various types of 5-ASAs, controlled, ileal-release budesonide and placebo.26 One of the NMAs reported on a comparison of budesonide MMX with budesonide 9 mg/day (i.e., Entocort);25 however, these data were described in the previous CADTH Reimbursement Review on this topic1 and are not resummarized in this report. Only the relevant comparisons not previously summarized are described further in this report.
Study Design
All 3 NMAs specified the use of SR to inform their findings.24-26 Two of the NMAs used a frequentist analytical approach,24,26 whereas 1 reported the use of a Bayesian method.25 For the NMA describing a Bayesian analytical approach, the use of flat (or uninformative) priors was reported.25 One NMA incorporated data from 15 RCTs with 4 network comparators,24 another synthesized data from 5 RCTs with 5 network comparators,25 and the other NMA included 75 RCTs describing 9 network comparators.26
The included RCT report was published in 201727 and used a multicentre, double-blind design. This study was also referenced in the previous CADTH Reimbursement Review but was not summarized in detail in that report because it was only available as an abstract at that time.1
The 2018 cost-effectiveness evaluation used a societal perspective across a 5-year time horizon with clinical inputs informed by published clinical sources as well as the NMA summarized in this report.25 Cost data were taken from sources specific to the Netherlands.25 An 8-state Markov model with various health and treatment states, which included budesonide MMX, other lines of therapy, remission, and death.25
Four evidence-based guidelines were identified. One was from the European Crohn’s and Colitis Organisation (ECCO)28 and 1 was from the Pan American Crohn’s and Colitis Organisation (PANCCO),29 both published in 2022.28,29 Two other evidence-based guidelines were identified, 1 from the American College of Gastroenterology30 and 1 from the British Society of Gastroenterology,31 both published in 2019.30,31 Three of the evidence-based guidelines clearly reported the use of SR to synthesize evidence informing development of the guideline,28,29,31 whereas 1 described evidence but did not clearly report the methods used for evidence assembly and/or synthesis.30 All 4 of the evidence-based guidelines reported the use of Grading of Recommendations, Assessment, Development, and Evaluations (GRADE) for rating the quality of the evidence used to develop recommendations and included information on the strength of each recommendation.28-31 Three of the evidence-based guidelines clearly reported a consensus-based process for drafting recommendations,28,29,31 while 1 did not.30
Country of Origin
The first authors of the NMAs were based in Italy,24 France,25 and the US.26 The included RCT was multinational and multicentre, with study centres in Canada, the US, and Europe.27 The economic evaluation produced cost-effectiveness estimates specific to the Netherlands.25 The evidence-based guidelines did not specify the jurisdictions to which they are intended to be applied,28-31 although ECCO is based in Europe, PANCCO comprises South American countries, the American College of Gastroenterology is based in the US, and the British Society of Gastroenterology is based in the UK.
Patient Population
All of the included studies reporting on clinical and cost-effectiveness24-27 specified a focus on patients with mild to moderate UC.
Of the included guidelines, 2 were focused on patients with mild, moderate, or severe UC,28,30 1 stated a focus on UC without specifying disease severity,29 and 1 was general to inflammatory bowel disease (including patients with UC)31 although all recommendations of relevance to this report were specific to patients with mild to moderate disease.28-31 Intended users of the included evidence-based guidelines were specified as clinicians and health care providers by 2 guidelines,28,31 and were not clearly stated by the other 2 guidelines.29,30
Interventions and Comparators
All the included sources described data and information addressing the use of budesonide MMX.24-31 Two NMAs,24,25 1 RCT,27 the cost-effectiveness study,25 and 1 evidence-based guideline30 specified a focus on the use of budesonide MMX at a dose of 9 mg/day, whereas 1 NMA,26 and 3 guidelines28,29,31 did not report the dose or scheduling of interest. In addition, the RCT specified that budesonide MMX or placebo was added to existing oral mesalamine therapy, which was being administered at baseline.27
Comparators described within the clinical and cost-effectiveness studies included 5-ASAs (i.e., mesalamine, sulfasalazine, olsalazine, balsalazide, or not reported),24,26 corticosteroids (i.e., prednisolone, other formulations of budesonide),25,26 and placebo.24,25,27 Another NMA also reported data on a placebo as a comparator for budesonide MMX;26 however, these data were based only on studies previously reviewed by CADTH,1 and were not included or summarized again in this report.
Outcomes
All 4 studies reporting on clinical effectiveness incorporated data on the clinical benefits of budesonide MMX,24-27 3 of which included data on induction of remission.24-27 Induction of remission was specified as clinical and/or endoscopic, with 3 studies presenting a composite outcome describing both clinical and endoscopic remission,24,25,27 3 studies presenting data on clinical remission only,25-27 and 2 studies describing endoscopic remission only.26,27 Other outcomes describing clinical benefit included histologic healing, clinical improvement (including measures of stool frequency, rectal bleeding, appearance of mucosa on sigmoidoscopy, and physician’s disease severity assessment), and quality of life.27
Three of the studies reporting on clinical effectiveness incorporated data on the clinical harms of budesonide MMX,24,26,27 including treatment discontinuation and/or study withdrawal,24,26 adverse events (AEs),27 and serious AEs.24
The economic evaluation reported on mean costs in euros, mean quality-adjusted life-years (QALYs) gained, and incremental cost-effectiveness ratios, expressed as euros per QALY gained.25
The evidence-based guidelines made recommendations about the induction of remission.
Additional details about the included publications are provided in Appendix 2.
Summary of Critical Appraisal
Network Meta-Analyses
The included NMAs described populations, interventions, outcomes, and context relevant and applicable to the current review. The trials included connected networks of RCTs, which were displayed using graphical representations.24-26 The SR methods were appropriate in 2 of the NMAs, including information describing appropriate searches and selection criteria,24,26 whereas 1 NMA did not describe the SR methods in detail (i.e., a reference to a systematic literature search was reported with no detail provided about the methods for the search, although study selection criteria were provided).25 Authors of all 3 NMAs described assessment of inconsistency, reporting that no or very little inconsistency between direct and indirect comparisons was present. However, none of the articles included data from the findings of their assessments.24-26 Potential conflicts of interest were included in all 3 reports, yet none of the NMA reports discussed the potential effects of these conflicts of interest on the findings of the studies.24-26 Conclusions were generally fair and balanced, reflecting the findings as described.24-26
Limitations of the NMAs included several single-study connections, lack of clarity concerning the extent to which bias may have influenced the findings, with some trials demonstrating unclear risk of bias in 2 NMAs24,26 and no description of an assessment of risk of bias in 1 NMA.25 The 3 NMAs did not provide a clear rationale for selection of the modelling methods used (i.e., fixed versus random effects), did not report individual study results, or report the findings of both direct and indirect effect estimates.24-26 Although a description of the assessment of heterogeneity was provided in 2 NMAs,24,26 1 NMA did not describe an assessment of heterogeneity.25 All 3 NMAs acknowledged that heterogeneity between RCTs included in their analyses could limit their findings (including variable definitions and/or measurement of outcomes), although none were specific about how these limitations might impact the interpretation of findings.24-26 Finally, none of the 3 NMAs made it clear whether statistical methods to preserve within-study randomization were used.24-26 This could represent a major limitation of the analyses in the event that naive, indirect comparisons that fail to account for treatment effects across studies were made.20
Primary Clinical Study
The RCT clearly reported the study objectives, patient characteristics, main outcomes, findings, and AEs.27 External validity may have been supported by a multinational, multicentre design in the RCT, although it was unclear whether the study centres and health care facilities were representative of those used in the general population.27 Methods to support internal validity were generally robust in the RCT, with a randomized, double-blind design, statistical methods to account for losses to follow-up, study withdrawals and missing data for the remission outcome (i.e., imputation using a worst case scenario, in which missing data were considered to be nonresponse), and the use of valid, reliable outcome measures.27 A power calculation specific to remission as an end point was reported by the authors of the RCT. Although the study did not retain the predicted necessary number of patients to inform the efficacy analyses, statistically significant between-group differences were observed for the primary end point.27
Economic Evaluation
The economic evaluation provided a clear description of its research objectives, viewpoint, appropriate rationale for the choice of comparators (i.e., in accordance with Dutch clinical practice and guidance), outcomes, and appropriate sources for clinical and cost data (i.e., published clinical data and findings from the supporting NMA).25 Key methods were reported clearly, including details of the modelling used and sensitivity analyses undertaken.25 Limitations included limited information on patients from whom valuations were obtained, and a lack of confidence intervals for main outcome data. Importantly, data for comparators (i.e., alternative formulations of budesonide) were also presented aggregately,25 preventing the reader from understanding the comparative cost-effectiveness of budesonide MMX with individual comparators.
Evidence-Based Guidelines
The scope and purpose of the 4 evidence-based guidelines were clearly described.28-31 Stakeholder involvement was clear and robust in 1 guideline,31 although 2 guidelines did not clearly describe the composition of the guideline development groups28,30 and 1 did not explicitly describe the involvement of patients or the public.29 The rigour of development was generally robust for 3 of the included guidelines.28,29,31 One guideline did not clearly describe systematic methods for evidence assembly, methods for developing recommendations, external review, or a procedure for updating the guideline.30 Three of the included guidelines demonstrated clear presentation of recommendations,28,30,31 whereas 1 guideline made reference to the strength of the recommendation being conditional on the strategy used, but did not make clear which strategies they were referring to.29 One guideline provided resources to support application of the guideline in practice,28 while the remaining 3 did not.29-31 Editorial independence was clearly demonstrated in 3 of the guidelines,28,29,31 but was not clear in 1 guideline.30
Additional details regarding the strengths and limitations of included publications are provided in Appendix 3.
Summary of Findings
This Rapid Review identified 3 NMAs24-26 and 1 RCT27 presenting findings regarding the clinical effectiveness of budesonide MMX for the induction of remission in patients with mild to moderate UC. All data describing budesonide MMX in the 3 NMAs were derived from the CORE I and CORE II studies, which compared budesonide MMX with placebo and were previously summarized in a CADTH Reimbursement Review.1
One economic evaluation25 about the cost-effectiveness of budesonide MMX for induction of remission in patients with mild to moderate UC, and 4 evidence-based guidelines28-31 regarding the use of budesonide MMX for the management of UC were identified.
Appendix 4 presents the main study findings.
Clinical Effectiveness in Patients With Active Mild to Moderate UC
The clinical evidence indicated that treatment with budesonide MMX demonstrated a benefit in terms of remission and clinical response compared to placebo in patients with mild to moderate UC. However, indirect comparisons between budesonide MMX and other active comparators did not clearly demonstrate a difference favouring 1 treatment. In terms of quality of life and AEs, no consistent differences between budesonide MMX and placebo were observed. Indirect comparisons between treatment with budesonide MMX and other active therapies also did not demonstrate a clear or consistent difference in AEs.
Detailed data can be found in Table 10.
Induction of Remission
Clinical and Endoscopic Remission (Composite Measure)
Two studies (1 NMA and 1 RCT) reported on a composite measure of clinical and endoscopic remission,24,27 with both describing a comparison of treatment with budesonide MMX versus placebo.24,27 The NMA also reported on a comparison with both low-dose and high-dose mesalamine.24
One NMA and 1 RCT reported a statistically significant benefit of treatment with budesonide MMX compared with placebo for the induction of clinical and endoscopic remission.24,27
One NMA reported no statistically significant difference between treatment with budesonide MMX and either low-dose or high-dose mesalamine for the induction of clinical and endoscopic remission.24
Clinical Remission
Three studies (2 NMAs and 1 RCT) reported on clinical remission. One NMA and 1 RCT described the odds or probability of clinical remission of treatment with budesonide MMX versus placebo,25,27 1 NMA described the odds of clinical remission of treatment with budesonide MMX versus 5-ASAs (including oral and topical diazo-bonded mesalamine and sulfasalazine),26 and 2 NMAs described the odds of clinical remission of treatment with budesonide MMX compared with other formulations of budesonide.25,26
The NMA reported the odds of clinical remission favoured treatment with budesonide MMX compared with placebo,25 whereas the RCT reported no statistically significant difference between treatment groups in the probability of clinical remission.27
One NMA reported no statistically significant differences between treatment groups in the odds of clinical remission compared with 5-ASAs (i.e., oral and topical diazo-bonded mesalamine). However, a statistically significant benefit of treatment with budesonide MMX was reported compared with sulfasalazine.26
Two NMAs reported no significant difference in the odds of clinical remission between treatment groups compared with other formulations of budesonide.25,26
Endoscopic Remission
Two studies (1 NMA and 1 RCT) reported on endoscopic remission. The RCT described the probability of endoscopic remission of treatment with budesonide MMX versus placebo,27 and the NMA described the odds of endoscopic remission of treatment with budesonide MMX versus 5-ASAs (including oral and topical diazo-bonded mesalamine and sulfasalazine) and controlled ileal-release budesonide.26
The RCT reported a statistically significant benefit of treatment with budesonide MMX in the probability of endoscopic remission compared with placebo.27
The NMA reported no statistically significant difference in the odds of endoscopic remission compared with 5-ASAs (oral and topical diazo-bonded mesalamine and sulfasalazine) and controlled ileal-release budesonide.26
Clinical and/or Endoscopic Response
Outcomes describing clinical and/or endoscopic response were reported in the RCT, which described treatment with budesonide MMX compared to placebo. A statistically significant improvement favouring budesonide MMX was found in histologic healing, whereas there was no statistically significant difference between treatment groups in clinical improvement at 8 weeks of follow-up.27 Detailed data can be found in Table 11.
Quality of Life
One RCT described quality of life and found no statistically significant difference between treatment with budesonide MMX and placebo at 2 and 8 weeks of follow-up. A statistically significant benefit of treatment with budesonide MMX at 4 weeks of follow-up was reported27 (no information on minimally importance difference was reported). Detailed data can be found in Table 12.
Adverse Events
Three studies reported on AEs.24,26,27 One NMA and 1 RCT described a comparison between treatment with budesonide MMX and placebo,24,27 2 NMAs reported on treatment with budesonide MMX versus 5-ASAs (i.e., mesalamine, sulfasalazine, diazo-bonded and oral and topical 5-ASAs),24,26 and 1 NMA described comparisons between treatment with budesonide MMX and other corticosteroids (i.e., ileal-release budesonide and prednisolone).26 Detailed data can be found in Table 13.
Compared with placebo:
One NMA found no statistically significant differences in serious AEs, treatment discontinuation, or study withdrawal between treatment with budesonide MMX and placebo.24
The RCT did not report any comparative statistics for AEs between the number of patients who received budesonide MMX or placebo and concluded that “adverse events rates were similar” (p. 785)27 (there were more AEs in the budesonide MMX group).
Compared with 5-ASAs:
One NMA found no statistically significant differences in the odds of patients experiencing a serious AE between treatment with budesonide MMX and low-dose or high-dose mesalamine.24
Two NMAs found that the odds of drug discontinuation, treatment discontinuation, or study withdrawal were statistically significantly higher in patients receiving budesonide MMX compared with diazo-bonded 5-ASAs, or standard-dose or high-dose mesalamine.24,26
Two NMAs found no difference in the odds of drug discontinuation, treatment discontinuation, or study withdrawal in patients who received budesonide MMX versus oral and topical 5-ASAs, low-dose mesalamine, or sulfasalazine.24,26
Compared with other corticosteroids:
No statistically significant differences were found in drug discontinuation (1 NMA comparing treatment with budesonide MMX and controlled ileal-release budesonide).26
Clinical Effectiveness in Patients With Active Moderate to Severe UC
No relevant evidence specific to active moderate to severe UC was identified; therefore, no summary can be provided.
Cost-Effectiveness in Patients With Active Mild to Moderate UC
The base-case analysis indicated a benefit of budesonide, with a mean gain of 0.009 QALYs, which the authors attributed to the higher remission rates with budesonide MMX versus the comparators (i.e., alternative formulations of budesonide). The incremental cost-effectiveness ratios value was not reported, although the authors indicated that budesonide MMX was dominant (i.e., less costly and more effective).25 One-way deterministic and probabilistic sensitivity and scenario analyses produced similar findings, with budesonide MMX demonstrating dominant cost-effectiveness versus most comparators for risk of relapse, hospitalization, surgery, AE costs, mortality, type of treatment, indirect costs, and disease type.25
Detailed findings are presented in Table 14.
Cost-Effectiveness in Patients With Active Moderate to Severe UC
No relevant evidence specific to active moderate to severe UC was identified; therefore, no summary can be provided.
Evidence-Based Guidelines in Patients With Active Mild, Moderate, or Severe UC
Three of the 4 identified evidence-based guidelines make specific recommendations in favour of budesonide MMX for induction of remission in patients with mild or mild to moderately active UC.29-31 One generalizes the recommendation to colonic-release corticosteroids, but references supporting evidence specific to budesonide MMX.28
Of the 3 evidence-based guidelines with recommendations specific to budesonide MMX, 1 includes an associated good practice point that suggests that budesonide MMX be initiated following nonresponse to 5-ASAs, and administered daily at a dose of 9 mg for an 8-week course of therapy.29 Similarly, another evidence-based guideline specifies within the relevant recommendations that budesonide MMX at a dose of 9 mg/day be provided to patients with mild to moderate UC who are nonresponsive to 5-ASAs, with an additional recommendation particular to moderate UC that does not specify whether budesonide MMX should be used as first- or second-line therapy or what the dose or scheduling should be.30 The third evidence-based guideline also indicates that patients who are nonresponsive to 5-ASAs should receive budesonide MMX if they choose not to take systemic corticosteroids (i.e., prednisolone), although the recommendation does not specify dosing or scheduling.31
All the evidence sources referenced in support of the recommendations made in the 4 evidence-based guidelines28-31 were either summarized in the previous CADTH Reimbursement Review (except 1 study which was excluded from the previous CADTH review)1 or summarized in this report (i.e., the included RCT).27 Two of the evidence-based guidelines indicate the quality of evidence informing their recommendations is moderate and that the recommendations are strong.30,31 Another evidence-based guideline indicates that the evidence informing their recommendation is of high quality, but that the recommendation is conditional on the strategy used (however, these strategies are not clear).29 Finally, the recommendation that was general to colonic-release corticosteroids was characterized as weak and described as being based on a low quality of evidence.28
Recommendations specific to the use of budesonide MMX for severe UC were not identified.
A detailed summary of recommendations is presented in Table 15.
Limitations
Since CADTH’s Reimbursement Review in 2017,1 all direct comparative evidence and recommendations identified by this review described budesonide MMX compared with placebo and most was generated from the CORE I and CORE II studies (which were previously reviewed by CADTH).1 As summarized previously, the CORE I and CORE II studies demonstrated some methodological limitations, including high rates of treatment discontinuation, potential loss of randomization due to exclusion of patients from the intention-to-treat analyses, the observed placebo effects, and insufficient power of both studies to compare budesonide MMX with active treatment arms (i.e., mesalamine and Entocort, respectively).1
No evidence was identified to answer the research questions posed in this report specific to moderate to severe UC. Consequently, no information could be summarized. Similarly, the relevant recommendations made in the evidence-based guidelines identified and summarized in this report were limited to mild to moderate UC.28-31 The potential for overlap in the definitions of mild to moderate and moderate to severe disease was highlighted in 1 of the guidelines included in this review, and has been described as a limitation of the literature describing this topic.28
CADTH summarized evidence comparing budesonide MMX with placebo previously1 and additional primary evidence from 1 RCT describing this comparison was summarized in this report.27 No primary, novel, or direct evidence describing comparisons of budesonide MMX with other active treatments was identified by this review. Indirect comparisons between budesonide MMX and other active therapies (i.e., 5-ASAs and other corticosteroids, including high-dose corticosteroids) were reported by the 3 NMAs summarized in this report.24-26 Methodological limitations of these studies warrant caution in the interpretation of their findings. Although the cost-effectiveness study included immunomodulators and biologics as third- and fourth-line therapies in their Markov model (i.e., 1 drug from each class) no evidence or information was identified comparing budesonide MMX with immunomodulators and biologics. This represents a current gap in the evidence base. Similarly, the evidence upon which the recommendations from the 4 included evidence-based guidelines are based was generated using placebo as the comparator to budesonide MMX,28-31 which limits their applicability for decision-making about the use of budesonide MMX compared with other active therapies.
Most of the clinical evidence and information identified was particular to the induction of remission,24-31 with 1 RCT describing other outcomes, such as clinical response and quality of life.27 Additional studies describing these and a broader range of outcomes (e.g., function, disability) would provide a more complete picture of the clinical effectiveness of budesonide MMX.
Cost-effectiveness data were also limited. One study used clinical data on budesonide MMX from the CORE I and II trials, which have been summarized previously,1 including methodological limitations that could affect the integrity of the model. Further, the economic evaluation was conducted in the Netherlands25 and may be limited in its generalizability to the Canadian context. Although the RCT reported the recruitment of patients in Canada (but did not report the number of centres or patients),27 the other studies and guidelines identified and summarized in this report were not specific to the Canadian context. This lack of data and recommendations specific to the Canadian population may limit generalizability within Canada.
Although there was considerable overlap in the evidence cited to support the recommendations made in the evidence-based guidelines, there was variation observed in the judgments made concerning quality of evidence and strength of recommendations.28-31 The source of this variability was not clear. It could represent differences in the methods used to assess the evidence by the various guideline development groups, although the actual reason for the observed variability is unclear.
This report simplified elements of the SR process by following Rapid Review methods (i.e., limited search strategy, the use of a single reviewer), which is distinct from CADTH Reimbursement Reviews, which rely on formal SR methodology. This report does not replace or formally update the previous CADTH Reimbursement Review.
Conclusions and Implications for Decision- or Policy-Making
This report identified evidence and information that was published since the 2017 CADTH Reimbursement Review and related CDEC recommendation against the reimbursement of budesonide MMX.1,19 The evidence and information included 3 NMAs,24-26 1 RCT,27 1 cost-effectiveness study, and 4 evidence-based guidelines28-31 that described data and recommendations specific to mild to moderate UC. No evidence was found about the effect of budesonide MMX in moderate to severe UC. Although the evidence identified in this review is limited to mild to moderate disease, the role of budesonide MMX for more severe forms of UC or across the course of the disease remains uncertain and has been questioned in the literature (e.g., is there a role for budesonide MMX as first-line therapy or in the maintenance of remission?).13 Additional research is also needed to clarify the potential role of budesonide MMX in longer-term therapy (i.e., for maintenance of remission).6,11
Data describing the clinical effectiveness of budesonide MMX compared with placebo remain consistent with the previous CADTH Reimbursement Review.1 The 1 RCT27 and 2 NMAs (which relied primarily on the CORE I and II trials)24,25 reported statistically significant improvement in clinical and/or endoscopic remission in patients receiving budesonide MMX.24,25,27 Similarly, the RCT summarized in this report found no statistically significant difference in clinical improvement or consistent difference in quality of life between budesonide MMX and placebo,27 which is consistent with the previous CADTH report.1 One finding from the RCT summarized in this report that differed from the findings describing the CORE I study in the previous CADTH report was histologic healing. The previous CADTH report found no difference between budesonide MMX and placebo as reported in CORE I,1 but the RCT from this report found a statistically significant benefit of budesonide MMX.27 The previous CADTH report did describe a statistically significant benefit of budesonide MMX for histologic healing in the CORE II study.1 In addition, the RCT summarized in this report added budesonide MMX to concomitant mesalamine, unlike the CORE I and CORE II studies summarized previously, which did not allow for concomitant use of mesalamine.1 It is not clear whether this or other possible differences between the studies may or may not account for the difference observed in histologic healing with the findings of from the CORE I study. Of relevance to this outcome, there is commentary in the literature describing an evolution of the goals of treatment for UC, with priorities shifting toward histologic and endoscopic healing3,10,33 as evidence builds to demonstrate their positive impact on such downstream outcomes as disease flares and hospitalizations.7 The potential for these outcomes to be prioritized could affect the way evidence is produced and/or treatments are assessed, provided, and sequenced.
No primary data or direct comparisons comparing budesonide MMX with other active therapies were identified in this review, which corroborates the findings of the previous CADTH report.1 The current lack of head-to-head comparative data between budesonide MMX and other active therapies has also been highlighted in the literature as a gap in the evidence.13 Most indirect comparisons between budesonide MMX and other therapies (i.e., 5-ASAs and other corticosteroids, including high-dose corticosteroids) indicated no statistically significant difference between treatment groups for induction of remission.24-26 Some indirect comparisons with 5-ASAs indicated statistically significantly fewer treatment discontinuations or study withdrawals with 5-ASAs compared with budesonide MMX.24,26 The lack of any comparative clinical evidence between budesonide MMX and immunomodulators or biologics has also been highlighted in the literature as an opportunity for further exploration in the treatment of UC.6,10,11
Cost-effectiveness data were also limited. One study specific to the Netherlands indicated dominant cost-effectiveness of budesonide MMX as a second-line therapy versus aggregated comparators.25 The authors highlighted the comparable (or marginally higher) gains in QALYs with lower costs as the drivers of cost-effectiveness in most of the analyses.25 These findings are consistent with CADTH’s previous pharmacoeconomic assessment of budesonide MMX, which used similar clinical outputs from CORE I and II, and also highlighted important limitations (i.e., a lack of direct comparative clinical evidence between budesonide MMX and active comparators).34 Recently published evidence-based guidelines made recommendations that generally favour the use of budesonide MMX — often as second-line therapy — in mild to moderate UC. However, these recommendations were based on evidence that was limited to comparisons of budesonide MMX with placebo.28-31
Limited data describing patient-oriented outcomes is also an opportunity for additional research on this topic. For instance, burdensome first-line treatment regimens for UC, with multiple doses per day, have been identified as a potential barrier for patient adherence to therapy.3,5 Budesonide MMX, with its once-daily oral administration, may offer patient-oriented benefits to those living with UC.4 The importance of a once-daily formula that requires less time and vigilance for patients than more frequently dosed formulations, as well as relative tolerability, may benefit patient preference and satisfaction, potentially improving treatment adherence, patient quality of life, and costs to health systems.7 Nonetheless, these potential benefits have yet to be supported by high-quality data.5
In conclusion, CADTH recommended against the reimbursement of budesonide MMX for mild to moderate UC in 2017. This was largely due to the lack of direct comparative evidence with other active therapies.19 Similarly, this review did not identify evidence describing direct comparisons of budesonide MMX with other active therapies. Further research is needed to evaluate the role of budesonide MMX in treating moderate to severe UC and its cost-effectiveness specific to the Canadian context. Decision-makers may also consider patient preferences and the potential benefits related to budesonide MMX’s once-daily oral administration.
References
1.Budesonide. CADTH Common Drug Review. Ottawa (ON): CADTH; 2017: https://www.cadth.ca/budesonide. Accessed 2023 Sep 14.
2.Bezzio C, Festa S, Zerboni G, Papi C, Manes G, Saibeni S. A safety evaluation of budesonide MMX for the treatment of ulcerative colitis. Expert Opin Drug Saf. 2018;17(4):437-444. PubMed
3.Solitano V, D'Amico F, Fiorino G, Paridaens K, Peyrin-Biroulet L, Danese S. Key strategies to optimize outcomes in mild-to-moderate ulcerative colitis. J Clin Med. 2020;9(9):08.
4.Salice M, Rizzello F, Calabrese C, Privitera Hrustemovic H, Gionchetti P. Budesonide MMX: efficacy and safety profile in the treatment of ulcerative colitis. Expert Rev Gastroenterol Hepatol. 2019;13(7):607-613. PubMed
5.Bezzio C, Fasci-Spurio F, Vigano C, Meucci G, Papi C, Saibeni S. The problem of adherence to therapy in ulcerative colitis and the potential utility of multi-matrix system (MMX) technology. Expert Rev Gastroenterol Hepatol. 2017;11(1):33-41. PubMed
6.Cross RK. Safety considerations with the use of corticosteroids and biologic therapies in mild-to-moderate ulcerative colitis. Inflamm Bowel Dis. 2017;23(10):1689-1701. PubMed
7.Lichtenstein GR. Budesonide multi-matrix for the treatment of patients with ulcerative colitis. Dig Dis Sci. 2016;61(2):358-370. PubMed
8.Benchimol EI, Bernstein CN, Bitton A, et al. The impact of inflammatory bowel disease in Canada 2018: a scientific report from the Canadian Gastro-Intestinal Epidemiology Consortium to Crohn's and Colitis Canada. J Can Assoc Gastroenterol. 2019;2(Suppl 1):S1-S5. PubMed
9.Danese S, Hart A, Dignass A, et al. A multicentre prospective cohort study assessing the effectiveness of budesonide MMX® (Cortiment®MMX®) for active, mild-to-moderate ulcerative colitis. United European Gastroenterol J. 2019;7(9):1171-1182. PubMed
10.Salice M, Rizzello F, Calabrese C, Calandrini L, Gionchetti P. A current overview of corticosteroid use in active ulcerative colitis. Expert Rev Gastroenterol Hepatol. 2019;13(6):557-561. PubMed
11.Maconi G, Camatta D, Cannatelli R, Ferretti F, Carvalhas Gabrielli A, Ardizzone S. Budesonide MMX in the treatment of ulcerative colitis: current perspectives on efficacy and safety. Ther Clin Risk Manag. 2021;17:285-292. PubMed
12.Vuitton L, Peyrin-Biroulet L, Colombel JF, et al. Defining endoscopic response and remission in ulcerative colitis clinical trials: an international consensus. Aliment Pharmacol Ther. 2017;45(6):801-813. PubMed
13.Magro F, Estevinho MM. Moving from efficacy to effectiveness: budesonide multimatrix in ulcerative colitis. United European Gastroenterol J. 2019;7(9):1153-1155. PubMed
14.Danese S, Bonovas S, Peyrin-Biroulet L. Budesonide MMX add-on to 5-aminosalicylic acid therapy in mild-to-moderate ulcerative colitis: a favourable risk-benefit profile. J Crohns Colitis. 2017;11(7):767-768. PubMed
15.Mahadevan U. Medical treatment of ulcerative colitis. Clin Colon Rectal Surg. 2004;17(1):7-19. PubMed
16.Zeng J, Lv L, Mei ZC. Budesonide foam for mild to moderate distal ulcerative colitis: a systematic review and meta-analysis. J Gastroenterol Hepatol. 2017;32(3):558-566. PubMed
17.Kornbluth A. Budesonide extended-release in patients with mild to moderate ulcerative colitis. Gastroenterol Hepatol (N Y). 2015;11(1):56-58. PubMed
18.Abdalla MI, Herfarth H. Budesonide for the treatment of ulcerative colitis. Expert Opin Pharmacother. 2016;17(11):1549-1559. PubMed
19.Budesonide MMX. CADTH Canadian drug expert committee: final recommendation. Ottawa (ON): CADTH; 2017: https://www.cadth.ca/sites/default/files/cdr/complete/SR0491_complete_Cortiment-Mar-24-17.pdf. Accessed 2023 Sep 14.
20.Jansen JP, Trikalinos T, Cappelleri JC, et al. Indirect treatment comparison/network meta-analysis study questionnaire to assess relevance and credibility to inform health care decision making: an ISPOR-AMCP-NPC Good Practice Task Force report. Value Health. 2014;17(2):157-173. PubMed
21.Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377-384. PubMed
22.Higgins JPT, Green S, editors. Figure 15.5.a: Drummond checklist (Drummond 1996). Cochrane handbook for systematic reviews of interventions. London (GB): The Cochrane Collaboration; 2011: http://handbook-5-1.cochrane.org/chapter_15/figure_15_5_a_drummond_checklist_drummond_1996.htm. Accessed 2023 Sep 14.
23.Agree Next Steps Consortium. The AGREE II Instrument. [Hamilton, ON]: AGREE Enterprise; 2017: https://www.agreetrust.org/wp-content/uploads/2017/12/AGREE-II-Users-Manual-and-23-item-Instrument-2009-Update-2017.pdf. Accessed 2023 Sep 14.
24.Bonovas S, Nikolopoulos GK, Piovani D, et al. Comparative assessment of budesonide-MMX and mesalamine in active, mild-to-moderate ulcerative colitis: a systematic review and network meta-analysis. Br J Clin Pharmacol. 2019;85(10):2244-2254. PubMed
25.Gherardi A, Roze S, Kuijvenhoven J, Ghatnekar O, Yip Sonderegger YL. Budesonide with multi-matrix technology as second-line treatment for ulcerative colitis: evaluation of long-term cost-effectiveness in the Netherlands. J Med Econ. 2018;21(9):869-877. PubMed
26.Nguyen NH, Fumery M, Dulai PS, et al. Comparative efficacy and tolerability of pharmacological agents for management of mild to moderate ulcerative colitis: a systematic review and network meta-analyses. Lancet Gastroenterol Hepatol. 2018;3(11):742-753. PubMed
27.Rubin DT, Cohen RD, Sandborn WJ, et al. Budesonide multimatrix is efficacious for mesalamine-refractory, mild to moderate ulcerative colitis: a randomised, placebo-controlled trial. J Crohns Colitis. 2017;11(7):785-791. PubMed
28.Raine T, Bonovas S, Burisch J, et al. ECCO guidelines on therapeutics in ulcerative colitis: medical treatment. J Crohns Colitis. 2022;16(1):2-17. PubMed
29.Juliao-Banos F, Grillo-Ardila CF, Alfaro I, et al. Update of the PANCCO clinical practice guidelines for the treatment of ulcerative colitis in the adult population. Rev Gastroenterol Mex. 2022;87(3):342-361. PubMed
30.Rubin DT, Ananthakrishnan AN, Siegel CA, Sauer BG, Long MD. ACG clinical guideline: ulcerative colitis in adults. Am J Gastroenterol. 2019;114(3):384-413. PubMed
31.Lamb CA, Kennedy NA, Raine T, et al. British Society of Gastroenterology consensus guidelines on the management of inflammatory bowel disease in adults. Gut. 2019;68(Suppl 3):s1-s106. PubMed
32.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
33.Mendell A, Le K, Vannabouathong C, Mahood Q. An overview of emerging trends and technologies in ulcerative colitis. Can J Health Technol. 2023;3(7). https://www.cadth.ca/sites/default/files/hs-eh/EH0117_HS%20Trends%20Technologies%20in%20UC%20Final.pdf. Accessed 2023 Sep 13.
34.Budesonide (Cortiment MMX). CADTH Common Drug Review pharmacoeconomic report. Ottawa (ON): CADTH; 2017: https://www.cadth.ca/sites/default/files/cdr/pharmacoeconomic/SR0491_Cortiment_PE_Report.pdf. Accessed 2023 Sep 15.
35.Adalimumab (Humira): appendix 5 validity of outcome measures. CADTH clinical review report. Ottawa (ON): CADTH; 2016 Apr: Available from: https://www.ncbi.nlm.nih.gov/books/NBK539018/. Accessed 2023 Sep 6.
36.Schoepfer AM, Beglinger C, Straumann A, Trummler M, Renzulli P, Seibold F. Ulcerative colitis: Correlation of the rachmilewitz endoscopic activity index with fecal calprotectin, clinical activity,c-reactive protein, and blood leukocytes. Inflamm Bowel Dis. 2009;15(12):1851-1858. PubMed
37.Walmsley RS, Ayres RCS, Pounder RE, Allan RN. A simple clinical colitis activity index. Gut. 1998;43(1):29-32. PubMed
38.Sutherland LR, Martin F, Greer S, et al. 5-Aminosalicylic acid enema in the treatment of distal ulcerative colitis, proctosigmoiditis, and proctitis. Gastroenterology. 1987;92(6):1894-1898. PubMed
39.Budesonide (Cortiment MMX): appendix 5 validity of outcome measures. Ottawa (ON): CADTH; 2017: https://www.ncbi.nlm.nih.gov/books/NBK476229/. Accessed 2023 Sep 6.
40.Mitropoulou MA, Fradelos EC, Lee KY, et al. Quality of life in patients with inflammatory bowel disease: importance of psychological symptoms. Cureus. 2022;14(8):e28502. PubMed
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Table 2: Characteristics of Included Network Meta-Analyses
Study citation, country, funding source | Study designs and numbers of primary studies included | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Bonovas et al. (2019)24 Country: Italy Funding source: Individual authors report potential conflicts of interest in the form of funding received from NGO and pharmaceutical company sources | SR and NMA using a frequentist approach RCTs containing the intervention of interest and/or relevant comparator(s), n = 15 | Adults (> 18 years) with active, mild to moderate UC | Intervention (dose/schedule): Budesonide MMX (9 mg/day) Comparators (dose/schedule): Mesalamine (low-dose = 1.6 to 2.4 g/day; high-dose > 2.4 g/day); placebo | Outcome (measure) Clinical benefits: Induction of clinical and endoscopic remission – compound (NR); SAE (occurrence of events presented as comparisons of treatment groups using OR) Clinical harms: Treatment/study withdrawals (occurrence of events presented as OR between pooled effects of treatment) Follow-up: Reported as duration of therapy, 6 to 8 weeks |
Gherardi et al. (2018)25 Country: Netherlands Funding source: Ferring Pharmaceuticals | SR and NMA using a Bayesian approach with uninformative priors (conducted to inform a CE analysis, also summarized in this report) RCTs containing the intervention of interest and/or relevant comparator(s), n = 5 | Patients with mild to moderate UC | Intervention (dose/schedule): Budesonide MMX (9 mg/day) Eligible comparators of relevance (dose/schedule): Budesonide foam (treatment effects from various doses/schedules were pooled); budesonide enema (2 mg/100 mL); placebo | Outcome (measures) Clinical benefit: Clinical remission (UCDAI, Mayo Clinic, NR) presented as comparisons between pooled effects for treatment groups using OR Follow-up: Reported as duration of therapy, 4 to 8 weeks |
Nguyen et al. (2018)26 Country: US Funding source: Reported as none; individual authors report potential conflicts of interest in the form of funding received from government, NGO, and pharmaceutical company sources | SR and NMA using a frequentist approach RCTs containing the intervention of interest and/or relevant comparator(s), n = 75 | Adults (≥ 17 years of age) with active, mild to moderate UC | Intervention (dose/schedule): Budesonide MMX (NR) Eligible comparators (dose/schedule): Oral and rectal 5-ASAs (NR); diazo-bonded 5-ASAs i.e., balsalazide and olsalazine (NR); sulfasalazine (NR); controlled ileal-release budesonide (NR); mesalamine (low dose = < 2 g/day, standard dose = 2 to 3 g/day, high dose, > 3 g/day) | Eligible outcomes (measures) Clinical benefit: Failure to induce clinical and/or endoscopic remission (UCDAI, Mayo Clinic Score, Simple Clinical Colitis Activity Index, Sutherland DAI, and the Rachmilewitz Clinical Activity Index), presented as OR between pooled effects of treatment Clinical harm: Drug discontinuation Follow-up: Reported as duration of therapy, 4 to 8 weeks |
ASA = aminosalicylic acid; CE = cost-effectiveness; d = day(s); DAI = Disease Activity Index MMX = multi-matrix; NGO = non-governmental organization; NMA = network meta-analysis; NR = not reported; OR = odds ratio; RCT = randomized controlled trial; SAE = severe adverse event(s); SR = systematic review; UC = ulcerative colitis; UCDAI = Ulcerative Colitis Disease Activity Index; yr = year(s)
Notes: This table has not been copy-edited.
Outcome Measures:
Mayo Clinic Score: a measure of rectal bleeding, stool frequency, physician assessment, and endoscopy appearance, each of which is scored from 0 to 3 producing a total score of 0 to 12 with higher scores indicating more severe disease.35
Rachmilewitz Clinical Activity Index: a measure of clinical and endoscopic activity with scores ranging from 0 to 29; higher scores indicate more severe disease.36
Simple Clinical Colitis Activity Index: a measure of disease severity, scored from 0 to 19, with higher scores indicating more severe disease.37
Sutherland Disease Activity Index = a measure of stool frequency, rectal bleeding, mucosal appearance on endoscopy, and physician’s rating of disease activity producing a score between 0 and 12 with higher scores indicating more severe disease.38
Ulcerative Colitis Disease Activity Index: a measure of stool frequency, rectal bleeding, appearance of mucosa on sigmoidoscopy, and physician’s disease severity assessment, producing a score between 0 and 12 with higher scores indicating more severe disease.39
Table 3: Characteristics of Included Primary Clinical Study
Study citation, country, funding source | Study design | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Rubin et al. (2017)27 Countries: US, Canada, Europe Funding source: Salix Pharmaceuticals | Multicentre, double-blind, placebo-controlled RCT with ITT analyses | Adults aged 18 to 75 years with mild to moderate UC who had not responded adequately to oral mesalamine (N = 458) Intervention group (n = 230): Age, mean (SD) = 44.5 (14.1) Male sex, n (%) = 121 (52.6) BMI, mean (SD) = 25.7 (5.2) Disease duration in months, mean (SD) = 80.4 (91.0) Baseline UCDAI score, mean (SD) = 6.5 (1.5) Control group (n = 228): Age, mean (SD) = 44.6 (13.7) Male sex, n (%) = 127 (55.7) BMI, mean (SD) = 25.6 (5.0) Disease duration in months, mean (SD) = 78.9 (90.5) Baseline UCDAI score, mean (SD) = 6.6 (1.6) | Intervention (dose/schedule): Budesonide MMX, (9 mg/day), added to ≥ 2.4 g/day of mesalamine, as at study initiation Comparator (dose/schedule): Placebo (NR), added to ≥ 2.4g/day of mesalamine, as at study initiation | Outcome (measures) Clinical benefit Primary end point: Clinical and endoscopic remission – compound (i.e., total UCDAI score ≤ 1; UCDAI subscale scores of 0 for rectal bleeding, stool frequency and mucosal appearance) Secondary end points: Clinical remission (UCDAI subscale scores of 0 for rectal bleeding and stool frequency) Endoscopic remission (UCDAI subscale score of 0 for mucosal appearance) Exploratory end points: Histological healing (Geboes grade of 0 on biopsy) Clinical improvement (improvement of ≥ 3 from baseline in UCDAI score; rectal bleeding score of ≤ 1) Other: QoL (IBD-QOL) Clinical harm AEs Follow-up: 8 weeks |
AE = adverse event(s); IBD-QOL = inflammatory bowel disease quality of life; ITT = intention-to-treat; MMX = multi-matrix; NR = not reported; RCT = randomized controlled trial; SD = standard deviation; UC = ulcerative colitis; UCDAI = Ulcerative Colitis Disease Activity Index
Notes: This table has not been copy-edited.
Outcome Measures:
Inflammatory bowel disease quality of life: a measure of quality of life, including intestinal symptoms (10 items), systemic symptoms (5 items), social (12 items), and emotional domains (5 items) with higher scores indicating improved quality of life.40
Ulcerative Colitis Disease Activity Index: a measure of stool frequency, rectal bleeding, appearance of mucosa on sigmoidoscopy, and physician’s disease severity assessment, producing a score between 0 and 12 with higher scores indicating more severe disease.39
Table 4: Characteristics of Included Economic Evaluation
Study citation country, funding source | Type of analysis, time horizon, perspective | Population characteristics | Intervention and comparator(s) | Approach | Source of clinical, cost, and utility data used in analysis | Main assumptions |
|---|---|---|---|---|---|---|
Gherardi et al. (2018)25 Country: Netherlands Funding source: Some authors claimed employment with HEVA-HEOR or Ferring Pharmaceuticals | Analysis: Cost-effectiveness, including one-way deterministic sensitivity analyses, and probabilistic sensitivity analyses (using 1000 replications) Time horizon: 5 years (8 week cycles) Perspective: Societal | Dutch cohort of patients diagnosed with mild to moderate UC between 2006 and 2010 Sex, % patients Male = 49.7 Age, mean years: 48.2 Weight, mean kg: 77 | Intervention: Budesonide MMX (as second-line therapy following 5-ASA therapy) Comparators: Oral budesonide; budesonide enema; budesonide foam; prednisolone; placebo (as second-line therapy following 5-ASA therapy) | Eight-state Markov model (i.e., steroid, 5-ASA, immunomodulator, infliximab therapy; remission; hospitalization; post-surgery; death) | NMA of clinical studies (as summarized in this report);25 NRS Cost data from published sources specific to the Dutch context (expressed in Euros) Utility data were drawn from published clinical studies and sources | Failure to achieve remission with first-line, 5-ASA therapy Similar adverse event profiles for all treatments and no additional costs associated with adverse events Discounts at an annual rate of 4% for future costs and 1.5% for clinical benefits |
ASA = amino salicylic acid; NRS = nonrandomized study; UC = ulcerative colitis.
Note that this table has not been copy-edited.
Table 5: Characteristics of Included Guidelines
Intended users, target population | Intervention and practice considered | Major outcomes considered | Evidence collection, selection, and synthesis | Evidence quality assessment | Recommendations development and evaluation | Guideline validation |
|---|---|---|---|---|---|---|
ECCO 202228 | ||||||
Intended Users: Clinicians Target Population: Patients with mild to moderate and moderate to severe, active UC | Medical treatment, including budesonide MMX | Induction and maintenance of remission | Systematic reviews of pre-established research questions developed by consensus of the panel of experts | GRADE approach for rating the quality of the body of evidence, including Cochrane Risk of Bias assessment | Panel of experts assessed the evidence and drafted recommendations, which were approved by consensus when ≥ 80% of panellists supported the recommendation | The final guideline recommendations were critically reviewed and approved by the Governing Board of ECCO |
PANCCO 202229 | ||||||
Intended users: Not clearly stated (only that the guideline is intended to inform management of patients) Target population: Patients > 15 years of age diagnosed with UC | Treatments, including budesonide MMX | Induction and maintenance of remission | Systematic reviews of pre-established research questions developed by consensus of the developer group | GRADE approach for rating the quality of the body of evidence, including Cochrane Risk of Bias assessment | A developer group of experts assessed the evidence and drafted recommendations using discussion and consensus | The final draft guideline recommendations underwent external peer review before publication |
ACG 201930 | ||||||
Intended Users: Not clearly stated (only that the guideline presents the preferred approach to the management of patients) Target Population: Adults with mild, moderate, severe, and acute UC in both inpatient and outpatient settings | Clinical management including the use of budesonide MMX | Induction and maintenance of remission | NR | GRADE approach for rating the quality of the body of evidence | NR | NR |
BSG 201931 | ||||||
Intended Users: Health care providers Target Population: Adults (≥ 16 years of age) with IBD (including those with UC) | Clinical management including the use of budesonide MMX | Induction of remission | Systematic reviews of pre-established research questions developed by consensus of the guideline development group | RoB was assessed (method NR) | The guideline development group, comprised of multidisciplinary experts, assessed the evidence, and drafted recommendations, including the use of GRADE, which were approved by consensus when ≥ 80% of the group supported the recommendation | The final guideline document was critically reviewed by the BSG CSSC and BSG Council before publication |
ASG = American College of Gastroenterology; BSG = British Society of Gastroenterology; CSSC = Clinical Services and Standards Committee; ECCO = European Crohn’s and Colitis Organisation; GRADE = Grading of Recommendations, Assessment, Development, and Evaluations; IBD = irritable bowel disease; MMX = multi-matrix; NR = not reported; PANCCO = Pan American Crohn’s and Colitis Organisation; UC = ulcerative colitis.
Note: This table has not been copy-edited.
Appendix 3: Critical Appraisal of Included Publications
Note that this appendix has not been copy-edited.
Table 6: Strengths and Limitations of Systematic Reviews With Network Meta-Analyses Using the ISPOR Questionnaire20
Strengths | Limitations |
|---|---|
Bonovas (2019)24 | |
|
|
Gherardi (2018)25 | |
|
|
Nguyen (2018)26 | |
|
|
ISPOR = International Society for Pharmacoeconomics and Outcomes Research; RCT = randomized controlled trial; SR = systematic review.
Table 7: Strengths and Limitations of Clinical Study Using the Downs and Black Checklist21
Strengths | Limitations |
|---|---|
Rubin (2017)27 | |
Reporting: Reporting was clear, with the study objective, main outcomes, patient characteristics, main findings, estimates of variability using actual values, adverse events and losses to follow-up clearly described External validity: Study used a multinational, multicentre design which was representative of various health care, community and national contexts Internal validity:
| External validity: It was unclear whether patients, study centres and health facilities were representative of the population Power: A power calculation was conducted and reported; however, the required number of patients per study arm was not achieved |
Table 8: Strengths and Limitations of Economic Evaluation Using the Drummond Checklist22
Strengths | Limitations |
|---|---|
Gherardi (2018)25 | |
|
|
NMA = network meta-analysis.
Table 9: Strengths and Limitations of Guidelines Using AGREE II23
Item | ECCO (2022)28 | PANCCO (2022)29 | ACG (2019)30 | BSG (2019)31 |
|---|---|---|---|---|
Domain 1: scope and purpose | ||||
1. The overall objective(s) of the guideline is (are) specifically described. | Yes | Yes | Yes | Yes |
2. The health question(s) covered by the guideline is (are) specifically described. | Yes | Yes | Yes | Yes |
3. The population (patients, public, etc.) to whom the guideline is meant to apply is specifically described. | Yes | Yes | Yes | Yes |
Domain 2: stakeholder involvement | ||||
4. The guideline development group includes individuals from all relevant professional groups. | Unclear | Yes | Unclear | Yes |
5. The views and preferences of the target population (patients, public, etc.) have been sought. | Yes | Yes | Unclear | Yes |
6. The target users of the guideline are clearly defined. | Yes | Unclear | No | Yes |
Domain 3: rigour of development | ||||
7. Systematic methods were used to search for evidence. | Yes | Yes | Unclear | Yes |
8. The criteria for selecting the evidence are clearly described. | Yes | Yes | No | Yes |
9. The strengths and limitations of the body of evidence are clearly described. | Yes | Yes | Yes | Yes |
10. The methods for formulating the recommendations are clearly described. | Yes | Yes | No | Yes |
11. The health benefits, side effects, and risks have been considered in formulating the recommendations. | Yes | Yes | Yes | Yes |
12. There is an explicit link between the recommendations and the supporting evidence. | Yes | Yes | Yes | Yes |
13. The guideline has been externally reviewed by experts before its publication. | Yes | Yes | Unclear | Yes |
14. A procedure for updating the guideline is provided. | Yes | Yes | No | Yes |
Domain 4: clarity of presentation | ||||
15. The recommendations are specific and unambiguous. | Yes | Yes | Yes | Yes |
16. The different options for management of the condition or health issue are clearly presented. | Yes | Unclear | Yes | Yes |
17. Key recommendations are easily identifiable. | Yes | Yes | Yes | Yes |
Domain 5: applicability | ||||
18. The guideline describes facilitators and barriers to its application. | No | No | No | Unclear |
19. The guideline provides advice and/or tools on how the recommendations can be put into practice. | Yes | No | No | Unclear |
20. The potential resource implications of applying the recommendations have been considered. | Unclear | No | No | Unclear |
21. The guideline presents monitoring and/or auditing criteria. | No | No | No | Yes |
Domain 6: editorial independence | ||||
22. The views of the funding body have not influenced the content of the guideline. | Yes | Yes | Unclear | Yes |
23. Competing interests of guideline development group members have been recorded and addressed. | Yes | Yes | Unclear | Yes |
AGREE II = Appraisal of Guidelines for Research and Evaluation II; ASG = American College of Gastroenterology; BSG = British Society of Gastroenterology; ECCO = European Crohn’s and Colitis Organisation; PANCCO = Pan American Crohn’s and Colitis Organisation.
Appendix 4: Main Study Findings
Note that this appendix has not been copy-edited.
Table 10: Summary of Findings by Outcome — Induction of Remission
End points | Summary statistics | Budesonide MMX | Comparator | Group differencea(direction of observed effect) |
|---|---|---|---|---|
Versus placebo | ||||
Bonovas (2019)24 | ||||
Clinical and endoscopic remission | OR, 95% CI | 2.68 | 1.75 to 4.10* (favours budesonide MMX) | |
Gherardi (2018)25 | ||||
Clinical remission | OR, 95% CI | 3.3 | 1.8 to 6.7* (favours budesonide MMX) | |
Rubin (2017)27 | ||||
Clinical and endoscopic remission | % patients, P value | 13.0 | 7.5 | 0.049* (favours budesonide MMX) |
Clinical remission | 24.3 | 22.8 | 0.0698 | |
Endoscopic remission | 20.0 | 12.3 | 0.025* (favours budesonide MMX) | |
Versus controlled ileal-release budesonide | ||||
Nguyen (2018)26 | ||||
Failure to induce clinical remission | OR, 95% CI | 0.63 | 0.38 to 1.04 | |
Failure to induce endoscopic remission | OR, 95% CI | 0.82 | 0.46 to 1.47 | |
Versus budesonide enema | ||||
Gherardi (2018)25 | ||||
Clinical remission | OR, 95% CI | 1.1 | 0.49 to 2.4 | |
Versus budesonide foam | ||||
Gherardi (2018)25 | ||||
Clinical remission | OR, 95% CI | 1.4 | 0.67 to 2.9 | |
Versus oral and topical 5-ASAs | ||||
Nguyen (2018)26 | ||||
Failure to induce clinical remission | OR, 95% CI | 0.49 | 0.24 to 1.02 | |
Failure to induce endoscopic remission | OR, 95% CI | 0.44 | 0.15 to 1.30 | |
Versus diazo-bonded 5-ASAs | ||||
Nguyen (2018)26 | ||||
Failure to induce clinical remission | OR, 95% CI | 1.10 | 0.70 to 1.74 | |
Failure to induce endoscopic remission | OR, 95% CI | 0.89 | 0.52 to 1.53 | |
Versus high-dose mesalamine | ||||
Bonovas (2019)24 | ||||
Clinical and endoscopic remission | OR, 95% CI | 0.97 | 0.59 to 1.60 | |
Nguyen (2018)26 | ||||
Failure to induce clinical remission | OR, 95% CI | 1.07 | 0.70 to 1.62 | |
Failure to induce endoscopic remission | OR, 95% CI | 1.29 | 0.76 to 2.20 | |
Versus standard-dose mesalamine | ||||
Nguyen (2018)26 | ||||
Failure to induce clinical remission | OR, 95% CI | 0.84 | 0.55 to 1.26 | |
Failure to induce endoscopic remission | OR, 95% CI | 1.03 | 0.64 to 1.65 | |
Versus low-dose mesalamine | ||||
Bonovas (2019)24 | ||||
Clinical and endoscopic remission | OR, 95% CI | 1.23 | 0.76 to 1.56 | |
Nguyen (2018)26 | ||||
Failure to induce clinical remission | OR, 95% CI | 0.64 | 0.40 to 1.02 | |
Failure to induce endoscopic remission | OR, 95% CI | 0.68 | 0.40 to 1.17 | |
Versus sulfasalazine | ||||
Nguyen (2018)26 | ||||
Failure to induce clinical remission | OR, 95% CI | 1.92 | 1.16 to 3.19* (favours budesonide MMX) | |
Failure to induce endoscopic remission | OR, 95% CI | 1.49 | 0.74 to 2.96 | |
ASA = amino salicylic acid; CI = confidence interval; MMX = multi-matrix; OR = odds ratio
a* indicates statistical significance.
Table 11: Summary of Findings by Outcome — Clinical and Endoscopic Response
End point | Summary statistic(s) | Budesonide MMX | Comparator | Group difference, P valuea(direction of observed effect) |
|---|---|---|---|---|
Versus Placebo | ||||
Rubin (2017)27 | ||||
Histological healing | % patients | 27.0 | 17.5 | 0.016* (favours budesonide MMX) |
Clinical improvement | 47.0 | 39.0 | 0.09 | |
MMX = multi-matrix.
a* indicates statistical significance.
Table 12: Summary of Findings by Outcome — Quality of Life
Rubin (2017)27 | IBD-QOL score, mean (SD) | ||
|---|---|---|---|
Budesonide MMX | Placebo | Group difference, P valuea(direction of observed effect) | |
Pre-treatment | 132.8 (31.4) | 134.1 (32.5) | NR |
2 weeks | 157.1 (31.6) | 155.7 (32.6) | 0.32 |
4 weeks | 164.6 (34.4) | 160.2 (35.1) | 0.04* (favours budesonide MMX) |
8 weeks | 163.9 (39.4) | 165.8 (36.8) | 0.88 |
NR = not reported; MMX = multi-matrix.
a* indicates statistical significance.
Table 13: Summary of Findings by Outcome — Adverse Events
Adverse event | Summary Statistic(s) | Budesonide MMX | Comparator | Group differencea(direction of observed effect) |
|---|---|---|---|---|
Versus placebo | ||||
Bonovas (2019)24 | ||||
Serious | OR, 95% CI | 1.35 | 0.60 to 3.04 | |
Treatment discontinuation or study withdrawal | 0.92 | 0.61 to 1.38 | ||
Rubin (2017)27 | ||||
Any | n patients (%) | NR (31.8) | NR (27.1) | NR |
Drug-related | 31 (12.2) | 15 (5.9) | ||
Treatment discontinuation | 12 (4.7) | 9 (3.5) | ||
Serious | 10 (3.9) | 2 (0.8) | ||
Drug-related serious | 2 (0.8) | 0 (0) | ||
Severity | ||||
Mild | n patients (%) | 44 (17.3) | 41 (16.1) | NR |
Moderate | 29 (11.4) | 26 (10.2) | ||
Severe | 8 (3.1) | 2 (0.8) | ||
Most common | ||||
UC | n patients (%) | 15 (5.9) | 10 (3.9) | NR |
Decreased blood cortisol | 10 (3.9) | 0 (0) | ||
Acne | 3 (1.2) | 5 (2.0) | ||
Serious | ||||
UC | n patients (%) | 6 (2.4) | 1 (0.4) | NR |
Acute pancreatitis | 1 (0.4) | 0 (0) | ||
Bronchitis | 1 (0.4) | 0 (0) | ||
Anemia | 1 (0.4) | 0 (0) | ||
Hypokalemia | 1 (0.4) | 0 (0) | ||
T2DM | 0 (0) | 1 (0.4) | ||
Versus controlled ileal-release budesonide | ||||
Nguyen (2018)26 | ||||
Drug discontinuation | OR, 95% CI | 1.06 | 0.56 to 2.00 | |
Versus oral and topical 5-ASAs | ||||
Nguyen (2018)26 | ||||
Drug discontinuation | OR, 95% CI | 0.64 | 0.46 to 4.32 | |
Versus diazo-bonded 5-ASAs | ||||
Nguyen (2018)26 | ||||
Drug discontinuation | OR, 95% CI | 0.52 | 0.28 to 0.98* (favours diazo-bonded 5-ASAs) | |
Versus low-dose mesalamine | ||||
Bonovas (2019)24 | ||||
Serious | OR, 95% CI | 1.44 | 0.52 to 3.97 | |
Treatment discontinuation or study withdrawal | 1.71 | 0.98 to 2.96 | ||
Nguyen (2018)26 | ||||
Drug discontinuation | OR, 95% CI | 1.08 | 0.50 to 2.31 | |
Versus standard-dose mesalamine | ||||
Nguyen (2018)26 | ||||
Drug discontinuation | OR, 95% CI | 1.76 | 1.04 to 2.97* (favours standard-dose mesalamine) | |
Versus high-dose mesalamine | ||||
Bonovas (2019)24 | ||||
Serious | OR, 95% CI | 1.85 | 0.59 to 5.79 | |
Treatment discontinuation or study withdrawal | 2.22 | 1.23 to 4.02* (favours high-dose mesalamine) | ||
Nguyen (2018)26 | ||||
Drug discontinuation | OR, 95% CI | 2.31 | 1.33 to 3.99* (favours high-dose mesalamine) | |
Versus sulfasalazine | ||||
Nguyen (2018)26 | ||||
Drug discontinuation | OR, 95% CI | 1.29 | 0.55 to 3.04 | |
ASA = amino salicylic acid; CI = confidence interval; MMX = multi-matrix; n = number(s); NR = not reported; OR = odds ratio.
a* indicates statistical significance.
Table 14: Summary of Findings of Included Economic Evaluation
Analyses and relevant parameters (upper/lower limits) | Mean costs (EUR) | Mean QALYs gained | ICER, EUR/QALY gained (dominant intervention) | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
Budesonide MMX | Comparators | Group difference | Budesonide MMX | Comparators | Group difference | |||||
Gherardi (2018)25 | ||||||||||
Base case (total cost) | 6,233 | 6,599 | 366 | 3.471 | 3.462 | 0.009 | NR (budesonide MMX) | |||
primary drug cost | 651 | 939 | 288 | — | — | — | — | |||
additional drug cost | 1,227 | 1,277 | 50 | — | — | — | — | |||
health care cost | 3,831 | 3,845 | 14 | — | — | — | — | |||
indirect cost | 524 | 538 | 14 | — | — | — | — | |||
Deterministic, one-way sensitivity | ||||||||||
risk of relapse (+ 20%) | 5,775 | 6,107 | 332 | 3.506 | 3.498 | 0.009 | NR (budesonide MMX) | |||
risk of relapse (−20%) | 6,650 | 7,045 | 395 | 3.438 | 3.429 | 0.010 | NR (budesonide MMX) | |||
proportion of patients requiring hospitalization and surgery (+ 20%) | 6,229 | 6,595 | 366 | 3.471 | 3.462 | 0.009 | NR (budesonide MMX) | |||
proportion of patients requiring hospitalization and surgery (−20%) | 6,237 | 6,602 | 366 | 3.471 | 3.461 | 0.009 | NR (budesonide MMX) | |||
mortality (+ 20%) | 6,256 | 6,622 | 367 | 3.486 | 3.476 | 0.009 | NR (budesonide MMX) | |||
mortality (−20%) | 6,211 | 6,575 | 364 | 3.456 | 3.447 | 0.009 | NR (budesonide MMX) | |||
OR vs. oral budesonide (95% CI) | 6,233 | 6,524 | 291 | 3.471 | 3.471 | 0 | NR (budesonide MMX) | |||
6,233 | 6,640 | 407 | 3.471 | 3.457 | 0.014 | NR (budesonide MMX) | ||||
OR vs. budesonide foam (95% CI) | 6,233 | 6,494 | 261 | 3.471 | 3.475 | 0.004 | NR (budesonide less costly and less effective) | |||
6,233 | 6,658 | 424 | 3.471 | 3.454 | 0.017 | NR (budesonide MMX) | ||||
adverse event costs for corticosteroids | 6,368 | 6,638 | 270 | 3.471 | 3.462 | 0.009 | NR (budesonide MMX) | |||
indirect costs (± 20%) | 6,128 | 6,491 | 363 | 3.471 | 3.462 | 0.009 | NR (budesonide MMX) | |||
Probabilistic sensitivity | 6,248 | 6,601 | 354 | 3.477 | 3.468 | 0.009 | NR (budesonide MMX) | |||
EUR = Euro(s); ICER = incremental cost-effectiveness ratio; MMX = multi-matrix; NR = not reported; OR = odds ratio; QALY = quality-adjusted life-year
Table 15: Summary of Recommendations in Included Guidelines
Recommendations and supporting evidence | Quality of evidence and strength of recommendations |
|---|---|
ECCO (2022)28 | |
Relevant recommendation: “We suggest the use of colonic-release corticosteroids for induction of remission in patients with active mild-to-moderate UC.” (p. 7)* Supporting evidence: CORE I, CORE II, CB-01-02/05 (summarized in the previous 2017 CADTH report1) *While budesonide MMX is not named in the recommendation, the summary of supporting evidence for the recommendation discusses only budesonide MMX. | Low quality of evidence; weak recommendation |
PANCCO (2022)29 | |
Relevant recommendation: “Budesonide MMX is recommended for inducing remission in patients with UC, of any extension, with mild-to-moderate activity.” (p. 347) Supporting evidence: Cochrane Systematic Review (summarized in the previous 2017 CADTH report1) The guideline also includes “good practice points,” which include suggesting the use of budesonide MMX in patients who do not respond to 5-ASAs as first-line therapy, and that budesonide MMX can be administered daily at a dose of 9mg for an 8-week course of therapy. | High quality of evidence; strength of the recommendation is described as conditional, in favour of the strategy used (which are NR). |
ACG (2019)30 | |
Relevant recommendation: “In patients with mildly active left-sided UC who are intolerant or nonresponsive to oral and rectal 5-ASA at appropriate doses (oral at least 2 g/d and rectal at least 1 g/d), we recommend oral budesonide MMX 9 mg/d for induction of remission.” (p. 395) Supporting evidence: CORE I (summarized in the previous 2017 CADTH report1), Rubin 201727 | Moderate quality of evidence; strong recommendation |
Relevant recommendation: “In patients with mildly to moderately active UC not responding to oral 5-ASA, we recommend the addition of budesonide MMX 9 mg/d to induce remission.” (p. 395) Supporting evidence: CORE I (summarized in the previous 2017 CADTH report1), Rubin 201727 | Moderate quality of evidence; strong recommendation |
Relevant recommendation: “In patients with moderately active UC, we recommend oral budesonide MMX for induction of remission.” (p. 397) Supporting evidence: CORE II (summarized in the previous 2017 CADTH report1) | Moderate quality of evidence; strong recommendation |
BSG (2019)31 | |
Relevant recommendation (emphasis added to the relevant portion of the recommendation): “We recommend that patients with mild to moderate ulcerative colitis in whom 5-ASA induction therapy fails or is not tolerated should be treated with oral prednisolone… We recommend that topically-acting oral corticosteroids such as budesonide MMX… can be used as alternative treatments for those wishing to avoid systemic corticosteroids (Agreement: 93.2%).” (p. s12) Supporting evidence: CORE I and II (summarized in the previous 2017 CADTH report);1 D’Haens 2010 (excluded from the previous 2017 CADTH report);1 Cochrane Systematic Review (summarized in the previous 2017 CADTH report);1 Rubin 201727 | Moderate quality of evidence; strong recommendation |
ASA = amino salicylic acid; ASG = American College of Gastroenterology; BSG = British Society of Gastroenterology; ECCO = European Crohn’s and Colitis Organisation; MMX = multi-matrix; NR = not reported; PANCCO = Pan American Crohn’s and Colitis Organisation; UC = ulcerative colitis.
Appendix 5: References of Potential Interest
Note that this appendix has not been copy-edited.
Mixed Population (Data Specific to UC Cannot Be Isolated)
Rosiou K, Ong Ming San E, Kumar A, et al. Comparative outcomes of budesonide mmx versus prednisolone for ulcerative colitis: results from a British retrospective multi-centre real-world study. J Clin Med. 2021;10(19):23. PubMed
Bonovas S, Nikolopoulos GK, Lytras T, Fiorino G, Peyrin-Biroulet L, Danese S. Comparative safety of systemic and low-bioavailability steroids in inflammatory bowel disease: systematic review and network meta-analysis. Br J Clin Pharmacol. 2018;84(2):239-251. PubMed
Studies With No Comparator
Fellermann K, Schiefke I, Racz I, et al. Efficacy and safety of prolonged release budesonide granules in mesalazine-refractory ulcerative colitis: a multi-centre phase IIa study (TOPICAL-1). United European Gastroenterol J. 2020;8(10):1186-1195. PubMed
Maconi G, Mezzina N, Landi S, et al. Use, effectiveness and tolerability of budesonide-MMX in ulcerative colitis: a real-life experience. United European Gastroenterol J. 2019;7(9):1164-1170. PubMed
Contributors: Calvin Young, Elizabeth Carson, Matthew McDonald
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca