CADTH Health Technology Review
Midline and Extended Dwell Catheters for IV Antibiotics
Rapid Review
Authors: Qiukui Hao, Jennifer Horton
Abbreviations
CI
confidence interval
CR-BSI
catheter-related bloodstream infection
CRC
catheter-related complication
DVA
difficult vascular access
HR
hazards ratio
LPC
long peripheral catheter
PICC
peripherally inserted central catheter
Key Messages
Midline catheters may be associated with longer uncomplicated indwelling time and a lower overall risk of catheter-related complications than extended dwell catheters.
The rates of catheter-related complications were low across different peripheral catheter types.
Midline catheters may have a lower proportion of catheter-related bloodstream infections, drug leakage from the exit site, and complete catheter occlusion, but a higher proportion of catheter-related thrombosis events compared with extended dwell catheters.
The findings were derived from 1 retrospective cohort study with imbalanced baseline characteristics of patients, and the limitations of the study may have favoured midline catheters; future studies are needed to confirm our findings.
We did not find any systematic reviews, health technology assessments, randomized controlled trials, or evidence-based guidelines that met our inclusion criteria.
Context and Policy Issues
Use of Antibiotics and IV Catheters
People with bacterial infections might need to take antibiotics after comprehensive assessments by clinicians. Antibiotics can be administered orally or by IV.1,2 Oral antibiotics are more common and convenient for treating infections; however, in some conditions, such as life-threatening infections and deep tissue infections, patients may not respond to oral antibiotics or may be unable to take or absorb them.1 In these cases, patients usually need to receive IV antibiotics, which are delivered directly to the bloodstream through a plastic catheter in a vein. Generally, the cost of IV antibiotics is higher than oral antibiotics and they require a trained medical professional to administer them.3
IV catheters are hollow and flexible tubes of varying lengths that are inserted into major veins to deliver fluids, medications, or nutrition directly into the bloodstream.4 Clinicians typically recommend IV catheters for patients requiring IV therapy over a long period of time or patients with difficult venous access conditions. Using IV catheters eliminates the need for health care professionals to repeatedly insert a needle into the vein.4,5 Instead, patients or medical professionals can introduce the needle into the dwelling site, simplifying the process of IV treatment. IV catheters can be categorized into central and peripheral catheters based on their placement. Central catheters, such as peripherally inserted central catheters (PICCs), extend into the vena cava and are often used for administering medications or nutritional supplements that require a substantial blood flow.6 However, central catheters are associated with a higher risk of bloodstream infection than peripheral IV catheters.7
Both central and peripheral IV catheters can be used for administering IV antibiotics.7-9 Peripherally compatible antibiotics are antibiotics that can be administered safely through a peripheral IV catheter without causing serious irritation to peripheral veins.10 Clinicians determine if an antibiotic is peripherally compatible by considering its concentration and pH level.10
Midline and Extended Dwell Catheters
Midline or extended dwell catheters are 2 kinds of peripheral IV catheters. They are characterized by their length and placement, and typically measure longer than standard long peripheral IV catheters (2 cm to 6 cm) while remaining shorter than PICCs (38 cm to 52 cm).11,12 The key distinctions between midline and extended dwell catheters are primarily in their length and catheter placement. A midline catheter, measuring between 15 cm and 25 cm, is inserted into the upper arm, with its internal tip positioned at or near the axilla, distal to the shoulder.11,12 In contrast, extended dwell catheters, measuring between 6 cm and 15 cm, are shorter than midline catheters and typically placed below the antecubital area, with their internal tip placed in a lower vessel position than midline catheters.11,12 It is important to note that the length of catheters can vary depending on the situation, with different lengths being used for midline or extended dwell catheters.12 Due to their noncentral positioning, midline or extended dwell catheters might be associated with a reduced risk of complications compared with central catheters.7 This makes peripheral catheters an increasingly popular choice for administering antibiotics that do not require central venous access. Among peripheral catheters, previous studies showed that midline or extended dwell catheters are favourable alternatives to standard long IV catheters in catheter survival or catheter-related complications.13,14
Why Is it Important to Do This Review?
Although standard long IV catheters are not the favoured choice of peripheral catheter for administering IV antibiotics, clinicians still need to determine whether to use a midline or extended dwell catheter for this purpose. For patients with difficult vascular access (DVA) who require IV antibiotics for up to 14 days, The Michigan Appropriateness Guide for Intravenous Catheters recommended midlines as the preferred vascular access in 2015.15 Previous studies primarily concentrated on comparing midline or extended dwell catheters with standard long peripheral IV catheters;13,14,16 however, the comparative clinical effectiveness and safety between midline catheters and extended dwell catheters for delivering antibiotics in adults remains unclear.
Objective
To support decision-making about the choice between using a midline catheter or an extended dwell catheter for delivering IV peripherally compatible antibiotics in adults, we summarize the latest evidence on the clinical effectiveness and safety of using a midline catheter versus an extended dwell catheter, as well as related clinical practice guidelines.
Research Questions
What is the clinical effectiveness of a midline catheter versus and an extended dwell catheter for delivering IV peripherally compatible antibiotics in adults?
What are the evidence-based guidelines regarding midline and extended dwell catheters for delivering IV peripherally compatible antibiotics in adults?
Methods
Literature Search Methods
An information specialist conducted a literature search on key resources including MEDLINE, Embase, the Cochrane Database of Systematic Reviews, the International HTA Database, and the websites of Canadian and major international health technology agencies, as well as a focused internet search. The search approach was customized to retrieve a limited set of results, balancing comprehensiveness with relevancy. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. Search concepts were developed based on the elements of the research questions and selection criteria. The main search concepts were midline and extended dwell catheters. A supplemental search with the same concepts was conducted with CADTH-developed search filters applied to limit retrieval to guidelines. The search was completed on August 2, 2023, and limited to English-language documents published since January 1, 2018.
Selection Criteria and Methods
One reviewer screened citations and selected studies. In the first level of screening, titles and abstracts were reviewed and potentially relevant articles were retrieved and assessed for inclusion. The final selection of full-text articles was based on the inclusion criteria presented in Table 1.
Criteria | Description |
|---|---|
Population | Adults with an infection receiving inpatient or outpatient care |
Intervention | Q1: Midline catheter to provide IV peripherally compatible antibiotics Q2: Midline or extended dwell catheters to provide IV peripherally compatible antibiotics |
Comparator | Q1: Extended dwell catheter to provide the same IV peripherally compatible antibiotics Q2: Not applicable |
Outcomes | Q1: Clinical benefits (e.g., vessel health and preservation, health-related quality of life) and harms (e.g., infections, phlebitis, leakage, dislodging, infiltrations, deep vein thrombosis, occlusion, failure) Q2: Recommendations regarding best practices for the indication and use of midline and extended dwell catheters (e.g., patient selection, length of IV therapy, placement) |
Study designs | Health technology assessments, systematic reviews, randomized controlled trials, nonrandomized studies, evidence-based guidelines |
Exclusion Criteria
Articles were excluded if they did not meet the selection criteria outlined in Table 1, they were duplicate publications, or were published before 2018. Guidelines with an unclear methodology or studies with unclear populations were also excluded.
Critical Appraisal of Individual Studies
The included publications were critically appraised by 1 reviewer using the Downs and Black checklist17 for the included nonrandomized study. Summary scores were not calculated for the included study; rather, its strengths and limitations were described narratively.
Summary of Evidence
Quantity of Research Available
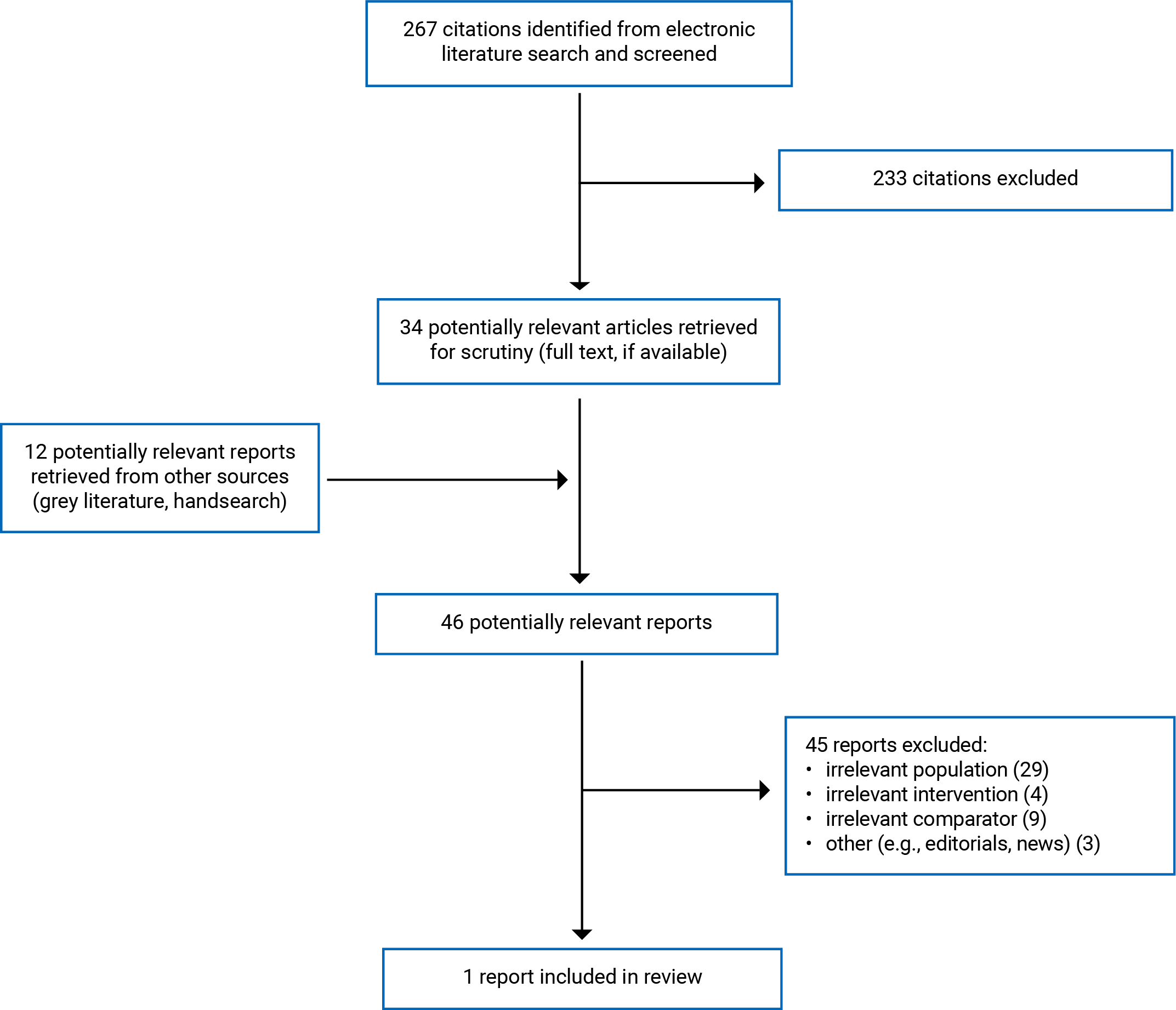
A total of 267 citations were identified in the literature search. Following screening of titles and abstracts, 233 citations were excluded and 34 potentially relevant reports from the electronic search were retrieved for full-text review. Twelve potentially relevant publications were retrieved from the grey literature search for full-text review. Of these potentially relevant articles, 45 publications were excluded for various reasons, and 1 publication of 1 retrospective cohort study met the inclusion criteria and was included in this report. Appendix 1 presents the PRISMA18 flow chart of the study selection.
Appendix 5 provides additional references of potential interest, including studies comparing midline catheters or extended dwell catheters to standard peripheral catheters and studies conducted in unclear populations.
Summary of Study Characteristics
This report included 1 retrospective cohort study conducted at an Italian university hospital that compared the clinical effectiveness of midline catheters to extended dwell catheters of 2 different lengths for delivering IV peripherally compatible antibiotics and other infusion products.19 In this study, the authors used long peripheral catheters (LPCs), which are extended dwell catheters.19 We use the term extended dwell catheters in our report instead of LPC. However, we kept LPC in the appendices.
The study included 184 consecutive adults with acute cardiovascular disease and DVA, defined as failure of at least 3 cannulation attempts on visible or palpable veins, who were admitted to a hospital between January 2014 and April 2019.19 The median age of participants was 70 years, with slightly more males (53.8%) than females, and the median Charlson Comorbidity Index was 3.
Polyurethane midline catheters of 20 cm were used for patients requiring venous access for over 10 days, while patients requiring venous access for 7 days to 10 days were given polyethylene extended dwell catheters.19 The study’s 184 patients were divided into 3 groups according to the type of peripherally inserted catheters used: a midline catheter group (80 patients), an 18 cm extended dwell catheter group (48 patients), and an 8 cm or 10 cm extended dwell catheter group (56 patients).
The study documented the administration of 25 antibiotics. The same catheter was used to infuse up to 5 different antibiotics, with a median of 1.0 and an interquartile range of 0 to 2 antibiotics. There was a significantly higher number of different antibiotics infused through midline catheters (with a median of 2.0) compared to 18 cm extended dwell catheters (with a median of 1.0) and 8 cm or 10 cm extended dwell catheters (with a median of 0.5). However, there was no difference seen in the specific antibiotics infused between the different catheter groups, except for ampicillin, oxacillin, and rifampicin, which had a higher percentage in midline catheters. There was no difference observed between the groups in relation to IV sodium heparin administration, or patients receiving oral or subcutaneous antiaggregant or anticoagulant medications.
The study reported uncomplicated indwelling time and catheter-related complications (CRCs), including catheter-related bloodstream infections (CR-BSIs), thrombosis, infiltration (leakage), occlusion, and fissuring.19
Appendix 2 presents additional details regarding the characteristics of the included publication.
Summary of Critical Appraisal
The study had several strengths related to reporting and choice of statistical analysis. Study objectives, inclusion and exclusion criteria, sample size calculations, CRC measures, intervention and comparators, and main findings were all clearly described.19 The multivariable Cox regression model was used to calculate the adjusted hazard ratio (HR) and corresponding estimates of the variability (interquartile range or 95% confidence interval [CI]) for the main outcomes were provided.19 The actual P values were reported for some outcomes, and the study authors declared no related conflicts of interest.19
There were also some methodological limitations that may have impacted the study’s internal and external validity. The disease that requires IV antibiotics was poorly described. Baseline characteristics were imbalanced between the midline catheter and extended dwell catheter groups, with patients receiving extended dwell catheters having a higher median Charlson Comorbidity Index, a lower vein-to-catheter ratio, a lower number of different antibiotics infused, and a shorter expected venous access period than those receiving midline catheters.19 A lower vein-to-catheter ratio and a higher Charlson Comorbidity Index may increase the risk of CRCs,20 potentially making the results on CRCs favour midline catheters due to a higher baseline CRC risk in patients who received extended dwell catheters. Additionally, patients with midline catheters had longer expected venous access compared to those with extended dwell catheters, which could explain the longer raw uncomplicated indwelling time observed for midline catheters than in the extended dwell catheters. The multivariable Cox regression adjusted the vein-to-catheter ratio, Charlson Comorbidity Index, and the number of different antibiotics infused; however, the model's stepwise methods lacked clarity, including unclear P values for entering and removing candidate variables from the model and selection of candidate variables.19 If the authors used small P values for entry, some important variables in the final model may have been missed. If the authors selected candidate variables based solely on univariate analysis results, the generality of the final model may be limited. Additionally, another potentially important treatment effect modifier, disease severity, was not considered.
Additional details regarding the strengths and limitations of the included publications are provided in Appendix 3
Summary of Findings
We identified 1 retrospective cohort study that compared the clinical effectiveness of midline catheters (20 cm) to 2 groups of extended dwell catheters, categorized by length (8 cm or 10 cm and 18 cm) for delivering IV peripherally compatible antibiotics and other infusion products.19 The study reported indwelling time, raw CRC events, and HRs for the risk of CRCs.19
Appendix 4 presents the main study findings.
Clinical Effectiveness of Midline Catheters Versus Extended Dwell Catheters
Uncomplicated Indwelling Time
Midline catheters had a statistically significantly longer median uncomplicated indwelling time than the extended dwell catheters of different lengths (these medians were presented graphically and the exact numbers were not available).19 In addition, the maximum indwell time for midline catheters was numerically longer than for the 2 types of extended dwell catheters.19
Overall CRCs
Midline catheters had a numerically lower incidence of CRCs than the extended dwell catheters of different lengths.19 In addition, compared to midline catheters, 8 cm and 10 cm extended dwell catheters showed a statistically significant increase in CRC risk (HR = 5.328; 95% CI, 2.118 to 13.404; P < 0.001).19 However, the 18 cm extended dwell catheters showed a statistically nonsignificant trend toward higher CRC risk (HR = 2.489; 95% CI, 0.961 to 6.448; P = 0.06) compared to midline catheters.19
Specific CRCs
The retrospective cohort study examined specific CRCs, including CR-BSIs, catheter-related thrombosis, fissuring, drug leakage from the exit site, and complete catheter occlusion.19 Although the incidence rate of each complication was low, with the percentage of patients with events ranging from 1.1% to 6.0%, there were mixed results in trends or directions among midline catheters and 8 cm, 10 cm, and 18 cm extended dwell catheters. The statistical test results (P values) were not available for any of these comparisons.
Catheter-related thrombosis: Midline catheters had a numerically higher percentage of patients with catheter-related thrombosis events than any length of extended dwell catheter.19
CR-BSIs: Midline catheters had a numerically lower incidence of CR-BSIs than the extended dwell catheters, both of 18 cm length and overall, but higher than 8 cm or 10 cm extended dwell catheters.19
Drug leakage from the exit site: Midline catheters had a numerically lower percentage of patients with drug leakage events from the exit site than any length of the extended dwell catheters.19
Complete catheter occlusion: Midline catheters had a numerically lower percentage of patients with complete catheter occlusion events than any length of the extended dwell catheters.19
Catheter fissuring: Midline catheters had a numerically lower percentage of catheter fissuring events than the 18 cm extended dwell catheters, but a higher percentage than the 8 cm or 10 cm extended dwell catheters.19
Guidelines Regarding the Use of Midline Catheters or Extended Dwell Catheters
No evidence-based guidelines regarding the use of midline catheters or extended dwell catheters were identified.
Limitations
The available evidence that we identified consisted of 1 retrospective cohort study with imbalanced baseline characteristics, including the Charlson Comorbidity Index, vein-to-catheter ratio, and preintervention-expected venous access.19 These imbalanced baseline characteristics may introduce bias in favour of midline catheters. Although the study used the multivariable Cox regression model to adjust for previously known imbalanced variables such as Charlson Comorbidity Index and vein-to-catheter ratio, a causal relationship should not be assumed due to the nature of a retrospective cohort study.
The retrospective cohort study was conducted in 1 Italian hospital among adults with acute cardiovascular disease and difficult venous access conditions.19 Therefore, it is uncertain if these findings can be generalized to other conditions, such as patients with normal venous access, or to settings in Canada. Based on a survey conducted among vascular access specialists,12 an extended dwell catheter typically measures between 6 cm and 15 cm, while a midline catheter is between 15 cm and 25 cm. In the study included, an 18 cm extended dwell catheter was used, which is 1 of the 2 lengths of catheters classified as “extended dwell” in this study. However, it is not clear whether the results from using the 18 cm extended dwell catheter can be applied to all extended dwell catheters measuring between 6 cm and 15 cm.
We did not find any systematic reviews, health technology assessments, randomized controlled trials, or evidence-based guidelines that met our inclusion criteria.
Appendix 5 provides some related references, including non–evidence-based guidelines and comparisons of midline catheters or extended dwell catheters versus standard long peripheral IV catheters.
Conclusions and Implications for Decision- or Policy-Making
This report included 1 retrospective cohort study comparing the clinical effectiveness of midline catheters to extended dwell catheters of different lengths for delivering IV peripherally compatible antibiotics.19 We did not identify any systematic reviews, health technology assessments, randomized controlled trials, or evidence-based guidelines for the use of midline or extended dwell catheters that met our inclusion criteria. Our report's findings align with The Michigan Appropriateness Guide for Intravenous Catheters' 2015 guideline,15 which recommends midline catheters as the preferred vascular access for patients who have DVA and need IV antibiotics for up to 14 days.
The body of identified evidence suggests that using midline catheters may be associated with longer uncomplicated indwelling time and lower overall risk of CRCs than extended dwell catheters.19 Midline catheters may also have a lower proportion or incidence of CR-BSIs, drug leakage from the exit site, and complete catheter occlusion, but a higher proportion of catheter-related thrombosis events than extended dwell catheters.19 Midline catheters had a numerically lower percentage of patients with catheter fissuring events than the 18 cm extended dwell catheters, but a higher percentage than the 8 cm or 10 cm extended dwell catheters.19 We observed that the incidence rates of specific CRCs were low and there were mixed results in trends or directions among midline catheters and extended dwell catheters of different lengths (8 cm or 10 cm, and 18 cm), with limited statistical testing to support conclusions on the significance of the findings. Due to limitations in the identified body of evidence, namely that findings were derived from 1 retrospective study with imbalanced baseline characteristics among a total of 184 patients; lack of statistical tests for some outcomes; and potential generalizability issues, caution is needed when interpreting these findings and there remains a high degree of uncertainty. Of note, we observed that the study-included catheters were made of different materials: polyurethane for midline catheters and polyethylene for extended dwell catheters.19 The study stated that polyethylene catheters may have a higher risk of infection than polyurethane catheters, although the data are controversial.19 It remains unclear if the difference in materials could account for the differences in outcome measures, including uncomplicated indwelling time or risk of CRCs.
Further studies are necessary to confirm the findings and examine the impact of different catheter materials on clinical effectiveness and safety outcomes. Future research should use a more robust design, such as randomized controlled trials with well-balanced baseline characteristics. Additionally, future studies should focus on patient-important outcomes, such as quality of life. During the full-text screening process, we identified several studies comparing midline catheters or extended dwell catheters to standard long IV catheters.12,13 A systematic review with network meta-analysis that provides an indirect comparison of midline catheters and extended dwell catheters through standard long IV catheters may be useful for decision-making.
References
1.McCarthy K, Avent M. Oral or intravenous antibiotics? Aust Prescr. 2020;43(2):45-48. PubMed
2.Li H-K, Rombach I, Zambellas R, et al. Oral versus Intravenous Antibiotics for Bone and Joint Infection. N Engl J Med. 2019;380(5):425-436. PubMed
3.Faller E, Jackson A. A cost minimisation analysis comparing oral linezolid and intravenous daptomycin administered via an outpatient parenteral antibiotic therapy programme in patients requiring prolonged antibiotic courses. J Chemother. 2023;35(5):411-424. PubMed
4.Zingg W, Barton A, Bitmead J, et al. Best practice in the use of peripheral venous catheters: A scoping review and expert consensus. Infect Prev Pract. 2023;5(2):100271. PubMed
5.Moureau N, Chopra V. Indications for peripheral, midline and central catheters: summary of the MAGIC recommendations. Br J Nurs. 2016;25(8):S15-24. PubMed
6.Duwadi S, Zhao Q, Budal BS. Peripherally inserted central catheters in critically ill patients - complications and its prevention: A review. Int J Nurs Sci. 2019;6(1):99-105. PubMed
7.Swaminathan L, Flanders S, Horowitz J, Zhang Q, O'Malley M, Chopra V. Safety and Outcomes of Midline Catheters vs Peripherally Inserted Central Catheters for Patients With Short-term Indications: A Multicenter Study. JAMA Intern Med. 2022;182(1):50-58. PubMed
8.Grennan D, Gottsch M. Home Intravenous Antibiotic Therapy. JAMA. 2019;322(1):90-90. PubMed
9.Keller SC, Dzintars K, Gorski LA, Williams D, Cosgrove SE. Antimicrobial Agents and Catheter Complications in Outpatient Parenteral Antimicrobial Therapy. Pharmacotherapy. 2018;38(4):476-481. PubMed
10.Spencer S, Ipema H, Hartke P, et al. Intravenous Push Administration of Antibiotics: Literature and Considerations. Hosp Pharm. 2018;53(3):157-169. PubMed
11.Lozano M. Use of Midline and Extended Dwell Catheters. Nursing Research. Orange (CA): CHOC Children's. 2018 https://www.choc.org/wp/wp-content/uploads/2021/05/02-Use-of-Midline-and-Extended-Dwell-Catheters.pdf Accessed 2023 Aug 14. .
12.Qin KR, Pittiruti M, Nataraja RM, Pacilli M. Long peripheral catheters and midline catheters: Insights from a survey of vascular access specialists. J Vasc Access. 2021;22(6):905-910. PubMed
13.Bahl A, Hang B, Brackney A, et al. Standard long IV catheters versus extended dwell catheters: A randomized comparison of ultrasound-guided catheter survival. Am J Emerg Med. 2019;37(4):715-721. PubMed
14.Harwood IR, Greene LM, Kozakowski-Koch JA, Rasor JS. New peripherally inserted midline catheter: a better alternative for intravenous antibiotic therapy in patients with cystic fibrosis. Pediatr Pulmonol. 1992;12(4):233-239. PubMed
15.Chopra V, Flanders SA, Saint S, et al. The Michigan Appropriateness Guide for Intravenous Catheters (MAGIC): Results From a Multispecialty Panel Using the RAND/UCLA Appropriateness Method. Ann Intern Med. 2015;163(6 Suppl):S1-40. PubMed
16.Nielsen EB, Antonsen L, Mensel C, et al. The efficacy of midline catheters-a prospective, randomized, active-controlled study. Int J Infect Dis. 2021;102:220-225. PubMed
17.Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377-384. PubMed
18.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-e34. PubMed
19.Fabiani A, Eletto V, Dreas L, Beltrame D, Sanson G. Midline or long peripheral catheters in difficult venous access conditions? A comparative study in patients with acute cardiovascular diseases. A J Infect Control. 2020;48(10):1158-1165. PubMed
20.van Loon FHJ, Korsten HHM, Dierick-van Daele ATM, Bouwman ARA. The impact of the catheter to vein ratio on peripheral intravenous cannulation success, a post-hoc analyses. PLoS One. 2021;16(5):e0252166. PubMed
Appendix 1: Selection of Included Studies
Appendix 2: Characteristics of Included Publications
Note that this appendix has not been copy-edited.
Table 2: Characteristics of Included Primary Clinical Study
Study citation, country, funding source | Study design | Population characteristics | Intervention and comparator(s) | Clinical outcomes, length of follow-up |
|---|---|---|---|---|
Fabiani et al. (2020)19 Italy Funding source: No specific grant support and the authors declared no related conflicts of interest. | A retrospective cohort study was conducted in a university hospital in Italy. | Consecutive adults with acute cardiovascular disease and DVA (i.e., a lack of readily visible or palpable veins when 3 or more cannulation attempts failed) were admitted to a hospital from January 2014 to April 2019.a Patients with immediate life-threatening conditions or need for central venous access were excluded. Sex: males: n = 99, 53.8% Age: median (IQR): 70 (63 to 77) years Number of patients: 184 (MCs: n = 80; 18-cm LPC: n = 48; 8- or 10-cm LPC: n = 56) Charlson comorbidity index: median (IQR): 3 (2 to 4) (median for MCs: 2; for the 2 LPC groups: 3). Vein-to-catheter ratio: median (IQR) for MCs: 32.5 (27.2 to 40.7); 8- or 10-cm LPC: 29.0 (21.9 to 36.0); 18-cm LPC: 29.6 (23.6 to 32.5). | Intervention: Polyurethane MCs (4 to 5 Fr, 55 cm single-lumen PICC were trimmed to a standard length of 20 cm) was placed when the expected venous access was needed over 10 days. Comparators: 2 lengths of polyethylene LPC: 18-cm (4 Fr) LPC and 8-cm (3 Fr) or 10-cm (4 Fr) LPC, chosen for patients who have an expected venous access need for 7 to 10 days. The intervention and comparators were managed by bedside nurses based on the same policies. | Outcomes:
Follow-up: NA |
DVA = difficult venous access; Fr = French; MCs = midline catheters; PICC = peripherally inserted central catheters; LPC = long peripheral catheters; NA = not applicable; NR = not reported.
aThe study documented the administration of 25 antibiotics. The same catheter was used to infuse up to 5 different antibiotics, with a median of 1.0 and an interquartile range of 0 to 2.
Appendix 3: Critical Appraisal of Included Publications
Note that this appendix has not been copy-edited.
Table 3: Strengths and Limitations of Clinical Study Using the Downs and Black Checklist17
Strengths | Limitations |
|---|---|
Fabiani et al. (2020)19 | |
The objectives of the study were clearly described. Inclusion and exclusion criteria were clearly described. The study conducted sample size calculations. The catheter-related complications measures were clearly described. The intervention and comparators were clearly described. The main findings of the study were clearly described. The adjusted HR with a corresponding 95% CI was calculated using the multivariable Cox regression model. The estimates of the variability (IQR or 95% CI) for the main outcomes were provided. The actual P values were reported. The study authors declared no related conflicts of interest. | The disease that requires IV antibiotics was unclear. The baseline characteristics of participants were not well balanced between the MCs and LPC groups; for example, patients receiving LPC had a higher median Charlson index than the MCs group, while the MCs group had a higher vein-to-catheter ratio than the LPC group. In the Cox regression models, details of the stepwise methods were not clearly reported, including p values used for entering and removing from the model and selection of candidate variables for the multivariable Cox regression model. The medians for the indwelling time were presented in Fabiani et al., but the actual values were not provided. |
CI = confidence interval; HR = hazard ratio; IQR = interquartile range; LPC = long peripheral catheters; MCs = Midline catheters
Appendix 4: Main Study Findings
Note that this appendix has not been copy-edited.
Table 4: Summary of Findings by Outcome — Uncomplicated Indwelling Time
Study | Groups | Number of patients | Median (days) | IQR (days) | Maximum (days) | Note |
|---|---|---|---|---|---|---|
Fabiani et al. (2020)19 Retrospective cohort study | 8- or 10-cm LPC | 56 | NR | NR | 54 | According to Fabiani et al., the median indwelling time for MCs was significantly longer than LPC (P < 0.001). |
18-cm LPC | 48 | NR | NR | 48 | ||
MCs | 80 | NR | NR | 153 | ||
Total | 184 | 14 | 7 to 25 | NR |
IQR = interquartile range; LPC = long peripheral catheters; MCs = Midline catheters; NR = not reported
Table 5: Summary of Findings by Outcome — Catheter-Related Complications
Study | Groups | Number of patients | Number of events (%) | Incidence (cases per 1000 catheter days) | HR (95% CI) | P-value | Note |
|---|---|---|---|---|---|---|---|
Fabiani et al. (2020)19 Retrospective cohort study | 8- or 10-cm LPC | 56 | 10 (17.9%) | 15.84 | 5.328 (2.118 to 13.404) | < 0.001 | Other variables in the final model that increased the risk of CRC include Ciprofloxacin, Levofloxacin, Rifampicin.a |
18-cm LPC | 48 | 8 (16.7%) | 10.64 | 2.489 (0.961 to 6.448) | 0.060 | ||
MCs | 80 | 13 (16.2%) | 6.27 | Reference (1) | NA | ||
Total | 184 | 31 (16.8%) | NR | NA | NA |
CI = confidence interval; CRC = catheter-related complications; HR = hazards ratio; LPC = long peripheral catheters; MCs = Midline catheters; NA = not applicable; NR = not reported.
aAge, Charlson index, heparin, ceftriaxone, number of different antibiotics infused, vein-to-catheter ratio were excluded from the final model.
Table 6: Summary of Findings by Outcome — Catheter-Related Thrombosis
Study | Groups | Number of patients | Number of events (%) | Note |
|---|---|---|---|---|
Fabiani et al. (2020)19 Retrospective cohort study | 8- or 10-cm LPC | 56 | 1 (1.8%) | The statistical test results (p-values) were not available. |
18-cm LPC | 48 | 1 (2.1%) | ||
MCs | 80 | 4 (5.0%) | ||
Total | 184 | 6 (3.3%) |
LPC = long peripheral catheters; MCs = Midline catheters
Table 7: Summary of Findings by Outcome — Catheter-Related Bloodstream Infections
Study | Groups | Number of patients | Number of events (%) | Incidence (cases per 1000 catheter days) | Note |
|---|---|---|---|---|---|
Fabiani et al. (2020)19 Retrospective cohort study | 8- or 10-cm LPC | 56 | 0 (0%) | 0 | The incidence of the 2 LPC lengths (8- or 10 cm and 18 cm) was 0.72 per 1000 catheter days. The statistical test results (p-values) were not available. |
18-cm LPC | 48 | 1 (2.1%) | 1.32 | ||
MCs | 80 | 1 (1.3%) | 0.48 | ||
Total | 184 | 2 (1.1%) | NR |
LPC = long peripheral catheters; MCs = Midline catheters; NR = not reported
Table 8: Summary of Findings by Outcome — Drug Leakage From the Exit Site
Study | Groups | Number of patients | Number of events (%) | Note |
|---|---|---|---|---|
Fabiani et al. (2020)19 Retrospective cohort study | 8- or 10-cm LPC | 56 | 6 (10.7%) | The statistical test results (p-value) were not available. |
18-cm LPC | 48 | 2 (4.2%) | ||
MCs | 80 | 3 (3.8%) | ||
Total | 184 | 11 (6.0%) |
LPC = long peripheral catheters; MCs = Midline catheters; NR = not reported
aThe denominator was the number of participants with any complications in the group.
Table 9: Summary of Findings by Outcome — Complete Catheter Occlusion
Study | Groups | Number of patients | Number of events (%) | Note |
|---|---|---|---|---|
Fabiani et al. (2020)19 Retrospective cohort study | 8- or 10-cm LPC | 56 | 3 (5.4%) | The statistical test results (p-value) were not available. |
18-cm LPC | 48 | 2 (4.2%) | ||
MCs | 80 | 3 (3.8%) | ||
Total | 184 | 8 (4.3%) |
LPC = long peripheral catheters; MCs = Midline catheters; NR = not reported
Table 10: Summary of Findings by Outcome — Catheter Fissuring
Study | Groups | Number of patients | Number of events (%) | Note |
|---|---|---|---|---|
Fabiani et al. (2020)19 Retrospective cohort study | 8- or 10-cm LPC | 56 | 0 (0%) | The statistical test results (p-value) were not available. |
18-cm LPC | 48 | 2 (4.2%) | ||
MCs | 80 | 2 (2.5%) | ||
Total | 184 | 4 (2.2%) |
LPC = long peripheral catheters; MCs = Midline catheters; NR = not reported
aThe denominator was the number of participants with any complications in the group.
Appendix 5: References of Potential Interest
Note that this appendix has not been copy-edited.
Extended Dwell Catheters Versus Standard Peripheral Catheters in Patients in the ED
Fung CM, Stayer DR, Terrasi JJ, et al. Extended dwell and standard ultrasound guided peripheral intravenous catheters: Comparison of durability and reliability. American Journal of Emergency Medicine. 2021;47:267-273. PubMed
Bahl A, Hang B, Brackney A, et al. Standard long IV catheters versus extended dwell catheters: A randomized comparison of ultrasound-guided catheter survival. American Journal of Emergency Medicine. 2019;37(4):715-721. PubMed
Midline Catheters Versus Other Peripheral or Central Catheters (e.g., Standard Long Peripheral Intravenous Catheters and PICCs)
Nielsen EB, Antonsen L, Mensel C, et al. The efficacy of midline catheters-a prospective, randomized, active-controlled study. International Journal of Infectious Diseases. 2021;102:220-225. PubMed
Villalba-Nicolau M, Chover-Sierra E, Saus-Ortega C, Ballestar-Tarin ML, Chover-Sierra P, Martinez-Sabater A. Usefulness of Midline Catheters versus Peripheral Venous Catheters in an Inpatient Unit: A Pilot Randomized Clinical Trial. Nursing Reports. 2022;12(4):814-823. PubMed
Marsh N, Larsen EN, O'Brien C, et al. Safety and efficacy of midline catheters versus peripheral intravenous catheters: A pilot randomized controlled trial. International Journal of Nursing Practice. 2023;29(2):e13110. PubMed
Extended Dwell Catheters — Noncomparative Studies
Badger J. Long peripheral catheters for deep arm vein venous access: A systematic review of complications. Heart and Lung. 2019;48(3):222-225. PubMed
Patel SA, Araujo T, Rodriguez LP, Sanchez CR, Snyder A, Chopra V. Long peripheral catheters: A retrospective review of major complications. Journal of Hospital Medicine. 2019;14(12):758-760. PubMed
Campagna S, Gonella S, Zerla PA, et al. The Risk of Adverse Events Related to Extended-Dwell Peripheral Intravenous Access. Infection Control and Hospital Epidemiology. 2018;39(7):875-877. PubMed
Midline Catheters — Noncomparative Studies
Tripathi S, Kumar S, Kaushik S. The Practice and Complications of Midline Catheters: A Systematic Review. Critical Care Medicine. 2021;49(2):E140-E150. PubMed
Queixalos N, Boisson M, Papet T, Kerforne T, Dahyot-Fizelier C. Infectious complications of Midline catheters: an epidemiological study. Anaesthesia Critical Care and Pain Medicine. 2021;40(3):100887. PubMed
Tran AT, Rizk E, Aryal DK, Soto FJ, Swan JT. Incidence of Midline Catheter Complications among Hospitalized Patients. Journal of Infusion Nursing. 2023;46(1):28-35. PubMed
Johnson A, Gupta A, Feierabend T, Lopus T, Schildhouse R, Paje D. Midline catheters: A 3-year experience at a veterans administration medical center. American Journal of Infection Control. 2023;51(5):563-566. PubMed
Pathak R, Gangina S, Jairam F, Hinton K. A vascular access and midlines program can decrease hospital-acquired central line-associated bloodstream infections and cost to a community-based hospital. Therapeutics and Clinical Risk Management. 2018;14:1453-1456. PubMed
Comparing Different Midline Catheter Tip Positions
Fan X, Zhao L, Cai Z, Jiang F, Zhao R. Midline catheter tip position and catheter-related complications in antimicrobial therapy: A multi-center randomized controlled trial. International Journal of Nursing Studies. 2023;141:104476. PubMed
Guidelines and Recommendations – Irrelevant or Unclear Populations.
Pittiruti M, Van Boxtel T, Scoppettuolo G, et al. European recommendations on the proper indication and use of peripheral venous access devices (the ERPIUP consensus): A WoCoVA project. Journal of Vascular Access. 2023;24(1):165-182. PubMed
Spina R, Mussa B, Tollapi L, Conti F, Cortesi E, Verna R. Adoption and application in Italy of the principal guidelines and international recommendations on venous access. Minerva Medica. 2018;109(3):153-202. PubMed
Additional References
Editorial: Marsh N, Corley A, Schults JA, Vemuri K, Rickard CM. Midline catheters - A good alternative device? Anaesthesia Critical Care and Pain Medicine. 2021;40(3):100885.
Qin KR, Pittiruti M, Nataraja RM, Pacilli M. Long peripheral catheters and midline catheters: Insights from a survey of vascular access specialists. Journal of Vascular Access. 2021;22(6):905-910. PubMed
Contributors: Kendra Brett, Elizabeth Carson
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up to date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.
Questions or requests for information about this report can be directed to Requests@CADTH.ca